
7
Programs and Research
Day 2 of the workshop began with a morning-long session highlighting programs that are successfully addressing the prevention of firearm injuries and death. The speakers in this session were Michael Levas, an associate professor of pediatrics at the Medical College of Wisconsin and the assistant medical director of Project Ujima; Ali Rowhani-Rahbar, the Bartley Dobb Professor for the study and prevention of violence, an associate professor of epidemiology and pediatrics, and the violence prevention section leader at the University of Washington’s Harborview Injury Prevention and Research Center; Rebecca Cunningham, an associate vice president for research at the University of Michigan, a principal investigator with the Firearm Safety Among Children and Teens (FACTS) consortium, the director of the Centers for Disease Control and Prevention (CDC)-funded University of Michigan Injury Prevention Center, a professor of emergency medicine at the University of Michigan School of Medicine, and a professor of health behavior and health education at the University of Michigan School of Public Health; Rinad Beidas, an associate professor of psychiatry, medical ethics, and health policy and the director of implementation research at the University of Pennsylvania Perelman School of Medicine; and Kyle Fischer, an adjunct assistant professor of health policy and the leadership fellowship director at the University of Maryland School of Medicine. A question-and-answer session and open discussion moderated by Joel Fein, a professor of pediatrics and emergency medicine at the University of Pennsylvania Perelman School of Medicine, a co-director of the Children’s Hospital of Philadelphia Violence Prevention Initiative, and the research co-director of
the National Network of Hospital-Based Violence Intervention Programs (NNHVIP), followed the five presentations.
Before introducing the first speaker, Fein noted that violence prevention initiatives focus on different types of violence, such as youth violence or intimate partner violence (IPV). However, as the speakers would show, there is a common thread that runs through all forms of violence and that the delineation among them is artificial.
PROJECT UJIMA
Addressing youth violence, Levas said, requires recognizing that there are four major components to account for the youth victims, the communities they come from, the health care system that for the most part has taken a patch-up-and-send-back-out-to-the-community response, and law enforcement and the legal system. Project Ujima was designed to work at the intersection of these four components. The project started some 20 years ago when a 16-year-old boy named Jason ended up dead of multiple firearm injuries at the Children’s Hospital of Wisconsin, and one of the emergency department nurses recognized this child from a previous visit. A review of his medical record showed that he had first been seen at age 8 for an accidental injury, then at age 11 for an assault, age 13 for stab wounds, and age 15 for a gunshot wound. “We had missed opportunity after missed opportunity, and the result was a dead child,” Levas said. “Can you imagine if we missed cancer that many times? That would not be acceptable.”
For children who are victims of violence, there are often upstream flags that could identify them as potential future victims of more serious violence. With Project Ujima, when a child between age 7 and 18 comes into the emergency department as a victim of a stabbing, physical assault, or gunshot wound, a Ujima staff member comes to the emergency department, tries to enroll the family in the program, and starts encouraging no retaliation. Levas said that data from the Milwaukee Homicide Review Commission show that 50 percent of violent injuries and deaths result from arguments or retaliation. For families that agree to join the program, Project Ujima wraps the children in services, starting with an assignment to a case manager who helps the child and family members get to their appointments, arranges for wheelchairs if necessary, and works to get the family home compliant with Americans with Disabilities Act requirements if the child is left paralyzed by the wounds. Levas explained that the program will even arrange for the family to move to new housing if the place the child was injured causes re-traumatization.
Project Ujima offers a variety of programming directed at the children, including afterschool programming for adolescents and teens and a summer camp for about 60 children in Milwaukee who have been victims of
violence. This camp gets the children to a safe location during the most dangerous time of year for youth violence, Levas said. It provides messages of empowerment and leadership and classes on a range of subjects, including conflict resolution, conflict avoidance, and, when needed, hygiene.
Project Ujima has expanded its reach by enrolling children who have had a family member killed, and of the 338 children enrolled in 2017 in Milwaukee, 126 had suffered vicarious trauma as a result of having a direct family member murdered. Another 178 children came into the program after being seen in the emergency department, and 34 children were victims of domestic violence.
To test Project Ujima’s effectiveness at curbing youth violence, Levas and his colleagues have been using validated patient-reported outcomes. A recent analysis of these reports showed that children who are victims of violence, even vicarious trauma associated with violence, show worse quality-of-life measures, physical functioning, psychosocial functioning, emotional functioning, and school functioning than youth with chronic disease (Levas et al., 2018) (see Table 7-1). These data show that being direct or vicarious victims of violence is as bad for a child’s ability to function normally as being morbidly obese or having cancer; Levas said he suspects that this is due at least in part to the victims of violence receiving less support than children with other health conditions. The good news is that participation in the 6-week Project Ujima summer camp can improve those scores (see Figure 7-1), as well as scores for depression, anxiety, and anger (Levas et al., 2016).
Currently, Levas and his colleagues are examining how much of the low scores seen in patient-reported outcomes results from the actual violent
| Category | Violently Injured | Healthy Individuals | Racially Similar Group | ||
|---|---|---|---|---|---|
| PedsQL™ | Mean | Mean | P Value | Mean | P Value |
| Total function | 71.43 | 83.91 | <0.001 | 76.92 | 0.001 |
| Physical function | 76.62 | 87.77 | <0.001 | 93.02 | <0.001 |
| Psychosocial function | 67.63 | 81.83 | <0.001 | 73.08 | 0.005 |
| Emotional function | 62.93 | 79.21 | <0.001 | 70.37 | 0.010 |
| Social function | 75.25 | 84.96 | <0.001 | 76.63 | 0.584 |
| School function | 63.79 | 81.31 | <0.001 | 72.23 | <0.001 |
SOURCES: Adapted from a presentation by Mike Levas at the workshop on Health Systems Interventions to Prevent Firearm Injuries and Death on October 18, 2018; Levas et al., 2018.
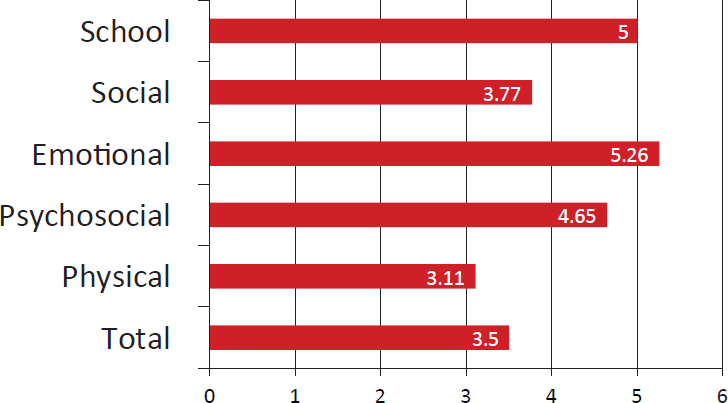
NOTE: On the scale, 0 is the worst ranking in terms of outcomes, and 6 is the best ranking.
SOURCES: As presented by Mike Levas at the workshop on Health Systems Interventions to Prevent Firearm Injuries and Death on October 18, 2018; Levas et al., 2016.
event and how much is tied to the place where these children live, given that Milwaukee is the most segregated city in the nation. The Project Ujima staff are now enrolling youth victims of violence along with youth from the same neighborhoods, matched on gender and race who have not been injured by violence. “What we want to do is try to take into account how much of the social determinants of health that are impacting them from their built environment,” Levas said.
After recording baseline scores from patient-reported outcomes, adverse childhood event scores, and measures of posttraumatic stress disorder, the researchers follow up on these children every 3 months in an attempt to find out which children are being helped most by the program’s interventions. “Traditionally we had a blanket approach with Project Ujima, where every kid would get just about every intervention,” Levas said, “but we realized that we could be smarter and more targeted if we look at the kids, look at their scores, look at the interventions that are being done, and really try to find out which kids might really benefit from camp and which kids do not, which kids need the behavioral specialist early before any other programing is going to really affect them.”
Levas acknowledged that Project Ujima is reactionary, not prevention oriented, in part because its funding comes from Victims of Crime Act dollars. He and his colleagues are now looking at markers, descriptive variables, and pre-enrollment experiences for Project Ujima participants so
that when the program can get funds for prevention, they will have already identified which children were at risk and perhaps be able to help them avoid Jason’s fate of repeat injuries and eventual death.
Levas said that Project Ujima does not make money for the Children’s Hospital of Wisconsin or the Medical College of Wisconsin. “It is the right thing to do, and the hospital recognizes that, matching every Victims of Crime Act dollar the program receives,” he said. At the same time, the Children’s Hospital has been an early adopter of other violence prevention and intervention initiatives, including one that looks at how the hospital system interacts with law enforcement and police to tackle youth violence. For the past 3 years, Levas and his colleagues at the Children’s Hospital and the Comprehensive Injury Center at the Medical College of Wisconsin have been implementing the Cardiff model in Milwaukee to collect data on injuries and combine those data with law enforcement data. The researchers have also partnered with the local level 1 trauma center and two other community hospitals to expand the program. The data collected so far show that only 7 percent of the incidents of youth violence recorded by these health systems were known by the police; when mapped, the combined data could lead to improved surveillance by law enforcement, Levas said. “This was another opportunity where the hospital was able to add to the narrative of where interventions should be done and really try to help civil society get better information to work on,” he said.
HELPING INDIVIDUALS WITH FIREARM INJURIES CLINICAL TRIAL
Some 35 years ago, Rowhani-Rahbar said, researchers observed that individuals who experience a trauma and also misuse alcohol are at high risk of recurrent injury (Rivara et al., 1993). Several years later, a randomized trial showed that providing a brief, motivational, interviewing-based intervention as a component of trauma care significantly reduced alcohol consumption and decreased the rate of trauma recidivism by 47 percent (Gentilello et al., 1999). The authors of that study concluded that because of the prevalence of alcohol problems in trauma center patients, screening, intervention, and counseling for alcohol problems should be routine, and today trauma centers are required to identify at least one member of the trauma team to receive training in how to administer these screenings and brief interventions.
What this has to do with firearm injuries, Rowhani-Rahbar said, is that it offers an approach that might work with modification to reduce the risk of gun violence recidivism. In fact, studies that he and his colleagues conducted in the aftermath of the Sandy Hook tragedy showed that individuals who had been shot and hospitalized were 21 times more likely than
those hospitalized for non-injury reasons to get shot again and return to the hospital (Rowhani-Rahbar et al., 2015, 2016a) (see Table 7-2). “Not that we did not know that these individuals are at risk of getting shot again, but these results showed the magnitude and scope of the problem,” he said. These studies also showed that members of the firearm injury group were more likely to be arrested within the first year after being shot.
Rowhani-Rahbar said that members of NNHVIP, formed in 2009, use a trauma-informed care model which includes taking advantage of a teachable moments to interrupt the costly cycle of violence. He added that while there is an accumulation of good evidence that these programs work and are cost-effective, there is still a long way to go to provide more evidence to support the effectiveness and implementation of these programs. Toward that end, his team launched the Helping Individuals with Firearm Injuries randomized controlled trial at Harborview Medical Center in Seattle, with data collection scheduled to end in 2019.
The intervention they are testing has three components: a motivational interview done at the bedside or in the emergency department; a critical time intervention (CTI); and attention from a multidisciplinary team comprising colleagues from community services, law enforcement, mental health, employment, education, and housing. Prior to delivering a CTI,
TABLE 7-2 Suffering a Gunshot Wound Increases the Risk of Getting Shot Again
| Index Hospitalization | Hospitalization | ||
|---|---|---|---|
| Firearm (Any Intent) |
Nonfirearm | ||
| Assault | Self-inflicted | ||
| Violent injury (n = 8,655) |
|||
| Firearm, assault (n = 613) |
21.2 (7.0–64.0) | 7.3 (3.5–14.9) | 1.7 (0.5–5.3) |
| Nonfirearm, assault (n = 2,453) |
3.1 (0.9–10.3) | 6.6 (4.0–10.7) | 2.1 (1.3–3.5) |
| Nonfirearm, self-inflicted (n = 5,589) |
0.8 (0.1–5.8) | 1.6 (0.8–3.3) | 11.9 (9.5–14.8) |
| Nonviolent injury (n = 62,428) |
1.7 (0.8–3.8) | 2.5 (1.7–3.5) | 2.1 (1.7–2.6) |
| Noninjury (n = 175,039) |
1.0 (reference) | 1.0 (reference) | 1.0 (reference) |
SOURCES: Adapted from a presentation by Ali Rowhani-Rahbar at the workshop on Health Systems Interventions to Prevent Firearm Injuries and Death on October 18, 2018; Rowhani-Rahbar et al., 2015.
the staff members work to develop a trusted relationship with the patient. Phase 1 of the CTI then provides support and begins to connect the patient to people and agencies that will assume the primary support role. Phase 2 of the intervention monitors and strengthens this support network and the patient’s skills, while Phase 3 terminates the CTI once the support network is in place, which typically takes 6 to 9 months.
The data collection, which relies on self-reported surveys and several administrative databases that together cover criminal justice involvement, health care use, depression, posttraumatic stress, substance use, life satisfaction, social support, physical and mental health–related quality of life, and exposure to violence, occurs at 1 month, 3 months, 6 months, 9 months, and 1 year. Rowhani-Rahbar explained that the frequently repeated surveys help retain individuals in the study, which is not an easy task. In fact, he said, the study has faced three challenges. The first is the cost of having staff available 24 hours per day, 7 days per week to reach every individual who comes into the trauma center. The second challenge has to do with the socioeconomic status of the participants, many of whom have low incomes, may have difficulty commuting from their residence to the trauma center, and may move frequently. The third challenge is to deal with the distrust that many of these individuals have for authorities and institutions. Dealing with this last challenge requires having support specialists or case managers with lived experiences who can talk with these individuals and provide them help guided by elements of trauma-informed care.
Though the study is still ongoing—it has enrolled 225 patients and hopes to enroll 250 by year end—positive feedback from participants in the trial has been quite motivating, Rowhani-Rahbar said. On a final note, he said, “I think we all have a duty to raise awareness about these HVIPs [hospital-based violence intervention programs]. We need to do enhanced communication among those involved in the implementation and evaluation of these programs—I can say that the more advocacy, the better—to get additional resources for this type of work.”
SAFERTEENS: AN EVIDENCE-BASED YOUTH VIOLENCE PREVENTION PROGRAM
In 2009, Cunningham and several colleagues authored a paper that presented some of their thinking about what the trauma community should be doing before and after a patient reaches the trauma bay (Cunningham et al., 2009). One conclusion they drew was that many of the young people seen in the emergency department for violence-associated injury use the emergency department as their primary or sole access point to the health care system. Another finding was that 97 percent of the injured youth seen in emergency departments are treated and released the same day, often in
the middle of the night when few social work resources are available. Data from the Pediatric Emergency Care Applied Research Network found that 52 percent of children with a firearm injury go home from the emergency department and receive no follow-up resources until the next time they come to the emergency department (Carter et al., 2017). Cunningham and her colleagues concluded that while many emergency departments are trying to do something to prevent youth violence, many others were not even doing risk assessment. The situation is better today, she said, but neither risk assessment or any intervention from the emergency room is still part of the standard of care for youth violence victims.
The SafERteens intervention model was developed when the National Institute on Alcohol Abuse and Alcoholism provided funding to help prevent violence among youth with a history of alcohol use and fighting. This upstream model serves youth ages 14 to 18 who come into the emergency department for any reason, as long as they are medically stable. If these individuals answer yes to questions about having engaged in fighting or alcohol use over the previous few months, they receive a 30-minute, single-session emergency department intervention from a trained counselor while they are waiting for various medical procedures. The screen is administered using a tablet computer to reduce the time requirements on the staff. The results of an assessment of the program showed that this brief intervention decreased severe peer aggression over the following 3 months and 1 year (Cunningham et al., 2012; Walton et al., 2010). In fact, the intervention decreased violent victimization and aggression among youth. It also reduced the frequency of consequences associated with engagement with violence, including getting in trouble with friends, having problems at school, and dating violence (number needed to treat = 40).
A cost analysis of the SafERteens program showed that a single-session, 30-minute intervention implemented by a large health system in all of its emergency departments would prevent some 4,000 violent events over 5 years and would cost approximately $4 to $55 per event prevented. Considering that an average emergency department visit costs more than $1,300, a tetanus shot costs $129, and an intravenous saline infusion costs $417 per hour in the emergency department, Cunningham argued that this is a cost-effective approach to upstream prevention and that cost should not be a significant barrier to implementation (Sharp et al., 2014).
One somewhat surprising finding, said Cunningham said, was that the youth who came to the emergency department for problems not related to violence, such a sore throat, were quite interested in talking about violence in their lives. “These kids are incredibly interested in talking about the violence,” she said, “because violence is one of the most important things that is going on in their life, overwhelmingly, and nobody is talking to them about that violence.” Another spinoff study from the SafERteens program found
that providing this intervention to every adolescent who walked through the emergency room door and lived in a known high-risk neighborhood, with no screening, decreased the violent victimization events those children experienced over the next 6 months by 52 percent (p < 0.001) and decreased violent aggression by the teens by 49 percent (p < 000.1) (Carter et al., 2016). Cunningham and her colleagues have now packaged this intervention and offer trainings to other health systems that want to implement the SafERteens program.
Cunningham cautioned that SafERteens is not a solution for all youth violence. “There are kids that have more severe needs and who need wraparound care, but we have kids [in the emergency department], and while we have them, this is something we can do for them at that time,” she said. It would be great, she added, to have funding to study the synergistic effects of deploying SafERteens and Project Ujima at the same time. “What we need for the National Network of Hospital Violence Programs is funding at the level our stroke centers are funded at to actually make a difference,” Cunningham said. She and her colleague, Patrick Carter, have since started thinking about how to apply this approach to firearm-related injuries and extend it beyond the emergency department using, for example, an app to facilitate multi-session counseling interventions once individuals leave the emergency department.
Another study that Cunningham discussed followed a cohort of youths who had come to the emergency department with any assault-related injury and a matched cohort of youths who came to the emergency department without an assault-related injury. Assaulted youth had twice the risk for a later violent injury than those who had not been assaulted, and 59 percent of the assaulted youth reported experiencing some form of firearm violence during the 2 years of the study, with 8 percent sustaining a fatal or nonfatal firearm injury and 77 percent reporting that firearm violence was not limited to a single episode (Carter et al., 2015).
Using the data from this study and a machine learning algorithm, Cunningham and her colleagues developed a SaFETy Score risk that predicts future firearm violence from four questions (Goldstick et al., 2017):
- In the past 6 months, including today, how often did you get into a serious physical fight?
- How many of your friends have carried a knife, razor, or gun?
- In the past 6 months, how often have you heard guns being shot?
- How often, in the past 6 months, including today, has someone pulled a gun on you?
Cunningham said that CDC has funded a series of youth violence prevention centers that looked at how multilevel interventions could decrease
violence in general over time in a community. Michigan’s Youth Violence Prevention Center worked with Flint, Michigan, to carry out six evidence-based interventions that spanned multiple ecological levels, with a version of SafERteens called Project Sync, and the evidence-based Youth Empowerment Solutions school resiliency program focused on the individual, mentoring models at the social level, and community policing and clean- and-green neighborhood improvement programs at the community level. “This is how a health system partners with a community to make it work,” Cunningham said. This multifaceted approach, she added, produced a significant decrease in assault offenses and violent injury presentations to the emergency department in youth ages 10 to 24 in the intervention neighborhood as compared with a control neighborhood (Heinze et al., 2016).
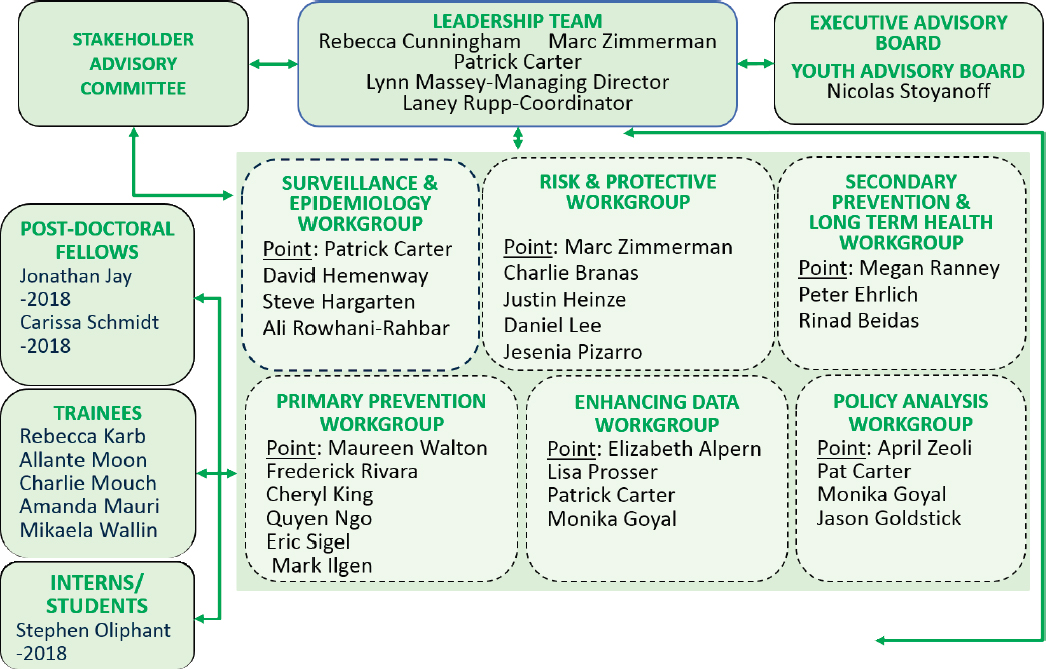
Before talking about the Firearm Safety Among Children and Teens (FACTS) consortium, Cunningham reiterated the need for more grants to fund firearm research, particularly given the number of deaths caused by firearms compared to other disorders that have been well funded over the years (see Table 7-3). In 2014, she said, there were fewer than 12 active and experienced U.S. investigators with careers focused primarily on firearm injury, only 2 of whom were physicians, despite the fact that firearms are responsible for 16 percent of the deaths among children ages 1 to 17, more than any other cause other than motor vehicle collisions.
The FACTS consortium (see Figure 7-2) was funded by an initiative of the Eunice Kennedy Shriver National Institute of Child Health & Human
TABLE 7-3 Federal Funding of Firearm Research and Number of Deaths Compared to Other Disorders
| Cause of Death | Number of Deaths Over 10 Years (ages 1–19) | Number of Research Awards Over the Past 10 Years (all ages) | U.S. Dollars of Public Funding for Research (all ages) |
|---|---|---|---|
| Motor vehicle collision | 44,821 | 2,902 | $1,084,364,160 |
| Firearm | 27,830 | 9 | $2,393,083 |
| Malignant neoplasms | 18,792 | 2,939 | $1,558,955,478 |
| Drowning | 9,766 | 101 | $27,556,259 |
| Congenital abnormalities | 10,199 | 15,616 | $6,344,957,752 |
| Meningitis | 585 | 75 | $34,063,406 |
| Polio | 0 | 456 | $464,966,937 |
SOURCE: Adapted from a presentation by Rebecca Cunningham at the workshop on Health Systems Interventions to Prevent Firearm Injuries and Death on October 18, 2018.
SOURCE: As presented by Rebecca Cunningham at the workshop on Health Systems Interventions to Prevent Firearm Injuries and Death on October 18, 2018.
Development in 2017 to jumpstart capacity building needed in the field. Currently, the consortium has some 25 content experts working across disciplines to improve firearm safety and reduce firearm injury and deaths among children. The consortium will define a pediatric-specific firearm injury research agenda, conduct core studies to provide preliminary data which will then inform large-scale studies and fill early data needs, establish a Web-based, searchable data archive for childhood firearm injury, and build a cadre of national research scholars that will serve as an emerging pipeline for future research. FACTS makes available a series of counseling videos created by investigators that demonstrate and model for young pediatricians how they can have a conversation with parents about safe firearm storage in a nonjudgmental way.
PARTICIPATORY APPROACHES TO IMPLEMENTING FIREARM SAFETY PROMOTION IN PEDIATRIC PRIMARY CARE
The rate of youth suicide in the United States has increased 56 percent since 2007, Beidas said, with firearms being among the most common and most lethal suicide methods, particularly for males. In 2016 the rate of suicide deaths in children was 6.1 per 100,000, with firearms responsible for half of those deaths. In her opinion, Beidas said, firearm access is a modifiable risk factor for suicide, and safer storage could save lives. The good news, she said, is that there is an evidence-based, office-based counseling intervention for increasing parental safe firearm storage called Safety Check (Barkin et al., 2008).
When thinking about how to reach the most youths with a universal intervention such as Safety Check, Beidas said, she and her colleagues concluded that pediatric primary care was the best option, given that more than 75 percent of youth visited primary care in 1 year proceeding an attempted or completed suicide, compared with only one-third of youth who visited a behavioral health provider. Collaborating with the Mental Health Research Network—a National Institute of Mental Health–funded consortium comprising 13 heath systems organized in a practice-based research network—Beidas and her colleagues conducted a 2-year study in two of those health systems located in Michigan and Texas. The study started with a quantitative survey that asked physicians and leaders of practices that saw youth about the acceptability of the intervention components of screening, counseling, and handing out firearm locks. Next, the researchers conducted in-depth interviews with 9 stakeholder groups and 70 individuals to gather richer and more nuanced information about the acceptability of the intervention as well as about barriers to and facilitators for implementation. Of the physicians who responded to the survey, 60 percent were female, 31 percent reported having a firearm in their
home, and 13 percent reported that there had been a youth suicide in a practice where they had worked.
The results from the quantitative portion of the study, which at the time of the workshop were under review prior to publication, found that 85 percent of the physicians reported that they used screening rarely or sometimes, 80 percent used counseling, and 9 percent handed out gun locks. However, only 28 percent of the physicians endorsed using screening and counseling most or all of the time, and only 2 percent would hand out gun locks most or all of the time. Beidas noted that previous studies, including a systematic review by Rowhani-Rahbar (Rowhani-Rahbar et al., 2016b), suggest that free safe storage devices may be the critical ingredient to preventing youth suicide by firearm, so these results suggest more research is needed before going to large-scale implementation.
One of the findings from the qualitative study was that recent high-profile gun-related incidents, such as the Sandy Hook and Las Vegas mass shootings, are making it easier for clinicians to initiate questions about firearm storage in the home (Wolk et al., 2018). Beidas said that she and her colleagues also heard about the importance for system buy-in and alignment with priorities before going forward with large-scale implementation as well as about variability in the comfort level that physicians had in talking about firearm safety, which depended on an individual’s knowledge about firearms and how much confidence they had in talking to parents about firearm safety. Regarding who might be tasked with implementing each of the three components, Beidas said that the message was clear that nurses or medical assistance could do screening and give out firearm locks, but that physicians should administer the counseling component.
The qualitative interviews revealed a high level of acceptability and feasibility concerning screening and counseling, Beidas said, and it was suggested the electronic health record (EHR) should be used for screening and providing written resources for safe storage recommendations. There were concerns about financing, storing, and distributing firearm locks as well as about liability. It was suggested that clinicians could refer patients referred to get free locks in the community rather than distributing them through primary care or in a hospital setting. One of the major barriers to implementation, Beidas reported, was the need to fit this intervention into an already packed schedule.
Analysis of the qualitative interviews with gun owners, who were individuals in law enforcement and from firearm advocacy groups as well as firearm safety course instructors and firearm retailers, one finding was that there was a concern among gun owners that screening would lead to documentation in the EHR and inclusion in a national registry. There was the sense that screening was not necessary to do the other parts of the intervention and also a lack of trust and a feeling among gun owners that
a public health platform is a disguise for firearm control. “I think we really need to heed this message and attend to it,” Beidas said, “and on the same side of that coin, the need for partnership, which may allow us to heal that rift and to build trust. Our gun owner constituents suggested that it would be critical for health systems to think about partnering with firearm safety experts, such as safety course instructors, who are more credible and knowledgeable to firearm owners.”
As part of this work, Beidas and her collaborators generated a list of implementation strategies that they hope to test in a future trial:
- Creating a plan for who on the medical team will be responsible for implementing each component of the Firearm Safety Check.
- Changing the clinic or health system policies to encourage the implementation of the Firearm Safety Check.
- Integrating the intervention into the EHR.
- Training providers how to implement the Firearm Safety Check.
- Making changes to the workflow to make it easier to implement the intervention.
- Sharing information with providers and caregivers about the importance of the intervention and the problem it addresses.
- Developing marketing strategies targeting leadership and providers.
- Identifying and preparing provider and leader champions.
- Identifying sources of funding to support implementation.
One insight Beidas said she has gained is that it will likely be necessary to expand thinking beyond suicide prevention. “If we are going to be taking a universal approach, we should be thinking about unintentional and intentional firearm injury prevention so that we can make it most relevant to the broadest swath of the health system,” she said. Based on these studies, though, she said that she believes that Firearm Safety Check is feasible, acceptable, and ready for implementation with some tweaks. “I think the time is ripe, and I might ask: what are we waiting for?” she said. “We know that there is something that works, and we should be thinking about implementing it and testing the success of that implementation.” One necessary tweak will be to consider safety tools other than cable locks, which are not acceptable to many firearm owners, she said. One possibility is to incorporate a decision aid into the intervention so that parents can make informed decisions about which locking mechanism makes the most sense for them.
In closing, Beidas noted that this work is about keeping youth safe by promoting firearm safety. “This is not about firearm control, and that message needs to be the message that underpins all this work,” she said. “This cannot be about docs versus Glocks.” She noted, too, the importance of
partnering with all constituents, particularly gun owners. “If we want to be trusted, we need to leave our politics outside of the exam room and work together around these issues related to firearms. I would go even further to say we must hear the voice of all stakeholders, not just the ones we want to hear.”
Going forward, she said, there is a great deal to learn about how best to partner with firearm owners around a shared agent and build trust. There are also questions related to how to adapt the intervention to optimize its effectiveness and whether the intervention should be universal or targeted. Effectiveness trials with rigorous endpoints are needed, she said, as are large implementation trials testing different implementation strategies to see which ones result in the best uptake.
STATE OF THE SCIENCE FOR HOSPITAL-BASED VIOLENCE: RESEARCH AND POLICY IMPLICATIONS
HVIPs, Fischer explained, combine a brief in-hospital intervention with intensive, community-based case management and provide targeted services to high-risk populations to reduce the risk factors for re-injury and retaliation while cultivating protective factors. What this means in practice, he said, is that when someone comes into the hospital having been injured violently, they must receive care using a team-based approach that extends long beyond leaving the hospital as a means of dealing with the traumas that started before the injury and the new traumas that persist after the injury (see Figure 7-3). “There are many things you need to do to make sure people heal,” Fischer said.
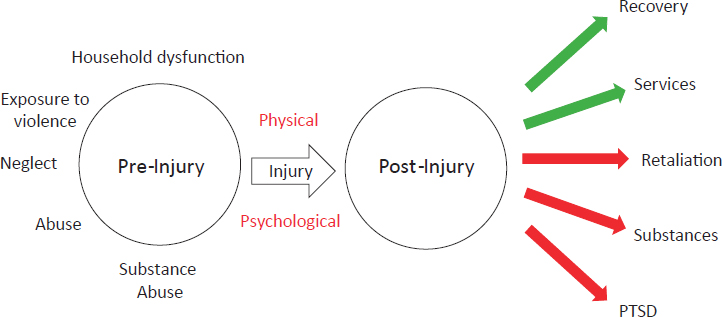
NOTE: PTSD = posttraumatic stress disorder.
SOURCE: As presented by Kyle Fischer at the workshop on Health Systems Interventions to Prevent Firearm Injuries and Death on October 18, 2018.
The HVIP takes a team-based approach centered on the patient to address all of these traumas preceding and resulting from violent injury. The team can include a doctor, case manager, trauma nurse, social workers, counselor, and the HVIP violence prevention professional. Fischer called the violence prevention professional the most important person on the team, the engineer that does all of the work and makes sure that everyone comes together to make sure the patient gets the services he or she needs. HVIPs typically hire these individuals from the communities in which they will work. Often, they also have a history of violent victimization and are therefore able to form a mentoring relationship with a victim and both translate and explain everything that team members say to them so that the patient follows through on their recommendations.
With that as background, Fischer highlighted some of the most important research on HVIPs. To begin with, data from 19 studies show clearly that without any program focused on people who have been injured violently, the rates of repeat violent injury range from 8 percent to 62 percent, with a median value of 27 percent (Greene, 2016). When an HVIP is involved, however, several observational trials have found the re-injury rate to be under 5 percent (Bell et al., 2018; Juillard et al., 2016). A retrospective cohort study that looked only at re-injury and death found no statistically significant benefit for an HVIP over the 18-month study period, but it did reduce the risk of criminal justice system involvement (Shibru et al., 2007), and two pediatric randomized controlled trials of programs similar to an HVIP though not as comprehensive found some benefits in terms of reducing fights and fight injuries in the months after an initial violent injury (Cheng et al., 2008a,b).
More data are needed in the pediatric realm, Fischer said, and he predicted that the work that Levas and others are doing will shed a great deal of light on what program components matter most for children. He noted that one common problem with doing randomized, controlled trials involving violence is that many institutional review boards consider them unethical and will not approve trials that do not provide the intervention to all participants.
For adults, there have been two randomized controlled trials showing a marked reduction in re-injury for individuals treated by an HVIP, with one trial showing a reduction in violent re-injury from 36 percent to 5 percent (Cooper et al., 2006) and the other from 20 percent to 8 percent (Zun et al., 2006). A third, small trial in which many of the individuals had already been sentenced to prison did not find a significant difference between the control and HVIP-treated group (Aboutanos et al., 2011). While none of these studies were perfect, Fischer said, they all found re-injury rates that were lower when an HVIP was administered than was seen in the 19 studies he mentioned earlier that did not include an HVIP. “Things are looking
promising,” he said, “and there are many places to fill in the gaps, but right now I am very encouraged by the data.” Currently, Fischer said, there is large trial of the Healing Hurt People program in Philadelphia that should be able to provide the most definitive data yet on the effectiveness of HVIPs.
Helping those who have been victims of violence is about more than just preventing re-injury and death, Fischer said, and there have been a variety of studies that have looked at the effect of HVIPs on the social determinants of health that play such an important role in firearm violence. One study, for example, found that over half of the victims of violence needed mental health services, and the HVIP was able to meet those needs for 85 percent of the participants (Juillard et al., 2016). Other studies, he noted, have looked at providing substance abuse treatments, services that address housing, education, and employment, and even tattoo removal.
In the policy realm, Fischer said, perhaps the most important change related to violence prevention programs has been the Patient Protection and Affordable Care Act’s (ACA’s) Medicaid expansion. “The Medicaid expansion includes young adults who earn less than 138 percent of the federal poverty level, and if you think about it, these are our patients,” Fischer said. In fact, he said, one analysis found that after the Medicaid expansion, U.S. taxpayers are now accountable for nearly half of the $10.7 billion in annual charges for the acute care of those injured by violence, which underscores the economic benefit to states and the federal government of preventing interpersonal violence. In fact, a modeling study that Fischer and his colleagues performed before the ACA went into effect found that states would find implementing HVIPs to be cost-effective and that it would perhaps save them money (Fischer et al., 2014).
DISCUSSION
Levas, responding to a question about data sharing among health care systems, community partners, and law enforcement, said that in an ideal world every partner would have access to all available data, which will require building partnerships and trust. The Health Insurance Portability and Accountability Act (HIPAA) creates some hurdles for the sharing of some hospital-level data, but data can be de-identified so that public health departments, for example, can request data without violating HIPAA regulations. “Getting the public health department within your city and state involved is crucial, because that can break down a lot of barriers,” Levas said. Political issues may create challenges for accessing police data, he added, but the district attorney’s office can often provide the same data.
Carol Pearson from Voice of America asked why someone would put a lock on a gun purchased for self-protection or store ammunition in one safe and the gun in another. Cunningham replied that, regardless of why a
family owns a gun, she does not know a single gun owner in the country that wants that gun used by their depressed teen or by their toddler. That, she said, is the reason to talk to families about why they need to store their guns safely, and that is the common ground around why safe storage needs to exist.
Pearson then asked why the panelists were optimistic, given the issues facing many of the victims of firearm injury and death and the lack of affordable mental health services in the communities most affected by gun violence. “This is a complex problem,” Cunningham replied, “but the idea that this problem is too complex for us to solve is simply garbage. There is no reason with proper investment that we cannot figure out how to get our head around a complex problem like this. In fact, even with almost no funding for the past 20 years to do any of this work, amazing groups around the country have bubbled up with innovative solutions, have put them into place, and have begun to find effects with even small programs along the way.” Levas added that mental health is receiving more funding—his group just received a large grant from the Department of Justice to expand mental health programming, for example, and it is planning to add embedded mental health workers to its team—because the community’s knowledge and funders’ knowledge about the importance of providing mental health services is evolving. Fein said that his program at the Children’s Hospital of Philadelphia has also added mental health workers to its team, and Beidas, a child psychologist, said that there are a number of evidence-based practices, such as trauma-focused cognitive behavioral therapy, that programs are drawing from to support their patients.
David Grossman asked the panel about the need to generate systematic evidence using common processes and outcomes to inform robust clinical guidelines. Fein replied that one goal of the research workgroup for NNHVIP was to formulate a set of common outcomes for its programs and measures for assessing those outcomes. The network is now working to develop a database to collect data on these common outcomes from multiple programs, he said.
An online workshop participant asked the panel to speak about the role that the American Academy of Pediatrics (AAP) plays in fostering practitioner and health system attention to violence. Levas replied that AAP has a council on injury and violence prevention that is working on recommendations, such as for car seat injuries, and is paying more attention to gun violence. “I think that the American Academy of Pediatrics has a large and important voice in recommending screening,” he said, “and right now they are talking about having screening in primary care clinics.” AAP has also supported large effectiveness trials, Beidas added.
Fischer noted that over the past few years physician specialty societies in general, including the American College of Surgeons’ committee on
trauma and the American College of Emergency Physicians (ACEP), have started looking at gun violence. In fact, ACEP recently passed a resolution saying that it believes violence to be a health-based problem with health-based solutions and public health–based solutions. Beidas cautioned that while it is important for physician specialty societies to give signals that firearm violence is something to attend to, practice will not change and guidelines will not be issued until there are strategies working at multiple levels to change clinician behavior.
Carnell Cooper asked the panelists about their screening procedures, and Beidas replied that when she does the implementation trial, she plans to work with health systems to tailor screening to fit the particular context of each clinical setting. Rowhani-Rahbar said that the intervention he and his colleagues are implementing includes multiphase screening that first determines if an individual meets the study’s eligibility criteria and then proceeds through tailored, case-by-case screening to determine what supports each individual needs.
Cunningham said that screening is complicated in health care settings, as illustrated by the challenges of screening for IPV. She strongly encouraged the field, as it moves to large-scale screening, to not get to the place that IPV screening is currently, which is that someone does it while looking at a computer with the spouse in the room and checks a box to move to a new screen in the EHR. One approach her team has taken has been to provide the patient with an iPad or laptop so that the patient can answer screening questions confidentially.
Cooper then asked if the panelists have support groups for their work, and Rowhani-Rahbar replied that part of the critical time intervention engages a patient’s support network to the extent possible. He said that he and his team have learned much about the role that mothers play in supporting many of the youths in the program. Cunningham stressed the importance of having support groups for program staff as well as for the participants.
Woodie Kessel from the Koop Institute at Dartmouth asked the panelists where the best opportunities for intervention are in terms of return on investment and where the best opportunities for scale-up exist. Regarding the first question, Cunningham said it is important to invest in a number of programs simultaneously, including resiliency-building components in communities or Project Ujima’s summer camps, in order to have the best chance of interrupting some of the early events that occur before guns become involved. Fischer added that investing in research networks would spur a great deal of activity. Levas, replying to the second question, said that identifying a strong adult in a child’s life plays an important role in getting a positive outcome, so his suggestion for scaling is to push an agenda that gets strong, innovative, smart-thinking community members involved in large numbers.
Daniel Webster commented that what has changed over the past 20 years is not the number of households with guns in them but instead the number of people walking around and driving around with guns in their possession. This, he said, is a new challenge that needs to be addressed, in addition to gun safety in the home. Beidas said she hopes that it will be possible to identify creative solutions for this new issue by working in partnership with gun owners. Cunningham added that research is needed to understand who is at a particularly bad or unstable moment in his or her life to be carrying a gun.
Meredith Wadman from Science magazine asked Beidas if she could explain why only 2 percent of the doctors in her study were routinely handing out gun locks, given that doing so does prevent suicides. Beidas replied that the reasons the physicians gave were mostly about operational concerns—who would pay for the gun locks, where would they be stored, how would they be distributed, who would teach people how to use the gun locks—rather than worries that they would offend parents by suggesting they lock their guns. In fact, she said, parents were excited about getting something free at the doctor’s office.




















