
1
Introduction
Despite significant advances achieved over the past 60 years in addressing the problem of traumatic injury, injury remains today an important cause of death and disability, by one estimate posing a burden of death and disability second only to that of cancer and just slightly greater than that of heart disease (Moses et al., 2015). Reflecting the magnitude of this burden, prior reports of the National Academies of Sciences, Engineering, and Medicine and others have addressed injury prevention and trauma care (see Box 1-1). Yet, funding directed at research on injury is not yet commensurate with the magnitude of the problem (see Figure 1-1).
Traumatic brain injury (TBI), defined in Box 1-2 and the focus of this report, represents only one type of accidental or deliberate injury. However, TBI was diagnosed in approximately 2 percent of the total emergency department (ED) visits, hospitalizations, and deaths in the United States in 2013 (Taylor et al., 2017), and half of military Veterans have reported a lifetime history of experiencing at least one TBI (Shura et al., 2019). TBI has been reported to contribute to 30 percent of injury-related deaths in a U.S. study (Taylor et al., 2017) and to 41 percent of years of life lost to premature death in a study of 16 European countries (Majdan et al., 2017). TBI thus represents a significant component of overall injury, providing an important opportunity to improve health and well-being if prevention, care, and recovery can be advanced.
STUDY CONTEXT
Every community and every segment of the population is affected by TBI. TBI affects civilian and military populations and occurs in both rural and urban settings. Causes as diverse as falls, sports injuries, vehicle collisions, intimate partner violence, and military incidents can result in such injuries across a spectrum of severity and among every age group, from babies and children, to adults, to the elderly.1Chapters 2 and 3 present a detailed look at the scope and burden of TBI.
___________________
1 Symptoms consistent with experiencing a TBI have also been reported after incidents among U.S. staff in Cuba, China, and other locations, and it has been suggested that these injures may be caused by radiofrequency energy. This report does not focus on such cases. (For a recent assessment, see NASEM, 2020.)
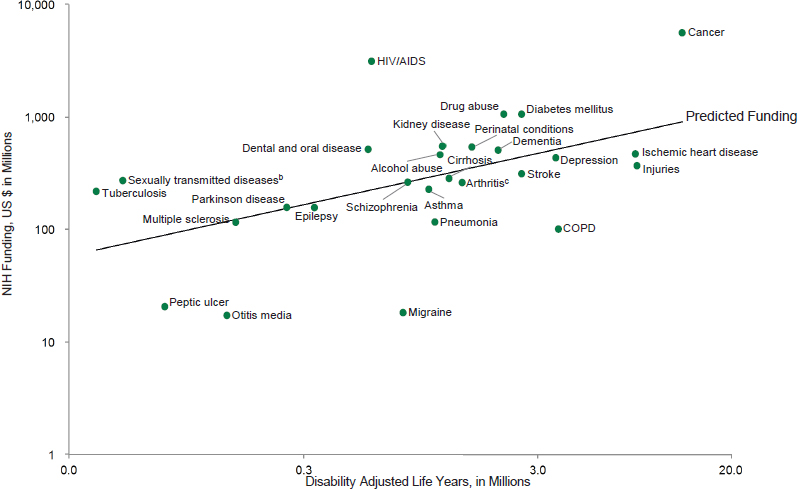
SOURCE: Moses et al., 2015. Reproduced with permission from the Journal of the American Medical Association. © 2015 American Medical Association. All rights reserved.
Just as the many causes of TBI and the people who experience it are diverse, so, too, are the physiological, cognitive, and behavioral changes that can occur following injury. An impact to the head, brain acceleration and deceleration, and the potential for the brain to shift internally and hit the opposite side of the skull can create bruising, damage the blood–brain barrier and blood vessels, and stretch or shear neurons and other cell types in the brain. These forces can lead to bleeding and swelling, as well as to a host of cellular and molecular events that lead to further damage, including disruption of neurotransmitter and ion flows in brain synapses, alterations in metabolism, and inflammatory responses. Although many people who experience a TBI have minor symptoms that resolve over hours or days, others experience alterations or loss of consciousness and have prolonged symptoms such as headaches, dizziness, vision and speech disturbances, agitation, cognitive dysfunction, and other long-term effects. One study found that even among those who had experienced an injury considered a mild TBI, 53 percent reported continued impairment a year later (Nelson et al., 2019). Headache is one of the most common symptoms after TBI (Lucas, 2015); however, experiencing one or more TBIs has also been connected to increased risk of developing anxiety, anger, depression, substance use disorders, and dementia, and to suicide and reduced life expectancy (Graham and Sharp, 2019; Harrison-Felix et al., 2015; Juengst et al., 2017; Madsen et al., 2018; Neumann et al., 2017; Shura et al., 2019). Table 1-1 lists examples of consequences that may arise after TBI.
The prevalence of TBI and the toll it can exact on those who experience it and their families make it an important area of investigation, although the vast heterogeneity of the condition makes assessment of TBI care and research particularly challenging. TBI is not a single type of injury with a single trajectory. Data from the Department of Defense indicate that more than 80 percent of TBIs are classified as “mild,” approximately 10–11 percent as “moderate,” and roughly 2 percent as “severe” or resulting from a penetrating head wound.2 Based on data from the Centers for Disease Control and Prevention (CDC), an unknown percentage of people do not seek or receive initial medical care after a potential TBI (CDC,
___________________
2 Information on TBI worldwide totals for the period 2000–2020 Q4, available online at DoD TBI Worldwide Numbers. https://health.mil/About-MHS/OASDHA/Defense-Health-Agency/Research-and-Development/Traumatic-Brain-Injury-Center-of-Excellence/DoD-TBI-Worldwide-Numbers (accessed October 4, 2021).
TABLE 1-1 Examples of Physical, Cognitive, and Behavioral Challenges Experienced After TBI
| Physical | Cognitive | Behavioral |
|---|---|---|
| Headache | Difficulty concentrating | Depression |
| Movement problems | Memory problems | Anxiety |
| Impaired or blurred vision | Reduced attention span | Agitation |
| Difficulties with speech or swallowing | Difficulty with problem solving | Reduced impulse control |
| Dizziness and balance problems | Confusion | Increased anger or irritability |
| Seizures | Increased risk of Alzheimer’s disease, Parkinson’s disease, and other neurodegenerative disorders | |
| Fatigue | ||
| Pain | ||
| Sleep problems |
NOTE: This list is intended to illustrate symptoms that can develop after TBI and is not intended to be exhaustive or to represent the experiences of all people who experience such an injury.
2015), while among those seeking care, the CDC data show that 86 percent of those who received initial care were treated and released from the ED (indicating a generally less serious injury), 12 percent were hospitalized and subsequently discharged, and 2 percent died.3Chapters 2 and 3 further explore who experiences TBI and what personal and social burdens the condition poses.
Patients with TBIs across the spectrum of severity may enter the medical system through multiple points, ranging from emergency medical services in the field, to presentation to an athletic trainer in a training room, to evaluation in a primary care setting. This breadth of entry points to clinical care for TBI, along with the variety of care providers potentially involved, presents challenges both to the medical system and to patients and families as they navigate care and recovery.
Differing mechanisms and severity of injury may also result in vastly different clinical courses. Adult patients sustaining moderate or severe TBI, such as from a motor vehicle crash, may find themselves transported by emergency medical services to the ED of a trauma center, with subsequent admission to the intensive care unit of the hospital, perhaps after urgent surgical intervention. This may be followed by an inpatient hospital stay and subsequent inpatient and outpatient rehabilitation, potentially over the course of months or even years. In contrast, a pediatric patient sustaining a mild TBI as the result of participation in a sport, such as soccer, may be evaluated immediately by school athletic personnel and referred to a sports medicine physician for evaluation, with management and oversight of return to learning and sports over the course of a few weeks. The many types of TBI and the many types of people who experience it thus contribute to a maze of clinical paths along which TBI patients may travel, making standardization of care for the optimization of outcomes challenging.
Areas for Improvement
Improving TBI care and research will require addressing essential components across the full spectrum of prevention, treatment, and recovery while recognizing and building on patient and community experiences. These components include the following:
- Understanding the scope and causes of TBI and the experiences of those who are faced with or at risk of injury. At the core of any process of improvement in TBI care and research are the needs and participation of those who experience these injuries. Care and research also need to be connected to population-level surveillance to gain insights on the scope of the problem and aid in designing prevention approaches.
- Developing, deploying, and improving prevention strategies. The most effective way to improve outcomes of TBI is to prevent people from experiencing such an injury in the first place. Although primary injury prevention is not the focus of this report, the committee emphasizes its importance in any comprehensive framework for understanding and improving the overall TBI system.
- Identifying everyone who has experienced a TBI and needs care. To this end, accurate and timely screening and diagnosis are required.
- Providing high-quality care to those who have experienced one or more TBIs and facilitating the most successful recovery achievable for that person. Care elements include sufficient access to care and appropriate treatment capacity, provision of the most effective care possible according to current medical understanding and best practices, and delivery of coordinated care. A multidisciplinary response to TBI is
___________________
3 See https://www.cohenveteransbioscience.org/traumatic-brain-injury (accessed December 1, 2021).
- Developing a research system capable of supporting improved understanding of TBI and the development of treatments and other interventions that can improve outcomes and address identified gaps and needs for persons with TBI and their families.
- Creating processes for feedback, learning, and improvement within the TBI system. Such processes are part of establishing an interconnected, learning health care system for TBI.
often required. No single medical specialty or care provider has the clear lead role in TBI.
The overall TBI ecosystem also encompasses networks beyond health care and research. It includes the related systems that administer and finance health care, accredit care facilities, and provide regulatory approval and oversight of products and therapies. It also intersects with the wide range of community organizations and institutions in which people return to learning, work, and play after experiencing a TBI, including the education system, work environments, professional and amateur sports associations, the criminal justice system, and others. In short, TBI affects a cross section of society and can touch nearly all health care and community institutions. And it involves more than biomedical factors, encompassing social, psychological, and ecological dimensions that significantly affect care and long-term outcomes (see further discussion in Chapters 2 and 3). The present report cannot delve into these many networks and intersections in detail, but emphasizes that TBI needs to be situated within this bigger picture.
Recent TBI Efforts
Efforts by military and civilian federal agencies, foundations, clinicians and researchers, and patient and family advocacy organizations over decades have focused attention on TBI and raised awareness of the needs and challenges it poses. In 2019, for example, federal agencies provided more than $300 million for TBI research.4 A variety of efforts to better understand TBI and its management are highlighted in Table 1-2; these and other developments are summarized in Appendix A. Additional efforts and networks address related issues in emergency medical services and trauma care, mental health, and other topics.
These various programs have generated valuable longitudinal data on the recovery trajectories of those who experience TBI, increased researchers’ and clinicians’ understanding of the pathophysiology of brain injuries, and resulted in such successes as a Food and Drug Administration (FDA)–approved blood-based biomarker to help identify concussion (see FDA, 2018).
Collectively, the knowledge gained represents an important base of information for analyzing both areas of progress and areas in which more widespread implementation of best practices or the acquisition of new knowledge can improve care and outcomes for those who experience TBI. Federal agencies involved in the decade-long National Research Action Plan (NRAP) on posttraumatic stress disorder, mental health conditions, and TBI, established in 2013, are looking ahead to next steps. The Brain Trauma Blueprint is designed to foster public–private collaboration around TBI research needs to advance precision medicine, and the Department of Defense (DoD) is moving forward with its Warfighter Brain Health Strategy. Now is the time to advance military and civilian TBI research and care, and this report is intended to contribute to those strategic planning efforts.
___________________
4 Based on a search for traumatic brain injury or TBI in the federal RePORTER database, available at https://federalreporter.nih.gov (accessed August 25, 2021). See also Appendix A for further information on federal support for TBI research.
TABLE 1-2 Selected TBI Research Efforts
| Effort | Key Funders | Year(s) | Target Population(s) | Description |
|---|---|---|---|---|
| Research Consortia, Initiatives, and Networks | ||||
| Collaborative European NeuroTrauma Effectiveness Research in TBI (CENTER-TBI) | 20 European universities | 2013–present | European civilians | Various efforts to study TBI, develop TBI databases, and translate research to policy |
| Chronic Effects of Neurotrauma Consortium (CENC) | DoD, VA | 2013–2019 | Military personnel (Veterans) | Study to investigate the long-term effects of mild TBI (mTBI) among military service personnel and Veterans |
| Collaborative Neuropathology Network Characterizing Outcomes of TBI (CONNECT-TBI) | NINDS, University of Pennsylvania | 2020–present | Athletes, military personnel, and civilians | Network to promote the sharing of tissue and datasets |
| Concussion Assessment, Research and Education Consortium (CARE) | NCAA, DoD | 2014–present | Student athletes and cadets | Study to explore concussive injury and recovery |
| International Initiative for Traumatic Brain Injury Research (InTBIR) | NIH, European Commission, Canadian Institutes of Health Research | 2011–2019 | Civilians, military personnel, athletes, and pediatric populations | International effort to reduce TBI burden by leveraging and coordinating TBI research |
| Long-term Impact of Military-relevant Brain Injury Consortium (LIMBIC) | DoD, VA, universities, private research institutions | 2019–present | Military (Veterans) | Further research for TBI military personnel and Veterans (newest iteration of CENC) |
| TBI Endpoint Development Initiative (TED) | DoD, FDA, PPPs | 2014–present | Civilians, athletes, military personnel | Efforts to identify/validate measures of TBI and recovery |
| TBI Model Systems (TBIMS) | NIDILRR, (Administration for Community Living, HHS) | 1987–present | Civilian | Longitudinal study of long-term outcomes of individuals with moderate-severe TBI who received inpatient rehabilitation; the network also supports projects aimed at meeting the needs of individuals with TBI |
| Transforming Research and Clinical Knowledge in TBI (TRACK-TBI) | NIH, DoD, OneMind, NeuroTrauma Sciences LLC, Abbott Laboratories | 2009–present | Civilian | Largest-scale initiative to analyze clinical TBI data and TBI outcomes |
| VA TBMIS Research Program | VA, NIDILRR (HHS) | 2008–present | Military service members and Veterans | Longitudinal study of outcomes after inpatient rehabilitation at 5 VA Polytrauma Rehabilitation Centers |
| Enabling Research Infrastructure | ||||
| Common Data Elements (CDE) | NIH, HHS | 2010–present | Effort to create data standards for TBI clinical research | |
| Effort | Key Funders | Year(s) | Target Population(s) | Description |
|---|---|---|---|---|
| Federal Interagency TBI Research Informatics System (FITBIR) | DoD, VA, NIH | 2011–present | Military personnel and civilians | Centralized TBI research database |
| Research Agenda and Priority Setting | ||||
| Brain Trauma Blueprint | Cohen Veterans Bioscience | 2019–present | Military personnel and civilians | Framework for identifying gaps and synthesizing information to advance precision diagnostics and therapeutics, building on a 2019 summit |
| Congressionally Directed Medical Research Program on TBI and Psychological Health | Congress | 2007–present | Military personnel | Support for research in TBI prevention, detection, diagnosis, treatment, and rehabilitation |
| National Research Action Plan on TBI and PTSD (NRAP) | DoD, VA, HHS | 2013–present | Military personnel and civilians | Established by a 2012 executive order to address research and care gaps |
| Education and Awareness | ||||
| HEADS UP | CDC | 2003–present | Youths and the elderly | Educational initiatives to improve TBI awareness and prevention among youths and the elderly |
NOTE: CDC = Centers for Disease Control and Prevention; DoD = Department of Defense; DOE = Department of Energy; FDA = Food and Drug Administration; HHS = Department of Health and Human Services; NCAA = National Collegiate Athletic Association; NFL = National Football League; NIDILRR = National Institute on Disability Independent Living and Rehabilitation Research; NIH = National Institutes of Health; NINDS = National Institute of Neurological Disorders and Stroke; PPP = public–private partnership; TBI = traumatic brain injury; UCSF = University of California, San Francisco; VA = Department of Veterans Affairs.
STUDY PURPOSE, SCOPE, AND APPROACH
Recognizing the importance of and opportunities for improving TBI care and research, DoD’s Combat Casualty Care Research Program asked the National Academies to convene an ad hoc committee of experts to consider the challenges entailed in achieving such improvements and recommending steps that can be taken to overcome those challenges. The committee’s statement of task is present in Box 1-3. The committee quickly realized that no one study could fully address the many networks and intersections outlined above, and so, while emphasizing the importance of situating TBI within that bigger picture, focused on identifying both gaps in and opportunities to advance TBI care and research. The committee also identified prevention as an essential topic, though not covered explicitly in its statement of task, sitting firmly at the beginning of the chain of care. This report represents the committee’s response to its statement of task, documenting its understanding of the many crucial elements that need to form part of an optimized system for TBI care and research and presenting a roadmap for accelerating progress toward achieving that system.
The committee formed to carry out this complex task included 18 members with expertise in basic, translational, and clinical research on TBI; epidemiology; neurotrauma; systems of care for TBI, from acute emergency medicine and trauma care through rehabilitation and community reintegration; neuropsychology and mental health; and health sciences and health care policy. The committee met virtually over the course of the study, holding meetings
approximately monthly to discuss and analyze the evidence and develop the conclusions and recommendations presented in this report. Evidence was gathered through a literature review, as well as a series of public virtual workshop sessions held in March and April 2021 and public webinars held in May and June 2021, with speakers who generously shared their knowledge and experiences with the committee. See Appendix C for further information on how the committee conducted its work and Appendix D for brief biographies of committee members and staff.
ORGANIZATION OF THE REPORT
Chapter 2 of this report describes the extent of the problems posed by TBI and the experiences and burdens reported by patients and families. Chapter 3 describes how bio-
logical, psychological, social, and ecological factors affect the experience of and outcomes following TBI, and introduces the care and recovery continuum. Chapter 4 highlights the role of prevention in reducing the numbers of TBIs that occur and explores awareness of and misconceptions about the condition. This information lays the foundation for the committee’s identification of actions that can be taken to make progress in improving TBI care and research.
The report then turns to the patient journey and care pathways following a TBI.
Chapter 5 focuses on the acute phase of care, from the point of injury and prehospital assessment through hospital care and transition to rehabilitation. Chapter 6 addresses the post-acute and longer-term phase of care, emphasizing rehabilitation, recovery to the extent possible, and community reintegration. Each of these chapters lays out the goals and main elements of care provided to a person who has experienced a TBI and identifies a number of remaining clinical gaps and needs for that phase of care.
In Chapter 7, the report examines major gaps, challenges, and opportunities for advancing TBI care and research. The opportunities identified include implementing a new clinical classification system for TBI; using emerging biomarkers as part of an expanded TBI toolkit; learning from and building on existing care systems and networks; increasing patient, family, and stakeholder engagement; and employing additional types of study designs.
Finally, Chapter 8 details the essential elements of an optimized system for accelerating progress in the TBI field, emphasizing the need for a coordinated system capable of more effectively connecting current programs and networks and providing a locus for efforts to advance TBI care and research. This chapter provides the committee’s recommendations for actions that can be taken to help achieve an optimized TBI system and a research agenda for addressing unanswered questions.
REFERENCES
ACS (American College of Surgeons) Committee on Trauma. 1976. Optimal hospital resources for care of the seriously injured. Bulletin of the American College of Surgeons 61(9):15-22.
APA (American Psychiatric Association). 2013. Diagnostic and statistical manual of mental disorders, fifth edition (DSM-5). Arlington, VA: APA.
Bulger, E. M., T. E. Rasmussen, G. J. Jurkovich, T. C. Fabian, R. A. Kozar, R. Coimbra, T. W. Costantini, J. Ficke, A. K. Malhotra, M. A. Price, S. L. Smith, W. G. Cioffi, and R. M. Stewart. 2018. Implementation of a National Trauma Research Action Plan (NTRAP). Journal of Trauma and Acute Care Surgery 84(6):1012-1016.
CDC (Centers for Disease Control and Prevention). 2015. Report to Congress on traumatic brain injury in the United States: Epidemiology and rehabilitation. National Center for Injury Prevention and Control; Division of Unintentional Injury Prevention: Atlanta, GA.
DoD (Department of Defense). 2012. Military acute concussion evaluation form. Defense and Veterans Brain Injury Center. https://health.mil/Reference-Center/Forms/2015/04/30/MACE-2012 (accessed July 31, 2021).
DoD. 2015. Traumatic brain injury: Updated definition and reporting. Memorandum for Assistant Secretary of the Army (Manpower and Reserve Affairs), Assistant Secretary of the Navy (Manpower and Reserve Affairs), Assistant Secretary of the Air Force (Manpower and Reserve Affairs), and Director, Joint Staff, from the Assistant Secretary of Defense, April 6, 2015. https://www.health.mil/Reference-Center/Policies/2015/04/06/Traumatic-Brain-Injury-Updated-Definition-and-Reporting (accessed July 31, 2021).
FDA (Food and Drug Administration). 2018. FDA authorizes marketing of first blood test to aid in the evaluation of concussion in adults. FDA News Release.https://www.fda.gov/news-events/press-announcements/fda-authorizes-marketing-first-blood-test-aid-evaluation-concussion-adults (accessed July 30, 2021).
French, L., M. McCrea, and M. Baggett. 2008. The Military Acute Concussion Evaluation (MACE). Journal of Special Operations Medicine 8(1):68-77.
Giza, C., J. Kutcher, S. Ashwal, J. Barth, T. Getchius, G. Gioia, G. Gronseth, K. Guskiewicz, S. Mandel, G. Manley, D. McKeag, D. Thurman, and R. Zafonte. 2013. Summary of evidence-based guideline update: Evaluation and management of concussion in sports: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 80(24):2250-2257.
Graham, N. S., and D. J. Sharp. 2019. Understanding neurodegeneration after traumatic brain injury: From mechanisms to clinical trials in dementia. Journal of Neurology, Neurosurgery & Psychiatry 90:1221-1233.
Harrison-Felix, C., C. Pretz, F. Hammond, J. Cuthbert, J. Bell, J. Corrigan, A. Miller, and J. Haarbauer-Krupa. 2015. Life expectancy after inpatient rehabilitation for traumatic brain injury in the United States. Journal of Neurotrauma 32(23):1893-1901.
Juengst, S. B., R. Kumar, and A. K. Wagner. 2017. A narrative literature review of depression following traumatic brain injury: Prevalence, impact, and management challenges. Psychology Research and Behavior Management 10:175-186.
Lucas, S. 2015. Posttraumatic headache: Clinical characterization and management. Current Pain and Headache Reports 19(10):48. https://doi.org/10.1007/s11916-015-0520-1.
Madsen T, A. Erlangsen, S. Orlovska, R. Mofaddy, M. Nordentoft, and M. E. Benros. 2018. Association between traumatic brain injury and risk of suicide. Journal of the American Medical Association 320(6):580-588.
Majdan, M., D. Plancikova, A. Maas, S. Polinder, V. Feigin, A. Theadom, M. Rusnak, A. Brazinova, and J. Haagsma. 2017. Years of life lost due to traumatic brain injury in Europe: A cross-sectional analysis of 16 countries. PLoS Medicine 14(7):e1002331. https://doi.org/10.1371/journal.pmed.1002331.
Malec, J. F., A. W. Brown, C. L. Leibson, J. T. Flaada, J. N. Mandrekar, N. N. Diehl, and P. K. Perkins. 2007. The Mayo classification system for traumatic brain injury severity. Journal of Neurotrauma 24(9):1417-1424.
McCrory, P., W. Meeuwisse, J. Dvorak, M. Aubry, J. Bailes, S. Broglio, R. C. Cantu, et al. 2017. Consensus statement on concussion in sport—The 5th International Conference on Concussion in Sport held in Berlin, October 2016. British Journal of Sports Medicine 51(11):838-847.
Menon, D. K., K. Schwab, D. W. Wright, and A. I. Maas. 2010. Demographics and Clinical Assessment Working Group of the International and Interagency Initiative toward common data elements for research on traumatic brain injury and psychological health. Position statement: Definition of traumatic brain injury. Archives of Physical Medicine and Rehabilitation 91(11):1637-1640.
Moses, H., D. Matheson, S. Cairns-Smith, B. P. George, C. Palisch, and E. R. Dorsey. 2015. The anatomy of medical research: US and international comparisons. Journal of the American Medical Association 313(2):174-189.
NAS and NRC (National Academy of Sciences and National Research Council). 1966. Accidental death and disability: The neglected disease of modern society. Washington, DC: National Academy Press.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2016. A national trauma care system: Integrating Military and civilian trauma systems to achieve zero preventable deaths after injury. Washington, DC: The National Academies Press.
NASEM. 2019. Evaluation of the disability determination process for traumatic brain injury in veterans. Washington, DC: The National Academies Press.
NASEM. 2020. An assessment of illness in U.S. government employees and their families at overseas embassies. Washington, DC: The National Academies Press.
Nelson, L. D., N. Temkin, S. Dikmen, J. Barber, J. Giacino, E. Yuh, H. Levin, et al. 2019. Recovery after mild traumatic brain injury in patients presenting to US level I trauma centers: A Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) study. JAMA Neurology 76(9):1049-1059.
Neumann, D., J. F. Malec, and F, M. Hammond. 2017. Negative attribution bias and anger after traumatic brain injury. Journal of Head Trauma Rehabilitation 32(3):197-204.
NRC and IOM (National Research Council and Institute of Medicine). 1985. Injury in America: A continuing public health problem. Washington, DC: National Academy Press.
Shura, R. D., S. Nazem, H. Miskey, T. Hostetter, J. Rowland, L. Brenner, VA Mid-Atlantic Mirecc Workgroup, and K. H. Taber. 2019. Relationship between traumatic brain injury history and recent suicidal ideation in Iraq/Afghanistan-era veterans. Psychological Services 16(2):312-320.
Taylor, C., J. M. Bell, M. J. Breiding, and L. Xu. 2017. Traumatic brain injury–related emergency department visits, hospitalizations, and deaths—United States, 2007 and 2013. Morbidity and Mortality Weekly Report 66(9):1-16.
VA (Department of Veterans Affairs). 2015. Fact sheet: Coding guidance for traumatic brain injury (TBI).http://www.rstce.pitt.edu/va_tbi/documents/11192015/11192015_03.pdf (accessed July 31, 2021).












