4
Leveraging Data and Digital Tools
Integrating social care into health care—through awareness, adjustment, assistance, alignment, and advocacy—requires the coordination of information, people, and services across and between organizations and across sectors, often in the presence of well-established silos. The data from these sectors and services necessary for effective integration are similarly siloed, if they are present at all. To date, successful alignment of services that address social needs and traditional medical care has largely been achieved through human capital–intensive approaches to information sharing, involving unstructured and non-automated information exchanges (e.g., many hours spent on communication via telephone, fax, and email) and marked by a lack of consistency or standardization of data within and between health and social care domains (Onie et al., 2018). Where electronic information is available, the information technology systems are marked by a general absence of interoperability and by unequal investments in information management infrastructure for different types of providers (NCCBH, 2012). However, relying on manual approaches to coordinate information in the support of integrated care is costly, inefficient, and difficult to scale, thus limiting the seamless implementation of near-upstream approaches to addressing social needs.
By leveraging data and technology, the health care sector and its social care partners have an opportunity to improve the efficiency, effectiveness, and sustainability of efforts that address health-related social needs as a regular component of health care delivery (Dameff et al., 2019). In this chapter, the committee has identified critical opportunities that must be addressed in order to create an environment in which data and
digital tools have the potential to meaningfully affect social care integration into health care, leading to a more effective and efficient set of care models. These opportunities also stand to improve the experience for the people served and the workforce serving them.
LAYING THE FOUNDATION FOR DATA AND TECHNOLOGY TO DRIVE SOCIAL CARE INTEGRATION IN HEALTH CARE
The past decade has seen a dramatic technological transformation within the health care sector, driven by large-scale federal policy and, more recently, by new payment models in both the public and private sectors that incentivize major investments in building core information infrastructure in order to better manage patient populations. The federal government has played a substantial role in steering and financing the digitization of the health care experience for Americans. The Health Information Technology for Economic and Clinical Health (HITECH) Act of 20091 stimulated unprecedented growth in the adoption of electronic health records (EHRs) through a combination of policies, programs, incentives, and penalties. “As of 2017, nearly 9 in 10 (86 percent) of office-based physicians had adopted any EHR, and nearly 4 in 5 (80%) had adopted a certified EHR. Since 2008, office-based physician adoption of any EHRs has more than doubled, from 42% to 86%” (ONC, 2019). The wide adoption of EHRs and electronic information as a more ubiquitous component of many aspects of health care delivery and operations now presents opportunities to harness the power of big data to continuously improve care quality, efficiency, and health outcomes (IOM, 2013).
Federal policy driven by Congress and the U.S. Department of Health and Human Services (HHS) has created a supportive environment for the improved use of data and technology to optimize the health care experience, with a focus on promoting interoperability between disparate systems and providing consumers electronic access to their health and other information. The Centers for Medicare & Medicaid Services (CMS) has provided financial support for and required the use of certified EHR technology by eligible professionals and hospitals under the Medicare and Medicaid EHR Incentive and Promoting Interoperability programs (CMS, 2019c). CMS efforts are coupled with policy efforts by The Office of the National Coordinator for Health Information Technology (ONC), which oversees health information technology (IT) certification and has recently shifted from a focus on driving EHR adoption to
___________________
1 Health Information Technology for Economic and Clinical Health Act. Public Law 111-5, § 13001, 111th Cong. (February 12, 2009).
encouraging the availability of clinical data for providers, payers, and patients (Washington et al., 2017).
ONC was tasked by the 21st Century Cures Act of 20162 to develop a trusted exchange framework to significantly improve data sharing and to administer penalties to any entity engaged in data-blocking practices, such as vendors requesting excessive fees to access health data (Rucker, 2018). This legislation also codified the use of open application program interface (API) technology to connect third-party apps to health IT systems in the same way many popular commercial applications use APIs to connect and share data across disparate apps (e.g., Google Maps and Uber). In the spring of 2019, ONC and CMS released notices of proposed rulemaking to advance interoperability, as directed by the 21st Century Cures Act; if finalized as proposed, insurers that offer qualified health plans through and outside of the federal marketplace, Medicare Advantage plans, Medicaid- and Children’s Health Insurance Program (CHIP)managed care organizations, and state Medicaid and CHIP agencies that offer fee-for-service programs would be required to implement an open API to allow third-party app access to claims data when such access has been approved by the patient (CMS, 2019b).
HHS is not the only agency with health data under its purview; the Federal Health Architecture (FHA), which is transitioning to the Federal Health IT Coordinating Committee, supports interagency collaboration at the federal level and coordinates among more than 20 federal agencies to enhance health information exchange and coordinate services (ONC, 2018). For example, the Blue Button initiative started in 2010 as an effort by the U.S. Department of Veterans Affairs (VA) to give veterans more ready access to their medical records; HHS expanded upon the standards developed by the VA to give patients view, download, and transmit access to their health data in a standard format (ONC, 2014). CMS is now advancing Blue Button 2.0, an initiative that uses standards-based API technology to enable patients to share their medical data with trusted apps and programs (CMS, 2019a).
Federal policies to advance interoperable health data systems have been joined by innovation in the private sector, including the exponentially growing capacity of cloud-based data storage and associated big data analytic opportunities. The past decade has seen a dramatic evolution of computing and analytic technologies, which promises to unveil new insights and interventions previously unavailable with traditional research methods and data availability (Raghupathi and Raghupathi, 2014). Artificial intelligence and machine-learning techniques have substantial potential to transform the use of health care data by enabling much more
___________________
2 21st Century Cures Act. Public Law 114-255, 114th Cong. (December 13, 2016).
sophisticated analytics to drive targeted interventions and improve efficiency (Beam and Kohane, 2018).
The private sector has been an important partner in federal efforts to improve data availability for individual-level care and population health. Such efforts as the High Level 7 (HL7) Argonaut Project3 and the CARIN Alliance4 are advancing data standards and technological capabilities and working to develop a “trust framework” that allows consumers’ data to be in machine-readable format and able to be aggregated by a trusted app or other third party (Dameff et al., 2019). The regulatory framework that HHS has proposed would promote greater use of third parties such as health information exchange organizations that can aggregate data across disparate systems to create longitudinal health records and that could also incorporate social care data. Venture capital firms have also invested heavily in health technology—with nearly $8.1 billion invested in digital health startups in 2018 alone—and have evinced a growing interest in platforms that support integrated care for patient populations with unmet social needs (Day and Zweig, 2018). As one example, Town Hall Ventures seeks to partner with mission-driven entrepreneurs and targets its investments in “businesses that serve underserved populations … [including] a range of opportunities across health care technology and services, as well as areas which address social determinants of health” (Town Hall Ventures, 2019). It remains to be seen whether using private capital in the social care arena will result in equitable improvements in access, or instead aggravate existing disparities in the health and social care systems.
This creation of a digitized health care system is associated with a growing set of opportunities to leverage data and digital tools that can not only improve health care, but also support efforts aimed at identifying social risks and addressing social needs along the spectrum described in Chapter 2. As other sectors, particularly those involved with the consumer experience (e.g., retail, banking, and entertainment), have become digitized, there has become a largely untapped opportunity to better incorporate data from multiple sources beyond the EHR to establish a broader view of the health status of individuals and communities, inclusive of health-related social factors. For example, eligibility and enrollment files for social services programs and experiences with care and services all may contribute to creating a more complete picture of individuals’ health needs and drivers. In addition, there is a flurry of activity aimed at using other data, including community-level information such as hardship indices or information on the availability of healthy food or public transportation. Other efforts are using personal and community
___________________
retail patterns (Messer et al., 2006). Researchers and businesses are exploring the potential of using patient- and neighborhood-level social need data to inform risk models and predict the need for wrap-around interventions or referrals to social services (Kasthurirathne et al., 2018).
The value of advanced analytic approaches in driving effective resource deployment and service delivery will depend on the quality and comprehensiveness of the available data. As an example, health care claims and encounter data, which are often used to risk-stratify patients for population health interventions, have limited utility in predicting hospital readmissions for individuals with social risk factors like homelessness or social isolation because information about social risk factors is more likely to be found in clinical notes (Navathe et al., 2018). Administrative data have even less value in identifying the need for or use of social care services for most people with social needs. Thus, efforts to enrich core datasets to include sociodemographics, family caregiver status, social interactions, consumer habits, and even social media use will be key to unlocking the potential of analytic tools and care models (Beam and Kohane, 2018).
Beyond the data and their application are new digital tools that are only just beginning to be used to address social risks and social needs. Smartphones, mobile technology, and the Internet are becoming more available even in low-income communities, and patients and their caregivers are increasingly accustomed to accessing information and services through a digital layer (Pew Research Center, 2019). The ease of use, autonomy, and flexibility that technology provides has transformed virtually every domain of modern life—from the way that most people shop to the way they maintain connections with friends and family. One notable exception to this is in accessing and coordinating health care and social care services. Yet, it is precisely in this space where the potential of technology to meaningfully enhance the provider and consumer experience is so great. Technology can help reduce the cognitive burden that individuals experience when having to navigate complex, disconnected systems to access health care and social care services by streamlining consent processes and information sharing (Shah et al., 2018). Unfortunately, much of the promise of big data and analytics for integrating social care with health care remains unrealized (NAAAA, 2015).
THE EVOLVING ROLE OF DATA AND TECHNOLOGY IN ENHANCING SOCIAL CARE AND ITS INTEGRATION IN HEALTH CARE
In Chapter 2 the committee identified five complementary types of activities that health care systems can adopt to strengthen social care integration—awareness, adjustment, assistance, alignment, and advocacy.
Data and technology are already being leveraged in each of these areas and will have an increasingly important role to play across the spectrum of integration. In this section the committee provides examples of data sources and technology applications that may improve the effectiveness and efficiency of field efforts to address the social determinants of health (SDOH) in the health care environment. These uses of data and digital tools also stand to improve the ability to systematically evaluate care and financing models and build a stronger evidence base to support integration (see Table 4-1). The digital systems for the social care environment should be developed building on lessons learned from federal efforts to digitize the health care system (Reisman, 2017). These lessons include from the outset requiring non-proprietary standards to enable
TABLE 4-1
Potential Sources of Data and Digital Tools to Support the Integration of Social Care into Health Care
| Social Care Integration Spectrum | Potential Data Sources | |||
|---|---|---|---|---|
| Health care claims | Structured and unstructured data from electronic health record | Social determinants data from surveys | Retail and purchasing data | |
| Awareness | X | X | X | X |
| Adjustment | X | X | X | X |
| Assistance | X | X | X | X |
| Alignment | X | X | X | X |
| Advocacy | X | X | X | X |
| Social Care Integration Spectrum | Potential Applied Analytic and Technology Tools | |||
| Predictive analytics | Natural-language processing of unstructured data | Geocoding/hotspotting | Point-of-care decision support | |
| Awareness | X | X | X | |
| Adjustment | X | X | X | |
| Assistance | X | X | X | X |
| Alignment | X | X | ||
| Advocacy | X | X | X | X |
interoperability and setting expectations of data sharing as a condition of participation in the health ecosystem. The digital systems should also be developed with input from persons with expertise in social care.
Awareness
Data and digital tools are instrumental to increasing the health care sector’s awareness of social risks. The tools and processes needed to facilitate the systematic assessment of individual-level, health-related social needs is an area of active development. A better understanding of a person’s social context is integral to identifying the presence of risk factors, such as food insecurity or exposure to violence that can have a substantial
| Community-level information (e.g., census) | Evidence-based protocols for decision support | Eligibility criteria for social services programs | Health and social program enrollment options | Local social determinants of health findings | Local public policy and statutes |
| X | |||||
| X | X | ||||
| X | X | X | X | ||
| X | X | X | X | X | X |
| X | X | X | X | X | X |
| Augmented intelligence | Internet of Things | Telehealth and other virtual care | Automated interactions (chat bots, holograms) | Drones and self-driving cars | Digital platforms for interoperability |
| X | X | ||||
| X | X | X | |||
| X | X | X | X | X | |
| X | X | X | X | X | |
| X | |||||
effect on the efficacy of care plans and health outcomes (Billioux et al., 2017). The identification of social factors that relate to health risk is an essential first step toward fulfilling unmet social needs and improving health by connecting people with the social care services. Such needs may occur at the patient level or at the neighborhood and community level, and thus efforts to collect both types of data may help increase awareness. The strengths and limitations of each approach are summarized in Table 4-2.
Most approaches to increasing the awareness of social risks within the health care sector have relied on patient-level data collected through surveys administered during the course of patients’ engagement with the health system (Freij et al., 2018; Gottlieb et al., 2018) (see Chapter 2 for examples; also see Box 4-1). Such approaches are endorsed by professional and medical organizations in the United States, but they have not been widely implemented or formally evaluated (AAFP, 2019a; Daniel et al., 2018).
The health care sector has been active in testing and learning the best approaches for deploying technology to identify social risk, though there is not yet a best practice or standard. While substantial progress has been made in better assessing social and environmental risk factors as a means of predicting and improving health outcomes, there remain many challenges with screening mechanisms and the utility and reliability of the data they produce (Byhoff et al., 2018; Gottlieb et al., 2018). As noted in Chapter 2, when individuals interact with the health care system, it presents an opportunity to screen them for social risk information, but there are few standard instruments and minimal research to support the validity of such screening tools.
Part of building screening capabilities into the clinical workflow includes the integration of data on health-related social risks into the EHR, which already houses important medical information. Federally qualified health centers (FQHCs) have been early adopters of tools to assess the social risk of the underserved patient populations served by these organizations; the Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences (PRAPARE) assessment tool developed by the National Association of Community Health Centers (see Box 4-1) helps FQHCs better coordinate clinical and non-clinical care by collecting and documenting social risk data in the EHR (NACHC et al., 2016).
Currently, no uniform, accepted data model exists for representing social determinants in an EHR (Cantor and Thorpe, 2018). Therefore, while the benefits to EHR integration are numerous, the investment required to successfully achieve functional integration can be substantial (Gold et al., 2018) (also see Chapter 6). A standard for non-medical data is integral to translation of social determinants information into meaningful
TABLE 4-2
Strengths and Limitations of Patient- and Neighborhood-Level Social Determinants of Health Data Application
| Health Data | Patient-Level Interventions | Neighborhood-Level Interventions |
|---|---|---|
| Patient-level data | Strengths: Screening data collected directly from patients are likely more sensitive and specific to condition. Screening and intervention are both in context of shared clinical decision making, so can more closely tie interventions to patients’ priority needs. |
Strengths: Using a patient lens may increase the health care system’s engagement in upstream activities. Data may be more quickly accessible and aggregated. |
| Limitations: Cost of screening entire clinical population. Sampling bias and social desirability bias may affect patients’ responses to health care practitioners. High cost of intervening at individual level to address neighborhood-level issues (e.g., housing inadequacy, food deserts). |
Limitations: Sampling bias and social desirability bias may affect patients’ responses to health care practitioners. Subject to “exception fallacy”: Patients from health care system may not reflect neighborhood population adequately. |
|
| Neighborhood-level data | Strengths: Increases health care system’s engagement in upstream, neighborhood-level activities. Potential to focus on entire population facing health consequences, which could enhance value of interventions. |
Strengths: Uses a population-level lens; may be more “objective.” More capacity to affect population-level change. |
| Limitations: Subject to “ecological fallacy”: Some patients in this neighborhood may not be at higher risk. Lack of timely and detailed data limits depth of understanding. Potential to increase stigma. Potential to reinforce inequity across factors other than neighborhood (i.e., easier to intervene on behalf of relatively healthier individuals in the same neighborhood). |
Limitations: Can use only social determinants of health data that are available (practitioner has less control over how data are collected). May not have a direct impact on health system’s catchment population. Lack of timely data limits ability to monitor and adjust interventions. |
|
SOURCE: Gottlieb et al., 2018. Reprinted with permission from The Permanente Journal.
outcomes or conditions (akin to ICD-10 codes for medical diagnoses) that lend themselves to clinical response; yet, many codes exist that describe social determinants with different coding vocabularies (Arons et al., 2018). Efforts are under way to develop documentation standards and to better align coding vocabularies used in EHRs in order to improve interoperability in this area (IOM, 2014). One such effort is the Gravity Project, led by the Social Interventions Research and Evaluation Network (SIREN), with funding from the Robert Wood Johnson Foundation, which is aimed at developing consensus-based code recommendations for capturing data on food security, housing stability and quality, and transportation access and to ultimately inform an HL7 Fast Healthcare Interoperability Resource implementation guide for priority-use cases (SIREN, 2019).
Ideally, integration of standardized data into EHRs will enable such functionalities as automatic referral to community-based organizations; however, this type of integration with entities outside the health care system will require an increased capacity of community-based organizations to comply with privacy and security standards related to the sharing of protected health information (PHI) as well as the health care sector’s willingness to share data. The Office for Civil Rights (OCR) governs the Health Insurance Portability and Accountability Act (HIPAA) and recently solicited public comments in a request for information on provisions of the privacy and security regulations that may impede transformation to a value-based health care system. The request for information noted that some HIPAA-covered entities have been reluctant to share PHI for care coordination purposes for fear of violating HIPAA, even though the rules
currently permit disclosure to third parties such as social service agencies or community-based support programs for the purpose of coordinating care and related services (HHS, 2018). OCR also solicited recommendations for improved HIPAA training for covered entities, which could address the knowledge gap in what data-sharing activities are currently permissible.
Organizations also are using big data from a wide range of sources and sectors to paint a detailed picture of social risks and needs at the population level in order to inform place-based community improvement strategies as well as individual interventions. Various tools are in use to integrate neighborhood-level data into EHRs to help inform patient-level interventions. Geographic information system (GIS) tools such as HealthLandscape (AAFP, 2019b) and Texas A&M University’s GeoServices (TAMU, 2019) allow for the analysis of geocoded patient datasets (Robert Grahm Center, 2019). These social risk assessment approaches may, for example, help alleviate the burden of primary screening and enhance population-level interventions within the public and private sectors targeted to the zip code level (Auger et al., 2017). They also can be used to track institutional progress on addressing disparities among target communities (Abu-Saad et al., 2018; Cookson et al., 2018; Hanak, 2018). In the case of the Flint water crisis, GIS tools were used to improve the validity of a blood lead level study by analyzing patient data from the precise neighborhoods that had been switched to tap water supplied from a more corrosive source (Hanna-Attisha et al., 2016).
The more common approaches of individual-level data collection for population health surveillance are time and resource-intensive, typically involving either a prolonged face-to-face interaction between the surveyor and the patient or the self-completion of paper surveys directly by patients, with the surveys manually entered and recorded into a database (Richards et al., 2017). The trade-offs between these two approaches of individual-level data collection largely involve compromising either efficiency, in the former case, or the quality and precision of the data gathered in the latter. For example, completing such surveys may add time to the clinical encounter and detract from the time that patients have available to interact with the care team (NASDOH, 2019). There are other challenges as well, including the burden on the patients who are asked to repeatedly describe their social needs, which in some cases may cause them embarrassment or a loss of dignity.
Adjustment
Understanding social risk and social need is only the beginning of addressing those issues. Health systems are deploying data and technology
strategies to support the development of individualized care plans and inform clinical care decision making. An immediate benefit derived from assessing social risk is the adjustment of clinical care plans to accommodate for social needs. In making such adjustments, doctors and other clinicians need patients’ social risk information to inform their diagnostic and care plan. As an example, people who are homeless may have their diabetic therapeutic regimens hampered by the addition of insulin because they do not have an easy opportunity to store insulin. When transportation poses a barrier to accessing care, a clinician may choose to call a patient to follow up on results of laboratory or diagnostic tests rather than expecting the patient to present for an in-person follow up visit. In addition to using patient-level data to inform patient-level interventions, neighborhood-level data also may help tailor care to maximize the chance of success (see Box 4-2).
Assistance
The health care system is deploying a range of data and technological interventions to assist patients in connecting with resources to address social needs. One evolving area with substantial potential for influence is the development of new technologies to mediate virtual interactions
between individuals and care teams, as well as to deliver goods and services (National Interoperability Collaborative, 2019). When applied to health and social care, these technologies hold the potential to improve access, reduce transaction costs, and enhance engagement. In some clinical environments, this includes the use of tools that have digitized resource guides that make the information searchable and allow for the identification of resources that match patient characteristics such as location, language, or access on public transportation (Alley et al., 2016). Digital resource guides available on the market include those that are produced with community input on available resources and increasingly allow for individuals to “rate” services provided by the social care organizations.
As the health sector transitions to more value-based payment arrangements that hold providers accountable for patient outcomes and the total cost of care, providers and payers have greater incentive to assist patients in addressing unmet social needs. The health sector must decide whether to build capacity to directly assist patients’ non-medical needs or, alternatively, to partner with community-based organizations that have experience in addressing social needs and the necessary capacity to address those needs. In the latter scenario, the health sector will also need to consider what data systems can be used in partnering with social care providers. North Carolina, through a public–private partnership, is establishing a shared utility for plans and providers to use across all populations and payers, including Medicare, Medicaid, and commercially insured and uninsured populations, to assist in making referrals to social service providers; one purpose is to avoid the need for each plan and provider to establish a separate referral platform. The referral platform will have a digitized resource directory and a feedback regulated referral functionality to track the outcome of the referrals and collect data on the delivery of social care. As North Carolina transitions to Medicaid managed care in the latter part of 2019, the North Carolina Medicaid program will use this shared utility for the state’s Medicaid plans and providers. The state’s technology-facilitated assistance platform, NCCARE360, is described in Box 4-3.
Alignment
The committee defined alignment activities as those generally led by health care organizations working to organize social care providers and services in their area. The ultimate goal is to harmonize activity, services, and funding for these resources in order to maximize effectiveness. An example of an organization involved in such an alignment approach—the Route 66 Consortium—is presented in Box 4-4. Because these alignment efforts extend beyond the support of individuals, community-level data
including asset maps of local social services and geocoded data population health needs are needed to connect people with social needs with the appropriate resources. Such work will require the sharing of health and social care information across a wide array of community partners and with the consumer. In addition to the use of digital-sharing platforms, the work will benefit from the regular updating of resource guides to keep them current, with care providers’ contact information, eligibility criteria, and online enrollment platforms. Social service resource lists that are integrated into the EHR and platforms that support closed-loop referrals (where only the specialist and primary care provider are involved) can support successful care coordination when individuals face care hand-offs between health care and social care providers. Alignment models will also benefit from shared data repositories that can be accessed by all partners to inform the development of resources to fill gaps or reduce redundancy in services identified in asset mapping.
Advocacy
The committee defined advocacy activities as those in which health care–related organizations work with partner social care agencies to create, develop, or redeploy assets or resources to address health and social care needs. Such changes involve systems-level changes that can affect the community as a whole and therefore require data and digital tools that transcend individual-level information and provide population-level asset and geographic data to enhance alignment models. Advocacy
efforts will be best supported by data from inventories of existing local and national best practices of legal and policy frameworks to inform opportunities for change such as in housing policy or transportation (CDC, 2019). These efforts will need to include data resources that are in community-based organizations and governmental organizations that are not typically sharing data with health care, such as departments of urban planning, environment, public works, education, and transportation. The work of the Louisville AIR project and how it addressed asthma with technology, crowdsourcing, cross-sector collaboration, and policy is one such example (see Box 4-5).
CHALLENGES
The committee identified a number of challenges that health care and social care systems are facing in working to use data and technology as part of their efforts to integrate care and services across the continuum, which have been discussed throughout this chapter. None of these challenges is insurmountable, but overcoming them will require deliberate action by policy makers and the private sector. Some will likely also require considerable financial investment. Some of the key challenges are:
- Access to sufficient social services data and digital infrastructure. HITECH provided billions of dollars to support the
-
transformational digitization of the U.S. health care sector, thus rapidly accelerating the uptake of digital technology by health care providers. The social services sector did not benefit from these funds, and in most cases the IT infrastructure of community-based organizations that provide services is incapable of meeting the data standards, cybersecurity, and other technological needs to build a robust health care and social care data sharing infrastructure (Amarasingham et al., 2018).
- Lack of data standards for social determinants of health. “Vendors that are developing products to facilitate the collection and use of social determinants of health data are seeking solutions to data standardization and interoperability challenges” (Freij et al., 2018, p. 2).
- Interoperability. The interoperability of health care data continues to improve year over year in the United States, but it still does not meet expectations. This is due largely to business decisions that cause the health care sector to block data. However, efforts to create business incentives for data sharing at the federal level in concert with private-sector action is showing progress (AHA, 2019). The interoperability landscape is already working to build a trust framework and set of incentives for sharing data between health and social care systems. As such, going forward the health care and social sectors will need to agree upon a shared trust framework for data exchange, sharing, and use. Part of building a transparent trust framework will be the need to have meaningful informed consent for individuals (California Governor’s Office of Planning and Research, 2018; Illinois Department of Human Services, 2013).
- Privacy and security. The data used in some models of social care information will move between health care systems and social services partners who are unaccustomed to the regulatory expectations included in HIPAA that govern the protection of personally identifiable data (see Figure 4-1). All of the organizations involved in this data sharing will need technical assistance to build informed consent for individuals and data sharing arrangements that can support information flow. In addition, some of the data that will be shared or included in risk prediction models will fall outside of HIPAA protections and therefore may require additional regulatory or statutory action (IOM, 2009).
- Data and technology skills for workforce and patients. As has been the case with the digitization of other human capital intensive industries, technology can enable skilled workers to focus on more technically complex activities while expanding access and
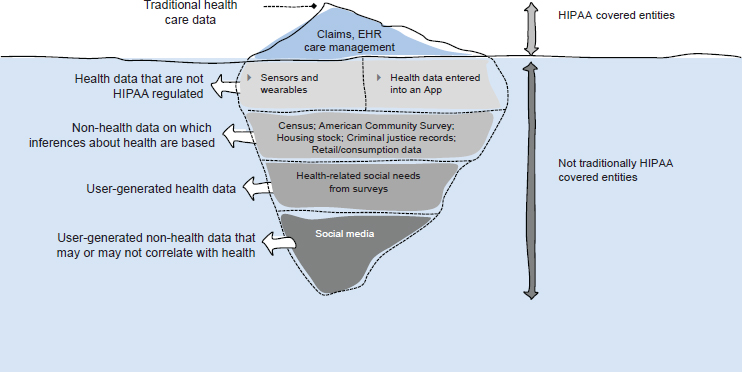
NOTE: HIPPA = Health Insurance Portability and Accountability Act.
SOURCE: Adapted from Price and Cohen, 2019. Reprinted with permission from Nature Medicine.
- Consumer demand and expectations. Amid the excitement on the payer and provider side concerning digital technology and its potential to improve the efficiency of resource deployment and overall health outcomes, there has been very little investigation of consumer desires and expectations. It remains to be seen whether and how individual patients (consumers) will embrace the use of data and technology to integrate services in some of the most personal, intimate parts of their lives. As an example, some individuals may not want their physician to know whether they receive meals from a food pantry or how often they sleep in a shelter. Others might be very uncomfortable to know that their health plan is gathering data on their credit score and grocery purchases to determine what type of care management services to offer them.
enhancing operational efficiency. But, to achieve that goal, the health care and social care incumbent and emerging workforce will need to be comfortable with data and technology. Though people working in the health care sector have become more accustomed to and comfortable with data and technology (as a result of the increased utilization of EHRs), the social care sector lags behind in these capabilities and will require adequate training and peer champions to ease the transition (Wyman and SeaChange Capital Partners, 2017).
- Balancing technology and human capital investments. Data and technology stand to accelerate the care models that can address and, where needed, mitigate the social factors that influence health. But data and technology alone are not the solution. Absent humanity, those truly with need will not be helped. Technology cannot and should not be a replacement for trusted human relationships. The goal should be to augment human capital and processes rather than supplant them.
- Inequitable access to technology and unintended consequences. There are instances when digitizing the social and health care infrastructure can result in negative consequences and exacerbate disparities. Such is the case where states have implemented Medicaid work requirements and required beneficiaries to report work hours online. In Arkansas, which has seen Medicaid coverage losses because of conditioning eligibility on work requirements (Rudowitz et al., 2019), more than half (53 percent) of nonexempt Medicaid beneficiaries that are working the required number of hours still face difficulty complying with the reporting requirement because they are in households with no broadband Internet access (Gangopadhyaya et al., 2018).
- Ethics of social risk profiling. Finally, potentially serious ethical considerations will need to be addressed in the application of artificial intelligence and other modalities in decision making and resource allocation for integrating social care into health care (Char et al., 2018; Gottlieb and Alderwick, 2019). Of particular concern is the risk that these technologies replicate or exacerbate the biases within the current social and health care systems that result in disparities in outcomes on the basis of race and ethnicity, sexual orientation, gender identity, history of trauma, or other status.
FINDINGS
- Data and technology have transformed the consumer experience in many sectors of life and are doing so in health care. This is only the beginning of a journey that has unlimited potential to use data and technology to improve effectiveness and transform the consumer experience.
- Billions of dollars in federal resources spurred the digitization of health care through the widespread adoption of the electronic health records and interoperability. Social care has not benefited from the same resources and policy attention as has the health care sector, and it lags far behind in digitization.
- Private equity has supported the health technology economy. Venture capitalists are increasingly investing in health technology startup companies that are working to address the social determinants of health.
- Local efforts to share health care and social care data exist, including an emerging set of private-sector solutions. These are not supported by a strategic national vision, nor coupled with resources or defined technology standards.
- Interoperability and data sharing between health care and social care are hampered by the lack of infrastructure, data standards, and modern technology architecture shared between and among organizations.
- With an increasing number of stakeholders sharing protected health information in order to coordinate care, data privacy and security remain challenging elements to manage. Concerns about compliance with regulations such as those governing health care data (e.g., Health Insurance Portability and Accountability Act information) and social data (e.g., educational information) are barriers to sharing at the local level.
- The deployment of digital approaches to integrating social care into health care may increase existing health disparities by exacerbating the digital divide or codifying bias within health and social systems.
- There is a paucity of rigorous research that can inform a collective understanding of best practices and outcomes of efforts to integrate social care with health care. Access to data will be critical to codifying approaches, quality assurance, and the dissemination of learnings—thus supporting more effective approaches to measuring outcomes, promoting equity, and informing resource allocation and policy.
REFERENCES
AAFP (American Academy of Family Physicians). 2019a. The EveryONE Project tool kit. https://www.aafp.org/patient-care/social-determinants-of-health/everyone-project/eop-tools.html (accessed May 22, 2019).
AAFP. 2019b. Turning statistics into information: HealthLandsdcape. https://www.healthlandscape.org (accessed April 15, 2019).
Abu-Saad, K., S. Avni, and O. Kalter-Leibovici. 2018. Health disparities monitoring in the U.S.: Lessons for monitoring efforts in Israel and other countries. Israel Journal of Health Policy Research 7(1):14.
AHA (American Hospital Association). 2019. Sharing data, saving lives: The hospital agenda for interoperability. https://www.aha.org/system/files/2019-01/Report01_18_19-Sharing-Data-Saving-Lives_FINAL.pdf (accessed May 22, 2019).
Alley, D. E., C. N. Asomugha, P. H. Conway, and D. M. Sanghavi. 2016. Accountable health communities—Addressing social needs through Medicare and Medicaid. New England Journal of Medicine 374(1):8–11.
Amarasingham, R., B. Kapoor, A. Karam, N. Nguyen, and B. Xie. 2018. Using community partnerships to integrate health and social services for high-need, high-cost patients. The Commonwealth Fund issue brief, January. https://www.commonwealthfund.org/sites/default/files/documents/___media_files_publications_issue_brief_2018_jan_amarasingham_integrating_health_social_services_high_need_high_cost_ib.pdf (accessed May 22, 2019).
Arons, A., S. DeSilvey, C. Fichtenberg, and L. Gottlieb. 2018. Documenting social determinants of health-related clinical activities using standardized medical vocabularies. Journal of the American Medical Informatics Association Open 2(1):81–88.
Auger, K. A., R. S. Kahn, J. M. Simmons, B. Huang, A. N. Shah, K. Timmons, and A. F. Beck. 2017. Using address information to identify hardships reported by families of children hospitalized with asthma. Academic Pediatrics 17(1):79–87.
Barrett, M., V. Combs, J. G. Su, K. Henderson, M. Tuffli, and AIR Louisville Collaborative. 2018. AIR Louisville: Addressing asthma with technology, crowdsourcing, cross-sector collaboration, and policy. Health Affairs (Millwood) 37(4):525–534.
Beam, A. L., and I. S. Kohane. 2018. Big data and machine learning in health care. JAMA 319(13):1317–1318.
Billioux, A., K. Verlander, S. Anthony, and D. Alley. 2017. Standardized screening for health-related social needs in clinical settings: The accountable health communities screening tool. Discussion Paper, National Academy of Medicine, Washington, DC. https://nam.edu/wp-content/uploads/2017/05/Standardized-Screening-for-Health-Related-Social-Needs-in-Clinical-Settings.pdf (accessed May 22, 2019).
Byhoff, E., A. J. Cohen, M. C. Hamati, J. Tatko, M. M. Davis, and R. Tipirneni. 2018. Screening for social determinants of health in Michigan health centers. Journal of the American Board of Family Medicine 30:418–427.
California Governor’s Office of Planning and Research. 2018. Precision medicine: An action plan for California. http://opr.ca.gov/docs/20190107-Precision_Medicine_An_Action_Plan_for_California.pdf (accessed May 22, 2019).
Cantor, M. N., and L. Thorpe. 2018. Integrating data on social determinants of health into electronic health records. Health Affairs (Millwood) 37(4):585–590.
CARIN Alliance. 2019. CARIN alliance. https://www.carinalliance.com (accessed March 18, 2019).
CDC (Centers for Disease Control and Prevention). 2019. Public health law. https://www.cdc.gov/phlp/publications/topic/index.html (accessed April 15, 2019).
Char, D. S., N. H. Shah, and D. Magnus. 2018. Implementing machine learning in health care—Addressing ethical challenges. New England Journal of Medicine 378(11):979–981.
CMS (Centers for Medicare & Medicaid Services). 2019a. Blue Button 2.0. https://bluebutton.cms.gov/#overview (accessed February 21, 2019).
CMS. 2019b. Medicare and Medicaid programs; Patient Protection and Affordable Care Act; interoperability and patient access for Medicare Advantage Organization and Medicaid managed care plans, state Medicaid agencies, CHIP agencies and CHIP managed care entities, issuers of qualified health plans in the federally-facilitated exchanges and health care providers. Federal Register. https://www.federalregister.gov/documents/2019/03/04/2019-02200/medicare-and-medicaid-programs-patient-protection-and-affordable-care-act-interoperability-and (accessed May 22, 2019).
CMS. 2019c. Promoting interoperability. https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/index.html (accessed April 12, 2019).
Cookson, R., M. Asaria, S. Ali, R. Shaw, T. Doran, and P. Goldblatt. 2018. Health equity monitoring for healthcare quality assurance. Social Science & Medicine 198:148–156.
Dameff, C., B. Clay, and C. A. Longhurst. 2019. Personal health records: More promising in the smartphone era? JAMA 321(4):339–340.
Daniel, H., S. S. Bornstein, G. C. Kane, Health and Public Policy Committee of the American College of Physicians. 2018. Addressing social determinants to improve patient care and promote health equity: An American College of Physicians position paper. Annals of Internal Medicine 168(8):577–578.
Day, S., and M. Zweig. 2018. 2018 Year End Funding Report: Is digital health in a bubble? In Rock Health: Reports. https://rockhealth.com/reports/2018-year-end-funding-report-is-digital-health-in-a-bubble (accessed April 15, 2019).
Freij, M., P. Dullabh, L. Hovey, J. Leonard, A. Card, and R. Dhopeshwarkar. 2018. Incorporating social determinants of health in electronic health records: A qualitative study of perspectives on current practices among top vendors. Report prepared for Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services. https://aspe.hhs.gov/system/files/pdf/259901/NORCSDH.pdf (accessed May 22, 2019).
Gangopadhyaya, A., G. M. Kenney, R. A. Burton, and J. Marks. 2018. Medicaid work requirements in Arkansas. The Urban Institute. https://www.urban.org/research/publication/medicaid-work-requirements-arkansas (accessed May 22, 2019).
Gold, R., A. Bruce, S. Cowburn, K. Dambrun, M. Dearing, M. Middendorf, N. Mossman, C. Hollombe, P. Mahr, G. Melgar, J. Davis, L. Gottlieb, and E. Cotrell. 2018. Adoption of social determinants of health EHR tools by community health centers. Annals of Family Medicine 16(5):399–407.
Gottlieb, L. M., and H. Alderwick. 2019. Integrating social and medical care: Could it worsen health and increase inequity. Annals of Family Medicine 17(1):77–81.
Gottlieb, L. M., D. E. Francis, and A. F. Beck. 2018. Uses and misuses of patient- and neighborhood-level social determinants of health data. The Permanente Journal 22:18-078.
Hanak, M. 2018. The numbers tell a story: How to use data to achieve health equity. Improvement Blog: Institute for Healthcare Improvement. March 27. http://www.ihi.org/communities/blogs/the-numbers-tell-a-story-how-to-use-data-to-achieve-health-equity (accessed May 22, 2019).
Hanna-Attisha, M., J. LaChance, R. C. Sadler, and A. Champney Schnepp. 2016. Elevated blood lead levels in children associated with the Flint drinking water crisis: A spatial analysis of risk and public health response. American Journal of Public Health 106(2):283–290.
HHS (U.S. Department of Health and Human Services). 2018. Request for information on modifying HIPAA rules to improve coordinated care. https://www.federalregister.gov/documents/2018/12/14/2018-27162/request-for-information-on-modifying-hipaa-rules-to-improve-coordinated-care (accessed April 15, 2019).
HL7 International. 2019. Argo-2018-projects. http://argonautwiki.hl7.org/index.php?title=Argo-2018-Projects (accessed March 18, 2019).
Illinois Department of Human Services. 2013. Establishing governance for health and human services interoperability initiatives: A handbook for states. https://www.acf.hhs.gov/sites/default/files/assets/establishing_governance_for_hhs_handbook_508compliant_final.pdf (accessed May 22, 2019).
IOM (Institute of Medicine). 2009. Beyond the HIPAA privacy rule: Enhancing privacy, improving health through research. Washington, DC: The National Academies Press.
IOM. 2013. Digital data improvement priorities for continuous learning in health and health care: Workshop summary. Washington, DC: The National Academies Press.
IOM. 2014. Capturing social and behavioral domains and measures in electronic health records: Phase 2. Washington, DC: The National Academies Press.
Kasthurirathne, S. N., J. R. Vest, N. Menachemi, P. K. Halverson, and S. J. Grannis. 2018. Assessing the capacity of social determinants of health data to augment predictive models identifying patients in need of wraparound social services. Journal of the American Medical Informatics Association 25(1):47–53.
Messer, L. C., B. A. Laraia, J. S. Kaufman, J. Eyster, C. Holzman, J. Culhane, I. Elo, J. G. Burke, and P. O’Campo. 2006. The development of a standardized neighborhood deprivation index. Journal of Urban Health 83(6):1041–1062.
MyHealth Access Network. 2019. Accountable health communities—Route 66 Consortium. https://myhealthaccess.net/ahc (accessed April 15, 2019).
NAAAA (National Association of Area Agencies on Aging). 2015. Information technology in area agencies on aging—Report from the 2015 National AAA Survey. https://www.n4a.org/Files/UPDATE%20Information%20Technology%20in%20AAAs%20-%20Report%20from%202015%20National%20Survey.pdf (accessed May 22, 2019).
NACHC (National Association of Community Health Centers). 2019. PRAPARE implementation and action toolkit. http://www.nachc.org/research-and-data/prapare/toolkit (accessed May 22, 2019).
NACHC, Association of Asian Pacific Community Health Organizations, Oregon Primary Care Assocation, and Institute for Alternative Futures. 2016. Accelerating strategies to address the social determinants of health—Protocol for responding to and addessing patients’ assets, risks, and experiences. http://www.nachc.org/wp-content/uploads/2016/07/PRAPARE-Abstract-4-20-16.pdf (accessed May 22, 2019).
NASDOH (National Alliance to Impact the Social Determinants of Health). 2019. Identifying social risk and needs in health care. http://www.nasdoh.org/wp-content/uploads/2019/01/NASDOH-Social-Risks-Issue-Brief.pdf (access May 22, 2019).
National Interoperability Collaborative. 2019. Partnerships, programs, and platforms. https://www.academyhealth.org/sites/default/files/partnerships_programs_platforms_april2019.pdf (acessed May 22, 2019).
Navathe, A. S., F. Zhong, V. J. Lei, F. Y. Chang, M. Sordo, M. Topaz, S. B. Navathe, R. A. Rocha, and L. Zhou. 2018. Hospital readmission and social risk factors identified from physician notes. Health Services Research 53(2):1110–1136.
NC DHHS (North Carolina Department of Health and Human Services). 2019. NCCARE 360. https://www.ncdhhs.gov/about/department-initiatives/healthy-opportunities/nccare360 (accessed June 6, 2019).
NCCBH (National Council for Community Behavioral Healthcare). 2012. HIT adoption and readiness for meaningful use in community behavioral health—report on the 2012 National Council Survey. https://www.thenationalcouncil.org/wp-content/uploads/2012/10/HIT-Survey-Full-Report.pdf (accessed May 22, 2019).
ONC (The Office of the National Coordinator for Health Information Technology). 2014. Blue Button fact sheet. https://www.healthit.gov/sites/default/files/blue-button-fact-sheet-2014-feb_0.pdf (accessed May 22, 2019).
ONC. 2016. Update on the adoption of the health information technology and related efforts to facilitate the electronic use and exchange of health information. Report to Congress, February. https://www.healthit.gov/sites/default/files/Attachment_1_-_2-26-16_RTC_Health_IT_Progress.pdf (accessed May 22, 2019).
ONC. 2018. Federal health architecture (FHS). https://www.healthit.gov/topic/onc-hitech-programs/federal-health-architecture-fha (accessed April 15, 2019).
ONC. 2019. Office-based physician electronic health record adoption. http:///quickstats/pages/physician-ehr-adoption-trends.php (accessed June 6. 2019).
Onie, R. D., R. Lavizzo-Mourey, T. H. Lee, J. S. Marks, and R. J. Perla. 2018. Integrating social needs into health care: A twenty-year case study of adaptation and diffusion. Health Affairs 37(2):240–247.
Pew Research Center. 2019. Demographics of mobile device ownership and adoption in the United States. https://www.pewinternet.org/fact-sheet/mobile (accessed April 15, 2019).
Price, W. N., 2nd, and I. G. Cohen. 2019. Privacy in the age of medical big data. Nature Medicine 25(1):37–43.
Raghupathi, W., and V. Raghupathi. 2014. Big data analytics in healthcare: Promise and potential. Health Information Science and Systems 2(3):PMC4341817.
Reisman, M. 2017. EHRs: The challenge of making electronic data usable and interoperable. Pharmacy and Therapeutics 42(9):572–575.
Richards, C. L., M. F. Iademarco, D. Atkinson, R. W. Pinner, P. Yoon, W. R. Mac Kenzie, B. Lee, J. R. Qualters, and T. R. Frieden. 2017. Advances in public health surveillance and information dissemination at the Centers for Disease Control and Prevention. Public Health Reports 132(4):403–410.
Robert Grahm Center. 2019. Community oriented primary care (COPC) curriculum. https://www.graham-center.org/rgc/maps-data-tools/tools/copc.html (accessed March 20, 2019).
Rucker, D. 2018. Achieving the interoperability promise of 21st Century Cures. Health Affairs blog. https://www.healthaffairs.org/do/10.1377/hblog20180618.138568/full (accessed May 22, 2019).
Rudowitz, R., M. Musumeci, and C. Hall. 2019. February state data for Medicaid work requirements in Arkansas. Kaiser Family Foundation. https://www.kff.org/medicaid/issue-brief/state-data-for-medicaid-work-requirements-in-arkansas (accessed May 22, 2019).
Shah, A. K., J. Zhao, S. Mullainathan, and E. Shafir. 2018. Money in the mental lives of the poor. Social Cognition 36(1):4–19.
SIREN (Social Interventions Research and Evaluation Network). 2019. The Gravity Project. https://sirenetwork.ucsf.edu/TheGravityProject (accessed April 15, 2019).
TAMU (Texas A&M University). 2019. TAMU geoservices. http://geoservices.tamu.edu (accessed April 15, 2019).
Town Hall Ventures. 2019. What we do—Town Hall Ventures. https://www.townhallventures.com/what-we-do (accessed April 15, 2019).
Washington, V., K. DeSalvo, F. Mostashari, and D. Blumenthal. 2017. The HITECH era and the path forward. New England Journal of Medicine 377(10):901–904.
Wyman, O., and SeaChange Capital Partners. 2017. A national imperative: Joining forces to strengthen human services in America in 2018. Alliance for Strong Families and Communities and American Public Human Services Association. https://www.alliance1.org/web/resources/pubs/national-imperative-joining-forces-strengthen-human-services-america.aspx (accessed April 15, 2019).