
Proceedings of a Workshop
INTRODUCTION1
Millions of Americans of all ages face the challenge of living with serious illnesses such as advanced cancer, heart, or lung disease. Many people with serious illness are increasingly cared for in community settings. While the number of community-based programs to provide care for those with serious illness has grown significantly, the quality of care provided is not consistent across geographic locations or care settings (Teno et al., 2017). Care for the serious illness population often features gaps in coordination across sites of care and poor patient and family perceptions as to the quality of care provided (Kelley and Bollens-Lund, 2018). In an effort to better understand and facilitate discussions about the challenges and opportunities related to identifying and implementing quality measures for accountability purposes in community-based serious illness care, the Roundtable on Quality Care for People with Serious Illness of the National Academies of Sciences, Engineering, and Medicine held a public workshop on April 17, 2018, in
___________________
1 The planning committee’s role was limited to planning the workshop, and the Proceedings of a Workshop was prepared by the workshop rapporteurs as a factual summary of what occurred at the workshop. Statements, recommendations, and opinions expressed are those of individual presenters and participants, and are not necessarily endorsed or verified by the National Academies of Sciences, Engineering, and Medicine, and they should not be construed as reflecting any group consensus.
Washington, DC. The workshop featured a broad range of experts and stakeholders including clinical care team members, researchers, policy analysts, patient advocates, representatives of federal agencies, as well as those involved in health care accreditation and the development of quality measures. Workshop presentations explored the current state of quality measurement for people with serious illness, their families, and caregivers, with the aim of identifying next steps toward effectively implementing measures to drive improvement in the quality of community-based care for those facing serious illness (see Box 1 for key definitions).
The roundtable serves to convene stakeholders from government, academia, industry, professional associations, nonprofit advocacy groups, and philanthropies. Inspired by and expanding on the work of the 2014 Institute of Medicine (IOM) consensus study report Dying in America: Improving Quality and Honoring Individual Preferences Near the End of Life (IOM, 2015a),2 the roundtable aims to foster ongoing dialogue about crucial policy and research issues to accelerate and sustain progress in care for people of all ages experiencing serious illness.
In his introductory remarks to the workshop, James Tulsky, chair of the department of psychosocial oncology and palliative care at the Dana-Farber Cancer Institute, thanked the Gordon and Betty Moore Foundation for supporting the workshop and other ongoing efforts to improve quality measurement.3 He pointed out that such work is essential to providing the best care to people with serious illness, reminding the workshop audience, “As we all know, if you do not measure it, you cannot improve it.” Tulsky went on to note the difficulty of measurement for the serious illness care population, but added that is why “it is important that we talk about and think deeply” about this topic.
Amy Melnick, executive director of the National Coalition for Hospice and Palliative Care, and the workshop planning committee co-chair, pointed out that the workshop aimed to further the discussion by explor-
___________________
2 As of March 2016, the Health and Medicine Division of the National Academies of Sciences, Engineering, and Medicine continues the consensus studies and convening activities previously carried out by the Institute of Medicine (IOM). The IOM name is used to refer to publications issued prior to July 2015.
3 In May 2017, the Gordon and Betty Moore Foundation convened a meeting of stakeholders and experts in serious illness care in Banff, Alberta, Canada, to identify a path forward for building an accountability system for high-quality, community-based serious illness care programs. The papers and discussions from that meeting were published in a special issue of the Journal of Palliative Medicine, Vol. 21, No. S2, March 2018.
ing the “real-world application of measurement that makes a difference.” In stressing the implementation of measures for accountability, Melnick noted that workshop speakers would address issues such the importance of capturing information in a non-burdensome way for clinicians and patients, as well as being cognizant of the unintended consequences that may arise from measures implementation. Melnick noted that ultimately the goal is to arrive at “that right set of feasible, valid, actionable, and meaningful quality measures.” She added that “the values and preferences of people with serious illness, their families, and their caregivers, has to drive the accountable measurement system we are seeking.” Amy Kelley, associate professor at Icahn School of Medicine at Mount Sinai, and the workshop planning committee co-chair, underscored the workshop’s focus on implementation of existing measures rather than measures development, though she acknowledged there is clearly more work to be done in that area. Kelley also pointed out that the goal of the workshop was to build on lessons learned and think about actionable next steps “rather than simply admiring the problem.”
Quality Measures for Accountability in Community-Based Serious Illness Care
The workshop aimed to contribute to ongoing efforts to implement meaningful measures for accountability purposes for people with serious illness cared for in community settings. Workshop presentations and discussions made clear that this is neither an easy nor straightforward process, as a number of speakers noted a broad range of issues and challenges to be addressed, not least of which is an absence of agreement as to what quality is and how to most effectively measure it. A number of workshop speakers referred to Donabedian’s framework, which identified structure, process, and outcomes as the essential foundation for evaluating the quality of health care (Ayanian and Markel, 2016; Donabedian, 1966).4 Several speakers noted that structure, process, and outcomes all have to be measured and the relationships between them understood in order to identify specific steps to improve quality. A number of workshop participants acknowledged important tensions and tradeoffs that need to be considered, and the importance of understanding the benefits and limitations of each type of measure.
___________________
4 Donabedian defined “structure” as the settings, qualifications of providers, and administrative systems through which care takes place; “process” as the components of care delivered; and “outcome” as recovery, restoration of function, and survival (Donabedian, 1966).
Several speakers also stressed that building measurement capacity among providers is critical to improving quality.
A number of workshop participants noted that the conceptual definition of serious illness, which is broader than palliative care or hospice alone, necessitates greater alignment across the entire health care system, public and private payers, and specialties. Patients with serious illness tend to have multiple chronic conditions and are seen in multiple settings by a diverse set of health care providers, yet the overarching goal is to improve care for patients in every care setting. Measures alignment presents its own set of challenges, however, as perceptions of quality measurement differ across specialties given variations in care settings and patient populations. Moreover, speakers noted the need to identify approaches to measure accurately function, frailty, and social risk among people with serious illness.
In considering measurement for accountability in the context of serious illness care, a number of speakers underscored the importance of measuring the patient experience and incorporating the values and preferences of the patient, family, and caregiver into patient care. As several of the workshop’s discussions and presentations highlighted, the system itself is often “deaf to the people that it cares for,” as characterized by workshop participant Amy Berman, senior program officer at The John A. Hartford Foundation. Progress toward accountability for quality may require new measurement paradigms that rely less on clinical guidelines and more on capturing the experience, goals, and quality of life of people with serious illness, as noted by Sean Morrison, chair of the department of geriatrics and palliative medicine at Mount Sinai. Current approaches to gathering information through electronic health records (EHRs), claims analyses, surveys, and accreditation protocols do not provide the critical data necessary to develop measures to enable the clinicians and the broader health care system truly to “hear” the needs, preferences, and values of seriously ill patients, their families, and caregivers.
Organization of Workshop and Proceedings
The workshop opened with an interview of the personal experiences of a patient and a family caregiver that highlighted the importance of listening to and truly hearing the expressed values and preferences of the patient, family, and caregiver, and ensuring that those values and preferences are incorporated into patient care. This opening session provided the real-world context for the importance of understanding what matters most to patients and their families.
Session One laid the foundation for the sessions that followed, with a discussion of the current state of quality measures for the care of people with serious illness, a conceptual definition of serious illness (see Box 1), and that the challenge of measuring function needs to be addressed in order to improve identification of the seriously ill population. Session speakers discussed the various types of measures and data sources, each of which presents its own opportunities and challenges. Speakers emphasized a focus on meaningful measures that drive real improvement and the need to consider alignment of measures across specialties and payers.
Session Two explored the implementation of quality measures from the perspective of health care providers and private-sector payers. The session highlighted the importance of engaging with clinicians and patients in the measurement process. Speakers addressed the challenges and opportunities of implementing quality measures in the health plan/health system context, including integration of quality measures into payment contracts and alignment of quality measures with broader organizational goals.
Shantanu Agrawal, chief executive officer and president of the National Quality Forum (NQF), provided the workshop’s keynote address. Agrawal described NQF’s process of reviewing and endorsing performance measures, which has undergone a significant redesign. Agrawal spoke about leveraging the existing evidence base for serious illness care, prioritizing measures according to how well they drive quality, and the importance of including patients and caregivers in the measure development process. Agrawal also highlighted the process of eliciting feedback on measures after they have been used by clinical teams.
Session Three complemented the earlier discussion about measures implementation in private-sector plans with an examination of implementing quality measures in public programs with examples and lessons learned from Medicare and Veterans Health Administration (VHA) programs. The session also included a view from Congress in terms of the policy opportunities to advance quality measures.
Session Four shifted the focus to a discussion of quality measures for accreditation and how accreditation might serve as a lever to support accountability for high-quality care for people with serious illness. Speakers addressed what shape a future accreditation system for community-based serious illness care might take, and the need to align data cross the various care settings that people with serious illness encounter.
Session Five provided a view into what elements are needed to create a culture of quality measurement and quality improvement among inter-
professional clinical care teams; how to use clinical registries to capture patient data in a non-burdensome way to improve quality; and the role of EHRs in quality improvement. The session also included a discussion of the quality measures implementation process, including the readiness for change, interprofessional team support, and the unintended consequences of measures implementation.
The workshop ended with the final session featuring experts in the field of serious illness care reflecting on the day and the lessons learned. They highlighted the major themes and notable messages they had heard from the workshop presentations and discussions.
Workshop speakers, panelists, and workshop participants presented a broad range of perspectives and insights. This proceedings describes the presentations and discussions that occurred throughout the day. Generally, each speaker’s presentation is reported in a section attributed to that individual, following the flow of the workshop described above. Headings of each section correspond to the focus of the specific workshop session. A summary of suggestions for potential actions from individual workshop participants is found in Box 2. The workshop Statement of Task can be found in Appendix A and the workshop agenda can be found in Appendix B. The workshop speakers’ presentations (as PDF and audio files) have been archived online.5
THE PATIENT–FAMILY PERSPECTIVE
Robert Bergamini, medical director for palliative care at Mercy Clinic Children’s Cancer and Hematology and chair-elect of the Supportive Care Coalition, opened the workshop with a session that focused on the patient–family perspective. Bergamini moderated the discussion with Martha Herrera, parent navigator at Children’s National Health System and caregiver for her 8-year-old daughter, who has pontine tegmental cap dysplasia (PTCD), a rare genetic developmental disorder,6 and Gwen Darien, executive vice president for patient advocacy at the National Patient Advocate Foundation and a three-time cancer survivor. When introducing
___________________
5 For additional information, see http://nationalacademies.org/hmd/Activities/HealthServices/QualityCareforSeriousIllnessRoundtable/2018-APR-17.aspx (accessed August 28, 2018).
6 For additional information, see https://rarediseases.info.nih.gov/diseases/10919/pontine-tegmental-cap-dysplasia (accessed May 14, 2018).
herself, Darien likened the patient and caregiver experience to jazz, where the musicians have both an individual and a group identity. When it comes to the patient and caregiver experience, she explained, much of that experience is universal and much is individual. She also noted that improving the
system of serious illness care will not occur without first understanding the individual’s experience.
For Herrera, the challenge of caring for her daughter, Angelica, began with the search for a proper diagnosis. When Angelica was about 3 months old, Herrera noticed that she was not responding to sounds. Her
pediatrician dismissed Herrera’s concerns as the ill-informed worries of a 19-year-old mother who was likely suffering from postpartum depression. A second pediatrician also attributed Herrera’s concerns to her young age, told her she was expecting too much from her daughter, and referred her to a mental health specialist. A third pediatrician blamed colic for her daughter’s difficulty sleeping and failure to engage. Angelica was nearly 7 months old when the fourth pediatrician Herrera saw referred her to Children’s National Health System for a hearing test, which revealed that her daughter was deaf. That diagnosis led to magnetic resonance imaging (MRI) to try to pinpoint the cause of her daughter’s hearing impairment. The MRI revealed a brain anomaly and a diagnosis of PTCD. At that point, Herrera’s daughter was nearly 3 years old. Herrera was presented with two options for dealing with her daughter’s deafness: cochlear implants or nothing. Herrera chose the implants, a decision she questions now knowing that learning sign language would have been a third option.
Herrera shared that, in her current role helping younger parents and non-English-speaking families navigate the health care system, she sees parents struggling to communicate with clinicians and clinicians failing to respect parents’ concerns. She finds this is particularly the case if the parents are young, lack formal education, or have difficulty with English. Herrera observes that parents become reluctant to bring their children to the doctor for fear of learning that something else is wrong with their child. This could be remedied, according to Herrera, if clinicians take the time to learn about the patients and their caregivers, find out what their lives are like outside of the clinic, and engage in what she termed “compassionate explaining.”
Bergamini remarked that Herrera’s story reminded him of what the person in charge of his residency once told him: his goal should be to do what a young parent can do intuitively, which is to know something is wrong with his or her child from 50 feet away. He added that spending the time to get to know a patient has become increasingly challenging given that clinicians within the predominantly fee-for-service reimbursement system are typically paid based on the number of patient encounters and procedures.
Darien observed that Herrera’s experience points to the need for trust to be mutual, with doctors trusting their patients as much as their patients trust them. She also noted that young adults often have the same discounting experience as young parents, recalling when she was diagnosed with non-Hodgkin’s lymphoma she was treated as if she was a hypochondriac because she was young and complaining about chest pain.
Darien spoke to the issue of survivorship and the failure of health systems to help with the transition from having cancer to being in remission. Treating, she said, is not the same as healing. “I have been treated extremely well by extremely competent, gifted physicians, but I have not been healed by those same physicians in the same way,” stated Darien. She added that a vital lesson for patients, caregivers, and providers is to understand that “healing has to be part of what we do with our communities, not just treating the disease.” Bergamini noted that this was a crucial point in terms of the care that individuals with serious illness receive. In his view, clinicians are accustomed to diagnosing and treating acute illness and getting through a specific episode of illness, but are not well versed in helping seriously ill patients with multiple issues transition from one “compartment” to another.
Darien also said she does not believe time is always the answer, just as money is not always the answer. She recounted how one of her oncologists rarely spent more than 10 or 15 minutes with her, but during that time, she truly listened to Darien. Bergamini pointed out that listening and understanding is not intuitive for many providers. Herrera noted that one advantage of her institution being a teaching hospital is that medical students and first-year residents are eager to learn about their patients’ conditions and concerns. Another benefit of working at Children’s, she said, is that she and her five navigator colleagues are consulted before a new program is implemented to provide a parent’s perspective on whether parents will engage with the program. “Starting the new initiative with the parent’s input really helps them get it right from the beginning” and to think about it being a patient-focused initiative, noted Herrera.
During the question-and-answer session following the presentations, Amy Berman, senior program officer at The John A. Hartford Foundation, asked Herrera and Darien if they could recommend a measure that would address the challenges they faced. Herrera replied that more measures around patient and caregiver goals would be useful, including ways to provide realistic timelines to families that would help them figure out how to balance caregiving with the rest of life’s demands, including caring for other children in the family.
Darien pointed out that the issue is not deciding on individual measures, but reframing the way measures reflect what is important to the patient and caregiver rather than what is important to the health care system. For Darien, many measures seem like what she called “hospitality measures,” with a focus on how good the hospital food is, rather than on whether the food is helping with the healing process, or how the furniture
looks, rather than how comfortable it is for patients and their long-term guests. “Quality measures have to be meaningful to patients and to patients’ outcomes and quality of life rather than meaningful to payment models and to checking the box,” emphasized Darien.
Lauren Cates, board chair and executive director of Healwell, as well as immediate past president and founding director of the board of the Society for Oncology Massage, said her organization talks with health care professionals about how being honest about their own mortality affects the care they provide and the importance of speaking honestly to patients when delivering a diagnosis. Both Herrera and Darien agreed that facing one’s mortality is very difficult and that it can be confusing to many patients when providers use percentages of possible survival while delivering a prognosis. Bergamini offered the question he hates the most as an oncologist is when parents want to know the chances of their child being cured. “One of the most difficult things to learn is how to discuss prognosis,” said Bergamini. “People will remember those words forever.” Bergamini closed the session, noting it set “a great tone for the day as we try to get away from the checkboxes and get to what matters to patients and families.”
GAPS, CHALLENGES, AND OPPORTUNITIES IN IMPLEMENTING QUALITY MEASURES FOR ACCOUNTABILITY
In her introduction to the first panel session, Amy Kelley, associate professor at the Icahn School of Medicine at Mount Sinai, pointed out that the focus of the workshop’s discussions is on implementing measures that exist today and not on developing new measures, though she acknowledged that work remains to be done in that area. She then offered a conceptual definition that holds serious illness to be a health condition that carries a high risk of mortality, though not bound by prognosis, and either negatively affects a person’s daily function or quality of life or excessively strains their caregivers (Kelley and Bollens-Lund, 2018). Kelley noted that the experiences shared by Herrera and Darien are “emblematic of why that conceptual definition stands as it is.”
Measuring High-Quality Care
Laura Hanson, professor of Geriatrics and Palliative Medicine at the University of North Carolina at Chapel Hill (UNC), director of the UNC
Palliative Care Program, and co-lead of the Measures Core for the Palliative Care Research Cooperative, defined high-quality care as the structural elements of the health care system and the processes that clinicians implement that increase the likelihood of the desired health outcomes and are consistent with current professional knowledge (IOM, 1999). “That attachment between structure, process, and outcome7 is part of how we think about measuring or capturing health care quality,” said Hanson.
The data to drive measures of high-quality care come from many sources, including claims data, clinician reports embedded in the EHR, and patient or caregiver surveys. Hanson emphasized that all three sources of data are important because together they provide a way to triangulate quality of care, and the different measures enable us to “learn different angles of the truth.” Hanson pointed out that a fundamental measurement challenge involves determining the denominator population for serious illness. Referring back to the opening session, Hanson noted that “the reality of the patient and caregiver story is that people with serious illness are everywhere in the U.S. health care system. They are found in multiple settings and are being cared for by a diverse set of health care providers.” She noted that it is hard to account for all of those who are experiencing serious illness, and yet the goal is to improve care for all of them in every setting. Those individuals who are in specialty palliative care and hospice provide some information, but that denominator has a downside because it only captures those people who have gained access to those parts of the health care system.
In order for measures to drive effective quality improvement, Hanson explained, they need to meet certain requirements (see Box 3). First, measures need to be important and relevant, and for something that is important to patients and caregivers, account for a large population, and thus have public health impact. Second, measures need to be scientifically acceptable, backed by evidence linking the structure and process measures to actual outcomes, and have strong operational definitions. Measures need to be reproducible so that those doing the measurement are capturing information in the same way. Third, measures need to be feasible, which means the data can be captured during the clinical care process, with an acceptable cost
___________________
7 Structure measures, for example, include staffing ratios, certification, and use of EHR; process measures include symptoms, preventive services and support, and outcome measures include mortality rates, surgical complications, access, and experience of care. For additional information, see https://www.ahrq.gov/professionals/quality-patient-safety/talkingquality/create/types.html (accessed July 29, 2018).
and burden to the health care system, clinical team, patients, and caregivers. Fourth, measures need to be usable and actionable today to address gaps in care quality. Finally, the measures themselves must be responsive: “If there is a difference in quality of care, the needle has to move,” Hanson explained.
Perhaps surprisingly, Hanson remarked, nursing homes have proven to be good models for implementing measures that lead to improvements in care and can provide lessons for the serious illness population. For example, in an attempt to improve quality of care, the Centers for Medicare & Medicaid Services (CMS) established Nursing Home Compare, a combination of measurement sources including safety inspection results, a mandated minimum data set that uses EHR data, staffing reports, and claims data to produce a publicly available star rating8 for all Medicare and Medicaid
___________________
8 For additional information, see https://www.medicare.gov/nursinghomecompare/Data/About.html#technicalDetails (accessed May 14, 2018).
certified nursing homes. While this set of measures may not be perfect, said Hanson, it is robust because of the diverse sources of data. More importantly, as Hanson pointed out, these measures have helped drive improvements in care because they led to public reporting and feedback, helped national- and state-level partnerships and coalitions target areas where caps in quality existed, prompted efforts to improve clinician training and engagement, and triggered support for quality improvement effects. In addition, surveyor training and guidance created an environment in which the regulatory arm has become part of the measurement and improvement process.
In closing, Hanson shared her key takeaway points. Focusing on implementing and using a small number of feasible measures, as well as building measurement capacity among providers, is critical to improving quality, she posited. Another key point Hanson identified is to combine structure, process, and outcome measures from multiple sources—not only the EHR or surveys—to get a comprehensive view of the quality of care. Hanson ended her remarks by emphasizing the importance of learning from existing quality initiatives involving serious illness populations, such as Nursing Home Compare; the Consumer Assessment of Healthcare Providers and Systems (CAHPS),9 which is providing lessons on how to expand across settings; and the Hospice Item Set,10 which has measures that are applicable directly to serious illness care. Hanson pointed to the most important lesson as the need to “keep our eyes on the prize.” The prize, she emphasized, is improved care and “not perfect measurement.”
Challenges in Implementing Quality Measures for Serious Illness Care
For Joan Teno, professor of medicine at Oregon Health & Science University, there are several challenges to implementing quality measures for serious illness care. First, an overemphasis on process measures has led to a lack of accountability and a “check the box” mentality that does not embrace the complexity of caring for patients with serious illness. A second key challenge that Teno identified is understanding who is in the denominator population. Third, too often, said Teno, what is easily counted becomes
___________________
9 For additional information, see https://www.ahrq.gov/cahps/index.html (accessed July 29, 2018).
10 For additional information, see https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Hospice-Quality-Reporting/Hospice-Item-Set-HIS.html (accessed July 29, 2018).
what is measured even if that measure paints an incomplete picture of the care being delivered and can even harm patients. For Teno, the “Holy Grail is goal-concordant care.”
While acknowledging that the Medicare hospice benefit has transformed care for a subset of individuals with serious illness, Teno said it does not fit the trajectory of diseases today. Lung cancer, for example, is now becoming a chronic disease and people are living with the disease for many years, she explained, yet the payment system does not reflect this new disease trajectory. One key step going forward, she suggested, is to “celebrate” the Medicare hospice benefit, but learn from its shortcomings and embrace quality from the very beginning. Another important lesson for Teno is the importance of having a balanced set of measures that embraces the complexity of serious illness. She added a final lesson learned from the Medicare hospice benefit: one size does not fit all. “We really need to have payment systems that reflect who the patient is,” Teno explained. “What is easily counted is not necessarily what you measure.” As an example, she recalled one health system that measures the number of physician’s orders for life-sustaining treatment (POLST) forms that are completed, even though a small study had shown that while nearly all have a POLST form, only a few nursing home residents remembered talking about the form. “You may complete the POLST form, but if you do not have that conversation, you are going to harm patients,” warned Teno. She gave the example of POLST forms that had been filled out and indicated aggressive care, but only a few patients had remembered filling them out—meaning that those forms had the potential to be incorrect or misunderstood. She noted that does not mean one should stop measuring things or trying to improve care; “it means we need to get it right.”
Another difficult problem for developing measures for accountability, Teno said, is that the sample size must be sufficient. “This is all about reliability,” she emphasized. She noted that only about 70 percent of hospices conduct a sufficient number of interviews to report on the quality of care they deliver.11
In conclusion, Teno said there is an urgent need to develop new accountability measures that can populate a balanced set of measures that are actionable and embrace complexity. Also needed is a policy solution for the “small N problem” and careful thought to measurement of goal concordance of care while avoiding unintended consequences from those
___________________
11 Information was under review/unpublished at time of this proceedings’ publication.
measures. As a final thought, Teno commented that if value is based on a preference-weighted combination of quality and outcomes without quality measures, value will end up being based solely on cost.
Helen Burstin, executive vice president and chief executive officer of the Council of Medical Specialty Societies, discussed several other measurement challenges. Burstin emphasized the importance of removing measures that do not add value and do not drive meaningful improvement, creating greater alignment from various stakeholders in focusing on the entire population of those with serious illness and not only those in palliative care or hospice. She further emphasized shifting to better data sources, including clinical registries, to drive outcomes and, perhaps more importantly, patient-reported outcomes. She warned against using measures for accountability that serve no other role. “We need to find a subset of measures that can be used for accountability but also for improvement,” said Burstin. Supporting points made by previous speakers, Burstin emphasized that measures need to be outcome-oriented, actionable, and meaningful to family and caregivers. Measures need to support an integrated, systematic view of care that reflects the experience of patients with serious illness over the course of the trajectory of their illness. In addition, measures need to reflect how patients interact with the dozens of medical specialties that can play a role in the care of patients with serious illness.
Burstin observed there has been a lack of feedback from either those being measured or those who are using the measures regarding which measures are effective and which should be eliminated. Moreover, many measures are used because they can be measured, not because they are appropriate or actionable, and that needs to stop, said Burstin. In her view, “It is okay to stop measuring something if it is not helping just because it fits a box on your chart of what we feel like we need to measure.”
Burstin emphasized the need to align measures across medical specialties, across public and private payers, and across levels of measurement. “We want to be able to think about how our state or federally reported measures relate to what we are increasingly measuring at the plan and system level and then how that ultimately comes down to the clinician level as well as the individual patient level across the trajectory,” Burstin explained. “It is hard to imagine what your improvement strategy is when you are pinging from level to level and measures that are not aligned.”
Burstin called for a shift to sources that are more reliable and valid for what is being measured. For example, claims data can capture usage, but not many of the other domains that are important, such as medical and social
complexity or frailty. Her hope is that the measurement field can work with medical specialty societies and others who are building clinical registries to capture the important data that will be included in those registries and that are not available in a preexisting data set. Those data will help to inform measures of patient-focused outcomes that are so important for the population of individuals with serious illness.
Returning to the conceptual definition she provided at the start of the session, Kelley reminded the workshop attendees that there are many challenges to operationalize that conceptual framework. The first challenge is that, while it is relatively easy to measure costs, utilization, mortality, and other quantifiable attributes and create regression models that predict those things, it is harder to measure need, which is fundamental to the conceptual definition. At the same time, rolling out services or demanding accountability requires being able to find the people for whom those services are going to make a difference, that is, those with high needs.
Kelley identified the tradeoff between sensitivity and specificity,12 which has implications for feasibility and cost-neutrality if used for eligibility. It is important, asserted Kelley, to understand whom a measure is missing and whom it is catching, strike a balance between the two depending the purpose of the measure, and understand the unintended consequences of getting that balance wrong. A third challenge relates to the inadequacy of the data currently available. Kelley identified the missing components as measures of function, cognition, and care needs, which are fundamental to identifying the seriously ill population. In her view, achievable approaches for improving the lack of data are within reach. The final challenge Kelley identified is that there are likely to be multiple denominators for various purposes and populations. She gave the example of seriously ill patients, such as those with heart failure, who are seeing a large number of specialists, but have not enrolled in a hospice program. Kelley underscored the need to identify the population of patients with serious illness with the data that is available before starting to look for patient-reported measures and other data sources.
___________________
12 Sensitivity refers to the proportion of people with disease who test positive (also known as true positive rate, the sensitivity of a clinical test refers to the ability of the test to correctly identify those patients with the disease). Specificity is the proportion of people without disease who test negative (also known as true negative rate, specificity of a clinical test refers to the ability of the test to correctly identify those patients without the disease).
SOURCES: As presented by Amy Kelley, April 17, 2018; Kelley et al., 2017.
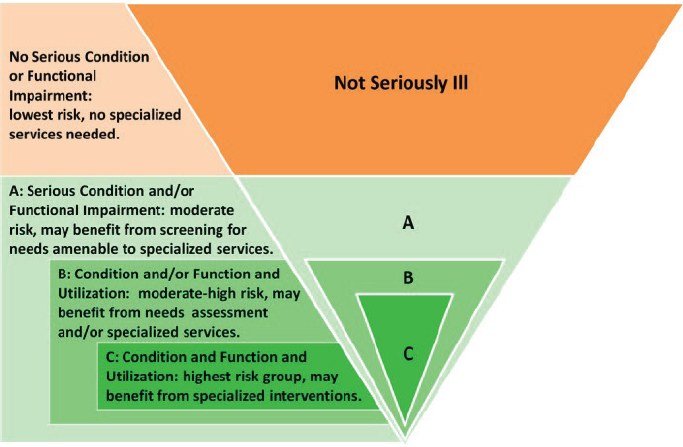
To address these challenges, Kelley and her research team have developed a nested population model of serious illness (see Figure 1) using a combination of diagnoses, self-reported functional measures, and utilization data (Kelley et al., 2017). “Depending on one’s purpose, you might want to choose a more narrow, smaller population, but for a different purpose, you might cast the net more broadly and get a bigger population,” she explained. In another study, she and her team attempted to identify suitable patient populations using simulations based on claims, self-reports, and various qualifiers (see Figure 2). This approach showed there are tradeoffs in how patients and their needs are identified and that there are many gaps. She noted that “this is a population of people of whom maybe 20 to 30 percent die within the coming year, yet the next column shows indicators of their needs—they are functionally impaired and have uncontrolled pain, and their caregivers are strained” (Kelley and Bollens-Lund, 2018).
In closing, Kelley noted that regarding the denominator, the existing data are poor in terms of care needs and severity of illness, and that approaches based solely on diagnosis, cost, and utilization will miss many individuals with significant need. “Function has to be added to improve our identification,” she said. Addressing sensitivity and specificity, Kelley
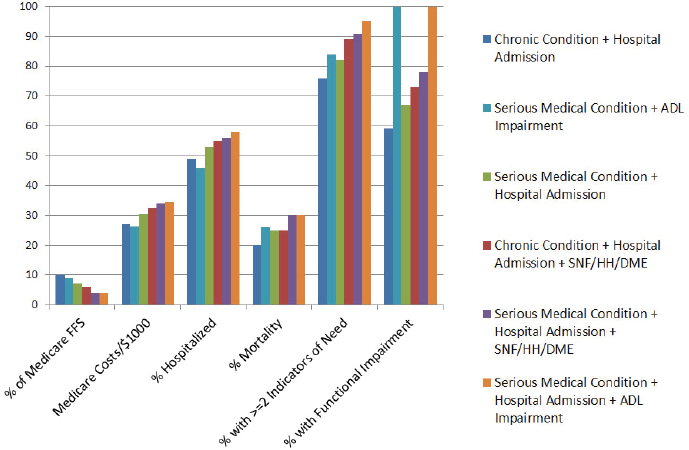
NOTES: Y-axis illustrates percentage of population listed on x-axis; to define serious illness and aid in systematic evaluation of serious illness populations, Kelley and Bollens-Lund start with data from the 2011 National Health and Aging Trends Study, which is then categorized based on diagnosis (using Dartmouth Atlas of Healthcare’s nine chronic conditions and a more complex approach from prior work to identify seriously ill), utilization (based on health care utilization in the past 6 months using acute care hospitalizations and home health and skilled nursing facility claims), and measures of need (identified through evaluation of alternative payment model proposals and expert panel consensus). ADL = activity of daily living; DME = durable medical equipment (e.g., hospital bed, wheelchair, or home oxygen); FFS = fee for service; HH = home health; SNF = skilled nursing facility.
SOURCES: As presented by Amy Kelley, April 17, 2018; Kelley and Bollens-Lund, 2018.
elaborated that in the context of purpose, multiple denominators are be needed because of the issue of unintended consequences.
Discussion
Responding to the presentations, Joanne Lynn, director of the Center for Elder Care and Advanced Illness at the Altarum Institute, proposed a different construct—one that focuses on accountability at the level of the community, rather that the provider organization or insurer. In this
construct, aspects such as the availability of housing, home-delivered food, transportation, and workforce all matter to those with serious illness. Lynn noted the possibility that measuring programs that enroll people might be making things worse for people who did not enroll in the program. For example, the existence of a palliative care or hospice program might worsen the experience of dementia patients living at home because providers might assume that these programs will take care of their patients and that they would not need to talk to families about the needs of their loved ones. Lynn stressed that she was not suggesting forgoing other approaches, but that in addition, the field needs to start developing measures that provide a picture of how communities are doing. In fact, observed Burstin, the Medicare Payment Advisory Commission (MedPAC) made that very recommendation to start looking more at the community level. The challenge, she asserted, is finding the data to use at that level, though she believes that measurement will ultimately occur at higher levels of aggregations such as at the community level. Hanson added that she wonders if better measures were available for identifying the serious illness population in the dimensions of function, cognition, and need that Kelley described, would the result be a variation on Lynn’s idea, though at the population rather than geographic level. Then, if an individual was in a particular population, the geography, payer, or clinical practice organization would be tracked by how well it serves that serious illness population. “Just being able to track that population, no matter where they are, could be as powerful as anything we talk about when we talk about what to measure,” said Hanson.
Concluding the session, Kelley made note of the Serious Illness Quality Alignment Hub,13 a 3-year effort by the Center to Advance Palliative Care and NQF to improve quality of care for people with serious illness by integrating measures, standards, and best practices into existing systems. The idea driving the Hub, she explained, is to leverage the power of regulation and financing to create incentives for adherence to best practices. This initiative has four guiding principles: achieving the goal must be feasible within 3 years; the resulting system must have a large-scale impact on patients and families; the targets for action are at the practice level or higher, rather than
___________________
13 The Serious Illness Quality Alignment Hub is funded by the Gordon and Betty Moore Foundation. For additional information, see https://www.capc.org/about/press-media/press-releases/2017-11-16/Center-to-Advance-Palliative-Care-Launches-the-Serious-Illness-Quality-Alignment-Hub (accessed August 2, 2018). Also see https://www.capc.org/payers-policymakers/quality-alignment-hub (accessed July 29, 2018).
at the clinician level; and the system must be relevant, but not limited, to use in community settings. The Hub’s three key functions will be to coordinate existing projects, identify new opportunities to pursue, and vet next steps with assembled experts and partners.
INNOVATIVE APPROACHES TO IMPLEMENTING QUALITY MEASURES FROM THE PERSPECTIVES OF HEALTH CARE PROVIDERS AND PAYERS
From the perspective of those who function at the front lines of care, whether they are providers or patients, people often seem to be talking past one another when conversation turns to measures and how best to use them, said Richard Baron, president and chief executive officer of the American Board of Internal Medicine. Baron began his remarks with several key messages. First, he noted that today’s health care environment for providers is challenging and complicated, and results in providers feeling overstressed and overburdened. Baron explained that providers feel that “measures are done to them rather than with them.” He recalled that when his practice adopted an EHR in 2004, it was one of the most “catastrophically difficult” things he and his colleagues had ever done and nearly led to the dissolution of the practice. He explained that, thankfully, that experience took place before the advent of meaningful use, so his practice was able to adopt the EHR to solve problems he and his colleagues thought they had, as opposed to problems other people thought they had and wanted to solve. In fact, part of what is driving the national rebellion that clinicians are having against boards and certification programs is their opposition to the requirement that practitioners demonstrate competence in systematic measurement and improvement in patient care to maintain certification, according to Baron. He argued that the more conversations about quality that can connect to why providers work in the health care profession, which is to provide excellent care to patients, the more successful those conversations will be.
In contrast to the requirement, which is known as Part 4 of the Maintenance of Certification14 requirements administered by specialty boards, the Choosing Wisely® initiative15 seeks to advance a national dialogue on avoiding unnecessary medical tests, treatments, and procedures by promot-
___________________
14 For additional information, see https://www.abp.org/content/improving-professional-practice-part-4 (accessed June 8, 2018).
15 For additional information, see http://www.choosingwisely.org (accessed May 15, 2018).
ing conversations between patients and clinicians. Though this program has been criticized for not having much of an effect on reducing usage, waste, and cost, Baron said it has been effective.
Baron also stressed the importance of engaging patients when implementing measures and thinking about measures that would make the patient’s experience better. Doing so would create common ground with providers because that is the reason why clinicians go to work in the first place, he said. The more the conversations about quality focus on topics that matter to patients, the more legitimacy it creates for measurement work. “If you do not think this work needs legitimacy, you are not paying attention,” said Baron. “The whole problem is that people are challenging whether this adds any value, whether it really does anything, whether it is all box-checking exercises. It is desperately in need of anchoring in the legitimacy and the coherence of clinical purpose and engaging patients in what matters to them and how providers can provide that,” noted Baron.
Baron emphasized that it is better to focus on structure than process or outcome. While outcomes are what everyone cares about, they are the product of complex interactions among individuals, teams, technology, systems, the way care is organized and funded, and many other factors. Taking that approach, he said, is more likely to lead to measures that matter and more likely to engage providers.
Lessons from Blue Shield of California’s Palliative Care Program
In 2015, California passed a law, SB-1004, requiring all Medicaid managed plans in the state to provide access to community-based palliative care.16 At the time of the workshop, Blue Shield of California was 4 months into implementing its program, explained Torrie Fields, the organization’s senior program manager for advanced illness and palliative care. One of the first lessons she and her colleagues have learned over the course of the past several years is that many primary care providers and specialists are not necessarily familiar with what palliative care entails. They are often reluctant to refer patients and families to palliative care, and when they do, they are actually referring a patient to hospice and do not want to call it hospice.
The confusion, stated Fields, stems from an adage in the palliative care community: when you have seen one palliative program, you have seen only
___________________
16 For additional information, see http://www.dhcs.ca.gov/provgovpart/Pages/Palliative-Care-and-SB-1004.aspx (accessed July 29, 2018).
one such program. The unique nature of each palliative program makes it difficult for providers to refer a patient to a program and trust what they will get from that program. “That is the first key takeaway,” said Fields. “We need to make sure that there is a structure in place, and structure matters in terms of what services you are delivering and what payment you are fixing to that.” She and her colleagues addressed this issue by training all Blue Shield of California’s complex case managers in serious illness communication skills, the operational structures they provide, and what is covered by alternative payments.
Blue Shield of California offers palliative care across the continuum of care, starting with advance care planning and at the time of diagnosis. It makes referrals to community-based palliative care providers in the outpatient and home settings, and it has worked with all its tertiary hospitals to develop inpatient palliative care programs, particularly when it has an established accountable care organizations arrangement. At the time of the workshop, Blue Shield of California had contracted with more than 30 home-based programs covering all the state’s counties, as well as with outpatient programs in every metropolitan service area and telemedicine-enabled programs in rural areas.
Fields noted that home-based palliative care is underdeveloped in both quality measurement and structure. She also pointed out that while the common perception of serious illness is that patients prefer to receive care and die at home, she clarified that what patients most likely want is to receive care and die at home with a certain level and expectation of care. Blue Shield of California started from that perspective to determine what that level of care should be, then how to pay for that level of care provided by an interdisciplinary team in a way that allows for flexibility, depending on a patient’s and family’s needs, she explained. Blue Shield of California only has access to administrative claims data, Fields noted, so it has to deal with two issues: the inability to identify patients proactively given that there is no measure of functional status in claims data, and the inability to collect data on social determinants of health.
The eligibility criteria for home-based palliative care that Blue Shield of California uses was developed in a state-wide consensus process by the California Advanced Illness Collaborative, a payer–provider collaborative, in partnership with the California Health Care Foundation and the Coalition for Compassionate Care of California. To be eligible, patients must:
- Be in remission, in recovery from serious illness, or in the late stage of illness;
- Have documented gaps in care, including a decline in health status and/or function;
- Use the hospital and/or emergency department to manage illness or late-stage disease;
- Not be enrolled in hospice; and
- Have an illness that is not psychiatric or related to substance use.
Diagnostic categories, said Fields, include but are not limited to cancer, organ failure, stroke, neurodegenerative disease, HIV/AIDS, dementia or Alzheimer’s disease, frailty or advanced age, and multiple comorbid conditions with exacerbated pain.
To standardize the palliative care clinical model, Blue Shield of California follows the National Consensus Project guidelines (NCPQPC, 2013). All interdisciplinary teams include a physician, nurse, social worker, home health aide, and chaplain, and they can include other members of the team covered by other Blue Shield of California benefits. The program requires that a nurse or social worker provide care coordination, depending on what is driving the underlying disease, and that the patient’s treating provider is seen as a core member of the team. “We do encourage our palliative care providers to integrate primary care providers or specialists into that conversation through medical team conferences or telehealth,” offered Fields. She explained that “the clinical model needs to be stabilized for there to be a clear expectation of what services are being provided to the patient across the state and so that we are able to create a standard financial model that would support home-based palliative care.”
Ultimately, said Fields, palliative care must be part of health care transformation. Given that, when palliative care is provided as part of an organization’s goals, structures need to be aligned so that it is not competing with other capitated payment and reimbursement structures or other programs. “What we are trying to do is make sure that we are simplifying the provision of care for people with serious illness rather than fragmenting it in a different way,” she expressed. “We already have siloed health care. We do not need to dissect it and re-silo health care.” Reaching that goal requires creating partnerships to educate Blue Shield of California’s case managers and clinicians and provide implementation support for palliative care delivery throughout the organization’s delivery system. A workforce shortage in palliative care, said Fields, has forced her organization to cross-train existing
staff. In rural areas, she and her team have worked with accountable care organizations to provide palliative care services via telemedicine.
Blue Shield of California’s focus in developing its palliative care program is on aligning incentives. All of its home-based programs, which are mostly coming out of home health agencies and hospices, are provided through a per-member, per-month case rate that covers all of the services an individual would need from the interdisciplinary team. The organization also helps coordinate services and benefits for those things that fall outside of the case rate. Fields explained that in its pilot studies, Blue Shield of California found that if it was not working to coordinate care and not providing timely access to opiates, durable medical equipment, or other supplies, patients will readmit to the hospital and likely die in the hospital during that readmission.
The pilot studies also found that copays and coinsurance were a major hindrance in the acceptance or continuing to accept palliative care. Fields noted that if measurement is going to include engagement rates, how long patients are engaged, or changes in usage, health plans would need to think about how to align processes and structures to support palliative care programs and the treatment teams that refer patients to these programs.
Blue Shield of California’s focus on quality relies on The Joint Commission’s advanced certification in in-patient palliative care, and starting in 2020, it will require all its home-based programs to have The Joint Commission certification in community-based palliative care. Fields said she would like to see the National Committee for Quality Assurance (NCQA) create a serious illness accreditation for health plans and accountable care organizations to improve the continuum of care. Fields added that Blue Shield of California has also collaborated with the Center to Advance Palliative Care to train its case managers in serious illness communication.
By establishing credentialing standards upfront, Blue Shield of California has reduced the burden on providers to report on additional measures. Fields and her colleagues have found that health plans in Colorado that are paying for palliative care under alternative reimbursement arrangements collect different measures from providers at varying times using different reporting guidelines. “What we need to do is be flexible in determining what actually is important to us and what we, as a health plan, can collect on our own rather than what our palliative care providers need to report on,” said Fields. Currently, Blue Shield of California only collects data on three items from its palliative care providers: patient and family satisfaction survey scores, advance
care planning, including documentation of a medical decision maker or medical surrogate, and documentation of treatment preferences.
In terms of opportunities and challenges, Fields noted Blue Shield of California is looking to achieve three goals: feasibility, scale, and replicability inside of Blue Shield of California as well as with other plans. There is a need, she said, for a model that standardizes payments and outcomes, and in that regard, she looks forward to the day when she can tier palliative care programs based on quality of care rather than just availability. She would also like to see measurements that account for resource need and availability. Other opportunities she suggested include aligning with other organizational value-based initiatives, reducing the reporting burden on providers and driving people toward national registries and national benchmarking, and thinking about how to help providers with the additional market demands that come with increasing their participation in palliative care programs.
Aspire Health’s Model of Home-Based Palliative Care
Aspire Health is a home-based palliative care program for patients who are not eligible for hospice, explained Katy Lanz, Aspire’s chief clinical officer. The organization operates on a co-management model in which its nurse practitioners develop working relationships with primary care physicians and specialists in the community, and it embeds social work and chaplaincy as part of the care team. Aspire Health provides 24/7 access to medical providers who will make urgent care house calls in response to patient needs, in addition to routine visits. What makes the program unusual, according to Lanz, is that it uses claims data and information gleaned through its relationships with primary care physicians and specialists to identify who will need palliative care as far upstream as possible.
Aspire Health has its own EHR designed for home-based palliative care. Lanz explained that because Aspire Health charges largely on a per-member, per-month basis, rather than on a fee-for-service model, it has been able to design its EHR for its particular needs and make changes quickly based on lessons learned. Aspire Health educates community-based generalists to serve as the lead palliative care physician in each of its markets. “Our population, because we are further upstream, is chronically comorbid and chronically seriously ill, so the providers need to have this ‘hybridness’ of good internal medicine, geriatrics, and family medicine with a little bit of ‘palliativist’ work,” Lanz clarified. Care teams do have palliative care specialists, but they also need team members with a myriad of skills to meet
patient needs, she added, which is why education plays such a significant role in the success of the program.
Educating generalists across fields has also allowed the program to scale using the same model across 67 markets in 26 states even though location has an impact on outcomes resulting from the unique nature of each community, which affects how quality measures are set. As an example, she suggested that hospice use might be lower in El Paso than in many of the communities it serves. At the same time, hospitalization use is also lower, and the reason for both is that the community takes care of its own in people’s homes.
Aspire identifies patients using a data-driven algorithm, along with physician and care manager referrals, explained Lanz. A nurse practitioner, who typically covers 65 patients, performs an initial home visit and needs assessment. Patients are also supported by social workers in the field, nurses, case managers, and chaplains via telephone, though she added that the program does work with community-based chaplains. Ongoing care includes monthly in-home visits by the nurse practitioners, with physician, nurse, social worker, and chaplain visits as necessary. Aspire Health also works closely with community-based home health care agencies, hospices, places of worship, and Meals on Wheels to provide additional support that families need for the program to be most effective.
The program’s patients have a mix of diagnoses with varied and largely unpredictable disease trajectories, said Lanz. The importance of this from a quality perspective, she expounded, is that patient goals change repeatedly over the course of the disease trajectory. “From a quality perspective, it is not just documenting what a patient’s goals of care are, but having a plan of action in place to meet the patient’s goals and needs,” she asserted.
Clinical outcomes, usage rates, and advance care planning have all improved, said Lanz, as have patient satisfaction scores. For the latter, Aspire asks three questions: How helpful has it been to have Aspire caring for you in the home? How helpful has Aspire been in helping you plan for the future? How helpful has Aspire been in managing your symptoms? Aspire also uses a variety of quality metrics that include both National Consensus Project and NQF metrics, as well as its own metrics on follow-up after hospitalization, medication reconciliation after hospitalization, and tracking hospital and emergency department readmissions. For each measure, Aspire considers the following:
- Will the answer to the question allow us to care for our patient differently?
- Will the answer truly impact outcomes of interest?
- If the question is needed, is there a way to pre-populate it?
- Is it a required piece of data, suggested, or optional?
- Do all patients need the question asked or only a subset?
- Could the question be asked in another way, by other team members?
Lanz identified her three issues of greatest concern. First, how can Aspire Health maintain a high-quality clinical workforce given its rapid growth over the past 5 years? Second, she struggles with measuring the quality of the serious illness conversations that team members have with patients. Third, given that national palliative care quality metrics focus on process—was a pain assessment completed, for example—versus outcomes, she wonders how to measure the true quality of care.
Lanz shared several lessons learned, including the importance of moving from collecting discrete data points to trended outcomes and shifting from using provider-focused metrics to team-focused metrics. From an operational perspective, Aspire is moving from providing palliative sub-specialty care to taking a population management approach to managing care for those with serious illness, and Lanz noted that they have much to learn from their population management colleagues about how they collect data over time, particularly in terms of geography and trends. Other changes she sees include using chronic care managers and accountable care managers instead of consultants and looking at whether patients are getting the care indicated in their advance directives rather than simply counting completion of advance directives.
As a final comment, Lanz noted that what providers such as herself want to know is why they are measuring certain things and how they compare to their peers. “Once I know why, I am actually really excited about collecting it. . . . If you give people information and tell them why you are collecting it and then give them a safe environment to benchmark them against their peers, it really does drive change,” concluded Lanz.
Anthem’s Perspective on Quality Measures
When considering quality measures and their uses, setting realistic goals is important, said Robert Krebbs, staff vice president for specialty pay-
ment models at Anthem. For the value-based program that he oversees, he stresses to his team that it not realistic to expect 100 percent as a goal for a measure. “Until measures get to the point where we actually have accounted for every possible contraindication or exclusion, we are not going to get to that point,” he hypothesized. The one exception, in his opinion, is setting a zero percent standard on early elective delivery for pregnant women prior to 39 weeks gestation, with the key word being elective.
Looking at measures with that mindset, said Krebbs, allows for a more relaxed view of quality measures because it eliminates the fear of having to be perfect. “It is really a message of: ‘we are using metrics not just to hold people accountable to performance,’” he explained. “It is also to identify and prioritize quality improvement opportunities.” Recognizing that measures are imperfect also puts the emphasis on the methodologies used with those measures, he added. In his opinion, scorecard measures associated with goals require the highest standards in terms of making the measure achievable in the way it is being used.
In his programs at Anthem, Krebbs described his increasing focus on more informational measures than scorecard measures. While looking at admission rates to hospice or time spent in chemotherapy before death may be a grey area in terms of what the admission rate should be and whether a health system can be accountable to that rate, it is valuable from an insight perspective, expounded Krebbs. “Providers in those arrangements where they are being held to an overall cost target of some sort are starved for that sort of information and looking for it at every chance they can get,” he said.
After learning the hard way that providers often believe that measures are something that is being done to them rather than with them, Anthem has embraced the idea of co-creation and having providers in the room to inform decisions on which measures to deploy. “We have seen a change in tone in our partnerships once we truly embraced that concept,” revealed Krebbs.
As an example of how Anthem decides to implement a measure in the palliative care space, Krebbs recounted the results of a survey his team conducted in late 2015 of the 800 hospitals in Anthem’s value-based payment program, which covers 75 percent of the company’s commercial admissions. Of the 220 hospitals that responded, only 49 percent said they offered a palliative care program. Of those that did have a program, 92 percent reported they used interdisciplinary teams to provide care, though only 70 percent had a policy defining how palliative care was structured and delivered in the facility. A closer look showed that fewer than 20 percent of the hospitals
would have met the standards of The Joint Commission’s advance palliative care certification. Partnering with Bon Secours Health System in Virginia, and Leanne Yanni, executive medical director of Comprehensive Care, as the clinical champion, the Anthem team worked to co-create a structural measure and developed a simple metric that rewarded hospitals with a bonus for either having advanced certification from The Joint Commission or an alternative path that satisfies four requirements. The first requirement was to have an interdisciplinary team that included a physician, registered nurse, nurse practitioner, social worker, and chaplain. Based on feedback from Bon Secours and other hospitals, Anthem included a provision for hospitals creating their program from scratch that allowed them to satisfy that requirement if their teams included at least two of those disciplines, with the expectation that the teams would grow over time.
The second requirement was to have a leadership-endorsed policy that outlines what palliative care means for the organization and how it will be used. The third requirement was to have an educational program for the clinical staff that outlines what the policy says and trains them on how palliative care can benefit them, when to ask for palliative care consults, and how to incorporate palliative care team members into the teams that care for their patients.
The fourth requirement was to have a process for screening patients at admission for a palliative care consult opportunity. In Krebbs’s experience, this requirement has been the most controversial, not among leadership, but among clinicians who may not be willing to engage in the process of assessing patients. Krebbs noted that although he did not yet have results of implementation—the program was first introduced in 2017—he expects that based on the questions he has received from participating facilities, improvements will be promising.
As a final note, Krebbs pointed out that while outcome measures are obviously important, they should not necessarily be the accountability measures in all cases. “Once you reach that point of being able to use an outcome measure for accountability, everyone should applaud themselves for being able to reach that point, but it is okay that it will take some time to get there. It is a journey, and having those structural, process, and outcomes measures together and working in aligned fashion could really help,” said Krebbs.
Discussion
Session moderator Zinnia Harrison, vice president of innovation and inclusion at the National Hospice and Palliative Care Organization, started off the discussion session with a question for the panelists. She wondered how long each of the speakers took to develop their serious illness programs. Krebbs responded that, in terms of Anthem’s integration of palliative care into its value-based programs, even though he does have to develop the measures and reimbursement structures, that is the easy part compared with actually establishing palliative care services. Based on what he knows now, he would “double down on that commitment to co-creation,” without which his efforts to develop measures would not have succeeded as they did. Referring to Baron’s earlier comment that providers feel that “measures are done to them rather than with them,” Krebbs emphasized that “we need to make sure we are not forcing quality measures on each other. It is something that has to be done in collaboration with all the stakeholders involved.” Fields responded that they had one “very forward-thinking, innovative leader at Blue Shield of California, who started to think about what measures matter, specifically starting with hospice measures and then looking upstream to palliative care.” She noted that was in 2011. Fields added that the organization learned over time that you “can create any measures you like, but if you don’t have patients to test them on, nothing happens.” She pointed out that the time it took to get the program up and running depended on not only the development and adoption of measures and contracts, but also on patient acceptance of receiving additional types of services.
Baron reminded the workshop participants that the quality measure movement began with insurance companies, not clinicians, because insurers had data from the Healthcare Effectiveness Data and Information Set they could use to calculate numerators and denominators. For clinicians, these data were useful for research, but not for clinical care. “It was a data manipulation exercise,” said Baron. “It was not a technique for answering a question about the quality of their work.” He argued that there needs to be an educational breakthrough to get clinicians to think about information technology as something that can help them answer questions that they care about in their practice. “If we do not use co-creation and other approaches to get there, we will miss an opportunity,” he urged.
MEASURE REVIEW AND ENDORSEMENT REDESIGN AT THE NATIONAL QUALITY FORUM
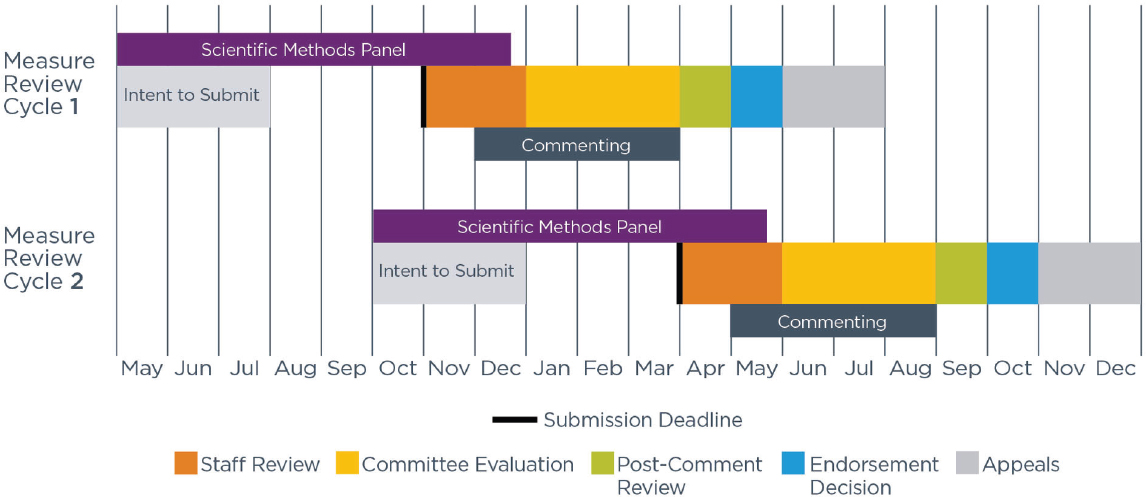
The process of reviewing and endorsing performance measures at NQF has undergone a significant redesign over the past year. NQF undertook this redesign in an effort to respond to stakeholder concerns about the length of time required to determine a measure’s appropriateness for endorsement, stated Shantanu Agrawal, NQF’s chief executive officer and president. Prior to the redesign, endorsement took an average of 20 months, which he acknowledged was too long to wait for health care quality measurement in general, and for serious illness care in particular. Agrawal explained that NQF has moved to a model where there are two endorsement cycles per year, each lasting approximately 7 months, with overlap between the two cycles (see Figure 3).
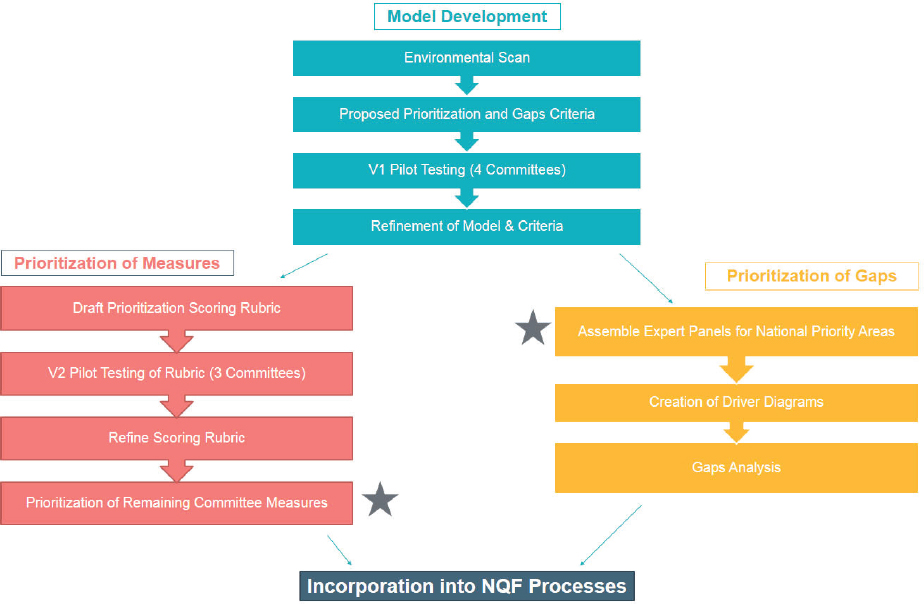
Agrawal explained that NQF is now addressing the proliferation of endorsed measures. Currently, there are more than 600 endorsed measures in NQF’s portfolio, and a key issue for NQR, according to Agrawal, is whether those are 600 high-value measures or whether there is a smaller number of high-value measures intermingled with a larger number of lower-value measures, measures that are “topped out,”17 and measures that are not helping providers and patients achieve desired outcomes. In order to address this issue, NQF has started a prioritization initiative, in which NQF and its endorsement committees have been tasked with reviewing the broad set of measures in their portfolios and consider which measures may better drive quality improvement (see Figure 4).
NQF’s goal is to complete this review by the end of 2018 and then engage in a policy discussion about what to do with low-priority or low-value measures. Given the effort that the developers have put into their measures, he expects these to be difficult, but necessary, conversations. He explained that having duplicate or low-value measures can create a situation where there is measure misalignment or burden from unnecessary measures across the health care system. He further noted that this review process is likely to identify critical gaps in NQF’s portfolio, such as in care coordination and even in well-established areas such as cardiovascular health.
___________________
17 A “topped out” measure is one for which overall performance is so high that meaningful distinctions and improvement in performance can no longer be made.
SOURCE: As presented by Shantanu Agrawal, April 17, 2018.
SOURCE: As presented by Shantanu Agrawal, April 17, 2018.
Identifying gaps, reported Agrawal, is proving to be harder than it sounds, noting, “If you have a clear and glaring measure gap, experts in the room are pretty good at identifying that.” Identifying a gap becomes much more difficult, he added, when there is insufficient evidence to understand what needs to be measured, and will consequently require a much longer-term conversation. These two efforts are occurring in parallel: filling important measurement gaps and prioritizing existing measures.
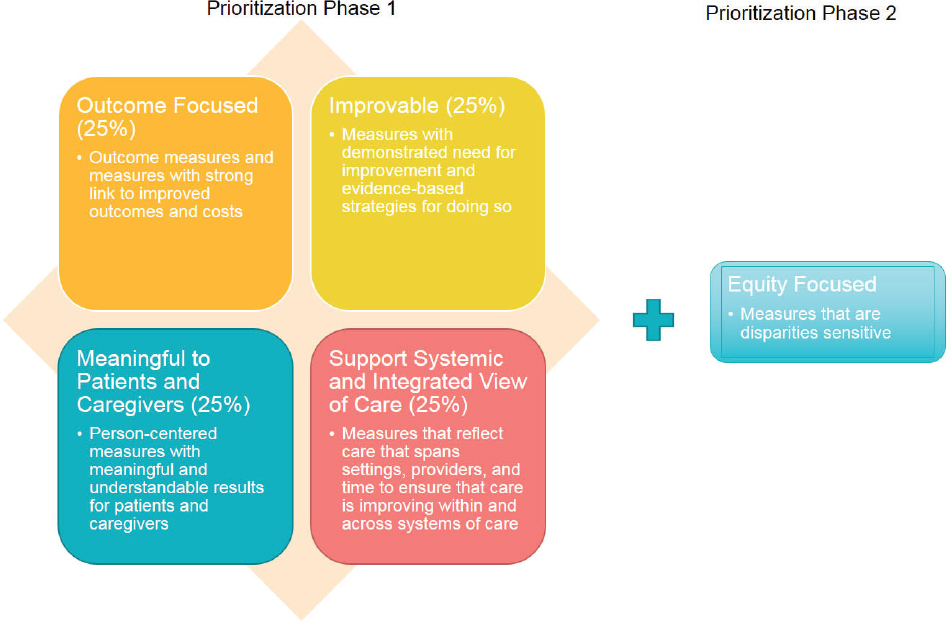
Agrawal described the methodology behind the prioritization process (see Figure 5). “We are trying to make the process as numerical as we can so that there is not a lot of subjective bias in what rises to the top as the most important measures,” he explained. Each measure is assessed based on whether it is outcome focused, improvable, meaningful to patients and caregivers, and supports a systemic and integrated view of care. Agrawal also noted that in future phases of the work, NQF “will be able to bring a focus on equity as one of the most important elements of prioritization.”
In Agrawal’s view, NQF’s role in measurement cannot end with the endorsement of a measure, which is why he also believes feedback is critical to the organization’s mission. “We need to have a better understanding of what the experience of measure implementation is and if there are any adverse consequences that are being produced,” he said. NQF is rolling out a system and process for getting feedback from as close to the frontlines as possible. One critical element of this system, he emphasized, will be for NQF to act as a consensus builder among stakeholder groups—the government, measure developers, and specialty societies—and produce a more granular understanding of where the burden of measurement lies and ways to generate solutions to measurement challenges.
Referring back to an earlier point, Agrawal wants NQF to help providers build capacity for measurement and quality improvement. He explained that although the general assumption might be that hospitals are inherently good at quality improvement, for example, his experience as an emergency medicine physician and health care consultant is that many institutions lack the core capabilities to engage in continuous improvement activities and understand the true purpose of measures. As an example, he recounted a recent experience when he was working a shift in the emergency department and was caring for a patient with decompensated heart failure who needed to be admitted to the hospital. He called the patient’s cardiologist, and after a heated debate about whether the patient needed to be admitted, the cardiologist revealed that he did not want to face the CMS penalty for readmissions. After Agrawal explained that he worked at CMS and that was
SOURCE: As presented by Shantanu Agrawal, April 17, 2018.
not the intention of the readmission penalties, the cardiologist relented, and the patient was admitted.
Agrawal subsequently learned that the cardiologist’s leadership had declared that emergency department staff had to reduce readmissions with no effort to identify the root causes of readmission nor any guidance on how to achieve that goal in a safe and effective manner. “It reinforced something that I had seen as a consultant with many of my clients, which is that quality improvement is sometimes not done in [an] as methodical and expert-driven way as we want, particularly in this important frontline setting,” concluded Agrawal.
Agrawal and his colleagues at NQF are asking how they can help build provider capabilities for quality improvement by connecting NQF’s measurement work to the frontlines and producing the change everyone wants to see. As a first step, NQF recently released a playbook on opioid stewardship and one on shared decision making in health care, and will release a playbook on antibiotic stewardship in the long-term care setting later in 2018.
Though NQF has a long history of working on health equity, the organization decided at the end of 2017 to take a more comprehensive approach to the subject to ensure that equity is a crosscutting issue in all of its major programs. Agrawal noted that while NQF must be thoughtful and careful about how it informs payment policies so as not to create potential conflicts with its measure endorsement role, he believes there is a role for NQF in bringing together the appropriate stakeholders to discuss how payment can be organized to empower communities and providers to address health inequity issues. “That is a convening and consensus role that I think we can adopt,” said Agrawal.
Agrawal discussed the NQF serious illness initiative, which was borne out of a collaboration with the Gordon and Betty Moore Foundation. The goals of this 3-year initiative are to align measures and incentives, to prepare and empower providers with more capabilities in care for people with serious illness, and to engage and activate stakeholders. The initiative will produce a playbook on serious illness using what he believes is a strong evidence base, particularly in terms of symptom reduction, improved patient satisfaction, and reductions of high-level use, such as emergency departments and hospitalizations.
Agrawal highlighted the importance of involving patients and caregivers in the measure development process and ensuring that this partnered approach continues throughout the measure testing and implementation
process. “Anything that developers can do to move that patient voice upstream and make sure they are involved in conceptualization through testing” yields useful input throughout the process, noted Agrawal.
Agrawal pointed out that, although there is a role for process and structures measures, NQF’s focus is to ensure that high-value outcome measures are getting through the endorsement process. In his opinion, NQF’s role as a convener is to point the way to what the right outcomes are for health systems. He observed that structural and process measures tend not to do well in the endorsement process, often because there is not the same evidence base as there is for outcomes. “We have tried to place the marker down on outcomes, realizing that there is a plethora of measurement underneath that helps to achieve that outcome,” explained Agrawal.
A further opportunity exists to create a plan around data needs and the infrastructure needed to get better and more extensive data. He pointed to the shortcomings of claims data, particularly concerning the large discordances among what happens in the clinical situation, the claim that is generated, and the reimbursement that occurs. At the same time, EHR data are not as clean as many believe, and registry data are often siloed in a variety of places. “I firmly believe we have to try to get to a future where we can leverage all of these data points to achieve what we want to in quality and to achieve what we want in measurement,” said Agrawal. However, he urged the community to start with claims data because they are widely available and provide the basis for so many critical health care decisions.
Regarding the denominator issue, Agrawal said he and his colleagues at NQF have had many conversations about the definition of serious illness care. “We have to be thoughtful about the populations we want to develop these measures for or engage in improvement work around,” said Agrawal. He argued for a practical approach of conducting pilot programs and working through the various populations of interest to get the desired high-value measures.
Responding to a comment from a workshop participant about the tension between quality improvement and accountability and the barrier built into publicly reported accountability measures, Agrawal noticed that quality measurement and improvement was a great exercise that health systems either took seriously or not very seriously until the accountability paradigm came along. “That notably changed the dialogue and put everybody on a similar page to try to improve quality,” he said. He acknowledged that while accountability is a “useful lever,” it is often the sole focus that distracts from day-to-day efforts to improve delivery systems. His hope is that focused
accountability and broader delivery system improvement work continue in tandem, and that the tension between the two will be resolved over time.
Berman remarked that individuals with serious illness report that maintaining independence is their number one priority, yet independence is not measured. She asked Agrawal if he had any suggestions on how to use claims data to look at independence. He replied that while claims data cannot produce all that is needed from measurement, he could imagine putting some information into claims data that might answer questions about independence, but he was not sure that would be the most useful approach. This is an example of an issue that highlights the limitation of claims data and argues for building alternative data sources that would be better suited to answering that type of question. In closing, Agrawal spoke to the reality of data asymmetry, as there are developers who do not have access to the right data even though those data exist. He noted the importance of addressing these issues: “Otherwise it will be more data in a black box and it will not be clear what it is measuring or how you are actually getting improvement from it.”
INNOVATIVE APPROACHES AND POLICY LEVERS FOR IMPLEMENTING QUALITY MEASURES FROM THE PERSPECTIVES OF PUBLIC PROGRAMS
In his introduction to the third panel session, moderator Eric Schneider, senior vice president for policy and research at The Commonwealth Fund, noted that the Fund is part of a six-foundation collaborative developing a playbook of evidence-based models of care for high-needs, high-cost patients.18 Referencing the government’s important role in paying for health care for those with serious illness, Schneider noted that the government also supports health care performance measurement and accountability, infrastructure, data assets, and standards.
Based on his three decades of experience as a researcher in measurement and accountability, Schneider observed care for the seriously ill is still operating with “version 1.0” of the performance measurement system because of the attempts to minimize the burden of measurement and use existing data. He characterized the current state of measurement as inadequate to the task
___________________
18 For additional information, see https://www.commonwealthfund.org/publications/journal-article/2016/jul/caring-high-need-high-cost-patients-urgent-priority (accessed July 29, 2018).
of improving care for those with serious illness. He believes, however, that the challenge of designing a measurement system for the seriously ill can be informed by three decades of experience.
Meaningful Measures Initiative at CMS
In 2017, CMS launched the Meaningful Measures Initiative19 in an effort to develop an innovative approach to meaningful outcomes. This initiative, explained Reena Duseja, director of the Division of Quality Measurement at CMS, has four key patient-centered aspects: empowering patients and doctors to make decisions about their health care; supporting innovative approaches to improving the quality, accessibility, and affordability with measurement; ushering in a new era of state flexibility and local leadership; and improving the experience for CMS beneficiaries and their caregivers. The initiative’s objective is to focus everyone’s efforts on the same quality areas that lend specificity, said Duseja. The initiative seeks to identify measures that:
- Address high-impact measure areas that safeguard public health;
- Are patient centered and meaningful to patients, clinicians, and providers;
- Are outcome based where possible to provide a target for improvement;
- Fulfill requirements in CMS programs’ statutes;
- Minimize the level of burden on providers;
- Identify significant opportunity for improvement;
- Address measure needs for population-based payment through alternative payment models; and
- Align across programs and/or with other payers.
The Meaningful Measures Initiative aims to achieve high-quality health care and meaningful outcomes for patients with criteria that are meaningful for patients and actionable by providers, expounded Duseja. The work that CMS uses to develop this framework draws on measure work done by the Health Care Payment Learning and Action Network, NQF’s High-Impact Outcomes initiative, and the IOM’s Vital Signs: Core Metrics for Health
___________________
19 For additional information, see https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/QualityInitiativesGenInfo/Downloads/CMS-MeaningfulMeasures_Overview-Fact-Sheet_508_2018-02-28.pdf (accessed June 13, 2018).
and Health Care Progress consensus study (IOM, 2015b). The framework includes the perspectives from experts and external stakeholders, including the Core Quality Measures Collaborative,20 the Agency for Healthcare Research and Quality, and others.
Duseja explained that Meaningful Measures Initiative has several focus areas, all centered on the four key aspects she mentioned earlier (see Figure 6), and she provided a few examples of the approach CMS is taking in several of those areas. In thinking about strengthening person and family engagement as partners in care, for example, CMS divided its efforts into four measurement areas, including end-of-life care according to a person’s preferences and patient-reported functional outcomes. Regarding the latter, she noted that total knee replacement is among the top five most frequent in-patient procedures, but there is no good measure for how those patients are doing after surgery. The Center for Medicare & Medicaid Innovation has a pilot under way that is asking providers to report on joint mobility and patient quality of life 6 months after surgery.
Duseja noted that she and her colleagues have been mapping available measures to each of these focus areas, which has helped them think about the value added for each measure regarding quality improvement. In terms of priority areas, she mentioned improving interoperability of EHRs across health systems, promoting effective management of chronic conditions, ensuring adequate screening and treatment of substance abuse, and hospice quality reporting on emotional and religious support at the end of life.
CMS Quality Payment Program
Duseja also spoke about CMS’s Quality Payment Program, which is in its second year of operation. Clinicians can choose to participate in one of two tracks, the Merit-Based Incentive Payment System (MIPS) or one of the Advanced Alternative Payment Models that allow qualified physicians to submit data on populations of particular conditions as the basis for being paid for the care they deliver. This work is enabled by the Medicare and CHIP (Children’s Health Insurance Program) Reauthorization Act of 2015,21 and both programs are developing suitable measures (CMS, 2018f).
___________________
20 For additional information, see https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/QualityMeasures/Core-Measures.html (accessed July 29, 2018).
21 Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) (H.R. 2, Pub.L. 114-10) changes the payment system for doctors who treat Medicare patients. For additional
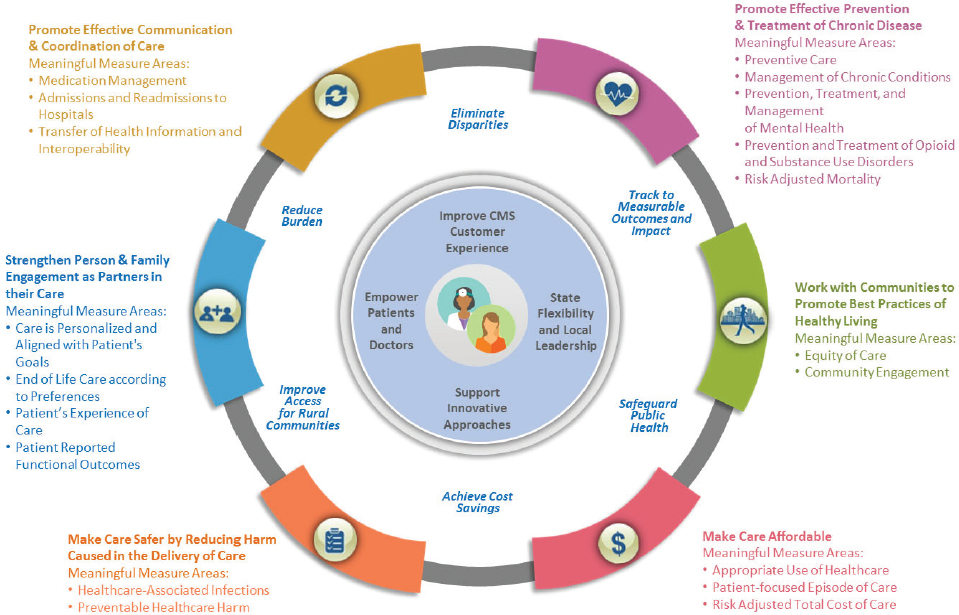
SOURCE: As presented by Reena Duseja, April 17, 2018.
To support measure development, CMS launched a funding opportunity in March 2018 to provide technical and funding assistance in the form of cooperative agreements to develop, improve, update, or expand quality measures for use in the Quality Payment Program (CMS, 2018b). “We want to utilize the expertise of clinical specialty societies, clinical professional organizations, patient advocacy organizations, and independent research organizations and other entities that are well suited to know what is happening at the frontline and what measures are meaningful in terms of improving care,” Duseja explained. The priority domains for this funding opportunity include clinical care, safety, care coordination, patient and caregiver experience, and population health and prevention. CMS has also identified specific medical specialties with pronounced measurement gaps, including orthopedic surgery, pathology, radiology, mental health, oncology, and emergency medicine (CMS, 2018b).
Overall, Duseja emphasized that CMS believes in the importance of aligning measures across public and private payers and shifting to less burdensome data sources. Duseja stated the serious illness field needs to be creative in thinking about data sources beyond claims. There are other ways, she noted, to think about how to have standardized data elements in EHRs to be able to collect data needed to develop quality metrics and test those measures. She and her colleagues see the Meaningful Measures Initiative as a means of engaging with the community and forming partnerships with patients and frontline providers to think about gaps and identify the areas that need attention to improve care not just for CMS beneficiaries but all Americans.
Caring for Patients with Chronic Complex Illnesses at the U.S. Department of Veterans Affairs
Susan Kirsh, acting assistant deputy under secretary for health for access at the U.S. Department of Veterans Affairs (VA), began her remarks by noting that, whenever she speaks about the VHA, she makes sure the audience is aware that the VHA takes care of approximately 9 million patients at 150 sites of care across the United States, Puerto Rico, Guam, and American Samoa. She explained that in 2010 the VA began to focus on the chronically ill population by first working to identify patients. As part of this effort, Kirsh’s colleague Stephan Fihn developed a clinical assessment needs score
___________________
information, see http://www.ncqa.org/public-policy/macra/the-medicare-access-and-chip-reauthorization-act-of-2015-macra-and-ncqa (accessed August 13, 2018).
that looked at risk for mortality and hospitalization, which helped inform the Patient Aligned Care Team (PACT) program that enrolled patients into hospitals that scored in the 90th percentile on this score (VA, 2018). Kirsh noted that many of these patients would be candidates for palliative care or hospice, but the goal was to reach to these individuals before that stage to see if team-based care and engagement of the families and caregivers would make a difference in their care.
The patients in the select group, explained Kirsh, had high rates of hospitalization and emergency department visits. Many suffered from complex and costly conditions, including cancer, heart failure, and renal failure. Approximately 65 percent had conditions spanning three or more organ systems, 50 percent had a mental health condition, 14 percent were homeless, and many had inadequate social support (Zulman et al., 2015).
The VA rolled out its PACT Intensive Management (PIM) program at six sites around the country, including both urban and rural locations. Patients were selected based on their clinical assessment needs score and randomized to work with either a team that intervened with intensive management or a team that did not intervene. The primary care-based teams worked with the VA’s patient-centered medical home program and served as liaisons to specialty clinics. The teams did not have a mandated composition, but all had a mental health professional, someone who could change medications, and a person responsible for setting goals (VA, 2017). The first finding from this study was that the cost of care did not change (Hebert et al., 2014). Another finding was that the primary care providers suffered less burnout and felt more supported (Helfrich et al., 2014). Patients in the intervention group reported having significantly more trust in their providers (Nelson et al., 2014) (see Figure 7). The test sites also increased engagement with community services to expand the reach of the program and provide needed services.
As a final note, Kirsh pointed out that, in an effort to improve care, the VA created a patient portal to counter misinformation, encourage shared decision making, and engage patients in the way they receive care and work with their providers to set goals.
Medicare Advantage Programs
Developing quality measures that cover everyone is difficult enough, but it is particularly complicated to develop measures for subpopulations, such as high-need patients. This is because high-needs patients involve a mini-
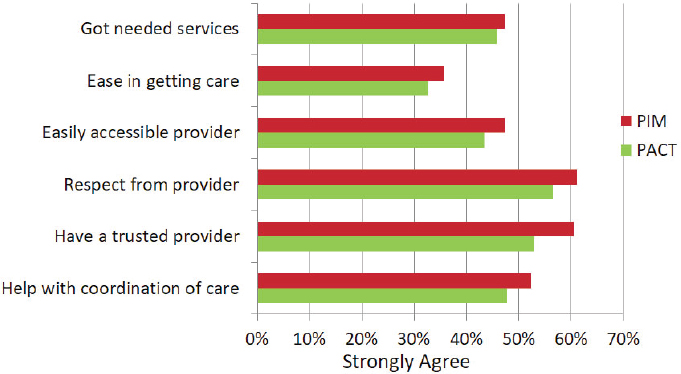
NOTE: PACT = Patient Aligned Care Team; PIM = PACT Intensive Management.
SOURCES: As presented by Susan Kirsh, April 17, 2018; Zulman et al., in press.
mum sample size, but patient numbers get smaller, particularly for clinically meaningful patient groups, explained Vincent Mor, the Florence Pirce Grant University Professor and a professor of health services, policy, and practice at the Brown University School of Public Health and research health scientist at the Providence VA Medical Center. Mor said one approach to addressing the “small numbers problem” is to aggregate across multiple years. This approach, however, leads to measures becoming less sensitive and responsive to interventions and policy changes. While meaningful measures for high-needs patients need to be actionable, that can lead to a checkbox mentality.
Complicating the matter further, expounded Mor, is that patients may choose to switch providers—they might be voting with their feet, he reasoned—but whether this is attributable to the plan encouraging high-need patients to exit or high-need patients choosing to exit due to dissatisfaction is unknown based on the available data. In addition, patients go from care setting to care setting, or “silo to silo” as Mor termed it, so while measures tend to be monolithic, accountability should span the entire continuum of care.
Looking at the Medicare Advantage Plan’s 5-Star rating system, for example, Mor noted that the system is a composite of more than 40 different parameters and types of quality measures, ranging from the CAHPS score to single chronic disease management measures. The disenrollment
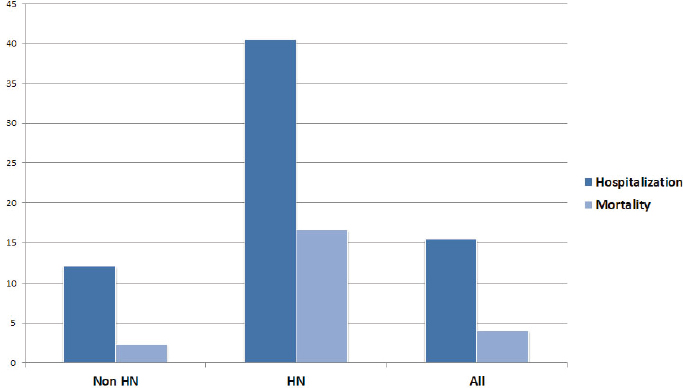
NOTE: HN = high need.
SOURCE: As presented by Vincent Mor, April 17, 2018.
rate is one of many performance measures in the 5-star composite rating, and therefore, by itself has a very small effect on the overall star rating, Mor emphasized (GAO, 2017).
Mor and his colleagues identified 6.47 million high-need Medicare beneficiaries, or 11.8 percent of the total population of 54.7 million Medicare beneficiaries by using Medicare Advantage and fee-for-service data and parsing the data using a variety of functional information from the Minimum Data Set (MDS), the Outcome and Assessment Information Set, and the Inpatient Rehabilitation Facility–Patient Assessment Instrument and Medicare Provider Analysis and Review data sets. Out of this high-need population, 1.53 million were enrolled in Medicare Advantage plans.22 An analysis showed that hospitalization and mortality rates were substantially higher among the identified high-need population (see Figure 8).
Mor observed that in the Medicare Advantage world, high-need patients are systematically selecting, or being selected, into lower quality plans (see Figure 9). “The quality of the plans is an important issue because the highest cost patients had the highest rate of leaving plans and the low-quality-rated plans have the highest disenrollment rates,” emphasized Mor.
___________________
22 Information was under review/unpublished at the time of this proceedings’ publication.
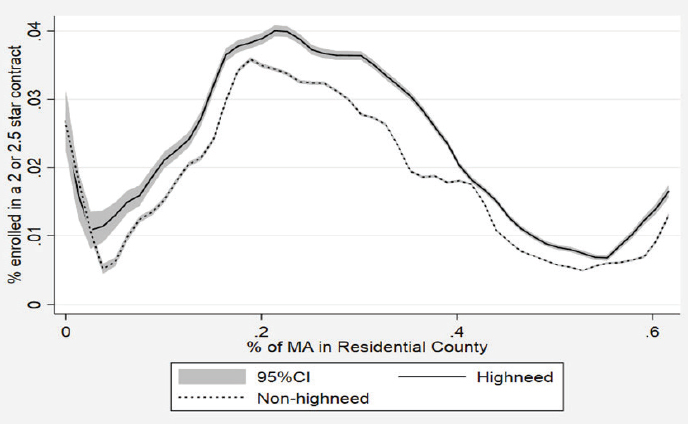
NOTE: CI = confidence interval; MA = Medicare Advantage.
SOURCE: As presented by Vincent Mor, April 17, 2018.
A closer look at who was leaving plans found that patients who have had a skilled nursing facility or home health experience were much more likely to leave (Rahman et al., 2015). For newly diagnosed patients with end-stage renal disease, the disenrollment rate from plans rated 2.5 stars or lower was 21.7 percent compared with 9.5 percent for plans rated 4 stars and higher (Li et al., 2018).
Additional analysis found that patients who are high-need are more likely to experience various forms of post-acute care need, and those who are in Medicare Advantage plans are more likely to enter lower-quality nursing facilities compared with those enrolled in fee-for-service plans (Meyers et al., 2018). “We were actually shocked by that,” reported Mor. High-need patients in lower-rated plans also have significantly higher hospitalization rates compared with those in higher-rated plans.23 The message from these findings, said Mor, is that lower-rated plans may be contracting with poorer-quality providers.
___________________
23 Information was under review/unpublished at the time of this proceedings’ publication.
Mor emphasized that these data do not argue that Medicare Advantage plans are bad for complex, seriously ill individuals, because 4-star and 5-star plans perform reasonably well. In fact, he highlighted, migration of patients in low-star plans to higher-star plans under the same corporate umbrella seems to be occurring. “There are plans that seem to do a good job,” said Mor. “My sense is we need some form of accountability. Someone has to be responding to these quality metrics, not just individual doctors but groups of doctors, since doctors have individual relationships with patients.”
To address this problem, Mor put forth what he called a “modest proposition.” He said, “we are looking at alternative payment models and they require value.” Population composite metrics are not sufficient for the task because they do not provide information specific for high-need patients who need higher quality care, which poses a challenge for the meaningfulness of quality metrics. Rather than developing new measures, one solution might be to weight existing quality measures more heavily based on high-need patients because Medicare Advantage plans’ payment is weighted in a similar fashion by case mix. This would result in the sickest patients counting more and “plans and ACOs [accountable care organizations] would be more accountable for the sickest patients,” reasoned Mor.
A Congressional Perspective
As the former health policy advisor to the U.S. Senate Committee on Finance, Becky Shipp attested to the fact that Congress is interested in evidence-based policies and outcome-based quality measures. Shipp, who is now vice president at the Sheridan Group, said there are opportunities to advance quality of care with the recently enacted legislation that supports social impact partnerships—also known as social impact bonds—or pay-for-success efforts.24 She explained that social impact bonds are used to fund an intervention that will improve outcomes based on agreed-upon metrics and save money in the process. If the intervention succeeds and produces savings, the investor is given a small return on investment and the intervention is scaled. If it fails, the investor is not paid and the intervention ends. “I believe there is a unique opportunity in this space, and Congress recently allocated $100 million for this effort to really experiment in the
___________________
24 For more information, see Supporting Social Impact Partnerships to Pay for Results: https://static1.squarespace.com/static/539e71d9e4b0ccf778116f69/t/5aa6db12ec212d0feebc031f/1520884687394/SIPPRA (accessed July 29, 2018).
quality measures outcome space,” stated Shipp. “I believe it would be well suited to the common goal of securing a reimbursement structure that is aligned with quality measures.”
While this approach has potential, Congress generally has relatively blunt instruments when it comes to supporting quality measures, she warned. The main lever is federal reimbursement through Medicare and Medicaid, programs that fall under the jurisdiction of the Senate Committee on Finance and the House Committee on Ways and Means, which has jurisdiction over Medicare, and the House Committee on Energy and Commerce, which oversees Medicaid. Shipp explained that the Senate Committee on Finance operates under different protocols and procedures than other congressional committees. To begin with, most committees mark up actual legislation, but the Senate Committee on Finance develops what she called conceptual marks. In addition, while staff in most committees are seen and not heard, Committee on Finance staff sit at the table and present analyses of bills to the committee members. The bottom line, she emphasized, is that “any process to implement quality measures needs to include a strategy to effectively engage with the relevant congressional committees and the staff with the goal of aligning federal reimbursement rates with best practices.”
In terms of timing, Shipp stressed there is a window of opportunity for anyone interested in advancing quality measures to engage with congressional staff in the weeks following enactment of the budget bill, when staff begin looking for new projects. While it was unlikely that much would be done before the elections in November 2018, she encouraged the workshop audience to use that relatively quiet time to meet with staff and educate them on the issues that are important in quality measurement. “The table needs to be set for future work and now is a good opportunity to have that conversation,” said Shipp, who pointed out that the serious illness community can add value to the current conversation in Congress about the opioid crisis. “I have seen many well-intended pieces of legislation reacting to a crisis that go over and above and, in some cases, exacerbate the crisis, and I do think we need to be wary of unintended consequences,” forewarned Shipp. In closing, Shipp emphasized, “I do think that there is an opportunity if not in this session of Congress, in the next session of Congress, to make a real step forward in terms of improving quality measures and improving patient outcomes.”
Discussion
Starting off the discussion session, moderator Eric Schneider noted there might be a legislative window opening for innovative ideas regarding Medicare Advantage and bundled payment models, two areas where there is a great deal of innovation occurring and in which private companies are developing new models of care. He commented that there has been a tendency in health care to use performance measurement as a lever to spur innovation, while in most other industries, it is the innovation that drives toward the measures. He then asked the panelists if they believe payment reform opportunities are the place to develop new measures and what factors they see driving new measures into payment reform.
Duseja replied that there are opportunities today to use multiple levers to drive innovation, and she has seen disruptive innovation take place without payment reform. One approach might be to use mobile device apps to collect data directly from patients that could be used for quality measurement, an idea that Mor supported to collect data on functional status. Duseja also noted that CMS’s quality payment program represents a good example of trying to align accountability with both quality and cost measures.
Shipp reminded attendees that policy tends to follow the money and “the thinking is that if the federal government will pay for it, the states, which run many of these programs, will do it.” However, states have an embedded fear of failure, she added, that acts as a barrier to innovation. Although researchers value a negative outcome as much as a positive one, states do not function from that perspective. “A negative outcome means that somebody might lose their job, so until there is the ability to experiment and to accept a non-successful outcome as just as valid as the successful outcome, there are going to be challenges [to innovation] in my opinion.” Kirsh said she would like to have some core concepts that are consistent across systems that will allow for some standardization in the way measures are implemented along with some ability for implementation to be adjusted to reflect local resource limitations or culture.
Workshop participant Louis Diamond, steering committee member with the Coalition for Supportive Care of Kidney Disease Patients, remarked that the end-stage renal disease program is unique in that it is a visible program with several payment reform initiatives and a robust set of measures. In addition, a burgeoning supportive care program is becoming operational. His question was how to deal with the seriously ill population
within the end-stage renal disease population without having a negative impact on the growing movement of providing palliative care to this population. “None of the palliative care and hospice measures are embedded in any of the measurement systems that are currently used for kidney disease patients,” explained Diamond.
In Duseja’s view, there is a need to start thinking about moving from disease-specific measures to broader measures at the population level. Doing so would focus systems to be thinking about system improvement for the overall population, versus developing interventions for specific populations, such as those with end-stage renal disease. “This is an important area for us to think about, particularly with the seriously ill with multiple chronic conditions,” emphasized Duseja. “Overall, we have to think a little bit more broadly and also think about interventions that are more systematic to get us to better outcomes,” she added.
FUTURE USE OF QUALITY MEASURES FOR ACCREDITATION TO SUPPORT ACCOUNTABILITY FOR HIGH-QUALITY CARE
Opening the fourth session, moderator Diane Meier, director of the Center to Advance Palliative Care, Gaisman Professor of Medical Ethics, and vice chair for public policy and professor in the Department of Geriatrics and Palliative Medicine at the Icahn School of Medicine at Mount Sinai, noted that until now, the field of palliative care has grown without the benefit of support from existing regulatory or accreditation frameworks. Much of that growth, she highlighted, has been achieved thanks to very generous private-sector philanthropy, strong specialty membership organizations, and other groups. Today, 94 percent of hospitals with more than 300 beds have a palliative care program and 70 percent of all hospitals with more than 50 beds report having a palliative program. “But that means 30 percent do not, and most of the 30 percent happen to be in the South and Southwest United States,” noted Meier (Center to Advance Palliative Care, 2018).
Meier began the discussion by asking the speakers what it would take to get to a point where high-quality serious illness care is not something you have to be lucky to get. Meier explained, “So many people who need what we have to offer never see us because it depends on the vagaries of individual attending physicians. Like patients with like needs should get like services, and that is not happening.” Meier challenged the session speakers to help the workshop participants understand what their organizations could do
to contribute to standardizing access to high-quality care for the nation’s most vulnerable patients. “What can we do to try to get to the point where high-quality serious illness care is integrated into the genome of American medicine?” she asked.
Maureen Henry, research scientist with NCQA, noted that for organizations to participate voluntarily in accountability programs, which are the majority of the programs NCQA develops, the programs must be of value to those organizations, given that the organizations pay to participate in them. Some of the program’s value includes structure, process, and outcome measures. Referring to Agrawal’s discussion of the increased push toward outcome measures, as opposed to structure and process measures, Henry pointed out that “the challenge is you cannot go straight to outcome measures when you do not have structures in place that allow people to report on those measures.” The same is true, reasoned Henry, for process measures.
Henry explained that NCQA is concerned about the absence of good clinical quality measures outside of assessment. Although the Hospice Item Set has several assessment measures, given the individuality of patients with serious illness, it is difficult to get measures that work reasonably well. Henry pointed out that something similar to the cardiovascular measures that indicate when someone should be discharged following a heart attack would be useful. “That is something that would be wonderful to develop to increase the meaningfulness of any accountability program,” she asserted.
Henry noted that health plans can influence the adoption of accountability measures by refusing to use a health system’s services if they do not have some stamp of approval from an accountability program. “If you are a health system, do you want to put money into a serious illness care program if you do not know the impact?” she asked.
Henry explained that NCQA has been experimenting with goal-based outcome measures for people living in the community with functional impairment, and it is now trying to take the lessons from those experiments and apply them to the serious illness population to identify measures related to the quality of conversations about serious illness. She noted that NCQA is “working with a learning collaborative to try to get closer to measures of outcomes that are feasible and useful and most importantly driven by the patients.” Henry added this project would benefit from several others also funded by the Gordon and Betty Moore Foundation that are working on patient registries and other data sources that will address shortcomings associated with claims and EHR data.
Henry described NCQA’s efforts to bring the patient voice into the design of accreditation programs and the development of measures. Two patients living with serious illness and a caregiver are on NCQA’s stakeholder panel, and each learning collaborative is required to establish a patient and family advisory panel.
Henry observed that only a handful of the 11 learning collaboratives have a process of identifying up-to-date, evidence-based recommendations for the care they provide, and even fewer track over time when they should update their clinical care quality processes. “If we cannot even be assured that they are looking at evidence-based guidelines and following them, which hopefully an accreditation or certification program could do, then how do we know what is happening to our loved ones?” asked Henry.
Accreditation and Certification at The Joint Commission
David Baker, executive vice president of the Division of Health Care Quality Evaluation at The Joint Commission, addressed the differences between accreditation and certification and their potential advantages and disadvantages. Accreditation and certification programs ideally should be measuring structure, process, and outcomes. He noted that it is important to have surveyors on the ground to look at structures and processes and see whether organizations are following the policies they have developed. The Joint Commission surveyors use “patient tracers,” for example, that examine the care patients receive throughout the hospital, and “system tracers” that look in detail at key structures and processes.
Baker explained that measure reporting and surveying have historically been separate, meaning that organizations report to The Joint Commission, CMS, and other entities, but those reports have not been integrated into the survey process. The Joint Commission has a new initiative to use both its measures and CMS measures to provide the surveyors with information that will enable them to examine the reasons why an organization is doing poorly on a measure. The Joint Commission is also working to improve the educational component of the survey process. The challenge is that the breadth of topics covered by the surveyors in the accreditation process makes it challenging to drill down on specific aspects of processes and structures.
Baker pointed out that The Joint Commission is not the only accrediting organization recognized by CMS, so if it pushes too hard to achieve its mission of improving quality and safety, a health system can switch to
another accrediting organization that may not have those specific requirements. Baker noted that CMS could address this issue by passing a new Condition of Participation for such requirements, which all accrediting organizations would then be required to assess on their surveys. However, he acknowledged that doing this would be difficult because it would require legislation to be passed.
Certification, explained Baker, is a similar process, but involves a deep dive into a narrow topic such as stroke and hip and knee replacement. Certification is optional, and gives The Joint Commission leverage to be able to push an organization to meet higher standards on relevant structure, process, and outcome measures. Referring to the example of hip and knee replacements, Baker explained that The Joint Commission is working with the American Joint Replacement Registry to develop a patient-reported outcome measure. “Ideally, certification becomes a learning collaborative;” though he added “we are not there yet.”
A particular advantage of certification is that it helps to identify high performing organizations that can serve as benchmarks for other systems. The disadvantage is that this approach is disease specific, except for palliative care programs. “If you think about the long list of individuals with different types of serious illness, no hospital would be able to support 17 different kinds of programs,” said Baker. Certification is also setting-specific, so it does not consider coordination of care across different settings. The Joint Commission recently developed an Integrated Care Certification that looks at integration in care between facilities named in the certification program, but the survey process does not currently examine whether patients are receiving well-coordinated care across all settings.
Certification, posited Baker, needs an economic driver, such as those that Fields and Krebbs discussed. The certification for stroke care, for instance, had an economic driver, in that paramedic protocols stated that patients needed to be taken to a primary stroke center or comprehensive stroke center. “Hospitals knew they had to get that certification,” reasoned Baker, who added that he believes the stroke certification program has made a major difference in stroke care in the United States.
Responding to Baker’s comments, Meier pointed out the terminology is confusing in terms of what is voluntary and what is not. She noted that The Joint Commission accreditation for hospitals is not voluntary if a hospital wants to be paid, and added that voluntary certification serves as a weak lever that lacks the power of mandatory certification or of a legislative or regulatory solution, particularly in the context of the current
cost-cutting environment. NCQA accreditation is voluntary, and does not tell you whether it is linked to payment or not. Certification is voluntary and sometimes has financial incentives such as Anthem and Blue Shield of California’s requirement that, if a program wants per-member, per-month payments for palliative care delivery, the program must be The Joint Commission certified. “The problem is that there is not standardization of that practice across the country,” highlighted Meier.
Measurement in the Context of Hospice and Home Health Care
Barbara McCann, president and chief executive officer of Community Health Accreditation Partner, an organization that she noted has spent “the past 52 years in the community,” opened her remarks by noting that when hospice first began in this country, standards were created by stakeholders who came together voluntarily. The process of developing those standards was pivotal, she said, because putting pen to paper made everyone begin to look more closely at the care they were delivering and the ways in which they were delivering that care. Referring to assessments, McCann stressed that there must be key points that everyone believes should be included, such as care coordination and how that manifests in hospice settings, and both the delivery of care and the ability to refuse it. McCann emphasized that a key lesson she and her colleagues have learned is to ask patients about their experiences that contribute to a good outcome.
McCann pointed out that emergency preparedness and infection control become important when the hospice setting is at home, as does the legitimacy of the organization that is providing hospice. “Home- and community-based care in and of itself does not mean that it is a legitimate organization,” said McCann. She noted that, in the absence of certification or licensure, it is hard to close bad programs. She added that hospice has not changed over time to reflect the reality that many of the diagnoses that were invariably fatal when hospice started are no longer so. As a serious illness advances, it will necessarily follow a predictable trajectory. As a result, an individual may be in the hospital for a while and then a skilled nursing home or home care and back to the primary care provider. Given these different care settings, one challenge going forward is deciding to whom an agency would award accreditation.
McCann observed that, in terms of the assessment of functional status in the post-acute world outside of the hospital setting, the nursing home, home health, and hospice all collect different data sets using different
instruments. “There is no common measure,” said McCann. She explained that her organization goes into homes to see what is really happening, to understand the psychosocial elements of chronic illness care in the home, and to respond to complaints from its complaint line with unannounced visits. The good news, she said, is that patients have figured out that they have rights and that their care should follow a plan.
McCann pointed out that within home- and community-based care, there is an incredible richness of data that can be stratified by diagnosis. According to McCann, approximately 9 percent of all Medicare beneficiaries have received home care over the past 3 years for a wide range of conditions (CMS, 2018c). She noted that standards have not been set for home care, though there are new conditions of participation. There is, however, experiential evidence, as there is with hospice, palliative care, and serious illness care, and that evidence needs to be used to develop existing accountability mechanisms and make them real for the people who are being cared for at home. “What they look like sitting on the chair in the clinic is not what you see around the kitchen table, and health decisions are made at the kitchen table every day in this country,” she said. In her view, there is a system to put accountability in place and make it work, and the accrediting bodies need to do that now.
Meier asked McCann if home care agencies must be accredited to be paid, and McCann replied they do not. “Any home care or hospice organization and hospital can have a free survey done by the state or through a voluntary accreditation survey for hospice or home care to demonstrate compliance with the conditions of participation,” she explained. “You are able to blend standards that folks need that have nothing to do with payment.” According to McCann, about 50 percent of all hospices and approximately 6,000 out of an estimated 11,000 home health care organizations are accredited (CMS, 2018d,e).
Challenges of Quality Improvement
Franziska Rokoske, director of the end-of-life, palliative, and hospice care research program at RTI International, emphasized that “even when we know the denominator, and who is accountable for what and in what settings, there are a variety of challenges that providers encounter when trying to improve quality of care.” One downside of focusing on outcome measures, she explained, is that “we lose some of the granularity of what is actionable” by clinicians to improve the quality of care they provide.
She recalled that she was working in a nursing home when the MDS was released. The first day she had to complete the MDS form, she wondered what filling out the form had to do with the physical therapy she was supposed to be delivering to her client, who was receiving rehabilitation therapy after hip replacement surgery. Her next thought was how she could get through this quickly, so she could get back to her work. At the same time, she observed all the ways in which the nursing home was falling short on serious quality-of-care issues. That story, she said, illustrates the importance of appreciating how measurement can enable clinicians to do better while meeting the needs of other stakeholders for accountability.
Returning to the initial focus of the day on patient and caregiver experiences, Rokoske said she does not know whether a typical caregiver or patient would know what an accreditation or certification means. She also said the workshop audience and broader community of people involved in caring for those with serious illness need to “think about how to leverage the patient and caregiver voice. We talked about some of the policy levers and the payment levers. Having engaged patients and caregivers is another key” lever to improve quality.
Discussion
Before opening the floor to questions, Meier observed that it was helpful to hear from the speakers about barriers to making access to high-quality serious illness care a reliable component of the U.S. health care system. A major constraint, she said, is that accreditation or certification is voluntary, and that there is competition when it is not voluntary. As Baker pointed out, when The Joint Commission was “the only game in town,” it could set a very high bar. It now has competition that is willing to set a lower bar. To address that “requires legislation, and working with legislation requires a different set of skills, money, and organized coalitions,” said Meier.
Meier also pointed out that the National Consensus Project for Quality Palliative Care25 first released guidelines in 2003, and has been through three editions with a fourth currently in process. The fourth edition is being developed specifically to ensure applicability across all settings, all patient populations, and all types of clinicians, and it is not directed only to hos-
___________________
25 For additional information, see https://www.nationalcoalitionhpc.org/ncp (accessed July 29, 2018).
pices and specialty palliative care programs, but to everyone who takes care of seriously ill people. It will serve as a set of principles and practices that should inform care across all settings and disease types, she said. “What would be nice is if these evidence-based, consensus guidelines were to be integrated into the measurement and accreditation process so that there are not different sets of measures and standards depending on who is paying you and who is accrediting you,” asserted Meier. “If we can get to even the basics of what a palliative care team looks like and what all hospitals should provide at some decent level of quality—not 100 percent perfection—we would be so much further along than we are now.”
Workshop participant Lauren Cates noted that The Joint Commission pain standard now includes a requirement that hospitals provide non-pharmacological pain interventions, but when she mentions this to decision makers at hospitals, they are not responsive. She asked the panel how requirements such as this could be used to change the conversation to push non-pharmacological interventions. Baker replied that the requirement says that hospitals need to provide some type of non-pharmacologic treatment, but The Joint Commission intentionally did not provide a list of what those should be because of the limited data that exist. “We wanted to be able to set the bar, and we know the evidence base is going to explode in this field,” said Baker. The way to expand on this initial requirement is to create a foundation upon which to build as the evidence accumulates to support specific approaches. CMS can do this through interpretive guidelines without the need for legislation, Baker added. “We will change and be more prescriptive according to what the evidence says.”
Laura Hanson commented that she and her colleagues often point families and patients to Nursing Home Compare, which gets them in trouble with the social work and care management staff because it delays rapid discharge to the first available nursing home bed. Nonetheless, she and her colleagues view that act as high-quality care because it empowers the consumer to understand that they have freedom of choice. “The freedom to choose is rather meaningless without information about the choice that you are being offered,” said Hanson. She wondered if there is a lever that needs to be pushed so that information about accreditation and higher-level certification is actually available to consumers. McCann noted nothing prohibits a hospital or a skilled nursing facility from putting ratings next to the names on the list of nursing homes or home care organizations. Henry called for “something like a movement from patients and people like us in
this room to figure out how to get systems in place that do allow us to assess the quality of care that people are receiving.”
Mor remarked that for years, hospitals have purposefully hidden behind a misinterpretation of the CMS directive regarding choice because it makes it easier for them to discharge patients more quickly. In addition, many discharge planners do not know how to work with nursing homes, home health, or Nursing Home Compare, and most do not have access to a computer to make that part of the facilitation process. It is only in those cities that are fully networked, Mor explained, that discharge planners know about specific nursing homes and home health agencies and their connection to specific providers.
SUPPORTING CLINICAL COMMUNITIES FOR QUALITY AND ACCOUNTABILITY
The Palliative Care Quality Network (PCQN) represents a practical approach to quality measurement in specialty palliative care for people with serious illness, said Steven Pantilat, professor of medicine in the department of medicine at the University of California, San Francisco (UCSF), the Kates-Burnard and Hellman Distinguished Professor in Palliative Care, and founding director of the UCSF Palliative Care Program. PCQN, he explained, is a national learning collaborative committed to improving care of seriously ill patients and their families in the context of palliative care. The network encompasses a total of 111 member organizations, including 69 community hospitals, 14 academic hospitals, 11 public hospitals, and 17 community-based organizations (PCQN, 2018).
A core component of the network is its data registry, and the network focuses on community education and quality improvement to engage people around those data. PCQN recognizes there is no such thing as non-burdensome data collection, said Pantilat, so the network developed a standardized, parsimonious, and focused data set of 23 elements that can be collected in the EHR through a note template with discrete fields. The data are then uploaded automatically into the PCQN data registry. There is also the option of uploading data via a website, and some teams collect the data on paper for later entry into the registry. The goal of the registry is to be clinically useful and reflect interdisciplinary care. It contains measures of spiritual care and screening, psychosocial measures, and patient-reported outcomes, including POLST form completion and pain management. PCQN also collects structural data to enable linking a team’s structures and
processes with outcomes. Pantilat said the registry could generate robust reports quickly, which PCQN members value as a means of engaging with the data and benchmarking themselves to the entire network and to the smaller subset of similar PCQN member programs.
The registry started collecting community-based data in 2017 and now contains data on more than 10,000 visits with about 3,500 patients that were used to generate more than 2,000 reports. PCQN has been collecting inpatient data for more than 5 years, and has data from more than 140,000 patient encounters that have been used to produce nearly 46,000 reports (Pantilat, 2018). Sharing an example from the UCSF team, Pantilat described how, with a click of a mouse, the registry produced a pain assessment score based on nearly 2,900 assessments. The report showed that approximately 30 percent of the people had moderate to severe pain on first assessment, 60 percent reported improved pain control by the second assessment, and 78 percent had improved by a final assessment. “These are reports that are generated in real time by the teams,” Pantilat noted.
He then presented a comparison report by team (see Figure 10) showing how his institution (the red bar) compared on improvement between first to last pain assessment. This report includes his institution’s denominator and 95 percent confidence interval. Comparing his institution’s progress to others is very helpful, explained Pantilat.
In summary, Pantilat said PCQN has demonstrated that it is feasible to collect standardized, patient-level outcome data in real time from busy clinicians and share those data with a community of organizations and individuals. He noted a key feature of the data set is that the data are focused and clinically meaningful. Pantilat pointed out that the network “gives you information that matters in your care of patients, and it has been integrated into the workflow,” he said. “We have found that the more we are able to integrate into the workflow, the easier it is,” he shared. The other noteworthy feature, he added, is that the registry generates reports quickly and easily, which enables team members to engage with the data. He noted that PCQN members use these data to give their team members feedback on how they are doing. For example, his institution’s previous score on spiritual assessment was in the 30s, prompting a review that has since improved that score.
Referring back to Fields’s presentation, Pantilat said several health plans in California now use PCQN data as part of their accountability strategy for the state’s requirement under SB-1004 that palliative care be available to all Medicaid patients. In addition, PCQN is already being used for accountability as the Partnership Health Plan in Northern California
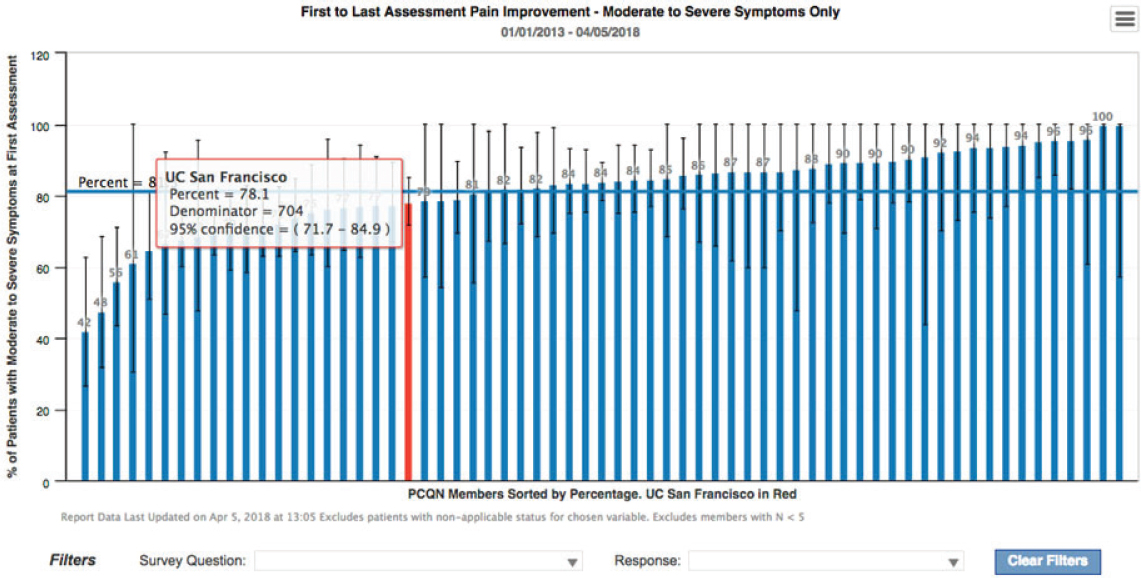
NOTE: UC = University of California.
SOURCE: As presented by Steve Pantilat, April 17, 2018.
pays teams a per-patient, per-month bonus if they use PCQN data as a quality measure, according to Pantilat (Partnership Health Plan in Northern California, 2018). He acknowledged that PCQN’s approach does not cover all individuals with serious illness, but it nonetheless provides some valuable lessons that can be applied more broadly to engage clinicians to improve care for all patients.
A Health Care Information Technology Company’s Approach to Support Accountability
Over the past few years, Cerner, the second largest health care information technology company in the United States, has been building an infrastructure and architecture for its HealtheIntent cloud-based population health platform. As of February 2018, this platform is connected to 38 EHRs and is used by 75 payer vendors, explained Hannah Luetke-Stahlman, strategist for population health at Cerner.
Luetke-Stahlman described several of the software programs that sit on this cloud platform. One is the organization’s Healthe record that spans a patient’s lifetime regardless of venue of care. She explained that the Healthe record dovetails with a longitudinal care plan focused on a patient’s goals and treatment preferences, HealtheCare care coordination, which provides an extra layer of support to patients as they transition across venues in the care continuum and the Healthe registry solution. The HealtheIntent engine, she noted, aggregates data across the care continuum, normalizes the data, populates the various population health solutions, and then pushes the data back into EHR systems from multiple vendors (Luetke-Stahlman, 2018).
Luetke-Stahlman explained that Cerner has produced more than 45 different registries covering a variety of different conditions, and the Healthe registry focuses on quality measures (Luetke-Stahlman, 2018). The goal, she said, is to use the registries to provide clinical intelligence that identifies at-risk patient populations and then highlights an organization’s gaps in care for those patients on an analytics dashboard.
In 2017, Cerner created an MIPS quality registry used by more than 1,200 providers to make submissions directly to CMS. The three validation partners reported that it took about half the time for providers and organizations to submit data to CMS using the registry (Luetke-Stahlman, 2018).
Real-World Implementation of Quality Measures
Referencing a point made earlier in the day, Debra Saliba, the Anna and Harry Borun Endowed Chair and director of the University of California, Los Angeles, JH Borun Center for Gerontological Research; physician scientist at the Los Angeles VA Geriatric Research Education and Clinical Center; and senior natural scientist at RAND Health, noted that providers do not walk into the door of a clinic or a hospital wanting to provide bad care. However, “reality can get in the way of intent, and implementation science is really about how we can systematize that drive for quality that we all had when we decided to go into clinical care.” Saliba asked, “How do we use measures to help us create a learning environment for our providers?”
Implementation of quality measures, asserted Saliba, is a staged activity that is harder than it looks and involves more than just collecting data. “Collecting data is not going to change outcomes, so we have to be prepared for how we are going to make change happen within an organization,” said Saliba. The first step is to assess an organization’s readiness for change. This includes an analysis of whether stakeholders and leadership support working toward improvement, as well as understanding that there are often gaps between an organization’s leadership and its frontline staff. This is notable because both leadership and staff need to be supportive in order for a change effort to succeed. She added that articulating a clear case for change is critical to obtaining such support. “This is where the whole idea of meaningful measures becomes particularly important,” emphasized Saliba. “If we cannot articulate that need for change, then we are not going to be able to drive it,” she added.
Saliba cautioned against having one person leading the change effort because it helps insure improvement to have redundancy, as well as group and team thinking to drive the process. Saliba pointed out that, when assessing readiness for change, it is important to remember “chaos does not equal opportunity;” in fact, if an organization is chaotic and unbalanced, team members are not going to be open to constructive change. She recalled one project in which she and her colleagues assessed a variety of sophisticated measures of readiness for change, but they found the most important predictor of the ability to implement high-quality care was whether people on the team thought their environment was undergoing unpredictable change. Some organizations will have established a sense of stability and some will
not, she said, but implementing change is very difficult without a firm foundation in place.
Saliba described the second step as managing change and clarifying the need for change (using quality measures) and identifying members of the interprofessional team who might be affected by change. As an example, she described the experience when her team was conducting training to test changes to the MDS, which included adding patient-reported measures into the MDS for the first time. Saliba said the trainees revolted, saying that they could not and would not collect those measures. After some investigation, it became clear that a major reason for opposition to the change was that the team members lacked training on how to conduct structured interviews with older adults. After taking a step back and building a training module on structured interviewing of older adults, they proceeded with the original training. Saliba noted that in the end, the people who originally opposed the change found that collecting these patient-reported outcomes was both meaningful and made them feel like they were a clinician and not only a data collector.
Saliba observed that in her experience, although many providers tend to be skeptical of patient self-reports, such reports of function are very reliable, and are highly predictive of other outcomes. She said it is unnecessary to develop complicated measures to be able to standardize the process and reach a measure that works. When thinking about function, Saliba pointed out, instrumental activities of daily living, in addition to activities of daily living, can be just as informative because, for many people, the instrumental activities drive quality of life.26
Saliba noted that while outcome measures are important, they can paint an incomplete picture of whether care is appropriate. These should be seen as potential indicators or signals of care. For example, she has been working with Mor on a project looking at transfers from nursing homes to hospitals. On the surface, the transfer rates seem too high, but a closer look revealed that a significant percentage of those transfers were appropriate. “For an organization trying to improve rehospitalization rates, it is impor-
___________________
26 Activities of daily living are activities in which people engage and include everyday personal care activities, such as bathing, dressing, grooming, toileting, eating, and walking. Instrumental activities of daily living are not necessary for fundamental functioning, but enable an individual to live independently and include activities such as cleaning and maintaining a home, shopping, driving or taking public transportation, managing money, preparing meals, and taking prescribed medications.
tant to understand the elements that are going into rehospitalization,” said Saliba.
The third step in the change process is to identify the practices and processes needed to attain the identified goal. Identifying best practices is important, but doing so can be a challenge when there is not enough data to determine best practices, said Saliba. She pointed out that “we have had very little discussion about significant mental illness as a primary chronic advanced illness that affects life expectancy and needs for support.” She remarked this is likely due to the fact that there are fewer data in that area, but stressed that does not make it “any less important as an area for quality improvement.”
Saliba observed that, to attain the desired goal, it will be necessary to customize or adapt the various aspects of care to the environment in which patients receive care. One challenge of implementation science, she explained, is to identify the elements of an intervention that worked in one setting that need to be reproduced for the intervention to work versus those elements that need to be adapted to the local organizational culture.
The final step in the change process is thinking about how to incorporate change into the workflow. Saliba recalled how she and her team went into an organization, conducted extensive training and role playing, and left with everyone excited and knowledgeable. Six months later, nothing had changed, and staff said that while they loved what they had learned, they could not implement any of it because their schedules and staffing could not be changed, and the facility was not set up to accommodate all the great things they had learned. “It is really important that we are humble about how to incorporate this into the workflow so that it actually becomes part of what folks are doing,” said Saliba. On a final note, she stressed that change implementation is not a linear process, but rather one that requires continual evaluation, reassessment, and adaptation.
Building on the theme of implementation, Carol Spence, an independent consultant and former vice president of research and quality at the National Hospice and Palliative Care Organization, shared the story of “a lived experience with a single measure.” She summarized the plot of the story as provider ignores measure, provider meets measure, provider does not like measure at first but does so once it gets to know it a little better. In the end provider embraces measure. Spence reminded the audience that the hospice community, as pointed out earlier in the day, decided long before quality was a watchword that it needed measures that captured and preserved the meaningful and unique nature of its approach to care. The
result was the development of a set of “end-result outcome measures,” one of which had to do with pain, and every patient was asked by a screener at the initial encounter if he or she was uncomfortable because of pain. Those patients who said yes became the denominator for hospice.
One of the main principles that drove this choice of a measure, said Spence, was that it incorporated the patient voice and did not, and was not intended to, impose any clinical judgment as to what comfort meant to each individual. In other words, pain and comfort were what the patient said they were. From there, the clinical team used its regular assessment tools and pain management skills, and 48 to 72 hours later, the patient was asked if their pain was brought to a comfortable level. For those who said yes, they went into the numerator.
The National Hospice and Palliative Care Organization put this and other measures into place, along with instructions on how to implement the measures. Spence and her colleagues started a national-level data collection initiative populated by aggregate data from hospices, and the organization would produce reports with national comparative results for the hospices to use for quality improvement. Spence explained that this was a strictly voluntary program. One hospice, which had been using the measure for several years, hired a new quality improvement staff member, who took a closer look at the measure and found that the hospice’s score on the measure was about 50 percent, which nobody had noticed before or tried to understand.
The first reaction to the score was denial, noted Spence, followed by acknowledgment that a problem existed, and then finally acceptance that the hospice needed to do something to address this issue. The team rolled up its sleeves, said Spence, and tackled the entire pain management program from the starting point of standardization and building the measure into the resulting protocol. The hospice introduced new processes, including asking someone who was not part of the care team to administer the follow-up question and adding a medical review of the appropriateness of its interventions. As a result, more extensive training was put into place, along with a rigorous assessment of competency. “This is a success story,” emphasized Spence, “that is built on looking at the results objectively and engaging the entire organization behind it.”
Discussion
Leading off the discussion session following the presentations, Tulsky remarked that integrating data collection into the workflow is essential
for provider acceptance, yet integrating a measure set into the EHR is a monumental task that requires a great deal of development work, not to mention joining a long list of other requests to develop something for the EHR. Given that, he asked the panelists if they had any ideas on how to move these projects forward. Luetke-Stahlman agreed that technology should support the clinician, and not create an additional burden. She noted, however, that her organization’s senior leadership is asked every day to prioritize requests from a large number of companies. In her 5 years with Cerner, she has observed that those items that get priority deal with regulations and policies, including quality measures. Her advice was to “continue to advocate on behalf of your field, all the way to the senior leadership of your own hospital and health organization, and all the way to the federal level.” She also suggested finding an information technology champion not only within one’s own health system, but also within the EHR vendor’s organization, and educating them about the importance of the specific measures that need to be implemented.
Pantilat advised adding data collection into the EHR note template and including more pull-down menus. He admitted that he was not sure that entering data into an EHR was faster than putting it on paper, but entering data in the EHR feels like part of the workflow, which leads to greater acceptance. In his opinion, entering data into the EHR is the easy part—trying to get them out in a meaningful and useful way is more difficult. His hope is that with a unified registry for the field it might be possible to build capability at a more fundamental level of the EHR of every vendor.
Saliba added that it is important that providers see the need to enter data into a blank field that pops up on the EHR screen as relevant to their practice. In her experience, she sees providers enter data into fields with data that were not obtained from the patient just to fill in the field. She asserted that providers need to agree that information added to the EHR is important for caring for their patients, and the system needs some quality checks to make sure that what is put into the database reflects the reality of the patient. Pantilat and Hanson both noted that EHRs are filled with elements that providers thought would be interesting, but in the end are too all-inclusive or more comprehensive than what is needed to focus on the culture of quality.
Marian Grant, an independent policy consultant and practicing palliative care nurse, wondered why the relevant set of measures has to be incorporated into EHRs one institution at time rather than as an off-the-shelf product. Luetke-Stahlman replied that her organization deals with
the balance between customization and standardization every day. Every provider, she said, wants to document information the way they want to document it, yet at the same time, large hospital systems want to be able to compare apples to apples and generate standard reports. Incorporating a national registry requires a great deal of resources, she said, to figure out how to capture the necessary data. What would help, she reasoned, would be standard definitions of concepts such as serious illness and advance care planning.
Joanne Lynn noted that the Office of the National Coordinator for Health Information Technology has completed work developing a 340-field template on primary care in geriatrics that will serve as the standard for all EHR systems. Similarly, CMS has developed a 10-element screener on social services for accountable health communities that will also be a standard for all systems. For Lynn, hospice, palliative care, home health care agencies, nursing homes, and hospitals should all be measuring functional status, cognitive function, pain, and other measures in the same way. “There is a certain wisdom to standardization, even if you do not like that way of measuring as much as the one you customized,” said Lynn. “Being able to translate across settings has become so important that it seems we ought to be engaged in these other activities.” Pantilat agreed completely with Lynn, noting that standardization is powerful, both in terms of it being easier than having to invent everything from scratch and because it enables meaningful comparisons. He added that standardization does not preclude the fact that specialty areas, such as specialty palliative care or hospice, may need specific measures for deeper exploration into certain areas.
Lori Bishop, vice president of palliative and advanced care at the National Hospice and Palliative Care Organization, voiced her support for standardization and added another benefit: patients will get used to being asked the same questions in the same way, which will lead to a better patient experience and better data for the provider. She also noted that there is an opportunity to collect data for functional measures in a healthy population, perhaps not as a quality measure but as an indicator to identify people with progressive illness that will enable clinicians to get them the appropriate care in a timelier manner. “We want to think about the development of tools and resources within an EHR that are longitudinal as well when they can be,” said Bishop.
CHARTING A PATH FORWARD
In the workshop’s final session, three panelists—Amy Berman; Sean Morrison, chair of the Brookdale Department of Geriatrics and Palliative Medicine at the Icahn School of Medicine at Mount Sinai and director of the National Palliative Care Research Center; and Murali Naidu, vice president and chief clinical officer at Sentara Healthcare—reflected on the day’s presentations and discussions. Berman started off the discussion by noting that she is living with terminal illness, having been diagnosed with Stage IV cancer more than 7 years ago. Thinking back to Herrera’s ordeal of seeing four different physicians for her daughter and Darien’s personal experiences as a cancer patient and survivor, she noted that her takeaway from those presentations is that “the system itself is deaf to the people that it cares for.” Referring to Herrera’s story about how her concerns about her daughter were ignored by the first three providers she saw, Berman said there was no good measure in place that supported good care at any level, and as a result, none of those three providers learned anything from their failure to truly listen to and address Herrera’s concerns about her daughter. “There was no systems learning to have a different type of care. So when we think about what we need to re-envision a deaf system, we need to have processes in place. We need a way of collecting data that really matters to the person, and communication and listening to the patient is one of those components,” she said.
Likening the health care system to a pre-Copernican model of the solar system, with the physician at the center of the universe instead of the patient, Berman said the focus is on the needs and siloed data of medical societies, yet those with serious illness often do not have one disease, but multiple chronic conditions and multiple clinicians. “We have to look more broadly from a systems perspective,” Berman commented, and stressed the need to untether the disease aspect from measurement and focus on the goals of care from the perspective of the individual and the sum of their conditions and social needs.
Berman shared that she was also struck by the fact that a focus on the denominator leads to a situation where there are stark guidelines that dictate care, even though the care goals of two people lumped into the same denominator might be very different. This situation, she said, is the cause of much of the unintended consequences of care. Acknowledging that people do not fit into simple denominators would reshape care, emphasized Berman.
Berman noted her final takeaway from the day was the promise of moving from data points to a data story, of triangulating data to get a better picture of patients and the care they need. The problem, she noted, is that most providers do not have access to the full scope of an individual’s data, particularly at the time that they need it to make care decisions and inform their patients. “It is time that we had data integration and data liberation so that we can make better decisions in partnership with the people that we care for,” asserted Berman.
Naidu, in reflecting on what he heard throughout the day, said that a constant theme was how critical it is to hear what people who have serious illness and are receiving care for it through the health care system want and need. The other key message Naidu identified was that measures need to drive improvement, whether through accountability, payment models, or other mechanisms. What makes that complicated, he said, is the diversity of both the patient population and the stakeholders who will use the information that comes from measurement. The solution, he said, will require taking risks, which means being willing to try new things, make some mistakes, and spend some money to see what works.
Naidu also reiterated Berman’s point about the timeliness of data availability. Using an analogy of being told what speed a car is going an hour after passing a speed limit sign, he highlighted how unhelpful such a delayed process was and posited that if the expectation is for data to drive improvement, it must be available in real time because providers are constantly taking care of patients.
For Morrison, the workshop presentations made him think back to a meeting nearly 20 years ago when researchers came together to try to address the issue of accountability for those with serious illness. Those in attendance included Joan Teno, who referred to H. L. Mencken’s quote that for every complex problem there is an answer that is clear, simple, and wrong. Noting this was exemplified by the workshop’s first speakers, Morrison’s first takeaway point was that the current way of measuring quality and determining accountability is a terrible fit for the population of people with serious illness. “Assessing quality for people with serious illness is not only going to need new measures, it is going to need new measurement techniques, and, folks, it is going to be burdensome,” cautioned Morrison. “There is just no way of getting around that. There is not a simple solution here.” In his opinion, society is going to have to decide if it is going to pay for that burden, because everything that the field has tried has been simple and straightforward, and has failed to solve the problem.
His second lesson from the day was that the field needs a new paradigm for measurement, one that recognizes that “what is important may simply not be measurable, and that is a really hard thing to come to grips with.” Morrison pointed out that if the mantra is to provide care concordant with goals, that implies the need to measure something that is going to change on a weekly to daily basis in the setting of progressive serious illness, and that the patients’ and families’ perspectives, for example, will be different after a death than the day before death. “Yet, that is what we are all focusing on trying to measure right now,” he said.
Morrison further emphasized that bad measures lead to bad outcomes, and used pain assessment as an example. He explained that the CAHPS survey used to ask patients during a hospital stay if they need medicine for pain and how often their pain was controlled. Morrison said that question was removed from the survey in January 2018 because they were deemed “bad measures,” because they were leading to an increased prescribing of opioids for inappropriate use. Morrison argued that the measure was not bad, what was bad was that the measure did not reflect the evidence that pain is not all the same and that some pain responds to opioids and some does not. He explained that the survey was changed to include a question about how often the hospital staff talked to patients about how much pain they were experiencing. Morrison pointed out that the measure still does not reflect the substantial body of evidence that these questions do not lead to improved outcomes, but rather to an improved assessment of pain and to patients feeling better that they were asked. Morrison emphasized the need to think about new ways of getting at measurement, because surveys do not work when the patient has died, is severely disabled, or when the family is overburdened, he said, and claims data will not suffice if the desired data are never going to be in them. “So we need to think about a broadened paradigm that focuses on proxy respondents,” he said.
In closing, Morrison commented, “it seems that hospitals, health systems, and others are accountable for the social determinants that are driving so much of the care quality.” He wondered if that was the case, “shouldn’t we be measuring and reimbursing for that kind of care?” In the same vein, he asked, “If measurement is so important, if we are asking our institutions and our clinicians to engage in this quality initiative, why aren’t they getting paid to do it? If it is as important as the care that is being delivered, that is assessing how well we are doing it, why aren’t we reimbursing for it?”
On a concluding note to close out the workshop, session moderator Christian Sinclair, assistant professor in the Division of Palliative Medicine
at the University of Kansas Health System, emphasized the message that quality measures must drive action and change. “Just having the quality measure is not enough,” he said. He pointed out that while many of those attending the workshop have been at this for years, the audience is getting larger. “We have more people’s ears, but it shows that this takes sustained effort and sustained advocacy, locally and more broadly. . . . Action and advocacy over time really is what makes the difference,” he concluded.
REFERENCES
Ayanian, J. Z., and H. Markel. 2016. Donabedian’s lasting framework for health care quality. New England Journal of Medicine 375(3):205–207. doi: 10.1056/NEJMp1605101.
CAPC (Center to Advance Palliative Care). 2018a. Palliative care, report card. https://reportcard.capc.org (accessed August 1, 2018).
CAPC. 2018b. About palliative care. https://www.capc.org/about/palliative-care (accessed August 1, 2018).
CDC (Centers for Disease Control and Prevention). 2014. Home health care. https://www.cdc.gov/nchs/fastats/home-health-care.htm (accessed August 1, 2018).
CMS (Centers for Medicare & Medicaid Services). 2018a. Home- and community-based services.https://www.cms.gov/Outreach-and-Education/American-Indian-Alaska-Native/AIAN/LTSS-TA-Center/info/hcbs.html (accessed August 22, 2018).
CMS. 2018b. MACRA: MIPS & APMs.https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/MACRA-MIPS-and-APMs/MACRA-MIPS-and-APMs.html (accessed August 7, 2018).
CMS. 2018c. MDCR HHA 1: Medicare home health agencies: Persons with utilization, total service visits, total episodes, and total program payments for original medicare beneficiaries, by type of entitlement, calendar year 2011–2016.https://qcor.cms.gov/main.jsp (accessed August 7, 2018).
CMS. 2018d. MDCR providers 5: Medicare providers: Number of medicare certified providers, by type of provider, by state, territories, possessions, and other areas, calendar year 2016.https://qcor.cms.gov/main.jsp (accessed August 7, 2018).
CMS. 2018e. Quality certification and oversight reports. https://qcor.cms.gov/main.jsp (accessed August 7, 2018).
CMS. 2018f. The quality payment program. https://qpp.cms.gov (accessed August 1, 2018).
Donabedian, A. 1966. Evaluating the quality of medical care. The Millbank Memorial Fund Quarterly 44(3):Suppl:166–206. Reprinted in Milbank Q. 2005;83(4):691–729.
GAO (U.S. Government Accountability Office). 2017. Medicare Advantage: CMS should use data on disenrollment and beneficiary health status to strengthen oversight. GAO-17-393. https://www.gao.gov/assets/690/684386.pdf (accessed August 1, 2018).
Hebert, P. L., C. F. Liu, E. S. Wong, S. E. Hernandez, A. Batten, S. Lo, J. M. Lemon, D. A. Conrad, D. Grembowski, K. Nelson, and S. D. Fihn. 2014. Patient-centered medical home initiative produced modest economic results for Veterans Health Administration, 2010–12. Health Affairs (Millwood) 33(6):980–987.
Helfrich, C. D., E. D. Dolan, J. Simonetti, R. J. Reid, S. Joos, B. J. Wakefield, G. Schectman, R. Stark, S. D. Fihn, H. B. Harvey, and K. Nelson. 2014. Elements of team-based care in a patient-centered medical home are associated with lower burnout among VA primary care employees. Journal of General Internal Medicine 29(Suppl 2):S659–S666.
IOM (Institute of Medicine). 1999. Measuring the quality of health care. Washington, DC: National Academy Press.
IOM. 2015a. Dying in America: Improving quality and honoring individual preferences near the end of life. Washington, DC: The National Academies Press.
IOM. 2015b. Vital signs: Core metrics for health and health care progress. Washington, DC: The National Academies Press.
The Joint Commission. 2018. Facts about home care accreditation. https://www.jointcommission.org/facts_about_home_care_accreditation (accessed August 1, 2018).
Kelley, A. S., and E. Bollens-Lund. 2018. Identifying the population with serious illness: The “denominator” challenge. Journal of Palliative Medicine 21(S2):S7–S16.
Kelley, A. S., K. E. Covinsky, R. J. Gorges, K. McKendrick, E. Bollens-Lund, R. S. Morrison, and C. S. Ritchie. 2017. Identifying older adults with serious illness: A critical step toward improving the value of health care. Health Services Research 52(1):113–131.
Li, Q., A. N. Trivedi, O. Galarraga, M. Chernew, D. Weiner, and V. Mor. 2018. Medicare advantage ratings and voluntary disenrollment among patients with end-stage renal disease. Health Affairs 37(1):70–77.
Luetke-Stahlman, H. 2018. HealtheIntent: A peek inside the engine. Presented at Implementing Quality Measures for Accountability in Community-Based Care for People with Serious Illness: A Workshop, Washington, DC.
Meyers, D. J., V. Mor, and M. Rahman. 2018. Medicare Advantage enrollees more likely to enter lower-quality nursing homes compared to fee-for-service enrollees. Health Affairs (Millwood) 37(1):78–85.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2017. Integrating the patient and caregiver voice into serious illness care: Proceedings of a workshop. Washington, DC: The National Academies Press.
National Hospice and Palliative Care Organization. 2018. Hospice care.https://www.nhpco.org/about/hospice-care (accessed August 22, 2018).
NCPQPC (National Consensus Project for Quality Palliative Care). 2013. Clinical practice guidelines for quality palliative care, 3rd ed. Pittsburgh, PA: National Consensus Project for Quality Palliative Care.
NCPQPC. 2018. Clinical practice guidelines for quality palliative care, 4th ed. Richmond, VA: National Coalition for Hospice and Palliative Care. https://www.nationalcoalitionhpc.org/ncp (accessed August 21, 2018).
Nelson, K. M., C. Helfrich, H. Sun, P. L. Hebert, C. F. Liu, E. Dolan, L. Taylor, E. Wong, C. Maynard, S. E. Hernandez, W. Sanders, I. Randall, I. Curtis, G. Schectman, R. Stark, and S. D. Fihn. 2014. Implementation of the patient-centered medical home in the Veterans Health Administration: Associations with patient satisfaction, quality of care, staff burnout, and hospital and emergency department use. JAMA Internal Medicine 174(8):1350–1358.
Pantilat, S. 2018. Palliative care quality network. Presented at Implementing Quality Measures for Accountability in Community-Based Care for People with Serious Illness: A Workshop, Washington, DC.
Partnership Health Plan in Northern California. 2018. Partnership Healthplan of California Quality/Utilization Advisory Committee Meeting Notice, edited by A. Thomas. Partnership Health Plan in Northern California Website. http://www.partnershiphp.org/About/Documents/QUAC/2018/QUAC%20Meeting%20Packet_%2001.17.2018_FINAL.pdf (accessed August 1, 2018).
PCQN (Palliative Care Quality Network). 2018. PCQN members. https://www.pcqn.org/about/pcqn-members (accessed June 25, 2018).
Rahman, M., L. Keohane, A. N. Trivedi, and V. Mor. 2015. High-cost patients had substantial rates of leaving Medicare Advantage and joining traditional Medicare. Health Affairs (Millwood) 34(10):1675–1681.
Teno, J. M., R. Anhang Price, and L. K. Makaroun. 2017. Challenges of measuring quality of community-based programs for seriously ill individuals and their families. Health Affairs 36(7):1227–1233.
VA (U.S. Department of Veterans Affairs). 2017. Centers of Excellence in Primary Care Education Compendium of Five Case Studies: Lessons for interprofessional teamwork in education and workplace learning environments 2011–2016. Washington, DC: U.S. Department of Veterans Affairs. https://www.va.gov/OAA/docs/VACaseStudiesCoEPCE.pdf (accessed August 1, 2018).
VA. 2018. Academic PACT (Patient Aligned Care Team). Office of Academic Affiliations. Washington, DC: U.S. Department of Veterans Affairs. https://www.va.gov/oaa/apact (accessed August 1, 2018).
Zulman, D. M., C. Pal Chee, T. H. Wagner, J. Yoon, D. M. Cohen, T. H. Holmes, C. Ritchie, and S. M. Asch. 2015. Multimorbidity and healthcare utilisation among high-cost patients in the US Veterans Affairs health care system. BMJ Open 5(4):e007771.
Zulman, D., E. Chang, A. Wong, S. Stockdale, N. Pathak, K. Hedrick, J. Yoon, M. Ong, L. Rubenstein, and S. Asch. In press. Randomized evaluation of intensive outpatient management for high-need veterans: Effects on patient experience. Paper presented at AcademyHealth, Seattle, WA.
This page intentionally left blank.
















































































