
4
Clinical Mental Health and Substance Use Services for Students in Higher Education
Many colleges and universities provide services to students in a clinical setting in addition to programs focusing on general student wellbeing. These services may include general health, as well as those for students experiencing mental health and substance use problems. However, there is considerable variation in the scope of services, the level of education and professional licensure of the clinical staff, the availability of clinical providers, and the training that the providers have received to work with specific populations of students. Because use of mental health services is to be held confidential by a range of state and federal laws (e.g., the Health Insurance Portability and Accountability Act), it can be challenging for institutions to balance collaborating services across the whole student while also respecting a student’s state/federal right to privacy.
In general, on-campus treatment centers and their staff are uniquely positioned, trained, and professionally focused to effectively navigate this important balancing act (e.g., working with residence life and student conduct units to proactively manage a perceived behavioral threat with mental health concerns). Depending on the size and financial resources of a campus, connections to independent, off-campus providers may also be an important part of the network of care for student mental health. Challenges exist, however, with referrals to private off-campus providers. In general, they are explicitly focused on the treatment of the individual and have considerably less training and dedicated time to overcome legal privacy concerns in order to coordinate with multiple on-campus offices. Other challenges can include distance from campus and students’ lack of transportation; difficulty navigating private health insurance systems; limited coverage
for mental health on many insurance plans; students’ lack of health insurance generally; costs of coverage and copays; and lack of community providers or limited providers that support college students. For students able to navigate and access mental health care in the community, issues may also arise in terms of releasing information from campus providers, receipt of records back to the college or university system (such as for accommodations for learning disabilities), and continuity of care if the student leaves for vacations, field work, an internship, or another off-campus experience.
Student access to these services differs as well. The students who use these services range from those with preexisting conditions looking for support and management to students developing issues during their enrollment. There may be limitations for students in terms of availability of services (how many sessions are provided or how quickly students can be seen), times when services can be accessed, and concern about cost (even if the services are covered by student fees). Stigma may also inhibit student use of needed services. While some students may feel willing to attend a student seminar focused on wellbeing with peers or to join a department workshop focused on building a work/life balance, the stigma around mental health and substance use may also be a barrier to seeking needed services. In addition, some clinical services may require referrals for access to a psychiatrist, be required to do additional intake forms, or go on a waiting list.
This chapter discusses some of the ways in which colleges and universities are providing mental health and substance use services, beyond the wellness programs addressed in Chapter 3. It also describes the various policies that govern how higher education provides services, such as mandated alcohol and substance use education.
THE HISTORICAL AND POLICY CONTEXT FOR MENTAL HEALTH AND SUBSTANCE USE SERVICES IN HIGHER EDUCATION
The history of student health care on campuses began at Amherst College in 1861, although mental health services were not offered until the establishment of a practice at Princeton University in 1910 (Kraft, 2011). Though the American Student Health Association included “mental hygiene” as a priority in 1920, it was not until 1957 that the American College Health Association formed a section for mental health professionals and for mental health and counseling services to become a more standard feature on campuses (Kraft, 2011). Until the 1960s, U.S. colleges and universities operated in loco parentis, meaning they had the authority and responsibility to oversee students’ personal lives and individual actions without due process (Lee, 2011).
After World War II and the increase of veterans using G.I. Bill benefits to pursue higher education, college and university enrollments increased alongside
the demand for mental health professionals (Kraft, 2011).1 At this time, mental health services were divided between psychiatric consultation and student health in one unit and counseling centers in another. While funding for counseling centers originally came from general institutional revenue, restructuring occurred when colleges and universities began to charge separate fees to cover health services.2 As campuses looked to streamline counseling services and shift costs for mental health counseling to student health fees and/or separate health insurance coverage, many schools merged counseling services with psychiatric and mental health services. As Kraft (2011) notes “the multidisciplinary mental health service became the norm on campuses rather than the exception.” In 1950, the Association of University and College Counseling Center Directors (AUCCCD) was founded to create a community of mental health leaders in higher education. Today, AUCCCD represents nearly 1,000 college and university counseling centers. The American College Counseling Association (ACCA), American Psychological Association, and American College Health Association also have sections and program devoted to student mental health.
Federal Regulations for Higher Education
Americans with Disabilities Act
In 1990, Congress passed the Americans with Disabilities Act (ADA) to protect the civil rights of individuals with disabilities related to employment, public services, and places of public use. Similar to laws passed to protect individuals from discrimination based on race, religion, sex, and national origin, the ADA’s goal is to “assure equal opportunity, full participation, independent living, and economic self-sufficiency for Americans with Disabilities” (ADA National Network, 2020).
The ADA includes provisions for access and participation in postsecondary education. U.S. legislation has included policies regarding support to transition from K-12 to higher education; efforts by disability services offices at universities to improve student access; principles of universal design and accommodations to ensure accessibility; and a growing emphasis on the use of technology and diversity within the student population (ADA National Network, 2020). For a student to receive protection under the ADA, they must have a “physical or mental impairment that substantially limits one or more major life activities” (e.g.,
___________________
1 The G.I. Bill did not make college more accessible for all veterans: “While the introduction of generous student aid through the G.I. Bill held the promise of significantly reducing black-white gaps in educational opportunity and long-run economic outcomes, the G.I. Bill exacerbated rather than narrowed the economic and educational differences between blacks and whites among men from the South” (Turner and Bound, 2003).
2 Information about current funding models and related challenges appear in Chapter 5 in the section Insufficient Funding.
learning, caring for oneself, walking, seeing, hearing, speaking, and working); have a record of having had this type of impairment; and be regarded as having this type of impairment (Jed Foundation, 2008).
On campus, colleges and universities must ensure that faculty, other instructors (including graduate students and postdoctoral researchers), and staff comply with the ADA in educational settings, including extracurricular activities, by extending the time for test taking or completing course work; by substituting specific courses to meet degree requirements; and by modifying test taking or performance evaluations so as not to discriminate against a person’s sensory, speaking, or motor impairments, unless that is what is being tested. Accommodations can also include providing auxiliary aids and services such as qualified sign language interpreters, note takers, and readers, as well as adaptive equipment and braille, large print, and electronic formats of print materials (American Psychological Association, 2020).
Students with disorders that impact their cognitive and emotional functions, such as attention deficit disorder and attention deficit and hyperactivity disorder (ADD/ADHD) and autism spectrum disorder can receive protection under the ADA, too (see the section on Neurodiverse Students in Chapter 3). Students who are pregnant or have pregnancy-related health issues may also seek accommodations through the ADA.
Drug-Free Schools and Communities Acts and Campus Recovery Programs
In 1989, under the Drug-Free Schools and Communities Act, legislators amended the Higher Education Act by requiring colleges and universities to “invest considerable energy in implementing substance abuse prevention programs, distributing written policies, and evaluating program outcomes” (Custer and Kent, 2019). Prevention programs must meet a number of minimum federal standards for employees and students regarding unlawful possession; description of laws regarding possession and distribution at the local, state, and federal level; description of health risks associated with substance use disorders; support, treatment, and recovery programs made available; and a clear statement about disciplinary actions used against those who violate policy (DeRicco, 2006). Colleges and universities may be subject to additional state and local regulations.
Family Educational Rights and Privacy Act of 1974
The Family Educational Rights and Privacy Act (FERPA) established in 1974 to protect student educational records, applies to all schools receiving funds from the Department of Education (ED, 2020). Without a waiver, FERPA precludes colleges and universities from sharing academic records except in limited circumstances, such as when there is an urgent need to protect the health and safety
of a student or another person on campus. In the event that an individual poses a risk to themselves or others, university officials are permitted but not required to inform appropriate individuals (HHS and ED, 2019). (See discussion of the Health Insurance Portability and Accountability Act of 1996 [HIPAA] below for additional information.)
Health Insurance Portability and Accountability Act of 1996
HIPAA ensures the privacy of medical records for all individuals, and it has specific implications for students. The act protects an individual’s medical records by limiting electronic access to the records to health care service providers. This means that families of students cannot access their health care records without a release of information signed by the student. It also means that student mental health records (included health care and counseling) cannot be transferred electronically to others at the college or university without a signed release of information, except to a very limited set of university personnel such as police or physicians in situations where there is a risk of imminent harm (HHS and ED, 2019).
Federal Funding for Mental Health, Substance Use, and Wellbeing Research and Programs
The Garrett Lee Smith Memorial Act
In addition to funding from sources within the college or university, there have been some federal programs that have sought to intervene in college mental health (see Box 4-1). The Garrett Lee Smith Memorial Act (GLSMA, 2004) was signed into law in October 2004 and with an original authorization for $82 million in grants related to suicide prevention to be administered by the Substance Abuse and Mental Health Services Administration (SAMHSA). GLSMA provided federal funding for the first time to states, tribes, and colleges to implement community-based suicide prevention programs for youth and young adults (Godoy Garraza et al., 2018). As of 2020, GLSMA had supported 243 total State tribal grants in 50 states and the District of Columbia, 67 tribes or tribal organizations, and 309 grants to 269 institutions of higher education. Institutions of higher education have used GLSMA funds to develop comprehensive, collaborative, well-coordinated, and evidence-based approaches to (1) enhance mental health services for all college students, including those at risk for suicide, depression, serious mental illness (SMI)/serious emotional disturbances (SED), and/or substance use disorders that can lead to school failure; (2) prevent mental and substance use disorders; (3) promote help-seeking behavior and reduce negative public attitudes; and (4) improve the identification and treatment of at-risk college students so they can successfully complete their studies. It is expected that this program will reduce the adverse consequences of SMI/SED and substance
use disorders, including suicidal behavior, substance-related injuries, and school failure (SAMHSA FOA SM18-003).
While students have been the primary audience for Campus GLSMA-funded efforts, gatekeeper training,3 intended to provide suicide prevention and awareness to a broader audience, reached other groups including college faculty, college counseling and health center staff, residential life staff, campus security, parents and guardians, and primary care staff (Godoy Garraza et al., 2018).
Figure 4-1 shows various suicide prevention strategies employed by GLSMA grantees, from outreach and awareness training to traditional healing practices. Data are available at the category level for state, tribal, and campus grantees in cohorts 1-12. Data collection at the strategy level began in 2010; therefore, data are available at the strategy level for state and tribal grantees in cohorts 4-12 and campus grantees in cohorts 3-12. Table 4-1 provides details on grantee participation by level of intervention.
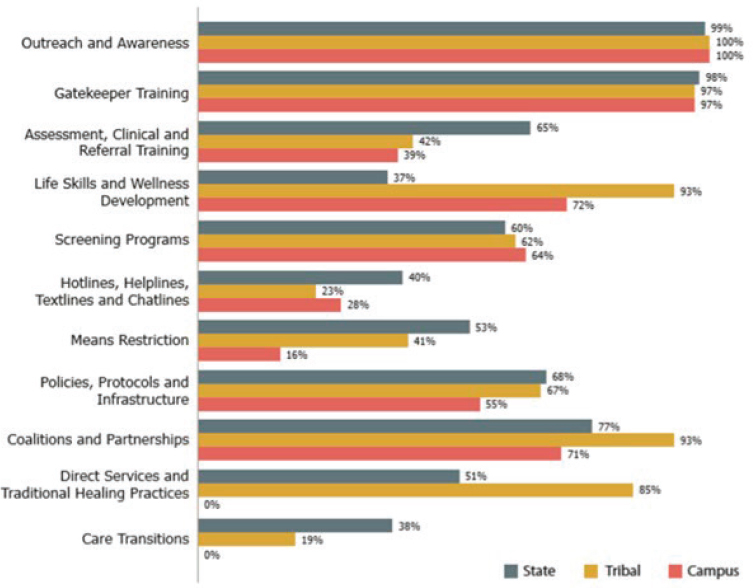
Source: SAMHSA. Prevention Strategies Inventory, June 2019, State/tribal cohorts 1-12, campus cohorts 1-12.
___________________
3Chapter 5 includes a more detailed discussion of gatekeeper training programs.
TABLE 4-1 Grantee Participation in Prevention Strategies Inventory
| Level of Data | State Grantees | Tribal Grantees | Campus Grantees |
|---|---|---|---|
| Category | 124 of 124 | 73 of 75 | 266 of 266 |
| Strategy | 93 of 93 | 66 of 68 | 211 of 211 |
Source: SAMHSA.
GLSMA grants require an evaluation plan, but the purpose of these grants is to fund programs and non-clinical services, not research. In terms of evaluating the funding program, the variety in program structure and data collection makes research challenging (Godoy Garraza et al., 2018). Nonetheless, some evaluations have provided insights into the context-specific needs of suicide prevention programs and site readiness for programs. Across sites, students who are suicidal often drop out of treatment, and there is a need for additional research4 on how to engage at-risk students for treatment and lower barriers to receiving services (Godoy Garraza et al., 2018).
Over the past 15 years, GLSMA has focused most of its funding on supporting interventions to increase help-seeking by students or increase the community’s ability to successfully identify and refer students in need. These themes are consistent with the original suicide prevention focus of the bill. However, because these interventions are designed to increase the number of students seeking mental health services (and thus preventing suicide), it is possible that some of the increase in demand for services being observed nationally is a result of interventions such as this. Future funding decisions will need to proactively align intervention efforts with growing clinical capacity to receive students who are identified and referred for help.
MENTAL HEALTH AND SUBSTANCE USE SERVICES AND STAFF
The range of clinical services that college and university centers provide varies substantially. For example, evidence-based treatments such as psychotherapy may not be available everywhere (IOM, 2015). According to ACCA, the majority of support takes the form of one-on-one therapy sessions, group counseling, testing and assessment, and emergency services (College Counseling Knowledge-Base: Comprehensive Database of College Counseling Research Publications in the College Counseling, Counseling Psychology, College Health, College Student Development and Professional Counseling Literatures 1998-2017) (see Chapter 3 for more information on general, non-clinical programs and services). Students who can benefit from short-term therapy might meet regularly with a therapist at the campus counseling center. For those students in need of long-term therapy or who have mental health issues beyond the scope of what the campus counseling staff can offer, a center can make referrals to local providers; however, issues related to off-campus providers can limit the degree to which students can access services (Brown, 2020). (Please see below for a section on Referrals to External and Community Providers and Chapter 5 for more information on referrals.)
The Association of University and College Counseling Center Directors’ 2019 survey of 562 university and college counseling center directors found
___________________
that “37.2 percent of counseling centers used a version of stepped care, offering a campus-wide menu of service options ranging from no care at all to weekly therapy at the counseling center. Depending on the center, options may include appropriate forms of self-help, wellness coaching, support groups, mindfulness classes, appropriate apps and online resources, etc.” (LeViness et al., 2019). In addition, 46.6 percent of counseling center directors reported that psychiatric services are offered on their campus, and 57 percent of directors whose centers have psychiatric services reported that they need more hours of psychiatric services than they currently have to meet student needs (LeViness et al., 2019).
While the overall model may be similar, the range of services, hours and locations, and the number and expertise of staff available at a given institution can vary considerably. The staffing model at an institution’s counseling center may include but is not limited to psychiatrists, counselors, other therapists, case workers, campus outreach coordinators, training directors, liaisons to community providers, group programming coordinators, student advisors, and graduate students in psychology, psychiatry, and social work. Staffing for centers continues to grow; the AUCCCD survey found that 43.9 percent of centers added staff positions between 2018 and 2019, while only 5.1 percent lost staff positions during the same time period.
Community colleges do not necessarily follow the same trends and may face a different set of expectations, as 96 percent of counselors in community colleges have other duties such as academic advising, career counseling, and other administrative duties (IACS, 2019). State licensing bodies for psychology, counseling, and social work may vary as well.
Community colleges may not have the same ability to dedicate funding to support mental health services and staff as more well-funded institutions, as they are less likely to have financial support from states and lack the security of the endowment funds that have safeguarded wealthy institutions. Community colleges tend to serve students from lower socio-economic backgrounds and have fewer options for recourse in terms of raising funds. In particular, these colleges may have dual-role counselors tasked with providing academic advising and general counseling to the student (Eisenberg et al., 2016). In a 2017 survey of community colleges in 30 states concerning dual-role staff, 51 percent of these staff provide academic advising (in addition to mental health counseling), and 73 percent provide mental health counseling in the same office where other student services are provided (Edwards and Lenhart, 2017). Some 66 percent of counseling center directors reported providing psychiatric services, and 56 percent of these directors report needing more hours of psychiatric services to meet the student need (IACS, 2019; LeViness et al., 2019)
Historically Black Colleges and Universities (HBCUs) and Tribal Colleges and Universities (TCUs) face similar challenges in terms of receiving less financial support from states. HBCUs and TCUs, along with community colleges, provide education to a broader group of students, have lower tuition and fees,
provide more flexibility and accommodations for working students, and services that provide an environment inclusive to Black and Indigenous students.
Similarly, several HBCUs and TCUs and other colleges and universities have a limited ability to provide psychiatric services to students. Some of the impediments are financial, such as lack of funding for a full-time position and only being able to offer limited hours and a part-time position, while others might be related to the more widespread paucity of psychiatrists in the community. In terms of access, the result is that students who need psychiatric evaluations, treatment, and oversight to manage medical approaches often do not have access on campus and given the general shortage of psychiatrists in the nation, may not have access to a community provider either (Pedrelli et al., 2015). Of the universities that can afford to have an on-campus psychiatrist, many have only one—and time constraints often limit their role to medication evaluation and management and crisis evaluation (Iarovici, 2014). Of the centers that offer psychiatric services, 56.3 percent reported that there is more demand than their current level of services can address. For students who require medications as a part of their treatment, challenges may arise identifying a psychiatrist on campus or in the community. Just as in the community, colleges and universities rely increasingly on primary care providers to step in and provide pharmacological treatments to students with mental health issues.
One limiting factor for staffing of campus counseling centers is compensation. Compensation in higher education positions tends to be lower than in other sectors, which often means that qualified applicants have the option of leaving for higher-paying positions elsewhere (LeViness et al., 2019). Other factors making it difficult to staff centers include burnout resulting from high caseloads and lack of flexibility in determining schedules as compared with private practice settings (Kafka, 2019).
Referrals to External and Community Providers
Depending on the scope of care and available services at a college or university mental health center, campuses may provide students with off-campus referrals. Centers may offer students information about community clinics, local hospitals, or formal or informal referral channels to private providers. However, the shift from a college counseling center to an external provider can present challenges for exchange of records, finding a provider, scheduling, insurance coverage and cost, transportation, and student comfort (King Lyn, 2015). In terms of student comfort, individuals with some historically excluded identities may feel comfortable seeking services on a campus if they feel a sense of belonging; however, depending on the surrounding region, some students may not be as willing to leave campus. Even for community colleges students who may not have the same connection to a physical campus, these institutions are more likely to serve students who have had less access to mental health resources and may seek
support from a place they are already know and trust. This may include students who are BIPOC in predominantly white areas or SGM students in states that have been hostile to people with their identities. The awareness that some communities may not feel welcoming or inclusive can help staff at some centers understand why students may not wish to seek off-campus services and work with students to update their centers’ resources and guidance accordingly.
There is also great variability in the availability of appropriate service providers in the communities surrounding institutions of higher education (King Lyn, 2015). To ease the process referring students, college and university mental health staff may build connections to local providers, refer students to practices where there are existing connections, and provide students with information about two-way communication that can occur between the campus center and external provider with a release of information. Other ways to support the process may include information about how to look for providers based on insurance; how to understand co-pays, costs, and providers with sliding scales; providers that offer extended hours, speak other languages, or have specialties related to specific identities or health issues; and ways to address frequently asked questions or misconceptions related to off-site care. Some colleges and universities have begun hiring case workers and other staff positions to help students navigate and manage off-campus services.
Additional challenges with off-campus services relate to the availability of psychological, therapeutic, and psychiatric services in the local community and region. Rural communities across the United States have seen a decline in general health care providers and have struggled to have medical providers of all specialties serve in more remote areas. Some urban areas have been historically limited in their access to health care as a result of bias in public funding; unwillingness of medical providers to work in neighborhoods that predominantly serve individuals who are BIPOC; and discriminatory urban planning. For students at campuses in communities with limited mental health resources, off-campus services may require long waiting periods and other barriers related to overwhelmed providers. It is also worth noting that not all health care services are equal, and students may determine that the available services do not merit the potential costs of seeking treatment. See Chapter 5 for recommendations for ways to address these issues.
Substance Use Treatment, Substance Use Recovery Programs, and Programs for Students in Recovery
The National Institute on Alcohol Abuse and Alcoholism published the College Alcohol Intervention Matrix (CollegeAIM) in 2015 to help college personnel create comprehensive, campus-specific alcohol intervention strategies. CollegeAIM provides a range of individual- and environmental-level policy
options aimed at reducing underage and excessive drinking among college students. These policies are ranked in CollegeAIM according to effectiveness, evidence-base, and cost; each policy is accompanied by information on barriers to effectiveness, the staffing required for policy enactment and implementation, and other factors. The authors of CollegeAIM emphasize that a mix of strategies is the best method to maximize positive effects and reduce excessive drinking and related problems among college students. Examples of the types of interventions included in the CollegeAIM matrix are:
- Enforcement of the age-21 drinking age
- Establishment of minimum unit pricing of alcoholic beverages and increasing the alcohol tax
- Prohibiting alcohol use and sales at campus sporting events and restricting alcohol sponsorship and advertising
- Retaining a ban on Sunday sales (where applicable) and limiting the number and density of alcohol establishments
- Conducting campus-wide social norms campaigns
- Personalized normative feedback programs that provide all students with information about their alcohol use in comparison with actual use by their peers
These strategies, practices, and policies are consistent with the Surgeon General’s Call to Action and 2016 Report on Alcohol, Drugs, and Health.
Another resource, The Guide to Best Practices, published by the Maryland Collaborative to Reduce Underage Drinking and Related Problems (MCRCDRP, 2013), similarly summarizes individual- and environmental-level strategies available to college campuses. At the individual level, the authors advise that campuses should develop a roadmap outlining how they screen for and identify students in need of services, and refer them to necessary treatment. This roadmap should state how institutions will provide training to key individuals on campus, use valid and reliable screening instruments, track student screening and identification, and engage parents in all stages of the student’s college career. At the environmental level, the guide asserts that campuses should build coalitions with the wider community, be proactive in enforcing existing alcohol laws, reduce the density of alcohol outlets near campus, address alcohol pricing and other promotional practices, and incorporate community-enhancing practices into landlord lease agreements.
Since the 1970s, colleges and universities have introduced collegiate recovery programs (CRPs) to support students with substance use disorders (Hazelden Betty Ford Foundation, 2020). While all institutions of higher education are required to conduct prevention and education efforts to reduce the presence of illegal and dangerous alcohol consumption for students, “most are lacking in specific
programming to support those students who are in recovery” (The Ohio State University, 2020). CRPs can provide integrated services for students in recovery with a combination of academic and health-oriented approaches. While services vary across providers, common features may include “substance-free housing and social events, dedicated space, on-campus twelve-step support meetings, full-time dedicated staff and professional counseling by addiction treatment specialists” (Hazelden Betty Ford Foundation, 2020). Some colleges and universities may require students to sign contracts to participate in these programs that include minimum standards for academic performance, sobriety, and participation in programs to remain eligible, while others are barrier-free and welcome all of those in recovery or in search of recovery (Hazelden Betty Ford Foundation, 2020).
CRPs are intended to support students who arrive on campus already in recovery as well as students who develop substance use disorders during their enrollment. Research estimates that approximately 250,000 students in higher education have received treatment for substance use in their lifetime (Hazelden Betty Ford Foundation, 2020). At present, there are approximately 100 schools who have joined the Association of Recovery in Higher Education with commitments to CRPs through the Transforming Youth Recovery effort (The Ohio State University, 2020). However, the increase in programs does not necessarily mean that treatment for all substance use issues has grown evenly: “Although many initiatives target active substance abuse problems on campus, particularly binge drinking, few services are available that specifically aid students in recovery from alcohol or drug addiction” (Perron et al., 2011).
CRPs and other programs may likely work best with colleges and universities that have a large on-campus population. Community colleges, some graduate programs, and virtual universities may face different challenges, and there is little research on substance use prevention and treatment specific to these populations. For community colleges, there are studies that correlate the increased number of students who have experienced an adverse childhood experience (see Chapter 3 for more on Student Survivors of Trauma) with both community college enrollment and substance use disorders (Cadigan and Lee, 2019).
Challenges and Opportunities in Utilizing Telehealth to Support Mental Health Services
Telehealth refers to a variety of methods of synchronous or asynchronous communication with a mental health professional via video conferencing, email, text, online chat tools, or the phone (Higher Education Mental Health Alliance, 2014). Telehealth services, which is a form of distance therapy offered by a mental health provider directly via online mechanisms, should not be confused with other online programs and virtual applications that support students with the goal of general wellbeing or stress management (see Chapter 3). The most popular
services were mental health screening online (27.5 percent) and telephone counseling (7.6 percent) (LeViness et al., 2019). While existing research focuses on synchronous delivery through video-conference platforms, which best simulate a face-to-face session, there is less information on new models of delivery such as text support or the use of third-party psychoeducational and self-help tools. (Higher Education Mental Health Alliance, 2014).
The COVID-19 pandemic has rapidly transformed both the treatment of mental health problems as well as the promotion of mental health, through the use of telehealth services. Prior to the pandemic, the American Psychiatric Association reported that most of its member clinicians did not use telehealth; however, as of June 2020, 85 percent said that they were serving more than three-quarters of their patients through telehealth (American Psychological Association, 2020). Telehealth services have also permitted students from many campuses to engage in group psychotherapy during COVID-19, mitigating mental health consequences of forced relocation, social distancing, and isolation. Similarly, according to a 2019 survey report from the Association of University and College Counseling Center Directors, greater than 50 percent of college counseling center directors said their center used no form of telehealth, and only 3.4 percent of the directors surveyed said they offered counseling via videoconferencing (LeViness et al., 2019). With COVID-19, the rapid expansion of these services has been seen on and off campus. With this expansion comes the need to understand the challenges and opportunities associated with these services; telehealth offers the safest opportunity in terms of COVID-19 risks for seeking health care in this moment and during the foreseeable future and will likely continue to expand and transform health care delivery. As a recent report notes, given that telehealth will likely continue to be a health service delivery mechanism beyond the pandemic, “it will be important for universities to identify and make available the best telehealth resources and incorporate them into [the] college or university’s health strategy” (Steve Fund, 2020). Under normal circumstances, telehealth services can be a method to support students who attend a college or university virtually, who are off-campus for a semester abroad or while conducting research, or for those who have life circumstances (e.g., conflicting schedules, transportation issues, and disability) that preclude them from visiting in-person services (Higher Education Mental Health Alliance, 2019). However, while this mode of delivery may increase access for some students, other groups of services may not provide the same benefits as in-person sessions, posing significant issues of equity. For example, students who have challenges accessing the internet or lack adequate devices may not be able to benefit from these services. Other students may lack a private space for accessing these services, either on or off campus. Access to telehealth services is a significant challenge. Opportunities to increase access may include providing students with a private space and access to high speed internet to support telehealth sessions. There may also be students who choose one delivery method over another because of personal preference alone. Finally, it is
important to note that many tele-mental-health companies employ a wide variety of “rule-outs” when determining who is appropriate for their services (e.g., drug abuse, suicidality, serious mental illness) that will limit access for many students.
In the wake of COVID-19, access to distance and tele-services has allowed many students to remain in touch with their on-campus counselors. This is a noteworthy shift, as one of the major issues that had limited students from getting teletherapy with an existing provider was the limitation of providing services across state or international boundaries, due to restrictions imposed by licensing boards and legislation. After the pandemic began, many states began to grant waivers to health care providers to provide tele-services. Penn State University and the University of Texas at Austin compiled and updated an omnibus guide on the changing rules/laws in each state related to providing mental health services via telehealth/telemedicine across state lines (CHMC, 2020).5 The future of the laws and regulations remains uncertain at the time of publication of this report. For more information about research questions related to telehealth, see Chapter 6.
While there is evidence that the provision of mental health services via telehealth has expanded greatly during the pandemic, the relative effectiveness of these services has not yet been well documented. Several studies of the application of telehealth services on campus prior to the pandemic have indicated that this may be an effective mechanism for reaching more students. Nobleza et al. (2018), for example, examined the telehealth experience of students in a college counseling center prior to the pandemic. Participants were health professional students who utilized at least one telehealth visit between November 2015 and April 2017 and were surveyed to assess the impact of telehealth on access, experience, effectiveness, and impact on therapeutic alliance. The majority of the 53.7 percent of students who responded indicated that telehealth was convenient (94.4 percent), time-saving (94.4 percent), and helped them to feel better (83.3 percent). The authors noted that “eighty-one percent reported telehealth as being as good, nearly as good, or no different than meeting in person… telehealth is a viable option for college counseling centers and is experienced as convenient, time-saving, and effective with little negative impact on therapeutic alliance.” (King et al., 2019).
Similarly, King et al. (2019) studied the effectiveness of a well-validated tool, termed the brief alcohol screening and intervention for college students (BASICS) when conducted face-to-face or through a videoconferencing system. The authors found that that the intervention “significantly reduced alcohol consumption and related problems regardless of condition.” King et al. (2019) also noted that the study suggested that “telehealth services should be further implemented and the BASICS intervention can be effectively delivered via telehealth for college students.”
___________________
5 The second version expanded the range of health care professionals, and it now includes marriage and family therapists, physicians, professional counselors, psychologists, and social workers, as well as advanced practice nurses, physician assistants, and physical therapists.
Despite initial positive evidence that telehealth may increase access to both mental health treatment and wellness services, further study with the advent of COVID-19 and the acceleration of these services is needed. In addition to understanding challenges associated with accessing services, research should examine the effectiveness of telehealth compared to standard in-person approaches, especially for specific populations.
















