
6
Health Systems
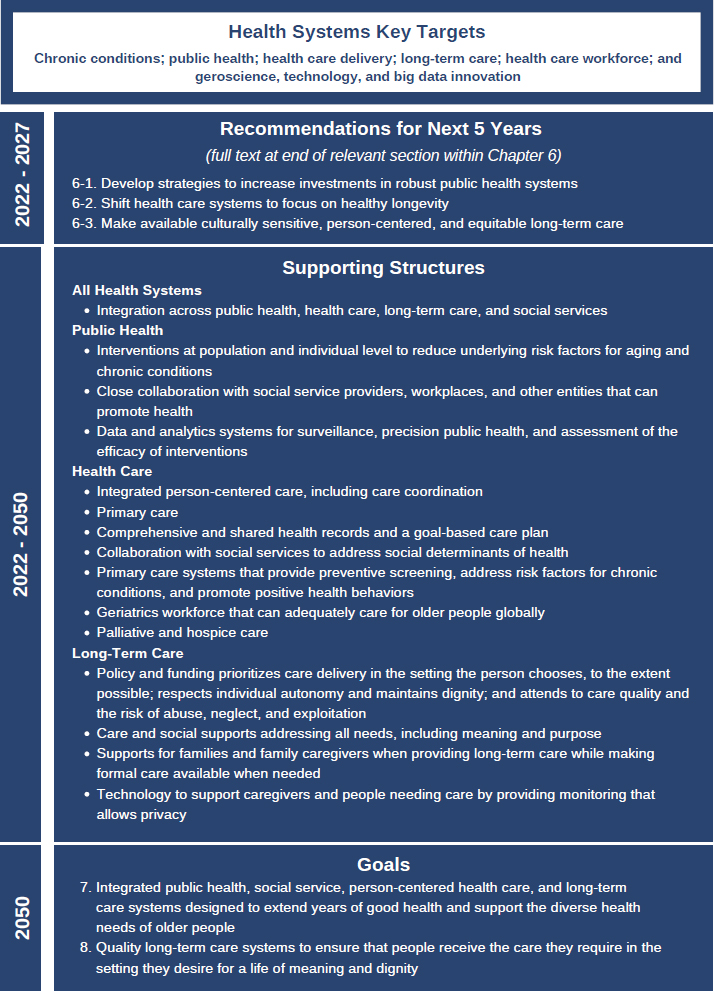
Before societies can reap the many benefits of healthy longevity discussed throughout this report, it will be necessary to maximize the percentage of life in good health. Accomplishing this will require a life-course perspective to minimize adverse exposures and promote health from the prenatal stage through the end of life. Prevention at the individual and societal levels will need to receive greater emphasis to decrease the burden of age-related chronic conditions.1 The goals for health systems by 2050, key targets to catalyze change, and examples of structures needed to achieve the goals are shown in Figure 6-1.
As discussed throughout the rest of this chapter, no country has perfected any one of the three main health systems—public health, health care, and long-term care—although some countries do better than others. Few countries are well positioned to provide the prevention and care required to decrease the prevalence of chronic conditions and associated symptom burden and functional decline. Public health is chronically underfunded and lacks influence in other government departments that influence health, limiting its ability to improve population health. Health care systems have focused on diagnosing and treating chronic conditions one disease at a time, with entrenched policies that result in far more spending on in-patient care for advanced chronic conditions than on prevention. Long-term care is also underfunded and inadequately integrated with health and social care in many countries. Often, long-term care is not available where the person needing care wants to live.
___________________
1 As used in this report, the term “chronic conditions” encompasses distinct chronic diseases, multimorbidity, and geriatric syndromes (frailty, sarcopenia, polypharmacy, cognitive decline, disability, and falls).
This chapter provides background information on the health of older adults today, global health spending patterns, and the value of good health. It then describes key targets needed achieve healthy longevity, including chronic conditions, the roles of public health and integrated person-centered primary care in
providing prevention and management of chronic conditions, the long-term care system needed to support people who lose functional ability, and the health care workforce. The final key target is innovation through geroscience, technology, and big data to prevent and manage chronic conditions and maintain people’s independence in the face of declining cognitive and physical functioning. The chapter concludes with an overview of related international efforts calling for similar actions, metrics that stakeholders can use to gauge progress toward achieving healthy longevity, and areas needing more research.
As with earlier chapters, commissioners selected key targets for action beginning in 2022 from the many factors affecting healthy longevity. Commissioners prioritized content based on actionability, impact on people across the life course, equity, and importance to (1) improving healthy longevity in the long term and (2) tackling needs of older people in the near term. They also identified actions to generate the multisector, all-of-society transformation essential to building healthy longevity for all. The commissioners chose not to focus on aspects of health systems that are on the agenda of other major international efforts, such as primary care and health care access and affordability, although they recognize their importance. The key targets that were selected will, in some instances, require major financial commitments. In other cases, such as emphasizing geriatric-sensitive care and delivering integrated, person-centered care, the investments should be feasible.
Given the diversity of political, social, and economic contexts across countries and communities, the commissioners chose broad recommendations that leave room for actors with the ability to improve healthy longevity to determine the right pathway and funding strategies, which will require trade-offs to move forward. In other instances, key targets would shift emphasis within existing structures, requiring political will and culture change.
VISION FOR HEALTH AND HEALTH SYSTEMS
The focus of interventions across health and social service systems changes from when people have good health and function to when people have advanced illness and functional loss. For those in good health and those with well-managed chronic conditions and minimal functional impairment, public health and health care systems focus on prevention, reversal, or management of chronic conditions, screening, and health promotion. Social and physical environments for this subpopulation should facilitate engagement and activity. For those with advanced illness and significant functional loss, health care focuses on management of advanced chronic conditions while long-term care focuses on compensating for loss of function and promoting engagement in a life with meaning and purpose. For this subpopulation, social and physical environments should remove barriers to participation and compensate for functional loss.
MEASURING HEALTH
To fully understand healthy longevity, data that directly measure poor health and its impacts on people, including functioning and symptom burden, will be critical. Direct measurement of disability in population-based studies and clinical care involves the individual’s self-report of difficulty or dependency in tasks of mobility, activities of daily living (ADLs), independent activities of daily living, and objective performance-based measurement of various dimensions of functioning (e.g., walking speed for physical function, and memory and recall for cognitive function). Most disability results from biological aging, alone or in concert with chronic diseases, cognitive decline, and frailty. Symptoms such as pain, shortness of breath, and fatigue can sometimes affect function, but they can also affect quality of life without major functional impairment; they require direct measurement as well. The degree to which symptoms are included in the measures described below is unclear.
Mortality is a primary outcome measure for health, but it becomes less relevant as people move closer to inevitable death. While death that occurs because a condition is undiagnosed or poorly managed is important, it is captured within the World Health Organization’s (WHO’s) Global Burden of Disease estimates only for people under age 70.2 Similarly, the United Nations (UN) Sustainable Development Goals (SDGs) use the same cutoff of age 70 for premature mortality (Ebrahim et al., 2020).
Assessing the health burden of chronic disease currently relies on indirect measures. One measure is the presence of a specified number of chronic conditions. Although the presence of chronic conditions is related to disability and mortality over time, people can live with well-controlled chronic conditions for long periods with minimal symptoms or other impacts on life, so it is an imperfect measure of the burden of illness. Since the early 1990s, WHO has sought to measure the burden of poor health using two related measures: years of healthy life lost due to disability (YLDs) and disability-adjusted life years (DALYs). These measures are critical to WHO’s ongoing effort to “define, measure and numerically value time lived in non-fatal health states.” The numeric values are calculated using disability weights between 0, a state equal to death, and 1, perfect health. Disability weights are used to measure YLDs, which are combined with years lost to premature death (a figure that excludes people over age 70) to calculate DALYs (WHO, 2013).
___________________
2 While death due to chronic conditions is common, it is important to understand when death results from undiagnosed or poorly managed conditions, described as “premature” by WHO. But the WHO Global Health Observatory measure of premature death is limited to deaths that occur before age 70, and therefore it misses those that could have been delayed among people over age 70. “The upper limit of 70 years was chosen for two reasons: (a) to identify an age range in which these chronic disease deaths can truly be considered premature deaths in almost all regions of the world.... in all regions except the African Region, the average expected age at death for 30 year olds already exceeds 70 years; (b) estimation of cause-specific death rates becomes increasingly uncertain at older ages because of increasing proportions of deaths coded to ill-defined causes, increasing levels of co-morbidity, and increasing rates of age mis-statement in mortality and population data sources” (WHO, 2022b).
The most recent iteration of the Global Burden of Disease study assigned disability weights based on household survey responses in five countries, plus a web survey. Although older adults have the greatest levels of disease and disability, 75 percent of those whose responses were used to determine the disability weights were under age 50, while only 5 percent of respondents were aged 70 and older (Salomon et al., 2012). In the meantime, this report and others must rely on indirect and imperfect quantification through YLDs and DALYs.
The Health of Older People
One myth about older people as a group is that most are in poor health and frail. The reality is that the health of older adults is heterogeneous, although at a population level it declines with age. All of the statistics below have limitations. The presence of a chronic condition, need for assistance with ADLs, and healthy/unhealthy health status does not mean that a person is not thriving. When the environment is supportive of people with disabilities and when the health care system effectively manages chronic conditions, people can still thrive and live lives of meaning and purpose. Moreover, data capture is inconsistent across countries, so reported numbers may not be comparable. Finally, researchers select the population of interest. In aging research, different cutoff ages are selected, as indicated below for the study by Garin and colleagues (2016) on chronic conditions (50 and older), for ADLs in Organisation for Economic Co-operation and Development (OECD) countries (65 and older), and in the publication by Rofman and Apella (2020) (60 and older). Harmonizing these differences is beyond the scope of this report.
One often reported measure of health is whether a person has two or more chronic conditions. One study revealed wide variation in the percentage of people over age 50 with more than one chronic condition: China (45 percent), Ghana (48 percent), India (58 percent), Mexico (64 percent), Russia (72 percent), and South Africa (63 percent) (Garin et al., 2016).3
Functional capacity, as measured by the need for long-term care, services, and supports, is also heterogeneous. Thirty percent of people aged 65 and older in OECD countries need assistance with ADLs (OECD, 2020). The following are percentages of people aged 60 and over reporting one or more ADL limitations (Rofman and Apella, 2020):
- Brazil 2013: 15.45 percent
- Mexico 2001: 14.57 percent; 2012: 21.19 percent
- Chile 2013: 13.13 percent
- Costa Rica 2009: 32.5 percent
- China 2011: 12.15 percent
- United States 2002: 26.33 percent; 2012: 22.1 percent
___________________
3 The conditions included in studies of the prevalence of chronic conditions are not standardized; therefore, studies may not be directly comparable.
The U.S. government estimates that one in three people aged 65 and older will never need long-term care, 20 percent will need it for more than 5 years, and the remainder will need it for less than 5 years (ACL, 2022).
Across countries, regardless of income level, the number of unhealthy years of life4 is increasing, with people in high-income countries having the most years in poor health (see Figure 6-2).
Health Spending
As discussed below, chronic conditions are the primary cause of illness, disability, and death globally. Therefore, the majority of health spending is for preventing, diagnosing, and providing care for chronic conditions.
Between 2000 and 2019, health spending per capita climbed 134 percent (Murphy and Topel, 2006). During this same period, health spending as a percentage of gross domestic product (GDP) increased globally from 8.63 to 9.845 percent, a 14.08 percent increase (Ohnsorge and Yu, 2021). The United States spends 18 percent of GDP on health.
A 2019 analysis calculated global health care spending to be USD8 trillion in 2016 and predicted it to climb to USD15 trillion in 2050. The authors describe
___________________
4 Staff calculated unhealthy life expectancy using data from WHO by subtracting healthy life expectancy at age 60 from life expectancy at age 60. Healthy life expectancy is defined “as average number of years that a person can expect to live in ‘“full health’” by taking into account years lived in less than full health due to disease and/or injury.” The calculation includes YLDs.
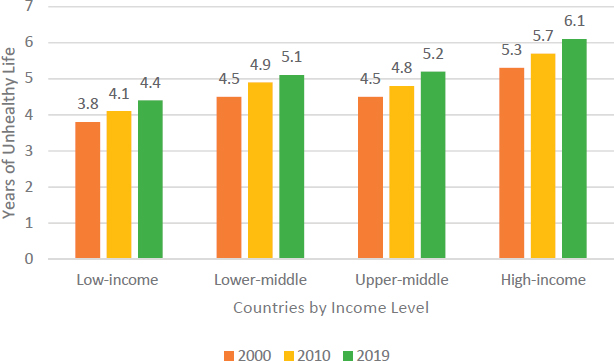
NOTES: Health measurement has been refined since 2000, and self-reported responses to the same questions have changed over time. Measures of health may therefore have deteriorated subjectively but not objectively.
SOURCE: Staff calculation using World Health Organization data (WHO, 2019).
extreme inequity between high- and low-income countries. The ratio of health care spending in high-income countries to that in low-income countries was 130 to 2 in 2016; the ratio is predicted to remain the same in 2050 (Chang et al., 2019). The limited government spending on health in low-income countries shifts the burden of paying for care to the individual and family; in these countries, 40 percent of health expenditures are out of pocket, limiting access to health care. Globally, per capita out-of-pocket expenditures rose by more than 100 percent between 2000 and 2018 (World Bank, 2021).
One measure of whether a country is tending to the social determinants of health is the relationship between health spending and social spending. Higher social spending is correlated with better health outcomes, while higher health care spending is negatively correlated with health outcomes (Bradley et al., 2016; Dutton et al., 2018). Among OECD countries, the United States is an outlier: its health care spending is far higher than that of other countries, while its social spending is near the middle. If U.S. Social Security retirement payments were excluded from the social spending calculation, the United States would be closer to the bottom of OECD countries in social spending.
Alignment with Other Efforts
As the commissioners conceptualized this chapter, they started from the baseline of the World Report on Ageing and Health and the WHO Decade of Healthy Ageing, which is scheduled to last through 2030 (WHO, 2020a). This chapter builds on those efforts to look beyond 2030. This chapter aligns with UN SDG 3, Good Health and Well-being. All of the targets within SDG 3 would promote healthy longevity (UN DESA, 2022).
Finding 6-1: The number of years in poor health has increased globally since 2000 along with life expectancy.
Finding 6-2: Health has gross domestic product value and intangible value. When economists have developed methods to assign numeric value to good health, they have found that people assign enormous value to good health.
Finding 6-3: Higher social spending is associated with better health outcomes; higher health spending is associated with worse health outcomes. U.S. spending, including dramatically higher spending on health care than on social programs, is out of balance compared with that of other Organisation for Economic Co-operation and Development countries.
KEY TARGET: CHRONIC CONDITIONS
Biological Aging and Risk Factors for Chronic Conditions
Chronic conditions are often portrayed as discrete pathologies, but researchers have begun to uncover the biological processes of aging and their relationships to chronic conditions. When aging processes are combined with unfavorable genetics, behaviors, and social and physical environments, and even with infectious diseases,5 they can increase people’s vulnerability to chronic conditions (Kennedy et al., 2014; Sierra, 2016). Aging processes can also lead to declines in capacity unrelated to the presence or absence of disease, such as geriatric syndromes, including delirium, falls, frailty, syncope, and urinary incontinence (Inouye et al., 2007).
The inevitability of chronic conditions and functional decline in older ages has been portrayed as fact. It is becoming increasingly evident, however, that the trajectory of health as people age may improve with a healthy social and physical environment and individual decisions about diet, physical activity, and substance use (Sierra, 2016). As discussed in Chapters 4 and 5, governments, employers, and other actors can influence health outcomes population-wide by reducing adverse social determinants of health—whether social factors, such as ageism, or physical environment factors, such as air pollution.
Four health behaviors (tobacco and unhealthy alcohol consumption, unhealthy diet, and physical inactivity) are major contributors to the development of the four conditions responsible for 80 percent of chronic disease deaths (“cardiovascular disease, cancer, chronic obstructive pulmonary disease, and diabetes”) (Hunter and Reddy, 2013, p. 1336). From a different perspective, Halpin and colleagues (2010) describe physical inactivity, unhealthy diet, and obesity as “a lethal combination” of risk factors, increasing the risk of cardiovascular disease, diabetes mellitus, cancers, metabolic syndrome, and osteoarthritis (p. 126). Research suggests that behavior change, such as improved sleep and midlife physical activity, may even reduce the risk of developing a chronic condition for which a person has a genetic predisposition, such as the apolipoprotein e4 gene, which increases the risk of developing Alzheimer’s disease (Mendelsohn and Larrick, 2013; Stephen et al., 2017).
The Global Impact of Chronic Conditions
Globally, chronic conditions are the greatest cause of death and YLDs (Lozano et al., 2012). Even in lower-income countries, which tend to have younger populations and a higher infectious disease burden relative to high-income countries, chronic conditions are the leading cause of death and disability. The percentage
___________________
5 The traditional distinction between communicable or infectious diseases and chronic or noncommunicable conditions has been discredited by research that links infectious diseases, especially viruses, to chronic conditions.
of YLDs attributed to chronic conditions in low-income countries is lower than the global average but still is more than 75 percent (IHME, 2019). It is therefore important to address chronic conditions in countries of all income levels.
Several factors in combination have created this growing global challenge. The increase in the number of people living with and dying from chronic conditions is a side effect of successfully increasing longevity globally in the past 100 years: more older people are living, and older people are more likely to develop chronic conditions (Lozano et al., 2012).
Economic and Fiscal Impacts of Chronic Conditions
Beyond the adverse impacts on people’s health as described earlier in this chapter, chronic conditions impose an enormous economic burden on individuals, families, and society, including the rising health care costs discussed above. Bloom and colleagues (2012) used three approaches to estimate the costs of chronic conditions: estimated direct and indirect costs, lost output, and the economic burden of life lost. Box 6-1 defines these approaches and presents the authors’ estimates of the cost burden of chronic conditions associated with each. The authors conclude that the impacts and costs are dauntingly large, regardless of approach (Bloom et al., 2012).
Finding 6-4: Health is malleable through efforts addressing modifiable factors that accelerate the aging process and contribute to earlier onset of chronic conditions.
Finding 6-5: Chronic conditions are responsible for 80 percent of deaths and years of healthy life lost due to disability globally, including in low-income countries, where the median age is lower than in high-income countries.
Finding 6-6: The costs associated with chronic conditions, including the costs of care, lost output, and the burden of lost life globally, are extremely high. Lost output due to cancer, cardiovascular disease, chronic respiratory diseases, diabetes, and mental health during 2011–2030 is estimated at USD47 trillion, and the burden of lost life annually is estimated to range from USD22.8 trillion in 2010 to USD43.3 trillion in 2030 (Bloom et al., 2012, p. 35).
Conclusion 6-1: The importance of slowing aging and the onset of chronic conditions and thereby prolonging good health supports the need for public health and health care systems that are preventive, proactive, and predictive, and that target shared risk factors for accelerated biological aging and onset of chronic conditions.
KEY TARGET: PUBLIC HEALTH
Public health systems6 are the single most powerful structure for tackling chronic conditions and equitably improving population health. Public health uses population-wide surveillance and interventions (e.g., policy, community-based programs, messaging about healthy behavior, screening, immunization, contact tracing, and inspection) to promote health across populations. According to DeSalvo and colleagues (2017, p. 3), “Public health is what we do as a society to ensure the conditions in which everyone can be healthy. It minimizes threats to health that can be averted or lessened only through collective actions aimed at the community.” Creating healthy longevity will require a “new public health” that works to prevent chronic conditions at the societal, community, and individual levels (Halpin et al., 2010).7
___________________
6 Public health systems have different functions in different countries. In this report, the definition of public health is limited to population-wide efforts and some direct contact with individuals by public health workers (e.g., community screening, vaccination clinics).
7 WHO essential public health operations to deliver public health services are (1) surveillance, (2) monitoring, (3) health protection, (4) health promotion, (5) disease prevention, (6) governance, (7) public health workforce, (8) funding, (9) communication, and (10) research (WHO, 2022c).
The Health Impact Pyramid Framework
The health impact pyramid depicted in Figure 6-3 can inform investments in prevention by identifying those interventions having the greatest population-wide impact and requiring the least individual effort (at the bottom) and those having the least population-wide impact and requiring the most individual effort (at the top) (CDC, 2022). The bottom two tiers of the pyramid, discussed below, comprise public health interventions targeted to populations. The top three tiers, which comprise efforts to improve population health one person at a time, are addressed in the next section, on the role of person-centered integrated health care in preventing and managing chronic conditions. Although the pyramid was developed in the United States, a 2019 review article emphasizes the need for low- and middle-income countries to shift away from a focus on identifying individual risk factors and screening to a focus on the interventions at the bottom of the pyramid (Miranda et al., 2019).
Socioeconomic Factors
Socioeconomic factors form the base of the health impact pyramid because they are foundational to health and are delivered at the population level (see Chapters 4 and 5). Public health organizations might be expected to use surveillance to identify the social, environmental, and financial threats to health; geographic areas at risk; and subgroups at high risk. But public health agencies, though within larger governmental structures, may have little or no access to or
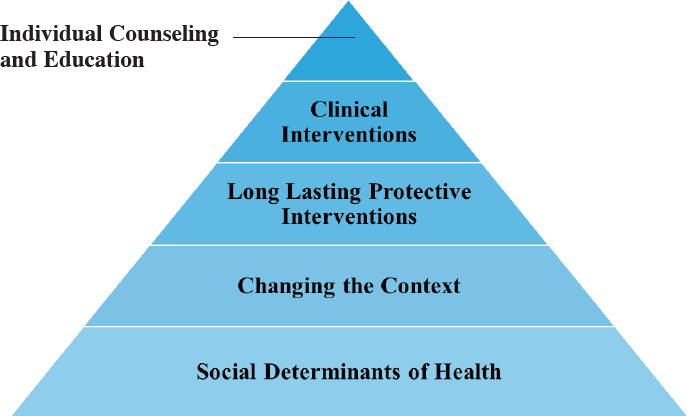
SOURCE: Adapted from CDC, 2022.
control over the government entities that address socioeconomic factors. They must therefore collaborate across government ministries, departments, and agencies. This observation is consistent with recommendations made by WHO in the Conceptual Framework for Action on the Social Determinants of Health, which states that public health systems will need to be involved in the efforts of other government entities, such as those that provide social services, to help target interventions with significant public health impacts (WHO, 2010a). One U.S.-based research team has recommended using a chief health strategist to connect local public health departments to other stakeholders to address adverse social determinants of health (DeSalvo et al., 2017).
Finding 6-7: Addressing social and economic risk factors is a necessary part of a public health strategy for preventing chronic conditions. To address social and economic risk factors successfully will require collaboration between public health and other government agencies and private-sector stakeholders that can influence health behaviors, such as unions and employers.
Changing the Context
Interventions at the next level of the health impact pyramid change the context in which health behaviors occur. They can include laws, policies, and regulations; public messaging about how to improve health (e.g., tobacco cessation, quality nutrition, and physical activity); and behavioral economics interventions (e.g., taxes on tobacco products, alcohol, and sugary drinks). The aim of changing the context is to make the default decision the healthy one.
Changing the context requires multipronged strategies. For example, a combination of urban design that creates safe bicycle or walking lanes, employer incentives to walk or bicycle to work, and public messaging about the importance of physical activity could change individuals’ default decisions about transportation, leading to improvements in the environment and physical activity levels. Chile, for instance, recently developed a multifaceted approach to promote healthy eating habits through food labeling and advertising policies. The Chilean law mandated front-of-package warning labels for products high in saturated fat, sugar, and sodium while also restricting positive marketing of these products and banning their sale in schools. Although researchers were unable to determine whether the labeling or the advertising policy had a greater effect on sales, they concluded that, in combination, the policies discouraged and reduced consumption (Taillie et al., 2021).
For public health to be inclusive of older people, the context must be relevant to them, which may require different messaging and methods. Educating people about the significant impact of daily health behaviors on cognitive function and giving them information about the impacts of specific behaviors is an example of an intervention that is relevant to older people. Examples of study results that
could influence older people’s choices include a study suggesting that people over age 45 with a higher daily intake of fruits and vegetables had better cognitive function (Jiang et al., 2017). Another study suggests that older people who engage in vigorous physical activity at least once a week may be half as likely as those who are inactive to develop cognitive impairment and 30 percent less likely to need assistance with daily living (Jiang et al., 2017). Public health messaging to older people could combine education about the benefits of a healthy diet and physical activity with information about how urban dwellers can access fresh fruits and vegetables, such as a program in New York City, whereby older people can purchase inexpensive bags of fresh produce at easily accessible locations (West Side Rag, 2021).
Across all ages, efforts to change the context through targeted messaging and methods are better at effecting behavior change than approaches that appear to blame the victims of social determinants of health for the behaviors they drive (Crawford, 1977). More recent publications also express concern about the fine line between health education and blame (Brown, 2018).
Finding 6-8: Multimodal interventions that change the context for health choices, making the default choice the healthy choice, show promise for decreasing the risk of chronic conditions and improving health by changing individual health behaviors.
Investment in and Return on Investment from Public Health Prevention
Despite its importance, public health is chronically underfunded in countries around the world. Even as the threat of increasing numbers of older people with chronic conditions and more years of poor health has grown, public health spending patterns have largely remained unchanged in higher-income countries. Among 32 OECD countries in 2015, none allocated more than 6 percent of total health expenditures to preventive care. In 2018, average spending across these countries was 2.4 percent for “any measure that aims to avoid or reduce the number or the severity of injuries and diseases, their sequelae and complications” (Kamal and Hudman, 2020).
Researchers have been evaluating the return on investment of structural public health interventions, as distinct from individually focused interventions, especially at the time governments were cutting programs following the global financial crisis from 2008 to 2015. A systematic review of 52 studies evaluating the return on investment or cost/benefit ratio of public health interventions in high-income countries found that the return on investment was 14.3 to 1, and the cost/benefit ratio was 8.3. The largest benefits were seen in studies of national public health initiatives, where the median return on investment was 27.2 to 1, and the cost/benefit ratio was 17.5 (Masters et al., 2017). Many of the public health interventions with positive cost-benefit ratios or documented
return on investment included in the review focused on structural changes, including speed cameras and speed zones, water fluoridation, preschool and school age education programs, bicycle and pedestrian trails, road safety campaigns, anti-stigma marketing campaigns, sugar sweetened beverage tax, and lead paint control. Similarly, the WHO Case for Investing in Public Health reports on cost-effective public health interventions including tobacco and alcohol legislation, salt reduction, violence reduction, walking and cycling promotion, green spaces, safe transportation and housing, and healthy employment (WHO, 2014). A U.S.-based evidence review highlighted evidence supporting the cost effectiveness of home meal delivery, meal planning, and improving access to healthy food; transportation to health care appointments; and home modifications for people with functional limitations (Tsega et al., 2019).
The commission anticipates that resource constraints will make rebalancing spending between public health and health care spending necessary in all countries, but especially in low- and middle-income countries with the greatest need for structures in both areas, and the most limited resources. Investing in structures to address social determinants of health, such as the examples shown in Boxes 6-2 and 6-3, has the potential to mitigate rapidly rising health care costs. The first, Box 6-2, describes changes made in Costa Rica in the 1940s that have resulted in a higher life expectancy than in countries with similar income levels.
The second, Box 6-3, describes structural factors that change the context of tobacco use identified in the WHO Framework Convention on Tobacco Control.
Conclusion 6-2: Changing the trajectory of increasing numbers of people with chronic conditions will require a change in how governments balance public health and health care spending. Strategies for making significant changes in spending allocations are most effective when they are multimodal, in contrast to attempts to achieve significant change through a one-dimensional intervention, such as changing methods for provider reimbursement.
Public Health Data and Analysis for Prevention of Chronic Conditions
Public health entities rely on epidemiological data and analysis to conduct surveillance on public health threats and improvement monitoring. Beyond traditional analytic methods, public health is increasingly benefiting from enhanced computational capabilities and data availability, as the COVID-19 pandemic has demonstrated. Globally, however, and especially in low-income countries, data are inadequate for effective surveillance, especially at the subpopulation level. The absence of these data makes it difficult to monitor progress toward health-related SDGs or toward healthy longevity at the national and subnational levels.
According to WHO, 68 percent of countries have good capacity for surveillance of public health threats, 40 percent of deaths are unregistered globally, fewer than 50 percent of countries are able to monitor care quality systematically, and 60 percent have good capacity to track the progress and performance of the health sector and use data in policy and planning (WHO, 2020b).
Disaggregated data will be particularly important in understanding the risks of subpopulations and targeting interventions to address those risks, as demonstrated by one study that used modeling to evaluate the effects of different strategies for primary prevention of cardiovascular disease. The study found that a public health approach focusing primary prevention efforts for cardiovascular disease on subpopulations with significant risk factors would be more cost-effective and save more lives than broad population-wide screening (Kypridemos et al., 2016). Capturing health data disaggregated by gender and age bands (e.g., exact age or decade age bands, not 0–14, 15–64, and 65+) will be necessary at the national and community levels to understand the most important contributors to health and healthy longevity. Capturing data on social determinants of health globally is critically important and more difficult relative to data on age and gender, requiring data collection methods not currently in use. The COVID-19 pandemic has illustrated the need for data that allow stratification, because stratified analysis of outcomes has highlighted disparities in outcomes across age, socioeconomic status, and race.
While current data collection efforts rely on methods that are costly and time-consuming, new technologies have the potential to collect relevant public health data using passive collection approaches. One study, for example, suggests the feasibility of using deidentified mobile phone data to understand the spread of cholera in Haiti and track the movement of people during an infectious disease outbreak (Bengtsson et al., 2015). Billions of people globally have smartphones or wearable devices with tracking capabilities, and with proper privacy protection, these data could be used, for example, to evaluate physical activity and walking speed down to the neighborhood level.
With new forms of data capture and analytics, precision public health is being proposed as an approach to “provid[e] the right intervention to the right population at the right time” (Khoury et al., 2016, p. 398). This approach will be important to achieving the vision for health laid out at the beginning of this chapter. Precision public health takes advantage of new techniques for surveillance of diseases, exposures to toxins or communicable diseases, health behaviors, and overall population health. Proponents emphasize that in contrast to precision medicine, which may be available only to people with higher incomes, precision public health is designed to use data to target services and interventions to those with the greatest need (Horton, 2018). Future use of this approach is, however, contingent on privacy protection and transparency of models, as discussed later in this chapter.
The current capabilities of precision public health and advanced analytics are still limited: classic statistical methods perform as well as artificial intelligence
(AI) models in identifying disparities (Khoury et al., 2020). AI is not yet in widespread use, so it remains unproven. But the commission predicts that significant change in data capture and analysis methods will take place in the coming decades, with AI becoming a powerful tool for segmenting populations and delivering targeted public health interventions where they will have the most impact.
Levers for Change
Public health organizations face two barriers to shifting the emphasis toward aging and chronic conditions. First, they have limited ability to influence other government agencies with authority for addressing social determinants of health, including availability of social services, clean air and water, safe housing, and walkable communities, among others. Public health also needs to be involved in decisions about health care and long-term care, and the three systems need to work in concert on prevention efforts, coordinating across the full health impact pyramid—something that is not yet a reality in most places. Public health messaging, about controlling hypertension, for example, lacks value if a person with hypertension cannot get quality, affordable care to manage the condition. Public health will need a seat at the table to ensure that there is a concerted effort across governments to respond to epidemiological evidence about what works and where resources are needed. Second, public health departments around the globe lack resources. If countries continue to allocate a third or more of their health expenditures to in-patient care, at least some of which is avoidable, public health will remain underfunded, and people, especially older people, will face avoidable illness, functional impairment, and early death. To make these changes, political will and reallocation of resources will be needed, but given the diversity of interests globally, the commission’s roadmap cannot make recommendations on how to achieve the changes.
Public health, in conjunction with biomedical research, has had tremendous successes during the COVID-19 pandemic. Notably, vaccine development and distribution was more effective and expeditious than most “moonshot” efforts, such as cancer moonshots in the United States and Europe. Harnessing that success could potentially overcome the historical inability to shift resources from health care to prevention.
Metrics
The UN SDGs related to public health (aside from specific disease focus) include the following:
- 3.4.1: Mortality from cardiovascular disease, cancer, diabetes or chronic respiratory disease, including adults aged ≥70 years
- 3.4.2: Mortality rate from suicide, by age and sex across the life course
- 3.a.1: Age-standardized prevalence of current tobacco use among persons aged 15 years and older
- 3.b.1: Proportion of the target population covered by all vaccines included in their national program
The metrics for the WHO Best Buys for public health interventions include
- tobacco use,
- physical activity,
- harmful substance use, and
- healthy diet.
(Note that the disease management best buys are included in the health care delivery section.)
Data Needs and Research Questions
The commission emphasized the need for more granular data about health than are currently available. Specifically, longitudinal data collection on health status, including physical and cognitive functioning, stratified in narrow (e.g., 10-year) age bands and by sex, will be necessary to understand the impacts of public health interventions and progress toward healthy longevity. The commission also emphasized the need to collect data on social determinants of health at the individual level. One potential source of such data is the United Nations’ Titchfield Group on Ageing-related statistics and Age-disaggregated Data (UN Statistics Division, 2021).
An important emphasis for research methods is the need to include older people in research design, not just as research subjects—for example, as coinvestigators.
One structural question about public health is how to shift health systems away from reactive, disease-focused health care toward preventive and proactive models. Despite widespread agreement on public health targets and the need to reallocate funding, this shift has not occurred. Answering this question will require cross-disciplinary expertise in systems change theory and complex systems dynamics, policy, and public health.
Another research question is how to effect behavior change across populations. This section has described how to change the context, but even with a context that supports healthy behaviors, many people still make unhealthy choices. The success of public health interventions is dependent on successful behavior change strategies at the individual level.
Recommendation 6-1: To achieve the goal of the best possible health for older people, governments, over the next 5 years, should develop strategies to increase investments in robust public health systems that build
and lead collective actions for promoting health at the population level and across the life course.
- Investments in public health systems may require governments to rebalance investments in health care and public health.
- Public policies should create incentives for individuals, employers, and communities to engage in prevention and wellness activities.
- All countries should establish 5-year targets for preventive health and measure progress toward those targets.
KEY TARGET: HEALTH CARE DELIVERY
The health care delivery system has multiple roles to play in promoting healthy longevity and reducing the burden of chronic conditions and their impacts at the individual and societal levels. Prevention roles for the health system include individual-level screening, preventive measures (e.g., vaccinations), long-lasting interventions (the third level of the health impact pyramid), clinical interventions (the fourth level), and education and counseling (the fifth level). Along with prevention, the most important roles of a health care system in caring for people of all ages are to identify, diagnose, and treat those at highest risk of developing disease (e.g., managing hypertension as a risk factor for cardiovascular disease).
If a disease progresses, the health care system should optimally manage the condition to avoid the onset of new complications, avoid acute exacerbations, minimize symptom burden, and slow the loss of function, in addition to addressing any acute care needs that arise. Even though the health impact pyramid is focused on prevention, its levels apply to the management of chronic conditions and long-term care across all stages of health. Every aspect of care should include a focus on the person’s social needs, whether access to clean water or refrigeration for medications, the ability to pay for medications, or avoidance of unsafe conditions in the home. Addressing social needs will contribute to preventing or slowing disease progression and providing the structures needed to maximize functional capacity in the face of decline (e.g., through the use of a supportive physical environment). Similarly, contextual factors that support prevention (e.g., enabling access to fresh fruits and vegetables) contribute to management of advancing chronic conditions.
The commission recognizes the importance of accessible and affordable quality health care as a critical component of healthy longevity. This section focuses on the delivery of integrated person-centered care, including geriatric care and primary care, that supports the health of older people. If actualized, this care would be of higher quality than that provided by current systems. The issue of accessible and affordable health care is left to other reports and publications, such as the World Report on Ageing and Health (WHO, 2015b) and the UN SDGs, and is not addressed further here.
Current health care systems that were designed to meet acute care needs in the mid-20th century do a poor job of preventing and managing chronic conditions, especially multiple chronic conditions and geriatric syndromes. Within most systems around the globe, health care systems and providers are paid for procedures and visits, not for health outcomes. Specialty care further entrenches a disease-centered, not person-centered, approach to care. Primary care in much of the world is underfunded, and providers are burdened with many obligations, which can make it difficult or even impossible to provide care for the whole person. These challenges affect people of all ages.
More than a decade ago, an editorial in the Journal of the American Geriatrics Society described the poor-quality and ineffective care of older people as “an emblem of what is wrong with health care” (Reuben, 2009, p. 2348). It described older people receiving “a lot of health care, some appropriate and some inappropriate, with little coordination or consideration of the big picture” (Reuben, 2009, p. 2348). There is consensus that treatment focused on individual conditions too often is either ineffective or harmful to older people, and that their care should be driven by their goals, values, and preferences. Experts in the care of older people advocate abandoning disease-focused care because “medical care that is centered on the diagnosis and treatment of individual diseases is at best out of date and at worst harmful [because a] primary focus on disease may inadvertently lead to under treatment, over treatment, or mistreatment” (Tinetti and Fried, 2004, p. 179). By following clinical guidelines for discrete medical conditions without taking the whole person and multiple conditions and context into account, providers can harm people with multiple chronic conditions, who represent the majority of older people.
Illustrations of how poorly current systems address the needs of older people are found in Boxes 6-4 and 6-5. The first, presented in Box 6-4, shows the decline following a stroke in a previously active 91-year-old woman and the challenges her family encountered in providing appropriate care, even though her son was a physician.
The second case study describes a woman who was unable to access timely and necessary care after sudden onset of symptoms of unknown origin that were ultimately diagnosed as a recurrence of cancer.
Primary Care
Primary care has a central role in the delivery of care within an integrated, person-centered health care system. A recent National Academies report defines high-quality primary care as “the provision of whole-person, integrated, accessible, and equitable health care by interprofessional teams that are accountable for addressing the majority of an individual’s health and wellness needs across settings and through sustained relationships with patients, families, and communities” (NASEM, 2021, p. 45). Primary care has also been shown to be the most
efficient mechanism for delivering high-quality, cost-effective care around the world (WHO, 2021). High-quality primary care is critical for health, and requires functional partnerships across systems to maximize the capacity of individuals by addressing social determinants of health (Kruk et al., 2010). Box 6-6 highlights Costa Rica’s successful primary care system.
Primary care is ideal for providing preventive care at the individual level across the life course, complementing public health measures at the population level. It includes screening, personal counseling about risk factors, and medication management as conditions that are precursors to more serious age-related conditions are detected. Primary care physicians with training in geriatrics understand the nuances of working with older people to determine what screening is appropriate for them given their goals and health status. But like public health, primary care is often underfunded. A 2012 report from Spain, where primary care makes up 70 percent of all health care, states that only 16 percent of health care funding was dedicated to primary care (Rada, 2012).
Primary care is beneficial in countries across all income levels. A scoping review found evidence that financing, policies, workforce, and core functions are important to primary care systems, but evidence is lacking for implementation strategies to create sustainable systems across different contexts. The research team also found less evidence for the value of population health management, fa-
cility management, safety, and improving quality of service delivery. In low- and lower-middle-income countries, integration of health care will require changes in health policy, health systems, and financing. Countries need to move away from siloed infectious disease and maternal and child care models toward integration and collaboration. To create integrated systems, countries will need to “adopt a diagonal approach that invests in system improvements across the board and demands measurable improvement in health outcomes for multiple conditions” (Kruk et al., 2015, p. 432).
Geriatric Care
As described above, current health systems do not provide the care older people need, especially as chronic conditions become more advanced and functioning declines. Geriatric care is a medical specialty, and many allied health professionals can receive certification in geriatrics. Geriatric care can be delivered as primary care, akin to pediatrics, or as a specialty consulting service. The commission emphasizes the importance of ensuring that all primary and specialty care providers who care for older people have training in geriatrics.
Geriatric care is provided to older people with a focus on the prevention, diagnosis, management, and rehabilitation of chronic conditions, including multimorbidity, geriatric syndromes, and functional decline. Geriatric medical competencies include knowledge of the physiology and biology of aging and causes of aging-related health outcomes, effective management of multimorbidity, and prevention and treatment of geriatric conditions. Box 6-7 describes the key characteristics of geriatric care. Geriatric care is inherently a well-established form of the integrated, person-centered care described below.
The term “geriatrician” typically refers to physicians, most often in internal medicine, or in some countries in family medicine, who have advanced training and board certification in geriatric medicine. The composition and duration of the training and the process for certification vary across countries. Geriatric care teams are interdisciplinary when possible, and may include providers in the disciplines of nursing, pharmacy, nutrition, and physical and occupational therapy. Health care providers in these disciplines can receive additional training and, in some cases, certification in geriatrics.
No specific chronological age qualifies a person for geriatric care, but the older people who benefit most are those with complex care needs, such as multimorbidity, and functional decline. Because most older people with complex care needs prioritize goals that require a threshold level of physical and cognitive function, geriatric care typically prioritizes improvement in or maintenance of cognitive and physical function over medical goals. That said, because decisions about care goals among older patients with chronic conditions are complicated by a lack of clinical guidelines and the challenge of polypharmacy, some geriatricians are encouraging goal-based care, which includes using the person’s
goals to guide care and in some cases to measure the quality of care the person receives.
Multiple geriatric care models have emerged in the United States in recent years, some of which have been exported to other countries. A review article written in 2009 for the Institute of Medicine (IOM) report Retooling for an Aging America: Building the Health Care Workforce describes 15 models of care for older people with chronic conditions, all found to be beneficial as measured by one or more outcomes (Boult et al., 2009). The different models had diverse targets, such as disease self-management, comprehensive geriatric assessment and management, pharmaceutical care, and caregiver support. And a 2019 study by 18 multidisciplinary experts from seven countries reviewed eight sets of guidelines for care of people with multimorbidity and polypharmacy alone, which include 250 discrete recommendations across multiple settings and aspects of clinical management and self-management (Muth et al., 2019). The authors highlight the need for further research on clinical guidelines and care models and recommend research questions that are included at the end of this chapter.
The Integrated Care for Older People (ICOPE) model developed by WHO stands out from many other models because it is evidence based, it is more comprehensive than other models, it has a primary focus on assessing and addressing functional outcomes, it embodies a model of integrated care, and it is focused on community dissemination. It is also being tested globally. The ICOPE model
includes guidance for community-level interventions that can be implemented by community health care workers, and provides implementation support to users through a handbook. It also includes an implementation framework for policy makers and program measures to support implementation (WHO, 2022a). The model’s domains of focus are “cognitive decline, mobility, malnutrition, visual impairment, hearing loss, depressive symptoms, social care and support,” and support for caregivers (WHO, 2022a). The ICOPE approach is highly aligned with multiple areas of emphasis in this chapter.
A detailed analysis of geriatric care models or guidelines is beyond the scope of this report, but a number of barriers have prevented large-scale implementation of these models. The proliferation of competing models is also a challenge, as evidenced by the sheer number of models and recommendations. The primary challenge to implementing the model is the current single-disease approach that dominates health care systems and financing globally. A third challenge is limited evidence of efficacy for discrete elements within the models or of models’ efficacy outside narrow settings. Research recommendations related to these barriers are addressed at the end of this chapter.
Integrated, Person-Centered Care
WHO developed a “global strategy on people-centered and integrated health services” to “encourage a fundamental paradigm shift in the way health services are funded, managed and delivered so all people have access to health services that respond to their preferences, are coordinated around their needs, and are safe, effective, timely, efficient and of an acceptable quality” (WHO, 2015b, p. 34). This care approach is important for people of all ages, but especially for people at any age with advanced illness, conditions requiring complex management, or multiple chronic conditions. For these people, clinical guidelines become less helpful in guiding care because treatment efficacy declines and side effect burdens increase, and treatment for one disease may undermine that for another. At this stage, the person’s preferences, goals, and values become the yardstick by which clinicians can measure the appropriateness of potential interventions.
According to WHO, integrated, person-centered care (including behavioral health care) is the most effective and appropriate care delivery model for maximizing health, function, and well-being across the life course (WHO, 2015b). It provides a structure and organizing principles for coordinating care across primary, specialty, acute, and long-term care settings. Integrated care “ensures people receive a continuum of services including health promotion, disease prevention, diagnosis, treatment, disease-management, rehabilitation, and palliative care at different levels and sites within the health system, and that care is provided according to their needs throughout their life course” (WHO, 2015b, p. 228). Aspects of care that are positively impacted by integrated care include pa-
tient satisfaction, perceived quality of care, and access to services, but evidence on how integrated care impacts quality of life is mixed (Flanagan et al., 2017).
Person-centered care “consciously adopts the perspectives of individuals, families and communities, and sees them as participants [and] beneficiaries of health care and long-term-care systems that respond to their needs and preferences in humane and holistic ways” (WHO, 2015b, p. 230). In contrast to current disease-focused care delivery, person-centered care is relationship-based; views disease and body systems as interrelated; and is designed around a person’s experiences, preferences, and goals (WHO, 2015b, p. 34).
Components Needed for Integrated, Person-Centered Care
WHO’s Global Strategy on People-Centred and Integrated Health Services builds on its earlier strategies to promote universal health care, primary health care, action on chronic conditions, action on social determinants of health, and enhanced health security through resilient health systems (WHO, 2015a). WHO emphasizes the importance of countries’ contexts in moving toward integrated, person-centered care, given that no country has fully achieved the goals of these earlier strategies, although some are further ahead in doing so than others. For example, universal health care is not a reality in some countries across all income levels. Instead of viewing integrated, person-centered care as a new model, WHO suggests that it be viewed as “a service design principle that can help to support and improve strategies that seek to enhance access, encourage universal health coverage, and encourage primary and community-based care” (WHO, 2015b, p. 19). A U.S.-based effort with the goal of promoting integrated, person-centered care in geriatric populations identified barriers that include physician-driven decision making, misaligned incentives, lack of appropriate performance measures, uncoordinated payment structures, and lack of continuity in health records (American Geriatrics Society Expert Panel on Person-Centered Care, 2016).
Integrated person-centered care is relevant across the life course. Even a healthy young adult without complex coordination or care needs can be faced with challenging health care choices influenced by cultural background, religious beliefs, or personal preferences. Moreover, people’s journeys through health care systems are established when they are young. Establishing expectations for and the experience of integrated, person-centered care before people face aging can help them reach later life with this approach embedded.
Care coordination, a key component of integrated care, need not be provided by clinicians. An example of a nonmedical approach to coordination is programs in African countries that use “patient guardians” for care continuity during and after hospitalization. The patient guardian is typically a family member who is educated about the role and the person’s needs and then continues to support the person after hospital discharge (Basu et al., 2014).
Levers for Change
Care for older people and all people with complex health needs is inadequate in much of the world. Models for integrated, person-centered care abound, but there has been limited success in their widespread adoption. A shift to this type of care would require a tremendous cultural change away from the traditional practice of medicine.
Metrics
Beyond metrics for universal health coverage, including financial risk protection and chronic condition screening and management (e.g., fasting blood glucose, obesity, and hypertension), metrics for evaluating integration and person-centeredness would typically require patient surveys, which are expensive to administer. Metrics using patient-reported outcomes are becoming increasingly feasible with technological advances, but they are still in their infancy.
Health care delivery metrics are extraordinarily complex. Process metrics are the opposite of person-centered in that they assume that every person meeting certain criteria should receive the same intervention, which becomes less true as people age. Second, they can distort incentives. For example, when outcomes related to one condition are measured but those related to another condition are not, funding for the other condition may be diverted to the measured one (Luyckx et al., 2021).
The International Consortium for Health Outcomes Measurement’s Older Person Working Group developed a set of outcome measures for older people designed for use in value-based care models. The measures include survival, place of death, frailty, “polypharmacy, falls, participation in decision making and time spent in hospital,” and “pain, mood and emotional health, autonomy and control and carer burden” (Akpan et al., 2018, p. 4).
Research Questions
Research is needed to investigate the following questions:
- effective interventions for real-world older people—not just clinical trials that include real-world conditions, such as cognitive function;
- how to promote self-management among people with multimorbidity and barriers to self-management;
- development and testing of value-based care outcome measures;
- effective priority setting between clinician and patient;
- development of consensus for evaluating the quality and efficacy of geriatric care models;
- delivery models for supports related to the social determinants of health in the context of health, such as co-locating services;
- models for sharing social services data with health care providers; and
- efficacy of models for financing integrated health care and social services.
Finding 6-9: Current health care systems do not effectively serve the needs of older people. Integrated, person-centered models informed by principles of geriatric medicine and the biology of older adults can provide coordinated and effective care.
Finding 6-10: Geriatric and geriatric-informed care ensures that care for older people is based on knowledge about their care needs and biology. Effective geriatric care is person-centered and integrated.
Conclusion 6-3: Integrated, person-centered care is the most effective and appropriate care delivery model for maximizing health, function, and well-being across the life span.
Recommendation 6-2: Health care systems should shift to enabling healthy longevity. To catalyze such a shift, actions to be taken by 2027 include
- Health systems, in concert with communities and the people they serve, should adopt affordable, accessible, culturally appropriate models, including geriatric care models, for providing person-centered, integrated care for older people facing functional limitations, multimorbidity, frailty, and complex care needs.
- Governments should develop plans to align health care payment and reimbursement systems with healthy longevity outcomes.
- Health care and long-term care systems should begin to develop the infrastructure needed to create integrated continua of care supported by interoperable data systems.
- Health care systems should measure care outcomes based on patient goals and preferences and patient-reported outcomes.
- Relevant licensing and certification bodies should ensure that all health care providers receive training on how the physiology and psychology of aging affect diagnosis and treatment of older patients.
- Governments, professional societies, and health systems should provide incentives to develop and/or maintain a geriatrics workforce, including allied health workers, to focus on older adults with multimorbidity, geriatric syndromes, and declining physical and cognitive functioning.
- Governments, employers, health systems, and communities should empower citizens with the tools and data needed to manage their own health.
KEY TARGET: LONG-TERM CARE
Long-term care is crucial to enable people with significant loss of capacity to experience lives of meaning and dignity. Even if the health span increases and healthy longevity is achieved at higher rates than today, some people will still need long-term care. Echoing the previous section’s emphasis on the importance of person-centered care, it is critical for long-term care to be driven by a person’s goals, including where the person wants to live, how care is delivered, and how life is lived. The goals of long-term care are to maximize function, support living with dignity and respect, optimize autonomy, ensure a life of meaning, and provide appropriate health care consistent with the person’s goals.
Community-Based, Long-Term Care
Family Caregiving
Globally, the most common site of long-term care is the person’s or a family member’s home, and the caregivers most often are family members. In the United States alone, AARP estimated that in 2017, 41 million family caregivers provided 34 billion hours of care to an adult, with an estimated value of USD470 billion (Reinhard et al., 2019). Little is known about the adequacy of care provided by family caregivers except that many have little knowledge of how to care for an older person with functional limitations, at least at the beginning of the caregiving relationship. People who receive care typically express gratitude for their caregivers, but abuse by family caregivers is also a concern globally. WHO reports that one in six people aged 60 and older were subject to caregiver abuse in 2017 (WHO, 2021). Such abuse is often associated with caregiver burden and stress (NASEM, 2016). As mentioned in Chapter 4, family caregiving is under strain from demographic changes, including smaller family sizes, women entering the workforce, and migration of younger people from rural to urban areas. Box 6-8 provides an example of quality concerns about family caregivers for people with dementia.
Using caregiving for people with dementia as an example, across 11 sites in Latin America, China, and India, more than half—and as many as 68 percent—of people with dementia live with adult children, except in the Dominican Republic (48.5 percent) and urban China (38.3 percent). Children or children-in-law are typically the main caregivers within the household across all 11 sites (41.6 percent in the Dominican Republic to 79.1 percent in Mexico), with spouses the next most common caregivers. In every location except for rural China, more than 66 percent of family caregivers in the household are female (WHO, 2012).
Caregiving experts agree that family caregivers need training to provide adequate care for older people; support for the emotional strain caregiving can bring; and, when possible, financial support, particularly for those who must forego paid work to provide care for a family member (NASEM, 2016). Caregivers have complex roles that may include personal care, help with daily tasks, medication administration, management of medical devices, scheduling of medical appointments, and medical decision making. They may also have physically demanding tasks, such as lifting or bathing a person. Care of people with dementia can be particularly challenging because their behaviors can be confusing or emotionally challenging, and demands such as repeatedly answering the same question can be frustrating. Strategies and programs are available to help caregivers minimize troubling behaviors and cope, but they are not always intuitive, so training is important.
Paid Home Care
Professional home care is less common than family caregiving, but the need is growing with the demographic changes described throughout this report. As with family caregiving, data on training for or quality of paid home care are sparse. Paid caregivers are not always subject to oversight and regulation. In a qualitative study of paid caregivers in the United States, most described the job as imposing intense mental demands due to uncertainty about staffing and the need to live paycheck to paycheck, factors exacerbated by the COVID-19 pandemic (Musumeci et al., 2021). For older people with resources, insurance, or government support, however, paid home care makes it possible to remain in their home, where most people say they want to live.
Nursing Homes
The International Association of Gerontology and Geriatrics (IAGG) and the American Medical Directors Association developed the following definition of a nursing home, sometimes called a care home, based on a survey involving many countries:
A nursing home provides 24-hour functional support and care for persons who require assistance with ADLs and who often have complex health needs and increased vulnerability. Residency within a nursing home may be relatively brief for respite purposes or short term (rehabilitative), or long term, and may also provide palliative/hospice and end-of-life care. In general, most nursing homes also provide some degree of support from health professionals, but a small subset provide socialization activities and basic assistance with ADLs but have no trained health professionals on staff. Although post-acute rehabilitation may be provided in the nursing home (i.e., in the United States and The Netherlands), in many countries this is provided in separate facilities (i.e., geriatric or cottage hospitals) or in a geriatric unit of the acute hospital. (Sanford et al., 2015, pp. 183–184)
Countries vary substantially in the percentage of older people living in nursing homes. In the United States, for example, 1.5 million people, or 0.05 percent of the population and 4 percent of older adults, live in nursing homes. In Asia, rates range from 0.01 percent of older adults in Indonesia to 5.9 percent in Japan (Hayashi, 2019) (see Figure 6-4).
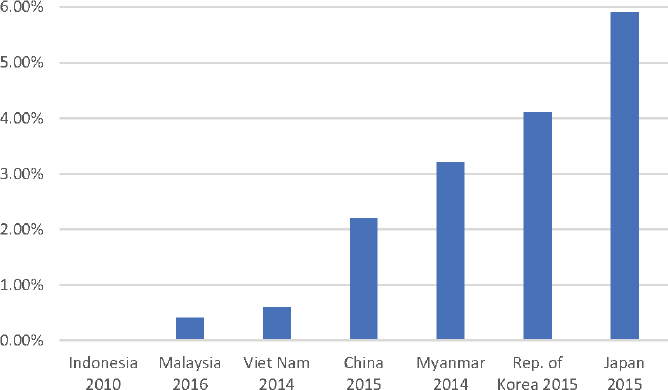
SOURCE: Staff generated graphic of data from Hayashi, 2019.
Nursing homes have a troubled past in many countries, rife with concerns about care quality and allegations of abuse, neglect, and exploitation (WHO, 2021). By their very nature, nursing homes limit the freedom of residents because they are required to keep residents safe; this was especially true during the COVID-19 pandemic. Nonetheless, many people will experience functional decline to the point that they can no longer receive care at home. Societies need to embrace new models of institutional care to ensure that older adults who need care in nonfamily settings can receive high-quality care.
In the United States, nursing homes that serve the poor are often underresourced, limiting such aspects of care as nurse-to-patient ratios. Research has found that nursing homes in the United States with higher percentages of Black residents are more often understaffed and receive deficient care and mistreatment ratings than nursing homes with lower percentages of Black residents (Harrington et al., 2017).
Funding for long-term care across countries is heterogeneous. In some high-income countries, including Japan, long-term care insurance covers all residents over age 65. In others, such as the United Kingdom, the cost of long-term care is based on income thresholds (OECD, 2021). In the United States, on the other hand, few people have insurance for long-term care, regardless of setting. Instead, Medicaid, the government-funded program for very-low-income people over age 65 (among other groups), guarantees payment for long-term care if delivered in a nursing home, but not if provided in the community. This approach limits direct government costs because many people will forego financial support for long-term care if it requires them to live in a nursing home. However, it also can impose significant burdens on families and costs to the broader economy, such as caregivers’ inability to work.
Levers for Change
To achieve the vision set forth at the outset of this chapter, much about long-term care will need to change, ideally in a thoughtful and strategic manner. In 2011, IAGG made 10 recommendations—both structural and care-focused—for improving nursing home care. Although these recommendations were made more than a decade ago, the targeted areas remain problematic (Tolson et al., 2011).
In the future, it will be important to design or redesign both community- and facility-based care to meet the growing demand for long-term care globally (in Asia, for example, the demand is predicted to rise) (Hayashi, 2019). Many countries will also need structures for long-term care costs. Although paying for long-term care is a major concern and will require political will and trade-offs, determining what political and policy trade-offs countries should make is beyond the scope of this report.
As with all systems addressing the needs of older adults and younger people with disabilities, systems should be codesigned by all stakeholders, especially those with long-term care needs, following user-centered design principles and other tools, such as community-based participatory design (Ferreira and Gendron,
2011). Systems will need to include basics such as hygiene and health care, sustainable funding structures, and training for family and paid caregivers. Nursing homes will need more programmatic flexibility. Ideally, they will have fewer residents,8 and the mixed population they currently house will be redistributed so that each group receives care in facilities better designed for their needs, such as rehabilitation centers, hospice, and memory care centers. New models, such as “care farms” piloted in the Netherlands, may become more widespread (Age Platform Europe, 2021). At the same time, the adverse experiences with COVID-19 in nursing homes globally may generate increased interest and investment in nursing home alternatives, such as hospital-based extended care units, home care, and other community-based care models. The COVID-19 experience also has highlighted the critical importance of strengthening the long-term care workforce.
Box 6-9 describes innovations in home-based, long-term care taking place in East Asia described in a report from the World Bank.
___________________
8 In the United States, larger nursing homes were more likely than smaller ones (Abrams et al., 2020).
Box 6-10 describes a creative approach to supporting the long-term care needs of people in Canada.
Finding 6-11: Many countries around the globe are ill prepared to provide long-term care to the increasing number of older people expected to need it.
Finding 6-12: Family caregivers provide the majority of long-term care globally, but most have inadequate training and experience to provide quality care, especially for people with dementia.
Conclusion 6-4: Family caregivers need training to provide adequate care to older persons; support for the emotional strain caregiving can bring; and, when possible, financial support, particularly for caregivers who must forego paid work to provide care to a family member.
Conclusion 6-5: Countries globally will need to build structures and financing models to provide long-term care to the growing number of older people predicted to have long-term care needs.
Recommendation 6-3: Governments should work with health and long-term care systems and researchers to develop strategies for making available culturally sensitive, person-centered, and equitable long-term care. To the greatest extent possible, strategies should honor people’s preferences about care settings, enabling them to age within their home or community when possible. By 2027, countries should take first steps toward enacting strategies by implementing
- pilot programs to identify effective, accessible, affordable, and scalable models for delivering long-term care services and supports; and
- models for providing financial and technological support, training, and career pathways for informal caregivers as well as the paid long-term care workforce.
Metrics
Metrics for long-term care include the number and demographic characteristics of paid and unpaid caregivers; availability of facility-based care; and quality of long-term care, whether home- or facility-based.
Data Needs and Research Questions
Data will be needed to predict the future need for long-term care and model feasible approaches to providing that care. Data on the quality of long-term care will also be important to model given that demand increases the risk of poor quality. Needed as well are data on the quality of family caregiving and paid home care providers, and on the needs of family and paid caregivers. The International Long-Term Care Policy Network captures and makes available data on long-term care, which have been critical to understanding the challenges posed by COVID-19 to long-term care systems and policy responses from countries.9
Research on the following questions also is needed:
___________________
- best practices for integrating long-term care and social service providers;
- interventions with family and paid caregivers that enable them to provide the best care;
- efficacy of models for delivering and financing long-term care systems;
- best practices for engaging residents and people receiving home-based, long-term care in the codesign and coredesign of long-term care systems; and
- best practices for enabling residents of nursing homes to live life fully and with meaning and purpose.
KEY TARGET: HEALTH CARE WORKFORCE
It is important for providers of care for older people to have knowledge of the principles of geriatrics and the biology of these patients. But the workforce of geriatricians and allied health professionals with this knowledge is inadequate to meet current, let alone future, needs. The IOM report Retooling for an Aging America highlights the shortage of geriatricians, as well as social workers, physician assistants, registered nurses, and pharmacists who specialize or are certified in geriatrics (IOM, 2008). The report also emphasizes the shortage of nurses and nursing assistants in long-term care, which has only grown during the COVID-19 pandemic.
WHO’s World Report on Ageing summarizes the inadequacy of geriatric training globally. A study of medical schools in 36 countries found that 27 percent—including 19 percent in high-income countries, 43 percent in economies in transition, and 38 percent in other countries—provided no training in geriatric medicine (WHO, 2015b). Medical trainees learn siloed, disease-based care, not the comprehensive biopsychosocial approaches needed to provide high-quality care to older people, especially those with complex needs. Other health care workers, especially those who provide direct services in low- and middle-income countries, also lack the training needed to provide high-quality care for this population.
A critical component of the care workforce for older people consists of those who provide personal care and other supports to people needing long-term care within and outside of facilities. This workforce is overwhelmingly female, often part of the informal economy, and typically very low-wage. The commissioners believe that improving the future of long-term care will require training, safety protections, and adequate pay for these workers.
Conclusion 6-6: The current geriatrics workforce is inadequate, and the need will grow. Plans to develop a geriatrics workforce for the future will be critical to ensuring adequate care for the growing number of older people globally.
KEY TARGET: GEROSCIENCE, TECHNOLOGY, AND BIG DATA INNOVATION
Innovations, along with a new understanding of aging, are emerging from geroscience, technology, and big data. These innovations have the potential to improve the lives of people living with the effects of age and chronic conditions.
Geroscience and Technology for Delaying Aging
Geroscience, which relies on interdisciplinary research teams, aims to describe the age-related biological mechanisms that cause chronic conditions, frailty, and functional decline, and to develop preventive and therapeutic interventions to slow the aging process and prevent or delay the onset of chronic conditions (Kennedy et al., 2014). The therapeutics identified through geroscience are not necessarily medical, but could include pollution reduction or increased physical activity, for example. Although geroscience has the potential to extend the life span, the commission chose to emphasize the “healthy” part of “healthy longevity”; thus, the goal is to improve the percentage of life in good health, not to further prolong the life span, recognizing that major disparities in life span exist globally.
In its focus on the underlying drivers of aging, geroscience differs from traditional biomedical research, which focuses on one disease at a time and often is conducted with carefully constructed study samples that are not representative of the larger population. For example, a clinical trial investigating a medication for chronic kidney disease may exclude patients with other chronic conditions, and in so doing will exclude the more than 80 percent of people with chronic kidney disease who have other chronic conditions (Hajat and Stein, 2018). In contrast, epidemiologic studies are conducted with population samples that represent the general population and, working in concert with geroscience, can combine chronic disease and aging research to explain how the human body ages and declines over time.
Prevention and care targeting aging pathways are predicted to have very different, and better, outcomes compared with the current discrete disease-focused approach. Early research suggests that in contrast with treating chronic conditions as discrete pathologies, interventions to delay aging would also increase resistance to multiple chronic conditions. Results of a study comparing health and economic returns from delaying aging and from treating chronic conditions separately suggest that the latter approach is a net negative (Goldman et al., 2013). While treating chronic conditions individually may enable people to live longer, they still suffer from other age-related chronic conditions and disabilities that develop from the same underlying age-related mechanisms that caused the original condition.
Discoveries in geroscience are changing the way people view aging, from the past view that aging comes with inevitable long periods of poor health toward
an optimistic view that targeting aging rather than single diseases can shorten periods of poor health in later life. Geroscience will be even more powerful in supporting healthy longevity when combined with the availability of more data and advanced analytics and integrated into both public health and medical care technology.
Care Delivery Technology
Digital technologies have the potential to play an important role in integrated care delivery for older people by enabling early detection and management of chronic diseases and functional impairments. Digital care technology is most effective when experts across sectors, such as engineers, medical professionals, and scientists, use human-centered design techniques to engage older adults throughout the design process. This codesign ensures that the final products meet older adults’ diverse needs. Device designs that are adaptable and can be personalized as circumstances change would provide older adults with the opportunity to become familiar and comfortable with the technology.
Telemedicine
Telemedicine is used to examine and diagnose people in their own homes or another site when in-person visits are challenging or impossible. Virtual care delivery enhances the accessibility, quality, efficiency, and cost-effectiveness of health care services (WHO, 2010b). During the COVID-19 pandemic, the rapid shift to telehealth, enabled by the removal of regulatory barriers that had been in place, allowed for continuity of care when in-person visits could not take place (ITU, 2021).
Telemedicine is widely accepted by older people. In lower- to middle-income countries, older adults can benefit from telehealth care in remote areas that lack a functioning medical center (WHO, 2010b). Telemedicine also allows patients with complex needs to meet with psychologists who may not work at nearby on-site facilities. In sub-Saharan Africa, for example, the Mental Health Preparedness and Action Framework suggests that telemedicine can be used more widely, first through the training of community health workers and volunteers, and second through an increase in mobile health services for mental health support in areas where psychologists are not widely available to see patients in person (Jaguga and Kwobah, 2021).
Telehealth and Remote Monitoring
Telehealth encompasses a broad range of electronic and telecommunications services and technologies used for purposes such as remote patient monitoring and health promotion messaging.
Wearable technologies, a form of telehealth, are increasingly being used to monitor older patients’ health and provide real-time feedback that informs both them and their providers about their health status and needs. The data produced by these devices are a more representative measure of a patient’s physical status than snapshot data collected from intermittent medical appointments. Most important, these devices can be used to study physical and cognitive issues that may go unnoticed with conventional monitoring processes.
The rising number of people with Alzheimer’s disease has sparked interest in the possibility of using wearable technology to capture cognitive, sensory, and motor changes that can be measured before symptoms of the disease become obvious. Research suggests that gait speed, stride length, and gait symmetry decrease at an early stage of Alzheimer’s disease and precede signs of cognitive impairment. Inertial measurement unit sensors on smartphones detect changes in routine walking movements. The gait metrics they produce, coupled with changes in verbal and visual skills, provide a composite analysis of predictors of Alzheimer’s disease to enable a proactive approach to treatment.
Wearable activity trackers also can provide baseline data and goals for physical activity, along with a platform for accountability, such as a personal dashboard, that may otherwise be difficult for older adults to access. Older adults thereby have a visible reminder to increase physical activity that supports healthy longevity and enables self-monitoring and feedback (Kononova et al., 2019). Box 6-11 describes the use of technology in developing a disaster-resilient community in Japan.
Big Data, Advanced Analytics, and Healthy Longevity
At the same time that geroscience has made leaps in understanding of aging processes, the world has entered a period of big data. The term “big data” refers to the vast amount of data about people that is being collected and stored across all domains of life, along with the use of AI to capture, process, store, and analyze the data. In the context of understanding the multiple dimensions of health, data in people’s health records are relevant. Beyond what traditional health records contain, other relevant data include factors such as the location of a person’s house (e.g., its proximity to a chemical plant or oil refinery) and the person’s education, net worth, marital status, gender, social media posts suggesting tobacco or alcohol use, and physical activity (as recorded by tracking apps). In the United States, health insurance companies are already using nonmedical data sources to make decisions, typically without the person’s knowledge (Allen, 2018).
On their own, these expansive data are of little value, but AI has rendered them far more valuable than in the past. A combination of unstructured AI and hypothesis-driven research is expected to enable the precision medicine and precision public health described earlier in this chapter. Unstructured AI detects patterns and clusters that are complex, multidimensional, and subtle, and that would be very difficult to identify using hypothesis-driven quantitative research methods.
In health, AI is being used for natural language processing (e.g., to read open text in health records), robotics, computer vision, pattern detection (e.g., reading X-ray images), and fall detection (Loveys et al., 2022). Researchers are investigating the use of AI in long-term care to support the long-term care workforce and improve access to data and information. In their recent systematic review of the literature on AI uses in long-term care, Loveys and colleagues (2022) concluded that interventions were somewhat acceptable but the evidence for their effectiveness was mixed when measured against desired outcomes.
The use of big data carries risks, however. First, unstructured AI can identify statistical “noise,” a term that denotes a meaningless statistical association. Second, data reflect the environment in which they are generated, so data captured in a community characterized by bias against a minority population will reflect that bias. In the United States, for example, a health insurance company restricted African Americans’ access to a home-based care program because the algorithm used to determine eligibility was developed using data that incorporated historical barriers to health care (Obermeyer et al., 2019). Finally, some “black box” algorithms are so complex that the factors driving decisions within them cannot be identified, creating the risk that troubling decisions made within an algorithm will be hidden. Consequently, while unstructured AI can be highly effective for generating hypotheses to be tested, findings must be validated using hypothesis-driven research before they can be used to create algorithms to support precision medicine or precision public health (Hulsen et al., 2019).
Finding 6-13: The technologies emerging across the health sector—including geroscience, precision medicine and precision public health, and remote monitoring to detect health threats earlier than is currently possible—offer great promise for advancing healthy longevity.
Conclusion 6-7: Technology and artificial intelligence will drive health systems of the future, but privacy protection and transparency will be essential to ensure that they are acceptable to people and help promote equity.
Research Questions
In addition to the efficacy and acceptability of AI use and interventions across health systems, Kennedy and colleagues (2014) suggest the following research goals for geroscience:
- “Continuum from psychological to molecular stresses
- Differentiate hormesis from toxic stress
- Better align human and animal studies
- Biomarker development: chronologic versus biologic aging
- Link age-related environmental inputs to epigenetic signatures
- Test small molecules that regulate enzymes controlling epigenetic events
- Differentiate adaptive and maladaptive inflammatory responses
- Define age-related inflammatory sources and their systemic effects
- Determine how obesity and metabolic dysfunction alter inflammation with age
- Generate systems-level understanding of the types of macromolecular damage and their roles in chronic disease states
- Understand how stochastic damage influences the variability of aging
- Define role of signal transduction pathways linked to metabolism in the aging process
- Understand contribution of circadian clocks to aging and metabolism
- Connect metabolic dysfunction with tissue-specific decline in aging
- Identify proteostatic pathways that are overwhelmed in specific chronic disease states
- Examine crosstalk between proteostasis machineries
- Understand non-cell-autonomous signaling and activation of proteostasis pathways
- Determine whether declining adult stem cell function drives aging and chronic disease
- Examine how aging and associated disease impair adult stem cell function
- Determine how macromolecular damage accumulates in aging adult stem cell pools” (Kennedy et al., 2014, p. 711)
CONCLUSION
As more people live into older ages, a corresponding increase in demand on health systems can be anticipated. While for many people, interventions and recommendations discussed in Chapters 4 and 5 can ideally delay biological aging and increase years of healthy life, others will continue to rely on public health, health care, and long-term care for support as they age and experience the onset of chronic conditions. Current care systems are disjointed, however, and a rebalancing of investment across the care spectrum will be necessary to ensure that adequate support and priority are given to preventing disease and promoting health, not just responding to illness. To this end, the focus will have to shift to primary, integrated, person-centered care, with increased investment in geriatrics and a health care workforce with the appropriate knowledge to care for older adults. Finally, geroscience and innovations in health data hold great promise for improving understanding of aging and health and enhancing access to care for those with limited mobility. Together, these improvements can enhance the quality of life for older adults as they live longer lives.
REFERENCES
Abrams, H. R., L. Loomer, A. Gandhi, and D. C. Grabowski. 2020. Characteristics of US nursing homes with COVID‐19 cases. Journal of the American Geriatrics Society 68(8):1653–1656.
ACL (Administration for Community Living). 2022. How much care will you need? https://acl.gov/ltc/basic-needs/how-much-care-will-you-need (accessed May 2, 2022).
Age Platform Europe. 2021. Care farms provide nursing home care in the Netherlands. https://www.age-platform.eu/good-practice/care-farms-provide-nursing-home-care-netherlands (accessed March 1, 2022).
Akpan, A., C. Roberts, K. Bandeen-Roche, B. Batty, C. Bausewein, D. Bell, D. Bramley, J. Bynum, I. D. Cameron, and L.-K. Chen. 2018. Standard set of health outcome measures for older persons. BMC Geriatrics 18(1):1–10.
Allen, M. 2018. Health insurers are vacuuming up details about you—and it could raise your rates. ProPublica, July 17. https://www.propublica.org/article/health-insurers-are-vacuuming-up-details-about-you-and-it-could-raise-your-rates (accessed May 2, 2022).
American Geriatrics Society Expert Panel on Person-Centered Care. 2016. Person-centered care: A definition and essential elements. Journal of the American Geriatrics Society 64(1):15–18.
Barr, E. C., and M. Marmot. 2020. Leadership, social determinants of health and health equity: The case of Costa Rica. Pan American Journal of Public Health (Revista Panamericana de Salud Pública) 44:e139. https://doi.org/10.26633.RPSP.2020.139.
Basu, L., R. Frescas, and H. Kiwelu. 2014. Patient guardians as an instrument for person centered care. Globalization and Health 10(1):1–3.
Bengtsson, L., J. Gaudart, X. Lu, S. Moore, E. Wetter, K. Sallah, S. Rebaudet, and R. Piarroux. 2015. Using mobile phone data to predict the spatial spread of cholera. Scientific Reports 5(1):1–5.
Bloom, D. E., E. Cafiero, E. Jané-Llopis, S. Abrahams-Gessel, L. R. Bloom, S. Fathima, A. B. Feigl, T. Gaziano, A. Hamandi, and M. Mowafi. 2012. The global economic burden of noncommunicable diseases. Geneva, Switzerland: World Economic Forum.
Boult, C., A. F. Green, L. B. Boult, J. T. Pacala, C. Snyder, and B. Leff. 2009. Successful models of comprehensive care for older adults with chronic conditions: Evidence for the Institute of Medicine’s “Retooling for an Aging America” report. Journal of the American Geriatrics Society 57(12):2328–2337.
Bradley, E. H., M. Canavan, E. Rogan, K. Talbert-Slagle, C. Ndumele, L. Taylor, and L. A. Curry. 2016. Variation in health outcomes: The role of spending on social services, public health, and health care, 2000–09. Health Affairs 35(5):760–768.
Brown, R. C. 2018. Resisting moralisation in health promotion. Ethical Theory and Moral Practice 21(4):997–1011.
CDC (Centers for Disease Control and Prevention). 2022. Health impact in 5 years. https://www.cdc.gov/policy/hst/hi5/index.html (accessed March 1, 2022).
Chang, A. Y., K. Cowling, A. E. Micah, A. Chapin, C. S. Chen, G. Ikilezi, N. Sadat, G. Tsakalos, J. Wu, and T. Younker. 2019. Past, present, and future of global health financing: A review of development assistance, government, out-of-pocket, and other private spending on health for 195 countries, 1995–2050. The Lancet 393(10187):2233–2260.
Crawford, R. 1977. You are dangerous to your health: The ideology and politics of victim blaming. International Journal of Health Services 7(4):663–680.
Cuccia, L., J. Chadwick, A. Hassan, A. Kim, R. Sivarajan, and V. Wong. 2019. Costa Rica’s health care reform: Impact and success of the Ebais model. The Prognosis: McGill’s Student Global Health Journal. https://mghjournal.com/wp-content/uploads/2019/07/costa-ricas-health-care-report_ebais-model_luca-cuccia-et-al..pdf (accessed May 2, 2022).
DeSalvo, K. B., Y. C. Wang, A. Harris, J. Auerbach, D. Koo, and P. O’Carroll. 2017. Public health 3.0: A call to action for public health to meet the challenges of the 21st century. Preventing Chronic Disease 14:170017. http://dx.doi.org/10.5888/pcd14.170017.
Dutton, D. J., P.-G. Forest, R. D. Kneebone, and J. D. Zwicker. 2018. Effect of provincial spending on social services and health care on health outcomes in Canada: An observational longitudinal study. Canadian Medical Association Journal 190(3):E66–E71.
Ebrahim, S., P. Ordunez, P. Lloyd-Sherlock, M. McKee, R. Martinez, and P. Soliz. 2020. Improving the indicator for premature deaths from noncommunicable diseases. Bulletin of the World Health Organization 98(6):438.
ESCAP (Economic and Social Commission for Asia and the Pacific). 2012. Reducing vulnerability and exposure to disasters: The Asia-Pacific disaster report 2012. Bangkok, Thailand: United Nations.
Ferreira, M. P., and F. Gendron. 2011. Community-based participatory research with traditional and indigenous communities of the Americas: Historical context and future directions. International Journal of Critical Pedagogy 3(3).
Flanagan, S., S. Damery, and G. Combes. 2017. The effectiveness of integrated care interventions in improving patient quality of life (QOL) for patients with chronic conditions. An overview of the systematic review evidence. Health and Quality of Life Outcomes 15(1):1–11.
Garin, N., A. Koyanagi, S. Chatterji, S. Tyrovolas, B. Olaya, M. Leonardi, E. Lara, S. Koskinen, B. Tobiasz-Adamczyk, and J. L. Ayuso-Mateos. 2016. Global multimorbidity patterns: A cross-sectional, population-based, multi-country study. Journals of Gerontology Series A: Biomedical Sciences and Medical Sciences 71(2):205–214.
Goldman, D. P., D. Cutler, J. W. Rowe, P.-C. Michaud, J. Sullivan, D. Peneva, and S. J. Olshansky. 2013. Substantial health and economic returns from delayed aging may warrant a new focus for medical research. Health Affairs 32(10):1698–1705.
Hajat, C., and E. Stein. 2018. The global burden of multiple chronic conditions: A narrative review. Preventive Medicine Reports 12:284–293.
Halpin, H. A., M. M. Morales-Suárez-Varela, and J. M. Martin-Moreno. 2010. Chronic disease prevention and the new public health. Public Health Reviews 32(1):120–154.
Harrington, C., J. M. Weiener, L. Ross, and M. Musumeci. 2017. Key issues in long-term services and supports quality. Kaiser Family Foundation. https://www.kff.org/medicaid/issue-brief/key-issues-in-long-term-services-and-supports-quality (accessed May 2, 2022).
Hashimoto, K., K. Yamada, K. Tabata, M. Oda, T. Suganuma, A. Rahim, P. Vlacheas, V. Stavroulaki, D. Kelaidonis, and A. Georgakopoulos. 2015. Ikaas data modeling: A data model for community services and environment monitoring in smart city. Paper read at 2015 IEEE International Conference on Autonomic Computing. Grenoble, France: July 7–10, 2015.
Hayashi, R. 2019. Demand and supply for long-term care for older persons in Asia. Economic Research Institute for ASEAN and East Asia. https://www.eria.org/publications/demand-and-supply-of-long-term-care-for-older-persons-in-asia (accessed May 2, 2022).
Horton, R. 2018. Offline: In defence of precision public health. The Lancet 392(10157):1504.
Hulsen, T., S. S. Jamuar, A. R. Moody, J. H. Karnes, O. Varga, S. Hedensted, R. Spreafico, D. A. Hafler, and E. F. McKinney. 2019. From big data to precision medicine. Frontiers in Medicine 6:34.
Hunter, D. J., and K. S. Reddy. 2013. Noncommunicable diseases. New England Journal of Medicine 369(14):1336–1343.
IHME (Institute for Health Metrics and Evaluation). 2019. GBD compare. https://vizhub.healthdata.org/gbd-compare (accessed December 15, 2021).
iKaaS. 2022. Town management and health support service in Tago-Nishi. http://ikaas.com/node/280 (accessed May 2, 2022).
Inouye, S. K., S. Studenski, M. E. Tinetti, and G. A. Kuchel. 2007. Geriatric syndromes: Clinical, research, and policy implications of a core geriatric concept. Journal of the American Geriatrics Society 55(5):780–791.
IOM (Institute of Medicine). 2008. Retooling for an aging America: Building the health care workforce. Washington, DC: The National Academies Press.
ITU (International Telecommunication Union). 2021. Ageing in a digital world—From vulnerable to valuable. https://www.itu.int/dms_pub/itu-d/opb/phcb/D-PHCB-DIG_AGE-2021-PDF-E.pdf (accessed May 2, 2022).
Jaguga, F., and E. Kwobah. 2021. Mental health response to the COVID-19 pandemic in Kenya: A review. International Journal of Mental Health Systems 14:68.
Jiang, X., J. Huang, D. Song, R. Deng, J. Wei, and Z. Zhang. 2017. Increased consumption of fruit and vegetables is related to a reduced risk of cognitive impairment and dementia: Meta-analysis. Frontiers in Aging Neuroscience 9:18.
Kamal, R., and J. Hudman. 2020. What do we know about spending related to public health in the U.S. and comparable countries? Health spending. Peterson Center on Healthcare, Kaiser Family Foundation. https://www.healthsystemtracker.org/about-us (accessed May 2, 2022).
Kennedy, B. K., S. L. Berger, A. Brunet, J. Campisi, A. M. Cuervo, E. S. Epel, C. Franceschi, G. J. Lithgow, R. I. Morimoto, and J. E. Pessin. 2014. Geroscience: Linking aging to chronic disease. Cell 159(4):709–713.
Khoury, M. J., M. F. Iademarco, and W. T. Riley. 2016. Precision public health for the era of precision medicine. American Journal of Preventive Medicine 50(3):398–401.
Khoury, M. J., G. L. Armstrong, R. E. Bunnell, J. Cyril, and M. F. Iademarco. 2020. The intersection of genomics and big data with public health: Opportunities for precision public health. PLoS Medicine 17(10):e1003373.
Kononova, A., L. Li, K. Kamp, M. Bowen, R. Rikard, S. Cotten, and W. Peng. 2019. The use of wearable activity trackers among older adults: Focus group study of tracker perceptions, motivators, and barriers in the maintenance stage of behavior change. JMIR mHealth and uHealth 7(4):e9832.
Kruk, M. E., D. Porignon, P. C. Rockers, and W. Van Lerberghe. 2010. The contribution of primary care to health and health systems in low-and middle-income countries: A critical review of major primary care initiatives. Social Science & Medicine 70(6):904–911.
Kruk, M. E., G. Nigenda, and F. M. Knaul. 2015. Redesigning primary care to tackle the global epidemic of noncommunicable disease. American Journal of Public Health 105(3):431–437.
Kypridemos, C., K. Allen, G. L. Hickey, M. Guzman-Castillo, P. Bandosz, I. Buchan, S. Capewell, and M. O’Flaherty. 2016. Cardiovascular screening to reduce the burden from cardiovascular disease: Microsimulation study to quantify policy options. BMJ 353.
Loveys, K., M. Prina, C. Axford, Ò. R. Domènec, W. Weng, E. Broadbent, S. Pujari, H. Jang, Z. A. Han, and J. A. Thiyagarajan. 2022. Artificial intelligence for older people receiving long-term care: A systematic review of acceptability and effectiveness studies. The Lancet Healthy Longevity 3(4):e286–e297.
Lozano, R., M. Naghavi, K. Foreman, S. Lim, K. Shibuya, V. Aboyans, J. Abraham, T. Adair, R. Aggarwal, and S. Y. Ahn. 2012. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the global burden of disease study 2010. The Lancet 380(9859):2095–2128.
Luyckx, V. A., Z. Al-Aly, A. K. Bello, E. Bellorin-Font, R. G. Carlini, J. Fabian, G. Garcia-Garcia, A. Iyengar, M. Sekkarie, and W. Van Biesen. 2021. Sustainable Development Goals relevant to kidney health: An update on progress. Nature Reviews Nephrology 17(1):15–32.
Masters, R., E. Anwar, B. Collins, R. Cookson, and S. Capewell. 2017. Return on investment of public health interventions: A systematic review. Journal of Epidemiology and Community Health 71(8):827–834.
Mendelsohn, A. R., and J. W. Larrick. 2013. Sleep facilitates clearance of metabolites from the brain: Glymphatic function in aging and neurodegenerative diseases. Rejuvenation Research 16(6):518–523.
Miranda, J. J., T. Barrientos-Gutierrez, C. Corvalan, A. A. Hyder, M. Lazo-Porras, T. Oni, and J. C. Wells. 2019. Understanding the rise of cardiometabolic diseases in low-and middle-income countries. Nature Medicine 25(11):1667–1679.
Morton-Chang, F., S. Majumder, and W. Berta. 2021. Seniors’ campus continuums: Local solutions for broad spectrum seniors care. BMC Geriatrics 21(1):1–23.
Murphy, K. M., and R. H. Topel. 2006. The value of health and longevity. Journal of Political Economy 114(5):871–904.
Musumeci, M., M. Ammula, and R. Rudowitz. 2021. Voices of paid and family caregivers for Medicaid enrollees receiving HCBS. Kaiser Family Foundation. https://www.kff.org/medicaid/issue-brief/voices-of-paid-and-family-caregivers-for-medicaid-enrollees-receiving-hcbs (accessed May 2, 2022).
Muth, C., J. Blom, S. Smith, K. Johnell, A. Gonzalez‐Gonzalez, T. Nguyen, M. S. Brueckle, M. Cesari, M. Tinetti, and J. Valderas. 2019. Evidence supporting the best clinical management of patients with multimorbidity and polypharmacy: A systematic guideline review and expert consensus. Journal of Internal Medicine 285(3):272–288.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2016. Families caring for an aging America. Washington, DC: The National Academies Press.
NASEM. 2021. Implementing high-quality primary care: Rebuilding the foundation of health care. Washington, DC: The National Academies Press.
Obermeyer, Z., B. Powers, C. Vogeli, and S. Mullainathan. 2019. Dissecting racial bias in an algorithm used to manage the health of populations. Science 366(6464):447–453.
OECD (Organisation for Economic Co-operation and Development). 2020. Pensions at a glance 2019: OECD and G20 indicators. https://www.oecd-ilibrary.org/social-issues-migration-health/pensions-at-a-glance-2019_b6d3dcfc-en (accessed May 2, 2022).
OECD. 2021. Public and private sector relationships in long-term care and healthcare insurance. https://www.oecd.org/daf/fin/insurance/Public-and-Private-Sector-Relationships-in-Long-term-Care-and-Healthcare-Insurance.pdf (accessed May 2, 2022).
Ohnsorge, F., and S. Yu. 2021. The long shadow of informality: Challenges and policies. Washington, DC: World Bank.
Rada, A. G. 2012. Primary care in Spain is underfunded and unattractive, says report. BMJ 344:e2508.
Reinhard, S., L. F. Feinberg, A. Houser, R. Choula, and M. Evans. 2019. Valuing the invaluable: 2019 update charting a path forward. AARP Public Policy Institute. https://www.aarp.org/ppi/info-2015/valuing-the-invaluable-2015-update.html (accessed May 2, 2022).
Reuben, D. B. 2009. Better ways to care for older persons: Is anybody listening? Journal of the American Geriatrics Society 57(12):2348–2349.
Rofman, R., and I. Apella. 2020. When we’re sixty-four: Opportunities and challenges for public policies in a population-aging context in Latin America. International Development in Focus. Washington, DC: World Bank. https://openknowledge.worldbank.org/handle/10986/34562 (accessed July 12, 2022).
Salomon, J. A., T. Vos, D. R. Hogan, M. Gagnon, M. Naghavi, A. Mokdad, N. Begum, R. Shah, M. Karyana, and S. Kosen. 2012. Common values in assessing health outcomes from disease and injury: Disability weights measurement study for the Global Burden of Disease Study 2010. The Lancet 380(9859):2129–2143.
Sanford, A. M., M. Orrell, D. Tolson, A. M. Abbatecola, H. Arai, J. M. Bauer, A. J. Cruz-Jentoft, B. Dong, H. Ga, and A. Goel. 2015. An international definition for “nursing home.” Journal of the American Medical Directors Association 16(3):181–184.
Sekisui House. 2021. Sekisui House sustainability report. https://www.sekisuihouse.co.jp/english/company/sustainable/2021 (accessed May 2, 2022).
Sierra, F. 2016. The emergence of geroscience as an interdisciplinary approach to the enhancement of health span and life span. Cold Spring Harbor Perspectives in Medicine 6(4):a025163.
Stephen, R., K. Hongisto, A. Solomon, and E. Lönnroos. 2017. Physical activity and Alzheimer’s disease: A systematic review. The Journals of Gerontology: Series A 72(6):733–739.
Taillie, L. S., M. Bercholz, B. Popkin, M. Reyes, M. A. Colchero, and C. Corvalán. 2021. Changes in food purchases after the Chilean policies on food labelling, marketing, and sales in schools: A before and after study. The Lancet Planetary Health 5(8):e526–e533.
Tinetti, M. E., and T. Fried. 2004. The end of the disease era. The American Journal of Medicine 116(3):179–185.
Tolson, D., Y. Rolland, S. Andrieu, J.-P. Aquino, J. Beard, A. Benetos, G. Berrut, L. Coll-Planas, B. Dong, and F. Forette. 2011. International Association of Gerontology and Geriatrics: A global agenda for clinical research and quality of care in nursing homes. Journal of the American Medical Directors Association 12(3):184–189.
Tsega, M., C. Lewis, D. McCarthy, T. Shah, and K. Coutts. 2017. Review of evidence for health-related social needs interventions. Journal of Preventive Medicine 53(5):719–729.
UN DESA (United Nations Department of Economic and Social Affairs). 2022. Transforming our world: The 2030 agenda for sustainable development. https://sdgs.un.org/2030agenda (accessed April 1, 2022).
UN Statistics Division. 2021. Titchfield Group on ageing-related statistics and age-disaggregated data. https://unstats.un.org/unsd/methodology/citygroups/Titchfield.cshtml (accessed April 6, 2022).
West Side Rag. 2021. Seniors can get $9 bag of fresh food from local farms at six UWS spots. https://www.westsiderag.com/2021/10/09/seniors-can-get-9-bag-of-fresh-food-from-local-farms-at-six-uws-spots (accessed July 12, 2022).
WHO (World Health Organization). 2003. WHO framework convention on tobacco control. Geneva, Switzerland: World Health Organization.
WHO. 2010a. A conceptual framework for action on the social determinants of health. Geneva, Switzerland: World Health Organization.
WHO. 2010b. Telemedicine: Opportunities and developments in member states. Geneva, Switzerland: World Health Organization.
WHO. 2012. Dementia: A public health priority. Geneva, Switzerland: World Health Organization.
WHO. 2013. WHO methods and data sources for global burden of disease estimates 2000–2011. Geneva, Switzerland: World Health Organization.
WHO. 2014. The case for investing in public health: A public health summary report for EPHO 8. Copenhagen, Denmark: World Health Organization Regional Office for Europe.
WHO. 2015a. WHO global strategy on people-centred and integrated health services: Interim report. Geneva, Switzerland: World Health Organization.
WHO. 2015b. World report on ageing and health. Geneva, Switzerland: World Health Organization.
WHO. 2019. Life expectancy and healthy life expectancy by World Bank Income Group. https://apps.who.int/gho/data/view.main.SDG2020LEXWBv?lang=en (accessed December 15, 2021).
WHO. 2020a. Decade of healthy ageing: Baseline report. Geneva, Switzerland: World Health Organization.
WHO. 2020b. Global report on health data systems and capacity, 2020. Geneva, Switzerland: World Health Organization.
WHO. 2021. Elder abuse. https://www.who.int/news-room/fact-sheets/detail/elder-abuse (accessed March 1, 2022).
WHO. 2022a. Integratedcare for older people (ICOPE). https://www.who.int/teams/maternal-newborn-child-adolescent-health-and-ageing/ageing-and-health/integrated-care-for-older-people-icope (accessed May 2, 2022).
WHO. 2022b. Premature mortality from noncommunicable disease. The Global Health Observatory. https://www.who.int/data/gho/indicator-metadata-registry/imr-details/3411 (accessed May 2, 2022).
WHO. 2022c. The 10 essential public health operations. https://www.euro.who.int/en/health-topics/Health-systems/public-health-services/policy/the-10-essential-public-health-operations (accessed May 10, 2022).
World Bank. 2016. Live long and prosper: Aging in east Asia and Pacific. Washington, DC: World Bank.
World Bank. 2021. Out-of-pocket expenditure per capita (current US$). https://data.worldbank.org/indicator/SH.XPD.OOPC.CH.ZS (accessed December 15, 2021).
















































