
3
The Health and Economic Burden of Resistance
As the previous chapter mentioned, antimicrobial-resistant infections are difficult to treat and contribute to a general increase in morbidity and mortality, while simultaneously adding high costs to the health system. But estimating disease burden associated with antimicrobial resistance is not straightforward. Analysis of death certificates and international diagnosis codes, common in epidemiological studies of disease burden, are not suitable to studies of antimicrobial-resistant infections (CDC, 2019; Denison and AV, 2010; Lopez et al., 2006). This is because the effects of resistant pathogens can manifest in many different ways. Methicillin-resistant Staphylococcus aureus (MRSA), for example, commonly causes skin, wound, and bone infections, pneumonia, and bloodstream infections (CDC, 2019). Though caused by the same pathogen, any one of these presentations would be diagnosed and coded differently. Should the patient die, the cause of death might be recorded as sepsis or pneumonia, but not MRSA. For these reasons, population estimates of the consequences of resistant infection have underestimated the true burden of disease (CDC, 2019).
There is also wide variability in where studies are conducted. Most research takes place in high-income countries where microbiological confirmation of a resistant infection is more readily available. Fewer studies have attempted to estimate the health or economic burden of resistance in low- or middle-income countries. Gradual improvements in surveillance of both antimicrobial use and resistance patterns, a topic discussed in more detail in the next chapter, could facilitate better understanding of the true burden of resistant infections in the future.
This chapter will review a cross section of relevant literature, mostly from the last several years. First, it discusses a series of recent landmark publications on the topic; next, it discusses some of the challenges of estimating the effects of resistance on health, the economy, and on animal agriculture. Though primarily a literature review, this chapter is not an exhaustive analysis of every publication on the question; rather, it presents an overview of trends in the literature and important patterns to emerge.
REVIEW OF RECENT REPORTS
Attention to the problem of antimicrobial resistance has grown in recent years, driven in part by a series of high-profile international reports. This section reviews the touchstone reports from the Centers for Disease Control and Prevention (CDC), the Organisation for Economic Co-operation and Development (OECD), the UK Prime Minister’s commission to Jim O’Neill, called the O’Neill report, and the World Bank.
Antibiotic Resistance Threats in the United States, 2019
The CDC’s Antibiotic Resistance Threats in the United States, 2013, was one of the earliest of the recent reports to attempt to quantify the health burden of resistance and to categorize pathogens by the level of threat they pose to public health (CDC, 2013). The CDC revisited this report in 2019, and the more recent publication contains estimates of the burden of resistant pathogens based on laboratory and population surveillance data, complemented with research from electronic medical records, and is weighted to allow for some extrapolation to the national level (CDC, 2019; Kadri, 2020).1
This analysis indicated there are 2.8 million resistant infections every year in the United States, causing 35,900 deaths; Clostridioides difficile (C.
___________________
1 The CDC report’s technical appendix thoroughly explains the methods used to estimate the burden of the 21 resistant pathogens included (CDC, 2019). The CDC’s Active Bacterial Core surveillance through the Emerging Infections Program was the starting point for many of the estimates presented, including those for group A and B Streptococcus, and Streptococcus pneumonia; a combination of active laboratory and population surveillance in study sites across the country informed estimates for several pathogens including Acinetobacter baumanii, Clostriodioides difficile, MRSA, and certain Candida spp. (CDC, 2019). Cohort studies using patient data from three nationally used electronic health record systems collected over 5 years were pooled and weighted to inform estimates of MRSA and another six pathogens (CDC, 2019). The National Antimicrobial Resistance Monitoring System data on the number of infections and the prevalence of resistance was used to estimate the prevalence of resistance among isolates of several species (CDC, 2019). The published, peer-reviewed methods papers describing how CDC researchers arrived at disease burden estimates for each pathogen are included in the report’s references.
difficile) infection, a problem caused by antimicrobial disruption of the gut flora, kills another 12,800 people a year (CDC, 2019). Despite sudden increases in certain infections, multidrug-resistant Candida auris, for example, was not spreading in the United States until 2015, total deaths from resistant infections declined 18 percent between 2013 and 2019 and deaths in hospitals have declined 28 percent (CDC, 2019). Table 3-1 shows the percentage change for those pathogens for which a longitudinal comparison was possible.
The report also explained that the economic costs of resistance can be difficult to estimate with any credibility. Resistant infections undoubtedly cost the health system more in terms of person hours needed to treat them and extended hospital stays. The medicines needed to treat them can be expensive and less well tolerated (CDC, 2019). Nevertheless, there is no consensus methodology to estimate the economic burden of resistant infections.
To put some economic parameters on the problem, the CDC used retrospective cost analysis of patients with six common resistant infections in the Veterans Health Administration medical centers, adjusted for the general population by the Veterans Affairs (VA) Health Economics Resource Center (Nelson et al., 2021). The analysis for C. difficile drew from peer-reviewed literature, and for some pathogens, no reliable cost estimate was available. Table 3-2 shows only the direct medical costs associated with a positive culture for the pathogens of interest, not the downstream costs associated with future disability or the cost to the patient of missed work or even the cost to the health system after discharge. (The
TABLE 3-1
Change in Infections Caused by Some CDC Priority Pathogens Between 2013 and 2019
| Pathogen | Increase or Decrease | % Change 2013 to 2019 |
|---|---|---|
| Vancomycin-resistant Enterococcus | Decrease | 41% |
| Multidrug-resistant Pseudomonas aeruginosa | Decrease | 29% |
| Carbapenem-resistant Acinetobacter | Decrease | 33% |
| Drug-resistant Candida auris | Decrease | 25% |
| Carbapenem-resistant Enterobacterales | Stable | — |
| Drug-resistant Neisseria gonorrhoeae | Increase | 124% |
| ESBL-producing Enterobacterales | Increase | 50% |
| Methicillin-resistant Staphylococcus aureus | Decrease | 21% |
| Erythromycin-resistant invasive group A strep | Increase | 315% |
NOTE: ESBL = extended-spectrum beta-lactamases.
SOURCE: CDC, 2019.
| Pathogen | Estimated Attributable Health Care Costs | Annual Direct Medical Costs | Annual Discounted Lifetime Direct Medical Costs |
|---|---|---|---|
| Carbapenem-resistant Acinetobacter | $281 million | — | — |
| Hospital-associated Clostridioides difficile | $1 billion | — | — |
| Carbapenem-resistant Enterobacterales | $130 million | — | — |
| Drug-resistant Neisseria gonorrhoeae | — | — | $133.4 million |
| Drug-resistant Campylobacter | — | $270 million | — |
| Drug-resistant Candida | — | $3 billion | — |
| ESBL-producing Enterobacterales | $1.2 billion | — | — |
| Vancomycin-resistant Enterococcus | $539 million | — | — |
| Multidrug-resistant Pseudomonas aeruginosa | $767 million | — | — |
| Drug-resistant nontyphoidal Salmonella | — | $400 million | — |
| Drug-resistant Shigella | — | $93 million | — |
| Methicillin-resistant Staphylococcus aureus | $1.7 billion | — | — |
| Drug-resistant Streptococcus pneumoniae | — | $1.3 billion | — |
NOTE: ESBL = extended-spectrum beta-lactamases.
SOURCE: CDC, 2019.
long-term asymptomatic nature of resistant gonorrhea infection made it necessary to present a lifetime estimate of costs.) The direct costs of treating six, common multidrug-resistant pathogens was $4.6 billion a year, C. difficile another billion, and drug-resistant gonorrhea another $133.4 million (CDC, 2019; Nelson et al., 2021).
OECD Development Work on Antimicrobial Resistance
The OECD, an intergovernmental economic organization, has also published several influential reports on antimicrobial resistance since 2015, often in collaboration with the European Centre for Disease Prevention and Control (ECDC).
The first of these publications, Antimicrobial Resistance in G7 Countries and Beyond, was released shortly after the O’Neill report and drew atten-
tion to the fact that only a quarter of the world’s countries had a national antimicrobial resistance plan (Cecchini et al., 2015). The OECD’s 2016 publication drew on data from the ECDC’s Surveillance of Antimicrobial Consumption Network and the Center for Disease Dynamics, Economics, and Policy’s national and subnational resistance data to analyze trends in the emergence of resistance between 2005 and 2014 (OECD, 2016). Using an aggregate measure of resistance based on six, high-priority pathogen–drug combinations, the report concluded that the prevalence of antimicrobial resistance had increased in 23 of 26 OECD countries (see Figure 3-1), though human use of antimicrobials remained largely stable (OECD, 2016).
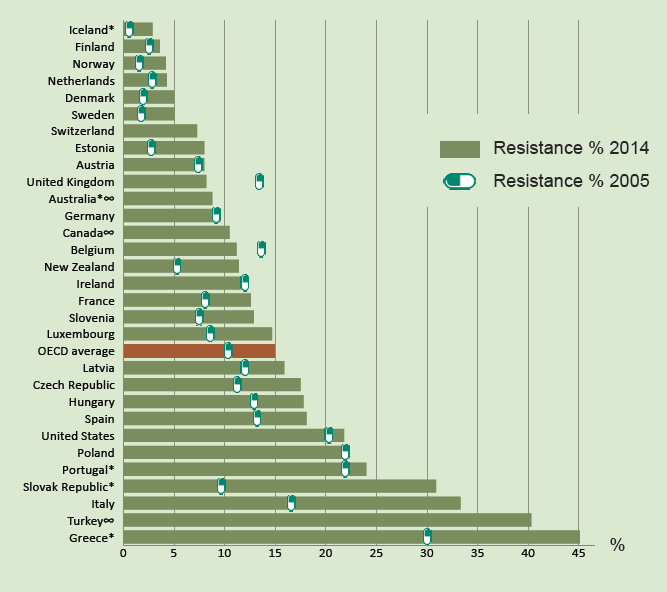
NOTE: * Greece missing S. pneumoniae (resistant to penicillin) 2005 and 2014, Slovakia and Belgium missing K. pneumoniae (resistant to third-generation cephalosporins and carbapenem) 2005, Portugal missing K. pneumoniae (resistant to carbapenem) 2005, New Zealand missing MRSA 2014, Australia missing S. pneumoniae (resistant to penicillin) 2014, Iceland missing K. pneumoniae (resistant to carbapenem) 2014; ∞ Includes resistant and intermediate data.
SOURCE: OECD, 2016.
The OECD Health Committee, in collaboration with the European Centre for Disease Prevention and Control, has also given considerable attention to estimating the future health and economic burden of antimicrobial-resistant infections (OECD, 2018). Their analysis was undertaken at the direction of the European Commission and published in Stemming the Superbug Tide. The researchers drew on data from the ECDC European Antimicrobial Resistance Surveillance Network and the laboratory networks that inform the Center for Disease Dynamics, Economics, and Policy’s Resistance Map (OECD, 2018). Their estimates of resistance in pathogen–drug combinations accounted for uncertainty using multiple imputation of missing historical values and estimating correlates of resistance from UN population data and weighted modeling, described in detail in the report (OECD, 2018). The analysis indicated that around 17 percent of bacterial infections in OECD countries overall are resistant to antibacterial medicines, but this prevalence is more than a third in some OECD countries such as Greece, the Republic of Korea, and Turkey (OECD, 2018). Resistance proportions are much higher outside the OECD, over 40 percent in some G20 countries, including China, India, and Russia (OECD, 2018).
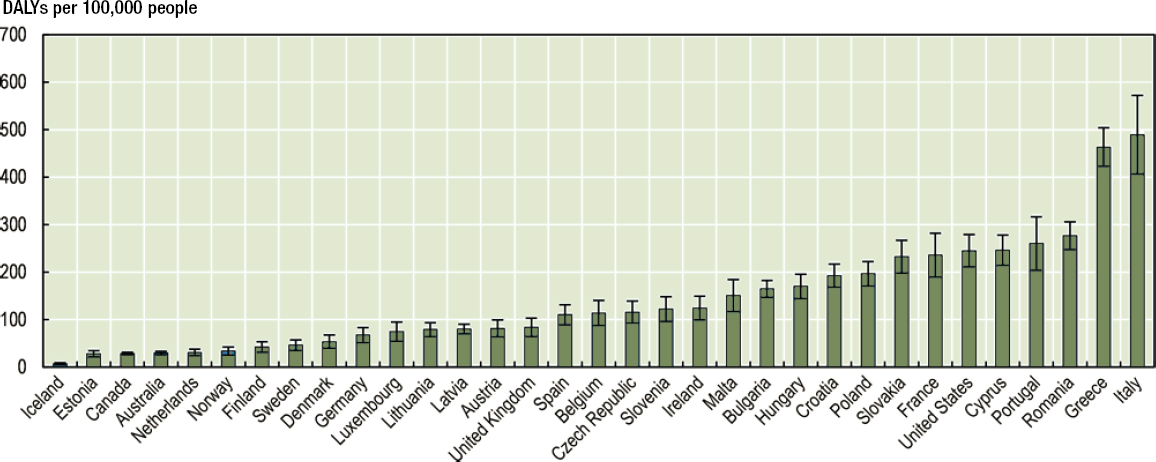
The large variation among countries in burden of resistant infections influences projections of mortality. OECD models indicate that there are about 60,000 deaths from resistant infections every year in the United States and Europe (OECD, 2018). By 2050, the OECD model suggests resistant infections will have caused 2.4 million deaths in the same countries (plus Canada, Mexico, and Australia), roughly 30,000 deaths a year in the United States alone (OECD, 2018) (see Figure 3-2). The effects of resistance on quality of life are even stronger. The OECD models of disability-adjusted life years (DALYs), an indicator that accounts for both untimely deaths and time spent in relatively compromised health, suggest 1.75 million years of healthy life are lost every year across 33 study countries (see Figure 3-3). In Italy alone, up to one person out of every 205 could lose a year of life because of infections caused by resistant organisms (OECD, 2018).
The OECD’s estimates of mortality and morbidity are the output of published models, the assumptions of which are clearly explained. There are only so many parameters modeling can accommodate, however. All the models presented in Stemming the Superbug Tide were based on resistance in eight common pathogen–drug combinations.2 Other resistance
___________________
2 Third-generation cephalosporin-resistant E. coli; fluoroquinolones-resistant E. coli; penicillin-resistant S. pneumonia; Methicillin-resistant S. aureus; carbapenem-resistant K. pneumonia; third-generation cephalosporin-resistant K. pneumonia; carbapenem-resistant P. aeruginosa; vancomycin-resistant E. faecalis and E. faecium.
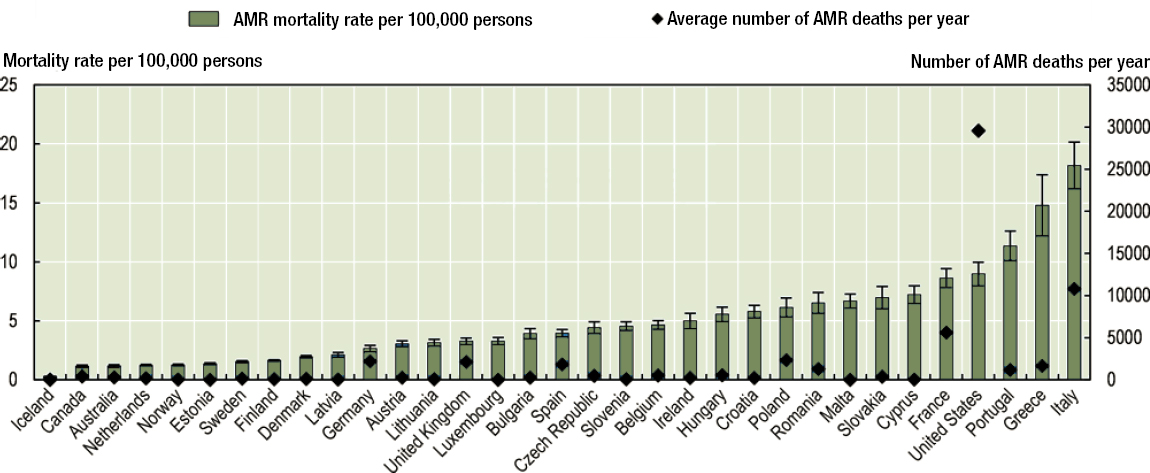
NOTE: AMR = antimicrobial resistance.
SOURCE: OECD, 2018.
patterns will emerge between now and 2050; there are other pathogen–drug combinations that cause serious excess illness and death even today. Accepting the methodological limitations of modeling, the work shows a clear and consistent increasing threat to human health from antimicrobial resistance.
OECD research has also made valuable contributions to understanding the economic consequences of resistant infections. Based on their calculations of morbidity and mortality associated with resistant infections, the report estimated that resistance costs the health system of the 33 countries studied about $3.5 billion a year (adjusted for purchasing power parity), $2 billion a year in the United States alone (OECD, 2018). This finding was consistent with a similar study that estimated the cost to the U.S. health system around $2.2 billion a year (Thorpe et al., 2018).
The OECD also drew attention to the negative externalities (costs to parties other than the patient and prescriber) associated with antimicrobial resistance (OECD, 2018). For example, antimicrobial resistance can undermine confidence in the health system, causing people to avoid in-patient treatment if possible; it can also hurt livelihoods dependent on tourism or agriculture (Thorpe et al., 2018). These kinds of effects are harder to model with any amount of precision, but are useful as a reminder of the potentially devastating downstream effects of a health problem with already devastating short-term consequences.
The O’Neill Report
One of the most influential reports on antimicrobial resistance was the O’Neill report, the 2014 commission from then UK Prime Minister David Cameron to economist Jim O’Neill to analyze the problem of antimicrobial resistance and suggest a mitigating strategy (O’Neill, 2016a). The commission’s final report, Tackling Drug-Resistant Infections Globally, was published in 2016 (O’Neill, 2016b). The report immediately attracted considerable attention in the scientific literature (Matthiessen et al., 2016; O’Neill, 2016a; PLOS Medicine Editors, 2016; Price, 2016; Sugden et al., 2016), from international organizations (FAO and UN, 2021; IACG, 2019; The World Bank, 2016, 2017b), and in the lay media (BBC News, 2016; Boseley, 2016; Roland, 2015; The Economist, 2016). Much of this attention centered around the report’s projection that by 2050 antimicrobial resistance would cause 10 million deaths a year, costing the global economy a cumulative $100 trillion in the same time (O’Neill, 2016b).
These estimates were based on analyses by the RAND Corporation, a nonprofit think tank, and by the management consulting and tax firm KPMG (O’Neill, 2016b). Both models considered resistance to medicines
used to treat malaria, HIV, and tuberculosis, as well as hospital-acquired Escherichia coli, Klebsiella pneumoniae, and Staphylococcus aureus (KPMG LLP, 2014; Taylor et al., 2014). Although both models report having made projections for different burden-of-resistance scenarios, only the extreme high-burden scenario were reflected in the O’Neill report (KPMG LLP, 2014; Taylor et al., 2014).
The pathogens causing HIV, malaria, and tuberculosis are not usually central to the discussion of antimicrobial resistance. The burden of disease associated with these infections is vastly greater than those caused by the CDC or the WHO priority pathogens, making it difficult to interpret estimates of their combined affects.
The RAND model assumed that in 15 years none of the medicines licensed to treat these infections will be effective, an assumption that lacks face validity (Friedman, 2020; Taylor et al., 2014). Even in the model appendices, the RAND team cites contemporary estimates of resistance to HIV drugs (~5 percent worldwide) and treatments for multidrug-resistant tuberculosis treatments (~3 percent globally, between 2 and 5 percent in every region except Europe where it is ~16 percent) (Taylor et al., 2014). It is not credible to conclude that total resistance to these medicines in 15 years is in any way likely.
Table 3-3 presents some key results from the RAND and KPMG analyses. These results informed the O’Neill report’s widely publicized estimates of 10 million lives lost to antimicrobial resistance every year by 2050 and $100 trillion cumulative loss in global production (O’Neill, 2016b).
None of the analysis informing the estimates in Table 3-3 were formally peer reviewed (de Kraker et al., 2016). The relationship between the commissioned models and the O’Neill report’s conclusions are also somewhat murky (de Kraker et al., 2016; O’Neill, 2014). The O’Neill report’s authors refer to original analyses and information not included in the RAND or KPMG models (e.g., “We estimate that caesarean sections contribute about 2% to world GDP”), but their methods and data are not presented (Friedman, 2020; O’Neill, 2014).
| Lives Lost by 2050 | Cumulative GDP Loss by 2050 | |
|---|---|---|
| RAND model | 11 to 444 million adults, cumulative | $5.8–$125 trillion |
| KPMG model | 200 to 700 million, cumulative | $5–$14.2 trillion |
| O’Neill report | 10 million a year by 2050 | $60–$100 trillion |
NOTE: GDP = gross domestic product.
SOURCES: KPMG LLP, 2014; Taylor et al., 2014.
The O’Neill team started from a reasonably credible 2014 base estimate of 700,000 deaths a year from resistant infections (about a third from multidrug-resistant tuberculosis alone) (O’Neill, 2016b; WHO, 2019b). This estimate also has methodological limitations (Schnall et al., 2019). Few if any of the other numbers in the report have such a clear attribution. Though their analytic steps are not clear, one critique concluded, “[T]he scenario that seems to be underlying the most often quoted line [10 million death a year] entails a sharp initial rise of current resistance rates by 40 percentage points, after which rates remain stable until 2050, and doubled infection rates” (de Kraker et al., 2016). A 40 percentage point increase in not consistent with what is presented in the CDC or the OECD analyses discussed previously. One may assume the O’Neill commission believed this to be plausible based on more (rightly) dire predictions in low- and middle-income countries, but it is not clear what scientific research informed their estimates or what their assumptions regarding resistance in different parts of the world might have been. A lack of data from low- and middle-income countries, where the burden of resistant infection is undoubtedly greatest, is a reason to support these countries in routine surveillance for, and prevalence surveys of, resistant infections (Islam et al., 2019). But no estimate of the global burden of resistance can be made in the absence of such data.
The O’Neill report writers may have damaged their credibility by promoting what appears to be only the upper limit of the uncertainty intervals for their conclusions (de Kraker et al., 2016). The writers give no confidence interval for their estimate of 10 million excess deaths a year by 2050 (O’Neill, 2014). (For comparison, 10 million deaths a year is comparable to the global sum of all cancer deaths combined [Sung et al., 2021].) Their estimate that resistance could “cost the world up to 100 trillion USD” contained an uncertainty interval ($60 to $100 trillion) that is usually dropped (O’Neill, 2014).
This is not to say that the O’Neill commission did not produce valuable policy analysis or that its report did not raise the global prominence of the problem. Nor is the modeling of extreme assumptions or worst-case scenarios without value (OECD, 2018). Such models can be useful, especially when they are presented as sensitivity analyses and the caveats on their interpretation made clear. But unfortunately, the O’Neill report’s estimates of both projected mortality and economic consequences of resistance took on a life of their own (Friedman, 2020). When cited, which is often, it is usually without mention of their limitations or the murky analysis that informed them. As a 2016 essay concluded, “Unreliable global estimates like those provided in the [O’Neill report] potentially undermine, rather than support, the fight against a post-antibiotic era” (de Kraker et al., 2016).
The World Bank Report
The World Bank (2017) report, Drug-Resistant Infections: A Threat to Our Economic Future, came out in 2017, building on the momentum of the previous year’s O’Neill report. The report presented estimates of the threat antimicrobial resistance poses to the global economy in terms of lost gross domestic product (GDP) between 2015 and 2050, giving particular attention to costs to international trade, livestock agriculture, and health (The World Bank, 2017).
The World Bank models drew on the RAND estimates that informed the O’Neill report (Ahmed et al., 2017). The model’s low-case scenario was based on the RAND scenario 1, assuming 5 percent antimicrobial resistance from 2015 on; the high-case scenario projected current rates of resistance for 15 years and 100 percent resistance to available treatments after year 15 (Ahmed et al., 2017). Possibly motivated by concerns about the validity of the RAND analyses, the working paper explained, “[W]e avoid the [Rand report’s] extreme cases of absolute resistance”3 (Ahmed et al., 2017). In its final report the World Bank team further clarified that its “simulations are not predictions (rather, a range of outcomes that are possible)” (The World Bank, 2017).
The caveats on the World Bank models are helpful. At the same time, using models driven mostly by data on HIV, tuberculosis, and malaria to inform conclusions about other resistant pathogens in humans and livestock is of questionable validity and should be kept in mind in reviewing the report’s main conclusions.
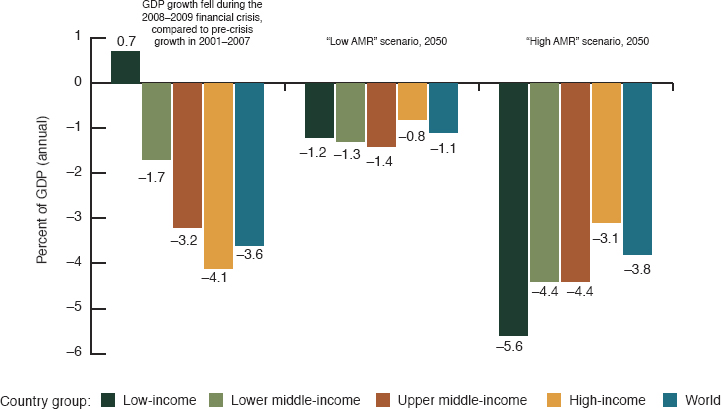
The World Bank report emphasized that trade and livestock production stand to be seriously affected by antimicrobial resistance, especially livestock production in low-income countries (The World Bank, 2017). Livestock is only a small part (about 2 percent) of the global economy, but its relative value—both in direct terms and as determinant of the health and economic mobility of women and children—is greater in low- and lower-middle-income countries (Ahmed et al., 2017). The World Bank working paper reported that livestock production in low-income countries could fall between 3.1 and 11.1 percent and in lower-middle income countries between 3.1 and 8.9 percent (Ahmed et al., 2017). The effects of reductions in livestock production also influence, but only partially, the projected 1.1 to 3.8 percent deficit in global exports (The World Bank, 2017).
The cost of health services could be perhaps the most directly affected by antimicrobial resistance, given that resistant infections cost more to treat. Increased health expenditures could be felt in cost of medicines,
___________________
3 Meaning the RAND projections that assumed 100 percent resistance started immediately (Ahmed et al., 2017; Taylor et al., 2014).
with more expensive antimicrobials being needed, as well as more days spent hospitalized, more consultation time with providers, and increased demand on laboratory diagnostic services. Increasing need for health services puts more pressure on both public and private spending for health, which, coupled with decreasing trade and livestock production, could drive a public deficit. The World Bank models estimate that under a low burden of antimicrobial resistance health costs could increase $330 billion; under a high-burden scenario this increase could be $1.2 trillion (The World Bank, 2017).
Figure 3-4 shows how protracted effects on global economic output might extend for the next 30 years, costing the world between 1.1 and 3.8 percent of annual GDP by 2050 (The World Bank, 2017). These shortfalls could be as serious as during the 2008–2009 global financial crisis (see Figure 3-5) but could extend for much longer. (The shocks of the 2008–2009 crisis lasted only a few years.)
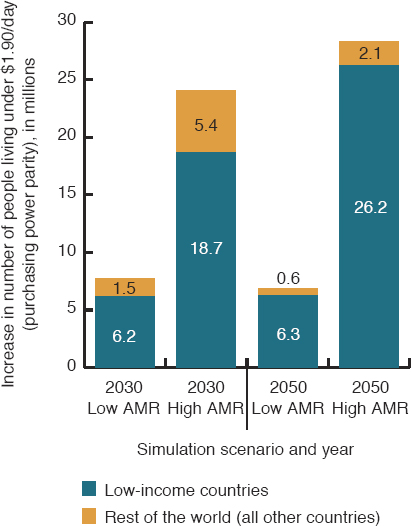
By taking a disproportionate toll on developing countries, antimicrobial resistance could derail progress on the Sustainable Development Goals, the United Nations’ goals for international development between 2015 and 2030 (UN, 2021; The World Bank, 2017). Through its effects on health costs, trade, and livestock production, the World Bank models indicate that antimicrobial resistance could push between 8 and 28 million people into extreme poverty by 2050 (The World Bank, 2017) (see Figure 3-6).4
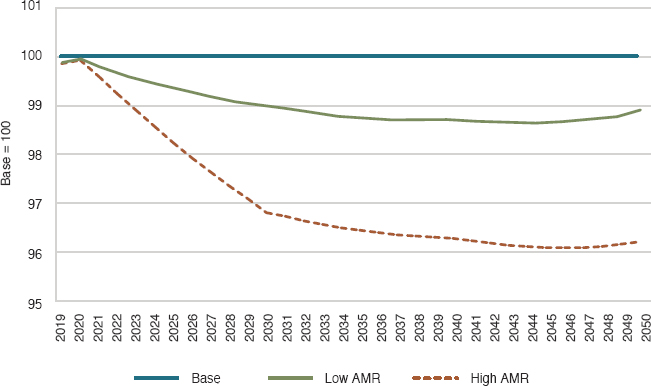
SOURCE: The World Bank, 2017.
___________________
4 Defined as living on less than $1.90 a day, adjusted for purchasing power parity (The World Bank, 2017).
SOURCE: The World Bank, 2017.
SOURCE: The World Bank, 2017.
CHALLENGES OF QUANTIFYING THE BURDEN OF RESISTANCE
The O’Neill report and the World Bank report it inspired are examples of how a lack of empirical evidence about antimicrobial resistance influences the discussion of the problem. Reliable modeling of the true burden of resistance is extremely challenging. Part of the challenge stems from uncertainty regarding the best ways to measure antimicrobial resistance in humans, animals, and the environment (Wernli et al., 2017). The global COVID-19 pandemic has made this task more challenging, increasing the strain on health systems and possibly leading to less interest in antimicrobial resistance (Kwon and Powderly, 2021; Pelfrene et al., 2021; Rodriguez-Bano et al., 2021). Information on the epidemiology of resistance, through surveillance of known risks and attention to emerging resistant pathogens, and their consequences for health, are essential pieces of information to quantify this burden (Wernli et al., 2017).
The Health Effects of Resistance in Humans
Chapter 4 discusses the challenges of surveillance for antimicrobial resistance. In short, measuring antimicrobial resistance requires a laboratory capacity and trained clinical microbiologists that are not widely available in low- and middle-income countries (Iskandar et al., 2021). The large, tertiary-care hospitals that can support the required microbiology labs provide a narrow window into the scope of resistance (Gandra et al., 2020; Tadesse et al., 2017; Walia et al., 2019; Wang, 2019). While valuable, this window is not necessarily representative of the national situation. Even in the United States, with its sophisticated laboratory infrastructure, there are challenges in reporting resistant isolates through the regional and national Antibiotic Resistance Laboratory Network, a problem discussed more in Chapter 5.
Regardless of the capacity of the national surveillance systems, there are also challenges in measuring mortality and morbidity from resistant infections. First of all, most resistant infections are seen in patients who have other underlying conditions, making it difficult to know what portion of the clinical outcomes observed can be attributed to the resistant infection (Cassini et al., 2019). For this reason, “scientific debate is ongoing on the appropriate epidemiological study design and statistical inference methods to measure reliable estimates of untoward clinical outcomes attributable to infections with antibiotic-resistant bacteria” (Cassini et al., 2019). For the time being, most research on the clinical outcomes associated with antimicrobial resistance is limited to readily observable, relatively short-term clinical outcomes, including deaths, number of days hospitalized, and risk of developing sequelae (e.g., developing C. difficile infection after treatment for a resistant infection) (Cassini et al., 2019).
Risk of death is clearly the most potentially devastating consequence of resistant infection, though only about half of the studies included in a recent systematic review found an increased risk of death in patients infected with a resistant pathogen relative to those infected with a susceptible one (Naylor et al., 2018). It is possible that these differing results are influenced by widely varying methodological approaches, a topic discussed later in the chapter.
Scientists from the ECDC recently published one such analysis of the health outcomes of resistant infections. Drawing on data from the European Antimcrobial Resistance Surveillance Network and health outcome models for specific types of infection (e.g., bloodstream infection, surgical site infection), they estimated between 583,148 and 763,966 infections with resistant bacteria occurred in Europe in 2015, almost two-thirds of them acquired during health care (Cassini et al., 2019). These infections ended in over 33,000 deaths, with the burden of disease (in terms of healthy life years lost) being most severe in infants and older adults; see Figure 3-7 (Cassini et al., 2019).
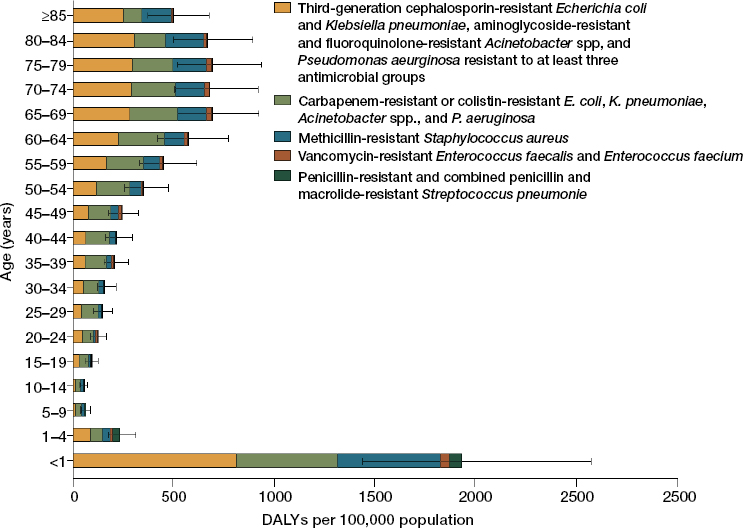
SOURCE: Cassini et al., 2019.
Studies such as these help put concrete parameters on the consequences of resistance, parameters that are compelling to policy makers precisely because of their narrow scope and clear boundaries. Nevertheless, some of the most potentially devastating consequences of resistance are the downstream effects that can manifest in increased mortality and complications from seemingly unrelated conditions.
As the previous chapter discussed, antimicrobials are essential for the medical management of surgical care, cancer, and transplant patients, many of whom are immunocompromised. A 2015 model, based on review of randomized and quasi-randomized controlled trials, estimated how loss of effective antibiotic prophylaxis might increase the burden of serious infections and related deaths in the United States (Teillant et al., 2015). The models presented scenarios of a loss of antibiotic efficacy of 10, 30, 70, and 100 percent (Teillant et al., 2015). The authors estimate that a 30 percent reduction in the efficacy of prophylactic antimicrobial treatment for 10 common surgeries and blood cancer chemotherapy would result in an additional 120,000 infections and 6,300 deaths a year (Teillant et al., 2015). Even a relatively minimal 10 percent loss of efficacy would result in 40,000 additional infections and 2,100 additional deaths; the more dire prediction of a 70 percent loss of efficacy would result in 280,000 additional infections and 15,000 additional deaths, as Figures 3-8 and 3-9 show (Teillant et al., 2015).
Models such as those of Teillant and colleagues draw on an extensive body of research on infection in cancer and surgery patients. The consequences of resistance associated with other common infections, though sometimes more serious, are less amenable to modeling. Drug-resistant infections in the bone and brain, for example, are serious because it is difficult to achieve clinically meaningful concentrations of antimicrobial medicines in these tissues (Nau et al., 1998, 2010; Thabit et al., 2019). Moreover, even small changes in susceptibility of pathogens to medicines can make more surgeries necessary and prompt months-long, or even lifelong, antimicrobial therapy with uncertain results.
Resistant infections can compromise the outcomes of almost every medical treatment. They could also have psychological affects that reduce public confidence in the health system (Foster, 2011; WHO, 2019a). The COVID-19 pandemic has made clear that an infectious disease crisis, accompanied by disruptions in health services and widespread fear or anxiety, can have profound effects on health. English models indicate that cancer mortality may have increased by an estimated 20 percent during the pandemic because of avoided or delayed treatments (Lai et al., 2020). Globally, about 28 million surgeries were cancelled or postponed in the first wave of COVID-19 alone (COVIDSurg Collaborative, 2020). It is not clear how long it will take to clear this backlog or how far-reaching the
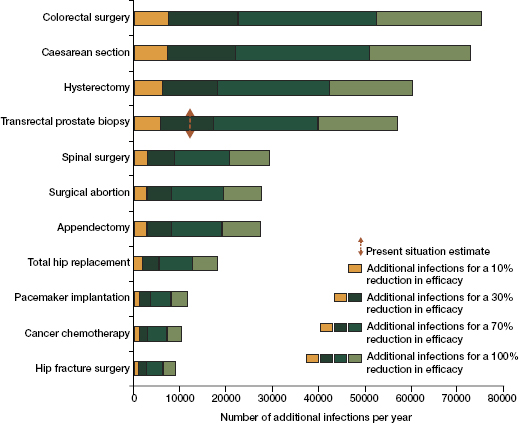
SOURCE: Reprinted from The Lancet, Vol. 15, Aude Teillant, Sumanth Gandra, Devra Barter, Daniel J. Morgan, Ramanan Laxminarayan, Potential burden of antibiotic resistance on surgery and cancer chemotherapy antibiotic prophylaxis in the USA: A literature review and modelling study, 1429-1437, Copyright (2015), with permission from Elsevier.
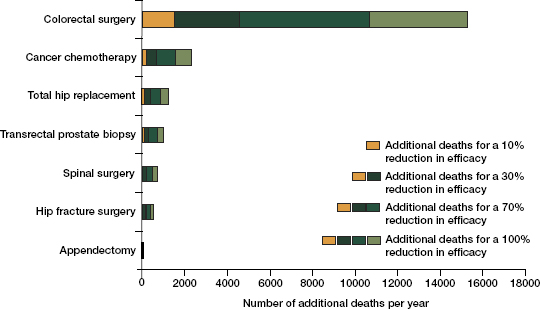
SOURCE: Reprinted from The Lancet, Vol. 15, Aude Teillant, Sumanth Gandra, Devra Barter, Daniel J. Morgan, Ramanan Laxminarayan, Potential burden of antibiotic resistance on surgery and cancer chemotherapy antibiotic prophylaxis in the USA: A literature review and modelling study, 1429-1437, Copyright (2015), with permission from Elsevier.
health consequences could be (Carr et al., 2021). In some ways the most serious risks antimicrobial resistance poses to society are some of the most challenging to quantify.
The overall effects of the COVID-19 pandemic on antimicrobial resistance are hard to predict. On one hand the increased emphasis on hygiene and the decrease in travel and elective medical procedures may have decreased the spread of resistant pathogens both in community and clinical practice (Knight et al., 2021). On the other hand, the vast majority of COVID-19 patients were treated with antimicrobials (Knight et al., 2021). One study found that despite only 7 percent of COVID-19 patients having bacterial infections over 70 percent were treated with antibiotics (Langford et al., 2020). Research in India found that COVID-19 drove over 200 million excess doses of antimicrobials (Sulis et al., 2021). Such extensive exposure to antimicrobials can predispose patients to colonization with resistant organisms. There may also be a cohort of COVID-19 survivors with residual predisposition to lung infections who will need more frequent antimicrobial therapy (Knight et al., 2021).
There has also been considerable presumptive antimicrobial use during the pandemic, both in COVID-19 patients presenting with nonspecific symptoms and “just in case” prescribing to patients with other illnesses who were deflected from care (Knight et al., 2021). As Figure 3-10 shows, the ways COVID-19 has and will continue to influence antimicrobial resistance are varied and warrant further research.
The Economic Effects of Resistance in Humans
Loss of life and disability are devastating health outcomes in their own right. They also affect society indirectly, through the loss of what might have been achieved in years of healthy life. Estimates of how health problems affect the workforce are often of particular interest to policy makers. Most health problems, resistant infections included, hurt the workforce in two ways: the lost productivity among patients suffering from resistant infections and, in some cases, the lost productivity of the workers looking after them (Tillotson and Zinner, 2017). In the same way the health effects of resistant infections can be both direct and indirect, so can the social and economic effects. Table 3-4 shows the many pathways through which health care–associated infections draw a social and economic toll.5
In estimating the economic consequences of resistance, researchers must base their analysis on estimates of the health effects. Therefore, the uncertainties and limitations in measuring the health consequences of
___________________
5 Infections acquired as a result of medical care, often stemming from inappropriate use of antimicrobials or problems with infection controls; health care–acquired infections are often drug resistant (CDC et al., 2021).
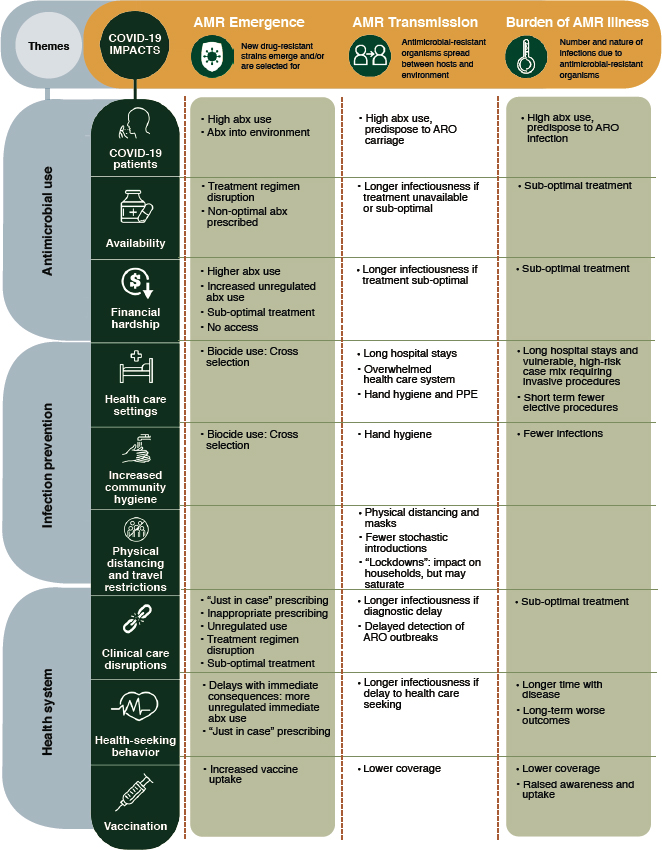
NOTE: abx = antibiotics; AMR = antimicrobial resistance; ARO = antibiotic-resistant organism.
SOURCE: Knight et al., 2021.
resistance carry forward to discussion of the costs. For this reason, there are fewer economic studies on antimicrobial resistance (Naylor et al., 2018). The quality of what is published is also lower, a recent systematic review concluded, and held back by a “lack of rigorous, transparent modelling studies which appropriately present or incorporate uncertainty” (Naylor et al., 2018).
TABLE 3-4
The Social Costs of Hospital-Acquired Infections
| Categories of Cost | ||
|---|---|---|
| Direct Hospital Costs | Fixed Costs | Buildings Utilities Equipment/Technology Labor (laundry, environmental control, administration) |
| Variable Costs | Medications Food Consultations Treatments Procedures Devices Testing (laboratory and radiographic) Supplies |
|
| Indirect Costs | Lost wages Diminished worker productivity on the job Short-term and long-term morbidity Mortality Income lost by family members Forgone leisure time Time spent by family and friends for hospital visits, travel costs, home care |
|
| Intangible Costs | Psychological Costs (i.e., anxiety, grief disability, job loss) Pain and suffering Change in social functioning and daily activities |
|
SOURCES: Scott, 2009. Adapted from Haddix AC and Shaffer PA. Cost-effectiveness analysis. In Prevention Effectiveness: A Guide to Decision Analysis and Economic Evaluation. Oxford University Press, 1996.
The potential for bias in the economic evaluation of antimicrobial resistance is at the root of the many widely variable estimates ($3 billion to $100 trillion) of the economic consequences of antimicrobial resistance published in recent years (Wozniak et al., 2019). In a systematic review on the economic burden of resistant infections, Wozniak and colleagues (2019) commented on this variability: “[E]rroneous or unclear estimates of impact can have alarming effects some of which may contribute to greater action but they also create confusion and potentially undermine the fight against antimicrobial resistance.”
Even a relatively straightforward economic outcome, excess time spent hospitalized, for example, is highly vulnerable to analytic and methodological bias (Naylor et al., 2018; Nelson et al., 2021). Figure 3-11 shows how one recent systematic review identified that different analytic methods, sometimes even reported in the same study, can influence the study’s estimate of excess days hospitalized (Naylor et al., 2018). When measuring excess costs associated with length of hospital stay, for example, studies will often fail to adjust the outcome (i.e., length of stay) to count only those days after the resistant infection started (Wozniak et al., 2019).
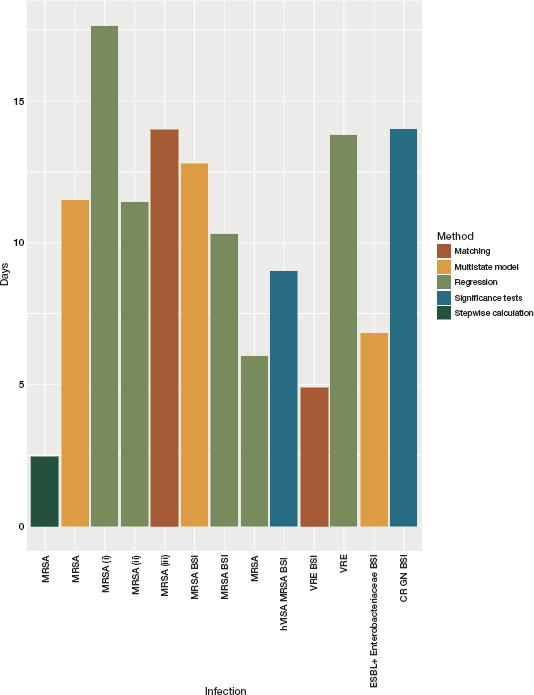
NOTE: BSI = bloodstream infection; CR = carbapenem-resistant; GN = gram-negative; hVISA = heterogeneous vancomycin-intermediate Staphylococcus aureus; MRSA = methicillin-resistant Staphylococcus aureus; VRE = vancomycin-resistant Enterococci.
SOURCE: Naylor et al., 2018.
This time-dependent bias tends to inflate estimates of costs. A recent systematic review found that of 14 studies on the excess costs associated with resistant infections, only two properly accounted for bias in their analyses (Wozniak et al., 2019). After reviewing over 1,000 abstracts the researchers concluded that, while economic valuations of the excess costs associated with resistant infections are sorely needed, especially in low- and middle-income countries, currently the only rigorous and unbiased research available is on health care–associated bloodstream infections with resistant Enterobacterales and MRSA (Wozniak et al., 2019).
Since Wozniak and colleagues published this meta-analysis, some U.S. papers meeting their criteria for adjusting for bias and confounders have come out. Data from the Department of Veterans Affairs (VA), the largest integrated health system in the United States, with linked records containing cost, microbiological, and clinical information, informed the CDC estimates of costs attributable to resistant pathogens presented earlier in this chapter (Nelson et al., 2021). From a final dataset that included almost 25,000 infections, researchers estimated the costs associated with both community- and hospital-acquired infection for six common resistant pathogens (see Table 3-5). Adjusted over the entire United States, estimates of the direct costs associated with these infections is between $4.1 and $5.1 billion (Nelson et al., 2021).
Another recent U.S. study compared costs and mortality in MRSA patients to those in patients infected with methicillin-susceptible Staphylococcus aureus (MSSA) (Klein et al., 2019). After adjusting for the many confounders that can influence difference between these groups of patients, the researchers found that costs of hospitalization for MRSA were roughly the same or less than those for hospitalization with MSSA (Klein et al., 2019). This may, ironically, stem from the increasing burden of MRSA infections acquired in the community (as opposed to in a health care setting), as community-acquired MRSA is generally susceptible to second-line medicines, bringing down the overall costs of treatment (Klein et al., 2019). Heightened attention to MRSA in hospitals may have led to the identification and treatment of some minimally invasive MRSA, which in turn influenced these results. It is also possible that aureus infections, even when susceptible to treatment, are simply difficult to manage in clinical practice.
A 2017 study of the burden of carbapenem-resistant Enterobacterales (CRE) found that the cost of one such infection to the hospital was between $22,993 and $35,503, to the insurer or payer between $13,701 and $18,286 (Bartsch et al., 2017). The authors also considered the cost such infections have on society, a cost influenced mainly by assumptions about mortality attributable to such infections. Assuming mortality attributable to the resistant infection was 35 percent, infection with CRE causes
TABLE 3-5
Adjusted Attributable Cost by Pathogen for Community and Hospital Onset Infections
| Pathogen | Invasivea | Noninvasivea | ||||
|---|---|---|---|---|---|---|
| Estimate | 95% Confidence Interval | Estimate | 95% Confidence Interval | |||
| Community Onset | ||||||
| MRSA | $19,749 | $17,414 | $22,084 | $596 | –$162 | $1,355 |
| VRE | $17,490 | $8,475 | $26,505 | $7,590 | $4,796 | $10,384 |
| ESBL | $7,352 | $3,903 | $10,802 | $3,914 | $1,880 | $5,948 |
| CRE | $8,354 | –$1,191 | $17,899 | $5,154 | $908 | $9,400 |
| CR Acinetobacter | $62,396 | $20,370 | $104,422 | $29,265 | $11,412 | $47,119 |
| MDR Pseudomonas | $13,442 | –$5,257 | $32,140 | $11,882 | $5,987 | $17,776 |
| Hospital Onset | ||||||
| MRSA | $30,998 | $25,272 | $36,724 | $9,588 | $7,088 | $12,087 |
| VRE | $37,893 | $31,598 | $44,188 | $6,835 | $3,630 | $10,039 |
| ESBL | $33,637 | $20,074 | $47,200 | $16,240 | $11,316 | $21,163 |
| CRE | $54,614 | $26,992 | $82,236 | $16,606 | $8,684 | $24,529 |
| CR Acinetobacter | $74,306 | $20,377 | $128,235 | $30,590 | $12,784 | $48,396 |
| MDR Pseudomonas | $66,934 | $32,943 | $100,925 | $50,810 | $41,062 | $60,558 |
NOTE: CI = confidence interval; CR = carbapenem-resistant; CRE = carbapenem-resistant Enterobacterales; ESBL = extended-spectrum beta-lactamase; ICU = intensive care unit; MDR = multidrug-resistant; MRSA = methicillin-resistant Staphylococcus aureus; VRE = vancomycin-resistant Enterococci.
a The CDC (2020) defines invasive disease as when pathogens invade parts of the body, like blood, that are normally free from germs. Noninvasive infections refer to bacteria that do not spread to or damage internal organs and tissues (New Mexico Department of Health, 2021).
SOURCE: Nelson et al., 2021.
between 1,131 and 5,790 deaths a year, costing society between $681 and $3,489 million (Bartsch et al., 2017). Assuming an attributable mortality of 9 percentage points higher would mean 1,422 to 7,279 deaths, costing society between $819 million and $4.2 billion (Bartsch et al., 2017). As a reference, this means the cost of CRE infection alone is higher than many chronic diseases such as high blood pressure (estimated cost to society $672 per patient per year), asthma (estimated direct cost $4,008 per patient per year) and diabetes ($13,015 estimated per patient per year) (Bartsch et al., 2017).
The incurred costs to society from resistant infections is an important point to capture in economic analysis of antimicrobial resistance, partly because of the negative externalities, or the harm associated with antimicrobial use not incurred to the patients or prescriber (Broughton, 2017). The largest part of the negative externality associated with misuse of antimicrobials is the loss of useful antimicrobial medicines in the future. As the previous section explained, the loss of these drugs would influence the risk calculation underlying many basic surgeries as well as more sophisticated treatments such as organ transplantation and cancer chemotherapy. It is difficult to even imagine the potential health consequences of antimicrobial resistance, making the consequent economic burden “at present inestimable” (Smith and Coast, 2013).
The Effects of Antimicrobial Resistance in Food-Producing Animals
As the previous chapter discussed, the contribution of antimicrobial use in food-producing animals to total antimicrobial use and the concentration of resistance genes and drug residues in the environment are a serious concern. Resistance traits that emerge in animals will be found also in manure and water; resistant pathogens from animals can be passed to their handlers, and from them to their family members (Ma et al., 2021). As early as the 1980s researchers have shown an association and plausible pathway through which resistant pathogens emerging in livestock eventually cause human infections (Ma et al., 2021). These include direct contact through consuming food from an infected animal, or indirect routes involving water or a shared environment. Produce can also be a link between resistant bacteria in water or soil and humans (ASM, 2017).
Part of the challenge is that, as in human medicine, it is difficult to know what antimicrobials are being used in livestock and in what doses. The best estimates of use come from U.S. Department of Agriculture (USDA) surveys, which, coupled with the Food and Drug Administration sales data give a rough picture of trends in use (although very little about actual consumption can be inferred from sales data, discussed more in Chapter 5) (Hope et al., 2020). In low- and middle-income countries, the
matter is much more difficult to discern. As emerging economies such as Brazil, Russia, India, and China face an increased demand for animal protein they are shifting to more intensive and more efficient systems for raising chickens and pigs (Van Boeckel et al., 2015). Intensive farming of cattle is generally limited to North America, Argentina, and Brazil (Laxminarayan et al., 2015). The shift in production systems will have an effect on global antimicrobial consumption (Laxminarayan et al., 2015).
The projected rise in the use of antimicrobials in livestock, mostly related to an increased demand for animal protein in low- and middle-income countries, has raised a more urgent need for clarity on if and to what extent antimicrobials use in livestock influences human health. Especially in regard to growth promoters, if the gains in efficiency of production are marginal, then it would be easy to justify prohibitions on antimicrobial growth promoters citing only public health concerns (Laxminarayan et al., 2015). But if the gains are larger, then the burden of proof shifts to establishing that the use of antimicrobial growth promoters in agriculture affects human health (Laxminarayan et al., 2015). This question is difficult to answer. Use of antimicrobial growth promoters has been banned in many countries, including the United States (EU, 2005; FDA, 2021). Data on antimicrobial use on farms are often high-level (i.e., sales data), few countries have farm-level data on antimicrobial use (Mesa Varona et al., 2020). What is more, linking antimicrobial use or resistance data from animals to human health outcomes is tenuous.
Antimicrobial Use and Productivity
Research from Denmark, Sweden, and the United States indicates that in modern production systems, when implemented against a background of good hygiene, feeding practices, and selective breeding, the gains in productivity from using antimicrobial growth promoters is minimal (Laxminarayan et al., 2015). A 2007 analysis found that, in the United States, antimicrobial growth promoters had a negligible effect on poultry productivity, insufficient to offset the cost of medicines used (Graham et al., 2007).
The same is not true in low- and middle-income countries. Research in Brazil and China, for example, has shown antimicrobials to be essential for optimal growth (Ryan, 2019). In China this production advantage helps ensure national food security; antimicrobial use is seen as a cost-effective alternative to expensive biosecurity and farm management systems, a way to compensate for problems with hygiene controls (Ryan, 2019). In Brazil, the economic calculation also favors the use of antimicrobial growth promoters, though the reasons have more to do with maximizing production efficiency in the face of very lean profit margins (Ryan,
2019). As a recent OECD paper concluded, “[F]armers will use preventative medicines such as antibiotics up to the point where the marginal cost of the input is equal to the marginal benefit from the use of this input in their production system” (Ryan, 2019).
Across countries, more attention to animal housing, breeding, feed, and the density of animals on the farm can reduce the need for antimicrobial growth promoters (Ryan, 2019). The same steps help prevent infection in animals, limiting the need for therapeutic antimicrobials as well. Some encouraging evidence indicates that, at least in China, government and public concern about antimicrobial growth promoters is leading to increased restrictions on antimicrobial growth promoters and improvements to infection control measures (Luo et al., 2020; Ryan, 2019; Schoenmakers, 2020).
In low- and middle-income countries, the most pressing economic questions concerning antimicrobial use tend to concern the economic fallout of withdrawing antimicrobial growth promoters. In the United States, European Union, and other high-income countries, where the use of medically important antibiotics as growth promoters is banned, growing momentum for restricting antimicrobial use in food-producing animals is driven by food companies in response to consumer pressure (FDA, 2021; Kesmodel et al., 2014; Singer et al., 2019; WHO, 2017). A major concern of restricting therapeutic and preventive antimicrobial use are the implications for productivity and animal welfare. Yet there is only modest empirical evidence regarding the health and welfare consequences of restricting antimicrobial use (Tang et al., 2019).
Removal of antibiotics could have serious economic consequences. By some estimates, removing preventive and therapeutic antibiotics would cost producers between $43 and $139 for every steer entering the feedlot system in the United States (Lhermie et al., 2020). Removal of metaphylaxis, the use of antimicrobials to treat a group of animals at risk for infectious diseases, could result in a loss in surplus of $1.8 billion to $2.3 billion to U.S. beef producers (Dennis et al., 2018). Prohibition of antimicrobial use in dairy cows could cost the U.S. dairy industry $152 million a year, though the price increase to the consumer would be relatively modest, about $0.42 a liter for milk (Lhermie et al., 2018). Modeling these effects is difficult, however, because of the price volatility of agricultural markets and potential unintended consequences on other domestic markets (increasing sales of organic meat, for example) (Lhermie et al., 2016). As the United States is a major exporter of animal commodities, there could also be effects in foreign markets (Lhermie et al., 2016).
For most farmers and veterinarians, such concerns pale in comparison to questions of animal welfare. Antimicrobial use prohibitions on farms would mean that sick animals were either left untreated or culled
and euthanized (Lhermie et al., 2020). The removal of antimicrobials in poultry production would lead to increasing eye burns, footpad lesions, and airsacculitis,6 for example (Karavolias et al., 2018). There are also, depending on the infection in question, moral obligations to treat and prevent the spread of infection in a flock or herd (Lhermie et al., 2020). In the case of highly contagious and potentially serious diseases, such as bovine respiratory disease, this imperative is more clear than for a disease like infectious liver abscess, which has fewer associated animal welfare consequences (Lhermie et al., 2020).
Removal of antimicrobials from animal agriculture could decrease productivity and increase infectious diseases harming the animals’ health and capability to grow or produce. But these increases in cost will depend on the production systems and diseases in question. Production cycles for poultry are short (several weeks), somewhat longer for swine. For cattle the production cycle is several years long and involves multiple producers (ERS, 2021). The wide difference in production time and producers makes it difficult to generalize the effect of removing antimicrobials. It is clear, however that without effective alternatives and enhanced infection control, removal of antimicrobials could increase disease and mortality, leading to culling and productivity losses.
Serious clinical resistance in animals could also decrease food production with implications for food security, famers’ livelihoods, and environmental contamination (OECD). Losses of animals to resistant infections and the premature culling of herds will mean financial losses to farmers and could cause food prices to rise (Founou et al., 2021).
The economic ramifications of antimicrobial resistance in animal agriculture extends to the cost-to-benefit analysis of upgrading to a more expensive animal management system or treating with more expensive drugs. These are all questions that would benefit from research attention.
The Effects of Resistance on Animal Health
There is growing evidence that livestock are colonized with resistant pathogens (Abdelfattah et al., 2021; Chehabi et al., 2019; de Jong et al., 2018; Harrison et al., 2017). Yet there are major gaps in our knowledge of the effects of resistant infections on animal health. Resistant infections in animals are less well studied than those in humans. In dairy cattle, for example, Staphylococcus aureus causes considerable clinical mastitis, though MRSA and beta-lactam resistance are uncommon (Patel et al., 2021). A better understanding of S. aureus in cattle would be helpful
___________________
6 An inflammation of the air sacs that can cause respiratory distress and watery eyes (Clarke, 2014).
because the pathogen is highly contagious and aggressive culling can be necessary to control it in a herd (Cousin et al., 2018).
In both livestock and companion animals there is concern that resistant infections may be increasing, but it is difficult to say precisely; there are no accepted, standardized definitions of multidrug resistance, extensive drug resistance, and pandrug resistance in veterinary medicine (Sweeney et al., 2018). There is also a lack of epidemiological research on the health consequences of resistant infections in animals.
As with resistant infections in humans, the burden of resistant infections varies considerably by country. Research on the pathogen causing clinical mastitis in dairy cows in Denmark found generally low levels of resistance, with the exception of about 83 percent of Klebsiella pneumoniae isolates being resistant to ampicillin (Chehabi et al., 2019). Research on feedlot cattle across southern Alberta, Canada, found that over 90 percent of the pathogens causing bovine respiratory disease were resistant to macrolide antimicrobials, almost half of the pathogens were resistant to four or five different antimicrobial classes, and about a quarter were resistant to six of the nine available drug classes (Anholt et al., 2017). In general, resistance was less common among the antimicrobials of critical importance to human health and more common among the tetracycline and macrolide medicines often added to cattle feeds to prevent liver abscess in the feedlot-raised cattle (Anholt et al., 2017).
As in humans, MRSA infections in livestock are difficult to treat. Contamination from retail meat is a source of MRSA infections in humans (Anjum et al., 2019; O’Brien et al., 2012). Heavy metal contamination, common on farms and in food production systems, can co-select for resistance in S. aureus and may be contributing to an increasing burden of MRSA infections in livestock (Dweba et al., 2018). At the same time, humans are the main reservoir of MRSA infections (Dweba et al., 2018). The transmission of MRSA from animals to human handlers is relatively well documented (Pirolo et al., 2019). Meta-analysis indicates that veterinarians and livestock workers, especially pig farmers, are at elevated risk for acquiring MRSA from animals (Chen and Wu, 2020). There are also examples of humans transmitting MRSA to animals (Magro et al., 2018). Most of the research on these pathways is from North America and Europe, however. It is likely that in parts of the world where contact between humans and livestock is more common in the general population, the risk of interspecies transmission is more general and not limited to farmers, animal handlers, or veterinarians.
In general, the way resistant pathogens spread between humans and animals is not well studied (Wee et al., 2020). Genomic sequencing has the potential to illuminate major pathways from which resistant bacteria travel directly between species and indirectly through a shared environ-
mental element, such as water or soil (Wee et al., 2020). Genomic analysis has, for example, indicated that Acinetobacter baumannii has likely spread from humans to animals (directly or via an environmental intermediary) (Argudin et al., 2017). Genomic studies also suggest that mecA, a gene that confers resistance to methicillin, may have originated in staphylococcal infections in animals (Argudin et al., 2017). In the reverse pathway, resistance linked to extended-spectrum beta-lactamase and carbapenemase, enzymes that destroy commonly used antimicrobials, may be emerging in animals (Hartantyo et al., 2018). There is a need for more research across human, animal, and environmental health to determine the health burden of resistance and clarify major pathways for the spread of resistant organisms.
DEVELOPING MORE PRECISE ESTIMATES OF THE BURDEN OF ANTIMICROBIAL RESISTANCE
Measuring antimicrobial resistance is difficult. Unlike most global health challenges, the problem is not any one disease or risk factor, but a process. Resistance can emerge in any number of microbial pathogens, and resistant infections can present in different ways (e.g., pneumonia, skin infection, urinary tract infection). For these reasons, traditional tools for estimating the burden of disease, such as analysis of cause of death on death certificates, are not suited to the problem (Dunachie et al., 2020). What is more, any analysis of disease burden depends on microbiological confirmation of the infective agent. A lack of microbiology laboratories seriously holds back surveillance in low- and middle-income countries. National estimates of resistance in India, for example, a country of over 1.3 billion people, are “drawn from a few thousand laboratory isolates and a handful of hospitals” (Islam et al., 2019).
The biggest barrier to producing better estimates of the burden of antimicrobial resistance is the lack of microbiological data (Dunachie et al., 2020). Figure 3-12 shows multiple barriers to producing this data, from limited capacity for microbiological analysis and difficulties with quality assurance to difficulties linking the data to patient records (Dunachie et al., 2020). There are also biases in blood culture data. Especially in low- and middle-income countries where blood cultures are paid entirely out of pocket, this data is available only for relatively affluent, urban patients (Dunachie et al., 2020; Hay et al., 2018).
Other barriers relate to data analysis. Data sharing is challenging around the world, partly because data about resistance is sensitive and the fear of being exposed as a resistance hotspot deters sharing from the clinic to the national level (Dunachie et al., 2020). Data sharing, while desirable, has to be done in an orderly and balanced way. Datasets can
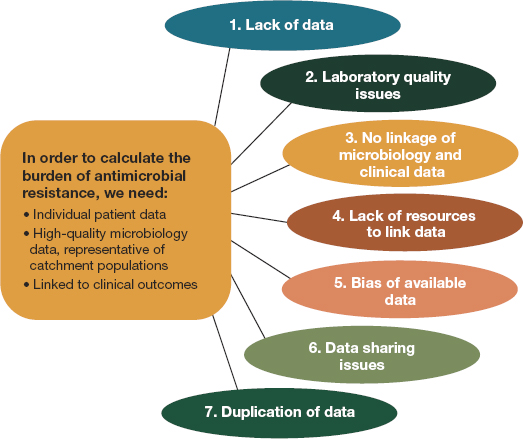
SOURCE: Dunachie et al., 2020.
easily be shared with many groups of researchers biasing perceptions of resistance if the same data informed multiple, seemingly different, studies (Dunachie et al., 2020).
The laboratory infrastructures that underlie surveillance are challenging to coordinate even in the United States and other high-income countries, a topic discussed more in the next chapter. While improving surveillance systems around the world will be essential to better measure the health and economic consequences of resistance, surveillance is not the only tool to this end. More research on the burden of antimicrobial resistance is needed, especially in low- and middle-income countries. But even with data of high quality, easily linked to the patient records in a single-payer system, as is available in the VA data that informs the CDC estimates discussed earlier in this chapter, different analytic strategies could yield widely different conclusions about the nature of the problem (Dunachie et al., 2020). For one thing, it is difficult to know the best comparator group for patients with resistant infections. Comparison to patients with susceptible infections or without infections are both complicated as the groups would not usually have the same comorbidities (Dunachie et al., 2020). Attention to such questions in study design, drawing on the research guidelines presented in Box 3-1 could help avoid some of the methodological problems studies on the burden of antimicrobial-resistant infections often face.
Another challenge related to measuring the burden and consequences of resistance stem from the complex, adaptive nature of the problem described in the previous chapter. The toll of resistance, be it on human health, the economy, animal agriculture, or farmers’ livelihoods, cannot be considered in isolation (Dunachie et al., 2020). This is not to say that researchers should incorporate human, animal, and environmental health indicators in all their work. Rather, across disciplines researchers, government officials, and private industry could all give better attention to capturing the costs associated with resistant infections.
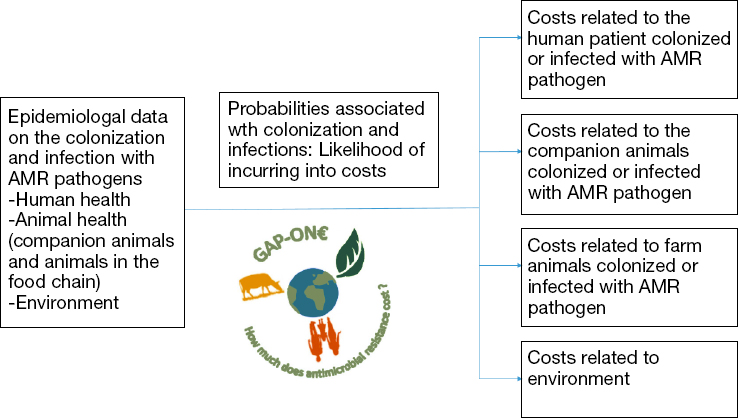
The Global Antimicrobial Resistance Platform for ONE-Burden Estimates, an international research network, recently released a One Health framework for estimating the costs of resistance (Morel et al., 2020). This framework, introduced in Figure 3-13, articulates what costs, both direct and indirect, will be affected by resistance in human and animal health and in the environment (Morel et al., 2020).
The international momentum for action against antimicrobial resistance driven by the O’Neill report and the other recent landmark publications described at the beginning of this chapter is commendable. Following through on this energy and translating it into meaningful policy
NOTE: AMR = antimicrobial resistance.
SOURCE: Adapted from Morel et al., 2020.
changes requires good evidence on the true burden of resistance and what interventions work to reduce that burden (Hay et al., 2018; IHME, 2020a; Morel et al., 2020).
The Global Research on Antimicrobial Resistance Project
The Global Burden of Disease, Injuries, and Risk Factors program on antimicrobial resistance (the Global Research on Antimicrobial Resistance project) is a welcome addition to the literature on the health consequences of antimicrobial resistance (IHME, 2020a).7 This analysis of the health consequences of 23 resistant bacteria (88 microbe–drug combinations) drew on 471 million patient records or isolates from collaborators and public data from around the world (AMR Collaborators, in review). Under a counterfactual assumption of infection with a susceptible pathogen, the authors estimated that antimicrobial resistance killed 1.27 million people in 2019 (95% confidence interval [CI]: 0.91 to 1.71 million) (AMR Collaborators, in review). Such analysis suggests that antimicrobial resistance is the 12th leading cause of death worldwide (AMR Collaborators, in
___________________
7 This study was in review during the committee’s final deliberations, and the committee thanks the researchers for sharing some key findings.
review).8 Under a counterfactual assumption of no infection the estimate was 4.95 million deaths associated with antimicrobial resistance (95% CI: 3.62 million to 6.57 million) (AMR Collaborators, in review). Despite limited data from low- and middle-income countries, the models indicated that this is where the burden of resistance is worst, with death rates from antimicrobial resistance highest in sub-Saharan Africa (AMR Collaborators, in review).
Of the 23 pathogens studied, six (E.coli, S. aureus, K. pneumoniae, Streptococcus pneumoniae, Acinetobacter baumannii, and Pseudomonas aeruginosa) accounted for a majority (about 72 percent) of deaths (AMR Collaborators, in review). MRSA, a serious burden in high-income countries, caused an estimated 100,000 deaths worldwide in 2019 (AMR Collaborators, in review).
The Global Research on Antimicrobial Resistance study provides a scientifically rigorous framework through which to evaluate antimicrobial resistance and an exhaustive review of the epidemiological data to estimate its burden (IHME, 2020b). Generating comparable estimates of the burden of resistance in key microbe-drug combinations across countries is especially valuable (IHME, 2020c). As Table 3-6 shows, even the estimates of the health consequences of resistant infections vary so widely, including variability in the way they are reported, that it is difficult to identify trends in the literature.
The Economic Component of Antimicrobial Resistance
The problem of wide variability in research is more obvious in reviewing estimates of the economic consequences of resistance. As Table 3-3 showed, even economic researchers working on similar datasets and making ostensibly similar analytic assumptions can arrive at such widely different estimates of the problem as to be unrecognizable. It may be that the most important message regarding the economic fallout of antimicrobial resistance is that it cannot be compartmentalized. As the COVID-19 epidemic has made clear, infectious outbreaks can devastate the global economy and people’s quality of life in far-reaching ways. Even estimates of the cost of the pandemic in the trillions do not account for the long-term, less tangible consequences of disrupted schooling and income (Cutler and Summers, 2020).
Antimicrobial resistance is a One Health problem, so estimating its economic component means untangling the relative contributions of resis-
___________________
8 Among Global Burden of Disease level three causes, “specific causes such as tuberculosis, stroke, and road injuries” sometimes the most detailed cause of death classifications available (Lancet, 2020).
| Publication Year | Report | Measure | Quantity | Geographic Area |
|---|---|---|---|---|
| 2019 | AR Threats Report | Deaths per year | 35,900 | United States |
| 2019 | AR Threats Report | Deaths per year (drug-resistant C. difficile) | 12,800 | United States |
| 2018 | Stemming the Superbug Tide | Deaths per year, 2015 to 2050 | 30,000 | United States |
| 2018 | Stemming the Superbug Tide | Deaths per year | 60,000 | United States, Europe |
| 2018 | Stemming the Superbug Tide | Deaths per year, 2015 to 2050 | 2.4 million | North America, Europe, Australia |
| 2018 | Stemming the Superbug Tide | DALYs lost per year | 1.75 million | 33 high-income countries |
| 2014 | O’Neill report’s RAND model | Cumulative deaths 2015 to 2050 | 11 to 444 million adults | Global |
| 2014 | O’Neill report’s KPMG model | Cumulative deaths 2015 to 2050 | 200 to 700 million | Global |
| 2014 | The O’Neill report | Deaths per year by 2050 | 10 million | Global |
| 2019 | European CDC, Cassini and colleagues | Deaths in 2015 | 33,000 | Europe |
| 2021 | The Global Burden of Disease | Deaths caused by infection with a resistant pathogen in 2019 | 0.91 to 1.71 million | Worldwide |
| 2021 | The Global Burden of Disease | Deaths associated with infection with a resistant pathogen in 2019 | 3.62 to 6.57 million | Worldwide |
SOURCES: AMR Collaborators; CDC, 2019; KPMG LLP, 2014; OECD, 2018; O’Neill, 2014; Taylor et al., 2014.
tance in any one sector and tying them to larger economic indicators. This is not a direct analytic question, and the economic fallout of resistance is not easily reduced to a number. The burden of any one resistant pathogen depends on context; the same resistant infections can have drastically different consequences in humans or animals, if acquired in a hospital or outside of it, in a high-income country or a low-income one. The downstream consequences of resistant infections can be felt on food safety, on livelihoods, on social relationships, and, of course, on health. A lack of communication among the different One Health disciplines may
contribute a relatively one-sided body of research on the health and economic effects of resistant infections in humans. This is a major barrier to developing better estimates of the consequences of resistance.
REFERENCES
Abdelfattah, E. M., P. S. Ekong, E. Okello, T. Chamchoy, B. M. Karle, R. A. Black, D. Sheedy, W. R. ElAshmawy, D. R. Williams, D. Califano, L. F. D. Tovar, J. Ongom, T. W. Lehenbauer, B. A. Byrne, and S. S. Aly. 2021. Epidemiology of antimicrobial resistance (AMR) on California dairies: Descriptive and cluster analyses of amr phenotype of fecal commensal bacteria isolated from adult cows. PeerJ 9:e11108.
Ahmed, S. A., E. Barış, D. S. Go, H. Lofgren, I. Osorio-Rodarte, and K. Thierfelder. 2017. Assessing the global economic and poverty effects of antimicrobial resistance. World Bank Policy Research Working Paper No. 8133. https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3006207 (accessed June 25, 2021).
AMR Collaborators. In Review. Global burden of bacterial antimicrobial resistance in 2019. Lancet.
Anholt, R. M., C. Klima, N. Allan, H. Matheson-Bird, C. Schatz, P. Ajitkumar, S. J. Otto, D. Peters, K. Schmid, M. Olson, T. McAllister, and B. Ralston. 2017. Antimicrobial susceptibility of bacteria that cause bovine respiratory disease complex in Alberta, Canada. Frontiers in Veterinary Science 4:207.
Anjum, M. F., F. Marco-Jimenez, D. Duncan, C. Marin, R. P. Smith, and S. J. Evans. 2019. Livestock-associated methicillin-resistant Staphylococcus aureus from animals and animal products in the UK. Frontiers in Microbiology 10:2136.
Argudin, M. A., A. Deplano, A. Meghraoui, M. Dodemont, A. Heinrichs, O. Denis, C. Nonhoff, and S. Roisin. 2017. Bacteria from animals as a pool of antimicrobial resistance genes. Antibiotics (Basel) 6(2):12.
ASM (American Society for Microbiology). 2017. Antibiotic-resistant bacteria in ready-to-eat foods. Science Daily. www.sciencedaily.com/releases/2017/06/170605121333.htm (accessed August 4, 2021).
Bartsch, S. M., J. A. McKinnell, L. E. Mueller, L. G. Miller, S. K. Gohil, S. S. Huang, and B. Y. Lee. 2017. Potential economic burden of carbapenem-resistant enterobacteriaceae (CRE) in the United States. Clinical Microbiology and Infection 23(1):48.e9-48.e16. https://www.sciencedirect.com/science/article/pii/S1198743X16303895 (accessed June 22, 2021).
BBC News. 2016. Global antibiotics “revolution” needed. BBC News Media. https://www.bbc.com/news/health-36321394 (accessed September 22, 2021).
Boseley, S. 2016. No antibiotics without a test, says report on rising antimicrobial resistance. The Guardian. https://www.theguardian.com/society/2016/may/19/no-antibiotics-without-a-test-says-report-on-rising-antimicrobial-resistance (accessed September 22, 2021).
Broughton, E. I. 2017. The economics of reducing antibiotic use to reduce antimicrobial resistance. http://resistancecontrol.info/2017/the-economics-of-reducing-antibiotic-use-to-reduce-antimicrobial-resistance (accessed June 23, 2021).
Carr, A., J. A. Smith, J. Camaradou, and D. Prieto-Alhambra. 2021. Growing backlog of planned surgery due to COVID-19. BMJ 372:n339.
Cassini, A., L. D. Hogberg, D. Plachouras, A. Quattrocchi, A. Hoxha, G. S. Simonsen, M. Colomb-Cotinat, M. E. Kretzschmar, B. Devleesschauwer, M. Cecchini, D. A. Ouakrim, T. C. Oliveira, M. J. Struelens, C. Suetens, D. L. Monnet, and Burden of AMR Collaborative Group. 2019. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European economic area in 2015: A population-level modelling analysis. Lancet Infectious Diseases 19(1):56-66.
CDC (Centers for Disease Control and Prevention). 2013. Antibiotic resistance threats in the United States. Atlanta, GA: Centers for Disease Control and Prevention, Department of Health and Human Services.
CDC. 2019. Antibiotic resistance threats in the United States, 2019. Atlanta, GA: Centers for Disease Control and Prevention. http://dx.doi.org/10.15620/cdc:82532.
CDC. 2020. Surveillance. https://www.cdc.gov/hi-disease/surveillance.html (accessed September 15, 2021).
CDC, NCEZID (National Center for Emerging and Zoonotic Diseases), and DHQP (Division of Healthcare Quality Promotion). 2021. Healthcare settings and antibiotic resistance. https://www.cdc.gov/drugresistance/solutions-initiative/healthcare.html#anchor_1576259604118 (accessed June 23, 2021).
Cecchini, M., J. Langer, and L. Slawomirski. 2015. Antimicrobial resistance in the G7 countries and beyond. Paris, France: Organisation for Economic Co-operation and Development. https://www.oecd.org/els/health-systems/Antimicrobial-Resistance-in-G7-Countries-and-Beyond.pdf (accessed June 23, 2021).
Chehabi, C. N., B. Nonnemann, L. B. Astrup, M. Farre, and K. Pedersen. 2019. In vitro antimicrobial resistance of causative agents to clinical mastitis in Danish dairy cows. Foodborne Pathogens and Disease 16(8):562-572.
Chen, C., and F. Wu. 2020. Livestock-associated methicillin-resistant Staphylococcus aureus (LA-MRSA) colonisation and infection among livestock workers and veterinarians: A systematic review and meta-analysis. Occupational and Environmental Medicine 78(7):530-540. https://oem.bmj.com/content/oemed/78/7/530.full.pdf (accessed July 14, 2021).
Clarke, P. 2014. How to control airsacculitis in broilers. https://www.fwi.co.uk/livestock/poultry/broilers/how-to-control-airsacculitis-in-chickens (accessed July 20, 2021).
Cousin, M. E., M. C. Hardi-Landerer, V. Volk, and M. Bodmer. 2018. Control of Staphylococcus aureus in dairy herds in a region with raw milk cheese production: Farmers’ attitudes, knowledge, behaviour and belief in self-efficacy. BMC Veterinary Research 14(1):46.
COVIDSurg Collaborative. 2020. Elective surgery cancellations due to the COVID-19 pandemic: Global predictive modelling to inform surgical recovery plans. British Journal of Surgery 107(11):1440-1449.
Cutler, D. M., and L. H. Summers. 2020. The COVID-19 pandemic and the $16 trillion virus. JAMA 324(15):1495-1496.
de Jong, A., F. E. Garch, S. Simjee, H. Moyaert, M. Rose, M. Youala, E. Siegwart, and G. VetPath Study. 2018. Monitoring of antimicrobial susceptibility of udder pathogens recovered from cases of clinical mastitis in dairy cows across Europe: Vetpath results. Veterinary Microbiology 213:73-81.
de Kraker, M. E., A. J. Stewardson, and S. Harbarth. 2016. Will 10 million people die a year due to antimicrobial resistance by 2050? PLoS Medicine 13(11):e1002184.
Denison, J., and P. AV. 2010. Accuracy of death certifications and the implications for studying disease burdens. In Handbook of disease burdens and quality of life measures, edited by V. R. Preedy and R. R. Watson. New York: Springer. Pp. 329–344.
Dennis, E. J., T. C. Schroeder, D. G. Renter, and D. L. Pendell. 2018. Value of arrival metaphylaxis in U.S. cattle industry. Faculty Publications: Agricultural Economics 181.
Dunachie, S. J., N. P. Day, and C. Dolecek. 2020. The challenges of estimating the human global burden of disease of antimicrobial resistant bacteria. Current Opinion in Microbiology 57:95-101.
Dweba, C. C., O. T. Zishiri, and M. E. El Zowalaty. 2018. Methicillin-resistant Staphylococcus aureus: Livestock-associated, antimicrobial, and heavy metal resistance. Infection and Drug Resistance 11:2497-2509.
ERS (Economic Research Service). 2021. Sector at a glance. https://www.ers.usda.gov/topics/animal-products/cattle-beef/sector-at-a-glance (accessed July 20, 2021).
EU (European Union). 2005. Ban on antibiotics as growth promoters in animal feed enters into effect. Brussels, Belgium: European Commission. https://ec.europa.eu/commission/presscorner/detail/en/IP_05_1687 (accessed July 20, 2021).
FAO and UN (Food and Agriculture of the United Nations and United Nations). 2021. Antimicrobial resistance. http://www.fao.org/antimicrobial-resistance/en (accessed September 22, 2021).
FDA (U.S. Food and Drug Administration). 2021. Timeline of FDA action on antimicrobial resistance. https://www.fda.gov/animal-veterinary/antimicrobial-resistance/timeline-fda-action-antimicrobial-resistance (accessed June 22, 2021).
Foster, S. 2011 (unpublished). Challenges for healthcare: The impact of AMR on costs of care. https://www.paho.org/hq/dmdocuments/2011/3_Foster_DMS_2011.pdf (accessed September 22, 2021).
Founou, L. L., R. C. Founou, and S. Y. Essack. 2021. Antimicrobial resistance in the farm-to-plate continuum: More than a food safety issue. Future Science OA 7(5):FSO692.
Friedman, E. A. 2020. Behind the headlines: 10 million deaths from antimicrobial resistance by 2050 (or not?). Georgetown Law 02/12/2020. https://oneill.law.georgetown.edu/behind-the-headlines-10-million-antimicrobial-deaths-by-2050-or-not (accessed September 22, 2021).
Gandra, S., G. Alvarez-Uria, P. Turner, J. Joshi, D. Limmathurotsakul, and H. R. van Doorn. 2020. Antimicrobial resistance surveillance in low- and middle-income countries: Progress and challenges in eight south Asian and southeast Asian countries. Clinical Microbiology Reviews 33(3):e00048-00019.
Graham, J. P., J. J. Boland, and E. Silbergeld. 2007. Growth promoting antibiotics in food animal production: An economic analysis. Public Health Reports 122(1):79-87.
Harrison, E. M., F. Coll, M. S. Toleman, B. Blane, N. M. Brown, M. E. Torok, J. Parkhill, and S. J. Peacock. 2017. Genomic surveillance reveals low prevalence of livestock-associated methicillin-resistant Staphylococcus aureus in the east of England. Scientific Reports 7(1):7406.
Hartantyo, S. H. P., M. L. Chau, L. Fillon, A. Ariff, J. S. L. Kang, K. T. Aung, and R. A. Gutierrez. 2018. Sick pets as potential reservoirs of antibiotic-resistant bacteria in Singapore. Antimicrobial Resistance & Infection Control 7(1):106.
Hay, S. I., P. C. Rao, C. Dolecek, N. P. J. Day, A. Stergachis, A. D. Lopez, and C. J. L. Murray. 2018. Measuring and mapping the global burden of antimicrobial resistance. BMC Medicine 16(1):78.
Hope, K. J., M. D. Apley, N. F. D. Schrag, B. V. Lubbers, and R. S. Singer. 2020. Antimicrobial use in 22 U.S. beef feedyards: 2016-2017. Zoonoses and Public Health 67(Suppl 1):94-110.
IACG (Interagency Coordination Group on Antimicrobial Resistance). 2019. No time to wait: Securing the future from drug-resistant infections. Geneva, Switzerland: World Health Organization.
IHME (Institute for Health Metrics and Evalution). 2020a. GRAM project deliverables and scope. http://www.healthdata.org/gram/scope (accessed July 14, 2021).
IHME. 2020b. Introducing the GRAM project: Estimating the global burden of antimicrobial resistance. http://www.healthdata.org/sites/default/files/files/infographics/Infographic_GRAM_Intro_2020.pdf (accessed July 14, 2021).
IHME. 2020c. What does the GRAM project need to estimate the global burden of antimicrobial resistance (AMR)? http://www.healthdata.org/sites/default/files/files/infographics/Infographic_GRAM_Data%20Needs_2020.pdf (accessed July, 14, 2021).
Iskandar, K., L. Molinier, S. Hallit, M. Sartelli, T. C. Hardcastle, M. Haque, H. Lugova, S. Dhingra, P. Sharma, S. Islam, I. Mohammed, I. Naina Mohamed, P. A. Hanna, S. E. Hajj, N. A. H. Jamaluddin, P. Salameh, and C. Roques. 2021. Surveillance of antimicrobial resistance in low- and middle-income countries: A scattered picture. Antimicrobial Resistance & Infection Control 10(1):63.
Islam, S., J. Aldstadt, and D. Aga. 2019. Global antimicrobial resistance: A complex and dire threat with few definite answers. Tropical Medicine and International Health 24(6):658-662.
Kadri, S. S. 2020. Key takeaways from the U.S. CDC’s 2019 antibiotic resistance threats report for frontline providers. Critical Care Medicine 48(7):939-945.
Karavolias, J., M. J. Salois, K. T. Baker, and K. Watkins. 2018. Raised without antibiotics: Impact on animal welfare and implications for food policy. Translational Animal Science 2(4):337-348. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7200433/pdf/txy016.pdf (accessed July 20, 2021).
Kesmodel, D., J. Bunge, and B. McKay. 2014. Meat companies go antibiotics-free as more consumers demand it. The Wall Street Journal. https://www.wsj.com/articles/meat-companies-go-antibiotics-free-as-more-consumers-demand-it-1415071802 (accessed June 25, 2021).
Klein, E. Y., W. Jiang, N. Mojica, K. K. Tseng, R. McNeill, S. E. Cosgrove, and T. M. Perl. 2019. National costs associated with methicillin-susceptible and methicillin-resistant Staphylococcus aureus hospitalizations in the United States, 2010-2014. Clinical Infectious Diseases 68(1):22-28.
Knight, G. M., R. E. Glover, C. F. McQuaid, I. D. Olaru, K. Gallandat, Q. J. Leclerc, N. M. Fuller, S. J. Willcocks, R. Hasan, E. van Kleef, and C. I. Chandler. 2021. Antimicrobial resistance and COVID-19: Intersections and implications. Elife 10.
KPMG LLP. 2014. The global economic impact of anti-microbial resistance. https://assets.kpmg/content/dam/kpmg/pdf/2014/12/amr-report-final.pdf (accessed June 23, 2021).
Kwon, J. H., and W. G. Powderly. 2021. The post-antibiotic era is here. Science 373(6554):471.
Lai, A. G., L. Pasea, A. Banerjee, G. Hall, S. Denaxas, W. H. Chang, M. Katsoulis, B. Williams, D. Pillay, M. Noursadeghi, D. Linch, D. Hughes, M. D. Forster, C. Turnbull, N. K. Fitzpatrick, K. Boyd, G. R. Foster, T. Enver, V. Nafilyan, B. Humberstone, R. D. Neal, M. Cooper, M. Jones, K. Pritchard-Jones, R. Sullivan, C. Davie, M. Lawler, and H. Hemingway. 2020. Estimated impact of the COVID-19 pandemic on cancer services and excess 1-year mortality in people with cancer and multimorbidity: Near real-time data on cancer care, cancer deaths and a population-based cohort study. BMJ Open 10(11):e043828.
Lancet. 2020. Global burden of disease 2019 disease, injury, and impairment summaries. Lancet 396. https://els-jbs-prod-cdn.jbs.elsevierhealth.com/pb-assets/Lancet/gbd/disease_injury_impairment_panel-1602684009960.pdf (accessed September 30, 2021).
Langford, B. J., M. So, S. Raybardhan, V. Leung, D. Westwood, D. R. MacFadden, J. R. Soucy, and N. Daneman. 2020. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clinical Microbiology and Infection 26(12):1622-1629.
Laxminarayan, R., T. V. Boeckel, and A. Teillant. 2015. The economic costs of withdrawing antimicrobial growth promoters from the livestock sector. Paris, France: Organisation for Economic Co-operation and Development. https://www.oecd-ilibrary.org/content/paper/5js64kst5wvl-en (accessed July 13, 2021).
Lhermie, G., Y. T. Grohn, and D. Raboisson. 2016. Addressing antimicrobial resistance: An overview of priority actions to prevent suboptimal antimicrobial use in food-animal production. Frontiers in Microbiology 7:2114.
Lhermie, G., L. W. Tauer, and Y. T. Gröhn. 2018. An assessment of the economic costs to the U.S. dairy market of antimicrobial use restrictions. Preventative Veterinary Medicine 160(1873-1716 (Electronic)):63-67.
Lhermie, G., P. Sauvage, L. W. Tauer, L. V. Chiu, K. Kanyiamattam, A. Ferchiou, D. Raboisson, H. M. Scott, D. R. Smith, and Y. T. Grohn. 2020. Economic effects of policy options restricting antimicrobial use for high risk cattle placed in U.S. feedlots. PloS One 15(9):e0239135.
Lopez, A. D., C. D. Mathers, M. Ezzati, D. T. Jamison, and C. J. L. Murray. 2006. Global burden of disease and risk factors, Global burden of disease and risk factors. New York: The World Bank.
Luo, Q., Y. Wang, and Y. Xiao. 2020. Prevalence and transmission of mobilized colistin resistance (MCR) gene in bacteria common to animals and humans. Biosafety and Health 2(2):71-78.
Ma, F., S. Xu, Z. Tang, Z. Li, and L. Zhang. 2021. Use of antimicrobials in food animals and impact of transmission of antimicrobial resistance on humans. Biosafety and Health 3(1):32-38.
Magro, G., M. Rebolini, D. Berettac, and R. Piccinini. 2018. Methicillin-resistant Staphylococcus aureus CC22-MRSA-IV as an agent of dairy cow intramammary infections. Veterinary Microbiology 227:29-33. https://www.sciencedirect.com/science/article/pii/S0378113518306060 (accessed July 14, 2021).
Matthiessen, L., R. Bergstrom, S. Dustdar, P. Meulien, and R. Draghia-Akli. 2016. Increased momentum in antimicrobial resistance research. Lancet 388(10047):865.
Mesa Varona, O., K. Chaintarli, B. Muller-Pebody, M. F. Anjum, T. Eckmanns, M. Norstrom, I. Boone, and B. A. Tenhagen. 2020. Monitoring antimicrobial resistance and drug usage in the human and livestock sector and foodborne antimicrobial resistance in six European countries. Infection and Drug Resistance 13:957-993.
Morel, C. M., R. A. Alm, C. Ardal, A. Bandera, G. M. Bruno, E. Carrara, G. L. Colombo, M. E. A. de Kraker, S. Essack, I. Frost, B. Gonzalez-Zorn, H. Goossens, L. Guardabassi, S. Harbarth, P. S. Jorgensen, S. S. Kanj, T. Kostyanev, R. Laxminarayan, F. Leonard, G. L. Hara, M. Mendelson, M. Mikulska, N. T. Mutters, K. Outterson, J. R. Bano, E. Tacconelli, L. Scudeller, and GAP-ON€ Network. 2020. A One Health framework to estimate the cost of antimicrobial resistance. Antimicrobial Resistance & Infection Control 9(1):187.
Nau, R., F. Sorgel, and H. W. Prange. 1998. Pharmacokinetic optimisation of the treatment of bacterial central nervous system infections. Clinical Pharmacokinetics 35(3):223-246.
Nau, R., F. Sorgel, and H. Eiffert. 2010. Penetration of drugs through the blood-cerebrospinal fluid/blood-brain barrier for treatment of central nervous system infections. Clinical Microbiology Reviews 23(4):858-883.
Naylor, N. R., R. Atun, N. Zhu, K. Kulasabanathan, S. Silva, A. Chatterjee, G. M. Knight, and J. V. Robotham. 2018. Estimating the burden of antimicrobial resistance: A systematic literature review. Antimicrobial Resistance & Infection Control 7:58.
Nelson, R. E., K. M. Hatfield, H. Wolford, M. H. Samore, R. D. Scott, S. C. Reddy, B. Olubajo, P. Paul, J. A. Jernigan, and J. Baggs. 2021. National estimates of healthcare costs associated with multidrug-resistant bacterial infections among hospitalized patients in the United States. Clinical Infectious Diseases 72(Suppl 1):S17-S26.
New Mexico Department of Health. 2021. Non-invasive group a streptococcus (gas). https://www.nmhealth.org/publication/view/general/5205 (accessed September 24, 2021).
O’Brien, A. M., B. M. Hanson, S. A. Farina, J. Y. Wu, J. E. Simmering, S. E. Wardyn, B. M. Forshey, M. E. Kulick, D. B. Wallinga, and T. C. Smith. 2012. MRSA in conventional and alternative retail pork products. PloS One 7(1):e30092.
OECD (Organisation for Economic Co-operation and Development). 2016. Antimicrobial resistance policy insights. Paris, France: Organisation for Economic Co-operation and Development. https://www.oecd.org/health/health-systems/AMR-Policy-Insights-November2016.pdf (accessed April 8, 2021).
OECD. 2018. Stemming the superbug tide, OECD health policy studies. https://doi.org/10.1787/9789264307599-en.
OECD. 2021. Anti-microbial resistance is a global challenge for food systems and public health. https://www.oecd.org/agriculture/topics/antimicrobial-resistance-and-agriculture (accessed June 25, 2021).
O’Neill, J. 2014. Antimicrobial resistance: Tackling a crisis for the health and wealth of nations. London, UK: Wellcome Trust.
O’Neill, J. 2016a. Jim O’Neill. Nature Reviews Drug Discovery 15(8):526.
O’Neill, J. 2016b. Tackling drug-resistant infections globally: Final report and recommendations. London, UK: Government of the United Kingdom and Wellcome Trust. https://wellcomecollection.org/works/thvwsuba (accessed April 8, 2021).
O’Neill, J. n.d. Review on antimicrobial resistance—tackling drug resistance globally. https://amr-review.org (accessed June 22, 2021).
Patel, K., S. M. Godden, E. E. Royster, B. A. Crooker, T. J. Johnson, E. A. Smith, and S. Sreevatsan. 2021. Prevalence, antibiotic resistance, virulence and genetic diversity of Staphylococcus aureus isolated from bulk tank milk samples of U.S. dairy herds. BMC Genomics 22(1):367.
Pelfrene, E., R. Botgros, and M. Cavaleri. 2021. Antimicrobial multidrug resistance in the era of COVID-19: A forgotten plight? Antimicrobial Resistance & Infection Control 10(1):21.
Pirolo, M., D. Visaggio, A. Gioffre, I. Artuso, M. Gherardi, G. Pavia, P. Samele, L. Ciambrone, R. Di Natale, G. Spatari, F. Casalinuovo, and P. Visca. 2019. Unidirectional animal-to-human transmission of methicillin-resistant staphylococcus aureus ST398 in pig farming; evidence from a surveillance study in southern Italy. Antimicrobial Resistance & Infection Control 8(1):187.
PLOS Medicine Editors. 2016. Antimicrobial resistance: Is the world unprepared? PLoS Medicine 13(9):e1002130.
Price, R. 2016. O’Neill report on antimicrobial resistance: Funding for antimicrobial specialists should be improved. European Journal of Hospital Pharmacy 23(4):245-247.
Rodriguez-Bano, J., G. M. Rossolini, C. Schultsz, E. Tacconelli, S. Murthy, N. Ohmagari, A. Holmes, T. Bachmann, H. Goossens, R. Canton, A. P. Roberts, B. Henriques-Normark, C. J. Clancy, B. Huttner, P. Fagerstedt, S. Lahiri, C. Kaushic, S. J. Hoffman, M. Warren, G. Zoubiane, S. Essack, R. Laxminarayan, and L. Plant. 2021. Key considerations on the potential impacts of the COVID-19 pandemic on antimicrobial resistance research and surveillance. Transactions of the Royal Society of Tropical Medicine and Hygiene 115(10):1122-1129.
Roland, D. 2015. Multibillion-dollar investment needed to fight drug-resistant “superbugs.” The Wall Street Journal. https://www.wsj.com/articles/pharma-industry-needs-billions-of-dollars-for-antibiotics-research-1431558248 (accessed June 23, 2021).
Ryan, M. 2019. Evaluating the economic benefits and costs of antimicrobial use in food-producing animals. In OECD Food, Agriculture and Fisheries Papers. Paris, France: Organisation for Economic Co-operation and Development.
Schnall, J., A. Rajkhowa, K. Ikuta, P. Rao, and C. E. Moore. 2019. Surveillance and monitoring of antimicrobial resistance: Limitations and lessons from the gram project. BMC Medicine 17(1):176.
Schoenmakers, K. 2020. How china is getting its farmers to kick their antibiotics habit. Nature 586:2.
Scott, R. D. 2009. The direct medical costs of healthcare-associated infections in U.S. hospitals and the benefits of prevention. National Center for Preparedness, Detection, and Control of Infectious Diseases (U.S.). Division of Healthcare Quality Promotion. https://stacks.cdc.gov/view/cdc/11550 (accessed June 23, 2021).
Singer, R. S., L. J. Porter, D. U. Thomson, M. Gage, A. Beaudoin, and J. K. Wishnie. 2019. Raising animals without antibiotics: U.S. producer and veterinarian experiences and opinions. Frontiers in Veterinary Science 6(452):452.
Smith, R., and J. Coast. 2013. The true cost of antimicrobial resistance. BMJ 346:f1493.
Sugden, R., R. Kelly, and S. Davies. 2016. Combating antimicrobial resistance globally. Nature Microbiology 1(10):16187.
Sulis, G., B. Batomen, A. Kotwani, M. Pai, and S. Gandra. 2021. Sales of antibiotics and hydroxychloroquine in India during the COVID-19 epidemic: An interrupted time series analysis. PLoS Medicine 18(7):e1003682.
Sung, H., J. Ferlay, R. L. Siegel, M. Laversanne, I. Soerjomataram, A. Jemal, and F. Bray. 2021. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians 71(3):209-249.
Sweeney, M. T., B. V. Lubbers, S. Schwarz, and J. L. Watts. 2018. Applying definitions for multidrug resistance, extensive drug resistance and pandrug resistance to clinically significant livestock and companion animal bacterial pathogens. Journal of Antimicrobial Chemotherapy 73(6):1460-1463.
Tadesse, B. T., E. A. Ashley, S. Ongarello, J. Havumaki, M. Wijegoonewardena, I. J. Gonzalez, and S. Dittrich. 2017. Antimicrobial resistance in Africa: A systematic review. BMC Infectious Diseases 17(1):616.
Tang, K. L., N. P. Caffrey, D. B. Nobrega, S. C. Cork, P. E. Ronksley, H. W. Barkema, A. J. Polachek, H. Ganshorn, N. Sharma, J. D. Kellner, S. L. Checkley, and W. A. Ghali. 2019. Examination of unintended consequences of antibiotic use restrictions in food-producing animals: Sub-analysis of a systematic review. One Health 7:100095.
Taylor, J., M. Hafner, E. Yerushalmi, R. Smith, J. Bellasio, R. Vardavas, T. Bienkowska-Gibbs, and J. Rubin. 2014. Estimating the economic costs of antimicrobial resistance: Model and results. Santa Monica, CA: RAND Corporation. https://www.rand.org/pubs/research_reports/RR911.html (accessed June 23, 2021).
Teillant, A., S. Gandra, D. Barter, D. J. Morgan, and R. Laxminarayan. 2015. Potential burden of antibiotic resistance on surgery and cancer chemotherapy antibiotic prophylaxis in the USA: A literature review and modelling study. Lancet Infectious Diseases 15(12):1429-1437.
Thabit, A. K., D. F. Fatani, M. S. Bamakhrama, O. A. Barnawi, L. O. Basudan, and S. F. Alhejaili. 2019. Antibiotic penetration into bone and joints: An updated review. International Journal of Infectious Diseases 81:128-136.
The Economist. 2016. When the drugs don’t work: How to combat the dangerous rise of antibiotic resistance. The Economist. https://www.economist.com/weeklyedition/2016-05-21 (accessed June 25, 2021).
Thorpe, K. E., P. Joski, and K. J. Johnston. 2018. Antibiotic-resistant infection treatment costs have doubled since 2002, now exceeding $2 billion annually. Health Affairs 37(4):662-669.
Tillotson, G. S., and S. H. Zinner. 2017. Burden of antimicrobial resistance in an era of decreasing susceptibility. Expert Review of Anti-Infective Therapy 15(7):663-676.
UN (United Nations). 2021. The 17 sustainable development goals. https://sdgs.un.org/goals (accessed June 23, 2021).
Van Boeckel, T. P., C. Brower, M. Gilbert, B. T. Grenfell, S. A. Levin, T. P. Robinson, A. Teillant, and R. Laxminarayan. 2015. Global trends in antimicrobial use in food animals. Proceedings of the National Academy of Sciences of the United States of America 112(18):5649-5654.
Walia, K., J. Madhumathi, B. Veeraraghavan, A. Chakrabarti, A. Kapil, P. Ray, H. Singh, S. Sistla, and V. C. Ohri. 2019. Establishing antimicrobial resistance surveillance & research network in India: Journey so far. Indian Journal of Medical Research 149(2):164-179.
Wang, J. 2019. The challenges of antimicrobial resistance surveillance in China. American Journal of Infection Control 47(11):1403-1404.
Wee, B. A., D. M. Muloi, and B. A. D. van Bunnik. 2020. Quantifying the transmission of antimicrobial resistance at the human and livestock interface with genomics. Clinical Microbiology and Infection 26(12):1612-1616.
Wernli, D., P. S. Jorgensen, S. Harbarth, S. P. Carroll, R. Laxminarayan, N. Levrat, J. A. Rottingen, and D. Pittet. 2017. Antimicrobial resistance: The complex challenge of measurement to inform policy and the public. PLoS Medicine 14(8):e1002378.
WHO (World Health Organization). 2017. Stop using antibiotics in healthy animals to prevent the spread of antibiotic resistance. Geneva, Switzerland: World Health Organization.
WHO. 2019a. Antimicrobial resistance (AMR)—a major public threat. https://www.who.int/infection-prevention/tools/IPC_AMR_A4.pdf?ua=1 (accessed June 25, 2021).
WHO. 2019b. New report calls for urgent action to avert antimicrobial resistance crisis. New York: World Health Organization.
The World Bank. 2016. By 2050, drug-resistant infections could cause global economic damage on par with 2008 financial crisis. New York: The World Bank.
The World Bank. 2017. Drug-resistant infections: A threat to our economic future. Washington, DC: The World Bank.
Wozniak, T. M., L. Barnsbee, X. J. Lee, and R. E. Pacella. 2019. Using the best available data to estimate the cost of antimicrobial resistance: A systematic review. Antimicrobial Resistance & Infection Control 8:26.
This page intentionally left blank.












































