
Appendix
Mental Health Disorders: Additional Information
GUIDELINES CONSULTED FOR REVIEW OF EFFECTIVE TREATMENTS FOR EACH MENTAL HEALTH DISORDER
The clinical guidelines listed in Tables A-1 through A-5 were selected for each of the mental health disorders based on their comprehensiveness and relevance to the questions; their transparency and the clarity about literature search strategies and approaches to evidence-based decisions; recently updated information; and whether the guideline had external peer review.
TABLE A-1 Selected Clinical Guidelines Related to Major Depressive Disorder
| Resource Title | Organization | Year |
|---|---|---|
| Clinical Practice Guideline for the Management of Major Depressive Disorder | U.S. Department of Veterans Affairs/U.S. Department of Defense | 2016 |
| Clinical Guidelines for the Management of Adults with Major Depressive Disorder | Canadian Network for Mood and Anxiety | 2016 |
| Practice Guideline for the Treatment of Patients with Major Depressive Disorder (also, “Quick Reference Guide,” APA, 2010) | American Psychiatric Association | 2010 |
| Depression in Adults: Recognition and Management | National Institute for Health and Care Excellence | 2009 |
TABLE A-2 Selected Clinical Guidelines Related to Bipolar Disorders
| Resource Title | Organization | Year |
|---|---|---|
| The World Federation of Societies of Biological Psychiatry (WFSBP) for the Biological Treatment of Bipolar Disorders: Acute and Long-term Treatment of Mixed States in Bipolar Disorders | World Federation of Societies of Biological Psychiatry | 2018 |
| Canadian Network for Mood and Anxiety Treatments and the International Society | Canadian Network for Mood and Anxiety | 2018 |
| for Bipolar Disorders 2018 Guidelines for the Management of Patients with Bipolar Disorders | International Society for Bipolar Disorders | |
| The International College of Neuro-Psychopharmacology Treatment Guidelines for Bipolar Disorder in Adults, Part 2: Review, Grading of the Evidence, and a Precise Algorithm | International College of Neuro-Psychopharmacology | 2017 |
| Evidence-Based Guidelines for Treating Bipolar Disorder: Revised Third Edition Recommendations from the British Association for Psychopharmacology | British Association for Psychopharmacology | 2016 |
| Royal Australian and New Zealand College of Psychiatrists Clinical Practice Guidelines for Mood Disorders | Royal Australian and New Zealand College of Psychiatrists | 2015 |
| Bipolar Disorder: Assessment and Management Guidelines | National Institute for Health and Care Excellence | 2014 |
| Management of Bipolar Disorders in Adults | U.S. Department of Veterans Affairs/U.S. Department of Defense | 2010 |
| World Federation of Societies of Biological Psychiatry Guidelines for the Biological Treatment of Bipolar Disorders: Update 2009 on the Treatment of Acute Mania | World Federation of Societies of Biological Psychiatry | 2009 |
| Practice Guideline for the Treatment of Patients with Bipolar Disorder | American Psychiatric Association | 2002 |
TABLE A-3 Selected Clinical Guidelines Related to Posttraumatic Stress Disorder
| Resource Title | Organization | Year |
|---|---|---|
| Clinical Practice Guideline for the Treatment of Posttraumatic Stress Disorder | American Psychological Association | 2017 |
| VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder and Acute Stress Disorder | U.S. Department of Veterans Affairs/U.S. Department of Defense | 2017 |
| ISTSS PTSD Prevention and Treatment Guidelines Methodology and Recommendations | International Society for Traumatic Stress Studies | 2019 |
| Psychological and Pharmacological Treatments for Adults with Posttraumatic Stress Disorder: A Systematic Review Update | Agency for Healthcare Research Quality | 2018 |
TABLE A-4 Selected Clinical Guidelines Related to Obsessive Compulsive Disorder
| Title | Organization | Year |
|---|---|---|
| Practice Parameter for the Assessment and Treatment of Children and Adolescents with Obsessive Compulsive Disorder | American Academy of Child and Adolescent Psychiatry | 2012 |
| Practice Guideline for the Treatment of Patients with Obsessive-Compulsive Disorder | American Psychiatric Association | 2007 |
| Obsessive-Compulsive Disorder and Body Dysmorphic Disorder: Treatment | National Institute for Health and Care Excellence | 2005 |
| Obsessive-Compulsive Disorder Evidence Update September 2013 | National Institute for Health and Care Excellence | 2013 |
| Evidence-Based Pharmacological Treatment of Anxiety Disorders, Post-Traumatic Stress Disorder and Obsessive-Compulsive Disorder: A Revision of the 2005 Guidelines from the British Association for Psychopharmacology | British Association for Psychopharmacology/Baldwin | 2014 |
| Canadian Clinical Practice Guidelines for the Management of Anxiety, Posttraumatic Stress and Obsessive-Compulsive Disorders | Anxiety Disorders Association of Canada | 2014 |
| World Federation of Societies of Biological Psychiatry Guidelines for the Pharmacological Treatment of Anxiety, Obsessive Compulsive and Post-Traumatic Stress Disorders—First Revision | World Federation of Societies of Biological Psychiatry | 2008 |
TABLE A-5 Selected Clinical Guidelines Related to Anxiety Disorders
| Generalized Anxiety Disorder | ||
|---|---|---|
| Guide Title | Organization | Year |
| Evidence-Based Pharmacological Treatment of Anxiety Disorders, Post-Traumatic Stress Disorder and Obsessive-Compulsive Disorder: A Revision of the 2005 Guidelines from the British Association for Psychopharmacology | British Association for Psychopharmacology | 2014 |
| Canadian Clinical Practice Guidelines for the Management of Anxiety, Posttraumatic Stress and Obsessive-Compulsive Disorders | Anxiety Disorders Association of Canada | 2014 |
| Guidelines for the Pharmacological Treatment of Anxiety Disorders, Obsessive–Compulsive Disorder and Posttraumatic Stress Disorder in Primary Care | World Federation of Biological Psychiatry | 2012 |
| Generalized Anxiety Disorder and Panic Disorder in Adults: Management | National Institute for Health and Care Excellence | 2011 |
| Royal Australian and New Zealand College of Psychiatrists Clinical Practice Guidelines for the Treatment of Panic Disorder, Social Anxiety Disorder and Generalized Anxiety Disorders | Royal Australian and New Zealand College of Psychiatrists | 2018 |
| Panic Disorder | ||
| Guide Title | Organization | Year |
| Evidence-Based Pharmacological Treatment of Anxiety Disorders, Post-Traumatic Stress Disorder and Obsessive-Compulsive Disorder: A Revision of the 2005 Guidelines from the British Association for Psychopharmacology | British Association for Psychopharmacology | 2014 |
| Canadian Clinical Practice Guidelines for the Management of Anxiety, Posttraumatic Stress and Obsessive-Compulsive Disorders | Anxiety Disorders Association of Canada | 2014 |
| Guidelines for the Pharmacological Treatment of Anxiety Disorders, Obsessive–Compulsive Disorder and Posttraumatic Stress Disorder in Primary Care | World Federation of Biological Psychiatry | 2012 |
| Generalized Anxiety Disorder and Panic Disorder in Adults: Management | National Institute for Health and Care Excellence | 2011 |
| Australian and New Zealand Clinical Practice Guidelines for the Treatment of Panic Disorder and Agoraphobia | Royal Australian and New Zealand College of Psychiatrists | 2003 |
| Social Anxiety Disorder | ||
|---|---|---|
| Guide Title | Organization | Year |
| Evidence-Based Pharmacological Treatment of Anxiety Disorders, Post-Traumatic Stress Disorder and Obsessive-Compulsive Disorder: A Revision of the 2005 Guidelines from the British Association for Psychopharmacology | British Association for Psychopharmacology | 2014 |
| Canadian Clinical Practice Guidelines for the Management of Anxiety, Posttraumatic Stress and Obsessive-Compulsive Disorders | Anxiety Disorders Association of Canada | 2014 |
| Social Anxiety Disorder: Recognition, Assessment, and Treatment | National Institute for Health and Care Excellence | 2013 |
| Guidelines for the Pharmacological Treatment of Anxiety Disorders, Obsessive–Compulsive Disorder and Posttraumatic Stress Disorder in Primary Care | World Federation of Biological Psychiatry | 2012 |
DECIDING ON A MANAGEMENT APPROACH
Once a full assessment has been conducted to identify the severity of the disorder (e.g., risk of suicide), clinicians are guided by decisions-making algorithms, depending on the patients’ status. Presented below are the algorithms for major depressive disorder (see Figure A-1) and for a mania/hypomania episode in bipolar disorder (see Figure A-2) from the U.S. Department of Veterans Affairs/U.S. Department of Defense (VA/DoD) guidelines as examples of how to decide on a management approach.
OBSESSIVE COMPULSIVE DISORDER DIAGNOSTIC CRITERIA COMPARISON
The committee notes that the diagnostic criteria for obsessive compulsive disorder changed to some extent between the Diagnostic and Statistical Manual for Mental Disorders, 4th Edition (DSM-IV), which was used before 2013, and the Diagnostic and Statistical Manual for Mental Disorders, 5th Edition (DSM-5). Table A-6 shows the differences between DSM-IV and DSM-5. In DSM-IV, obsessive compulsive disorder was considered in the class of Anxiety Disorders. This changed to a new class in DSM-5, Obsessive-Compulsive and Related Disorders. The changes allow the individual to have a diagnosis of obsessive compulsive disorder without any insight into the fact that the thoughts/behaviors are a product of the
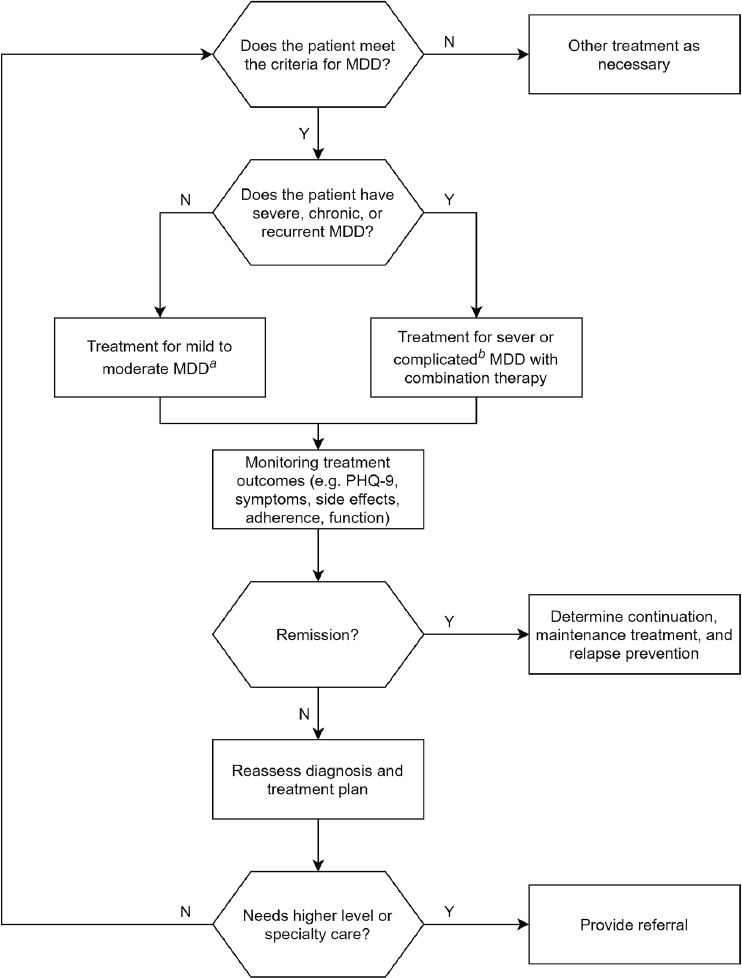
aFor mild to moderate major depressive disorder (MDD), monotherapy with psychotherapy or pharmacotherapy is recommended.
bFor severe or complicated MDD, a combination of a psychotherapy modality and pharmacotherapy is recommended. The DoD/VA guidelines define complicated MDD as when mania, depression with psychosis, or co-existing cognitive impairment co-exist.
SOURCE: Adapted from the VA/DoD guidelines.
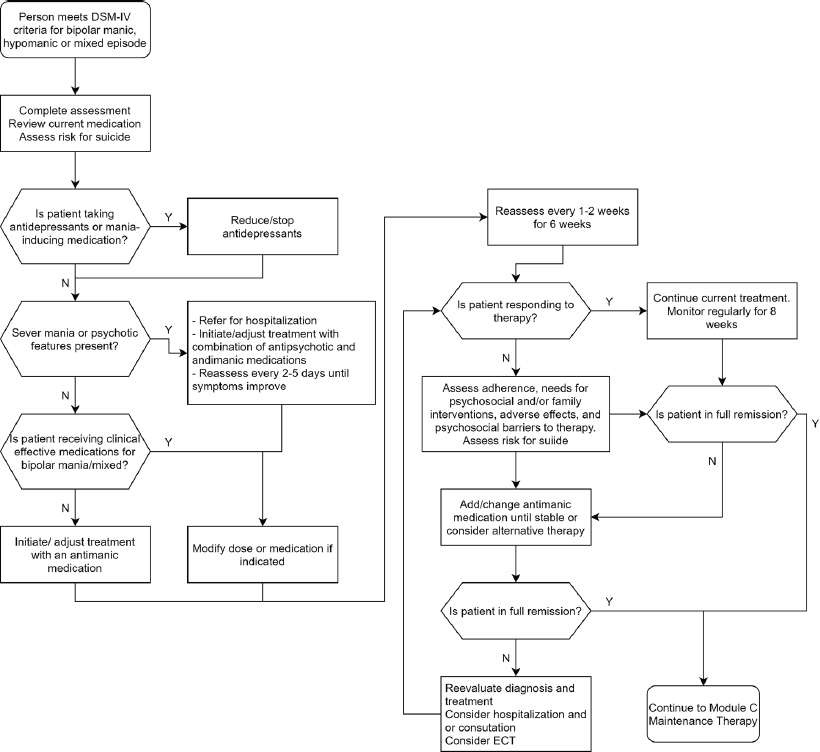
SOURCE: Adapted from the VA/DoD guidelines.
individual’s mind or reach the threshold of delusion. DSM-5 also allows specification of the presence of a current or past tic disorder. The fact that obsessive compulsive disorder in DSM-IV allows for a psychosis suggests that a diagnosis of obsessive compulsive disorder could be even more severe than under DSM-IV.
TABLE A-6 DSM-IV to DSM-5 Obsessive Compulsive Disorder Comparison
| DSM-IV | DSM-5 |
|---|---|
| Disorder class: Anxiety Disorders | Disorder class: Obsessive-Compulsive and Related Disorders |
| Presence of either obsessions or compulsions: | Presence of obsessions, compulsions, or both: |
| Obsessions as defined by (1), (2), (3), and (4): | Obsessions are defined by (1) and (2): |
| 1. Recurrent and persistent thoughts, impulses, or images that are experienced, at some time during the disturbance, as intrusive and inappropriate and that cause marked anxiety or distress. | 1. Recurrent and persistent thoughts, urges, or images that are experienced, at some time during the disturbance, as intrusive, unwanted, and that in most individuals cause marked anxiety or distress. |
| 2. The thoughts, impulses, or images are not simply excessive worries about real-life problems. | DROPPED |
| 3. The person attempts to ignore or suppress such thoughts, impulses, or images or to neutralize them with some other thought or action. | 2. The individual attempts to ignore or suppress such thoughts, urges, or images, or to neutralize them with some thought or action (i.e., by performing a compulsion). |
| 4. The person recognizes that the obsessional thoughts, impulses, or images are a product of his or her own mind (not imposed from without as with thought insertion). | DROPPED |
| Compulsions as defined by (1) and (2): | Compulsions are defined by (1) and (2): |
| 1. Repetitive behaviors (e.g., hand washing, ordering, checking) or mental acts (e.g., praying, counting, repeating words silently) that the person feels driven to perform in response to an obsession, or according to the rules that must be applied rigidly. | 1. Repetitive behaviors (e.g., hand washing, ordering, checking) or mental acts (e.g., praying, counting, repeating words silently) that the person feels driven to perform in response to an obsession, or according to the rules that must be applied rigidly. |
| 2. The behaviors or mental acts are aimed at preventing or reducing distress or preventing some dreaded event or situation. However, these behaviors or mental acts either are not connected in a realistic way with what they are designed to neutralize or prevent or are clearly excessive. | 2. The behaviors or mental acts are aimed at preventing or reducing distress or preventing some dreaded event or situation. However, these behaviors or mental acts either are not connected in a realistic way with what they are designed to neutralize or prevent or are clearly excessive. |
| At some point during the course of the disorder, the person has recognized that the obsessions or compulsions are excessive or unreasonable. | DROPPED |
| The obsessions and compulsions cause marked distress, are time consuming (take more than 1 hour per day), or significantly interfere with the person’s normal routine, occupational (or academic) functioning, or usual social activities or relationships. | The obsessions or compulsions are time consuming (e.g., take more than 1 hour per day) or cause clinically significant distress or impairment in social, occupational, or other important areas of functioning. |
| If another Axis I disorder is present, the content of the obsessions or compulsions is not restricted to it (e.g., preoccupation with food in the presence of an eating disorder, hair pulling in the presence of trichotillomania; concern with appearance in the presence of body dysmorphic disorder; preoccupation with drugs in the presence of a substance use disorder; preoccupation with having a serious illness in the presence of hypochondriasis; preoccupation with sexual urges or fantasies in the presence of a paraphilia; or guilty ruminations in the presence of major depressive disorder). | The disturbance is not better explained by the symptoms of another mental disorder (e.g., excessive worries, as in generalized anxiety disorder; preoccupation with appearance, as in body dysmorphic disorder; difficulty discarding or parting with possession, as in hoarding disorder; hair pulling, as in trichotillomania [hair-pulling disorder]; skin picking, as in excoriation [skin-picking] disorder; stereotypies, as in stereotypic movement disorder; ritualized eating behavior, as in eating disorders; preoccupation with substances or gambling, as in substance-related and addictive disorders; sexual urges or fantasies, as in paraphilic disorders; impulses, as in disruptive, impulse-control, and conduct disorders; guilty ruminations, as in major depressive disorder; thought insertion or delusional preoccupations, as in schizophrenia spectrum and other psychotic disorders; or repetitive patterns of behavior, as in autism spectrum disorder). |
| The disturbance is not due to the direct physiological effects of a substance (e.g., drug of abuse, a medication) or a general medical condition. | The disturbance is not due to the direct physiological effects of a substance (e.g., drug of abuse, a medication) or a general medical condition. |
| Specify if: | Specify if: |
| With poor insight: If, for most of the time during the current episode, the person does not recognize that the obsessions and compulsions are excessive or unreasonable. | With good or fair insight: The individual recognizes that obsessive-compulsive beliefs are definitely or probably not true or that they may or may not be true. With poor insight: The individual thinks obsessive-compulsive disorder beliefs are probably true. With absent insight/delusional beliefs: The individual is completely convinced that obsessive-compulsive disorder beliefs are true. |
| Specify if: Tic related: The individual has a current or past history of a tic disorder. |
REFERENCES
Andrews, G., C. Bell, P. Boyce, C. Gale, L. Lampe, O. Marwat, R. Rapee, and G. Wilkins. 2018. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the treatment of panic disorder, social anxiety disorder and generalised anxiety disorder. Australian and New Zealand Journal of Psychiatry 52(12):1109–1172.
APA (American Psychiatric Association). 2010. Practice guideline for the treatment of patients with panic disorders. Washington, DC: American Psychiatric Association.
APA. 2015. Practice guideline for the treatment of patients with major depressive disorder. Washington, DC: American Psychiatric Association.
APA. 2017. Clinical practice guideline for the treatment of posttraumatic stress disorder (PTSD) in adults. Washington, DC: American Psychiatric Association.
Baldwin, D. S., I. M. Anderson, D. J. Nutt, C. Allgulander, B. Bandelow, J. A. den Boer, D. M. Christmas, S. Davies, N. Fineberg, N. Lidbetter, A. Malizia, P. McCrone, D. Nabarro, C. O’Neill, J. Scott, N. van der Wee, and H. U. Wittchen. 2014. Evidence-based pharmacologic treatment of anxiety disorders, post-traumatic stress disorder and obsessive–compulsive disorder: A revision of the 2005 guidelines from the British Association for Psychopharmacology. Journal of Psychopharmacology 28(5):403–439.
Bandelow, B., J. Zohar, E. Hollander, S. Kasper, H. J. Moller, J. Zohar, E. Hollander, S. Kasper, H. J. Moller, B. Bandelow, C. Allgulander, J. Ayuso-Gutierrez, D. S. Baldwin, R. Buenvicius, G. Cassano, N. Fineberg, L. Gabriels, I. Hindmarch, H. Kaiya, D. F. Klein, M. Lader, Y. Lecrubier, J. P. Lepine, M. R. Liebowitz, J. J. Lopez-Ibor, D. Marazziti, E. C. Miguel, K. S. Oh, M. Preter, R. Rupprecht, M. Sato, V. Starcevic, D. J. Stein, M. van Ameringen, and J. Vega. 2008. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the pharmacologic treatment of anxiety, obsessive–compulsive and post-traumatic stress disorders—First revision. World Journal of Biological Psychiatry 9(4):248–312.
Bandelow, B., L. Sher, R. Bunevicius, E. Hollander, S. Kasper, J. Zohar, and H. J. Moller. 2012. Guidelines for the pharmacologic treatment of anxiety disorders, obsessive–compulsive disorder and posttraumatic stress disorder in primary care. International Journal of Psychiatry in Clinical Practice 16(2):77–84.
CANMAT (Canadian Network for Mood and Anxiety Treatments). 2016. CANMAT 2016 clinical guidelines for the management of adults with major depressive disorder. Canadian Journal of Psychiatry 61(9):504–603.
Janardhan Reddy, Y. C., A. S. Sundar, J. C. Narayanaswamy, and S. B. Math. 2017. Clinical practice guidelines for obsessive–compulsive disorder. Indian Journal of Psychiatry 59(Suppl 1):S74–S90.
Katzman, M. A., P. Bleau, P. Blier, P. Chokka, K. Kjernisted, M. Van Ameringen, M. M. Antony, S. Bouchard, A. Brunet, M. Flament, S. Grigoriadis, S. Mendlowitz, K. O’Connor, K. Rabheru, P. M. Richter, M. Robichaud, and J. R. Walker. 2014. Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive–compulsive disorders. BMC Psychiatry 14(Suppl 1):S1.
Koran, L. M., G. L. Hanna, E. Hollander, G. Nestadt, and H. B. Simpson. 2007. Practice guideline for the treatment of patients with obsessive–compulsive disorder. American Journal of Psychiatry 164(7 Suppl):5–53.
NICE (National Institute for Health and Care Excellence). 2009. Depression in adults: Recognition and management. London, UK: National Institute for Health and Care Excellence.
Parikh, S. V., Z. V. Segal, S. Grigoriadis, A. V. Ravindran, S. H. Kennedy, R. W. Lam, and S. B. Patten. 2009. Canadian Network for Mood and Anxiety Treatments (CANMAT) clinical guidelines for the management of major depressive disorder in adults. II. Psychotherapy alone or in combination with antidepressant medication. Journal of Affective Disorders 117(Suppl 1):S15–S25.
VA/DoD (U.S. Department of Veterans Affairs and U.S. Department of Defense). 2016. VA/DoD clinical practice guideline for the management of major depressive disorder. Washington, DC: U.S. Department of Veterans Affairs.
VA/DoD. 2017. VA/DoD clinical practice guideline for the management of posttraumatic stress disorder and acute stress disorder. Washington, DC: U.S. Department of Veterans Affairs.
Yatham, L. N., S. H. Kennedy, S. V. Parikh, A. Schaffer, D. J. Bond, B. N. Frey, V. Sharma, B. I. Goldstein, S. Rej, S. Beaulieu, M. Alda, G. MacQueen, R. V. Milev, A. Ravindran, C. O’Donovan, D. McIntosh, R. W. Lam, G. Vazquez, F. Kapczinski, R. S. McIntyre, J. Kozicky, S. Kanba, B. Lafer, T. Suppes, J. R. Calabrese, E. Vieta, G. Malhi, R. M. Post, and M. Berk. 2018. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disorders 20(2):97–170.
This page intentionally left blank.












