
4
Core Components of Programs Focused on Optimal Health
As described in Chapter 1, the committee was charged with identifying the key elements or core components of programs that may be successful in preventing risk behaviors and improving outcomes for youth using an optimal health lens. In particular, the sponsor was interested in using a core components methodology to align with work on other current federal research and evaluation initiatives (Blase and Fixsen, 2013). This chapter describes the committee’s approach to this task. First, we provide a brief description of the core components approach. We then describe the methods we used to identify and summarize the evidence on core components of adolescent health programs. Finally, we describe the results of our systematic review and the findings from a complementary review of papers that use a core components approach.
___________________
1 Response to MyVoice survey question: “Specifically, what could your school do to help you live your best life (now or in the past)?” See the discussion of the MyVoice methodology in Appendix B for more detail.
THE CORE COMPONENTS APPROACH TO EVIDENCE-BASED PRACTICE
Core program or intervention components are discrete, reliably identifiable techniques, strategies, or practices that are intended to influence the behavior, outcomes, or well-being of a service recipient (Blase and Fixsen, 2013). Core components may reflect aspects of intervention content, defined as specific knowledge or actions thought to influence behavior (e.g., communication skills); the processes, methods, or techniques through which service providers deliver content components and support the behavior change process (e.g., modeling); the locations and formats that make up the intervention delivery circumstances; and the implementation strategies used to facilitate intervention delivery (e.g., provider training, availability of manuals). In this report, we use the term core components to refer to any of these aspects of interventions, although other terms are also used to refer to this family of approaches to evidence-based practice, including common elements, kernels, and core practice elements (Barth and Liggett-Creel, 2014; Chorpita, Delaiden, and Weisz, 2005; Embry and Biglan, 2008; Hogue et al., 2017). In general, these approaches share being based on the idea that interventions comprise discrete components that can be identified, organized, and combined in different ways to achieve the intended results.
Core components approaches have emerged as a complement to the common approach to evidence-based programs (EBPs) that focuses on identifying distinct model programs that have demonstrated positive impacts. Such model programs usually have a brand name (e.g., Reducing the Risk, Positive Action, Be Proud! Be Responsible!), are generally accompanied by a program manual, and sometimes offer training or certification by the program developer. These programs typically receive the “evidence-based” designation as a result of at least one experimental or quasi-experimental study that demonstrates a statistically significant positive impact on an outcome of interest. Registries such as Blueprints for Healthy Youth Development2 review the research on candidate programs and provide listings of those that meet their evidence standards. More recently, tiered evidence schemes and some federal grant funding have begun mandating or incentivizing the use of model programs.
While the evidence backing model programs is derived from some of the highest-quality research available, the focus on EBPs has several drawbacks. First, often only one or, at best, a few studies of a program have assessed its impact, leaving open the question of generalizability. Second, this approach implies that the program must be implemented with fidelity
___________________
2 For more information, see https://www.blueprintsprograms.org.
to the original model to achieve similar results, which requires significant training of facilitators and inhibits what might be effective local adaptations. Finally, most programs already in operation are likely to be reluctant to abandon their current practice to adopt something new because of cost, provider resistance to change, contractual obligations, local support for the current program, or other factors (Blase and Fixsen, 2013).
Core components approaches to EBPs seek to address some of these drawbacks. For example, because core components approaches unpack programs into discrete components and often examine aspects of their delivery format, dosage, implementation strategies, and delivery personnel, they afford more flexibility or creativity in what and how services are delivered. In an environment of limited resources and competing priorities, such flexibility may promote more widespread adoption of effective practices. Because aspects of adolescent health overlap and are interrelated, core components approaches also offer an efficient strategy for supporting multiple aspects of youth development.
Recent research has shown the utility of this approach for adolescent opioid use disorder (OUD), as well as youth program management and quality improvement. For instance, researchers at the Center on Addiction were able to identify 21 core techniques focused on family psychoeducation, medication options, and shared decision making that were most effective in adolescent OUD treatment (National Academies of Sciences, Engineering, and Medicine [NASEM], 2019). Additionally, the David P. Weikart Center for Youth Program Quality (2019) used this approach to identify high-quality practices for after-school programs, which led to the development of the Youth Program Quality Assessment (NASEM, 2019).
As the use of core components approaches to EBPs has spread, a variety of methodologies for identifying such components have emerged. For example, the distillation and matching method focuses on identifying and distilling key practices from program manuals and then matching those practices to particular client needs (Chorpita and Daleiden, 2009; Chorpita, Delaiden, and Weisz, 2005). Embry and Biglan’s (2008) kernels method relies on evidence from peer-reviewed experimental studies to identify practices that can be delivered alone or in combination or added on to existing programs. More recently, adaptive research designs have emerged that can provide an analytic strategy for identifying core components (Pallmann et al., 2018). Other approaches to identifying core components involve systematic reviews of evidence, meta-analyses, or reviews of systematic reviews or meta-analyses (Boustani et al., 2015; Lipsey, 2018; Peters et al., 2009).
THE COMMITTEE’S APPROACH
Strategy
The committee’s primary strategy involved a systematic review of systematic reviews and meta-analyses, conducted in April 2019. We considered other approaches, including a meta-analysis of primary studies; however, such a task was not possible within the time constraints for this consensus study. The approach we took enabled examination of the largest possible body of evidence in the available time.
To supplement our systematic review, we examined research papers focused on identifying and integrating the core components of effective youth programs. More specifically, the purpose of this secondary strategy was to (1) provide additional evidence in support of or in contrast to the core components identified in our systematic review, and (2) find any additional core components not previously identified.
Eligibility Criteria
To identify the most relevant systematic reviews and meta-analyses for our review, stay within the scope of the charge in our statement of task, and ensure that the articles we reviewed met minimum quality standards for systematic reviews and meta-analyses, we used a set of eligibility criteria to determine which documents would be eligible for this review. These criteria were informed by the scoring methods used by the U.S. Department of Justice’s Office of Justice Programs (2013) to analyze programs and practices as part of its CrimeSolutions.gov initiative. Our set of criteria is described below.
Type of review. To be eligible, a manuscript must have been clearly described as a systematic review or meta-analysis and to have evidence of peer review. Narrative literature reviews were not eligible for our systematic review.
Literature search. The literature search that guided the inclusion of primary studies in a meta-analysis or systematic review must have included at least two sources and must have provided evidence that unpublished literature was sought in the search.
Intervention. A meta-analysis or systematic review must have included at least two studies of the practice of interest, as defined below under the criterion “primary aim of the intervention.”
Aggregation. If there was a meta-analysis, it must have aggregated the results from at least two studies.
Primary aim of the intervention. The programs included in a meta-analysis or systematic review had to address behaviors and outcomes in
one of the five dimensions of optimal health on which this report focuses.3 Reviews that included programs targeting risk behaviors or negative outcomes relating to the optimal health dimensions (e.g., substance use, sexual behavior) were also eligible.
-
Physical health. Two aspects of physical health were prioritized for the review.
- Substance use. A meta-analysis or systematic review must have focused on prevention or intervention programs intended to prevent or reduce tobacco use (including e-cigarettes), alcohol use, or illicit drug use.4 Programs could be educational, skill-building, or psychosocial. Primary, secondary, and tertiary prevention programs were eligible. Medical intervention or treatment programs were excluded because they were not generalizable or representative of the broader youth population.
- Pregnancy prevention/sexual health and/or reproductive health. A meta-analysis or systematic review must have covered programs intended to reduce teenage pregnancy, sexually transmitted infections (STIs), or related sexual risk behaviors through educational, skill-building, and/or psychosocial intervention or programming. Primary, secondary, and tertiary prevention programs were eligible.
- Emotional health. A meta-analysis or systematic review must have included interventions targeting resilience, mental or emotional health, stress management, emotion regulation, or self-regulation.
- Social health. A meta-analysis or systematic review must have included interventions targeting social-emotional learning, conflict resolution, assertiveness, or social skills.
- Intellectual health. A meta-analysis or systematic review must have included interventions broadly targeting academic achievement, academic performance, or learning, including academic programs, after-school programs, and mentoring.
- Spiritual health. A meta-analysis or systematic review must have included interventions targeting mindfulness, character education, or moral or spiritual development.
___________________
3 The five dimensions of optimal health are broad and cover many aspects of adolescent health and development. The committee selected several topics within each of these broad categories that are of particular relevance to healthy adolescent development.
4 Although the committee specifically targeted tobacco and alcohol use in this report, illicit drug use was included in the search criteria since many substance use programs for tobacco and alcohol also target illicit drugs. However, “illicit drugs” were rarely defined or disaggregated in these studies, so a focus on specific illicit drugs was not possible in this report.
Primary outcomes. A meta-analysis or systematic review must have reported on at least one of the following eligible outcomes related to the dimensions of optimal adolescent health that are the focus of this report:
- sexual activity, including sexual initiation, frequency, and number of partners;
- contraceptive use, including condom use;
- pregnancy;
- STIs;
- behavioral intentions regarding use of substances, including tobacco, alcohol, and illicit drugs;
- substance use or misuse, including frequency or quantity of use, type of use, use/no use, time since last use, etc., and encompassing use of tobacco, alcohol, and illicit drugs alone or in combination;
- social skills or social-emotional skills;
- mental health, reduced stress, resilience, and self-regulation;
- academic achievement or performance; and
- mindfulness, moral development, and religiosity.
Age of samples. Samples included in a meta-analysis or systematic review were restricted to adolescents ages 10–19. If a sample combined adolescents with adults, the results for the youth must have been reported separately.
Control groups. All studies included in a meta-analysis or systematic review had to include an appropriate control, comparison, or counter-factual condition, or the meta-analysis or systematic review must have analyzed those studies without appropriate comparison conditions separately from those with appropriate counterfactuals.
Single group. A meta-analysis or systematic review could include pre–post or head-to-head comparison studies, but these must have been separated from those with comparison groups.
Specialized sample. A meta-analysis or systematic review must not have been conducted on narrowly focused samples of adolescents, including but not limited to those with diagnosed medical conditions (e.g., chronic physical disability or disease, mental health condition).
Reporting of results. A meta-analysis or systematic review must have reported effect sizes that represent the magnitude of the treatment effect.
Combining effect sizes. When an average effect size was reported for multiple studies, all effect sizes in the combination must have addressed the same type of relationship.
Publication date. At least 50 percent of the studies included in a meta-analysis or systematic review must have been published or otherwise available in or after 1980.
Publication location. The studies in a meta-analysis or systematic review must not have been conducted exclusively in low- or middle-income countries or be single-country studies other than in the United States (e.g., meta-analyses of research conducted entirely in Spanish locations were not eligible).
Results of Literature Search
Using the above eligibility criteria as a guide, the committee conducted a comprehensive literature search to identify relevant studies. We searched the following electronic bibliographic databases for articles published between 2009 and 2019: Cochrane Database of Systematic Reviews, Campbell Collaboration Library, PubMed, and PsycINFO. Also included were meta-analyses and systematic reviews meeting our criteria that were recommended by committee members, by individuals attending our public information-gathering session, and by members of the public.
The search terms were adapted to each database, and separate searches were conducted around the different domains of optimal adolescent health. Generally, three blocks of terms were used: one block describing the sample or population of interest (e.g., teens, adolescents), one block describing the optimal adolescent health domain or subdomain of interest (e.g., sexual risk behavior, pregnancy), and one block identifying meta-analyses and systematic reviews. Our full search strategy is detailed in Appendix A.
Once potential articles had been identified, committee members screened the titles and abstracts of all of these articles for relevance to this review. The full-text versions of all articles deemed relevant based on the title and abstract screening were then evaluated by two committee members against the full eligibility criteria. Conflicts were resolved by consensus. The title/abstract screening and full eligibility review were conducted using Covidence systematic review software (Veritas Health Innovation, 2019).
These procedures resulted in the identification of 31 meta-analyses and systematic reviews. Figure 4-1 shows the flow of manuscripts through the search and screening process using the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines (Moher et al., 2009).
Eighteen of the 31 articles were focused on the domain of physical health, which was further subdivided into articles focused on substance use (n = 10) and sexual health (n = 8).5,6 Another 6 articles focused on
___________________
5 Although many adolescent behaviors and outcomes fall under physical health (e.g., eating, obesity), the committee’s review focused on substance use (alcohol and tobacco, as well as other drugs when combined with alcohol or tobacco) and sexual health, as described in Chapter 3 and in the search and exclusion criteria noted above.
6 Three papers that report on the same data or study as other articles were used to supplement study information but were not included in this count.
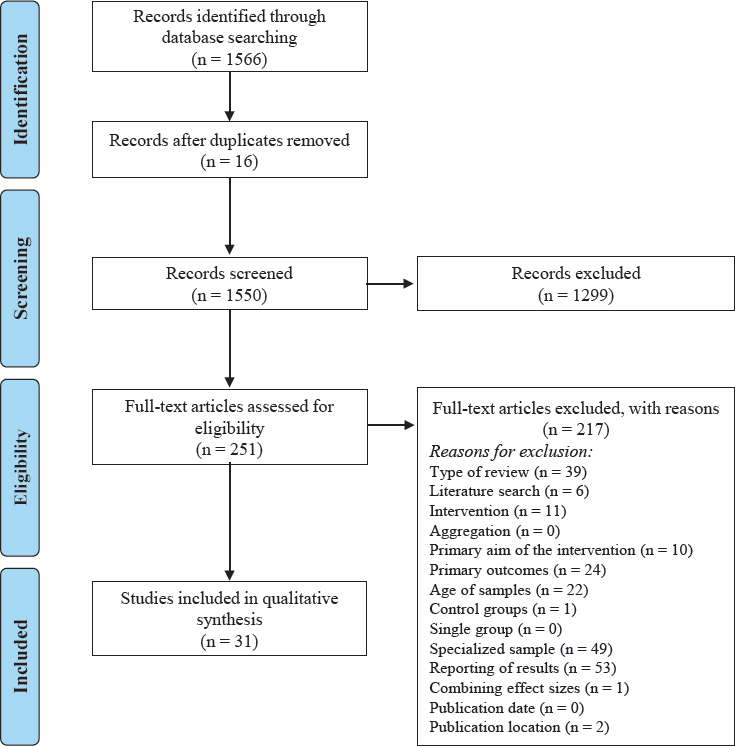
NOTES: Articles with ineligible publication dates were excluded during the screening process.
Three articles reported on the same set of papers as another eligible study and were considered together as one review in the qualitative synthesis.
SOURCE: Adapted from PRISMA reporting guidelines (Moher et al., 2009).
outcomes related to emotional health. One article focused on intellectual health. None of the studies identified in this review focused exclusively on social or spiritual health. The remaining articles considered a variety of behaviors and outcomes that mapped onto multiple optimal health domains (n = 6). Table 4-1 shows the articles that fell into each category.
TABLE 4-1 Articles Identified in the Systematic Review by Optimal Health Domains (n = 31)
| Physical Health (n = 18) | Emotional Health (n = 6) | Social Health (n = 0) | Intellectual Health (n = 1) | Spiritual Health (n = 0) | |
| Substance Use (n = 10) | Sexual Health (n = 8) | ||||
| Multiple Optimal Health Areas (n = 6) | |||||
* Indicates two articles that were identified that were part of the same project and used the same set of studies for their manuscript, and were reviewed together.
Our inability to find studies that focused exclusively on social or spiritual health is reflected in the limitations of O’Donnell’s (2009) optimal health definition (see Chapter 2). First, these dimensions of optimal health are much more difficult to measure than the physical, emotional, and intellectual domains, whose measurement can often rely on standardized tools or the presence/absence of a disease or condition. Second, the interdependence and interaction among the dimensions can make them difficult to disentangle. Accordingly, many programs incorporating social or spiritual health are categorized under “multiple optimal health domains.”
Organizing Framework
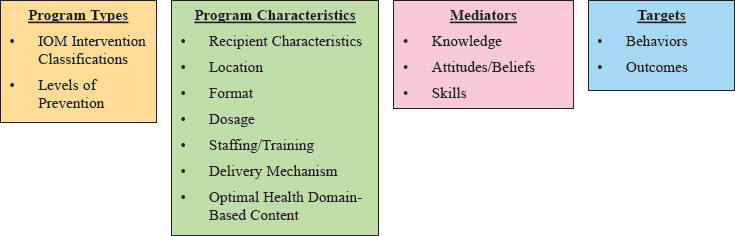
The committee’s methodological approach for extracting information from each article drew on the methods used by other core components researchers and was guided by the organizing framework illustrated in Figure 4-2. This framework represents the committee’s consensus about the common features of programs and interventions targeting adolescent behavior. Beyond its utility for this report, the committee’s framework provides an important structure for identifying what matters for promoting optimal adolescent health. Each of the areas identified in this framework is described in greater detail below.
Program Types
Program types were classified using the Institute of Medicine’s (IOM, 1994) intervention classifications and the levels of prevention in the public health prevention framework (Katz and Ali, 2009) (see Figure 4-3).
Institute of Medicine (IOM) intervention classifications The IOM intervention classifications—universal, selective, and indicated—were based on those proposed by Gordon (1983). Universal interventions target an entire population, regardless of the members’ levels of risk. Selective interventions are those that target a subset of the population that may be considered “at risk.” Finally, indicated interventions are provided to those who are already beginning to experience the effects of a specific health outcome (Institute of Medicine, 1994).
Levels of prevention The committee chose to use the three-level public health prevention framework to guide its identification of programs and interventions (Katz and Ali, 2009). As noted in Chapter 1, the prevention framework is designed with health outcomes as the key target. Although a health behavior is an important predictor of a health outcome, behaviors
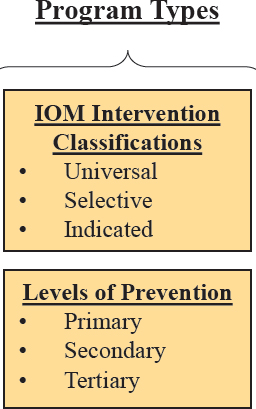
are considered to be modifiable risk factors that are a focus in primary prevention activities rather than outcomes themselves.
In this model, primary prevention targets the risk factors for a disease or condition, with the intent of intervening before the disease or condition occurs. Included in primary prevention are vaccination and behavior change programs, both of which can prevent the onset or impact of the disease or condition (Centers for Disease Control and Prevention [CDC], 2017; U.S. Preventive Services Task Force, 2018). Secondary prevention focuses on early identification of high-risk populations, which can help
slow or stop the progression of a disease or condition (CDC, 2017; U.S. Preventive Services Task Force, 2018). These activities may include early testing or monitoring for signs or symptoms of the disease or condition. Tertiary prevention encompasses treatment and rehabilitation after onset or diagnosis, which may prevent future incidence of the disease or condition (CDC, 2017; U.S. Preventive Services Task Force, 2018).
Program Characteristics
The committee identified a comprehensive list of characteristics that could describe the programs and interventions included in our review (see Figure 4-4). These characteristics were categorized by recipient character-
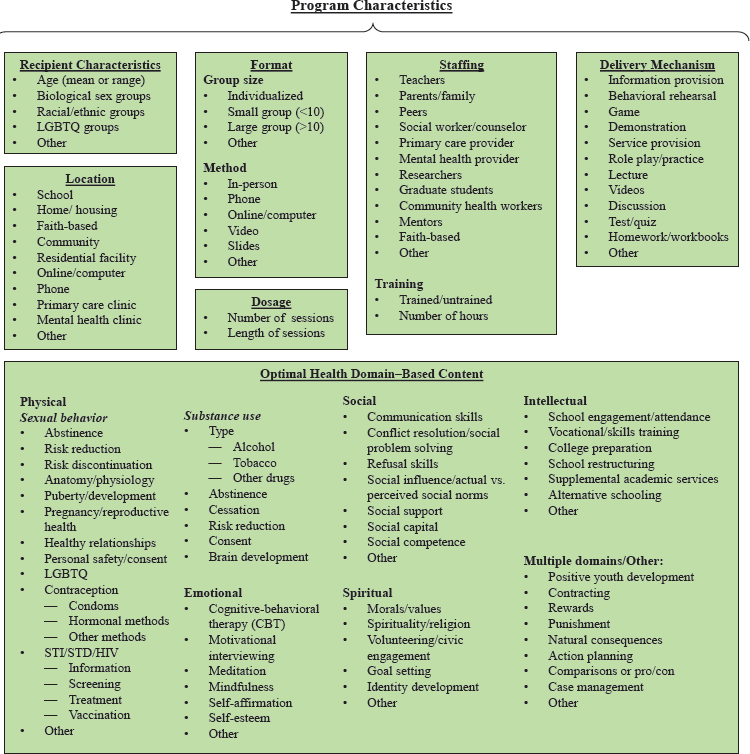
istics, location, format, dosage, staffing, delivery mechanism, and optimal health domain–based content. Programs and interventions were not limited to one identifying characteristic per category. Recognizing that this list was not exhaustive, each category also included space for the identification of “other” characteristics that could emerge in the review.
Recipient characteristics Recipient characteristics identified by the committee were age, biological sex, race/ethnicity, and sexual orientation/gender identity (LGBTQ). For age, either the range of ages or the mean age of recipients in the program or intervention needed to be 10–19 (see the discussion of eligibility criteria in the previous section). Biological sex, racial/ethnic, and LGBTQ group information was recorded to note whether an intervention was targeted to a particular demographic group (e.g., females only, black/African American adolescents).
Location Location referred to the place where the program or intervention occurred. Locations could include schools; homes or housing; faith-based settings; community settings; residential facilities; online or on a computer; by phone; or in a clinic, such as a primary care or mental health provider office.
Format Format included both group size and the method by which the program or intervention was delivered. Group sizes identified by the committee were individualized or one-on-one, small groups of fewer than 10 adolescents, and larger groups of 10 or more. Methods referred to how the intervention was provided, and included in-person, phone, online/computer-based, video, or slides.
Dosage Dosage represented the amount of the program or intervention that was provided. Included in this category were the number and duration of sessions or programs.
Staffing Program staffing referred to the person or people who delivered the program or intervention. The committee identified teachers, parents or family members, peers, social workers or counselors, primary care providers, mental health providers, researchers, graduate students, community health workers, mentors, and faith-based staff in the initial list. Staffing also referred to whether program staff were trained and if so, the number of training hours.
Delivery mechanism Delivery mechanisms were the ways in which the material was delivered in the program or intervention. Delivery mechanisms identified by the committee included providing information, behavioral
rehearsal, games, demonstrations, service provision, role play or practice, lectures, videos, discussions, tests or quizzes, and homework or workbooks.
Optimal Health Domain–Based Content
Content referred to the types of information, messages, or skills that the program sought to provide, enhance, or encourage. The committee identified a number of different types of content, which were further categorized by optimal health domain and, in the case of physical health, the behavior of interest. Again, understanding that this list was not exhaustive, we included space to identify any other content that was not on the initial list.
Physical health
- Substance use. Content for substance use included substance type (alcohol, tobacco, other drugs), abstinence messaging, cessation, risk reduction, consent, and brain development.
- Sexual behavior. Content for sexual health programs included abstinence messaging; risk reduction or risk discontinuation; anatomy and physiology; puberty and pubertal development; pregnancy and reproductive health; healthy relationships; personal safety and consent; sexual orientation and gender identity (LGBTQ); contraception (including condoms, hormonal methods, and other methods); and STI, sexually transmitted disease (STD), or HIV information, screening, treatment, and vaccination.
Emotional health Emotional health–based content included cognitive-behavioral therapy–based techniques, motivational interviewing, meditation, mindfulness, self-affirmation, and self-esteem.
Social health Content based in social health included communication skills, conflict resolution and social problem solving, refusal skills, social influences or social norms, social support, social capital, and social competence.
Spiritual health Spiritual health content included morals and values, spirituality or religion, volunteering and civic engagement, goal setting, and identity development.
Intellectual health Content in the intellectual health category included school engagement, vocational or skills training, college preparatory activities, school restructuring, supplemental academic services, and alternative schooling.
Multiple domains Finally, there were a number of topics that did not fit into a single optimal health domain. These included positive youth development, contracting, rewards and punishments, natural consequences, action planning, making comparisons, and case management.
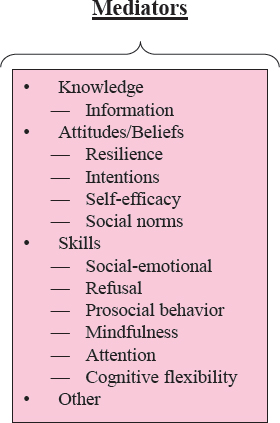
Mediators
Program or intervention mediators were the mechanisms or processes through which the targeted behaviors or outcomes were influenced (see Figure 4-5). The initial set of mediators identified by the committee included the knowledge, attitudes or beliefs, and skills that a program may promote, enhance, or encourage. Knowledge included providing information, while attitudes and beliefs included resilience, behavioral intentions, self-efficacy, and social norms. Most mediators were specific skills (i.e., knowing how and being able to do something), and were further categorized as social-emotional, refusal, prosocial behavior, mindfulness, attention, and cognitive flexibility.
Targets
The targets of programs were the behaviors and outcomes that each program sought to prevent or promote, and were categorized by optimal health domain (see Figure 4-6). In line with the levels of public health prevention framework, the outcomes were the conditions of interest, while the behaviors represented modifiable precursors for primary prevention activities.
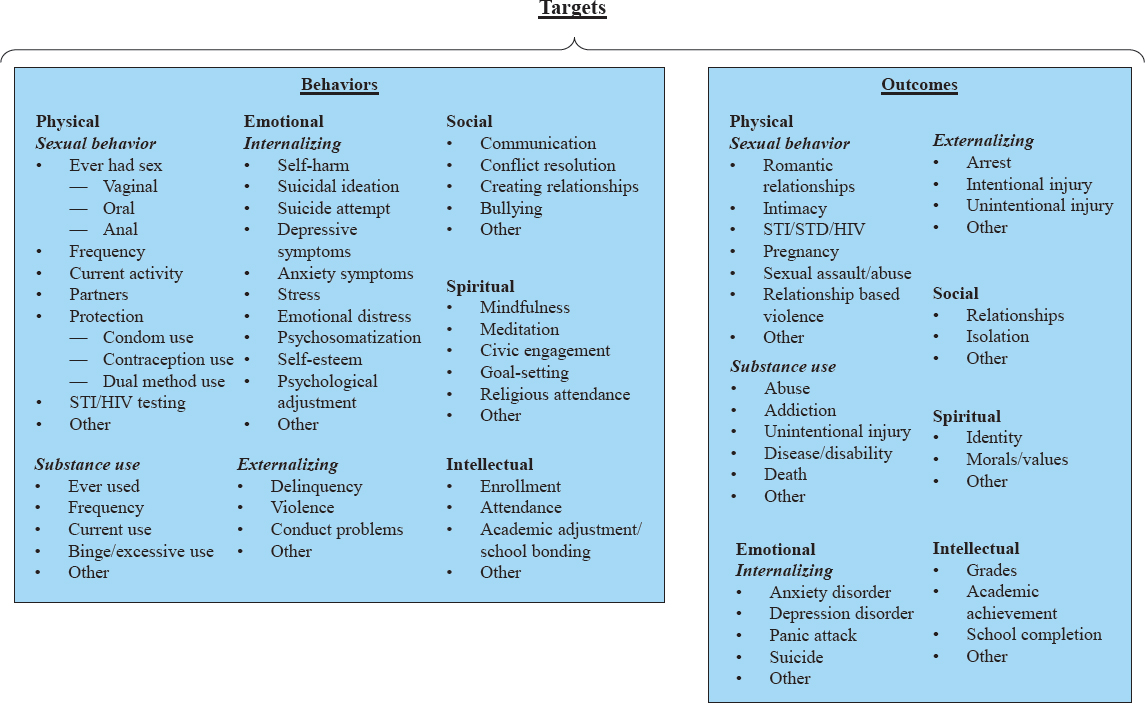
Physical health
- Substance use. For each substance type, behaviors included ever using, frequency of use, current use, and binging or excessive use. The outcomes associated with substance use included substance abuse or addiction, unintentional injury, disease or disability, and death.
- Sexual behavior. Sexual behaviors included ever having sex (vaginal, oral, anal, or unspecified); sex frequency; current sexual activity; number of sexual partners; use of protection including condoms (for prevention of STI or pregnancy), contraception (pregnancy), or dual methods (STI and pregnancy); and STI or HIV testing. Sexual behavior outcomes were romantic relationships, intimacy, STIs/STDs/HIV, pregnancy, sexual assault or abuse, and relationship-based violence.
Emotional health Although emotional health targets often have similar content, the behaviors and outcomes may differ, and are often categorized as internalizing or externalizing. Internalizing behaviors included self-harm, suicidal ideation, suicide attempt, depression symptoms, anxiety symptoms, stress, emotional distress, self-esteem, and psychological adjustment, while internalizing outcomes were anxiety or depression disorders, panic attacks, and suicide. Externalizing behaviors included delinquency, violence, and conduct problems, and externalizing outcomes were arrest, intentional injuries, and unintentional injuries.
Social health Social health behaviors included communication, conflict resolution, creating relationships, and bullying. Outcomes were formed relationships and social inclusion.
Spiritual health Spiritual health behaviors were mindfulness, meditation, civic engagement, goal setting, and religious attendance. Outcomes included established identity and moral or value systems.
Intellectual health Intellectual health behaviors were school enrollment and attendance, and academic adjustment or school bonding. Associated outcomes included grades, academic achievements, and school completion.
RESULTS OF THE COMMITTEE’S SYSTEMATIC REVIEW
The committee examined several types of information from the eligible systematic reviews and meta-analyses, including the findings reported and any core components of the programs and interventions that were recorded
or identified in the manuscripts. Most important, we carefully reviewed the moderator and subgroup analyses reported in each review in order to identify any core components with empirical support. The results of our systematic review of reviews and meta-analyses are summarized below by optimal health domain.
Physical Health
Substance Use
The committee reviewed 10 systematic reviews and meta-analyses that examined programs and interventions focused on prevention or reduction of youth substance use, including alcohol, tobacco, marijuana, and other drugs, or a combination of two or more of these substances. More specifically, 1 study focused on tobacco use only (Thomas, McLellan, and Perera, 2015); 2 on illicit drug use only (Faggiano et al., 2014; Ferri et al., 2013); 3 on alcohol and other drug use but not tobacco use (Champion et al., 2013; Tanner-Smith et al., 2015; Thomas, Lorenzetti, and Spragins, 2013); and the remaining 4 on tobacco, alcohol, and other drugs or substance use more broadly (Carney et al., 2016; Hodder et al., 2017; MacArthur et al., 2016; Onrust et al., 2016).
Most programs and interventions in this category were delivered in schools and included universal prevention programs, targeted interventions, or a combination of the two. Additional delivery settings included home or the community (MacArthur et al., 2016), emergency rooms (Tanner-Smith et al., 2015), and mass media campaigns (Ferri et al., 2013). Evidence was not sufficient to suggest that one setting was better than any other, but the overwhelming number of programs provided in schools suggests their utility in reaching a larger population of young people relative to other settings, including those who may not be able to access services outside of school.
Universal programs were delivered in large groups (e.g., whole class), while targeted programs were more often delivered to individuals or in smaller groups. Teachers, peers, and other mentors were the most common facilitators of these programs. In general, adult-led programs were more effective than peer-led programs (Thomas, McLellan, and Perera, 2015), although the latter programs showed some small effects (MacArthur et al., 2016). Some programs also involved parents, who represent an important protective factor for adolescent substance use. For example, Thomas, Lorenzetti, and Spragins (2013) examined the role of mentors and showed that strong family acceptance and community partners helped reduce drug use.
The majority of programs focused exclusively on adolescent populations (range or mean age of 10 to 19), although two of the systematic
reviews and meta-analyses also included studies of elementary school–aged children (Faggiano et al., 2014; Hodder et al., 2017; Onrust et al., 2016). In particular, Onrust and colleagues (2016) found significant effects by age, indicating that there are developmental differences in response to program foci and that beginning substance use prevention programs before adolescence can be effective.
Program duration varied considerably, from one brief session to multiple sessions over the course of 2 or more years, and no clear evidence emerged that a specific number of sessions or time spent in a program was more or less beneficial overall. Among targeted programs, two of the studies (Carney et al., 2016; Tanner-Smith et al., 2015) focused on the effects of brief interventions for substance-using adolescents and showed some small effects. Other, more extensive targeted interventions were also effective. For example, Thomas, Lorenzetti, and Spragins (2013) found that frequent meetings helped reduce drug use among substance-using adolescents. Universal prevention programs also ranged in duration, although most of these programs in the reviewed articles were provided over longer periods of time. As mentioned previously, some of these programs began in childhood, highlighting both the developmental differences in program effects and the utility of starting prevention programs early and continuing them through adolescence (Onrust et al., 2016).
Many of the programs were informed by theory, with most using a social competence approach (Botvin, 1983), a social influence approach (Cialdini and Goldstein, 2004), or the transtheoretical model of behavior change (Prochaska and Velicer, 1997). Those using a social competence approach, which aims to reduce or prevent drug use by improving personal and interpersonal skills as well as problem-specific skills, were generally more effective, although the improvement usually was not statistically significant. Those programs based on the social influence model, which attempts to reduce substance use by focusing on social norms and peer influence, were generally less effective and rarely showed statistically significant results. However, programs that used a combination of both the social competence and social influence approaches (e.g., developing interpersonal skills and discussing social norms) were more effective, especially with respect to longer-term outcomes (Faggiano et al., 2014; Thomas, McLellan, and Perera, 2015).
The committee’s review of systematic reviews and meta-analyses of programs targeting substance use revealed several promising components, including the utility of school-based programs for universal prevention, programs that begin in childhood, and those that combine social competence and social influence approaches by incorporating skill development with social norm education. Because the studies included were not necessarily designed to identify effective components, our review did not uncover
strong evidence in support of specific core components that were consistently effective across multiple studies. Importantly, this lack of evidence may not mean that no such effective components exist. Rather, it represents an opportunity for future research to evaluate the effectiveness of identifiable core components of programs and practices that may be generalizable across different settings and target populations.
Sexual Behavior
Eight different systematic reviews and meta-analyses focused on sexual health. The targeted outcomes varied widely and included both behaviors and health outcomes. Specifically, one article focused on overall sexual health promotion (DeSmet et al., 2015), two focused exclusively on teen pregnancy prevention (Harden et al., 2009; Marseille et al., 2018), one focused exclusively on contraceptive use (Lopez et al., 2016), and one focused on repeat pregnancy prevention (Aslam et al., 2017; Whitaker et al., 2016). The remaining three reviews targeted more than one behavior or outcome: two focused on teen pregnancy and STI prevention (Oringanje et al., 2016; Picot et al., 2012; Shepherd et al., 2010), and one included teen pregnancy and STI prevention as well as sexual risk behaviors (Chin et al., 2012).
Most programs in this category were universal prevention programs, although some were targeted to populations at greater risk for pregnancy and/or STIs, such as teen mothers (Aslam et al., 2017; Whitaker et al., 2016) or specific racial/ethnic groups (Aslam et al., 2017; Whitaker et al., 2016; Marseille et al., 2018; Picot et al., 2012; Shepherd et al., 2010). Some programs were also delivered to separate groups based on biological sex (Harden et al., 2009; Picot et al., 2012; Shepherd et al., 2010).
The most common program settings were schools, followed by community centers. Some programs also occurred at home or in primary care and reproductive health clinics. Programs were most often delivered by teachers and health educators, peers or near-peers, and medical professionals.
The effectiveness of programs delivered in similar settings varied for several reasons. First, not all programs were implemented with fidelity. In school-based settings, for example, implementation was often affected by whether the school was characterized by a supportive school culture, flexible school administration, and enthusiasm and expertise for delivering interactive sessions among teachers and peers (Picot et al., 2012; Shepherd et al., 2010). This finding suggests that creating a supportive and inclusive culture in schools and other program settings can help improve program effectiveness.
Second, not all young people found the programs to be engaging or acceptable. One influential factor in this regard was the qualities of the intervention providers—enthusiasm, credibility, and expertise (in content
and in managing groups) (Picot et al., 2012; Shepherd et al., 2010). Other factors were whether the interventions met young people’s own needs in relation to sexual health, including sexual feelings, emotions and relationships, the operation of gendered norms, the age-appropriateness of the intervention, and the level of discomfort felt in the classroom setting (Picot et al., 2012; Shepherd et al., 2010). These findings not only provide evidence for creating a supportive and inclusive culture in program settings, but also highlight the importance of including diverse youth and their communities in program development, implementation, and evaluation to ensure that a program meets their needs.
The vast majority of studies reviewed programs for youth ages 10–19, although younger students were sometimes included (Harden et al., 2009; Lopez et al., 2016). The latter were most often early childhood interventions and other youth development programs that provided social support, educational support, and skills training. Many of these early childhood intervention programs also targeted social determinants (e.g., race/ethnicity, socioeconomic status, ability) and structural and systemic issues (e.g., housing, employment opportunities) that affect health, development, and well-being (Harden et al., 2009). Importantly, these early childhood programs appeared to exert a long-term positive influence on the risk of teenage pregnancy, as well as other outcomes associated with social and economic disadvantage, such as unemployment and criminality (Harden et al., 2009). Social and economic disadvantage have not been well addressed in programs and evaluations as determinants of teenage pregnancy (Harden et al., 2009). More research is therefore needed to understand the interdependence of social determinants, structural and systemic issues, behavior, and health outcomes. Furthermore, programs that aim to improve young people’s life opportunities, financial circumstances, and future expectations represent an important avenue for future work.
The frequency and duration of the programs studied varied significantly, from brief, single sessions to multiple sessions over a number of years. Comparisons by program duration showed that those provided over a longer period were more effective than those delivered as single sessions, a finding attributed to the fact that such programs give participants more opportunities to practice the skills they have learned (Picot et al., 2012; Shepherd et al., 2010).
As was found for the substance use studies, the sexual health studies included in the committee’s review generally were not designed to identify program components that were more effective than others. However, the body of evidence presented in these reviews highlights the potential effectiveness and generalizability of particular approaches. First, creating a supportive and inclusive culture in program settings and including diverse youth and their communities in program development, implementation,
and evaluation efforts can ensure that such programs meet the needs of the youth they target. This is a prevalent theme not only in the literature, but also in the experiences of current Teen Pregnancy Prevention (TPP) program Tier 1B implementation grantees (Baltimore City Health Department, 2019; Mary Black Foundation, 2019; Methodist Le Bonheur Community Outreach, 2019; Morehouse School of Medicine, 2019; San Diego Youth Services, 2019; The Center for Black Women’s Wellness Inc., 2019).
Second, traditional approaches to reducing teenage pregnancy rates, such as inclusive sex education and better sexual health services, can be complemented, but not replaced, by positive youth development programs. The latter programs use behavioral theory–based approaches to increase adolescents’ knowledge; influence their attitudes and beliefs; create supportive norms; and build relevant communication, decision-making, and practical skills that help build self-efficacy. These programs are associated with prevention and decreased risk of pregnancy, HIV infection, and STIs (Chin et al., 2012; DeSmet et al., 2015; Lopez et al., 2016; Marseille et al., 2018). Future research is needed to evaluate the core components of these programs that can be effective across multiple behaviors and outcomes.
Emotional Health
Six of the systematic reviews and meta-analyses focused on emotional health (Calear and Christensen, 2010; Clarke, Kuosmanen, and Barry, 2015; Corrieri et al., 2014; Das et al., 2016; Dray et al., 2017; van Genugten et al., 2017). All six addressed specific types of internalizing symptoms or behaviors (e.g., depression or anxiety symptoms, low self-esteem, stress), while three also included externalizing symptoms or behaviors (e.g., conduct problems, violence) (Das et al., 2016; Dray et al., 2017; van Genugten et al., 2017).7
Four of the systematic reviews and meta-analyses included programs delivered only in school settings (Calear and Christensen, 2010; Corrieri et al., 2014; Dray et al., 2017; van Genugten et al., 2017). The other two included programs provided in schools and at least one other setting, including primary care clinics (Das et al., 2016) or through digital platforms (Clarke, Kuosmanen, and Barry, 2015). All six systematic reviews and meta-analyses included programs focused on universal prevention of emotional health problems, while most also included programs targeted to adolescents considered at risk based on family history or symptoms (Calear and Christensen, 2010; Clarke, Kuosmanen, and Barry, 2015;
___________________
7 Articles that focused only on samples of adolescents with diagnosed mental health disorders (e.g., depression, anxiety, attention deficit-hyperactivity disorder) were excluded because these represent chronic medical conditions.
Corrieri et al., 2014; Das et al., 2016; van Genugten et al., 2017). The fact that the majority of these programs occurred, at least in part, in schools again suggests the usefulness of schools in addressing adolescent health and well-being.
Most universal programs were administered in group settings, except for those in the Clarke, Kuosmanen, and Barry (2015) study, which were all self-administered through digital media platforms. Targeted programs were delivered both individually and in group settings. Programs were most often provided by teachers, trained external facilitators (e.g., mental health providers, researchers, health professionals), or some combination of the two. Although digital e-health interventions showed some promise for improving emotional health, participant retention was lower in programs delivered exclusively through digital media compared with those that also included an in-person component, indicating the value of in-person time for these types of programs (Clarke, Kuosmanen, and Barry, 2015; Das et al., 2016).
In general, emotional health programs involved more frequent and more consistent sessions relative to the substance use and sexual health programs included in our review. The majority of programs included multiple sessions, ranging from two total meetings to daily sessions over the course of 36 weeks.
The average age of program recipients for each study was 10–19, although children as young as 5 and late adolescents as old as 25 were included in some of the systematic reviews and meta-analyses. Four of the studies also examined programs involving parents as a complement to school-based programs (Calear and Christensen, 2010; Corrieri et al., 2014; Das et al., 2016; Dray et al., 2017).
Overall, programs informed by cognitive-behavioral therapy (CBT) techniques were shown to be effective in improving emotional health across all the systematic reviews and meta-analyses. The goal of CBT is to change the automatic negative thoughts that contribute to emotional distress and related behavior problems, and such therapies have strong evidence of effectiveness for a variety of internalizing and externalizing problems across ages and demographic subgroups (Hofmann et al., 2012). Among the studies included in our review, those that used CBT techniques to promote resilience, self-regulation, and coping skills were most consistently associated with decreased internalizing and externalizing symptoms and improved emotional well-being (Calear and Christensen, 2010; Clarke, Kuosmanen, and Barry, 2015; Corrieri et al., 2014; Das et al., 2016; Dray et al., 2017; van Genugten et al., 2017).
As with the studies in the physical health domain, none of those identified in the emotional health domain were specifically designed to identify core components. This made it difficult for the committee to definitively iso-
late those program elements that are most effective in promoting emotional health. However, several key characteristics of programs show great promise in addressing internalizing and/or externalizing symptoms or behaviors related to emotional health. In general, programs that were provided universally, in school, with some in-person meeting, with multiple sessions over a greater number of weeks, and with the incorporation of CBT techniques showed some effectiveness for promoting emotional health among adolescents.
These results reflect those of other research on core components of mental health programs for youth. While our review did not include studies of adolescents with diagnosed mental health conditions, much of the seminal work on core components comes from this field. For example, core components research has shown that exposure to a fear or stressor may be the most important component of CBT for anxiety and traumatic stress (Seligman and Ollendick, 2011). Studies using similar approaches to identify the core components of prevention programs for emotional health will therefore be an important area for future research.
Social Health
No studies in our review focused exclusively on social health. This is likely because social health is often integrated into programs focused on social-emotional learning and positive youth development. Studies that include social health among the domains covered are discussed in greater detail in the section below on multiple optimal health domains.
Spiritual Health
As with social health, no studies in our review focused exclusively on spiritual health. However, a number of studies included outcomes related to spiritual health in combination with other areas of optimal health. These are described in the section on multiple optimal health domains as well.
Intellectual Health
Only one study in our review exclusively examined intellectual health outcomes (Hahn et al., 2015; Wilson et al., 2011). Unlike the studies in the other domains, this comprehensive meta-analysis was designed specifically to identify core components and thus to provide evidence for effective components of programs targeting intellectual health outcomes.
The authors of this study conducted a meta-analysis of programs and interventions aimed at increasing high school participation rates. They
included 152 studies in their meta-analysis,8 and the outcomes of interest included school enrollment, school dropout, and completion of a high school degree or the General Education Development (GED) tests. Programs included in the review fell into the following categories: attendance monitoring, multiservice packages, alternative schools, supplemental academic training, case management, school/class restructuring, skills training/CBT, college preparation, mentoring/counseling, vocational training, community service, and others. The vast majority of programs took place in schools, with others being delivered in community settings or in a combination of school and community settings. Most programs entailed daily contact with participants, and program duration averaged about two school years. The average age of participants was 15, although some programs targeted elementary school–aged children.
Broadly, this meta-analysis found that programs taking place in schools and those delivered in multiple settings (including schools) were more effective than those offered in community settings. It also found that all program types except those designated as “other” showed significant effectiveness in decreasing school dropout rates among program participants compared with the average dropout rate. Furthermore, while most categories of programs were equally effective, programs focused on attendance monitoring were significantly less successful than programs in most of the other categories.
It is significant that almost half of the studies in this review reported issues with program implementation, including structural issues (e.g., access to resources), staffing issues, funding issues, and difficulties obtaining administrator buy-in. This suggests that having supportive school environments and improved access to resources may help promote positive program effects. In addition, given the economic and health benefits of education, the provision of these additional services to socially disadvantaged youth can help improve their life opportunities and promote equity. Therefore, actions to create supportive school culture and promote equitable access to resources can have major impacts on adolescents’ overall health and well-being.
Multiple Optimal Health Domains
Given the interrelatedness of the dimensions of optimal health, it is not surprising that six of the systematic reviews and meta-analyses considered the effects of programs on outcomes in multiple optimal health domains
___________________
8 An additional 15 programs for teen mothers were included in the review but were analyzed separately given these participants’ specialized needs. Our summary is based on the 152 studies that were offered to broader populations of youth.
(Ciocanel et al., 2017; Durlak et al., 2011; Durlak, Weissberg, and Pachan, 2010; Klingbeil et al., 2017; MacArthur et al., 2018; Taylor et al., 2017). The behaviors and outcomes targeted in these reviews included substance use, pregnancy, sexual behavior, positive social behavior, academic performance, emotional distress, mindfulness, and self-regulation skills, among others. Despite this broad scope of outcomes, this part of the committee’s review ultimately encompasses the most consequential components of optimal health. Instead of focusing on a narrowly targeted behavior, the programs reviewed in this section attempted to teach skills that, if learned successfully, underlie and impact health in multiple domains and across the life course.
Most of the programs reviewed in these articles used a social-emotional learning or positive youth development framework. Both of these frameworks posit that supporting social and emotional skills and positive attitudes helps youth develop social and emotional assets that have positive effects on well-being and are protective against negative outcomes (Ciocanel et al., 2017; Durlak et al., 2011; Durlak, Weissberg, and Pachan, 2010; Taylor et al., 2017).
Klingbeil and colleagues (2017) studied mindfulness-based interventions, which similarly sought to provide youth with self-regulation and acceptance skills to improve physical, emotional, social, spiritual, and intellectual health outcomes. These skills are challenging to target through interventions, perhaps because they are difficult to measure and test. That said, these are skills that are required for some of the most important developmental tasks of adolescence. Also, many programs included in this study did show significant measurable effects on the outcomes of interest, effects that were maintained for as long as 18 months or more.
The programs addressed in these articles were most often delivered in schools or multiple locations that included schools (Dray et al., 2017; Durlak et al., 2011; MacArthur et al., 2018; Taylor et al., 2017) or in after school and community-based settings (Ciocanel et al., 2017; Durlak, Weissberg, and Pachan, 2010). Across multiple articles in our review, school-based programs that were provided universally to all students showed the strongest evidence of effectiveness (Durlak et al., 2011; MacArthur et al., 2018). This finding provides further support for the findings described earlier, suggesting that schools are particularly well suited for providing programs that have positive effects on multiple optimal health-related outcomes.
Participants in these programs were ages 5–18. Although the average age of participants was 10–19, these programs were more likely to include younger children relative to those described in previous subsections. Notably, there were reported differences in program effects by age. In particular, the Taylor et al. (2017) study found that programs for younger children (ages 5–10) had significantly greater effects on measured out-
comes compared with those for early adolescents (ages 11–13). However, effects did not differ between mid- to late adolescents (ages 14–18) and the younger age groups. Similarly, Dray and colleagues (2017) found that for younger children, resilience-focused programs were more effective in decreasing anxiety symptoms and emotional distress, whereas for adolescents, these programs were more effective in decreasing internalizing problems. Evidence from these studies provides further support for the value of starting programs early in the life course and for providing such programs at multiple stages of development to capitalize on the critical developmental windows between early childhood and young adulthood.
Another important finding from Taylor et al. (2017) and other studies was that there were few to no differences in program effects by demographic characteristics. More specifically, the positive effects of social-emotional learning and positive youth development programs were statistically equivalent for students of different racial/ethnic backgrounds and socioeconomic levels. Such findings indicate the value of these programs in achieving equitable, positive outcomes for all youth, regardless of background.
Program design and implementation were also critical components for program success. Programs that could be described by the SAFE acronym were most successful in producing positive effects on social, emotional, and intellectual health outcomes (Durlak et al., 2011; Durlak, Weissberg, and Pachan, 2010; Taylor et al., 2017). The SAFE acronym, which represents the design and implementation components that have been shown to be effective in producing positive outcomes, refers to programs that are (1) sequenced and have step-by-step training for facilitators, (2) include aspects of active learning, (3) have focused attention and adequate time devoted to skills training, and (4) have explicit definitions of program goals. Programs with the SAFE designation were consistently found to be more effective than those that did not have these characteristics, highlighting the importance of program design and fidelity in prevention and intervention programs.
Overall, the committee’s examination of this literature aligns with the five core social-emotional learning competencies developed by the Collaborative for Academic, Social, and Emotional Learning (CASEL) (2019). These competencies represent the foundational skills that programs might seek to achieve to promote healthy behaviors and outcomes for youth:
- Self-awareness: “The ability to accurately recognize one’s own emotions, thoughts, and values and how they influence behavior. The ability to accurately assess one’s strengths and limitations, with a well-grounded sense of confidence, optimism, and a ‘growth mindset.’” (para. 2)
- Self-management: “The ability to successfully regulate one’s emotions, thoughts, and behaviors in different situations—effectively managing stress, controlling impulses, and motivating oneself. The ability to set and work toward personal and academic goals.” (para. 3)
- Social awareness: “The ability to take the perspective of and empathize with others, including those from diverse backgrounds and cultures. The ability to understand social and ethical norms for behavior and to recognize family, school, and community resources and supports.” (para. 4)
- Relationship skills: “The ability to establish and maintain healthy and rewarding relationships with diverse individuals and groups. The ability to communicate clearly, listen well, cooperate with others, resist inappropriate social pressure, negotiate conflict constructively, and seek and offer help when needed.” (para. 5)
- Responsible decision making: “The ability to make constructive choices about personal behavior and social interactions based on ethical standards, safety concerns, and social norms. The realistic evaluation of consequences of various actions, and a consideration of the well-being of oneself and others.” (para. 6)
Summary
In summary, the committee’s ability to identify specific and discrete core program components was limited by the scope of the systematic reviews and meta-analyses currently available in the literature. Although we did not find consistent evidence of effectiveness for particular core components across all of the studies reviewed, several of the evaluated programs show promise across multiple domains of optimal health (see Box 4-1). In particular, social-emotional learning and positive youth development programs offer great potential benefit, as they are aimed at equipping children and adolescents with the foundational skills they need to engage in impulse control and self-regulation, skills that ultimately help them make healthy decisions in a variety of situations.
Importantly, while few of the papers in our review included digital e-health interventions, we recognize that this is more likely due to the age of the included studies rather than a representation of their utility. Since smartphones and computers have become nearly ubiquitous among adolescents today compared with even 5 years ago (Anderson and Jiang, 2018) (see Chapter 2), further investigation of the effectiveness of digitally delivered interventions among more contemporary cohorts of youth is needed.
RESULTS OF CORE COMPONENTS PAPER REVIEW
In addition to the systematic review of systematic reviews and meta-analyses reported above, the committee identified a selected group of papers that were clearly focused on core components of effective practice for improving outcomes in each of the optimal health domains. These papers used methodologies of systematic reviews or meta-analyses (Boustani et al., 2015) or were reviews of reviews (Peters et al., 2009). We used the results of our review of these papers to supplement the findings obtained from
our systematic review and to ensure that the most current research on core components would be explored and considered.
While a number of papers made reference to core components or elements, these articles were often focused on a specific program instead of considering the shared components of multiple programs. Findings from the four articles that met the final criteria for our core components review are summarized below (Boustani et al., 2015; Lawson et al., 2019; Peters et al., 2009; Tolan et al., 2016).
Boustani et al. (2015)
Boustani and colleagues (2015) identified common elements that exist across evidence-based prevention programs for multiple health behaviors and outcomes, including substance use, life skills, sexual health, violence, and depression/anxiety. To this end, they used a distillation and matching approach, which entails systematically reviewing EBPs to aggregate the core components that are most common to these programs and are thus likely to be the most effective (Chorpita et al., 2005). As the authors state:
The current findings lend initial support for this method of knowledge aggregation to identify a core set of skills designed to reduce common pathways to risk behaviors such as conduct problems and substance use—and to prepare youth for healthy trajectories characterized by successful relationships, prosocial behaviors, sexual health, and positive adjustment (Boustani et al., 2015, p. 215).
Across prevention programs for all outcomes, Boustani and colleagues (2015) found that problem solving was the most common practice component, followed by communication skills, assertiveness training, and insight building. The most common instructional components were psychoeducation, modeling, and role play (see Figure 4-7).
Although their review identified common components of these programs, the authors provide no statistical evidence that any of these components were more or less effective than others. This represents an important next step for future research.
Lawson et al. (2019)
CASEL is a compilation of evidence-based programs meant to facilitate social-emotional learning. While a number of such programs have been found to be successful, Lawson and colleagues (2019) suggest that a core set of components appears across programs. They first selected programs from the CASEL database that met the following criteria:
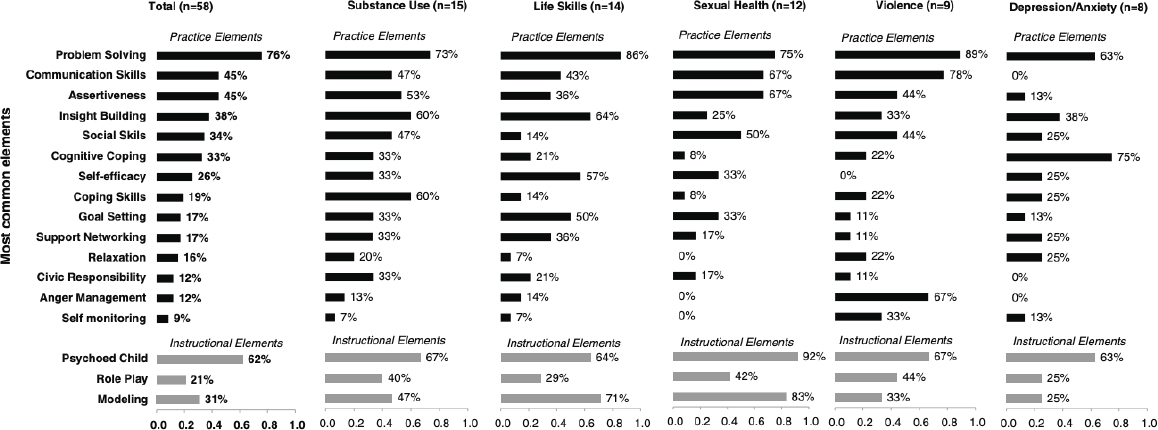
SOURCE: Boustani et al. (2015). Republished with permission of Taylor & Francis, Ltd. Permission conveyed through Copyright Clearance Center, Inc.
- targets all five areas of CASEL competence (self-awareness, self-management, social awareness, relationship skills, and responsible decision making);
- provides opportunities to practice;
- offers multiyear programming;
- offers training and other implementation support;
- has at least one evaluation study that included a comparison group and pre–post measures; and
- documents a positive impact on one of the four outcome domains (academics, conduct problems, emotional distress, prosocial behavior).
Next, the authors coded the components present in each of the 14 programs included in their final sample. The most common components were social skills (100% of programs), identifying others’ feelings (100% of programs), behavioral coping skills/relaxation (92.9% of programs), and identifying one’s own feelings (87.7% of programs). The least commonly addressed components were mindfulness (20% of programs), valuing diversity (63.6% of programs), cognitive coping/self-talk (75% of programs), and goal setting and planning (75% of programs).
Importantly, this review identified components that were present or absent in programs that had been determined to be efficacious, rather than testing the effectiveness of each component on its own. Testing for the effectiveness of each of these core components of social-emotional learning programs thus represents an important area for future research.
Tolan et al. (2016)
Tolan and colleagues (2016) took a broad and integrative approach to understanding a range of factors that might influence positive youth development. They compared four interrelated frameworks: social competence (SC) (Waters and Sroufe, 1983), social-emotional learning (SEL) (Elias, Zins, and Weissberg, 1997), positive youth development (PYD) (Lerner et al., 2002), and positive psychology (PPsy) (Seligman and Csikszentmihalyi, 2014). A major objective of the review was to identify core components across orientations, with a focus on developing a “unified framework to guide interventions” (Tolan et al., 2016, p. 215). The authors concluded that four core components are consistent across the models they reviewed and that these components facilitate positive outcomes: self-control, positive self-orientation, engagement with others, and societal bonding/moral ethical standards. Although each framework defines and measures these constructs slightly differently (see Table 4-2), they are nevertheless consistent themes that could serve as intervention targets to promote optimal
TABLE 4-2 Common Construct Threads and Potential Alignment Across the Four Frameworks
| Overarching constructs | SC | SEL | PYD | PPsy |
| Self-control | Self-control | Self-management | Character Competence | Accomplishment/Achievement |
| Positive self-orientation | Positive sense of self | Self-awareness | Confidence | Positive emotions |
| Engagement with others | Prosocial connectedness | Relationship skills Social awareness | Connection | Engagement & positive relationships |
| Societal bonding/Moral ethical standards | Moral system of belief & decision-making skills | Responsible decision making | Caring/Compassion | Meaning |
SOURCE: Tolan et al. (2016). Republished with permission of Springer Nature. Permission conveyed through Copyright Clearance Center, Inc.
health. Again, isolating and measuring the effects of these common components will be an important consideration for future research.
Peters et al. (2009)
As noted above in the discussion of the committee’s systematic review, schools are a common setting for many behavioral interventions; however, many school health education programs focus on a single behavioral domain. In contrast, integrative, multicomponent programs that address multiple behaviors may be more efficient. The review by Peters and colleagues (2009) suggests that this efficiency is enhanced if the elements of change are similar across all of the targeted behaviors and outcomes.
These authors conducted a systematic review of the effectiveness of school-based health promotion programs targeting substance use, sexual behavior, and nutrition.9 The 55 reviews included in their analysis yielded five core components deemed effective across all three targeted behaviors: being theory-based; addressing social influences (especially social norms); addressing cognitive-behavioral skills; including the training of facilitators; and consisting of multiple components. “Tentative” evidence also suggested
___________________
9 This paper indicates positive, negative, or no statistically significant effect of each program component, but does not report effect sizes. This reporting method makes it more difficult to compare the magnitudes of these effects.
positive effects of parent involvement and a greater number of sessions. In contrast, a knowledge-only approach was not effective in any of the above three domains, although the strength of evidence varied. All of these findings complement those identified in our systematic review.
Some components were more effective than others for certain groups of outcomes. In the domains of sexuality and nutrition programs, programs with a specific behavioral focus were more effective than those that addressed general issues (e.g., condom use vs. general sexuality). In addition, evidence indicated that addressing behavioral determinants and tailoring to cognitive ability or age were effective in these two domains. Strong and moderate reviews of sexuality and substance use programs indicated that tailoring interventions to the culture of the target group was also effective.
Sexuality and substance use programs both addressed abstinence goals, and strong reviews in both domains indicated their ineffectiveness and even their negative effects in some cases. Specifically, the authors state that “not one sexuality review stated positive conclusions about the effectiveness of abstinence-only programs, which portray abstinence from sex as the only or very best prevention option and usually do not discuss contraception,” and further state that one sexuality review “even reported negative effects.” For substance use, the authors state that “harm reduction or prevention of abuse may be more effective than a goal of abstinence or delayed use, at least for youth who already use.”
Summary
In summary, the additional papers the committee reviewed identify common components of effective programs, although statistical evidence is rarely provided to suggest that any of the components is more or less effective than others (see Box 4-2). Future work is needed in this area to provide a more complete understanding of the ways in which these components compare directly with one another, as well as the ways in which their efficacy may vary by particular demographic groups.
CONCLUSIONS
With respect to core components of programs that are effective in promoting positive adolescent health behaviors and outcomes, the committee drew the following conclusions.
CONCLUSION 4-1: Most current research is not designed to identify which components of adolescent risk behavior programs or interventions are more effective than others.
CONCLUSION 4-2: More research is needed to determine how, when, and for whom the common components of programs are effective in promoting positive adolescent health behaviors and outcomes.
CONCLUSION 4-3: Programs that are sequenced, include an active learning technique, have focused time devoted to skills training, and have explicit program goals are more effective than those that lack these characteristics.
CONCLUSION 4-4: Programs that incorporate approaches based on behavioral theory, social-emotional learning, and positive youth development are more successful in promoting positive adolescent health behaviors and outcomes across multiple optimal health domains relative to those that do not use these approaches to inform programmatic efforts.
CONCLUSION 4-5: Multicomponent, multisession programs focused on social-emotional learning and positive youth development that emphasize knowledge, attitudes, and skills are more successful in supporting healthy adolescent development than programs focused on individual risk behaviors.
CONCLUSION 4-6: Efforts to assist adolescents in making healthy decisions related to risk-taking behaviors—including alcohol and tobacco use and sexual activity, among others—need to begin in early childhood and continue through adolescence.
CONCLUSION 4-7: Programs that target social determinants of health and well-being can have widespread, positive effects on multiple behaviors and outcomes.
CONCLUSION 4-8: Having supportive environments and improved access to resources can lead to greater positive program effects.
CONCLUSION 4-9: Program development, implementation, and evaluation efforts would benefit from including youth of diverse ages, racial/ethnic backgrounds, socioeconomic status, rurality/urbanity, sexual orientations, sexes/genders, and disability/ability status.
The next and final chapter of this report provides the committee’s recommendations—based on the conclusions presented in Chapters 2 through 4—for research and the Office of the Assistant Secretary for Health’s programs and policies.
REFERENCES
Anderson, M., and Jiang, J. (2018). Teens, Social Media & Technology 2018. Washington, DC: Pew Research Center.
Aslam, R.W., Hendry, M., Booth, A., Carter, B., Charles, J.M., Craine, N., Edwards, R.T., Noyes, J., Ntambwe, L.I., Pasterfield, D., Rycroft-Malone, J., Williams, N., and Whitaker, R. (2017). Intervention now to eliminate repeat unintended pregnancy in teenagers (INTERUPT): A systematic review of intervention effectiveness and cost-effectiveness, and qualitative and realist synthesis of implementation factors and user engagement. BMC Medicine, 15(1), 155.
Baltimore City Health Department. (2019). TPP Grantee Memo: Baltimore City Health Department U Choose program. Memo to the Committee on Applying Lessons of Optimal Adolescent Health to Improve Behavioral Outcomes for Youth. Baltimore City, MD: Baltimore City Health Department.
Barth, R.P., and Liggett-Creel, K. (2014). Common components of parenting programs for children birth to eight years of age involved with child welfare services. Children and Youth Services Review, 40, 6–12.
Blase, K., and Fixsen, D. (2013). Core Intervention Components: Identifying and Operationalizing What Makes Programs Work. ASPE Research Brief. U.S. Department of Health and Human Services. Available: https://aspe.hhs.gov/report/core-intervention-componentsidentifying-and-operationalizing-what-makes-programs-work.
Botvin, G.J. (1983). Prevention of adolescent substance abuse through the development of personal and social competence. Preventing Adolescent Drug Abuse: Intervention Strategies, 115–140.
Boustani, M.M., Frazier, S.L., Becker, K.D., Bechor, M., Dinizulu, S.M., Hedemann, E.R., Ogle, R.R., and Pasalich, D.S. (2015). Common elements of adolescent prevention programs: Minimizing burden while maximizing reach. Administration and Policy in Mental Health and Mental Health Services Research, 42(2), 209–219.
Calear, A.L., and Christensen, H. (2010). Systematic review of school-based prevention and early intervention programs for depression. Journal of Adolescence, 33(3), 429–438.
Carney, T., Myers, B.J., Louw, J., and Okwundu, C.I. (2016). Brief school-based interventions and behavioural outcomes for substance-using adolescents. Cochrane Database of Systematic Reviews(1), Cd008969.
Centers for Disease Control and Prevention (CDC). (2017). Picture of America: Prevention. Atlanta, GA: Author.
Champion, K.E., Newton, N.C., Barrett, E.L., and Teesson, M. (2013). A systematic review of school-based alcohol and other drug prevention programs facilitated by computers or the internet. Drug and Alcohol Review, 32(2), 115–123.
Chin, H.B., Sipe, T.A., Elder, R., Mercer, S.L., Chattopadhyay, S.K., Jacob, V., Wethington, H.R., Kirby, D., Elliston, D.B., Griffith, M., Chuke, S.O., Briss, S.C., Ericksen, I., Galbraith, J.S., Herbst, J.H., Johnson, R.L., Kraft, J.M., Noar, S.M., Romero, L.M., and Santelli, J. (2012). The effectiveness of group-based comprehensive risk-reduction and abstinence education interventions to prevent or reduce the risk of adolescent pregnancy, human immunodeficiency virus, and sexually transmitted infections: Two systematic reviews for the Guide to Community Preventive Services. American Journal of Preventive Medicine, 42(3), 272–294.
Chorpita, B.F., and Daleiden, E.L. (2009). Mapping evidence-based treatments for children and adolescents: Application of the distillation and matching model to 615 treatments from 322 randomized trials. Journal of Consulting and Clinical Psychology, 77(3), 566–579.
Chorpita, B.F., Delaiden, E.L., and Weisz, J.R. (2005). Identifying and selecting the common elements of evidence based interventions: A distillation and matching model. Mental Health Services Research, 7, 5–20.
Cialdini, R.B., and Goldstein, N.J. (2004). Social influence: Compliance and conformity. Annual Review of Psychology, 55, 591–621.
Ciocanel, O., Power, K., Eriksen, A., and Gillings, K. (2017). Effectiveness of positive youth development interventions: A meta-analysis of randomized controlled trials. Journal of Youth and Adolescence, 46(3), 483–504.
Clarke, A.M., Kuosmanen, T., and Barry, M.M. (2015). A systematic review of online youth mental health promotion and prevention interventions. Journal of Youth and Adolescence, 44(1), 90–113.
Collaborative for Academic, Social, and Emotional Learning. (2019). Core SEL Competencies. Available: https://casel.org/core-competencies.
Corrieri, S., Heider, D., Conrad, I., Blume, A., Konig, H-H., and Riedel-Heller, S.G. (2014). School-based prevention programs for depression and anxiety in adolescence: A systematic review. Health Promotion International, 29(3), 427–441.
Das, J.K., Salam, R.A., Lassi, Z.S., Khan, M.N., Mahmood, W., Patel, V., and Bhutta, Z.A. (2016). Interventions for adolescent mental health: An overview of systematic reviews. Journal of Adolescent Health, 59(4S), S49–S60.
David P. Weikart Center for Youth Program Quality. (2019). Youth Program Quality Assessment® and School-Age Program Quality Assessment. Available: http://cypq.org/assessment.
DeSmet, A., Shegog, R., Van Ryckeghem, D., Crombez, G., and De Bourdeaudhuij, I. (2015). A systematic review and meta-analysis of interventions for sexual health promotion involving serious digital games. Games and Health Journal, 4(2), 78–90.
Dray, J., Bowman, J., Campbell, E., Freund, M., Wolfenden, L., Hodder, R.K., McElwaine, K., Tremain, D., Bartlem, K., Bailey, J., Small, T., Palazzi, K., Oldmeadow, C., and Wiggers, J. (2017). Systematic review of universal resilience-focused interventions targeting child and adolescent mental health in the school setting. Journal of the American Academy of Child & Adolescent Psychiatry, 56(10), 813–824.
Durlak, J.A., Weissberg, R.P., Dymnicki, A.B., Taylor, R.D., and Schellinger, K.B. (2011). The impact of enhancing students’ social and emotional learning: A meta-analysis of school-based universal interventions. Child Development, 82(1), 405–432.
Durlak, J.A., Weissberg, R.P., and Pachan, M. (2010). A meta-analysis of after-school programs that seek to promote personal and social skills in children and adolescents. American Journal of Community Psychology, 45(3–4), 294–309.
Elias, M.J., Zins, J.E., and Weissberg, R.P. (1997). Promoting Social and Emotional Learning: Guidelines for Educators. Alexandria, VA: Association for Supervision and Curriculum Development.
Embry, D.D., and Biglan, A. (2008). Evidence-based kernels: Fundamental units of behavioral influence. Clinical Child and Family Psychology Review, 11(3), 75–113.
Faggiano, F., Minozzi, S., Versino, E., and Buscemi, D. (2014). Universal school-based prevention for illicit drug use. Cochrane Database of Systematic Reviews(12), Cd003020.
Ferri, M., Allara, E., Bo, A., Gasparrini, A., and Faggiano, F. (2013). Media campaigns for the prevention of illicit drug use in young people. Cochrane Database of Systematic Reviews(6), Cd009287.
Gordon, R.S. (1983). An operational classification of disease prevention. Public Health Reports, 98(2), 107.
Hahn, R.A., Knopf, J.A., Wilson, S.J., Truman, B.I., Milstein, B., Johnson, R.L., Fielding, J.E., Muntaner, C.J.M., Jones, C.P., Fullilove, M.T., Moss, R.D., Ueffing, E., and Hunt, P.C. (2015). Programs to increase high school completion: A Community Guide systematic health equity review. American Journal of Preventive Medicine, 48(5), 599–608.
Harden, A., Brunton, G., Fletcher, A., and Oakley, A. (2009). Teenage pregnancy and social disadvantage: Systematic review integrating controlled trials and qualitative studies. British Medical Journal, 339, b4254.
Hodder, R.K., Freund, M., Wolfenden, L., Bowman, J., Nepal, S., Dray, J., Kingsland, M., Yoong, S.L., and Wiggers, J. (2017). Systematic review of universal school-based ‘resilience’ interventions targeting adolescent tobacco, alcohol or illicit substance use: A meta-analysis. Preventive Medicine, 100, 248–268.
Hofmann, S.G., Asnaani, A., Vonk, I.J.J., Sawyer, A.T., and Fang, A. (2012). The efficacy of cognitive behavioral therapy: A review of meta-analyses. Cognitive Therapy and Research, 36(5), 427–440.
Hogue, A., Bobek, M., Dauber, S., Henderson, C.E., McLeod, B.D., and Southam-Gerow, M.A. (2017). Distilling the core elements of family therapy for adolescent substance use: Conceptual and empirical solutions. Journal of Child & Adolescent Substance Abuse, 26(6), 437–453.
Institute of Medicine. (1994). Reducing Risks for Mental Disorders: Frontiers for Preventive Intervention Research. Washington, DC: The National Academies Press.
Katz, D.L., and Ali, A. (2009). Preventive Medicine, Integrative Medicine, and the Health of the Public. Washington, DC: Institute of Medicine.
Klingbeil, D.A., Renshaw, T.L., Willenbrink, J.B., Copek, R.A., Chan, K.T., Haddock, A., Yassine, J., and Clifton, J. (2017). Mindfulness-based interventions with youth: A comprehensive meta-analysis of group-design studies. Journal of School Psychology, 63, 77–103.
Lawson, G.M., McKenzie, M.E., Becker, K.D., Selby, L., and Hoover, S.A. (2019). The core components of evidence-based social emotional learning programs. Prevention Science, 20(4), 457–467.
Lerner, R.M., Brentano, C., Dowling, E.M., and Anderson, P.M. (2002). Positive youth development: Thriving as the basis of personhood and civil society. New Directions for Youth Development, 2002(95), 11–34.
Lipsey, M.W. (2018). Effective use of the large body of research on the effectiveness of programs for juvenile offenders and the failure of the model programs approach. Criminology & Public Policy, 17(1), 189–198.
Lopez, L.M., Bernholc, A., Chen, M., and Tolley, E.E. (2016). School-based interventions for improving contraceptive use in adolescents. Cochrane Database of Systematic Reviews(6), Cd012249.
MacArthur, G., Caldwell, D.M., Redmore, J., Watkins, S.H., Kipping, R., White, J., Chittleborough, C., Langford, R., Er, V., Lingam, R., Pasch, K., Gunnell, D., Hickman, M., and Campbell, R. (2018). Individual-, family-, and school-level interventions targeting multiple risk behaviours in young people. Cochrane Database of Systematic Reviews(10).
MacArthur, G.J., Harrison, S., Caldwell, D.M., Hickman, M., and Campbell, R. (2016). Peer-led interventions to prevent tobacco, alcohol and/or drug use among young people aged 11–21 years: A systematic review and meta-analysis. Addiction, 111(3), 391–407.
Marseille, E., Mirzazadeh, A., Biggs, M.A., Miller, A.P., Horvath, H., Lightfoot, M., Malekinejad, M., and Kahn, J.G. (2018). Effectiveness of school-based teen pregnancy prevention programs in the USA: A systematic review and meta-analysis. Prevention Science, 19(4), 468–489.
Mary Black Foundation. (2019). TPP grantee memo: Mary Black Foundation. Memo to the Committee on Applying Lessons of Optimal Adolescent Health to Improve Behavioral Outcomes for Youth. Spartanburg, SC: Mary Black Foundation.
Methodist Le Bonheur Community Outreach. (2019). TPP grantee memo: Methodist Le Bonheur Community Outreach. Memo to the Committee on Applying Lessons of Optimal Adolescent Health to Improve Behavioral Outcomes for Youth. Memphis, TN: Methodist Le Bonheur Community Outreach.
Moher, D., Liberati, A., Tetzlaff, J., and Altman, D.G. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Annals of Internal Medicine, 151(4), 264–269.
Morehouse School of Medicine. (2019). TPP Grantee Memo: Morehouse School of Medicine’s Carrera Program. Memo to the Committee on Applying Lessons of Optimal Adolescent Health to Improve Behavioral Outcomes for Youth. Atlanta, GA: Morehouse School of Medicine.
National Academies of Sciences, Engineering, and Medicine (NASEM). (2019). Applying Lessons of Optimal Adolescent Health to Improve Behavioral Outcomes for Youth: Public Information-Gathering Session: Proceedings of a Workshop-In Brief. Washington, DC: The National Academies Press.
O’Donnell, M.P. (2009). Definition of health promotion 2.0: Embracing passion, enhancing motivation, recognizing dynamic balance, and creating opportunities. American Journal of Health Promotion, 24(1), iv.
Onrust, S.A., Otten, R., Lammers, J., and Smit, F. (2016). School-based programmes to reduce and prevent substance use in different age groups: What works for whom? Systematic review and meta-regression analysis. Clinical Psychology Review, 44, 45–59.
Oringanje, C., Meremikwu, M.M., Eko, H., Esu, E., Meremikwu, A., and Ehiri, J.E. (2016). Interventions for preventing unintended pregnancies among adolescents. Cochrane Database of Systematic Reviews(2).
Pallmann, P., Bedding, A.W., Choodari-Oskooei, B., Dimairo, M., Flight, L., Hampson, L.V., Holmes, J., Mander, A.P., Odondi, L., Sydes, M.R., Villar, S.S., Wason, J.M.S., Weir, C.J., Wheeler, G.M., Yap, C., and Jaki, T. (2018). Adaptive designs in clinical trials: Why use them, and how to run and report them. BMC Medicine, 16(1), 29.
Peters, L.W.H., Kok, G., Ten Dam, G.T.M., Buijs, G.J., and Paulussen, T.G.W.M. (2009). Effective elements of school health promotion across behavioral domains: A systematic review of reviews. BMC Public Health, 9, 182.
Picot, J., Shepherd, J., Kavanagh, J., Cooper, K., Harden, A., Barnett-Page, E., Jones, J., Clegg, A., Hartwell, D., and Frampton, G.K. (2012). Behavioural interventions for the prevention of sexually transmitted infections in young people aged 13–19 years: A systematic review. Health Education Research, 27(3), 495–512.
Prochaska, J.O. and Velicer, W.F. (1997). The transtheoretical model of health behavior change. American Journal of Health Promotion, 12(1), 38–48.
San Diego Youth Services. (2019). TPP Grantee Memo: San Diego Youth Services. Memo to the Committee on Applying Lessons of Optimal Adolescent Health to Improve Behavioral Outcomes for Youth. San Diego, CA: San Diego Youth Services.
Seligman, L.D. and Ollendick, T.H. (2011). Cognitive-behavioral therapy for anxiety disorders in youth. Child and Adolescent Psychiatric Clinics of North America, 20(2), 217–238.
Seligman, M.E.P., and Csikszentmihalyi, M. (2014). Positive psychology: An introduction. In M. Csikszentmihalyi (Ed.), Flow and the Foundations of Positive Psychology (279–298). Berlin, Germany: Springer Science+Business Media.
Shepherd, J., Kavanagh, J., Picot, J., Cooper, K., Harden, A., Barnett-Page, E., Jones, J., Clegg, A., Hartwell, D., Frampton, G.K., and Price, A. (2010). The effectiveness and cost-effectiveness of behavioural interventions for the prevention of sexually transmitted infections in young people aged 13–19: A systematic review and economic evaluation. Health Technology Assessment, 14(7), 1–206, iii–iv.
Tanner-Smith, E.E., Steinka-Fry, K.T., Hennessy, E.A., Lipsey, M.W., and Winters, K.C. (2015). Can brief alcohol interventions for youth also address concurrent illicit drug use? Results from a meta-analysis. Journal of Youth and Adolescence, 44(5), 1011–1023.
Taylor, R.D., Oberle, E., Durlak, J.A., and Weissberg, R.P. (2017). Promoting positive youth development through school-based social and emotional learning interventions: A meta-analysis of follow-up effects. Child Development, 88(4), 1156–1171.
The Center for Black Women’s Wellness Inc. (2019). TPP Grantee Memo: The Center for Black Women’s Wellness, Inc. Memo to the Committee on Applying Lessons of Optimal Adolescent Health to Improve Behavioral Outcomes for Youth. Fulton County, GA: The Center for Black Women’s Wellness, Inc.
Thomas, R.E., Lorenzetti, D.L., and Spragins, W. (2013). Systematic review of mentoring to prevent or reduce alcohol and drug use by adolescents. Academic Pediatrics, 13(4), 292–299.
Thomas, R.E., McLellan, J., and Perera, R. (2015). Effectiveness of school-based smoking prevention curricula: Systematic review and meta-analysis. BMJ Open, 5(3), e006976.
Tolan, P., Ross, K., Arkin, N., Godine, N., and Clark, E. (2016). Toward an integrated approach to positive development: Implications for intervention. Applied Developmental Science, 20(3), 214–236.
U.S. Department of Justice. (2013). CrimeSolutions.gov Practices Scoring Instrument. Washington, DC: Office of Justice Programs.
U.S. Preventive Services Task Force. (2018). Procedure Manual. Available: https://www.uspreventiveservicestaskforce.org/Page/Name/procedure-manual.
van Genugten, L., Dusseldorp, E., Massey, E.K., and van Empelen, P. (2017). Effective self-regulation change techniques to promote mental wellbeing among adolescents: A meta-analysis. Health Psychology Review, 11(1), 53–71.
Veritas Health Innovation. (2019). Covidence Systematic Review Software. Available: http://www.covidence.org.
Waters, E. and Sroufe, L.A. (1983). Social competence as a developmental construct. Developmental Review, 3(1), 79–97.
Whitaker, R., Hendry, M., Aslam, R.W., Booth, A., Carter, B., Charles, J.M., Craine, N., Edwards, R.T., Noyes, J., Ntambwe, L.I., Pasterfield, D., Rycroft-Malone, J., and Williams, N. (2016). Intervention now to eliminate repeat unintended pregnancy in teenagers (INTERUPT): A systematic review of intervention effectiveness and cost-effectiveness, and qualitative and realist synthesis of implementation factors and user engagement. Health Technology Assessment, 20(16), 1–214.
Wilson, S.J., Tanner-Smith, E.E., Lipsey, M.W., Steinka-Fry, K., and Morrison, J. (2011). Dropout prevention and intervention programs: Effects on school completion and dropout among school aged children and youth. Campbell Systematic Reviews, 8, 61.
This page intentionally left blank.










































