
Shiriki Kumanyika, research professor in the Department of Community Health and Prevention, Drexel University Dornsife School of Public Health, and professor emerita of epidemiology at the University of Pennsylvania Perelman School of Medicine, set the stage with a contextual overview of the workshop. She echoed Purcell’s comments about the roundtable’s continuing discussions on health equity, remarking that this workshop’s equity focus “may indeed be a transformative moment” for the group and perhaps for health equity issues in obesity prevention and treatment in the United States overall.
KEY DEFINITIONS
Kumanyika began by posing the question that she said the workshop aspired to answer: “Why is obesity a health equity issue, and what can we do about it?” She offered definitions for the terms “health equity,” “disparities,” and “excluded or marginalized groups” (see Box 2-1), emphasizing the importance of using common definitions for the workshop. She noted that although “disparities” is a more familiar term, the field has moved toward the term “health equity,” which she identified as the aspirational
goal. She clarified further that disparities are the measure of a lack of health equity, and that health equity means reducing and ultimately eliminating disparities in both health and its determinants that adversely affect excluded or marginalized groups. Kumanyika stressed the importance of reducing disparities in both absolute and relative terms, explaining that closing the gaps is to be achieved by making special efforts to improve the health of such groups, not by worsening the health of those who are better off. Although the latter would technically reduce disparities, she added, the goal is to simultaneously improve the trajectory of health across the population and close the gaps that exist today.
Kumanyika remarked further that the term “excluded and marginalized groups” has broadened to include any economically and/or socially disadvantaged group. She clarified that the workshop would focus on racial, ethnic, and minority groups, and in some cases, low-income populations. Excluded or marginalized groups have also been referred to as “priority populations,” she continued, a term she said was developed to refer to populations that deserve priority in public health, prevention, and treatment efforts. She urged participants to consider these populations as groups with assets and power to overcome disadvantages, instead of focusing on their economic and/or social deficits, a framing that she called “disempowering.”
CONTEXTUAL INFLUENCES ON OBESITY
Next, Kumanyika presented a conceptual framework to describe how contexts influence obesity (see Figure 2-1). The focus of prevention and treatment efforts tends to be on the weight-related behaviors and outcomes shown at the right of the figure, she explained, listing as examples food security, food intake, dietary quality, child feeding and parenting, physical activity, sedentary behavior, excess weight gain, ability to lose and maintain weight, body composition and fitness, and child growth and development. Kumanyika observed that this focus on individual behaviors can result in overlooking the intermediate variables shown in the center of the figure—such as those that influence food and physical activity behaviors, sleep health, chronic stress, and resource limitations—that perpetuate those behaviors (see Box 2-2).
Further upstream, Kumanyika went on, are the broader historical, social, economic, physical, and policy contexts at the left of Figure 2-1 that influence the intermediate variables. These upstream determinants include legal risks and the protection of the law, institutionalized racism or other forms of discrimination, employment, education, neighborhood/locality, and political voice. According to Kumanyika, many of these contexts are often taken for granted, and if all of them are favorable, weight control looks easy or at least feasible. But if these broad upstream determinants
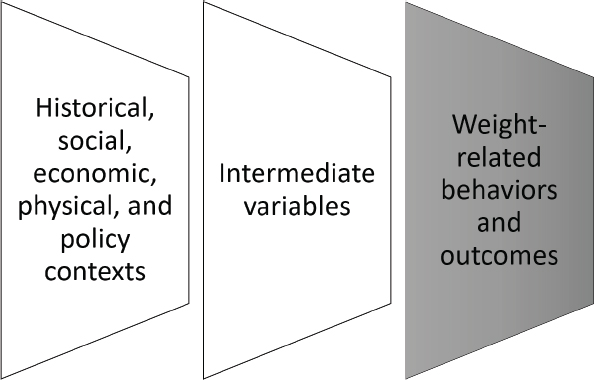
SOURCE: Presented by Shiriki Kumanyika, April 1, 2019. Reprinted with permission.
are absent or unfavorable, she asserted, the many other factors embedded within them (see Box 2-3) can present challenges.
In summary, Kumanyika stressed that the issues involved in considering health equity and addressing disparities cannot be oversimplified, adding that the average person who is in a socially disadvantaged situation is dealing with a cumulative set of factors that must be overcome to work toward achieving a healthier weight. Finally, she emphasized that political voice cannot be taken for granted, as it is an important tool for overcoming social disadvantage, especially for those experiencing discrimination.






