
2
Airborne Hazards in Southwest Asia
An airborne hazard is any chemical, physical, or biological agent in the air that has a potential to cause harm. There are numerous airborne hazards that military personnel may have experienced when deployed to Southwest Asia, including regional environmental exposures, such as air pollution from dusts, and local point and area sources, such as traffic, waste management, or local industries. Exposures related to military operations are also contributors, such as exhaust from heaters, military vehicles, and aircraft and smoke from structural fires, blasts, burning oil wells, and burn pits (VA, 2018). The exposures from military operations differ by conflict and vary by location and over time; for example, veterans of the post-9/11 conflicts are more likely to have been exposed to burn pits, whereas the 1990–1991 Gulf War veterans are more likely to have been exposed to smoke from oil-well fires. Additionally, some military personnel have occupations, job duties, or tasks that expose them to a variety of vapors, gases, dusts, and fumes. All these airborne hazards meet the definition of “hazard” in that they have the potential to cause harm and may influence the health of military personnel. The definition of “hazard” differs from “risk,” which is the probability that the hazard will cause harm and is a function of the extent of exposure (NRC, 1996).
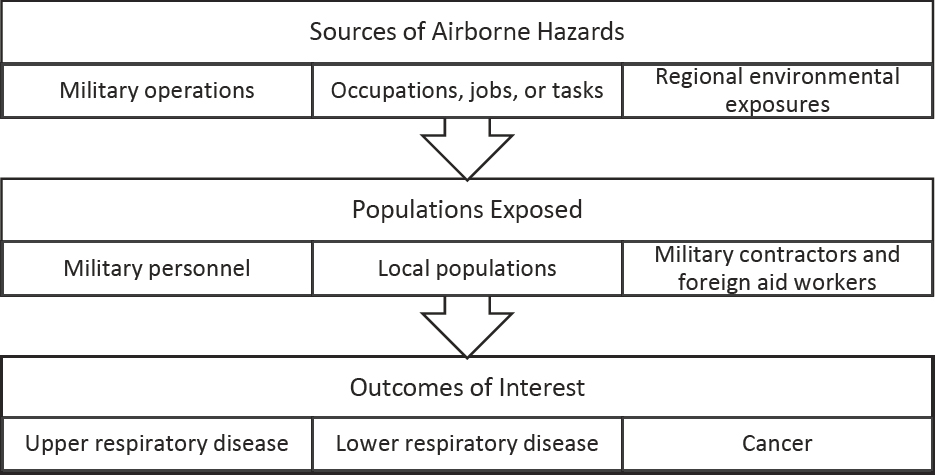
The Statement of Task charges the committee to “comprehensively review, evaluate, and summarize the available scientific and medical literature regarding the respiratory health effects of exposure to airborne hazards encountered during service in the Southwest Asia theater of military operations.” Exposures from the regional environment in Southwest Asia—and those that occur specifically from military operations—are thus the most relevant to the committee’s charge. However, military occupational exposures may compound the effects of other environmental and military exposures. Figure 2-1 provides a framework of how complex exposures from multiple sources and environments may influence the health of military personnel.
This chapter characterizes and describes airborne hazards related to military operations, military occupations, and regional environmental exposures that might be encountered by personnel deployed to the Southwest Asia theater.1 These hazards are listed in Box 2-1.
The following sections provide information on the levels of the hazards from military reports or the published literature, and where applicable they provide a summary of studies that have aimed to characterize the hazards using toxicity studies. The committee took a broad view of what might constitute an in-theater airborne hazard but notes that information on some these—occupational exposures, for example—is lacking.2
___________________
1 Cigarette smoking, an airborne hazard that has been shown to be associated with deployment (Krefft et al., 2015), is addressed in Chapters 4 and 5.
2 Studies of the health effects of some of the airborne exposures noted in Table 2-1 are in some cases available in the (non-military) occupational health literature, as are Material Safety Data Sheets that summarize the state of toxicologic and epidemiologic knowledge on these exposures.
The chapter ends with a brief discussion of factors that may increase the vulnerability of military personnel to airborne exposures while in theater and a description of how the committee approached the task of considering the respiratory health effects of these exposures.
EXPOSURES ASSOCIATED WITH MILITARY OPERATIONS IN THE SOUTHWEST ASIA THEATER
Military operations generate airborne hazards. While these operations are in some respects similar to those encountered in some occupational settings, military personnel are likely to be exposed to hazards not just at work but also at leisure and when sleeping due to the circumscribed realities of deployment to a location such as the Southwest Asia theater. This section provides an overview of some the primary airborne exposures of concern.
Open Burn Pits
One source of combustion-related air pollution that is central to the charge of the committee is the military burn pits used for open-air waste burning. The military has long used burn pits when other waste-disposal options have not been available. Technologic advances and changes in military practices in recent conflicts mean that items are being burned—plastic bottles and electronics, for example—that present new health risks (IOM, 2011). Burn pits were the primary solid-waste management solution in Afghanistan and Iraq from the beginning of the conflicts in 2001 and 2003, respectively. However, their use was restricted by law in 2009 (Public Law [PL] 111-84, § 317). By the end of 2010 their use in Iraq had been phased out, but it continues in Afghanistan. The Department of Defense (DoD) reported that as of March 2019 there was still one U.S.-operated open burn pit in Afghanistan and eight more in other DoD operations locations (DoD, 2019). In addition, that report indicated that “in countries such (as) Iraq, Syria, or Afghanistan it is common practice to burn waste in open pits. Our host nation partners dispose of waste for us; however, there are many cases where trash is burned just outside the gate by contractors” (DoD, 2019). DoD Instruction 4715.19 governs the circumstances under which a burn pit may be operated (DoD, 2018).
DoD estimates that an average of 8–10 lb of waste is generated each day by each person in theater. On the basis of the average populations of large bases in Iraq and Afghanistan (those with more than 1,000 personnel), an average of about 30–42 tons of solid waste per day might be produced on a base. Joint Base Balad, with a population that sometimes surpassed 25,000, including U.S. troops, host-nation soldiers, coalition troops, civilians, and contractors, burned perhaps 100–200 tons of waste per day in 2007. In 2009, three incinerators were operational at Joint Base Balad and burned about 10 tons of waste per day in the pit; the burn pit ceased operation on October 1, 2009. A 2010 Army Institute of Public Health study of burn pits in Iraq and Afghanistan reported that large bases burned waste that consisted generally of 5–6% plastics, 6–7% wood, 3–4% miscellaneous non-combustibles, 1–2% metals, and 81–84% combustible materials. While the mixture of materials that enter a burn pit waste stream remains complex and is not consistent day to day, efforts have been made to reduce or eliminate wastes “covered” under PL 113-66, § 314, such as
tires; treated wood; batteries; plastics …; munitions and explosives …; compressed gas cylinders …; fuel containers …; aerosol cans; polychlorinated biphenyls; petroleum, oils, and lubricants, other than waste fuel for initial combustion); asbestos; mercury; and foam tent material. (PL 113-66, § 314)
In response to complaints of odor, poor visibility, and health effects attributed to burn pit emissions, the U.S. Army Public Health Command and the Air Force Institute for Operational Health conducted ambient-air sampling and screening health-risk assessments of burn pit exposures at Joint Base Balad in 2007 and again in 2009. The assessments were designed to detect potentially harmful inhalation exposures of personnel at Joint Base Balad to chemicals expected to be released by the burn pit.
A 2011 review of air monitoring efforts at Joint Base Balad conducted by the Institute of Medicine (IOM) found that:
- Particulate matter (PM) concentrations in ambient air were on average higher than U.S. pollution standards. The air samples taken at Joint Base Balad in 2007 and 2009 were analyzed for PM10. The average of the 90 PM10 measurements at Joint Base Balad in 2007 was 126 µg/m3 (range 2–535 µg/m3); the 24-hour National Ambient Air Quality Standards (NAAQS) limit of 150 µg/m3 for PM10 was exceeded 26 out of 90 times at the three measurement locations. In 2009 the average of the 51 PM10 measurements (excluding those that the 2011 committee considered unusable; see IOM, 2011, Appendix B) was 709 µg/m3 (range 104–9,576 µg/m3), and NAAQS was exceeded for 49 of the 51 samples. The three highest measured PM10 values (9,576, 2,481, and 1,951 µg/m3) occurred on the same day during a sandstorm (USAPHC, 2010). The committee concluded that the measured PM was primarily from local sources (vehicle traffic, aircraft emissions) and regional sources (long-range anthropogenic sources, dust storms), although the burn pit likely made some contribution.
- Polychlorinated dibenzo-p-dioxins and dibenzo-p-furans (PCDD/Fs) were detected at low concentrations. Although the levels of species associated with greater toxicity were higher in these samples than in the air generally found in the United States or urban environments worldwide, they were lower than levels associated with some non-military sources present in the theater.
- Concentrations of volatile organic compounds (VOCs) and polycyclic aromatic hydrocarbons (PAHs) were similar to those reported in major urban areas outside the United States, with the major sources being regional background, ground transportation, stationary power generation, and the airport at Joint Base Balad (IOM, 2011).
Subsequent studies also noted the contribution of the Joint Base Balad burn pit to PCDD/Fs on base as well as the important role of other sources of emissions, including the airfield, as the primary source of PAHs. Other important contributors to PAH levels were aircraft, vehicle emissions, space heaters, and diesel generators (Masiol et al., 2016a,b).
The Joint Base Balad observations were limited to the pollutants that were targeted by DoD. Thus, the available monitoring data provide information on exposures to the major types of constituents from burn pit emissions, but they lack information on other chemicals that were likely present as well as on the exposure variability among burn pits and over time (IOM, 2011; NASEM, 2017a). Further details on the strengths and weaknesses of the pollutant measurements and exposure assessment are available from these publications.
Other data collected as part of a monitoring program for a solid waste disposal facility at the Bagram Airfield in Afghanistan underline the variability of exposures associated with burn pits (Blasch et al., 2016). That facility operated a burn pit from 2005 to 2012. Investigators collected breathing zone samples, unlike the case with Joint Base Balad, but only PM and VOCs were studied. Sampling was conducted at four security locations (up to 125 meters from the burn pit) and a control location (4 km from the burn pit) during 30 12-hour shifts. Among the VOCs detected, only Acrolein exceeded the 1-year military exposure guideline, but benzene was detected in all samples. The range of PM concentrations varied considerably in association with airfield activity (vegetation removal, demining, road construction, vehicle traffic, industrial activity, and air traffic). The highest recorded concentrations of environmental PM2.5 (615 µg/m3) occurred at the solid waste disposal facility where the burn pit and incinerators were located. High PM2.5 and PM10 concentrations were also noted at the bazaar, a highly populated site with unpaved roads and considerable vehicular traffic. The investigators concluded that “[t]he diversity of results support the concept of a complex environment with multiple polluting sources and changing meteorological and operational conditions” (Blasch et al., 2016, p. S38). The committee responsible for the 2011 report did not identify other systematic sampling data on in-theater burn pit emissions.
Toxicity Studies of Open Burn Pits
Scientists at Wright-Patterson Air Force Base in Dayton, Ohio, have conducted several experimental animal studies to evaluate the toxicity of burn pits compared with the PM collected in 2013 by the U.S. Army Corps of Engineers from Camp Slayer (in Camp Victory), Iraq, and a soil sample from an undisturbed area. The burn pit exposures were from a simulated burn pit that is designed to reflect solid waste combusted in-theater as based on the U.S. Army
Central Area of Responsibility contingency base waste stream analysis (USALIA, 2013). The burned waste included cardboard, food waste, mixed paper, non-combustibles, plastics, textiles, wood, and miscellaneous wastes. Studies have evaluated the impact of burn pits on epigenetic changes, proteomic changes, and metabolomic changes as well as the impacts on the lung microbiome using the same set of exposures and experimental groups (Mauzy, 2019).
In an investigation of epigenetic changes, the results of which were presented to the committee at its October 2019 meeting, Air Force Research Laboratory researchers used four groups of rats, one of which was an unexposed control group, for the 127-day study (Mauzy, 2019). Rats in the three other groups were exposed to Southwest Asia sand only (20 days), sand (20 days) followed by burn pit emissions (5 days), or burn pit emissions only (5 days). All three exposure groups were also exposed to sand from days 67 to 127. Blood, urine, bronchiolar aspiration fluid, and tissue samples were collected from the animals at various time increments based on the endpoints of interest. Burn pit emission exposures were found to initiate molecular host responses much more strongly than sand inhalation exposures. Exposure to the 5 days of burn pit emissions had a greater impact on epigenomic markers than 20 days of sand exposure. The researchers observed that these acute exposures initiated strong host responses—as would also be expected from chronic exposures—and the results indicated a need for concern with even shorter exposures. The sand exposure response was stronger at 90 days post-exposure than at 1 day post-exposure. Based on this work, host response to emissions exposure is relatively fast, whereas host response to sand inhalation is slower. The chronically exposed groups showed more epigenetic changes than those exposed acutely. The data did not indicate any additive effect of sand and burn pit emission exposures. There were sets of differentially expressed micro RNAs (miRNAs) identified in lung tissue. Two chemical species were found in both Affymetrix and sequence-based discovery data sets, both of which are seen in pathways leading to lung cancer or disease (Mauzy, 2019).
The study of proteomic changes again used four groups of rats: a control and three exposure groups: Southwest Asia sand, burn pit emissions, and burn pit emissions followed by sand. Tissues and blood samples were collected from the animals at baseline (both at the start of the study and prior to the burn pit exposure) and at days 4, 30, and 90 after the exposure periods ended. Samples were analyzed using the SEQUEST algorithm in the Proteome Discoverer 2.2 software suite (ThermoFisher, San Jose, California). In the sand-only group, seven burn pit emissions-based markers and four sand-based markers were observed. In the group exposed to sand and emissions, 24 sand and emissions markers were observed but only in the combination exposure group, which may indicate an additive effect. In the burn pit emissions-only group, 20 other markers were found that were not seen in the combination exposure set (Mauzy, 2019).
The metabolomic study evaluated whether changes in urinary metabolite profiles would correlate with exposures and adverse health effects. Again, the researchers used four groups of rats: a control, Southwest Asia sand, burn pit emissions, and burn pit emissions followed by sand. Animals were continuously monitored for 90 days following the exposure period. A cohort of rats provided urine samples at specific times during the 127-day protocol at 12 specific time points. The largest observed effect on urinary metabolite profiles was time, in both the control group and the experimental exposure groups. The greatest difference in urine metabolite profiles occurred during the exposure timeframe (days 1–38) and the least during the recovery period (days 39–97) (DelRaso et al., 2018).
In the microbiome study, the aim was to evaluate whether the burn pit emissions and sand exposures resulted in changes to the lung microbiome. This study also used four groups of rats: a control, Southwest Asia sand, burn pit emissions, and burn pit emissions followed by sand. Following exposure, the researchers removed bronchoalveolar lavage from the left lung of each rat. DNA was extracted from the samples and sequenced to evaluate the diversity of the lung microbiome. The two groups with emissions exposure had the most differences in microbial diversity compared with the control group (Mauzy, 2019).
Taken together, these toxicity studies provide some evidence that exposure to burn pits may have different toxicologic effects than exposure to other airborne hazards in Southwest Asia. These experiments have some advantages over observational studies because the investigators know the nature and temporal pattern of the exposure. However, the outcomes ascertained are mechanistic and not clinically relevant. Additionally, the doses used in the studies may be higher than those experienced by military personnel in theater, and differences in the deposition and clearance of particulates from rat and human lungs (Schlesinger, 1988) affect the interpretation of their results.
Emissions from the 2003 Al-Mishraq Sulfur Plant Fire
On June 24, 2003, U.S. military field reports indicated that a large fire had started at the state-run Al-Mishraq Sulfur Plant near Mosul, Iraq. The fire burned continuously for almost 1 month, until approximately July 21, 2003, and emitted dense clouds of sulfur dioxide, a byproduct of the combustion of elemental sulfur piles. Hydrogen sulfide (H2S) was also released. Calculations from the Earth Probe Total Ozone Mapping Spectrometer, a National Aeronautics and Space Administration satellite-based instrument, estimated that the amount of SO2 released averaged 21 kilotons/day over the time that the facility burned—a daily total similar to the amount of SO2 emitted from a highly polluting plant in the United States in 1 year. At the time of this incident, thousands of U.S. military personnel were deployed to the area in support of Operation Iraqi Freedom. Troops in the area were called on to assist local Iraqis fighting the fire, others assisted in evacuating civilians from local towns nearby, and others continued their military missions and transport operations in the area (Baird et al., 2012).
Fuels
Several petroleum-derived fuels were present in Southwest Asia during U.S. military operations, including gasoline, kerosene, diesel, and jet propellant fuels (JP-4, JP-5, and JP-8). These fuels powered aircraft, ground vehicles, tent heaters, and cooking stoves. They were also used for less conventional purposes, such as suppressing sand and dust aerosolization, cleaning equipment, and burning trash. Other exposures include diesel exhaust from motor pools and diesel-powered vehicles and emissions from the kerosene heaters used in sleeping quarters for warmth. There are anecdotal reports of personnel sleeping in or on running vehicles when other sources of warmth were not available. Deployed military personnel may also experience exposure to exhaust from fixed- and rotary-wing flight-line activities and to complex airborne mixtures, such as those associated with a burn pit.
Military personnel serving in the theater could thus have been exposed to the uncombusted fuels, the combustion products from the burning of those fuels, or a combination of uncombusted and combusted materials. No studies evaluating fuel exposures or their associated combustion byproducts in theater were identified, although, based on the reported widespread use, these are likely a significant source of exposures to airborne hazards in theater (Masiol et al., 2016a).
Oil-Well Fires
Oil-well fires and the smoke they emitted were the most visually dramatic environmental event of the 1990–1991 Gulf War (IOM, 2005). A DoD online publication reported that smoke from the burning oil wells was first visible from satellite images as early as February 8, 1991 (Rostker, 2000). Satellite images showed that the number of oil fires peaked during February 22–24, 1991. In total, Iraqi forces ignited or damaged more than 750 of Kuwait’s 943 oil wells distributed among eight fields. The first fires were extinguished in early April 1991, with the last well capped on November 6, 1991. During this period, various sources estimated that the damaged well heads had released approximately 4–6 million barrels of crude oil and 70–100 million cubic meters of natural gas per day. The burning crude oil smoke was a mixture of heated, potentially noxious gases and coated carbon particles, including a wide range of combustion products: carbon dioxide (CO2) and carbon monoxide (CO), sulfur dioxide (SO2), oxides of nitrogen (NOx), VOCs, hydrogen sulfide (H2S), ozone (O3), various PAHs, and acid aerosols. The smoke also contained other components that are common impurities in crude oil, such as vanadium, iron, nickel, aluminum, beryllium, cadmium, calcium, chromium, arsenic, silicon, zinc, and lead (Rostker, 2000).
No systematic monitoring of the airborne hazards from the fires occurred until May 1991, when several independent teams from multiple U.S. agencies (including the Army Public Health Agency and the Environmental Protection Agency [EPA]) and international agencies went into Kuwait to monitor the ambient air contamination due to oil-well fire emissions (Spektor, 1998). The monitoring data indicate that concentrations of NOx, CO, SO2, H2S, other pollutant gases, and PAHs did not exceed those in the air of a typical U.S. industrial city (IOM, 2006). PAH concentrations in the samples were low (PAC, 1996). High concentrations of PM from sand and soot were
often observed at multiple monitoring sites; an estimated 20,000 tons of soot, or fine-particle mass, was generated by the fires (Thomas et al., 2000) and made up about 23% of the PM in the Persian Gulf, often at concentrations twice those considered acceptable (Rostker, 2000).
The potential exposures of troops to smoke and combustion products from the oil-well fires were also modeled (Draxler et al., 1994). Daily and seasonal normalized air concentrations due to emissions from the oil-well fires were computed using a modified Lagrangian transport, dispersion, and deposition model for the period of February through October 1991. The highest normalized concentrations were located near the coast between Kuwait and Qatar, with peak values moving farther west and inland with each season (i.e., the smoke and combustion products moved from over the Gulf in the spring to the west over the Saudi Peninsula by autumn).
Nerve Agents
Another hazard specific to the 1990–1991 Gulf War was exposure to nerve agents following the demolition of a large storage complex at Khamisiyah, Iraq, which occurred during a cease-fire period in March 1991. The total amount released, according to estimates, was 371 kg of sarin and cyclosarin combined (Winkenwerder, 2002). U.S. troops performing the demolitions were unaware of the presence of nerve agents, and no air monitoring was conducted at the time of the demolition. Exposure models estimated that the exposures were low, and there were no medical reports at the time of any cases exhibiting signs or symptoms of exposure to sarin or acute cholinergic syndrome (IOM, 2004).
Depleted Uranium
Depleted uranium (DU) is a weakly radioactive, chemically toxic heavy metal derived from natural uranium which is used by the U.S. military for munitions and for armor on some tanks. DU is well suited as a munition because of its high density and “self-sharpening” nature, both of which help it to penetrate armor. Its high density also makes DU an effective shield. DU has been used by all branches of the U.S. military since the 1980s and was used on the battlefield in the 1990–1991 Gulf War and the post-9/11 conflicts (NRC, 2008).
Concern about the adverse health effects on survivors of combat exposure to DU arose in response to “friendly-fire” incidents in which U.S. vehicles were accidentally struck with DU rounds. In the Gulf War, about 115 U.S. soldiers in or on 6 Abrams tanks and 14 Bradley fighting vehicles were caught in friendly-fire events that involved the use of large-caliber munitions containing DU penetrators. Some of the soldiers were injured by DU shrapnel. Most of the large metal embedded fragments in the surviving 104 soldiers were removed during treatment for their injuries. However, many small fragments were left embedded in their muscle tissue because their removal might lead to other health complications (NRC, 2008).
When used as an antitank armor-piercing munition, a DU penetrator can create an airborne spray of uranium with particles of various sizes that can be inhaled by the tank crew or escape into the environment (NRC, 2008). Studies in uranium miners found associations between exposure to uranium and respiratory diseases, including pneumoconiosis, chronic obstructive pulmonary disease, pulmonary fibrosis, and tuberculosis (Hines et al., 2013). However, the committee responsible for Gulf War and Health: Updated Literature Review of Depleted Uranium concluded that there was inadequate or insufficient evidence to determine whether exposure to DU is associated with long-term health problems (IOM, 2008).
REGIONAL ENVIRONMENTAL EXPOSURES
The Southwest Asia regional climate is hot and arid, which exposes military personnel to intense heat and sunlight during the day, while nights are cool. Pressure gradients cause frequent and severe dust storms in the region, and the relative lack of vegetation permits large areas of loose soil to be moved great distances (Goudie, 2014). Variations in climatic and vegetation conditions are associated with changes in dust levels in arid regions (Li et al., 2020). In some instances, winds are high enough to cause larger dust and sand particles to impact and
eject smaller particles into the air via a process called “saltation,”3 which can lead to the large-scale transport of particulate matter across several hundred miles (Jayaratne et al., 2011). Wildfires, in which forests, crops, and brush can catch fire and which result from natural drought and human activity, also contribute to air pollution. And Southwest Asia is becoming increasingly industrialized, with more vehicle traffic, and the only country within the theater of operations with air quality standards is Saudi Arabia. The region is resource rich, and thus its primary industries are extractive, such as mining and oil and gas development, which affects air quality (Tsiouri et al., 2015).
Toxicity of Air Pollution Exposures
Traffic-related air pollution has been associated with a variety of respiratory effects. In 2010, a panel of the Health Effects Institute reviewed more than 700 studies on the health effects of traffic-related air pollution and concluded that the evidence is sufficient to support a causal relationship between exposure to traffic-related air pollution and exacerbation of asthma. It also found suggestive evidence of a causal relationship between traffic-related air pollution and both nonasthma respiratory symptoms and impaired lung function (HEI, 2010).
Exposures to emissions from diesel engines and their potential impact on human health have also been of concern. Epidemiologic and toxicologic studies have reported associations between short- and long-term exposures to diesel exhaust and its components and a range of acute and chronic adverse health effects, including lung cancer. In 2012 the International Agency for Research on Cancer reviewed the body of scientific evidence on the carcinogenicity of diesel exhaust and concluded that there was sufficient evidence in humans and experimental animals to classify diesel exhaust as a Group 1 carcinogen (carcinogenic to humans) (Benbrahim-Tallaa et al., 2012).
Particulate Matter
Particulate matter is characterized by its physical size and chemical properties and includes total suspended particles (TSP), inhalable particles with aerodynamic diameters less than 10 micrometers (PM10), coarse particles with aerodynamic diameter between 10 and 2.5 micrometers (PM10–2.5), and fine inhalable particles with diameters less than 2.5 micrometers (PM2.5). In Southwest Asia, PM sources may include dust storms, dust from motor-vehicle disturbance of the desert floor, agricultural activities, lead–zinc smelters, battery-processing facilities, refineries, power stations, fertilizer plants, and emissions from vehicles (UNEP, 2007). Dust storms may carry large amounts of PM great distances, and the chemical composition can change during transport (Mori et al., 2003). The long-range transport of desert dusts significantly affects the air-quality over large regions. Dust transport and anthropogenic emission sources (petrochemical and power plants and industrial operations) have affected the levels of TSP throughout Southwest Asia and neighboring countries, and dust storms increase the concentrations of PM10 and PM2.5 (Querol et al., 2019).
There have been several efforts to characterize ambient PM levels in Southwest Asia. These studies vary in a number of ways, particularly in terms of the exposure assessment methods used and the time, location, and area. In general, the studies have found that PM exposures in Southwest Asia appear higher than those generally observed in the United States and that they often exceed the NAAQS for PM2.5 (12 µg/m3 [annual average]; 35 µg/m3 [24-hour average]) and PM10 150 µg/m3 (24-hour average not to exceed more than once per year over 3 years) (see Table 2-1).
Masri et al. (2017b) published PM2.5 exposure estimates that have the most coverage to date in terms of time and geography throughout the region. They determined the relationship between daily airport visual range measurements and PM2.5 samples collected during 2004–2005 (Brown et al., 2008) to develop a PM2.5 prediction model that could be applied more generally to airport visual range data. In their application, the prediction model was used on location-specific visibility data at 104 regional sites in Iraq, Afghanistan, United Arab Emirates, Kuwait, Djibouti, and Qatar during the period 2000–2012 to estimate monthly average PM2.5 concentrations. Predicted
___________________
3 “Saltation is the movement of large particles (about 100–500 µm) that bounce a few centimeters above the surface and then fall back down, thereby bombarding the surface; upon impact, they dislodge smaller particles (less than 100 µm) from the surface, which can be entrained in the prevailing airflow” (NASEM, 2017b, p. 35).
TABLE 2-1 Summary of Studies That Measured Particulate Matter in Southwest Asia
| Reference | Sample Type | Location | Year | PM2.5 µg/m3 Mean (SD) | PM10 µg/m3 Mean (SD) | TSP µg/m3 Mean (SD) |
|---|---|---|---|---|---|---|
| Brown et al. (2008) | 24-hr samples, Rupprecht and Patashnick Co., Inc., Model 3500 ChemCombs speciation samplers | Northern Kuwait | 2004–2005 | 30.8 (16.6) | 65.8 (37.0) | |
| Kuwait City | 2004–2005 | 37.6 (17.3) | 92.8 (38.9) | |||
| Southern Kuwait | 2004–2005 | 36.5 (18.2) | 90.4 (52.1) | |||
| Engelbrecht et al. (2008) | 24-hr active air sampling with Airmetrics MiniVol particulate sampler, one each for TSP, PM10, and PM2.5 using a 1-in-6 day sampling schedule across the sites | Djibouti | 2006–2007 | 33 | 72 | 94 |
| Bagram, Afghanistan | 2006–2007 | 40 | 120 | 174 | ||
| Khowst, Afghanistan | 2006–2007 | 75 | 126 | 185 | ||
| Qatar | 2006–2007 | 67 | 166 | 282 | ||
| United Arab Emirates | 2006–2007 | 52 | 140 | 196 | ||
| Balad, Iraq | 2006–2007 | 56 | 183 | 242 | ||
| Baghdad, Iraq | 2006–2007 | 103 | 250 | 371 | ||
| Tallil, Iraq | 2006–2007 | 65 | 303 | 411 | ||
| Tikrit, Iraq | 2006–2007 | 114 | 300 | 628 | ||
| Taji, Iraq | 2006–2007 | 81 | 213 | 348 | ||
| Al Asad, Iraq | 2006–2007 | 38 | 96 | 142 | ||
| Northern Kuwait | 2006–2007 | 67 | 211 | 416 | ||
| Central Kuwait | 2006–2007 | 117 | 298 | 352 | ||
| Coastal Kuwait | 2006–2007 | 60 | 180 | 264 | ||
| Southern Kuwait | 2006–2007 | 62 | 199 | 290 | ||
| Javed et al. (2019) | 24-hr PM2.5 and PM10 samples were collected on pre-weighed, polypropylene-ring-supported 2-µm pore-size Teflon 37 mm filters, using a low-volume air-sampling pump | One site in Doha, Qatar | May to December 2015 | 40 (15) | 145 (70) | |
| Lim et al. (2018) | PM samples were collected onto Teflon filters (GelmanTeflo, 37-mm, 0.2-µm pore-size) using PM2.5 and PM10 Harvard impactors connected to calibrated vacuum pumps, at a rate of 10.0 L/min | Jeddah, Saudi Arabia | 2011–2012 | 21.9 (11.6) | 107.8 (72.6) | |
| Masri et al. (2017a) | Monthly predicted PM2.5 using airport visual range measurement calibrated and aerosol optical depth | 17,000 km2 region surrounding Joint Base Balad and Baghdad, Iraq | 2005–2008 | 45.4 | ||
| Masri et al. (2017b) | Compared daily airport visual range measurements with PM2.5 samples collected from 2004–2005 develop a model to predict monthly PM2.5 using ground-level airport visual range data | 104 sites in Iraq, Afghanistan, United Arab Emirates, Kuwait, Djibouti, and Qatar | 2000–2012 | 42.8 (22.7) |
| Reference | Sample Type | Location | Year | PM2.5 µg/m3 Mean (SD) | PM10 µg/m3 Mean (SD) | TSP µg/m3 Mean (SD) |
|---|---|---|---|---|---|---|
| Nayebare et al. (2017) | 24-hr PM2.5 samples were collected on pre-weighed, sequentially numbered polypropylene-ring-supported Whatman 2-µm pore-size PTFE 46.2 mm filters, using a low-volume air-sampling pump | One site in Rabigh, Saudi Arabia | May to June 2013 | 37 (16.2) |
NOTE: PM, particulate matter; PTFE, polytetrafluoroethylene; SD, standard deviation; TSP, total suspended particle.
PM2.5 concentrations averaged from 10–365 µg/m3 across the locations, with an overall mean of 42.8 µg/m3 and a standard deviation of 22.7 µg/m3.
In a related study, visibility data obtained for 2006–2007 from seven U.S. Air Force 14th Weather Squadron sites located in a 17,000-km2 region in Iraq that includes Joint Base Balad were used to predict PM2.5. The authors coupled visibility measurements with aerosol optical depth observed by satellite to create a visibility prediction model, and then, using the previously defined calibration between visibility and PM2.5 (Masri et al., 2017b), they converted the spatially and temporally resolved satellite observations to ground-level PM2.5 concentrations over the region (Masri et al., 2017a). Predicted PM2.5 was variable across space and time, but overall the highest concentrations were in the Baghdad and Balad regions. Two-year average predicted PM2.5 ranged from 34.79 µg/m3 to 231.30 µg/m3. At the Air Force sites, mean predicted PM2.5 was 45.4 µg/m3 (min [December]: 32.7 µg/m3, max [June]: 63.5 µg/m3). The advantage of this study is that employing both satellite aerosol optical depth observations and airport visibility data provides a measure of particle abundance near the ground with fine (1 × 1 km) resolution (Masri et al., 2017a).
Other studies have measured PM in the region, including the aforementioned study by Brown et al. (2008), who characterized PM concentrations by collecting 24-hour samples at varying frequencies at three sites in Kuwait in 2004–2005, and DoD’s Enhanced Particulate Matter Surveillance Program, which characterized PM (TSP, PM10, PM2.5) in ambient air at 15 sites in 2006–2007 (Engelbrecht et al., 2008). DoD’s program was limited in that the sampler used for this study (the Airmetrics MiniVol portable air sampler) was not well suited to sampling in circumstances where concentrations may be excessively high, for example, during a dust storm, so that the samplers may have been overloaded, leading to overestimated exposures (NRC, 2010).
Between May 6 and June 17, 2013, Nayebare et al. (2017) collected 40 24-hour PM2.5 samples on pre-weighed, sequentially numbered polypropylene-ring-supported Whatman 2-µm pore-size polytetrafluoroethylene 46.2-mm filters, using a low-volume air-sampling pump at a location in Rabigh, Saudi Arabia. They observed significant variability in concentrations, ranging from 12.2 µg/m3 to 75.9 µg/m3, with an average of 37 µg/m3 and a standard deviation of 16.2 µg/m3.
At a location in Jeddah, Saudi Arabia, Lim et al. (2018) collected PM2.5 and PM10 samples on Teflon filters (GelmanTeflo, 37-mm, 0.2-µm pore-size) using Harvard impactors connected to calibrated vacuum pumps, at a rate of 10.0 L/min, from midnight to midnight over a year-long period from June 2011 to May 2012. They collected samples once on a Thursday or Friday and twice on Saturday through Wednesday to capture both variation through the week and seasonal differences. The annual average concentrations of PM2.5 were 21.9 µg/m3 with a standard deviation of 11.6 µg/m3, and the annual average PM10 concentration was 107.8 µg/m3 with a standard deviation of 72.6 µg/m3. Seasonally, the highest concentrations for both PM10 and PM2.5 were observed in spring (due to dust storm activity), while the lowest concentrations were observed in autumn. Coarse particles were predominant in Jeddah, with a smaller PM2.5/PM10 mass ratio (0.20) observed there than in other cities.
Regardless of the temporal, geographical, and compositional variations of airborne PM in Southwest Asia, the concentrations of PM often exceeded EPA’s NAAQS or the World Health Organization’s air quality guideline values for PM2.5 and PM10. Relying on the extrapolation of results derived from studies performed in the United
States to estimate the health effects attributed to air pollution in this area seems inappropriate (Li et al., 2019). The only airborne hazard that has complexity similar to those encountered in Southwest Asia by military personnel during service in the Southwest Asia theater was the smoke and dust discharged into the air after the collapse of the World Trade Center twin towers and a number of surrounding skyscrapers on September 11, 2001. The unprecedented event released millions of tons of material into the air from pulverized and incinerated building materials, furniture, equipment, and unburned jet fuels (Maciejczyk et al., 2005). The plume from the collapse covered a large area around the World Trade Center and penetrated many buildings in downtown Manhattan (CDC, 2002). Additional pollutants were released by the ensuing fire, which persisted until December 20, 2001, and by the recovery and clean up processes that followed (Lioy et al., 2002; Maciejczyk et al., 2005).
A 2002 EPA analysis estimated that “individuals engulfed in the initial dust/smoke cloud may have been exposed for several hours to concentrations of both fine and coarse inhalable particles anywhere in the range from milligrams per cubic meter (>1,000 µg/m3) to perhaps hundreds of milligrams per cubic meter (>100,000 µg/m3)” (EPA, 2002, p. 30). Concentrations had decreased to near ambient levels in December 2001, with a few peak concentrations ranging from 20 to 55 µg/m3 (Maciejczyk et al., 2005). Numerous World Trade Center–related health effects research studies have shown increased incidences of respiratory and other illnesses in World Trade Center responders, who were exposed to extremely high concentrations of dust (in the >15,000 µg/m3 range) (Li et al., 2016; Lippmann et al., 2015; Singh et al., 2018; Solan et al., 2013). Studies of residents near the former World Trade Center site, who were exposed to much lower concentrations of World Trade Center dust than the responders, showed an increased rate of new-onset and persistent bronchial hyperresponsiveness and symptoms as compared with a control population (Reibman et al., 2005). These studies provide biologic plausibility for the claim that exposures to airborne hazards in Southwest Asia have the potential to influence the health of military personnel, although clearly the World Trade Center exposure was much more intense and over a shorter time period.
Source Apportionment Studies
Several studies have investigated the sources and chemical composition of PM and dusts in Southwest Asia. Brown et al. (2008) conducted source apportionment using specimens that the authors collected in 2004–2005. The investigators analyzed for the presence of elemental and organic carbon and calculated the fraction of PM that was contributed by coarse particles. They found that coarse particles made up 50–60% of PM10. The high levels of PM10 and the large fraction of coarse particles making up PM10 are an indication that resuspension of dust and soil from the desert crust was a significant source. However, levels of elemental carbon, organic carbon, and most of the elements—including toxic heavy metals—that were identified were higher in urban location specimens, indicating contributions from local mobile and stationary sources.
Alolayan et al. (2013) investigated PM2.5 in the atmosphere of Kuwait based on the sampling program described in Brown et al. (2008). They used three methods of source identification; a positive matrix factorization model; backward trajectory profiles; and concentration rose plots. Contributions from five major sources of PM2.5 were estimated: sand dust or sandstorms; oil combustion or power plants; petrochemical industry, fertilizer, nylon or catalyst regeneration facilities; traffic, vehicle emissions, and road dust; and transported emissions (that is, emissions from outside Kuwait). The researchers found that 54% of PM2.5 emissions were from sand dust, 18% from oil combustion, 12% from the petrochemical industry, 11% from traffic, and 5% from sources transported from outside the country. The contributions from oil combustion, petrochemical industry, and traffic were found to originate from local sources, whereas sand dust and some emissions from traffic, and possibly smelters, appeared to originate from sources outside of Kuwait.
Engelbrecht et al. (2009) conducted a source apportionment analysis of the samples collected as part of DoD’s Enhanced Particulate Matter Surveillance Program. The researchers used trace-element analysis to measure the concentrations of metals and major elements and ion-chemistry analyses to estimate the mineral components. Scanning electron microscopy with energy dispersive spectroscopy was used to analyze the chemical composition of small individual particles. The three main air pollutant types found were geological dust, smoke from burn pits, and heavy metal condensates. Non-dust-storm events resulted in elevated trace metal concentrations in samples from Baghdad, Balad, and Taji in Iraq. In all instances, quartz grains had rounded edges, and mineral grains were
generally coated by clay minerals and iron oxides. The design of the sampling schema in this study does not permit complete characterization of the particle mass for any given set of samples because there needed to be more clearly defined objectives of the sampling and analysis scheme at the outset of the program (NRC, 2010). While the study provides a perspective on the airborne sources present in the Southwest Asia theater, there is reason to be skeptical of the conclusions drawn, which were based on a pooled analysis of sites that were widely separated in space (Djibouti, Afghanistan, Qatar, United Arab Emirates, Iraq, and Kuwait) and time (over an approximately 1-year period).
Lim et al. (2018) conducted source apportionment analysis of the samples they collected in Jeddah, Saudi Arabia. Using absolute principal component analysis, concentration roses, and backward trajectories, they identified the following source categories for both PM2.5 and PM2.5–10: soil/road dust; incineration; and traffic; and for PM2.5 only, residual oil burning. Soil/road dust accounted for a major portion of both the PM2.5 (27%) and PM2.5–10 (77%) mass, and the largest source for PM2.5 was residual oil burning (63%).
Javed et al. (2019) examined PAHs, n-alkane homologs, hopanes, and steranes in airborne PM2.5 and PM10 specimens collected in Doha, Qatar. This organic pollutant apportionment study was conducted in May–December 2015. Analyses indicated that the primary sources of these pollutants were fossil fuel combustion (emissions from vehicles, shipping, and petroleum refineries), fugitive dust, and vegetative and other biogenic sources.
Biologic Agents and Allergens
Biologic agents can contribute to disease in military personnel through causing infections or by initiating an allergic response from the immune system. A previous National Academies committee found that several infections endemic to Southwest Asia could have long-term adverse outcomes, including brucellosis, Campylobacter infection, leishmaniasis, malaria, Q fever, salmonellosis, and shigellosis. Of these, only brucellosis was found to be associated with a respiratory health outcome: respiratory system infections (IOM, 2007).
In addition, numerous aeroallergens have been observed across Southwest Asia: pollen from hundreds of different grasses, weeds, shrubs, and trees; spores from hundreds of species of molds; allergens from insects such as cockroaches and mosquitos; dander from domestic animals, rodents, and farm animals; and dozens of types of house dust mites and storage mites. Among the pollens specific to the region are those from the date palm and from the invasive shrub Prosopis juliflora (Goronfolah, 2016).
Toxicity of Sand and Dusts
Concerns about the toxicity of the sand and dusts encountered in the Southwest Asia theater have led to various studies to characterize the composition and the toxicity of dusts from the region. In 2004 the U.S. Central Command Area of Responsibility began Operation Sandbox to characterize the mineral, chemical, physical, and microbiologic composition of airborne Kuwaiti and Iraqi dust surface soil or dust samples normally encountered in other desert regions. The study found a number of bioavailable metals, including arsenic, chromium, lead, nickel, cobalt, strontium, tin, vanadium, zinc, manganese, barium, and aluminum. The investigators also identified more than 147 different microbial isolates (six different genera), of which about 30% are known human pathogens; 13 isolates were α- or β-hemolytic species (Lyles, 2018). These data suggest that the microbial and metal content of the mineralized dust could pose an inhalation hazard due to the presence of metals and pathogens.
There has also been research to characterize the toxicity using both in vitro (cell-based) and in vivo (animal) toxicity studies. Szema et al. (2014) obtained dusts from a grab sample taken from Camp Victory, Iraq, and examined the dusts using X-ray diffraction and X-ray fluorescence. They then conducted a small toxicity study using male C57BL/6 mice to compare the toxicity of the Camp Victory dust (n = 3) with that of untreated controls (n = 5) and of two positive control groups, a group treated with Montana mining dust (n = 2) and an inert negative-control soil sample from San Joaquin, California (n = 3). Both control dusts were obtained from the National Institute of Standards and Technology. The dust was administered intratracheally to age-matched C57BL/6 mice. The authors found increased interleukin-2 (IL-2) from bronchiolar lavage in the mice treated with Iraq dust compared with the control groups, demonstrating that Iraq dust may lead to lung inflammation. This small study provides some
information with respect to the possible histologic and immunologic effects of Iraq dusts; however; the route of exposure—intratracheal administration—does not correspond well with the exposure route experienced by humans in real-world situations.
Dorman et al. (2012) conducted a study in adult rats to characterize the respiratory toxicity of inhaled Iraqi sand. Adult rats underwent a 6-week inhalation regimen exposing them to air or to common cigarette smoke (3 hours per day, 5 days per week) that included exposure to Iraqi or crystalline silica (1 mg/m3, 19 hours per day, 7 days per week) or air during the last 2 weeks. Assessments included motor activity, whole-body plethysmography, cytological and biochemical analysis of bronchoalveolar lavage fluid, lung metal burden, nasal and lung pathology, and changes in lung protein and gene expression. Chemical analysis of the Iraqi sand showed that it contains nickel, manganese, vanadium, and chromium. The authors found evidence that the metals in Iraqi sand are bioavailable because they observed elevated lung parenchyma aluminum, silica, barium, manganese, and vanadium concentrations in Iraqi sand–exposed rats. Rats exposed to Iraqi sand only developed mild inflammation in the anterior nose and lung. Rats exposed to silica inhalation had some pulmonary responses that were not seen in Iraqi sand–exposed rats, such as mild laryngeal and tracheal inflammation, mild tracheal epithelial hyperplasia, and elevated lung silica concentrations. Cigarette smoke inhalation with or without co-exposure to either Iraqi sand or silica resulted in changes consistent with pulmonary inflammation and stress response. Rats exposed to cigarette smoke and silica had more widespread airway lesions than rats exposed to cigarette smoke only. Silica-exposed rats had more robust pulmonary gene expression and proteomic responses than seen in Iraqi sand–exposed rats. This study showed that the respiratory toxicity of Iraqi sand is similar to that of silica. It has the advantage of being an inhalation study that evaluated for interactions with cigarette smoking, a common exposure in military personnel. However, the exposure duration was only 6 weeks, which may not be representative of the exposure durations that service members experience during their deployments to the theater.
In a third experimental study using rats, Taylor et al. (2013) evaluated the respiratory toxicity of sand particles collected at military bases near Fort Irwin in Barstow, California; camps Victory, Taji, and Tallil in Iraq; and Khost, Afghanistan. The goal of the study was to assess the role of soluble metals in the respiratory toxicity of the sand particles using cell lines and animal models. Rat type II alveolar cell cultures were exposed to sand extracts or vehicle control in serum-free media for up to 24 hours. The researchers then determined cytotoxicity using the 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide assay and assessment of lactate dehydrogenase leakage. Male Crl:CD(SD) rats were used to assess the acute and delayed pulmonary toxicity of extracts of sand from Camp Victory, Camp Taji, and Khost, Afghanistan, and of Taji sand following intratracheal administration. Assessments included a biochemical analysis of bronchoalveolar lavage fluid (BALF) and lung histopathology. Based on the cell-culture assays, the researchers found that the sand from Taji and Tallil was the most toxic, followed by the sand from Khost, Afghanistan, Camp Victory, and Fort Irwin. The in vitro cytotoxicity assay results were partially predictive of in vivo responses. The more cytotoxic Taji sand extract induced an acute irritant response in rats following intratracheal administration. Rats that were administered the less cytotoxic Camp Victory sand extract had minimal biochemical or cytologic BALF changes, whereas rats given either the Afghanistan or the Taji sand extracts demonstrated BALF changes that were suggestive of mild lung inflammation. Similar lung pathologies were observed in all extract-exposed rats.
Taken together these toxicity studies provide some evidence that sands and dusts in Southwest Asia may have different toxic effects than dusts found in other regions. Such experiments have some advantages over observational studies because investigators have control over a number of influential factors, including the nature and temporal pattern of the exposure; the selection of the test subjects in terms of species, ages, gender, and known or suspected susceptibilities; and the nature and timing of the response assays before, during, and after the exposures. It is also the case that animal studies can have a good correlation with human disease; acutely toxic doses are similar in human and a variety of animal systems, and many respiratory system anatomic, physiologic, and biochemical parameters are similar in humans and other mammals. However, it is unclear how relevant these studies are for understanding human exposures. The outcomes ascertained are mechanistic in nature and provide evidence of harmful toxicological effects, but they lack clinical relevance. Two of the studies reviewed by the committee used intratracheal administration as the exposure method, which is of low relevance to human exposures. Additionally, the doses used in the studies may be higher than those experienced by military personnel in theater.
OCCUPATIONAL EXPOSURES
Occupational exposures akin to those experienced in civilian settings also occur in the Southwest Asia theater. For example, a military mechanic will experience exposures to fuels, engine fluids, and solvents just as that person’s civilian counterpart would, and military and civilian facilities management personnel may be exposed to both insecticides and pesticides as part of their duties. Exposure to such hazards has been associated with long-term adverse health outcomes (IOM, 2011). The military occupations with the highest exposure to vapors, gases, dusts, and fumes include firefighters; ground crew; fuel handlers; maintenance workers; infantry/combat engineers; artillery; motor transport; aviation; special forces; combat medicine; ordinance disposal; maintenance of vehicle, aircraft, or weapons systems; airfield services; and military police (Zell-Baran, 2018).
Certain job duties or tasks can also increase exposures to vapors, gases, dusts, and fumes. For example, military personnel who painted combat vehicles and equipment during their military service may have been exposed to chemical agent resistant coating (CARC) paint or to vapors. CARC is used on military vehicles to make metal surfaces more highly resistant to corrosion and to the penetration of chemical agents. CARC paints contain several inhalation hazards, including hexamethylene di-isocyanate, toluene diisocyanate, and other solvents.
While a number of papers considered by the committee mention military occupational exposures among the many airborne hazards experienced by deployed personnel, the committee did not identify any studies that specifically examined these exposures and adverse respiratory health outcomes.
EXPOSURE TRACKING BY THE DEPARTMENT OF DEFENSE
DoD and the Department of Veterans Affairs are working on a number of information management and technology efforts to support linking exposure and health effects information. The Individual Longitudinal Exposure Record (ILER) is a web-based application that provides the ability to link an individual to occupational and environmental exposures to improve the efficiency, effectiveness, and quality of health care. ILER is supposed to create a complete record of a service member’s occupational and environmental health exposures over the course of his or her career by linking individuals to known exposure events and incidents and compiling the exposure history in order to distill and report the relevant data and information (e.g., handling, diagnosis, and action thresholds). ILER uses multiple data sources, such as the Defense Manpower Data Center, Defense Occupational and Environmental Health Readiness System–Industrial Hygiene, and the Military Health System Data Repository. The goal of ILER is to provide epidemiologists, researchers, and policy makers with greater access to and insights on exposure events and to give them the ability to develop cohorts more efficiently by reducing the number of external information management and information technology systems they need to access in order to assess exposure impacts. ILER is planned to have full operating capability by September 2023 (Shuping, 2019).
FACTORS THAT MAY LEAD TO INCREASED VULNERABILITY TO AIRBORNE HAZARDS
There are factors that are common to military operations in Southwest Asia that, while they are not airborne hazards, may modify the relationship between exposure to airborne hazards and respiratory health effects. These include temperature extremes, stress, and noise. Other influences, such as obesity and poor diet, may also increase the individual susceptibility to some airborne hazards but are not discussed in this brief overview of the topic because they are less directly related to military service in theater. The risks from these hazards may have been increased due to the personnel having co-occurring exposures from their military occupations, tasks, or job duties that act on similar targets. The committee did not identify any literature that addressed the effect of these factors on respiratory health outcomes in deployed personnel but notes them here for completeness.
In addition to these, deployed military personnel may also be at higher risk than their nondeployed counterparts because of the characteristics of the structures in which they work, eat, and sleep. The committee could not identify any literature on this subject with the exception of a conference paper (Aldred and Corsi, 2011) that suggested that PM exposure in indoor environments in the Middle East might pose serious health problems because of high outdoor PM levels and high outdoor-indoor penetration factors in military buildings. This was also pointed out in the 2011 IOM report Long-Term Health Consequences of Exposure to Burn Pits in Iraq and Afghanistan (IOM,
2011), which observed that it was likely that much of the available in-theater housing would allow penetration of fine particles into the living spaces. However, neither of these sources cites data on penetration factors nor measurements in indoor environments. Information on this would help to better characterize potential airborne exposures encountered in indoor spaces in theater.
Temperature Extremes
Heat may increase exposure to air pollution through increased respiration, and prolonged exposure to extreme heat can cause heat exhaustion, heat cramps, heat stroke, and—in severe cases—death. It can also exacerbate preexisting chronic conditions, including respiratory diseases (WHO, 2019). In a study of heat illness hospitalizations and deaths in the U.S. Army from 1980–2002, infantry soldiers and gun crewman were found to have the greatest rate of heat illness among all military occupational specialties that were examined (Carter et al., 2005). Low temperatures may also have an effect on health. When temperatures drop, heat may rapidly leave the body, which can lead to shivering, fatigue, loss of coordination, or, in more serious cases, hypothermia. Epidemiologic literature shows growing evidence of the acute effects of high and low temperatures in the United States, Europe, and other parts of the world (Baccini et al., 2008; Turner et al., 2012; Zanobetti and Schwarz, 2008). More recently, in a time series analysis, Alahmad et al. (2019) found that both high and low ambient temperatures were significantly associated with an increased risk of short-term mortality in Kuwait. Another analysis of this population (Alhamed et al., 2020a) showed a U-shaped exposure–response relationship to heat and cardiovascular mortality, with the risk tripling at extreme high temperature (108° Fahrenheit), and males showing a higher risk than females. In those aged 15–64 years, which encompasses the age span of U.S. military personnel, risk was significantly increased. After further stratifying the 15–64 age group, there was a significantly increased risk of cardiovascular and non-accidental mortality at extreme high temperature in those most likely to work outside and perform demanding jobs (Alahamed et al., 2020b). These results suggest that in-theater ambient conditions may represent a risk even for young and healthy people. There have been some studies of how hot temperature modify the health effects of air pollutants in non-military populations, but the findings have been equivocal (Analitis et al., 2018; Lee, 2019).
Stress
Acute and chronic stress affect health through a wide range of biological pathways, including the hypothalamic-pituitary-adrenal and sympathetic-adrenal-medullary axes and other key regulatory systems of the body, including respiratory, immune, endocrine, central nervous system, cardiovascular, and metabolic functions (Clougherty and Kubzansky, 2009). The body’s response to stress is adaptive, meaning it responds to changing conditions and demands. However, over-extension of an acute stress response over time (also known as chronic stress) and the consequent failure to achieve homeostasis lead to physiologic damage and increase an individual’s susceptibility to injury from exposures to social and environmental stressors (Payne-Sturges et al., 2018). This condition is commonly referred to as “allostatic load” and includes systemic impacts to cardiovascular, immune, endocrine, and metabolic function as well as neurodevelopmental and cognitive effects (McEwen, 1998). A contrasting model in which cortisol production lessens following chronic stress has been proposed to explain the pro-inflammatory effects of chronic stress (Hannibal and Bishop, 2014). Chronic, repeated activation of acute stress responses may down-regulate, or blunt, adaptive acute stress responses either via dis-regulation of cortisol or catecholamine release at the target tissue. Psychosocial stressors and chemical pollutants affect many of the same physiologic systems (e.g., neurologic, metabolic, immune, and cardiovascular), which are key regulatory systems of the body. Therefore, it is highly plausible that combined psychosocial and environmental exposures may interact to increase or amplify the risks of adverse respiratory health outcomes.
Noise
Chronic environmental noise is associated with a wide variety of adverse health effects, including sleep disturbance, annoyance, noise-induced hearing loss, cardiovascular disease, endocrine effects, and diabetes (Hammer
et al., 2014). Also, service members have a significantly increased risk of hearing impairment (Lie et al., 2016). Contemporaneous exposures to particulate matter and noise may contribute to an increased susceptibility to the development or exacerbation of cardiopulmonary diseases. In a small study of male highway workers in the United States, increased levels of PM2.5 and noise were associated with increased heart rate variability, but no effects were observed with lung function or nitric oxide concentrations in exhaled air (Meier et al., 2014).
FINAL OBSERVATIONS ON AIRBORNE HAZARDS
The information developed in this chapter is used to inform the evaluation of respiratory outcomes evidence that is reviewed in Chapters 3 and 4. Some of the studies considered in these chapters examine the potential association between a particular exposure—burn pit emissions, for example—and a health effect or outcome. However, the committee is mindful of the fact that everyone who was deployed to the theater was potentially exposed to a broad range of airborne hazards, whether these were explicitly considered in an epidemiologic analysis or not. This is particularly true of airborne particulate matter, which was ubiquitous and ever-present in the form of environmental dust and sand. The committee therefore does not draw conclusions on the influence of specific exposures on specific outcomes in deployed personnel, an exercise that is in any case rendered largely impractical by the current lack of good exposure information. Chapter 5 goes on to address how some of the knowledge deficits identified here could be addressed.
REFERENCES
Alahmad, B., A. Shakarchi, M. Alseaidan, and M. Fox. 2019. The effects of temperature on short-term mortality risk in Kuwait: A time-series analysis. Environmental Research 171:278–284.
Alahmad, B., H. Khaishah, A. F. Shakarchi, M. Albagdadi, S. Rajgopalan, P. Koutrakis, and F. A. Jaffer. 2020a. Cardiovascular mortality and exposure to heat in an inherently hot region implications for climate change. Circulation Research Letter 141:1271–1273.
Alahmad, B., A. F. Shakarchi, H. Kharaisah, M. Alsaidan, J. Gasana, A. Al-Hemoud, P. Koutrakis, and M. A. Fox. 2020b. Extreme temperatures and mortality in Kuwait: Who is vulnerable? Science of the Total Environment 732:139289.
Aldred, J. R., and R. L. Corsi. 2011, December. Investigating the exposure of military personnel serving in the Middle East to ambient particulate matter. In 12th International Conference on Indoor Air Quality and Climate 2011. Pp. 143–148. https://www.isiaq.org/docs/presentations/0102_Aldred.pdf (accessed July 16, 2020).
Alolayan, M. A., K. W. Brown, J. S. Evans, W. S. Bouhamra, and P. Koutrakis. 2013. Source apportionment of fine particles in Kuwait City. Science of the Total Environment 448:14–25.
Analitis, A., F. De’Donato, M. Scortichini, T. Lanki, X. Basagana, F. Ballester, C. Astom, A. Paldy, M. Pascal, A. Gasparrini, P. Michelozzi, and K. Katsouyanni. 2018. Synergistic effects of ambient temperature and air pollution on health in Europe: Results from the PHASE Project. International Journal of Environmental Research and Public Health 15(9):1856.
Baccini, M., A. Biggeri, G. Accetta, T. Kosatsky, K. Katsouyanni, A. Analitis, H. R. Anderson, L. Bisanti, D. D’Ippoliti, J. Danova, B. Forsberg, S. Medina, A. Paldy, D. Rabczenko, C. Schindler, and P. Michelozzi. 2008. Heat effects on mortality in 15 European cities. Epidemiology 19:711–719.
Baird, C. P., S. DeBakey, L. Reid, V. D. Hauschild, B. Petruccelli, and J. H. Abraham. 2012. Respiratory health status of U.S. Army personnel potentially exposed to smoke from 2003 Al-Mishraq sulfur plant fire. Journal of Occupational and Environmental Medicine 54(6):717–723.
Benbrahim-Tallaa, L., R. A. Baan, Y. Grosse, B. Lauby-Secretan, F. El Ghissassi, V. Bouvard, N. Guha, D. Loomis, K. Straif, and International Agency for Research on Cancer Monograph Working Group. 2012. Carcinogenicity of diesel-engine and gasoline-engine exhausts and some nitroarenes. Lancet Oncology 13(7):663–664.
Blasch, K. W., J. E. Kolivosky, and J. M. Heller. 2016. Environmental air sampling near burn pit and incinerator operations at Bagram Airfield, Afghanistan. Journal of Occupational and Environmental Medicine 58(8 Suppl 1):S38–S43.
Brown, K.W., W. Bouhamra, D. P. Lamoureux, J. S. Evans, and P. Koutrakis. 2008. Characterization of particulate matter for three sites in Kuwait. Journal of the Air and Waste Management Association 58(8):994–1003.
Carter, R., S. N. Cheuvront, J. O. Williams, M. A. Kolka, L. A. Stephenson, M. N. Sawka, and P. J. Amoroso. 2005. Epidemiology of hospitalizations and deaths from heat illness in soldiers. Medicine & Science in Sports & Exercise 37(8):1338–1344.
CDC (Centers for Disease Control and Prevention). 2002. Occupational exposures to air contaminants at the World Trade Center Disaster Site–New York, September–October, 2001. JAMA 287(24):3201–3202.
Clougherty, J. E., and L. D. Kubzansky. 2009. A framework for examining social stress and susceptibility to air pollution in respiratory health. Environmental Health Perspectives 117:1351–1358.
DelRaso, N. J., C. A. Mauzy, B. A. Wong, and N. V. Reo. 2018. Burn pit emission and respirable sand exposures in rats: NMR-based urinary metabolomic assessment. No. AFRL-RH-WP-TR-2018-0061. Henry M. Jackson Foundation for the Advancement of Military Medicine. Wright-Patterson Air Force Base United States.
DoD (Department of Defense). 2018. DOD Instruction 4715.19: Use of open-air burn pits in contingency operations. Office of the Under Secretary of Defense for Acquisition and Sustainment. https://fas.org/irp/doddir/dod/i4715_19.pdf (accessed May 22, 2020).
DoD. 2019. Open Burn Pit Report to Congress: April 2019. Office of the Under Secretary of Defense for Acquisition and Sustainment. https://www.acq.osd.mil/eie/Downloads/Congress/Open%20Burn%20Pit%20Report-2019.pdf (accessed May 22, 2020).
Dorman, D. C., V. Mokashi, D. J. Wagner, A. O. Olabisi, B. A. Wong, O. R. Moss, J. A. Centeno, G. Guandalini, D. A. Jackson, W. E. Dennis, J. A. Lewis, R. S. Thomas, and G. D. Chapman. 2012. Biological responses in rats exposed to cigarette smoke and Middle East sand (dust). Inhalation Toxicology 24(2):109–124.
Draxler, R. R., J. T. McQueen and B. J. B. Stunder. 1994. An evaluation of air pollutant exposures due to the 1991 Kuwait oil fires using a Lagrangian model. Atmospheric Environment 28(13):2197–2210.
Engelbrecht, J. P., E. V. McDonald, J. A. Gillies, and A. W. Gertler. 2008. Department of Defense Enhanced Particulate Matter Surveillance Program (EPMSP): Final report. Desert Research Institute, Reno, NV. February. https://pdfs.semanticscholar.org/18af/a824db71d54eb0242659b5b224c71e32aaba.pdf (accessed June 17, 2020).
Engelbrecht, J. P., E. V. McDonald, J. A. Gillies, R. K. M. Jayanty, G. Casuccio, and A. W. Gertler. 2009. Characterizing mineral dusts and other aerosols from the Middle East—Part 1: Ambient sampling. Inhalation Toxicology 21(4):297–326.
EPA (Environmental Protection Agency). 2002. Exposure and human health evaluation of airborne pollution from the World Trade Center disaster (External review draft). Washington, DC: Environmental Protection Agency.
Goronfolah, L. 2016. Aeroallergens, atopy and allergic rhinitis in the Middle East. European Annals of Allergy and Clinical Immunology 48(1):5–21.
Goudie, A. S. 2014. Desert dust and human health disorders. Environment International 63:101–113.
Hammer, M. S., T. K. Swinburn, and R. L. Neitzel. 2014. Environmental noise pollution in the United States: Developing an effective public health response. Environmental Health Perspectives 122(2):115–119.
Hannibal, K. E., and M. D. Bishop. 2014. Chronic stress, cortisol dysfunction, and pain: A psychoneuroendocrine rationale for stress management in pain rehabilitation. Physical Therapy 94(12):1816–1825.
HEI (Health Effects Institute). 2010. Traffic-related air pollution: A critical review of the literature on emissions, exposure, and health effects. Special Report 17. Health Effects Institute. https://www.healtheffects.org/publication/traffic-related-air-pollution-critical-review-literature-emissions-exposure-and-health (accessed May 23, 2020).
Hines, S. E., P. Gucer, S. Kligerman, R. Breyer, J. Centeno, J.Gaitens, M. Oliver, S. Engelhardt, K. Squibb, and M. McDiarmid. 2013. Pulmonary health effects in Gulf War I service members exposed to depleted uranium. Journal of Occupational and Environmental Medicine 55(8):937–944.
IOM (Institute of Medicine). 2004. Gulf War and health: Updated literature review of sarin. Washington, DC: The National Academies Press.
IOM. 2005. Gulf War and health: Volume 3: Fuels, combustion products, and propellants. Washington, DC: The National Academies Press.
IOM. 2006. Gulf War and health: Volume 4: Health effects of serving in the Gulf War. Washington, DC: The National Academies Press.
IOM. 2007. Gulf War and health: Volume 5: Infectious diseases. Washington, DC: The National Academies Press.
IOM. 2008. Gulf War and health: Updated literature review of depleted uranium. Washington, DC: The National Academies Press.
IOM. 2011. Long-term health consequences of exposure to burn pits in Iraq and Afghanistan. Washington, DC: The National Academies Press.
Javed, W., M. Iakovides, R. Garaga, E. G. Stephanou, S. H. Kota, Q. Ying, J. M. Wolfson, P. Koutrakis, and B. Guo. 2019. Source apportionment of organic pollutants in fine and coarse atmospheric particles in Doha, Qatar. Journal of the Air & Waste Management Association 69(11):1277–1292.
Jayaratne, E. R., G. R. Johnson, P. McGarry, H. C. Cheung, and L. Morawska. 2011. Characteristics of airborne ultrafine and coarse particles during the Australian dust storm of 23 September 2009. Atmospheric Environment 45(24):3996–4001.
Krefft, S. D., C. S. Rose, S. Nawaz, and Y. E. Miller. 2015. Deployment-related lung disorders. Federal Practitioner 32(6):32–38.
Lee, W. 2019. Synergic effect between high temperature and air pollution on mortality in Northeast Asia. Environmental Research 178:108735.
Li, J., R. M. Brackbill, T. S. Liao, B. Qiao, J. E. Cone, M. R. Farfel, J. L. Hadler, A. R. Kahn, K. J. Konty, L. T. Stayner, and S. D. Stellman. 2016. Ten-year cancer incidence in rescue/recovery workers and civilians exposed to the September 11, 2001 terrorist attacks on the World Trade Center. American Journal of Industrial Medicine 59(9):709–721.
Li, J., E. Garshick, A. Al-Hemoud, S. Huang, and P. Koutrakis. 2020. Impacts of meteorology and vegetation on surface dust concentrations in Middle Eastern countries. Science of the Total Environment 712:136597.
Li, X., L. Jin, and H. Kan. 2019. Air pollution: A global problem needs local fixes. Nature 570(7762):437–439.
Lie, A., M. Skogstad, H. A. Johannessen, T. Tynes, I. S. Mehlum, K. Nordby, B. Engdahl, and K. Tambs. 2016. Occupational noise exposure and hearing: A systematic review. International Archives of Occupational and Environmental Health 89(3):351–372.
Lim, C. C., G. D. Thurston, M. Shamy, M. Alghamdi, M. Khoder, A. M. Mohorjy, A. Alkhalaf, J. Brocato, L. C. Chen, and M. Costa. 2018. Temporal variations of fine and coarse particulate matter sources in Jeddah, Saudi Arabia. Journal of the Air & Waste Management Association 68(2):123–138.
Lioy, P. J., C. P. Weisel, J. R. Millette, S. Eisenreich, D. Vallero, J. Offenberg, B. Buckley, B. Turpin, M. Zhong, M. D. Cohen, C. Prophete, I. Yang, R. Stiles, G. Chee, W. Johnson, R. Porcja, S. Alimokhtari, R. C. Hale, C. Weschler, and L. C. Chen. 2002. Characterization of the dust/smoke aerosol that settled east of the World Trade Center (WTC) in lower Manhattan after the collapse of the WTC 11 September 2001. Environmental Health Perspectives 110(7):703–714.
Lippmann, M., M. D. Cohen, and L. C. Chen. 2015. Health effects of World Trade Center (WTC) dust: An unprecedented disaster’s inadequate risk management. Critical Reviews in Toxicology 45(6):492–530.
Lyles, M.B. 2018. Chapter 18: Biological, chemical, and environmental hazards of desert dust to military personnel. Environmental Geochemistry: Site Characterization, Data Analysis, and Case Histories (Second Edition). Cambridge, MA: Elsevier. Pp. 467–485.
Maciejczyk, P. B., R. L. Zeisler, J. S. Hwang, G. D. Thurston, and L. C. Chen. 2005. Characterization of size-fractionated World Trade Center dust and estimation of relative dust contribution to ambient particulate concentrations. Urban Aerosols and Their Impacts: Lessons Learned from the World Trade Center Tragedy (ACS Symposium Series): Volume 919. Washington, DC: American Chemical Society. Pp. 114–131.
Masiol, M., C. T. M. Mallon, K. M. Haines, Jr., M. J. Utell, and P. K. Hopke. 2016a. Airborne dioxins, furans, and polycyclic aromatic hydrocarbons exposure to military personnel in Iraq. Journal of Occupational and Environmental Medicine 58(8S):S22–S30.
Masiol, M., C. T. M. Mallon, K. M. Haines, Jr., M. J. Utell, and P. K. Hopke. 2016b. Source apportionment of airborne dioxins, furans, and polycyclic aromatic hydrocarbons at a United States forward operating air base during the Iraq war. Journal of Occupational and Environmental Medicine 58(8S):S31–S37.
Masri, S., E. Garshick, B. A. Coull, and P. Koutrakis. 2017a. A novel calibration approach using satellite and visibility observations to estimate fine particulate matter exposures in Southwest Asia and Afghanistan. Journal of the Air & Waste Management Association 67(1):86–95.
Masri, S., E. Garshick, J. Hart, W. Bouhamra, and P. Koutrakis. 2017b. Use of visual range measurements to predict fine particulate matter exposures in Southwest Asia and Afghanistan. Journal of the Air & Waste Management Association 67(1):75–85.
Mauzy, C. 2019. Toxicity evaluation and biomarker identification in rats exposed to burn pit emissions and respirable sand from Afghanistan. Air Force Research Laboratory. Presentation to the Committee on the Respiratory Health Effects of Airborne Hazards Exposures in the Southwest Asia Theater of Military Operations. October 4, 2019.
McEwen, B. S. 1998. Protective and damaging effects of stress mediators. New England Journal of Medicine 338(3):171–179.
Meier, R., W. E. Cascio, A. J. Ghio, P. Wild, B. Danuser, and M. Riediker. 2014. Associations of short-term particle and noise exposures with markers of cardiovascular and respiratory health among highway maintenance workers. Environmental Health Perspectives 122:726–732.
Mori, I., M. Nishikawa, T. Tanimura, and H. Quan. 2003. Change in size distribution and chemical composition of kosa (Asian dust) aerosol during long-range transport. Atmospheric Environment 37(30):4253–4263.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2017a. Assessment of the Department of Veterans Affairs Airborne Hazards and Open Burn Pit Registry. Washington, DC: The National Academies Press.
NASEM. 2017b. Investigative strategies for lead-source attribution at Superfund sites associated with mining activities. Washington, DC: The National Academies Press.
Nayebare, S. R., O. S. Aburizaiza, A. Siddique, D. O. Carpenter, J. Zeb, A. J. Aburizaiza, C. Pantea, M. M. Hussain, and H. A. Khwaja. 2017. Association of fine particulate air pollution with cardiopulmonary morbidity in Western Coast of Saudi Arabia. Saudi Medical Journal 38(9):905–912.
NRC (National Research Council). 1996. Understanding risk: Informing decisions in a democratic society. Washington, DC: National Academy Press.
NRC. 2008. Review of toxicologic and radiologic risks to military personnel from exposure to depleted uranium during and after combat. Washington, DC: The National Academies Press.
NRC. 2010. Review of the Department of Defense Enhanced Particulate Matter Surveillance Program report. Washington, DC: The National Academies Press.
PAC (Presidential Advisory Committee). 1996. Presidential Advisory Committee on Gulf War Veterans’ Illnesses: Final Report. Washington, DC: Government Printing Office.
Payne-Sturges, D., M. Scammell, J. Levy, D. Cory-Slechta, E. Symanski, J. C. Shmool, R. Laumbach, S. Linder, and J. Clougherty. 2018. Methods for evaluating the combined effects of chemical and nonchemical exposures for cumulative environmental health risk assessment. International Journal of Environmental Research and Public Health 15(12):2797.
Querol, X., A. Tobías, N. Pérez, A. Karanasiou, F. Amato, M. Stafoggia, C. Pérez García-Pando, P. Ginoux, F. Forastiere, S. Gumy, P. Mudu, and A. Alastuey. 2019. Monitoring the impact of desert dust outbreaks for air quality for health studies. Environment International 130:104867.
Reibman, J., S. Lin, S.-A. A. Hwang, M. Gulati, J. A. Bowers, L. Rogers, K. I. Berger, A. Hoerning, M. Gomez, and E. F. Fitzgerald. 2005. The World Trade Center residents’ respiratory health study: New-onset respiratory symptoms and pulmonary function. Environmental Health Perspectives 113(4):406–411.
Rostker, B. 2000. Environmental exposure report: Oil well fires. Department of Defense. https://gulflink.health.mil/owf_ii/index.htm (accessed May 12, 2020).
Schlesinger, R. B. 1988. Biological disposition of airborne particles: Basic principles and application to vehicular emissions. In Air Pollution, the Automobile, and Public Health, pp. 239–298. https://www.ncbi.nlm.nih.gov/books/NBK218161 (accessed July 16, 2020).
Shuping, E. 2019. Individual Longitudinal Exposure Record (ILER). Briefing to Office of Research and Development and Clinical Staff. PowerPoint presentation. Department of Veterans Affairs. https://www.hsrd.research.va.gov/for_researchers/cyber_seminars/archives/3699-notes.pdf (accessed May 13, 2020).
Singh, A., R. Zeig-Owens, W. Moir, C. B. Hall, T. Schwartz, M. Vossbrinck, N. Jaber, M. P. Webber, K. J. Kelly, V. Ortiz, E. Koffler, and D. J. Prezant. 2018. Estimation of future cancer burden among rescue and recovery workers exposed to the World Trade Center disaster. JAMA Oncology 4(6):828–831.
Solan, S., S. Wallenstein, M. Shapiro, S. L. Teitelbaum, L. Stevenson, A. Kochman, J. Kaplan, C. Dellenbaugh, A. Kahn, F. N. Biro, M. Crane, L. Crowley, J. Gabrilove, L. Gonsalves, D. Harrison, R. Herbert, B. Luft, S. B. Markowitz, J. Moline, X. Niu, H. Sacks, G. Shukla, I. Udasin, R. G. Lucchini, P. Boffetta, and P. J. Landrigan. 2013. Cancer incidence in World Trade Center rescue and recovery workers, 2001–2008. Environmental Health Perspectives 121(6):699–704.
Spektor, D. M. 1998. A review of the scientific literature as it pertains to Gulf War illnesses—Volume 6: Oil well fires. National Defense Research Institute. Santa Monica, CA: RAND Corporation.
Szema, A. M., R. J. Reeder, A. D. Harrington, M. Schmidt, J. Liu, M. Golightly, T. Rueb, and S. A. Hamidi. 2014. Iraq dust is respirable, sharp, metal-laden, and induces lung inflammation with fibrosis in mice via IL-2 upregulation and depletion of regulatory T cells. Journal of Occupational and Environmental Medicine 56(3):243–251.
Taylor, K., M. L. Foster, J. M. Law, J. A. Centeno, E. Fornero, M. S. Henderson, S. A. Trager, M. G. Stockelman, and D. C. Dorman. 2013. Assessment of geographical variation in the respiratory toxicity of desert dust particles. Inhalation Toxicology 25(7):405–416.
Thomas, R., T. Vigerstad, J. Meagher, and C. McMullin. 2000. Particulate exposure during the Persian Gulf War. Washington, DC: Department of Defense.
Tsiouri V., K. E. Kakosimos, and P. Kumar. 2015. Concentrations, sources and exposure risks associated with particulate matter in the Middle East Area—a review. Air Quality, Atmosphere, and Health 8:67–80.
Turner, L. R., A. G. Barnett, D. Connell, and S. Tong. 2012. Ambient temperature and cardiorespiratory morbidity: A systematic review and meta-analysis. Epidemiology 23(4):594–606.
UNEP (United Nations Environment Programme). 2007. Air quality and atmospheric pollution in the Arab Region. Draft. League of Arab States and United Nations Economic and Social Commission for Western Asia. http://www.un.org/esa/sustdev/csd/csd14/escwaRIM_bp1.pdf (accessed May 22, 2020).
USALIA (U.S. Army Logistics Innovation Agency). 2013. U.S. Army Central area of responsibility contingency base waste stream analysis. Fort Belvoir, VA: Pacific Northwest National Laboratory. https://apps.dtic.mil/dtic/tr/fulltext/u2/a579439.pdf (accessed May 22, 2020).
USAPHC (U.S. Army Public Health Command). 2010. Screening health risk assessments, Joint Base Balad, Iraq, 11 May–19 June 2009. Aberdeen Proving Ground, MD: U.S. Army Center for Health Promotion and Preventive Medicine.
VA (Department of Veterans Affairs). 2018. Airborne hazards concerns: Information for veterans. War Related Illness and Injury Study Center. https://www.warrelatedillness.va.gov/education/factsheets/airborne-hazards-concerns-info-for-veterans.pdf (accessed April 7, 2020).
WHO (World Health Organization). 2019. Information and public health advice: Heat and health. https://www.who.int/globalchange/publications/heat-and-health/en (accessed May 13, 2020).
Winkenwerder, W. 2002. Case narrative: US demolition operations at Khamisiyah. Final report. Washington, DC: Department of Defense. https://gulflink.health.mil/khamisiyah_iii (accessed May 12, 2020).
Zanobetti, A., and J. Schwartz. 2008. Temperature and mortality in nine U.S. cities. Epidemiology 19:563–570.
Zell-Baran, L. 2018. Are military occupational specialty codes (MOS) useful epidemiologic tools to predict inhalational exposures during deployment? PowerPoint presentation. National Jewish Health. https://cdn.ymaws.com/www.cste.org/resource/resmgr/weston/2018weston/Zell_Baran_20180907.pdf (accessed September 2, 2019).




















