
3
Development Happens in Contexts: Overview of Early Life Critical Influences
INTRODUCTION
To ensure healthy and optimal development for all children, there is a need to understand how the context that a child grows in and the cumulative risk associated with that specific context shape the odds for thriving. Sir Michael Rutter, the first professor of child psychiatry in the United Kingdom, is credited as one of the first to bring the concept of cumulative risk to the study of child development. In his now classic work studying 10-year-old children, he documented that children who had two or more risk factors had a four-fold risk for having a psychiatric disorder (Rutter, 1979). Approximately a decade later, Sameroff and colleagues extended this work to young children’s social and emotional competences (Sameroff et al., 1987a) and cognitive outcomes (Sameroff et al., 1987b). Since these studies, and the subsequent publication of From Neurons to Neighborhoods (NRC and IOM, 2000), there has been a rapid increase of cross-disciplinary research using an accumulation of risk models to assess early childhood social risk factors in relation to outcomes across the life course. Understanding the origins and mechanisms of the contextual factors and cumulative risk that produce inequities for children and families is a prerequisite to advance health equity.
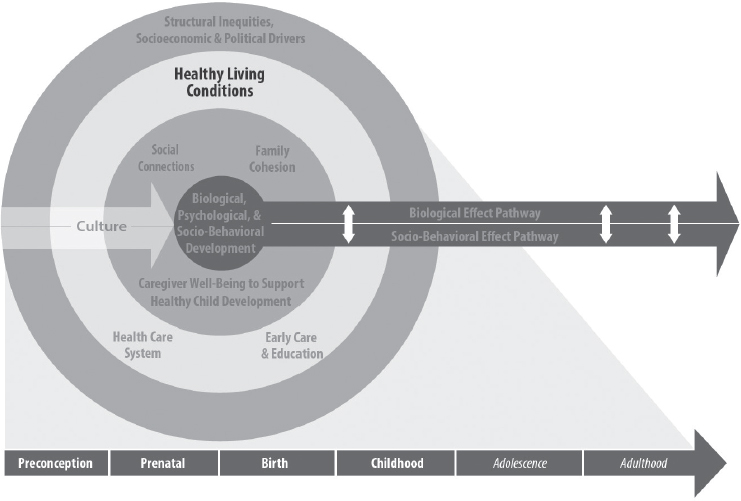
While Chapter 2 discusses the mechanisms of healthy development within the growing child, this chapter provides an overview of the key early life protective and risk factors associated with development, as indicated in the committee’s Statement of Task. This chapter discusses how each of these factors and conditions shapes health and safety, mental
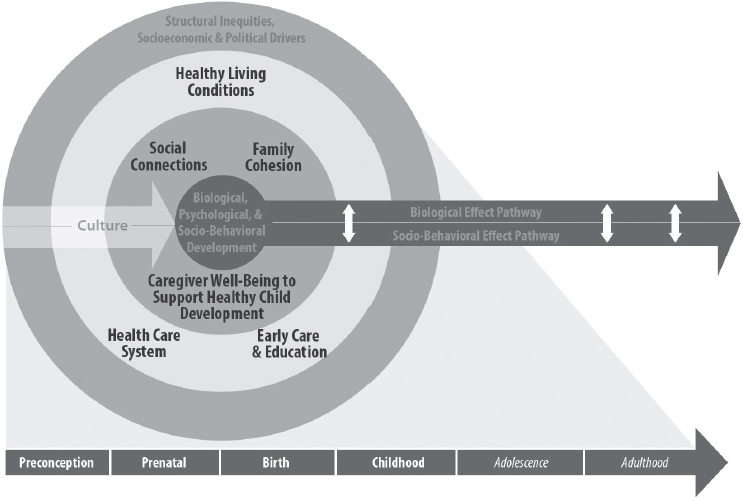
NOTES: The domains of focus in this chapter are reflected in the second and third rings in the model. These elements are bolded for emphasis.
and emotional well-being, and cognitive health during the prenatal and early childhood phases by mapping each factor to both the conceptual model and the forthcoming solution-driven Chapters 4–8 (see Figure 3-1 and Table 3-1 for how the content in this chapter maps to the conceptual model and the following chapters, and Box 3-1 for a high-level chapter overview). The committee identified domains by which to group these critical influences, with a focus on factors that shape inequities at the
TABLE 3-1 Mapping Chapter 3 Content to Chapters 4–7
| Critical Influences in Prenatal and/or Early Childhood Stages Discussed in This Chapter | Corresponding “Action” Chapter |
|---|---|
| Family cohesion and social connections | Chapter 4 |
| Health care | Chapter 5 |
| Economic security | Chapter 6 |
| Neighborhood conditions (e.g., concentrated disadvantage, physical and social environments, violence and crime, housing, environmental exposures) | Chapter 6 |
| Early care and education | Chapter 7 |
child, family, community, and population levels. These domains include family cohesion and healthy social connections (see Chapter 4); health care (see Chapter 5); healthy living conditions (i.e., economic security, nutrition and food security, housing, and environmental safety) (see Chapter 6); and early care and education (ECE) (see Chapter 7).
Committee’s Approach to Early Life Critical Influences
While there are many critical factors that shape development, the committee limited the scope of this chapter to include those with strong evidence for shaping affecting outcomes from the prenatal through early childhood periods. Where possible, the committee relied on high-quality systematic reviews and meta-analyses to provide a brief overview. To the extent possible, this chapter includes data and outcomes specific to the prenatal through early childhood periods; however, when those data are not available, data for caregivers and families are presented. The committee takes a life course approach in this report (see Figure 1-1), so, as such, it is important to note that many of the influences discussed in this
chapter manifest in adolescent and adult outcomes. In each domain, critical factors are addressed in terms of definition, overall prevalence and disparities, and prenatal, birth, and early childhood outcomes, including information on potential mechanisms when the evidence points to these.
Crosscutting Elements: Discrimination and Racism
Across all of the critical factors in this chapter, there are two crosscutting elements that the committee has identified as being pervasive and rooted in health inequities—discrimination and racism—that can be thought of as the mechanisms by which structural inequities operate. (See Box 3-2 for a description of the root causes of health inequities and key definitions from a related report.) The crosscutting elements operate at multiple levels (i.e., intrapersonal, interpersonal, institutional, structural) and shape the experiences of children and families across the domains discussed in the rest of this chapter (and this report). While race is considered a social rather than biological construct (i.e., created from prevailing social perceptions, historical policies, and practices), the consequences of racism and the experiences of racial and ethnic minorities have psychological, biological, and social consequences (NASEM, 2017a). For example, historical policies and practices, such as residential segregation, redlining of districts, and discriminatory banking practices, are structural
forms of racism that have long-lasting ramifications for the health of communities of color (NASEM, 2017a). This type of structural racism unfolds across many of the domains discussed in this chapter, including housing, economic stability, physical environment, and community violence. Furthermore, structural racism has been linked to historical trauma, which manifests from past treatment of specific racial or ethnic groups (NASEM, 2017a). This type of trauma is an important yet often “invisible” context that sets the stage for risk and resilience. Another example of a crosscutting element that is salient for this chapter is immigration-related experiences and challenges. For immigrant children or children of immigrants, there are unique barriers to achieving optimal health that play out at multiple levels and have serious implications for food security, housing stability, safety, and access to quality health care services. These important crosscutting elements will be highlighted throughout the chapter as they relate to the various factors that influence early development. The chapter will also discuss specific subgroups with unique needs or circumstances as they relate to these crosscutting elements, where appropriate.
FAMILY COHESION AND SOCIAL CONNECTIONS
Relationships in early childhood form the foundation for how children interact with their environment and other individuals across the life-span. This section discusses key influences that exist within the most proximal microsystem for children, consisting of family and peers. The following discussions include the scientific findings on experiences or factors that either enhance or undermine family cohesion and healthy social connections. Chapter 4 describes the interventions and mechanisms needed to support the family and promote healthy relationships. See Figure 3-2 for a visual of how this section ties to the report conceptual model.
Parental Factors
Parental well-being is a critical determinant of child health and developmental outcomes; therefore, what happens to the parent before, during, and after pregnancy has serious implications for the child. Parental mental health is inextricably linked to child well-being and there is consistent evidence that maternal depression compromises healthy child development (Center on the Developing Child at Harvard University, 2009; Goodman and Garber, 2017). Estimates show that 10–20 percent of mothers have lifetime prevalence of depression and the rates are much higher for mothers in low-income households. Because of the socioeconomic disparities in maternal depression and the implications for children’s development, maternal depression has been thought of as a contributing factor to the cycle of intergenerational poverty (Reeves and Krause, 2019).
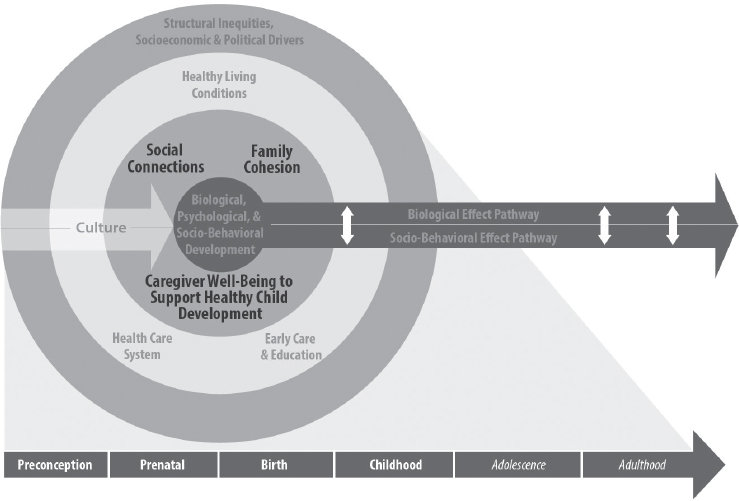
NOTES: The elements of focus in this section are reflected in the second innermost ring in the model: caregiver well-being and support, family cohesion, and social connections. These elements are bolded for emphasis.
For children, the consequences of maternal depression include neurodevelopmental and other biological disruptions and psychological and behavioral difficulties. Postpartum maternal depression specifically has been linked to the neurobiological pathways that shape emotional regulation, cognitive and executive function, and physiological stress response systems—all of which are critical functions and systems for ensuring optimal development (Drury et al., 2016). The Center on the Developing Child at Harvard University (2009) published a paper on the effects of maternal depression that indicated the following:
- Chronic depression can manifest in two types of problematic parenting patterns that disrupt the “serve and return”1 interaction that is essential for healthy brain development: hostile or intrusive, and disengaged or withdrawn.
___________________
1 “Serve and return” interactions occur when young children innately reach out for connection by babbling, using facial expressions, and gestures (i.e., serve), and adults respond with similar vocalization or gestures (i.e., return) (National Scientific Council on the Developing Child, 2004).
- Children who experience maternal depression early in life may have lasting effects on their brain architecture and persistent disruptions of their stress response systems.
- Maternal depression may begin to affect brain development in the fetus before birth.
While evidence exists that maternal depression is significantly related to children’s behavioral and emotional functioning, more research is needed to better understand moderating effects for various subgroups of children (Goodman et al., 2011). In addition to maternal depression, paternal depression has also been shown to negatively affect parenting behaviors and child developmental outcomes (Gutierrez-Galve et al., 2015; Ramchandani et al., 2011; Wilson and Durbin, 2010). Sweeney and MacBeth (2016) identify the following mediators of the effect of paternal depression on children: paternal negative expressiveness, hostility, and involvement and marital conflict. There are other aspects of parental well-being for which evidence exists of an association with child health and well-being (e.g., parental alcohol or substance abuse or incarceration) (Conners et al., 2004; Lieb et al., 2002; Luthar et al., 2007; Nichols and Loper, 2012; VanDeMark et al., 2005). Additional select parent-specific factors that have been shown to be associated with child health and well-being outcomes include incarceration (see Chapter 4), interaction with the welfare system (see Chapter 4), adverse childhood experiences (ACEs) (see the Adverse Childhood Experiences section at the end of this chapter), and intimate partner violence (IPV).
IPV has adverse effects on pregnancy and birth outcomes (Boy and Salihu, 2004; Iliopoulou et al., 2012). A systematic review found that pregnant women who have experienced IPV are more likely to suffer from maternal mortality and have children who suffer from low birth weight (LBW) and infant mortality when compared to women who have not experienced IPV (Boy and Salihu, 2004). Research also suggests that children can suffer from harmful consequences associated with exposure to IPV, even if they have not directly observed the violence (Wathen and Macmillan, 2013). These consequences include social, emotional, and behavioral problems, such as mood and anxiety disorders, posttraumatic stress disorders, substance abuse, and school-related problems in childhood and adolescence. Rates of comorbidity between exposure to IPV and child maltreatment are high—some data show that 60–75 percent of families that have experiences of IPV also include children exposed to maltreatment (Osofsky, 2003).
Child Maltreatment
In the absence of safe and nurturing relationships, children are vulnerable to the effects of maltreatment, or child abuse and neglect.
The Child Abuse Prevention and Treatment Act defines child abuse and neglect as
any recent act or set of acts or failure to act on the part of a parent or caretaker, which results in death, serious physical or emotional harm, sexual abuse or exploitation, or an act or failure to act, which presents an imminent risk of serious harm.2
Generally, child abuse and neglect are grouped into four types: neglect and physical, sexual, and emotional abuse. See Box 3-3 for descriptions of the four types of maltreatment. Despite this definition, there remain challenges related to varying state legal definitions, data collection, and calculating accurate incidence and prevalence rates in population-based studies (IOM and NRC, 2014). Therefore, the magnitude of child abuse and neglect is more than likely underestimated in the United States (Fortson et al., 2016). Not only is child maltreatment detrimental to children’s health and well-being, it is also costly for the United States. Data from 2008 indicate that the total lifetime economic cost associated with child abuse and neglect amounted to approximately $124 billion (Fang et al., 2012).
Trends and Disparities
Despite the well-known consequences, child maltreatment is still too common today. At least one in seven children have experienced child abuse
___________________
2 42 U.S.C. § 5101 note.
or neglect in the past year, which is likely an underestimate (Finkelhor et al., 2015). State-level data on reports of child abuse and neglect show a 2.7 percent increase in the national rate of victims of child maltreatment from 2013 to 2017 (HHS, 2019).
Disparities in child maltreatment exist across groups by race and ethnicity, age, and socioeconomic status (SES). According to 2017 data from the National Child Abuse and Neglect Data System, rates of child abuse or neglect were reported to be highest for American Indian/Alaska Native (AI/AN) children (14.3 per 1,000 children). Following those are rates for African American (13.9 per 1,000), multiracial (11.3 per 1,000), Pacific Islander (8.7 per 1,000), white (8.1 per 1,000), Hispanic (8.0 per 1,000), and Asian (1.6 per 1,000) children. Likewise, the rate of fatalities due to maltreatment for African American children (4.86 per 100,000 children) is 2.6 times greater than that of white children and 3.1 times higher than that of Hispanic children (HHS, 2019).
Young children are the most vulnerable to child maltreatment (HHS, 2019), and more than one-fourth (28.5 percent) of child maltreatment victims are younger than 3 years. Overall, children under the age of 1 year are most likely to die from child abuse or neglect (see Figure 3-3). Very young children with disabilities have increased risk of child maltreatment when compared to children without disabilities—and rates of disability are higher among low-income populations that experience higher rates of preterm birth (Hibbard et al., 2007; NASEM, 2015a). Children living in poverty are disproportionately exposed to child abuse and neglect and experience five times the risk of child abuse or neglect as children from higher SES
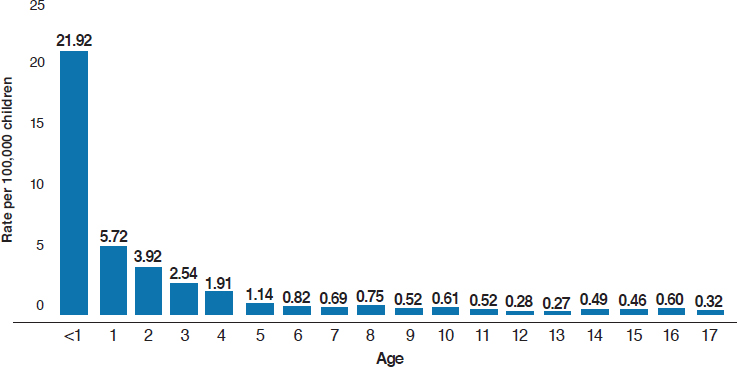
NOTE: Based on data from 44 states.
SOURCE: HHS, 2019.
households (Sedlak et al., 2010).3 It is important to note that disparities in child maltreatment have been attributed to other social, environmental, or economic factors, pointing to the need for a multilevel approach to preventing maltreatment (Fortson et al., 2016; Gilbert et al., 2009).
Outcomes Related to Child Maltreatment
Child maltreatment has a pervasive and harmful influence on many aspects of development and children who are exposed to a certain type of maltreatment are frequently exposed to others (Gilbert et al., 2009). Exposure to child abuse and neglect has serious ramifications for a child’s biological, behavioral, cognitive, and emotional development (Cicchetti and Handley, 2017). The relationship between child abuse and neglect and physiological, psychological, and behavioral outcomes has been well documented throughout the child development literature, and a comprehensive review was published in the 2014 Institute of Medicine (IOM) and National Research Council (NRC) report New Directions in Child Abuse and Neglect Research. Therefore, the literature review is not repeated here; key findings related to the effects of maltreatment from the 2014 IOM and NRC report are provided in Box 3-4. See Chapter 2 for more on biological mechanisms of development that can be hindered or enhanced through early experiences.
Peer Social Connections
For children, an important source of social connections is the peer group that they interact with. After experiences with primary caregivers and family members, peers are the most proximal interpersonal relationships for young children. Through peer relationships and interactions, young children learn and reinforce notions of reciprocal interactions. For example, young children learn how to share, take turns, and give and receive from interactions with other young children. From these experiences, they can also learn to interpret and take into account the needs and desires of others and to manage their own impulses (National Scientific Council on the Developing Child, 2004). From early on, peer interactions can have positive and/or negative effects on children’s mental, behavioral, and emotional health. (See Box 3-5 for findings and conclusions from a report on preventing bullying.)
___________________
3 In the Fourth National Incidence Study of Child Abuse and Neglect (NIS-4): Report to Congress, a low-socioeconomic status household was defined as having a household income below $15,000 per year; parent education level less than high school; or any member of the household receiving poverty program benefits (e.g., Temporary Assistance for Needy Families, food stamps, public housing, energy assistance, or subsidized school meals) (Sedlak et al., 2010).
Safe, Stable, Nurturing Relationships and Environments
While child abuse and neglect increase the risk for a host of mental and physical ailments, lifelong mental and/or physical anguish is not a foregone conclusion. There is clear scientific evidence that the presence of safe, stable, and nurturing relationships is critical to healthy development and can buffer the mechanisms of adversity and support positive trajectories (Bornstein and Leventhal, 2015; Bronfenbrenner and Morris, 2006; CDC, 2014; Luthar, 2006; Masten, 2014; National Scientific Council on the Developing Child, 2004). (For information on mechanisms of buffering
the stress response, see Chapter 2.) Safe, stable, and nurturing relationships are also important for preventing maltreatment, as they have been identified as a moderator of intergenerational child maltreatment. A meta-analysis found that adult relationships and parent–child relationships had a protective effect against intergenerational child maltreatment when they were safe, stable, and nurturing (Schofield et al., 2013). A stable relationship with caring adults is also important in child care settings, which can affect social competence, behavioral issues, and thinking and reasoning skills. In a 2004 summary of key scientific findings on relationships, the National Scientific Council on the Developing Child identified nurturing and stable relationships with caring adults as a cornerstone of healthy development. The Council identified “serve and return” as a key mechanism of healthy interactions between parents and babies, by which the brain architecture is strengthened. This is also important in child care settings, which can affect social competence, behavioral issues, and thinking and reasoning skills. Finally, the Council concluded based on the science that secure and stable relationships can protect children from illness, chronic stress, exposure to toxicants, and preventable injuries.
HEALTH CARE
In addition to the social determinants of health (SDOH) described throughout this report, health care itself plays a major role in child development through the life course. From preconception through early childhood, there are several aspects of health care that are critically important from an equity perspective: access to quality care, coverage, provider bias (or lack thereof), and provider cultural/linguistic competency. The following section provides an introduction to these issues along the continuum of preconception, prenatal, and pediatric health care; Chapter 5 provides a more in-depth look into opportunities to enhance these systems. See Figure 3-4 for a visual of how this section ties to the report conceptual model.
Preconception Care
The number of studies devoted to understanding preconception health and the interventions intended to improve health among women who may become pregnant have increased in recent years, but there is still a general paucity of data. According to a 2016 review of this research, results are mixed, and the studies themselves are generally of moderate to poor quality (Hussein et al., 2016). While preconception care may increase women’s knowledge about certain health conditions and pregnancy (Callec et al., 2014; Chuang et al., 2010), it is not clear if this translates to healthier outcomes for infants and children. Across eight randomized
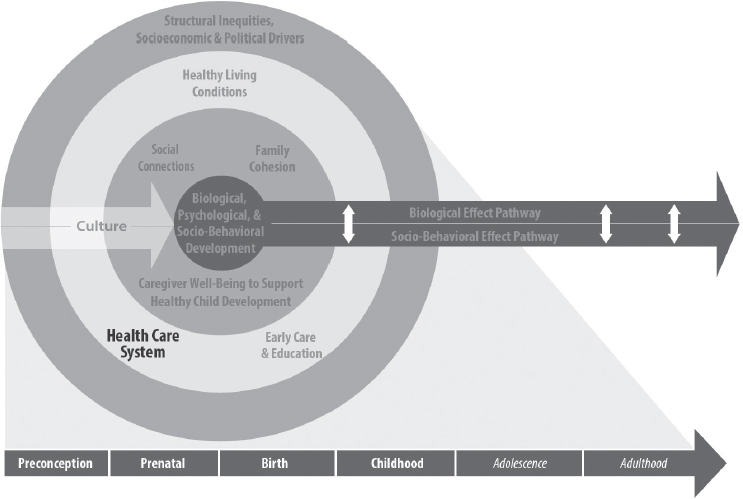
NOTES: The element of focus in this section is reflected in the second outermost ring in the model: the health care system. This element is bolded for emphasis.
controlled trials (RCTs) of preconception health care interventions, there was little evidence that interventions reduced adverse pregnancy outcomes (Hussein et al., 2016). This was true even though the interventions appeared to increase maternal knowledge and locus of control and reduce risky behaviors (Hussein et al., 2016).
It is also true that only a small minority of women receive preconception care, making it difficult to draw broad generalizations about its effectiveness (Hemsing et al., 2017). This is likely because access to preconception care is not widespread (Hemsing et al., 2017), and a recent review outlined several reasons why (Goossens, 2018). First, a lack of reimbursement mechanisms for administering preconception care reduces providers’ incentive to deliver it. Lack of reimbursement, payment mechanisms, or insurance are also reasons that preventive services and health promotion services are not delivered more generally (Goossens, 2018). Limited time and heavy workloads were a second reason that health care providers do not engage in preconception care with widespread frequency. A third reason was simply a lack of knowledge on the part of clients themselves (i.e., they were not aware of preconception care or did not seek it out) (Goossens, 2018). A fourth reason was that providers themselves did not think it was their duty to provide preconception care; primary care
providers, for instance, were likely to think it was the role of the obstetrician, and vice versa (Goossens, 2018). A final reason could be that, given the lack of strong evidence for improving birth outcomes (Hussein et al., 2016), women simply choose not to engage in preconception care because they do not think it will be effective.
Preconception care as currently conceptualized—typically a single medical visit initiated when one wants to become pregnant—is likely insufficient to address the accumulated life and medical risks up to that point for both parents. Thus, a broader, multisector view of preconception care seen through an SDOH lens is likely necessary to achieve the significant impact that would be expected when one mitigates potential risks prior to achieving pregnancy.
Prenatal Care
Delivered early and often, prenatal care increases the chances of delivering a healthy baby (Kilpatrick et al., 2017). Conversely, women who do not receive prenatal care are three to four times as likely to die from pregnancy-related issues compared to women who do receive such care (Bingham et al., 2011). There are well-documented negative effects on babies as well (Cox et al., 2011). Women who do not receive prenatal care are more likely to deliver babies that are underweight, preterm, and are more likely to die in infancy from respiratory problems, sudden infant death syndrome, and gastrointestinal issues; however, these outcomes are not solely due to lack of prenatal care (Association of Maternal & Child Health Programs, 2016).
In contrast to preconception care, prenatal care is one of the most common types of health care in the United States. In 2016, 77 percent of pregnant women initiated prenatal care in the first trimester of pregnancy (Osterman and Martin, 2018). Despite advances in prenatal care, there are significant disparities in coverage and access. Women who are young, are not white, have low educational attainment, or lack private insurance are more likely to have late or inadequate prenatal care (Osterman and Martin, 2018), and issues related to insurance coverage and access persist into postnatal life for the baby.
Pediatric Care
In general, the preponderance of evidence suggests that higher rates of health insurance have led to higher rates of pediatric health care access and better health outcomes for children (Leininger and Levy, 2015). Still, disparities in health care access remain, especially among those who do not have health insurance or have intermittent coverage (Leininger and Levy, 2015). While the number of children who are uninsured is low
(~5 percent of children 0–18 years old), this varies from 1 to 11 percent based on state of residence (Kaiser Family Foundation, 2017). Immigrant children, including those who are undocumented, are less likely to be insured than children of the same age with U.S. citizenship (Leininger and Levy, 2015). Some studies suggest that intermittent losses of coverage—which is more common among families with income near the Medicaid eligibility line—decreases children’s use of care (Leininger and Levy, 2015). For instance, one study found that even small gaps in insurance coverage decrease a visit to any doctor or a well-child visit by 4 and 9 percent, respectively (Leininger, 2009). Importantly, minority children are disproportionately likely to be from low-income families, particularly African American, AI/AN, and Hispanic children (Jiang et al., 2016). As a consequence of periodic bouts of being uninsured due to poverty (Leininger and Levy, 2015), these groups are less likely to receive routine pediatric care or treatment for medical conditions (Hodgkinson et al., 2017). These disparities in use are reflected in reported health statistics from parents: ethnic minority children are at least four times as likely to be described as in “fair or poor health” by their parents compared to white children. Similarly, children living in poverty are less likely to be described as in “excellent or very good health” by their parents (71 percent) compared to those not living in poverty (87 percent) (Kuo et al., 2012).
Barriers to Accessing Quality Health Care
There are a number of plausible reasons for the existing disparities in access to care, including lack of time and flexibility to seek services, long wait times, or the requirement of multiple appointments (Hodgkinson et al., 2017), and the decline of prenatal care in rural settings (Hung et al., 2017). These factors may make prioritizing pediatric care or treatment untenable for those living in poverty or enduring stress (Hodgkinson et al., 2017; Santiago et al., 2013).
It is important to note that, just as with other aspects of health care, bias and unequal treatment may play a role in women’s preventative services and prenatal care (IOM, 2002). Stereotyping and bias on the part of health care providers may increase disparities in preconception care, as has been suggested of prenatal care (Kogan et al., 1994). In particular, messaging that places all of the responsibility for the fetus’ health on mothers may serve to exacerbate stigmas among those already facing significant societal disparities (Greaves et al., 2014; Sue, 2019).
Stigma, bias, or lack of training on the part of health care professionals may also exacerbate pediatric health care disparities (Sue, 2019). Some studies have shown that providers for lower-income families admit to these challenges, including a lack of understanding and training about the effects of poverty on children, confrontation of their own personal
prejudice and biases, stigma that comes with working with low-income families and children, and difficulty applying typical diagnostic frameworks to children from low-income families (Smith et al., 2011, 2013).
As outlined in the 2016 National Academies report Parenting Matters: Supporting Parents of Children Ages 0–8, medical providers (and service providers more generally) are met with increasing pressure to provide care in a culturally and linguistically sensitive way. Because of rapid changes in demographics, medical providers may face difficulty in adapting to language barriers or cultural norms, which may in turn reduce the willingness of ethnic minorities and families in poverty to access the health care system (NASEM, 2016a). Medical providers require the knowledge and tools to provide appropriate care to diverse populations in order to address the aforementioned health care disparities. Chapter 5 provides a more in-depth look into opportunities to enhance systems along the continuum of preconception, prenatal, and pediatric health care.
HEALTHY LIVING CONDITIONS
In the report’s conceptual model, the committee identifies healthy living conditions as an important domain for study and intervention (see Figure 3-5 for a visual of how this section ties to the conceptual model). For the purposes of this report, healthy living conditions are the social, economic, cultural, and environmental factors that shape the odds for optimal child health and development. Specifically, these include economic security, nutrition and food security, neighborhood conditions, housing, and environmental exposures. These living conditions interact with multiple levels of the conceptual model. For example, adequate nutrition and food security encompass individual behaviors, such as breastfeeding, but they can also be shaped by the larger policy context, such as government programs (e.g., the Supplemental Nutrition Assistance Program [SNAP] and the Special Supplemental Nutrition Program for Women, Infants, and Children [WIC]). The following sections delve into the evidence on how healthy living conditions are critical for early development. Chapter 6 follows this thread and discusses the evidence for interventions (i.e., programs, policies, and systems) that show the most promise for promoting equitable healthy living conditions for all children.
ECONOMIC SECURITY
Household Socioeconomic Status
Household SES, a construct often measured using income, occupation, and education, is an important social determinant of child health and well-being. For children, SES not only reflects household income but is
NOTES: The element of focus in this section is reflected in the second outermost ring in the model: healthy living conditions (i.e., economic security, nutrition and food security, housing, and environmental safety). This element is bolded for emphasis.
also indicative of their neighborhood and housing conditions, food security, parental well-being and educational attainment, exposure to violence and other stressors, quality of ECE, and more. This section specifically explores how household SES as it relates to income, poverty, wealth, class, and education affects early developmental outcomes.
Poverty can be defined broadly as the lack of financial resources or material possessions to meet basic needs, such as shelter, food, and clothing. Poverty, income, and wealth are considered to be determinants of health, and there is a robust literature base that ties income and wealth to key health indicators, such as life expectancy, risk of chronic disease, and health-promoting behaviors (e.g., physical activity, healthy eating) (Chetty et al., 2016; NASEM, 2017a; Woolf et al., 2015). Poverty is a multidimensional construct that has many implications for the living conditions and environment that shape health and development.
For children, living in poverty is associated with negative health and developmental outcomes. The existing research suggests at least two pathways by which living in poverty can influence child outcomes (Evans, 2004). The first is through access to material resources and services (e.g., safe housing, nutrition, exercise, health care) (Braveman et al., 2018;
Johnson et al., 2016; Woolf et al., 2015). The second is through psychosocial stress (e.g., parental job strain, exposure to violence, housing instability, food insecurity) (Braveman et al., 2018; Johnson et al., 2016; Lefmann and Combs-Orme, 2014). The convergence of these factors shapes early living conditions, which can lead to cumulative risk exposure for those living in poverty. Therefore, income and poverty can be conceptualized as upstream determinants of many of the social, economic, and environmental factors discussed in this chapter.
Trends and Disparities
While children under the age of 18 represent 23 percent of the nation’s population, they make up 32 percent of people living in poverty (Koball and Jiang, 2018a). In 2016, 44 percent of young children (i.e., under the age of 9) lived in low-income households (i.e., below 200 percent of the federal poverty threshold). In addition, approximately one in five young children lived in poor households (i.e., below 100 percent of the federal poverty threshold) (Koball and Jiang, 2018b). It is important to note that child poverty, and poverty in general, can be measured in a variety of ways, which has implications for how trends are measured. For example, consumption-based measures of poverty—as opposed to those based on income alone—reflect permanent income and government benefits, and some argue that these are more likely to capture the effects of saving, ownership of goods (e.g., property), and access to credit (Meyer and Sullivan, 2009).
Socioeconomic disparities exist across race, ethnicity, age group, and geographic region. For example, black, AI/AN, and Hispanic children disproportionately live in low-income and poor households; they are also most likely to live in deep poverty (below 50 percent of the federal poverty threshold). In terms of upward economic mobility, there are differences among racial groups as well. In particular, research suggests that black and AI/AN children have the lowest rates of upward mobility, even when controlling for parental income (Chetty et al., 2018). When looking across age groups, younger children (up to 11 years old) are more likely to live in low-income or poor households. However, when stratified by racial or ethnic group, there are stark differences in the proportions (see Table 3-2).
Effects of Income and Poverty
Pregnancy and birth outcomes Blumenshine et al. (2010) conducted a systematic review examining the association between socioeconomic disadvantage and adverse birth outcomes (e.g., outcomes related to birth weight, gestational age, or growth restriction). The authors determined that 91 studies found significant associations between at least one measure of socioeconomic disadvantage and one adverse birth outcome.
TABLE 3-2 Percentage of Children (ages 0–11 years) Living in High Poverty Areas from 2013 to 2017, by Race and Ethnicity
| Race or Ethnicity | Percentage of Children (0–11 years) Living in Low-Income or Poor Households |
|---|---|
| American Indian/Alaska Native | 28% |
| Asian and Pacific Islander | 6% |
| Black or African American | 28% |
| Hispanic or Latino | 19% |
| Multiracial | 10% |
| Non-Hispanic White | 4% |
NOTES: High poverty areas are defined as census tracts with poverty rates of 30 percent or more. These data are sourced from the Population Reference Bureau analysis of data from the 2013–2017 American Community Survey 5-year data.
SOURCE: Kids Count Data Center, 2019.
While differences in birth outcomes based on individual-level socioeconomic factors were almost always observed among non-Hispanic white women, the results were less consistent for African American and Hispanic women. For example, no studies included in this review found birth outcomes to be associated with individual-level socioeconomic factors among foreign-born Hispanic women. However, other studies show associations between neighborhood-level poverty and pregnancy and birth outcomes across racial and ethnic groups. The authors postulate that the cumulative effects of neighborhood conditions (e.g., poor housing, crime, pollution, stress), which are more common for communities of color, may have stronger health impacts than those associated with individual-level income or educational attainment, pointing to the need for community-level interventions (see the section Concentrated Disadvantage for more discussion of these studies at the neighborhood level).
Childhood outcomes Living in poverty during early childhood can have long-lasting implications for health and well-being. Family income has been found to be associated with risk of child maltreatment, where families with limited economic resources are at a higher risk (Berger et al., 2017; Cancian, 2010). Other research points to allostatic load as an important proximal outcome of living in an environment in the context of poverty. Blair et al. (2011) found that two aspects of the poverty environment were related to salivary cortisol (a measure of the stress response) in infancy: adult exits from the home and perceived economic insufficiency. In terms of neurodevelopmental and cognitive outcomes, the existing literature suggests that poverty affects the developing brain. This includes the structure and function of areas that regulate memory, emotion,
cognitive functioning, and language and literacy (Johnson et al., 2016). There is also research that demonstrates the impact of family income on academic achievement, whereby a $1,000 increase in annual income could increase achievement by 5–6 percent of a standard deviation (Duncan et al., 2011; Wolf et al., 2017). Box 3-6 enumerates a few conclusions on the consequences of poverty from the 2019 National Academies report A Roadmap to Reducing Child Poverty.
Implications of the Wealth Gap
Income is often the target of many policies and interventions and is important for short-term outcomes, but a focus on the more encompassing construct of wealth is important for a health equity agenda because it has long-term and intergenerational implications. That is, income is necessary for building wealth, and wealth could buffer families from periods of income instability and low income.
Wealth, or economic assets accumulated over time, is calculated by subtracting outstanding debts and liabilities from the cash value of currently owned assets—such as houses, land, cars, savings accounts, pension plans, stocks and other financial investments, and businesses. Wealth measured at a single time period may provide a more complete picture than income of a person’s economic resources. (NASEM, 2017a, p. 127)
U.S. Census data show that the median household wealth in 2013 was $1,700 for black families, $2,000 for Latinos, and an astonishing $116,800 for whites. The median household wealth in 1983 was $6,800 for black families, $4,000 for Latinos, and $102,200 for whites (Asante-Muhammad et al., 2017). Using data from the Panel Study of Income Dynamics, Williams (2004) found that level of income was not as good of an indicator for black children’s outcomes as it was for white children. Rather, having assets such as stocks or an IRA mattered more for black than for white children. Though focused on older individuals, Zhan and Sherraden (2010) found that household income was more associated with white children’s college attendance and graduation, whereas wealth seemed to be more salient for black and Latino college students. This is also consistent with findings from Williams Shanks (2007) that family income is associated with white children’s test scores but not those of black children. Kaushal and Nepomnyaschy (2009) find that although wealth, along with family sociodemographics and parental resources, accounts for the disparities in the black-white and Hispanic-white gap in children’s participation in gifted programs, extracurricular activities, and grade retention, black children continued to face high risk of expulsion or suspension from school relative to white children regardless of wealth status. Furthermore, intergenerational transmission of wealth may not be as common, especially for black families (Chetty et al., 2018). While Latino families are moving up in their incomes across generation, black families have substantially lower rates of upward mobility and higher rates of downward mobility (Chetty et al., 2018). That is, black children from higher-income households are likely to become poor as adults compared to their white peers. This indicates that the pathway to wealth accumulation and maintenance differs across racial groups, which has implications for policies that are developed and implemented, especially if they do not address the continued loss of wealth for minority families and communities.
Parental Educational Attainment
Evidence shows that higher levels of caregiver/parental educational attainment are associated with positive child educational outcomes (e.g., school readiness, educational achievement), physical health outcomes (e.g., rates of LBW), and health behaviors (e.g., rates of smoking and binge drinking) (Child Trends, 2015). Research indicates that caregiver/parental educational attainment may also serve as a protective factor for outcomes in childhood, adolescence, and adulthood (Dubow et al., 2009).
Higher levels of maternal educational attainment, in particular, have been linked with improved health and well-being for children (Cutler and Lleras-Muney, 2006). Conversely, low levels of maternal educational attainment have been found to be significantly associated with negative
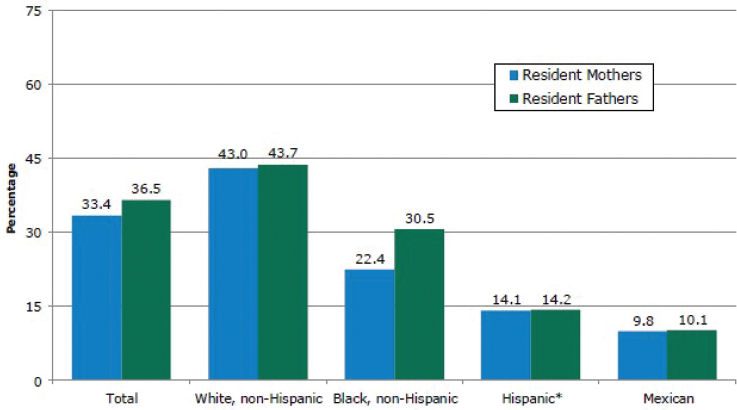
NOTES: * Hispanic includes Mexican. Data are sourced from Child Trends analysis of Current Population Survey, March Supplement.
SOURCE: Child Trends, 2015.
infant and child outcomes. Infants whose mothers have not completed high school have been found to have twice the risk of dying before their first birthday compared to those of mothers who have completed college (Egerter et al., 2011b; Mathews and MacDorman, 2007).
Since 1974, the percentage of parents (with children ages 6–18) with less than a high school diploma has decreased, while the percent of those with a bachelor’s degree or higher has increased (Child Trends, 2015). However, disparities by race and ethnicity have persisted, particularly for African American and Hispanic mothers and fathers (see Figure 3-6).
Education is often touted as the gateway to prosperity or ensuring stability for families and children. However, accumulating evidence shows that there are racial differences in the impact of college attainment on income and wealth. Asante-Muhammad and colleagues of Prosperity Now show that
[w]hite families whose head of household holds a high school diploma have nearly enough wealth ($64,200) to be considered middle class [see Figure 3-7]. A typical black or Latino family whose head of household has a college degree, however, owns just $37,600 and $32,600, respectively, in wealth. In fact, only black and Latino households at the median with an advanced degree have enough wealth to fit into [their] middle-class definition. By contrast, all white households except those who fail to attain a high school diploma could be considered middle class. (Asante-Muhammad et al., 2017, p. 10)
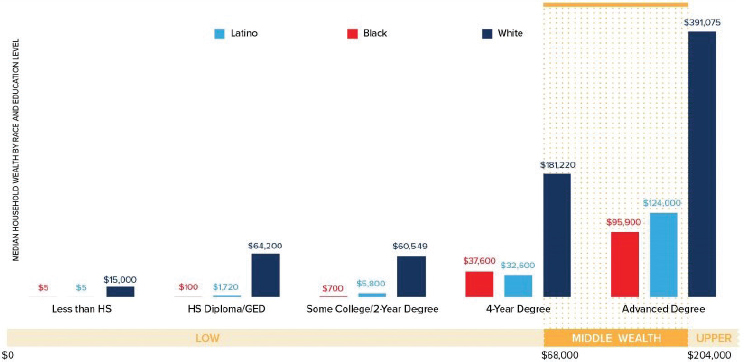
NOTES: Wealth figures depicted above exclude durable goods. Data are sourced from the U.S. Census Bureau Survey of Income and Program Participation, 2014.
SOURCE: Asante-Muhammad et al., 2017.
Black and Latino families with college degrees have less than half of the wealth of white families with a high school diploma. This differential impact of higher education is also seen with unemployment rates: black individuals with college degrees have a 19, 65, 31, and 31 percent greater chance of unemployment than Latinos, Hispanics, whites, and Asian Americans, respectively (Andolfatto, 2017). This is particularly concerning when many blacks and Latinos are less likely to have higher education degrees compared to their white peers. Thus, while educational attainment is associated with better child outcomes, more research is needed to better uncover how racial disparities in education coupled with availability of wealth may be associated with the racial disparities in health and education.
NUTRITION AND FOOD SECURITY
Although access to adequate and nutritious foods affects development across the life course, it is particularly important for the preconception, prenatal, and early childhood periods. Furthermore, the period from conception to 2 years of age (about the first 1,000 days) is especially critical, as the brain undergoes significant developmental changes during this period that may not be possible later in life (Schwarzenberg and Georgieff, 2018). In addition to macronutrients (protein, fat, and glucose), certain micronutrients (zinc, copper, iodine, iron, and selenium) and vitamins
and cofactors (vitamin B6, vitamin B12, vitamin A, vitamin K, folate, and choline) are particularly important for healthy early brain development (American Pregnancy Association, 2017; Cusick and Georgieff, 2016; Georgieff et al., 2015; IOM, 1990; March of Dimes, 2018; Schwarzenberg and Georgieff, 2018). Malnutrition can take the form of undernutrition (inadequate intake of macro- and/or micronutrients) and/or overweight/obesity (excessive intake of calories but not necessarily adequate intake of macro- and micronutrients). Inadequate intake of macro- and micronutrients during critical or sensitive periods of development can result in negative developmental effects across the life course, with long-term effects being more likely the earlier such nutrient deficiencies occur (Georgieff et al., 2015; Schwarzenberg and Georgieff, 2018).
Access to healthy and nutritious foods for pregnant mothers is important to ensure healthy birth and developmental outcomes for their infants (Borge et al., 2017; Ramakrishnan et al., 2012; Thorne-Lyman and Fawzi, 2012; Veena et al., 2016; Yakoob and Lo, 2017; Zerfu and Ayele, 2013). In an overview of systematic reviews of international interventions to improve nutrition during pregnancy, infants of pregnant women who were provided oral supplements of vitamin A, low-dose calcium, zinc, and multiple micronutrients as well as nutrition education and preventive antimalarials were found to have a lower risk of LBW (da Silva Lopes et al., 2017).
Maternal nutrition during pregnancy can also affect overweight and obesity in children (Lau, 2014; Leonard et al., 2017). Tabacchi et al. (2007) describe that “the prenatal interactions between genetics and environment play an important role in determining the postnatal phenotype related to obesity” (see Chapter 2 for more detailed information on fetal programming and the interplay of genetics and environment). Evidence also suggests a correlation between maternal obesity and poor infant and birth outcomes (e.g., higher risk of preterm birth, being large for gestational age, fetal defects, perinatal death) (Aviram et al., 2011; Marchi et al., 2015), poor health outcomes in infancy and early childhood, including childhood obesity (Beckhaus et al., 2015; Mameli et al., 2016; Marques et al., 2013; Monasta et al., 2010; Nyaradi et al., 2013; Van Lieshout et al., 2011; Woo Baidal et al., 2016), and negative implications for disease and other poor health outcomes in adulthood (Langley-Evans, 2015; Poston et al., 2011).
Despite clear evidence linking maternal and infant nutrition with positive health and development outcomes, many communities, particularly low-income communities and communities of color, do not have access to affordable, high-quality, nutritious food (Harrington et al., 2009). The lack of access in these communities is compounded by greater exposure to unhealthy foods and beverages, including targeted
advertising for such products (NASEM, 2017b). To achieve health equity for all children, it is critically important for all families to have access to healthy and nutritious foods. (For a discussion of the policies and programs in the United States that aim to decrease food insecurity and improve nutrition and healthy eating in the prenatal and early childhood periods, e.g., Temporary Assistance for Needy Families, SNAP, and WIC, see Chapter 6.) See Box 3-7 for statistics on food insecurity during childhood.
Breastfeeding
Exclusive breastfeeding4 offers complete nutrition for infants during the first 6 months of life. Because of this, the World Health Organization (WHO) and the American Academy of Pediatrics (AAP) recommend that infants receive only breast milk during this time to achieve optimal growth, development, and health. After that, WHO and AAP recommend continued breastfeeding combined with complementary foods up until at least 1 year of age.
___________________
4 Exclusive breastfeeding is defined by WHO as not giving the infant any other food or drink, including water, except needed vitamins and medications (WHO, n.d.-b). WHO recommends that infants start receiving complementary foods at 6 months of age, in addition to breast milk (WHO, n.d.-a).
Breastfeeding provides important health benefits for mothers and children, but it is important to note methodological difficulties in studying the health impact of breastfeeding. RCTs comparing breastfeeding to formula would be unethical, and observational study designs limit causal inferences. However, this is an area that has been studied for many decades, and there are several areas where the science has converged on the understanding of how breastfeeding promotes healthy outcomes for children and breastfeeding mothers.
There is evidence that exclusively breastfed infants have lower rates of infant mortality, otitis media, and gastrointestinal infections (Bowatte et al., 2015; Kramer and Kakuma, 2012; Sankar et al., 2015). The impact of breastfeeding on the child’s health seems to endure, because breastfeeding (and longer breastfeeding duration) is protective against overweight and obesity in children, although reviews and meta-analyses describe such correlations as small (but consistent) and difficult to prove, with research needed to further elucidate the relationship (Arenz et al., 2004; Beyerlein and von Kries, 2011; Dewey, 2003; Harder et al., 2005; Horta et al., 2015; Lodge et al., 2015; Ryan, 2007; Wang et al., 2017). A growing body of research demonstrates important psychological effects of breastfeeding on children, including an impact on brain, cognitive, and socio-emotional development (Krol and Grossmann, 2018).
Breastfeeding may also be protective for mothers, with lower rates of breast and ovarian carcinoma, type 2 diabetes, and postpartum depression (Chowdhury et al., 2015; Dias and Figueiredo, 2015; Hahn-Holbrook et al., 2013; Ip et al., 2007). However, a study by Borra et al. (2015) showed that there is an increased risk of postpartum depression when women who had planned to breastfeed had not gone on to breastfeed, and it concluded that breastfeeding intentions during pregnancy and mothers’ mental health during pregnancy both mediated the effect of breastfeeding on maternal depression. This aspect points to the need to provide not only “expert breastfeeding support to women who want to breastfeed but also . . . compassionate support for women who had intended to breastfeed, but who find themselves unable to.”
Breastfeeding Disparities
In the United States, breastfeeding rates as a whole have been increasing (CDC, 2018a). According to the Centers for Disease Control and Prevention (CDC), of infants born in 2015 in the United States, 83.2 percent started to breastfeed, more than half (57.6 percent) were breastfeeding at 6 months, and 35.9 percent were breastfeeding at 12 months. However, there are disparities in breastfeeding rates along a number of demographics.
Breastfeeding rates are lowest among African American mothers and mothers living in rural areas. From 2011 to 2015, the percentage of women
who initiated breastfeeding was 64.3 percent for African Americans, 81.5 percent for whites, and 81.9 percent for Hispanics (Anstey et al., 2017). Rates of breastfeeding are also lower in mothers who are young, have lower educational attainment, and have lower incomes (ASTHO, 2017). Roughly 80 percent of higher-income women were still breastfeeding at 1 year compared to 20 percent of lower-income women (ASTHO, 2017).
A multitude of factors impact a woman’s decision to start and continue breastfeeding. Social factors, such as unsupportive cultural and social norms, concerns about milk supply, poor family and social support, and unsupportive work and child care arrangements, can make it difficult for many mothers to meet their breastfeeding goals (HHS, 2011). Black women disproportionally experience some of these barriers, such as returning to work soon after a child is born, lack of breastfeeding information from providers, and lack of access to professional breastfeeding support (Johnson et al., 2015). Black mothers also might not have consistent access to evidence-based supportive practices. A study by Chapman and Pérez-Escamilla (2012) on hospital support for breastfeeding indicated that facilities in areas with higher proportions of black residents were less likely to fulfill supportive breastfeeding practices than those located in areas with lower percentages of black residents. Health care provider practices may also account for reduced rates of breastfeeding among black mothers, particularly with respect to breastfeeding encouragement and information (Jones et al., 2015). For mothers in rural communities, factors such as poverty and inadequate access to needed maternity and health services may serve as obstacles to breastfeeding (CDC, n.d.-b). Supportive programs and policies for mothers who plan to breastfeed are needed; see Chapter 6 for a discussion of some of these interventions (e.g., paid parental leave) (Pac et al., 2019).
NEIGHBORHOOD AND COMMUNITY CONDITIONS
A community is the place where a child lives, learns, and plays. By this notion, communities serve as the bedrock of health where experiences and behaviors are shaped by the conditions in which a child lives (NASEM, 2017a). The conditions that make up a community or neighborhood are critical for supporting healthy behaviors and providing safe environments for children. This section of the chapter explores the community conditions that can either promote or hinder optimal development during the prenatal through early childhood periods. These include factors that are deeply rooted in historical policies and structural inequities (as was introduced in the beginning of the chapter) and protective factors that can prevent or mitigate the manifestation of negative developmental outcomes among children. The following sections discuss disparities
and scientific evidence related to developmental outcomes, including mechanisms across a number of neighborhood-level factors: concentrated disadvantage, physical environment, social environment, and exposure to violence. These factors are all interrelated, and despite the serious effects that some can have on early development, it is important to note that they are not immutable circumstances or effects (NASEM, 2017a).
Concentrated Disadvantage
Trends and Disparities
Beyond poverty at the household level, which was discussed in the previous section, nationally, 12 percent of children live in neighborhoods with concentrated poverty (i.e., Census tracts with poverty rates of 30 percent or more) (Kids Count Data Center, 2019). Concentrated disadvantage and neighborhood-level deprivation are important factors to examine because of the cumulative risk that is associated with these neighborhood conditions. Data from the Early Childhood Longitudinal Study indicate that the proportion of kindergarten children living in moderate and high-poverty neighborhoods increased from 1998 to 2010, which has important implications for school readiness (Wolf et al., 2017).
Neighborhood Disadvantage and Prenatal Through Childhood Outcomes
Individual-, household-, and neighborhood-level economic deprivation shows a graded relationship to health outcomes (Pickett and Pearl, 2001). The Whitehall (Kumari et al., 2004) and GLOBE (Global Leadership and Organizational Behaviour Effectiveness) studies (van Lenthe et al., 2004) both offer strong evidence that individual and neighborhood-level economic conditions each contribute to health outcomes. Twin studies offer other compelling evidence; one such study of 3,738 same-sex twin pairs found that neighborhood deprivation had a significant within-pair association with depression after adjusting for individual socioeconomic indicators and other factors (Cohen-Cline et al., 2018). There is a strong body of associational evidence linking neighborhood economic environments to depression (Paczkowski and Galea, 2010) and other chronic diseases (Pickett and Pearl, 2001). Box 3-8 describes asthma disparities as an example of a health outcome in the context of neighborhood disadvantage.
Neighborhood-level economic deprivation has also been widely associated with pregnancy and birth outcomes, including reduced use of prenatal care (Schempf et al., 2009) and an increased risk of a range of adverse birth outcomes (Messer et al., 2006; O’Campo et al., 2008; Zeka et al., 2008). Studies have linked neighborhood-level economic deprivation
indicators with birth weight (Buka et al., 2003; Morenoff, 2003; Pearl et al., 2001; Rich-Edwards et al., 2003; Subramanian et al., 2006), preterm birth (Ahern et al., 2003; Kaufman et al., 2003; O’Campo et al., 2008), and gestational age and fetal growth (Farley et al., 2006). However, this is not to suggest that neighborhood economic deprivation is the cause of poor health—Jokela’s (2014, 2015) analyses of data from the British Household Panel Survey suggest that the observed associations may in fact reflect more fundamental social inequalities that shape health and hinder some people’s ability to move to less deprived neighborhoods. Research has consistently shown an association between neighborhood deprivation and health, but a firm causal connection has not been established.
While there is evidence connecting neighborhood-level poverty and birth outcomes, the mechanism of this link remains unclear; one theory is allostatic load due to stress (Lefmann and Combs-Orme, 2014; Wallace et al., 2013). Wallace and colleagues (2013) found that while African American mothers who resided in poor neighborhoods had higher allostatic load than white mothers, allostatic load was not associated with preterm birth or LBW after accounting for race, neighborhood SES, maternal education, maternal age at time of birth, and smoking during pregnancy, among other things. This lack of link between allostatic load
and pregnancy was also found in another study (Morrison et al., 2013). Nevertheless, African American women living in low-poverty neighborhoods were more than five times as likely to have an LBW infant and to have given birth preterm than white women in low-poverty neighborhoods. This racial disparity link between neighborhood disadvantage and LBW and preterm birth was also found in a systematic review and meta-analysis of population-based studies (Ncube et al., 2016). Margerison-Zilko and colleagues (2015) stress that it is not just about living in a poor neighborhood that is related to preterm birth but the length of time spent in a low-resourced, high-poverty neighborhood. In their systemic review and meta-analysis examining the link between residential segregation and adverse birth outcomes, Mehra et al. (2017) found that black mothers living in segregated neighborhoods have the highest risk of LBW and multiple adverse birth outcomes.
Physical Environment
A number of studies have assessed how various physical characteristics of neighborhoods—the “built environment”—may shape health or birth outcomes, either through direct exposure or by limiting access to or the effectiveness of traditional health care strategies. Green infrastructure, such as vegetation or tree canopy, has been associated with reduced depression rates (Cohen-Cline et al., 2018; Fan et al., 2011), which may in turn impact birth outcomes (Accortt et al., 2015). The presence of active living attributes, such as walkability, mixed land use, and active transit options, has been associated with increased physical activity and reduced obesity in general (Feng et al., 2010; Saelens et al., 2003a,b). However, the evidence is unclear on whether this ultimately affects birth outcomes: the one study assessing built environments in terms of adverse birth outcomes did not yield clear evidence of impact (Vinikoor-Imler et al., 2011). It is possible that the condition of early built environments could be associated with “sleeper effects,” whereby outcomes are observed later in life.
The importance of food security and nutrition has long been identified as a key determinant of prenatal and postnatal health outcomes. However, the food environment people live in—the accessibility of healthy food options in their neighborhoods—is an additional contextual factor that may shape their prenatal outcomes by facilitating or limiting their ability to follow prenatal nutritional advice. A few studies have found positive effects of healthy food environments on reducing obesity (Auchincloss et al., 2013), hypertension (Kaiser et al., 2016), and type 2 diabetes (Christine et al., 2015). However, a number of other studies of the food environment’s impact on health outcomes have reported null results,
leading to an overall mixed body of evidence (Cobb et al., 2015), and few such studies have moved beyond overall health outcomes to assess specific adverse birth outcomes. Two studies have found associational evidence that women living in neighborhoods with a high concentration of convenience stores versus healthier food sources (Ma et al., 2016) or in areas lacking proximity to supermarkets (Lane et al., 2008) had increased risk of some adverse birth outcomes. However, other studies have not found evidence that neighborhood food environments significantly impacted birth outcomes (Farley et al., 2006). Overall, the evidence in this area remains preliminary and somewhat mixed.
Social Neighborhood Environment
The social environment people live in can be as important as their physical environment. Social support has been hypothesized to benefit birth outcomes both by moderating or buffering the stress of pregnancy (or of other contextual challenges to a healthy pregnancy) and by exerting a direct positive influence on the health of a prospective mother (Cohen and Wills, 1985). Social isolation has been associated with whether women receive adequate prenatal care (Heaman et al., 2018) and with late antenatal presentation (i.e., delayed access to antenatal care) and poor fetal outcomes (Kapaya et al., 2015), while better social support has been associated with higher birth weight and Apgar scores at birth (Collins et al., 1993), reduced risk of maternal depression (Uebelacker et al., 2013), and improved fetal growth (Hoffman and Hatch, 1996). However, studies of interventions aimed at improving social support for pregnant women have not been uniformly shown to be effective (Lu et al., 2005), and the mechanisms by which social support may impact birth outcomes remains somewhat unclear.
Social support can refer to personal networks but also to neighborhood environmental context. These “neighborhood cohesion” measures have been associated with physical and mental health and well-being outcomes in some studies (Bures, 2003; Fone et al., 2007; Hutchinson et al., 2009), perhaps acting to help protect individuals from the harmful or stressful effects of neighborhood deprivation (Robinette et al., 2013). They have also been specifically associated with improved birth weight outcomes in several studies (Buka et al., 2003; Morenoff, 2003).
Exposure to Violence
Childhood exposure to violence can take on many forms, including primary exposure or direct victimization (e.g., maltreatment or abuse by an adult caregiver or bullying by peers) and secondary exposure
(e.g., witnessing IPV between parents or community violence) (Gilbert et al., 2009). Regardless of the mechanism, the body of evidence on early exposure to violence shows that this is harmful to children’s health and well-being (Egerter et al., 2011a; Moffitt and Tank, 2013; Shonkoff et al., 2012). Data also show that specific subgroups are at higher risk of being exposed to violence based on certain demographics, such as race and ethnicity, gender, SES, and parental education level. Research also indicates that children who are exposed to one incident of violent victimization are likely to be exposed to violence again, including other forms (Finkelhor et al., 2007, 2009, 2015).
Trends and Disparities
Data from the National Survey of Children’s Exposure to Violence (2013–2014) including a nationally representative sample of children (n = 4,000; 0–17 years old) showed that 37.3 percent had experienced any physical assault in the past year, 51.4 percent had experienced physical assault in their lifetime, and 24.5 and 38.3 percent witnessed violence in the past year and in their lifetime, respectively (Finkelhor et al., 2015). For women, disparities in violence have been documented. For example, for 2003–2014, non-Hispanic black and AI/AN women experienced the highest homicide rates nationally, at 4.4 and 4.3 per 100,000, respectively (Petrosky et al., 2017). Furthermore, more than half of all female homicides (55.3 percent) were related to IPV, which is considered an ACE for children who are exposed to it. (See the section at the end of this chapter on Accumulation of Risk for more on ACEs.)
Neighborhood Violence and Child Well-Being
Research has linked neighborhood violence with negative health and well-being outcomes across the continuum of early development. For example, there is evidence to suggest that high rates of youth violence (e.g., assault, kidnapping, homicide, robbery, larceny, destruction of property) measured at the Census tract level are associated with elevated odds of preterm birth (Masho et al., 2017). The presence of community violence has also been shown to have a direct negative relationship with children’s self-regulatory behavior and cognitive performance indicators (Sharkey, 2010; Sharkey et al., 2012). A systematic review of studies examined exposure to community violence and health outcomes in youth (0–18 years old) (Wright et al., 2017). Across the 28 studies included, the most consistent finding was that early exposure to community violence was associated with elevated blood pressure, asthma, and sleep disturbance, which the authors note can contribute to other health-related
problems when it persists over an extended period. Among the studies in this review, one found that the level of collective efficacy5 in a community moderated the effect of exposure to community violence on increased asthma risk, particularly among African Americans (Sternthal et al., 2010). In addition, social support has been identified as a critical buffer for children against the negative effects of violence (Margolin and Gordis, 2004).
More recent studies have begun to examine the underlying pathways through which violence specifically influences health outcomes (Finegood et al., 2017; Theall et al., 2017). For example, a 2012–2013 study of African American children in New Orleans found that reports of domestic violence and rates of violent crime within a 500-meter radius of a child’s home were associated with decreases in mean telomere length and the likelihood of reducing cortisol levels after a stress reactivity test (Theall et al., 2017). Some research suggests that underlying disadvantage (e.g., poverty, high unemployment, lower levels of educational attainment) associated with neighborhood violence partially explains the relationship between exposure to violence and negative cognitive and behavioral outcomes (Aizer, 2008). Egerter et al. (2011a) postulate that social and economic disadvantage increases the likelihood of exposure to violence, which can diminish levels of trust, social cohesion, and perceptions of safety in a community.
Limitations of the Evidence on Neighborhood Effects
Despite these associations, the relationship between neighborhood characteristics and health outcomes is complex, making causal connections difficult to establish in this literature. Associations may vary based on individual-level characteristics, such as age or sex (Meijer et al., 2013), and may be quite sensitive to the inclusion of other covariates in the models (Auchincloss et al., 2013; Blair et al., 2014; Paczkowski and Galea, 2010). As stated previously, it is also difficult to separate out the effects of factors that tend to cluster together (i.e., concentrated disadvantage) or are systematically present for specific populations, such as poor housing quality, poverty, and exposure to environmental toxicants. Results also vary widely depending on how a specific health domain is measured or how a neighborhood is defined (Paczkowski and Galea, 2010), and many studies capture only limited domains of neighborhood characteristics, leaving unanswered the question of which characteristics are most
___________________
5 Collective efficacy can be defined as the level of trust among residents and their perceived willingness to engage in collective action (Sternthal et al., 2010).
important or how those characteristics interplay with one another to shape outcomes. Last, few studies establish a causal connection between these endogenous neighborhood characteristics and health (Dohrenwend et al., 1992; Jokela, 2014; Ritsher et al., 2001).
HOUSING
Housing affordability, stability, and quality are well studied and documented SDOH across the life-span. This is also true, of course, during the prenatal and early childhood years. Quality, stability, affordability, and loss of housing in the prenatal and childhood periods can have significant effects on health, cognition, and neurodevelopment. As described previously, residential segregation has had persistent effects on communities, including limiting the availability of safe and affordable housing for some. In this section, housing instability, quality of housing, and affordability will be addressed in turn.
Housing Instability
According to a 2017 report from the U.S. Department of Housing and Urban Development, there were more than 550,000 individuals considered to be homeless on any given night in the United States in that year. More than 1.4 million people were homeless in sheltered locations (e.g., emergency shelter, transitional housing, safe haven) at some point in 2017 (Henry et al., 2017). Moreover, the risk of homelessness is high for many individuals: according to recent studies, nearly 3 million individuals renting are at risk of eviction, which indicates high rates of potential instability (Sandel and Desmond, 2017). The data indicate a vast imbalance in equitable access to stable housing, such that those experiencing homelessness are disproportionately likely to be black. Only 13 percent of the general population is black, compared to more than 40 percent of the homeless population (Olivet et al., 2018).
While housing instability and homelessness are notoriously difficult to measure accurately, families with children are estimated to make up 33 percent of homeless populations (Henry et al., 2017). A 2008 cross-sectional study of 12,746 children from low-income families suggests that nearly 30 percent of children from these households are in households with housing instability (Ma et al., 2008). This includes frequent moves, difficulty paying bills or rent, spending a large proportion of income on rent, being evicted, or living in overcrowded conditions.
Housing instability—either chronic or intermittent homelessness—has well-documented negative health effects on developing children. A 2014 study of nearly 10,000 women found that mothers who were
homeless while pregnant were more likely to deliver LBW children compared to those who were homeless after delivery (Cutts et al., 2015). Following birth, housing instability is associated with a wide range of cognitive, emotional, and behavioral outcomes. In a nationally representative, longitudinal study of children 2–21 years old, Coley and colleagues (2013) found that residential instability was associated with negative internalizing and externalizing behaviors—particularly for children with multiple housing moves. It was hypothesized that the negative effects of housing instability are due to changes in social structures, schooling, and the emotional health of the family (Coley et al., 2013). In a 2008 study, housing instability was associated with delays in seeking medical care or medications and increased emergency department (ED) visits among children from low-income families (Ma et al., 2008).
More broadly, it has been shown that homeless children—or children with frequent moves—are at increased risk for conduct problems at school, social difficulties, and low academic achievement (Buckner, 2008; Miller, 2011; NRC and IOM, 2010). These effects appear to be independent of low-income status; data on academic achievement and improvement on standardized tests suggest that students with frequent moves perform consistently worse in reading and math compared to other low-income students without frequent moves or housing instability (Masten et al., 2014; Obradović et al., 2009). Overall, the picture of housing instability is one of pervasive and sometimes long-term outcomes on children’s health and well-being.
Housing Affordability
Housing is widely considered “affordable” if less than 30 percent of pretax income is required to own or rent (Schwartz and Wilson, n.d.; The Pew Charitable Trusts, 2018). By this definition, approximately 31.8 million U.S. households are living in housing that is unaffordable (Joint Center for Housing Studies of Harvard University, 2018). This population is generally low income. In 2015, 84 percent of renters in the lowest quintile of income were living in unaffordable housing; 70 percent of this group spent more than 50 percent of their income on housing costs (Fenelon et al., 2018). In 2016, 47 percent of all renters, and more than three-quarters of families earning between $15,000 and $30,000, had unaffordable housing (Joint Center for Housing Studies of Harvard University, 2017).
According to the most recent data available, racial/ethnic minorities and single-parent families disproportionately experience high housing cost burden, with 55 and 54 percent of black and Hispanic renters in
unaffordable housing, respectively, compared to 43 percent of white renters. Furthermore, 63 percent of single-parent renters are in unaffordable homes, compared to 39 percent for married or partnered parents, and finding affordable housing in large metropolitan areas is particularly challenging (Joint Center for Housing Studies of Harvard University, 2017). Across the United States, there are only 37 available and affordable rentals for every 100 low-income households that require housing (National Low Income Housing Coalition, 2018).
There is mixed evidence for housing affordability on health and well-being outcomes among children. A 2010 critical review of housing characteristics and child development found that affordability was not well studied and was only marginally associated with children’s health (Leventhal and Newman, 2010). These findings suggest that affordability, per se, is not the primary concern; rather, the amount invested in a child’s health and enrichment may be a more robust predictor of developmental trajectories (Newman and Holupka, 2016). This includes spending in other domains that are important for optimal child development (Newman and Holupka, 2016), such as quality child care (Campbell et al., 2014), schools, and neighborhoods (Beyers et al., 2003; Knopf et al., 2016; Theall et al., 2017; Xue et al., 2005). Research suggests that a high housing cost burden is associated with lower spending on child enrichment (Newman and Holupka, 2016) and elevated maternal stress (Warren and Font, 2015), but its impact on maternal depression or anxiety is unclear (Harkness and Newman, 2005; Newman and Holupka, 2014). Families in unaffordable housing are more likely to miss rent payments (Warren, 2018) and therefore may be forced to move (Crowley, 2003; Desmond and Shollenberger, 2015). At the same time, research also suggests that by allocating a higher fraction of household income to housing, families may gain access to higher-quality homes (Kull and Coley, 2014), neighborhoods (Acevedo-Garcia et al., 2016b), and/or schools, and these contextual advantages of high housing costs may outweigh any negatives (Kull and Coley, 2014).
While high housing costs can be problematic, very low housing costs for low-income families may also present risks for healthy child development because they can be indicative of substandard or poor-quality housing conditions (Newman and Holupka, 2014, 2016). Accordingly, for low-income families, high or low housing cost burden could be harmful (Newman, 2008). Although prior research suggests risk associated with high and low housing cost burden (Newman and Holupka, 2014, 2016), we focus our discussion on high housing cost burden because this is the main problem for low-income families.
Economic and developmental theories used in child research (Becker and Tomes, 1986; Garner and Shonkoff, 2012; Shonkoff et al., 2012) and
the scientific literature on the influence of poverty and child development (Brooks-Gunn and Duncan, 1997; Duncan, 2012; Duncan et al., 1994) suggest that understanding the role of housing affordability for child development requires considering (a) the multiple and interacting contexts in which children develop into adults (Bronfenbrenner, 1979; Bronfenbrenner and Evans, 2000; Bronfenbrenner and Morris, 2007), such as the home, school, and neighborhood; (b) the developmental timing and duration of unaffordable housing across childhood (Ben-Schlomo and Kuh, 2002; Ben-Schlomo et al., 2014; Brooks-Gunn and Duncan, 1997; Coley et al., 2013; Harkness and Newman, 2005; Hicks et al., 2018; Slopen et al., 2010); and (c) unequal health or educational benefits associated with a given level of parental income or education across racial/ethnic groups (Acevedo-Garcia et al., 2005; Assari, 2018; Assari et al., 2018; Chen et al., 2006; Shervin, 2018; Williams et al., 2010). For example, research suggests that youth are particularly influenced by socioeconomic variables during early childhood (Duncan et al., 1998; Ziol-Guest et al., 2009). Other research suggests that black and Hispanic children may be disproportionately harmed by unaffordable housing because investments in housing costs may have smaller returns for minority families (i.e., these investments may have diminished returns to school and neighborhood quality for minority children, relative to those for white children) (Assari, 2018; Shervin, 2018; Williams et al., 2010).
Housing Quality and Crowding
Families living in poverty are less likely to be able to afford high-quality housing, a factor clearly associated with child health (Rauh et al., 2008; Sandel et al., 2004). Although causal relationships are not always clear because most research is observational (Leventhal and Newman, 2010), many studies have explored the connection between child health and conditions in old and inadequately maintained residences, such as dampness, disrepair, poor ventilation, and lead paint. For instance, a study of low-income families waiting for housing vouchers found that poor-quality housing was associated with parents rating their child’s health as “fair” or “poor” (Sharfstein et al., 2001). Overall, poor housing quality is consistently associated with “worse emotional and behavioral functioning and lower cognitive skills” (Coley et al., 2013). In addition, another common feature of low-income housing is overcrowding, which has been demonstrated to negatively impact children’s well-being (Solari and Mare, 2012). The three subsections below focus on the relationship between child health and (1) exposure to allergens that cause asthma, (2) exposure to lead, and (3) overcrowding.
Allergens and Asthma
According to the National Health Interview Survey, more than 6 million (8.4 percent) of U.S. children under the age of 18 had asthma in 2017 (Black and Benson, 2018). While the management of childhood asthma improved from 2001 to 2016, its prevalence remained relatively consistent (Zahran et al., 2018). This warrants an increased focus on the root causes and triggers, and especially on the housing conditions of children who are disparately impacted.
Poor housing conditions can lead to increased risk of asthma. Several studies have found connections between asthma and exposure to allergens, such as cockroaches (Rauh et al., 2008; Wu and Takaro, 2007). Other research has found a causal association between dust mite exposure and asthma (IOM, 2000). Dampness and mold are also associated with asthma and other respiratory conditions (Rauh et al., 2008; Wu and Takaro, 2007). One study found that density in housing code violations was associated with a greater likelihood of a revisit to an ED or a hospital readmission (Beck et al., 2014). Another study found that children living in improved public housing were less likely to experience repeat ED and urgent care visits for conditions unrelated to an initial visit (Kersten et al., 2014). Some researchers have estimated that eliminating specific asthma triggers in older children could reduce asthma prevalence by more than 40 percent (Lanphear et al., 2001). Previous IOM studies have explored these connections in detail (IOM, 2000, 2004).
Exposure to Lead
While there is no known safe amount of lead exposure, in 2012, CDC established a reference level of 5 micrograms per deciliter to identify children who have been exposed (Wheeler and Brown, 2013). The percentage of children estimated to have blood lead levels (BLLs) greater than this amount has decreased significantly over the past decades, from an estimated 8.6 percent for 1999–2002 to 2.6 percent for 2007–2010 (Wheeler and Brown, 2013). These reductions are attributed to the phased elimination of lead from gasoline from the mid-1970s to the mid-1980s (President’s Task Force on Environmental Health Risks and Safety Risks to Children, 2018) and from paint in 1978 (Markowitz and Rosner, 2014). Lead paint was banned in 1978, but older homes, primarily in the Northeastern and Midwestern parts of the country, have a higher prevalence of lead paint (Rauh et al., 2008). When these homes are poorly maintained, this paint can chip or peel, and a child may ingest it or breathe in dust, resulting in elevated BLLs (Muller et al., 2018). In addition, lead remains in the soil in areas that were in close proximity to certain manufacturing sites (Muller et al., 2018).
Despite some improvements over time, current estimates suggest that more than 500,000 children ages 1–5 have BLLs over the reference level. Young black children are more than twice as likely (5.6 percent) than white children (2.4 percent) to have a BLL greater than 5 micrograms (Wheeler and Brown, 2013). Children who are living in poverty or who have Medicaid coverage are up to eight times more likely to have elevated BLLs (Wheeler and Brown, 2013).
Young children are particularly susceptible to absorption of lead (Lidsky and Schneider, 2003). Reviews of multiple studies have associated exposure to lead—even in low amounts—with IQ, test scores, impulsivity, and attention-deficit/hyperactivity disorder (Leventhal and Newman, 2010; Muller et al., 2018; Rauh et al., 2008). Some studies have linked perinatal or childhood lead exposure to adolescent body mass index (BMI), impulsivity, anxiety, and depression (Kim and Williams, 2017; Winter and Sampson, 2017).
Overcrowding
The U.S. Census collects information on the number of occupants per unit and defines crowding at more than one occupant per room within a single unit. By this metric, 4.3 percent of houses in the United States are overcrowded (U.S. Census Bureau, 2015). Units are most likely to be overcrowded in regions with disproportionately high rental prices. According to the U.S. Census from 2000, for instance, Los Angeles had more than four times the number of crowded units per capita compared to the United States as a whole (Solari and Mare, 2012).
Research has shown that living in a crowded home may have several detrimental effects on child development, although the overall picture is decidedly mixed. Solari and Mare (2012) found that living in a crowded home negatively impacts children’s academic achievement, externalizing behaviors, and physical health, even when controlling for several dimensions of SES. While this research is cross-sectional, making causal interpretations difficult, it does suggest several mechanisms by which crowding could impact child development. One hypothesis is that living in a crowded home reduces time spent studying and reading for school, thereby decreasing comprehension and test scores. Another is that overcrowding may disrupt a child’s sleep, leading to mood changes and difficulty concentrating on academics. A final hypothesis is that overcrowding increases the chances that children will become sick, preventing them from attending school or concentrating while there. All of this, coupled with a lack of privacy, could impact a child’s sociability and increase stress and behavioral problems. Each of these hypotheses need to be studied in more detail.
Other studies have shown mixed results. A 2010 study found that crowding during infancy was linked to negative cognitive and social skills, mediated primarily by mothers being less responsive to children in crowded homes (Evans et al., 2010). On the other hand, in 2012, Martin and colleagues found that overcrowding at age 2 was not a significant predictor of age 5 vocabulary, attention, or control of effortful behavior when accounting for other measures of household chaos (e.g., noise, family instability, lack of routine, and television watching) (Martin et al., 2012). This particular factor of housing requires more research, particularly because children growing up in crowded homes are more likely than their peers to end up in similar situations as adults (Leventhal and Newman, 2010), thereby “contributing to the intergenerational transmission of social inequality” (Solari and Mare, 2012, p. 3).
ENVIRONMENTAL EXPOSURES
While environmental exposures to toxicants and limited access to green spaces and healthy living areas have been found to be associated with poor health outcomes at multiple stages throughout the life course, the preconception, prenatal, neonatal, and early childhood periods represent several key developmental phases when humans may be particularly vulnerable to toxic environmental exposures. To best protect women, men, and children, it is important to understand how these substances can affect health and the methods to limit toxic exposures at these critical phases in development.
Environmental Toxicants
There are thousands of potential environmental toxicants that may be transmitted through the air we breathe, the water we use, and the soil and consumer products with which we, our food, and our water come into contact (Giudice et al., 2017). Many of these substances occur naturally in the environment (e.g., arsenic, radon, etc.), and many more are released through human-based processes (e.g., heavy metals, chemicals from plastic production and degradation, and particulates), such as through manufacturing by-products, fossil fuel use, mining, and disposal of waste (Di Renzo et al., 2015).
Several of these compounds are associated with poor preconception and prenatal outcomes. In particular, lead, methyl mercury, polybrominated biphenyls, polychlorinated biphenyls, and the pesticide chlorpyrifos have been shown to result in developmental neurotoxicity, leading experts in fetal development, obstetrics and gynecology, and fertility to conclude that there is no “safe” exposure. Furthermore, endocrine
disrupters, such as the pesticides and herbicides atrazine, glyphosate, and chlorpyrifos, are associated with cancer and neurodevelopmental disorders (Diamanti-Kandarakis et al., 2009; Gore et al., 2015). Animal models align with these human studies; endocrine disruptors in animal studies indicate that in-utero exposure leads to obesity (Manikkam et al., 2013), abnormal sexual anatomy and sexual performance (Vandenbergh, 2004), and abnormal neuronal migration (Nakamura et al., 2012), similar to that seen in children with autism. Moreover, chemicals in personal products, such as phthalates, bisphenol A (BPA), and fluoroacetic acid, are related to reproductive outcomes (Giudice et al., 2017). However, hundreds of these chemicals remain untested, and researchers estimate that the markedly rapid increase in noncommunicable diseases, particularly those related to endocrine disruption, exceeds the expected natural occurrence of change due to evolution alone. Researchers conclude that these chemicals, on their own or in combination, are likely the drivers of this change (Di Renzo et al., 2015).
In addition, several substances are associated with poor early childhood development outcomes and long-term health problems. For example, particulate matter, ozone, and carbon monoxide are associated with poor child health outcomes (Giudice et al., 2017), including impaired lung function and neurodevelopment, as well as exacerbation of existing issues, such as asthma (Webb et al., 2016). Lead, mercury, and arsenic are associated with cognitive disorders and kidney disease among children (Weidemann et al., 2016). Certain groups in the United States are more likely than others to come into contact with these environmental toxicants or to be unable to access healthy living areas and green space. In particular, certain racial and ethnic groups and families and children living in poverty are disproportionally more likely to experience exposures and see poor health outcomes related to contact with environmental toxicants (ACOG Committee Opinion, 2013; Oberg et al., 2016). For example, a Chicago longitudinal study documented marked, persistent disparities in elevated BLLs of African American children compared to white children (Sampson and Winter, 2016). African American women exposed to higher levels of PM2.5 were more likely to report higher depression severity during pregnancy and postpartum (Sheffield et al., 2018). In addition, African Americans and other people of color experienced higher PM2.5 exposure compared to whites, as did those living in poverty (Mikati et al., 2018).
Specifically, the research literature has documented strong evidence of adverse pregnancy outcomes, such as increased risk of preterm delivery, related to exposure to certain metals, including lead, which may be transmitted to the fetus through maternal BLLs (Taylor et al., 2015). This study also documented an increased risk of reduced birth weight,
smaller head circumference, and reduced crown to heel infant length related to exposure to lead from maternal BLLs. Similarly, higher maternal blood cadmium levels are associated with reduced birth weight, smaller head circumference, and reduced crown to heel length (Taylor et al., 2016), particularly for female infants. Mercury has long been shown to have negative effects on the developing fetus. One study demonstrated that levels greater than or equal to 10 parts per million of mercury can be harmful to fetal development, causing brain pathologies that result in Minamata disease, microencephaly, seizures, intellectual disability, and stillbirth, as evidenced by methylmercury poisoning in Japan and Iraq from industrial waste and the use of an imported grain treated with a fungicide containing methylmercury (Cox et al., 1989; Kalter, 2003).
Higher exposure to phthalates, chemicals added to plastics to increase flexibility and make other physical changes for use in consumer products, is associated with an increased risk of preterm delivery and spontaneous preterm delivery (Ferguson et al., 2014). In a Swedish case-control study, higher levels of butyl benzyl phthalate (BBzP), bis(2-ethylhexyl) phthalate (DEHP), and polyvinyl chloride were more likely to be found in children with a diagnosis of rhinitis and eczema; asthma; and asthma, rhinitis, and eczema, respectively (Bornehag et al., 2004). A Bulgarian case-control study found evidence of a higher risk of asthma among cases with high levels of DEHP (Kolarik et al., 2008). The presence of urinary concentrations of phthalate metabolites, particularly diethyl phthalate and BBzP, was associated with 6.6 and 8.7 percent increases, respectively, of fractional nitric oxide, a biomarker of airway inflammation. The BBzP association with fractional nitric oxide levels was particularly strong for children who wheeze (Just et al., 2012).
Phenols, particularly BPA, have been found to be associated with endocrine and neurodevelopmental problems. Prenatal BPA exposure among boys is significantly associated with a risk of decreased anogenital distance, a marker of testosterone production (Miao et al., 2011). The odds of preterm birth among infants with mothers who had higher plasma BPA levels was between 4.12 and 4.78 times higher than those without high BPA levels (Behnia et al., 2016). Each 10-fold increase in maternal urinary BPA level is associated with an increased risk of anxious and depressed behavior and poorer emotional control among 3-year-old girls (Braun et al., 2017). There is evidence that exposure to composite fillings that leach BPA can have detrimental effects on early neurodevelopment, including a heightened risk of internalizing, problem, and delinquent behaviors in children, along with increased risk of anxiety, depression, social stress, and problems with interpersonal relationships (Bellinger et al., 2008). Heightened risk of asthma is associated with prenatal exposure to BPA,
depending on the phase of fetal development in which the exposure took place (Spanier et al., 2012). Prenatal exposure among male infants is associated with a higher risk of high BMI, increased waist circumference, higher fat mass, and overweight/obesity (Gascon et al., 2015; Midoro-Horiuti et al., 2010; Spanier et al., 2012). Higher maternal blood BPA levels are associated with lower thyroid-stimulating hormone levels in male infants, suggesting poorer thyroid function (Chevrier et al., 2013; Harley et al., 2013). Higher maternal blood levels of 2,4-DCP (dichlorophenols), 2,5-DCP, and triclosan (phenols other than BPA) are associated with lower weight among male infants. A higher maternal blood level of bisphenol-S is associated with lower weight among female infants (Ferguson et al., 2018). In the same study, Ferguson et al. (2018) also demonstrated that higher maternal blood levels of parabens and benxophenone-3 are associated with lower weight among male infants.
Among young children, postnatal exposure to BPA is associated with a heightened risk of asthma, depending on the phase of child development in which the exposure took place (Donohue et al., 2013). In studies of African American, Dominican American, and Chinese children, high BPA levels were associated with a higher risk of obesity (Donohue et al., 2013; Wang et al., 2012). Increased urinary BPA levels among children is also associated with an increased risk of albuminuria, which is an indicator of future health problems, including type 2 diabetes and cardiovascular disease (Trasande et al., 2013).
Limited and Developing Evidence
A number of studies have established a relationship between poor health or birth outcomes and living in places with close proximity to potential pollution challenges. Air quality through the gestational period has been associated with increased risk of LBW, preterm birth, and infant death (Padula et al., 2012). Exposure to metals such as cadmium and arsenic has been shown to increase incidence of LBW and preterm birth (Ahmad et al., 2001; Hopenhayn et al., 2003), as have other measures of poor water quality (ChangeLab Solutions, 2017). Maternal residences near power plants have been associated with high risk for preterm birth and LBW (Ha et al., 2015; Tsai et al., 2004), while women living in neighborhoods with high exposure to natural gas wells were 1.4 times more likely to have preterm birth outcomes (Casey et al., 2016). Living in areas with high traffic density, or near high-traffic roadways, has also been associated with increased risk of preterm births in a number of studies (Currie and Walker, 2011; Fleisch et al., 2017; Harris et al., 2016; Miranda et al., 2013; Woodward et al., 2015), as has living near landfill sites (Elliott et al., 2001) or being exposed to pesticides (Wolff et al., 2007).
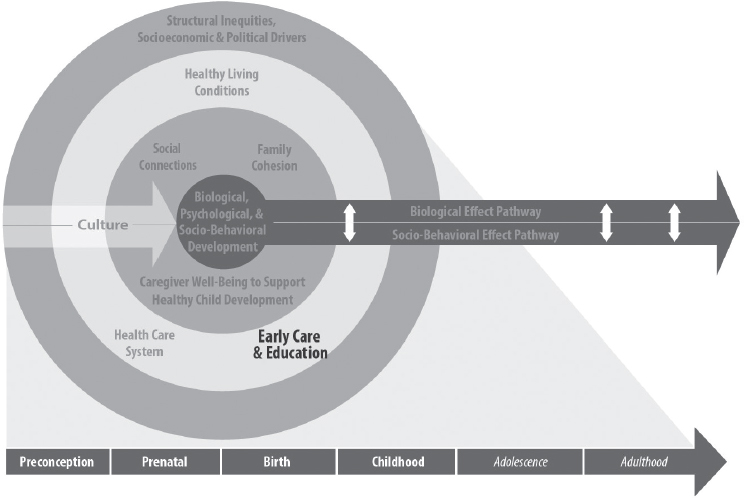
NOTES: The element of focus in this section is reflected in the second outermost ring in the model: healthy living conditions (i.e., economic security, nutrition and food security, housing, and environmental safety). This element is bolded for emphasis.
EARLY CARE AND EDUCATION
ECE6 has significant effects on children’s academic readiness and cognitive and socio-emotional development. ECE also impacts children’s physical, emotional, and mental health and well-being, and access to high-quality ECE creates many pathways through which greater health equity can be achieved (Hahn et al., 2016). The following section describes disparities in access to ECE, including specific programs such as Head Start/Early Head Start and state-funded preschool programs. See Chapter 7 for a more detailed discussion of the link between ECE interventions and outcomes related to children’s health, development, and well-being as well as recommendations to advance health equity through ECE. See Figure 3-8 for a visual of how this section ties to the report conceptual model.
___________________
6 Early care and education can be defined as nonparental care that occurs outside the child’s home. ECE services may be delivered in center-, school-, or home-based settings (NASEM, 2018).
Access to Early Care and Education
Currently, about 60 percent of all children age 5 or younger who are not in kindergarten are enrolled in at least one nonparental care arrangement. The most common primary arrangement of early child care for all children was center-based care (29 percent), followed by home-based relative care (19 percent), home-based nonrelative care (10 percent), and multiple arrangements (2 percent) (de Brey et al., 2019). These percentages varied by race and ethnicity—see Figure 3-9 for the percentages of
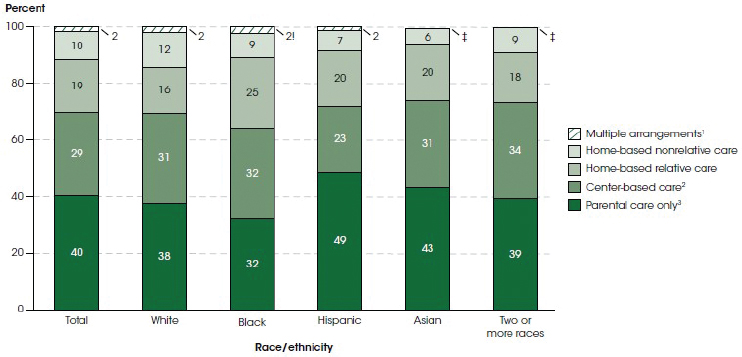
! Interpret data with caution. The coefficient of variation (CV) for this estimate is between 30 and 50 percent.
‡ Reporting standards not met. The CV for this estimate is 50 percent or greater.
1 Children who spent an equal number of hours per week in multiple nonparental care arrangements.
2 Center-based arrangements include day care centers, Head Start programs, preschools, pre-kindergartens, and other early childhood programs.
3 Children who had no regularly scheduled nonparental care arrangement and mainly received care only from their parents.
NOTES: A child’s primary arrangement is the regular nonparental care arrangement or early childhood education program in which the child spent the most time per week. Data for Pacific Islanders and American Indians/Alaska Natives not shown because reporting standards were not met. Race categories exclude persons of Hispanic ethnicity. Although rounded numbers are displayed, the figures are based on unrounded estimates. Detail may not sum to totals because of rounding. Data are sourced from the U.S. Department of Education, National Center for Education Statistics, Early Childhood Program Participation Survey of the National Household Education Surveys Program (ECPP-NHES:2016). See Digest of Education Statistics 2017, Table 202.30.
SOURCE: de Brey et al., 2019.
white, black, Hispanic, Asian, and two or more race children by type of early child care. In the United States, children under 2 years spend several more hours in informal care when compared to children in other Organisation for Economic Co-operation and Development countries (25 hours per week compared to 3.5 hours per week) (Mathur, 2016).
Enrollment in ECE (including home-based care by a relative or a nonrelative and center/school-based arrangements) is associated with the following:
- Age: Preschool-aged children from 3 to 5 years old are more likely to participate than younger children.
- Race: White and black children are more likely to participate in one of these arrangements (62 and 68 percent of all young children, respectively) than Hispanic and Asian children (51 and 57 percent, respectively). However, white and Asian children are more likely to be placed in center/school-based programs (61 and 63 percent, respectively) than black and Hispanic children (57 and 52 percent, respectively).
- Home language: Children from homes where no parents or guardians speak English are less likely to participate in any ECE.
- Parental education: The lower the level of education of the parents, the less likely their children are to participate in ECE.
- Income: The lower the level of income of the parents, the less likely their children are to participate in ECE (see Figure 3-10).
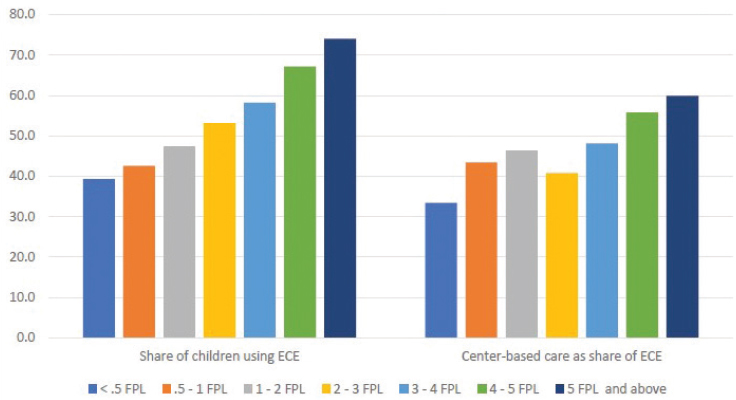
NOTE: ECE = early care and education; FPL = federal poverty level.
SOURCE: NASEM, 2018.
- Fifty-four percent of poor children do not participate in any nonparental care arrangements, compared to 31 percent of nonpoor children (de Brey et al., 2019). While about three-quarters of 4-year-olds from the highest income quintile attend preschool, only half of those from the lowest-income quintile do (Cascio and Schanzenbach, 2016). However, the relationship is not completely linear. Children from households with an income from $50,001 to $75,000 are less likely to participate in center/school-based programs than those from the poorest ($20,000 or less) or highest ($100,001 or more) income groups. That said, poor children are much less likely than their nonpoor peers to be enrolled in center-based care or home-based nonrelative care as their primary form of ECE, defined as the arrangement where the child spends most of his or her time per week (Corcoran et al., 2019).
It is important to note that access to ECE does not guarantee access to quality care, especially for children from poor households and black and Hispanic children, who are more likely to be in lower-quality care than white and Asian children (Barnett et al., 2013; Valentino, 2018). Quality of access is also not available for AI/AN children.
The federal government subsidizes the cost of child care and provides early education programs for some low-income families through the Child Care & Development Block Grant (CCDBG) and Head Start,7 which may explain the greater access to ECE among low-income families compared to those who earn slightly more. CCDBG provides child care subsidies to low-income families whose parents are working, going to school, or in a job training program. Children up to 13 years of age can be served in centers or family child care settings. (Two-thirds of children served are younger than six [Office of Child Care, n.d.].) These funds are also used to improve the quality of care, coordinate resources, conduct research and evaluation, and provide technical assistance to grantees. There have been limited studies linking child care subsidies and child health and well-being, with mixed findings. In their econometric analyses drawing on the Early Childhood Longitudinal Study, Herbst and Tekin (2010) found that subsidy use was associated with poor outcomes (i.e., reading, math, externalizing problems, approaches to learning, and interpersonal skills) for children compared to peers in the year prior to kindergarten entry. This was also found by Hawkinson et al. (2013) for math outcomes using the same dataset. The authors hypothesize that these
___________________
7 Head Start is a program of the U.S. Department of Health and Human Services that provides comprehensive early childhood education, health, nutrition, and parent involvement services to low-income children and their families. See the following section and Box 7-3 for more information on Head Start.
negative findings linking subsidy use and poor child outcomes may be due to the quality of care that children with subsidies are likely to receive and the lack of availability of high-quality child care meeting the needs of low-resource families. In contrast, Krafft et al. (2017), using a fixed effects approach that sought to adjust for selection bias, found that children receiving a child care subsidy experienced higher-quality care as reported by parents but there were no differences in the stability of arrangements or having multiple arrangements. The differences in these findings may be due to data used, methodology, analytical procedures, and how quality was defined and measured. However, these studies underscore the importance of ensuring that children from low-income families are able to access high-quality programs that meet their unique cognitive, emotional, social, and health needs.
Head Start is a federally funded preschool program for 3- and 4-year-olds from low-income households, created as part of President Lyndon Johnson’s War on Poverty. In addition to focusing on children’s learning and development, it also provides a range of services that address the holistic needs of children and families, such as health, nutrition, and parent education. Early Head Start was created in 1995 to focus on pregnant women and younger children from birth to age 3 (Office of Head Start, 2018a). Families receive services in homes, centers, or sometimes both settings (Office of Head Start, 2018b).
As of 2012, only about 15 percent of eligible families received CCDBG subsidies (Walker and Matthews, 2017), and Head Start serves less than half of all eligible 3- and 4-year-olds due to insufficient funding (Barnett and Friedman-Krauss, 2016). Early Head Start reaches about 5 percent of all eligible children (Schmit and Walker, 2016). Children from ages 2 to 4 and those living in deep poverty receive the highest rates of CCDBG subsidies (Chien, 2017). See Figure 3-11 for the percentage of children eligible for federal subsidies who receive such subsidies, by age and household income in 2013.
In terms of race and ethnicity, Latino, Asian, and AI/AN children tend to be underrepresented among eligible CCDBG recipients and Head Start children. In fiscal year 2016, 15 percent of eligible black children had access to CCDBG, but only 3 percent of eligible Asian children, 6 percent of eligible Hispanic children, and 7 percent of eligible AI/AN children were served (Ullrich et al., 2019).8 As for Head Start, Asian and Latino children are somewhat underrepresented at 36 and 38 percent of eligible children served, respectively, while 54 percent of eligible African American children are enrolled in the program (Schmit and Walker, 2016). It is important to note that these patterns differ markedly across states.
___________________
8 These data reflect federal eligibility parameters for CCDBG (Ullrich et al., 2019).
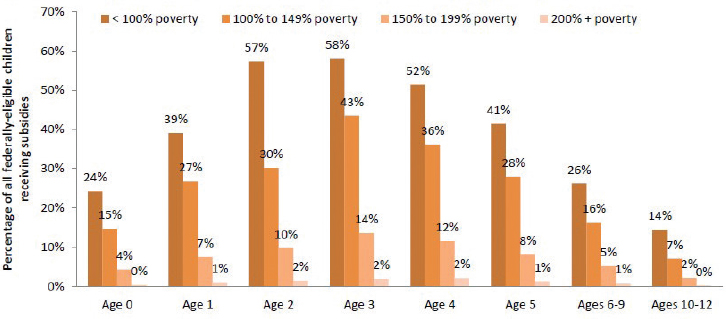
NOTES: Poverty figures are based on 2013 poverty thresholds published by the U.S. Census Bureau. For families with one adult and two children, 150 percent of poverty is $28,154 ($2,346 monthly).
SOURCE: Chien, 2017.
Pre-K programs are funded and regulated by the state. Currently, 43 states and Washington, DC, provide pre-K programs to 4-year-olds, with many also extending the program to 3-year-olds. Policies governing these programs are highly variable across states. Generally, unlike child care programs, state pre-K does not have any work or education requirements for the parents. Programs also tend to be more focused on early learning and school readiness and less on other needs of children and families, although there are exceptions.
Access data for state pre-K programs are less available, since eligibility levels and data collection vary by state. Nationwide, 5 percent of 3-year-olds and 33 percent of 4-year-olds are served in a state-funded pre-K program. More than half of all programs target low-income children, with eligibility criteria ranging from 100 to 300 percent of the federal poverty line. About half of the programs also take other risk factors or family backgrounds into consideration, including disabilities, abuse and neglect, homelessness, linguistic background, military duty, LBW, substance abuse, and teen parent status (Friedman-Krauss et al., 2018). Enrollment varies greatly by state. For 4-year-olds, 12 states9 enrolled less than 10 percent, 10 states enrolled more than 50 percent, and 5 states enrolled more than 70 percent. Only Washington, DC, and Vermont
___________________
9 Alaska, Arizona, Delaware, Hawaii, Indiana, Massachusetts, Minnesota, Mississippi, Missouri, Nevada, Rhode Island, and Washington.
enrolled more than 50 percent of 3-year-olds. Seven states10 continued to lack state-funded preschool programs. Washington, DC, enrolled the highest percentages of 3- and 4-year-olds (66 and 88 percent, respectively) (Friedman-Krauss et al., 2018).
Head Start and state pre-K programs tend to have higher quality standards in terms of teacher qualifications and supports, learning standards for children, curriculum, group size, and adult–child ratios than child care programs outside those systems. To the extent that higher-quality programs are more likely to promote children’s health and well-being, it is important for these programs to serve those with experiences of concentrated disadvantage, ACEs, and chronic stress. As mentioned earlier, while Head Start targets poor children, it currently serves only about half of all eligible children, and access by different racial groups is uneven.
Access to Special Education Services
About 2.9 percent of children from birth through age 2 are served under Part C (the Program for Infants and Toddlers with Disabilities) of the Individuals with Disabilities Education Act (IDEA), and most were served at home in 2014 (Davis, 2016). Native Hawaiian or Other Pacific Islander and white infants and toddlers had risk ratios of 1.4 and 1.2, respectively, indicating that those in each of these racial/ethnic groups were slightly more likely than those in all other racial/ethnic groups combined to be served under Part C. In 2014, 6.1 percent of children ages 3 through 5 were served under Part B (Assistance for Education of All Children with Disabilities) of IDEA. In 2014, AI/AN, Native Hawaiian or Other Pacific Islander, and white children ages 3–5 had risk ratios above 1 (1.4, 1.5, and 1.2, respectively), indicating they were more likely to be served under Part B than were children ages 3 through 5 in all other racial/ethnic groups combined. In 2014, 8.7 percent of individuals ages 6 through 21 were served under Part B, with the most in specific learning disabilities. AI/AN, black or African American, and Native Hawaiian or Other Pacific Islander children ages 6–21 had risk ratios above 1 (1.7, 1.4, and 1.6, respectively), indicating that they were more likely to be served under Part B than children in all other racial/ethnic groups combined.
Unfortunately, access to early intervention and special education services is variable due to the wide discrepancy in eligibility criteria (Twardzik et al., 2017). Using data from the 2007 National Survey of Children’s Health, Bethell and colleagues (2011) found that 19.5 percent of children received a parent-completed developmental screening. This varied across states and demographics. Screening was highest for
___________________
10 Idaho, Montana, New Hampshire, North Dakota, South Dakota, Utah, and Wyoming.
children who were young, black, and publicly insured and lowest for children who were uninsured and had gaps in insurance coverage. They also found a significant gap between the developmental screening that is recommended by the American Academic of Pediatrics and what is reported nationally.
Public Education
Educational attainment is correlated with health outcomes (NASEM, 2017a). Studies indicate that individuals with more education are more likely to have economic stability and better health outcomes (Heckman et al., 2018). Yet, disparities exist among income and racial groups in terms of both education inputs and outcomes. For example, recent data indicate increasing school segregation, with a growing trend of more schools that are high poverty and high minority, from 10 percent of schools in 2000 to 17 percent in 2013 (Chang, 2018). Other research examining longitudinal data established an association between court-ordered desegregation of schools (from 1954 to 1990) and subsequent adult outcomes for African Americans (e.g., educational attainment, adult earnings, probability of incarceration) through 2013 (Johnson, 2011). However, some contend that it is not segregation that is increasing but rather the number of non-minority students in public schools. Regardless, research also indicates that school districts serving the largest populations of minority (e.g., black, Latino, or AI/AN) students receive approximately $1,800, or 13 percent, less per student in state and local funding than those serving the fewest students of color. The United States spends approximately 7 percent—or $1,000—less per pupil on students in the highest poverty districts than those educated in the wealthiest (Morgan and Amerikaner, 2018). Another estimate suggests a funding gap of $23 billion between school districts serving predominantly nonwhite students and those with mostly white students, despite serving the same number of children (EdBuild, 2019).
Funding inequities between rich and poor or majority-white and majority-minority schools are likely one factor contributing to the achievement gaps. Numerous studies have shown a relationship between school socioeconomic and racial/ethnic composition and student achievement outcomes (Kainz and Pan, 2014; Ready and Silander, 2011). Specifically, schools with large proportions of poor, African American, and Hispanic students have been shown to have lower rates of learning growth compared to schools serving larger proportions of white and high-income students. There are conflicting patterns of evidence regarding unique and overlapping effects of racial/ethnic and poverty concentrations on children’s academic achievement. However, recent analyses of test data from the national public K–12 system have indicated that concentrations
of poverty are the proximal explanation for observed negative associations between racial concentration and student achievement (Reardon, 2016). That is, racial segregation has a negative effect on education performance precisely because racial segregation is an indicator of students’ exposure to poverty concentration and isolation and limited access to needed supports.
For example, data from the U.S. Department of Education’s National Center for Education Statistics show that graduation rates collected from 2010–2011 to 2015–2016 increased from 79 to 84 percent (National Center for Education Statistics, n.d.). That is, more than four out of five students who were first-time 9th-graders in 2012–2013 had completed high school by 2015–2016 (within 4 years). There are some racial differences, with Asian/Pacific Islanders and white students graduating at higher rates, 91 and 88 percent, respectively, compared to Hispanic (79 percent), black (76 percent), and AI/AN (72 percent) students.
Similarly, the dropout rate has declined from 15 percent in 1970 to 6 percent in 2016. The youth dropout rate in 1972 was 12 percent for whites, 21 percent for blacks, and 34 percent for Hispanics. In 2016, the youth dropout rate for blacks was 6 percent (close to the national average) and 9 percent for Hispanics, compared to 5 percent for whites and 3 percent for Asians (Child Trends DataBank, 2018). It is important to note that these estimates do not include those who were institutionalized, which is particularly pronounced for black and Hispanic male youth. There is a link between non-graduation and incarcerations (Kearney et al., 2014; Skiba et al., 2014).
There are many factors that lead to educational attainment or lack of education (i.e., dropout). However, one predictor of high school graduation or dropout is reading proficiency at the end of 3rd grade. In a study of nearly 4,000 students born between 1979 and 1989, Hernandez (2012) found that those who did not read proficiently by 3rd grade were four times more likely to leave school without a diploma than proficient readers, with the rates increasing for those who could not master basic reading skills. According to the National Assessment of Education Progress, in 2017, while 47 percent of white and 59 percent of Asian 4th graders were proficient in reading, only 20 percent of African American and AI/AN students and 23 percent of Hispanic students achieved at that level (The Nation’s Report Card, 2017). (A similar gap exists between low-income and nonpoor students.) Furthermore, the relationship between reading proficiency and dropout was particularly pronounced for students from poor households. Hernandez found that 31 percent of African American students and 33 percent of Hispanic students from poor households who were not proficient in 3rd grade reading did not graduate, compared to 22 percent for white children from poor households. The racial and
education gaps disappear when students are proficient in 3rd-grade reading and not living in poverty. However, the confound between poverty and race and ethnicity often makes it difficult to isolate the unique effects of each characteristic.
REVISITING CROSSCUTTING ELEMENTS
Racism and Discrimination
The 2017 report Communities in Action: Pathways to Health Equity describes racism as “an umbrella concept that encompasses specific mechanisms that operate at the intrapersonal, interpersonal, institutional, and systemic levels of a socioecological framework” (NASEM, 2017a, pp. 104–105) (see Figure 3-12 for examples of how racism plays out at these levels). The report makes the distinction that racism is “not an
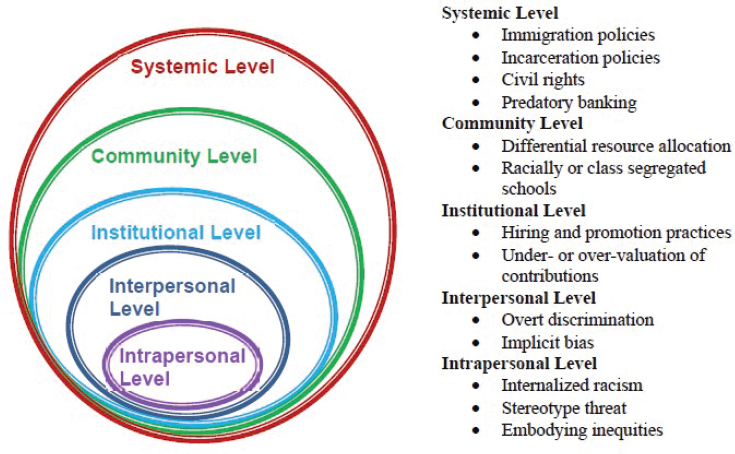
NOTES: The mechanisms by which the social determinants of health operate differ with respect to the level. For the intrapersonal level, these mechanisms are individual knowledge, attitudes/beliefs, and skills. At the interpersonal level, they are families, friends, and social networks. At the institutional level, they are organizations and social institutions. At the community level, they are relationships among organizations. At the systemic level, the mechanisms are national, state, and local policies, laws, and regulations.
SOURCE: Adapted from NASEM, 2017a.
attribute of minority groups; rather it is an aspect of the social context and is linked with differential power relations among racial and ethnic groups” (NASEM, 2017a, p. 105; see also Guess, 2006). Camara Jones’s (2000) theoretic framework for racism uses an allegory of a garden to illustrate the relationships between these multiple levels and to provide a framework to guide interventions that would address these mechanisms of racism. It is also important to note that discrimination can affect a variety of racial and ethnic minority groups. For example, Asian Americans are often ascribed the stereotype of “model minority”; however, they can experience discrimination and its effects, as well as social or economic conditions that affect health (Chou and Feagin, 2015).
Reported racism11 has been documented as a determinant of poor health outcomes across the life-span, particularly for mental health (e.g., depression, anxiety, psychological stress), with weaker evidence for physical health (Paradies et al., 2015). Bailey et al. (2017) highlight structural racism as an important but understudied driver of inequities, defining structural racism as “the totality of ways in which societies foster racial discrimination, via mutually reinforcing inequitable systems (e.g., in housing, education, employment, earnings, benefits, credit, media, health care, criminal justice, etc.) that in turn reinforce discriminatory beliefs, values, and distribution of resources, reflected in history, culture, and interconnected institutions” (p. 1454). For more information on racism and discrimination as root causes of inequities, see Chapter 3 of Communities in Action: Pathways to Health Equity (NASEM, 2017a).
Childhood exposure to racism is mostly documented as experiences of discrimination. For example, the National Survey of Children’s Health includes an item that asks parents if their child has ever been treated or judged unfairly because of their race or ethnic group. Data from 2016–2017 indicate that the overall prevalence of exposure to discrimination is low, at 3.7 percent nationwide. However, when these data are examined by subgroups, there are disparities. For instance, black and other, non-Hispanic children were most likely to be treated or judged unfairly due to their race or ethnicity. (See Table 3-3 for a breakdown by race and ethnicity.)
___________________
11 This meta-analysis defined reported racism as self-reported racism experienced directly in interpersonal contact; racism directed toward a group (e.g., based on ethnicity/race/nationality) of which the person is a member; vicarious experiences of racism (e.g., witnessing racism experienced by family members or friends); proxy reports of racism (e.g., a child’s experiences of racism as reported by their parent); and internalized racism (i.e., the incorporation of racist attitudes and/or beliefs within an individual’s worldview) (Paradies et al., 2015).
TABLE 3-3 Childhood Experiences of Discrimination by Race and Ethnicity
| Race or Ethnicity | Percent of Children Who Have Ever Been Treated or Judged Unfairly Because of Their Race or Ethnic Group |
|---|---|
| Black, non-Hispanic | 10.4 |
| Hispanic | 4.2 |
| Other, non-Hispanic | 7.4 |
| White, non-Hispanic | 1.0 |
SOURCE: National Survey of Children’s Health, 2016–2017, from the Data Resource Center for Child and Adolescent Health, 2019.
There is an existing literature stream that draws connections between racism and early development and well-being outcomes. Specifically, negative prenatal and birth outcomes have been shown to be associated with discrimination or unfair treatment. An integrative review of 15 studies assessing adverse birth outcomes and discrimination found significant relationships between racial discrimination and LBW, preterm birth, and small size for gestational age (Alhusen et al., 2016). Studies in this review that examined mediating variables that are proximally related to birth outcomes (e.g., prenatal care, employment opportunities, neighborhood characteristics, or inflammatory markers) also found a significant association between these specific variables and racial discrimination. Another review found similar outcomes when investigating the relationship between racial discrimination and black-white disparities in birth outcomes, showing a consistent positive relationship between discrimination and preterm birth and LBW or very LBW (Giurgescu et al., 2011). The review findings also suggest that parental lifetime and childhood experiences of discrimination could have a stronger association with birth weight than experiences of discrimination reported during pregnancy.
For childhood outcomes, the available evidence suggests that discrimination affects children through two pathways: (1) direct transmission to the child and (2) discrimination that affects the parent directly (sometimes called “vicarious racism”). A systematic review examining mostly cross-sectional studies synthesized the study findings related to racial discrimination and child health and well-being outcomes (Priest et al., 2013). Associations were most salient among mental health outcomes (e.g., depression and anxiety). The authors reported statistically significant associations between discrimination and 76 percent of the mental health outcomes studied. The findings also showed a consistent relationship between discrimination and reduced positive
mental health outcomes, such as self-esteem, self-worth, and psychological adaption and adjustment. The authors reported weaker results for child physical health outcomes, but they also note that this likely reflects the extended period of time that it takes for physical health outcomes to manifest. With respect to vicarious racism effects, there is some evidence to suggest that there is a link between secondhand exposure to racism and socio-emotional (e.g., externalizing behavior) and mental health (e.g., depression) outcomes among children (Heard-Garris et al., 2018). Acevedo-Garcia et al. (2013) identify three directions for research on interpersonal and institutional discrimination and child health:
- Incorporating a life course perspective into studies of discrimination and children’s health,
- Linking residential segregation with geography of opportunity12 conceptual frameworks and measure, and
- Considering residential segregation along with segregation in other contexts that influence children’s health.
American Indian/Alaska Native Children and Children of Immigrant Background: A Closer Look
This section describes two populations of children and families for whom the crosscutting elements in this chapter are particularly salient: AI/AN children and children of an immigrant background. While there are many subgroups that have unique needs and historical contexts related to health equity, these are two that the committee has identified as important to highlight here because of the lack of attention given to these groups, often due to data collection or sampling issues (ASPE, 2007; NASEM, 2017a; National Congress of American Indians, n.d.). For these subgroups, racism and discrimination operate at multiple levels, including interpersonal, everyday experiences of discrimination and policies that obstruct access to health-promoting goods and services or induce historical trauma that can affect multiple generations. Their experiences across the domains discussed in this chapter (e.g., family cohesion, access to health care, neighborhood conditions) are amplified when examined with the additional lens of structural inequities.
___________________
12 One tool for measuring opportunity by units of geography is the Child Opportunity Index, a data resource that compiles neighborhood-level indicators related to educational, health and environmental, and social and economic opportunity (Acevedo-Garcia et al., 2016a).
American Indians and Alaska Natives
Health outcomes across AI/AN populations AI/AN populations experience stark disparities across a number of health indicators. Researchers hypothesize that a combination of factors may be related to these disparities, including the SDOH (i.e., poverty, unemployment, and education) (Elder et al., 2016), the effect of high rates of obesity and inactivity, alcohol and tobacco use, and a lack of access to health care (Bhaskar and O’Hara, 2017; Cobb et al., 2014; Rutman et al., 2016), particularly care that is culturally congruent (Lewis and Myhra, 2018; Rentner et al., 2012). This stems in large part from the population’s unique history in relation to U.S. policies, historical trauma, and the consequences for the health and well-being of generations (for more information on the historical and legal context of AI/ANs, see Appendix A in NASEM, 2017a). Moreover, health disparities and inequities vary by region, with some tribes experiencing high levels and intensity of alcohol use (Fortin et al., 2016), poor birth outcomes (Coughlin et al., 2013; Hwang et al., 2013; Kim et al., 2014), and poorer reproductive health (Rutman et al., 2012). AI/AN communities also experience higher levels of racial misclassification, which reduce the reliability of existing health data for these populations (Jim et al., 2014). In addition, certain SDOH, such as violence against AI/AN women, is not consistently tracked across jurisdictions, making the justification for systemic changes challenging. For example, in some counties in the United States, AI/AN women are 10 times more likely to be murdered as compared to the national average, are 3 times as likely to be raped in their lifetimes compared to any other racial or ethnic group, and the perpetrator of rape against AI/AN women is more likely to be white compared to other racial and ethnic groups. More research is needed to fully explicate the potential health impacts for AI/AN women living with the disproportionate level of violence specific to their race and gender in these contexts (Bachman et al., 2008).
Birth and postpartum outcomes While the research on AI/AN populations remains limited, major disparities have been documented, particularly concerning birth outcomes. The mortality rate for AI/AN infants aged 0 to 1 year of age is 1.61 times higher than that of white children, with sudden infant death syndrome, unintentional injuries, and influenza/pneumonia being the top three causes of death (Wong et al., 2014). Concomitantly, AI/AN women experience some of the highest rates of diabetes and hypertension in the nation, as well as preeclampsia-eclampsia (Zamora-Kapoor et al., 2016), which are related to poor birth outcomes (Anderson et al., 2016; Dorfman et al., 2015). In a comparison between AI/AN, black, and Hispanic women, significantly lower rates of fetal and first-day mortality were found among black and Hispanic women for
2005–2008 as compared to 1995–1998 rates. However, among AI/AN, the rates did not decline significantly for AI/AN women.
Studies have found that preterm birth rates among AI/AN women (13.0 percent) are significantly higher as compared to the rate for all women in the United States (11.4 percent). Stress before and during pregnancy constitutes one of the biggest contributors to preterm birth. Research has demonstrated that AI/AN women experience the highest number of major stressors in the 12 months before becoming pregnant and in the 12 months before giving birth. Interpersonal violence rates, including rates of childhood physical abuse, rape, and multiple victimizations, are highest among AI/AN women. Access to prenatal care is limited for AI/AN women, with twice the rate of AI/AN women accessing prenatal care late or receiving no prenatal care compared with other women (Raglan et al., 2016). In a study of nearly 300 AI/AN women, about 30 percent reported depressive symptoms 13–24 months postpartum. Nearly 70 percent of the sample reported financial events, 60 percent reported emotional events, 46 percent reported partner-related events, 38 percent reported traumatic events, and 19 percent reported IPV. Having had at least one partner-related or traumatic stressful life event or at least one traumatic stressful life event was significantly related to depression symptoms (Ness et al., 2017).
Adverse childhood experiences In data from the 2011–2012 National Survey of Children’s Health, AI/AN children were more likely to report eight of nine ACEs, including income deprivation, witnessing or experiencing violent victimization, racial/ethnic discrimination, household substance abuse, domestic violence, parental incarceration, divorce, and death of a parent. AI/AN children were also more likely to report more than one ACE compared to non-Hispanic white children. After adjusting for sociodemographic factors, the difference between AI/AN and white children was no longer significant, which suggests that the heightened risk for AI/AN children was explained by family and neighborhood factors. For AI/AN children reporting with one or more ACE, parents reported an increasing prevalence of behavioral issues, including arguing, lack of emotional control, and school problems, and more provider-diagnosed behavioral disorders, such as depression, anxiety, and attention-deficit/hyperactivity disorder (Kenney and Singh, 2016).
Health system challenges Studies of health systems issues within AI/AN communities remain limited. The Indian Health Service provides national access to care statistics, but updated reports are lacking, and few focus specifically on the needs of early childhood. In one study of 59 emergency medical service agencies, or ambulance services, 46,761 annual emergency
responses were reported, with 9,981 annual inter-facility transports. Pediatric emergency responses represented 15 percent (n = 7,190) of the total emergency responses, with an annual average of 180 pediatric responses per agency. Nine agencies (15 percent) reported that their agency did not have a medical director. Agencies with a medical director were more likely to report availability of pediatric medical direction than agencies without one. About 80 percent of agencies reported that their emergency medical services (EMS) providers needed pediatric continuing education for certification and recertification. About one-quarter of agencies reported that all of their EMS providers received pediatric continuation education training, while six agencies reported that no providers had received pediatric training. About half of agencies reported having a mass casualties plan, and of these, 15 had participated in a pediatric-focused mass casualties drill within 2 years of the survey. About 30 percent of all agencies had responded to a mass casualty incident involving a large number of pediatric patients that overwhelmed their service. Of these, about half of the agencies reported that they did not have enough pediatric equipment available when they responded to the incident at that time (Genovesi et al., 2014).
Resilience Few studies examine factors contributing to resilience among AI/AN people; however, one review found that, across eight relevant research studies examining resilience among AI/ANs, resilience was an ongoing, dynamic process that responds to a changing environment, is evident within the life course, and can be accessed through culture. Cultural values, beliefs, and practices were identified as essential resources for AI/AN resilience along the life course and across generations. Three studies found culture could be best accessed through the use of narratives, lived experiences, and traditional stories (Ore et al., 2016).
Children of Immigrant Backgrounds
Children of immigrant backgrounds are one of the largest growing population segments among the U.S. population of 0- to 10-year-olds. Nearly 90 percent of children in immigrant families are U.S. citizens, and about one-quarter of them have an unauthorized immigrant parent (Koball et al., 2015). Thus, many children who live in immigrant families—irrespective of their own citizenship status—are greatly impacted by not only the household context but also the larger policy context for immigrant families (Filindra et al., 2011; Koball et al., 2015; Yoshikawa, 2011). In addition, research suggests that the United States will increasingly need to depend on immigrants and their children to maintain its workforce (Singer, 2012). To that end, supporting children of immigrant
background and their families is essential to ensure not only individual healthy developmental trajectories, but also the future of the country. Much of the following discussion applies to documented immigrants, unless otherwise specified.
Many children of immigrant background face unique stressors that influence their development. For example, many parents who are first-generation immigrants have fled extreme poverty, political persecution, sexual violence, and other sources of oppression, which are traumatic experiences with long-term consequences (Petrosky et al., 2017). In addition, many have experienced discrimination in housing and employment, as well as overt expressions of racism in their daily lives. These traumatic experiences can have implications for their parenting.
Residential segregation, among other factors, is one contributing factor as to why immigrants tend to end up living in concentrated poverty, which might lead to unhealthy levels of stress during pregnancy and in the infant’s first years of life (NASEM, 2015b). Living in poverty in addition to an undocumented status may result in inadequate supports for caregiving: lack of high-quality day care, preschool, and elementary/middle school; and lack of access to adequate housing and health care (Yoshikawa and Kalil, 2011). There is growing evidence that documents the harm to children of parents with unauthorized status in terms of economic and socio-emotional hardship. For example, children fearing the deportation of a parent may show psychological distress by experiencing problems eating or sleeping, increases in headaches and stomachaches, anger or detachment, and depression and anxiety (Artiga and Ubri, 2017; Rojas-Flores et al., 2017).
The current policies toward immigrants in the United States have become another source of the toxic stress response for these families and their children. In particular, the dramatic recent increases in deportation of U.S. immigrants and the detention of parents at the borders seeking asylum have resulted in the separation of thousands of children from their parents (HHS Office of Inspector General, 2019). Research conducted since the 1950s shows that the scientific evidence is clear: separating children from families has long-term damaging health consequences for the children (Acker et al., 2019). These traumatic experiences can have cascading effects in multiple areas, even after reunification. Furthermore, recent immigration policies have had a documented effect on parents’ willingness to enroll their children of immigrant background in public programs, including those in ECE settings (Cervantes et al., 2018). This could have serious implications because it increases the environmental barriers for these families; they refrain from using programs that could ameliorate or prevent educational and health problems (Koball et al., 2015; Yoshikawa, 2011). These barriers could
be exacerbated as the increasing efforts to limit access to government services, such as education and health care, take effect at the federal or state levels.
However, research conducted both in the United States and internationally shows that if the right conditions are attainable and present, children of immigrant background can not only thrive, but also excel (García Coll et al., 2012; Motti-Stefanidi and García Coll, 2018). Many countries have policies that support children of immigrant backgrounds at the state and national levels (Bachega, 2018; Line and Poon, 2013; OECD, 2018; Shinkman, 2018). Domestic and international studies show that policies providing support for immigrant families facilitate increases in positive outcomes, such as high school graduation rates. A U.S. national study showed that state family-supportive policies, such as allowing immigrant families to obtain driver’s licenses and health care benefits, among others, lead to higher high school graduation rates (Filindra et al., 2011). An international study showed that immigrant-supportive public policies at the country level also contribute to more optimal health outcomes in children of immigrants (Marks et al., 2018).
At the community and neighborhood levels, research shows that school programs that support dual-language learners facilitate positive developmental trajectories for children of immigrant background (NASEM, 2017b). In addition, interventions with a two-generation preventive focus also provide promising models and strategies to further support the healthy development of children of immigrant background (Valdez et al., 2013; Williamson et al., 2014).
ACCUMULATION OF RISK
This chapter has provided an overview of how family cohesion and social connections (see Chapter 4), health care (see Chapter 5), early living conditions (i.e., economic security, nutrition and food security, housing, and environmental exposures) (see Chapter 6), ECE (see Chapter 7), and racism converge through an accumulation of risk factors that influence a child’s entire life course. Extensive evidence shows that exposure to multiple social risk factors or continuous exposure to a single risk factor is more harmful to children than one-time exposure to a single risk, across a broad range of outcomes (Evans et al., 2013; Sameroff, 1998). It is most common for researchers to calculate composite scores to represent the accumulation of risk factors by summing dichotomous indicators for each risk factor, although other, more complex methods exist (Evans et al., 2013). Across studies, there is variation in what is included within cumulative risk scores; in some studies, researchers focus on information about the family and residential context, whereas other studies may
include information about the residential neighborhood context and/or school experiences.
Cumulative risk scores offer an easily interpreted measure and are strong predictors of child health (Evans et al., 2013). Notably, however, studies using cumulative risk scores typically do not consider the sequential timing or intensity of risk factors and are limited by the assumption that each type of risk is equally weighted and additive (i.e., not considering synergistic or interactive effects between risk and/or protective factors) (Dohrenwend, 2006; Evans et al., 2013). Longitudinal birth cohort studies with frequent assessments, such as the Dunedin Multidisciplinary Health and Development Study (Poulton et al., 2015) or the Avon Longitudinal Study of Parents and Children (Boyd et al., 2012; Fraser et al., 2012), provide an opportunity to investigate the chronicity of multiple risk factors over time (Danese et al., 2009; Dunn et al., 2018). The next section of this chapter explores the Adverse Childhood Experiences (ACEs) Study as an example of a composite approach to investigate the relationship between cumulative risk through childhood experiences and outcomes in adulthood (Felitti et al., 1998).
Adverse Childhood Experiences
As elaborated in Chapter 2, prenatal and early life environments have a profound role in shaping life course health, and even the health of the next generation, through a complex interplay of contextual and biological factors, including individual genetic characteristics, gene–environment interactions, family supports or stressors, environmental factors, and developmental experiences. This chapter looks more closely at the social and environmental contexts in which the aforementioned biological processes unfold and which structures promote the accumulation of risk or resilience. Perhaps the most well-known study of accumulated risk is the ACEs Study conducted by CDC and Kaiser Permanente and published by Felitti et al. in 1998 (see Box 3-9).
Since the publication of the ACEs Study, subsequent research has demonstrated that the health impacts of ACEs are evident as early as infancy, and even in the prenatal and preconception periods. Parental ACEs are associated with increased risk of negative preconception and prenatal outcomes, including menstrual irregularity, reduced odds of conception, chronic health complications, preeclampsia, psychological risk (prenatal and postpartum depression), social risk (age at first pregnancy, education level, income, relational resilience, perceived stress, IPV, partner’s drug abuse, maternal hostile behavior in infancy), behavioral risk (alcohol use, drug use, smoking), and negative pregnancy outcomes (miscarriage, premature delivery, reduced birth weight, shorter gestational age) (Ångerud
et al., 2018; Brunton, 2013; Christiaens et al., 2015; Leeners et al., 2014; Li et al., 2018; Liu et al., 2018; Olsen, 2018; Racine et al., 2018; Smith et al., 2016).
Outcomes related to prenatal and early childhood exposure to ACEs in children include altered neurodevelopment, neurocognitive function, cerebral processing, functional and structural brain connectivity involving the amygdala and (pre)frontal cortex, hypothalamic-pituitary-adrenal axis, and autonomous nervous system (Brunton, 2013; McGowan and Matthews, 2018; Provençal and Binder, 2015; van den Bergh et al., 2018). Infants and children exposed to ACEs demonstrate increased risk of sleep disturbance, failure to thrive, growth and developmental delays, viral and bacterial infection, atopic disease (including asthma, allergies,
TABLE 3-4 Leading Causes of Death in 2015 and Their Relationship with the Experience of Four or More ACES
| Leading Causes of Death in the United States, 2015 | Odds Ratio Associated with ≥4 ACEsa | |
|---|---|---|
| 1 | Heart disease | 2.1 |
| 2 | Cancer | 2.3 |
| 3 | Chronic lower respiratory disease | 3.0 |
| 4 | Accidents | — |
| 5 | Stroke | 2.4 |
| 6 | Alzheimer’s disease | 11.2 |
| 7 | Diabetes | 1.5 |
| 8 | Influenza and pneumonia | — |
| 9 | Kidney disease | — |
| 10 | Suicide | 30.1 |
a Hughes et al., 2017, for all odds ratios except for stroke and Alzheimer’s disease; Felitti et al., 1998, for stroke; Center for Youth Wellness, 2014, for Alzheimer’s disease.
SOURCE: CDC, 2017.
and eczema), overweight and obesity, and learning and behavioral difficulties (Björkenstam et al., 2015; Burke et al., 2011; Giordano et al., 2014; Kerker et al., 2015; Matheson et al., 2016; Oh et al., 2017; Rhodes et al., 2012; Ryan et al., 2016; Shen et al., 2016; Thompson et al., 2017). Studies have also shown that ACEs are associated with increased risk-taking behaviors in adolescents, including early sexual initiation, teen pregnancy, teen paternity, substance use, and victimization (Hughes et al., 2017; Shin et al., 2009; Thompson et al., 2017).
Evidence points to several mechanisms by which ACEs and other early life stressors affect preconception, prenatal, and postnatal health:
- Neuro-endocrine-immune dysregulation, metabolic regulation, and gene expression (as discussed in Chapter 2);
- Increased risk of health problems that may affect pregnancy outcomes, including obesity, diabetes, and autoimmune disease;
- Increased risk of parental mental health disorders;
- Increased risk behaviors, such as smoking, and substance use and risk exposures, such as victimization;
- Changes in epigenetic regulation that may be passed down via maternal or paternal germ lines; and
- Difficulty with emotional regulation.
Beginning in 2009, many states began to systematically collect population-based representative data on ACEs, beginning with adults via the Behavioral Risk Factor Surveillance System (BRFSS). In 2011–2012, a modified ACE inventory was introduced into the National Survey of Children’s Health. These surveillance activities provide scientists and policy makers with information on the prevalence of ACEs and data to study associations with health outcomes. According to the most recent published CDC data reporting from the BRFSS, in 23 states, 62 percent of American adults have experienced at least one of the eight ACEs, and 15 percent have experienced four or more (Merrick et al., 2018). In 2012, the Institute for Safe Families formed the ACE Task Force to assess the prevalence of ACEs in Philadelphia in order to broaden the concept of ACEs to reflect the experiences of children of color in urban communities (Public Health Management Corporation, 2013).13
While the term refers specifically to the 10 categories identified in the ACEs Study, it is recognized that other forms of early life adversity, such as economic hardship, food and housing insecurity, unsafe toxic environments, and discrimination, are also critical in shaping health and developmental outcomes. Cumulative exposure to negative experiences increases the risk of negative outcomes, but the converse is also true—supportive, nurturing, and buffering experiences also add up in a manner that is protective of health and neurodevelopmental outcomes. Thus, family, social, neighborhood, and structural environmental factors play an important role in shaping life course health and the health of future generations.
CONCLUSION
This chapter provides an overview of the risk and protective factors relevant to each level of the committee’s conceptual model (see Figure 1-9). These factors are interrelated and complex, but they also demonstrate critical areas where there are opportunities for change and the science may be applied to inform interventions for children and families. In the chapters that follow, the committee takes the vast science base described in Chapters 2 and 3 and applies it to the necessary actions to advance child and family health outcomes and health equity across the domains discussed in this chapter (see Table 3-1 at the beginning of this chapter).
___________________
13 The original ACEs study sample was composed of primarily white, middle-class, and educated individuals (Felitti et al., 1998).
REFERENCES
Accortt, E. E., A. C. Cheadle, and C. Dunkel Schetter. 2015. Prenatal depression and adverse birth outcomes: An updated systematic review. Maternal and Child Health Journal 19(6):1306–1337.
Acevedo-Garcia, D., M. J. Soobader, and L. F. Berkman. 2005. The differential effect of foreign-born status on low birth weight by race/ethnicity and education. Pediatrics 115(1):e20–e30.
Acevedo-Garcia, D., L. E. Rosenfeld, E. Hardy, N. McArdle, and T. L. Osypuk. 2013. Future directions in research on institutional and interpersonal discrimination and children’s health. American Journal of Public Health 103(10):1754–1763.
Acevedo-Garcia, D., E. F. Hardy, N. McArdle, U. I. Crisan, B. Romano, D. Norris, M. Baek, and J. Reece. 2016a. The Child Opportunity Index: Measuring and mapping neighborhood-based opportunities for children. Waltham, MA, and Columbus, OH: diversitydatakids. org and Kirwan Institute for the Study of Race and Ethnicity.
Acevedo-Garcia, D., N. McArdle, E. Hardy, K.-N. Dillman, J. Reece, U. I. Crisan, D. Norris, and T. L. Osypuk. 2016b. Neighborhood opportunity and location affordability for low-income renter families. Housing Policy Debate 26(4–5):607–645.
Acker, J., P. Braveman, E. Arkin, L. Leviton, J. Parsons, and G. Hobor. 2019. Mass incarceration threatens health equity in America. Princeton, NJ: Robert Wood Johnson Foundation.
ACOG (American College of Obstetricians and Gynecologists) Committee Opinion No. 575. 2013. Exposure to toxic environmental agents. Fertility and Sterility 122(4):931–935.
Ahern, J., K. E. Pickett, S. Selvin, and B. Abrams. 2003. Preterm birth among African American and white women: A multilevel analysis of socioeconomic characteristics and cigarette smoking. Journal of Epidemiology and Community Health 57(8):606–611.
Ahmad, S. A., M. H. Sayed, S. Barua, M. H. Khan, M. H. Faruquee, A. Jalil, S. A. Hadi, and H. K. Talukder. 2001. Arsenic in drinking water and pregnancy outcomes. Environmental Health Perspectives 109(6):629–631.
Aizer, A. 2008. Neighborhood violence and urban youth: NBER working paper no. 13773. https://www.nber.org/papers/w13773 (accessed April 18, 2019).
Akinbami, L. J., J. E. Moorman, P. L. Garbe, and E. J. Sondik. 2009. Status of childhood asthma in the United States, 1980–2007. Pediatrics 123:S131–S145.
Akinbami, L. J., J. E. Moorman, A. E. Simon, and K. C. Schoendorf. 2014. Trends in racial disparities for asthma outcomes among children 0 to 17 years, 2001–2010. Journal of Allergy and Clinical Immunology 134(3):547–553.
Alexander, D., and J. Currie. 2017. Is it who you are or where you live? Residential segregation and racial gaps in childhood asthma. Journal of Health Economics 55:186–200.
Alhusen, J. L., K. M. Bower, E. Epstein, and P. Sharps. 2016. Racial discrimination and adverse birth outcomes: An integrative review. Journal of Midwifery & Women’s Health 61(6):707–720.
American Pregnancy Association. 2017. Nutrients & vitamins for pregnancy. https://americanpregnancy.org/pregnancy-health/nutrients-vitamins-pregnancy (accessed April 22, 2019).
Anderson, K., P. Spicer, and M. Peercy. 2016. Obesity, diabetes, and birth outcomes among American Indians and Alaska Natives. Maternal and Child Health Journal 20(12):2548–2556.
Andolfatto, D. 2017. Why do unemployment rates vary by race and ethnicity? https://www.stlouisfed.org/on-the-economy/2017/february/why-unemployment-rates-vary-races-ethnicity (accessed April 18, 2019).
Ångerud, K., E. M. Annerbäck, T. Tydén, S. Boddeti, and P. Kristiansson. 2018. Adverse childhood experiences and depressive symptomatology among pregnant women. Acta Obstetricia et Gynecologica Scandinavica 97(6):701–708.
Anstey, E. H., J. Chen, L. D. Elam-Evans, and C. G. Perrine. 2017. Racial and geographic differences in breastfeeding—United States, 2011–2015. Morbidity Mortality Weekly Report 66:723–727.
Arenz, S., R. Ruckerl, B. Koletzko, and R. von Kries. 2004. Breast-feeding and childhood obesity—a systematic review. International Journal of Obesity and Related Metabolic Disorders 28(10):1247–1256.
Artiga, S., and P. Ubri. 2017. Living in an immigrant family in America: How fear and toxic stress are affecting daily life, well-being, and health. Menlo Park, CA: Kaiser Family Foundation.
Asante-Muhammad, D., C. Collins, J. Hoxie, and E. Nieves. 2017. The road to zero wealth: How the racial wealth divide is hollowing out America’s middle class. Washington, DC: Prosperity Now and Institute for Policy Studies.
ASPE (Assistant Secretary for Planning and Evaluation). 2007. Gaps and strategies for improving American Indian/Alaska Native/Native American data. Washington, DC: Office of the Assistant Secretary for Planning and Evaluation.
Assari, S. 2018. Diminished economic return of socioeconomic status for black families. Social Sciences 7(5):74.
Assari, S., A. Thomas, C. H. Caldwell, and R. B. Mincy. 2018. Blacks diminished health return of family structure and socioeconomic status; 15 years of follow-up of a national urban sample of youth. Journal of Urban Health 95:21–35.
Association of Maternal & Child Health Programs. 2016. Opportunities to optimize access to prenatal care through health transformation. Washington, DC: Association of Maternal & Child Health Programs.
ASTHO (Association of State and Territorial Health Officials). 2017. Enhancing health equity in breastfeeding opportunities and outcomes. Issue brief. Arlington, VA: Association of State and Territorial Health Officials.
Auchincloss, A. H., M. S. Mujahid, M. Shen, E. D. Michos, M. C. Whitt-Glover, and A. V. Diez Roux. 2013. Neighborhood health-promoting resources and obesity risk (the Multi-ethnic Study of Atherosclerosis). Obesity 21(3):621–628.
Aviram, A., M. Hod, and Y. Yogev. 2011. Maternal obesity: Implications for pregnancy outcome and long-term risks—a link to maternal nutrition. International Journal of Gynecology & Obstetrics 115:S6–S10.
Bachega, H. 2018. Separation of migrant families: What other countries do. BBC News, https://www.bbc.com/news/world-us-canada-44374756 (accessed April 23, 2019).
Bachman, R., H. Zaykowski, R. Kallmyer, M. Poteyeva, and C. Lanier. 2008. Violence against American Indian and Alaska Native women and the criminal justice response: What is known. Washington, DC: U.S. Department of Justice, Office of Justice Programs, National Institute of Justice.
Bailey, Z. D., N. Krieger, M. Agenor, J. Graves, N. Linos, and M. T. Bassett. 2017. Structural racism and health inequities in the USA: Evidence and interventions. The Lancet 389(10077):1453–1463.
Barnett, S., M. Carolan, and D. Johns. 2013. Equity and excellence: African-American children’s access to quality preschool. New Brunswick, NJ: Center on Enhancing Early Learning Outcomes.
Barnett, W. S., and A. H. Friedman-Krauss. 2016. State(s) of Head Start. New Brunswick, NJ: National Institute for Early Education Research.
Beck, A. F., B. Huang, R. Chundur, and R. S. Kahn. 2014. Housing code violation density associated with emergency department and hospital use by children with asthma. Health Affairs 33(11):1993–2002.
Becker, G. S., and N. Tomes. 1986. Human capital and the rise and fall of families. Journal of Labor Economics 4:S1–S39.
Beckhaus, A. A., L. Garcia-Marcos, E. Forno, R. M. Pacheco-Gonzalez, J. C. Celedón, and J. A. Castro-Rodriguez. 2015. Maternal nutrition during pregnancy and risk of asthma, wheeze, and atopic diseases during childhood: A systematic review and meta-analysis. Allergy 70(12):1588–1604.
Behnia, F., M. Peltier, D. Getahun, C. Watson, G. Saade, and R. Menon. 2016. High bisphenol A (BPA) concentration in the maternal, but not fetal, compartment increases the risk of spontaneous preterm delivery. Journal of Maternal-Fetal and Neonatal Medicine 29(22):3583–3589.
Bellinger, D. C., F. Trachtenberg, A. Zhang, M. Tavares, D. Daniel, and S. McKinlay. 2008. Dental amalgam and psychosocial status: The New England Children’s Amalgam Trial. Journal of Dental Research 87(5):470–474.
Ben-Schlomo, Y., and D. Kuh. 2002. A life course approach to chronic disease epidemiology: Conceptual models, empirical challenges and interdisciplinary perspectives. International Journal of Epidemiology 31(2):285–293.
Ben-Schlomo, Y., G. Mishra, and D. Kuh. 2014. Life course epidemiology, 1521–1549. In Handbook of epidemiology, edited by W. Ahrens and I. Pigeot. New York: Springer.
Berger, L. M., S. A. Font, K. S. Slack, and J. Waldfogel. 2017. Income and child maltreatment in unmarried families: Evidence from the Earned Income Tax Credit. Review of Economics of the Household 15(4):1345–1372.
Bethell, C., C. Reuland, E. Schor, M. Abrahms, and N. Halfon. 2011. Rates of parent-centered developmental screening: Disparities and links to services access. Pediatrics 128(1):146–155.
Beyerlein, A., and R. von Kries. 2011. Breastfeeding and body composition in children: Will there ever be conclusive empirical evidence for a protective effect against overweight? American Journal of Clinical Nutrition 94(6 Suppl):1772s–1775s.
Beyers, J. M., J. E. Bates, G. S. Pettit, and K. A. Dodge. 2003. Neighborhood structure, parenting processes, and the development of youths’ externalizing behaviors: A multilevel analysis. American Journal of Community Psychology 31(1–2):35–53.
Bhaskar, R., and B. O’Hara. 2017. Indian health service coverage among American Indians and Alaska Natives in federal tribal areas. Journal of Health Care for the Poor and Underserved 28(4):1361.
Bingham, D., N. Strauss, and F. Coeytaux. 2011. Maternal mortality in the United States: A human rights failure. Contraception 83(3):189–193.
Björkenstam, E., B. Burström, L. Brännström, B. Vinnerljung, C. Björkenstam, and A. R. Pebley. 2015. Cumulative exposure to childhood stressors and subsequent psychological distress. An analysis of US panel data. Social Science & Medicine 142:109–117.
Black, L. I., and V. Benson. 2018. Tables of summary health statistics for U.S. children: 2017 National Health Interview Survey. https://www.cdc.gov/nchs/nhis/SHS/tables.htm (accessed May 21, 2019).
Blair, A., N. A. Ross, G. Gariepy, and N. Schmitz. 2014. How do neighborhoods affect depression outcomes? A realist review and a call for the examination of causal pathways. Social Psychiatry and Psychiatric Epidemiology 49(6):873–887.
Blair, C., C. C. Raver, D. Granger, R. Mills-Koonce, and L. Hibel. 2011. Allostasis and allostatic load in the context of poverty in early childhood. Development and Psychopathology 23(3):845–857.
Blumenshine, P., S. Egerter, C. J. Barclay, C. Cubbin, and P. A. Braveman. 2010. Socioeconomic disparities in adverse birth outcomes: A systematic review. American Journal of Preventive Medicine 39(3):263–272.
Borge, T. C., H. Aase, A. L. Brantsaeter, and G. Biele. 2017. The importance of maternal diet quality during pregnancy on cognitive and behavioural outcomes in children: A systematic review and meta-analysis. BMJ Open 7(9):e016777.
Bornehag, C. G., J. Sundell, C. J. Weschler, T. Sigsgaard, B. Lundgren, M. Hasselgren, and L. Hägerhed-Engman. 2004. The association between asthma and allergic symptoms in children and phthalates in house dust: A nested case-control study. Environmental Health Perspectives 112(14):1393–1397.
Bornstein, M. H., and T. Leventhal. 2015. Children in bioecological landscapes of development. In Handbook of child psychology and developmental science, 7th ed. Vol. 4, Ecological settings and processes, edited by R. M. Lerner. Hoboken, NJ: Wiley. Pp. 1–5.
Borra, C., M. Iacovou, and A. Sevilla. 2015. New evidence on breastfeeding and postpartum depression: The importance of understanding women’s intentions. Maternal and Child Health Journal 19(4):897–907.
Bowatte, G., R. Tham, K. J. Allen, D. J. Tan, M. X. Z. Lau, X. Dai, and C. J. Lodge. 2015. Breastfeeding and childhood acute otitis media: A systematic review and meta-analysis. Acta Paediatrica 104(S467):85–95.
Boy, A., and H. M. Salihu. 2004. Intimate partner violence and birth outcomes: A systematic review. International Journal of Fertility and Women’s Medicine 49(4):159–164.
Boyd, A., J. Golding, J. Macleod, D. A. Lawlor, A. Fraser, J. Henderson, L. Molloy, A. Ness, S. Ring, and G. Davey Smith. 2012. Cohort profile: The “children of the 90s”—the index offspring of the Avon Longitudinal Study of Parents and Children. International Journal of Epidemiology 42(1):11–127.
Braun, J. M., G. Muckle, T. Arbuckle, M. F. Bouchard, W. D. Fraser, E. Ouellet, J. R. Seguin, Y. Oulhote, G. M. Webster, and B. P. Lanphear. 2017. Associations of prenatal urinary bisphenol a concentrations with child behaviors and cognitive abilities. Environmental Health Perspectives 125(6):067008.
Braveman, P., J. Acker, E. Arkin, J. Bussel, K. Wehr, and D. Proctor. 2018. Early childhood is critical to health equity. Princeton, NJ: Robert Wood Johnson Foundation.
Bronfenbrenner, U. 1979. Contexts of child rearing: Problems and prospects. American Psychologist 34(10):844–850.
Bronfenbrenner, U., and G. W. Evans. 2000. Developmental science in the 21st century: Emerging questions, theoretical models, research designs and empirical findings. Social Development 9(1):115–125.
Bronfenbrenner, U., and P. A. Morris. 2006. The bioecological model of human development. In Handbook of child psychology and developmental science, 7th ed. Vol. 1, Theory and method, edited by R. M. Lerner. New York: Wiley. Pp. 793–828.
Bronfenbrenner, U., and P. A. Morris. 2007. The bioecological model of human development. Handbook of child psychology. Hoboken, NJ: John Wiley & Sons, Inc.
Brooks-Gunn, J., and G. J. Duncan. 1997. The effects of poverty on children. The Future of Children 7(2):55–71.
Brunton, P. J. 2013. Effects of maternal exposure to social stress during pregnancy: Consequences for mother and offspring. Reproduction 146(5):R175–R189.
Buckner, J. 2008. Understanding the impact of homelessness on children: Challenges and future research directions. American Behavioral Scientist 51(6):721–736.
Buka, S. L., R. T. Brennan, J. W. Rich-Edwards, S. W. Raudenbush, and F. Earls. 2003. Neighborhood support and the birth weight of urban infants. American Journal of Epidemiology 157(1):1–8.
Bures, R. M. 2003. Childhood residential stability and health at midlife. American Journal of Public Health 93(7):1144–1148.
Burke, N. J., J. L. Hellman, B. G. Scott, C. F. Weems, and V. G. Carrion. 2011. The impact of adverse childhood experiences on an urban pediatric population. Child Abuse & Neglect 35(6):408–413.
Callec, R., E. Perdriolle-Galet, G.-A. Sery, and O. Morel. 2014. Type 2 diabetes in pregnancy: Rates of fetal malformations and level of preconception care. Journal of Obstetrics and Gynaecology 34(7):648–649.
Campbell, F., G. Conti, J. J. Heckman, S. H. Moon, R. Pinto, E. Pungello, and Y. Pan. 2014. Early childhood investments substantially boost adult health. Science 343(6178):1478–1485.
Cancian, M. 2010. The effect of family income on risk of child maltreatment. Madison, WI: Institute for Research on Poverty.
Cascio, E. U., and D. W. Schanzenbach. 2016. Expanding preschool access for disadvanaged children. Washington, DC: The Brookings Institution.
Casey, J. A., D. A. Savitz, S. G. Rasmussen, E. L. Ogburn, J. Pollak, D. G. Mercer, and B. S. Schwartz. 2016. Unconventional natural gas development and birth outcomes in Pennsylvania, USA. Epidemiology 27(2):163–172.
CDC (Centers for Disease Control and Prevention). 2014. Essentials for childhood: Steps to create safe, stable, and nurturing relationships and environments. Atlanta, GA: Centers for Disease Control and Prevention.
CDC. 2017. Leading causes of death. https://www.cdc.gov/nchs/fastats/leading-causes-ofdeath.htm (accessed April 23, 2019).
CDC. 2018a. Breastfeeding report card, United States, 2018. https://www.cdc.gov/breastfeeding/data/reportcard.htm (accessed April 18, 2019).
CDC. 2018b. Table 4-1 Current Asthma Prevalence Percents by Age, United States: National Health Interview Survey, 2016. https://www.cdc.gov/asthma/nhis/2016/table4-1.htm (accessed July 15, 2019).
CDC. 2019. Preventing child abuse & neglect. https://www.cdc.gov/violenceprevention/pdf/CAN-factsheet.pdf (accessed April 22, 2019).
CDC. n.d.-a. About the CDC-Kaiser ACE study. https://www.cdc.gov/violenceprevention/acestudy/about.html (accessed July 18, 2018).
CDC. n.d.-b. Breastfeeding practices and policies. https://www.cdc.gov/nccdphp/dnpao/state-local-programs/health-equity-guide/pdf/health-equity-guide/Health-EquityGuide-sect-3-5.pdf (accessed July 13, 2019).
Center for Youth Wellness. 2014. Data report: A hidden crisis. Findings on adverse childhood experiences in California. https://centerforyouthwellness.org/wp-content/themes/cyw/build/img/building-a-movement/hidden-crisis.pdf (accessed July 15, 2019).
Center on the Developing Child at Harvard University. 2009. Maternal depression can undermine the development of young children: Working paper no. 8. Cambridge, MA: Harvard University.
Cervantes, W., R. Ullrich, and H. Matthews. 2018. Our children’s fear: Immigration policy’s effects on young children. Washington, DC: Center for Law and Social Policy.
Chang, A. 2018. The data proves that school segregation is getting worse. Vox, https://www.vox.com/2018/3/5/17080218/school-segregation-getting-worse-data (accessed April 22, 2019).
ChangeLab Solutions. 2017. Closing the water quality gap: Using policy to improve drinking water in federally-unregulated water systems. Oakland, CA: ChangeLab Solutions.
Chapman, D. J., and R. Pérez-Escamilla. 2012. Breastfeeding among minority women: Moving from risk factors to interventions. Advances in Nutrition 3:95–104.
Chen, E., A. D. Martin, and K. A. Matthews. 2006. Understanding health disparities: The role of race and socioeconomic status in children’s health. American Journal of Public Health 96(4):702–708.
Chetty, R., M. Stepner, S. Abraham, S. Lin, B. Scuderi, N. Turner, A. Bergeron, and D. Cutler. 2016. The association between income and life expectancy in the United States, 2001–2014. JAMA 315(16):1750–1766.
Chetty, R., N. Hendren, M. R. Jones, and S. R. Porter. 2018. Race and economic opportunity in the United States: An intergenerational perspective. NBER working paper no. 24441. National Bureau of Economic Research.
Chevrier, J., R. B. Gunier, A. Bradman, N. T. Holland, A. M. Calafat, B. Eskenazi, and K. G. Harley. 2013. Maternal urinary bisphenol A during pregnancy and maternal and neonatal thyroid function in the Chamacos Study. Environmental Health Perspectives 121(1):138–144.
Chien, N. 2017. Factsheet: Estimates of child care eligibility & receipt for fiscal year 2013. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation.
Child Trends. 2015. Parental education. Indicators of child and youth well-being. Bethesda, MD: Child Trends.
Child Trends DataBank. 2018. High school dropout rates. https://www.childtrends.org/indicators/high-school-dropout-rates (accessed April 22, 2019).
Chou, R. S., and J. R. Feagin. 2015. The myth of the model minority: Asian Americans facing racism. Boulder, CO: Paradigm Publishers.
Chowdhury, R., B. Sinha, M. J. Sankar, S. Taneja, N. Bhandari, N. Rollins, R. Bahl, and J. Martines. 2015. Breastfeeding and maternal health outcomes: A systematic review and meta-analysis. Acta Paediatrica 104(467):96–113.
Christiaens, I., K. Hegadoren, and D. M. Olson. 2015. Adverse childhood experiences are associated with spontaneous preterm birth: A case-control study. BMC Medicine 13:124.
Christine, P. J., A. H. Auchincloss, A. G. Bertoni, M. R. Carnethon, B. N. Sanchez, K. Moore, S. D. Adar, T. B. Horwich, K. E. Watson, and A. V. Diez Roux. 2015. Longitudinal associations between neighborhood physical and social environments and incident type 2 diabetes mellitus: The Multi-Ethnic Study of Atherosclerosis (MESA). JAMA Internal Medicine 175(8):1311–1320.
Chuang, C. H., D. L. Velott, and C. S. Weisman. 2010. Exploring knowledge and attitudes related to pregnancy and preconception health in women with chronic medical conditions. Maternal and Child Health Journal 14(5):713–719.
Cicchetti, D., and E. D. Handley. 2017. Methylation of the glucocorticoid receptor gene, nuclear receptor subfamily 3, group c, member 1 (NR3C1), in maltreated and nonmaltreated children: Associations with behavioral undercontrol, emotional lability/negativity, and externalizing and internalizing symptoms. Development and Psychopathology 29(5):1795–1806.
Cobb, L. K., L. J. Appel, M. Franco, J. C. Jones-Smith, A. Nur, and C. A. Anderson. 2015. The relationship of the local food environment with obesity: A systematic review of methods, study quality, and results. Obesity 23(7):1331–1344.
Cobb, N., D. Espey, and J. King. 2014. Health behaviors and risk factors among American Indians and Alaska Natives, 2000–2010. American Journal of Public Health 104(S3):S481–S489.
Cohen, S., and T. A. Wills. 1985. Stress, social support, and the buffering hypothesis. Psychological Bulletin 98(2):310–357.
Cohen-Cline, H., S. A. A. Beresford, W. E. Barrington, R. L. Matsueda, J. Wakefield, and G. E. Duncan. 2018. Associations between neighbourhood characteristics and depression: A twin study. Journal of Epidemiology and Community Health 72(3):202–207.
Coleman-Jensen, A., M. P. Rabbitt, C. A. Gregory, and A. Singh. 2017. Household food security in the United States in 2016, ERR-237. Washington, DC: U.S. Department of Agriculture, Economic Research Service.
Coley, R. L., T. Leventhal, A. D. Lynch, and M. Kull. 2013. Relations between housing characteristics and the well-being of low-income children and adolescents. Developmental Psychology 49(9):1775–1789.
Collins, N. L., C. Dunkel-Schetter, M. Lobel, and S. C. Scrimshaw. 1993. Social support in pregnancy: Psychosocial correlates of birth outcomes and postpartum depression. Journal of Personality and Social Psychology 65(6):1243–1258.
Conners, N. A., R. H. Bradley, L. W. Mansell, J. Y. Liu, T. J. Roberts, K. Burgdorf, and J. M. Herrell. 2004. Children of mothers with serious substance abuse problems: An accumulation of risks. American Journal of Drug and Alcohol Abuse 30(1):85–100.
Corcoran, L., K. Steinley, and S. Grady. 2019. Early childhood program participation, results from the national household education surveys program of 2016. Washington, DC: U.S. Department of Education, National Center for Education Statistics, Institute of Education Sciences.
Coughlin, R., E. Kushman, G. Copeland, and M. Wilson. 2013. Pregnancy and birth outcome improvements for American Indians in the healthy start project of the inter-tribal council of Michigan, 1998–2008. Maternal and Child Health Journal 17(6):1005–1015.
Cox, C., T. W. Clarkson, D. O. Marsh, L. Amin-Zaki, S. Tikriti, and G. G. Myers. 1989. Dose-response analysis of infants prenatally exposed to methyl mercury: An application of a single compartment model to single-strand hair analysis. Environmental Research 49(2):318–332.
Cox, R. G., L. Zhang, M. E. Zotti, and J. Graham. 2011. Prenatal care utilization in Mississippi: Racial disparities and implications for unfavorable birth outcomes. Maternal and Child Health Journal 15(7):931–942.
Crowley, S. 2003. The affordable housing crisis: Residential mobility of poor families and school mobility of poor children. Journal of Negro Education 72(1):22–38.
Currie, J., and R. Walker. 2011. Traffic congestion and infant health: Evidence from E-ZPass American Economic Journal: Applied Economics 3(1):65–90.
Cusick, S. E., and M. K. Georgieff. 2016. The role of nutrition in brain development: The golden opportunity of the “first 1000 days.” The Journal of Pediatrics 175:16–21.
Cutler, D. M., and A. Lleras-Muney. 2006. Education and health: Evaluating theories and evidence. National Bureau of Economic Research Working Paper no. 12352. https://www.nber.org/papers/w12352 (accessed February 10, 2019).
Cutts, D. B., S. Coleman, M. M. Black, M. M. Chilton, J. T. Cook, S. E. de Cuba, T. C. Heeren, A. Meyers, M. Sandel, P. H. Casey, and D. A. Frank. 2015. Homelessness during pregnancy: A unique, time-dependent risk factor of birth outcomes. Maternal and Child Health Journal 19(6):1276–1283.
da Silva Lopes, K., E. Ota, P. Shakya, A. Dagvadorj, O. O. Balogun, J. P. Pena-Rosas, L. M. De-Regil, and R. Mori. 2017. Effects of nutrition interventions during pregnancy on low birth weight: An overview of systematic reviews. BMJ Global Health 2(3):e000389.
Danese, A., T. E. Moffitt, H. Harrington, B. J. Milne, G. Polanczyk, and C. M. Pariante. 2009. Adverse childhood experiences and adult risk factors for age-related disease: Depression, inflammation, and clustering of metabolic risk markers. Archives of Pediatric & Adolescent Medicine 163(12):1135–1143.
Data Resource Center for Child and Adolescent Health. 2019. Explore the data > NSCH interactive data query (2016–present) > data search results. https://www.childhealthdata.org/browse/survey/results?q=5554&r=1&g=652 (accessed April 5, 2019).
Davis, R. 2016. 38th annual report to Congress on the implementation of the Individuals with Disabilities Education Act, 2016. Washington, DC: U.S. Department of Education.
de Brey, C., L. Musu, J. McFarland, S. Wilkinson-Flicker, M. Diliberti, A. Zhang, C. Branstetter, and X. Wang. 2019. Status and trends in the education of racial and ethnic groups 2018. NCES 2019-038. Washington, DC: U.S. Department of Education, National Center for Education Statistics.
Desmond, M., and T. Shollenberger. 2015. Forced displacement from rental housing: Prevalence and neighborhood consequences. Demography 52(5):1751–1772.
Dewey, K. G. 2003. Is breastfeeding protective against child obesity? Journal of Human Lactation 19(1):9–18.
Di Renzo, G. C., J. A. Conry, J. Blake, M. S. Defrancesco, N. Denicola, J. N. Martin, K. A. McCue, D. Richmond, A. Shah, P. Sutton, T. J. Woodruff, S. Z. Van Der Poel, and L. C. Giudice. 2015. International Federation of Gynecology and Obstetrics opinion on reproductive health impacts of exposure to toxic environmental chemicals. International Journal of Gynecology & Obstetrics 131(3):219–225.
Diamanti-Kandarakis, E., J.-P. Bourguignon, L. C. Giudice, R. Hauser, G. S. Prins, A. M. Soto, R. T. Zoeller, and A. C. Gore. 2009. Endocrine-disrupting chemicals: An Endocrine Society scientific statement. Endocrine Reviews 30(4):293.
Dias, C. C., and B. Figueiredo. 2015. Breastfeeding and depression: A systematic review of the literature. Journal of Affective Disorders 171:142–154.
Dohrenwend, B. P. 2006. Inventorying stressful life events as risk factors for psychopathology: Toward resolution of the problem of intracategory variability. Psychological Bulletin 132(3):477–495.
Dohrenwend, B. P., I. Levav, P. E. Shrout, S. Schwartz, G. Naveh, B. G. Link, A. E. Skodol, and A. Stueve. 1992. Socioeconomic status and psychiatric disorders: The causation-selection issue. Science 255(5047):946–952.
Donohue, K. M., R. L. Miller, M. S. Perzanowski, A. C. Just, L. A. Hoepner, S. Arunajadai, S. Canfield, D. Resnick, A. M. Calafat, F. P. Perera, and R. M. Whyatt. 2013. Prenatal and postnatal bisphenol A exposure and asthma development among inner-city children. Journal of Allergy and Clinical Immunology 131(3):736–742.
Dorfman, H., M. Srinath, K. Rockhill, and C. Hogue. 2015. The association between diabetes mellitus among American Indian/Alaska Native populations with preterm birth in eight US states from 2004–2011. Maternal and Child Health Journal 19(11):2419–2428.
Drury, S. S., L. Scaramella, and C. H. Zeanah. 2016. The neurobiological impact of postpartum maternal depression: Prevention and intervention approaches. Child and Adolescent Psychiatric Clinics of North America 25(2):179–200.
Dubow, E. F., P. Boxer, and L. R. Huesmann. 2009. Long-term effects of parents’ education on children’s educational and occupational success: Mediation by family interactions, child aggression, and teenage aspirations. Merrill-Palmer Quarterly 55(3):224–249.
Duncan, G. J. 2012. Give us this day our daily breadth. Child Development 83(1):6–15.
Duncan, G. J., J. Brooks-Gunn, and P. K. Klebanov. 1994. Economic deprivation and early childhood development. Child Development 65(2 Spec No):296–318.
Duncan, G. J., W. J. Yeung, J. Brooks-Gunn, and J. R. Smith. 1998. How much does childhood poverty affect the life chances of children? American Sociological Review 63(3):406–423.
Duncan, G. J., P. A. Morris, and C. Rodrigues. 2011. Does money really matter? Estimating impacts of family income on young children’s achievement with data from random-assignment experiments. Developmental Psychology 47(5):1263–1279.
Dunn, E. C., T. W. Soare, M. R. Raffeld, D. S. Busso, K. M. Crawford, K. A. Davis, V. A. Fisher, N. Slopen, A. D. Smith, and H. Tiemeier. 2018. What life course theoretical models best explain the relationship between exposure to childhood adversity and psychopathology symptoms: Recency, accumulation, or sensitive periods? Psychological Medicine 48(15):2562–2572.
EdBuild. 2019. Nonwhite school districts get $23 billion less than white districts despite serving the same number of students. https://edbuild.org/content/23-billion/full-report.pdf (accessed July 14, 2019).
Egerter, S., C. Barclay, R. Grossman-Kahn, and P. A. Braveman. 2011a. Violence, social disadvantage and health. Princeton, NJ: Robert Wood Johnson Foundation.
Egerter, S., P. Braveman, T. Sadegh-Nobari, R. Grossman-Kahn, and M. Dekker. 2011b. Education and health. Princeton, NJ: Robert Wood Johnson Foundation.
Elder, T. E., J. H. Goddeeris, and S. J. Haider. 2016. Racial and ethnic infant mortality gaps and the role of socio-economic status. Labour Economics 43:42–54.
Elliott, P., D. Briggs, S. Morris, C. de Hoogh, C. Hurt, T. K. Jensen, I. Maitland, S. Richardson, J. Wakefield, and L. Jarup. 2001. Risk of adverse birth outcomes in populations living near landfill sites. BMJ 323(7309):363–368.
Evans, G. W. 2004. The environment of childhood poverty. American Psychologist 59(2):77–92.
Evans, G. W., H. N. Ricciuti, S. Hope, I. Schoon, R. H. Bradley, R. F. Corwyn, and C. Hazan. 2010. Crowding and cognitive development: The mediating role of maternal responsiveness among 36-month-old children. Environment and Behavior 42(1):135–148.
Evans, G. W., D. Li, and S. Sepanski Whipple. 2013. Cumulative risk and child development. Psychological Bulletin 139(6):1342–1396.
Fan, Y., K. V. Das, and Q. Chen. 2011. Neighborhood green, social support, physical activity, and stress: Assessing the cumulative impact. Health and Place 17(6):1202–1211.
Fang, X., D. S. Brown, C. S. Florence, and J. A. Mercy. 2012. The economic burden of child maltreatment in the United States and implications for prevention. Child Abuse & Neglect 36(2):156–165.
Farley, T. A., K. Mason, J. Rice, J. D. Habel, R. Scribner, and D. A. Cohen. 2006. The relationship between the neighbourhood environment and adverse birth outcomes. Paediatric and Perinatal Epidemiology 20(3):188–200.
Felitti, V. J., R. F. Anda, D. Nordenberg, D. F. Williamson, A. M. Spitz, V. Edwards, M. P. Koss, and J. S. Marks. 1998. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine 14(4):245–258.
Fenelon, A., N. Slopen, M. Boudreaux, and S. J. Newman. 2018. The impact of housing assistance on the mental health of children in the United States. Journal of Health and Social Behavior 59(3):447–463.
Feng, J., T. A. Glass, F. C. Curriero, W. F. Stewart, and B. S. Schwartz. 2010. The built environment and obesity: A systematic review of the epidemiologic evidence. Health and Place 16(2):175–190.
Ferguson, K. K., T. F. McElrath, and J. D. Meeker. 2014. Environmental phthalate exposure and preterm birth. JAMA Pediatrics 168(1):61–67.
Ferguson, K. K., J. D. Meeker, D. E. Cantonwine, B. Mukherjee, G. G. Pace, D. Weller, and T. F. McElrath. 2018. Environmental phenol associations with ultrasound and delivery measures of fetal growth. Environment International 112:243–250.
Filindra, A., D. Blanding, and C. García Coll. 2011. The power of context: State-level policies and politics and the educational performance of the children of immigrants in the United States. Harvard Educational Review 81(3):407–438.
Finegood, E. D., J. R. D. Rarick, and C. Blair. 2017. Exploring longitudinal associations between neighborhood disadvantage and cortisol levels in early childhood. Development and Psychopathology 29(5):1649–1662.
Finkelhor, D., R. K. Ormrod, and H. A. Turner. 2007. Re-victimization patterns in a national longitudinal sample of children and youth. Child Abuse & Neglect 31:479–502.
Finkelhor, D., R. K. Ormrod, and H. A. Turner. 2009. Lifetime assessment of poly-victimization in a national sample of children and youth. Child Abuse & Neglect 33:403–411.
Finkelhor, D., H. A. Turner, A. Shattuck, and S. L. Hamby. 2015. Prevalence of childhood exposure to violence, crime, and abuse: Results from the national survey of children’s exposure to violence. JAMA Pediatrics 169(8):746–754.
Fleisch, A. F., H. Luttmann-Gibson, W. Perng, S. L. Rifas-Shiman, B. A. Coull, I. Kloog, P. Koutrakis, J. D. Schwartz, A. Zanobetti, C. S. Mantzoros, M. W. Gillman, D. R. Gold, and E. Oken. 2017. Prenatal and early life exposure to traffic pollution and cardiometabolic health in childhood. Pediatric Obesity 12(1):48–57.
Fone, D., F. Dunstan, K. Lloyd, G. Williams, J. Watkins, and S. Palmer. 2007. Does social cohesion modify the association between area income deprivation and mental health? A multilevel analysis. International Journal of Epidemiology 36(2):338–345.
Fortin, M., G. Muckle, E. Anassour-Laouan-Sidi, S. W. Jacobson, J. L. Jacobson, and R. E. Belanger. 2016. Trajectories of alcohol use and binge drinking among pregnant Inuit women. Alcohol and Alcoholism 51(3):339–346.
Fortson, B. L., J. Klevens, M. T. Merrick, L. K. Gilbert, and S. P. Alexander. 2016. Preventing child abuse and neglect: A technical package for policy, norm, and programmatic activities. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention.
Fraser, A., C. Macdonald-Wallis, K. Tilling, A. Boyd, J. Golding, G. Davey Smith, J. Henderson, J. Macleod, L. Molloy, A. Ness, S. Ring, S. M. Nelson, and D. A. Lawlor. 2012. Cohort profile: The Avon Longitudinal Study of Parents and Children: ALSPAC mothers cohort. International Journal of Epidemiology 42(1):97–110.
Friedman-Krauss, A. H., W. S. Barnett, G. G. Weisenfeld, R. Kasmin, N. DiCrecchio, and M. Horowitz. 2018. The state of preschool 2017. State preschool yearbook. New Brunswick, NJ: National Institute for Early Education Research.
García Coll, C., F. Patton, A. K. Marks, R. Dimitrova, H. Yang, G. Suarez-Aviles, and A. Batchelor. 2012. Understanding the immigrant paradox in youth: Developmental and contextual considerations. In Realizing the potential of immigrant youth, edited by A. S. Masten, K. Liebkind, and D. J. Hernandez. New York: Cambridge University Press.
Garner, A. S., and J. P. Shonkoff. 2012. Early childhood adversity, toxic stress, and the role of the pediatrician: Translating developmental science into lifelong health. Pediatrics 129(1):e224–e231.
Gascon, M., D. Valvi, J. Forns, M. Casas, D. Martinez, J. Julvez, N. Monfort, R. Ventura, J. Sunyer, and M. Vrijheid. 2015. Prenatal exposure to phthalates and neuropsychological development during childhood. International Journal of Hygiene and Environmental Health 218(6):550–558.
Genovesi, A. L., B. Hastings, E. Edgerton, and L. Olson. 2014. Pediatric emergency care capabilities of Indian health service emergency medical service agencies serving American Indians/Alaska Natives in rural and frontier. Rural and Remote Health 14(2):2688.
Georgieff, M. K., K. E. Brunette, and P. V. Tran. 2015. Early life nutrition and neural plasticity. Development and Psychopathology 27(2):411–423.
Gilbert, R., A. Kemp, J. Thoburn, P. Sidelbotham, L. Radford, and D. Glaser. 2009. Recognising and responding to child maltreatment. The Lancet 373:167–180.
Giordano, G. N., H. Ohlsson, K. S. Kendler, K. Sundquist, and J. Sundquist. 2014. Unexpected adverse childhood experiences and subsequent drug use disorder: A Swedish population study (1995–2011). Addiction 109(7):1119–1127.
Giudice, L., T. Woodruff, and J. Conry. 2017. Reproductive and developmental environmental health. Obstetrics, Gynaecology & Reproductive Medicine 27(3):99–101.
Giurgescu, C., B. L. McFarlin, J. Lomax, C. Craddock, and A. Albrecht. 2011. Racial discrimination and the black-white gap in adverse birth outcomes: A review. Journal of Midwifery & Women’s Health 56(4):362–370.
Goodman, S. H., and J. Garber. 2017. Evidence-based interventions for depressed mothers and their young children. Child Development 88(2):368–377.
Goodman, S. H., M. H. Rouse, A. M. Connell, M. R. Broth, C. M. Hall, and D. Heyward. 2011. Maternal depression and child psychopathology: A meta-analytic review. Clinical Child and Family Psychology Review 14(1):1–27.
Goossens, J. 2018. Barriers and facilitators to the provision of preconception care by healthcare providers: A systematic review. International Journal of Nursing Studies 87C:113–130.
Gore, A., V. A. Chappell, S. Fenton, J. Flaws, A. Nadal, G. Prins, J. Toppari, and R. Zoeller. 2015. Executive summary to EDC-2: The Endocrine Society’s second scientific statement on endocrine-disrupting chemicals. Endocrine Reviews 36(6):593–602.
Greaves, L., A. P. Pederson, and N. Poole. 2014. Making it better: Gender-transformative health promotion. Toronto, Ontario: Canadian Scholars’ Press.
Guess, T. J. 2006. The social construction of whiteness: Racism by intent, racism by consequence. Critical Sociology 32(4):649–673.
Gutierrez-Galve, L., A. Stein, L. Hanington, J. Heron, and P. Ramchandani. 2015. Paternal depression in the postnatal period and child development: Mediators and moderators. Pediatrics 135(2):e339–e347.
Ha, S., H. Hu, J. Roth, H. Kan, and X. Xu. 2015. Associations between residential proximity to power plants and adverse birth outcomes. American Journal of Epidemiology 182(3):215–224.
Hahn, R. A., W. S. Barnett, J. A. Knopf, B. I. Truman, R. L. Johnson, J. E. Fielding, C. Muntaner, C. P. Jones, M. T. Fullilove, and P. C. Hunt. 2016. Early childhood education to promote health equity: A community guide systematic review. Journal of Public Health Management and Practice 22(5):e1–e8.
Hahn-Holbrook, J., M. G. Haselton, C. Dunkel Schetter, and L. M. Glynn. 2013. Does breastfeeding offer protection against maternal depressive symptomatology?: A prospective study from pregnancy to 2 years after birth. Archives of Women’s Mental Health 16(5):411–422.
Harder, T., R. Bergmann, G. Kallischnigg, and A. Plagemann. 2005. Duration of breastfeeding and risk of overweight: A meta-analysis. American Journal of Epidemiology 162(5):397–403.
Harkness, J., and S. J. Newman. 2005. Housing affordability and children’s well-being: Evidence from the national survey of America’s families. Housing Policy Debate 16(2):223–255.
Harley, K. G., R. B. Gunier, K. Kogut, C. Johnson, A. Bradman, A. M. Calafat, and B. Eskenazi. 2013. Prenatal and early childhood bisphenol A concentrations and behavior in school-aged children. Environmental Research 126:43–50.
Harrington, J., J. Lutomski, M. Molcho, and I. J. Perry. 2009. Food poverty and dietary quality: Is there a relationship? Journal of Epidemiology and Community Health 63(Suppl 2):16.
Harris, M. H., D. R. Gold, S. L. Rifas-Shiman, S. J. Melly, A. Zanobetti, B. A. Coull, J. D. Schwartz, A. Gryparis, I. Kloog, P. Koutrakis, D. C. Bellinger, M. B. Belfort, T. F. Webster, R. F. White, S. K. Sagiv, and E. Oken. 2016. Prenatal and childhood traffic-related air pollution exposure and childhood executive function and behavior. Neurotoxicology & Teratology 57:60–70.
Hawkinson, L. E., A. S. Griffen, N. Dong, and R. A. Maynard. 2013. The relationship between child care subsidies and children’s cognitive development. Early Childhood Research Quarterly 28(2):388–404.
Heaman, M. I., P. J. Martens, M. D. Brownell, M. J. Chartier, K. R. Thiessen, S. A. Derksen, and M. E. Helewa. 2018. Inequities in utilization of prenatal care: A population-based study in the Canadian province of Manitoba. BMC Pregnancy Childbirth 18(1):430.
Heard-Garris, N. J., M. Cale, L. Camaj, M. C. Hamati, and T. P. Dominguez. 2018. Transmitting trauma: A systematic review of vicarious racism and child health. Social Science & Medicine 199:230–240.
Heckman, J. J., J. E. Humphries, and G. Veramendi. 2018. Returns to education: The causal effects of education on earnings, health, and smoking. Journal of Political Economy 126(Suppl 1):S197–S246.
Hemsing, N., L. Greaves, and N. Poole. 2017. Preconception health care interventions: A scoping review. Sexual and Reproductive Healthcare 14:24–32.
Henry, M., R. Watt, L. Rosenthal, and A. Shivji. 2017. The 2017 Annual Homeless Assessment Report (AHAR) to Congress. Washington, DC: U.S. Department of Housing and Urban Development.
Herbst, C. M., and E. Tekin. 2010. Child care subsidies and child development. Economics of Education Review 29(4):618–638.
Hernandez, D. J. 2012. Double jeopardy: How third-grade reading skills and poverty influence high school graduation. Baltimore, MD: The Annie E. Casey Foundation.
HHS (U.S. Department of Health and Human Services). 2011. The Surgeon General’s call to action to support breastfeeding. Rockville, MD: Office of the Surgeon General, Centers for Disease Control and Prevention, Office on Women’s Health.
HHS. 2019. Child maltreatment 2017. Washington, DC: U.S. Department of Health and Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau.
HHS Office of Inspector General. 2019. Separated children placed in office of refugee resettlement care. Washington, DC: U.S. Department of Health and Human Services.
Hibbard, R. A., L. W. Desch, and the Committee on Child Abuse and Neglect, and Council on Children with Disabilities. 2007. Maltreatment of children with disabilities. Pediatrics 119(5):1018–1025.
Hicks, A. L., M. S. Handcock, N. Sastry, and A. R. Pebley. 2018. Sequential neighborhood effects: The effect of long-term exposure to concentrated disadvantage on children’s reading and math test scores. Demography 55(1):1–31.
Hodgkinson, S., L. Godoy, L. S. Beers, and A. Lewin. 2017. Improving mental health access for low-income children and families in the primary care setting. Pediatrics 139(1):e20151175.
Hoffman, S., and M. C. Hatch. 1996. Stress, social support and pregnancy outcome: A reassessment based on recent research. Paediatric and Perinatal Epidemiology 10(4):380–405.
Hopenhayn, C., C. Ferreccio, S. R. Browning, B. Huang, C. Peralta, H. Gibb, and I. Hertz-Picciotto. 2003. Arsenic exposure from drinking water and birth weight. Epidemiology 14(5):593–602.
Horta, B. L., C. Loret de Mola, and C. G. Victora. 2015. Long-term consequences of breastfeeding on cholesterol, obesity, systolic blood pressure and type 2 diabetes: A systematic review and meta-analysis. Acta Paediatrica 104(467):30–37.
Hughes, K., M. A. Bellis, K. A. Hardcastle, D. Sethi, A. Butchart, C. Mikton, L. Jones, and M. P. Dunne. 2017. The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. Lancet Public Health 2(8):e356–e366.
Hung, P., K. B. Kozhimannil, M. Casey, and C. Henning-Smith. 2017. State variability in access to hospital-based obstetric services in rural U.S. counties. Minneapolis, MN: University of Minnesota Rural Health Research Center.
Hussein, N., J. Kai, and N. Qureshi. 2016. The effects of preconception interventions on improving reproductive health and pregnancy outcomes in primary care: A systematic review. European Journal of General Practice 22(1):42–52.
Hutchinson, R. N., M. A. Putt, L. T. Dean, J. A. Long, C. A. Montagnet, and K. Armstrong. 2009. Neighborhood racial composition, social capital and black all-cause mortality in Philadelphia. Social Science & Medicine 68(10):1859–1865.
Hwang, M., A. Shrestha, S. Yazzie, and M. Jackson. 2013. Preterm birth among American Indian/Alaskan Natives in Washington and Montana: Comparison with non-Hispanic whites. Maternal and Child Health Journal 17(10):1908–1912.
Iliopoulou, I. M. S. M., P. Kanavidis, I. Matsoukis, and E. Petridou. 2012. Pregnancy outcomes linked to intimate partner violence: A systematic review. Injury Prevention 18(Suppl 1):A184.
IOM (Institute of Medicine). 1990. Nutrition during pregnancy. Part I: Weight gain, part II: Nutrient supplements. Washington, DC: National Academy Press.
IOM. 2000. Clearing the air: Asthma and indoor air exposures. Washington, DC: National Academy Press.
IOM. 2002. Unequal treatment: Confronting racial and ethnic disparities in health care. Washington, DC: The National Academies Press.
IOM. 2004. Damp indoor spaces and health. Washington, DC: The National Academies Press.
IOM and NRC (National Research Council). 2014. New directions in child abuse and neglect research. Washington, DC: The National Academies Press.
Ip, S., M. Chung, G. Raman, P. Chew, N. Magula, D. DeVine, T. Trikalinos, and J. Lau. 2007. Breastfeeding and maternal and infant health outcomes in developed countries. Evidence Report/Technology Assessment 153:1–186.
Jiang, Y., M. Ekono, and C. Skinner. 2016. Basic facts about low-income children: Children under 18 years. New York: National Center for Children in Poverty, Mailman School of Public Health, Columbia University.
Jim, M., E. Arias, D. Seneca, M. Hoopes, C. Jim, N. Johnson, and C. Wiggins. 2014. Racial misclassification of American Indians and Alaska Natives by Indian Health Service contract health service delivery area. American Journal of Public Health 104(Suppl 3):S295–S302.
Johnson, A., R. Kirk, K. L. Rosenblum, and M. Muzik. 2015. Enhancing breastfeeding rates among African American women: A systematic review of current psychosocial interventions. Breastfeeding Medicine: The Official Journal of the Academy of Breastfeeding Medicine 10:45–62.
Johnson, R. C. 2011. Long-run impacts of school desegregation & school quality. Cambridge, MA: National Bureau of Economic Research.
Johnson, S. B., J. L. Riis, and K. G. Noble. 2016. State of the art review: Poverty and the developing brain. Pediatrics 137(4):e20153075.
Joint Center for Housing Studies of Harvard University. 2017. America’s rental housing 2017. Cambridge, MA: Harvard University.
Joint Center for Housing Studies of Harvard University. 2018. The state of the nation’s housing 2018. Cambridge, MA: Harvard University.
Jokela, M. 2014. Are neighborhood health associations causal? A 10-year prospective cohort study with repeated measurements. American Journal of Epidemiology 180(8):776–784.
Jokela, M. 2015. Does neighbourhood deprivation cause poor health? Within-individual analysis of movers in a prospective cohort study. Journal of Epidemiology and Community Health 69(9):899–904.
Jones, C. P. 2000. Levels of racism: A theoretic framework and a gardener’s tale. American Journal of Public Health 90(8):1212–1215.
Jones, K. M., M. L. Power, J. T. Queenan, and J. Schulkin. 2015. Racial and ethnic disparities in breastfeeding. Breastfeeding Medicine: The Official Journal of the Academy of Breastfeeding Medicine 10(4):186–196.
Just, A. C., R. M. Whyatt, R. L. Miller, A. G. Rundle, Q. Chen, A. M. Calafat, A. Divjan, M. J. Rosa, H. Zhang, F. P. Perera, I. F. Goldstein, and M. S. Perzanowski. 2012. Children’s urinary phthalate metabolites and fractional exhaled nitric oxide in an urban cohort. American Journal of Respiratory and Critical Care Medicine 186(9):830–837.
Kainz, K., and Y. Pan. 2014. Segregated school effects on first grade reading gains: Using propensity score matching to disentangle effects for African-American, Latino, and European-American students. EARCHI Early Childhood Research Quarterly 29(4):531–537.
Kaiser, P., A. V. Diez Roux, M. Mujahid, M. Carnethon, A. Bertoni, S. D. Adar, S. Shea, R. McClelland, and L. Lisabeth. 2016. Neighborhood environments and incident hypertension in the Multi-ethnic Study of Atherosclerosis. American Journal of Epidemiology 183(11):988–997.
Kaiser Family Foundation. 2017. Health insurance coverage of children 0–18. https://www.kff.org/other/state-indicator/children-0-18/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Uninsured%22,%22sort%22:%22desc%22%7D (accessed April 12, 2019).
Kalter, H. 2003. Teratology in the 20th century: Environmental causes of congenital malformations in humans and how they were established. Neurotoxicology and Teratology 25(2):131–282.
Kapaya, H., E. Mercer, F. Boffey, G. Jones, C. Mitchell, and D. Anumba. 2015. Deprivation and poor psychosocial support are key determinants of late antenatal presentation and poor fetal outcomes—a combined retrospective and prospective study. BMC Pregnancy Childbirth 15:309.
Kaufman, J. S., N. Dole, D. A. Savitz, and A. H. Herring. 2003. Modeling community-level effects on preterm birth. Annals of Epidemiology 13(5):377–384.
Kaushal, N., and L. Nepomnyaschy. 2009. Wealth, race/ethnicity, and children’s educational outcomes. Children and Youth Services Review 31(9):963–971.
Kearney, M. S., B. H. Harris, E. Jácome, and L. Parker. 2014. Ten economic facts about crime and incarceration in the United States. Washington, DC: The Hamilton Project.
Kenney, M. K., and G. K. Singh. 2016. Adverse childhood experiences among American Indian/Alaska Native children: The 2011–2012 national survey of children’s health. Scientifica 2016:7424239.
Kerker, B. D., J. Zhang, E. Nadeem, R. E. Stein, M. S. Hurlburt, A. Heneghan, and S. McCue Horwitz. 2015. Adverse childhood experiences and mental health, chronic medical conditions, and development in young children. Academic Pediatrics 15:510–517.
Kersten, E. E., K. Z. LeWinn, L. Gottlieb, D. P. Jutte, and N. E. Adler. 2014. San Francisco children living in redeveloped public housing used acute services less than children in older public housing. Health Affairs 33(12):2230–2237.
Kids Count Data Center. 2019. Children living in high poverty areas by race and ethnicity in the United States. https://datacenter.kidscount.org/data/tables/7753-children-living-in-areas-of-concentrated-poverty-by-race-and-ethnicity (accessed July 15, 2019).
Kilpatrick, S. J., L.-A. Papile, and G. A. Macones. 2017. Guidelines for perinatal care. Washington, DC: American Academy of Pediatrics.
Kim, M. A., and K. A. Williams. 2017. Lead levels in landfill areas and childhood exposure: An integrative review. Public Health Nursing 34(1):87–97.
Kim, S., L. England, C. Shapiro-Mendoza, H. Wilson, J. Klejka, M. Tucker, C. Lewis, and J. Kendrick. 2014. Community and federal collaboration to assess pregnancy outcomes in Alaska Native women, 1997–2005. Maternal and Child Health Journal 18(3):634–639.
Knopf, J. A., R. K. Finnie, Y. Peng, R. A. Hahn, B. I. Truman, M. Vernon-Smiley, V. C. Johnson, R. L. Johnson, J. E. Fielding, C. Muntaner, P. C. Hunt, C. Phyllis Jones, M. T. Fullilove, and Community Preventive Services Task Force. 2016. School-based health centers to advance health equity: A community guide systematic review. American Journal of Preventive Medicine 51(1):114–126.
Koball, H., and Y. Jiang. 2018a. Basic facts about low-income children. Children under 18 years, 2016. New York: National Center for Children in Poverty, Columbia University Mailman School of Public Health.
Koball, H., and Y. Jiang. 2018b. Basic facts about low-income children: Children under 9 years, 2016. New York: National Center for Children in Poverty, Columbia University Mailman School of Public Health.
Koball, H., R. Capps, S. Hooker, K. Perreira, A. Campetella, J. M. Pedroza, W. Monson, and S. Huerta. 2015. Health and social service needs of U.S. citizen children with detained or deported immigrant parents. Washington, DC: Migration Policy Institute.
Kogan, M. D., M. Kotelchuck, G. R. Alexander, and W. E. Johnson. 1994. Racial disparities in reported prenatal care advice from health care providers. American Journal of Public Health 84(1):82–88.
Kolarik, B., K. Naydenov, M. Larsson, C. G. Bornehag, and J. Sundell. 2008. The association between phthalates in dust and allergic diseases among Bulgarian children. Environmental Health Perspectives 116(1):98–103.
Krafft, C., E. E. Davis, and K. Tout. 2017. Child care subsidies and the stability and quality of child care arrangements. Early Childhood Research Quarterly 39:14–34.
Kramer, M. S., and R. Kakuma. 2012. Optimal duration of exclusive breastfeeding. Cochrane Database of Systematic Reviews 8:CD003517.
Krol, K. M., and T. Grossmann. 2018. Psychological effects of breastfeeding on children and mothers. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 61(8):977–985.
Kull, M. A., and R. L. Coley. 2014. Housing costs and child functioning: Processes through investments and financial strains. Children and Youth Services Review 39:25–38.
Kumari, M., J. Head, and M. Marmot. 2004. Prospective study of social and other risk factors for incidence of type 2 diabetes in the Whitehall II Study. Archives of Internal Medicine 164(17):1873–1880.
Kuo, A. A., R. A. Etzel, L. A. Chilton, C. Watson, and P. A. Gorski. 2012. Primary care pediatrics and public health: Meeting the needs of today’s children. American Journal of Public Health 102(12):e17–e23.
Lane, S. D., R. H. Keefe, R. Rubinstein, B. A. Levandowski, N. Webster, D. A. Cibula, A. K. Boahene, O. Dele-Michael, D. Carter, T. Jones, M. Wojtowycz, and J. Brill. 2008. Structural violence, urban retail food markets, and low birth weight. Health and Place 14(3):415–423.
Langley-Evans, S. C. 2015. Nutrition in early life and the programming of adult disease: A review. Journal of Human Nutrition and Dietetics 28(Suppl 1):1–14.
Lanphear, B. P., R. S. Kahn, O. Berger, P. Auinger, S. M. Bortnick, and R. W. Nahhas. 2001. Contribution of residential exposures to asthma in US children and adolescents. Pediatrics 107(6):e98.
Lau, E. Y., J. Liu, E. Archer, S. M. McDonald, and J. Liu. 2014. Maternal weight gain in pregnancy and risk of obesity among offspring: A systematic review. Journal of Obesity 2014(524939).
Leeners, B., W. Rath, E. Block, G. Gorres, and S. Tschudin. 2014. Risk factors for unfavorable pregnancy outcome in women with adverse childhood experiences. Journal of Perinatal Medicine 42(2):171–178.
Lefmann, T., and T. Combs-Orme. 2014. Prenatal stress, poverty, and child outcomes. Child and Adolescent Social Work Journal 31(6):577–590.
Leininger, L. J. 2009. Partial-year insurance coverage and the health care utilization of children. Medical Care Research and Review 66(1):49–67.
Leininger, L., and H. Levy. 2015. Child health and access to medical care. The Future of Children 25(1):65–90.
Leonard, S. A., K. M. Rasmussen, J. C. King, and B. Abrams. 2017. Trajectories of maternal weight from before pregnancy through postpartum and associations with childhood obesity. American Journal of Clinical Nutrition 106(5):1295–1301.
Leventhal, T., and S. Newman. 2010. Housing and child development. Children and Youth Services Review 32(9):1165–1174.
Lewis, M., and L. Myhra. 2018. Integrated care with indigenous populations: Considering the role of health care systems in health disparities. Journal of Health Care for the Poor and Underserved 29(3):1083–1107.
Li, Y., C. Margerison-Zilko, K. L. Strutz, and C. Holzman. 2018. Life course adversity and prior miscarriage in a pregnancy cohort. Women’s Health Issues 28(3):232–238.
Lidsky, T. I., and J. S. Schneider. 2003. Lead neurotoxicity in children: Basic mechanisms and clinical correlates. Brain 126(1):5–19.
Lieb, R., K. R. Merikangas, M. Hofler, H. Pfister, B. Isensee, and H. U. Wittchen. 2002. Parental alcohol use disorders and alcohol use and disorders in offspring: A community study. Psychological Medicine 32(1):63–78.
Line, B., and L. Poon. 2013. How other countries handle immigration. National Geographic, https://news.nationalgeographic.com/news/2013/06/130630-immigration-reform-world-refugees-asylum-canada-japan-australia-sweden-denmark-united-kingdomundocumented-immigrants (accessed April 23, 2019).
Liu, C., B. Vinnerljung, V. Östberg, K. Gauffin, S. Juarez, S. Cnattingius, and A. Hjern. 2018. Out-of-home care and subsequent preterm delivery: An intergenerational cohort study. Pediatrics 142(2):e20172729.
Lodge, C. J., D. J. Tan, M. X. Lau, X. Dai, R. Tham, A. J. Lowe, G. Bowatte, K. J. Allen, and S. C. Dharmage. 2015. Breastfeeding and asthma and allergies: A systematic review and meta-analysis. Acta Paediatrica 104(467):38–53.
Lu, Q., M. C. Lu, and C. D. Schetter. 2005. Learning from success and failure in psychosocial intervention: An evaluation of low birth weight prevention trials. Journal of Health Psychology 10(2):185–195.
Luthar, S. 2006. Resilience in development: A synthesis of research across five decades. In Developmental psychopathology, 3rd ed. Vol. 2, Risk, disorder, and adaptation, edited by D. Cicchetti and D. J. Cohen. New York: Wiley. Pp. 740–795.
Luthar, S. S., N. E. Suchman, and M. Altomare. 2007. Relational psychotherapy mothers’ group: A randomized clinical trial for substance abusing mothers. Development and Psychopathology 19(1):243–261.
Ma, C. T., L. Gee, and M. B. Kushel. 2008. Associations between housing instability and food insecurity with health care access in low-income children. Ambulatory Pediatrics 8(1):50–57.
Ma, X., J. Liu, J. W. Hardin, G. Zhao, and A. D. Liese. 2016. Neighborhood food access and birth outcomes in South Carolina. Maternal and Child Health Journal 20(1):187–195.
Mameli, C., S. Mazzantini, and G. V. Zuccotti. 2016. Nutrition in the first 1000 days: The origin of childhood obesity. International Journal of Environmental Research and Public Health 13(9):838.
Manikkam, M., R. Tracey, C. Guerrero-Bosagna, and M. K. Skinner. 2013. Plastics derived endocrine disruptors (BPA, DEHP and DBP) induce epigenetic transgenerational inheritance of obesity, reproductive disease and sperm epimutations. PLoS ONE 8(1):e55387.
March of Dimes. 2018. Vitamins and other nutrients during pregnancy. https://www.marchofdimes.org/pregnancy/vitamins-and-other-nutrients-during-pregnancy.aspx (accessed April 22, 2019).
Marchi, J., M. Berg, A. Dencker, E. K. Olander, and C. Begley. 2015. Risks associated with obesity in pregnancy, for the mother and baby: A systematic review of reviews. Obesity Reviews 16(8):621–638.
Margerison-Zilko, C., C. Cubbin, J. Jun, K. Marchi, K. Fingar, and P. Braveman. 2015. Beyond the cross-sectional: Neighborhood poverty histories and preterm birth. American Journal of Public Health 105(6):1174–1180.
Margolin, G., and E. B. Gordis. 2004. Children’s exposure to violence in the family and community. Current Directions in Psychological Science 13(4):152–155.
Markowitz, G., and D. Rosner. 2014. Lead wars: The politics of science and the fate of America’s children, Vol. 24. Berkeley, CA: University of California Press.
Marks, A. K., J. L. McKenna, and C. García Coll. 2018. National immigration receiving contexts: A critical aspect of native-born, immigrant, and refugee youth well-being. European Psychologist 23(1):6–20.
Marques, A., T. O’Connor, C. Roth, E. Susser, and A.-L. Bjørke-Monsen. 2013. The influence of maternal prenatal and early childhood nutrition and maternal prenatal stress on offspring immune system development and neurodevelopmental disorders. Frontiers in Neuroscience 7:120.
Martin, A., R. A. Razza, and J. Brooks-Gunn. 2012. Specifying the links between household chaos and preschool children’s development. Early Child Development and Care 182(10):1247–1263.
Masho, S. W., S. Cha, D. A. Chapman, and D. Chelmow. 2017. Understanding the role of violence as a social determinant of preterm birth. American Journal of Obstetrics and Gynecology 216(2):183.e1–183.e7.
Masten, A. S. 2014. Ordinary magic: Resilience in development. New York: Guilford Press.
Masten, A. S., J. J. Cutuli, J. E. Herbers, E. Hinz, J. Obradović, and A. J. Wenzel. 2014. Academic risk and resilience in the context of homelessness. Child Development Perspectives 8(4):201–206.
Matheson, S. L., M. Kariuki, M. J. Green, K. Dean, F. Harris, S. Tzoumakis, M. TarrenSweeney, S. Brinkman, M. Chilvers, T. Sprague, V. J. Carr, and K. R. Laurens. 2017. Effects of maltreatment and parental schizophrenia spectrum disorders on early childhood social-emotional functioning: A population record linkage study. Epidemiology and Psychiatric Sciences 26(6):612–623.
Mathews, T. J., and M. F. MacDorman. 2007. Infant mortality statistics from the 2004 period linked birth/infant death data set. National Vital Statistics Reports 55(14):1–32. Hyattsville, MD: National Center for Health Statistics.
Mathur, A. 2016. Childcare costs: Yet another way we’re failing the poor. http://www.aei.org/publication/childcare-costs-yet-another-way-were-failing-the-poor (accessed July 14, 2019).
McGowan, P. O., and S. G. Matthews. 2018. Prenatal stress, glucocorticoids, and developmental programming of the stress response. Endocrinology 159(1):69–82.
Medlin, C., and E. McDonald. 2018. Map the meal gap 2018. A report on county and congressional district food insecurity and county food cost in the United States in 2016. Chicago, IL: Feeding American.
Mehra, R., L. M. Boyd, and J. R. Ickovics. 2017. Racial residential segregation and adverse birth outcomes: A systematic review and meta-analysis. Social Science & Medicine 191:237–250.
Meijer, M., K. Bloomfield, and G. Engholm. 2013. Neighbourhoods matter too: The association between neighbourhood socioeconomic position, population density and breast, prostate and lung cancer incidence in Denmark between 2004 and 2008. Journal of Epidemiology and Community Health 67(1):6–13.
Merrick, M. T., D. C. Ford, K. A. Ports, and A. S. Guinn. 2018. Prevalence of adverse childhood experiences from the 2011–2014 Behavioral Risk Factor Surveillance System in 23 states. JAMA Pediatrics 172(11):1038–1044.
Messer, L. C., J. S. Kaufman, N. Dole, A. Herring, and B. A. Laraia. 2006. Violent crime exposure classification and adverse birth outcomes: A geographically-defined cohort study. International Journal of Health Geographics 5:22.
Meyer, B. D., and J. X. Sullivan. 2009. Five decades of consumption and income poverty. Working paper 14827. Cambridge, MA: National Bureau of Economic Research.
Miao, M., W. Yuan, Y. He, Z. Zhou, J. Wang, E. Gao, G. Li, and D. K. Li. 2011. In utero exposure to bisphenol-A and anogenital distance of male offspring. Birth Defects Research (Part A) 91(10):867–872.
Midoro-Horiuti, T., R. Tiwari, C. S. Watson, and R. M. Goldblum. 2010. Maternal bisphenol A exposure promotes the development of experimental asthma in mouse pups. Environmental Health Perspectives 118(2):273–277.
Mikati, I., A. F. Benson, T. J. Luben, J. D. Sacks, and J. Richmond-Bryant. 2018. Disparities in distribution of particulate matter emission sources by race and poverty status. American Journal of Public Health 108(4):480–485.
Miller, P. 2011. A critical analysis of the research on student homelessness. Review of Educational Research 81(3):308–337.
Miranda, M. L., S. E. Edwards, H. H. Chang, and R. L. Auten. 2013. Proximity to roadways and pregnancy outcomes. Journal of Exposure Science & Environmental Epidemiology 23(1):32–38.
Moffitt, T. E., and K.-G. T. Tank. 2013. Childhood exposure to violence and lifelong health; clinical intervention science and stress-biology research join forces. Developmental Psychopathology 24:1619–1634.
Monasta, L., G. D. Batty, A. Cattaneo, V. Lutje, L. Ronfani, F. J. Van Lenthe, and J. Brug. 2010. Early-life determinants of overweight and obesity: A review of systematic reviews. Obesity Reviews 11(10):695–708.
Morenoff, J. D. 2003. Neighborhood mechanisms and the spatial dynamics of birth weight. American Journal of Sociology 108(5):976–1017.
Morgan, I., and A. Amerikaner. 2018. An Analysis of School Funding Equity across the U.S. and within Each State. Washington, DC: The Education Trust.
Morrison, S., E. D. Shenassa, P. Mendola, T. Wu, and K. Schoendorf. 2013. Allostatic load may not be associated with chronic stress in pregnant women, NHANES 1999–2006. Annals of Epidemiology 23(5):294–297.
Motti-Stefanidi, F., and C. García Coll. 2018. We have come a long way, baby: “Explaining positive adaptation of immigrant youth across cultures.” Journal of Adolescence 62:218–221.
Muller, C., R. J. Sampson, and A. S. Winter. 2018. Environmental inequality: The social causes and consequences of lead exposure. Annual Review of Sociology 44:263–282.
Nakamura, K., K. Itoh, H. Dai, L. Han, X. Wang, S. Kato, T. Sugimoto, and S. Fushiki. 2012. Prenatal and lactational exposure to low-doses of bisphenol A alters adult mice behavior. Brain and Development 34(1):57–63.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2015a. Mental disorders and disabilities among low-income children. Washington, DC: The National Academies Press.
NASEM. 2015b. The integration of immigrants into American society. Washington, DC: The National Academies Press.
NASEM. 2016a. Parenting matters: Supporting parents of children ages 0–8. Washington, DC: The National Academies Press.
NASEM. 2016b. Preventing bullying through science, policy, and practice. Washington, DC: The National Academies Press.
NASEM. 2017a. Communities in action: Pathways to health equity. Washington, DC: The National Academies Press.
NASEM. 2017b. Promoting the educational success of children and youth learning English: Promising futures. Washington, DC: The National Academies Press.
NASEM. 2018. Transforming the financing of early care and education. Washington, DC: The National Academies Press.
NASEM. 2019. A roadmap to reducing child poverty. Washington, DC: The National Academies Press.
National Center for Education Statistics. n.d. Trends in high school dropout and completion rates in the United States. https://nces.ed.gov/programs/dropout/ind_05.asp (accessed April 22, 2019).
National Congress of American Indians. n.d. Data disaggregation. The asterisk nation. http://www.ncai.org/policy-research-center/research-data/data (accessed April 23, 2019).
National Low Income Housing Coalition. 2018. The gap: A shortage of affordable rental homes. https://reports.nlihc.org/gap (accessed July 15, 2019).
National Scientific Council on the Developing Child. 2004. Young children develop in an environment of relationships (working paper 1). Cambridge, MA: Harvard University.
Ncube, C. N., D. A. Enquobahrie, S. M. Albert, A. L. Herrick, and J. G. Burke. 2016. Association of neighborhood context with offspring risk of preterm birth and low birthweight: A systematic review and meta-analysis of population-based studies. Social Science & Medicine 153:156–164.
Ness, M. N., K. D. Rosenberg, T. Abrahamson-Richards, A. P. Sandoval, T. M. Weiser, and V. Warren-Mears. 2017. Stressful life events and self-reported postpartum depressive symptoms 13–24 months after live birth among non-Hispanic American Indian/Alaska Native mothers in Oregon: Results from a population-based survey. American Indian and Alaska Native Mental Health Research 24(2):76–98.
Newman, S. J. 2008. Does housing matter for poor families? A critical summary of research and issues still to be resolved. Journal of Policy Analysis and Management 27(4):895–925.
Newman, S. J., and C. S. Holupka. 2014. Housing affordability and investments in children. Journal of Housing Economics 24:89–100.
Newman, S., and C. S. Holupka. 2016. Housing affordability and children’s cognitive achievement. Health Affairs 35(11):2092–2099.
Nichols, E. B., and A. B. Loper. 2012. Incarceration in the household: Academic outcomes of adolescents with an incarcerated household member. Journal of Youth and Adolescence 41(11):1455–1471.
NRC and IOM. 2000. From neurons to neighborhoods: The science of early childhood development. Washington, DC: National Academy Press.
NRC and IOM. 2010. Student mobility: Exploring the impacts of frequent moves on achievement: Summary of a workshop. Washington, DC: The National Academies Press.
Nyaradi, A., J. Li, S. Hickling, J. Foster, and W. Oddy. 2013. The role of nutrition in children’s neurocognitive development, from pregnancy through childhood. Frontiers in Human Neuroscience 7:97.
Oberg, C., S. Colianni, and L. King-Schultz. 2016. Child health disparities in the 21st century. Current Problems in Pediatric and Adolescent Health Care 46(9):291–312.
Obradović, J., J. D. Long, J. Cutuli, C.-K. Chan, E. Hinz, D. Heistad, and A. S. Masten. 2009. Academic achievement of homeless and highly mobile children in an urban school district: Longitudinal evidence on risk, growth, and resilience. Development Psychopathology 21(2):493–518.
O’Campo, P., J. G. Burke, J. Culhane, I. T. Elo, J. Eyster, C. Holzman, L. C. Messer, J. S. Kaufman, and B. A. Laraia. 2008. Neighborhood deprivation and preterm birth among non-Hispanic black and white women in eight geographic areas in the United States. American Journal of Epidemiology 167(2):155–163.
OECD (Organisation for Economic Co-operation and Development). 2018. Policies and practices to support the resilience of students with an immigrant background. In The resilience of students with an immigrant background: Factors that shape well-being. Paris, France: OECD Publishing.
Office of Child Care. n.d. Quick fact. https://www.acf.hhs.gov/occ/quick-fact (accessed April 22, 2019).
Office of Head Start. 2018a. History of Head Start. https://www.acf.hhs.gov/ohs/about/history-of-head-start (accessed April 22, 2019).
Office of Head Start. 2018b. Head Start program facts. Fiscal year 2017. https://eclkc.ohs.acf.hhs.gov/about-us/article/head-start-program-facts-fiscal-year-2017 (accessed April 22, 2019).
Oh, D. L., P. Jerman, S. Silverio Marques, K. Koita, S. K. Purewal Boparai, N. Burke Harris, and M. Bucci. 2018. Systematic review of pediatric health outcomes associated with childhood adversity. BMC Pediatrics 18(1):83.
Olivet, J., M. Dones, M. Richard, C. Wilkey, S. Yampolskaya, M. Beit-Arie, and L. Joseph. 2018. Supporting partnerships for anti-racist communities: Phase one study findings. Needham, MA: Center for Social Innovation.
Olsen, J. M. 2018. Integrative review of pregnancy health risks and outcomes associated with adverse childhood experiences. Journal of Obstetric, Gynecologic, & Neonatal Nursing 47(6):783–794.
Ore, C. E., N. Teufel-Shone, and T. M. Chico-Jarillo. 2016. American Indian and Alaska Native resilience along the life course and across generations: A literature review. American Indian and Alaska Native Mental Health Research 23(3):134–157.
Osofsky, J. D. 2003. Prevalence of children’s exposure to domestic violence and child maltreatment: Implications for prevention and intervention. Clinical Child and Family Psychology Review 6(3):161–170.
Osterman, M. J. K., and J. A. Martin. 2018. Timing and adequacy of prenatal care in the United States, 2016. National Vital Statistics Reports 67(3):1–14.
Pac, J. E., A. P. Bartel, C. J. Ruhm, and J. Waldfogel. 2019. Paid family leave and breastfeeding—evidence from California. Cambridge, MA: National Bureau of Economic Research.
Paczkowski, M. M., and S. Galea. 2010. Sociodemographic characteristics of the neighborhood and depressive symptoms. Current Opinion in Psychiatry 23(4):337–341.
Padula, A. M., O. Humblet, K. Mortimer, F. Lurmann, and I. Tager. 2012. Exposure to air pollution during pregnancy and pulmonary function growth in the FACES LiTE Cohort. Meeting Abstracts. American Journal of Respiratory and Critical Care Medicine. Conference: American Thoracic Society International Conference, ATS 185(1):A1725.
Paradies, Y., J. Ben, N. Denson, A. Elias, N. Priest, A. Pieterse, A. Gupta, M. Kelaher, and G. Gee. 2015. Racism as a determinant of health: A systematic review and meta-analysis. PLoS ONE 10(9):e0138511.
Pearl, M., P. Braveman, and B. Abrams. 2001. The relationship of neighborhood socioeconomic characteristics to birthweight among 5 ethnic groups in California. American Journal of Public Health 91(11):1808–1814.
Petrosky, E., J. M. Blair, C. J. Betz, K. A. Fowler, S. P. D. Jack, and B. H. Lyons. 2017. Racial and ethnic differences in homicides of adult women and the role of intimate partner violence—United States, 2003–2014. Morbidity and Mortality Weekly Report 66(28):741–746.
Pickett, K. E., and M. Pearl. 2001. Multilevel analyses of neighbourhood socioeconomic context and health outcomes: A critical review. Journal of Epidemiology and Community Health 55(2):111–122.
Poston, L., L. F. Harthoorn, and E. M. Van Der Beek. 2011. Obesity in pregnancy: Implications for the mother and lifelong health of the child. A consensus statement. Pediatric Research 69(2):175–180.
Poulton, R., T. E. Moffitt, and P. A. Silva. 2015. The Dunedin Multidisciplinary Health and Development Study: Overview of the first 40 years, with an eye to the future. Social Psychiatry and Psychiatric Epidemiology 50(5):679–693.
President’s Task Force on Environmental Health Risks and Safety Risks to Children. 2018. Federal action plan to reduce childhood lead exposure. Washington, DC: U.S. Environmental Protection Agency.
Priest, N., Y. Paradies, B. Trenerry, M. Truong, S. Karlsen, and Y. Kelly. 2013. A systematic review of studies examining the relationship between reported racism and health and wellbeing for children and young people. Social Science & Medicine 95:115–127.
Provençal, N., and E. B. Binder. 2015. The effects of early life stress on the epigenome: From the womb to adulthood and even before. Experimental Neurology 268:10–20.
Public Health Management Corporation. 2013. Findings from the Philadelphia Urban ACE Survey. Philadelphia, PA: The Research and Evaluation Group at Public Health Management Corporation.
Racine, N., A. Plamondon, S. Madigan, S. McDonald, and S. Tough. 2018. Maternal adverse childhood experiences and infant development. Pediatrics 141(4):e20172495.
Raglan, G., S. Lannon, K. Jones, and J. Schulkin. 2016. Racial and ethnic disparities in preterm birth among American Indian and Alaska Native women. Maternal and Child Health Journal 20(1):16–24.
Ramakrishnan, U., F. Grant, T. Goldenberg, A. Zongrone, and R. Martorell. 2012. Effect of women’s nutrition before and during early pregnancy on maternal and infant outcomes: A systematic review. Paediatric and Perinatal Epidemiology 26(Suppl 1):285–301.
Ramchandani, P. G., L. Psychogiou, H. Vlachos, J. Iles, V. Sethna, E. Netsi, and A. Lodder. 2011. Paternal depression: An examination of its links with father, child and family functioning in the postnatal period. Depression and Anxiety 28(6):471–477.
Rauh, V. A., P. J. Landrigan, and L. Claudio. 2008. Housing and health. Annals of the New York Academy of Sciences 1136(1):276–288.
Ready, D., and M. Silander. 2011. School racial and ethnic composition and young children’s cognitive development. In Integrating schools in a changing society: New policies and legal options for a multiracial generation, edited by E. Frankenberg and E. Debray-Pelot. Chapel Hill, NC: University of North Carolina. Pp. 91–113.
Reardon, S. F. 2016. School district socioeconomic status, race, and academic achievement. Stanford, CA: Stanford Center for Educational Policy Analysis.
Reeves, R. V., and E. Krause. 2019. The effects of maternal depression on early childhood development and implications for economic mobility. Washington, DC: The Brookings Institution.
Rentner, T. L., L. D. Dixon, and L. Lengel. 2012. Critiquing fetal alcohol syndrome health communication campaigns targeted to American Indians. Journal of Health Communication 17(1):6–21.
Rhodes, A. E., M. H. Boyle, J. Bethell, C. Wekerle, D. Goodman, L. Tonmyr, and I. Manion. 2012. Child maltreatment and onset of emergency department presentations for suicide-related behaviors. Child Abuse and Neglect 36:542–551.
Rich-Edwards, J. W., S. L. Buka, R. T. Brennan, and F. Earls. 2003. Diverging associations of maternal age with low birthweight for black and white mothers. International Journal of Epidemiology 32(1):83–90.
Ritsher, J. E., V. Warner, J. G. Johnson, and B. P. Dohrenwend. 2001. Inter-generational longitudinal study of social class and depression: A test of social causation and social selection models. The British Journal of Psychiatry 40:S84–S90.
Robinette, J. W., S. T. Charles, J. A. Mogle, and D. M. Almeida. 2013. Neighborhood cohesion and daily well-being: Results from a diary study. Social Science & Medicine 96:174–182.
Rojas-Flores, L., M. L. Clements, J. H. Koo, and J. London. 2017. Trauma and psychological distress in Latino citizen children following parental detention and deportation. Psychological Trauma: Theory, Research, Practice, and Policy 9(3):352–361.
Rutman, S., M. Taualii, D. Ned, and C. Tetrick. 2012. Reproductive health and sexual violence among urban American Indian and Alaska Native young women: Select findings from the National Survey of Family Growth (2002). Maternal and Child Health Journal 16(Suppl 2):347–352.
Rutman, S., L. Phillips, and A. Sparck. 2016. Health care access and use by urban American Indians and Alaska Natives: Findings from the national health interview survey (2006–09). Journal of Health Care for the Poor and Underserved 27(3):1521–1536.
Rutter, M. 1979. Protective factors in children’s responses to stress and disadvantage. In Primary prevention of psychopathology, Vol. 3, edited by W. M. Kent and J. E. Rolf. Hanover, NH: University Press of New England. Pp. 49–74.
Ryan, A. S. 2007. Breastfeeding and the risk of childhood obesity. Collegium Antropologicum 31(1):19–28.
Ryan, J. P., B. E. Perron, and H. Huang. 2016. Child welfare and the transition to adulthood: Investigating placement status and subsequent arrests. Journal of Youth and Adolescence 45(1):172–182.
Saelens, B. E., J. F. Sallis, J. B. Black, and D. Chen. 2003a. Neighborhood-based differences in physical activity: An environment scale evaluation. American Journal of Public Health 93(9):1552–1558.
Saelens, B. E., J. F. Sallis, and L. D. Frank. 2003b. Environmental correlates of walking and cycling: Findings from the transportation, urban design, and planning literatures. Annals of Behavioral Medicine 25(2):80–91.
Sameroff, A. J. 1998. Environmental risk factors in infancy. Pediatrics 102(Suppl E1):1287–1292.
Sameroff, A., R. Seifer, M. Zax, and R. Barocas. 1987a. Early indicators of developmental risk: Rochester longitudinal study. Schizophrenia Bulletin 13(3):383–394.
Sameroff, A. J., R. Seifer, R. Barocas, M. Zax, and S. Greenspan. 1987b. Intelligence quotient scores of 4-year-old children: Social-environmental risk factors. Pediatrics 79(3):343–350.
Sampson, R. J., and A. S. Winter. 2016. The racial ecology of lead poisoning. Du Bois Review 13(2):261–283.
Sandel, M., and M. Desmond. 2017. Investing in housing for health improves both mission and margin. JAMA 318(23):2291–2292.
Sandel, M., K. Phelan, R. Wright, H. P. Hynes, and B. P. Lanphear. 2004. The effects of housing interventions on child health. Pediatric Annals 33(7):474–481.
Sankar, M. J. S., R. B. Chowdhury, R. N. Bhandari, S. Teneja, and J. Martines. 2015. Optimal breastfeeding practices and infant and child mortality: A systematic review and meta-analysis. Acta Paediatrica 104:3–13.
Santiago, C. D., S. Kaltman, and J. Miranda. 2013. Poverty and mental health: How do low-income adults and children fare in psychotherapy? Journal of Clinical Psychology 69(2):115–126.
Schempf, A., D. Strobino, and P. O’Campo. 2009. Neighborhood effects on birthweight: An exploration of psychosocial and behavioral pathways in Baltimore, 1995–1996. Social Science & Medicine 68(1):100–110.
Schmit, S., and C. Walker. 2016. Disparate access. Head Start and CCDBG data by race and ethnicity. Washington, DC: Center for Law and Social Policy.
Schofield, T. J., R. D. Lee, and M. T. Merrick. 2013. Safe, stable, nurturing relationships as a moderator of intergenerational continuity of child maltreatment: A meta-analysis. Journal of Adolescent Health 53:S32–S38.
Schwartz, M., and E. Wilson. n.d. Who can afford to live in a home? A look at data from the 2006 American community survey. https://www.census.gov/housing/census/publications/who-can-afford.pdf (accessed April 22, 2019).
Schwarzenberg, S. J., and M. K. Georgieff. 2018. Advocacy for improving nutrition in the first 1000 days to support childhood development and adult health. Pediatrics 141(2):e20173716.
Sedlak, A. J., J. Mettenburg, M. Basena, I. Petta, K. McPherson, A. Greene, and S. Li. 2010. Fourth National Incidence Study of Child Abuse and Neglect (NIS-4): Report to Congress. Washington, DC: U.S. Department of Health and Human Services, Administration for Children and Families.
Sharfstein, J., M. Sandel, R. Kahn, and H. Bauchner. 2001. Is child health at risk while families wait for housing vouchers? American Journal of Public Health 91(8):1191–1192.
Sharkey, P. 2010. The acute effect of local homicides on children’s cognitive performance. Proceedings of the National Academy of Sciences of the United States of America 107(26):11733–11738.
Sharkey, P. T., N. Tirado-Strayer, A. V. Papachristos, and C. C. Raver. 2012. The effect of local violence on children’s attention and impulse control. American Journal of Public Health 102(12):2287–2293.
Sheffield, P. E., R. A. Coulombe, R. Speranza, Y.-H. M. Chiu, H.-H. L. Hsu, P. C. Curtin, S. Renzetti, A. Pajak, B. Coull, J. Schwartz, I. Kloog, and R. J. Wright. 2018. Association between particulate air pollution exposure during pregnancy and postpartum maternal psychological functioning. PLoS ONE 13(4):e0195267.
Shen, H., C. Magnusson, D. Rai, M. Lundberg, F. Lê-Scherban, C. Dalman, and B. K. Lee. 2016. Associations of parental depression with child school performance at age 16 years in Sweden. JAMA Psychiatry 7:239–246.
Shervin, A. 2018. Health disparities due to diminished return among black Americans: Public policy solutions. Social Issues and Policy Review 12(1):112–145.
Shin, S. H., E. Edwards, T. Heeren, and M. Amodeo. 2009. Relationship between multiple forms of maltreatment by a parent or guardian and adolescent alcohol use. The American Journal on Addictions 18(3):226–234.
Shinkman, P. D. 2018. Comparing the policies and practices of detaining children. U.S. News & World Report. https://www.usnews.com/news/best-countries/articles/2018-06-25/how-other-countries-treatment-of-detained-migrant-children-compare-to-the-us (accessed April 23, 2019).
Shonkoff, J. P., A. S. Garner, Committee on Psychosocial Aspects of Child and Family Health, Committee on Early Childhood, Adoption, and Dependent Care, Section on Developmental and Behavioral Pediatrics. 2012. The lifelong effects of early childhood adversity and toxic stress. Pediatrics 129(1):e232–e246.
Singer, A. 2012. Immigrant workers in the U.S. labor force. Washington, DC: The Brookings Institution.
Skiba, R. J., M. I. Arredondo, and M. K. Rausch. 2014. Discipline disparities: A research-to-practice collaborative. Bloomington, IN: The Equity Project at Indiana University, Center for Evaluation and Education Policy.
Slopen, N., G. Fitzmaurice, D. R. Williams, and S. E. Gilman. 2010. Poverty, food insecurity, and the behavior for childhood internalizing and externalizing disorders. Journal of the American Academy of Child and Adolescent Psychiatry 49(5):444–452.
Smith, L., V. Li, S. Dykema, D. Hamlet, and A. Shellman. 2013. “Honoring somebody that society doesn’t honor”: Therapists working in the context of poverty. Journal of Clinical Psychology 69(2):138–151.
Smith, M. V., N. Gotman, and K. A. Yonkers. 2016. Early childhood adversity and pregnancy outcomes. Maternal and Child Health Journal 20(4):790–798.
Smith, S., S. Stagman, S. Blank, C. Ong, and K. McDow. 2011. Building strong systems of support for young children’s mental health: Key strategies for states and a planning tool. New York: National Center for Children in Poverty, Mailman School of Public Health, Columbia University.
Solari, C. D., and R. D. Mare. 2012. Housing crowding effects on children’s wellbeing. Social Science Research 41(2):464–476.
Spanier, A. J., R. S. Kahn, A. R. Kunselman, R. Hornung, Y. Xu, A. M. Calafat, and B. P. Lanphear. 2012. Prenatal exposure to bisphenol A and child wheeze from birth to 3 years of age. Environmental Health Perspectives 120(6):916–920.
Sternthal, M. J., H. J. Jun, F. Earls, and R. J. Wright. 2010. Community violence and urban childhood asthma: A multilevel analysis. European Respiratory Journal 36(6):1400–1409.
Subramanian, S. V., J. T. Chen, D. H. Rehkopf, P. D. Waterman, and N. Krieger. 2006. Comparing individual- and area-based socioeconomic measures for the surveillance of health disparities: A multilevel analysis of Massachusetts births, 1989–1991. American Journal of Epidemiology 164(9):823–834.
Sue, D. W. 2019. Counseling the culturally diverse: Theory and practice, 8th ed. Hoboken, NJ: John Wiley & Sons.
Sweeney, S., and A. MacBeth. 2016. The effects of paternal depression on child and adolescent outcomes: A systematic review. Journal of Affective Disorders 205:44–59.
Tabacchi, G., S. Giammanco, M. La Guardia, and M. Giammanco. 2007. A review of the literature and a new classification of the early determinants of childhood obesity: From pregnancy to the first years of life. NTR Nutrition Research 27(10):587–604.
Taylor, C. M., J. Golding, and A. M. Emond. 2015. Adverse effects of maternal lead levels on birth outcomes in the ALSPAC study: A prospective birth cohort study. BJOG: An International Journal of Obstetrics and Gynaecology 122(3):322–328.
Taylor, C. M., J. Golding, and A. M. Emond. 2016. Moderate prenatal cadmium exposure and adverse birth outcomes: A role for sex-specific differences? Paediatric and Perinatal Epidemiology 30(6):603–611.
The Nation’s Report Card. 2017. National achievement-level results. https://www.nationsreportcard.gov/reading_2017/nation/achievement/?grade=4 (accessed April 22, 2019).
The Pew Charitable Trusts. 2018. American families face a growing rent burden. Washington, DC: The Pew Charitable Trusts.
Theall, K. P., E. A. Shirtcliff, A. R. Dismukes, M. Wallace, and S. S. Drury. 2017. Association between neighborhood violence and biological stress in children. JAMA Pediatrics 171(1):53–60.
Thompson, R., T. Lewis, E. C. Neilson, D. J. English, A. J. Litrownik, B. Margolis, and H. Dubowitz. 2017. Child maltreatment and risky sexual behavior. Child Maltreatment 22:69–78.
Thorne-Lyman, A. L., and W. W. Fawzi. 2012. Vitamin A and carotenoids during pregnancy and maternal, neonatal and infant health outcomes: A systematic review and meta-analysis. Paediatric and Perinatal Epidemiology 26(Suppl 1):36–54.
Trasande, L., T. M. Attina, and H. Trachtman. 2013. Bisphenol A exposure is associated with low-grade urinary albumin excretion in children of the United States. Kidney International 83(4):741–748.
Tsai, S. S., H. S. Yu, C. C. Chang, H. Y. Chuang, and C. Y. Yang. 2004. Increased risk of preterm delivery in women residing near thermal power plants in Taiwan. Archives of Environmental Health 59(9):478–483.
Twardzik, E., C. Cotto-Negron, and M. MacDonald. 2017. Factors related to early intervention Part C enrollment: A systematic review. Disability and Health Journal 10(4):467–474.
Uebelacker, L. A., C. B. Eaton, R. Weisberg, M. Sands, C. Williams, D. Calhoun, J. E. Manson, N. L. Denburg, and T. Taylor. 2013. Social support and physical activity as moderators of life stress in predicting baseline depression and change in depression over time in the Women’s Health Initiative. Social Psychiatry and Psychiatric Epidemiology 48(12):1971–1982.
Ullrich, R., S. Schmitt, and R. Cosse. 2019. Inequitable access to child care subsidies. Washington, DC: Center for Law and Social Policy.
U.S. Census Bureau. 2015. American Community Survey. https://www.census.gov/topics/housing.html (accessed July 14, 2019).
Valdez, C. R., B. Padilla, S. M. Moore, and S. Magana. 2013. Feasibility, acceptability, and preliminary outcomes of the Fortalezas Familiares intervention for Latino families facing maternal depression. Family Process 52(3):394–410.
Valentino, R. 2018. Will public pre-K really close achievement gaps? Gaps in prekindergarten quality between students and across states. American Educational Research Journal 55(1):79–116.
van den Bergh, B. R. H., R. Dahnke, and M. Mennes. 2018. Prenatal stress and the developing brain: Risks for neurodevelopmental disorders. Development and Psychopathology 30(3):743–762.
van Lenthe, F. J., C. T. Schrijvers, M. Droomers, I. M. Joung, M. J. Louwman, and J. P. Mackenbach. 2004. Investigating explanations of socio-economic inequalities in health: The Dutch Globe Study. European Journal of Public Health 14(1):63–70.
Van Lieshout, R. J., V. H. Taylor, and M. H. Boyle. 2011. Pre-pregnancy and pregnancy obesity and neurodevelopmental outcomes in offspring: A systematic review. Obesity Reviews 12(5):e548–e559.
VanDeMark, N. R., L. A. Russell, M. O’Keefe, N. Finkelstein, C. D. Noether, and J. C. Gampel. 2005. Children of mothers with histories of substance abuse, mental illness, and trauma. Journal of Community Psychology 33(4):445–459.
Vandenbergh, J. G. 2004. Animal models and studies of in utero endocrine disruptor effects. ILAR Journal 45(4):438–442.
Veena, S. R., C. R. Gale, G. V. Krishnaveni, S. H. Kehoe, K. Srinivasan, and C. H. Fall. 2016. Association between maternal nutritional status in pregnancy and offspring cognitive function during childhood and adolescence; a systematic review. BMC Pregnancy Childbirth 16:220.
Vinikoor-Imler, L. C., L. C. Messer, K. R. Evenson, and B. A. Laraia. 2011. Neighborhood conditions are associated with maternal health behaviors and pregnancy outcomes. Social Science & Medicine 73(9):1302–1311.
Walker, C., and H. Matthews. 2017. CCDBG participation drops to historic low. Washington, DC: Center for Law and Social Policy.
Wallace, M., E. Harville, K. Theall, L. Webber, W. Chen, and G. Berenson. 2013. Neighborhood poverty, allostatic load, and birth outcomes in African American and white women: Findings from the Bogalusa Heart Study. Health and Place 24:260–266.
Wang, H. X., Y. Zhou, C. X. Tang, J. G. Wu, Y. Chen, and Q. W. Jiang. 2012. Association between bisphenol A exposure and body mass index in Chinese school children: A cross-sectional study. Environmental Health 11:79.
Wang, L., C. Collins, M. Ratliff, B. Xie, and Y. Wang. 2017. Breastfeeding reduces childhood obesity risks. Childhood Obesity 13(3):197–204.
Warren, E. J. 2018. Housing affordability and material hardship: Does affordability measurement matter? Journal of Poverty 22(3):228–247.
Warren, E. J., and S. A. Font. 2015. Housing insecurity, maternal stress, and child maltreatment: An application of the family stress model. Social Service Review 89(1):9–39.
Wathen, C. N., and H. L. Macmillan. 2013. Children’s exposure to intimate partner violence: Impacts and interventions. Paediatrics & Child Health 18(8):419–422.
Webb, E., J. Hays, L. Dyrszka, B. Rodriguez, C. Cox, K. Huffling, and S. Bushkin-Bedient. 2016. Potential hazards of air pollutant emissions from unconventional oil and natural gas operations on the respiratory health of children and infants. Reviews on Environmental Health 31(2):225–243.
Weidemann, D., V. Weaver, and J. Fadrowski. 2016. Toxic environmental exposures and kidney health in children. Pediatric Nephrology 31(11):2043–2054.
Wheeler, W., and M. J. Brown. 2013. Blood lead levels in children aged 1–5 years—United States, 1999–2010. Morbidity and Mortality Weekly Report 62(13):245.
WHO (World Health Organization). n.d.-a. Breastfeeding. https://www.who.int/nutrition/topics/exclusive_breastfeeding/en (accessed April 22, 2019).
WHO. n.d.-b. Exclusive breastfeeding for optimal growth, development and health of infants. https://www.who.int/elena/titles/exclusive_breastfeeding/en (accessed April 19, 2019).
Williams, D. R., S. A. Mohammed, J. Leavell, and C. Collins. 2010. Race, socioeconomic status, and health: Complexities, ongoing challenges, and research opportunities. Annals of the New York Academy of Sciences 1186:69–101.
Williams, T. R. 2004. The impacts of household wealth on child development (CSD Working Paper No. 04-07). St. Louis, MO: Washington University, Center for Social Development.
Williams Shanks, T. R. 2007. The impacts of household wealth on child development. Journal of Poverty 11(2):93–116.
Williamson, A. A., L. Knox, N. G. Guerra, and K. R. Williams. 2014. A pilot randomized trial of community-based parent training for immigrant Latina mothers. American Journal of Community Psychology 53(1–2):47–59.
Wilson, S., and C. E. Durbin. 2010. Effects of paternal depression on fathers’ parenting behaviors: A meta-analytic review. Clinical Psychology Review 30(2):167–180.
Winter, A. S., and R. J. Sampson. 2017. From lead exposure in early childhood to adolescent health: A Chicago birth cohort. American Journal of Public Health 107(9):1496–1501.
Wolf, S., K. A. Magnuson, and R. T. Kimbro. 2017. Family poverty and neighborhood poverty: Links with children’s school readiness before and after the Great Recession. Children and Youth Services Review 79:368–384.
Wolff, M. S., S. Engel, G. Berkowitz, S. Teitelbaum, J. Siskind, D. B. Barr, and J. Wetmur. 2007. Prenatal pesticide and PCB exposures and birth outcomes. Pediatric Research 61(2):243–250.
Wong, C., F. Gachupin, R. Holman, M. Macdorman, J. Cheek, S. Holve, and R. Singleton. 2014. American Indian and Alaska Native infant and pediatric mortality, United States, 1999–2009. American Journal of Public Health 104(Suppl 3):S320–S328.
Woo Baidal, J. A., L. M. Locks, E. R. Cheng, T. L. Blake-Lamb, M. E. Perkins, and E. M. Taveras. 2016. Risk factors for childhood obesity in the first 1,000 days: A systematic review. American Journal of Preventive Medicine 50(6):761–779.
Woodward, N., C. E. Finch, and T. E. Morgan. 2015. Traffic-related air pollution and brain development. Aims Environmental Science 2(2):353–373.
Woolf, S. H., L. Aron, D. L, S. M. Simon, E. Zimmerman, and K. X. Luk. 2015. How are income and wealth linked to health and longevity? Washington, DC, and Richmond, VA: Urban Institute and Center on Society and Health.
Wright, A. W., M. Austin, C. Booth, and W. Kliewer. 2017. Systematic review: Exposure to community violence and physical health outcomes in youth. Journal of Pediatric Psychology 42(4):364–378.
Wu, F., and T. K. Takaro. 2007. Childhood asthma and environmental interventions. Environmental Health Perspectives 115(6):971–975.
Xue, Y., T. Leventhal, J. Brooks-Gunn, and F. J. Earls. 2005. Neighborhood residence and mental health problems of 5- to 11-year-olds. Archives of General Psychiatry 62(5):554–563.
Yakoob, M. Y., and C. W. Lo. 2017. Nutrition (micronutrients) in child growth and development: A systematic review on current evidence, recommendations and opportunities for further research. Journal of Developmental and Behavioral Pediatrics 38(8):665–679.
Yoshikawa, H. 2011. Immigrants raising citizens: Undocumented parents and their children. New York: Russell Sage Foundation.
Yoshikawa, H., and A. Kalil. 2011. The effects of parental undocumented status on the developmental contexts of young children in immigrant families. Child Development Perspectives 5(4):291–297.
Zahran, H. S., C. M. Bailey, S. A. Damon, P. L. Garbe, and P. N. Breysse. 2018. Vital signs: Asthma in children—United States, 2001–2016. Morbidity and Mortality Weekly Report 67(5):149.
Zamora-Kapoor, A., L. Nelson, D. Buchwald, L. Walker, and B. Mueller. 2016. Pre-eclampsia in American Indians/Alaska Natives and whites: The significance of body mass index. Maternal and Child Health Journal 20(11):2233–2238.
Zeka, A., S. J. Melly, and J. Schwartz. 2008. The effects of socioeconomic status and indices of physical environment on reduced birth weight and preterm births in eastern Massachusetts. Environmental Health 7:60.
Zerfu, T. A., and H. T. Ayele. 2013. Micronutrients and pregnancy; effect of supplementation on pregnancy and pregnancy outcomes: A systematic review. Nutrition Journal 12:20.
Zhan, M., and M. Sherraden. 2010. Assets and liabilities, race/ethnicity, and children’s college education: Working paper. https://openscholarship.wustl.edu/csd_research/115 (accessed April 18, 2019).
Ziol-Guest, K. M., G. J. Duncan, and A. Kalil. 2009. Early childhood poverty and adult body mass index. American Journal of Public Health 99(3):527–532.




























































































