
Suicide is the 10th leading cause of death in the United States (see Figure 2-1), and among young people ages 10 through 34 it is the second leading cause, observed Holly Wilcox, associate professor in the Johns Hopkins Bloomberg School of Public Health’s Department of Mental Health and the Johns Hopkins University School of Medicine’s Department of Psychiatry, in her overview of patterns of risk and the prevention landscape at the workshop. Beginning in adolescence, which is also an important developmental stage for the onset of mental illness, suicide becomes more common in males than in females (see Figure 2-2). In contrast, women typically report more suicide attempts than men. Men are more likely to use highly lethal means in a suicide attempt such as firearms. The economic impact of suicidal behaviors has been estimated to exceed $90 billion annually in the United States, mostly due to lost productivity (Shepard et al., 2016).
Firearms account for the majority of suicides in the United States (see Figure 2-3), and 60 percent of firearm deaths are by suicide. A promising new development, said Wilcox, is that 13 states have current legislation planned or in place for extreme risk protection orders, which give family members, first responders, and, in some instances, health care professionals the opportunity to petition to restrict purchase or possession of firearms by those who are deemed to be dangerous to self or others.
Case and Deaton (2017) found that the cohort of Americans who were born around 1950 and entered the workforce around 1970 have had particularly high suicide rates, which points to the toll that economic conditions may have on suicide risk, said Wilcox. This increase has been especially notable for men and women with a high school degree or less, though the rates have also increased, although to a lesser extent, for people with a 4-year college degree or more. To illustrate this point, Wilcox presented Figure 2-4.
According to data from the Centers for Disease Control and Prevention (CDC), the number of suicides in the year 2016 in the United States was approximately 45,000 (Stone et al., 2018). Stone et al. (2018) using
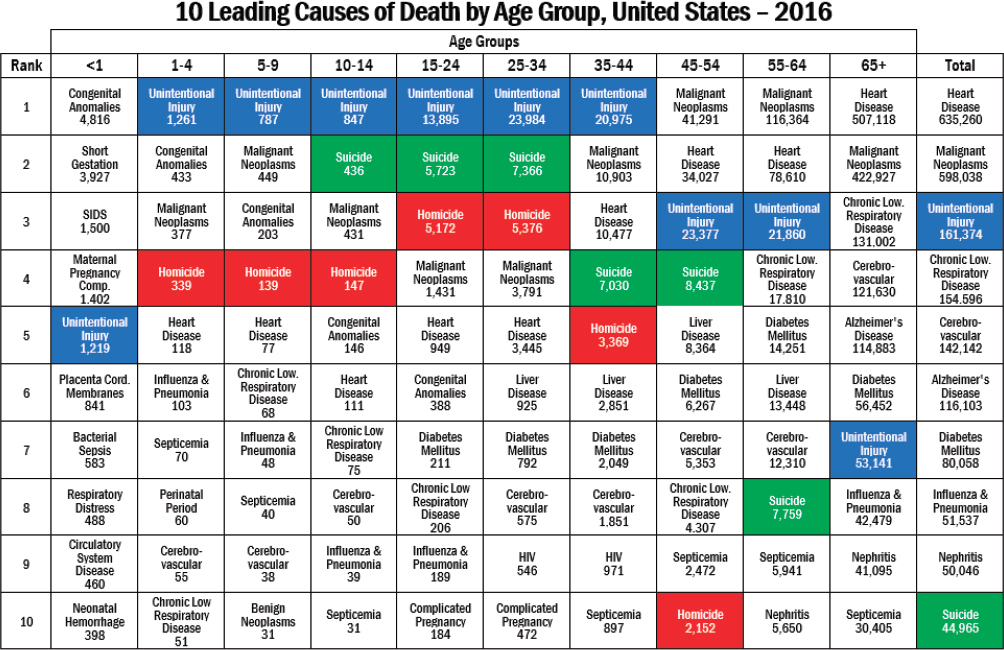
NOTE: HIV = human immunodeficiency virus; SIDS = sudden infant death syndrome.
SOURCES: Presented by Holly Wilcox on September 11, 2018, at the Workshop on Improving Care to Prevent Suicide Among People with Serious Mental Illness. From Centers for Disease Control and Prevention Web-based Injury Statistics Query and Reporting System data.
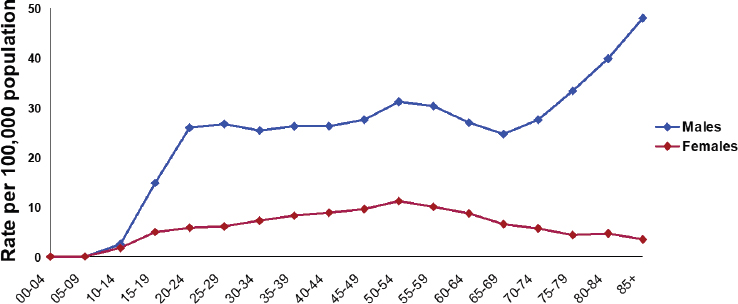
SOURCES: Presented by Holly Wilcox on September 11, 2018, at the Workshop on Improving Care to Prevent Suicide Among People with Serious Mental Illness. Data from National Vital Statistics System, National Center for Health Statistics, CDC.
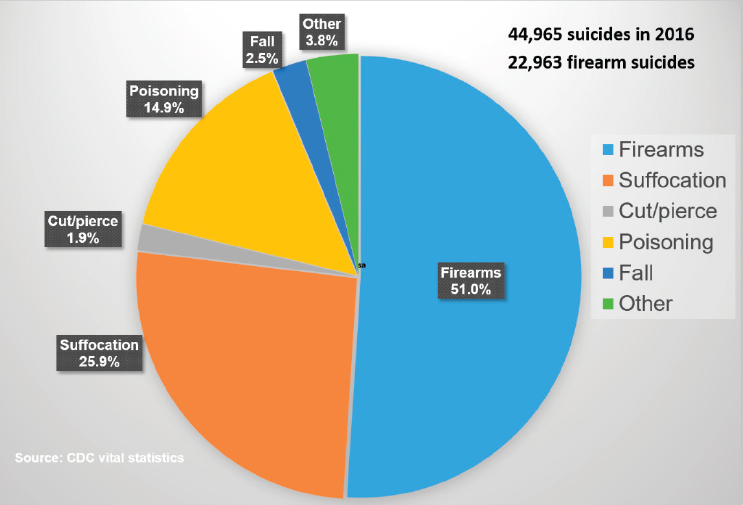
SOURCES: Presented by Holly Wilcox on September 11, 2018, at the Workshop on Improving Care to Prevent Suicide Among People with Serious Mental Illness. Data from National Vital Statistics System, National Center for Health Statistics, CDC.
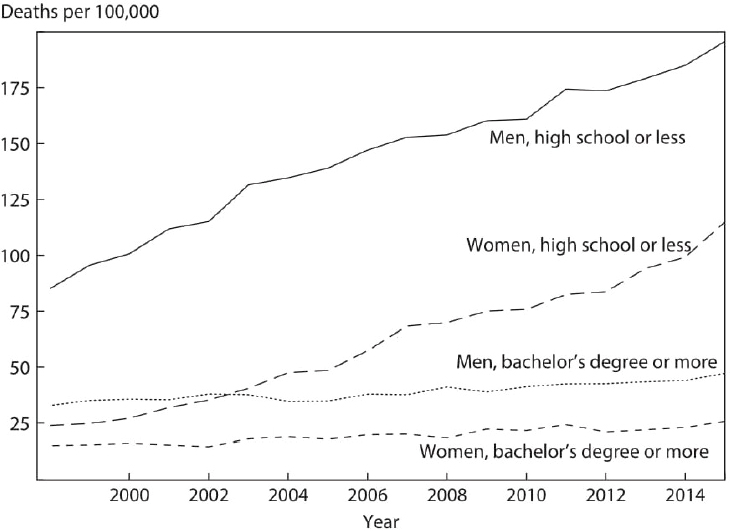
SOURCES: Presented by Holly Wilcox on September 11, 2018, at the Workshop on Improving Care to Prevent Suicide Among People with Serious Mental Illness. From Case and Deaton (2017), used with permission.
the National Violent Death Reporting System to examine demographic and descriptive characteristics and contributing circumstances to suicide among people with and without known mental health conditions, found that suicide rates had increased by 30 percent or more since 1999 in more than half the 27 states examined. Stone et al. also found that, among those who died by suicide, 54 percent of people did not have a known mental health condition. This seemingly contradicts the conclusions from several studies based on psychological autopsy, Wilcox noted, which have found that more than 90 percent of people who die by suicide have at least one type of psychiatric disorder at the time of death, whether diagnosed or not (Cavanagh et al., 2003). Both are important pieces of information, and the actual number is likely somewhere in between, said Wilcox. The National Violent Death Reporting System does not actively assess for psychiatric status at the time of death, thus reflecting only what has otherwise been reported. When family members and others respond to psychological autopsies the information can indicate the presence of unreported psychiatric diagnoses, but in the context
of losing a loved one to suicide family members may also overreport the extent of mental health concerns the individual had.
Studies that have examined the percentage of suicide attempts attributable to specific mental health disorders in nationally representative samples have noted that although many mental illnesses were associated with suicide attempts, elevated rates were mostly attributed to the presence of major depressive disorder, borderline personality disorder, nicotine dependence, and post-traumatic stress disorder (Bolton and Robinson, 2010). A whole population study from Sweden that studied risk for suicide after hospitalization for suicide attempts found that the risk and timing of suicide was particularly strong for people with unipolar and bipolar depression and schizophrenia, particularly among males (Tidemalm et al., 2008). This study underscored the need for more focused care during the first 2 years after a suicide attempt.
PUBLIC HEALTH AND SYSTEMS-LEVEL INITIATIVES
A public health initiative that was effective for a period of time in reducing suicides is the U.S. Air Force Suicide Prevention Program, said Wilcox. It is a comprehensive, system-level strategy with 11 components (Knox et al., 2010):
- Leadership involvement
- Professional military education
- Guidelines for commanders on use of mental health services
- Community preventive services
- Community education and training
- Investigative interview policy
- Trauma stress response team
- Integrated Delivery System (IDS) and Community Action Information Board (CAIB)
- Limited Privilege Suicide Prevention Program—Patients at risk for suicide are afforded increased confidentiality
- IDS Consultation Assessment Tool (originally the Behavioral Health Survey)
- Suicide Event Surveillance System
From a suicide rate in 1994 of 16.4 per 100,000 people, the rate dropped to 9.4 in 1998 after the suicide prevention program was implemented across the service. However, the rate went back up to 20.5 in 2015, despite the program’s existence. This regression draws attention to the need for attention to the quality of implementation and continued support for interventions and monitoring, Wilcox said.
Another systems approach took place in the United Kingdom and included nine evidence-based components (While et al., 2012):
- Inpatient psychiatric unit safety
- Assertive outreach team
- 24/7 crisis team
- 7-day follow-up
- Written policy on nonadherence
- Dual diagnosis treatment
- Criminal justice sharing
- Debriefing and family contact after suicide
- Frontline clinical staff trained in management of suicide risk at least every 3 years
Mental health systems were encouraged to introduce as many of these components as possible. Those that implemented seven to nine components had significantly lower suicide rates than those implementing fewer components. Particularly effective approaches were 24-hour crisis teams that were able to intervene in crises, managing patients with dual diagnoses, and multidisciplinary reviews after suicides that shared information with families.
This work is especially relevant in the United States, as limited access to care is likely a contributing factor to the increasing U.S. suicide rate, Wilcox continued. The number of psychiatric beds in the United States has dropped in the past two decades even as the suicide rate has increased (Bastiampillai et al., 2016). This highlights the importance of high-quality community-based mental health services, said Wilcox.
Wilcox particularly emphasized the need to use data to inform suicide prevention. The combined effect of multiple risk and protective factors needs to be assessed in real time (Franklin et al., 2017). In addition, data linkage and predictive analytics with machine learning can identify those at risk and evaluate as well as identify the most effective policies and programs in reducing suicide, though privacy protection for individuals is a concern. Examples of projects using data to inform suicide prevention include approaches applied to U.S. veterans (McCarthy et al., 2015), the U.S. Army (Kessler et al., 2015; Nock et al., 2018), and health care patients (Tran et al., 2014; Simon et al., 2018).
Treatments targeting depression and anxiety in childhood and adolescence have been shown to reduce future risk for suicide ideation and attempts (March et al., 2006; Wolk et al., 2015). In addition, family and school-based universal prevention programs implemented as early as first grade reduce the incidence of suicidal ideation and attempt more than a decade later (Hawkins et al., 2005; Wilcox et al., 2008; Wasserman et al.,
2015; Connell et al., 2016). These interventions, Wilcox said, are highly practical, sustainable, and cost-effective and prevent multiple outcomes at a population level while producing cost savings for taxpayers and society.
Many policies and programs exist that simultaneously reduce or prevent addiction and multiple domains of violence, including suicide. Examples include evidence-based early childhood universal prevention programs (Hawkins et al., 2005; Wilcox et al., 2008; Connell et al., 2016); restricting firearm access, though vague definitions and enforcement can be challenging, Wilcox acknowledged (Kellerman et al., 1992; Miller and Hemenway, 2008; Miller et al., 2013; Anglemyer et al., 2014; Crifasi et al., 2015; Wintemute, 2015); maltreatment interventions such as early childhood home visitation programs (Hahn et al., 2003; Bilukha et al., 2005); and family-based policies such as divorce and child custody laws (Stevenson and Wolfers, 2006; Halla, 2013). A particular example Wilcox cited is the Good Behavior Game, which has demonstrated that it can reduce not only suicidal behaviors but other forms of violence and negative outcomes as well. Furthermore, the Good Behavior Game has been estimated to produce a return of more than $64 for every dollar invested in terms of long-term outcomes such as increases in high school graduation and prevention of the incidence of adverse mental health and behavioral outcomes.
Comprehensive system-wide programs can prevent suicide (Knox et al., 2003; McCarthy et al., 2009; While et al., 2012; Cwik et al., 2016), but they need to be embedded within systems to be sustained and they require attention to the quality of implementation, Wilcox said. Supportive contacts after being treated for a suicide attempt during the return to the community are also critical, with peer-to-peer approaches showing strong potential for being effective.
Wilcox also pointed out, in response to a question, that demonstrating the effect of specific suicide prevention programs can be difficult. Large studies are needed, since suicide is still a relatively infrequent outcome.
PERCEPTIONS AND AWARENESS OF SUICIDE PREVENTION
Public perceptions around mental health and suicide prevention have been undergoing dramatic changes, said Christine Moutier, chief medical officer of the American Foundation for Suicide Prevention, who also presented an overview of suicide prevention programs and policies during the workshop’s first panel. First, the science informing mental health, psychology, psychiatry, neuroscience, and suicide has been growing rapidly in recent decades, and the results of that science are being disseminated and promoted much more actively. As just one example, the idea that mental health exists on a continuum, as for other aspects of health, is much more widely understood, though this idea still needs to be more widely disseminated, she said.
At the same time, the suicide prevention movement has gained momentum as organizations, advocates, and others who have who have been personally affected by suicide have spoken out. In addition, the field of suicide prevention is characterized by much more collaboration and consensus on effective strategies than has been the case in the past, which has helped shift public attitudes. According to a recent Harris poll sponsored by the American Foundation for Suicide Prevention and the National Action Alliance for Suicide Prevention, nearly 90 percent of people view physical and mental health as equally important, 93 percent of people would do something to help if someone close to them was thinking about suicide, and 96 percent of people think suicide is preventable. People also said that they would not be sure of what to do or say, Moutier added, so they need more knowledge.
Another shift Moutier identified as important is in the words people use to refer to suicide. In 2016 the Associated Press changed its stylebook. Its guidance is to avoid the phrase commit suicide and instead say died by suicide or ended his or her life and to say that someone attempted suicide instead of referring to a successful or failed suicide attempt. Another sign of a changed culture is rapid growth of the Out of the Darkness community, campus, and overnight walks, which began as a fledgling awareness and fundraising activity 15 years ago and have grown tremendously. “They started at a time when families and people were not sure that they could say the word suicide out loud in public,” said Moutier. “Now hundreds of thousands of people are coming out to use their voice and to raise awareness.”
On this point, Moutier added, in response to a question, that people in the field are seeing the use of language start to change. For example, after Anthony Bourdain’s and Kate Spade’s suicide deaths in June 2018, many more interviews with journalists started with requests to get the language right. “There’s clearly a progression going on with regard to awareness about that. It doesn’t mean they’re always getting it right, of course, but there does seem to be movement in that regard.”
Since 2006, continued Moutier, 32 states have passed laws mandating K–12 teacher training, and 18 states have enacted laws governing prevention and postvention in K–12 schools since 2012. States have also passed laws covering suicide prevention in health care training and in higher education. States have been calling for the enforcement of the federal law requiring parity for mental health benefits, and 13 federal laws have passed over the last decade involving suicide prevention.
As an example of how education of community and family members is occurring, Moutier briefly described the American Foundation for Suicide Prevention’s Talk Saves Lives program, which has been delivered to tens of thousands of people in all 50 states. A sort of suicide prevention 101, the Talk Saves Lives program tells people that suicide is a health issue and that
suicide can be prevented. It teaches people about the scope and epidemiology of suicide, about the risk factors demonstrated by research to drive up suicide risk, and about effective suicide prevention. The program teaches people about limiting access to lethal means through carbon dioxide sensors in cars, barriers on bridges, blister packaging for medications, firearm controls, and other means, especially during periods of risk. It disseminates educational materials at walks, health fairs, workplaces, and clinics. Examples of educational materials available from the American Foundation for Suicide Prevention include “After a Suicide Attempt,” “Firearms and Suicide Prevention,” and “After a Suicide.”
This education effort, Moutier said, shows that everyone has a role to play in suicide prevention and culminates in the message that people should bring those who are at risk for suicide to a health care provider, “just as we want people to come to health care settings at the earliest indication that they might have diabetes or any other kind of health problem.” Just as for other health problems, health care systems need to know what to do and deliver care for people at the earliest stages of deterioration in mental health or increase in suicide risk.
TREATMENT AS A PART OF SUICIDE PREVENTION
Moutier described several innovations in clinical treatments that are related to suicide prevention. First, several newly developed and evidence-based ways to reduce the risk of suicide are now available. For example, brief interventions are now being widely used, such as safety planning and lethal means counseling, that can be done during a single outpatient or emergency department visit. Treatments and peer support are now available online, and predictive analytics are being used to guide treatment and outreach. Such interventions have been shown to reduce the risk of suicide and need to be made much more accessible to the public, she said.
Health care systems need to consider suicide a health-related outcome and measure indicators related to suicide, she added. Critical windows exist for suicide risk, including the week after a psychiatric admission, the week after a psychiatric discharge, discharge from an emergency department following presentation for suicidal ideation or attempt, and the first weeks after starting an antidepressant (see Figure 2-5). Other periods of transition, such as a soldier transitioning to civilian status or a middle-aged man changing jobs or getting divorced, also have proven to be times of increased risk.
Several psychotherapies have been shown to reduce the risk of suicide; Moutier described two in detail. Dialectic behavioral therapy (DBT) has been evaluated in several landmark studies involving people with borderline personality disorder, substance use disorders, and eating disorders;

SOURCES: Presented by Christine Moutier on September 11, 2018, at the Workshop on Improving Care to Prevent Suicide Among People with Serious Mental Illness. Used with permission from Elizabeth Ballard.
prepubescent children with disruptive mood dysregulation disorder; and adolescents with a suicide attempt history. For example, Linehan et al. (2006) conducted a randomized controlled trial of 101 women with borderline personality disorder who had recently attempted suicide. They were randomized into one of two groups and followed for 2 years. One group received DBT, while the other group received community expert therapy. The rate of reattempt was about 50 percent lower among the women who received DBT, and they had significantly fewer hospitalizations.
In a study of cognitive behavioral therapy (CBT), Brown et al. (2005) randomized 120 adults seen in an emergency department after a suicide attempt to either 10 sessions of CBT versus enhanced treatment as usual in the community. The study targeted the suicidal cognitions of these individuals, who were followed for 18 months. The participants who received CBT were 50 percent less likely to reattempt suicide than the usual care group, and their depression scores were significantly lower than the usual care group. “I want you to note that they had the same rate of suicidal ideation, so people can live with suicidal thoughts,” said Moutier, adding:
But the quality of their mental health and their behavior changed significantly. This is a new way to think about it. For many clinicians, we have not learned these things and have avoided honing in on our patient’s suicidal thoughts. . . . This needs to start being incorporated as a part of treatment.
In a study of brief cognitive behavioral therapy, Rudd et al. (2015) customized CBT for a group of army soldiers who were either postsuicide attempt or had suicidal ideation with intent. Over a 2-year follow-up
period, the group that received the brief CBT had a 60 percent lower risk of suicide attempts. On a larger scale, a meta-analysis of CBT targeted at suicidal ideations and behaviors found that the therapy was effective in five of six studies examined (Mewton and Andrews, 2016).
Moutier talked briefly about medications while noting that her discussion could not be comprehensive. She emphasized the need both to optimally manage primary psychiatric conditions, whether with medications or other approaches, and to incorporate considerations specific to suicide in treatment planning. A robust literature shows that lithium, compared with other mood stabilizers and other medications, and for both bipolar and unipolar mood disorders, reduces the risk of suicide attempts and death by suicide between 60 and 80 percent (Baldessarini et al., 2003, 2006), yet lithium is “a very underutilized medication.” Clozapine is the only medication with a Food and Drug Administration (FDA) indication specific to suicide risk reduction for people with schizophrenia (Meltzer et al., 2003). With regard to antidepressants, the FDA black box warning has had the unintended consequence of confusing and alarming the public and leading to undertreatment of depressions among primary care doctors, Moutier said, but “there is a place for antidepressants in terms of risk reduction for suicide.”
A newer class of medications, the NMDA blockers and related medications, has been given the “breakthrough therapy” designation by FDA because their efficacy data look so positive. For example, a single intravenous infusion of ketamine, a dissociative anesthetic from the 1960s, has shown evidence of an acute therapeutic effect for treatment-refractory depression (Muller et al., 2016). It also has produced a rapid reduction in suicidal ideation, starting in just a few hours and being sustained for about 1 week.
“That effect on reducing suicidal ideation has been shown to be partially independent of whether or not the mood effect occurs,” said Moutier, “which is fascinating to separate out depression from suicidal ideation.” The controversy around ketamine relates to the small size of most studies, the potential for abuse, potential side effects such as dissociation, and the relatively short length of therapeutic effect. Other medications similar to Ketamine, such as esketamine and rapastinel, are in the pipeline.
PROJECT 2025
Several years ago, a group of organizations, including the Substance Abuse and Mental Health Services Administration, the National Institute of Mental Health, the National Action Alliance for Suicide Prevention, and CDC, joined the American Foundation for Suicide Prevention in setting a goal of reducing the annual suicide rate in the United States 20 percent by 2025. Informed by an American Foundation for Suicide Prevention expert
panel thorough analysis of the research literature, and using a system dynamic model to project potential lives saved, they are taking four pathways toward the goal. The first was to infuse suicide prevention education into communities that own firearms. The second was to change practices in emergency departments, because 39 percent of people make an emergency department visit in the year prior to a suicide and 70 percent do not attend the first outpatient appointment after an attempt. The third was to work with health care systems, because up to 45 percent of individuals who die by suicide visit their primary care physician in the month prior. The fourth was to focus on corrections systems, because suicide accounts for 35 percent of all deaths in jails.
Project 2025 takes an evidence-based, pragmatic approach to reducing the national suicide rate. Many other organizations have now joined in this project, including accrediting bodies, trade organizations, and professional organizations, Moutier observed. These organizations can recommend, suggest, mandate, and set new standards to significantly reduce the suicide rate.
CLOSING THE GAPS
Finally, Moutier discussed some of the gaps in suicide prevention and ways of filling those gaps. She noted that federal investments in research in such leading causes of death as HIV/AIDS, heart disease, and prostate cancer have led to substantial declines in the death rate from those conditions (see Figure 2-6). For suicide, however, federal investments have been “rather meager,” she observed, and the suicide rate is continuing to climb.
Another gap has, until recently, been standards of care in clinical practice for people at risk for suicide. The publication by the National Action Alliance for Suicide Prevention (2018) of a recommended standard care for people with suicide risk has helped meet this need.
Other gaps described by Moutier include the need to achieve universal mental health literacy so that people know what to do well upstream of suicide risk becoming apparent, implementation science to measure the effect of clinical treatments and community-based programs, inclusion rather than exclusion of people at risk for suicide in clinical trials, better surveillance and health systems to capture data about suicide-related events and deaths, clinician training in prevention, integrated mental health care and screening in primary care, the ability to bill for services such as lethal means counseling or peer-to-peer and telemedicine services, and enforcement of mental health parity.
“By doing all of these things together, we can save lives and improve the quality of many more,” said Moutier. “We are gaining traction in creating a culture that is much more savvy about mental health and suicide prevention, and that’s a wonderful thing.”
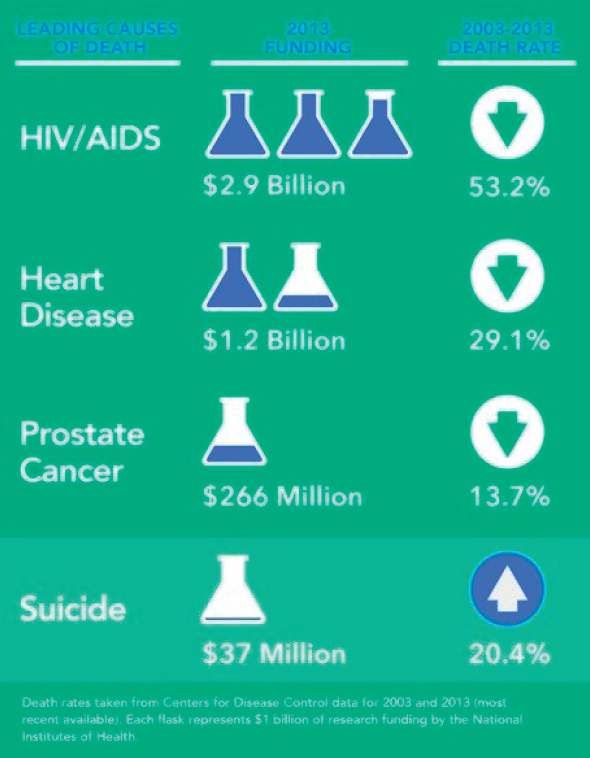
NOTE: HIV/AIDS = human immunodeficiency virus/acquired immunodeficiency syndrome.
SOURCES: Presented by Christine Moutier on September 11, 2018, at the Workshop on Improving Care to Prevent Suicide Among People with Serious Mental Illness. From American Foundation for Suicide Prevention.
THE EFFECTS OF SCREENING
In response to a question about screening for suicide during primary care visits, Moutier discussed data from the Emergency Department Safety Assessment and Follow-up Evaluation (ED-SAFE) study, which sought to apply universal screening to the extent possible in emergency departments. Screening approximately doubled the identification of patients in eight emergency departments who were having current suicidal ideation or had a
recent suicide attempt. “Certainly our first step is to identify those patients who are at risk and then of course to apply the appropriate care steps.”
Wilcox added that suicide risk screening has gained momentum with the Joint Commission encouraging hospitals to detect suicidal ideation through screening. Screening is not able to catch everyone at risk at the right time. “That being said, I find from my experience it to be useful, because . . . multiple studies are showing converging evidence that screening can substantially increase detection.”
On this point, Michael Schoenbaum, senior advisor for mental health services, epidemiology, and economics in the Division of Services and Intervention Research at the National Institute of Mental Health, observed that the best evidence for the efficacy of screening occurs not in general wellness or outpatient primary care settings but in emergency care settings, as in the ED-SAFE study. He also noted that the ED-SAFE study had a phase in which it did universal screening but did not enhance care for the people identified, which revealed that screening by itself did not change the subsequent suicide risk outcomes. Screening needs to be followed by safety planning and follow-up contact after discharge to be effective, he said. The ED-SAFE study also found that patients who were identified through screening and patients who volunteered the information that they had suicidal ideation or had physical problems that indicated self-harm were statistically indistinguishable in terms of their subsequent risk. In other words, the people who are being identified through screening are “not just answering the question lightly because somebody asked them. They’re the people you need to be looking for.”
PERSONAL INTERVENTIONS
Linda Beeber, president of the board of directors for the American Psychiatric Nurses Association and Francis Hill Fox Distinguished Term Professor at the University of North Carolina at Chapel Hill School of Nursing, noted that the association is equipping 12,000 nurses with scripts and slide sets to educate their communities about such subjects as mental health, violence, and suicide; it also is reaching out to the 3 million registered nurses to increase their mental health literacy. But what about educating the general public about suicide prevention, she asked.
Moutier responded that the American Foundation for Suicide Prevention has scripted a series of steps for having a caring conversation. “It’s as simple as the type of caring conversation you would have with anyone in your life that you’re worried about for any reason.” The script calls for explaining that you are there to support a person and not to pass judgment. For a parent, it is important to say that no challenge a child is facing will change the way they feel about their child. “That expression of unconditional love is
something that we often assume, and sometimes our behavior doesn’t always stay consistent, so we need to say it in that moment.” The script then addresses suicidal ideation and knowing where 24/7 resources are and how to access them. She also noted that suicidal ideation is a common phenomenon. “We don’t necessarily need to bring everyone who’s having suicidal thoughts straight to the ER. Many people are living with that.” Providing that understanding to people is part of deepening mental health literacy. But exactly what to do and when to do it can be challenging, Moutier said.
She also mentioned an ad campaign launched by the Ad Council, the American Foundation for Suicide Prevention, and the Jed Foundation called Seize the Awkward that targets 16- to 24-year-olds who are concerned about a friend but do not know how to reach out.1 “There’s a whole toolkit around how to start the conversation, how to continue the conversation, how to come back to it, [how not to] take it personally if they rebuff you.” In response to a related question, she also noted that social media and broadcast media can spread awareness:
We work with anyone who will work with us in the industry, including some major media people who have become interested. Accurate, safe, and effective messaging can save lives, so partnering with media and entertainment industry leaders is key. It just requires relationship development, trust, and empathy to understand the challenges that they’re facing.
COVERAGE, DIGITAL TECHNOLOGIES, AND PHYSICIAN CARE
In response to a question about covering peer-support services under Medicare, Wilcox praised the peer-support model, though she noted that issues continue to surround how best to train and support peers, especially if they are in recovery. “These are all things that hopefully will be sorted out as we move more toward implementing that model in communities.” Beeber from the American Psychiatric Nurses Association added that she is on the congressionally mandated Interdepartmental Serious Mental Illness Coordinating Committee, which has been examining the issue of Medicare coverage for peer support, and that the issue has come up and will continue to be pursued.
In response to a question about digital health technologies, Moutier said that advances in this area require truly interdisciplinary science. “It’s a new kind of way to do science, and investments clearly could be utilized to motivate more of those disciplines to come together. It’s already happening, but much more needs to happen.” An example is the Resources for Enhancing Alzheimer’s Caregivers Health Veterans Affairs (REACH VA) program
___________________
1 The campaign can be found at https://seizetheawkward.org (accessed November 27, 2018).
at the Veterans Health Administration, which is using data analytics to analyze 100 data points in electronic health records and using that information to actively reach out to veterans. “Once we know more about how that’s going, we can learn from that,” Moutier said. Wilcox, too, pointed to the benefits of being able to use data in real time for intervention. It can take years to get suicide data, making it difficult to use data for action. One option, she said, is to use social media data for targeted interventions, which is “an area of great promise for the future.”
With regard to integrated data systems, Moutier noted that the Zero Suicide program is building a system that is integrated in such a way as to pay attention to all the data points that indicate suicide risk. Then people are trained to respond to that information and to make sure that patients do not fall through the cracks. Wilcox added that one complication involves data coding for predictive analytics. Important data often reside in the notes, but these typically are not coded. Work in such areas as natural language processing may be able to overcome this problem, “but it’s a complex issue that’s going to take some time to get all the technology sorted out to be able to do this in a large scale.” In particular, issues of privacy and data protection are major concerns in this area.
Finally, a question about preventing suicide among physicians led Moutier to respond “thanks for bringing my passion area up.” Physicians live in a culture where seeking help has been stigmatized and mental health has been erroneously equated with impairment. But change is happening at both the system and local levels. For example, the American Council for Graduate Medical Education now requires that all residency training programs in the United States have programs for wellness and access to 24/7 mental health support for residents. “There’s been a radical shift over the last about 4 years in academic medicine,” Moutier said.
REFERENCES
Anglemyer, A., T. Horvath, and G. Rutherford. 2014. The accessibility of firearms and risk for suicide and homicide victimization among household members: A systematic review and meta-analysis. Annals of Internal Medicine 160(2):101-110.
Baldessarini, R. J., L. Tondo, and J. Hennen. 2003. Lithium treatment and suicide risk in major affective disorders: Update and new findings. Journal of Clinical Psychiatry 64(Suppl 5):44-52.
Baldessarini, R. J., L. Tondo, P. Davis, M. Pompili, F. K. Goodwin, and J. Hennen. 2006. Decreased risk of suicides and attempts during long-term lithium treatment: A meta-analytic review. Bipolar Disorders 8(5 Pt 2):625-639.
Bastiampillai, T., S. S. Sharfstein, and S. Allison. 2016. Increase in US suicide rates and the critical decline in psychiatric beds. JAMA 316(24):2591-2592.
Bilukha, O., R. A. Hahn, A. Crosby, M. T. Fullilove, A. Liberman, E. Moscicki, S. Snyder, F. Tuma, P. Corso, A. Schofield, P. A. Briss, and the Task Force on Community Preventive Services. 2005. The effectiveness of early childhood home visitation in preventing violence: A systematic review. American Journal of Preventive Medicine 28(2 Suppl 1):11-39.
Bolton, J. M., and J. Robinson. 2010. Population-attributable fractions of Axis I and Axis II mental disorders for suicide attempts: Findings from a representative sample of the adult, noninstitutionalized U.S. population. American Journal of Public Health 100(12):2473-2480.
Brown, G. K., T. Ten Have, G. R. Henriques, S. X. Xie, J. E. Hollander, and A. T. Beck. 2005. Cognitive therapy for the prevention of suicide attempts: A randomized controlled trial. Journal of the American Medical Association 294(5):563-570.
Case, A., and A. Deaton. 2017. Mortality and Morbidity in the 21st century. Brookings Papers on Economic Activity Spring 397-476.
Cavanagh, J. T., A. J. Carson, M. Sharpe, and S. M. Lawrie. 2003. Psychological autopsy studies of suicide: A systematic review. Psychological Medicine 33(3):395-405.
Connell, A. M., H. N. McKillop, and T. J. Dishion. 2016. Long-term effects of the family check-up in early adolescence on risk of suicide in early adulthood. Suicide and Life-Threatening Behavior 46(Suppl 1):S15-S22.
Crifasi, C. K., J. S. Meyers, J. S. Vernick, and D. W. Webster. 2015. Effects of changes in permit-to-purchase handgun laws in Connecticut and Missouri on suicide rates. Preventive Medicine 79:43-49.
Cwik, M. F., L. Tingey, A. Maschino, N. Goklish, F. Larzelere-Hinton, J. Walkup, and A. Barlow. 2016. Decreases in suicide deaths and attempts linked to the White Mountain Apache Suicide Surveillance and Prevention System, 2001-2012. American Journal of Public Health 106(12):2183-2189.
Franklin, J. C., J. D. Ribeiro, K. R. Fox, K. H. Bentley, E. M. Kleiman, X. Huang, K. M. Musacchio, A. C. Jaroszewski, B. P. Chang, and M. K. Nock. 2017. Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research. Psychological Bulletin 143(2):187-232.
Hahn, R. A., O. O. Bilukha, A. Crosby, M. T. Fullilove, A. Liberman, E. K. Moscicki, S. Snyder, F. Tuma, A. Schofield, P. S. Corso, P. Briss, and Task Force on Community Preventive Services. 2003. First reports evaluating the effectiveness of strategies for preventing violence: Early childhood home visitation. Findings from the Task Force on Community Preventive Services. Morbidity and Mortality Weekly Report 52(RR-14):1-9.
Halla, M. 2013. The effect of joint custody on family outcomes. Journal of the European Economic Association 11(2):278-315.
Hawkins, J. S., R. Kosterman, R. F. Catalano, K. G. Hill, and R. D. Abbott. 2005. Promoting positive adult functioning through social development intervention in childhood: Long-term effects from the Seattle Social Development Project. Archives of Pediatrics and Adolescent Medicine 159(1):25-31.
Kellermann, A. L., F. P. Rivara, G. Somes, D. T. Reay, J. Francisco, J. G. Banton, J. Prodzinski, C. Fligner, and B. B. Hackman. 1992. Suicide in the home in relation to gun ownership. New England Journal of Medicine 327(7):467-472.
Kessler, R. C., C. H. Warner, C. Ivany, M. V. Petukhova, S. Rose, E. J. Bromet, M. Brown 3rd, T. Cai, L. J. Colpe, K. L. Cox, C. S. Fullerton, S. E. Gilman, M. J. Gruber, S. G. Heeringa, L. Lewandowski-Romps, J. Li, A. M. Millikan-Bell, J. A. Naifeh, M. K. Nock, A. J. Rosellini, N. A. Sampson, M. Schoenbaum, M. B. Stein, S. Wessely, A. M. Zaslavsky, R. J. Ursano, and the Army STARRS Collaborators. 2015. Predicting suicides after psychiatric hospitalization in U.S. Army soldiers: The Army Study To Assess Risk and Resilience in Servicemembers (Army STARRS). Journal of the American Medical Association Psychiatry 72(1):49-57.
Knox, K. L., D. A. Lotts, G. W. Talcott, J. C. Feig, and E. D Caine. 2003. Risk of suicide and related adverse outcomes after exposure to a suicide prevention programme in the U.S. Air Force: Cohort study. BMJ 327(7428):1376.
Knox, K. L., S. Pflanz, G. W. Talcott, R. L. Campise, J. E. Lavigne, A. Bajorska, X. Tu, and E. D. Caine. 2010. The U.S. Air Force suicide prevention program: Implications for public health policy. American Journal of Public Health 100(12):2457-2463.
Linehan, M. M., K. A. Comtois, A. M. Murray, M. Z. Brown, R. J. Gallop, H. L. Heard, K. E. Korslund, D. A. Tutek, S. K. Reynolds, and N. Lindenboim. 2006. Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder. Archives of General Psychiatry 63(7):757-766.
March, J. S., B. J. Klee, and C. M. Kremer. 2006. Treatment benefit and the risk of suicidality in multicenter, randomized, controlled trials of sertraline in children and adolescents. Journal of Child and Adolescent Psychopharmacology 16(1-2):91-102.
McCarthy, J. F., M. Valenstein, H. M. Kim, M. Ilgen, K. Zivin, and F. C. Blow. 2009. Suicide mortality among patients receiving care in the Veterans Health Administration health system. American Journal of Epidemiology 169(8):1033-1038.
McCarthy, J. F., R. M. Bossarte, I. R. Katz, C. Thompson, J. Kemp, C. M. Hannemann, C. Nielson, and M. Schoenbaum. 2015. Predictive modeling and concentration of the risk of suicide: Implications for preventive interventions in the U.S. Department of Veterans Affairs. American Journal of Public Health 105(9):1935-1942.
Meltzer, H. Y., L. Alphs, A. I. Green, A. C. Altamura, R. Anand, A. Bertoldi, M. Bourgeois, G. Chouinard, M. Z. Islam, J. Kane, R. Krishnan, J. P. Lindenmayer, S. Potkin, and the International Suicide Prevention Trial Study Group. 2003. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT). Archives of General Psychiatry 60(1):82-91.
Mewton, L., and G. Andrews. 2016. Cognitive behavioral therapy for suicidal behaviors: Improving patient outcomes. Psychology Research and Behavior Management 9:21-29.
Miller, M., and D. Hemenway. 2008. Guns and suicide in the United States. New England Journal of Medicine 359(10):989-991.
Miller, M., C. Barber, R. A. White, and D. Azrael. 2013. Firearms and suicide in the United States: Is risk independent of underlying suicidal behavior? American Journal of Epidemiology 178(6):946-955.
Muller, J., S. Pentyala, J. Dilger, and S. Pentyala S. 2016. Ketamine enantiomers in the rapid and sustained antidepressant effects. Therapeutic Advances in Psychopharmacology 6(3):185-192.
National Action Alliance for Suicide Prevention: Transforming Health Systems Initiative Work Group. 2018. Recommended standard care for people with suicide risk: Making health care suicide safe. Washington, DC: Education Development Center, Inc.
Nock, M. K., A. J. Millner, P. M. Gutierrez, J. A. Naifeh, M. B. Stein, R. C. Kessler, T. E. Joiner, G. Han, I. Hwang, A. King, N. A. Sampson, A. M. Zaslavsky, and R. J. Ursano. 2018. Risk factors for the transition from suicide ideation to suicide attempt: Results from the Army Study to Assess Risk and Resilience in Servicemembers (Army STARRS). Journal of Abnormal Psychology 127(2):139-149. https://nocklab.fas.harvard.edu/files/nocklab/files/29528668-nock-2018.pdf (accessed December 5, 2018).
Rudd, M. D., C. J. Bryan, E. G. Wertenberger, A. L. Peterson, S. Young-McCaughan, J. Mintz, S. R. Williams, K. A. Arne, J. Breitbach, K. Delano, E. Wilkinson, and T. O. Bruce. 2015. Brief cognitive-behavioral therapy effects on post-treatment suicide attempts in a military sample: Results of a randomized clinical trial with 2-year follow-up. American Journal of Psychiatry 172(5):441-449.
Shepard, D. S., D. Gurewich, A. K. Lwin, G. A. Reed, Jr., and M. M. Silverman. 2016. Suicide and suicidal attempts in the United States: Costs and policy implications. Suicide and Life-Threatening Behavior 46(3):352-362.
Simon, G. E., E. Johnson, J. M. Lawrence, R. C. Rossom, B. Ahmedani, F. L. Lynch, A. Beck, B. Waitzfelder, R. Ziebell, R. B. Penfold, and S. M. Shortreed. 2018. Predicting suicide attempts and suicide deaths following outpatient visits using electronic health records. American Journal of Psychiatry 175(10):951-960.
Stevenson, B., and J. Wolfers. 2006. Bargaining in the shadow of the law: Divorce laws and family distress. Quarterly Journal of Economics 121(1):267-288.
Stone, D. M., T. R. Simon, K. A. Fowler, S. R. Kegler, K. Yuan, K. M. Holland, A. Z. IveyStephenson, and A. E. Crosby. 2018. Vital signs: Trends in state suicide rates—United States, 1999-2016 and circumstances contributing to suicide—27 States, 2015. Morbidity and Mortality Weekly Report 67(22):617-624.
Tidemalm, D., N. Långström, P. Lichtenstein, and B. Runeson. 2008. Risk of suicide after suicide attempt according to coexisting psychiatric disorder: Swedish cohort study with long term follow-up. BMJ 337:a2205.
Tran, T., W. Luo, D. Phung, R. Harvey, M. Berk, R. L. Kennedy, and S. Venkatesh. 2014. Risk stratification using data from electronic medical records better predicts suicide risks than clinician assessments. 2014. BMC Psychiatry 14:76.
Wasserman, D., C. W. Hoven, C. Wasserman, M. Wall, R. Eisenberg, G. Hadlaczky, I. Kelleher, M. Sarchiapone, A. Apter, J. Balazs, J. Bobes, R. Brunner, P. Corcoran, D. Cosman, F. Guillemin, C. Haring, M. Iosue, M. Kaess, J. P. Kahn, H. Keeley, G. J. Musa, B. Nemes, V. Postuvan, P. Saiz, S. Reiter-Theil, A. Varnik, P. Varnik, and V. Carli. 2015. School-based suicide prevention programmes: The SEYLE cluster-randomised, controlled trial. Lancet 385(9977):1536-1544.
While, D., H. Bickley, A. Roscoe, K. Windfuhr, S. Rahman, J. Shaw, L. Appleby, and N. Kapur. 2012. Implementation of mental health service recommendations in England and Wales and suicide rates, 1997-2006: A cross-section and before-and-after observational study. Lancet 379:1005-1012.
Wilcox, H. C., S. G. Kellam, C. H. Brown, J. M. Poduska, N. S. Ialongo, W. Wang, and J. C. Anthony. 2008. The impact of two universal randomized first- and second-grade classroom interventions on young adult suicide ideation and attempts. Drug and Alcohol Dependence 95(Suppl 1):S60-S73.
Wintemute, G. J. 2015. Alcohol misuse, firearm violence perpetration, and public policy in the United States. Preventive Medicine 79:15-21.
Wolk, C. B., P. C. Kendall, and R. S. Beidas. 2015. Cognitive-behavioral therapy for child anxiety confers long-term protection from suicidality. Journal of the American Academy of Child and Adolescent Psychiatry 54(3):175-179.




















