
Proceedings of a Workshop
| IN BRIEF | |
|
September 2020 |
Developing a Patient-Centered Approach to Optimizing Veterans’ Access to Health Care Services
Proceedings of a Workshop—in Brief
On July 9–10, 2020, the Board on Health Care Services of the National Academies of Sciences, Engineering, and Medicine hosted a virtual workshop titled Developing a Patient-Centered Approach to Optimizing Veterans’ Access to Health Care Services.1 The workshop featured invited speakers and discussions on strategies for conceptualizing and measuring access, strategies for increasing access capacity, access needs of special populations, and priorities for the future. This Proceedings of a Workshop—in Brief highlights the presentations and discussions that occurred at the workshop.2
BACKGROUND AND CONTEXT
Kenneth W. Kizer of Atlas Research noted that although there has been extensive research on the subject of access, there is no single definition of—or method for assessing or measuring—access to care. He stated that access is inherently multidimensional and a function of both supply and demand for health care services. Health system factors such as the number and location of facilities and the number and types of clinicians shape the supply of health care, while patient factors such as the number of patients seeking care, the types of care they require, and their perceptions about the quality of care drive demand. Kizer noted that it is important to consider the processes and methods through which services are delivered, and to focus on providing access to care that is appropriate to each patient’s need. David Pryor of Ascension agreed, stating that it is essential to ensure that the right care is provided at the right time and in the right way.
Susan Kirsh from the U.S. Department of Veterans Affairs’ (VA’s) Office of Veterans Access to Care, provided an overview of the Veterans Health Administration (VHA). More than 9 million veterans are currently enrolled in VA health services (VA, 2019), with 1 in 12 identifying as female (U.S. Census Bureau, 2017).
Kirsh noted that approximately 25 percent of the VA patient population lives in rural areas, and the average age of VA patients is older than for nonveterans (VA, 2020). Veteran populations also experience high rates of chronic pain and complex chronic illnesses, in addition to combat-related conditions such as posttraumatic stress disorder (PTSD), traumatic brain injury, and polytrauma (VA, 2020). Kameron Matthews from VA’s Office of Community Care also addressed the complexity of veterans’ health care needs. She noted that coordinating patient care is a high priority
___________________
1 The workshop agenda and presentations are available at https://www.nationalacademies.org/event/07-09-2020/developing-a-patient-centered-approach-to-optimizing-veterans-access-to-health-care-services-a-workshop (accessed July 23, 2020).
2 This Proceedings of a Workshop—in Brief is not intended to provide a comprehensive summary of information shared during the workshop. The information summarized here reflects the knowledge and opinions of individual workshop participants and should not be seen as a consensus of the workshop participants, the planning committee, or the National Academies of Sciences, Engineering, and Medicine.
![]()
for VHA, and that the integration of VHA and community care has reach historically high levels following the passage and implementation of the VA MISSION Act of 2018.3
Kirsh summarized discussions from a VHA roundtable event held in January 2020 as part of the Office of Veterans Access to Care’s Strategic Access Management Initiative, which convened non-VA health care leaders to discuss health care access. She identified three key suggestions for improving access that emerged from the event: prioritize patients’ needs and their perspectives regarding care, examine measures of access that go beyond wait times for care, and emphasize wait times for time-sensitive conditions. Kirsh added that the group also made the point that there is no standard industry-wide definition of access or method of assessing access. She noted that VA is working to implement suggestions from the Strategic Access Management Initiative roundtable and further leverage technology in its efforts to improve patient access. This workshop is intended to inform those efforts.
CONCEPTUALIZING ACCESS
Adrian Atizado, a veteran and veteran advocate, said that timely access to care goes beyond seeing a clinician or receiving needed services. It is also about the quality of care veterans receive and the relationships they build within the health system to improve their health and quality of life.
John Fortney of the University of Washington and VA Puget Sound Health Care System discussed reconceptualizing access, highlighting the importance of differentiating between objective measures of access to care (e.g., wait times) and perceived access to care. Perceived access to care captures subjective dimensions of access that predict the use of health care services, but it can be difficult to measure. Building on previous work (e.g., Penchansky and Thomas, 1981), Fortney described five dimensions of perceived access to health care—geographic, temporal, digital, financial, and cultural—within a theoretical framework for access (Fortney et al., 2011) (see Figure 1). Fortney noted that access depends on the structure of the health care system and each patient’s social determinants of access. He also highlighted the role of trust in ensuring access to health care services, He said that patients’ lack of trust in VA clinicians is an important barrier to receiving care for PTSD and other mental health conditions (Pyne et al., 2019).
Hal Yee of the Los Angeles County Department of Health Services suggested that the key question of access is how to provide the right health care at the right time, emphasizing that providing the right care (i.e., appropriate care), not just more care, is critical. He described initiatives in Los Angeles to improve access and patient care, noting that they have shown that high-quality patient care can be provided without face-to-face meetings for one-third of patient requests. Regarding delivery of care at the “right time,” Yee said that it is important to implement flexible
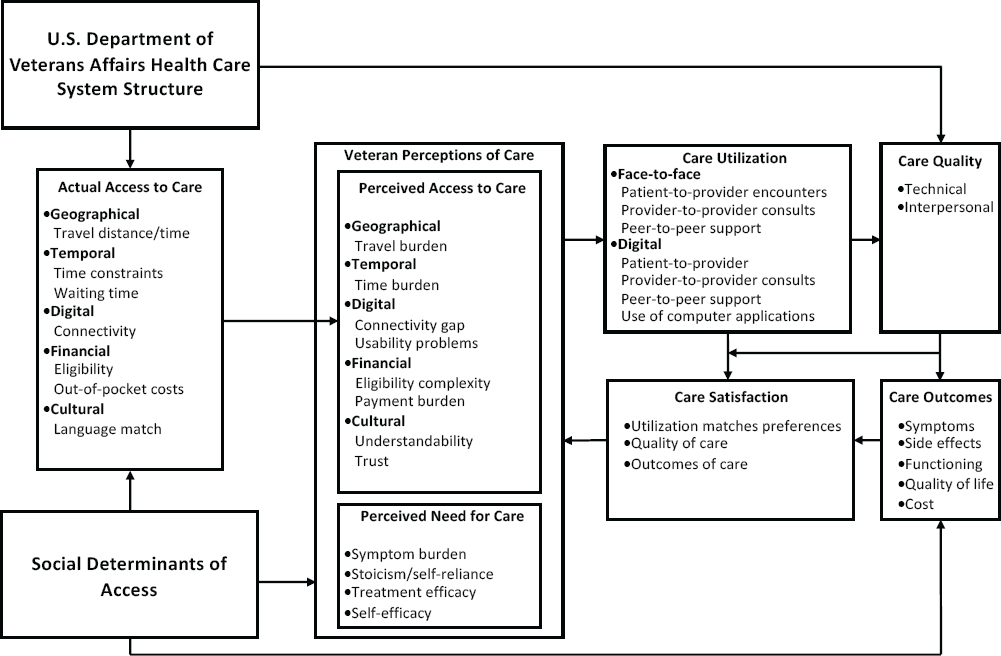
SOURCES: John Fortney presentation, July 9, 2020; Fortney et al., 2011.
___________________
3 For more on the VA MISSION Act of 2018, see https://missionact.va.gov (accessed July 23, 2020).
patient scheduling. He noted that general access standards (e.g., specialty care appointments must be provided within 30 days) are often arbitrary and not responsive to patient needs. Instead, he recommended a “precision” system in which timing for specialty visits is determined according to the individual needs of each patient (e.g., his or her specific clinical condition or need for care, as well as social circumstances). Yee concluded that focusing on the appropriateness of health care delivery can help solve the problems with perceived lack of access.
Lillian Gelberg of the VA Greater Los Angeles Healthcare System noted that conceptualizing and measuring access are key to formulating health policy because of their potential to predict health care use; promote social justice; and improve patient outcomes, including health status (perceived and evaluated), satisfaction with care, quality of life, and housing stability. She outlined seven domains of access that can be used to improve health care use and outcomes for veterans (Anderson et al., 2013).
- Access—Veterans’ use of personal health services and everything that facilitates or impedes their use
- Potential access—Presence of veterans’ enabling characteristics that affect use of services
- Realized access—Veterans’ use of services
- Effective access—Realized access (use of services) that improves veterans’ health outcomes
- Efficient access—Realized access (use of services) that improves veterans’ health outcomes while minimizing health care cost
- Equitable access—Use of services is predicted by veterans’ demographics, genetic susceptibility, and need
- Inequitable access—Use of services is predicted by veterans’ social and enabling characteristics and vulnerabilities
Gelberg additionally presented the Behavioral Model for Vulnerable Populations to help frame the challenge of health care access for veterans (Gelberg et al., 2000). The model outlines individual and contextual characteristics that contribute to health behaviors and health outcomes including access to care and use of health services. As an example of applying the model to veterans experiencing homelessness, she reviewed the Humanism Pocket Tool, which helps clinicians place the veteran at the center of care through a well-defined set of techniques (Soh et al., 2018). This reframes the veteran’s story and helps him or her feel supported by services tailored to individual needs and preferences, increasing the likelihood that he or she will return for follow-up visits, said Gelberg.
Andrew Bindman of the University of California, San Francisco (UCSF), asked whether wait times for care constitute a sufficient conceptualization of access. Both Fortney and Yee suggested that access is a multidimensional construct—while wait times are one component of access, they are insufficient for a full conceptual definition. Yee added that having a universal time-based metric for access (e.g., the requirement for scheduling an appointment within 7 days) fails to account for differences in individual patient needs. Bindman also asked about the interaction between choice and access, and to what degree patient choice is a necessary component of high-quality access, especially for specialized services or complex multisystem care. Gelberg responded that the experiences of homeless veterans have highlighted the importance of balancing access and choice. She added that health systems and clinicians can provide access to care, but they need to be available when the veteran is ready for care. She noted that this match between patient needs and availability of services is essential to patient-centered care—for example, virtual mental health services may improve access in many patient populations, but they may not be accessible to homeless veterans.
CONSIDERATIONS FOR MEASURING ACCESS
Lisa Rubenstein of the RAND Corporation noted that there are multiple stakeholders—including patients, clinicians, and health systems—in assessments of health care access, and a key question is which perspective should be measured. Shantanu Agrawal of the National Quality Forum (NQF) noted that there are numerous challenges in measuring access. He explained that research on health care quality has historically focused less on access than on other dimensions of quality. Agrawal noted that many of the quality measures endorsed by NQF have items that capture access, but access is rarely assessed as a stand-alone measure.
Kevin Grumbach of UCSF suggested that the form of measurement should follow from its desired function. Keeping the goal of measurement in mind during its design will help to streamline development and implementation, avoiding issues of measure overload for clinicians and making resulting data more actionable. He noted that while global measures can be useful tools, developing optimal precision measures requires the identification of functional goals and the consideration of purpose, audience, and practicality.
Mary Barton of the National Committee for Quality Assurance reviewed the Healthcare Effectiveness Data and Information Set (HEDIS) measures to explain the history and current state of measuring access to care. The HEDIS measures are used and reported by more than 1,000 health insurance plans as a component of accreditation and for state and federal mandates to improve performance. Barton emphasized that validity is a key requirement in selecting appropriate measures. She noted that actionability of measures is also an important requirement because it is essential to measure constructs that are amenable to intervention. She suggested that VA could consider a “threshold management strategy” in which all care delivery organizations within the department are assessed as to whether they meet benchmarks for access to care. Finally, Barton cautioned about the burden of measurement—noting that both clinicians and patients can be overwhelmed by requests to contribute to data collection.
Patrick Romano of the University of California, Davis, suggested that VA has done well in its efforts to measure access to care but there is still opportunity for improvement. He echoed Grumbach’s assertion that the fundamental purpose of quality measurement is to drive quality improvement, with access being an important component of quality. He presented a conceptual model for developing and implementing measures for quality assessment, describing an iterative process that moves from theoretical concepts to data collection and interpretation, and finally back to theoretical concepts (Lloyd, 2004). Romano noted that single measures of access are too narrow to capture this multidimensional construct, and that this conceptual model could be used to develop, implement, and assess novel measures. For example, integrating Donabedian’s structure-process-outcome framework (1980) with Fortney and colleagues’ VA-focused framework (2011), a suite of access measures could include site policy on scheduling appointments, wait time for urgent appointments, and potentially avoidable hospitalizations or emergency department (ED) visits for asthma or heart failure. Romano also echoed Barton’s comments on assessing measure performance and emphasized the importance of assessing reliability and actionability in addition to validity. He suggested that access measures should not be static; instead, they should be integrated into a life cycle of measurement, subject to improvement, refinement, and potentially retirement.
Martin Roland of the University of Cambridge offered several observations from the single-payer National Health System in the United Kingdom, which he noted is similar to VA (see Box 1). He emphasized that neither measurement nor improvement of access is simple and that all initiatives to improve access should be cautious of supply-induced demand and consider potential unintended consequences of interventions (e.g., increased disparities or reduced continuity of care).
When asked to recommend optimal measures of access, Grumbach and Barton both suggested using a global measure that asks patients if they are able to access care when they feel it is needed. Romano suggested measures that capture avoidable and unnecessary health care use, and Roland called for measuring continuity of care based on whether patients are able to access their preferred clinicians or services. Yee agreed that assessments of access should be responsive to patient needs, noting that sometimes the most appropriate care is a brief phone call and the traditional standard of scheduling an in-person appointment within 2 weeks would represent an unreasonable and unnecessary delay. Agrawal agreed, noting that the modality through which care is delivered should be a function of clinical appropriateness as well as patient needs and expectations.
INCREASING ACCESS CAPACITY
Eva Lee of the Georgia Institute of Technology suggested that using multiple virtual modalities of care to supplement face-to-face consultations is a key strategy for improving access capacity. She noted that the ability to deliver care through diverse modalities promotes system resilience and enables a health care system to expand capacity in response to surges in demand. Lee suggested that an additional strategy for improving care capacity, particularly for vulnerable populations, is to anticipate changes in demand and proactively scale services accordingly. This avoids delays associated with a reactive system in which the expansion of services lags behind the changes in demand. She suggested that systematically examining usage patterns within health care systems can facilitate early interventions to increase capacity, improving patients’ access to health care services.
Several speakers discussed telehealth as an important strategy to build access capacity.4 Leonie Heyworth of VA stated that VA strives to meet four goals in the implementation of telehealth services: improving accessibility, building capacity, delivering high-quality care, and providing a “simple and delightful” experience for patients. She noted that VA provided more than 2.6 million episodes of care via telehealth in 2019. Since March 2020, the provision of telehealth services has risen dramatically in response to the coronavirus 2019 (COVID-19) pandemic. Kirsh elaborated on virtual care management during the COVID-19 pandemic, describing how VA has substantially increased the provision of phone and video appointments, particularly for mental health (Heyworth et al., 2020) (see Figure 2). Kirsh noted that VA will continue to expand virtual services for specialty care. Heyworth explained that VA had previously established a strong foundation for telehealth services, which allowed for rapid expansion in response to the pandemic. Initiatives to equip both clinicians and patients with technologies for virtual care have been key to this strong foundation.
Brian Skow of Avera Health described the company’s work in telehealth, noting that the company works with underserved populations that include patients in rural health care settings, prisons, and the Indian Health Service. The company is in its third decade of virtual health delivery, spanning school services, behavioral health, and pharmacy services. Skow described ways in which the company’s virtual health initiatives have improved patients’ access to high-quality care. For example, Avera has enhanced access to specialty care in rural settings by providing peer-to-peer sup-
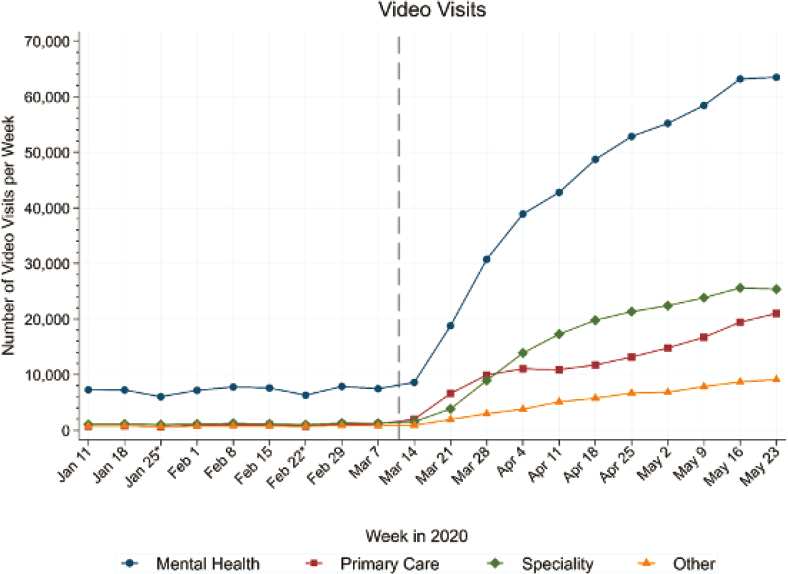
NOTES: “Other” includes social work and some other nonphysician visits. The dotted line indicates the time at which VA converted from in-person care to virtual care whenever clinically appropriate.
SOURCE: Leonie Heyworth presentation, July 9, 2020. Republished with permission of the Massachusetts Medical Society from Expanding access through virtual care: The VA’s early experience with COVID-19, Heyworth, L., S. Kirsh, D. Zulman, J. M. Ferguson, and K. W. Kizer, 2020; permission conveyed through Copyright Clearance Center, Inc.
___________________
4 Telehealth is “[t]he delivery of health care services, where distance is a critical factor, by all health care professionals using information and communication technologies for the exchange of valid information for diagnosis, treatment, and prevention of disease and injuries; research and evaluation; and for the continuing education of health care providers, all in the interests of advancing the health of individuals and their communities” (WHO, 2010, p. 9).
port for family clinicians staffing rural hospitals. Skow also described how Avera has adapted to new demand for virtual care during the COVID-19 pandemic. A previously established nurse hotline was converted to a COVID-19 call center that is able to triage patients and route them to virtual visits with clinicians. If patients do not have reliable access to technology, they are sent iPads to ensure access to virtual health services. Skow reflected that effective telehealth implementation depends on both effective training for staff and technology access for patients. He concluded that telehealth has the potential to significantly improve patient care across the care continuum.
B. Rao Tripuraneni from Kaiser Permanente described the “health care access cycle” as a cyclical relationship among long-term planning for supply and demand, monitoring the availability of appointments, and retrospective evaluations of performance. He noted that a system’s ability to supply access to health care is dependent on each of these three factors. Tripuraneni explained that one strategy to build access capacity is to improve supply by reducing unnecessary care. He described a system of chart review in which primary care providers request virtual consultation from specialists. This allows specialists to offer opinions on complex cases while avoiding unnecessary referrals and subsequent delays. Tripuraneni noted that while the implementation of steps to improve access may be rocky at the outset, it does get easier, and optimizing access to care should be an ongoing endeavor within all health systems.
ENSURING ACCESS FOR SPECIAL POPULATIONS
Atizado noted that veterans often share similar exposures through their military experiences, but they may also have unique exposures to violence, injury, and harmful environments that require different types of care. Jeannette South-Paul of the University of Pittsburgh elaborated on care required for veteran populations, noting that VA has designated “special populations” that may require particular care, including minority veterans, veterans with substance use disorders, women veterans, veterans experiencing homelessness, veterans with spinal cord injuries or amputations, and veterans living in rural areas.
Donna Washington of the VA Greater Los Angeles Healthcare System discussed how barriers to health care access contribute to health disparities. She noted that it is important to consider patients’ resources and to tailor care to the social context and specific needs of veterans. Washington presented strategies to improve equity across four dimensions of access: availability, accessibility, accommodation, and acceptability (Penchansky and Thomas, 1981). For equity in availability and accessibility, she recommended promoting diversity in the clinician workforce, assisting patients with technology to promote access to telehealth, and expanding access to after-hours care. For equity in accommodation, she suggested addressing patients’ social determinants of health and expanding the use of patient navigators. To address equity in acceptability, Washington proposed systematic assessment and reporting for measures of trust in VA health care. She noted that these data should be reported separately for each designated special population, because patients’ trust and satisfaction in clinicians often varies by race and gender.
Building on this discussion of equity, Laura Taylor of VA highlighted the important role of social workers and the need to consider social determinants of health in veterans’ health care. She noted that addressing these determinants can improve access and quality by reducing missed appointments, reducing ED visits, and improving adherence to treatment plans. Taylor emphasized the importance of patient-centered care, noting that social workers take a holistic view of each patient to develop treatment plans that acknowledge the person’s life experiences, family unit, and systems of care. She also highlighted the importance of supporting each patient’s ability to make his or her own decisions and align care with his or her individual preferences. Taylor noted that VA has begun embedding social workers in rural care settings to increase veterans’ access to social work interventions. A recent evaluation found that this program has reduced hospital admissions by 4 percent, reduced ED visits by 3 percent, and increased social work visits by 35 percent (Cornell et al., 2020).
Bevanne Bean-Mayberry of the VA Center for the Study of Healthcare Innovation, Implementation and Policy within the Health Services Research and Development Service reviewed the historical role of women in the military and the health needs of women veterans. In 2015, women accounted for approximately 16 percent of active duty forces and 19 percent of military reserves, and approximately 500,000 women veterans received health care through VA (National Center for Veterans Analysis and Statistics, 2017). While the largest proportion of women veterans are between the ages of 45 and 64, there has been an almost three-fold increase in women veterans between the ages of 18 and 34 (Frayne et al., 2018). Bean-Mayberry noted that individuals in this age range will potentially be VA patients for much of their life spans. The VA Office of Women’s Health Services has responded to this influx of patients by hiring primary care clinicians with expertise in women’s health and by training current clinicians on women’s health issues. Evaluations have found that women veterans treated by primary care providers who focus on women’s health report greater satisfaction with their clinicians (Bastian et al., 2014) and are more likely to receive age-appropriate cancer screenings (Bean-Mayberry et al., 2015) than women veterans treated by traditional primary care providers.
Evelyn Chang of the VA Greater Los Angeles Healthcare System noted that veterans with complex medical conditions, characterized by multiple chronic illnesses and intense use of medical and mental health care services, also
have unique needs for health care access. Both within and outside VA, 5 percent of patients account for approximately half of all health care expenditures (Zulman et al., 2015). Chang noted that these patients often have high unmet medical needs and often lack access to trusted clinicians. She described the results of a VA intervention to offer intensive case management to patients at high risk of hospitalization. Patients randomized to participate in the program reported greater trust in their VA clinicians, indicating that improving access to health services can improve patient–clinician relationships (Zulman et al., 2019). Chang stated that mistrust in health care is often rooted in access problems (Kizer and Jha, 2014) and that low-cost contact such as returning a phone call or responding to an email in a timely manner allows patients to feel more connected with the VA system and helps build trust in their medical team.
FINAL THOUGHTS
Offering a veteran’s perspective, Atizado stated that VA health care is an earned benefit, and it must reflect veterans’ needs, preferences, and values. This sentiment was echoed by several other speakers throughout the workshop. Pryor added that veterans’ voices are key to improving access and should serve as the foundation of any intervention. Several speakers highlighted the progress that VA has made in optimizing access but noted that there is still work to be done to address residual barriers. Participants also highlighted the potential of virtual care to improve access and emphasized the importance of providing the right care in the right way at the right time. Individual participants made suggestions for conceptualization and measurement of access, as well as strategies to improve access (see Box 2). Pryor concluded the workshop by stating
There is no current system like this anywhere in the world, and the lessons learned in VA would be broadly applicable to health care everywhere. In the final analysis, such a system is what our veterans have earned, and what we all want for ourselves and families. ◆◆◆
REFERENCES
Andersen, R. M., P. L. Davidson, and S. E. Baumeister. 2013. Improving access to care. In Changing the US health care system: Key issues in health services policy and management, edited by G. F. Kominski. San Francisco, CA: John Wiley & Sons. Pp. 33–70.
Bastian, L. A., M. Trentalange, T. E. Murphy, C. Brandt, B. Bean-Mayberry, N. C. Maisel, S. M. Wright, V. S. Gaetano, H. Allore, M. Skanderson, and E. Reyes-Harvey. 2014. Association between women veterans’ experiences with VA outpatient health care and designation as a women’s health provider in primary care clinics. Women’s Health Issues 24(6):605–612.
Bean-Mayberry, B., L. Bastian, M. Trentalange, T. E. Murphy, M. Skanderson, H. Allore, E. Reyes-Harvey, N. C. Maisel, V. Gaetano, S. Wright, S. Haskell, and C. Brandt. 2015. Associations between provider designation and female-specific cancer screening in women veterans. Medical Care 53(4 Suppl 1):S47–S54.
Blunt, I., M. Bardsley, and J. Dixon. 2010. Trends in emergency admissions in England 2004–2009. https://www.nuffieldtrust.org.uk/files/2017-01/trends-emergency-admissions-report-web-final.pdf (accessed August 4, 2020).
Cornell, P. Y., C. W. Halladay, J. Ader, J. Halaszynski, M. Hogue, C. E. McClain, J. W. Silva, L. D. Taylor, and J. L. Rudolph. 2020. Embedding social workers in Veterans Health Administration primary care teams reduces emergency department visits. Health Affairs 39(4):603–612.
Donabedian, A. 1980. The definition of quality and approached to its assessment. Ann Arbor, MI: Health Administration Press.
Fortney, J. C., J. F. Burgess, H. B. Bosworth, B. M. Booth, and P. J. Kaboli. 2011. A re-conceptualization of access for 21st century healthcare. Journal of General Internal Medicine 26(2):639.
Frayne, S. M., C. S. Phibbs, F. Saechao, S. A. Friedman, J. G. Shaw, Y. Romodan, E. Berg, J. Lee, L. Ananth, S. Iqbal, P. M. Hayes, and S. Haskell. 2018. Sourcebook: Women veterans in the Veterans Health Administration: Volume 4: Longitudinal trends in sociodemographics, utilization, health profile, and geographic distribution. https://www.womenshealth.va.gov/WOMENSHEALTH/docs/WHS_Sourcebook_Vol-IV_508c.pdf (accessed September 10, 2020).
Gelberg, L., R. M. Andersen, and B. D. Leake. 2000. The behavioral model for vulnerable populations: Application to medical care use and outcomes for homeless people. Health Services Research 34(6):1273–1302.
Heyworth, L., S. Kirsh, D. Zulman, J. M. Ferguson, and K. W. Kizer. 2020. Expanding access through virtual care: The VA’s early experience with COVID-19. New England Journal of Medicine Catalyst 1(4).
Kizer, K. W., and A. K. Jha. 2014. Restoring trust in VA health care. New England Journal of Medicine 371(4):295–297.
Lloyd, R. 2004. Quality health care: A guide to developing and using indicators. Sudbury, MA: Jones & Bartlett Learning.
National Center for Veterans Analysis and Statistics. 2017. Women veterans report: The past, present, and future of women veterans. https://www.spokane.va.gov/docs/VAReport_AmericasWomenVeterans.pdf (accessed September 10, 2020).
Newbould, J., G. Abel, S. Ball, J. Corbett, M. Elliott, J. Exley, A. Martin, C. Saunders, E. Wilson, E. Winpenny, M. Yang, and M. Roland. 2017. Evaluation of telephone first approach to demand management in English general practice: Observational study. BMJ 358:j4197.
NHS (National Health Service). 2020. GP patient survey. http://www.gp-patient.co.uk (accessed August 28, 2020).
Penchansky, R., and J. W. Thomas. 1981. The concept of access: Definition and relationship to consumer satisfaction. Medical Care 19(2):127–140.
Pyne, J. M. U., P. A. Kelly, E. P. Fischer, C. J. Miller, P. Wright, K. Zamora, C. J. Koenig, R. Stanley, K. Seal, and J. C. Fortney. 2019. Development of a perceived access inventory for community care mental healthcare services for veterans. Military Medicine 184(7–8):e301–e308.
Roland, M., M. Elliott, G. Lyratzopoulos, J. Barbiere, R. A. Parker, P. Smith, P. Bower, and J. Campbell. 2009. Reliability of patient responses in pay for performance schemes: Analysis of national General Practitioner Patient Survey data in England. BMJ 339:b3851.
Soh, M., A. Shaner, L. Gelberg, K. Kopelson, M. Stuber, D. Fessler, and C. Warde. 2018. Using the Humanism Pocket Tool for patients with challenging behaviors. Annals of Family Medicine 16(5):467.
U.S. Census Bureau. 2017. Today, 1 in 12 veterans are women. https://www.census.gov/library/visualizations/2017/comm/cb17-ff03_women_veterans.html (accessed August 31, 2020).
VA (U.S. Department of Veterans Affairs). 2019. About VHA. https://www.va.gov/health/aboutvha.asp#:~:text=The%20Veterans%20Health%20Administration%20(VHA,Veterans%20enrolled%20in%20the%20VA (accessed August 31, 2020).
VA. 2020. Rural veterans. https://www.ruralhealth.va.gov/aboutus/ruralvets.asp (accessed August 31, 2020).
WHO (World Health Organization). 2010. Telemedicine: Opportunities and developments in member states. Report on the second global survey for eHealth. https://www.who.int/goe/publications/goe_telemedicine_2010.pdf (accessed August 20, 2020).
Zulman, D. M., C. P. Chee, T. H. Wagner, J. Yoon, D. M. Cohen, T. H. Holmes, C. Ritchie, and S. M. Asch. 2015. Multimorbidity and healthcare utilisation among high-cost patients in the US Veterans Affairs Health Care System. BMJ Open 5(4).
Zulman, D. M., E. T. Chang, A. Wong, J. Yoon, S. E. Stockdale, M. K. Ong, L. V. Rubenstein, and S. M. Asch. 2019. Effects of intensive primary care on high-need patient experiences: Survey findings from a Veterans Affairs randomized quality improvement trial. Journal of General Internal Medicine 34(1):75–81.
DISCLAIMER: This Proceedings of a Workshop—in Brief was prepared by Megan Snair, Emily Zevon, and Cyndi Trang as a factual summary of what occurred at the workshop. The statements made are those of the rapporteurs or individual workshop participants and do not necessarily represent the views of all workshop participants; the planning committee; or the National Academies of Sciences, Engineering, and Medicine.
*The National Academies of Sciences, Engineering, and Medicine’s planning committees are solely responsible for organizing the workshop, identifying topics, and choosing speakers. The responsibility for the published Proceedings of a Workshop—in Brief rests with the rapporteurs and the institution.
The members of the planning committee are Kenneth W. Kizer (Chair), Atlas Research; Adrian Atizado, Veteran Advocate; David Au, University of Washington and U.S. Department of Veterans Affairs; Andrew Bindman, University of California, San Francisco; Joseph Kimura, Atrius Health; Timi Leslie, BluePath Health; Mark Murray, Mark Murray and Associates; Lisa Rubenstein, RAND Corporation and University of California, Los Angeles; Jeannette South-Paul, University of Pittsburgh School of Medicine; and Heather Young, University of California, Davis.
REVIEWERS: To ensure that it meets institutional standards for quality and objectivity, this Proceedings of a Workshop—in Brief was reviewed by Adrian Atizado, Veteran Advocate, and Lillian Gelberg, University of California, Los Angeles, and VA Greater Los Angeles Healthcare System. Lauren Shern, National Academies of Sciences, Engineering, and Medicine, served as the review coordinator.
STAFF: Emily Zevon, Cyndi Trang, Carol Sandoval, and Sharyl Nass, Board on Health Care Services, Health and Medicine Division, National Academies of Sciences, Engineering, and Medicine
SPONSOR: This workshop was supported by the U.S. Department of Veterans Affairs.
For additional information regarding the workshop, visit https://www.nationalacademies.org/event/07-09-2020/developing-a-patient-centered-approach-to-optimizing-veterans-access-to-health-care-services-a-workshop.
Suggested citation: National Academies of Sciences, Engineering, and Medicine. 2020. Developing a patient-centered approach to optimizing veterans’ access to health care services: Proceedings of a workshop—in brief. Washington, DC: The National Academies Press. https://doi.org/10.17226/25935.
Health and Medicine Division
![]()
Copyright 2020 by the National Academy of Sciences. All rights reserved.









