
4
Managing the Global Epidemic: Challenges and Cross-Cultural Insights
Rachel Nugent, vice president for noncommunicable diseases (NCDs) at RTI International, returned to moderate the workshop’s third session. In this session, three speakers explored in greater depth the challenges and cross-cultural insights associated with efforts to prevent and control obesity.
NAVIGATING THE OBESITY EPIDEMIC: THE MEXICO EXPERIENCE
Simón Barquera, director of the Nutrition and Health Research Center at the Mexican National Institute of Public Health, discussed some of the challenges associated with Mexico’s efforts to prevent and control obesity. He noted that the country’s prevalence of overweight and obesity has been increasing since measurement began in 1999, and is currently at nearly 73 percent. Relatedly, he observed, Mexico’s mortality attributable to diabetes (9.34 percent) is among the highest in the world (GBD 2013 Mortality and Causes of Death Collaborators, 2015). In 2016, the Mexican government declared the diabetes epidemic a national health emergency, he said, explaining that this epidemiological alert was the first one Mexico had issued for an NCD.
Barquera highlighted what he characterized as successful initiatives to help prevent and control obesity in Latin America, including a soda tax implemented in Mexico in 2014 and later in Chile, Ecuador, and Peru. He cited evaluation data for Mexico’s soda tax showing a reduction in purchases of sugar-sweetened beverages that was sustained 2 years after the tax had been implemented and averaged 7.6 percent (Colchero et al., 2017). This may sound like a small effect, he observed, “but in a country of 126 million inhabitants, this represents about 67,000 tons of sugar that were not consumed in these 2 years.” Mexico’s soda tax model has been used in other countries, he added, and it will continue to be refined. He also highlighted contrasts in the packaging of the same cereal product in Mexico and in Chile, noting that Chile has stricter front-of-package regulations.
Barquera cited several challenges for obesity prevention efforts in Latin America: the presence of the double burden of malnutrition and inequalities in obesity prevalence associated with socioeconomic status (see Chapter 2), scarce resources to invest in obesity prevention and in evaluation of interventions, and primary health care systems that were created when infectious diseases were the main concern and thus lack the resources to handle chronic diseases.
Barquera highlighted as another challenge that Mexico experiences interference from industry, such as aggressive marketing of unhealthy foods in poor communities. He pointed out that healthy foods such as fruits and vegetables are inexpensive in Mexico, so to sell junk foods and soft drinks, Mexican companies are more aggressive than those in other nations. He cited results of an evaluation in five countries that found point-of-purchase advertisements directed at children in a higher proportion of low-income than high-income stores. These type of advertisements are common, he observed, and include cartoon characters on packages, price discounts, and free gifts. And they work, he noted, because sugar-sweetened beverages
and sweet and salty snacks are the top products customers reported buying without prior planning.
Considering opportunities in obesity prevention in Latin America, Barquera explained that the obesity problem has high political visibility in the region. He explained that close connections among the region’s countries have led to a domino effect for some policies as countries have consulted with each other. Because many cost-effective interventions to prevent obesity do not involve expensive technology, he added, they can be replicated in low- and middle-income countries worldwide.
Barquera then shifted his attention to front-of-package nutrition labels as a strategy for helping consumers make healthier food choices. He contrasted the Guideline Daily Amount (GDA) label system developed by the food industry in Mexico with Chile’s warning label system, which was developed by academics (see Figure 4-1).
The GDA label is complex, misleading, and difficult to interpret in making food decisions, Barquera argued. He cited research suggesting that this label is not well understood by Mexican nutrition students at the university level (Stern et al., 2011), and that only 13.8 percent of respondents in a Mexican national survey said they understood it. In a multinational survey of high-income populations, 54 percent responded that they understood the GDA label, while 83 percent responded that they understood the warning label, he reported. That study also found that lower-income populations had a lower probability of understanding and using the GDAs to make healthier choices, he added. The warning label is easily interpreted,
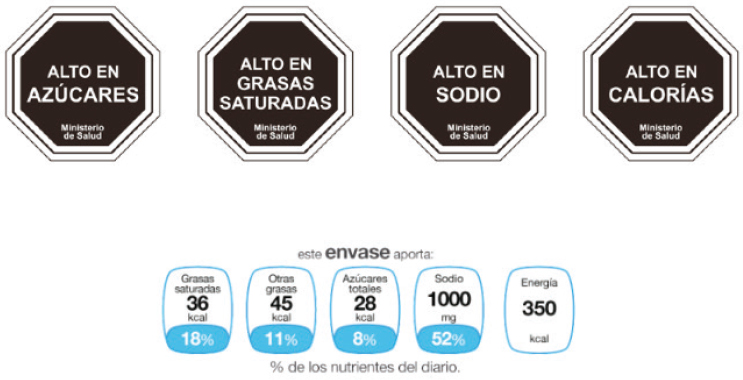
SOURCE: Presented by Simón Barquera, October 9, 2018.
he argued. “In Chile, even the kids know that when they have this octagon, it means that there is something wrong with the product. It’s high in something.”
Barquera then turned to the Mexican Observatory for Obesity, describing it as a government-appointed advisory council that makes decisions about obesity prevention actions in Mexico. About half of the council members are associated with the food industry, he said, adding that these members opposed public health and obesity prevention initiatives that were submitted to the council. He stated that he and his colleagues have tried to expose this coordinated response of opposition by publishing evaluations of “how the process goes when you have this kind of interference from industry” (Barquera et al., 2018).
The Mexican National Institute of Public Health convened what Barquera called a “conflict of interest–free” group of academics to make evidence-based recommendations for front-of-package labeling. The group observed that the GDA label is not an effective system for promoting healthier choices, he reported, and it suggested that a front-of-package label could be simple and based on established national or international nutrition standards. Barquera noted that the group’s report will be presented to Mexico’s incoming national political administration.
Barquera moved on to describe the Mexican health system’s lack of capacity for obesity prevention and control. The country’s total health budget is relatively low, he observed, and he characterized the proportion of the budget dedicated to chronic disease prevention as inadequate (Barquera and White, 2018). He asserted further that physicians are not adequately trained to screen for and treat obesity, and there are not enough specialists to whom patients can be referred. He argued that major adjustments in the budget and in the organization of health services could control the spread of obesity with effective treatment.
Barquera ended by calling for (1) the promotion of “double-duty policies” that can affect both undernutrition and obesity, with a focus on groups of low socioeconomic status (see Chapter 2); (2) refinement of tax policies and implementation of other regulations to improve obesogenic environments; and (3) mitigation of industry interference, particularly from multinational companies, in the decision-making parts of the system. “We need to speak out about this,” he concluded, “because many of these companies say they want to be part of the solution in international meetings . . . but at the local level, they are really part of the problem and they are not willing to accept any type of regulation or attempt of the government to improve the environment.”
COMMON THREADS IN OBESITY RISK AMONG RACIAL/ETHNIC AND MIGRANT MINORITY POPULATIONS
Shiriki Kumanyika, research professor in the Department of Community Health and Prevention, Drexel Dornsife School of Public Health, Drexel University, and emeritus professor of epidemiology, Perelman School of Medicine, University of Pennsylvania, shared cross-cultural insights about populations at above-average risk for obesity within high-income countries.
Kumanyika took a health inequities perspective in her presentation, exploring common threads in obesity risk among racial/ethnic and migrant minority populations. Pointing out that racial/ethnic minority status is associated with above-average obesity risk compared with white majority populations, she asserted that examining patterns of obesity risk in populations of color in different country contexts can lead to new insights and potentially to solutions (Kumanyika et al., 2012). For context, she noted that population-wide increases in obesity are driven by societal forces—and the policies governing them—that relate directly or indirectly to food systems or physical activity and converge to make it difficult for people to control their weight. Apparently, she continued, within high-income countries these forces operate differentially for minority populations, and the question is why.
Kumanyika went on to review data on obesity prevalence stratified by racial/ethnic group for adults in Australia, England, the Netherlands, New Zealand, and the United States (Australian Bureau of Statistics, 2013; CDC, 2016; Hales et al., 2017; New Zealand Ministry of Health, 2018; Public Health England, 2016; Schmengler et al., 2017). She highlighted a tendency toward higher obesity prevalence in minority populations of color relative to reference or host populations in these countries, especially among women. She also flagged the lower prevalence of obesity in Asian populations in these countries and reminded the audience that the data are based on a body mass index (BMI) cutoff of 30. Referencing the discussion of ethnic-specific BMI cutoffs in session 1 of the workshop (see Chapter 2), she expressed concern about the continued use of this cutoff for obesity in Asian populations, arguing that it will yield “an answer that’s misleading in terms of health risk.”
Kumanyika proceeded to observe that, according to longitudinal studies, migrants’ lower weights yield to excess weight gain over time. This phenomenon is sometimes attributed to acculturation or studied as a matter of duration of residence in the host country, she noted, adding that cross-national studies within these ethnic groups point to effects of Western environments compared with the environments in migrants’ countries of origin. “These data have been critical to refute the idea of default genetic explanations,” she explained, because the finding that people with the same
general genetic background have higher weights when living in different circumstances suggests a role for nongenetic (i.e., environmental) factors. Accordingly, she observed, environmental explanations now dominate the discussion. She added that cross-national studies within Western environments indicate effects of national contexts, and she reminded participants of Meeks’s data on the differences among Ghanaian populations living in three European cities (see Chapter 2).
Kumanyika went on to identify one key question to consider: What is different about minority populations of color compared with host or reference populations? She then cited a second key question: What is similar in different societies with respect to minority populations of color? She noted that these questions are important to explore for children as well as adults but are much more complex, pointing out that in children, one must account for weight gain patterns during growth and development in relation to age at migration, among other factors.
Kumanyika paused to consider historical aspects of the collection of data on race and ethnicity. She suggested that when such data are collected, the implication is that the data have societal importance, such as relevance for policy making. She pointed out that the collection of racial and ethnic data is routine in the United States, although the categories used in the research evolve. In contrast, she said, Europe has in the past been reluctant to collect data on residents’ ethnicity, preferring “color blindness” and distinguishing health inequities by social class (Loring and Robertson, 2014; Simon, 2012). She noted, however, a recent movement toward collecting racial and ethnic data based on their importance to health policy.
Kumanyika then referenced a World Health Organization (WHO) Commission report on ending childhood obesity (2016b), which makes the point that effects of socioeconomic status in high-income countries differ from those in low- and middle-income countries. In high-income countries, she explained, risks of childhood obesity are greatest among groups of lower socioeconomic status, but the converse is true in most low- and middle-income countries, although these patterns are becoming more complex. Within high-income countries, certain population subgroups (such as migrant and indigenous children) are at particularly high risk of obesity, she elaborated, which the WHO report attributes to rapid acculturation and poor access to public health information. However, Kumanyika emphasized that these two factors are only a part of the story of how environmental factors operate differentially in these subgroups.
Kumanyika then turned her attention to potential influences on obesity in minority populations of color (which include migrant groups), citing the following variables: racial/ethnic category, socioeconomic status and social position, migration and migration stress, language and literacy, cultural assets, structural empowerment and resilience, and stress. For each set of
variables, she discussed the associated contextual factors that might influence weight (see Table 4-1). She pointed out that although stress is listed separately, it is highlighted because its influence is moderated through pathways related to all of the other variables.
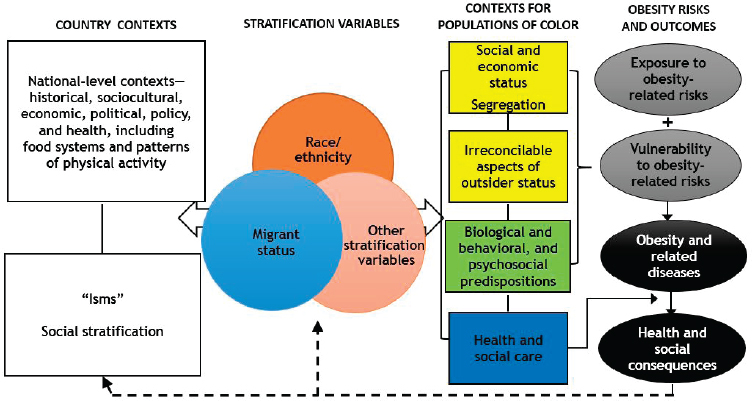
Finally, Kumanyika described her framework for depicting pathways that produce racial/ethnic and migrant inequities in obesity, along with potential intervention points (see Figure 4-2). She hypothesized an intersection among race/ethnicity, migrant status, and any other stratification
TABLE 4-1 Potential Influences on Obesity in Minority Populations of Color
| Variable | Contexts |
|---|---|
| Racial/ethnic category (explicit or implicit, i.e., not being white) |
|
| Socioeconomic status; social position |
|
| Migration and migration stress |
|
| Language/literacy |
|
| Cultural assets and protection |
|
| Structural empowerment and resilience |
|
| Stress |
|
NOTE: Stress is highlighted to denote that its influence is moderated through pathways related to all of the other variables.
SOURCES: Adapted from Kumanyika, 2018. Presented by Shiriki Kumanyika, October 9, 2018.
variables that apply in a country to determine health inequities, as outlined in the WHO conceptual framework for action on the social determinants of health (Solar and Irwin, 2010). These inequities, she explained, then condition the social determinants of health (such as neighborhood of residence and access to health care).
Kumanyika ended by reiterating that obesity is often more prevalent in racial and ethnic minorities and migrants versus reference or host populations, and that race/ethnicity and migration intersect. She suggested that studying these patterns in diverse high-income countries could yield new insights to inform policy actions. She challenged the audience to consider that “if the pathways arise solely or in part from social stratification, then the ultimate solutions to this excess risk in populations of color require a major disruption in the ‘isms’ that got [us to] where we are today.”
THE CONTRIBUTION OF TRADITIONAL CULTURES TO RESOLVING THE OBESITY PANDEMIC
Harriet Kuhnlein, emerita professor at McGill University, focused on Indigenous Peoples as she explored how traditional cultures can inform solutions for the obesity pandemic. Although many countries lack census data disaggregated by ethnicity, she began, the United Nations has on record 370 million Indigenous and tribal people in more than 90 countries, repre-
SOURCES: Adapted from Kumanyika, 2018. Presented by Shiriki Kumanyika, October 9, 2018.
senting 5,000 identified groups and about 4,000 languages. These people are among the poorest in the world, she observed, and face intractable poverty, racism, and discrimination. They also have lower life expectancy; less access to education, employment, and standard housing; and more violence and incarceration. The United Nations has recognized that their marginalization is due to violation of their right to traditional lands and territories, Kuhnlein added (UN, 2009, 2013, 2017b).
According to Kuhnlein, researchers look to Indigenous Peoples in rural areas to gain insights as to what their food systems might offer in terms of obesity solutions because of their connectedness to nature. They have inhabited their territories for long periods of time, she elaborated, so they have been sustainable with their food systems. And based on the limited information available, she added, “we recognize that most of these people were not obese.” Indigenous Peoples’ knowledge of food systems is derived from their collective experience in managing 22 percent of the world’s ecosystems and land mass, she explained, as well as understanding the planet’s animal and plant natural resources and preserving much of its biodiversity (Burlingame and Dernini, 2019).
Kuhnlein described a study of the local food resources of 12 cultures, reporting that the researchers discovered unique and delicious foods with surprising nutrient values. They tallied the number of species used as food in each culture, finding that it reached nearly 400 in some tropical locations. Based on dietary records collected in the field, Kuhnlein noted, those traditional local foods represented anywhere from 10 to 98 percent of the energy consumed by people in these 12 cultures (Kuhnlein et al., 2009). The researchers also learned how those foods are being lost to global agricultural and food marketing practices (Kuhnlein et al., 2009, 2013).
Kuhnlein stressed that the loss of indigenous food system knowledge poses a number of risks. Those risks include habitat destruction and ecosystem threats such as resource (e.g., oil) extraction, land grabs, and climate change, in addition to displacement from indigenous territory, loss of language and culture, urbanization and migration of knowledge holders and youth, acceptance of more commercial foods, and loss of seeds and wildlife (Kuhnlein et al., 2009, 2013; UN, 2009, 2013, 2017b).
Kuhnlein then transitioned to discuss current statistics on obesity and stunting among Indigenous Peoples. Citing data from the Centers for Disease Control and Prevention (CDC), she stated that nearly 75 percent of American Indian and Alaska Native adults have overweight or obesity, compared with about 61 percent of non-Hispanic white adults (CDC, 2017b). However, the prevalence of diabetes among these adult indigenous peoples is more than double that among their non-Hispanic white counterparts (17.6 versus 7.3 percent), she pointed out (CDC, 2010). She added that the figures for adolescent overweight and obesity are similar for
indigenous populations and non-Hispanic whites, and suggested further research to track when those numbers diverge. Turning to undernutrition, she referenced census and health data from Brazil, Colombia, India, and Peru, revealing that the prevalence of stunting in children less than 5 years of age is much greater among indigenous populations than benchmark populations in each country (Anderson et al., 2016).
Kuhnlein asserted that a systems approach is key to preventing obesity in Indigenous Peoples, as is understanding the ecology and the environment in their home territories. She highlighted self-determination as an element that can lead to sustainable food systems, food security, and health. To build capacity for self-determination, she called for using community-specific information as a platform for health promotion activities; respecting indigenous ways of knowing and being; and recognizing the “global megaforces” that undermine Indigenous cultures, as well as the historical trauma that those cultures have experienced. She also stressed the importance of helping these communities understand the nutrient composition of their foods and the impact of a transition to commercial foods. At the same time, however, she cautioned that “the impact of our education and awareness can be swamped out by the larger ecological factors such as poverty or food access.”
Kuhnlein then shared Lemke and Delormier’s (2017) views on how to meet the challenges of obesity in Indigenous Peoples: (1) decolonize public health programs to express holistic worldviews to prevent obesity and undernutrition; (2) use the Indigenous values of respect, responsibilities, and relationships to each other and to nature; (3) recognize locally specific conditions and the broader historical, political, cultural, economic, and environmental contexts; and (4) build the indigenous public health workforce to promote well-being based on human rights, and rebuild cultural morale with local practices.
According to Kuhnlein, Indigenous Peoples’ experience can inform strategies for combating the obesity epidemic to the extent that researchers document and learn from their health strategies and the diversity of their food systems. “Indigenous Peoples understand that food use touches everything,” she remarked, including mental, physical, social, and spiritual well-being. She proposed building an international platform for gathering knowledge of traditional and Indigenous holistic food systems and health systems with ecological sustainability, and urged intercultural education as a way to help resolve the obesity pandemic.
DISCUSSION
A brief discussion period followed this third session of the workshop. Topics included co-creation of strategies for addressing obesity in minority
populations of color, acculturation, building an international knowledge platform, and globalization and global megaforces.
Co-Creation of Strategies for Addressing Obesity
A participant observed that the influences on obesity in minority populations, as outlined by Kumanyika, are serious problems in and of themselves. She asked Kumanyika how to ensure that these populations consider obesity a priority. Kumanyika suggested engaging with a community and learning about its members’ priorities to build on their “insider knowledge and experience” in devising a sustainable solution, co-created with community members. This does not necessarily mean starting from the beginning and ignoring the interventions already developed, she clarified. However, she said, trying to just tweak an existing intervention to fit the community is too superficial, “so the movement toward co-creation could probably open some new doors.”
Acculturation
Acculturation is a survival strategy for most populations that are migrating, a participant stated. She asked whether factors exist that are typically positive or negative with regard to obesity that are present as migrants acculturate. Kumanyika replied that both positives and negatives are related to the acculturation process, but suggested that it is problematic to use acculturation as the primary explanation for high obesity risk. A singular focus on acculturation, which is common, she elaborated, places the emphasis on how migrants are reacting without looking at how they are viewed and treated in the society. According to Kumanyika, acculturation implies that people may attempt, sometimes seemingly “against all odds,” to integrate into a community, but what she termed their “irreconcilable outsider status” can make those attempts counterproductive in some respects. She proposed that it may be more productive for people to retain their cultural group perspectives and leverage the associated strengths, but acknowledged that the topic is extremely complex.
Kuhnlein recounted her experience broaching the topic of obesity with Indigenous Peoples in British Columbia. She recalled that they asked, “Oh, you want to deculturize us?” She emphasized the importance of allowing people to recognize their strengths and find solutions from within those strengths.
Building an International Knowledge Platform
A participant asked Kuhnlein to elaborate on her suggestion about building an international knowledge platform. Kuhnlein replied that some
cultures want to handle obesity in their own way, while others are more interested in learning from others. In any case, she suggested that the many ideas about promoting consumption of healthy food are worth documenting, and noted that the Food and Agriculture Organization is building a platform to record Indigenous experiences.
Globalization and Global Megaforces
The impact of globalization on food and physical activity patterns throughout the world is apparent, observed a participant. He asked what Indigenous Peoples can teach others about how to decolonize from the globalized food economy. Kuhnlein agreed that Indigenous Peoples can offer wisdom about how to effect change within their own communities. She advised public health practitioners to conduct formative research in communities of interest, arguing that doing so is useful for building a good public health promotion program.
Nugent asked Barquera to elaborate on how Mexico is handling global mega-forces in its local obesity prevention efforts. Barquera replied that, because Mexico is a large market, lobbying efforts to oppose public health policies have been strong. As an example of how globalization of trade has impacted obesity prevention efforts, he cited the recent negotiation of a global trade agreement in North America, which included an attempt to limit countries’ power to require warning labels on food products. This attempt was ultimately defeated, he noted, because public health and civil society groups spoke up. He added that countries with smaller economies may not experience as much opposition from multinational companies, and thus may have an easier time implementing regulations.












