
1
Introduction
Advances in science and technology targeting human longevity have proven that the way people age is not predetermined but malleable. Healthy longevity is defined in this report as follows:
In healthy longevity, years of good health approach the biological life span, with physical, cognitive, and social functioning that enables well-being.
As they age, more people in every country around the globe have the potential to live healthy lives, supporting a vision that people of all ages can live with meaning, purpose, and dignity. People can stay engaged with their families and communities, contribute to society, and lead enjoyable and productive lives well into their older years. The promise of extending the number of years lived in good health to accord with the increased life span achieved globally over the past century is closer to being realized than ever before. To achieve healthy longevity, a universal goal all societies need to be redesigned to support longer, healthier lives.
Health systems have generally been built to treat diseases. In many high-income countries, the heavy emphasis on acute- and hospital-centered care is poorly suited to promoting healthy longevity through prevention, screening, and management of chronic conditions. Middle- and low-income countries that are building health systems as their now young populations age can learn from and avoid the challenges faced by high-income countries today by thoughtfully balancing their limited resources between health promotion and health care to treat illness.
Across all countries, socioeconomic infrastructure supporting work and education typically emphasize achievements during the early years of life. And many physical environments are largely dominated by construction designed for able-bodied people living in the mid-20th century. Evidence shows that changes can be made to these systems to support healthier lives from birth to death. But unanswered questions remain about how to close the gap between current achievements in health and a vision of healthy longevity. Research is still needed to inform the specific configuration of such changes especially in the context of low- and middle-income countries. But incremental, concrete, evidence-based steps can be taken by governments, private-sector organizations, and communities around the world. This report sets out a roadmap including long-term goals and evidence-based recommendations for achieving those goals to move toward a future of global healthy longevity.
THE STATE OF DEMOGRAPHIC CHANGE GLOBALLY
Significant gains in longevity were achieved beginning in the 20th century in part as a result of advances in public health, including infrastructure (sanitation and water systems), food quality and safety, hygiene, immunizations and antibiotics, prenatal and maternity care, and medical care (Partridge et al., 2018). Increased physical security through protection from violence and conflict has also contributed to longer lives. In some countries, longevity has been driven by improved labor conditions and higher incomes. While these advances initially meant that more people had the opportunity to live longer, these gains in longevity have not necessarily come with similar gains in years lived in good health. On average globally, people now live longer than they did in 2000, but an increased number of people live longer with chronic conditions1 and declining function and well-being, resulting in what some call a “decompression of morbidity” (Rowe and Berkman, 2022).
The benefits of increased longevity have not been equally shared, with disadvantaged populations experiencing neither the longevity nor the health gains of more privileged populations within countries, and significant differences in longevity from country to country (Permanyer and Scholl, 2019). Much of the evidence about trends in longevity presented throughout this report predates the onset of the COVID-19 pandemic, and evidence of its impact continues to emerge. A recent study of 37 upper-middle- and high-income countries showed increased life expectancy in only three countries, no change in two countries, and decreased life expectancy in the remaining 32 countries (Islam et al., 2021). Across the countries, 28.1 million more years of life were lost than expected.
___________________
1 This report uses the term “chronic conditions” to encompass distinct chronic diseases, multimorbidity (multiple chronic conditions in the same person), and geriatric syndromes (frailty, sarcopenia, polypharmacy, cognitive decline, disability, and falls) (Inouye et al., 2007).
Future trends in life expectancy are uncertain, and many trends described in this report (e.g., life expectancy, health status, employment trends) are in flux as a result of COVID-19.
Today the global population is projected to age rapidly as the result of two distinct trends: the rise in longevity and falling birth rates. Nearly 20 percent of the global population is estimated to be over age 65 by 2050, double the percentage in 2019, while the population aged 15–65 is predicted to rise by 20 percent. The contours of demographic change will be unique to each country and population around the world. Figures 1-1 through 1-3 show the dramatic rise in the population aged 65 and older as a percentage of the population in 1950, 2000, and 2050 (projected) in the world, Singapore, and Nigeria (note that the scales of the figures differ because of the dramatic differences in total population) (UN DESA, 2019a). The models show that the population of older people is increasing, but the patterns of population growth and aging over time differ, as indicated by the horizontal and vertical shapes of the graphs, respectively.2 Typically, the wealthiest nations are furthest along in this demographic transition and have the highest proportion of older people, but the number of older people living in low- and middle-income countries is higher than the number in high-income countries. While many countries, such as Nigeria, currently have a large younger population, this large young cohort is projected to become a large old cohort. Therefore, an aging society is a reality for countries across income levels, with the only question being when they will become an aging society.
Differences in age structures create different challenges among countries in the near term, such as countries in sub-Saharan Africa that face high rates of youth unemployment while many high-income countries face a shrinking workforce. A country’s challenges will drive how it allocates resources. Moreover, low- and middle-income countries will have few resources available to develop the systems needed for healthy longevity, such as health care and long-term care.
Nonetheless, to respond to this demographic shift, it will be imperative for countries to take steps, however incremental, to redesign society for longer lives, including how older people can engage with and contribute to family, community, and society.
In recent decades, the average household size in most countries has declined, and fewer people are living in multigenerational households, although this trend may have changed during the COVID-19 pandemic. In addition to these rapid demographic shifts, populations are changing, and demography will be influenced by climate change and rapid investments in information technology. Countries are also facing socioeconomic changes that are altering family structures and living arrangements, potentially putting older people at risk. Changes in fertility levels,
___________________
2 “Older people” applies to people in the second half of their life, depending on the life expectancy where they reside. As people age, the prevalence of age-related conditions climbs. The onset of age-related chronic conditions is about 10 years later in high-income versus low-income countries.
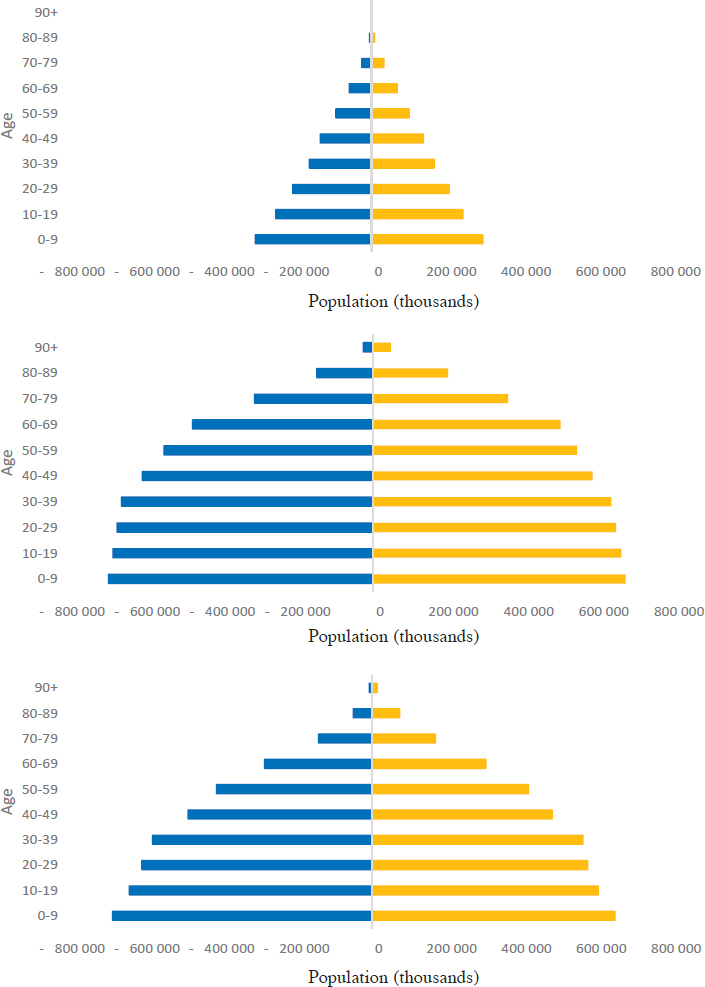
NOTE: Blue = male population; yellow = female population.
SOURCE: UN DESA, 2019a. This work is licensed under a Creative Commons Attribution 3.0 IGO License (https://creativecommons.org/licenses/by/3.0/igo).
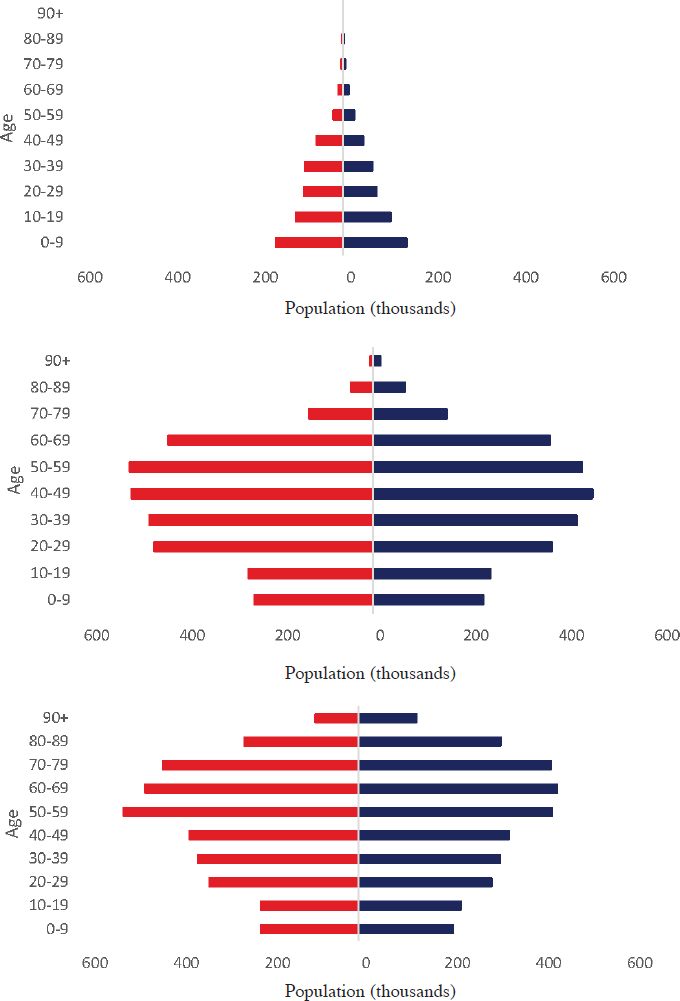
NOTE: Red = male population; dark blue = female population.
SOURCE: UN DESA, 2019a. This work is licensed under a Creative Commons Attribution 3.0 IGO License (https://creativecommons.org/licenses/by/3.0/igo).
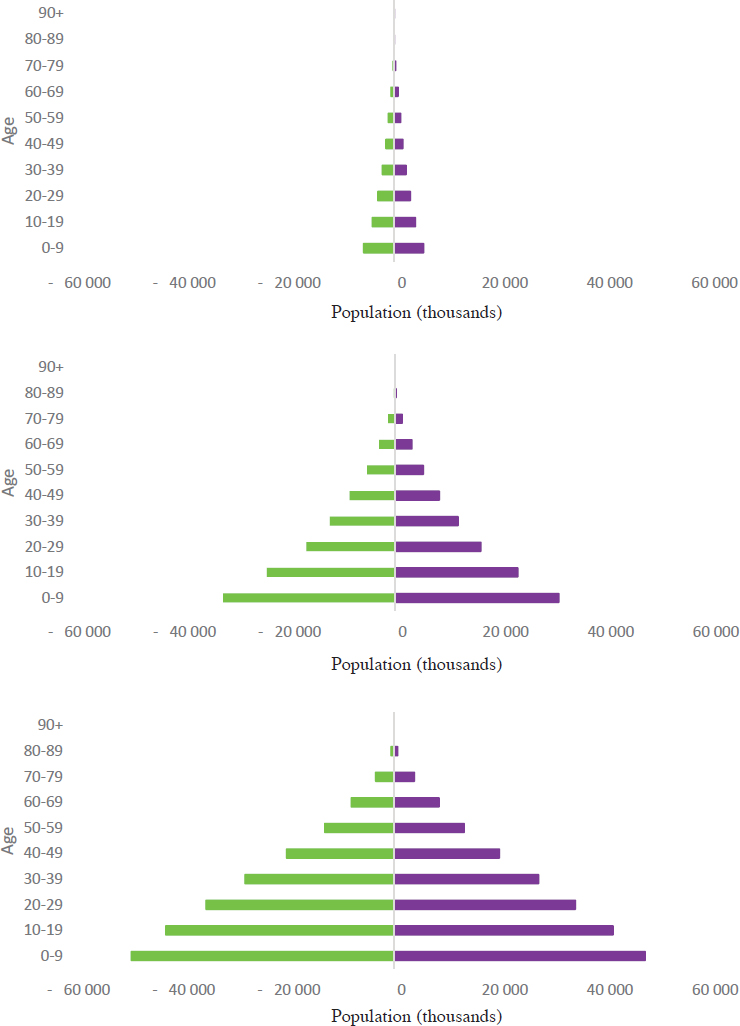
NOTE: Green = male population; purple = female population.
SOURCE: UN DESA, 2019a. This work is licensed under a Creative Commons Attribution 3.0 IGO License (https://creativecommons.org/licenses/by/3.0/igo).
marriage patterns, educational attainment, urbanization, migration, and economic development are all influencing the lives of older people (UN DESA, 2021). Living alone or with a spouse and no other family members is widely valued in many high-income countries, but it is less often valued in low- and middle-income countries. In low- and middle-income countries, those not living within a larger family unit are likely to experience worse health outcomes, higher rates of poverty, and worse quality of life (Kamiya and Hertog, 2020). These changes in family structure and living arrangements also have important and potentially detrimental ramifications for intergenerational caregiving, financial security, and social connection. In Africa and Latin America, for example, older adults and grandparents are often the caregivers for children orphaned by HIV/AIDS (He et al., 2020; UN DESA, 2019b), and there is a disconnect between older adults’ knowledge of modern medicine and basic pediatric health needs, such as vaccinations. Additionally, tension exists in some countries between older and younger people, the latter believing that older people receive a disproportionate share of jobs and government benefits (see Appendix C).
THE SCIENCE OF HEALTHY LONGEVITY
Heterogeneity of Aging and New Developments in Understanding Aging
Advances in healthy longevity are uneven among countries, among communities, and among individuals. According to the World Health Organization (WHO, 2021a), “The longer we live, the more different from each other we become, making diversity a hallmark of older age.” Over time, individuals accrue biomedical and sociological advantages or disadvantages that lead to different life trajectories, resulting in substantial heterogeneity in the rate of aging. Thus, while disease, disability, and dependency increase with advancing age, especially after age 75, differential exposures across the life course to risk factors, such as social and economic factors, cause health outcomes of older people to differ markedly. Many older people have physical and cognitive impairments as well as chronic conditions, but an increasingly large proportion of older persons function at notably high levels into advanced ages. It will be important to observe changes to these trends caused by the COVID-19 pandemic. The emerging evidence of long-term effects on infected people points to raised rates of cognitive damage and damage to other body systems, which may impact the way people age (Schou et al., 2021).
Evidence on cognitive, emotional, and motivational aging indicates that societies can benefit from supporting positive aging trends. Recent evidence suggests that cognitive decline and a weakening of information processing speed and efficiency need not be a normal part of aging. Differences among birth cohorts are substantial, yielding significant individual differences in cognitive processing (Zelinski and Kennison, 2007). The prevalence of dementia is declining, partic-
ularly in high-income countries (Langa et al., 2017; Roehr et al., 2018; Walsh et al., 2022; Wolters et al., 2020), and evidence indicates that its prevalence can be predicted by education (Tucker-Drob, 2019). In contrast to cognitive processing, knowledge increases with age, especially in expert domains. Workers in knowledge-based jobs show no evidence of reduced performance, and those in “high-knowledge” jobs see performance gains with increased age (Baltes and Staudinger, 1993; Bangen et al., 2013; Grossmann et al., 2012). Evidence suggests further that emotional experience improves with age, as documented in countries around the world (Burr et al., 2020; Carstensen et al., 2011; Stone et al., 2010; Sun and Sauter, 2021). Finally, evidence indicates that as people age, they prioritize emotional meaning, giving greater priority to important social relationships, which in turn leads to greater prosociality, whereby older people are more likely to help others and give back to society.
Also worth noting are gender differences in the adaptation to aging societies. A study on all Organisation for Economic Co-operation and Development countries using the Aging Society Index compared the status of older men and older women. After accounting for the fact that women live longer than men, findings for all countries showed advantages for older men in productivity and engagement, financial security, and intergenerational cohesion. The results for well-being and equity were mixed but still generally favored men. These gender differences have many important implications for the development of policies and programs designed to foster equitable healthy longevity (Chen et al., 2021).
The Role of Biology in Healthy Longevity
The global increase in the life span can be credited in part to advances in science, one of humanity’s greatest triumphs. In recent decades, researchers in geroscience,3 nutrition, public health, and age-related chronic conditions have identified factors that, alone and in concert, have the potential to reduce disease and improve functioning and well-being to a degree not previously understood. As one example, sleep quality and quantity, which can contribute to a number of chronic conditions, such as Alzheimer’s disease (Clark and Warren, 2013), are influenced by factors that can be manipulated, such as exposure to light and noise, as well as one’s social environment (Muzet, 2007). Similar evidence exists for the potential of physical activity, nutrition, stress reduction, medication, and technology, especially in combination, to improve health and avert age-related
___________________
3 Gerontology, geroscience, and geriatric medicine are interrelated. “Gerontology is the study of the biological, psychological, and social aspects of aging” (Birren, 1996). Geroscience, a subset of gerontology, “is an interdisciplinary field that seeks to define the biological mechanisms of aging that give rise to numerous age-related diseases and disorders” (Kaeberlein, 2017). Geriatric medicine, which is grounded in gerontological and geroscience research, “is a subspecialty of internal medicine or family medicine that deals with the complex medical and psychosocial problems of older adults” (AAMC, 2021).
conditions. It is now understood that the rate of physiological aging is malleable and not an immutable part of life (Sierra, 2016).
Aging has been called the strongest risk factor for age-related conditions (Niccoli and Partridge, 2012). Many of the causes of early mortality in 1900—primarily infectious diseases—have been replaced by a series of chronic conditions linked to aging, including atherosclerosis (leading to heart attack and stroke), some forms of cancer, osteoarthritis, osteoporosis, type 2 diabetes, Alzheimer’s disease, Parkinson’s disease, sarcopenia, glaucoma, macular degeneration, and hearing loss (Barzilai et al., 2018; Verdin, 2021). The risk for the most common chronic conditions increases exponentially with age (St Sauver et al., 2015). Research is ongoing to understand the molecular links between the aging process and the development of disease in order to identify further ways of mitigating the risk factor of age. Shifting the target from studying specific diseases in isolation to studying aging therefore holds promise for changing the orientation of medicine from an organ-focused system that treats disease to a holistic, proactive, and ultimately preventive system focused on keeping people healthy.
Biological advances can unlock life’s potential, dramatically changing the future of aging. Researchers are studying a multitude of biological pathways for slowing or even reversing the progression of aging. Some research has demonstrated the role of the environment in aging, such as the damaging effects of oxygen-rich environments on macromolecules and the effect of sunlight on joints and skin. Of particular importance, a series of genes has been identified that can exert control over the life span. Kenyon and colleagues (1993) discovered that the mutation of a single gene could induce a dramatic gain of function. Molecular biomarkers of aging may be a future avenue for evaluation of antiaging therapies in clinical trials. For example, shortened telomere length is associated with age-related conditions such as osteoporosis, cardiovascular disease, and Alzheimer’s disease (Herrmann et al., 2018). Importantly, the characteristics of aging have shifted over historical time (e.g., incidence of dementia falling, cognitive performance increasing) (Langa et al., 2017). Other advances—such as human genome editing, partial reprogramming in which aging cells are reprogrammed into pluripotent stem cells, and regenerative medicine in which cell therapy targets senescent cells rather than a disease—also promise to shift the path of aging and disease. Researchers are working to understand the nature of these mechanisms and how they can be activated most effectively.
The Role of Data and Technology in Healthy Longevity
The use of technology to increase years lived in good health represents another shift away from medicine’s traditional focus on treating disease. Technology for an aging society has undergone four waves, none of which has receded (Coughlin, 2021). The first wave resulted in assistive technologies designed to improve functionality. The second treated technology and aging as a “smart”
problem, with a focus on managing, monitoring, and motivating people’s behavior, such as through smart homes. In the current, third wave, the role of technology in aging is viewed as an economic opportunity for companies that can innovate products with the potential to incorporate vitality, functionality, activity, and fun and thus help create aging-friendly societies. In a parallel fourth wave, aging is seen as a problem of equity and inclusion that can be addressed in part by technology.
Digital technologies have the potential to improve healthy longevity at the individual and system levels. During the COVID-19 pandemic, purchases of smart speakers, tablets, and devices increased among older adults in many countries, as did their use of internet-based platforms to communicate, receive health care services, arrange for grocery deliveries, and more. These increases in older people’s uptake of technology illustrate the opportunity presented by the current digital era to implement transformative innovations to advance the creation of aging-friendly societies that meet the needs of older adults and allow them to participate actively in and enrich their communities. Digital technology also offers the potential to transform reactive health systems to make them proactive, predictive, and preventive (WHO, 2021b).
Technology presents opportunities to improve healthy longevity, but challenges will need to be addressed. One key challenge is determining the endpoints for aging and the logistics of conducting clinical trials targeting aging processes. A second challenge is ensuring equitable access to and affordability of potential treatments and technologies. A third challenge is tackling inequities, such as those related to the digital divide, and addressing underlying social and digital determinants of health (WHO, 2021b). A final challenge is avoiding the misuse of data generated by smart technology and the need to ensure that personal data are used only for the intended purposes.
AGING MYTHS AND AGEISM
Steady declines in health, physical and cognitive function, and well-being associated with aging have long been viewed as an inevitable part of life (Sierra, 2016). Many people in the later stages of life experience prolonged periods of debilitating chronic conditions, functional decline, and diminished well-being (Diehl et al., 2020). These declines have long led to perceptions that older people as a group are inevitably dependent and a drain on society, despite the fact that many live without functional limitations (Achenbaum, 2021). In numerous countries in North and South America, a majority of adults over age 65 live without serious physical or cognitive limitations, with many living independently in the community (Fausset et al., 2011; Houser et al., 2009; Rofman and Apella, 2020). Furthermore, aging brings on average more positive emotional well-being, emotional stability, and emotional complexity; an array of mature capabilities; and greater prosocial motivation (Carstensen et al., 2011).
WHO defines ageism as “when age is used to categorize and divide people in ways that lead to harm, disadvantage and injustice and erode solidarity across generations” (WHO, 2021a, p. xv). Ageism affects people of all ages and is socially accepted in a way that other forms of prejudice are not. Nonetheless, because ageism leads to discrimination and unequal treatment, “ageism shortens lives; leads to poorer physical health and worse health behaviours; impedes recovery from disability; results in poorer mental health; exacerbates social isolation and loneliness; and reduces quality of life” (WHO, 2021a, p. 48).
The COVID-19 pandemic brought to the surface deep-seated ageism in some countries, such as the United States, manifesting in intergenerational resentment toward older people.4 This resentment can be interpreted as reflecting younger people’s views of older people as a drain on the economy and government finances (see Appendix B). Even within the health care system, chronological age was used to determine some people’s access to a mechanical ventilator, despite arguments that use of chronological age to allocate scarce resources is not ethi-
___________________
4 Despite some resentment, young people across most countries made sacrifices—such as missing out on education, work, and social activities—to protect older people who were most likely to face serious harm or death if infected.
cally justifiable (Jecker and Pearlman, 1989; Joebges and Biller-Andorno, 2020; Montero-Odasso et al., 2020).
Ageism often manifests in the form of myths (see Box 1-1). While science has disproven many myths about aging that form the basis of age-based prejudice and stereotypes, the health care systems, socioeconomic structures, and policies designed around those myths have not changed. If ageism is overcome at the same time that health and function in older people improve, the inevitable shifts in population age structure and changing family structures can become drivers of a thriving society with the many positive characteristics described in this report.
REFRAMING THE CHALLENGE OF AGING SOCIETIES
Healthy longevity reframes the false assumptions that aging societies reduce workforce productivity and increase burdens on families and that older people disproportionately consume resources. A clear-eyed, evidence-informed view of the capabilities and vulnerabilities of older people points to the very real potential of aging societies to be, on balance, positive. It is important to recognize the substantial socioeconomic gradients that drive vast differences between advantaged and disadvantaged populations within and across countries. Together these observations suggest that long-lived populations are not an inherent problem for societies; rather, the problem for societies is the barriers that systematically prevent people from reaching their later years with the good health needed to thrive and contribute to family and society. To the extent that healthy longevity is accelerated on a global scale, a social resource can be developed that has never existed in human history—age-diverse societies that build on the complementarity of skills and qualities typical of both younger and older people. An evidence-based reframing of the potential of longevity suggests the need to move away from an exclusive focus on “coping with aging populations” toward removing existing barriers so the global community can age successfully and reap the economic and societal benefits of healthy older people. Accordingly, the focus of this report is on understanding how societies can create environments that provide support across the life course for people who need it while maximizing the contributions and capacities of individuals of older age.
THE COMPLEX SYSTEM OF GLOBAL HEALTHY LONGEVITY
Based on the evidence provided in this report, the commission argues that healthy longevity, or the lack thereof, is the result of the interactions of complex systems. To achieve the vision for healthy longevity described in the next chapter, multiple systems within society will need to be activated, transformed, and coordinated because healthy longevity is about all aspects of life. Advances in medicine have lengthened human life by preventing and treating diseases and developing
systems to better control for the multitude of factors that influence human health. As discussed throughout this report, however, a person’s health is determined by social context, environment, and public health as experienced throughout life, in addition to biology and health care. Socioeconomic determinants of health, such as income security, education, and work, are critical drivers of healthy longevity.
While people are living longer, they are experiencing longer periods in poor health. No country or society has implemented a system that maximizes the potential of healthy older people and has achieved healthy longevity across the population. Too often, the systems influencing healthy longevity operate in isolation from one another. Diverse systems such as public health, income security, and a healthy environment are generally not connected by a goal of achieving healthy longevity for populations. A paradigm shift is needed to capitalize on opportunities lost when societies fail to maximize contributions from all people.
In making widespread change addressing all of these elements of a complex system, effort must be directed to reducing current and preventing further disparities between, within, and across countries. In many low-income countries, making breakthrough scientific advances in aging widely available to all citizens may not be achievable while also attending to, for example, gains in providing primary education. In middle- and high-income countries, trade-offs will also need to be considered in determining how best to achieve healthy longevity for all people. With more than half of the World Economic Forum’s top 10 global risks in 2022 focused on environmental risks, resources are limited for making these broad systems changes (WEF, 2022). Nevertheless, the commission believes that the overall condition of a complex social, economic, and environmental system requires multipronged solutions to be devised and implemented by communities at the local level while being coordinated at the national and regional levels. By aligning efforts, activating all parts of society, and intentionally focusing on the interactions and relationships among these systems, the commission believes progress can be made toward developing healthier, longer lives for people around the world.
THE NATIONAL ACADEMY OF MEDICINE’S HEALTHY LONGEVITY GLOBAL GRAND CHALLENGE: CHARGE AND APPROACH
The National Academy of Medicine’s (NAM’s) Healthy Longevity Global Grand Challenge is a worldwide movement initiated in 2018 to improve physical, mental, and social well-being for people as they age. The aims of the initiative are to (1) comprehensively address the challenges and opportunities presented by global population aging; (2) catalyze breakthrough ideas and research that will extend the human health span; (3) generate transformative and scalable innovations worldwide; and (4) build a broad ecosystem of support by enabling
scientists, engineers, innovators, entrepreneurs, health leaders, policy makers, and the public to work together to achieve the promise of healthy longevity. Indeed, the commission approached the report with the goal of changing the perspectives of leaders across the public and private sectors to make an evidence-based case for achieving healthy longevity. Primary audiences for this report include leaders of health systems, employers, unions, nongovernmental organizations, faith institutions, and the news media. The report may also have applications for families and individuals seeking to learn more about the possibilities of healthy longevity and the opportunities to catalyze change in their communities.
In choosing to focus on healthy longevity, NAM recognized the convergence of multiple factors that have placed society on a precipice between an optimistic future of healthy longevity and avoidable disability and social challenges. These factors include the following:
- rising numbers of older adults globally compared with other age segments within the population, with rapidly rising numbers of older adults in many countries;
- rising rates of age-related chronic illnesses that, absent changes from the current trajectory, will increasingly burden individuals, families, and governments with rising health care costs;
- loss of human value, well-being, function, and dignity to disability caused by chronic illness, frailty, and cognitive decline;
- shifting family structures, dynamics, and norms within contexts of globalization, economic development, and crises and trends in urbanization and migration;
- a growing recognition that the current system of retirement, for those who are able to retire, is suboptimal for many individuals, organizations and institutions, and society as a whole;
- increasing social fraying, in some contexts, between younger and older generations;
- identification of social determinants of healthy longevity and the role of the built environment;
- evidence of the significant impacts of climate change and pollution on people across the life course; and
- a growing body of evidence demonstrating how to promote healthy longevity.
This report is the product of one of the two parts of the Grand Challenge. An international, independent, and multidisciplinary commission was charged with developing a comprehensive report assessing the challenges and opportunities presented by population aging and making evidence-based recommendations for how the challenges can be translated into opportunities for societies globally (see Box 1-2). The second part of the Grand Challenge is the Healthy Longevity
Global Competition. Through inducement prizes and awards, the initiative catalyzes transformative innovation and informs policies and priorities to advance healthy aging and longevity globally. The Global Competition is an ongoing separate activity from this report and is not discussed here in detail.
Where possible, the commission coordinated with other related global initiatives to achieve an integrated and synergistic effort. With equity as a central focus, the commission considered how evidence should inform policy and practice, innovation, financing, and monitoring metrics with respect to healthy longevity. The commission approached its work by collecting evidence across three domains: (1) social, behavioral, and environmental enablers; (2) health care systems and public health; and (3) science and technology. In three workshops, each dedicated to one of those three domains, the commission convened thought leaders from biological and behavioral sciences, medicine, health care, public health, engineering, technology, economics, and policy to identify the essential priorities and directions for improving health, productivity, and quality of life for older adults worldwide.
The commission also identified the need for consultations in two areas. First, it sought information about the state of aging from experts in global regions not adequately represented among the commission members, such as roles for older adults, filial piety, employment and retirement, and intergenerational cohesion, with an emphasis on low- and middle-income countries. Second, the commission sought information from experts in economics about how the economy and government spending affect healthy longevity and, conversely, how healthy longevity has the potential to affect the economy and government spending. Commissioners and NAM staff identified and invited experts to provide responses to targeted questions either in writing or during a brief discussion with staff (see Appendix C).
The commission used a “future-back vision” approach5 to imagine a world in 2050 in which healthy longevity is a reality. This approach entails first an unrestrained imagining of what the future could look like based on the evidence, and then articulation of the steps needed to reach that vision. The future-back approach contrasts with the more common “present-forward” approach, whereby imagination is limited to evolution of the current state. Given that the society and systems of today were designed for lives much shorter than the current life span, the commission recognized the need for redesign to look across systems and reflect the vision of a future unconstrained by the status quo. Once imagined, the future-back vision is deconstructed to provide a roadmap of targets starting from the present and working toward the ideal future. Planning entails consid-
___________________
5 The future-back approach originated in the method of “backward-looking analysis,” used in the energy field and described in Amory Lovins’s Foreign Affairs article on energy strategy (Lovins, 1974). Subsequently, the approach was termed “backcasting” in several studies beginning in 1982 (Dreborg, 1996; Holmberg and Robert, 2011; Robinson, 1982). Backcasting, now synonymous with the future-back approach, has since expanded beyond the sustainability, energy, and urban planning fields to include such fields as economics; strategic business consulting; and, to a limited extent, health (WHO, 2020).
ering current limitations and barriers; identifying priority areas; and developing strategies, policies for implementation, and measures of success. By detailing the new future and specific targets for attaining it, including actionable goals, the approach ensures a continued focus on the end goal—the realized vision of a future of healthy longevity.
The commission met numerous times over the course of the study and collected and assessed research from a range of fields relevant to healthy longevity. This report also builds on and is consistent with previous reports of WHO, including Decade of Healthy Ageing Baseline Report (2021c); the United Nations, including Political Declaration and Madrid International Plan of Action on Ageing (2002); and the National Academies, such as Social Isolation and Loneliness in Older Adults: Opportunities for the Health Care System (2020), Aging and Disability: Beyond Stereotypes to Inclusion: Proceedings of a Workshop (2018), Nutrition Across the Lifespan for Healthy Aging: Proceedings of a Workshop (2017a), Communities in Action: Pathways to Health Equity (2017b), Understanding Pathways to Successful Aging: How Social and Behavioral Factors Affect Health at Older Ages: Workshop in Brief (2015), and Retooling for an Aging America: Building the Health Care Workforce (IOM, 2008), among others.
A HEALTHY LONGEVITY ROADMAP
Currently, the world is unprepared to address the challenges of rapid global aging and has not been able to translate this disruptive change into opportunity (He et al., 2016). Countries with the largest proportion of older people are experiencing many undesirable outcomes related to aging, including negative economic impacts, with increasing numbers of people leaving the workforce and rapidly rising health and social care costs, as well as increases in social isolation, loneliness, and suicide rates (Bloom et al., 2015; Holt-Lunstad et al., 2010; NASEM, 2020). Many of these negative outcomes will impact all countries, even those with a slower aging trajectory and younger populations. Specifically, the rise in chronic conditions, which develop about a decade earlier in low-income countries than high-income countries (see Chapter 6), will contribute to increased health and social care costs in all countries. If not addressed, avoidable or modifiable age-related decline that impairs health, function, and well-being will continue to burden older people and their families. Younger people may live with fear and trepidation with respect to their own aging. Societies will bear avoidable care costs, and humanity will lose the benefits that could have been realized from the contributions of older people with healthy longevity.
Demographic aging can be translated into a better world for all with thoughtful, strategic change. Science can provide direction for action that societies around the world can take to seize the opportunity to prepare for a future in which healthy longevity is realized for all people. This report is grounded in the belief that healthy longevity can initiate and perpetuate the virtuous cycle depicted in Figure 1-4. Healthy longevity enables health and productive engagement
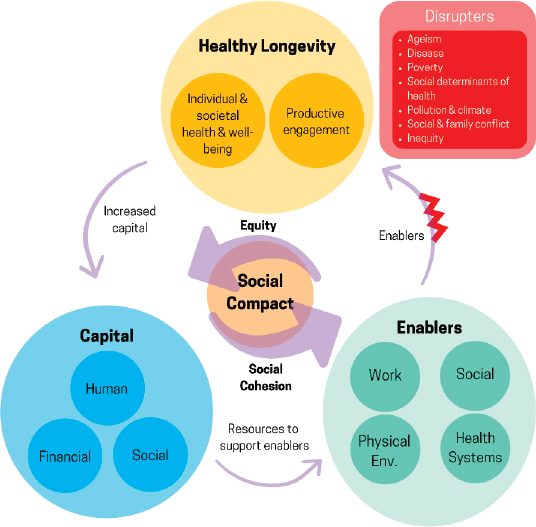
throughout the life course; the benefits of healthy longevity build social, human, and economic capital; these expanded resources allow governments to ensure that healthy longevity is sustained by supporting enablers that stem from the health system, work, volunteering, socioeconomic conditions, and the physical environment; and the cycle repeats. At the center of this cycle is a new social compact driven by equity and social cohesion.
REPORT STRUCTURE
This report, the culmination of efforts summarized above, describes the significant untapped human potential of older people within society, as well as the benefits that would accrue to individuals and society if this potential were to be unleashed. It provides evidence-based recommendations for how countries can pursue an optimistic vision of healthy longevity for individuals and societies, a vision whereby prolonged periods of functional and cognitive decline as people age are no longer viewed as inevitable. This is also a vision of a cohesive, productive society that supports the aspirations of people in the first and second halves of life. Public- and private-sector organizations and institutions can use the findings, conclusions, and recommendations in this report to shape a future
of healthy longevity by 2050 that is appropriate to a variety of cultural norms, stages of development, maturity of care systems, and resources.
The commission emphasizes cross-cutting themes across all chapters of the report. These themes include equity and nondiscrimination, lessons learned from the COVID-19 pandemic, and science and technology as enablers of healthy longevity. The importance of a life-course approach to healthy longevity is a central recurring theme; it is impossible to separate healthy longevity in older adults from what has affected them in younger years.
Following this introduction, the report is organized into six chapters. Chapter 2 presents the commission’s vision for healthy longevity in 2050. It describes an aspirational society in which healthy longevity has been achieved, based on the elements depicted in Figure 1-4. Chapter 3 describes the longevity dividend that would result from longer, healthier lives and the “capital”—human, financial, and social—that can result from healthy longevity, as seen in the bottom-left portion of Figure 1-4. Social enablers, physical environment enablers, and health systems—the enablers in the bottom-right portion of Figure 1-4—are discussed in Chapters 4 through 6, respectively. Finally, Chapter 7 presents the commission’s roadmap for achieving its vision of healthy longevity.
This report is offered as a roadmap for all countries to begin a process of engagement and shared learning across all sectors and all actors in the global community as they develop plans and programs to ensure healthy longevity. The report necessarily relies heavily on evidence from and experience of high-income countries. The majority of the evidence on healthy longevity was developed within and for high-income countries. The experience of addressing rapid aging, to date, has happened primarily in high-income countries. The commission selected targets that, with few exceptions, are relevant to all countries.
REFERENCES
AAMC (Association of American Medical Colleges). 2021. Geriatric medicine. https://www.aamc.org/cim/explore-options/specialty-profiles/geriatric-medicine-0 (accessed February 23, 2021).
Achenbaum, W. 2021. Dr. Robert Butler’s legacy in defining and fighting ageism. University of Toronto Quarterly 90(2):80–95.
Backes-Gellner, U., U. Keil, and J. Baumert. 2010. More years, more life: Recommendations of the Joint Academy Initiative on Aging. Halle, Germany: Deutsche Akademie der Naturforscher Leopoldina.
Baltes, P. B., and U. M. Staudinger. 1993. The search for a psychology of wisdom. Current Directions in Psychological Science 2(3):75–81.
Bangen, K. J., T. W. Meeks, and D. V. Jeste. 2013. Defining and assessing wisdom: A review of the literature. The American Journal of Geriatric Psychiatry 21(12):1254–1266.
Barzilai, N., A. M. Cuervo, and S. Austad. 2018. Aging as a biological target for prevention and therapy. Journal of the American Medical Association 320(13):1321–1322.
Birren, J. E. 1996. Encyclopedia of gerontology: Age, aging, and the aged. Vol. 1–2. Cambridge, MA: Academic Press.
Bloom, D. E., S. Chatterji, P. Kowal, P. Lloyd-Sherlock, M. McKee, B. Rechel, L. Rosenberg, and J. P. Smith. 2015. Macroeconomic implications of population ageing and selected policy responses. The Lancet 385(9968):649–657.
Burr, D. A., J. J. Castrellon, D. H. Zald, and G. R. Samanez-Larkin. 2020. Emotion dynamics across adulthood in everyday life: Older adults are more emotionally stable and better at regulating desires. Emotion 21:453–464.
Carstensen, L. L., B. Turan, S. Scheibe, N. Ram, H. Ersner-Hershfield, G. R. Samanez-Larkin, K. P. Brooks, and J. R. Nesselroade. 2011. Emotional experience improves with age: Evidence based on over 10 years of experience sampling. Psychology and Aging 26(1):21.
Chen, C., K. Maung, J. W. Rowe, T. Antonucci, L. Berkman, A. Börsch-Supan, L. Carstensen, D. P. Goldman, L. Fried, and F. Furstenberg. 2021. Gender differences in countries’ adaptation to societal ageing: An international cross-sectional comparison. The Lancet Healthy Longevity 2(8):e460–e469.
Clark, C. N., and J. D. Warren. 2013. A hypnic hypothesis of Alzheimer’s disease. Neurodegenerative Diseases 12(4):165–176.
Coughlin, J. 2021. International workshop on science and technology for healthy longevity day 1. Presentation at the Global Roadmap for Healthy Longevity: Science and Technology Workshop. https://nam.edu/event/international-workshop-on-science-technology-for-healthy-longevity-day-1 (accessed April 25, 2022).
Diehl, M., M. A. Smyer, and C. M. Mehrotra. 2020. Optimizing aging: A call for a new narrative. American Psychologist Journal 75(4):577–589.
Dreborg, K. H. 1996. Essence of backcasting. Futures 28(9):813–828.
Fausset, C. B., A. J. Kelly, W. A. Rogers, and A. D. Fisk. 2011. Challenges to aging in place: Understanding home maintenance difficulties. Journal of Housing for the Elderly 25(2):125–141.
Grossmann, I., M. Karasawa, S. Izumi, J. Na, M. E. Varnum, S. Kitayama, and R. E. Nisbett. 2012. Aging and wisdom: Culture matters. Psychological Science 23(10):1059–1066.
He, W., D. Goodkind, and P. R. Kowal. 2016. An aging world: 2015. Washington, DC: U.S. Census Bureau.
He, W., I. Aboderin, and D. Adjaye-Gbewonyo. 2020. Africa aging: 2020. Washington, DC: U.S. Government Printing Office.
Herrmann, M., I. Pusceddu, W. März, and W. Herrmann. 2018. Telomere biology and age-related diseases. Clinical Chemistry and Laboratory Medicine 56(8):1210–1222.
Holmberg, J., and K. H. Robert. 2011. Backcasting—A framework for strategic planning. International Journal of Sustainable Development & World Ecology 7(4):291–308.
Holt-Lunstad, J., T. B. Smith, and J. B. Layton. 2010. Social relationships and mortality risk: A meta-analytic review. PLoS Medicine 7(7):e1000316.
Houser, A. N., W. Fox-Grage, and M. J. S. Gibson. 2009. Across the states: Profiles of long-term care and independent living. Washington, DC: AARP Public Policy Institute.
Inouye, S. K., S. Studenski, M. E. Tinetti, and G. A. Kuchel. 2007. Geriatric syndromes: Clinical, research, and policy implications of a core geriatric concept. Journal of the American Geriatrics Society 55(5):780–791.
IOM (Institute of Medicine). 2008. Retooling for an aging America: Building the health care workforce. Washington, DC: The National Academies Press. https://doi.org/10.17226/12089.
Islam, N., D. A. Jdanov, V. M. Shkolnikov, K. Khunti, I. Kawachi, M. White, S. Lewington, and B. Lacey. 2021. Effects of COVID-19 pandemic on life expectancy and premature mortality in 2020: Time series analysis in 37 countries. BMJ 375:e066768.
Jecker, N. S., and R. A. Pearlman. 1989. Ethical constraints on rationing medical care by age. Journal of the American Geriatrics Society 37:1067–1075.
Joebges, S., and N. Biller-Andorno. 2020. Ethics guidelines on COVID-19 triage—An emerging international consensus. Critical Care 24(201).
Kaeberlein, M. 2017. Translational geroscience: A new paradigm for 21st century medicine. Translational Medicine of Aging 1:1–4.
Kamiya, Y., and S. Hertog. 2020. Measuring household and living arrangements of older persons around the world: The United Nations database on the households and living arrangements of older persons. Technical paper no. 3. Population Division, Department of Economic and Social Affairs. New York: United Nations.
Kenyon, C., J. Chang, E. Gensch, A. Rudner, and R. Tabtiang. 1993. A C. elegans mutant that lives twice as long as wild type. Nature 366(6454):461–464.
Langa, K. M., E. B. Larson, E. M. Crimmins, J. D. Faul, D. A. Levine, M. U. Kabeto, and D. R. Weir. 2017. A comparison of the prevalence of dementia in the United States in 2000 and 2012. JAMA Internal Medicine 177(1):51–58.
Lovins, A. 1974. Energy strategy: The road not taken? Foreign Affairs. https://www.foreignaffairs.com/articles/united-states/1976-10-01/energy-strategy-road-not-taken (accessed February 23, 2021).
Montero-Odasso, M., D. B. Hogan, R. Lam, K. Madden, C. MacKnight, F. Molnar, and K. Rock-wood. 2020. Age alone is not adequate to determine health-care resource allocation during the COVID-19 pandemic. Canadian Geriatrics Journal 23(1):152–154. https://doi.org/10.5770/cgj.23.452.
Muzet, A. 2007. Environmental noise, sleep and health. Sleep Medicine Reviews 11(2):135–142.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2015. Understanding pathways to successful aging: How social and behavioral factors affect health at older ages: Workshop in brief. Washington, DC: The National Academies Press. https://doi.org/10.17226/21815.
NASEM. 2017a. Nutrition across the lifespan for healthy aging: Proceedings of a workshop. Washington, DC: The National Academies Press. https://doi.org/10.17226/24735.
NASEM. 2017b. Communities in action: Pathways to health equity. Washington, DC: The National Academies Press. https://doi.org/10.17226/24624.
NASEM. 2018. Aging and disability: Beyond stereotypes to inclusion: Proceedings of a workshop. Washington, DC: The National Academies Press. https://doi.org/10.17226/25029.
NASEM. 2020. Social isolation and loneliness in older adults: Opportunities for the health care system. Washington, DC: The National Academies Press. https://doi.org/10.17226/25663.
Niccoli, T., and L. Partridge. 2012. Ageing as a risk factor for disease. Current Biology 22(17):R741–R752.
Partridge, L., J. Deelen, and P. E. Slagboom. 2018. Facing up to the global challenges of ageing. Nature 561(7721):45–56.
Permanyer, I., and N. Scholl. 2019. Global trends in lifespan inequality: 1950-2015. PloS One 14(5):e0215742.
Robinson, J. 1982. Energy backcasting: A proposed method of policy analysis. Energy Policy 10(4):337–344.
Roehr, S., A. Pabst, T. Luck, and S. G. Riedel-Heller. 2018. Is dementia incidence declining in high-income countries? A systematic review and meta-analysis. Clinical Epidemiology 10:1233.
Rofman, R., and I. Apella. 2020. When we’re sixty-four: Opportunities and challenges for public policies in a population-aging context in Latin America. Washington, DC: World Bank.
Rowe, J. W., and L. Berkman. 2022. Decompression of morbidity and the workforce. Nature Aging 2(1):3–4.
Schou, T. M., S. Joca, G. Wegener, and C. Bay-Richter. 2021. Psychiatric and neuropsychiatric sequelae of COVID-19—A systematic review. Brain, Behavior, and Immunity 97:328–348.
Sierra, F. 2016. The emergence of geroscience as an interdisciplinary approach to the enhancement of health span and life span. Cold Spring Harbor Perspectives in Medicine 6(4):a025163.
St. Sauver, J. L., C. M. Boyd, B. R. Grossardt, W. V. Bobo, L. J. F. Rutten, V. L. Roger, J. O. Ebbert, T. M. Therneau, B. P. Yawn, and W. A. Rocca. 2015. Risk of developing multimorbidity across all ages in an historical cohort study: Differences by sex and ethnicity. BMJ Open 5(2):e006413.
Stone, A. A., J. E. Schwartz, J. E. Broderick, and A. Deaton. 2010. A snapshot of the age distribution of psychological well-being in the United States. Proceedings of the National Academy of Sciences 107(22):9985–9990.
Sun, R., and D. Sauter. 2021. Sustained stress reduces the age advantages in emotional experience of older adults: Commentary on Carstensen et al. (2020). Psychological Science 32(12):2035–2041.
Tucker-Drob, E. M. 2019. Cognitive aging and dementia: A life-span perspective. Annual Review of Developmental Psychology 1:177–196.
UN (United Nations). 2002. Political declaration and Madrid international plan of action on ageing. https://www.un.org/esa/socdev/documents/ageing/MIPAA/political-declaration-en.pdf (accessed May 13, 2022).
UN DESA (Department of Economic and Social Affairs). 2019a. World population prospects. https://population.un.org/wpp/Graphs/DemographicProfiles/Pyramid/900 (accessed February 23, 2021).
UN DESA. 2019b. Living arrangements of older people around the world. Population Facts 2019(2). https://www.un.org/en/development/desa/population/publications/pdf/popfacts/PopFacts_2019-2.pdf (accessed April 25, 2022).
UN DESA. 2021. Global population growth and sustainable development. New York: United Nations Department of Economic and Social Affairs.
Verdin, E. 2021. Science and technology for healthy longevity: A workshop for the global roadmap for healthy aging. Presented at the International Workshop on Science and Technology for Healthy Longevity day 1. https://nam.edu/event/international-workshop-on-science-technology-for-healthy-longevity-day-1 (accessed April 25, 2022).
Walsh, S., I. Govia, L. Wallace, E. Richard, R. Peters, K. Anstey, and C. Brayne. 2022. A whole-population approach is required for dementia risk reduction. The Lancet Healthy Longevity 3:e6–e8.
WEF (World Economic Forum). 2022. The global risks report 2022, 17th ed. Geneva, Switzerland: World Economic Forum.
WHO (World Health Organization). 1946. Constitution of the World Health Organization. Geneva, Switzerland: World Health Organization.
WHO. 2020. For the future: Towards the healthiest and safest region: A vision for the WHO work with member states and partners in the western Pacific. Manila, Philippines: WHO Regional Office for the Western Pacific.
WHO. 2021a. Global report on ageism. Geneva, Switzerland: World Health Organization.
WHO. 2021b. Ethics and governance of artificial intelligence for health. Geneva, Switzerland: World Health Organization.
WHO. 2021c. Decade of healthy ageing: Baseline report. Geneva, Switzerland: World Health Organization.
Wolters, F. J., L. B. Chibnik, R. Waziry, R. Anderson, C. Berr, A. Beiser, J. C. Bis, D. Blacker, D. Bos, and C. Brayne. 2020. Twenty-seven-year time trends in dementia incidence in Europe and the United States: The Alzheimer Cohorts Consortium. Neurology 95(5):e519–e531.
Zelinski, E. M., and R. F. Kennison. 2007. Not your parents’ test scores: Cohort reduces psychometric aging effects. Psychology and Aging 22(3):546.






















