
The focus of this segment of the four-part workshop was on the elements needed to build a more resilient, sustainable, and transparent clinical trials enterprise by 2030. Participants discussed the need for convergence and integration of clinical research and clinical practice; data sharing and management; and more efficient, engaging scientific communication.
THE ROAD TO 2030: PERSPECTIVES FROM THE FIELD
Martin Landray, professor of medicine and epidemiology at the Nuffield Department of Population Health at the University of Oxford, discussed the Randomized Evaluation of COVID-19 Therapy (RECOVERY) Trial as an example to highlight the importance of conducting randomized clinical trials and demonstrate how clinical trials can be a core component of clinical care. Three panelists then shared their frontline experience addressing some of the challenges facing the clinical trials enterprise.
The “Magic” of Randomization: The RECOVERY Trial Experience
In response to the significant mortality associated with COVID-19, hundreds of different treatments were being tried in practice. There were many opinions about the value of these treatments, often based on small, inconclusive randomized trials, uncontrolled case series, and theoretical work, but reliable data supporting the use of these treatments was not available, Landray said. RECOVERY1 was designed to evaluate the efficacy of a range of interventions repurposed to treat individuals hospitalized with COVID-19 in the United Kingdom. For COVID-19, as for many other diseases, Landray said finding a single treatment that quickly cures all patients is unlikely, and large-scale randomization is required to identify effective treatments that offer modest improvements in outcomes of importance (e.g., reduced mortality).
___________________
1ClinicalTrials.gov Identifier: NCT04381936. See also https://www.recoverytrial.net (accessed July 1, 2021).
Design of the RECOVERY Trial
Three key principles were embedded within the design of RECOVERY: (1) to obtain robust results that can rapidly impact care; (2) to consider the well-being of the patients; and (3) to consider the well-being of the staff, Landray explained. The study was designed to focus strictly on identifying products that could save lives, he said. The trial entailed randomization of the relevant populations and comprehensive follow-up, as well as communication, collaboration, and broad transparency (e.g., communication with researchers, the medical community, patients, the public). Landray referred workshop participants to a recent publication in which he describes how smart trial design and streamlined operations, integrated data and technology, and flexible regulatory approaches can lead to improved patient care and public health (Collins et al., 2020).
These principles were put into practice for the launch of RECOVERY in March 2020. The relevant population to be randomized was patients who were hospitalized and believed to have COVID-19 (see Figure 5-1). Enrollment in RECOVERY was open to anyone admitted to any hospital in the United Kingdom, which Landray said enhanced diversity and inclusivity. “You cannot recruit people from diverse communities if you
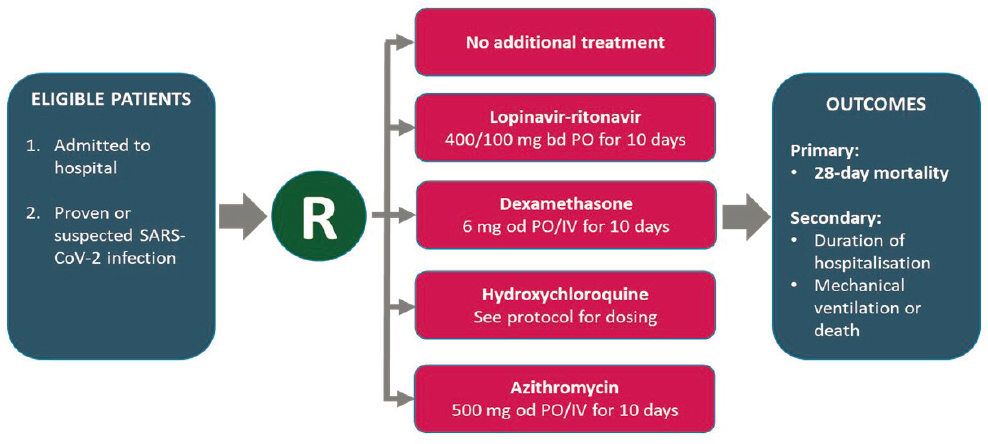
NOTES: Exclusion criteria were applied prior to randomization (e.g., if there was a contraindication for the participant to receive a particular intervention, that treatment arm would be removed as an option before randomization of that participant, which Landray said provides for an unbiased assessment of the treatments). The protocol was subsequently adapted to include multiple, factorial randomization.
NOTE: R = randomization; SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
SOURCE: Landray presentation, March 24, 2021.
don’t locate the studies in diverse locations,” he said. As a result of the simplified recruitment, enrollment, and consent processes, more than 10,000 participants were enrolled during the first 8 weeks of the study. RECOVERY continues to enroll, and Landray noted that 20,000 participants were enrolled from December 2020 through February 2021.
The primary outcome for RECOVERY was mortality. Follow-up was facilitated using a one-page, online case report form and supplemented by linkage to existing UK National Health Service (NHS) datasets on hospitalization, mortality, primary care, critical care, specific diseases, and COVID-19. Leveraging existing information reduces workload for the trialists and facilitates long-term follow-up, Landray explained. He noted that, although NHS is the primary provider of health care in the United Kingdom, data are collected in many different databases as NHS spans 4 nations, nearly 200 acute hospital organizations, and 10,000 primary care practices. As an example, he said that six different datasets were accessed for information about mortality for the primary outcome. The associated data integration challenges were significant, but worthwhile to obtain more robust information, he said.
Results from RECOVERY
Landray briefly described some of the results from RECOVERY thus far. He shared, for example, that hydroxychloroquine, lopinavir–ritonavir, and azithromycin were not shown to have a clinically meaningful benefit for hospitalized COVID-19 patients, despite having been widely recommended, promoted, and used by clinicians in the United States and many other parts of the world.
By contrast, although the use of dexamethasone was considered to be contraindicated by many doctors, the clear and compelling data from RECOVERY showed that it reduced mortality in those patients who required oxygen or ventilation. As evidence of the impact of sufficiently powered randomized trials, Landray said these results were publicized at lunchtime on June 16, 2020, and by teatime, dexamethasone treatment of hospitalized COVID-19 patients who needed oxygen or ventilation was national policy in every UK hospital.2 Other nations followed suit and it had been estimated that, at the time of the workshop, at least 600,000 lives had been saved as a result of this policy change.
As another example, Landray showed how data from RECOVERY provided clear results regarding the ability of the anti-inflammatory drug tocilizumab to reduce mortality for some COVID-19 patients with
___________________
2 See https://www.nejm.org/doi/10.1056/NEJMoa2021436 (accessed February 14, 2022).
hypoxia and inflammation, after numerous prior small studies were inconclusive.
Lessons from RECOVERY
Beyond the clinical findings, RECOVERY demonstrates how randomized trials can be a core component of quality clinical care. RECOVERY was embedded within existing hospital processes and procedures, Landray said, and on average about 10 percent of patients admitted with COVID-19 across NHS hospitals were enrolled in the trial. In addition, he discussed six takeaway lessons from RECOVERY (see Box 5-1) and said that involvement with the trial has inspired more junior doctors to want to become active in clinical research.
“Clinical trial[s are] part of good quality clinical care; they are not an optional extra,” Landray said. He emphasized that the “arbitrary use of unproven treatments is a disservice to patient care and public health,” raising false hopes, wasting resources, and missing opportunities to learn and improve care.
In closing, Landray reiterated that trials need to be feasible for trial participants and staff, inclusive, and focused on outcomes of importance to patients. Transforming to a system in which trials are part of care
requires leadership, coordination, fairness, and transparency, and creation of a culture in which clinical research is for everyone—including participants and frontline medical staff.
Frontline Experience: A Panel Discussion
Elizabeth Ofili, contact principal investigator at the Research Centers in Minority Institutions Coordinating Center, shared her perspective as a physician on integrating clinical care and clinical research to promote inclusivity and enhance the quality of care. Bárbara Segarra-Vázquez, dean of the School of Health Professions at the University of Puerto Rico, shared her perspective as a patient on what is needed to sustain the clinical trials enterprise. Freda Lewis-Hall, former senior medical advisor at Pfizer Inc. (retired), drew on her career experience in the pharmaceutical industry as she discussed building out the community-based clinical research infrastructure. The session was moderated by Chris Austin, director of the National Center for Advancing Translational Sciences (NCATS) at NIH.
Integrating Care and Research to Promote Inclusivity
The current clinical trials model is centered in academia, and there is a need to decentralize trials and engage the community and community practitioners. Until representation of certain populations and groups in trials is improved, it will be impossible to achieve health equity, Ofili said. For the clinical trials enterprise to be sustainable, it has to be worthwhile for frontline health care providers who care for predominantly underrepresented populations to participate as investigators. “Community providers are interested and want to participate,” she said, but there are practical issues to be addressed. With an innovation award from NCATS, Ofili and colleagues are working directly with some of these practitioners to overcome critical barriers to inclusivity. One barrier is the inability during a brief patient encounter to extract data from their EHR that could enhance quality of care. Combining quality care and clinical research at the point of care requires investment, she said, and providers need training on how to use the technology and platforms to extract data. Ofili also highlighted the need for metrics to track progress as new provider groups become part of the clinical trials enterprise.
Engaging Patients in the Trial Process to Drive Sustainability
As an investigator and a two-time breast cancer survivor, Segarra-Vázquez has experience on both sides of clinical trials, and she said that sustainability of the enterprise requires informing the public about trials,
listening to patients, and dispelling myths about the willingness of diverse populations to participate in trials.
“Knowledge is power,” Segarra-Vázquez said, and the public should be informed about clinical trials so they are armed with the knowledge when the opportunity to participate arises. Patients are often approached about enrolling in a clinical trial when they have just been diagnosed with a disease, or even while being prepped for a procedure. They are focused on dealing with concerns and unknowns about their future, and most have little to no familiarity with clinical trials. Grasping the information about enrolling in a trial is even more challenging for those whose native language differs from that spoken by the trial staff, and she added that learning about a trial in an unfamiliar language does not instill trust in the enterprise. Just as people are constantly learning about products through commercials, social media, and the Internet, they should be constantly learning about clinical trials, Segarra-Vázquez said. She emphasized the power of storytelling to convey information about clinical trials.
It is a myth that Latinos and other minority groups do not want to participate in clinical trials, Segarra-Vázquez said. In her experience, people in Puerto Rico want to participate and the retention rate is high. However, minorities are often not told about trials or asked to participate. She also noted the importance of having a trial coordinator and other trial staff from traditionally underrepresented communities to interact with participants.
Patients are the experts in their own disease, and should be engaged in the trial process from the start, not as an afterthought, Segarra-Vázquez said. As a patient, “We can tell you what we want, how we want it, and how it will be successful,” she said. It is especially important to ensure that diverse patients are included when collecting patient input. She noted that around 20 percent of cancer clinical trials fail to enroll as many patients as they need and close due to lack of recruitment (Korn et al., 2010). Listening to patients and “meeting the people where they are” to make trials more accessible can help to address this issue.
Envisioning and Achieving a Collaborative, Community-Based Clinical Research Infrastructure
Lewis-Hall observed that there is no master plan for transforming the clinical trials enterprise. Instead there are many different plans, and many people working “with great passion” who are making an impact, but there is no central action plan in which everyone can participate.
Drawing on her career experience in the pharmaceutical industry, Lewis-Hall suggested that a fresh, unencumbered perspective combined with the purposeful use of existing resources and networks are both
needed to build out a community-based clinical research infrastructure. Starting with an unencumbered perspective, she asked, what does the structure of a clinical trials enterprise that can serve as the national evidence-generation platform look like? What incentives, regulations, and policies are needed to support those structures? What should the clinical trials workforce of the future look like? How can the clinical care environment participate in the collection of data to answer critical research questions in times of urgent need (e.g., during a pandemic), as well as ongoing questions of interest to patients, providers, and researchers to improve care?
At the same time, how can existing networks, such as the Patient-Centered Clinical Research Network, be coordinated to support this vision for the future? As an example, Lewis-Hall mentioned the Cancer Moonshot3 approach to accelerating research, in which oncology networks are facilitating rapid, affordable oncology trials by using master protocols, platform trials, and other tools. In this regard, she said that the pharmaceutical industry is working to improve inclusion and productivity both through their actions as a collective of individual companies and through “meta-collaboration” with members of the communities the industry serves.
Overcoming Embedded Barriers to Collaboration
Austin pointed out that fundamental, curiosity-driven research forms the foundation of much of the research conducted in the United States. It is deeply embedded in an academic culture that has long rewarded individual ingenuity over the type of collaboration needed for the clinical trials enterprise envisioned for the future.
Ofili suggested that individual and institutional curiosity-driven research and collaborative, community-based research do not need to be mutually exclusive. The key is to identify “the right question to activate that curiosity” by partnering with those who know the disease or condition best, the patients, and their caregivers. Segarra-Vázquez added, “We have to train our young investigators to trust patients, talk to patients, and listen to patients.” The interconnectedness of care and research, with the patient as a driver, will begin to decentralize and democratize clinical research, benefiting both the academic institutions and the community-based practices, Ofili said. Lewis-Hall agreed and said there is an opportunity to align goals and incentives by developing clear research questions with input from patients and caregivers, academia and industry, and the
___________________
3 For more information, see https://www.cancer.gov/research/key-initiatives/moonshot-cancer-initiative (accessed August 3, 2021).
public. A practical action plan could begin with, for example, identifying the top 10 disparities in health outcomes to be addressed, the stakeholders who need to be at the table to address them, and the incentives that would inspire people to participate. Austin noted that empowering the community takes funding, and Ofili agreed that community providers involved in research need resources, guidance, and support. She added that, in her experience, community providers have innovative ideas for how to make the process of care more efficient.
THE ROAD TO 2030: VISIONS OF WHAT IS POSSIBLE
Brian Southwell, senior director of the Science in the Public Sphere Program at RTI International, discussed trust, transparency, and promoting public understanding of clinical trials. Dyan Bryson, founder and patient engagement strategist at Inspired Health Strategies, discussed facilitating the cultural change needed to support patient-centric and diverse clinical trials. Pamela Tenaerts shared insights on creating solutions and promoting trust and transparency. The session was moderated by Khair ElZarrad, deputy director of the Office of Medical Policy at FDA.
Embracing Person-Centered Communications About Clinical Trials4
A variety of factors can influence public understanding of drug research and development, Southwell said, including the salience of public information; the diffusion of misinformation; how information in the news is framed over time; existing understanding of science processes; and the state of science education. The vision of clinical trials for the future necessarily intersects with the public information environment.
Southwell described how a transformed clinical trials enterprise for 2030 might look.
- “Trials are advancing science by enrolling people who are the most directly impacted by and most directly burdened by diseases.”
- Trial enrollment is at sufficient levels and people are less hesitant to participate.
- There are “partnerships [among] trial staff, media outlets, community-based organizations, and patients,” and credible, locally relevant information is available to potential trial participants.
___________________
4 This presentation is based on a blog post titled A Future of Trusted Clinical Trials: Communication Strategies to Encourage Trust and Transparency, available at https://www.healthaffairs.org/do/10.1377/hblog20210503.292254/full (accessed July 1, 2021).
- The results of trials are readily accessible to the public and are reported and celebrated in the media for contributing to community well-being.
There are crucial steps that must be taken to realize this vision, Southwell said, and resources will be needed to achieve the desired outcomes. A core element underlying this vision is person-centered communication about clinical trials. Developing a person-centered communication approach requires an understanding of what trust and transparency mean to different people, Southwell said.
Trust
From an academic perspective, trust is often associated with a perception of intellectual credibility or competence, Southwell said. Another popular and consequential dimension of trust is a perception of reliability or consistency (i.e., an expectation that an individual or institution will behave dependably or predictably). A related dimension of trust that is particularly relevant to clinical trials, Southwell explained, is trust as a perception of shared interest (also called encapsulated interest). In this sense, trust stems from the belief that others will act in your interest and to your benefit.
“If trust is rooted in both perception of shared interest and longstanding relationships,” Southwell said, then investing in existing relationships and infrastructures would likely achieve better outcomes than launching new initiatives when, for example, working to increase diversity and inclusivity in clinical trials. In this example, trusted institutions might include the National Medical Association or Historically Black Colleges and Universities (HBCUs). Building trust between patients and the health care system can also help to counter the spread of misinformation, Southwell said.5
Transparency
Transparency is often thought of as simply making data and analyses available to others for their use. Research has shown, however, that simply making information (e.g., study results) available may not on its own guarantee public understanding, Southwell said.6 Understanding
___________________
5 Southwell referred participants to a blog post he authored for the ABIM Foundation titled Trust as an Antidote to the Viral Spread of Medical Misinformation, available at https://medium.com/@briansouthwell_94233/trust-as-an-antidote-to-the-viral-spread-of-medical-misinformation-12b0f2d3905a (accessed April 13, 2022).
6 Southwell referred participants to a blog post he authored for the Medical Care Blog titled Beyond Evidence Reporting: Evidence Translation in an Era of Uncertainty, available at https://www.themedicalcareblog.com/evidence-translation (accessed July 1, 2021).
information about clinical trials is impacted by the general level of health and science literacy, but also by the public’s ability to understand the concepts, vocabulary, acronyms, and statistics associated with research results. To facilitate transparency, Southwell said that researchers should take opportunities to translate their study data “in venues outside of peer-reviewed journals.” As an example, he described how Michele Andrasik of the University of Washington discussed clinical trials for HIV vaccines on a public radio show (hosted by Southwell).7 Andrasik told a “dramatic and compelling” story about how HIV vaccine research is conducted, which Southwell said lays groundwork for the public to understand and trust the clinical trials process and the results.
In closing, Southwell summarized three key steps needed for person-centered communication about clinical trials: “Acknowledge participant values, needs, and motivations” as they relate to participation in clinical trials; “build and maintain trust between researchers and participants by acknowledging shared interests”; and translate clinical trial methods and results to promote understanding and improve transparency of shared information.
Facilitating the Cultural Change Needed to Improve Trial Diversity
Envisioning the clinical trials enterprise for 2030, Bryson anticipated changes with regard to decentralizing clinical trials, the use of technology, and diversity in clinical trials. She focused her remarks on some of the changes needed to improve diversity in clinical trials, noting that decentralizing clinical trials can help to improve recruitment of diverse populations, and the use of technology for ongoing communication with trial participants can promote retention for existing trials and formation of positive long-term relationships that provide value to participants and potentially influence their decision to participate in future trials.
Bryson described three steps that clinical trial sponsors could take to improve the recruitment of diverse participants to clinical trials. She noted that these steps would be applied differently depending on the community.
- Investing in building longitudinal relationships. The prevalence of the disease or condition the investigational product is intended to treat will determine which communities and community-based organizations to engage, Bryson said. She emphasized the importance of investing in longitudinal relationships with the community in order to build trust.
___________________
7 See https://measureradio.libsyn.com/encouraging-participation-in-clinical-trials (accessed July 1, 2021).
- Building trust. Bryson reiterated the point by Southwell that trust is a key element in successful recruitment of diverse participants for clinical trials. Consistency is important for maintaining trust, she said, and she advised trial sponsors to only commit to what they can deliver. Sponsors should also compensate partner organizations for the access they provide to the community and out of respect for their time spent in community engagement on behalf of the sponsor.
- Coming to the community well before the recruitment is needed. Speaking from her experience in industry, Bryson said that establishing community-based programs has consistently helped pharmaceutical companies to build long-term relationships that foster trust within the community. She emphasized the value of collaborating on existing efforts and the importance of putting in the time and work to build relationships well before attempting to recruit for a clinical trial (at least 6 months), and cautioned against “one-time only” events, which can damage credibility.
To emphasize the value of relationship building, Bryson said the average person spends only 67 minutes each year interacting with a health care provider. The rest of the time is spent interacting with their community, including family, friends, coworkers, classmates, and others with whom they have trusted relationships. These relationships outside of the formal health care system are the ones that most influence the health-related decisions people make and the habits they adopt.
Bryson referred participants to the work of author Glenna Crooks, who has mapped how an individual’s decision making is influenced by the communities, or networks, with which they routinely interact (e.g., networks associated with their home/personal affairs, career, social life, spiritual life, family, and health/vitality).8 Bryson shared Crooks’s example of the influential networks for a hypothetical person, designated “Lucy” (see Figure 5-2). An estimated 71 of Lucy’s connections will directly or indirectly influence a given decision. For example, Bryson explained, Lucy might consult five people directly about her decision, each of whom is influenced by other people in their own networks, and so on. This indicates that taking opportunities to raise awareness about participating in clinical trials among the people in Lucy’s networks can ultimately influence Lucy’s decision on whether she will choose to participate. To influence thinking or behavior, Bryson continued, “you don’t have to always go directly to the person whose mind you want to change. You go to the people that they trust, [their] community.”
___________________
8 See https://glennacrooks.com (accessed July 1, 2021).
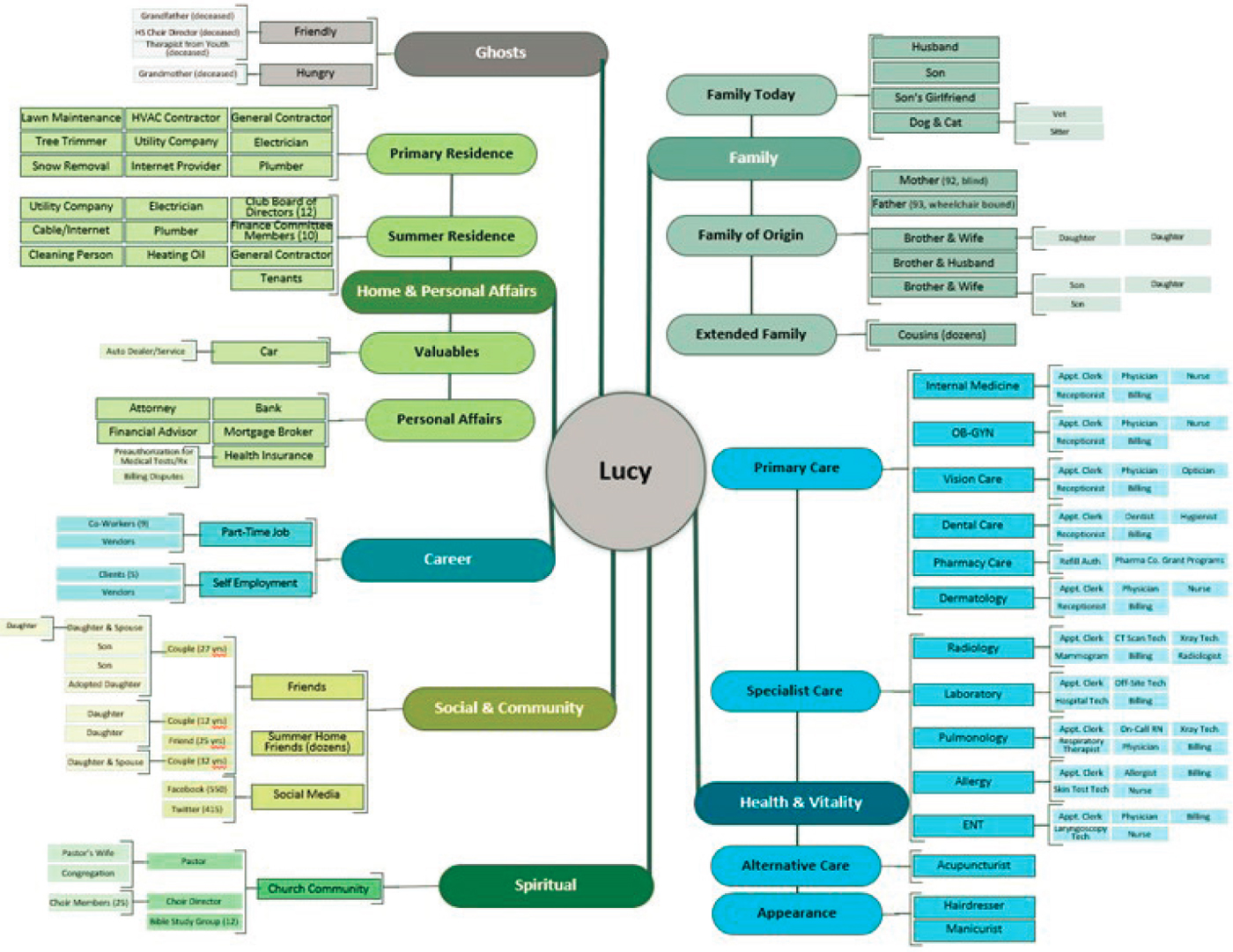
SOURCES: Bryson presentation, March 24, 2021, and Glenna Crooks.
Creating Solutions That Promote Trust
Tenaerts described the approach taken by CTTI to promote a more sustainable and resilient clinical trials enterprise. CTTI aims to create structure and frameworks to support change, she said. As background, she referred participants to the Institute of Medicine workshop summary on envisioning the clinical trials enterprise for 2020 (IOM, 2012), and to CTTI’s recently released vision statement on transforming clinical trials for 2030.9
A participatory, evidence-based approach to problem solving helps to build trust in the solutions developed, Tenaerts said. As a multi-stakeholder, public–private partnership, CTTI strives to be inclusive and give all stakeholders an equal voice in creating evidence-based solutions that will be relevant and have impact. Partners include clinical investi-
___________________
9 See Transforming Trials 2030, available at https://ctti-clinicaltrials.org/who_we_are/transforming-trials-2030 (accessed April 13, 2022).
gators; patients, caregivers, and advocacy groups; academia; trade and professional organizations; IRBs; government and regulatory agencies; and industry. Tenaerts noted that CTTI is working to include data and technology companies as equal partners, rather than as vendors. To help enable an equal voice for patients, she said that the patient participants in their activities are reimbursed for their time away from work. Using quantitative and qualitative research methods, CTTI works to identify and understand issues and stakeholders’ motivations and disincentives for change. CTTI then develops tools and recommendations to promote change and new norms. In the case of clinical trials, for example, a new norm would be including the patient voice from the beginning of the trial process. “Patients and patient advocates need to be included when the research questions are created, … because they are the ones who … are the experts on living with the disease,” Tenaerts said.
One research method used by CTTI is the survey. Interestingly, a survey of CTTI members found that CTTI projects that had not yet issued recommendations had already begun to create change and have impact. Tenaerts reported that just being part of the project team and participating in the cross-stakeholder group discussions led to insights that inspired stakeholders to implement changes in the way they conduct their work. As a result, CTTI takes care to ensure diverse participation in projects and to allow for wider participation from different organizations. Tenaerts highlighted two general principles for CTTI projects. First, foster respect and collaboration among the project participants through open discussion. Second, recognize that these conversations can be difficult and there will be disagreement. “To maximize the benefit of collaboration you need to diverge before you converge,” she said. In this regard, she said it is important to ensure that minority perspectives are heard, and to determine if those who have not contributed are simply in agreement or are not comfortable speaking up in the team setting.
One approach CTTI uses to develop recommendations is seeking to apply lessons learned from positive deviants. For a given area of interest, and under the same circumstances and constraints, there are isolated cases where applying innovative strategies has resulted in greater success (positive deviants). For example, Tenaerts said, CTTI will collect data to identify researchers who have been able to conduct a trial in a given health care setting when others have been less successful. These positive deviants are then engaged in CTTI’s expert meetings and are interviewed in depth to identify themes underlying their success. This information is then used to develop and disseminate recommendations so that others can benefit (see Baxter et al., 2016).
Tenaerts said CTTI’s experience has been that only issuing recommendations is not sufficient to change behavior. In 2013, CTTI began
providing operational tools to aid stakeholders in implementing its policy and practice recommendations to improve clinical trials. In 2016, CTTI initiated activities designed to drive adoption of its recommendations. Most recently, in 2020, CTTI launched its vision for clinical trials in 2030 to provide a path for moving forward. She referred participants to the CTTI website for links to its recommendations, tools, and publications.10
Change takes time, and as an example, Tenaerts showed the time line of the ongoing efforts to implement a central IRB process for multicenter clinical trials from 2006 to the present. To help enable change, CTTI launched Building Better Clinical Trials: A Case Study Exchange, a database through which organizations can learn how others have implemented CTTI recommendations and tools.11 The exchange has case studies from more than 30 organizations that are willing to share how they have used CTTI resources to improve clinical trial efficiency.
Short-Term Goals to Ensure a More Resilient, Sustainable, and Transparent Clinical Trials Enterprise: Panel and Breakout Discussion Highlights
Following the panel discussion, online participants were divided into virtual Zoom breakout rooms to consider short-term, tangible, measurable goals and actions to ensure a more resilient, sustainable, and transparent clinical trials enterprise, and to discuss relevant technologies, tools, techniques, and models that could be used to support this transformation. Upon reconvening in plenary session, Austin and several participants reflected on the panel and breakout group discussions and highlighted the following themes, as described below.
Improving Outreach
Participants discussed ways to improve community outreach and engagement with patients and clinicians. Elena Rios of the National Hispanic Medical Association listed PCORI, the NIH All of Us research program, the Veterans Health Administration, and the teaching clinics of the Health Resources and Services Administration (HRSA) as examples of organizations with connections to communities with diverse populations. She also suggested NIH could reach out to HBCUs and HRSA-designated Hispanic Centers of Excellence to elevate the importance of clinical research in their communities. Partnering with patient advocacy organizations that are already connected to patients was also suggested,
___________________
10 See https://www.ctti-clinicaltrials.org (accessed July 1, 2021).
11 See https://connects.ctti-clinicaltrials.org/case_study_exchange (accessed July 1, 2021).
as well as engaging pharmacists, social workers, and others who have frequent patient contact. The need for a public information campaign about what clinical trials are and the advantages of participation was also reiterated during the discussions. It was also suggested that a patient-friendly source for clinical trial enrollment information is needed.
Shifting the Academic Culture in the United States
Discussion of the U.S. academic culture as it relates to the clinical trials enterprise continued in the breakout groups. As relayed by Austin, participants emphasized the need for change in the academic system for appointments, promotions, and tenure so that participation by academic research faculty in collaborative clinical studies and team-based research is recognized and rewarded. Recalling the discussion of the RECOVERY trial by Landray, Austin pointed out that nearly all practitioners in the United Kingdom are part of the NHS. In the absence of such a centralized system facilitating clinical research in the United States, some individuals proposed creating a separate but affiliated system for clinical research, Austin said, which would not be part of the tenured academic system.
It was suggested that the Association of American Medical Colleges (AAMC) and the National Academies collaborate to consider how the current academic system could better reward the contributions of faculty who recruit participants for clinical trials, especially from underrepresented groups, and how to make clinical research a more appealing career path. Ross McKinney of AAMC agreed that structural change at academic medical centers could help, but added that there are challenges inherent to such change. Other suggestions were that grants could include metrics for community engagement and recruitment to quantify success and recognize achievement, and that recruiting for clinical trials as part of routine care could be part of quality metrics for practices.
Robert Califf pointed out that clinical practices are now commonly part of large health care systems, and many of these systems are now associated with medical schools. He described these large health systems as being partitioned into academic faculty and practitioners that are governed by distinct rules and expectations with little opportunity to work together. The leaders of these systems need to be held accountable for creating a more collaborative environment, he said.
Supporting Providers and Practice-Based Research Networks
There was much discussion of the challenges and barriers to incorporating clinical research into clinical care. Califf cautioned that providers are already overburdened, and adding clinical trials to a practitioner’s
responsibilities should not further strain the provision of care. A participant added that many providers simply do not have the time to explain a clinical trial opportunity to a patient in the course of a caregiving encounter. Austin agreed and said the academic medical centers in the NCATS Clinical and Translational Science Awards program have links with community centers and practice-based research networks, but these remote sites have limited resources and research capacity. Participants also discussed how busy clinicians might be more effectively engaged in formulating clinical research questions during the early stages of trial development.
Lana Skirboll of Sanofi observed that being an investigator for a clinical trial does not fit into a health care business model in which providers are rewarded based on the volume of patients seen or procedures completed. Hannah Valantine of Stanford University agreed and said that stakeholders in clinical trials (e.g., NIH, PCORI, payers, industry) need to collaborate on shaping “a major systems change,” including finding ways to make better use of the existing resources. Barbara Bierer supported remodeling the current system, but noted her concern about creating a separate or parallel system for clinical trials. She observed that many community health centers are not formally linked to an academic health center and said HRSA and CMS should also be included in discussions of the clinical trials enterprise.
Long-Term Goals to Ensure a More Resilient, Sustainable, and Transparent Clinical Trials Enterprise: Panel and Breakout Discussion Highlights
In this breakout session, groups considered longer-term, tangible, measurable goals and actions to ensure a more resilient, sustainable, transparent clinical trials enterprise, and discussed relevant technologies, tools, techniques, and models that could be used to support this transformation. Upon reconvening in plenary session, ElZarrad reflected on the panel and breakout group discussions and highlighted the following themes:
- Committing resources to a community-based trials system. There was discussion throughout the workshop about community-based clinical trials and incorporating research seamlessly into routine practice. Participants discussed the role of dedicated resources and funding to build and support the infrastructure for such a system, ElZarrad reported.
- Engaging payers. Participants discussed public and private payers as important stakeholders in creating a community-based trials
- system. It was pointed out, ElZarrad said, that payers could contribute substantially to discussions of integrating research into care and building efficient systems that generate evidence of value.
- Eliminating underpowered, uninformative trials. Participants discussed tools and mechanisms to limit the conduct of clinical trials that are not designed to produce robust data. The role of journals as partners in ensuring the quality of published trials was mentioned, ElZarrad said, and it was pointed out that there has been a proliferation of journals that perpetuate the dissemination of bad information from poorly conducted trials. Valda Vinson of Science suggested that more information clearly articulating characteristics of high-quality pragmatic trials could be helpful for journals and peer reviewers.
- Informing the media and the public about clinical trials and trial quality. Participants discussed the importance of publicizing positive examples of well-designed, well-executed clinical trials, ElZarrad said, and working with the media to improve the quality of reporting on clinical trials.
REFLECTIONS ON RESILIENCE, SUSTAINABILITY, AND TRANSPARENCY OF THE CLINICAL TRIALS ENTERPRISE
To close this part of the workshop, Krofah and Steven Galson reflected on the key messages they heard during the discussions.
- Pragmatic, randomized controlled trials can achieve diverse and inclusive enrollment, as demonstrated by the RECOVERY trial, but there is still much progress to be made, Krofah said. Who is recruited is directly impacted by where clinical trial sites are located, and this could be addressed by designing more community-based trials. The roles of technology and decentralized trials in expanding inclusivity were also discussed.
- For community-based trials to be sustainable, participating as investigators must be worthwhile for community health care providers, and appropriate incentives can drive more participation, Krofah said.
- Trust and transparency are core elements of a transformed 2030 clinical trials enterprise, Krofah summarized. Participants discussed leveraging existing relationships and building on shared values to establish trust of the clinical trials enterprise within the community. Galson added that the tools for creating more transparency exist, and highlighted workshop participants’ calls for prioritizing it.
- Patients are the experts in their disease, but participants asked: Is the clinical trials enterprise listening to patients? There was much discussion about improving outreach and engaging patients in the trial process from the start of study development to understand what matters to them. “Invest in building longitudinal relationships and come to the community well before you need those participants to enroll in the trial,” Krofah said, recalling the panel discussions.
- There are impediments and disincentives to progress that are inherent in the clinical trials system, Galson reported (e.g., the current academic culture in the United States). However, discussions trended toward transforming the current trials system rather than creating an entirely separate system for clinical trials.
- A coordinated, central plan for transforming the clinical trials enterprise could be a beneficial next step, Krofah concluded, drawing from the discussion by Lewis-Hall. A multi-stakeholder approach to developing such a plan could ensure that all voices are represented in the effort to create a more inclusive clinical trials enterprise. “We cannot do this in our own individual siloes,” she said. Galson highlighted the importance of including experts in social sciences in these discussions as well. Participants discussed a role for the National Academies in convening stakeholders from across the clinical trials ecosystem to develop a national action plan.
This page intentionally left blank.




















