
4
Interventions Addressing Food Insecurity
The workshop’s third panel featured short presentations by four panelists who spoke about different interventions designed to address food insecurity. The panelists were Seth A. Berkowitz, Assistant Professor
of Medicine in the Division of General Medicine and Clinical Epidemiology at the University of North Carolina at Chapel Hill School of Medicine; Allison Hess, Vice President for Health and Wellness at Geisinger Health; Andrew Renda, Associate Vice President of Population Health at Humana; and Kate Leone, Chief Government Relations Officer at Feeding America. A discussion and question-and-answer session, moderated by Karen DeSalvo, Professor of Medicine at The University of Texas at Austin Dell Medical School and co-convener of the National Alliance to Impact the Social Determinants of Health, followed the presentations.
FOOD INSECURITY AND HEALTH: CONSEQUENCES AND INTERVENTIONS
Food insecurity worsens health and is associated with increased incidence of diabetes, heart disease, high blood pressure, obesity, chronic kidney disease, and osteoporosis, said Seth A. Berkowitz as an explanation for why it is so important to address food insecurity. In addition, food insecurity can make disease management more difficult. For example, an individual undergoing cancer chemotherapy is not likely to recover as well and get the full benefit from the treatment without adequate nutrition. Moreover, the association between food insecurity and poor health often leads to higher health care utilization and higher health care costs, Berkowitz added. In fact, a study he and his colleagues conducted found that health care expenditures averaged $1,800 per year more for people with food insecurity compared to those who can access adequate nutrition (Berkowitz et al., 2018). This difference is often driven by higher inpatient admissions and higher emergency department (ED) utilization. “For these reasons, food insecurity has been a factor people have wanted to look at in programs to reduce adverse health care utilization,” he said.
While the effect of food insecurity on health is clear, how best to intervene is not, said Berkowitz. This statement was not meant to discount the numerous efforts to address hunger, but to point out that it has only been during the past 5 years or so that researchers have been conducting well-designed and rigorous studies to link food insecurity interventions with health outcomes. The evidence base, however, is growing with the publication of results from three randomized trials, each of which found important effects of diet quality on some patient-reported outcomes (Berkowitz et al., 2019; Hummel et al., 2018; Seligman et al., 2018). Ongoing studies, including one he is conducting, are examining how diet quality affects a variety of outcomes, including quality metrics, health care utilization, and cost.
The results from these and other studies are generating excitement around addressing food insecurity as a means of improving health out-
comes, but Berkowitz cautioned that it will take time to build the evidence base. He said,
We want to avoid hype and move from thinking about whether we should address [food insecurity] to what is the best way to address it, and that inevitably means we will find some ways that do not work so well on our way to finding other ways that do work well. I think we need to be prepared to be in this for the long haul and not give up the first time we start seeing the things that are not panning out exactly as expected or do not live up to inflated expectations, but realize that this is an evidence base that that is worth growing.
To Berkowitz, the goal should be to understand all aspects of return on investment (ROI), both in terms of health care dollars and health care utilization and regarding other outcomes such as patient-reported, health-related quality of life or quality metrics associated with disease control. Looking at the ROI from a broader perspective, he noted in closing, is necessary to understand the full effect of interventions to address food insecurity.
A NATIONAL VISION TO IMPROVE DIABETES HEALTH OUTCOMES USING FOOD AS MEDICINE
It is a fact of life today that many individuals do not earn enough to cover basic household expenses, said Allison Hess. Data from Feeding America show that 66 percent of its clients have had to choose between paying for medicine and buying food (Feeding America, 2019). “If you look at the data, there are many times when our patients are deciding whether they should eat or treat,” she said, noting that this is becoming increasingly common in some rural populations that do not have as many social services available as do urban populations.
Looking across clinical outcomes, Geisinger Health recognized that the extensive and comprehensive clinical work on improving type 2 diabetes management was not as successful as expected largely because patients were unable to consistently access healthy food for their very diet-responsive condition. Working with the Central Pennsylvania Food Bank, Hess and her colleagues established the Fresh Food Farmacy program that treats prescriptive food as medicine to treat type 2 diabetes (Feinberg et al., 2018; Hess et al., 2019). Reiterating comments from other speakers regarding the importance of working with community-based organizations, Hess explained that as a health care organization, Geisinger had limited knowledge about running a food pantry, which is why the collaboration with the Central Pennsylvania Food Bank was so important. This program is a great example of why strong collaboration between health care and social care is so important.
The Fresh Food Farmacy model has several key elements, said Hess. Identifying individuals who might be experiencing food insecurity is the first element, and Geisinger Health does this by embedding two questions about food insecurity in its electronic health record and asking them of every patient at every visit. The answers to those questions are then linked with clinical data to find those clients who have uncontrolled type 2 diabetes and who live in an area with one of its participating food banks. “We chose to stand up those Fresh Food Farmacies in geographies within our footprints that had high rates of food insecurity and high prevalence of uncontrolled type 2 diabetes,” she explained. These facilities are large—the most recent covers 5,000 square feet—and operate on a self-serve model much like shopping in a regular grocery store. Clients have options on which items to take home based on recipes and education the program provides.
Each week, clients receive 10 meals for themselves and their entire household. Hess noted the importance of providing a large majority of the food a patient needs given that type 2 diabetes is a diet-responsive condition. She also emphasized how critical it is to provide education and clinical support, as well as transportation. As an example of a typical outcome, she described how one patient named Rita, a 55-year-old married grandmother raising her three grandchildren, lowered her hemoglobin A1C from 12.8 to 5.4, lost 46 pounds, and reduced her low-density lipoprotein (LDL) cholesterol reading from 209 to 47 and triglyceride reading from 312 to a healthy 76. “Based on existing research that demonstrates an ROI of $8,000 to $12,000 per every one-point reduction [in A1C], it is easy to recognize that providing the food for this patient was definitely worth the long-term clinical and financial benefits,” said Hess.
In terms of clinical measures, Geisinger clients participating in the program are averaging a two-point reduction in A1C values and a 31.3 percent improvement in glucose measurements, in addition to achieving a 15.8 percent reduction in cholesterol levels, a 17 percent reduction in LDL levels, and a 24.3 percent reduction in serum triglycerides. All told, medical expenses fell between $16,000 and $24,000 per client. In addition, said Hess, overall compliance rates for adult prevention and diabetes quality measures rose significantly. Annual eye exams, for example, increased by 16 percent, annual foot exams rose by 24 percent, and mammograms increased by more than 7 percent, for patients enrolled in the program. She noted, too, that Geisinger is seeing a 74 percent difference in admission rates between its enrolled and nonenrolled client population, as well as a 27 percent difference in ED visits and an increase in visits to primary care physicians. Geisinger is now expanding the program to two additional cities.
A BOLD GOAL: IMPROVING HEALTH BY ADDRESSING FOOD INSECURITY
In 2014, Humana’s chief executive officer declared what has become known within the organization as the Bold Goal1: improve the health of the communities it serves by 20 percent using the Centers for Disease Control and Prevention’s Health Days tool as the metric.2 In some preliminary research, Andrew Renda and his colleagues combined Humana’s Healthy Days data with the County Health Rankings Report from the Robert Wood Johnson Foundation and looked to identify the social determinants that would have the biggest positive effect on health-related quality of life (Cordier et al., 2018). Loneliness was first, he said, and food insecurity was second (see Figure 4-1). Humana now has research and intervention pipelines aimed at addressing both of these social determinants.
To test primary care physician clinics as a primary channel to address food insecurity, Renda and his colleagues conducted a pilot with over 500 clients and found that physicians could successfully screen their patients for food insecurity during office visits and then refer them to food resources—all without disrupting practice flow. They then developed a physician toolkit to educate them on how food insecurity affects health,3 why it is important to screen in a clinic setting, and how to do it using the U.S. Department of Agriculture (USDA) two-question Hunger Vital Signs tool. In 2017, Humana launched a randomized controlled trial in collaboration with Feeding South Florida, with 1,000 clients, of a high-touch intervention involving screening, mobile food distributions, connecting patients to resources, enrolling them in the Supplemental Nutrition Assistance Program (SNAP), and providing case management. This ongoing trial will look at outcomes in health-related quality of life, clinical outcomes, and reductions in utilization and cost.
Renda and his colleagues are also using advanced analytics to develop a predictive model for food insecurity that it can run against Humana’s entire Medicare and Medicaid populations. The idea here is to proactively identify those members who are likely to be food insecure and reach out to them with education, services, and connections to internal and external resources. They have also integrated social determinants of health screening into many of Humana’s clinical operating models, resulting in more than 500,000 Humana members being screened (and if positive, referred
___________________
1 Information available at https://populationhealth.humana.com (accessed May 28, 2019).
2 Information available at https://www.cdc.gov/hrqol/methods.htm (accessed May 28, 2019).
3 Information available at https://populationhealth.humana.com/wp-content/themes/humana/docs/Food-Insecurity-Toolkit.pdf (accessed May 28, 2019).
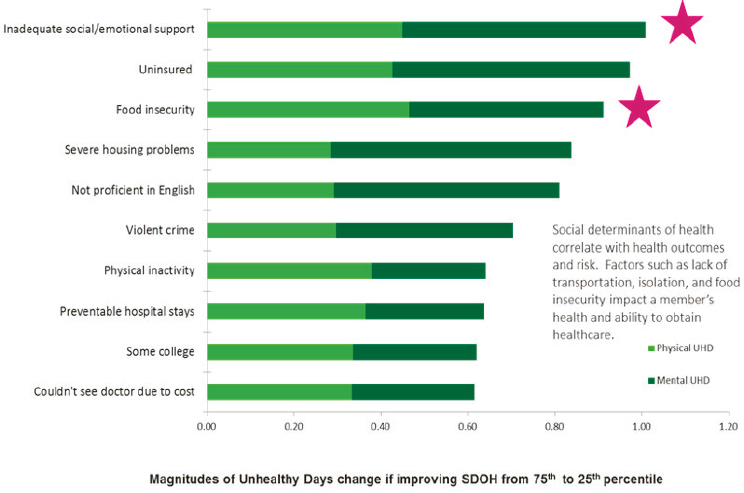
NOTE: SDOH = social determinants of health; UHD = unhealthy days.
SOURCES: Presented by Andrew Renda, April 26, 2019, at the Workshop on Investing in Interventions That Address Non-Medical, Health-Related Social Needs. Figure adapted from Cordier et al., 2018.
to resources) for food insecurity, loneliness, and other social determinants of health in 2018. Their 2019 goal is 1 million screenings and eventually to create a health ecosystem that assesses all patients for social determinants of health needs alongside other clinical gaps in care.
Humana is now working with the National Quality Forum to develop food insecurity quality measures. Renda and his colleagues have also developed a tool called ZoomIn for creating hyperlocal heat maps for social determinants that uses publicly available data sets to identify food deserts and overlay them with community resources.4 For example, plugging an individual’s address into the tool reveals if they live in a food desert and identifies community resources that individuals can access to line up transportation to the nearest grocery store or food bank.
___________________
4 Information available at https://zoomin.humana.com (accessed May 28, 2019).
FEEDING AMERICA:
INTERVENTIONS ADDRESSING FOOD INSECURITY
Feeding America, explained Kate Leone, is a nationwide network of 200 member food banks serving more than 60,000 food pantries and meal programs. All told, Feeding America’s network covers every congressional district and serves 46 million Americans annually. Health, she said, is a priority concern for her organization’s clients, with 58 percent of the households it serves having a member with high blood pressure and 33 percent having a member with diabetes. Some 47 percent of Feeding America’s clients report they are in fair or poor health, 29 percent have no health insurance, and 55 percent have some medical debt.
Feeding America is taking two approaches to addressing the food insecurity affecting its clients’ health. The first approach is to address it when people show up at a food distribution site and provide them with healthier food and information on nutrition and health. This approach is expensive, said Leone, because it involves providing fresh and perishable food. Nonetheless, Feeding America is ramping up its efforts to provide more healthy offerings and get clients to take that food and consume it. It is also hosting health screenings and helping with benefits enrollment. As an aside, Leone mentioned that some of her organization’s food banks in Ohio have engaged local hospital executives to speak with their members of Congress and advocate for SNAP, which she noted provides nine meals for every meal provided by food banks.
The second approach, and perhaps more effective one, addresses food insecurity at health care sites. “There is a great deal of shame involved in asking for help around food, but when your doctor tells you to go get healthy food from a food pantry, it proves to be a very effective way to get someone to walk through [the food pantry] door,” said Leone. “The health care sector can provide an important motivation for people to get the help they need.”
Referring to the joint work Feeding America is doing with Geisinger and the Central Pennsylvania Food Bank, Leone said the key to that effort’s success is getting patients connected with the resources they need. “There is a transportation issue, a follow-up issue, and an adherence issue,” she said in closing, “but to the extent that the health care sector and charitable food network work together, we have been able to increase people’s access to food and improve their quality of life.”
DISCUSSION
Lisa Patrick, a physician and epidemiologist from the Washington, DC, area who lives in a food desert, asked the panelists if they were also working on food literacy and on changing behavior. Hess replied that
food literacy is an incredibly important piece of Geisinger’s program, as is providing recipes to help clients use healthy food with which they may not be familiar and helping clients make what can be a challenging lifestyle change. One unexpected benefit of standing up one of its Fresh Food Farmacies in a food desert is that it raises the quality of food delivered to other food pantries in those neighborhoods. Leone added that a familiar criticism of food banks—and the food industry in general—is that they do not do enough to encourage people to make the right choices; Feeding America has included a focus in its strategic plan on increasing access to and consumption of produce and protein.
Renda noted that nutrition literacy is multifactorial. Basic education on how to eat healthy is one component, but so is how to shop and eat healthy on a budget. It is also important to consider culture and ethnicity when thinking about nutrition literacy. Berkowitz added that all good food insecurity interventions have an educational component, and he agreed with Renda that affordability must be addressed. He then pointed out that there is a significant body of literature around interventions designed to improve the healthfulness of offerings at corner grocery stores, and at least two cities—Philadelphia and San Francisco—have local policy initiatives that enable corner stores to upgrade their facilities and add refrigeration to store fresh fruits and vegetables.
Daphne Delgado from Trust for America’s Health asked the panelists for policy recommendations that would address food insecurity. Berkowitz replied that expanding SNAP would be the place to start given there is good evidence that it works and is efficient in terms of the dollars put into the program that reach eligible individuals and their multiplier effects in the community. Hess agreed, noting that getting clients enrolled in SNAP and optimizing the benefit is one of the first steps in Geisinger’s program. The long-term goal to have food become a covered benefit by insurers, as it costs $1,200 annually to feed a family of four in the Fresh Food Farmacy program and diabetes medication can cost $1,000–$1,500 per month. Renda also concurred that SNAP is the place to start, and beyond that, he proposed expanding benefits in Medicare and Medicaid to include food and food delivery. Leone also agreed that increasing the SNAP benefit and reducing barriers to enrollment would be the top priority given how it is not pegged to a realistic evaluation of what healthy food truly costs. She noted that enrollees in Medicare Savings Programs are more likely to be food insecure, so perhaps there should be some mechanism to link those enrollees to other benefits.
Another area for policy change, said Leone, would be to reduce the barriers associated with the Health Insurance Portability and Accountability Act (HIPAA) that impede coordination between health organizations and the charitable food sector. Karen DeSalvo added that it is possible
to address the data-sharing barrier because HIPAA allows patients to share their data at their discretion. She noted that in North Carolina and Louisiana, enrollment in Medicaid includes a check to see if an individual is eligible for other social care programs, including SNAP. DeSalvo also pointed out that USDA announced a pilot program that will allow online retailers to take SNAP benefits so that food can be delivered to SNAP beneficiaries. Larry McNeely, a workshop participant, noted that the Special Supplemental Nutrition Program for Women, Infants, and Children, like SNAP, works to provide nutritional support for children.
Joanne Lynn commented how grateful she is for research that fuels advocacy for a better food supply but said it should be unacceptable to have a study arm that does not provide food. There should also be a strategy, she said, that makes it unacceptable for people to have to join a waiting list to get food. Leone said Feeding America’s vision is to make hunger in America unacceptable, but part of the problem is that hunger is a largely invisible issue. Renda, agreeing with both Lynn and Leone, said the way to design a clinical trial without an unethical “no food” arm is to make the control arm one in which the individuals have access to SNAP and a food bank and compare that arm to the intervention arm. Hess and Berkowitz both agreed that it is imperative to move to more sophisticated research models such as the one Renda proposed.
An unidentified participant noted that her institution worked with the Greater Chicago Food Depository to create seven hospital-based food pantries that are open 24 hours per day, every day. They are self-serve and do not require a food prescription. Some hospital employees take advantage of it, in addition to patients and families of children who are hospitalized. She noted that in many cases, individuals who take advantage of these pantries then volunteer to give back to the pantry. Hess commented that the volunteers in her program are largely those individuals who participate in it. Leone added that her organization has a strong effort to bring people with lived experience to Washington to speak with lawmakers. Berkowitz added that he included participants in study design work.
This page intentionally left blank.










