
2
Mental Health, Substance Use, and Wellbeing in Higher Education in the United States
The system of higher education in the United States is complex and diverse—both in terms of the types of degree-granting institutions and the diversity of the student populations. Both are critical considerations in framing approaches to dealing with an increasing prevalence of mental health problems and substance use within this system. This chapter begins with broad trends in higher education structures and the types of students attending them, as a foundation for the discussion of mental health trends.
THE STRUCTURE OF THE HIGHER EDUCATION SYSTEM
There are more than 4,000 institutions of higher education in the United States, both publicly and privately funded. Publicly funded institutions—most institutions of higher education—are overseen by elected or appointed boards of directors or regents. Even though similar boards oversee private institutions, both not-for-profit and for-profit, these are appointed by the institutions themselves. As a result, the individuals or entities in control of private, for-profit institutions can receive bonuses, dividends, and other financial benefits in the event of net profit. Chapter 5 provides more information about the ways in which changes come about in different types of institutions.
“Community college” is a term used in the United States to refer primarily to institutions of higher education that confer associate degrees as the terminal degree. This report will reference data related to associate degree–granting institutions, even as some community colleges have begun to offer bachelor’s degrees (AACC, 2019). In 2018-2019, the approximately 1,300 community colleges in the United States served 5.7 million students or 35 percent of all
undergraduate students (NCES, 2020). Community colleges are more likely to serve students who are Black, Indigenous, and people of color (BIPOC), of lower socioeconomic status, and/or are the first in their family to attend college, known as first-generation students (Snyder, de Brey, and Dillow, 2019). As of 2018, community colleges as a whole had passed the minority-majority threshold, meaning that greater than 50 percent of the students are from groups other than white. Demographic factors such as socioeconomic status, race/ethnicity, and first-generation status can increase the likelihood of academic vulnerabilities that correlate with lower rates of completion, often increasing the need for remedial coursework that community college students require at higher rates than do those at bachelor’s degree–granting colleges and universities (Snyder, de Brey, and Dillow, 2019). Community colleges often have fewer resources than bachelor’s degree–granting colleges and universities to serve more students who are less likely to have benefited from a strong K-12 education, safe communities, and other factors that correlate with higher socioeconomic status; thus increasing the need to make counseling and resources more available at community colleges
Under the umbrella of graduate schools, this report includes master’s and doctoral degree–granting programs, as well as medical and other professional degree programs beyond the bachelor’s degree. The U.S. Department of Education (ED) describes master’s programs as a first-level graduate degree that takes approximately two years to complete. For research doctoral degrees (not including professional degrees), ED describes the degree as a program that includes advanced study and independent research with supervision, culminating in a dissertation or thesis. Distinct from a research doctoral degree, ED considers the Doctor of Medicine (M.D.) as a first-professional degree. In 2018-2019, there were 154 institutions that offered programs for medical education (AAMC, 2019, chart 5).
The United States also has a number of institutions that are classified as Minority Serving Institutions (MSIs), which cut across two- and four-year degree-granting institutions. MSIs traditionally fall into two categories: historically defined or enrollment-defined (see Table B-1 and Table B-2 in Appendix B).
According to the National Academies 2019 report Minority Serving Institutions: America’s Underutilized Resource for Strengthening the STEM Workforce (NASEM, 2019a), “there are more than 700 federally designated MSIs that represent approximately 14 percent of all degree-granting, Title IV-eligible institutions of higher education. Taken together, MSIs enroll roughly five million students, or nearly 30 percent of all undergraduates in U.S. higher education” (NASEM, 2019a). MSIs as a category are themselves diverse in nature (Núñez, Hurtado, and Calderón Galdeano, 2015), and there is some disagreement among different stakeholders as to how to count the number of MSIs, resulting in varying estimates of the total number of MSIs in the United States (NASEM, 2019a).
CHANGES IN STUDENT DEMOGRAPHICS
The composition of the student body at U.S. institutions of higher education has become increasingly diverse over the past decades (ACE, 2020). Colleges and universities, originally designed to serve a predominantly white and male population, have experienced a shift in the proportions of students who can be characterized by gender, race and ethnicity, socioeconomic status, citizenship, veteran status, disability status, and sexual and gender minority (SGM) status,1 first-generation students, and students with dependents. As the representation of historically excluded groups has increased in the United States, colleges and universities have had to learn to expand their view of how to support students from different backgrounds so that the diversity of the entering classes is reflected in the diversity of those students who graduate and enter the workforce or pursue additional educational experiences (see Box 2-1 for terminology in the report).
In postsecondary education, the overall enrollment of female students achieved parity with males in the late 1970s, and the share of female students has continued to increase, reaching 57 percent of overall enrollment by 2018-2019 (Snyder, de Brey, and Dillow, 2019). There remain disciplines such as computer science, engineering, physics, and mathematics where women have been underrepresented and continue to comprise a smaller proportion of degrees conferred. Similarly, the increase in diversity in terms of race and ethnicity, both in absolute numbers and the proportion of students who are Black, Hispanic, Asian, Pacific Islander, Native Indian/Alaska Native, or of two or more races, has not translated into equal rates of graduation or fields of study (Snyder, de Brey, and Dillow, 2019).
Varying completion rates for racial and ethnic minority students suggest there are factors within higher education that fail to provide equitable support to students from BIPOC groups. It is also more likely that students from historically underrepresented racial and ethnic backgrounds come from a lower socioeconomic background and are first-generation students, two other factors that correlate with lower rates of completion (Reynolds and Cruise, 2020; Wilbur and Roscigno, 2016). Looking to future trends, the proportion of students who are Black, Hispanic, Asian, Pacific Islander, Native American/Alaska Native, and multiple-race non-Hispanic is projected to increase, and institutions of higher education will need to continue to search for opportunities to provide additional supports for these students (see Figure 2-1).
___________________
1 Sexual and gender minority (SGM) populations “include, but are not limited to, individuals who identify as lesbian, gay, bisexual, asexual, transgender, Two-Spirit, queer, and/or intersex. Individuals with same-sex or -gender attractions or behaviors and those with a difference in sex development are also included. These populations also encompass those who do not self-identify with one of these terms but whose sexual orientation, gender identity or expression, or reproductive development is characterized by non-binary constructs of sexual orientation, gender, and/or sex.” This definition has been provided by the Sexual & Gender Minority Research Office (SGMRO) that coordinates (SGM)related research and activities at the National Institutes of Health.
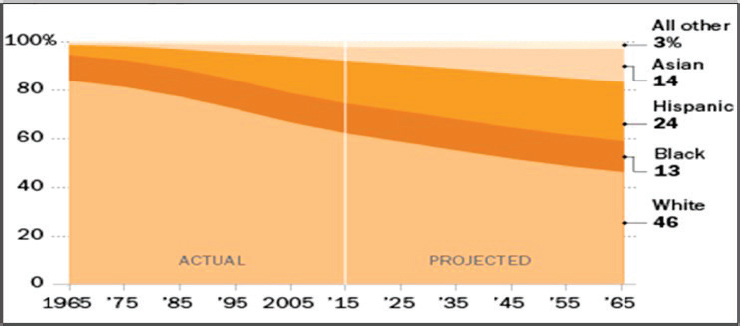
Note: Whites, Blacks, and Asians include only single-race non-Hispanics; Asians include Pacific Islanders. Other races include Native American/Alaska Native and multiple-race non-Hispanics. Hispanics can be of any race.
Source: Taylor, 2016.
The data above reflect gender as a category and race and ethnic background as a separate category; however, the tendency to disaggregate and present data by these dimensions alone does not reflect the fact that people live with overlapping identities and belong to many groups. The term “intersectionality” refers to the multiple identities that students hold and how those identities interact. The term intersectionality was originally coined by legal scholar Kimberlé Crenshaw to describe the combined experience of Black women facing both sexism and racism, but has been broadened to describe “the interconnected nature of social categorizations such as race, class, and gender, regarded as creating overlapping and interdependent systems of discrimination or disadvantage” (Crenshaw, 1989; McCall, 2005).
This report also examines other groups of interest to higher education, including, but not limited to, students with disabilities, students from lower socioeconomic status, first-generation students, veterans, student-atheletes, and students who are SGM students. Many of these students often fall into the category of what the Postsecondary National Policy Institute (PNPI) calls the “post-traditional student.” According to PNPI, nearly 15 percent of the U.S. undergraduate population would be considered “traditional” students, i.e., those between 17 and 21 years old who attend 4-year colleges and live on campus (PNPI, 2020b). The remaining 85 percent of students enrolled in the nation’s colleges and universities include adult learners, working parents, full-time workers, low-income students, and students who commute to school.
Some demographic groups and identities intersect more often than others do. For example, student veterans are more likely to be older, have dependents, and have a higher rate of reporting disability than non-veteran students (26 percent versus 19 percent) (NCES, 2019). As will be described later in this chapter, students who are BIPOC are also more likely to be first-generation students and to come from lower socioeconomic status. An intersectional understanding of student identities is a way to see the cumulative impact of discriminatory policies, unequal distribution of wealth across demographic groups, and other systemic inequities that have caused harm. Colleges and universities seeking to create equitable representation in enrollment across all groups must recognize the ways that the legacy of these historical practices fail to serve the many dimensions of the students who seek degrees today.
TRENDS IN MENTAL HEALTH AND SUBSTANCE USE IN HIGHER EDUCATION
Over the past two decades, numerous reports from higher education stakeholders have drawn attention to the increasingly complex concerns relating to mental health among students in postsecondary education (Duffy et al., 2019, 2020). The media, as well as some leaders in higher education, has categorized the current situation as a crisis—citing the facts that more students than ever
report symptoms consistent with mental illness, that substance use continues to be a serious problem on campuses, and that there has been a dramatic increase in students’ being referred to and utilizing mental health services. The COVID-19 pandemic has exacerbated the situation. It is negatively impacting students, as it is the entire population, in ways we do not yet fully understand. Some recent studies have identified examples of that impact at specific institutions; in one study, students reported more stress and anxiety due to the COVID-19 outbreak (Son et al., 2020), and in another, researchers found that, compared with prior academic terms, students who were enrolled during COVID-19, “were more sedentary, anxious, and depressed” (Huckins et al., 2020). How those impacts compare with increases in anxiety and stress in the general population is unknown.
However, the current situation, including the long-term impact of the pandemic, is difficult to assess accurately and quite complex. As one group of researchers has argued, “[…] based on this evidence, it is tempting to conclude that more college students in recent years are suffering from mood disorders. However, increases in service utilization could be caused by many factors other than increased prevalence, including greater awareness, better accessibility of services, improved outreach, or other factors not rooted in a true increase in prevalence” (Duffy, Twenge, and Joiner, 2019).
In addition, over the past 15 years numerous federal, state, and private funding mechanisms, including the Garret Lee Smith Memorial Act, have invested hundreds of millions of dollars toward reducing stigma, increasing help-seeking, and training gate-keepers; all of which lead to increased rates of identification and referral of students for treatment. Whether or not the state of mental health in higher education constituted a crisis, the simultaneous triad of COVID-19, the economic downturn, and long-standing racism and racial oppression did not improve the general living conditions of those living and receiving education in the United States.
Thus, institutions of higher education face the challenge of meeting a broad range of students’ needs in the context of increasing distress and demand for services at the same moment in time when leadership must make decisions about virtual or in-person enrollment, pandemic protocols, and even more uncertain budgets. These challenges come at a time when higher education has received the greatest decline in public financial support in decades, resulting in tight budgets and difficult allocation decisions. In terms of mental health, colleges and universities are also operating in the larger U.S. context of unequally distributed therapeutic, psychological, and psychiatric services across the nation. Access to these services may be reduced as a result of the cost of health insurance, limited coverage of mental health services by insurance companies, the number of private providers who accept insurance or referrals for a given insurance type, and the concentration of providers in any given area. The challenges for colleges and universities, aligned with the state of U.S. mental health services generally, serves as the context for the following trends.
National Data Sources and Considerations
While the overall trends presented in the sections above provide a starting point for understanding the trends in mental health and substance use in higher education, the existing data do not provide a thorough understanding of all populations in higher education. Articles on college and university mental health, for example, often cite age-matched data. These data are useful for understanding context and broader mental health trends in young adults as a whole, but they may not necessarily reflect the prevalence of mental health issues in students. For example, having national data that can be disaggregated between students enrolled in higher education and those who are not would allow researchers to make comparisons between college and age-matched peers (see Box 2-2).
The degree to which existing datasets can be disaggregated by gender, race and ethnic group, nationality, veteran status, SGM status, first-generation student status, socioeconomic status, and other characteristics varies. As colleges and universities address discrimination and bias in admissions, campus leaders, researchers, and public health providers would benefit from understanding national trends for these groups, as well as for those at their own institution (see Chapter 3). Going forward, it would be helpful to collect information that could be disaggregated by types of institutions and programs, notably community colleges, MSIs, graduate programs, and programs that enroll students primarily in hybrid or online models. Community colleges and MSIs, which serve more students who are BIPOC and first-generation students, often have fewer financial resources to collect data. A better understanding of their circumstances could help those campuses make more effective decisions in terms of programs and avenues for support (see Box 2-3).
An additional data issue arises from the fact that general population estimates are affected by survey nonresponse. Students who participate in the surveys could be systematically different from those who do not (e.g., more attuned to or interested in mental health concerns), which could bias the estimates upwards or downwards relative to the true population values. Similarly, screening instruments used in general population surveys, such as the nine-item major depression module of the Patient Health Questionnaire (PHQ-9), are known to significantly overestimate prevalence rates (Levis et al., 2020). The useful and oft-cited Healthy Minds Study, for example, uses survey sample weights based on known characteristics of the full population (e.g., gender, race/ethnicity, academic level, and grade point average distribution), but a follow-up study indicated that initial survey participants were more likely than nonrespondents to have symptoms of depression and use mental health services (Eisenberg, Golberstein, and Gollust, 2007). Additional discussion of self-reported data from general population surveys compared to data from clinical diagnoses can be found in Chapter 1.
TRENDS IN MENTAL HEALTH IN HIGHER EDUCATION
In the sections that follow regarding trends in mental health, it is important to understand how trend data are interpreted. In addition to the differences mentioned previously between self-reported data and clinical data, there is also variation in the types of instruments used for screens and diagnostics that can yield significantly different results. For this reason, some of the figures associated with each trend include data points from multiple sources with notations on the instrument used to create a more nuanced understanding of the trend. Figures with multiple data sets include data from the 2013-14 and 2018-19 academic years.
Trends in Student Anxiety
According to the National Institute of Mental Health (NIMH), people with generalized anxiety disorder (GAD) “display excessive anxiety or worry, most days for at least six months, about a number of things such as personal health,
work, social interactions, and everyday routine life circumstances. The fear and anxiety can cause significant problems in areas of their life” (NIMH, 2020a). Symptoms may include restlessness, fatigue, difficulty concentrating, irritability, muscle tension, intrusive feelings of worry, and sleep problems.
Data from HMS2 show there has been an increase in the percentage of students self-reporting symptoms of generalized anxiety (based on the GAD-7
___________________
2 Each participating school provides the Health Minds Study team with a randomly selected sample of currently enrolled students over the age of 18. Large schools typically provide a random sample of 4,000 students, while smaller schools typically provide a sample of all students. Schools with graduate students typically include both undergraduates and graduate students in the sample. The overall participation rate for the 2018-2019 study was 16 percent. It is important to raise the question of whether the 16 percent who participated are different in important ways from the 84 percent who did not participate. We address this issue by constructing nonresponse weights using administrative data on full student populations. Most of the 79 schools in the 2018-2019 HMS were able to provide administrative data about all randomly selected students.
screen) from 17.2 percent with a positive screen (GAD-7 ≥10) in 2013 to 31.2 percent in 2019.3 There has also been an increase in students screening positive for severe anxiety (GAD-7 ≥15) from 6 percent in 2013 to 13.5 percent in 2018 (see Table 2-1).
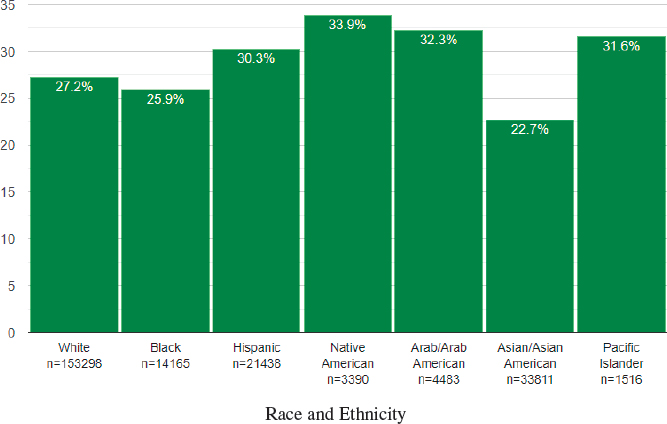
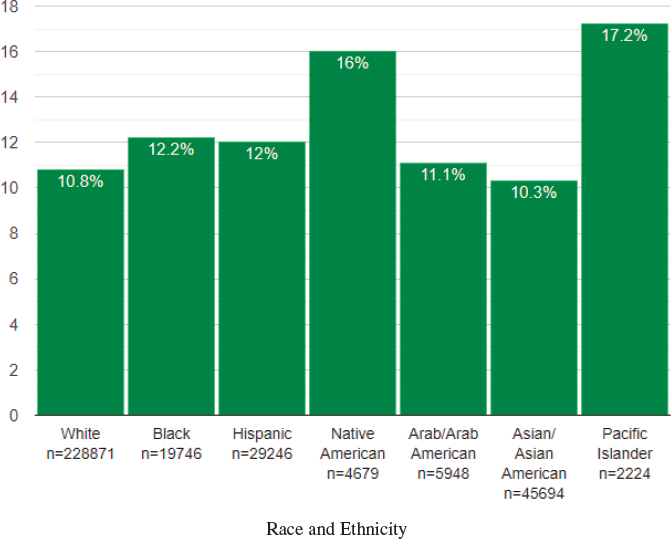
Over the 2007-2019 time period, 30.7 percent of female students reported anxiety in comparison to 19.7 percent of male students. There are also differences over the same time period by race and ethnic group (see Figure 2-2).
There are other more generalized ways that surveys have captured the sense of anxiety from students. NCHA includes the following question to the undergraduate participants, who self-report their symptoms: “Have you ever felt
TABLE 2-1 Comparison of Measures of Anxiety in Higher Education Students from Multiple Sources in 2013 and 2018
| Measures of Anxiety | Year | ||
|---|---|---|---|
| Fall 2013 | Fall 2018 | % Change 2013-2018 | |
| CCMH: CAPPS-34 Subscale scores for generalized anxietya | 1.86 | 2.03 | 9.1 |
| CCMH: CAPPS-34 Subscale scores social anxietya | 1.87 | 2.03 | 8.6 |
| HMS: Percentage of students self-reporting anxiety (based on the GAD-7 ≥10 screen)b | 17.2% | 31.3% | 81.9 |
| HMS: Percent of students self-reporting severe anxiety (GAD-7 ≥15 Screen) b | 6.0% | 13.5% | 125.0 |
| ACHA-NCHA: Have you ever felt overwhelming anxiety anytime within the last 12 months? c | 51.0% | 62.3% | 22.2 |
| NCHA: Have you felt overwhelming anger in the last 12 months? c | 35.6% | 41.7% | 17.1 |
| NCHA: Within the last 12 months, have you been diagnosed or treated by a professional for anxiety? c | 8.0% | 22.0% | 175.0 |
aCCMH (clinical data); bHMS (general population data); cNCHA (general population data)
Sources: ACHA, 2014, 2018; CCMH, 2015, 2020b; HMN, 2020.
___________________
3 Using the GAD 7-item scale. Each participating school provides the HMS team with a randomly selected sample of currently enrolled students over the age of 18. Large schools typically provide a random sample of 4,000 students, while smaller schools typically provide a sample of all students. Schools with graduate students typically include both undergraduates and graduate students in the sample. Undergraduate students include community college students.
Source: Healthy Minds Network.
overwhelming anxiety?”4 In the 2011-2012 the response was 51.1 percent compared to 63.6 in 2017-2018. While not the same as anxiety, the study reports that 37.7 percent of students felt overwhelming anger in 2011-2012 and 42.9 percent in 2017-2018 (Duffy, Twenge, and Joiner, 2019). On the other hand, clinical data provided by CCMH suggest smaller increases in average levels of student-self-reported generalized and social anxiety from 2013 to 2018 (9.1 percent and 8.6 percent, respectively), alongside massive increases in the number of students being treated in college counseling centers.
___________________
4 Response options for all items were “No, never,” “No, not in the last 12 months,” “Yes, in the last 2 weeks,” “Yes, in the last 30 days,” and “Yes, in the last 12 months.” For analyses, frequencies of each item endorsed within the last 2 weeks, 30 days, or 12 months were summed to produce an incidence value for 12-month prevalence for each semester. These were then weighted and summed within academic years, resulting in one value per academic year for each item. The wording of these items and their administration did not differ during the assessed years.
Participants were 610,543 undergraduate U.S. college students who participated in the American College Health Association’s NCHA between fall 2011 and spring 2018. The NCHA is a large, national survey of college health administered each semester. Participating universities recruited random samples of enrolled students to complete either paper or web-based surveys of past-year beliefs and behaviors regarding a variety of health and health-risk variables. Participants are required to be aged 18 years or older. Participation is voluntary, and response rates averaged 22 percent from 2011 to 2018. Data for the current project were drawn from biannual Undergraduate Reference Group Reports made publicly available online by the American College Health Association for the 2011-2012 to 2017-2018 academic years (available at https://www.acha.org/NCHA/ACHA-NCHA_Data/Publications_and_Reports/NCHA/Data/Publications_and_Reports.aspx?hkey=d5fb767c-d15d-4efc-8c41-3546d92032c5 [accessed October 1, 2020].
Trends in Depression
Depression is a common and serious mood disorder that can affect how the individual feels, thinks, and manages daily activities with inhibitions and limitations lasting for two weeks or more. The presentation of depression varies, and it may develop in specific situations, including during specific seasons or after giving birth. Major symptoms can include feeling sad or angry, hopeless, worthless, or irritable; decreased energy; loss of interest in previously enjoyed activities; difficulty with concentration or memory recall; difficulty sleeping; changes in weight; thoughts of death or self-harm; and physical ailments that do not have a clear connection to another physical cause (NIMH, 2020e).
The Healthy Minds Network study reported an increase in positive screens for depression (PHQ09 score ≥10) from 22 percent of students in 2007 to 36.4 percent in 2019.5 There has also been an increase in the rate of students self-reporting symptoms of major depression (PHQ-9 ≥15), from 8.8 percent in 2013 to 18 percent in 2019 (see Table 2-2).6
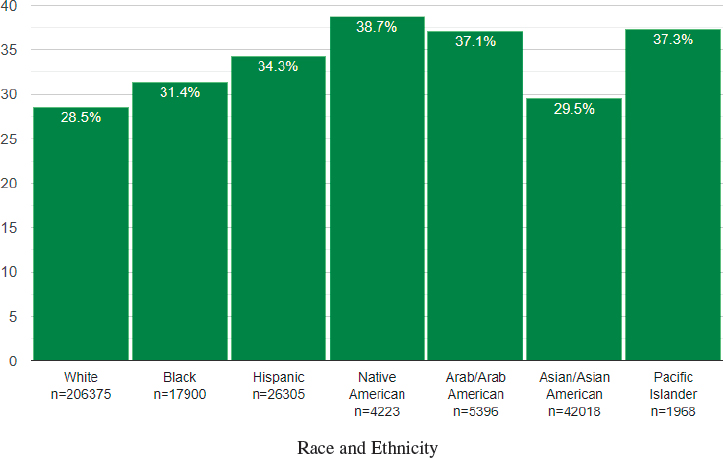
Over the same timeframe, more women (31.5 percent) reported symptoms consistent with any level of depression than men (24.8 percent). There are also differences in depression rates by race and ethnicity, with Native American students reporting the highest level of depression (38.7 percent) (see Figure 2-3); by citizenship, with more U.S. citizens reporting having depression (29.5 percent) than international students (25.9 percent); and by degree level, with 31.3 percent of undergraduates, 21.1 percent of master’s degree students, and 21.1 percent of students pursuing other degrees (HMN, 2007-2019).
NCHA provides another data point for depression in undergraduates, with the survey asking students to self-report to the question, “Have you ever felt so depressed that it was difficult to function?” For this data set, participants responded at 31.5 percent in 2011-12 and 42.2 percent in 2017-18 (Duffy, Twenge, and Joiner, 2019). Over the same period of time, and again in contrast to nonclinical population surveys, clinical data from CCMH indicated a dramatically smaller increase (6.7 percent) in self-reported levels of depression among college students seeking counseling, despite increases in the numbers of students in treatment.
___________________
5 Using the Patient Health Questionnaire (PHQ), a nine-item instrument based on the symptoms provided in the Diagnostic and Statistical Manual for Mental Disorders for a major depressive episode in the past two weeks (Spitzer, Kroenke, and Williams, 1999). Following the standard algorithm for interpreting the PHQ-9, symptom levels are categorized as severe (score of 15+), moderate (score of 10-14), or mild/minimal (score <10).
6 Some studies suggest that the PHQ overestimates diagnoses of depression: “The PHQ-9 is often used to generate what are described by researchers as depression prevalence estimates. The present study found that using PHQ-9 ≥10 to assess depression prevalence, which is commonly done, overestimated depression prevalence compared with prevalence based on actual diagnostic criteria by 11.9 percent (mean ratio: 2.5 times)” (Levis et al., 2020).
TABLE 2-2 Comparison of Measures of Depression in Higher Education Students from Multiple Sources in 2013 and 2018
| Measures of Depression | Year | ||
|---|---|---|---|
| Fall 2013 | Fall 2018 | % Change 2013-2018 | |
| CCMH: CAPS-34 Subscale scores for depressiona | 1.63 | 1.74 | 6.7 |
| HMS: Percentage of students self-reporting positive screens for any depression (PHQ-9 Score Screening ≥10) b | 22.3% | 37.1% | 66.4 |
| HMS: Percent of students self-reporting major depression (PHQ-9 Score Screening ≥15)b | 8.8% | 18.4% | 109.0 |
| NCHA: Have you felt very sad within the last 12 months? c | 59.5% | 67.9% | 14.6 |
| NCHA: Have you felt so depressed that it was difficult to function in the last 12 months?c | 30.9% | 41.4% | 34.0 |
| NCHA: Within the last 12 months, have you been diagnosed or treated by a professional for depression?c | 7.5% | 17.3% | 130.7 |
aCCMH (clinical data); bHMS (general population data); cNCHA (general population data)
Sources: ACHA, 2014, 2018; CCMH, 2015, 2020b; HMN, 2007-2019.
Source: Healthy Minds Network.
Trends in Other Mental Disorders
While the number of students being treated or self-reporting diagnoses for the mental disorders described may be smaller than for anxiety and depression, they remain important considerations for institutions of higher education. Anorexia nervosa, attention-deficit/hyperactivity disorder, autism spectrum disorder, bipolar disorder, bulimia nervosa, obsessive-compulsive disorder (OCD), and schizophrenia all appear on the ACHA’s annual National College Health Survey.7
- Anorexia nervosa: “People with anorexia nervosa may see themselves as overweight, even when they are dangerously underweight. People with anorexia nervosa typically weigh themselves repeatedly, severely restrict the amount of food they eat, often exercise excessively, and/or may force themselves to vomit or use laxatives to lose weight. Anorexia nervosa has the highest mortality rate of any mental disorder. While many people with this disorder die from complications associated with starvation, others die of suicide” (NIMH, 2020f).
- Attention-deficit/hyperactivity disorder (ADHD): “ADHD is a disorder that makes it difficult for a person to pay attention and control impulsive behaviors. He or she may also be restless and almost constantly active…Although the symptoms of ADHD begin in childhood, ADHD can continue through adolescence and adulthood. Even though hyperactivity tends to improve as a child becomes a teen, problems with inattention, disorganization, and poor impulse control often continue through the teen years and into adulthood” (NIMH, 2020b).
- Autism spectrum disorder (ASD): “ASD is a developmental disorder that affects communication, behavior, and the ability to function in school, work, or other areas of life. Although ASD can be diagnosed at any age, symptoms generally appear in the first two years of life” (NIMH, 2020c).
- Bipolar disorder “(formerly called manic-depressive illness or manic depression) is a mental disorder that causes unusual shifts in mood, energy, activity levels, concentration, and the ability to carry out day-to-day tasks. There are three types of bipolar disorder. All three types involve clear
___________________
7 134 postsecondary institutions self-selected to participate in the Spring 2019 ACHA National College Health Assessment (ACHA, 2019b), and 86,851 surveys were completed by students on these campuses. For the purpose of forming the Reference Group, only institutions located in the United States that surveyed all students or used a random sampling technique are included in the analysis, yielding a final data set consisting of 67,972 students at 98 schools. Demographic characteristics of the 98 campuses including public, private, two-year and four-year institutions, as well as associate through doctoral programs.
- changes in mood, energy, and activity levels. These moods range from periods of extremely ‘up,’ elated, irritable, or energized behavior (known as manic episodes) to very ‘down,’ sad, indifferent, or hopeless periods (known as depressive episodes). Less severe manic periods are known as hypomanic episodes” (NIMH, 2020d).
- Bulimia nervosa: “People with bulimia nervosa have recurrent and frequent episodes of eating unusually large amounts of food and feeling a lack of control over these episodes. This binge-eating is followed by behavior that compensates for the overeating such as forced vomiting, excessive use of laxatives or diuretics, fasting, excessive exercise, or a combination of these behaviors. People with bulimia nervosa may be slightly underweight, normal weight, or overweight” (NIMH, 2020f).
- Obsessive-compulsive disorder (OCD) “is a common, chronic, and long-lasting disorder in which a person has uncontrollable, reoccurring thoughts (obsessions) and/or behaviors (compulsions) that he or she feels the urge to repeat over and over” (NIMH, 2020i).
- Schizophrenia “is a chronic and severe mental disorder that affects how a person thinks, feels, and behaves. People with schizophrenia may seem like they have lost touch with reality. Although schizophrenia is not as common as other mental disorders, the symptoms can be very disabling” (NIMH, 2020j).
These conditions, some of which are chronic, may require more specialized treatment beyond the scope of a campus counseling center. Students report having a diagnosis or treatment for each of these disorders within the past 12 months at higher rates in both genders in 2018 than 2008, with the exception of bulimia in female students with remained flat at 1.4 percent.
For ADHD, the use of drugs such as Ritalin and Adderall in children since the early 1990s has changed management and treatment. These drugs were developed to help support learning and focus in students, garnering widespread use over the decade (Advokat and Scheithauer, 2013; Scheffler et al., 2007). The Centers for Disease Control and Prevention (CDC) reported in 2016 that some 6.1 million (9.4 percent) of children between ages 2-17 years had a diagnosis of ADHD, up from 4.4 million in 2003. Over time, more individuals who received diagnoses of ADHD and began treatment at a young age have graduated from secondary education, and many have entered postsecondary education. Increased awareness of and treatment for ADHD have raised the number of students with mental illness who may not have been able to complete a postsecondary education previously;
however, the change in the student population may not have been met by the appropriate changes in resources or support for those students.
Trends in Self-Harm, Suicidal Ideation, and Suicidality
The National Alliance on Mental Illness describes non-suicidal self-injury or self-harm as act where an individual hurts themselves on purpose. This act, which can present as cutting, burning, pulling out hair, or picking at wounds, is considered a sign of emotional distress (NAMI, 2020). NCHA, which contains data related to undergraduate students, shows an increase in the self-reporting to the question “Have you ever intentionally cut, burned, bruised, or otherwise injured yourself?” from 5.9 percent in 2012-2013 to 8.5 percent in 2017-2018 (see Table 2-3). In addition to intentional self-harm, public health officials list suicide and associated behavior as a major concern:
- Suicide is defined as death caused by self-directed injurious behavior with intent to die as a result of the behavior.
- A suicide attempt is a non-fatal, self-directed, potentially injurious behavior with intent to die as a result of the behavior. A suicide attempt might not result in injury.
- Suicidal ideation refers to thinking about, considering, or planning suicide (NIMH, 2020k).
The Healthy Minds Network reports an increase in students reporting non-suicidal self-injury in the past year from 14.3 percent in 2007 to 23.8 percent in 2019. Women had a higher rate of non-suicidal self-injury in the past year (20.8 percent) than men (17.4 percent), and U.S. citizens and permanent residents had a higher rate than international students (20.4 percent compared to 16 percent, respectively). Undergraduate students had a higher rate (21.9 percent) than master’s students (12.1 percent). There are differences in rates reported across racial and ethnic groups, as shown in Figure 2-4.
From the NCHA, the responses from undergraduate students to the question “Have you ever seriously considered suicide” rose from 7.4 percent in 2011-2012 to 13.0 percent in 2017-2018. There have been increases in self-reported suicidal ideation over the previous 12 months from 6 percent of students in 2007 to 14.1 percent in 2019. According to data from HMS, the proportion of students reporting having a plan of suicide within the past year also increased from 1.5 percent in 2007 to 6.3 percent in 2019, while attempts to die by suicide rose from 0.6 percent in 2007 to 1.5 percent in 2019. Women reported a slightly higher rate of suicidal ideation (10.7 percent) than men (9.7 percent), as did U.S. students (11.0 percent) compared to international students (7.5 percent); and undergraduate students compared to master’s students and those pursuing other degrees (11.7
TABLE 2-3 Comparison of Measures of Self-Harm, Suicidal Ideation, and Death by Suicide in Higher Education Students from Multiple Sources in 2013 and 2018
| Measures of Self-Harm, Suicidal Ideation, and Death by Suicide | Year | ||
|---|---|---|---|
| Fall 2013 (%) | Fall 2018 (%) | Change 2013-2018 (%) | |
| CCMH: Percentage of students reporting a non-suicidal self-injury (lifetime) a | 23.8 | 28.7 | 20.6 |
| CCMH: Serious suicidal ideation (lifetime) b | 30.9 | 36.7 | 18.8 |
| CCMH: Suicide attempts (lifetime) a | 8.9 | 10.6 | 21.3 |
| HMS: Non-suicidal self-injury within last yearb | 16.7 | 23.8 | 42.5 |
| HMS: Suicidal ideation within last yearb | 8.3 | 13.4 | 61.4 |
| HMS: Suicide plan within last yearb | 2.4 | 5.8 | 141.7 |
| HMS: Suicide attempt within last yearb | 0.6 | 1.5 | 150.0 |
| NCHA: Have you intentionally cut, burned, bruised, or otherwise hurt yourself in the last 12 months? c | 5.9 | 7.4 | 25.4 |
| NCHA: Have you seriously considered suicide in the last 12 months? c | 7.5 | 11.3 | 50.7 |
| NCHA: Have you attempted suicide in the last 12 months? c | 1.4 | 1.9 | 35.7 |
aCCMH (clinical data); bHMS (general population data); cNCHA (general population data)
Sources: ACHA, 2014, 2018; CCMH, 2015, 2020b; HMN, 2007-2019.
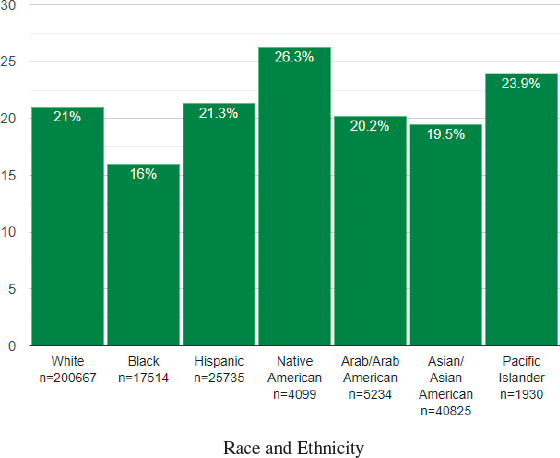
percent vs. 6.3 percent vs. 6.8 percent, respectively). A breakdown by race and ethnicity is provided in Figure 2-5.
During the same period, clinical data related to self-harm and suicidality reported by CCMH illustrated variable rates of change in comparison to nonclinical data from HMS and NCHA. These differential rates and trends raise important questions related to determining prevalence rates. For example, in 2018 CCMH reported that 28.7 percent of students reported lifetime prevalence of self-harm within the population of students seeking mental health services whereas HMS reported that 23.8 percent of those responding to a general population survey reported self-injuring in [just] the last year. The similarity of these data points for such different populations across such different time periods highlights the challenges associated with accurately measuring prevalence rates for difficult-to-assess concerns such as suicidal ideation. Further underscoring this challenge, clinical data provided by CCMH in 2018 indicated that 39.6 percent of students seeking treatment reported “thoughts of ending my life” (in the last two weeks) (0< on a scale of 0 to 4) in comparison to 8.2 percent of students “seriously considered attempting suicide” (in the last month). Moreover, following a clinical assessment, clinicians identified suicidality as a presenting concern for 9.9 percent of students seeking services. Thus, even within population-level clinical data, it
Source: Healthy Minds Network.
appears that students may endorse different items in dramatically different ways and that professional assessment of student distress, when compared to student self-report, may produce dramatically different results. Examples such as this, viewed alongside the known tendency for screening instruments used in general population surveys, to overestimate prevalence rates, should encourage caution when interpreting data points as evidence of prevalence.
A comparison of students enrolled full-time with those of similar age (18-22) not attending college indicates that enrollment in higher education may offer a small protective factor against suicidal ideation, plans, and attempts. For example, up to 7.7 percent of full-time undergraduate and graduate students reported seriously considering suicide as compared to 9 percent of those people not enrolled in higher education (ACHA, 2012; SAMHSA and NSDUH, 2014). Similarly, up to 1.2 percent of enrolled students reported attempting suicide as compared with 2.2 percent of their age-matched peers not enrolled in college (ACHA, 2012).
In terms of demographics, there are correlations that are worth noting given the importance of the issues related to self-harm and death by suicide. In the general population men die by suicide more than women, although women engage in self-harm and related behaviors more frequently than men. Non-Hispanic white students (Nock et al., 2008) and non-heterosexual students (Figueiredo and Abreu, 2015) have a higher risk of engaging in suicidal behavior, and while the extent to which culture and identity predict suicidal behavior in college and university students is unknown, students with disabilities tend to have more suicidal ideation than students without disabilities (Coduti et al., 2016). Research has found that students who seek psychotherapy are more depressed, hostile, and anxious than students who do not seek such help, and they are three times more likely to report high levels of suicide ideation and five times more likely to have made a previous suicide attempt (Hayes et al., 2020; McAleavey et al., 2012). These latter findings also highlight questions about why rates in the general population appear to be rising so much faster than rates in the clinical populations.
Research has also identified protective factors that can lower the risk of suicidal behavior in the general public. For college students, in addition to being enrolled in higher education, research has found that not living alone is a protective factor (Hayes et al., 2020).
While there have been great attention and concern raised in recent decades in media following student death by suicide, formally identifying the annual number of deaths per year is difficult to ascertain. There is no national database, registry, or single study that collects data on death by suicide. In addition, student deaths by suicide that occur during breaks, in off-campus housing, or when a student has taken medical leave to address health concerns may not be counted consistently. CDC notes that the rates for death by suicide for age-matched individuals ages 20-24 increased 36 percent from 12.5 deaths per 100,000 in 2000 to 17.0 deaths per 100,000 in 2017, with a greater rate of increase from 2013 to 2017 (6 percent annually, on average) than from 2000 to 2013 (1 percent annually) (Curtin and
Heron, 2019). As of 2018, for age groups 15-24 and 24-35, suicide was the second highest cause of death after unintentional injury (CDC, 2019).
An important source of information on student deaths on college campuses is the ongoing study of suicides at 13 Big Ten university campuses conducted by the Big Ten Counseling Centers, based on a comprehensive 10-year study by Silverman et al. in 1997. A follow-up study of student deaths by suicide from 2009 to 2018 on these campuses was commissioned for this report. It is described in Box 2-4 (below) and included as Appendix D.
The information in Box 2-4 should not be taken as representative of the breadth of the scope of this report, as it only includes the institutions in the Big Ten Counseling Centers. These colleges and universities are large, research-oriented institutions that include undergraduate and graduate students. The Big Ten Counseling Centers does not include any community colleges or minority serving institutions.
Despite this caution, this study is actually quite consistent with other studies in the past two decades examining available data to determine rates of suicide for college students; these studies have consistently found that rates of suicide for college students are much lower than the general population—suggesting that being a college student is very likely a protective factor for suicide risk. An ongoing, longitudinal national surveillance system that identifies student death by suicide would contribute to the research agenda.
CURRENT TRENDS IN SUBSTANCE USE IN HIGHER EDUCATION
Substance use remains a concern on colleges across the country given the effects illicit drugs and alcohol can have on the developing brains of young adults, many of which can have significant behavioral and cognitive consequences. The Substance Abuse and Mental Health Services Administration (SAMHSA) describes substance use disorders as occurring when they reach the level when “the recurrent use of alcohol and/or drugs causes clinically significant impairment, including health problems, disability, and failure to meet major responsibilities at work, school, or home” (SAMHSA, 2020c). Trends in use of substances, from recreational to abuse, are detailed in the sections below. Similar to mental health data, unless noted the data on substance use are self-reported.
Trends in Alcohol Use
In 2018, 60 percent of current U.S. college students reported past-month alcohol use, 28 percent reported binge drinking8 in the past two weeks, and 10
___________________
8 Binge drinking is defined as a pattern of drinking that brings blood alcohol concentration (BAC) levels to 0.08 percent. This typically occurs after four drinks for women and five drinks for men—in about two hours. High-intensity drinking is defined as alcohol intake at levels twice or more the threshold for binge drinking (NIAAA, 2018).
percent reported high-intensity drinking in the past two weeks. In the same year, 11 percent of full-time college students met clinical criteria for an alcohol use disorder (AUD) in the past year (SAMHSA, 2019d).
While alcohol use by college students remains high, data from several sources show that binge drinking among students has gone down over the past several years (see Table 2-6). For example, data from HMS show that self-reports of binge drinking “any time in the past two weeks” and “three or more times in the past 2 weeks” was down 18.16 percent and 28.09 percent, respectively, between 2013 and 2018. Similarly, self-reported data from ACHA-NCHA and clinical data from CCMH show a reduction in binge drinking among students between 2013 and 2018 (see Table 2-4).
One factor that may explain the drop in the percentage of students reporting binge drinking over time is a reduction in binge drinking among men. In a survey of the nation’s college students and adults from ages 19 through 60, the authors found that prevalence of past-month alcohol consumption has declined modestly since 1980, when men had slightly higher use; the gender gap disappeared by 2000. Among college students, binge drinking has traditionally shown a significant gender difference, but a gradual long-term decline in binge drinking among college men since 1985 and little change among college women has narrowed the gap (in 2018, 32 percent of male college students binge drank compared to 27 percent of females) (Schulenberg et al., 2019).
However, another consistent finding has been that female students are more at risk for alcohol-related problems and have higher risk for meeting criteria for AUD (Clarke et al., 2013; Slutske, 2005). In 2018, 12 percent of male college students and 11 percent of female college students met criteria for AUD (SAMHSA, 2019d). An increase in the proportion of students with an AUD from 2017 to 2018 was significant among female students, but not male students.
TABLE 2-4 Comparison of Measures of Binge Drinking in Higher Education Students from Multiple Sources in 2013 and 2018
| Measures of Binge Drinking | Year | ||
|---|---|---|---|
| Fall 2013 (%) | Fall 2018 (%) | % Change 2013-2018 | |
| CCMH: Binge drinking (Any in the past 2 weeks)a | 41.1 | 37.4 | - 8.10 |
| CCMH: Binge drinking (3+ times in the past 2 weeks)a | 12.6 | 10.1 | - 19.84 |
| HMS: Binge Drinking (Any in the past 2 weeks)b | 45.7 | 37.4 | - 18.16 |
| HMS: Binge Drinking (3+ times in the past 2 weeks)b | 17.8 | 12.8 | - 28.09 |
| NCHA: Binge Drinking (Any in the past 2 weeks)c | 29.8 | 28.4 | - 4.7 |
| NCHA: Binge Drinking (3+ times in the past 2 weeks)c | 9.2 | 7.0 | - 23.9 |
aCCMH (clinical data); bHMS (general population data); cNCHA (general population data)
Sources: ACHA, 2014, 2018; CCMH, 2015, 2020a; HMN, 2007-2019.
College students are at increased risk for problematic patterns of alcohol use compared to their non-college-attending peers (Schulenberg et al., 2019). This has long been true. For example, although the 2001-2002 National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) found that college students and their non-college peers consume alcohol at similarly heavy rates (Chen et al., 2004), college students had a higher prevalence of drinking and risk drinking than did their non-college peers. Nevertheless, the “rates of alcohol abuse and dependence are roughly equivalent for college and non-college individuals, and the development of alcohol-use disorders among young adults is more related to their living situation (e.g., at home with parents, on campus, off campus) than to college status itself” (Carter, Brandon, and Goldman, 2010; Dawson et al., 2004).
Furthermore, certain student groups are at higher risk for excessive alcohol use compared to their peers. For example, undergraduates have higher rates of binge drinking than graduate students (Cranford, Eisenberg, and Serras, 2009). A stable trend in college alcohol use since the 1980s is that white college students are the heaviest drinkers followed by Hispanic and Black students (Borsari, Murphy, and Barnett, 2007; Ham and Hope, 2003). Students who began drinking at an earlier age and come to college as established drinkers maintain or increase their drinking levels in their first year of college to levels well above their peers who were light drinkers or abstainers in high school (Borsari et al., 2007; Ham and Hope, 2003). College athletes drink alcohol more often, consume higher quantities of alcohol, and experience more negative alcohol-related consequences than non-athlete college students (Martens, Dams-O’Connor, and Beck, 2006). Similarly, involvement in a Greek organization (a fraternity or sorority) is consistently shown to be associated with heavier alcohol use compared to other students (Borsari et al., 2007; Ham and Hope, 2003).
College-level factors can also increase risk for excessive alcohol use among students. Students at 4-year colleges are more likely to binge drink compared to students at 2-year institutions. However, an important factor to consider is a student’s living situation, since living with family has been shown to be a protective factor against excessive alcohol use. A larger proportion of students at 2-year colleges live with family compared to students at 4-year colleges (Velazquez et al., 2011). Regarding “dry” campuses, one study found that students had lower rates of alcohol use and binge drinking at schools that prohibited the use of alcohol on campus compared to schools that allowed alcohol use (Wechsler et al., 2001). Students were 30 percent less likely to be heavy episodic drinkers and 80 percent more likely to be abstainers at schools that prohibited alcohol use. The research literature shows a consistent association between a campus’ proximity to alcohol outlets and increased alcohol use and related harms among college students and may be a more relevant risk factor than the geographic characteristics of the college itself (e.g., rural, urban) (Scribner et al., 2008; Weitzman et al., 2003).
Trends in Marijuana Use
Marijuana use by college students has increased over the past several years. Data from the HMS, CCMH, and ACHA-NCHA each show a roughly 30 percent increase in marijuana use by students between 2013 and 2018 (see Table 2-5). The primary driving force behind these increases is higher marijuana use by women in recent years.
Gender differences observed in past-year marijuana use prior to 2010 have vanished in 2018 (43 percent for college men and 42 percent for college women) as a result of steady levels of use among males and increasing use among females. Past-month vaping of marijuana is also following this trend, with use among male students increasing more modestly in recent years compared to females; in 2018, 13.1 percent of male college students vaped marijuana compared to 9.3 percent of females (Schulenberg et al., 2019). Daily marijuana use remains twice as high among college men (8.4 percent) compared to college women (4.3 percent).
Marijuana use among college students today may reflect new use patterns and products. The average level of tetrahydrocannabinol (THC), the main compound in marijuana responsible for mind-altering effects, in marijuana rose from 4 percent in 1995 to 15 percent in 2017 (NASEM, 2017). The rise in potency can be attributed to the different types of marijuana products on the market and new methods of production in recent years compared to decades ago. For example, extremely potent forms of marijuana concentrates are becoming more prevalent in the United States. These trends suggest that people who use marijuana may be more at risk of harms compared to previous years (Marconi et al., 2016; Murray et al., 2016; Volkow et al., 2016).
Trends in Prescription Medication Misuse
In 2018, 4 percent of full-time college students misused a prescription medication in the past month, a decrease from 5 percent in 2017, with stimulants being
TABLE 2-5 Comparison of Measures of Marijuana Use in Higher Education Students from Multiple Sources in 2013 and 2018
| Measures of Marijuana Use | Year | ||
|---|---|---|---|
| Fall 2013 (%) | Fall 2018 (%) | % Change 2013-2018 | |
| CCMH: Marijuana use (any in the past 2 weeks)a | 20.1 | 25.8 | 28.36 |
| CCMH: Marijuana use (3+ times in the past 2 weeks)a | 11.4 | 15.3 | 34.21 |
| HMS: Marijuana use (any time in the past month)b | 16.1 | 21.5 | 33.5 |
| ACHA-NCHA: Marijuana use (any use in the past 30 days)c | 14.1 | 19.0 | 34.8 |
aCCMH (clinical data); bHMS (general population data); cNCHA (general population data)
Sources: ACHA, 2014, 2018; CCMH, 2015, 2020a; HMN, 2007-2019.
the most common prescription medication used non-medically among college students (McCabe et al., 2005a; SAMHSA, 2019d).9 Risk factors for non-medical use of prescription stimulants include being male, white, a member of a Greek organization, and having a lower grade point average (Cranford et al., 2009). At the campus level, rates of non-medical stimulant use are higher at colleges in the Northeast region of the United States and at colleges with more competitive admission standards (McCabe et al., 2005a). Prescription drug misuse rarely occurs alone. Students who report non-medical stimulant use are also more likely to report alcohol, cigarette, marijuana, ecstasy, and cocaine use. Specifically, 70 percent of students who misused prescription stimulants in a national study were excessive drinkers and 68 percent used marijuana during the past month.
Opioid use (particularly heroin and synthetic opioid use) is less common in college students compared to their non-college-attending peers. In 2018, 1 percent of full-time college students in the United States used a prescription opioid non-medically in the past year (SAMHSA, 2019d). The college population has not been the focus of opioid research in recent years (McCabe et al., 2005b).
Impact of Substance Use on College Students
In 2004, the last year for which estimates are available, 599,000 college students were injured because of their alcohol use, 696,000 were hit or assaulted by another drinking college student, and 97,000 experienced a sexual assault or date rape perpetrated by another college student who had been drinking (Hingson, Zha, and Weitzman, 2009). Male students tend to experience more alcohol-related consequences that involve public deviance while consequences experienced by female students tend to be more personal; females also experience more dependence symptoms (Clarke et al., 2013; Ham and Hope, 2003).
A quarter of women in the United States have experienced sexual assault, and approximately half of those cases involve alcohol consumption by the perpetrator, victim, or both. Among college students, 22 percent report experiencing at least one incident of sexual assault (Mellins et al., 2017). In one study with a large
___________________
9 From SAMHSA: Questions about past-year use and misuse in the 2018 NSDUH covered the following subcategories of stimulants: amphetamine products (Adderall®, Adderall® XR, Dexedrine®, Vyvanse®, generic dextroamphetamine, generic amphetamine/dextroamphetamine combinations, or generic extended-release A-71 amphetamine-dextroamphetamine combinations); methylphenidate products (Ritalin®, Ritalin® LA, Concerta®, Daytrana®, Metadate® CD, Metadate® ER, Focalin®, Focalin® XR, generic methylphenidate, generic extended-release methylphenidate, generic dexmethylphenidate, or generic extended-release dexmethylphenidate); anorectic (weight-loss) stimulants (Didrex®, benzphetamine, Tenuate®, diethylpropion, phendimetrazine, or phentermine); Provigil®; or any other prescription stimulant. Other prescription stimulants could include products similar to the specific stimulants listed previously. Since 2015, methamphetamine has not been included as a prescription stimulant. Questions were not asked about past-month stimulant use or misuse for the subtype categories.
college student sample, female students and gender nonconforming students reported the highest rates of sexual assault (28 percent for both), while 12.5 percent of men experienced assault. The most frequent correlate of experiencing assault was incapacitation as a result of alcohol and drug use (greater than 50 percent). Factors that increased risk for sexual assault included non-heterosexual identity, membership in a Greek organization, and binge drinking, among others. Drug- or alcohol-facilitated/incapacitated rape survivors are less likely to acknowledge their rape and therefore less likely to seek services or treatment (Walsh et al., 2016).
The 2019 Association of American Universities (AAU) Campus Climate Survey on Sexual Assault and Misconduct included 181,752 students from 33 colleges and universities, including 32 AAU member schools. The authors found that the “overall rate of non-consensual sexual contact by physical force or inability to consent since a respondent enrolled as a student at their school was 13 percent, with the rates for women and transgender, genderqueer, and non-binary (TGQN, defined as transgender, genderqueer, questioning or not listed) students being significantly higher than for men” (AAU, 2019).
American Psychiatric Association research shows consistently that the increasing intensity of marijuana use is associated with increasing risk for psychosis later in life (Marconi et al., 2016; Murray et al., 2016). Higher potency marijuana products and synthetic marijuana carry the most risk for psychotic outcomes. Marijuana use is also consistently shown to have a detrimental effect on cognitive function, and these consequences are magnified if use starts early in adolescence (Shrivastava, Johnson, and Tsuang, 2011). Further, a robust meta-analysis concluded that marijuana use is a significant predictor of developing depression, suicidal ideation, and experiencing a suicide attempt (Gobbi et al., 2019). Overall, the risk for these mental health outcomes remains moderate to low among young adults using marijuana. However, the increasing numbers of young people using marijuana creates a larger population who could develop depression or suicidality attributable to marijuana use and exacerbate the mental health situation among college students in the United States. Regarding the acute impacts of marijuana use, research is consistent in showing that marijuana use causes acute impairment of learning and memory, attention, and working memory, but whether there is enduring neuropsychological impairment is less clear (Volkow et al., 2016).
COMORBIDITY BETWEEN MENTAL HEALTH AND SUBSTANCE USE IN HIGHER EDUCATION
“Comorbidity” is the term used to describe the presence of two or more illnesses at the same time. According to the National Institute on Drug Abuse (NIDA), comorbidities “can occur at the same time or one after the other. Comorbidity also implies interactions between the illnesses that can worsen the course
of both” (NIDA, 2020c). It is also possible that the presence of one condition may contribute to the development of another. Individuals with mental illness, for example, may use substances as a coping mechanism to deal with the symptoms of this disorder, even though substance use can also exacerbate underlying conditions. Similarly, the repeated use of drugs or alcohol can affect the way the brain works, which can increase an individual’s susceptibility to developing mental health issues (NIDA, 2020c).
The use of substances in adolescents and young adults poses a particular set of risks, as these years are critical to brain development. In fact, research shows that “early drug use is a strong risk factor for later development of substance use disorders, and it may also be a risk factor for the later occurrence of other mental illnesses” (NIDA, 2020a). While this is not a causal link, adolescence and young adulthood are times when both mental illness and substance use disorders are likely to begin.
While not specific to college students, for young adults, approximately 8.9 million individuals aged 18-25 had any mental illness (AMI) in the past year, and 5.1 million had a past-year substance use disorder (SUD). In this age group, 2.4 million had both AMI and an SUD in the past year (approximately 7.2 percent of young adults). In that group, 43.8 percent received substance use or mental health care in 2018. Of that group, 37.9 percent received only mental health care, 3.7 percent received care for both, and 2.0 percent for substance abuse only (CBHSQ, 2019).
Approximately 1.7 million young adults aged 18-25 had a severe mental illness coinciding with an SUD, or 1.7 of adults in this age group. In this age group, 60.1 percent received either mental health care or substance use treatment. Within this group that received treatment, 52.8 received only mental health care, 5.8 percent received treatment for both, and 1.5 percent received substance use treatment only (CBHSQ, 2019). The rates of parallel treatment for comorbid conditions, however, do not align with the latest research findings suggesting that treating mental health and substance use disorders in concert can provide longer-lasting effects.
There are other types of comorbidity in addition to mental illness and substance use. Different mental health disorders can occur together—comorbid anxiety and depression, for example—and they can co-occur with physical health disorders—depression and diabetes, for instance (OPA, 2020). The links between mental health, substance use, and physical health may tie into an individual’s environment from infancy through young adulthood. A multitude of factors can contribute to the development of comorbid issues: “The interaction between childhood activities and biology could affect brain development and—ultimately—social, behavioral, academic, health, and other outcomes” (OPA, 2020).
This page intentionally left blank.






























