
4
Crisis Standards of Care Application Across Sectors
Whereas some professionals have been working on this specific type of planning for more than a decade, others are just getting started. The key concepts of crisis standards of care (CSC) have permeated some sectors more than others, but real-life disasters and situations have continued to demonstrate the need for this type of scarce resource allocation planning to ensure that efforts are optimized to save lives. This chapter presents experiences from various levels and perspectives on CSC in action, including planning, response, and recovery phases. Case studies are discussed from the federal and state levels, as well as from the clinical and supply-chain settings, to highlight the diversity in issues that need to be considered in this multisectoral effort.
FEDERAL PLANNING AND RESPONSE
Speakers discussed CSC examples from the planning, response, and recovery phases across a variety of disaster types over the past several years.
Centers for Disease Control and Prevention Anthrax Guidance
Satish Pillai, acting director of the Division on Preparedness and Emerging Infections at the Centers for Disease Control and Prevention (CDC), described the efforts at CDC to develop clinical guidelines for catastrophic situations such as an anthrax event. Doing this at the federal level, he explained, allows for consideration of key principles that can be uniformly considered across jurisdictions. CDC can also assist state, local, and health
care partners through facilitated communication and lesson sharing in real time. Because most of the medical countermeasures (MCMs) for anthrax would come from the strategic national stockpile, CDC guidelines are needed to guide their use during an incident. In 2015, CDC developed a clinical framework during an anthrax mass-casualty incident, leveraging CSC principles for a variety of topics related to the evaluation and management of anthrax (e.g., diagnosis of anthrax meningitis; use of MCMs such as antimicrobials and antitoxin). In certain situations, for example, if resources were constrained in a crisis setting such that it might not be possible to perform lumbar puncture for all potential patients, the framework provides potential alternative options for the evaluation of meningitis. Similarly, considerations regarding dual and triple antimicrobial therapy and antitoxin therapy for systemic anthrax for conventional care settings as well as scenarios with potential shortages were presented.
These do not just apply during catastrophic events, Pillai noted, but are used on smaller problems, such as botulism outbreaks, which can still stretch health care and public health resources. CSC principles and planning considerations also apply to pandemic planning, including scenarios where there may be supply limitations for items such as respiratory protective devices.
Finally, Pillai offered a few unique challenges that CDC has encountered while developing the anthrax guidance, namely the lack of randomized control human trial data to inform the guidance, rather than the data informing the guidance from predominantly historical human clinical case reports and case series and animal studies. In addition, Pillai added, most U.S. clinicians have limited experience in managing these types of conditions, so rapid training efforts and provider education will be critical in an event.
Repatriation Following the 2010 Haiti Earthquake
Nicole Lurie, former Assistant Secretary for Preparedness and Response (ASPR), reiterated how instrumental this work has been and extended gratitude to all of those involved. She revisited the devastation of the Haiti earthquake in January 2010, where more than 3 million people were affected, and some estimate the death toll was as high as 300,000. Many key personnel from the government were killed, she said, and because so many buildings were destroyed, the first incident command-type meetings were held under a tree. People everywhere were being cared for haphazardly by numerous nongovernmental organizations, responders, and U.S. government providers through the USNS Comfort off the coast of the island, Lurie recalled. As time went on, she explained, responders began flying Haitian citizens to the United States from the Comfort to receive additional higher-level care. Pretty quickly, this began overwhelming usual care resources,
and the capacity to care for people in the states nearest to the island, such as Florida and Georgia. The National Disaster Medical System team was doing patient regulation, she said, but there was no clear source of payment for the care these patients were receiving so hospitals began getting nervous about reimbursement and the ability to provide so much free care. We realized there was a need to stem this flow of evacuated patients, she said, but in a fair and equitable way, Lurie said. Responders needed to use the guidelines of CSC—equity, rule of law, community engagement, and stewardship, she added.
To attempt this, they started to convene a committee, and fully engaged Haitian clinicians about who should be flown to the United States to receive care. Through this process, they learned the top reasons people were being flown back to the United States, and found they could partially address this problem by, instead, flying the right people to Haiti to fix devices so scans could be done in the country; they flew neurosurgeons and plastic surgeons to Haiti to conduct the needed care. She emphasized the principles of conserve, substitute, adapt, reuse, and reallocate in this process. Based on this experience, Lurie offered suggestions on future applications of CSC:
- Anticipate day-to-day applications and emergent applications.
- Recognize that many decisions have political implications.
- Identify proactive and anticipatory triggers (before systems become overwhelmed).
- Develop on-call support for difficult situations that can be leveraged in real time (such as having an ethicist on call).
Recovery in Puerto Rico Following Hurricane Maria
Jonathan White, director of the Recovery Division within the Office of the ASPR, shared his perspective of CSC within the context of recovery in Puerto Rico following Hurricane Maria in 2017. While we thought the real driver of the crisis would be a surge in the number of patients and impacts in acute care, he said, the challenges that really tested us were impacts in systems affecting the communities that patients were returning to. Increasingly, the need for altered standards of care was related to industrial infrastructure breakdowns and interdependencies of health care systems. The top two examples of this were power and transportation, he added. Power outage is the single foremost health security problem in the United States in the 21st century. We learned this critical lesson in New York City after Superstorm Sandy in 2012, he commented, again from Hurricane Irma in the islands, and from Hurricane Maria in Puerto Rico, and it was a defining lesson during Hurricane Harvey in Texas in 2017. Transportation is also critical, especially with regard to medical supplies, durable
medical equipment, and our transnational (sometimes even international) supply chain, making it difficult to get items where they are needed on an appropriate timeline. The long-term consequences of recovery will be the increasing role of market forces following a disaster, White argued. Health care will increasingly be available to the highest bidder as it becomes more constrained and circumstances more austere.
To demonstrate this challenge, he gave an example he encountered in Puerto Rico following Hurricane Maria, where two liquid oxygen plants that supplied the entire island lost power for a sustained period of time. Because they are not typically classified as critical infrastructure, they had not been accounted for in preparedness planning. Very few hospitals had oxygen generation capability, and while they were able to get standard containers to the island, there was trouble getting them from the ports to the hospitals where they were needed, especially those in the mountains. Because of this disruption, the secretary of health in Puerto Rico issued a letter authorizing hospitals to conserve oxygen. However, some hospitals had not yet used their emergency supply, and did not want to require clinicians to conserve oxygen when their individual system had not reached a crisis threshold demanding altered standards of care. He emphasized that this is a critical point—that CSC is driven by a globally dependent health care supply chain, but many people visualize the standards from an individual hospital-level perspective.
He concluded with thoughts on the recovery phase of disasters more broadly, and stressed that during this latter phase, the locus of altered standards may shift. This could include crisis standards of discharge planning from acute care, or crisis standards of subspecialties such as behavioral health or pediatrics. During the Camp Fire in California in 2018, entire skilled nursing facilities were destroyed, disrupting an important facet of subacute care in the community. With the addition of chronic intermittent power outages, it can be extremely difficult to decide which interventions are safe and when patients can reenter their communities following a disaster. This degradation or alteration of capacity or availability of health care creates altered standards of care—whether tacitly or implicitly. Communities where displaced populations relocate will be key sites of pressures, even though they are generally outside federal and state systems to surge, or supplementally fund medical services, so jurisdictions should take this into account.
STATE-LEVEL PLANNING
Though planning at the state level is variable across the country, two representatives from state health departments who have been involved in CSC planning for several years described their lessons and desires for further developing the frameworks and applications.
Minnesota
Judy Seaberg, director of the emergency preparedness and response division at the Minnesota Department of Health, shared her experience with the development of a CSC framework for the state. Initially, she said, we were planning for a potential pandemic. She showed the state’s timeline of activities since 2001, demonstrating the long-term effort this type of planning demands. She said they started out reviewing the current legal environment, then moved toward establishing an advisory team, which produced patient care strategies for scarce resource situations. Eventually, they were able to roll out toolkits and the framework in 2017, and from there began working on community engagement.
One of the key lessons learned from this experience, Seaberg noted, was that planning occurs in fits and starts. This is not a linear process, and considering the impacts of staff turnover, changing political leadership, and shifting priorities, this type of work often needs to take a backseat to other activities. She said that working with other sectors has been a challenge, as hospitals have not been able to incorporate it in a meaningful way because it is not seen as a priority by their executive leadership, and emergency medical services actors do not generally have these types of plans. As far as next steps, she said they are hoping to operationalize the framework at the facility level, which will probably be the most difficult stage. Partnering with their state hospital association, she said they have conducted interviews with emergency managers across the state and confirmed the assumption that most hospitals do not have this type of planning in place. They are also hoping to dedicate more time to define triggers and when a response flips from bottom up to top down. Moving forward, they will also be working closely with their health care coalitions to develop strong communication strategies to advance their state-wide effort.
Illinois
“With nearly 13 million people in Illinois, we knew that starting work on CSC would be a daunting task,” explained Winfred Rawls, director of the preparedness division at the Illinois Department of Health. Its statewide effort began around 2015, included the concept in hospital preparedness program plans, created ongoing subcommittees, and eventually resulted in a state-wide workshop in 2017 with 147 participants. This workshop resulted in the draft of an annex to Emergency Support Function #8 (ESF-8). This was then tested through tabletop exercises in 2018 and 2019, followed by the execution of a large functional exercise called Crimson Contagion in August 2019, with participants from across the state of Illinois.
Rawls remarked on the strengths of their efforts—mainly that all regions are now able to develop recommendations on how to conserve resources and assets in an emergency when needed. The various entities also demonstrated their ability to activate the processes and consider important ethical issues. All regions discussed multiple needs for their individual organizations to return to conventional care or baseline operations as well as multiple processes for getting staff to return to work. Several issues arose that needed improvement as well. He noted a lack of familiarity with their catastrophic incident response annex, a lack of CSC planning at the local level, lack of plans for regional fatality management, dependence on the state level for guidance, and lack of sufficient plans for the mental and behavioral health of responders and staff. He advocated for continuing to socialize the idea of CSC with hospital administration personnel and C-suite executives, as well as with physicians, to help the concept continue to percolate through health care systems. He also said that future applications should include translating the state CSC plan to the local levels and continuing to develop state fatality management response coordination and responsibilities.
CLINICAL SETTINGS
Colleen Ryan, professor of surgery at the Harvard Medical School, provided insight into the application of triage tables related to a mass-casualty event that results in overwhelming numbers of burn patients. Burn care remains one of the most complex and time-sensitive treatment interventions in medicine, she said, and an enormous quantity of limited and highly specialized resources, including workforce (~300 practicing burn surgeons in the United States and Canada), beds (~2,000 beds nationwide), and operating rooms, equipment, and supplies are required to meet the conventional standard of care in this field. She shared the novel first-time deployment of American Burn Association (ABA) actionable triage tables used during a fictional event exercise called “Operation Minute’s Notice.” This fictional exercise was held as a part of the ASPR MA Region 1 Partnership for Regional Health Disaster Response. The exercise took place in Massachusetts, and simulated a colored dust explosion at a family concert, resulting in a chain reaction that caused 1,500 injuries, with 450 critical burn/trauma patients (including children). For context, she said the ABA Northeast Burn Region has 27 burn centers and extends from Washington, DC, to Maine. The ABA Northeast Burn Region,1 one of five burn regions in the United States has a multi-year mean burn bed availability of 72 beds (range 48–107) (Conlon et al., 2019). They wanted to test exceeding the capacity of the region in the design of the exercise.
___________________
1 See ameriburn.org (accessed February 23, 2021).
As part of the regional disaster health response, following the explosion, they followed new protocols to activate a catastrophic access tactical center that included a burn clinical subject-matter expert (SME), one of several SMEs who advised the medical director who interacted with the local incident commander. The burn SME activated the ABA national disaster system response, which triggered a national (and Canadian) available burn bed count, deployment of media packages that had bystander care, just-in-time education, notifications to supply chains, and—importantly for this discussion—actual selection of severity matched triage tables and matching of patients based on altered standards of care (Kearns et al., 2020). Ryan explained that the new triage tables were tools to interpret existing mortality tables, developed from previous work based on the data from the National Burn Registry (Saffle et al., 2005; Taylor et al., 2014). The new triage tables were designed to follow the National Academies’ recommendations for CSC levels. The Conventional Burn Care Table (1) was designed for 50–200 patients nationwide and used age and burn size to select who would be treated at the available burn centers (see Figure 4-1).
A small group of patients (the white cells in the table) who were young and fairly stable or who had relatively small burns could be treated at home or another hospital, and another small group (gray cells) represented those who would be triaged to comfort care or secondary triage once more resources became available. The majority of patients (yellow cells) would be transferred to burn centers for care. The contingency table was designed for 100–500 patients, the crisis table for 500–2,000 patients, and a catastrophic table was created for scenarios with more than 2,000 patients, which would represent a complete breakdown overwhelming the system. As the tables moved away from conventional care, the white cells in the table representing those treated at other hospitals and the gray cells represent-
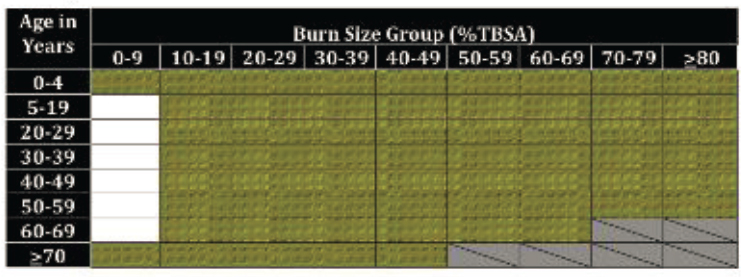
NOTE: Estimated 50–200 significant burn victims.
SOURCE: Colleen Ryan presentation, November 21, 2019.
ing those triaged to comfort care or secondary triage increased due to the increased burden. The decision for the selection of the table to be used was shared between the local burn SME and command and ABA’s leadership based on the current situational awareness provided.
Ryan said that for this fictional exercise, there were 217 burn patients in trauma centers that needed additional care. There were 67 burn beds available in the Northeast Region outside of Massachusetts, 9 of which were pediatric. So, their question was, how to best match the patients with available beds. They first assigned everyone to a cell based on age and burn size. Then, they began matching them in available hospitals but encountered challenges such as how to handle families with multiple patients, who ideally should not be split up. The age range that burn centers use for pediatrics, defined as 5–19 years old, also created a challenge, she said, because that is not how all hospitals identify pediatric patients. Once they were able to use tables to fill the available beds in the Northeast Region, they understood when it would be necessary to go to the national level. At the end of the allotted period of the exercise, 124 out of 217 patients met criteria from the selected Contingency Table 2 to be placed in the available 67 burn beds in the northeast, with 57 patients requiring transfer outside of the Northeast Region. Fifteen fictional patients were triaged to comfort care, and 78 were triaged to care outside of burn centers.
This was the first instance of actionable triage table deployment in a large-scale functional exercise, Ryan noted. Some of the lessons they took away from the experience were that they were deeply dependent on the quality of situational awareness available, and that diffusion of responsibility was really important for an event of this size. When the burn SME activated the national office, there was a joint decision of which table to use for a particular situation, so the accountability was on more than just one person. The value of ABA authority was really appreciated, she said. But there were some areas they needed to work on—most especially, she said, there was a desperate need for electronic automation to help categorize everyone. They did it manually and it took an inordinate amount of time. They also saw a need for just-in-time education, she said, as well as for ways to extend the reach of the burn center and improve prehospital care, especially for those patients in the white and gray areas who would not be treated at a specialized burn center. Finally, she said the austere guidelines that ABA had published were a valuable guide to their work (Jeng, 2017).
SUPPLY CHAIN
Nicolette Louissant, executive director of Healthcare Ready, provided insights from the supply-chain perspective following their response to Hurricane Harvey in 2017. As many would recall, the main consequence of
Hurricane Harvey in Houston, the third most populated county in the United States, was flooding caused by 5 days of continuous rainfall. Typically, in this 5-day window, resupply for hospitals and other health care facilities would happen at least once, she explained. With the rainfall came delays in medical supply-chain deliveries, so many organizations were forced to make decisions on which orders should be prioritized. Often, there was a mismatch between what was deemed to be a point of criticality from a supply-chain vendor perspective versus that of ESF-8 leaders. For example, a vendor may realize a shortage is imminent because they know the frequency of normal deliveries, but if a hospital has not reached a critical level of inventory yet, they have not reported any alerts. This made it difficult to ascertain the true level of urgency among hospitals in the area. Another challenge that was often encountered, she added, was that in states with home rule, moving products across counties is subject to the access and reentry policies at the county level. So, in addition to not knowing whether roads are safe to travel, there can be uncertainty about which access and reentry rules apply for road transport.
For future applications of CSC, Louissant suggested taking a more proactive posture during hurricane season and highlighted the different considerations for wind, versus water, events. She added, there is also a need in this space to continue identifying adequate substitutes and developing critical product lists. She mentioned that having supply-chain managers work directly with distributors and providers to understand what exactly is needed is really helpful, saying this type of communication can help alleviate the challenge of getting the necessary supplies the last mile in a crisis event.
DISCUSSION
To begin the discussion, McKinney noted that engagement of elected officials is one area that was not included in federal requirements for CSC, and asked presenters what the challenges are, and whether this was done during the responses to the Haiti earthquake and Hurricane Harvey. Lurie responded that all decisions made in this type of scenario will likely have important political implications. During the Haiti response, she explained, we heard from people in Florida and Georgia that hospitals were full, but at the same time had senators facilitating volunteer trips to Haiti, potentially resulting in more patients. She acknowledged the difficulty in engaging political leadership in a meaningful way before an event happens, given their limited bandwidth and competing priorities. But after an event, there is usually about a 3-month window where you do have their attention and can get some buy-in. That was the impetus for starting the ASPR Technical Resources, Assistance Center, and Information Exchange program,
also known as TRACIE, she added. White said that in any disaster there is a personal disaster, followed by a political disaster, often followed by a bureaucratic disaster. Local and state officials play a critical role in convening the stakeholders needed in something that spans so many sectors, he explained, adding that industry also has a critical role to play, because they are responsible for the delivery of health care in nearly all situations.
Questions also emerged related to the infrastructure challenges described in Puerto Rico. One participant said that after doing a gap analysis of health care on the island, he found water and Internet access to be clear deficits for health care, in addition to power and transportation. Following electronic health record requirements, most of that information is stored in “the cloud,” and even 6 weeks after the storm, hospitals still did not have Internet access. He asked if a consideration for CSC would be having mirrored files locally or going back to paper records. White replied that they are focusing on a hub-and-spoke model for hospital readiness on the island. They are currently looking at building capacity for hyperpurified water to ensure dialysis capacity can be maintained. Another pillar of their mission is examining communication more comprehensively, saying that in the response effort they learned that there was not a comprehensive set of hospital addresses, and the physical locations of all of the hospitals were not previously mapped, making it difficult to deliver even simple messages. These are a few examples of how we were trying to support our territory partners to create a more sustainable health care infrastructure for Puerto Rico, he noted.
Matthew Wynia, director of the Center for Bioethics and Humanities at the University of Colorado, asked about an incident regarding conservation of oxygen at area hospitals in Puerto Rico, where hospitals were asked to conserve due to reduced production even if they were not experiencing a direct shortage themselves, saying he could see a strong argument on either side for complying or not. On the one hand, initiating severe conservation efforts that might reduce the quality of care a site is able to provide, before the conservation is truly needed there, runs afoul of the principle of proportionality, which calls for rationing only when doing so is truly necessary. But on the other hand, failing to implement conservation efforts in advance of a severe shortage might result in the shortage coming sooner and being more severe than it otherwise might have been. Wynia noted that this really highlights a disconnect in their algorithm: At the territory government level, we saw the island as a system, but that was different from how the hospital saw things at an individual level. The plan did not recognize that the decisions being made at the territory level and at the hospital leadership level were not done through the same lens, which highlights some questions in the decision-making methodology. Hick added that this is a great case study in how CSC gets used. We often think of it as being binary decisions,
he said, but in this case the initial letter was just authorizing and recommending conservation of oxygen, which left a lot of latitude for how clinical decision makers and hospital executives interpreted it. Ros Schulman, American Hospital Association, shared a similar story from Puerto Rico related to conservation of resources. She said they experienced a situation with drug manufacturers who made small-volume parenteral solutions, but that went offline for a while due to power issues, resulting in a drug shortage on the island. The American Society of Health-System Pharmacists quickly developed some guidance and posted it for the nation’s hospitals to follow (ASHP, 2017)—just one example of standing guidance that can be adapted for just-in-time needs.
Some insights emerged from the Ebola outbreak of 2014–2015, related to both caregiver fatigue and language and terminology. When asked how to balance the need for staff to work during an emergency while also giving them choices in case they are fearful for themselves, Lurie highlighted the importance of creating an environment where people felt safe when treating those types of patients—saying that when that occurs it is easier to find people willing to volunteer. White added that one of the basic CSC principles is to adapt—sometimes on the fly. He said it is our responsibility to provide the proper tools and training to stem that kind of fear. Similarly around language, a participant asked about different terminology being used, saying that CSC has been established, but now increasingly one hears the use of “altered standards of care.” Does this change matter, she asked? Or does it mean something different? Lurie responded that often we have a habit of using different words to mean the same thing, and also encountered this difficulty during the Ebola response. She explained that there was never a defined standard of care, so even though they were operating in countries that have austere health systems, nongovernmental organizations who had the capability were not conducting routine testing or using intravenous fluids because it was not clear what the accepted standard should be. She said it took a long time for the World Health Organization and others to put out guidance on this, but regardless of what we call it moving forward, we need normative guidance on what the expected standard of care is in these types of events.
Finally, McKinney brought up the issue of equity. When we think about how catastrophic these issues are becoming, she said, we are always thinking about the medically vulnerable, but what about populations that have historically been marginalized and vulnerable in other ways? How can we maintain a key focus on this issue of equity, she asked? Pillai responded that in terms of the anthrax clinical guidance, CDC sought to highlight populations that could be more vulnerable than others in an anthrax mass-casualty event, thinking strategically about the unique guidance needs for those populations. Lurie emphasized that all of this work needs to be done
through an equity lens. When it comes to CSC, she said, it is often easy to overlook the fact that populations most in need may not be immediately visible. Care is often available to the highest bidder, not those who need it most. Louissant reinforced McKinney’s point, saying there are indeed two lenses—one is populations who may be medically fragile, and another encompasses those who have been systemically oppressed and disadvantaged. We need to have these community conversations at the right level to think about how to provide the most equitable care at the time of a crisis, she pleaded. From the specific viewpoint of supply chain and how private companies play a role, stakeholders should be thinking about opportunities to consider workforce and community education in understanding and crafting an equitable response.












