
3
The Current Landscape of Adolescent Risk Behavior
Adolescence has long been considered a period when people are especially susceptible to engaging in risky behaviors. This chapter first examines the nature of adolescent risk taking. It then turns to the three behaviors that the committee selected for targeted inclusion in this report—alcohol use, tobacco use, and sexual behaviors—and their related health outcomes.
As described in Chapter 1, the committee limited itself to three specific behaviors for this report given the limited time frame for the study. In general, these selections were based on (1) the prevalence of these behaviors among today’s adolescents, (2) the significant amount of data describing their demographic trends, and (3) the large number of peer-reviewed studies of evidence-based programs that have targeted these behaviors and outcomes. We selected sexual behavior because of the focus in the statement of task on the Teen Pregnancy Prevention (TPP) program; alcohol use because, like sexual behavior, it generally becomes socially acceptable or appropri-
___________________
1 Response to MyVoice survey question: “Describe what it would look like to live your best life.” See the discussion of the MyVoice methodology in Appendix B for more detail.
ate once a person reaches a particular age or developmental milestone; and tobacco use, because of the decades of research on primary and secondary prevention programs and interventions for nicotine addiction and tobacco-related diseases, which we believed would be informative to our task. We recognize, of course, that selecting only three behaviors resulted in excluding a number of highly prevalent risk behaviors from our in-depth review. We found this to be a particularly difficult decision with regard to violence, which encompasses a set of risk behaviors that are associated with some of the most common causes of morbidity and mortality among adolescents (Centers for Disease Control and Prevention [CDC], 2019a) (see Box 3-1). It is also important to note that violent behaviors often co-occur with the three risk behaviors that are covered in this report. For example, violence in the form of bullying can lead to increased substance use behaviors, and sexual behavior under the influence of alcohol may result in violence in the form of sexual assault. We therefore highlight these connections between violence and our three focal behaviors where relevant.
THE NATURE OF ADOLESCENT RISK TAKING
Risk behavior tends to follow a typical trajectory: it is low in childhood, increases around puberty, peaks in late adolescence to early adulthood, and then decreases in adulthood (Romer, Reyna, and Satterthwaite, 2017). Researchers posit that risky adolescent behaviors reflect a gap between an adolescent’s biological and social maturity. Many studies have also found that adolescents’ decision-making processes differ in significant ways from those of adults. First, adolescents often underestimate risks and perceive greater potential benefits from risky behavior (Smith, Chein, and Steinberg, 2014). Second, while adults avoid risky behavior by engaging in gist-based reasoning (defined as reasoning based on intuitive reactions derived from education and experiences), adolescents lack the experience to employ such reasoning (Reyna, 2012). Third, adolescents use emotion-based reasoning, meaning that rather than just weighing the risks, they also think about the social consequences of their decisions (Blakemore and Robbins, 2012). Finally, when adolescents do engage in risky behaviors, they often have a limited understanding of the possible consequences of their actions (van den Bos and Hertwig, 2017).
Healthy Adolescent Risk Taking
Risk is a general construct that is not confined to illicit or unsafe behaviors. Healthy risk taking involves socially acceptable and constructive risk behaviors, and as discussed previously, is considered a necessary and normative part of adolescence (Duell and Steinberg, 2019). These behaviors
are risky because of the uncertainty of their potential outcomes rather than the severity of their potential costs, and engaging in healthy risk taking allows adolescents to learn, grow, and thrive.
Researchers also refer to healthy risk taking as safe, positive, prosocial, or adaptive risk taking (Duell and Steinberg, 2019; Wood, Dawe, and Gullo, 2013). Such risk taking allows adolescents to explore and become more autonomous. Taking risks also enables adolescents to challenge the values, morals, and beliefs they were taught in order to develop their own identities separate from those of their parents, families, and peers. In addition, healthy risk taking gives adolescents the chance to practice making decisions; test out their new problem-solving skills; and develop realistic assessments of themselves, other people, and the world around them. In all five dimensions of optimal health discussed in Chapter 2 (O’Donnell, 2017), some degree of risk taking is necessary to promote positive health outcomes and prepare for adulthood (Duell and Steinberg, 2019).
Duell and Steinberg (2019) propose three features that characterize healthy risks. First, healthy risks benefit adolescents’ well-being. Second, they carry mild potential costs compared with unhealthy risks. And third, they are generally socially acceptable. In this context, social acceptability refers to the views of adults rather than those of other adolescents; although the social acceptability of certain healthy risks may be controversial among adults, social acceptability in adolescence is often more strongly associated with peer culture and contextual influences.
The following are examples of healthy risk taking within each of the five dimensions of optimal health:
- Physical
- Participating in a team sport
- Trying a new food
- Emotional
- Reaching out for help
- Apologizing for a mistake
- Social
- Public speaking
- Asking someone out on a date
- Intellectual
- Enrolling in a challenging course
- Applying knowledge to a new situation
- Spiritual
- Experimenting with different values systems and identities
- Volunteering for a good cause
Unhealthy Adolescent Risk Taking
In contrast to healthy risk taking, unhealthy risk taking encompasses behaviors that can result in adverse consequences that outweigh the potential gains and may delay or harm adolescents’ development. From childhood to adolescence, a significant increase occurs in such unhealthy risk-taking behaviors as substance abuse, smoking, violence, and unprotected sexual activity (Institute of Medicine, 2011). Not all adolescents engage in these behaviors often, although many experiment with them. Generally, research has found that serious problems tend to cluster in a small percentage of youth (Cross, Lotfipour, and Leslie, 2017). In addition, adolescents at highest risk for negative consequences often engage in multiple unhealthy risk behaviors, such as drug or alcohol use and unprotected sexual intercourse (Wu et al., 2010).
The following are examples of unhealthy adolescent risk taking within each of the five dimensions of optimal health:
- Physical
- Driving under the influence of alcohol
- Engaging in sexual intercourse without protection
- Emotional
- Using coercion
- Lying
- Social
- Provoking a physical fight
- Bullying or cyberbullying
- Intellectual
- Cheating on a test
- Skipping school
- Spiritual
- Engaging in behaviors that go against one’s ethical code
- Doing something because of peer pressure rather than personal beliefs
Characteristics of Adolescent Risk Taking
Although scientists have yet to reach consensus on what exactly drives adolescent risk taking, most agree on certain key components of adolescent risk behavior, including impulsivity, sensation seeking, self-regulation/impulse control, working memory, and response inhibition (Hartley and Somerville, 2015; Roditis et al., 2016).
Some of the most unhealthy adolescent risk behaviors are linked to impulsive traits that appear in early childhood. Higher levels of impulsivity
in children as early as age 3 have been associated with drug use and aggressive behavior in adolescence (Romer, 2010). Similarly, sensation seeking, or the tendency to seek out new or thrilling experiences, can also lead to increased unhealthy risk-taking behavior (Duell and Steinberg, 2019).
Self-regulation, also termed impulse control, denotes the process through which individuals effectively handle impulsivity and sensation seeking. Higher self-regulation is associated with fewer unhealthy risk-taking behaviors, including substance use and antisocial behavior, among middle school students (Fosco et al., 2013). Furthermore, research suggests that self-regulation skills can be improved by engaging in positive risk behaviors that require planning and impulse control (Wood, Dawe, and Gullo, 2013). Taken together, these findings indicate that healthy risk taking can provide adolescents with important opportunities to practice self-regulatory skills, and thus narrow the developmental gap between sensation seeking and self-regulation during adolescence.
Another component of adolescent risk behavior is working memory, or the capacity to temporarily store and manipulate a limited quantity of goal-relevant information in order to perform complex cognitive tasks (Murty, Calabro, and Luna, 2016). Working memory supports more goal-oriented versus impulsive actions because adolescents can use past risk-taking experiences to inform future behavior (Hofmann, Schmeichel, and Baddeley, 2012; Romer, Reyna, and Satterthwaite, 2017). In contrast, adolescents with worse working memory may be more likely to engage in unhealthy risk-taking behavior and may be less likely to incorporate learning from past experiences into their decision-making processes.
Strongly related to working memory, response inhibition is the capacity to suppress a behavioral response in favor of one that is more appropriate or goal oriented. Research has found that lower response inhibition in adolescents is related to more unhealthy risk behaviors, including unsafe driving, early cigarette smoking, and alcohol use (Henges and Marczinski, 2012; Mashhoon et al., 2018; Ross et al., 2015).
Ultimately, adolescent risk-taking behavior is influenced by many complex and interacting variables, including aspects of brain development and biological processes, as well as proximal and distal contextual factors. In general, most theorists agree that risk taking during adolescence is normal, but that the key to healthy risk taking is to provide guidance in decision making and to encourage adolescents to engage in less dangerous and more constructive risks.
Neurobiological Factors in Adolescent Risk Taking
Advances in understanding of human brain development have yielded insights into why adolescents may be more predisposed to unhealthy risk
taking relative to children or adults (Graber, Nichols, and Brooks-Gunn, 2010). At the onset of puberty, adolescent boys produce more testosterone, a hormone associated with sensation seeking and aggressive risk taking. For girls, increased testosterone is associated with the tendency to affiliate with peers who engage in unhealthy risk behaviors (Vermeersch et al., 2008). In line with more comprehensive, whole-brain approaches, neuroscientists have begun to investigate how increases in these gonadal hormones at puberty may contribute to risk-taking behaviors during adolescence by altering neural responses to rewards (Braams et al., 2015).
The hormonal changes that occur during puberty remodel the socio-emotional network in the limbic and paralimbic areas of the brain. This network, which is particularly important for thrill seeking and sensitivity to rewards, develops more quickly and is more active during adolescence than during childhood or adulthood. In contrast, the cognitive-control network, which engages the prefrontal cortex, develops more slowly and continues to mature over the course of adolescence and into young adulthood. Studies have found that the competitive dynamic between these two networks is associated with numerous decision-making contexts, including drug use, social decision processing, moral judgments, and the valuation of alternative rewards and costs (Smith, Chein, and Steinberg, 2013).
Context Matters: Social and Environmental Influences on Risk Taking
While there are some developmental constants in terms of the neurocognitive and hormonal changes that take place during adolescence, these biological changes occur in the broader socioecological contexts of the parents and family, peer groups, school, and the community (Bronfenbrenner, 1994). The following sections explore these contexts and how they can serve as either risk or protective factors. Many of these contexts are also highlighted in the youth perspectives in Box 3-2.
Individual Influences
Beyond the neurobiological developments that occur during adolescence, individual factors can protect against unhealthy risk taking. These include engagement in meaningful activities, life skills and social competence, positive personal traits, and future orientation (Judd, 2019). Meaningful activities promote positive development, including the development of important skills. Life skills and social competence—encompassing social-emotional skills related to self-awareness, self-management, social awareness, and communication—help adolescents make positive choices, maintain healthy relationships, and promote their own well-being. Positive personal traits that are protective against unhealthy risk behaviors include
an easy-going temperament, a sense of purpose, and a feeling of control over one’s environment. And future orientation, or the ability to set future plans or goals, can also protect adolescents against unhealthy risk taking by making them more strategic in choosing risks that have the most potential benefit while posing the least threat to their future plans (Maslowsky et al., 2019).
Parent and Family Influences
A large proportion of U.S. children spend at least some part of their childhood or adolescence in a single-parent family, and an increasing number live with cohabiting, unmarried parents (Livingston, 2018). Generally, research suggests that adolescents who live in single-parent families are more likely to engage in unhealthy risk behaviors and fare worse on a wide range of developmental outcomes relative to their counterparts in families with two biological parents (Langton and Berger, 2011).
Adolescents model their own behavior on that of their family members, peers, and role models. Parents’ own risk-taking behavior therefore factors strongly into how adolescents engage with risky activities, which can be related to genetics and to aspects of early learning about substance use (Smit et al., 2018). In addition, exposure to various forms of stress during childhood is associated with later unhealthy risk taking (Institute of Medicine, 2011). Early stressors in the household, including physical and emotional abuse, emotional neglect, parental substance use, and exposure to family violence, are associated with poor health outcomes during adolescence, including drug use, addiction, and suicide. Adolescents who experience such stressors in childhood also tend to have more difficulty with emotion regulation, response inhibition, and executive functioning, and are more likely to fail school, to be excluded from prosocial groups, and to associate with peers who engage in substance use (Romer, 2010).
Parents are often faced with difficult decisions as their children enter adolescence, as adolescents’ increasing autonomy from their parents and greater propensity for unhealthy risk taking requires a balance of both trust and behavioral monitoring. Parenting styles characterized by setting high expectations for behavior, establishing clear family rules, applying fair and consistent discipline, and engaging in age-appropriate supervision and monitoring can be protective against unhealthy risk-taking behaviors (Judd, 2019).
As discussed in Chapter 2, adolescents frequently drift away from their parents and toward peer groups. Yet despite this trend, parents continue to play an important role in adolescents’ lives, although the changing nature of these relationships can have significant effects on risk taking and associated health outcomes (Tsai, Telzer, and Fuligni, 2013). Family connectedness,
which refers to feelings of warmth, love, caring, and communication, is also a major protective factor against adolescent risk taking. Adolescents who feel family support and connection report a high degree of closeness with their parents and feelings of being understood, loved, and wanted (Sieving et al., 2017).
Peer Influences
Increasing involvement with peers is one of the primary features distinguishing adolescence from childhood. Research suggests that there are four modes of direct or indirect peer influence, which can operate independently or concurrently: (1) direct peer pressure, (2) peer influence through modeling, (3) influences through group norms, and (4) the creation of structured opportunities (Goliath and Pretorius, 2016; McWhirter et al., 2013).
Numerous studies have shown that, in the presence of peers, adolescents prefer more immediate rewards and engage in more risky behaviors even when they are presented with the potential harms (Knoll et al., 2015; Smith, Chein, and Steinberg, 2014). In addition to peer influence, adolescent peer groups congregate in new, often unsupervised contexts that can facilitate risk-taking behaviors (Institute of Medicine, 2011).
Peers also serve as adolescents’ primary source of information about social norms. Peers socialize one another to norms in two ways: by modeling behavior and by reinforcing behavior in other people (Albert, Chein, and Steinberg, 2013). This influence can have both positive and negative effects on risk taking. For instance, teenagers who believe that their peers disapprove of having sex are less likely to become sexually active, whereas teenagers who believe their peers are having sex are more likely to become sexually active (Warner et al., 2011).
In a similar vein, risk taking also relates to the traits adolescents seek in their friends. For instance, adolescents prone to sensation seeking often gravitate toward peers with the same interests. Likewise, adolescents who lack social skills or social competence may incur a negative reputation, which may lead them to peers who share the same deficits and reinforce negative social pressures (Institute of Medicine, 2011).
Peer conflict and exclusion are also associated with increased unhealthy risk-taking behavior (Falk et al., 2014; Peake et al., 2013; Telzer et al., 2015). Blakemore (2018) suggests that because adolescents are fundamentally motivated to prevent social rejection by their peers, they may engage in unhealthy risk behaviors that have adverse health or disciplinary consequences. Adolescents may therefore seek and engage in behaviors that adults view as unhealthy risks in order to win peer approval, or at the very least to avoid peer rejection (Maslowsky et al., 2019).
School Influences
School connectedness, which refers to adolescents’ beliefs that adults and peers in the school care about them, is an important protective factor for a range of risk behaviors, including early sexual initiation; alcohol, tobacco, and other drug use; and violence (CDC, 2018a). Schools can foster school connectedness by establishing positive norms, providing clear expectations for behavior, and fostering physical and psychological safety for all students (Thapa et al., 2013).
Another important protective factor is positive school climate, which refers to whether adolescents feel that the school environment promotes and encourages connectedness and support. Characteristics of a positive school climate include having high expectations for student academics, behavior, and responsibility; using proactive classroom management strategies; employing interactive teaching and cooperative learning styles; consistently acknowledging all students and recognizing good work; and allowing students to express themselves in school activities and class management (Judd, 2019).
Adolescents need opportunities to engage as learners, leaders, team members, and workers. For this reason, in-school or after-school programs can offer healthy alternatives to unhealthy risk behavior. In addition, such programs and interventions delivered in and after school may be specifically oriented toward the prevention or reduction of unhealthy risk taking, as in the case of drug prevention and sexual education (CDC, 2018a).
Youth–adult connectedness is also essential for adolescent health and well-being. Teachers and coaches can have important influences on adolescents’ goals, which are strongly associated with risk-taking behavior. Research shows that close, positive relationships with caring adults outside of the family can protect adolescents from a range of poor health outcomes and promote positive youth development (Sieving et al., 2017).
Finally, parental engagement in schools can be protective against unhealthy risk taking. Research has found that it reduces the likelihood that adolescents will engage in such unhealthy risk behaviors as alcohol use, tobacco use, and unprotected sexual activity. In addition, parental engagement is associated with better student behavior, higher academic achievement, and enhanced social skills (CDC, 2018a).
Community Influences
Structural (e.g., poverty) and social (e.g., norms) characteristics of neighborhoods can shape adolescent risk taking (Leventhal, Dupéré, and Brooks-Gunn, 2009). Neighborhood or community risk factors for unhealthy adolescent risk behaviors include the availability of drugs or firearms, extreme poverty, community disorganization, and low neighborhood
attachment. On the other hand, neighborhood resources and opportunities can protect against unhealthy risk taking by increasing structures and supports, particularly for at-risk youth (Holmes et al., 2019).
In particular, access to high-quality, teen-friendly health care can reduce, prevent, and mitigate the effects of unhealthy risk behaviors. Adolescents need medical, dental, and behavioral health services with health care providers who respect and understand their particular needs. In addition, health care that is teen-friendly, culturally competent, affordable, convenient, and confidential can promote adolescent autonomy (U.S. Department of Health and Human Services [HHS}, 2018a).
Beyond improving health services, local, state, and federal governments can take additional measures to discourage unhealthy risk behaviors among adolescents. One successful example is graduated driver’s licensing laws, which have been associated with a 42 percent reduction in the nationwide rate of crashes involving 16-year-olds (Institute of Medicine, 2011). Accordingly, similar legislative measures, such as raising the minimum age for smoking and drinking and providing free and easier access to contraception, may also help to mitigate unhealthy adolescent risk taking (Catalano et al., 2012).
Technological Influences
The rapid rise of new technologies has vastly expanded the ways in which adolescents interact and spend their time. Social media are one of the primary ways in which teenagers engage with technology. Studies have found that social media can have a substantial influence on adolescents’ social norms, as they involve simple, fast, and quantifiable measures of peer endorsement (e.g., “Likes”) (Sherman et al., 2016). In addition to social media, teenagers use technology in a variety of other ways, such as texting, gaming, streaming, and recording, all of which can facilitate adolescent risk behaviors. For instance, text messaging while driving is widely recognized as an unhealthy risk behavior, making it difficult to react during a potential crash (Gershon et al., 2017; Lee et al., 2014). In contrast, technology can also facilitate healthy risk taking, as in the case of assistive and interactive digital media and social media platforms, which can help youth learn new information, find and communicate with similar peers, and engage with broader social support networks (O’Dea and Campbell, 2011; O’Keeffe and Clarke-Pearson, 2011; Odom et al., 2015).
ALCOHOL USE, TOBACCO USE, AND SEXUAL BEHAVIOR: TRENDS AND INFLUENCES
As stated in Chapter 1, the committee was charged with identifying the risk behaviors and outcomes to review for this report. This section describes
the demographic trends and social and environmental factors associated with the three adolescent risk behaviors selected by the committee—alcohol use, tobacco use, and sexual behavior—as well as their related adverse health outcomes.
Data Sources
Data on health outcomes in this section come from various federal data sources, including the Centers for Disease Control and Prevention’s (CDC’s) surveillance systems, the U.S. Department of Transportation (DOT), and the National Survey of Family Growth (NSFG). To evaluate trends in risk behavior in the above three areas, we decided to use data from the Youth Risk Behavior Survey (YRBS).
The Youth Risk Behavior Surveillance System (YRBSS) was established in 1990 to monitor the prevalence of a variety of health behaviors among U.S. adolescents that are associated with later morbidity and mortality outcomes (CDC, 2018b). Every 2 years since 1991, the YRBS has been administered to a nationally representative, cross-sectional sample of in-school adolescents in grades 9–12. Approximately 15,000 youth participated in the most recent survey, in 2017, and more than 4.4 million have participated since 1991.
The YRBS has a number of strengths for the purposes of this study. First, it provides information on all three behaviors of interest (alcohol use, tobacco use, and sexual behavior) among the same population of adolescents. None of the other datasets we considered included all of these behaviors. Second, the YRBS has been conducted consistently since 1991, whereas other surveys either lack similar longevity (e.g., the National Youth Tobacco Survey [NYTS]) or may present results from aggregated time intervals (e.g., the NSFG). Finally, a major strength of the YRBS is the way in which items have been updated or added to reflect changing behavior trends (e.g., use of e-cigarettes, cyberbullying) and diverse populations (e.g., LGBTQ youth) (see Figure 3-1).
At the same time, as with all datasets, the YRBS has critical limitations that necessitate caution when interpreting its results for the broader U.S. adolescent population. First and foremost, the YRBS includes only in-school youth. This is a serious limitation when one is examining behavior trends, since research shows that youth who are not in school (e.g., dropped out, incarcerated, homeless) have the highest incidence of risk behaviors and related adverse health outcomes (Edidin et al., 2012; Odgers, Robins, and Russell, 2010; Tolou-Shams et al., 2019). Although the CDC estimates that out-of-school youth represent only 3.4 percent of the adolescent population, recent research using data from the National Center for Education Statistics suggests that this figure could be as high as 10.1 percent

SOURCE: Generated using documentation from the YRBS questionnaires (CDC, 2018c).
(Brener et al., 2013; King, Marino, and Barry, 2018). It is also important to note that the reasons these adolescents are not in school may be related to these risk behaviors. For example, pregnant or parenting teens are more likely to drop out of school (Freudenberg and Ruglis, 2007; Wilson et al., 2011). In addition, substance use or violence in or around school can lead to suspensions, expulsions, and/or juvenile justice involvement (Heitzeg, 2009). Importantly, marginalized youth, particularly adolescents of color, are more likely to experience all of these outcomes (Heitzeg, 2009; Kearney and Levine, 2012).2
Similarly, the context in which surveys are administered can affect how participants respond. There is conflicting evidence in the literature regarding the ideal survey setting and mode for asking sensitive behavior questions of adolescents. For example, a study conducted by the CDC in 2004 examined differences in YRBS behavior prevalence estimates by setting (school vs. home) and mode (paper-and-pencil instrument [PAPI] or computer-assisted self-interview [CASI]) (Brener et al., 2006). Results showed that for the majority of YRBS items, including questions about alcohol use and sexual behavior, students who completed the survey in school were more likely to report sensitive behaviors than were those who completed the survey at home. There were fewer differences by survey administration mode; however, those in the CASI condition were more likely to report lifetime alcohol use, current alcohol use, and cigarette smoking before age 13 compared with those in the PAPI condition. Given the relatively few significant differences by mode, the CDC continued using PAPI surveys in school settings because of the relatively greater cost and complexity of CASI administration (Brener et al., 2013).
In 2008, the CDC conducted another study in which students completed the YRBS using (1) a PAPI in school, (2) a Web-based survey in school, or (3) a Web-based survey “on your own” (Eaton et al., 2010). The PAPI and Web-based surveys that were administered in schools showed similar results (Eaton et al., 2010), but more data were missing from the Web-based surveys (Denniston et al., 2010). In addition, the in-school Web-based survey was found to compromise perceived anonymity and both perceived and actual privacy (Denniston et al., 2010). Finally, the response rate was very low among those in the Web-based “on your own” condition (Denniston et al., 2010; Eaton et al., 2010). As a result, the CDC has continued to administer the YRBS in schools using the PAPI mode (Brener et al., 2013).
___________________
2 Because of limited reporting, we are unable to present data for all health behaviors and outcomes for all racial/ethnic groups. This is the case in particular for smaller racial/ethnic groups, where small sample sizes required data suppression. In addition, racial/ethnic groups are often defined differently across surveys and over time (e.g., Native Hawaiian/Pacific Islander vs. Asian/Pacific Islander), making them more difficult to compare.
However, recent research suggests that a computer-based mode may be more appropriate for contemporary surveys. A 2015 meta-analysis found that computer-based surveys led to increased response rates to questions about sensitive behaviors among both adolescents and adults (Gnambs and Kaspar, 2015). In addition, there was a significant time trend, with computerized surveys yielding lower response rates in the late 1990s and early 2000s but higher response rates in more recent years, a finding that may be attributable to the overall increase in the use of web-based surveys and widespread access to technology (Gnambs and Kaspar, 2015). Accordingly, further research is needed to understand whether the ideal setting and survey mode for the YRBS have changed within the last decade.
It is also important to note that while YRBS questions have been added or changed over time to reflect more current behavior trends and populations, some questions, particularly those related to sexual behavior, are still ambiguous and exclusive of diverse populations. For example, the first question in the sexual behavior section asks respondents whether they have ever had “sexual intercourse” without defining this term (CDC, 2018c). Therefore, youth may interpret this term to include vaginal sex only, or other types of sexual contact as well, including oral and anal sex (Peck et al., 2016; Sanders and Reinisch, 1999). This is a particularly salient limitation for LGBTQ youth, who may not engage in penile–vaginal intercourse.
Moreover, the subsequent sexual behavior questions present sexual intercourse in a heteronormative way. For example, questions about protection and contraceptive methods are written implicitly and explicitly with pregnancy as the targeted outcome (CDC, 2018c). This is a significant limitation of the YRBS for both heterosexual and LGBTQ youth since, like vaginal sex, oral and anal sex can also lead to sexually transmitted infections (STIs). By contrast, the NSFG asks more specific questions about each type of sexual behavior in a similar age group, which (1) allows for greater precision of the prevalence estimates for each behavior, (2) is more inclusive of diverse behaviors and populations, and (3) provides a better understanding of sequences of sexual behavior initiation.3
Other caveats to the national YRBS data need to be considered when interpreting the behavior trends presented in this report. First, the YRBS trends presented in this chapter represent only high school students (approximately 14–18 years old). Although the YRBS is conducted with middle school students in certain sites, these data cannot be analyzed to produce nationally representative estimates (Brener et al., 2013). As mentioned in Chapter 1, although the NYTS and the Monitoring the Future (MTF) survey include middle school students, these surveys report only on substance
___________________
3 See Appendix C for a table that compares the wording of sexual behavior items in the YRBS and NSFG.
use. However, the national high school YRBS does include items that ask about experiences before age 13 for each of our behaviors of interest, and therefore serve as a proxy for the prevalence of these behaviors during early adolescence in this report.
Additionally, although schools that participate in the national YRBS are generally not permitted to modify the standard 89-item questionnaire,4 there are two exceptions to this rule (Brener, 2019).5 First, many states and localities conduct their own YRBS, for which they have the option of modifying the standard questionnaire within certain parameters (Brener et al., 2013). These data are generally presented separately from the national data; however, if a school is selected into both the national sample and a state/local YRBS sample, the survey is conducted only once (Brener, 2019). In these cases, whether the national or state/local questionnaire is used for the national dataset is dependent on whether the survey is administered by the national contractor or a state/local agency (Brener, 2019). In 2017, for example, 16 of the 144 schools participating in the national survey provided data from a modified state/local questionnaire for the national dataset (Brener, 2019). As a result, the national dataset may be missing information on certain behaviors if the state/local surveys excluded the corresponding items.
The second exception to this rule, although much more rare, occurs when a school or state that is selected into the national sampling frame refuses to participate unless the questionnaire is modified (Brener, 2019). In 2017, this occurred when two schools required that the sexual behavior questions be removed from the survey as a condition of their participation (Brener, 2019). In these scenarios, specific items may not have been asked of a large number of students, which could lead to biased results at the national level. As a result of these limitations, the demographic trends presented in this chapter should be interpreted with caution.
Alcohol Use in Adolescence
Trends
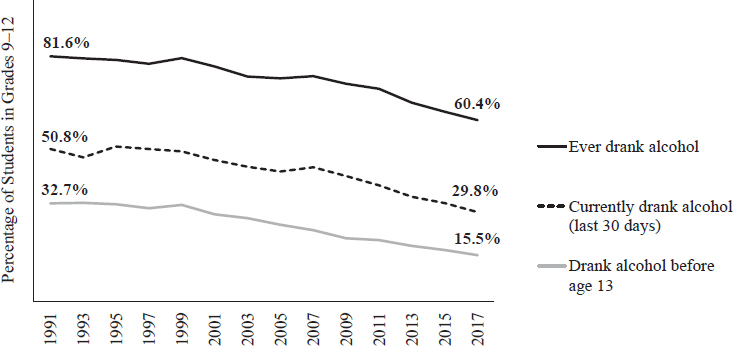
According to the 2017 YRBS, 60.4 percent of U.S. high school students have had at least one drink of alcohol on at least 1 day during their life, compared with 86.1 percent in 1991 (Kann et al., 2018). Trends in current alcohol use, defined as any use in the past 30 days, are similar with
___________________
4 Five to 11 questions are added to the standard, national YRBS questionnaire each cycle, and these items generally cover topics that are not covered by the priority health-risk behavior categories (e.g., sun protection) (Brener et al., 2013).
5 Brener, N. (2019). Personal communication.
50.8 percent of students reporting current alcohol use in 1991 compared with 29.8 percent in 2017 (Kann et al., 2018). Furthermore, early adolescent alcohol use (before age 13) decreased by more than one-half, from 32.7 percent in 1991 to 15.5 percent in 2017 (Kann et al., 2018) (see Figure 3-2).
Underage drinking is associated with many adverse health outcomes, including school and social problems, violence, arrest, unintentional injuries, sexual assault, substance use disorders, and death (Harding et al., 2016; National Research Council and Institute of Medicine, 2004). Heavy alcohol use in adolescence is also neurotoxic to the brain. Alcohol misuse is associated with dysfunction in brain regions underlying impulse control, reward processing, and executive function (Adger Jr. and Saha, 2013). In addition, adolescent alcohol use may increase the risk of developing an alcohol use disorder in early adulthood by altering neural functioning related to rewards (Squeglia et al., 2014).
Alcohol use does not vary significantly by biological sex, but it does vary by race and ethnicity (Kann et al., 2018; NASEM, 2019). In 2017, Asian adolescents reported the lowest rates of current alcohol use (12.2%), followed by black/African American (20.8%), Native Hawaiian/Pacific Islander (26.8%), Hispanic/Latino (31.3%), American Indian/Alaska Native (31.8%), and white (32.4%) youth (CDC, 2019b; Kann et al., 2018) (see Figure 3-3).
Early initiation of alcohol use is a risk factor for a number of adverse consequences. Substance use before age 15 is the most significant predictor of substance dependencies and abuse in late adolescence and adulthood (Lopez-Quintero et al., 2011; HHS, 2017a). Additionally, adolescents who start drinking before age 15 are four times more likely to meet criteria for
SOURCE: Generated using Youth Risk Behavior Survey data (CDC, 2019b).
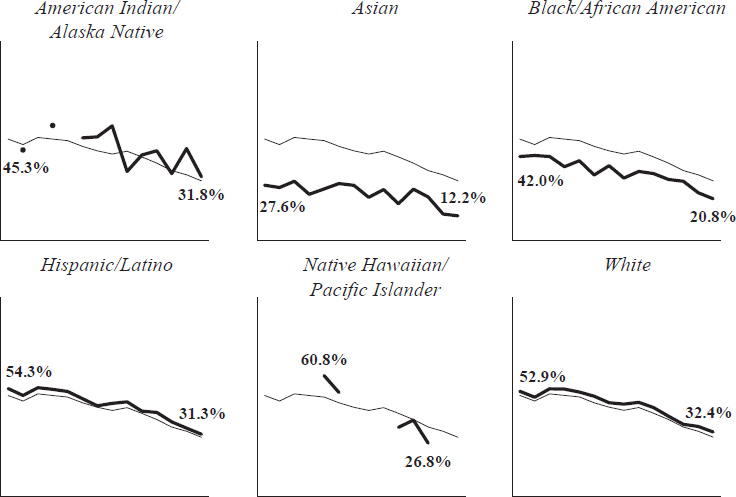
NOTE: Racial/ethnic groups and labels vary by source.
SOURCE: Generated using Youth Risk Behavior Survey data (CDC, 2019b).
alcohol dependence at some point in their lives (HHS, 2017b). However, statistics on early initiation of alcohol are promising. In 2017, 15.5 percent of high school students reported that they had had their first drink of alcohol (other than a few sips) before age 13, compared with 32.7 percent in 1991 (Kann et al., 2018) (see Figure 3-2).
Adolescents who do drink tend to do so less often than adults, yet they are more likely to consume higher quantities of alcohol per occasion (Chung et al., 2018). Underage drinkers ages 12–20 typically consume four to five drinks per occasion, nearly double the average of two to three drinks among adults over age 25 (HHS, 2017a). Binge drinking, defined as having five or more drinks on one occasion for males and four or more drinks on one occasion for females, is the most dangerous way adolescents consume alcohol. Extreme binge drinking is defined as having 10 or more drinks on a single occasion.
The onset of binge drinking and binge drinking episodes typically occurs in early to mid-adolescence (i.e., ages 12–16). Early substance use and rapid progression from first drink to first intoxication are both predictors of binge drinking (Chung, 2018). According to the 2017 YRBS,
13.5 percent of American high school students had engaged in binge drinking during the 30 days before the survey. Nationally, 4.4 percent of students reported that they had consumed 10 or more alcoholic drinks in a row within a couple of hours during the 30 days before the survey. Between 2013 and 2017, there was a noteworthy decrease (6.1% to 4.4%) in the overall prevalence of reporting consumption of 10 or more drinks in a row (Kann et al., 2018).
Substantial research has identified and examined the acute health effects of binge drinking, which include alcohol poisoning, alcohol-related blackouts and injury, car crashes and fatalities, physical and sexual assault, unprotected sexual behavior, and problems at school or work (Hingson and White, 2014; Siqueira and Smith, 2015). The long-term effects of alcohol consumption include an increased risk for heart disease, brain shrinkage, dementia, stroke, liver damage, pancreatitis, lung disease, bone loss, and multiple types of cancer.
Driving under the influence of alcohol is a particular concern with respect to adolescents’ alcohol use. Unintentional injuries represent the leading cause of death among adolescents overall,6 and more than one-half of these deaths result from motor vehicle crashes (CDC, 2019c). The risk is highest among those ages 16–19: in 2017, 2,364 adolescents in this age group died as a result of a motor vehicle crash, and about 300,000 were treated in emergency departments for injuries due to crashes (CDC, 2019d).
Driving under the influence of alcohol and riding with a driver who is under the influence significantly increase the risk of road crashes (Markkula, Härkänen, and Raitasalo, 2019). Drivers are considered to be alcohol impaired when their blood alcohol concentration (BAC) is 0.08 grams per deciliter or greater. Despite declines since 1994, the most recent data from 2017 show that approximately 19 percent of all teen driver fatalities were among those with a BAC over 0.08 g/dl (U.S. Department of Transportation, 2019) (see Figure 3-4).
Social and Environmental Influences
Families play a major role in the development of alcohol-related problems during adolescence. Parental alcohol abuse is a risk factor for adolescent alcohol abuse. Parenting practices including lack of monitoring or supervision of youth, permissive attitudes toward drug use, unclear expec-
___________________
6 Although unintentional injury is the overall leading cause of death in the population ages 10–19, this is not true for all racial/ethnic subgroups. In every year since 1999, homicide has represented the leading cause of death among black/African American adolescents, and since 2016, suicide has surpassed unintentional injury as the leading cause of death among Asian/Pacific Islander youth (CDC, 2019c).
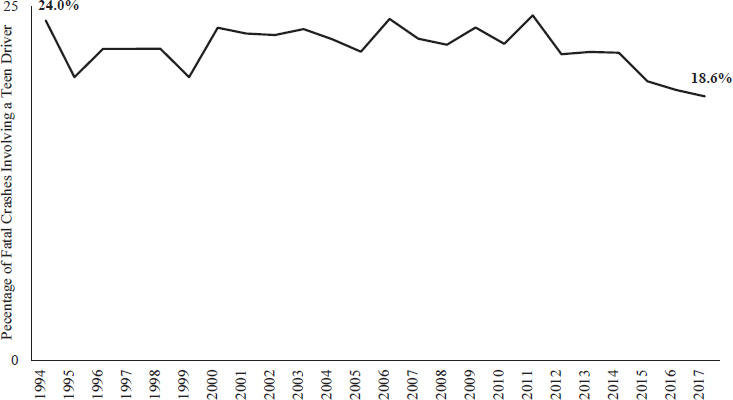
NOTE: Data from the U.S. Department of Transportation were not disaggregated by biological sex or race/ethnicity.
SOURCE: Generated using data from Young Driver Safety Fact Sheets (U.S. Department of Transportation, 2019).
tations of youth behavior, and no or rare rewarding of positive behavior are also risk factors for the development of substance abuse problems during adolescence (HHS, 2016b).
Equally influential for underage drinking are peer substance use and peer pressure. In particular, selection of peers who engage in binge drinking has been associated with early initiation and increased frequency of substance use (HHS, 2016b). Other social mechanisms that may contribute to high-volume alcohol consumption include peers providing access to alcohol and peer norms that are favorable to binge-drinking behavior (Chung et al., 2018).
Patterns of community use can also predict individual substance use by adolescents. Rates of underage drinking are higher in communities in which alcohol is less expensive and more easily obtainable (HHS, 2016b). Factors associated with where an adolescent chooses to drink, including the level of supervision, privacy, safety, and remoteness, can also impact an adolescent’s drinking behavior over time (Chung et al., 2018).
Teenagers are bombarded by positive portrayals of alcohol in the media. Television, movies, and the Internet frequently show alcohol’s positive social effects while avoiding its negative effects. Frequent exposure to alcohol advertising, particularly when these advertisements are tar-
geted specifically at teenagers, contributes to social norms around underage drinking (Meisel and Colder, 2019). Furthermore, many studies have shown that media exposure, including portrayals of teenagers drinking on television, can increase adolescents’ experimentation with alcohol (Moreno and Whitehill, 2014; Smith and Foxcroft, 2009).
Industry, local, state, and federal alcohol policies also influence adolescent alcohol consumption. In the United States, stronger state alcohol policies and taxes are associated with decreased alcohol consumption among underage youth. In addition, comprehensive and stringent local alcohol control policies and enforcement have been associated with lower levels of youth binge drinking (Paschall, Lipperman-Kreda, and Grube, 2014).
Tobacco Use in Adolescence
Trends
Smoking is the leading cause of preventable death in the United States. Worldwide, tobacco use causes more than 7 million deaths each year, and it is responsible for more than 480,000 deaths annually in the United States, including more than 41,000 deaths resulting from exposure to secondhand smoke (HHS, 2014; World Health Organization, 2017). In addition, more than 16 million Americans are living with a disease caused by smoking (HHS, 2014). On average, smokers die at least 10 years earlier than nonsmokers (Jha et al., 2013), and according to the U.S. Surgeon General, if smoking continues at the current rate among U.S. youth, 5.6 million of today’s Americans under age 18 are expected to die prematurely from a smoking-related illness (HHS, 2014).
Tobacco use among adolescents is related to a number of negative health outcomes. Youth smoking is strongly associated with depression, anxiety, and stress, such that smoking may precede or develop as a result of these mental and emotional health problems. Youth smoking can also lead to increased respiratory illnesses, decreased physical fitness, and detrimental effects on lung growth and function (HHS, 2012). If continued into adulthood, smoking can lead to disease and disability in nearly every organ of the body. Indeed, the major causes of excess mortality among smokers are diseases that are related to smoking, including cancer, respiratory disease, and vascular disease (HHS, 2014).
Use of tobacco products typically begins during adolescence, with nearly 9 of 10 cigarette smokers trying their first cigarette by age 18 (HHS, 2014). Fortunately, combustible cigarette use among youth has been decreasing over the last 20 years. The YRBSS has documented a significant decrease in the prevalence of having ever tried a cigarette between 1991 (70.1%) and 2017 (28.9%; Kann et al., 2018) (see Figure 3-5).
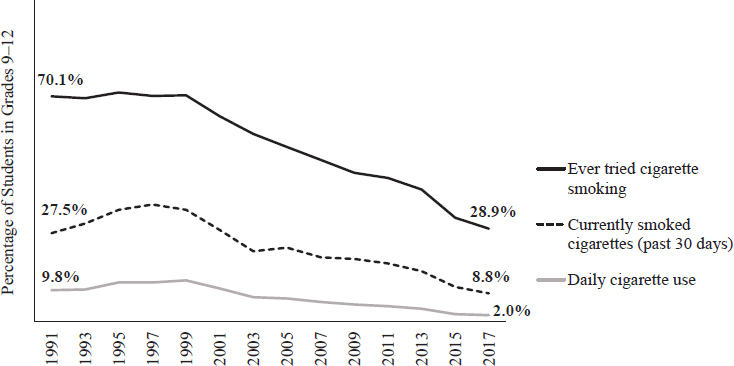
NOTES: The Youth Risk Behavior Survey asked about cigarette use before age 13 only in 2017 (9.5%; Kann et al., 2018). See Figure 3-6 below for data from the National Youth Tobacco Survey on trends in cigarette use for middle school students.
SOURCE: Generated using Youth Risk Behavior Survey data (CDC, 2019b).
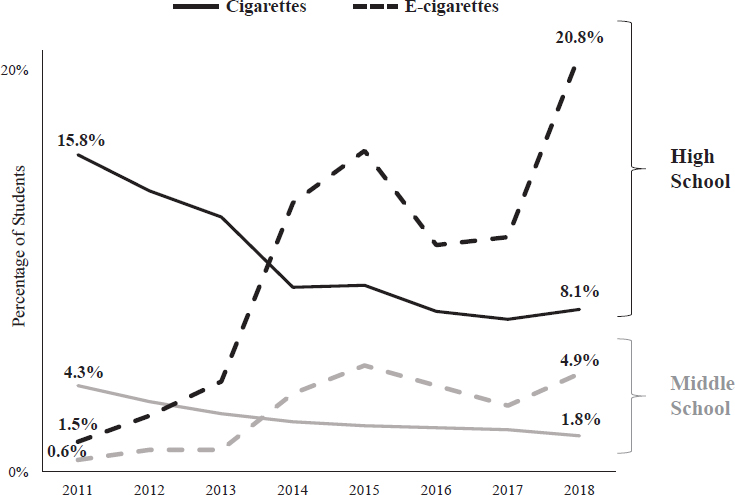
However, overall tobacco use has been increasing. According to the NYTS, 7.2 percent of middle school students and 27.1 percent of high school students reported current use of any tobacco product (past 30 days) in 2018, compared with 6.5 percent of middle school students and 22.9 percent of high school students in 2013 (Arrazola et al., 2014; Gentzke et al., 2019).7
This increase in adolescent tobacco use is most notably related to electronic vapor products, including e-cigarettes, e-cigars, e-pipes, vape pipes, vaping pens, e-hookahs, and hookah pens. E-cigarettes entered the U.S. marketplace in 2006 as an alternative to cigarettes (Cahn and Siegel, 2011; HHS, 2016a). By 2014, e-cigarettes were the most commonly used tobacco product among U.S. youth, and their use in this population has continued to increase (HHS, 2016a). In 2018, 20.8 percent of high school and 4.9 percent of middle school students reported current e-cigarette use, compared with 1.5 percent and 0.6 percent, respectively, in 2011 (Gentzke et al., 2019) (see Figure 3-6). Given concerns about health, nicotine exposure, nicotine dependence, and the transition to combustible tobacco products,
___________________
7 Trends in current tobacco and e-cigarette use are from the NYTS because this survey provides the most up-to-date information on the rapidly growing e-cigarette epidemic.
SOURCE: Generated using National Youth Tobacco Survey data, as presented by Gentzke et al. (2019), Jamal et al. (2017), and HHS (2016a).
the U.S. Surgeon General and the Food and Drug Administration (FDA) commissioner have declared e-cigarette use among youth to be a public health epidemic (HHS, 2018b; U.S. Food and Drug Administration, 2018a).
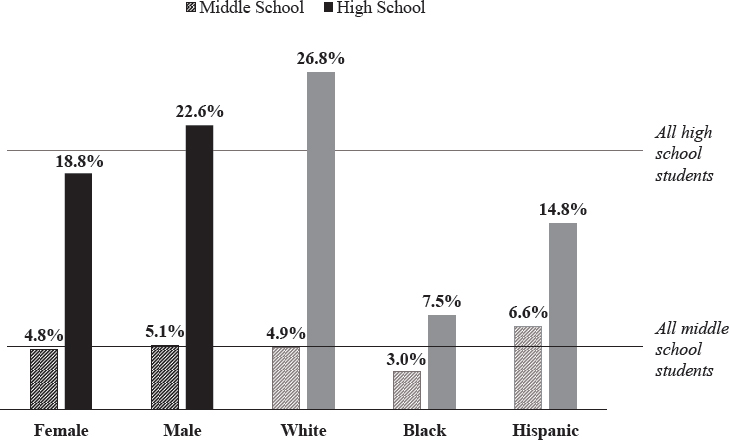
Current e-cigarette use varies by biological sex and race/ethnicity. In 2018, current use was higher for males in both high school (22.6%) and middle school (5.1%) compared with their female peers (18.8% and 4.9%, respectively). With respect to race/ethnicity, more white high schoolers reported current e-cigarette use (26.8%) compared with their black (7.5%) and Hispanic (14.8%) counterparts. However, current e-cigarette use among middle schoolers was highest among Hispanic (6.6%) compared with white (4.9%) and black (3.0%) students (Gentzke et al., 2019) (see Figure 3-7).
Adolescent perceptions of the health risks associated with e-cigarettes can affect their use. In general, research shows that the main factors accounting for why adolescents are more susceptible than other groups to initiating use of tobacco products are flavors; marketing; social pressures; and the belief that alternative tobacco products, such as e-cigarettes, are not harmful (Ambrose et al., 2014; Amrock, Lee, and Weitzman, 2016; Cooper et al., 2016; Gorukanti et al., 2017; Harrell et al., 2017; Hebert et al.,
NOTES: Data for other specific racial/ethnic populations were not available in this source.
“Other race” was excluded because (1) middle school data are not available, and (2) the significant heterogeneity of this group limits the conclusions that can be drawn.
SOURCE: Generated using National Youth Tobacco Survey data, as presented by Gentzke et al. (2019).
2017; McKelvey, Baiocchi, and Halpern-Felsher, 2018; Meyers, Delucchi, and Halpern-Felsher, 2017; Nguyen, McKelvey, and Halpern-Felsher, 2019; Pepper, Ribisl, and Brewer, 2016; Roditis et al., 2016; Schaefer, Adams, and Haas, 2013). Among modern e-cigarette devices, the most well-known is JUUL, which was first introduced in 2015 and has quickly become the most common device used by youth because of its sleek design, user-friendly function, desirable flavors, and ability to be used discreetly (Fadus, Smith, and Squeglia, 2019; Kavuluru, Han, and Hahn, 2019; Willett et al., 2019).
As opposed to many adult smokers, a large percentage of youth who have used e-cigarettes have never tried traditional cigarettes (Hughes et al., 2015). Additionally, e-cigarettes drive many adolescents to become dual or poly tobacco product users. Among adolescent e-cigarette users, 75 percent reported concurrent use of other forms of tobacco (Anand et al., 2015). This is important because youth who use multiple tobacco products have been found to be at higher risk for developing nicotine dependence and continuing tobacco use into adulthood (HHS, 2012).
E-cigarette vapor contains many of the same harmful toxins as traditional cigarettes (NASEM, 2018b). However, the safety and long-term effects of e-cigarettes are still vague. The CDC and FDA, along with state and local health departments and other partners from the health sector, are currently responding to a national outbreak of e-cigarette or vaping product use–associated lung injuries (EVALI). Current evidence suggests that EVALI may be associated with THC-containing products. This outbreak aside, however, the CDC reiterates that e-cigarette or vaping products should never be used by youth (CDC, 2019e).
Social and Environmental Influences
Risk factors associated with cigarette use include risk perceptions, social influences from family and friends, and individual affective characteristics such as depression and sensation seeking (Wellman et al., 2016). A recent study found that the most common trends in characteristics of adolescent e-cigarette users are being male, older age, having more pocket money, and having peers who smoke (Perikleous et al., 2018).
Parental influences are strongly related to adolescent tobacco use. Young people may be more likely to use tobacco products if one of their parents uses cigarettes or smokeless tobacco products (Vassoler and Sadri-Vakili, 2014). Lack of support or involvement from parents is also associated with youth tobacco use (HHS, 2012, 2016a).
Adolescents are more also likely to use tobacco products if they see peers using these products and are more motivated to participate in social smoking compared with adult smokers (Bonilha et al., 2013). There is also concern that e-cigarette use may renormalize a smoking culture among young people, subverting decades of antismoking efforts (Bell and Keane, 2014; Kandel and Kandel, 2015; Stanwick, 2015).
Just as the media play an enormous role in underage drinking, they portray tobacco use as normative. Manufacturers and retailers of tobacco products market aggressively to youth through the Internet, social media, television, radio, event sponsorship, celebrity placement, and strategic positioning in convenience stores (Cobb, Brookover, and Cobb, 2015; de Andrade, Hastings, and Angus, 2013; Grana and Ling, 2014). In particular, much of the rise in the popularity of e-cigarettes has stemmed from innovative advertising campaigns that target adolescents through social media (Jackler et al., 2019; Mantey et al., 2016). An analysis of e-cigarette retail websites and marketing and promotional campaigns revealed recurrent appeals to adolescents, such as use by celebrities, feature cartoons, and sexual appeal (Grana and Ling, 2014).
The active enforcement of youth access laws is critical to preventing adolescent tobacco use. E-cigarettes are illegal to purchase under the age
of 18, and even 21 in many states (Morain and Malek, 2017; Murthy, 2017; Wang et al., 2014). However, youth frequently report purchasing these devices from retail locations in person as well as online (Mantey et al., 2019; Meyers, Delucchi, and Halpern-Felsher, 2017). As of November 2018, a new FDA regulation requires stronger age verification for online sales of e-cigarettes, as well as the removal of e-cigarette products from the market that are marketed to children or are appealing to youth (U.S. Food and Drug Administration, 2018b).
Sexual Behavior in Adolescence
Trends
First sexual intercourse, or sexual debut, is an important milestone in sexual and human development. While there appear to be no consistent negative consequences of protected and consensual intercourse between adolescents, the empirical literature reflects broad consensus that earlier age of first intercourse is associated with a higher risk of not using contraception, not using barrier methods of protection against STIs, and higher rates of unintended pregnancy and STIs (Burke, Gabhainn, and Kelly, 2018; Santelli et al., 2017).
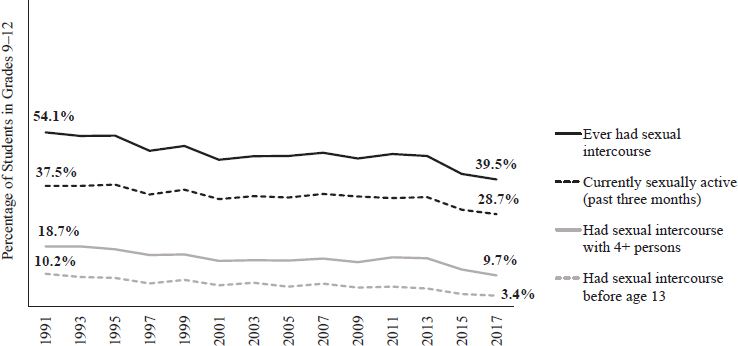
The prevalence of sexual intercourse among adolescents has decreased overall since 1991 (CDC, 2019b) (see Figure 3-8).8 According to the YRBS, the percentage of students in grades 9–12 who reported ever having sexual intercourse decreased from 54.1 percent in 1991 to 39.5 percent in 2017 (CDC, 2019b). In the same time period, the percentage who first had sexual intercourse before age 13 decreased from 10.2 percent to 3.4 percent. Among those reporting sexual experience, the percentage who were currently sexually active (in the past 3 months) also decreased overall, from 37.5 percent to 28.7 percent, and the percentage who had had sexual intercourse with four or more people in their lifetime decreased from 18.7 percent to 9.7 percent. These decreasing trends were consistent by both biological sex and race/ethnicity.
Research has shown that those who engage in vaginal sex at an earlier age also have more sexual partners (Sandfort et al., 2008). However, more recent research also suggests that numbers of sexual partners may be more consequential for health outcomes than age at sexual debut. Kahn and Halpern (2018) found that those who initiated sex early but had fewer lifetime partners exhibited better health outcomes from adolescence to early adulthood, including fewer STI/sexually transmitted disease (STD) diagnoses
___________________
8 As noted previously, “sexual intercourse” is not defined in the YRBS. The result can be biased estimates, particularly for LGBTQ youth.
SOURCE: Generated using Youth Risk Behavior Survey data (CDC, 2019b).
and unintended pregnancies and better romantic relationship quality relative to those who initiated later but reported more sexual partners.
With respect to sexuality in relation to adolescent risk taking, risk factors associated with sexual activity among adolescents are those that increase the likelihood of unintended pregnancy and/or an STI. Teenagers can reduce their chances of experiencing these outcomes by using proper and effective contraception. Indeed, cross-national research suggests that most teenagers can engage safely in sexual behavior if provided with adequate access to contraception and sexual education (Harden, 2014; Santelli, Sandfort, and Orr, 2008). Unfortunately, the potential negative or unintended consequences of unprotected sexual behavior, such as having an unintended pregnancy or acquiring an STI, affect adolescents disproportionately (NASEM, 2019).
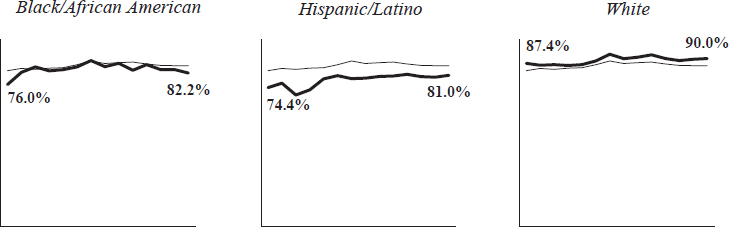
In every YRBS year, a consistent majority of sexually active adolescents reported using a method to prevent pregnancy, whether condoms or some other method, at last sexual intercourse. Furthermore, use of any method increased overall from 1991 (83.5%) to 2017 (86.2%). However, despite greater increases in use of contraception among black/African American (76.0% to 82.2%) and Hispanic (74.4% to 81.0%) adolescents compared with their white counterparts (87.4% to 90.0%), overall disparities still exist among these racial/ethnic groups (CDC, 2019b) (see Figure 3-9).9
Although YRBS data suggest a number of promising trends in sexual behavior among adolescents, including later onset of sexual intercourse, fewer lifetime sexual partners, and high rates of contraceptive use
___________________
9 There were insufficient data to report trends for American Indian/Alaska Native, Asian, and Native Hawaiian/Pacific Islander populations.
NOTE: Consistent data for American Indian/Alaska Native, Asian, and Native Hawaiian/Pacific Islander populations were not available for this Youth Risk Behavior Survey item.
SOURCE: Generated using Youth Risk Behavior Survey data (CDC, 2019b).
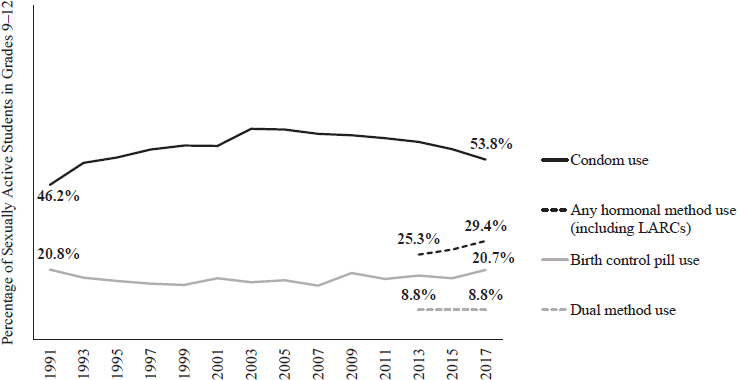
among both males and females and across racial/ethnic groups, condom use among sexually active adolescents fell from 61.5 percent in 2007 to 53.8 percent in 2017 (CDC, 2019b). Importantly, while the proportion of sexually active adolescents who used effective hormonal birth control (long-acting reversible contraceptives [LARCs] or other hormonal methods) increased by 4.1 percent from 2013 to 2017 (CDC, 2019b), these forms of contraception are not effective against STIs. Dual protection (a condom and a hormonal birth control method) can help prevent both STIs and pregnancy; consistently, however, only 8.8 percent of sexually active high school students reported using both a condom and effective hormonal birth control at last intercourse (Kann et al., 2018) (see Figure 3-10).
Health Outcomes Associated with Sexual Behavior During Adolescence
As noted, both unintended pregnancy and STIs/STDs are among the most important adverse health outcomes associated with sexual behavior.
Pregnancy
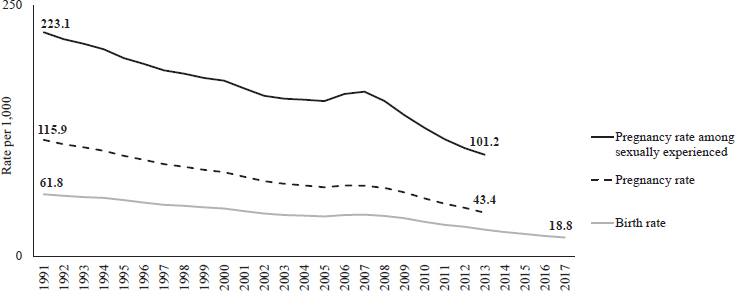
Pregnancy and birth rates among 15- to 19-year-olds in the United States have decreased over time (CDC, 2018d; Kost, Maddow-Zimet, and Arpaia, 2017; Martin et al., 2018). Between 1991 and 2013, pregnancy rates for all 15- to 19-year-old females decreased from 115.9 to 43.4 per 1,000, while pregnancy rates among sexually experienced females decreased from 223.1 to 101.2 per 1,000. Birth rates also decreased, from 61.8 per
SOURCE: Generated using Youth Risk Behavior Survey data (CDC, 2019b).
1,000 in 1991 to 18.8 per 1,000 in 2017 (CDC, 2018d; Martin et al., 2018) (see Figure 3-11).
Much of the decrease in the teen pregnancy and birth rates has been attributed to greater access to contraception rather than to overall reductions in sexual behavior (Lindberg, Santelli, and Desai, 2016, 2018; Santelli et al., 2007). Furthermore, recent research suggests that reality television, such as the MTV shows “16 and Pregnant” and “Teen Mom,” which depict the struggles of teen mothers, may have contributed to up to a third of the decline in teenage births between when they first aired in 2009 and 2010 (Kearney and Levine, 2015).
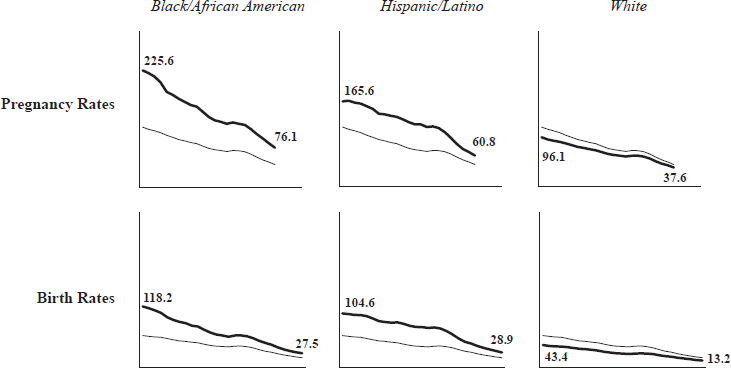
Despite promising trends overall, racial and ethnic differences in teen pregnancy and birth rates persist. In 2013, teen pregnancy rates were 76.1 per 1,000 for black adolescents and 60.8 per 1,000 for Hispanic adolescents, compared with 37.6 per 1,000 for white adolescents (Kost, Maddow-Zimet, and Arpaia, 2017) (see Figure 3-12). In 2017, birth rates were 27.5 per 1,000 for black adolescents and 28.9 per 1,000 for Hispanic adolescents, compared with 13.2 per 1,000 for white adolescents (CDC, 2018d; Martin et al., 2018) (refer to Figure 3-12). Although much progress has been made in reducing teen pregnancy overall, these significant racial/ethnic disparities indicate that black/African American and Hispanic/Latino female adolescents still need additional services and supports.
Social and economic disadvantage are strongly associated with disparities in teen pregnancy and birth rates (Kearney and Levine, 2012). For
SOURCE: Generated using pregnancy data from the National Survey of Family Growth, as analyzed by Kost, Maddow-Zimet, and Arpaia (2017) and birth surveillance data from the Centers for Disease Control and Prevention (2018d) and Martin et al. (2018).
NOTES: Pregnancy rate data for other racial/ethnic populations were not available in this source.
“Other” race was excluded because (1) the composition of this group varies by data source, and (2) the significant heterogeneity of this group limits the conclusions that can be drawn.
SOURCES: Generated using pregnancy data from the National Survey of Family Growth, as analyzed by Kost, Maddow-Zimet, and Arpaia (2017) and birth surveillance data from the Centers for Disease Control and Prevention (2018d) and Martin et al. (2018).
example, adolescents who are in child welfare systems are at a higher risk of teenage pregnancy and birth relative to other groups (Boonstra, 2011). Additionally, adolescents living in lower-income neighborhoods with high levels of unemployment are more likely to become pregnant and give birth compared with adolescents living in neighborhoods with greater income and employment opportunities (Penman-Aguilar et al., 2013).
A variety of evidence-based teen pregnancy prevention programs and interventions, including a number of those on the TPP registry of programs, have shown effectiveness in preventing unintended teen pregnancies in diverse populations and settings (Fish et al., 2014; Lugo-Gil et al., 2018). In addition to prevention programs, adolescents need support from parents and other trusted adults in making healthy choices about relationships, sex, and birth control. Adolescents also need access to youth-friendly contraceptive and reproductive health services. Community efforts to address the social and economic factors associated with teenage pregnancy can play a major role as well in tackling racial/ethnic and geographic disparities in teen birth rates (CDC, 2019f; Kearney and Levine, 2012).
Sexually Transmitted Infections and Diseases
The United States has the highest rate of STIs in the industrialized world. A combination of behavioral, biological, and cultural factors put sexually active adolescents at higher risk of contracting STIs compared with other age groups. Young people ages 15 to 24 account for nearly half of all new cases of STIs each year (CDC, 2018e). In particular, female and black young people are significantly more likely to contract an STI (CDC, 2018e, 2018f).
The most effective way to prevent STIs is to abstain from sexual activity. For those who are sexually active, using a condom correctly every time one has sex can reduce the likelihood of contracting an STI. Yet while condoms are the most effective way to prevent STIs, they are not the most effective way to prevent pregnancy. As mentioned previously, the best way to prevent both STIs and pregnancy is using dual protection, defined as using both a condom and a form of hormonal birth control (CDC, 2018g).
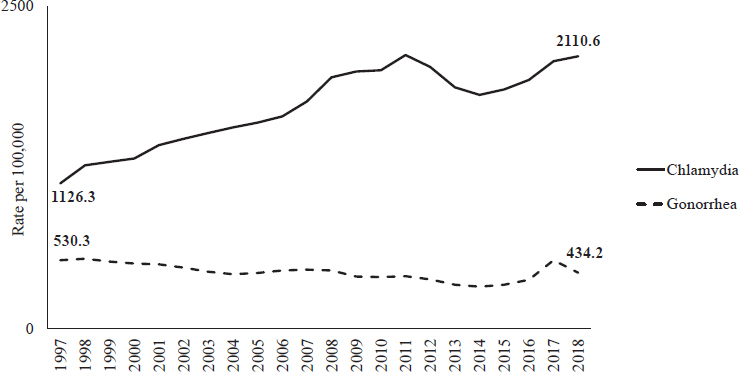
The most common STIs among young people in the United States are chlamydia and gonorrhea. Chlamydia rates among 15- to 19-year-olds have increased over time, from 1,126.3 per 100,000 in 1997 to 2,110.6 per 100,000 in 2018, peaking at 2,082.7 per 100,000 in 2011. In contrast, gonorrhea rates per 100,000 15- to 19-year-olds decreased from 1997 (530.3) to 2014 (325.0), but increased from 2014 to 2017 (438.2) (CDC, 2019g, 2019h) (see Figure 3-13).
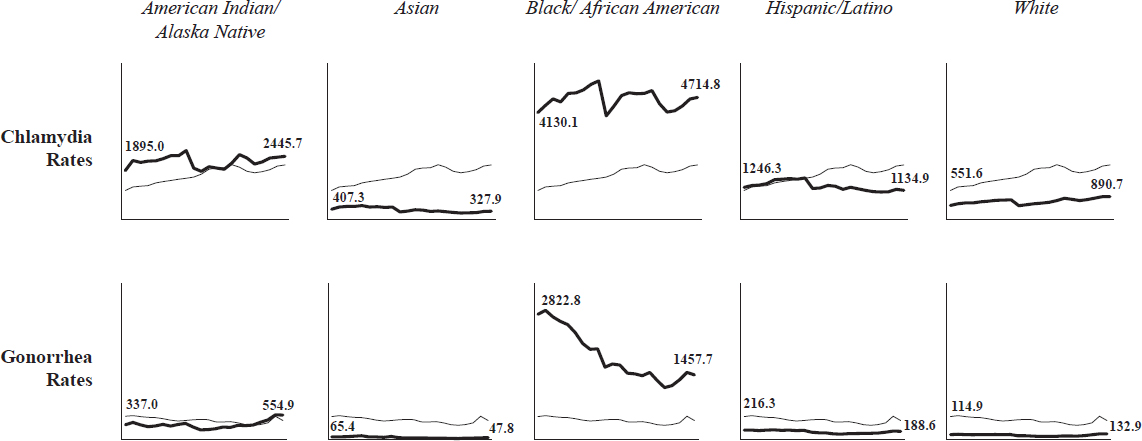
There are also significant and persistent disparities in chlamydia and gonorrhea rates among 15- to 19-year-olds by race/ethnicity, with sig-
SOURCE: Generated using sexually transmitted disease surveillance data from the Centers for Disease Control and Prevention (2019g, 2019h).
nificantly higher rates among black teens at every time point. In 2018, chlamydia rates per 100,000 for black youth were 4,714.8, compared with 2,445.7 for American Indian/Alaska Native, 327.9 for Asian, 1,134.9 for Hispanic/Latino, and 890.7 for white adolescents. Similarly, gonorrhea rates per 100,000 were highest among black adolescents (1,457.7), followed by American Indian/Alaska Native (554.9), Hispanic/Latino (188.6), white (132.9) and Asian (47.8) youth (CDC, 2019g, 2019h) (see Figure 3-14).
Social and Environmental Influences
As mentioned in Chapter 1, sexual development is distinctly different from alcohol and tobacco use because it represents a critical task of adolescence. As a part of their sexual development, adolescents typically form intimate partnerships, affirm gender identities, identify sexual orientations, situate sexuality in the context of their religious beliefs, and incorporate cultural attitudes toward sexuality into their own value systems, all of which help them prepare for adult roles and relationships (Diamond and Savin-Williams, 2009; Everett, 2019; NASEM, 2019; Suleiman et al, 2017; Tulloch and Kaufman, 2013).
Based on growing scientific evidence, sexual activity is increasingly considered a normative aspect of adolescent development (NASEM, 2019; Tolman and McClelland, 2011). However, rather than navigating a binary
SOURCE: Generated using sexually transmitted disease surveillance data from the Centers for Disease Control and Prevention (2019g, 2019h).
division between positive or risky, adolescent sexual activity can be characterized as both positive and risky. This framework embraces the reality that adolescents must learn about themselves, their bodies, intimate partners, and relationships within contexts in which they are required to both manage risks and develop positive patterns for sexuality into adulthood (Harden, 2014; Tolman and McClelland, 2011).
While unhealthy risk behaviors can occur within a sexual context, having sex is not necessarily unhealthy or problematic, even in adolescence. However, this does not imply that all sexual activity is healthy and positive or that abstinence is unhealthy. Rather, whether sexual behaviors are labeled “healthy” or “unhealthy” is highly dependent on the individual, the context, and cultural influences (Harden, 2014; Tolman and McClelland, 2011).
Parental attitudes toward sexuality and parenting style are important factors contributing to an adolescent’s sexual attitudes and behaviors, as parents typically serve as models for normative behaviors and attitudes (Tulloch and Kaufman, 2013). Parents can also support healthy sexual development by providing age- and developmentally appropriate information on sexual topics including puberty, reproduction, pregnancy prevention, STIs, healthy relationships, sexual orientation, gender identity, consent, boundaries, and body image. Furthermore, parents can help adolescents build critical thinking skills with which to assess the reliability of sexual information portrayed in the media, teach them about their rights and responsibilities in romantic relationships and sexual activities, and address ways to deal with peer pressure (Ashcraft and Murray, 2017; Berkel, 2019; Hagan, Shaw, and Duncan, 2017; McNeely and Blanchard, 2010; NASEM, 2019).
Adolescents also use peers as a resource to learn about sexuality (McNeely and Blanchard, 2010; Tolman and McClelland, 2011). Unfortunately, peers can be a source of inaccurate and misleading information. For instance, many adolescents overestimate the sexual activity of their peers, which can result in feeling pressured to “catch up” (Warner et al., 2011). Peers often exert pressure to conform to the “normal behavior” of their peer group. An adolescent’s sexual activities or experience can also affect social standing, leading to damaging rumors, peer group rejection, partner rejection, regret or remorse, vulnerability, and depression.
Physicians can also play a role in an adolescent’s understanding of sexuality. According to the CDC (2018h), six major elements are involved in youth-friendly sexual and reproductive health services: (1) confidentiality, (2) privacy, (3) consent, (4) cultural and linguistic appropriateness, (5) comprehensive services, and (6) parent/guardian involvement. The best services provide youth with clear, accurate information about their rights, make them feel respected and engaged in their health care, and address their
contraceptive and reproductive health needs at every visit (CDC, 2018h). Adolescents with developmental disabilities, chronic health conditions, or physical disabilities in particular may benefit from these services, as conversations with physicians may be one of the only ways they can receive accurate information related to sexuality and their conditions (Horner-Johnson and Sauvé, 2019).
Finally, the prominent and multifaceted role of the media in adolescent sexual development is one of the greatest differences between today’s adolescents and those of prior generations. Adolescents can access a large amount of sexual content online, some of which is misleading and can lead to unhealthy sexual behaviors. In recent decades, moreover, adolescents have had more access to literature related to sexuality, to media coverage of sexual crimes and violence, and to portrayals of sexuality on television and the Internet (Harris, 2011). Media use can also facilitate dating and romantic relationships. In particular, dating apps and websites have revolutionized how people meet and engage, and access to technology and social media has made it even easier to establish and maintain romantic relationships (Lenhart and Duggan, 2014; Seemiller and Grace, 2018).
CONCLUSIONS
Based on the findings presented in this chapter, the committee drew the following conclusions.
CONCLUSION 3-1: Risk-taking activities are a normal and necessary part of adolescence because of the heightened neurological plasticity of the brain that makes it especially malleable and responsive to experiences, as well as the developmental purpose of such activities of preparing youth for adulthood. Therefore, “discontinuation of risk” is applicable only to those unhealthy risk behaviors (e.g., substance abuse, unprotected sexual activity) that can lead to negative health outcomes (e.g., diseases, unintended pregnancy, sexually transmitted infections).
CONCLUSION 3-2: The current Youth Risk Behavior Survey does not reflect the experiences of out-of-school adolescents (e.g., dropped out, homeless), many of whom are more likely to engage or have engaged in unhealthy risk behaviors.
CONCLUSION 3-3: The sexual behavior items included in the Youth Risk Behavior Survey are neither specific nor comprehensive enough to (1) provide the most accurate estimates of the sexual behaviors in which today’s youth engage and (2) represent the experiences of LGBTQ populations.
CONCLUSION 3-4: There are significant racial and ethnic disparities in health behaviors and outcomes, which are related to differences in access to opportunities and supports (see Conclusion 2-1 in Chapter 2). Therefore, disadvantaged youth need more resources to reduce such disparities and ensure access to comparable opportunities (see Conclusion 2-3 in Chapter 2).
CONCLUSION 3-5: Unlike alcohol and tobacco use, sexual development represents a critical developmental task that prepares adolescents for adult roles and relationships. It is therefore just as important to support healthy sexual development as it is to prevent the negative health outcomes associated with sexual behavior (e.g., unintended pregnancy, sexually transmitted infections) during adolescence.
The next chapter of this report documents the process and findings of the committee’s review of core components of programs and interventions that have been found to be successful in promoting positive health behaviors and outcomes among adolescents using the optimal health framework.
REFERENCES
Adger Jr., H., and Saha, S. (2013). Alcohol use disorders in adolescents. Pediatrics in Review, 34(3), 103–113.
Albert, D., Chein, J., and Steinberg, L. (2013). The teenage brain: Peer influences on adolescent decision making. Current Directions in Psychological Science, 22(2), 114–120.
Ambrose, B.K., Rostron, B.L., Johnson, S.E., Portnoy, D.B., Apelberg, B.J., Kaufman, A.R., and Choiniere, C.J. (2014). Perceptions of the relative harm of cigarettes and e-cigarettes among U.S. youth. American Journal of Preventive Medicine, 47(2 Suppl 1), S53–S60.
Amrock, S.M., Lee, L., and Weitzman, M. (2016). Perceptions of e-cigarettes and noncigarette tobacco products among U.S. youth. Pediatrics, 138(5).
Anand, V., McGinty, K.L., O’Brien, K., Guenthner, G., Hahn, E., and Martin, C.A. (2015). E-cigarette use and beliefs among urban public high school students in North Carolina. Journal of Adolescent Health, 57(1), 46–51.
Arrazola, R.A., Neff, L.J., Kennedy, S.M., Holder-Hayes, E., and Jones, C.D. (2014). Tobacco use among middle and high school students—United States, 2013. Morbidity and Mortality Weekly Report, 63(45), 1021–1026.
Ashcraft, A.M., and Murray, P.J. (2017). Talking to parents about adolescent sexuality. Pediatric Clinics of North America, 64(2), 305–320.
Bell, K., and Keane, H. (2014). All gates lead to smoking: The ‘gateway theory,’ e-cigarettes and the remaking of nicotine. Social Science & Medicine, 119, 45–52.
Berkel, C. (2019). The Role of Sexual Agency and Consent in Healthy Adolescent Development. Paper commissioned by the Committee on Applying Lessons of Optimal Adolescent Health to Improve Behavioral Outcomes for Youth. Available: https://www.nap.edu/resource/25552/The%20Role%20of%20Sexual%20Agency%20and%20Consent%20in%20Healthy%20Adolescent%20Development.pdf.
Blakemore, S-J. (2018). Avoiding social risk in adolescence. Current Directions in Psychological Science, 27(2), 116–122.
Blakemore, S-J., and Robbins, T.W. (2012). Decision-making in the adolescent brain. Nature Neuroscience, 15, 1184.
Bonilha, A.G., de Souza, E.S., Sicchieri, M.P., Achcar, J.A., Crippa, J.A., and Baddini-Martinez, J. (2013). A motivational profile for smoking among adolescents. Journal of Addiction Medicine, 7(6), 439–446.
Boonstra, H.D. (2011). Teen pregnancy among young women in foster care: A primer. Policy Review, 14(2), 8–19.
Braams, B.R., van Duijvenvoorde, A.C., Peper, J.S., and Crone, E.A. (2015). Longitudinal changes in adolescent risk-taking: A comprehensive study of neural responses to rewards, pubertal development, and risk-taking behavior. Journal of Neuroscience, 35(18), 7226–7238.
Brener, N.D., Eaton, D.K., Kann, L., Grunbaum, J.A., Gross, L.A., Kyle, T.M., and Ross, J.G. (2006). The association of survey setting and mode with self-reported health risk behaviors among high school students. Public Opinion Quarterly, 70(3), 354–374.
Brener, N.D., Kann, L., Shanklin, S., Kinchen, S., Eaton, D.K., Hawkins, J., and Flint, K.H. (2013). Methodology of the Youth Risk Behavior Surveillance System—2013. Morbidity and Mortality Weekly Report: Recommendations and Reports, 62(1), 1–20.
Bronfenbrenner, U. (1994). Ecological models of human development. Readings on the Development of Children, 2(1), 37–43.
Burke, L., Gabhainn, S.N., and Kelly, C. (2018). Socio-demographic, health and lifestyle factors influencing age of sexual initiation among adolescents. International Journal of Environmental Research and Public Health, 15(9).
Cahn, Z. and Siegel, M. (2011). Electronic cigarettes as a harm reduction strategy for tobacco control: A step forward or a repeat of past mistakes? Journal of Public Health Policy, 32(1), 16–31.
Catalano, R.F., Fagan, A.A., Gavin, L.E., Greenberg, M.T., Irwin Jr., C.E., Ross, D.A., and Shek, D.T.L. (2012). Worldwide application of prevention science in adolescent health. The Lancet, 379(9826), 1653–1664.
Centers for Disease Control and Prevention (CDC). (2018a). School Connectedness. Available: https://www.cdc.gov/healthyyouth/protective/school_connectedness.htm.
———. (2018b). Youth Risk Behavior Surveillance System (YRBSS) Overview. Available: https://www.cdc.gov/healthyyouth/data/yrbs/overview.htm.
———. (2018c). YRBS Questionnaires: 1991–2019. Atlanta, GA: Author.
———. (2018d). Birth Rates for Females by Age Group: United States. Hyattsville, MD: Author.
———. (2018e). STDs in adolescents and young adults. Sexually Transmitted Disease Surveillance 2017: Special Focus Profiles. Available: https://www.cdc.gov/std/stats17/adolescents.htm.
———. (2018f). STDs in racial and ethnic minorities. Sexually Transmitted Disease Surveillance 2017: Special Focus Profiles Available: https://www.cdc.gov/std/stats17/minorities.htm.
———. (2018g). Contraception. Available: https://www.cdc.gov/reproductivehealth/contraception/index.htm.
———. (2018h). Teen-Friendly Reproductive Health Visit. Available: https://www.cdc.gov/teenpregnancy/health-care-providers/teen-friendly-health-visit.htm.
———. (2019a). Youth Violence. Available: https://www.cdc.gov/violenceprevention/youthviolence/index.html.
———. (2019b). Youth Risk Behavior Surveillance System (YRBSS) Youth Online High School Results. Available: https://nccd.cdc.gov/Youthonline/App/Results.aspx.
———. (2019c). Leading Causes of Death Reports, 1981–2017. Available: https://webappa.cdc.gov/sasweb/ncipc/leadcause.html.
———. (2019d). Teen Drivers: Get the Facts. Available: https://www.cdc.gov/motorvehiclesafety/teen_drivers/teendrivers_factsheet.html.
———. (2019e). Outbreak of Lung Injury Associated with the Use of E-cigarette, or Vaping, Products. Available: https://www.cdc.gov/tobacco/basic_information/e-cigarettes/severelung-disease.html.
———. (2019f). Social Determinants and Eliminating Disparities in Teen Pregnancy. Available: https://www.cdc.gov/teenpregnancy/about/social-determinants-disparities-teen-pregnancy.htm.
———. (2019g). CDC Sexually Transmitted Diseases (STDs) Data and Statistics–Archive. Available: https://www.cdc.gov/std/stats/archive.htm.
———. (2019h). Sexually Transmitted Disease Surveillance 2018. Atlanta, GA: Author.
Chung, T., Creswell, K.G., Bachrach, R., Clark, D.B., and Martin, C.S. (2018). Adolescent binge drinking. Alcohol Research, 39(1), 5–15.
Cobb, N.K., Brookover, J., and Cobb, C.O. (2015). Forensic analysis of online marketing for electronic nicotine delivery systems. Tobacco Control, 24(2), 128–131.
Cooper, M., Harrell, M.B., Perez, A., Delk, J., and Perry, C.L. (2016). Flavorings and perceived harm and addictiveness of e-cigarettes among youth. Tobacco Regulatory Science, 2(3), 278–289.
Cross, S.J., Lotfipour, S., and Leslie, F.M. (2017). Mechanisms and genetic factors underlying co-use of nicotine and alcohol or other drugs of abuse. American Journal of Drug and Alcohol Abuse, 43(2), 171–185.
Curtin, S.C., Heron, M., Minino, A.M., and Warner, M. (2018). Recent increases in injury mortality among children and adolescents aged 10–19 years in the United States: 1999–2016. National Vital Statistics Reports, 67(4), 1–16.
David-Ferdon, C., Vivolo-Kantor, A.M., Dahlberg, L.L., Marshall, K.J., Rainford, N., and Hall, J.E. (2016). A Comprehensive Technical Package for the Prevention of Youth Violence and Associated Risk Behaviors. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention.
de Andrade, M., Hastings, G., and Angus, K. (2013). Promotion of electronic cigarettes: Tobacco marketing reinvented? British Medical Journal, 347, f7473.
Denniston, M.M., Brener, N.D., Kann, L., Eaton, D.K., McManus, T., Kyle, T.M., Roberts, A.M., Flint, K.H., and Ross, J.G. (2010). Comparison of paper-and-pencil versus web administration of the Youth Risk Behavior Survey (YRBS): Participation, data quality, and perceived privacy and anonymity. Computers in Human Behavior, 26(5), 1054–1060.
Diamond, L.M., and Savin-Williams, R.C. (2009). Adolescent sexuality. In R.M. Lerner and L. Steinberg (Eds.), Handbook of Adolescent Psychology: Individual Bases of Adolescent Development (pp. 479–524). Hoboken, NJ: John Wiley & Sons, Inc.
Duell, N., and Steinberg, L. (2019). Positive risk taking in adolescence. Child Development Perspectives, 13(1), 48–52.
Eaton, D.K., Brener, N.D., Kann, L., Denniston, M.M., McManus, T., Kyle, T.M., Roberts, A.M., Flint, K.H., and Ross, J.G. (2010). Comparison of paper-and-pencil versus web administration of the Youth Risk Behavior Survey (YRBS): Risk behavior prevalence estimates. Evaluation Review, 34(2), 137–153.
Edidin, J.P., Ganim, Z., Hunter, S.J., and Karnik, N.S. (2012). The mental and physical health of homeless youth: A literature review. Child Psychiatry & Human Development, 43(3), 354–375.
Everett, B.G. (2019). Optimal Adolescent Health to Improve Behavioral Outcomes for LGBTQ Youth. Paper commissioned by the Committee on Applying Lessons of Optimal Adolescent Health to Improve Behavioral Outcomes for Youth. Available: https://www.nap.edu/resource/25552/Optimal%20Adolescent%20Health%20to%20Improve%20Behavioral%20Outcomes%20for%20LGBTQ%20Youth.pdf.
Fadus, M.C., Smith, T.T., and Squeglia, L.M. (2019). The rise of e-cigarettes, pod mod devices, and JUUL among youth: Factors influencing use, health implications, and downstream effects. Drug and Alcohol Dependence, 201, 85–93.
Falk, E.B., Cascio, C.N., O’Donnell, M.B., Carp, J., Tinney Jr., F.J., Bingham, C.R., Shope, J.T., Ouimet, M.C., Pradhan, A.K., and Simons-Morton, B.G. (2014). Neural responses to exclusion predict susceptibility to social influence. Journal of Adolescent Health, 54(5 Suppl), S22–S31.
Fish, H., Manlove, J., Moore, K.A., and Mass, E. (2014). What Works for Adolescent Sexual and Reproductive Health: Lessons from Experimental Evaluations of Programs and Interventions. Bethesda, MD: Child Trends.
Fosco, G.M., Frank, J.L., Stormshak, E.A., and Dishion, T.J. (2013). Opening the “black box”: Family check-up intervention effects on self-regulation that prevents growth in problem behavior and substance use. Journal of School Psychology, 51(4), 455–468.
Freudenberg, N. and Ruglis, J. (2007). Reframing school dropout as a public health issue. Preventing Chronic Disease: Public Health Research, Practice, and Policy, 4(4).
Gentzke, A.S., Creamer, M., Cullen, K.A., Ambrose, B.K., Willis, G., Jamal, A., and King, B.A. (2019). Vital signs: Tobacco product use among middle and high school students—United States, 2011–2018. Morbidity and Mortality Weekly Report, 68(6), 157–164.
Gershon, P., Zhu, C., Klauer, S.G., Dingus, T., and Simons-Morton, B. (2017). Teens’ distracted driving behavior: Prevalence and predictors. Journal of Safety Research, 63, 157–161.
Gnambs, T. and Kaspar, K. (2015). Disclosure of sensitive behaviors across self-administered survey modes: A meta-analysis. Behavior Research Methods, 47(4), 1237–1259.
Goliath, V. and Pretorius, B. (2016). Peer risk and protective factors in adolescence: Implications for drug use prevention. Social Work, 52(1), 113–129.
Gorukanti, A., Delucchi, K., Ling, P., Fisher-Travis, R., and Halpern-Felsher, B. (2017). Adolescents’ attitudes towards e-cigarette ingredients, safety, addictive properties, social norms, and regulation. Preventive Medicine, 94, 65–71.
Graber, J.A., Nichols, T.R., and Brooks-Gunn, J. (2010). Putting pubertal timing in developmental context: Implications for prevention. Developmental Psychobiology, 52(3), 254–262.
Grana, R.A., and Ling, P.M. (2014). “Smoking revolution”: A content analysis of electronic cigarette retail websites. American Journal of Preventive Medicine, 46(4), 395–403.
Hagan, J.F., Shaw, J.S., and Duncan, P.M. (2017). Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents (4th ed.). Elk Grove, IL: American Academy of Pediatrics.
Harden, K.P. (2014). A sex-positive framework for research on adolescent sexuality. Perspectives on Psychological Science, 9(5), 455–469.
Harding, F.M., Hingson, R.W., Klitzner, M., Mosher, J.F., Brown, J., Vincent, R.M., Dahl, E., and Cannon, C.L. (2016). Underage drinking: A review of trends and prevention strategies. American Journal of Preventive Medicine, 51(4), S148–S157.
Harrell, M.B., Loukas, A., Jackson, C.D., Marti, C.N., and Perry, C.L. (2017). Flavored tobacco product use among youth and young adults: What if flavors didn’t exist? Tobacco Regulatory Science, 3(2), 168–173.
Harris, A.L. (2011). Media and technology in adolescent sexual education and safety. Journal of Obstetric, Gynecologic & Neonatal Nursing, 40(2), 235–242.
Hartley, C.A., and Somerville, L.H. (2015). The neuroscience of adolescent decision-making. Current Opinion in Behavioral Sciences, 5, 108–115.
Haydon, A.A., Herring, A.H., Prinstein, M.J., and Halpern, C.T. (2012). Beyond age at first sex: Patterns of emerging sexual behavior in adolescence and young adulthood. Journal of Adolescent Health, 50(5), 456–463.
Hebert, E.T., Case, K.R., Kelder, S.H., Delk, J., Perry, C.L., and Harrell, M.B. (2017). Exposure and engagement with tobacco- and e-cigarette-related social media. Journal of Adolescent Health, 61(3), 371–377.
Heitzeg, N.A. (2009). Education or incarceration: Zero tolerance policies and the school to prison pipeline. Forum on Public Policy, 9(2).
Henges, A.L., and Marczinski, C.A. (2012). Impulsivity and alcohol consumption in young social drinkers. Addictive Behaviors, 37(2), 217–220.
Hingson, R., and White, A. (2014). New research findings since the 2007 Surgeon General’s call to action to prevent and reduce underage drinking: A review. Journal of Studies on Alcohol and Drugs, 75(1), 158–169.
Hofmann, W., Schmeichel, B.J., and Baddeley, A.D. (2012). Executive functions and self-regulation. Trends in Cognitive Sciences, 16(3), 174–180.
Holmes, C., Brieant, A., Kahn, R., Deater-Deckard, K., and Kim-Spoon, J. (2019). Structural home environment effects on developmental trajectories of self-control and adolescent risk taking. Journal of Youth and Adolescence, 48(1), 43–55.
Horner-Johnson, W. and Sauvé, L. (2019). Applying Lessons of Optimal Adolescent Health to Improve Behavioral Outcomes for Youth with Disabilities. Paper commissioned by the Committee on Applying Lessons of Optimal Adolescent Health to Improve Behavioral Outcomes for Youth. Available: https://www.nap.edu/resource/25552/Applying%20Lessons%20of%20Optimal%20Adolescent%20Health%20to%20Improve%20Behavioral%20Outcomes%20for%20Youth%20with%20Disabilities.pdf.
Hughes, K., Bellis, M.A., Hardcastle, K.A., McHale, P., Bennett, A., Ireland, R., and Pike, K. (2015). Associations between e-cigarette access and smoking and drinking behaviours in teenagers. BMC Public Health, 15, 244.
Institute of Medicine. (2011). The Science of Adolescent Risk-Taking: Workshop Report. Washington, DC: The National Academies Press.
Institute of Medicine and National Research Council. (2013). Priorities for Research to Reduce the Threat of Firearm-Related Violence. Washington, DC: The National Academies Press.
Institute of Medicine and National Research Council. (2014). The Evidence for Violence Prevention Across the Lifespan and Around the World: Workshop Summary. Washington, DC: The National Academies Press.
Jackler, R.K., Li, V.Y., Cardiff, R.A.L., and Ramamurthi, D. (2019). Promotion of tobacco products on Facebook: Policy versus practice. Tobacco Control, 28, 67–73.
Jamal, A., Gentzke, A., Hu, S.S., Cullen, K.A., Apelberg, B.J., Homa, D.M., and King, B.A. (2017). Tobacco use among middle and high school students—United States, 2011–2016. Morbidity and Mortality Weekly Report, 66(23), 597–603.
Jha, P., Ramasundarahettige, C., Landsman, V., Rostron, B., Thun, M., Anderson, R.N., McAfee, T., and Peto, R. (2013). 21st-century hazards of smoking and benefits of cessation in the United States. New England Journal of Medicine, 368(4), 341–350.
Judd, B. (2019). Shared Risk and Protective Factors Impacting Adolescent Behavior and Positive Development. Anchorage, AK: Alaska Division of Behavioral Health.
Kahn, N.F., and Halpern, C.T. (2018). Associations between patterns of sexual initiation, sexual partnering, and sexual health outcomes from adolescence to early adulthood. Archives of Sexual Behavior, 47(6), 1791–1810.
Kandel, D., and Kandel, E. (2015). The gateway hypothesis of substance abuse: Developmental, biological and societal perspectives. Acta Paediatrica, 104(2), 130–137.
Kann, L., McManus, T., Harris, W.A., Shanklin, S.L., Flint, K.H., Queen, B., Lowry, R., Chyen, D., Whittle, L., Thornton, J., Lim, C., Bradford, D., Yamakawa, Y., Leon, M., Brener, N., and Ethier, K.A. (2018). Youth risk behavior surveillance—United States, 2017. Morbidity and Mortality Weekly Report Surveillance Summaries, 67(8).
Kavuluru, R., Han, S., and Hahn, E.J. (2019). On the popularity of the USB flash drive-shaped electronic cigarette JUUL. Tobacco Control, 28(1), 110–112.
Kearney, M.S., and Levine, P.B. (2012). Why is the teen birth rate in the United States so high and why does it matter? Journal of Economic Perspectives, 26(2), 141–163.
Kearney, M.S., and Levine, P.B. (2015). Media influences on social outcomes: The impact of MTV’s 16 and Pregnant on teen childbearing. American Economic Review, 105(12), 3597–3632.
King, B.M., Marino, L.E., and Barry, K.R. (2018). Does the Centers for Disease Control and Prevention’s Youth Risk Behavior Survey underreport risky sexual behavior? Sexually Transmitted Diseases, 45(3), e10–e11.
Knoll, L.J., Magis-Weinberg, L., Speekenbrink, M., and Blakemore, S-J. (2015). Social influence on risk perception during adolescence. Psychological Science, 26(5), 583–592.
Kost, K., Maddow-Zimet, I., and Arpaia, A. (2017). Pregnancies, Births and Abortions among Adolescents and Young Women in the United States, 2013: National and State Trends by Age, Race and Ethnicity. New York, NY: Guttmacher Institute.
Langton, C.E. and Berger, L.M. (2011). Family structure and adolescent physical health, behavior, and emotional well-being. Social Services Review, 85(3), 323–357.
Lee, Y-K., Chang, C-T., Lin, Y., and Cheng, Z-H. (2014). The dark side of smartphone usage: Psychological traits, compulsive behavior and technostress. Computers in Human Behavior, 31, 373–383.
Lenhart, A., and Duggan, M. (2014). Couples, the Internet, and Social Media. Washington, DC: Pew Research Center.
Leventhal, T., Dupéré, V., and Brooks-Gunn, J. (2009). Neighborhood influences on adolescent development. In R.M. Lerner, and L. Steinberg (Eds.), Handbook of Adolescent Psychology (vol. 2, pp. 411–443). Hoboken, NJ: John Wiley & Sons, Inc.
Lindberg, L.D., Santelli, J.S., and Desai, S. (2016). Understanding the decline in adolescent fertility in the United States, 2007–2012. Journal of Adolescent Health, 59(5), 577–583.
Lindberg, L.D., Santelli, J.S., and Desai, S. (2018). Changing patterns of contraceptive use and the decline in rates of pregnancy and birth among U.S. adolescents, 2007–2014. Journal of Adolescent Health, 63(2), 253–256.
Livingston, G. (2018). The Changing Profile of Unmarried Parents. Washington, DC: Pew Research Center.
Lopez-Quintero, C., de los Cobos, J.P., Hasin, D.S., Okuda, M., Wang, S., Grant, B.F., and Blanco, C. (2011). Probability and predictors of transition from first use to dependence on nicotine, alcohol, cannabis, and cocaine: Results of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). Drug and Alcohol Dependence, 115(1–2), 120–130.
Lugo-Gil, J., Lee, A., Vohra, D., Harding, J., Ochoa, L., and Goesling, B. (2018). Updated Findings from the HHS Teen Pregnancy Prevention Evidence Review: August 2015 through October 2016. Washington, DC: U.S. Department of Health and Human Services.
Mantey, D.S., Cooper, M.R., Clendennen, S.L., Pasch, K.E., and Perry, C.L. (2016). E-cigarette marketing exposure is associated with e-cigarette use among U.S. youth. Journal of Adolescent Health, 58(6), 686–690.
Mantey, D.S., Barroso, C.S., Kelder, B.T., and Kelder, S.H. (2019). Retail access to e-cigarettes and frequency of e-cigarette use in high school students. Tobacco Regulatory Science, 5(3), 280–290.
Martin, J.A., Hamilton, B.E., Osterman, M.J.K., Driscoll, A.K., and Drake, P. (2018). Births: Final data for 2017. National Vital Statistics Reports, 67(8), 1–50.
Markkula, J., Härkänen, T., and Raitasalo, K. (2019). Drunken driving and riding with a drunken driver: Adolescent types at higher risk. Drugs: Education, Prevention and Policy, 1–8.
Mashhoon, Y., Betts, J., Farmer, S.L., and Lukas, S.E. (2018). Early onset tobacco cigarette smokers exhibit deficits in response inhibition and sustained attention. Drug and Alcohol Dependence, 184, 48–56.
Maslowsky, J., Owotomo, O., Huntley, E.D., and Keating, D. (2019). Adolescent risk behavior: Differentiating reasoned and reactive risk-taking. Journal of Youth and Adolescence, 48(2), 243–255.
McKelvey, K., Baiocchi, M., and Halpern-Felsher, B. (2018). Adolescents’ and young adults’ use and perceptions of pod-based electronic cigarettes. Journal of the American Medical Association Network Open, 1(6), e183535.
McNeely, C. and Blanchard, J. (2010). The Teen Years Explained: A Guide to Healthy Adolescent Development. Baltimore, MD: Johns Hopkins Bloomberg School of Public Health, Center for Adolescent Health.
McWhirter, B.T., McWhirter, E.H., McWhirter, J.J., and McWhirter, R.J. (2013). At-Risk Youth: A Comprehensive Response for Counsellors, Teachers, Psychologists, and Human Services Professionals. Belmont, CA: Thompson Brooks/Cole.
Meisel, S.N. and Colder, C.R. (2019). Adolescent social norms and alcohol use: Separating between- and within-person associations to test reciprocal determinism. Journal of Research on Adolescence. Available: https://doi.org/10.1111/jora.12494.
Meyers, M.J., Delucchi, K., and Halpern-Felsher, B. (2017). Access to tobacco among California high school students: The role of family members, peers, and retail venues. Journal of Adolescent Health, 61(3), 385–388.
Morain, S.R. and Malek, J. (2017). Minimum age of sale for tobacco products and electronic cigarettes: Ethical acceptability of U.S. “tobacco 21 laws.” American Journal of Public Health, 107(9), 1401–1405.
Moreno, M.A., and Whitehill, J.M. (2014). Influence of social media on alcohol use in adolescents and young adults. Alcohol Research: Current Reviews, 36(1), 91.
Murthy, V.H. (2017). E-cigarette use among youth and young adults: A major public health concern. Journal of the American Medical Association Pediatrics, 171(3), 209–210.
Murty, V.P., Calabro, F., and Luna, B. (2016). The role of experience in adolescent cognitive development: Integration of executive, memory, and mesolimbic systems. Neuroscience & Biobehavioral Reviews, 70, 46–58.
MyVoice. (2019). Youth Perspectives on Being Healthy and Thriving. Report commissioned by the Committee on Applying Lessons of Optimal Adolescent Health to Improve Behavioral Outcomes for Youth. Available: https://www.nap.edu/resource/25552/Youth%20Perspectives%20on%20Being%20Healthy%20and%20Thriving.pdf.
National Academies of Sciences, Engineering, and Medicine (NASEM). (2016). Preventing Bullying Through Science, Policy, and Practice. Washington, DC: The National Academies Press.
———. (2017). Community Violence as a Population Health Issue: Proceedings of a Workshop. Washington, DC: The National Academies Press.
———. (2018a). Violence and Mental Health: Opportunities for Prevention and Early Detection: Proceedings of a Workshop. Washington, DC: The National Academies Press.
———. (2018b). Public Health Consequences of E-cigarettes. Washington, DC: The National Academies Press.
———. (2019). The Promise of Adolescence: Realizing Opportunity for All Youth. Washington, DC: The National Academies Press.
National Research Council and Institute of Medicine. (2004). Reducing Underage Drinking: A Collective Responsibility. Washington, DC: The National Academies Press.
Nguyen, N., McKelvey, K., and Halpern-Felsher, B. (2019). Popular flavors used in alternative tobacco products among young adults. Journal of Adolescent Health, 65(2), 306–308.
O’Dea, B., and Campbell, A. (2011). Healthy connections: Online social networks and their potential for peer support. Studies in Health Technology and Informatics, 168, 133–140.
Odgers, C.L., Robins, S.J., and Russell, M.A. (2010). Morbidity and mortality risk among the “forgotten few”: Why are girls in the justice system in such poor health? Law and Human Behavior, 34(6), 429–444.
Odom, S.L., Thompson, J.L., Hedges, S., Boyd, B.A., Dykstra, J.R., Duda, M.A., Szidon, K.L., Smith, L.E., and Bord, A. (2015). Technology-aided interventions and instruction for adolescents with autism spectrum disorder. Journal of Autism and Developmental Disorders, 45(12), 3805–3819.
O’Donnell, M.P. (2017). Health Promotion in the Workplace (5th ed.). Troy, MI: Art & Science of Health Promotion Institute.
O’Keeffe, G.S., and Clarke-Pearson, K. (2011). The impact of social media on children, adolescents, and families. Pediatrics, 127(4), 800–804.
Paschall, M.J., Lipperman-Kreda, S., and Grube, J.W. (2014). Effects of the local alcohol environment on adolescents’ drinking behaviors and beliefs. Addiction, 109(3), 407–416.
Peake, S.J., Dishion, T.J., Stormshak, E.A., Moore, W.E., and Pfeifer, J.H. (2013). Risk-taking and social exclusion in adolescence: Neural mechanisms underlying peer influences on decision-making. Neuroimage, 82, 23–34.
Peck, B., Manning, J., Tri, A., Skrzypczynski, D., Summers, M., and Grubb, K. (2016). What do people mean when they say they “had sex”? Connecting communication and behavior. In J. Manning and C. Noland (Eds.), Contemporary Studies of Sexuality & Communication: Theoretical and Applied Perspectives (pp. 3–13). Dubuque, IA: Kendall Hunt.
Penman-Aguilar, A., Carter, M., Snead, M.C., and Kourtis, A.P. (2013). Socioeconomic disadvantage as a social determinant of teen childbearing in the U.S. Public Health Reports, 128 (Suppl 1), 5–22.
Pepper, J.K., Ribisl, K.M., and Brewer, N.T. (2016). Adolescents’ interest in trying flavoured e-cigarettes. Tobacco Control, 25(Suppl 2), ii62–ii66.
Perikleous, E.P., Steiropoulos, P., Paraskakis, E., Constantinidis, T.C., and Nena, E. (2018). E-cigarette use among adolescents: An overview of the literature and future perspectives. Frontiers in Public Health, 6, 86.
Reyna, V.F. (2012). A new intuitionism: Meaning, memory, and development in fuzzy-trace theory. Judgment and Decision Making, 7(3), 332–359.
Roditis, M., Delucchi, K., Cash, D., and Halpern-Felsher, B. (2016). Adolescents’ perceptions of health risks, social risks, and benefits differ across tobacco products. Journal of Adolescent Health, 58(5), 558–566.
Romer, D. (2010). Adolescent risk taking, impulsivity, and brain development: Implications for prevention. Developmental Psychobiology, 52(3), 263–276.
Romer, D., Reyna, V.F., and Satterthwaite, T.D. (2017). Beyond stereotypes of adolescent risk taking: Placing the adolescent brain in developmental context. Developmental Cognitive Neuroscience, 27, 19–34.
Ross, V., Jongen, E., Brijs, T., Ruiter, R., Brijs, K., and Wets, G. (2015). The relation between cognitive control and risky driving in young novice drivers. Applied Neuropsychology, 22(1), 61–72.
Sanders, S.A., and Reinisch, J.M. (1999). Would you say you had sex if…? Journal of the American Medical Association, 281(3), 275–277.
Sandfort, T.G.M., Orr, M., Hirsch, J.S., and Santelli, J. (2008). Long-term health correlates of timing of sexual debut: Results from a national U.S. study. American Journal of Public Health, 98(1), 155–161.
Santelli, J.S., Lindberg, L.D., Finer, L.B., and Singh, S. (2007). Explaining recent declines in adolescent pregnancy in the United States: The contribution of abstinence and improved contraceptive use. American Journal of Public Health, 97(1), 150–156.
Santelli, J., Sandfort, T., and Orr, M. (2008). Transnational comparisons of adolescent contraceptive use: What can we learn from these comparisons? Archives of Pediatrics and Adolescent Medicine, 162(1), 92–94.
Santelli, J.S., Kantor, L.M., Grilo, S.A., Speizer, I.S., Lindberg, L.D., Heitel, J., Schalet, A.T., Lyon, M.E., Mason-Jones, A.J., McGovern, T., Heck, C.J., Rogers, J., and Ott, M.A. (2017). Abstinence-only-until-marriage: An updated review of U.S. policies and programs and their impact. Journal of Adolescent Health, 61(3), 273–280.
Schaefer, D.R., Adams, J., and Haas, S.A. (2013). Social networks and smoking: Exploring the effects of peer influence and smoker popularity through simulations. Health Education & Behavior, 40(Suppl 1), 24s–32s.
Seemiller, C., and Grace, M. (2018). Generation Z: A Century in the Making. Abingdon, UK: Routledge.
Sherman, L.E., Payton, A.A., Hernandez, L.M., Greenfield, P.M., and Dapretto, M. (2016). The power of the like in adolescence: Effects of peer influence on neural and behavioral responses to social media. Psychological Science, 27(7), 1027–1035.
Sieving, R.E., McRee, A-L., McMorris, B.J., Shlafer, R.J., Gower, A.L., Kapa, H.M., Beckman, K.J., Doty, J.L., Plowman, S.L., and Resnick, M.D. (2017). Youth-adult connectedness: A key protective factor for adolescent health. American Journal of Preventive Medicine, 52(3s3), s275–s278.
Siqueira, L., and Smith, V.C. (2015). Binge drinking. Pediatrics, 136(3), e718–e726.
Sleiman, M., Logue, J.M., Montesinos, V.N., Russell, M.L., Litter, M.I., Gundel, L.A., and Destaillats, H. (2016). Emissions from electronic cigarettes: Key parameters affecting the release of harmful chemicals. Environmental Science & Technology, 50(17), 9644–9651.
Smit, K., Voogt, C., Hiemstra, M., Kleinjan, M., Otten, R., and Kuntsche, E. (2018). Development of alcohol expectancies and early alcohol use in children and adolescents: A systematic review. Clinical Psychology Review, 60, 136–146.
Smith, A.R., Chein, J., and Steinberg, L. (2013). Impact of socio-emotional context, brain development, and pubertal maturation on adolescent risk-taking. Hormones and Behavior, 64(2), 323–332.
Smith, A.R., Chein, J., and Steinberg, L. (2014). Peers increase adolescent risk taking even when the probabilities of negative outcomes are known. Developmental Psychology, 50(5), 1564–1568.
Smith, L.A., and Foxcroft, D.R. (2009). The effect of alcohol advertising, marketing and portrayal on drinking behaviour in young people: Systematic review of prospective cohort studies. BMC Public Health, 9(1), 51.
Squeglia, L.M., Rinker, D.A., Bartsch, H., Castro, N., Chung, Y., Dale, A.M., Jernigan, T.L., and Tapert, S.F. (2014). Brain volume reductions in adolescent heavy drinkers. Developmental Cognitive Neuroscience, 9, 117–125.
Stanwick, R. (2015). E-cigarettes: Are we renormalizing public smoking? Reversing five decades of tobacco control and revitalizing nicotine dependency in children and youth in Canada. Paediatrics & Child Health, 20(2), 101–105.
Suleiman, A.B., Galván, A., Harden, K.P., and Dahl, R.E. (2017). Becoming a sexual being: The “elephant in the room” of adolescent brain development. Developmental Cognitive Neuroscience, 25, 209–220.
Telzer, E.H., Fuligni, A.J., Lieberman, M.D., Miernicki, M.E., and Galvan, A. (2015). The quality of adolescents’ peer relationships modulates neural sensitivity to risk taking. Social Cognitive and Affective Neuroscience, 10(3), 389–398.
Thapa, A., Cohen, J., Guffey, S., and Higgins-D’Alessandro, A. (2013). A review of school climate research. Review of Educational Research, 83(3), 357–385.
Tolman, D.L., and McClelland, S.I. (2011). Normative sexuality development in adolescence: A decade in review, 2000–2009. Journal of Research on Adolescence, 21(1), 242–255.
Tolou-Shams, M., Harrison, A., Hirschtritt, M.E., Dauria, E., and Barr-Walker, J. (2019). Substance use and HIV among justice-involved youth: Intersecting risks. Current HIV/AIDS Reports, 16(1), 37–47.
Tsai, K.M., Telzer, E.H., and Fuligni, A.J. (2013). Continuity and discontinuity in perceptions of family relationships from adolescence to young adulthood. Child Development, 84(2), 471–484.
Tulloch, T., and Kaufman, M. (2013). Adolescent sexuality. Pediatrics in Review, 34(1), 29–37.
U.S. Department of Health and Human Services (HHS). (2012). Preventing Tobacco Use among Youth and Young Adults: A Report of the Surgeon General. Atlanta, GA: Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
———. (2014). The Health Consequences of Smoking: 50 Years of Progress: A Report of the Surgeon General. Atlanta, GA: Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
———. (2016a). E-cigarette Use Among Youth and Young Adults: A Report of the Surgeon General. Atlanta, GA: Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
———. (2016b). Facing Addiction in America: The Surgeon General’s Report on Alcohol, Drugs, and Health. Washington, DC: Office of the Surgeon General.
———. (2017a). Report to Congress on the Prevention and Reduction of Underage Drinking. Rockville, MD: Substance Use and Mental Health Services Administration.
———. (2017b). Underage Drinking Fact Sheet. Bethesda, MD: National Institutes of Health, National Institute on Alcohol Abuse and Alcoholism.
———. (2018a). Adolescent Health: Think, Act, Grow® Playbook. Washington, DC: Office of Population Affairs, Office of Adolescent Health.
———. (2018b). Surgeon General’s Advisory on E-cigarette Use among Youth. Atlanta, GA: Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
U.S. Department of Transportation. (2019). 1999–2017 Young Drivers Traffic Safety Fact Sheets. Available: https://crashstats.nhtsa.dot.gov.
U.S. Food and Drug Administration. (2018a). Statement from FDA Commissioner Scott Gottlieb, MD, on New Steps to Address Epidemic of Youth E-cigarette Use. Available: https://www.fda.gov/news-events/press-announcements/statement-fda-commissionerscott-gottlieb-md-new-steps-address-epidemic-youth-e-cigarette-use.
U.S. Food and Drug Administration. (2018b). Statement from FDA Commissioner Scott Gottlieb, MD, on Proposed New Steps to Protect Youth by Preventing Access to Flavored Tobacco Products and Banning Menthol in Cigarettes. Available: https://www.fda.gov/news-events/press-announcements/statement-fda-commissioner-scott-gottlieb-mdproposed-new-steps-protect-youth-preventing-access.
van den Bos, W., and Hertwig, R. (2017). Adolescents display distinctive tolerance to ambiguity and to uncertainty during risky decision making. Scientific Reports, 7, 40962.
Vassoler, F.M., and Sadri-Vakili, G. (2014). Mechanisms of transgenerational inheritance of addictive-like behaviors. Neuroscience, 264, 198–206.
Vermeersch, H., T’Sjoen, G., Kaufman, J-M., and Vincke, J. (2008). The role of testosterone in aggressive and non-aggressive risk-taking in adolescent boys. Hormones and Behavior, 53(3), 463–471.
Wang, B., King, B.A., Corey, C.G., Arrazola, R.A., and Johnson, S.E. (2014). Awareness and use of non-conventional tobacco products among U.S. students, 2012. American Journal of Preventive Medicine, 47(2 Suppl 1), S36–S52.
Warner, T.D., Giordano, P.C., Manning, W.D., and Longmore, M.A. (2011). Everybody’s doin’ it (right?): Neighborhood norms and sexual activity in adolescence. Social Science Research, 40(6), 1676–1690.
Wellman, R.J., Dugas, E.N., Dutczak, H., O’Loughlin, E.K., Datta, G.D., Lauzon, B., and O’Loughlin, J. (2016). Predictors of the onset of cigarette smoking: A systematic review of longitudinal population-based studies in youth. American Journal of Preventive Medicine, 51(5), 767–778.
Willett, J.G., Bennett, M., Hair, E.C., Xiao, H., Greenberg, M.S., Harvey, E., Cantrell, J., and Vallone, D. (2019). Recognition, use and perceptions of JUUL among youth and young adults. Tobacco Control, 28(1), 115–116.
Wilson, S.J., Tanner-Smith, E.E., Lipsey, M.W., Steinka-Fry, K., and Morrison, J. (2011). Dropout prevention and intervention programs: Effects on school completion and dropout among school aged children and youth. Campbell Systematic Reviews, 8, 61.
Wood, A.P., Dawe, S., and Gullo, M.J. (2013). The role of personality, family influences, and prosocial risk-taking behavior on substance use in early adolescence. Journal of Adolescence, 36(5), 871–881.
World Health Organization. (2017). WHO Report on the Global Tobacco Epidemic, 2017: Monitoring Tobacco Use and Prevention Policies (No. 9241512822). Geneva, Switzerland: Author.
Wu, J., Witkiewitz, K., McMahon, R.J., and Dodge, K.A. (2010). A parallel process growth mixture model of conduct problems and substance use with risky sexual behavior. Drug and Alcohol Dependence, 111(3), 207–214.
This page intentionally left blank.
















































