
Workshop speakers offered success stories that provided lessons concerning what has worked and what has not in the fight against chronic diseases. Robert Coughlin, managing director of JLL’s life sciences group and former president and CEO of MassBio, a Massachusetts biotech consortium, described how combined efforts from clinical researchers, hospitals, the biotech industry, and funders resulted in the development of a breakthrough drug to treat cystic fibrosis (CF). Raolat Abdulai, global clinical lead for immunology and inflammation at Sanofi, discussed how new digital technologies are playing a role in the understanding and treatment of COPD and other chronic diseases. Robert Heine, a distinguished Eli Lilly Scholar, called for a new way of thinking about the treatment of chronic diseases, one in which a single drug is used to affect multiple outcomes, with obesity and the metabolic syndrome as a case study.
CYSTIC FIBROSIS
Coughlin was 30 years old and running for the Massachusetts House of Representatives when he and his wife found out that the 21-week-old fetus his wife was carrying had CF. The amniocentesis test was still relatively new at the time, and they were one of the first couples in the country to be diagnosed with a baby in utero that was going to have CF. “We were basically told we were going to have a baby in several months that was going to have a disease for which there is no cure and the life expectancy isn’t great.”
Coughlin made a decision to continue to run for the House of Representatives to do what he could to encourage medical research “because government plays a major role in creating an environment so that people can cure disease and solve unmet medical needs.” He also decided to work with the Cystic Fibrosis Foundation to raise money to invest in the innovation pipeline.
Getting involved with the Cystic Fibrosis Foundation was an eyeopening experience for him. Before that, he had assumed that doctors and scientists just cured diseases. He had not realized that it would take advocacy, fundraising, and an average of 10 years and $1 billion—or more—to
develop a new drug. His son, Bobby, was in six clinical trials before he was 6 years old. Coughlin learned firsthand how the system worked. “I realized the system wasn’t very efficient,” he said. “It didn’t work very well. The drug discovery process was hard.”
In 2007 Coughlin decided to leave the legislature and join MassBio,1 a trade organization with a mission to advance the life sciences sector in Massachusetts and improve patients’ lives. At the same time, the Cystic Fibrosis Foundation was incentivizing a variety of biotech companies to do more research on CF by making early-stage research investments to limit the risk that these companies would otherwise face. The ultimate goal, he said, was to find drugs that, instead of treating the systems of the disease, changed the course of the disease by treating its underlying cause. One focus was gene therapy; another was precision medicine.
The results have paid off for people living with CF. In October 2019 FDA approved Trikafta for the treatment of CF in patients with an F508del mutation in the cystic fibrosis transmembrane conductor regulator (CFTR) gene; those patients represent about 90 percent of all people with CF (FDA, 2019). The drug, which is a combination of three individual molecules, works by helping the protein made by the CFTR gene function more effectively.
The breakthrough drug does not help everyone with CF, but, Coughlin said, it has made an amazing difference for his son. “He has gained 25 pounds, and his lung function has gone back up to 100 percent,” he said. Although he recognized that there is still much work to be done in treating CF patients, Coughlin said he no longer has nightmares of seeing his son die.
Coughlin stated, “We’re not just talking about drugs that treat symptoms of disease. We have drugs that change the course of disease by treating the underlying cause of the disease. We have gene therapy and precision medicine, some gene therapy that is actually curing disease now, and we don’t have a health care system that can absorb those upfront costs.” The early-stage investment by the Cystic Fibrosis Foundation helped reduce some of the risk for industry to develop much-needed therapies.
Coughlin emphasized the importance of advocacy. Advocacy groups raise money and awareness of a particular disease and the importance of addressing it. “If we don’t go raise money and invest in our own early-stage research and identify mutations and help fund research moving forward, no one else is going to do it for our kids. I love doing it.”
___________________
1 For more information, see https://www.massbio.org (accessed June 29, 2021).
CHRONIC OBSTRUCTIVE PULMONARY DISEASE
Abdulai spoke about the use of digital health technology in the management of chronic diseases and also in clinical trials. If used correctly, digital health technology can help streamline health care and make it more effective, she said (Bashi et al., 2020; Morton et al., 2017). For example, diabetes can be monitored with the use of glucometers and different connected apps. Technology can also be used to manage the use of medications and monitor adherence. There are inhalers that make it possible to access whether a patient has been using them. Telemedicine is another example of using technology to manage chronic diseases. Since the COVID-19 pandemic started, Abdulai said, the number of patient visits carried out via telemedicine and telehealth applications has increased by a factor of 50 to 175, according to data from a recent report (Bestsennyy et al., 2020). Other uses of technology in chronic diseases include patient advocacy and community building, medical record management, and comorbidity monitoring and management.
If digital health technologies are to be used widely and successfully, Abdulai said, they must be able to meet specific patient needs. Chronic disease patients may have different comorbidities, be on different types of therapies, live in different environments, and have differing social determinants of health. Digital health technologies are also needed to accommodate different types of patient needs—medical, personal, emotional, and functional—as well as be able to engage patients, make patients feel efficacious in terms of their disease self-management, allow for effective communication between patients and providers, and increase overall accessibility.
With so many requirements, not all technologies are up to the task, she said. Many tools can be difficult for patients to navigate and use, which can limit their use. It is not always easy to determine which tools would be practical and applicable for individual patients. A resource that clinicians could use to help them evaluate these different tools would be beneficial, but an effective version does not currently exist, she said.
Moving from the clinic to industry, Abdulai said that biopharmaceutical companies are also using digital technologies in a large number of ways—in preclinical work, in data storage, and in the clinical/regulatory stage. She listed eight specific areas in which digital technologies are being used in the clinical research process:
- Protocol design and review;
- Site selection and startup;
- Patient recruitment;
- Operational management;
- Drug and supply logistics;
- The collection of digital biomarkers;
- Patient and outcome data management; and
- Conducting virtual trials.
Abdulai offered a case study of a digital technology designed to address an unmet need concerning physical activity in COPD patients, highlighting the role that collaboration among government, academia, industry, and patients can have in bringing treatments and technologies to market. COPD, the third leading cause of death in the United States, is a disease characterized by persistent limitation of airflow in the lungs, with symptoms that include chronic cough, sputum, and shortness of breath. Patients are often debilitated and limited in their activities because they are so short of breath, leading to a reduced quality of life. The cost of caring for COPD patients in 2020 was estimated at around $49 billion, she said (CDC, 2018).
The Physical Activity as a Crucial Patient-Reported Outcome in COPD (PROactive) project2 was designed to more effectively assess physical activity and independence in COPD patients, and to better estimate the burden of disease. The project was carried out by the Innovative Medicines Initiative (IMI)3 from 2009 to 2016.
In the case of the PROactive tool, the development of which cost was more than $15 million, the objective was to develop a method to assess physical activity objectively using a validated activity monitor, combined with a set of questions, to capture the experience with physical activity in COPD patients. Abdulai emphasized the importance of making sure that digital technologies are well validated; in particular, health equity requires that the technology be validated across populations.
To do this, the development group first worked with patient groups to create a concept of how a COPD patient experiences physical activity. How does the patient experience walking outside, doing chores, doing leisure activities, dressing, bathing? What is their breathing like? Do they get fatigued? Do they have trouble with specific activities? Do they need to take breaks or slow down or get help from others? From the resulting conceptualization, the developers created a questionnaire tailored to the experiences of COPD patients.
They then integrated that questionnaire with two digital activity monitors, the Actigraph GT3X, which is worn around the wrist as a watch, and the DynaPort MoveMonitor, which is worn around the waist. With those
___________________
2 For more information, see https://www.imi.europa.eu/projects-results/project-factsheets/pro-active (accessed July 4, 2021).
3 IMI is a European public–private partnership founded to improve health by speeding up the development of—and patient access to—innovative medicines in areas of unmet need (IMI, n.d.). It includes universities, research centers, the pharmaceutical and other industries, small and medium-size enterprises, patient organizations, and regulators.
integrated activity monitors, the researchers created two patient-reported outcome tools for capturing physical activity, a daily measure of physical activity (Daily PROactive Physical Activity in COPD, D-PPAC) and a clinical visit measure that relied on a 7-day recall of activity (Clinical Visit PROactive Physical Activity in COPD, C-PPAC). By combining the responses on the questionnaires with the measurements of the digital monitoring devices, the resulting tool makes it possible to better understand the actual disease burden of reduced physical activity and physical functioning in COPD patients, Abdulai said.
The PROactive tool can be used in clinical trial settings to assess, for example, how well a drug for COPD is improving a patient’s symptoms. This allows clinicians to move beyond simply assessing respiratory symptoms to see if a treatment is actually improving a particular patient’s physical activity and functional status—measures of quality of life. In March 2018 the tool was adopted by the European Medicines Agency’s Committee for Medicinal Products for Human Use (EMA, 2018).
In conclusion, Abdulai said digital health tools have an important role to play in the development of treatments, in clinical trials, and in health care. The development of the PROactive tool was the result of collaboration among multiple actors, including patients, to create a tool that incorporates both the traditional questionnaire and new digital tools, and that can now be used in clinical trials and beyond. She suggested that this approach to collaboration could be adopted in the United States to develop high-quality tools and treatments for prevalent chronic diseases.
INVESTING IN ONE DISEASE, APPLYING TO MULTIPLE DISEASES
The traditional approach to developing a new drug is to target one disease and test a drug against it, declaring success if it helps with that one disease. However, with so many patients experiencing comorbidities, Heine suggested that a more efficient approach might be to find one treatment that can apply to multiple diseases. In his talk he sketched out one way that might be done.
Heine discussed the obesity epidemic and the related health effects. In the United States, obesity rates have been growing since the 1970s, and it is projected that by 2030 about half of the U.S. population will be obese, that is, have a body mass index (BMI) greater than 30 (Ward et al., 2019). Estimates indicate that as many as 20 percent of all U.S. deaths are caused by obesity-related disorders (Masters et al., 2013).
Obesity and obesity-related diseases are also a growing problem in most of the rest of the world, Heine said. China is one compelling example. Average BMI has been increasing steadily, he said, and prevalence of diabetes in China has risen to 120 million people (Chan et al., 2014).
He noted that 25 percent of the global population of people with type 2 diabetes live in China. Furthermore, in just one decade the mortality rate for ischemic heart disease has quadrupled (Zhang et al., 2017), and about one-quarter of the adult population living in Shanghai are diagnosed with fatty liver (Fan et al., 2017).
Some causes of the obesity epidemic, he said, can be found in the abundance and easy availability of high-calorie foods—epitomized by fast foods—combined with a drop in average energy expenditure as people lead less active lives and use more labor-saving devices. The health implications have been deadly. Obesity leads to insulin resistance, hypertension, dyslipidemia, beta-cell dysfunction, fatty liver, and low-grade inflammation, leading in turn to a wide variety of diseases, including cardiovascular disease, hyperglycemia and diabetes, non-alcoholic steatohepatitis (NASH), cancer, chronic kidney disease, cognitive decline, and arthritis.
Metabolically, when a person becomes obese, the adipose tissue is no longer capable of taking up fatty acids and storing fat in a safe way, and the adipocytes become inflamed and start dying. Fatty acids are then stored in and around organs that are not equipped to store them, such as the liver or the heart. This in turn leads to high levels of lipids in the blood and the suite of disorders associated with metabolic syndrome—hypertension, type 2 diabetes, chronic kidney disease, atherosclerosis, and heart failure.
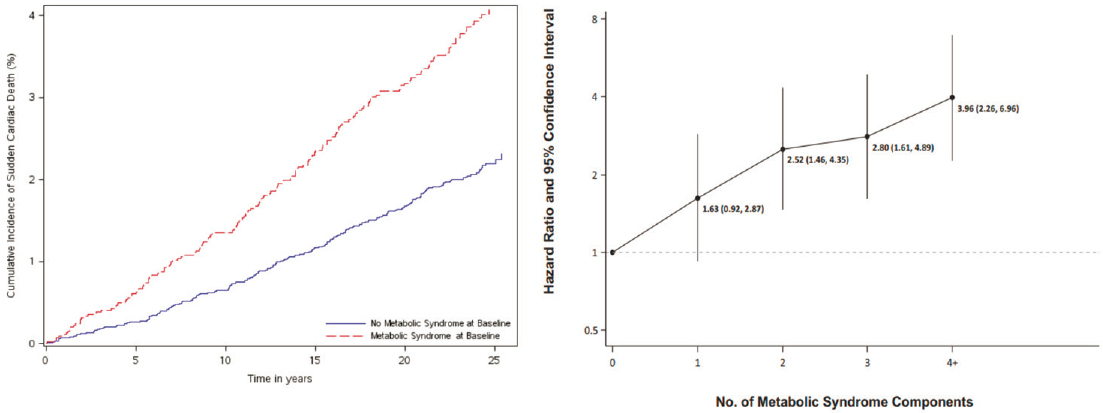
A standard way of identifying people at increased risk for these metabolic abnormalities is to look for the defining characteristics of metabolic syndrome. A person is diagnosed with metabolic syndrome when three or more of the following features are present: a large waist circumference (greater than 35 inches for women and 40 inches for men), elevated fasting glucose, elevated blood pressure (systolic greater than 130 or diastolic greater than 85), elevated serum triglycerides, and low levels of high-density lipoproteins (Huang, 2009). People with metabolic syndrome have a greater mortality risk, independent of obesity, and the risk increases with an increasing number of metabolic syndrome features (see Figure 5-1).
The goal in treating obesity or weight gain–associated metabolic disorders, Heine said, should be “to reinstitute metabolic health, which can be defined as the absence of the metabolic syndrome components.” Doing so should result in lowering the risk of developing multiple disorders related to metabolic syndrome. A therapeutic that improves overall metabolic health could also be evaluated for the treatment of specific metabolic conditions—cardiovascular disease, heart failure, diabetes, chronic kidney disease, NASH, and more—if the clinical endpoints are well defined.
One existing class of drugs has been shown to have effects on a number of these endpoints, Heine said: SGLT2 inhibitors, originally developed as glucose-lowering drugs to treat diabetes. The original clinical trial of an SGLT2 inhibitor tested its cardiovascular safety, as required by FDA.
SOURCES: Presented by Robert Heine on March 8, 2021, at the Innovation in Drug Research and Development for Prevalent Chronic Diseases workshop; Hess et al., 2017.
Researchers found a reduction in cardiovascular disease outcomes with the SGLT2 inhibitor as compared with the placebo, which was mainly attributable to a reduction in heart failure (Sharma et al., 2020). Another trial demonstrated that SGLT2 inhibitors also reduce the risks of chronic kidney disease (Perkovic et al., 2019).
A new drug that helps obese patients to reliably lose weight could similarly hold promise against multiple aspects of the metabolic syndrome. For instance, Heine said, patients who have had bariatric surgery and lost a significant percentage of body weight have seen significantly improved outcomes in terms of mortality, cardiovascular disease, and microvascular disease (Doumouras et al., 2021). Weight loss of as little as 10 percent of body mass can result in a reduction of dyslipidemia, hypertension, hyperglycemia, insulin resistance, and fatty liver, improving metabolic health (CDC, 2020).
Recently, he said, several drugs—particularly the GLP-1 agonists—have produced weight loss that can render these major benefits (Trujillo et al., 2015). Thus, they offer a potential example of developing one treatment that can have positive effects on multiple diseases and outcomes. However, he discussed three major hurdles still facing successful R&D for obesity:
- Developing obesity drugs is expensive. Several companies have ceased R&D programs in the metabolic field because they did not see a practical way forward.
- Identifying the right patient for a particular therapy can be difficult. Not every person who is obese has a metabolic syndrome or is at the same risk as others with the metabolic syndrome.
- Many people do not consider obesity to be a disease, but rather a lifestyle problem. Though lifestyle is one contributing factor, moving forward will require the destigmatization of obesity and acceptance of obesity as a disease and a major risk factor for multiple serious outcomes. Advocacy groups could potentially have a positive effect on this challenge, he said.
Heine suggested designing and carrying out studies that are focused more on total disease burden than on individual indications. For example, a single patient may be suffering from chronic kidney disease, cardiovascular disease, and diabetes, and clinical trials would ideally examine outcomes relevant to patients with comorbidities. This broader approach to drug R&D contrasts with the targeted approach on individual diseases that was suggested by Ehlert. However, both Heine and Ehlert stressed the need to understand the biology of the diseases being studied, including well-defined biomarkers and endpoints, in order to successfully evaluate the treatments being developed. Furthermore, Heine explained, as the experience with
bariatric surgery has demonstrated, it may be possible to use real-world evidence and pragmatic trials to demonstrate the effectiveness of some of these medicines. “This is a challenge,” he said, “but also an invitation to everyone to start thinking about other ways to develop drugs for this metabolic disease that poses a huge challenge to the whole society.”
REFERENCES
Bashi, N., F. Fatehi, M. Mosadeghi-Nik, M. S. Askari, and M. Karunanithi. 2020. Digital health interventions for chronic diseases: A scoping review of evaluation frameworks. BMJ Health & Care Informatics 27(1):e100066.
Bestsennyy, O., G. Gilbert, A. Harris, and J. Rost. 2020. Telehealth: A quarter-trillion-dollar post-COVID-19 reality? https://www.mckinsey.com/industries/healthcare-systems-andservices/our-insights/telehealth-a-quarter-trillion-dollar-post-covid-19-reality (accessed July 4, 2021).
CDC (Centers for Disease Control and Prevention). 2018. COPD costs. https://www.cdc.gov/copd/infographics/copd-costs.html (accessed June 29, 2021).
CDC. 2020. Losing weight. https://www.cdc.gov/healthyweight/losing_weight/index.html (accessed July 4, 2021).
Chan, J. C. N., Y. Zhang, and G. Ning. 2014. Diabetes in China: A societal solution for a personal challenge. Lancet Diabetes and Endocrinology 2(12):969–979.
Doumouras, A. G., J. A. Wong, J. M. Paterson, Y. Lee, B. Sivapathasundaram, J.-E. Tarride, L. Thabane, D. Hong, S. Yusuf, and M. Anvari. 2021. Bariatric surgery and cardiovascular outcomes in patients with obesity and cardiovascular disease. Circulation 143(15):1468–1480.
EMA (European Medicines Agency). 2018. Qualification opinion on PROactive in COPD. https://www.ema.europa.eu/en/documents/regulatory-procedural-guideline/qualificationopinion-proactive-chronic-obstructive-pulmonary-disease-copd_en.pdf (accessed June 29, 2021).
Fan, J. G., S. U. Kim, and V. W. Wong. 2017. New trends on obesity and NAFLD in Asia. Journal of Hepatology 67:862–873.
FDA (U.S. Food and Drug Administration). 2019. FDA approves new breakthrough therapy for cystic fibrosis. FDA news release. https://www.fda.gov/news-events/press-announcements/fda-approves-new-breakthrough-therapy-cystic-fibrosis (accessed May 20, 2021).
Hess, P. L., H. R. Al-Khalidi, D. J. Friedman, H. Mulder, A. Kucharska-Newton, W. R. Rosamond, R. D. Lopes, B. J. Gersh, D. B. Mark, L. H. Curtis, W. S. Post, R. J. Prineas, N. Sotoodehnia, and S. M. Al-Khatib. 2017. The metabolic syndrome and risk of sudden cardiac death: The Atherosclerosis Risk in Communities study. Journal of the American Heart Association 6(8):e006103.
Huang, P. L. 2009. A comprehensive definition for metabolic syndrome. Disease Models & Mechanisms 2(5–6):231–237.
IMI (Innovative Medicines Initiative). n.d. About IMI. https://www.imi.europa.eu/about-imi (accessed July 4, 2021).
Masters, R. K., E. N. Reither, D. A. Powers, Y. C. Yang, A. E. Burger, and B. G. Link. 2013. The impact of obesity on U.S. mortality levels: The importance of age and cohort factors in population estimates. American Journal of Public Health 103(10):1895–1901.
Morton, K., L. Dennison, C. May, E. Murray, P. Little, R. J. McManus, and L. Yardley. 2017. Using digital interventions for self-management of chronic physical health conditions: A meta-ethnography review of published studies. Patient Education and Counseling 100(4):616–635.
Perkovic, V., M. J. Jardine, B. Neal, S. Bompoint, H. J. L. Heerspink, D. M. Charytan, R. Edwards, R. Agarwal, G. Bakris, S. Bull, C. P. Cannon, G. Capuano, P.- L. Chu, D. de Zeeuw, T. Greene, A. Levin, C. Pollock, D. C. Wheeler, Y. Yavin, H. Zhang, B. Zinman, G. Meininger, B. M. Brenner, and K. W. Mahaffey. 2019. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. New England Journal of Medicine 380(24):2295–2306.
Sharma, A., N. J. Pagidipati, R. M. Califf, D. K. McGuire, J. B. Green, D. Demets, J. T. George, H. C. Gerstein, T. Hobbs, R. R. Holman, F. C. Lawson, L. A. Leiter, M. A. Pfeffer, J. Reusch, J. S. Riesmeyer, M. T. Roe, Y. Rosenberg, R. Temple, S. Wiviott, J. McMurray, and C. Granger. 2020. Impact of regulatory guidance on evaluating cardiovascular risk of new glucose-lowering therapies to treat type 2 diabetes mellitus: Lessons learned and future directions. Circulation 141(10):843–862.
Trujillo, J. M., W. Nuffer, and S. L. Ellis. 2015. GLP-1 receptor agonists: A review of head-to-head clinical studies. Therapeutic Advances in Endocrinology and Metabolism 6(1):19–28.
Ward, Z. J., S. N. Bleich, A. L. Cradock, J. L. Barrett, C. M. Giles, C. Flax, M. W. Long, and S. L. Gortmaker. 2019. Projected U.S. state-level prevalence of adult obesity and severe obesity. New England Journal of Medicine 381:2440–2450.
Zhang, X., A. A. Khan, E. U. Haq, A. Rahim, D. Hu, J. Attia, C. Oldmeadow, X. Ma, R. Ding, and A. J. Boyle. 2017. Increasing mortality from ischaemic heart disease in China from 2004 to 2010: Disproportionate rise in rural areas and elderly subjects. 438 million person-years follow-up. European Heart Journal: Quality of Care & Clinical Outcomes 3(1):47–52.
This page intentionally left blank.












