
INTRODUCTION
Psychosocial and behavioral interventions represent a fundamental component of a comprehensive and effective national strategy to promote sexual health and prevent and control sexually transmitted infections (STIs). Such interventions aim to change individual behavior (e.g., promote condom use) or group interactions (e.g., parent–adolescent communication about STI prevention) to reduce morbidity and mortality (e.g., STI incidence). These interventions’ important contributions to promote sexual health and prevent and control STIs can be categorized as having three distinct types of influence: (1) direct effects on reductions in STI incidence (Globerman et al., 2017; Long et al., 2016); (2) direct effects on behavioral outcomes associated with STI risk (e.g., reduced condomless sex) (De Vasconcelos et al., 2018; Globerman et al., 2017); and (3) synergistic effects between these interventions and structural, biomedical, or health service interventions that improve STI prevention or control (e.g., improved uptake of human papillomavirus vaccines; improved STI testing) (Long et al., 2016; Walling et al., 2016) (see the report conceptual framework in Chapter 1).
Considerable empirical research demonstrates that psychosocial and behavioral interventions are efficacious and effective in preventing and reducing STIs and/or sexual risk behaviors associated with greater likelihood of STI acquisition (e.g., condomless sex). Evidence-based
interventions have targeted diverse populations, including ethnic, racial, and sexual minorities, across the life span (De Vasconcelos et al., 2018). Additionally, such interventions’ effects on STI and sexual risk behavior outcomes have been reported across intervention levels (e.g., individual, family, social and sexual networks, community), delivery settings (e.g., schools, primary care), and delivery modalities (e.g., individual face-to-face, group, telephone, online). These interventions also impact STI outcomes and associated risk factors across varying levels of dosage (e.g., single versus multiple sessions) and interventions.
Because of the synergistic effects with biomedical interventions (Walling et al., 2016), psychosocial and behavioral interventions are necessary to optimize the effectiveness of biomedical strategies for STI prevention and control and vice versa (Padian et al., 2008). For example, interventions that target social and behavioral factors associated with sexual health decision making and behaviors can improve the uptake and sustainment or adherence of biomedical strategies for STI prevention and control (Brown et al., 2017). With respect to HIV, although pre-exposure prophylaxis has been found to be effective in prevention (Pinto et al., 2018), adherence rates are less than optimal when not coupled with psychosocial and behavioral intervention strategies. Despite strong evidence for the utility of psychosocial and behavioral interventions, scale-up and widespread dissemination is absent (Hanley et al., 2010). Thus, evidence-based interventions need to be scaled up and new interventions developed to address the increasing rates of STIs in the United States.
This chapter discusses the extant literature on psychosocial and behavioral STI interventions using five organizing themes. First, the chapter provides an overview of psychosocial and behavioral theories and conceptual models that commonly inform the development of these interventions. Second, the chapter offers an overview of interventions at the individual, interpersonal, and community levels, with attention to various key groups. Consistent with the report’s social ecological framework for sexual health promotion and STI prevention, the highlighted interventions target factors across all levels of the social ecology—from individual to community and across the life span. See Chapter 9 for interventions targeting structural factors. Given the significant number of meta-analyses and systematic reviews and of registries listing evidence-based psychosocial and behavioral interventions (e.g., the Centers for Disease Control and Prevention’s [CDC’s] Compendium of Evidence-Based Interventions) (CDC, 2020a), this chapter does not include a comprehensive review of them. Instead, it provides an overview of individual-, interpersonal-, and community-level interventions, including successes, gaps, lessons learned, and future directions. A summary lists key findings from meta-analyses for priority populations. The third section offers
an overview of technological interventions and considerations for how and why technology has become an essential part of all STI intervention campaigns. Fourth, the chapter raises programmatic considerations for promoting, accelerating, and sustaining the scale-up of existing and new psychosocial and behavioral STI interventions in practice settings. Fifth, implementation science is discussed in terms of outcomes, strategies, and study designs to consider in sexual health and promotion interventions. Finally, the chapter offers conclusions and recommendations for future directions.
CONTRIBUTIONS OF PSYCHOSOCIAL AND BEHAVIORAL INTERVENTIONS ON STI PREVENTION AND CONTROL
Psychosocial and Behavioral Theories and Conceptual Models
Psychosocial and behavioral theories and conceptual models of health and behavior change have guided the development of interventions to prevent STIs and reduce associated health risk behaviors. Below is a summary of commonly used theories and conceptual models.
Health Belief Model
The Health Belief Model postulates that individuals will take action to prevent illness if they believe they are susceptible, if the consequences are severe, and if the benefits of action outweigh the costs (Janz and Becker, 1984). As it pertains to preventing health conditions, such as STIs, this model is useful for predicting why people will take action to prevent, screen, or seek treatment for symptoms (Champion and Skinner, 2008).
Theory of Reasoned Action
The Theory of Reasoned Action (Ajzen and Fishbein, 1980; Fishbein and Ajzen, 1975) and its later evolution the Theory of Planned Behavior (Ajzen, 1991) focus on motivational factors that determine the likelihood of engaging in a particular behavior, such as condomless sex. The Theory of Reasoned Action assumes that the most important determinant of a behavior is a person’s intention to enact it. Behavioral intention includes attitudes toward performing the behavior and subjective norms associated with it. The attitudinal component consists of a set of beliefs regarding the behavior’s value and its consequences. For example, condom use attitude is more favorable when the consequences of using them are valued (e.g., preventing STIs) and the benefits of their use are viewed
as a positive aspect of the sexual encounter (Conner and Norman, 2005; Espada et al., 2016). The Theory of Planned Behavior added the construct of perceived control over the behavior, which takes into account situations where a person may not have complete volitional control, such as through a gender power imbalance that prevents condom use negotiations (Montano and Kasprzyk, 2015).
Social Cognitive Theory
Social cognitive theory asserts that information alone about a particular outcome or behavior does not necessarily influence or change a behavior; instead, people need to be provided not only reasons for adopting or changing a behavior, but also the requisite means, resources and social supports, and skills to do so (Bandura, 1986). It posits that behavior is determined by reciprocal and continuous interactions of cognitive, behavioral, and environmental influences and emphasizes people’s potential abilities to alter and construct their environment to fit their desired goals (Bandura, 1986, 1994; Espada et al., 2016; McAlister et al., 2008). Specifically, the cognitive influences reflect confidence in the ability to perform a task or accomplish a particular goal (e.g., perceived self-efficacy to correctly use condoms); behavioral influences include consequences of a particular behavior and the likelihood of correctly performing the behavior by developing new skills (e.g., communication skills to effectively negotiate condom use), and environmental influences involve opportunities for learning or enacting a behavior through interpersonal or social modeling (e.g., adolescents are more likely to use condoms if they perceive that their friends do so) (Bandura, 2011; Espada et al., 2016; McAlister et al., 2008).
Social Ecological Theory
The social ecological theory describes the multiple and interrelated influences on STIs and associated behaviors (Bronfenbrenner, 1979, 1986). It is organized by multiple influences (e.g., structural, environmental, social) according to proximity, from furthest to closest to the individual: macrosystems (the broad social and philosophical ideals that define a particular society or culture); exosystems (contexts in which the individual does not participate directly but that impact important members of the individual’s life); mesosystems (contexts that comprise the interactions between important members of the different contexts in which the individual participates directly); and microsystems (contexts in which the individual participates directly).
Cognitive-Affective Dual Process Models
Cognitive-affective dual process models have been proposed as an alternative to traditional theories of behavior change (Bauermeister et al., 2019; Gerrard et al., 2008). These models take into account affective motivations (e.g., emotions), in addition to the cognitive factors usually considered in behavioral theories, that may impact decision making and behavior change (Bauermeister et al., 2019; Gerrard et al., 2008). Affective motivators can function as both risk and protective factors.
Integrative Theoretical Models
Building on these frameworks, a number of integrative theoretical models that were primarily developed to examine constructs associated with HIV have been adapted to STIs and related risk and protective factors in adolescents (e.g., Bangi et al., 2013; Boyer et al., 1999, 2000; Champion et al., 2013; Dolcini et al., 2010; Fisher et al., 1999; Johnson, 2011), including the AIDS Risk Reduction Model (ARRM) and the Information Motivation Behavior (IMB) model.
The ARRM is a conceptual framework for organizing factors known to influence behavior change into classification categories for people (Catania et al., 1990). The ARRM integrates elements of the Health Belief Model (Janz and Becker, 1984), efficacy theory (Bandura, 1977), emotional influences (Leventhal, 1973), and interpersonal processes (Rogers, 1983). The ARRM involves three stages: (1) recognizing and labeling one’s behavior as high risk for infection, (2) making a commitment to change one’s behavior to reduce risk and adopt safer practices, and (3) enacting change by seeking solutions and adopting behaviors that decrease STI risk. Individuals may progress through certain stages, regress to a previous stage, and move back and forth between stages before behavior change is sustained (Catania et al., 1990). Specifically, in the labeling stage, knowledge of STI risk and transmission and beliefs that one is vulnerable to acquiring STIs are proposed determinants for labeling a behavior as risky (Boyer et al., 1999). Factors involved in making a commitment to change behaviors associated with risk for STIs include perceived self-efficacy, perceived peer norms, and adverse emotional states, such as anxiety (Zimmerman et al., 2007). Finally, behavior change (e.g., condom use or other risk prevention strategies) is determined by individual characteristics (e.g., previous behaviors) and perceived social support for engaging in health-promoting behaviors (Logan et al., 2002).
The IMB model is another framework that has been widely used to characterize STI risk and prevention (Fisher and Fisher, 1992; Fisher et al., 1994). Specifically, it integrates constructs from the Theory of Reasoned Action (Ajzen and Fishbein, 1980; Fishbein and Ajzen, 1975), efficacy
theory (Bandura, 1977), and the Health Belief Model (Janz and Becker, 1984). It posits that information, motivation, and behavioral skills are the primary determinants of STI-preventive behavior. Specifically, the model asserts that information regarding STI transmission and prevention is a necessary prerequisite of risk-reduction behavior (Rotheram-Borus et al., 2009). Motivation (psychosocial factors) to change risk behaviors is a determinant of prevention and affects whether a person acts on such knowledge. The IMB also asserts that motivation to engage in preventive behaviors is a function of a person’s attitudes toward and perceived peer norms about them. Other critical factors hypothesized to influence motivation to engage in STI-preventive behaviors are perceived vulnerability to STIs and intention to enact the behaviors. The necessary skills for specific preventive behaviors are the third determinant and affect whether even a knowledgeable, highly motivated person will be able to do so (Rotheram-Borus et al., 2009). These skills include the abilities to communicate effectively with sexual partners about safer sex, competence to engage in condomless sexual practices, and the ability to properly use condoms. Individuals who practice preventive skills are also presumed to have a strong self-belief (self-efficacy) in their ability to do so. Limits of IMB include its relative lower emphasis on environmental- or structural-level barriers to behavior change, social and community support, and maintenance across time (Rotheram-Borus et al., 2009).
The following sections provide an overview of psychosocial and behavioral interventions at the individual, interpersonal, and community levels that use these theories and models (see Box 8-1 for definitions of key terms used in the remainder of the chapter).
PSYCHOSOCIAL AND BEHAVIORAL INTERVENTIONS
As described previously in the committee’s conceptual framework (see Figure 1-3), STI risks are influenced by individual, interpersonal, and community-level factors. Interventions that target factors across multiple levels and delivery systems (e.g., schools, clinics, places of worship) increase their impact on preventing and reducing STIs and related outcomes, including condomless sex (DiClemente et al., 2008; Estrada et al., 2017; Guilamo-Ramos et al., 2020). This section provides a brief overview of STI behavioral multi-level interventions, followed by a summary of meta-analyses highlighting key findings for priority populations.
INDIVIDUAL-LEVEL INTERVENTIONS
Research seeking to understand and shape the determinants of sexual decision making and behavior emerged as a growing discipline during
the 1970s, as federal and private funders identified developing programs to reduce teen pregnancy as a national public health and social welfare priority (NRC, 1987). While these early sexual and reproductive health intervention programs were designed to promote behaviors associated with reduced STI risk among adolescents, such as delay of sexual debut, preventing sexual transmission of infection was not a primary target outcome. This focus shifted during the early years of the HIV pandemic
in the 1980s, with increasing recognition of the need for psychosocial and behavioral prevention interventions to target additional key populations at increased risk of STI and HIV infection (Rietmeijer and Scahill, 2012). A growing number of evidence-based individual-level behavioral counseling interventions grounded in rigorous decision and behavioral science began to emerge in the 1990s, and individual-level interventions became a cornerstone of national STI prevention efforts (Rietmeijer and Scahill,
2012). Today, the efficacy/effectiveness of individual-level psychosocial and behavioral interventions for STI prevention is well supported by empirical evidence (Covey et al., 2016; Crepaz et al., 2009; De Vasconcelos et al., 2018; Eaton et al., 2012; Morales et al., 2018). Most recently, in an updated evidence report and systematic review, the United States Preventive Services Task Force concluded that behavioral counseling interventions were effective in reducing both STI incidence and behavioral outcomes associated with STI risk, including condomless sex (Henderson et al., 2020). This review, which included 39 studies, showed that most interventions were conducted in STI clinics, general primary care, obstetrics and gynecology, women’s health clinics, adolescent medicine, and family planning clinics. Of these studies, 9 consisted of interventions with less than 30 minutes (low contact), 13 studies had interventions of 30–120 minutes (moderate contact), and about 50 percent of studies offered more than 2 hours of intervention (high contact). Motivational interviewing was the most commonly used approach, followed by cognitive behavioral therapy. Group counseling was the most frequently used intervention component, often in tandem with other components, such as individual counseling videos or phone calls. Of the studies that reported on effectiveness for STI prevention, the findings indicated a statistically significant effect, with most reports occurring between 6 and 12 months. Greater effect sizes were found for studies with adolescents, high-contact interventions, or group counseling sessions. Studies with adolescent boys, men (including gay, bisexual, same gender loving, and other men who have sex with men [MSM]), and populations with average risk levels were not well represented. Studies reporting behavioral outcomes (34 studies [e.g., condom use, condomless sex, number of sexual partners]), consisting of individuals at high risk for STIs, had effects on behavioral outcomes, although the effects diminished in studies with follow-ups greater than 1 year (Henderson et al., 2020).
Incorporating important shared principles and characteristics of these effective existing interventions into the development of future STI prevention programs represents a meaningful step toward strengthening sexual health promotion in the United States. The following section discusses three lessons learned from existing effective individual-level behavioral STI prevention interventions: the importance of (1) a strong theoretical basis to the content, (2) delivery mechanisms that are aligned with theoretically identified mediators of intervention effects, and (3) population- and context-specific tailoring (Guilamo-Ramos et al., 2019). Finally, a review of the extant literature on individual-level sexual education programs delivered in school-based settings in the United States is provided.
Theoretical Basis and Content
Most individual-level STI prevention interventions are based on psychosocial and behavioral theories (Crepaz et al., 2007, 2009), and meta-analytic reviews found that applying theories of behavior in content development enhanced the efficacy/effectiveness of the interventions (Covey et al., 2016). Specifically, using a psychosocial and behavioral theory in intervention development has been identified as one of the most important moderators of efficacy/effectiveness (Covey et al., 2016). Beyond using theory to inform intervention development in general, formative research that explores the relative importance of theoretically identified mediators for predicting target behaviors has utility to inform intervention content that specifically addresses the individual-level determinants of behavior (Covey et al., 2016).
Intervention Delivery Mechanisms
Individual-level STI psychosocial and behavioral interventions are heterogeneous in modes of content delivery, delivery setting, and session format (Henderson et al., 2020). In general, strong evidence is absent to support specific delivery mechanisms as increasing efficacy/effectiveness (Covey et al., 2016; Henderson et al., 2020). Yet, the importance of aligning intervention delivery mechanisms with theoretically identified mediators of intervention effects has been discussed (Guilamo-Ramos et al., 2019). Selecting delivery mechanisms that are best suited to address the hypothesized pathways through which the intervention shapes the target outcome can amplify the effect of theoretically informed intervention content (Guilamo-Ramos et al., 2019). Therefore, empirical formative research that increases the understanding of hypothesized mediators of intervention effects also represents an opportunity to inform the selection of intervention delivery mechanisms (Guilamo-Ramos et al., 2019).
Population and Context-Specific Tailoring
Tailoring STI psychosocial and behavioral interventions is associated with efficacy/effectiveness (Covey et al., 2016; Crepaz et al., 2009). It involves specifically designing or adapting interventions for a particular key population at increased risk of STIs, such as racial and ethnic minority adolescents and women or STI clinic patients, by considering and addressing population- and context-specific facilitators and barriers of intervention effectiveness in both content and delivery. For example, in a review of meta-analytic evidence, psychosocial and behavioral interventions delivered by a facilitator who matched the target population in race/ethnicity and gender showed better efficacy/effectiveness than
interventions that did not (Covey et al., 2016). Another meta-analysis found improved efficacy/effectiveness for interventions that included content addressing cultural factors specific to the target population (Crepaz et al., 2009). Furthermore, interventions had increased efficacy when they targeted developmentally appropriate outcomes, such as condom use among older adolescents who are more likely to be sexually active, as compared to young adolescents (Henderson et al., 2020). In addition, tailoring can address important aspects of cultural and linguistic appropriateness of individual-level psychosocial and behavioral interventions (Escoffery et al., 2018) and considering contextual feasibility constraints during development or adaptation facilitates adoption at scale (Guilamo-Ramos et al., 2004).
Incorporating lessons learned from decades of successful intervention science into the development of future STI prevention programs represents a meaningful step toward strengthening sexual health promotion in the United States and also can be leveraged to improve school-based sexual education (Rankin et al., 2016).
Sexual Education
Existing evidence evaluating the efficacy and/or effectiveness of sexual education programs in preventing STIs among adolescents have focused on two distinct approaches: abstinence-only education and comprehensive sexual education (Chin et al., 2012; Lugo-Gil et al., 2016; Santelli et al., 2017). This section reviews the evidence regarding (1) abstinence-only and comprehensive sexual education programs, (2) gaps in the literature, and (3) the state of sexual education in the United States today.
Abstinence-only education, also referred to as AOUM or sexual risk avoidance programs (see Table 8-1), instructs students that the only morally acceptable option for youth, and the only safe and effective way to prevent unintended pregnancies and STIs, is abstinence from sexual activity (KFF, 2018; Santelli et al., 2017). It does not educate youth about effective use of contraception or condoms and only discusses these to highlight their failure rates (Santelli et al., 2017). In contrast, comprehensive sexual education programs typically include medically accurate, evidence-based information about both contraception and abstinence to prevent pregnancy and promote condom use to forestall STI transmission (KFF, 2018; Miedema et al., 2020; Santelli et al., 2017). Abstinence-only programs have not been found to be effective in reducing adolescent sexual risk behaviors or STI rates (Chin et al., 2012; Hogben et al., 2010; Trenholm et al., 2008); adolescents who participate in them are more likely than those who received comprehensive sex education to be unaware of their STI status and engage in condomless sex (Brückner and Bearman, 2005; Shepherd
TABLE 8-1 Types of Sexual Health Education Programs
| Types of Sexual Education Programs | |
|---|---|
| Abstinence-Only Education | Education that emphasizes the importance of delaying sex and excludes content regarding contraception and barrier methods in preventing sexually transmitted infections (STIs) and/or unplanned pregnancies. This has also been referred to as “sexual risk avoidance” education. |
| Abstinence-Only Until Marriage Education | Content that strictly defines sexual intercourse in the context of marriage, stressing the importance of abstaining from sex until after marriage for moral and/or religious reasons. |
| Abstinence “Plus” Education | Education on the importance of abstinence in tandem with information on barrier and contraceptive methods in preventing STIs and unplanned pregnancies. This has also been referred to as “sexual risk reduction” education. |
| Comprehensive Sex Education | The provision of medically accurate, developmentally appropriate information on abstinence and safe sex practices, including barrier and contraceptive methods, in preventing STIs and unplanned pregnancies. Such programs also offer information regarding the importance of healthy relationships, communication skills, and developmental considerations, as well as other topics. |
SOURCE: Adapted from KFF, 2018.
et al., 2017). Furthermore, analyses have indicated that states with mandates for abstinence-only education had among the highest gonorrhea and chlamydia rates (Carr and Packham, 2017; Hogben et al., 2010). These programs’ lack of effectiveness has been tied to including content that is medically inaccurate, developmentally inappropriate, heteronormative, and stigmatizing (Santelli et al., 2017).
Comprehensive sexual education, also referred to as “abstinence plus” or “sexual risk reduction,” promotes abstinence as the primary approach to prevent STIs but also encourages sexually active adolescents to use available barrier and contraceptive methods (Denford et al., 2017; Santelli et al., 2017). Adolescents who participate in such programs delay initiating sexual behavior, have increased knowledge of STI risks and consequences, and report enhanced contraceptive use (Chin et al., 2012; Denford et al., 2017; Kirby, 2007; Lopez et al., 2016; Santelli et al., 2017; Underhill et al., 2007). In addition, evidence suggests that comprehensive sexual education programs and medically accurate programs are effective in reducing STI prevalence among adolescents (Chin et al., 2012) and have been efficacious in delaying sexual debut among young adolescents (Guilamo-Ramos et al., 2011).
Having school nurses deliver comprehensive sexual education to parents represents a novel approach in school-based settings that warrants additional attention. The vast majority of U.S. individuals, including parents, supports comprehensive sexual education delivery in school settings (Cameron et al., 2020; Santelli et al., 2017). Parents are cited as having the most significant influence in shaping adolescent sexual decision making (Power to Decide, 2016), yet they frequently identify their lack of sexual health expertise as the primary reason that schools need to provide comprehensive content and resources (Johnson-Motoyama et al., 2016). Despite parents’ important role, schools primarily deliver sexual education in the classroom directly to adolescents, often neglecting to include parents for reasons unrelated to parental consent (Denford et al., 2017). Successfully including parents in designing and delivering sexual education programs takes into account the perspectives and specific needs of families, including consideration of time limitations, tailoring of program content to local epidemiological context, and flexibility in program delivery (Smokowski et al., 2018). Furthermore, comprehensive sexual education programs, such as Families Talking Together, delivered to parents in school settings have been efficacious in shaping multiple adolescent outcomes, including delay of sexual debut (Guilamo-Ramos et al., 2011).
Nurses in school-based health clinics represent an important opportunity for enhancing existing sexual education programs. They have been rated consistently as a trusted source of information (Reinhart, 2020) and have training that enables them to provide STI testing, treatment, contraception, including condoms, and specific guidance to adolescents in such clinics. Nurse-led psychosocial and behavioral interventions have been associated with increased uptake of STI testing and contraception in school-based health centers (Brigham et al., 2020; Ethier et al., 2011). Despite significant progress in expanding these centers in the past decade, only 1 in 10 (10.4 percent) of U.S. schools has one (Love et al., 2018, 2019).
Research with school staff, parents, and adolescents has explored facilitators of and barriers to implementation of sexual education in U.S. schools (Eisenberg et al., 2013; Kocsis, 2020; Peskin et al., 2011; Thompson, 2020), including sexual education delivered by school nurses (Brewin et al., 2014). Important barriers to sexual education that emerged from the literature include restrictions imposed by state legislature, school boards, or administrators; educator concerns regarding criticism from parents and administrators; inadequate funding, resources, and lack of sexual education curricula; inadequate self-efficacy for delivery of sexual education among educators (i.e., inadequate preparation and training); and religiosity (Brewin et al., 2014; Eisenberg et al., 2013; Peskin et al., 2011). In contrast, training, experience, and comfort in delivery of sexual
education among educators; adequate prioritization and time allocation to sexual education in curricula; parent advocates; community engagement; perceived support from administrators and outside stakeholders, such as parents and community leaders; and parental and public health professional involvement in sex education content development have been identified as facilitators of implementing sexual education (Brewin et al., 2014; Kocsis, 2020; Peskin et al., 2011). These facilitators can be leveraged to improve sexual education in U.S. schools.
According to the Guttmacher Institute, sexual health education across the United States is variable (Guttmacher Institute, 2020) (see Table 8-2). While 39 states and Washington, DC, require sexual and/or HIV education in the classroom, less than half of all states (17 states) require medical accuracy of sexual health education content or content on contraception (Guttmacher Institute, 2020). Furthermore, no consistent nationwide policy exists for teaching sexual education in schools, resulting in wide variation by state (Hall et al., 2016; Santelli et al., 2017). States typically pass laws that offer broad guidelines but do not require that sex education be taught or offered (Hall et al., 2016). While state, districts, and school boards set standards and requirements for sexual health education, the adopted approach varies by school district and often even by school (Hall et al., 2016). According to CDC’s School Health Profiles 2018, only about half of U.S. middle and high schools teach all 20 CDC-recommended sexual health topics (CDC, 2019b). Moreover, approximately one-third of federal funding for sexual education programs each year is for abstinence-only education (KFF, 2018). Allocated federal funding to schools from the Title V AOUM program cannot be used to educate adolescents regarding barrier or contraceptive methods (Santelli et al., 2017). In sum, school-based comprehensive sexual health education programs that seek to meaningfully involve parents are sorely needed. Funding for their ongoing development, implementation, and broad uptake represent an overlooked opportunity to reduce STIs among youth in the United States.
INTERPERSONAL-LEVEL INTERVENTIONS
Family-Level Interventions
Family-level psychosocial and behavioral interventions are designed to address challenges affecting the functioning and well-being of individuals and the family system. Specifically, they target risk factors, such as poor family communication, and protective factors, such as family support related to sexual health, STIs, and associated behaviors, including condom use (Guilamo-Ramos et al., 2020; Prado et al., 2007). These interventions may also modify maladaptive interaction patterns (e.g.,
TABLE 8-2 Sex and HIV Education in Schools
| State | Sex and HIV Education | |||
|---|---|---|---|---|
| Mandate Sex and/or HIV Education | Require Sex and HIV Programs to Be Medically Accurate | When Provided, Sex Education Must Include Contraception | When Provided, HIV Education Must Include Condoms | |
| U.S. Total | 39 states and Washington, DC | 17 states and Washington, DC | 20 states and Washington, DC | 19 states |
| Alabama | HIV | X | X | |
| Alaska | ||||
| Arizona | HIV | |||
| Arkansas | HIV | |||
| California | Sex and HIV | X | X | X |
| Colorado | X | X | ||
| Connecticut | HIV | X | ||
| Delaware | Sex and HIV | X | X | |
| DC | Sex and HIV | X | ||
| Florida | Sex and HIV | |||
| Georgia | Sex and HIV | |||
| Hawaii | Sex and HIV | X | X | X |
| Idaho | ||||
| Illinois | HIV | X | X | X |
| Indiana | HIV | |||
| Iowa | Sex and HIV | X | ||
| Kansas | Sex | |||
| Kentucky | Sex and HIV | |||
| Louisiana | X | |||
| Maine | Sex and HIV | X | X | X |
| Maryland | Sex and HIV | X | X | |
| Massachusetts | ||||
| Michigan | HIV | |||
| Minnesota | Sex and HIV | |||
| Mississippia | Sex | |||
| Missouri | HIV | X | ||
| Montana | Sex and HIV | |||
| Nebraska | ||||
| Nevada | Sex and HIV | |||
| State | Sex and HIV Education | |||
|---|---|---|---|---|
| Mandate Sex and/or HIV Education | Require Sex and HIV Programs to Be Medically Accurate | When Provided, Sex Education Must Include Contraception | When Provided, HIV Education Must Include Condoms | |
| New Hampshire | Sex and HIV | |||
| New Jersey | Sex and HIV | X | X | X |
| New Mexico | Sex and HIV | X | X | |
| New York | HIV | |||
| North Carolina | Sex and HIV | X | X | X |
| North Dakota | Sex and HIV | |||
| Ohio | Sex and HIV | |||
| Oklahoma | HIV | HIV | X | |
| Oregon | Sex and HIV | X | X | X |
| Pennsylvania | HIV | |||
| Rhode Island | Sex and HIV | X | X | X |
| South Carolina | Sex and HIV | X | ||
| South Dakota | ||||
| Tennesseeb | Sex and HIV | X | ||
| Texas | Sex and HIV | X | X | |
| Utahc | Sex and HIV | |||
| Vermont | Sex and HIV | X | X | |
| Virginia | Sex and HIV | X | X | |
| Washington | HIV | X | X | |
| West Virginia | Sex and HIV | X | X | |
| Wisconsin | HIV | |||
| Wyoming | ||||
NOTE: Sex education typically includes discussion of sexually transmitted infections (STIs).
a Localities may include topics such as contraception or STIs only with permission from the state Department of Education.
b Sex education is required in a county if pregnancy rate is at least 19.5 or higher per 1,000 young women aged 15–17.
c State also prohibits teachers from responding to students’ spontaneous questions in ways that conflict with law’s requirements, State Laws and Policies, Sex and HIV Education, as of June 1, 2020.
SOURCE: Guttmacher Institute, 2020.
misaligned family hierarchy) within the family system. Family-level interventions are informed by several models, including family systems theory and social ecological theory. For sexual health and preventing STIs, these interventions typically occur during adolescence, generally incorporate the adolescent and parent(s), guardian(s), and, potentially, other extended and nonbiological family members, and commonly use the parent as the agent of change for modifying adolescent behavior.
Researchers and clinicians have recognized the importance of social ecological factors in developing family-level interventions to promote well-being and prevent risk behaviors, including condomless sex (DiClemente et al., 2007; Prado et al., 2009). These factors include not only familial influences, which directly impact the adolescent, but also different levels of the social ecology, such as parental stress. Techniques can include psychoeducation, restructuring of family subsystems, and behavior modification components that are implemented depending on the intervention modality and the needs of the family. Family-level interventions may include various components, such as individual youth and/or parent sessions, parent group sessions, youth group sessions, or a combination. For example, in parent group sessions, parents learn and acquire skills (e.g., effective communication on sexual health, condom use) that are then practiced with youth in individual youth and parent sessions.
Family-level interventions to prevent STIs and behaviors associated with STIs emerged in the late 1990s after the National Institute of Mental Health, the National Institute on Drug Abuse, the National Institute on Alcohol Abuse and Alcoholism, and the National Institute on Aging requested research applications in 1995 for investigators to evaluate “family process interventions to enhance the ability of families to prevent the spread of HIV/AIDS and/or its consequences” (NIH, 1995). Although the funding was aimed at evaluating the efficacy of family interventions in preventing HIV and its consequences in adolescents and adults (across racial and ethnic minority groups), many of these interventions examined and reported on sexual risk behavior outcomes associated with STIs (Pequegnat and Szapocznik, 2000). The literature on family-level intervention has grown considerably since. The resulting body of research, which requires some level of parental or family participation, has documented that preventive interventions targeting the family context have been successful in preventing STIs (DiClemente et al., 2014; Prado et al., 2007), preventing decreases in condom use (Estrada et al., 2017), and increasing condom use (Guilamo-Ramos et al., 2020; Jemmott et al., 1999; Pantin et al., 2009).
Family-level preventive interventions have demonstrated efficacy and effectiveness (Sandler et al., 2014) in a number of populations, including African American adolescents (Jemmott et al., 2020; Sutton et al., 2014), Latino/a people (Estrada et al., 2017; Guilamo-Ramos et al., 2020),
criminally involved populations (Prado et al., 2012; Tolou-Shams et al., 2017), and homeless youth (Rotheram-Borus et al., 1991a,b). One population with little to no attention in the literature is sexual and gender minority youth. Because parental participation is key in family-level interventions and some such youth may not disclose their identity to at least one parent, they may not be able to participate in these interventions.
Family interventions, particularly those where the parent is the agent of change, have long-term sustained effects. For example, interventions delivered in childhood and adolescence affect condom use and STIs in adulthood (Spoth et al., 2015). Family interventions with core components focused on improving parent–child communication, teaching parents the importance of effective and consistent parenting, and requiring parents to practice acquired skills with their youth have the largest effects (Estrada et al., 2017). In fact, in many of the trials demonstrating intervention effects on condom use and STIs, the mechanism of change or mediator has been improvements in parent–adolescent communication, family support, or positive parenting practices (McDade et al., 2019; Prado et al., 2007). Specifically, the literature has demonstrated that immediate improvements in family functioning indicators, such as parent–adolescent communication, impact later outcomes, including condomless sex and STIs. These mediators are the same factors that drive the effects of family interventions developed to address outcomes (e.g., internalizing symptoms) other than STIs or condom use (Jensen et al., 2014). Therefore, it is not surprising that family-level interventions often have crossover effects on several outcomes. Research has shown that family-level interventions that target conduct problems and mental health outcomes have affected sexual health outcomes (Caruthers et al., 2014). Specifically, a brief family-level intervention designed to target adolescent adjustment problems influenced five high-risk sexual behaviors (e.g., condom use and sex with people who were engaging in sex with others) at age 22 (Caruthers et al., 2014). Similarly, Spoth et al. (2014), who delivered a family-centered intervention to reduce early substance use initiation among youth in the sixth grade, showed long-term reductions in high-risk sexual behaviors and STIs at age 21. In both studies, the intervention effects on the sexual health outcomes and/or STIs were mediated by improvements in parent–youth interactions (Caruthers et al., 2014; Spoth et al., 2014). These findings are important and consistent with Syndemic Theory, which posits that social and environmental factors (e.g., effective parent–youth interactions) are not associated with just one health condition but are related to multiple intertwined health outcomes (González-Guarda et al., 2011; Singer et al., 2006). Therefore, psychosocial interventions that have an effect on STIs may also affect substance use and mental health (and vice versa). Additionally, the crossover effects of these family interventions increase their
public health benefits (Reider et al., 2014) and may also substitute for sexual education in communities where implementing it in schools may be challenging or not feasible (Jenkins, 2014). Thus, family interventions that can address multiple risk behaviors or health outcomes may be an effective and cost-efficient strategy to prevent STIs and other adverse health outcomes.
Family interventions have also been found to be efficacious in promoting condom use and preventing STIs among ethnic minority samples at increased risk (Jemmott et al., 2020; Sutton et al., 2014). Interventions that are culturally syntonic to the target population (e.g., for a specific ethnic group) are most efficacious, and the most efficacious family-level interventions have a cultural component (Szapocznik et al., 2007). For example, the Strong African American Families Program, which was specifically developed for African American families, has been efficacious in reducing condomless sex (e.g., Brody et al., 2004). For Hispanic people, family interventions such as Familias Unidas, which focuses on acculturation, acculturative stress, and familismo (central Latino/a cultural value involving dedication, commitment, and loyalty to family), have also prevented decreases in condom use (Estrada et al., 2017) and prevent STIs over time (Prado et al., 2007).
Family-level interventions have been delivered in a variety of settings, including schools (Estrada et al., 2017), places of worship (Jemmott et al., 2020), and primary care (Guilamo-Ramos et al., 2020; Prado et al., 2019). They have recently been tested more often in primary care and pediatric care (IOM, 2014) because these are routinely used by youth and families and often offer a nonstigmatizing setting (Leslie et al., 2016), where they have been found to be efficacious and effective for a wide array of behavioral and health outcomes (Perrin et al., 2014; Reedtz et al., 2011), including sexual health outcomes (Guilamo-Ramos et al., 2020) and STI outcomes (Prado et al., 2007). Despite their efficacy and cost effectiveness (e.g., Spoth et al., 2002), family-level interventions have not been sustained in primary and pediatric care because physicians and other clinic staff do not have the time or resources. Moving in-person interventions online may be one mechanism to sustain them in primary care (Estrada et al., 2019). Future research is needed on how to effectively integrate and sustain family-level interventions in primary care.
Although the efficacy of family-level interventions is well documented, they face several challenges to implementation, including that parental participation is difficult to sustain (Perrino et al., 2000; Spoth et al., 1999). Families with social needs face many barriers to participation (e.g., low income, lack of transportation, child care) (Fernandez and Eyberg, 2009; Spoth et al., 1996). Parent engagement and participation in intervention sessions is as important as adherence to a medication
regimen: lack of either one reduces the benefits (Prado et al., 2006). An important future direction is to refine and evaluate strategies to engage and retain parents. Another challenge is that these interventions often have delayed effects (Estrada et al., 2017). That is, they often do not produce changes in outcomes, such as condomless sex or STIs, for several years. Given that the maximum funding cycle of the National Institutes of Health (NIH), the primary funder for evaluating psychosocial and behavioral interventions, is 5 years and that such evaluation studies need ample preparation time and a dissemination phase, it may be challenging to evaluate the efficacy and effectiveness of family interventions on STI outcomes in a single NIH funding cycle.
Other important gaps in the family intervention literature are a lack of interventions for sexual minority, American Indian, or Alaska Native adolescents to promote sexual health and prevent STIs. Interventions must be developed for these populations. This gap is noteworthy given that Indigenous youth and young adults are at greatest risk for STIs (and currently the highest rate of STIs). Despite these challenges and gaps, family interventions have significant potential to curb the epidemic of STIs and improve sexual health in children, adolescents, and young adults. Future research to address current gaps in family interventions to promote sexual health and to prevent STIs is sorely needed, with adequate resources for development, implementation, and long-term follow-up.
Social Network Interventions
Social networks have been demonstrated to be important in STI transmission (Ellen et al., 2006; Klovdahl et al., 1994; Wylie and Jolly, 2001); therefore, addressing social networks is an important intervention strategy (see Chapter 2 for more on social networks). Network mobilization is an intervention strategy that stimulates peer-to-peer interaction to create and promote peer influence along existing network pathways to impact the members (Valente, 2012). Research has shown that individuals in the same social network are more likely to have similar STI risk potential (Amirkhanian, 2014). As a result, recruiting social contacts in addition to risk contacts, known as the Social Network Strategy (SNS) (Lightfoot et al., 2018; McGoy et al., 2018), has been used with modest results for identifying new HIV infection (Boyer et al., 2013, 2014), and CDC recently promoted it as an effective HIV testing intervention (Lightfoot et al., 2018; McGoy et al., 2018). This strategy identifies individuals with STIs and individuals at risk and asks them to recruit persons from their social network for testing in exchange for an incentive. Some data have indicated SNS to be effective in identifying new HIV infections (Boyer et al., 2013, 2014), showing that a proportion of those tested were
newly diagnosed with HIV or STIs; this is routinely higher than the prevalence found via publicly funded counseling, testing, and referral (Kimbrough et al., 2009).
Building on classical partner services and SNS, the Transmission Reduction Intervention Project conducted network-based recruiting, counseling, and testing in Odessa, Ukraine; Athens, Greece; and Chicago, Illinois. The primary goal was to increase early detection of individuals with recent HIV infections (Schueler et al., 2019). A secondary goal, at the Chicago site only, was to identify additional active syphilis infections (Friedman et al., 2014). A two-step approach (a person who recently seroconverted was followed for two rounds of the study to capture additional contacts who were positive for HIV) was used; network chain recruitment started with “seeds”—people who were recently or long-term HIV positive—and continued no further than two steps from a person living with HIV, repeating the process if another person living with HIV was identified at either the first or second step (Nikolopoulos et al., 2016). The two-step approach was used in order to remain within each individual’s immediate risk network environment; anything beyond this was considered to be too far removed. The project was effective at yielding individuals with active syphilis infection (Morgan et al., 2019; Nikolopoulos et al., 2016). Variations on chain length can be considered, such as three-step partner services (or SNS). Future work to determine the optimal network mobilization strategy following STI outbreaks is a growing area of interest and investigation that follows HIV molecular cluster analyses (Grabowski et al., 2018; Smith et al., 2011).
SNS extends beyond testing and partner notification. Interventions can be used to deliver a curriculum to an individual’s social network. These interventions extend beyond the individual-level interventions because, much like family interventions, social network interventions consider interpersonal factors that contribute to STI risk. In a systematic review and meta-analysis (Hunter et al., 2019), social network interventions showed a significant effect on sexual health outcomes that was consistent across a myriad of populations (e.g., ethnic minorities, MSM). Other reviews (e.g., Wang et al., 2011) have drawn similar conclusions on the efficacy of social network interventions on sexual health outcomes and STI incidence. Such interventions have also been applied online to successfully change sexual health and HIV-related behaviors (Bull et al., 2012; Young et al., 2014). Because of the large and growing impact that online tools have on people’s behaviors, interventions that leverage online social influencers will be increasingly important for promoting sexual health.
Challenges in implementing and evaluating social network interventions include the potential contamination in social network intervention studies (particularly in networks that are highly connected), where
participants randomized to the experimental intervention may also receive the control condition (and vice versa) (see, e.g., Schneider et al., 2021). Additionally, social network intervention studies require the index participant to recruit a network of their peers and disseminate the intervention to their network. Notwithstanding these challenges, social network interventions are efficacious and may also facilitate the diffusion of other efficacious and effective interventions (Kanamori et al., 2019).
COMMUNITY-LEVEL INTERVENTIONS
Community interventions are effective public health tools for reducing health disparities in large geographic locations, such as entire cities or neighborhoods, or smaller entities within communities, such as schools, faith institutions, or workplaces (Merzel and D’Afflitti, 2003; Trickett et al., 2011). This approach to health promotion and illness prevention reflects a shift from individual-level influences to a focus on social and environmental influences, as suggested by social ecological models of health (McLeroy et al., 1988, 2003; Merzel and D’Afflitti, 2003). In contrast to prevention interventions that seek to change behaviors solely within individuals, community interventions focus on behavior change within entire communities or a subset of them. In addition to changing knowledge, attitudes, and intentions among community participants, community interventions emphasize changing community (social) norms to support individuals’ effort to reduce their risk and adopt health-promoting practices (Merzel and D’Afflitti, 2003; Nababan et al., 2011; Ross and Williams, 2002). Factors that community interventions target also influence and are influenced by upstream social and structural determinants of health (Adimora and Auerbach, 2010; Charania et al., 2011; Israel et al., 2005; Nababan et al., 2011). For example, community interventions that address social norms, such as fear and stigma associated with STIs, or, in contrast, empower communities to normalize STI screening, are likely to be effective in reducing risk (Adimora and Auerbach, 2010; Nababan et al., 2011). These social ecological principles rooted in community interventions are consistent with the committee’s conceptual framework, described in Chapter 1.
Beyond the central social ecological perspective, there is no singular definition of community interventions related to STI prevention and control. Of more than three decades of interventions focused on sexual health, most were designed for HIV prevention, leading to a dearth of evidence-based interventions to reduce STI incidence. Moreover, definitions vary widely in terms of level or reach (community level, community-wide, community base), strategy (e.g., community outreach, community engagement, community empowerment, community driven), unit of focus (e.g.,
groups within specified community organizations or particular locations), target group (e.g., heterosexual male adolescents, adult MSM, Latino/a people, homeless individuals, commercial sex workers), and outcome(s) of interest (e.g., STI incidence, STI testing, condom use, change in community norms, community capacity). These disparate views demonstrate the inherent complexities of the field and also underscore the difficulty in summarizing community interventions’ impact on STI prevention and control.
Meta-Analytic and Systematic Reviews of Community Interventions for HIV/STIs
Many reviews of community interventions examined effects in studies including the individual, group, community, and structural levels, some focus on specific populations, and others have focused on a particular type of community intervention. Below is a brief review of several systematic and meta-analytic reviews that highlight some such variation.
Community-Level Interventions for MSM
HIV/STI behavioral and social interventions determined by CDC to be effective behavioral interventions (CDC, 2020a) include three interventions designed for the community level: the Popular Opinion Leader program (Kelly et al., 1991), the MPowerment program (Kegeles et al., 1996), and the AIDS Community Demonstration Projects, later known as “Community Promise” (CDC AIDS Community Demonstration Projects Research Group, 1999). While these three interventions differ in level and details, they have a number of important commonalities. They aim to affect behavior change through community mobilization; they target specific communities disproportionally affected by HIV/STIs, including MSM; they are based on established behavior change theories; and, importantly, they use peer models as change agents in the community to affect behavioral outcomes. Furthermore, the initial studies that evaluated the interventions were controlled trials with intervention and control groups and, while they did not include HIV or STI incidence outcomes, they all showed efficacy in changing behaviors, including decreases in condomless sex.
Other systematic reviews that focused on adult MSM indicate that community-level HIV behavioral interventions have demonstrated effectiveness in reducing the odds of condomless anal sex. Moreover, economic evaluation indicates that community-level HIV behavioral interventions
for adult MSM are not only cost effective but also provide cost savings (Community Preventive Services Task Force, 2015; Herbst et al., 2007).
Community-Based, Skills-Building Interventions for Adolescents
A systematic review of interventions for adolescents implemented in schools, clinics, community-based settings, and specialized locations for particular populations (e.g., juvenile detention facilities for incarcerated youth) indicates that all the interventions identified changes in behaviors among participants, including a decline in the frequency of condomless sex, fewer sexual partners, and less sexual activity. The authors concluded that the most successful interventions included several key elements: (1) a theoretical foundation, (2) tailoring to the target groups of focus and implementation by trained facilitators, (3) comprehensive content, and (4) various implementation methodologies (Sales et al., 2006). Another systematic review of interventions, including but not limited to community-level interventions, that target adolescents identified factors associated with effective programs, including a focus on sexual communication, decision making, and problem-solving skills building. Moreover, programs that included a variety of content delivery strategies, such as arts and crafts, school councils, and community service learning, had a longer duration, and had trained facilitators were more likely to be effective in increasing condom use and other risk prevention outcomes (Robin et al., 2004).
Condom Distribution Interventions Targeting Diverse Groups
An extensive systematic review that focused on community-based interventions that made condoms widely available or accessible in community settings with outcomes for HIV infection, STIs, condom use, and multiple sexual partnerships identified nine such studies from 10 U.S. states between 1989 and 2011. Across all studies, three types of condom distributions were identified: unlimited access to condoms, unlimited access to condoms and other intervention activities, and coupons-based condom distribution. The findings indicated that no studies reported incident HIV, but community-based unlimited condom distributions modestly reduced condomless sex, while the condom distribution interventions along with other intervention activities significantly reduced multiple sexual partnerships. One coupon-based study, which was a not a randomized controlled trial (RCT), showed reduction in condomless sex in female participants; the second such study (an RCT) showed no effect on STI incidence. The authors conclude that community-level condom
distribution interventions may reduce some sexual risk behaviors (Malekinejad et al., 2017).
Another systematic review examined the overall efficacy of U.S. and international community-level structural condom distribution interventions on HIV risk behaviors and STIs (Charania et al., 2011). Twenty-one such studies were identified, covering January 1988 through September 2007. Significant intervention effects were identified for condom use, obtaining and carrying condoms, delayed sexual initiation among youth, and reduced incident STIs. Community condom distribution interventions targeting structural factors were efficacious for several groups, including youth, adults, men, commercial sex workers, clinic populations, and populations in areas with high STI incidence. Interventions that increased the availability and/or accessibility to condoms or including additional individual, small-group, or community-level components along with condom distribution were efficacious in increasing condom use behaviors (Charania et al., 2011). A study of a campus-based HIV prevention condom distribution intervention for African American women attending a historically Black college in North Carolina showed promise for this low-cost method for increasing condom use (Francis et al., 2018).
Community Empowerment Interventions for Sex Workers
Research has focused on community empowerment to activate participation and mobilization in marginalized settings, such as in the sex work industry (Abad et al., 2015; Evans and Lambert, 2008; Kerrigan et al., 2013). Kerrigan et al.’s (2013) systematic review and meta-analysis of community empowerment interventions for HIV prevention among sex workers in low- and middle-income countries from 1990 to 2010 revealed a reduction in gonorrhea and chlamydia in a longitudinal study and a reduction gonorrhea in an observational study. For this group, community empowerment included the traditional core elements of peer education, condom distribution, and periodic STI screening, but also emphasized principles that support the perspective that “sex work is work and should be respected as such, that sex workers know best how to identify their priorities and areas of concern, and that meaningful and sustainable responses to these challenges should be led by sex workers” to reduce their risk for HIV and to improve their overall health and well-being (Kerrigan et al., 2013, p. 1927). Another systematic review of U.S. community-based interventions for sex workers, without an empowerment framework, found that while most interventions included information on HIV and substance use prevention, few provided tailored content specific to commercial sex work (Abad et al., 2015). These findings highlight the
significance of using a community empowerment framework to guide interventions for this marginalized group.
Community Engagement Interventions for Latinas
Although few HIV prevention interventions have focused exclusively on Latinas, one meta-analysis of seven interventions that specifically targeted Latinas found that interventions that include content on relationships and negotiation skills were effective at reducing HIV risk. Community engagement with Latinas was important to recruit study participants, maintain the cohort, and ensure the cultural appropriateness of the interventions’ design and implementation (Daniel-Ulloa et al., 2016). Given the paucity of these community interventions, additional such research is needed. Community stakeholders should be enlisted to serve in partnership to ensure that interventions are culturally tailored and community situated to build on strengths and address unique needs.
Promising Community-Based Strategies
Partnering with Faith Institutions to Build Capacity and Sustainability
To address cultural and structural influences on HIV awareness, testing, risk-reduction behaviors, and stigma, community interventions have focused on forming collaborations with African American churches and other faith-based institutions (Abad et al., 2015; Derose et al., 2016; Griffith et al., 2010; Lightfoot et al., 2014). Project Fostering AIDS Initiatives That Heal (Project FAITH) is a faith-based model for developing, implementing, and sustaining locally developed HIV/AIDS prevention interventions in African American churches in South Carolina (Abara et al., 2015). The following are key steps and lessons learned that contributed to the success of this effort: (1) identify, educate, and build skills in existing community assets and resources to ensure that the interventions will be independently managed and sustained; (2) engage local and sometimes national faith leaders about the high burden of HIV/AIDS within their local communities and the role of places of worship in mitigating its effects; (3) provide ongoing technical assistance via information, advice, or assistance with managing the administrative affairs during implementation; (4) allocate funding specifically to support implementation; (5) cultivate and promote HIV messages that are acceptable to faith-based settings; and (6) have faith leadership explicitly demonstrate compassion toward and acceptance of people living with HIV, which was critical to dispelling HIV-related myths. Collectively, these activities and steps to address challenges provided a foundation for successful partnerships
with faith institutions to build capacity for developing, implementing, and sustaining efforts to prevent HIV in African American communities. Future consideration should be given to how faith communities can be leveraged to partner with local health departments and public health researchers to educate and provide resources and technical assistance to diverse communities (e.g., urban, rural, low resourced, high STI prevalence) to promote sexual health, wellness, and STI prevention.
Engaging Local Businesses Through Community-Based Participatory Research (CBPR)
Barbershops in African American communities have a long-standing tradition of serving as a central location where Black men gather, not only for haircuts, but to engage in lively “discussions and debates about local happenings, racial and electoral politics, sports, news, and sexual encounters” (Brawner et al., 2013, p. 2). Given barbershops’ prominence in African American communities and the trust and rapport between barbers and their clients, “barbershops are potentially one venue that is culturally situated and contextually appropriate” to reach diverse groups of African American men to disseminate information about sexual health, wellness, and STI prevention (Brawner et al., 2013, p. 2). A number of studies have examined the feasibility and acceptability of using this nontraditional community venue for prevention education, STI/HIV screening, and referral to other services (Brawner et al., 2013; Jemmott et al., 2017; Wilson et al., 2014). For example, Jemmott et al. (2017) developed and implemented a randomized controlled cluster intervention trial in 48 barbershops in Philadelphia, Pennsylvania, neighborhoods with high HIV/STI prevalence. Shape Up: Barbers Building Better Brothers is a theory-based, culturally and contextually competent, and gender-specific behavioral intervention to reduce the risk of clinically diagnosed STI/HIV infections among African American men aged 18–24 years. Barbers delivered the intervention, with the goals of increasing consistent and proper condom use and reducing multiple sex partnerships. The trial is still ongoing. Based on CBPR principles, steps for developing the intervention included (1) assembling a community advisory board (CAB) of barbers and barbershop owners, (2) identifying a theoretical framework to guide development, (3) conducting formative research to assess the feasibility of implementation, (4) developing the intervention in partnership with the CAB and manualizing all educational materials for standardization, and (5) assessing intervention acceptability. Although this is a culturally acceptable approach for this hard-to-reach group, few studies have been evaluated for their short- and long-term efficacy or brought to scale. Given the high burden of STIs in young, African American men
and their low use of health care services, such novel community-engaged approaches are worthy of future consideration as a means for preventing and controlling STIs.
Training and Supporting Lay Health Advisers to Extend Community Reach
Local sports leagues provide an opportunity to reach adolescents and adult men who may not readily access sexual health services for education and STI/HIV screening. To address this gap, lay health advisers (LHAs) were enlisted to facilitate an intervention to increase condom use and HIV testing among Latino men in a soccer league. The intervention was developed in partnership with community members, relied on male-centered intrapersonal networks, and was culturally tailored. Fifteen LHAs from 15 Latino soccer teams were trained and worked with their teammates for 18 months, with another 15 teams serving the control group. Thirty days after, participants (N = 222) were more likely to report condom use and HIV testing than controls were, indicating that LHA interventions for Latino men could be a viable option for both outcomes (Rhodes et al., 2009). Consideration should be given to how groups of LHAs could be trained and provided resources so this approach could be extended to other sports leagues (e.g., football, baseball, and basketball), tailored to reach other groups of racial and ethnic men, and adapted to focus on sexual health, including STI prevention. Clearly, more rigorously designed trials using LHAs are needed to determine the long-term efficacy of this promising approach.
Reaching Minoritized and Marginalized Groups Using Street-Based and Alternative Venue Outreach
Community intervention approaches that use street-intercept and venue-based outreach strategies are designed to reach groups of individuals who do not typically access health care services in clinics or medical centers and, often, do not frequent mainstream community-based organizations. Thus, nontraditional approaches for these stigmatized and hard-to-reach individuals are needed to engage them in risk reduction education, STI screening, and treatment. Both street- and venue-based outreach approaches have been shown to be feasible and acceptable means for successfully reducing sexual risk behavior, improving STI testing and treatment, and increasing use of health resources in gay men (Kegeles and Hart, 1998), sex workers (Pitpitan et al., 2013), homeless individuals (Auerswald et al., 2006; Rotheram-Borus et al., 1991b), and individuals residing in neighborhoods with high STI prevalence (Boyer et al., 2007; Chutuape et al., 2009; Johnson et al., 2001; Ott et al., 2018; Rothenberg et al., 2007; Wendell et al., 2003). Both strategies rely on effectively recruiting and training peer educators and outreach workers and require strong
public health research and community collaborations and deliberate and systematic steps for community engagement, such as venue mapping, focus groups, street observations, and key informant interviews in advance (Chutuape et al., 2009; Johnson et al., 2001; Ott et al., 2018; Sieverding et al., 2005).
Building on and sustaining gains made in prior community street- and venue-based outreach efforts warrant continued capacity building and targeted community engagement and prevention efforts. The sustainability of evidence-based efforts will require ongoing technical assistance and building a well-trained and resourced cadre of community peer educators and outreach workers to provide prevention education, screening, and referral to local services for further health care needs and follow-up.
Taken together, these community intervention strategies have shown promising results, including community feasibility and acceptability. However, a great deal more research is needed to further develop and evaluate the efficacy of the interventions and resources to replicate them in other settings to actualize their full potential in reducing community transmission. Despite the current limitations, novel and creative intervention approaches, such as those highlighted here, may be worthy of future consideration to address the current STI epidemic. More than ever, strategies need to be explored for reaching deeper within communities most affected by the epidemic, including racial and ethnic minorities and marginalized groups who live and socialize in low-resourced communities with high STI prevalence. The demonstrated feasibility and acceptability of these approaches should not be undervalued. Moreover, these lesser-known community approaches to sexual health promotion and STI prevention have shown the importance of community engagement and capacity building through deliberate and ongoing partnership with key community stakeholders, collaboration between public health researchers and key community members, and allocation of dedicated resources for formative work, intervention implementation, evaluation, replication, and scale-up.
COST EFFECTIVENESS OF PSYCHOSOCIAL AND BEHAVIORAL INTERVENTIONS
In addition to STI-preventive interventions being efficacious and effective, evidence indicates that they are cost effective. For example, a systematic review on the effectiveness and economic efficiency of individual-, group-, and community-level behavioral interventions to prevent HIV in MSM found that group- and community-level interventions were not only cost effective but resulted in actual cost savings (Herbst et al., 2007). Furthermore, individual-level STI behavioral prevention
interventions have been found to be cost effective across a vast majority of reviewed studies (Herbst et al., 2007) even after excluding associated benefits, such as STI prevention, decreases in lost productivity, intangible benefits (such as reduced pain and suffering), HIV incidence, and the effects on STI outcomes other than those measured (Barham et al., 2007). For example, Blandford and Gift (2006) estimated productivity losses to untreated chlamydia to be $130 among reproductive-aged women. Other studies exclude intervention effects on quality of life, which is often difficult to assign a dollar value to (see Chapter 4 for more information on STI cost estimates, burden, and quality of life measures).
Psychosocial and behavioral interventions aimed at increasing condom use among youth are also cost effective. Nonpartisan groups, such as the Washington State Institute for Public Policy (WSIPP),1 conduct research to determine the benefit–cost analyses of prevention programs and provide a percentage on the chance that a program’s benefit will exceed its costs, information that is used to make policy determinations. WSIPP’s work has included a number of different areas, including criminal justice, education, child welfare, behavioral health, workforce development, public health, and prevention and thus interventions that target risk factors (e.g., alcohol use) for sexual health promotion and STI prevention and management. Unfortunately, WSIPP has not addressed interventions that only target condom use and STIs, but it has included those with condom use or STIs as outcomes combined with other outcomes. For example, Familias Unidas, an evidence-based, family-centered intervention found to be efficacious and effective in reducing condomless sex, substance use, and preventing STIs in Hispanic adolescents, produced benefits greater than the costs 68 percent of the time.2 Interventions such as the Nurse Family Partnership that have had an impact on risk factors for STIs and condomless sex (e.g., early alcohol use initiation, substance use) are also included. The program has a 64 percent chance that benefits will exceed costs and a benefit–cost ratio of $1.38.3
TECHNOLOGY-BASED INTERVENTIONS
Chapter 6 provides an overview of different types of technologies that can be applied to prevent and control STIs. This section builds on Chapter 6 and focuses on how to apply these technologies. In the context of STI research and prevention, technologies are typically viewed as a tool to deliver interventions, similar to word-of-mouth methods, radio
___________________
1 See www.wsipp.wa.gov (accessed January 27, 2021).
2 See http://www.wsipp.wa.gov/BenefitCost/Program/644 (accessed January 27, 2021).
3 See http://www.wsipp.wa.gov/BenefitCost/Program/35 (accessed January 27, 2021).
broadcasts, newspaper advertisements, or any other method that can be used to deliver interventions. Technologies also play a more nuanced role in sexual health, however, including affecting people’s attitudes and social norms. This requires extensive consideration of when, how, and why they should be incorporated into interventions. For example, in addition to acting as a delivery tool, technologies such as social media can influence people’s perceptions of sexual health and related STI risk, moral and sexual-related judgments about themselves and their peer groups, and social normative behaviors around sex (Young and Jaganath, 2013; Young and Jordan, 2013). The relationship between people and technologies is complicated and dialectical: technologies not only affect people’s sexual health–related attitudes and behaviors, but people’s sexual health–related attitudes and behaviors also affect technologies (e.g., people’s desire to find new sex and dating partners influences the development of new dating/hookup apps, and their growing use affects people’s attitudes and ability to find sex and dating partners). It therefore becomes important to recognize the large and ever-changing role that technologies play in sexual health and intervention delivery.
As discussed in Chapter 6, the committee sees technology as a tool that can be helpful to control, prevent, and treat STIs but may also contribute to STIs. The term “tool” is emphasized, as these are platforms that allow for rapidly delivering a theory or intervention to a large group of people, rather than stand-alone products that can change behavior without incorporating the correct psychology/psychosocial-behavioral approach. This distinction is important so that researchers and policy makers are aware of the benefits and limitations of social technologies in STI interventions.
Technology as a delivery platform is more than an option for disseminating traditional content, as it may have certain characteristics that assist in promoting health behavior change. Technology-based interventions come in a variety of forms, across platforms, and with differing names and definitions. Electronic health (eHealth)4 and mobile health (mHealth)5 are umbrella concepts that may encompass a variety of intervention types. Some reviews focus on digital health, others on social media. This report primarily addresses technology-based interventions and is specific when discussing different programs and the platforms through which they were administered, as affordances may vary by technology.
___________________
4 eHealth is health care practice supported by electronic processes (e.g., electronic health records, patient administration systems, and lab systems).
5 mHealth is the use of mobile devices, such as a mobile phone or a tablet, to support the practice of health care.
Technology-Based Intervention Benefits
eHealth interventions have been found to appeal to individuals and offer convenience, privacy, anonymity, flexibility, and the ability to tailor (Noar and Harrington, 2012). A meta-analysis not focused specifically on STIs found tailored health communication efforts to be more efficacious than non-tailored materials in Web-based settings (Lustria et al., 2013). Similarly, a meta-analysis of text message–based health promotion interventions found tailored interventions to be more efficacious (Head et al., 2013). Tailoring can be built into the system offerings, and it may be more practical in certain technology-based programs. Research that has specifically assessed tailoring in technology-based sexual health interventions, however, is limited, with one meta-analysis not finding an effect in influencing the interventions’ effect on abstinence and condom use (Widman et al., 2018). This could in part be due to the wide variety of variables on which one may tailor. Previous research into tailoring through technology not focused specifically on STIs has found that it is common to tailor health interventions on more than one construct and to use a combination of theory-based and non-theory-based constructs (Krebs et al., 2010; Lustria et al., 2009; Noar et al., 2007).
In addition to the affordances listed previously, research has found that features of technology may influence program liking and, therefore, possibly impact further downstream effects. For example, participants who perceived a sexual health text message intervention as more interactive, regardless of actual differences in technological affordances, self-reported an increased likelihood to recommend the service to a friend and showed increased levels of repeat use (Willoughby and L’Engle, 2015). Similarly, finding an eHealth intervention interactive and engaging may lead to high rates of participation (Perrino et al., 2018). These outcomes highlight program factors that may affect attention, which may be a necessary first step in influencing behavior change. In one meta-analysis, the interactivity level of technology-based interventions was not found to impact outcomes associated with STIs and unintended pregnancies (Widman et al., 2018), but a previous meta-analysis found that interactivity influenced condom use, with interventions that included more interactive components yielding significant effects (Swanton et al., 2015). Part of this difference could be based on definitions used to conceptualize certain features of technology, as the definition of interactivity may vary (Kiousis, 2002; Sundar et al., 2003). The impact may also be based not on the technical affordances, but on user perceptions of such affordances.
Reviews and Meta-Analyses of Technology-Based Sexual Health Behavior Interventions
Reviews and meta-analyses have found technology-based interventions for sexual health to be promising, including for addressing behaviors associated with STIs, such as increased condom use and STI testing. In a meta-analysis, Swanton et al. (2015) found that new media interventions (defined by the authors as including social networking sites, text messaging, chat rooms, websites, e-mail, and smartphone apps) led to significant changes in both condom use and STI testing but that not all interventions had such outcomes. Interactivity (increased interactivity), target audience (young adults), and study design (RCTs) moderated the effects on condom use, with intervention duration influencing the impact on STI testing (more than a single session had increased effects) (Swanton et al., 2015). Therefore, more substantial interventions may have greater effects. The authors also found differences among interventions targeted to specific populations. Interventions targeting condom use were more effective with women and less effective with MSM and young people, and interventions that targeted STI testing were more effective for young people than for MSM.
A newer meta-analysis found that technology-based interventions positively influenced condom use and abstinence, but that interactivity and other factors did not moderate the outcomes (Widman et al., 2018). The duration from intervention to assessment, however, did influence outcomes, with stronger effects in the short term (assessed between 1 and 5 months) compared to the long term (more than 6 months). This supports the idea that the effects may dissipate, in both technology-based interventions and face-to-face ones.
Specific to text messaging and sexual health, a meta-analysis of 35 studies examined intervention effects on prevention, detection, treatment, and knowledge of STIs and HIV (Taylor et al., 2019). Most studies (N = 8) focused on the effectiveness of text messages for STI clinic appointments. Studies were conducted across 14 countries, the majority of which included the United States (13 studies). Participant age was 16–84, followup occurred on a range of 7 days to 24 months, and text messages were delivered daily, weekly, monthly, or as one-off reminders; 83 percent of studies consisted of one-way texting. The main outcomes examined included prevention, HIV drug adherence, and HIV treatment outcomes. Overall results point to mixed evidence regarding effectiveness for STI/HIV outcomes. Part of this ambiguity is due to the great degree of variance in methods and a high percentage of studies (75 percent) with risk of selection bias and performance bias caused by an inability to conceal randomization allocation, blind study participants, and blind study
personnel (Taylor et al., 2019). The authors noted that the lack of certainty around effects may have been due to the variations in the program types (e.g., one-way versus two-way versus frequency of messaging). Differences in text message delivery (e.g., Willoughby and Muldrow, 2017) may influence program features, experiences with the interventions, and perceptions of the content to which individuals are exposed, and work has yet to parse out which specific components lead to the greatest chance of success. Work in text messaging health interventions more generally, however, has provided some guidance on content timing and delivery (see Head et al., 2013).
Theoretical Frameworks for Technology-Based Interventions
The effect of technology-based interventions is likely not from the technology itself (i.e., simply putting the intervention online or on social media), but from identifying and applying the correct theoretical basis for behavior change (i.e., the specific way these technologies were used to deliver the intervention).
For example, individuals in the Keep It Up! 2.0 intervention—rooted in the IMB Skills model of HIV risk behavior change—compared to those in a matched eHealth control group (with static text and content not tailored to young MSM), had improved STI-related outcomes. Specifically, compared to control group participants, STIs (urethral or rectal chlamydia or gonorrhea) were significantly less likely (40 percent) at 12-month follow-up. Although there are a variety of theories that could guide intervention development (e.g., IMB model), it is important that the intervention is delivered with an understanding and tailoring of the psychosocial and behavioral needs of the population, rather than just assuming the technology will work by itself. For Keep It Up! 2.0, it likely was the psychological elements, such as engaging content, videos, and information tailored for young MSM, that led to the study results, as the equivalent technology without these factors did not perform as well.
The specific choice of technology for delivery is also important in digital STI interventions, as characteristics of the technology affect how it is used, by whom, and where. For example, the social media video site YouTube might be a good tool for delivering STI prevention-related videos, but only if the channel being promoted already has a large following (i.e., leveraging already engaging technologies and websites will likely work better than trying to develop one from scratch and expecting people to visit it).
An Example Framework for Technology-Based Interventions
A growing body of research on theoretical frameworks can be used to improve delivery of digital behavioral interventions (Hekler et al., 2016; Simoni et al., 2018). One recent option that might be applied for integrating technologies into STI interventions is the Adaptive Behavioral Components (ABC) model (Young, 2020) (see Figure 8-1). ABC applies research from the fields of social and behavioral psychology, informatics, and marketing that can be used to develop a model tailored to the needs of various digital technology interventionists. The model is based on five overarching factors that are needed to develop sustainable technology-based interventions: (1) basic behavior change components; (2) intervention and problem-focused characteristics; (3) population, social, and behavioral characteristics; (4) individual-level and personality characteristics; and (5) technology characteristics (Young, 2020).
As this chapter already provides the science on the elements needed to deliver effective STI interventions, the ABC model can be used to integrate these elements and potentially scale their reach and impact by using social technologies. Importantly, the ABC model helps to address the planning for potential changing technological trends and features, which is important, especially for long-term sustainment (see Chapter 6 for more information on types of technologies and important considerations for the future).
Technology characteristics can impact intervention engagement and therefore may have a large impact on efficacy. For example, the success of an intervention delivered using technologies can be impacted by trends in popular communication styles (e.g., it is better to choose the preferred communication medium), changes in ethical considerations (e.g., a breach of security could decrease trust in a particular platform), or changes in the features of a technology (e.g., adding an online community feature to a software app may change user engagement rates) (Garett and Young, 2019; Young, 2020). Therefore, to deliver effective longitudinal technology-based interventions, it is important to be aware of the current technology landscape, understand the implications of such changes, and be prepared with adaptations.
The most recent Harnessing Online Peer Education (HOPE) HIV intervention serves as an example of how technology-related changes can impact delivery and require adaptation. This second HOPE HIV intervention is a multi-wave, 5-year HIV testing intervention funded in 2014 based on earlier methods and results from HOPE interventions in 2010 and 2012 that showed success in using Facebook groups as a delivery platform (Young et al., 2013, 2015). From 2010 to 2014, and throughout the next 5 years, however, a large number of changes occurred on social media, including Facebook no longer being the dominant technology
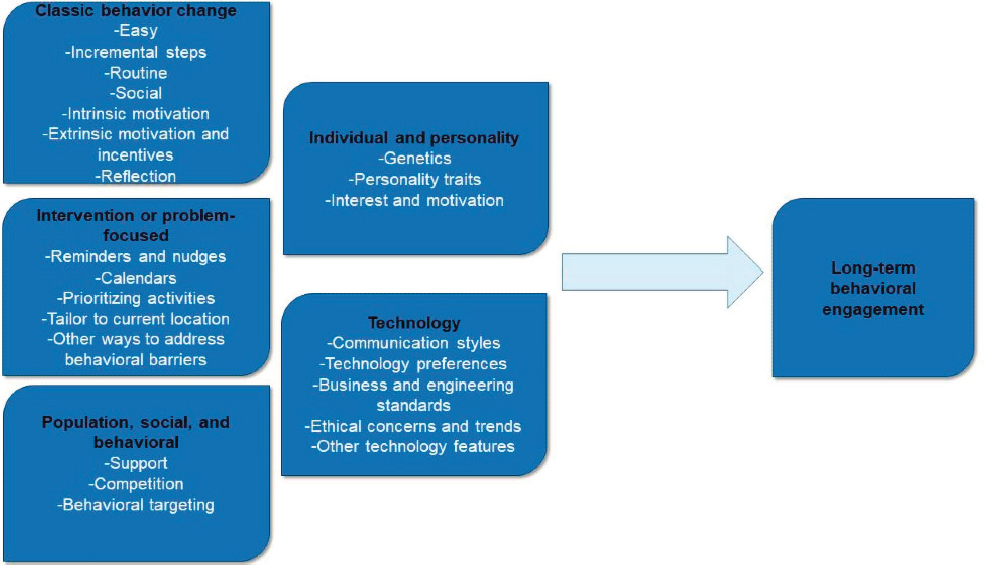
SOURCE: Young, 2020.
among all age groups and populations. With the introduction of other platforms, such as Snapchat and Instagram, Facebook use waned, especially among youth (Fox, n.d.), which might reduce the engagement and potential efficacy of interventions delivered on it that rely on previous rates of engagement.
Similarly, throughout the 5-year period, Facebook made a number of changes to its interface, affecting HOPE’s engagement. For example, Facebook announced that it was planning to change the way its algorithm displayed content, potentially affecting the advertising and outreach methods being used by businesses and researchers, possibly leading these methods to cease working (Facebook, 2018). The HOPE intervention (and other interventions leveraging Facebook groups) was impacted by these changes; analysis of the HOPE study found that intervention participants received fewer notifications about HIV prevention and testing compared with control (Facebook) group participants (Young, 2020).
Although the intervention group remained significantly more engaged in posting compared with the control group (as intended by the intervention), the large number of posts within the intervention group combined with the changes to the way Facebook groups and the Facebook algorithm were used initially resulted in fewer testing-related posts being viewed by the intervention group compared with the control group. (Young, 2020)
HOPE illustrates the importance of not relying on a single technology as a delivery platform for longitudinal interventions but instead using multiple platforms that are dominant at that point in time and being able to adapt to changing platforms and trends.
Technology as a Dissemination Strategy
Given the increasing popularity of technologies among populations most affected by STIs and more broadly (see Chapter 6 on technology for more detail), offline/face-to-face interventions need to be able to be adapted online. This has become urgent during the COVID-19 pandemic; related policies have required socially distanced interventions, as can be done with remote technologies. It is therefore important to understand the challenges in moving or adapting offline interventions. The Familias Unidas intervention is an example of this concept. It was originally developed for face-to-face delivery, and one of the challenges in moving to online delivery was recreating its participatory nature (Estrada et al., 2017). A central tenet of Familias Unidas is that, with facilitator guidance, parents are empowered to become the agents of change for their families and youth. This means that through skills building and parent group
discussions focused on problem solving and effective communication, parents can work on and achieve their goals. For the online adaptation, the study team (Estrada et al., 2017) made it participatory in three ways. First, parent video group discussions were developed, keeping in mind the viewer at home. Videos were recorded so as to foster a sense of inclusiveness and interaction via pointed questions, such as “you watching at home, please think about what goals you have for your adolescent” and “for viewers at home, what do you think about what was just said?” Second, interactive exercises were incorporated to adapt the participatory learning strategy used in the face-to-face version; these varied from session to session and included multiple-choice questions, true or false, fill in the blank, and point-and-click responses, with instant feedback for all responses. Third, the four facilitator-led family sessions were moved to a live online delivery format. This highlights some of the necessary considerations to adapt interventions for technology-based delivery. One option to help with technology as a dissemination strategy is social marketing, which has been applied more broadly, but could be leveraged for technologies. A review of how social marketing principles were applied in sexual health campaigns found that some elements were limited in campaign creation (Akbar et al., 2020). Even with the understanding that campaigns will likely focus on different elements, in a review of 26 articles that covered 16 health communication and social marketing campaigns specific to STD testing or prevention, nearly all campaigns reported differences in behavioral outcomes between people exposed to their messages and those who were not (Friedman et al., 2016). The researchers concluded that campaigns can be useful for targeting STD-related behaviors.
Technology-Based Interventions Research and Future Directions
Despite multiple technology-based interventions, the efficacy may not be clear for many. Reviews and meta-analyses are limited by the specific technology types and affordances examined. While such reviews can provide guidance on possible effectiveness, interventions developed with such differing characteristics (e.g., peer-to-peer interaction, one-way messaging, differences in frequency) make it important to consider evaluation and research strategies that may help to parse out the effects to determine which characteristics and affordances of the technology may develop the strongest interventions possible. One option is the Multiphase Optimization Strategy (Collins, 2018; Collins et al., 2016), in which randomized experimentation is conducted to evaluate the efficacy or effectiveness of each component and whether its presence/absence affects the performance of other components (Collins, 2018).
Additionally, technology-based interventions offer the benefit of scalability, but they may not be done to scale, even if efficacious, because
funding, resources, and/or a lack of partnerships with organizations (e.g., those serving adolescents and young adults) may prevent this.
Technology-based interventions can play an important role in psychosocial and behavioral interventions, perhaps more so than ever due to the rapidly changing environment and increased access to technology (the COVID-19 pandemic is a current example). Understanding the varied characteristics of different tools and how users interact with them and grounding the intervention in theories and psychology, however, are essential. Box 8-2 outlines important considerations when developing interventions that use technology or adapting an offline intervention to be online.
DISSEMINATION OF EVIDENCE-BASED BEHAVIORAL INTERVENTIONS
Psychosocial and behavioral interventions with documented efficacy in preventing STIs have generally not been widely disseminated. For example, adoption of an intervention into a specific delivery setting (e.g., schools, health care, community agencies) may not occur for a number of reasons, including (1) an organization’s structure, (2) available resources, (3) costs, (4) number of providers available or willing to deliver the intervention, or (5) competing demands within the organization. This lack of dissemination is not unique to the STI field. A systemic review by Hanley
et al. (2010), for example, estimated that only 35 percent of evidence-based substance abuse preventive interventions used in U.S. elementary schools were evidence based. Despite this lack of wide-scale adoption and sustainment of behavioral interventions, registries of evidence-based interventions have facilitated the wide-scale dissemination of some. For example, CDC’s compendium of evidence-based interventions and best practices for HIV (and other STIs) disseminated dozens of behavioral interventions to health departments and community organizations across communities in the United States. Although these were not always implemented with high fidelity (Rotheram-Borus et al., 2009), largely because community organizations adapted them for local use, CDC’s effort was successful in reducing sexual risk behaviors and STIs (Dworkin et al., 2008). Unfortunately, with a few exceptions, the wide-scale dissemination of evidence-based, behavioral interventions to prevent STIs is not common practice, and it is critical to find solutions to overcome barriers.
One solution to facilitating the adoption, integration, and sustainment of evidence-based interventions to prevent and manage STIs into service delivery systems is to involve key stakeholders, defined as “individual, organizations or communities that have a direct interest in the process and outcomes of a project, research or policy endeavor” (Deverka et al., 2012). Their role in the entire process cannot be overstated. Key stakeholders are vital individuals who act as gatekeepers in bridging research to practice. For example, implementing an evidence-based intervention within pediatric primary care settings to prevent STIs involves strategically forming alliances with key administrative staff and winning support from physicians (Molleda et al., 2017). Without stakeholder buy-in, evidence-based interventions likely will not make the transition from research to practice. Key stakeholders also include intervention recipients, such as adolescents and families. Including them in developing and/or adapting existing interventions can help address challenges with engagement, inform intervention content, and give a voice to the needs of those who will ultimately use the intervention in community practice.
Historically, key stakeholders have played a minimal role in the research process. With the increased use of qualitative research and inclusive methods, such as community-based participatory research, however, the psychosocial and behavioral intervention field is increasingly including them earlier on. Doing so as early as possible, even as early as in the study design, has important implications for adopting and sustaining behavioral interventions. For example, stakeholders can inform whether an intervention is sustainable, culturally syntonic, or a good contextual fit within a community or practice setting. Participatory approaches in research are gradually increasing (Ewan et al., 2016; Vaughn et al., 2013) and particularly important among minority populations (Ewan et al.,
2016; Israel et al., 2005). Frameworks such as Communities That Care (CTC) can identify community needs and provide guidance in selecting behavioral interventions that align well with those needs and context, all through harnessing the voices of community stakeholders (Hawkins et al., 2009).
Another potential solution to overcoming barriers to adoption of STI evidence-based intervention is developing mHealth or eHealth interventions or adapting existing interventions for online delivery. As discussed, some literature documents the efficacy or effectiveness of eHealth interventions in reducing rates of condomless sex, increasing STI testing, and reducing STI incidence (Bauermeister et al., 2015; Mevissen et al., 2011; Swanton et al., 2015). Unfortunately, despite this evidence, the number of scientifically proven online STI preventive interventions remains low, and even fewer are integrated into practice. This is surprising given that these interventions are less resource intensive and provide greater flexibility as to where, how, and when they can be disseminated (Prado et al., 2019). Furthermore, they have greater potential to reach populations (e.g., youth, ethnic minorities) disproportionately affected by STIs. Therefore, developing and evaluating evidence-based interventions and adapting them for online are important priorities for STI prevention. Such adaptations, if successful (Li et al., 2020; Prado et al., 2019), could lead to greater rates of adoption and sustainment. Models such as the ABC described earlier can also be used to sustain technology-based interventions.
IMPLEMENTATION SCIENCE
It is also important to turn to the field of implementation science for methods to facilitate the adoption and sustainment of evidence-based interventions to promote sexual health and STI prevention. The field is not novel, but NIH and other federal agencies have paid it significant attention over the past 10 years. In 2013, NIH issued the first funding opportunity announcement specific to dissemination and implementation research to “support innovative approaches to identifying, understanding, and overcoming barriers to the adoption, adaptation, integration, scale-up and sustainability of evidence-based interventions.”6 Since then, the emphasis has shifted from developing behavioral interventions to prevent and control STIs to disseminating existing evidence-based interventions. Research on how to accelerate the implementation process, however, remains very limited.
___________________
6 See https://grants.nih.gov/grants/guide/pa-files/par-13-054.html (accessed November 16, 2020).
Few studies have clearly measured implementation outcomes—most still only focus on individual behavioral (e.g., condomless sex) or disease (e.g., STI incidence) endpoints. Important implementation outcomes to measure include intervention sustainability, perceived fit in the target setting, fidelity, number of providers delivering or participants receiving the intervention in a given practice, and financial feasibility (Proctor et al., 2011). Furthermore, even fewer trials exist with an implementation-level outcome, and none specifically involve an STI behavioral intervention. Implementation trials may not take the form of a traditional randomized clinical trial, which may not be feasible for many reasons. For example, they are not appropriate in all settings, especially at the community level, and randomization can be considered ethically objectionable if it denies an intervention known to be beneficial. Such circumstances may require alternative study designs, such as a step-wedged (Brown and Lilford, 2006) or rollout (Brown et al., 2017) design, where the intervention is sequentially rolled out to participants so that all participants receive it by the end of a study. That is, the randomization unit is the time when participants receive the intervention. This type of design may be appropriate to evaluate implementation-related outcomes (e.g., sustainment) when the intervention is already known to be effective and no one should be denied it. That is, a step-wedge design may be used to evaluate whether an evidence-based intervention can be sustained (i.e., the implementation outcome) in primary care or pediatric care clinics over time. In such a study, clinics would be randomized to when they receive the intervention. For clinics or communities, there may be advantages to receiving the intervention either first or last. Clinics going first may have immediate access to an evidence-based intervention, whereas if they are later, they may be better prepared to adopt and sustain the intervention.
It is also important to evaluate implementation strategies that facilitate the adoption, integration, and/or sustainment of evidence-based interventions in practice. To date, no intervention strategies have been evaluated to examine the adoption of evidence-based sexual health and STI behavioral interventions. The following section briefly reviews some implementation strategies and systems that have been found to be effective in integrating behavioral interventions, although not specific to sexual health and STIs.
Getting to Outcomes (GTO) was developed as a tailored tool and guide to assist communities and organizations build performance and individual capacity for delivering effective prevention interventions (Chinman et al., 2001, 2008; Wandersman et al., 2000). The main goals are to help organizations run an effective prevention program well so that it can obtain its desired outcomes and facilitate the implementation process, including sustaining the intervention. GTO consists of an intervention and
a process component. The intervention component comprises the GTO Manual, face-to-face training, and onsite technical assistance. The process component includes ten steps, which should be properly addressed to achieve positive results, tied into a step-by-step GTO process that includes topics such as assisting the organization in choosing an evidence-based intervention that is a good fit, ensuring the organization has the capacity needed to run the program, and ensuring the organization is thinking about and planning for sustainment. In a cluster RCT evaluating sexual health outcomes, 32 Boys and Girls Clubs were randomized to either Making Proud Choices, an evidence-based teen pregnancy preventive intervention, or GTO + Making Proud Choices. Youth in GTO + Making Proud Choices reported improvements in condom use attitudes and intentions (Chinman et al., 2018).
CTC is an implementation system to strategically guide communities, or coalitions, in planning and implementing evidence-based prevention programming (Hawkins et al., 2008). The CTC system is designed to help communities define the outcomes, prioritize factors to be targeted, offer a menu of programs, and guide the community selecting, implementing, and evaluating the selected program in their organization system. Research demonstrates that CTC has positive outcomes (e.g., alcohol use, cigarette use) for youth. For example, in an RCT with 24 communities across 7 states, communities randomized to CTC had students who were 32 percent less likely to initiate drugs and 33 percent less likely to initiate cigarette use, compared to the control communities (Rhew et al., 2016). Furthermore, CTC has long-term effects, with reductions in lifetime incidence of health-risk behaviors extending into young adulthood (Oesterle et al., 2018). CTC has been implemented in hundreds of communities in the United States.
CDC’s Community Approaches to Reducing Sexually Transmitted Diseases (CARS) program began in 2011 (CDC, 2020b). CARS seeks to support planning, implementing, and evaluating projects to reduce STI disparities, promote individual sexual health, and support overall community wellness and health equity. A toolkit is offered to support communities in implementing the CARS framework (CDC, 2019a). CARS emphasizes community engagement and attention to the social determinants of health throughout the process of intervention development, implementation, evaluation, and dissemination. The specific steps of the CARS process are laid out in the toolkit: (1) conduct a community health needs assessment; (2) establish a CAB and develop initial community partnerships; (3) train CAB members; (4) support CAB STI intervention design and engage implementation partners; (5) engage the CAB in social determinants of health prioritization; (6) facilitate CAB review of additional community health assessment components; (7) implement
interventions; (8) evaluate community engagement, partnerships, and interventions; (9) build and ensure sustainability through partnerships; and (10) celebrate successes with the CAB and partners. The toolkit emphasizes that this process may not always be linear, and certain steps may entail multiple iterations and or need to occur throughout the program period (CDC, 2019a).
The Leadership and Organizational Change for Implementation (LOCI) strategy addresses leadership and organizational development in implementing evidence-based practice (Aarons et al., 2015). LOCI aims to achieve positive changes in implementation leadership, and quality in service delivery systems, thus increasing the adoption and sustainment of evidence-based interventions with fidelity (Aarons et al., 2015, 2017a). LOCI targets leadership at multiple levels, including first-level leaders, such as supervisors of direct service providers, and high-level administrative leaders (Aarons et al., 2014; Egeland et al., 2019). LOCI has well-established feasibility, acceptability, and perceived utility and demonstrated positive changes in leadership and climate (Aarons et al., 2015, 2017a). LOCI has also been found to adapt and respond to changes (e.g., staff and/or leader turnover) commonly faced by service delivery systems implementing effective behavioral interventions (Aaron et al., 2015).
Implementation strategies, such those reviewed above (except CARS), have been rigorously evaluated and shown to affect outcomes such as adoption, reach, penetration, fidelity, and sustainment. Specifically, these strategies (e.g., LOCI) have been found to change leadership and climate, which, in turn, may likely impact intervention adoption and sustainment. Unfortunately, the evaluation of implementation strategies is virtually nonexistent in the field of STI prevention. Other disciplines, such as drug abuse prevention and treatment, have benefited from rigorously evaluating these strategies. For example, CTC has led to incorporating evidence-based interventions in hundreds of U.S. cities/communities. The challenge with evaluating both behavioral interventions and implementation strategies are the costs and time required. One strategy to reduce both is to evaluate psychosocial and behavioral interventions for effectiveness (e.g., individual-level outcomes), as well as implementation outcomes. For example, Hybrid II effectiveness-implementation trials (Brown et al., 2009) that evaluate individual-level outcomes (e.g., STI incidence, condomless sex) for STI prevention and implementation outcomes (e.g., sustainment) will reduce the costs of having to perform multiple studies and the time associated with conducting them. As with other health research, the time lag between basic science (intervention development) and practice (dissemination and implementation) is 17 years (Morris et al., 2011). Acceleration is critical for the field to integrate evidence-based STI behavioral interventions into practice. Moreover, these types of trials
in combination with other innovative study designs may provide an opportunity to uniquely evaluate behavioral interventions on individual-level STI-related outcomes and implementation strategies/systems-level interventions on implementation-related outcomes. For example, a hybrid type II head-to-head randomized rollout trial with two different random assignments may be used to evaluate an evidence-based intervention and an implementation strategy. Specifically, randomization occurs at two levels: during development of the implementation strategy and when implementation begins (Brown and Lilford, 2006; Brown et al., 2009). Such study designs can accelerate the translation of knowledge into practice, improve the sexual health outcomes, and reduce STIs in the United States.
CONCLUSIONS AND RECOMMENDATION
Based on its review of the evidence, the committee provides the following conclusions, and Recommendation 8-1:
Conclusion 8-1: Psychosocial and behavioral interventions, in conjunction with biomedical, structural, informatics/technological, and health service interventions, are integral to a comprehensive strategy for sexual health and STI prevention and control. Therefore, multidisciplinary investigative teams are needed when developing psychosocial and behavioral interventions.
Conclusion 8-2: Psychosocial and behavioral interventions to promote sexual health and prevent and control STIs are efficacious and effective for diverse populations, but are underused and have not been adopted and sustained in clinical or community practice. Future considerations for research for intervention development include the following:
- Development and evaluation of effective implementation strategies of these interventions;
- Use of varied scientific methodological designs (e.g., effectiveness–implementation hybrid designs, step-wedge designs) to provide outcome measures and inputs for implementation science analyses.
Conclusion 8-3: Evidence-based family interventions have demonstrated effects on mental health and behavioral outcomes (e.g., drug use, suicide behavior) with crossover effects on condom use and STIs. Funding for psychosocial and behavioral interventions, however, historically has been siloed by disease outcomes, which has not allowed studying multiple and interrelated health outcomes, such as STIs, substance use, and mental health conditions. As such, funding opportunities that cut across multiple health conditions and behavioral outcomes are sorely needed in addition to funding for outcome-specific interventions. Identifying these crossover effects could
lead to greater cost effectiveness and more sustainable impacts on health outcomes, such as STIs.
Conclusion 8-4: Comprehensive sexual health education taught in schools is effective in delaying the initiation of sexual behavior, promoting sexual health, and reducing risk for STIs in students. In the 1990s, federal policy adopted the promotion of abstinence-only until marriage as the singular approach to school-based sexual health education. Rigorous research has demonstrated the ineffectiveness of this approach, yet federal funds still support such instruction even as comprehensive models also now receive federal funding. Political conflict over abstinence-only education, combined with pronounced conflict over addressing sexual orientation and gender identity diversity in schools, has meant that many young people do not receive sufficient instruction of guidance in these areas. School-based sexual health education programs across the United States are highly variable, with no nationwide policy regarding how sexual education is taught in schools. Nonetheless, research indicates that parents broadly support comprehensive school-based sexual health education for elementary, middle, and high school students even when stratified by political party.
Conclusion 8-5: Community intervention strategies to promote sexual health and prevent STIs have demonstrated feasibility and acceptability in communities most affected by STIs, including racial and ethnic minorities and marginalized groups who live and socialize in high–STI prevalence, low-resourced communities. Additional research is needed, however, to evaluate the efficacy and effectiveness of community-level interventions on reducing community transmission of STIs. Community interventions that specifically address social and structural determinants of health are needed.
Conclusion 8-6: Technologies, when combined with appropriate psychosocial and behavioral interventions, have successfully changed STI-related attitudes and behaviors. It is critical to consider incorporating these technologies when developing or adapting psychosocial and behavioral interventions. These technological tools can be used to deliver and/or scale up evidence-based sexual health and STI prevention. Interventions that use technology should be developed leveraging psychosocial, digital behavioral and informatics intervention frameworks, including taking into account the affordances of the specific technology for prevention efforts as well as intervention-development best practices.
Recommendation 8-1: The Department of Health and Human Services (HHS) should take steps to expand the reach of psychosocial and behavioral interventions to prevent and control sexually
transmitted infections at the individual, interpersonal, and community level. This can be accomplished by developing sustainable funding mechanisms to deliver those interventions; establishing standard guidelines for school-based comprehensive sexual health education; and developing, evaluating, and disseminating community-based approaches:
- HHS should develop new mechanisms that provide sustainable funding for dissemination, adoption, and scale-up of evidence-based psychosocial and behavioral interventions by a wide range of stakeholders, including community-based organizations, parent–teacher associations, workplaces, faith-based organizations, and pediatric and primary care practices.
- The Centers for Disease Control and Prevention (CDC) Division of Adolescent and School Health should work in partnership with parents and guardians, parent–teacher associations, states, districts, and local school boards to establish standard evidence-based guidelines for school-based comprehensive sexual health education that is grounded in psychosocial and behavioral theories and research. To ensure that each student receives medically accurate, age-appropriate, and culturally inclusive comprehensive sexual health education in elementary, middle, and high school, dedicated staff, including school-based nurses and health educators, should be trained, provided adequate time, and given necessary resources.
- CDC, in collaboration with state and local departments of health, should develop and evaluate the efficacy of promising community-based approaches that are grounded in psychosocial and behavioral research, extend reach into affected communities, foster ongoing collaboration with community stakeholders for capacity building and sustainability, and provide allocation of sustained dedicated resources for formative work, intervention implementation, evaluation, replication, and scale-up of evidence-based interventions.
REFERENCES
Aarons, G. A., M. G. Ehrhart, L. R. Farahnak, and M. Sklar. 2014. Aligning leadership across systems and organizations to develop a strategic climate for evidence-based practice implementation. Annual Review of Public Health 35:255-274.
Aarons, G. A., M. G. Ehrhart, L. R. Farahnak, and M. S. Hurlburt. 2015. Leadership and Organizational Change for Implementation (LOCI): A randomized mixed method pilot study of a leadership and organization development intervention for evidence-based practice implementation. Implementation Science 10:11.
Aarons, G. A., M. G. Ehrhart, J. C. Moullin, E. M. Torres, and A. E. Green. 2017a. Testing the Leadership and Organizational Change for Implementation (LOCI) intervention in substance abuse treatment: A cluster randomized trial study protocol. Implementation Science 12(1):29.
Aarons, G. A., M. Sklar, B. Mustanski, N. Benbow, and C. H. Brown. 2017b. “Scaling-out” evidence-based interventions to new populations or new health care delivery systems. Implementation Science 12(1):111.
Abad, N., B. N. Baack, A. O’Leary, Y. Mizuno, J. H. Herbst, and C. M. Lyles. 2015. A systematic review of HIV and STI behavior change interventions for female sex workers in the United States. AIDS and Behavior 19(9):1701-1719.
Abara, W., J. D. Coleman, A. Fairchild, B. Gaddist, and J. White. 2015. A faith-based community partnership to address HIV/AIDS in the southern United States: Implementation, challenges, and lessons learned. Journal of Religion and Health 54(1):122-133.
Adimora, A. A., and J. D. Auerbach. 2010. Structural interventions for HIV prevention in the United States. Journal of Acquired Immune Deficiency Syndromes 55:S132-S135.
Ajzen, I. 1991. The theory of planned behavior. Organizational Behavior and Human Decision Processes 50(2):179-211.
Ajzen, I., and M. Fishbein. 1980. Understanding attitudes and predicting social behavior. Englewood Cliffs, NJ: Prentice-Hall.
Akbar, M. B., J. French, and A. Lawson. 2020. Use of social marketing principles in sexual health: An exploratory review. Social Business. 1-25.
Allen, J. D., L. A. Linnan, K. M. Emmons, R. Brownson, G. Colditz, and E. Proctor. 2012. Fidelity and its relationship to implementation effectiveness, adaptation, and dissemination. In Dissemination and implementation research in health: Translating science to practice. Oxford, England: Oxford University Press. Pp. 281-304.
Amirkhanian, Y. A. 2014. Social networks, sexual networks and HIV risk in men who have sex with men. Current HIV/AIDS Reports 11(1):81-92.
Auerswald, C. L., E. Sugano, J. M. Ellen, and J. D. Klausner. 2006. Street-based STD testing and treatment of homeless youth are feasible, acceptable and effective. Journal of Adolescent Health 38(3):208-212.
Bandura, A. 1977. Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review 84(2):191-215.
Bandura, A. 1986. Social foundations of thought and action: A social cognitive theory. Englewood Cliffs, NJ: Prentice-Hall.
Bandura, A. 1994. Social cognitive theory of mass communication. In Media effects: Advances in theory and research, LEA communication series. Hillsdale, NJ: Lawrence Erlbaum Associates. Pp. 61-90.
Bandura, A. 2011. The social and policy impact of social cognitive theory. In Social psychology and evaluation, edited by M. M. Mark, S. I. Donaldson, and B. Campbell. New York: The Guilford Press. Pp. 31-71.
Bangi, A., M. M. Dolcini, G. W. Harper, C. B. Boyer, and L. M. Pollack. 2013. Psychosocial outcomes of sexual risk reduction in a brief intervention for urban African American female adolescents. Journal of HIV/AIDS & Social Services 12(2):146-159.
Barham, L., D. Lewis, and N. Latimer. 2007. One to one interventions to reduce sexually transmitted infections and under the age of 18 conceptions: A systematic review of the economic evaluations. Sexually Transmitted Infections 83(6):441.
Bauermeister, J. A., E. S. Pingel, L. Jadwin-Cakmak, G. W. Harper, K. Horvath, G. Weiss, and P. Dittus. 2015. Acceptability and preliminary efficacy of a tailored online HIV/STI testing intervention for young men who have sex with men: The Get Connected! Program. AIDS and Behavior 19(10):1860-1874.
Bauermeister, J. A., R. C. Tingler, M. Demers, D. Connochie, G. Gillard, J. Shaver, T. Chavanduka, and G. W. Harper. 2019. Acceptability and preliminary efficacy of an online HIV prevention intervention for single young men who have sex with men seeking partners online: The Mydex project. AIDS and Behavior 23(11):3064-3077.
Blandford, J. M., and T. L. Gift. 2006. Productivity losses attributable to untreated chlamydial infection and associated pelvic inflammatory disease in reproductive-aged women. Sexually Transmitted Diseases 33(10 Suppl):S117-S121.
Boyer, C. B., J. M. Tschann, and M.-A. Shafer. 1999. Predictors of risk for sexually transmitted diseases in ninth grade urban high school students. Journal of Adolescent Research 14(4):448-465.
Boyer, C. B., M.-A. Shafer, C. J. Wibbelsman, D. Seeberg, E. Teitle, and N. Lovell. 2000. Associations of sociodemographic, psychosocial, and behavioral factors with sexual risk and sexually transmitted diseases in teen clinic patients. Journal of Adolescent Health 27(2):102-111.
Boyer, C. B., J. Sieverding, J. Siller, A. Gallaread, and Y. J. Chang. 2007. Youth united through health education: Community-level, peer-led outreach to increase awareness and improve noninvasive sexually transmitted infection screening in urban African American youth. Journal of Adolescent Health 40(6):499-505.
Boyer, C. B., L. Hightow-Weidman, J. Bethel, S. X. Li, L. Henry-Reid, D. Futterman, D. Maturo, D. M. Straub, K. Howell, S. Reid, J. Lowe, B. G. Kapogiannis, and J. M. Ellen. 2013. An assessment of the feasibility and acceptability of a friendship-based social network recruitment strategy to screen at-risk African American and Hispanic/Latina young women for HIV infection. JAMA Pediatrics 167(3):289-296.
Boyer, C. B., G. M. Robles-Schrader, S. X. Li, R. L. Miller, J. Korelitz, G. N. Price, C. M. Rivera Torres, K. S. Chutuape, S. J. Stines, D. M. Straub, L. Peralta, I. Febo, L. Hightow-Weidman, R. Gonin, B. G. Kapogiannis, and J. M. Ellen. 2014. A comparison of network-based strategies for screening at-risk Hispanic/Latino adolescents and young adults for undiagnosed asymptomatic HIV infection. Journal of Adolescent Health 55(6):765-773.
Brawner, B. M., J. L. Baker, J. Stewart, Z. M. Davis, J. Cederbaum, and L. S. Jemmott. 2013. “The black man’s country club”: Assessing the feasibility of an HIV risk-reduction program for young heterosexual African American men in barbershops. Family & Community Health 36(2):109-118.
Brewin, D., A. Koren, B. Morgan, S. Shipley, and R. L. Hardy. 2014. Behind closed doors: School nurses and sexual education. Journal of School Nursing 30(1):31-41.
Brigham, K. S., M. J. Peer, B. B. Ghoshhajra, and J. P. T. Co. 2020. Increasing vaginal chlamydia trachomatis testing in adolescent and young adults. Pediatrics 146(2).
Brody, G. H., V. M. Murry, M. Gerrard, F. X. Gibbons, V. Molgaard, L. McNair, A. C. Brown, T. A. Wills, R. L. Spoth, Z. Luo, Y. F. Chen, and E. Neubaum-Carlan. 2004. The strong African American families program: Translating research into prevention programming. Child Development 75(3):900-917.
Bronfenbrenner, U. 1979. The ecology of human development. Cambridge, MA: Harvard University Press.
Bronfenbrenner, U. 1986. Ecology of the family as a context for human development: Research perspectives. Developmental Psychology 22(6):723-742.
Brown, C. A., and R. J. Lilford. 2006. The stepped wedge trial design: A systematic review. BMC Medical Research Methodology 6(1):54.
Brown, C. H., T. R. Ten Have, B. Jo, G. Dagne, P. A. Wyman, B. Muthén, and R. D. Gibbons. 2009. Adaptive designs for randomized trials in public health. Annual Review of Public Health 30:1-25.
Brown, C. H., G. Curran, L. A. Palinkas, G. A. Aarons, K. B. Wells, L. Jones, L. M. Collins, N. Duan, B. S. Mittman, A. Wallace, R. G. Tabak, L. Ducharme, D. A. Chambers, G. Neta, T. Wiley, J. Landsverk, K. Cheung, and G. Cruden. 2017. An overview of research and evaluation designs for dissemination and implementation. Annual Review of Public Health 38:1-22.
Brückner, H., and P. Bearman. 2005. After the promise: The STD consequences of adolescent virginity pledges. Journal of Adolescent Health 36(4):271-278.
Bull, S. S., D. K. Levine, S. R. Black, S. J. Schmiege, and J. Santelli. 2012. Social media-delivered sexual health intervention: A cluster randomized controlled trial. American Journal of Preventive Medicine 43(5):467-474.
Cameron, A., E. Smith, N. Mercer, and B. Sundstrom. 2020. “It is our duty”: Understanding parents’ perspectives on reproductive and sexual health education. Sexual Education 20(5):535-551.
Carr, J. B., and A. Packham. 2017. The effects of state-mandated abstinence-based sex education on teen health outcomes. Health Economics 26(4):403-420.
Caruthers, A. S., M. J. Van Ryzin, and T. J. Dishion. 2014. Preventing high-risk sexual behavior in early adulthood with family interventions in adolescence: Outcomes and developmental processes. Prevention Science (15 Suppl 1):S59-S69.
Catania, J. A., S. M. Kegeles, and T. J. Coates. 1990. Towards an understanding of risk behavior: An AIDS Risk Reduction Model (ARRM). Health Education Quarterly 17(1):53-72.
CDC (Centers for Disease Control and Prevention). 2019a. Community approaches to reducing STDs: Community engagement toolkit. Atlanta, GA: Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, Division of STD Prevention, Office of Health Equity.
CDC. 2019b. School health profiles 2018: Characteristics of health programs among secondary schools. Atlanta, GA: Centers for Disease Control and Prevention.
CDC. 2020a. Compendium of evidence-based interventions and best practices for HIV prevention. https://www.cdc.gov/hiv/research/interventionresearch/compendium/index.html (accessed November 12, 2020).
CDC. 2020b. Community approaches to reducing sexually transmitted diseases. Atlanta, GA: Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, Division of STD Prevention, Office of Health Equity.
CDC AIDS Community Demonstration Projects Research Group. 1999. Community-level HIV intervention in 5 cities: Final outcome data from the CDC AIDS community demonstration projects. American Journal of Public Health 89(3):336-345.
Champion, J. D., B. Harlin, and J. L. Collins. 2013. Sexual risk behavior and STI health literacy among ethnic minority adolescent women. Applied Nursing Research 26(4):204-209.
Champion, V. L., and C. S. Skinner. 2008. The health belief model. In Health behavior and health education: Theory, research, and practice, 4th ed., edited by K. Glanz, B. K. Rimer, and K. Viswanath. San Francisco, CA: Jossey-Bass. Pp. 45-65.
Charania, M. R., N. Crepaz, C. Guenther-Gray, K. Henny, A. Liau, L. A. Willis, and C. M. Lyles. 2011. Efficacy of structural-level condom distribution interventions: A meta-analysis of U.S. and international studies, 1998-2007. AIDS and Behavior 15(7):1283-1297.
Chin, H. B., T. A. Sipe, R. Elder, S. L. Mercer, S. K. Chattopadhyay, V. Jacob, H. R. Wethington, D. Kirby, D. B. Elliston, M. Griffith, S. O. Chuke, S. C. Briss, I. Ericksen, J. S. Galbraith, J. H. Herbst, R. L. Johnson, J. M. Kraft, S. M. Noar, L. M. Romero, and J. Santelli. 2012. The effectiveness of group-based comprehensive risk-reduction and abstinence education interventions to prevent or reduce the risk of adolescent pregnancy, human immunodeficiency virus, and sexually transmitted infections: Two systematic reviews for the guide to community preventive services. American Journal of Preventative Medicine 42(3):272-294.
Chinman, M., P. Imm, A. Wandersman, S. Kaftarian, J. Neal, K. T. Pendleton, and C. Ringwalt. 2001. Using the Getting to Outcomes (GTO) model in a statewide prevention initiative. Health Promotion Practice 2(4):302-309.
Chinman, M., S. B. Hunter, P. Ebener, S. M. Paddock, L. Stillman, P. Imm, and A. Wandersman. 2008. The Getting to Outcomes demonstration and evaluation: An illustration of the prevention support system. American Journal of Community Psychology 41(3-4):206-224.
Chinman, M., J. Acosta, P. Ebener, P. S. Malone, and M. E. Slaughter. 2018. A cluster-randomized trial of Getting to Outcomes’ impact on sexual health outcomes in community-based settings. Prevention Science 19(4):437-448.
Chutuape, K. S., M. Ziff, C. Auerswald, M. Castillo, A. McFadden, and J. Ellen. 2009. Examining differences in types and location of recruitment venues for young males and females from urban neighborhoods: Findings from a multi-site HIV prevention study. Journal of Urban Health 86(1):31-42.
Collins, L. M. 2018. Optimization of behavioral, biobehavioral, and biomedical interventions: The multiphase optimization strategy (MOST). Cham, Switzerland: Springer International Publishing AG.
Collins, L. M., K. C. Kugler, and M. V. Gwadz. 2016. Optimization of multicomponent behavioral and biobehavioral interventions for the prevention and treatment of HIV/AIDS. AIDS and Behavior (20 Suppl 1):S197-S214.
Community Preventive Services Task Force. 2015. 2014-2015 annual report to Congress, federal agencies and prevention stakeholders, including a special update on recommendations to prevent cancers. https://www.thecommunityguide.org/sites/default/files/assets/2015congress-report-full_0.pdf (accessed February 22, 2021).
Conner, M., and P. Norman. 2005. Predicting health behaviour: A social cognition approach. Predicting Health Behaviour:1-27.
Covey, J., H. E. Rosenthal-Stott, and S. J. Howell. 2016. A synthesis of meta-analytic evidence of behavioral interventions to reduce HIV/STIs. Journal of Behavioral Medicine 39(3):371-385.
Crepaz, N., A. K. Horn, S. M. Rama, T. Griffin, J. B. Deluca, M. M. Mullins, and S. O. Aral. 2007. The efficacy of behavioral interventions in reducing HIV risk sex behaviors and incident sexually transmitted disease in black and Hispanic sexually transmitted disease clinic patients in the United States: A meta-analytic review. Sexually Transmitted Diseases 34(6):319-332.
Crepaz, N., K. J. Marshall, L. W. Aupont, E. D. Jacobs, Y. Mizuno, L. S. Kay, P. Jones, D. H. McCree, and A. O’Leary. 2009. The efficacy of HIV/STI behavioral interventions for African American females in the United States: A meta-analysis. American Journal of Public Health 99(11):2069-2078.
Daniel-Ulloa, J., M. Ulibarri, B. Baquero, C. Sleeth, H. Harig, and S. D. Rhodes. 2016. Behavioral HIV prevention interventions among Latinas in the U.S.: A systematic review of the evidence. Journal of Immigrant and Minority Health 18(6):1498-1521.
De Vasconcelos, S., I. Toskin, B. Cooper, M. Chollier, R. Stephenson, K. Blondeel, T. Troussier, and J. Kiarie. 2018. Behaviour change techniques in brief interventions to prevent HIV, STI and unintended pregnancies: A systematic review. PLoS One 13(9):e0204088.
Dearing, J. W., and K. F. Kee. 2012. Historical roots of dissemination and implementation science. Dissemination and Implementation Research in Health: Translating Science to Practice 55:71.
Denford, S., C. Abraham, R. Campbell, and H. Busse. 2017. A comprehensive review of reviews of school-based interventions to improve sexual-health. Health Psychology Review 11(1):33-52.
Derose, K. P., B. A. Griffin, D. E. Kanouse, L. M. Bogart, M. V. Williams, A. C. Haas, K. R. Flórez, D. O. Collins, J. Hawes-Dawson, M. A. Mata, C. W. Oden, and B. D. Stucky. 2016. Effects of a pilot church-based intervention to reduce HIV stigma and promote HIV testing among African Americans and Latinos. AIDS and Behavior 20(8):1692-1705.
Deverka, P. A., D. C. Lavallee, P. J. Desai, L. C. Esmail, S. D. Ramsey, D. L. Veenstra, and S. R. Tunis. 2012. Stakeholder participation in comparative effectiveness research: Defining a framework for effective engagement. Journal of Comparative Effectiveness Research 1(2):181-194.
DiClemente, R. J., L. F. Salazar, and R. A. Crosby. 2007. A review of STD/HIV preventive interventions for adolescents: Sustaining effects using an ecological approach. Journal of Pediatric Psychology 32(8):888-906.
DiClemente, R. J., C. P. Crittenden, E. Rose, J. M. Sales, G. M. Wingood, R. A. Crosby, and L. F. Salazar. 2008. Psychosocial predictors of HIV-associated sexual behaviors and the efficacy of prevention interventions in adolescents at-risk for HIV infection: What works and what doesn’t work? Psychosomatic Medicine 70(5):598-605.
DiClemente, R. J., G. M. Wingood, J. M. Sales, J. L. Brown, E. S. Rose, T. L. Davis, D. L. Lang, A. Caliendo, and J. W. Hardin. 2014. Efficacy of a telephone-delivered sexually transmitted infection/human immunodeficiency virus prevention maintenance intervention for adolescents: A randomized clinical trial. JAMA Pediatrics 168(10):938-946.
Dolcini, M. M., G. W. Harper, C. B. Boyer, and L. M. Pollack. 2010. Project ORE: A friendship-based intervention to prevent HIV/STI in urban African American adolescent females. Health Education & Behavior 37(1):115-132.
Dworkin, S. L., R. M. Pinto, J. Hunter, B. Rapkin, and R. H. Remien. 2008. Keeping the spirit of community partnerships alive in the scale up of HIV/AIDS prevention: Critical reflections on the roll out of DEBI (diffusion of effective behavioral interventions). American Journal of Community Psychology 42(1-2):51-59.
Eaton, L. A., T. B. Huedo-Medina, S. C. Kalichman, J. A. Pellowski, M. J. Sagherian, M. Warren, A. R. Popat, and B. T. Johnson. 2012. Meta-analysis of single-session behavioral interventions to prevent sexually transmitted infections: Implications for bundling prevention packages. American Journal of Public Health 102(11):e34-e44.
Egeland, K. M., A. S. Skar, M. Endsjø, E. H. Laukvik, H. Bækkelund, A. Babaii, L. B. Granly, G. K. Husebø, R. H. Borge, M. G. Ehrhart, M. Sklar, C. H. Brown, and G. A. Aarons. 2019. Testing the Leadership and Organizational Change for Implementation (LOCI) intervention in Norwegian mental health clinics: A stepped-wedge cluster randomized design study protocol. Implementation Science 14(1):28.
Eisenberg, M. E., N. Madsen, J. A. Oliphant, and R. E. Sieving. 2013. Barriers to providing the sexuality education that teachers believe students need. Journal of School Health 83(5):335-342.
Ellen, J. M., C. Gaydos, S. E. Chung, N. Willard, L. V. Lloyd, and C. A. Rietmeijer. 2006. Sex partner selection, social networks, and repeat sexually transmitted infections in young men: A preliminary report. Sexually Transmitted Diseases 33(1):18-21.
Escoffery, C., E. Lebow-Skelley, R. Haardoerfer, E. Boing, H. Udelson, R. Wood, M. Hartman, M. E. Fernandez, and P. D. Mullen. 2018. A systematic review of adaptations of evidence-based public health interventions globally. Implementation Science 13(1):125.
Espada, J. P., A. Morales, A. Guillén-Riquelme, R. Ballester, and M. Orgilés. 2016. Predicting condom use in adolescents: A test of three socio-cognitive models using a structural equation modeling approach. BMC Public Health 16:35.
Estrada, Y., T. K. Lee, S. Huang, M. I. Tapia, M. R. Velázquez, M. J. Martinez, H. Pantin, M. A. Ocasio, D. C. Vidot, L. Molleda, J. Villamar, B. A. Stepanenko, C. H. Brown, and G. Prado. 2017. Parent-centered prevention of risky behaviors among Hispanic youths in Florida. American Journal of Public Health 107(4):607-613.
Estrada, Y., T. K. Lee, R. Wagstaff, M. R. L, M. I. Tapia, M. R. Velázquez, K. Sardinas, H. Pantin, M. Y. Sutton, and G. Prado. 2019. eHealth Familias Unidas: Efficacy trial of an evidence-based intervention adapted for use on the Internet with Hispanic families. Prevention Science 20(1):68-77.
Ethier, K. A., P. J. Dittus, C. J. DeRosa, E. Q. Chung, E. Martinez, and P. R. Kerndt. 2011. School-based health center access, reproductive health care, and contraceptive use among sexually experienced high school students. Journal of Adolescent Health 48(6):562-565.
Evans, C., and H. Lambert. 2008. Implementing community interventions for HIV prevention: Insights from project ethnography. Social Science & Medicine 66(2):467-478.
Ewan, L. A., D. McLinden, F. Biro, M. DeJonckheere, and L. M. Vaughn. 2016. Mapping the views of adolescent health stakeholders. Journal of Adolescent Health 58(1):24-32.
Facebook. 2018. Mark Zuckerberg facebook post. https://www.facebook.com/zuck/posts/10104413015393571 (accessed November 16, 2020).
Fernandez, M. A., and S. M. Eyberg. 2009. Predicting treatment and follow-up attrition in parent-child interaction therapy. Journal of Abnormal Child Psychology 37(3):431-441.
Fishbein, M., and I. Ajzen. 1975. Belief, attitude, intention and behaviour: An introduction to theory and research. Reading, MA: Addison-Wesley.
Fisher, J. D., and W. A. Fisher. 1992. Changing AIDS-risk behavior. Psychological Bulletin 111(3):455-474.
Fisher, J., W. Fisher, S. Williams, and T. Malloy. 1994. Empirical tests of an information-motivation-behavioral skills model of AIDS-preventive behavior with gay men and heterosexual university students. Health Psychology 13:238-250.
Fisher, W. A., S. S. Williams, J. D. Fisher, and T. E. Malloy. 1999. Understanding AIDS risk behavior among sexually active urban adolescents: An empirical test of the information–motivation–behavioral skills model. AIDS and Behavior 3(1):13-23.
Flay, B. R., A. Biglan, R. F. Boruch, F. G. Castro, D. Gottfredson, S. Kellam, E. K. Mościcki, S. Schinke, J. C. Valentine, and P. Ji. 2005. Standards of evidence: Criteria for efficacy, effectiveness and dissemination. Prevention Science 6(3):151-175.
Fox, S. n.d. Key data points on U.S. teens and adults. https://susannahfox.com/research (accessed November 17, 2020).
Francis, D. B., S. M. Noar, D. A. Fortune, and A. A. Adimora. 2018. “Be straight up and so will he”: Evaluation of a novel HIV prevention condom distribution and health communication intervention targeting young African American females. AIDS Education and Prevention 30(2):137-151.
Friedman, A. L., R. E. Kachur, S. M. Noar, and M. McFarlane. 2016. Health communication and social marketing campaigns for sexually transmitted disease prevention and control: What is the evidence of their effectiveness? Sexually Transmitted Diseases 43(2):S83-S101.
Friedman, S. R., M. J. Downing, Jr., P. Smyrnov, G. Nikolopoulos, J. A. Schneider, B. Livak, G. Magiorkinis, L. Slobodianyk, T. I. Vasylyeva, D. Paraskevis, M. Psichogiou, V. Sypsa, M. M. Malliori, and A. Hatzakis. 2014. Socially-integrated transdisciplinary HIV prevention. AIDS and Behavior 18(10):1821-1834.
Garett, R., and S. D. Young. 2019. Health care gamification: A study of game mechanics and elements. Technology, Knowledge and Learning 24(3):341-353.
Gerrard, M., F. X. Gibbons, A. E. Houlihan, M. L. Stock, and E. A. Pomery. 2008. A dual-process approach to health risk decision making: The prototype willingness model. Developmental Review 28(1):29-61.
Globerman, J., S. Mitra, D. Gogolishvili, S. Rueda, L. Schoffel, K. Gangbar, Q. Shi, and S. B. Rourke. 2017. HIV/STI prevention interventions: A systematic review and meta-analysis. Open Medicine 12:450-467.
González-Guarda, R. M., B. E. McCabe, A. Florom-Smith, R. Cianelli, and N. Peragallo. 2011. Substance abuse, violence, HIV, and depression: An underlying syndemic factor among latinas. Nursing Research 60(3):182-189.
Grabowski, M. K., J. T. Herbeck, and A. F. Y. Poon. 2018. Genetic cluster analysis for HIV prevention. Current HIV/AIDS Reports 15(2):182-189.
Griffith, D. M., L. C. Pichon, B. Campbell, and J. O. Allen. 2010. Your blessed health: A faith-based CBPR approach to addressing HIV/AIDS among African Americans. AIDS Education and Prevention 22(3):203-217.
Guilamo-Ramos, V., J. Jaccard, and E. Casillas. 2004. The Parents Matter! Program: Practical, theoretical and methodological perspectives. Journal of Child and Family Studies 13(1):113-123.
Guilamo-Ramos, V., J. Jaccard, P. Dittus, A. Bouris, B. Gonzalez, E. Casillas, and S. Banspach. 2011. A comparative study of interventions for delaying the initiation of sexual intercourse among Latino and black youth. Perspectives on Sexual Reproductive Health 43(4):247-254.
Guilamo-Ramos, V., A. Benzekri, and M. Thimm-Kaiser. 2019. Parent-based interventions to affect adolescent sexual and reproductive health: Reconsidering the best evidence vs all evidence. JAMA Pediatrics 173(9):821-823.
Guilamo-Ramos, V., A. Benzekri, M. Thimm-Kaiser, P. Dittus, Y. Ruiz, C. M. Cleland, and W. McCoy. 2020. A triadic intervention for adolescent sexual health: A randomized clinical trial. Pediatrics 145(5):e20192808.
Guttmacher Institute. 2020. Sex and HIV education. https://www.guttmacher.org/statepolicy/explore/sex-and-hiv-education (accessed November 12, 2020).
Hall, K. S., J. McDermott Sales, K. A. Komro, and J. Santelli. 2016. The state of sex education in the United States. Journal of Adolescent Health 58(6):595-597.
Hanley, S. M., C. Ringwalt, S. T. Ennett, A. A. Vincus, J. M. Bowling, S. W. Haws, and L. A. Rohrbach. 2010. The prevalence of evidence-based substance use prevention curricula in the nation’s elementary schools. Journal of Drug Education 40(1):51-60.
Hawkins, J. D., R. F. Catalano, M. W. Arthur, E. Egan, E. C. Brown, R. D. Abbott, and D. M. Murray. 2008. Testing Communities That Care: The rationale, design and behavioral baseline equivalence of the community youth development study. Prevention Science 9(3):178-190.
Hawkins, J. D., S. Oesterle, E. C. Brown, M. W. Arthur, R. D. Abbott, A. A. Fagan, and R. F. Catalano. 2009. Results of a type 2 translational research trial to prevent adolescent drug use and delinquency: A test of Communities That Care. Archives of Pediatrics & Adolescent Medicine 163(9):789-798.
Head, K. J., S. M. Noar, N. T. Iannarino, and N. Grant Harrington. 2013. Efficacy of text messaging-based interventions for health promotion: A meta-analysis. Social Science & Medicine 97:41-48.
Hekler, E. B., S. Michie, M. Pavel, D. E. Rivera, L. M. Collins, H. B. Jimison, C. Garnett, S. Parral, and D. Spruijt-Metz. 2016. Advancing models and theories for digital behavior change interventions. American Journal of Preventive Medicine 51(5):825-832.
Henderson, J. T., C. A. Senger, M. Henninger, S. I. Bean, N. Redmond, and E. A. O’Connor. 2020. Behavioral counseling interventions to prevent sexually transmitted infections: Updated evidence report and systematic review for the U.S. Preventive Services Task Force. JAMA 324(7):682-699.
Herbst, J. H., C. Beeker, A. Mathew, T. McNally, W. F. Passin, L. S. Kay, N. Crepaz, C. M. Lyles, P. Briss, S. Chattopadhyay, and R. L. Johnson. 2007. The effectiveness of individual-, group-, and community-level HIV behavioral risk-reduction interventions for adult men who have sex with men: A systematic review. American Journal of Preventative Medicine 32(4 Suppl):S38-S67.
Hogben, M., H. Chesson, and S. O. Aral. 2010. Sexuality education policies and sexually transmitted disease rates in the United States of America. International Journal of STD & AIDS 21(4):293-297.
Hunter, R. F., K. de la Haye, J. M. Murray, J. Badham, T. W. Valente, M. Clarke, and F. Kee. 2019. Social network interventions for health behaviours and outcomes: A systematic review and meta-analysis. PLoS Medicine 16(9):e1002890.
IOM (Institute of Medicine). 2014. Strategies for scaling effective family-focused preventive interventions to promote children’s cognitive, affective, and behavioral health: Workshop summary. Washington, DC: The National Academies Press.
Israel, B. A., E. A. Parker, Z. Rowe, A. Salvatore, M. Minkler, J. López, A. Butz, A. Mosley, L. Coates, G. Lambert, P. A. Potito, B. Brenner, M. Rivera, H. Romero, B. Thompson, G. Coronado, and S. Halstead. 2005. Community-based participatory research: Lessons learned from the Centers for Children’s Environmental Health and Disease Prevention Research. Environmental Health Perspectives 113(10):1463-1471.
Janz, N. K., and M. H. Becker. 1984. The health belief model: A decade later. Health Education Quarterly 11(1):1-47.
Jemmott, J. B., 3rd, L. S. Jemmott, G. T. Fong, and K. McCaffree. 1999. Reducing HIV risk-associated sexual behavior among African American adolescents: Testing the generality of intervention effects. American Journal of Community Psychology 27(2):161-187.
Jemmott, L. S., J. B. Jemmott, Y. Lanier, C. Thompson, and J. L. Baker. 2017. Development of a barbershop-based HIV/STI risk reduction intervention for young heterosexual African American men. Health Promotion Practice 18(1):110-118.
Jemmott, L. S., J. B. Jemmott, 3rd, L. D. Icard, and J. Hsu. 2020. Effects of church-based parent-child abstinence-only interventions on adolescents’ sexual behaviors. Journal of Adolescent Health 66(1):107-114.
Jenkins, R. A. 2014. Supplemental issue on does early intervention prevent health-risking sexual behaviors related to HIV/AIDS: Commentary on effects. Prevention Science 15(1):84-86.
Jensen, M. R., J. J. Wong, N. A. Gonzales, L. E. Dumka, R. Millsap, and S. Coxe. 2014. Long-term effects of a universal family intervention: Mediation through parent-adolescent conflict. Journal of Clinical Child & Adolescent Psychology 43(3):415-427.
Johnson, M. O. 2011. The shifting landscape of health care: Toward a model of health care empowerment. American Journal of Public Health 101(2):265-270.
Johnson, R. L., P. D. Stanford, W. Douglas, Jr., G. Botwinick, and E. Marino. 2001. High-risk sexual behaviors among adolescents engaged through a street-based peer outreach program—(the Adolescent HIV Project). Journal of the National Medical Association 93(5):170-177.
Johnson-Motoyama, M., M. Moses, T. K. Kann, E. S. Mariscal, M. Levy, C. Navarro, and P. J. Fite. 2016. Parent, teacher, and school stakeholder perspectives on adolescent pregnancy prevention programming for Latino youth. Journal of Primary Prevention 37(6):513-525.
Kanamori, M., M. Rosa, C. H. Shrader, C. Munayco, S. Doblecki-Lewis, G. Prado, S. Safren, M. J. Trepka, and K. Fujimoto. 2019. Progreso en salud: Findings from two adapted social network HIV risk reduction interventions for Latina seasonal workers. International Journal of Environmental Research and Public Health 16(22).
Kegeles, S. M., and G. J. Hart. 1998. Recent HIV-prevention interventions for gay men: Individual, small-group and community-based studies. AIDS (12 Suppl A):S209-S215.
Kegeles, S. M., R. B. Hays, and T. J. Coates. 1996. The Mpowerment Project: A community-level HIV prevention intervention for young gay men. American Journal of Public Health 86(8):1129-1136.
Kelly, J. A., J. S. St Lawrence, Y. E. Diaz, L. Y. Stevenson, A. C. Hauth, T. L. Brasfield, S. C. Kalichman, J. E. Smith, and M. E. Andrew. 1991. HIV risk behavior reduction following intervention with key opinion leaders of population: An experimental analysis. American Journal of Public Health 81(2):168-171.
Kerrigan, D. L., V. A. Fonner, S. Stromdahl, and C. E. Kennedy. 2013. Community empowerment among female sex workers is an effective HIV prevention intervention: A systematic review of the peer-reviewed evidence from low- and middle-income countries. AIDS and Behavior 17(6):1926-1940.
KFF (Kaiser Family Foundation). 2018. Abstinence education programs: Definition, funding, and impact on teen sexual behavior. https://www.kff.org/womens-health-policy/factsheet/abstinence-education-programs-definition-funding-and-impact-on-teen-sexualbehavior (accessed November 12, 2020).
Kimbrough, L. W., H. E. Fisher, K. T. Jones, W. Johnson, S. Thadiparthi, and S. Dooley. 2009. Accessing social networks with high rates of undiagnosed HIV infection: The Social Networks demonstration project. American Journal of Public Health 99(6):1093-1099.
Kiousis, S. 2002. Interactivity: A concept explication. New Media and Society 4(3):355-384.
Kirby, D. 2007. Emerging answers: Research findings on programs to reduce teen pregnancy and sexually transmitted diseases. https://powertodecide.org/sites/default/files/resources/primary-download/emerging-answers.pdf (accessed November 12, 2020).
Klovdahl, A. S., J. J. Potterat, D. E. Woodhouse, J. B. Muth, S. Q. Muth, and W. W. Darrow. 1994. Social networks and infectious disease: The Colorado Springs study. Social Science & Medicine 38(1):79-88.
Kocsis, T. 2020. A critical analysis of sexuality education in the United States: Toward an inclusive curriculum for social justice. New York: Routledge.
Krebs, P., J. O. Prochaska, and J. S. Rossi. 2010. A meta-analysis of computer-tailored interventions for health behavior change. Preventive Medicine 51(3-4):214-221.
Leslie, L. K., C. J. Mehus, J. D. Hawkins, T. Boat, M. A. McCabe, S. Barkin, E. C. Perrin, C. W. Metzler, G. Prado, V. F. Tait, R. Brown, and W. Beardslee. 2016. Primary health care: Potential home for family-focused preventive interventions. American Journal of Preventative Medicine 51(4 Suppl 2):S106-S118.
Leventhal, H. 1973. Changing attitudes and habits to reduce risk factors in chronic disease. American Journal of Cardiology 31(5):571-580.
Li, D. H., D. A. Moskowitz, K. Macapagal, R. Saber, and B. Mustanski. 2020. Using intervention mapping to developmentally adapt an online HIV risk reduction program for adolescent men who have sex with men. Prevention Science 21(7):885-897.
Lightfoot, A. F., T. Taggart, B. A. Woods-Jaeger, L. Riggins, M. R. Jackson, and E. Eng. 2014. Where is the faith? Using a CBPR approach to propose adaptations to an evidence-based HIV prevention intervention for adolescents in African American faith settings. Journal of Religion and Health 53(4):1223-1235.
Lightfoot, M. A., C. K. Campbell, N. Moss, S. Treves-Kagan, E. Agnew, M. S. Kang Dufour, H. Scott, A. M. Sa’id, and S. A. Lippman. 2018. Using a social network strategy to distribute HIV self-test kits to African American and Latino MSM. Journal of Acquired Immune Deficiency Syndromes 79(1):38-45.
Logan, T. K., J. Cole, and C. Leukefeld. 2002. Women, sex, and HIV: Social and contextual factors, meta-analysis of published interventions, and implications for practice and research. Psychological Bulletin 128(6):851-885.
Long, L., C. Abraham, R. Paquette, M. Shahmanesh, C. Llewellyn, A. Townsend, and R. Gilson. 2016. Brief interventions to prevent sexually transmitted infections suitable for in-service use: A systematic review. Preventive Medicine 91:364-382.
Lopez, L. M., T. W. Grey, M. Chen, E. E. Tolley, and L. L. Stockton. 2016. Theory-based interventions for contraception. Cochrane Database of Systematic Reviews 11(11):CD007249.
Love, H., S. Soleimanpour, N. Panchal, J. Schlitt, C. Behr, and M. Even. 2018. 2016-17 national school-based health care census report. Washington, DC: School-Based Health Alliance.
Love, H. E., J. Schlitt, S. Soleimanpour, N. Panchal, and C. Behr. 2019. Twenty years of school-based health care growth and expansion. Health Affairs (Millwood) 38(5):755-764.
Lugo-Gil, J., A. Lee, D. Vohra, K. Adamek, J. Lacoe, and B. Goesling. 2016. Updated findings from the HHS teen pregnancy prevention evidence review: July 2014 through August 2015. Washington, DC: Department of Health and Human Services.
Lustria, M. L. A., J. Cortese, S. M. Noar, and R. L. Glueckauf. 2009. Computer-tailored health interventions delivered over the web: Review and analysis of key components. Patient Education and Counseling 74(2):156-173.
Lustria, M. L. A., S. M. Noar, J. Cortese, S. K. Van Stee, R. L. Glueckauf, and J. Lee. 2013. A meta-analysis of web-delivered tailored health behavior change interventions. Journal of Health Communication 18(9):1039-1069.
Malekinejad, M., A. Parriott, J. C. Blodgett, H. Horvath, R. K. Shrestha, A. B. Hutchinson, P. Volberding, and J. G. Kahn. 2017. Effectiveness of community-based condom distribution interventions to prevent HIV in the United States: A systematic review and meta-analysis. PLoS One 12(8):e0180718.
McAlister, A. L., C. L. Perry, and G. S. Parcel. 2008. How individuals, environments, and health behaviors interact: Social cognitive theory. In Health behavior and health education: Theory, research, and practice, 4th ed., edited by K. Glanz, B. K. Rimer, and K. Viswanath. San Francisco, CA: Jossey-Bass. Pp. 169-188.
McDade, R. S., R. A. Vidourek, K. S. Biradar, K. A. King, and A. A. Merianos. 2019. Impact of parental communication on African American adolescent sexual behavior: A mini literature review. Sexuality and Culture 24(5):1579-1593.
McGoy, S. L., A. C. Pettit, M. Morrison, L. R. Alexander, P. Johnson, B. Williams, D. Banister, M. K. Young, C. Wester, and P. F. Rebeiro. 2018. Use of social network strategy among young Black men who have sex with men for HIV testing, linkage to care, and reengagement in care, Tennessee, 2013-2016. Public Health Reports 133(2 Suppl):43s-51s.
McLeroy, K., D. Bibeau, A. Steckler, and K. D. Glanz. 1988. An ecology perspective on health promotion programs. Health Education Quarterly 15:351-377.
McLeroy, K. R., B. L. Norton, M. C. Kegler, J. N. Burdine, and C. V. Sumaya. 2003. Community-based interventions. American Journal of Public Health 93(4):529-533.
Merzel, C., and J. D’Afflitti. 2003. Reconsidering community-based health promotion: Promise, performance, and potential. American Journal of Public Health 93(4):557-574.
Mevissen, F. E., R. A. Ruiter, R. M. Meertens, F. Zimbile, and H. P. Schaalma. 2011. Justify your love: Testing an online STI-risk communication intervention designed to promote condom use and STI-testing. Psychology and Health 26(2):205-221.
Miedema, E., M. L. J. Le Mat, and F. Hague. 2020. But is it comprehensive? Unpacking the “comprehensive” in comprehensive sexuality education. Health Education Journal 79(7):747-762.
Milat, A. J., L. King, A. E. Bauman, and S. Redman. 2013. The concept of scalability: Increasing the scale and potential adoption of health promotion interventions into policy and practice. Health Promotion International 28(3):285-298.
Molleda, L., M. Bahamon, S. M. St George, T. Perrino, Y. Estrada, D. Correa Herrera, H. Pantin, and G. Prado. 2017. Clinic personnel, facilitator, and parent perspectives of ehealth Familias Unidas in primary care. Journal of Pediatric Health Care 31(3):350-361.
Montano, D., and D. Kasprzyk. 2015. Theory of reasoned action, theory of planned behavior, and the integrated behavioral model. In Health behavior: Theory, research, and practice. Vol. 4, edited by K. Glanz, B. K. Rimer, and K. V. Viswanath. San Francisco, CA: Jossey-Bass. Pp. 95-124.
Morales, A., J. P. Espada, M. Orgilés, S. Escribano, B. T. Johnson, and M. Lightfoot. 2018. Interventions to reduce risk for sexually transmitted infections in adolescents: A meta-analysis of trials, 2008-2016. PLoS One 13(6).
Morgan, E., B. Skaathun, G. K. Nikolopoulos, D. Paraskevis, L. D. Williams, P. Smyrnov, S. R. Friedman, and J. A. Schneider. 2019. A network intervention to locate newly HIV infected persons within MSM networks in Chicago. AIDS and Behavior 23(1):15-20.
Morris, Z. S., S. Wooding, and J. Grant. 2011. The answer is 17 years, what is the question: Understanding time lags in translational research. Journal of the Royal Society of Medicine 104(12):510-520.
Nababan, H., E. Ota, W. Wariki, A. Koyanagi, S. Ezoe, K. Shibuya, and R. Tobe-Gai. 2011. Structural and community-level interventions for increasing condom use to prevent HIV and other sexually transmitted infections. (Protocol). Cochrane Database of Systematic Reviews 11:CD003363.
NCI (National Cancer Institute). n.d. About implementation science. https://cancercontrol.cancer.gov/is (accessed January 25, 2021).
NIH (National Institutes of Health). 1995. Family interventions and HIV/AIDS. https://grants.nih.gov/grants/guide/rfa-files/RFA-MH-95-002.html (accessed November 12, 2020).
Nikolopoulos, G. K., E. Pavlitina, S. Q. Muth, J. Schneider, M. Psichogiou, L. D. Williams, D. Paraskevis, V. Sypsa, G. Magiorkinis, P. Smyrnov, A. Korobchuk, T. I. Vasylyeva, B. Skaathun, M. Malliori, E. Kafetzopoulos, A. Hatzakis, and S. R. Friedman. 2016. A network intervention that locates and intervenes with recently HIV-infected persons: The Transmission Reduction Intervention Project (TRIP). Scientific Reports 6:38100.
Noar, S. M., and N. G. Harrington. 2012. eHealth applications: An introduction and overview. In eHealth applications: Promising strategies for behavior change, edited by S. M. Noar and N. G. Harrington. New York: Routledge.
Noar, S. M., C. N. Benac, and M. S. Harris. 2007. Does tailoring matter? Meta-analytic review of tailored print health behavior change interventions. Psychological Bulletin 133(4):673.
NRC (National Research Council). 1987. Risking the future: Adolescent sexuality, pregnancy, and childbearing, volume II: Working papers and statistical appendices, edited by S. L. Hofferth and C. D. Hayes. Washington, DC: National Academy Press.
OBSSR (Office of Behavioral and Social Sciences Research). 2019. BSSR definition. https://obssr.od.nih.gov/about/bssr-definition/#ref1 (accessed December 31, 2020).
Oesterle, S., M. R. Kuklinski, J. D. Hawkins, M. L. Skinner, K. Guttmannova, and I. C. Rhew. 2018. Long-term effects of the Communities That Care trial on substance use, antisocial behavior, and violence through age 21 years. American Journal of Public Health 108(5):659-665.
Ott, M. A., J. Campbell, T. M. Imburgia, Z. Yang, W. Tu, and C. L. Auerswald. 2018. Community engagement and venue-based sampling in adolescent male sexually transmitted infection prevention research. Journal of Adolescent Health 62(3 Suppl):S58-S64.
Padian, N. S., A. Buvé, J. Balkus, D. Serwadda, and W. Cates. 2008. Biomedical interventions to prevent HIV infection: Evidence, challenges, and way forward. Lancet 372(9638):585-599.
Pantin, H., G. Prado, B. Lopez, S. Huang, M. I. Tapia, S. J. Schwartz, E. Sabillon, C. H. Brown, and J. Branchini. 2009. A randomized controlled trial of Familias Unidas for Hispanic adolescents with behavior problems. Psychosomatic Medicine 71(9):987-995.
Pequegnat, W., and J. Szapocznik. 2000. Working with families in the era of HIV/AIDS. London, UK: Sage Publications.
Perrin, E. C., R. C. Sheldrick, J. M. McMenamy, B. S. Henson, and A. S. Carter. 2014. Improving parenting skills for families of young children in pediatric settings: A randomized clinical trial. JAMA Pediatrics 168(1):16-24.
Perrino, T., A. Gonzalez-Soldevilla, H. Pantin, and J. Szapocznik. 2000. The role of families in adolescent HIV prevention: A review. Clinical Child and Family Psychology Review 3(2):81-96.
Perrino, T., Y. Estrada, S. Huang, S. S. George, H. Pantin, M. Á. Cano, T. K. Lee, and G. Prado. 2018. Predictors of participation in an ehealth, family-based preventive intervention for Hispanic youth. Prevention Science 19(5):630-641.
Peskin, M., B. Hernandez, C. Markham, K. Baker, S. Tyrrell, R. Addy, R. Shegog, P. Cuccaro, P. DeRoulet, and S. Tortolero. 2011. Sexual health education from the perspective of school staff: Implications for adoption and implementation of effective programs in middle school. Journal of Applied Research on Children 2(2):Article 9.
Pinto, R. M., K. R. Berringer, R. Melendez, and O. Mmeje. 2018. Improving PrEP implementation through multilevel interventions: A synthesis of the literature. AIDS Behavior 22(11):3681-3691.
Pitpitan, E. V., S. C. Kalichman, L. A. Eaton, S. A. Strathdee, and T. L. Patterson. 2013. HIV/STI risk among venue-based female sex workers across the globe: A look back and the way forward. Current HIV/AIDS Reports 10(1):65-78.
Power to Decide. 2016. Survey says: Parent power. https://powertodecide.org/system/files/resources/primary-download/Talking%20is%20Power_Survey%20Says_002.pdf (accessed November 4, 2020).
Prado, G., H. Pantin, S. J. Schwartz, N. S. Lupei, and J. Szapocznik. 2006. Predictors of engagement and retention into a parent-centered, ecodevelopmental HIV preventive intervention for Hispanic adolescents and their families. Journal of Pediatric Psychology 31(9):874-890.
Prado, G., H. Pantin, E. Briones, S. J. Schwartz, D. Feaster, S. Huang, S. Sullivan, M. I. Tapia, E. Sabillon, B. Lopez, and J. Szapocznik. 2007. A randomized controlled trial of a parent-centered intervention in preventing substance use and HIV risk behaviors in Hispanic adolescents. Journal of Consulting and Clinical Psychology 75(6):914-926.
Prado, G. J., S. J. Schwartz, M. Maldonado-Molina, S. Huang, H. M. Pantin, B. Lopez, and J. Szapocznik. 2009. Ecodevelopmental × intrapersonal risk: Substance use and sexual behavior in Hispanic adolescents. Health Education & Behavior 36(1):45-61.
Prado, G., D. Cordova, S. Huang, Y. Estrada, A. Rosen, G. A. Bacio, G. Leon Jimenez, H. Pantin, C. H. Brown, M. R. Velazquez, J. Villamar, D. Freitas, M. I. Tapia, and K. McCollister. 2012. The efficacy of Familias Unidas on drug and alcohol outcomes for Hispanic delinquent youth: Main effects and interaction effects by parental stress and social support. Drug and Alcohol Dependence 125(Suppl 1):S18-S25.
Prado, G., Y. Estrada, L. M. Rojas, M. Bahamon, H. Pantin, M. Nagarsheth, L. Gwynn, A. Y. Ofir, L. Q. Forster, N. Torres, and C. H. Brown. 2019. Rationale and design for ehealth Familias Unidas primary care: A drug use, sexual risk behavior, and STI preventive intervention for Hispanic youth in pediatric primary care clinics. Contemporary Clinical Trials 76:64-71.
Proctor, E., H. Silmere, R. Raghavan, P. Hovmand, G. Aarons, A. Bunger, R. Griffey, and M. Hensley. 2011. Outcomes for implementation research: Conceptual distinctions, measurement challenges, and research agenda. Administration and Policy in Mental Health 38(2):65-76.
Rabin, B. A., and R. C. Brownson. 2017. Terminology for dissemination and implementation research. Dissemination and Implementation Research in Health: Translating Science to Practice 2:19-45.
Rabin, B. A., R. C. Brownson, D. Haire-Joshu, M. W. Kreuter, and N. L. Weaver. 2008. A glossary for dissemination and implementation research in health. Journal of Public Health Management and Practice 14(2):117-123.
Rankin, K., J. Jarvis-Thiébault, N. Pfeifer, M. Englebert, J. Perng, S. Yoon, and A. Heard. 2016. Adolescent sexual and reproductive health: An evidence gap map (report 5). Washington, DC: International Initiative for Impact Evaluation (3ie).
Reedtz, C., B. H. Handegård, and W. T. Mørch. 2011. Promoting positive parenting practices in primary pare: Outcomes and mechanisms of change in a randomized controlled risk reduction trial. Scandinavian Journal of Psychology 52(2):131-137.
Reider, E. E., E. B. Robertson, and B. E. Sims. 2014. Does early intervention prevent health-risking sexual behaviors related to HIV/AIDS? Prevention Science (15 Suppl 1):S1-S5.
Reinhart, R. J. 2020. Nurses continue to rate highest in honesty, ethics. https://news.gallup.com/poll/274673/nurses-continue-rate-highest-honesty-ethics.aspx (accessed November 12, 2020).
Rhew, I. C., J. D. Hawkins, D. M. Murray, A. A. Fagan, S. Oesterle, R. D. Abbott, and R. F. Catalano. 2016. Evaluation of community-level effects of Communities That Care on adolescent drug use and delinquency using a repeated cross-sectional design. Prevention Science 17(2):177-187.
Rhodes, S. D., K. C. Hergenrather, F. R. Bloom, J. S. Leichliter, and J. Montaño. 2009. Outcomes from a community-based, participatory lay health adviser HIV/STD prevention intervention for recently arrived immigrant Latino men in rural North Carolina. AIDS Education and Prevention 21(5 Suppl):103-108.
Rietmeijer, K., and M. Scahill. 2012. Behavioral interventions for STD/HIV prevention. https://www.cdc.gov/std/training/std101/presentations-2012/behavioral-interventions.pdf (accessed February 22, 2021).
Robin, L., P. Dittus, D. Whitaker, R. Crosby, K. Ethier, J. Mezoff, K. Miller, and K. PappasDeluca. 2004. Behavioral interventions to reduce incidence of HIV, STD, and pregnancy among adolescents: A decade in review. Journal of Adolescent Health 34(1):3-26.
Rogers, R. W. 1983. Cognitive and physiological processes in fear appeals and attitude change: A revised theory of protection motivation. In Social psychophysiology: A source-book, edited by J. T. Cacioppo and R. E. Petty. New York: Guilford Press. Pp. 153-176.
Ross, M. W., and M. L. Williams. 2002. Effective targeted and community HIV/STD prevention programs. Journal of Sex Research 39(1):58-62.
Rothenberg, R., T. D. M. Hoang, S. Q. Muth, and R. Crosby. 2007. The Atlanta Urban Adolescent Network study: A network view of STD prevalence. Sexually Transmitted Diseases 34(8):525-531.
Rotheram-Borus, M. J., C. Koopman, and A. A. Ehrhardt. 1991a. Homeless youths and HIV infection. American Psychologist 46(11):1188.
Rotheram-Borus, M. J., C. Koopman, C. Haignere, and M. Davies. 1991b. Reducing HIV sexual risk behaviors among runaway adolescents. JAMA 266(9):1237-1241.
Rotheram-Borus, M. J., D. Swendeman, D. Flannery, E. Rice, D. M. Adamson, and B. Ingram. 2009. Common factors in effective HIV prevention programs. AIDS and Behavior 13(3):399-408.
Sales, J. M., R. R. Milhausen, and R. J. Diclemente. 2006. A decade in review: Building on the experiences of past adolescent STI/HIV interventions to optimise future prevention efforts. Sexually Transmitted Infections 82(6):431-436.
Sandler, I., S. A. Wolchik, G. Cruden, N. E. Mahrer, S. Ahn, A. Brincks, and C. H. Brown. 2014. Overview of meta-analyses of the prevention of mental health, substance use, and conduct problems. Annual Review of Clinical Psychology 10:243-273.
Santelli, J. S., L. M. Kantor, S. A. Grilo, I. S. Speizer, L. D. Lindberg, J. Heitel, A. T. Schalet, M. E. Lyon, A. J. Mason-Jones, T. McGovern, C. J. Heck, J. Rogers, and M. A. Ott. 2017. Abstinence-only-until-marriage: An updated review of U.S. policies and programs and their impact. Journal of Adolescent Health 61(3):273-280.
Schneider, J. A., L. Young, A. Ramachandran, S. Michaels, H. Cohen, I. Robinson, L. Alon, B. Hill, S. Nakasone, M. Balenciaga, D. Motley, A. Bouris, A. Khanna, M. Ferreira, T. Valente, P. Schumm, and PrEP Chicago Network Intervention Team. 2021. A pragmatic randomized controlled trial to increase pre-exposure prophylaxis uptake for HIV prevention: 55-week results from PrEPChicago. Journal of Acquired Immune Deficiency Syndromes 86(1):31-37.
Schueler, K., M. Ferreira, G. Nikolopoulos, B. Skaathun, D. Paraskevis, A. Hatzakis, S. R. Friedman, and J. A. Schneider. 2019. Pre-exposure prophylaxis (PrEP) awareness and use within high HIV transmission networks. AIDS and Behavior 23(7):1893-1903.
Shepherd, L. M., K. F. Sly, and J. M. Girard. 2017. Comparison of comprehensive and abstinence-only sexuality education in young African American adolescents. Journal of Adolescence 61:50-63.
Sieverding, J., C. B. Boyer, J. Siller, A. Gallaread, M. Krone, and Y. J. Chang. 2005. Youth united through health education: Building capacity through a community collaborative intervention to prevent HIV/STD in adolescents residing in a high STD prevalent neighborhood. AIDS Education and Prevention 17(4):375-385.
Simoni, J. M., K. Ronen, and F. M. Aunon. 2018. Health behavior theory to enhance ehealth intervention research in HIV: Rationale and review. Current HIV/AIDS Reports 15(6):423-430.
Singer, M. C., P. I. Erickson, L. Badiane, R. Diaz, D. Ortiz, T. Abraham, and A. M. Nicolaysen. 2006. Syndemics, sex and the city: Understanding sexually transmitted diseases in social and cultural context. Social Science & Medicine 63(8):2010-2021.
Smith, B. D., E. Teshale, A. Jewett, C. M. Weinbaum, A. Neaigus, H. Hagan, S. M. Jenness, S. K. Melville, R. Burt, H. Thiede, A. Al-Tayyib, P. R. Pannala, I. W. Miles, A. M. Oster, A. Smith, T. Finlayson, K. E. Bowles, and E. A. Dinenno. 2011. Performance of premarket rapid hepatitis C virus antibody assays in 4 national human immunodeficiency virus behavioral surveillance system sites. Clinical Infectious Diseases 53(8):780-786.
Smokowski, P., R. Corona, M. Bacallao, B. L. Fortson, K. J. Marshall, and A. Yaros. 2018. Addressing barriers to recruitment and retention in the implementation of parenting programs: Lessons learned for effective program delivery in rural and urban areas. Journal of Child and Family Studies 27(9):2925-2942.
Spoth, R., C. Redmond, C. Hockaday, and C. Y. Shin. 1996. Barriers to participation in family skills preventive interventions and their evaluations: A replication and extension. Family Relations 45(3):247-254.
Spoth, R., C. Goldberg, and C. Redmond. 1999. Engaging families in longitudinal preventive intervention research: Discrete-time survival analysis of socioeconomic and social–emotional risk factors. Journal of Consulting and Clinical Psychology 67(1):157-163.
Spoth, R. L., M. Guyll, and S. X. Day. 2002. Universal family-focused interventions in alcohol-use disorder prevention: Cost-effectiveness and cost-benefit analyses of two interventions. Journal of Studies on Alcohol and Drugs 63(2):219-228.
Spoth, R., S. Clair, and L. Trudeau. 2014. Universal family-focused intervention with young adolescents: Effects on health-risking sexual behaviors and STDs among young adults. Prevention Science (15 Suppl 1):S47-S58.
Spoth, R. L., L. S. Trudeau, C. Redmond, C. Shin, M. T. Greenberg, M. E. Feinberg, and G. H. Hyun. 2015. Prosper Partnership delivery system: Effects on adolescent conduct problem behavior outcomes through 6.5 years past baseline. Journal of Adolescence 45:44-55.
Sundar, S. S., S. Kalyanaraman, and J. Brown. 2003. Explicating web site interactivity: Impression formation effects in political campaign sites. Communication Research 30(1):30-59.
Sundell, K., and T. Olsson. 2017. Social intervention research. https://www.oxfordbibliographies.com/view/document/obo-9780195389678/obo-9780195389678-0254.xml (accessed December 31, 2020).
Sutton, M. Y., S. M. Lasswell, Y. Lanier, and K. S. Miller. 2014. Impact of parent–child communication interventions on sex behaviors and cognitive outcomes for Black/African-American and Hispanic/Latino youth: A systematic review, 1988-2012. Journal of Adolescent Health 54(4):369-384.
Swanton, R., V. Allom, and B. Mullan. 2015. A meta-analysis of the effect of new-media interventions on sexual-health behaviours. Sexually Transmitted Infections 91(1):14-20.
Szapocznik, J., G. Prado, A. K. Burlew, R. A. Williams, and D. A. Santisteban. 2007. Drug abuse in African American and Hispanic adolescents: Culture, development, and behavior. Annual Review of Clinical Psychology 3:77-105.
Taylor, D., C. Lunny, P. Lolic, O. Warje, J. Geldman, T. Wong, M. Gilbert, R. Lester, and G. Ogilvie. 2019. Effectiveness of text messaging interventions on prevention, detection, treatment, and knowledge outcomes for sexually transmitted infections (STIs)/HIV: A systematic review and meta-analysis. Systematic Reviews 8(1):12.
Thompson, C. T. 2020. Tiffani Kocsis: Critical analysis of sexuality education in the United States: Toward an inclusive curriculum for social justice. Journal of Youth and Adolescence 49(8):1751-1753.
Tolou-Shams, M., E. Dauria, S. M. Conrad, K. Kemp, S. Johnson, and L. K. Brown. 2017. Outcomes of a family-based HIV prevention intervention for substance using juvenile offenders. Journal of Substance Abuse Treatment 77:115-125.
Trenholm, C., B. Devaney, K. Fortson, M. Clark, L. Q. Bridgespan, and J. Wheeler. 2008. Impacts of abstinence education on teen sexual activity, risk of pregnancy, and risk of sexually transmitted diseases. Journal of Policy Analysis and Management 27(2):255-276.
Trickett, E. J., S. Beehler, C. Deutsch, L. W. Green, P. Hawe, K. McLeroy, R. L. Miller, B. D. Rapkin, J. J. Schensul, A. J. Schulz, and J. E. Trimble. 2011. Advancing the science of community-level interventions. American Journal of Public Health 101(8):1410-1419.
Underhill, K., D. Operario, and P. Montgomery. 2007. Abstinence-only programs for HIV infection prevention in high-income countries. Cochrane Database of Systematic Reviews (4):CD005421.
Valente, T. W. 2012. Network interventions. Science 337(6090):49-53.
Vaughn, L. M., E. Wagner, and F. Jacquez. 2013. A review of community-based participatory research in child health. American Journal of Maternal/Child Nursing 38(1):48-53.
Walling, E. B., N. Benzoni, J. Dornfeld, R. Bhandari, B. A. Sisk, J. Garbutt, and G. Colditz. 2016. Interventions to improve HPV vaccine uptake: A systematic review. Pediatrics 138(1).
Wandersman, A., P. Imm, M. Chinman, and S. Kaftarian. 2000. Getting to Outcomes: A results-based approach to accountability. Evaluation and Program Planning 23(3):389-395.
Wang, K., K. Brown, S. Y. Shen, and J. Tucker. 2011. Social network-based interventions to promote condom use: A systematic review. AIDS and Behavior 15(7):1298-1308.
Wendell, D. A., D. A. Cohen, D. LeSage, and T. A. Farley. 2003. Street outreach for HIV prevention: Effectiveness of a state-wide programme. International Journal of STD & AIDS 14(5):334-340.
Widman, L., J. Nesi, K. Kamke, S. Choukas-Bradley, and J. L. Stewart. 2018. Technology-based interventions to reduce sexually transmitted infections and unintended pregnancy among youth. Journal of Adolescent Health 62(6):651-660.
Willoughby, J. F., and K. L. L’Engle. 2015. Influence of perceived interactivity of a sexual health text message service on young people’s attitudes, satisfaction and repeat use. Health Education Research 30(6):996-1003.
Willoughby, J. F., and A. Muldrow. 2017. SMS for sexual health: A comparison of service types and recommendations for sexual health text message service providers. Health Education Journal 76(2):231-243.
Wilson, T. E., M. Fraser-White, K. M. Williams, A. Pinto, F. Agbetor, B. Camilien, K. Henny, R. C. Browne, Y. Gousse, T. Taylor, H. Brown, R. Taylor, and M. A. Joseph. 2014. Barbershop talk with brothers: Using community-based participatory research to develop and pilot test a program to reduce HIV risk among Black heterosexual men. AIDS Education and Prevention 26(5):383-397.
Wylie, J. L., and A. N. N. Jolly. 2001. Patterns of chlamydia and gonorrhea infection in sexual networks in Manitoba, Canada. Sexually Transmitted Diseases 28(1).
Young, S. D. 2020. The Adaptive Behavioral Components (ABC) model for planning longitudinal behavioral technology-based health interventions: A theoretical framework. Journal of Medical Internet Research 22(6):e15563.
Young, S. D., and D. Jaganath. 2013. Online social networking for HIV education and prevention: A mixed-methods analysis. Sexually Transmitted Diseases 40(2):162-167.
Young, S. D., and A. H. Jordan. 2013. The influence of social networking photos on social norms and sexual health behaviors. Cyberpsychology, Behavior, and Social Networking 16(4):243-247.
Young, S. D., W. G. Cumberland, S. J. Lee, D. Jaganath, G. Szekeres, and T. Coates. 2013. Social networking technologies as an emerging tool for HIV prevention. Annals of Internal Medicine 159(5):318-324.
Young, S. D., I. Holloway, D. Jaganath, E. Rice, D. Westmoreland, and T. Coates. 2014. Project Hope: Online social network changes in an HIV prevention randomized controlled trial for African American and Latino men who have sex with men. American Journal of Public Health 104(9):1707-1712.
Young, S. D., W. G. Cumberland, R. Nianogo, L. A. Menacho, J. T. Galea, and T. Coates. 2015. The HOPE social media intervention for global HIV prevention in Peru: A cluster randomised controlled trial. Lancet HIV 2(1):27-32.
Zimmerman, R. S., S. M. Noar, S. Feist-Price, O. Dekthar, P. K. Cupp, E. Anderman, and S. Lock. 2007. Longitudinal test of a multiple domain model of adolescent condom use. Journal of Sex Research 44(4):380-394.
































































