
1
Introduction and Study Context
From its beginnings on December 23, 1954—when a surgical team in Boston removed a healthy kidney from one 23-year-old and implanted it in his identical twin whose own kidneys had failed—the modern era of transplantation has engendered both admiration and disapproval. Over the next 13 years, surgeons performed successful transplantation of livers, lungs, and hearts, using organs obtained from recently deceased patients, and soon most kidney transplants were also relying mostly on such “cadaver donors.” In the 1980s, the introduction of more effective immune rejection drugs, beginning with cyclosporine, made “matching” organs to recipients easier. Over the past seven decades, more than 875,000 patients with organ failure have been able to live better and longer lives with transplanted organs,1 about 700,000 of which came from deceased donors while the rest—almost all kidneys—were provided by living donors, a category that rose rapidly in the 1990s (from 2,123 in 1990, to 5,939 in 2000).2 At the request of the sponsor, this study and report focus on organ transplants from deceased donors.
MOVEMENT TOWARD A NATIONAL SYSTEM
In the early years, hospitals that created transplant programs established relationships with other hospitals in their locality from which they could obtain deceased patients’
___________________
1 The term “organ transplantation” encompasses a range of procedures, including transplantation of solid organs from living donors; transplantation of donated organs from persons after neurological or circulatory determination of death; multiorgan transplantation (e.g., kidney and pancreas for diabetics with renal failure); and vascularized composite allotransplantations (such as face, hand, penis, uterus). Kidney, liver, pancreas, heart, and lung transplants are the most common forms of organ transplantation; indeed, by the end of 2021, kidneys alone had accounted for 58.9% of all U.S. transplants and 95.1% of those involving a living donor, versus 49.7% of all transplants from deceased donors. See https://optn.transplant.hrsa.gov/data/view-data-reports/national-data (accessed January 20, 2022).
2 The number of living donors annually, which had increased to 7,397 by 2019, fell by more than 1,600 donors in 2020 on account of the COVID-19 pandemic; half that loss was reversed in 2021, when 6,541 living donors were recorded. The annual number of deceased donors (from each of whom multiple organs can usually be obtained) has been rising fairly steadily for decades and reached 34,813 in 2021, more than double the number in 2000. Id.
organs. The groups handling this function—now known as organ procurement organizations (OPOs)—developed expertise in the psychosocial as well as the medical aspects of facilitating organ donations. While some of these organizations remained based in a transplant program, the scope of others broadened to serve transplant teams at several hospitals in their area. The Uniform Anatomical Gift Act (UAGA), promulgated in 1968 and rapidly adopted by all states, facilitated the task of obtaining organs by allowing people to fill out a simple, wallet-sized card donating their organs upon death and by empowering the next of kin to donate if the deceased had not filled out a donor card. The UAGA also established that the persons doing the procurement and transplantation were the custodians rather than the owners of the donated organs.
Nonetheless, from the beginning, the gap between the number of patients with organ failure and the number of transplants increased each year. This was especially true for kidneys; not only were more patients added to the waiting list than were transplanted but an even larger number received dialysis for chronic kidney disease than were listed for a transplant. At a 1983 congressional hearing on improving organ procurement, H. Barry Jacobs, a Virginia physician who established the “International Kidney Exchange, Ltd.” after losing his medical license, described his plan to serve as a broker between U.S. patients needing a kidney transplant and people from poor countries who would be willing to sell one of theirs. Opposition to—actually, disgust at—his proposal helped to push the bill that emerged from the House committee to rapid, bipartisan passage. The National Organ Transplant Act of 1984 (NOTA) not only forbids the giving or receiving of “valuable consideration” for an organ for transplantation but also established a unified, standardized system to oversee and support the procuring and distribution of deceased donor organs for transplantation, to coordinate other aspects of the transplant process, and to gather and analyze data about outcomes. NOTA began the still-ongoing process of creating a national system out of the patchwork of transplant centers and OPOs, which had grown organically in response to local circumstances, along with other professionals involved in patient care, with responsibility to ensure equitable and efficient use of donated organs as a “national resource.”3
COMPLEXITY, SCARCITY, AND PUBLIC CONCERNS
Organ transplants depend on the generosity of organ donors and their families as well as the successful completion of a highly complex array of specialized tasks performed by numerous individuals and organizations, referred to in this report as the “organ transplantation system” or “transplantation system.” The term “system” is somewhat metaphorical since many of the activities involved in obtaining, allocating, and transplanting organs are carried out independently by health care professionals and organizations rather than under the direction or review of a single controlling authority. As concerns deceased donation (the topic of this report), the specific activities and tasks include
- identifying persons who may be candidates for receiving organs and referring them for transplant evaluation;
___________________
3 NOTA instructed the Department of Health and Human Services to appoint a Task Force on Organ Transplantation to develop the basis for regulating the system established by the Act. In its 1986 report, the Task Force recommended “that each donated organ be considered a national resource to be used for the public good; the public must participate in the decisions of how this resource can be used to best serve the public interest.” Organ Transplantation: Issues and Recommendations: Report of the Task Force on Organ Transplantation, Jan 1986. U.S. Department of Health and Human Services, Public Health Service, Health Resources and Services Administration, Office of Organ Transplantation, at p. xxi, 9 (Jan. 1986).
- medically evaluating these candidates for their suitability to receive an organ;
- treating and, when appropriate, diagnosing death in potential donors;
- procuring organs from potential donors;
- allocating donated organs to individuals who have been medically screened and placed on an organ transplant waiting list;
- matching donated organs with waiting list candidates;
- transporting organs to hospitals where the matched recipients will receive a transplant;
- surgically transplanting the donated organs;
- caring for the organ recipients after transplantation, both immediately after surgery and often for many years or decades afterwards; and
- compiling, analyzing, and reporting data on transplants and patient outcomes.
Importantly, the organ transplantation journey for most patients actually begins well before they are placed on the waiting list for an organ transplant when the person is diagnosed and treated for a condition that has significant likelihood of ending in organ failure, has already gotten to that point, or has significant tissue damage that is unresponsive to reconstructive surgery. Figure 1-1 shows the points encountered along the path of a typical recipient of an organ transplant. Yet many factors—such as patients’ gender, economic resources, or ethnicity—affect how they experience the journey and, indeed, whether they survive it and receive a transplant.
The gap between patients on waiting lists and the number of transplants performed is largest for kidneys. In 2020, 91,099 kidneys were needed by individuals on the waiting list, but only 22,817 (25 percent) were transplanted (HRSA, 2021b). While data sources vary, it is estimated that 17 people die waiting for an organ transplant each day and one person is added to the transplant waiting list every 9 minutes (HRSA, 2021a). Yet deaths on the waiting list provide an imperfect picture of the number of patients who need, but do not receive, a transplant. The Organ Procurement and Transplantation Network (OPTN) reports that 5,758 patients were removed from the waiting list in 2021 because they died and another 5,371 because they became “too sick to transplant.” This means that 11,129 patients—about 30 a day—who had been listed for an organ transplant died without receiving one that year. Additionally, and as expounded upon elsewhere in this report, many patients whose lives could be saved by an organ transplant never even reach the waiting list.
Additionally, many patients whose lives could be saved or improved by an organ transplant never even reach the waiting list. For example, the pool of possible kidney transplant candidates in 2020 was even larger than the 91,099 on the waiting list, since more than 558,000 patients with end-stage kidney disease (ESKD) received dialysis in 2020. As explicated later in this report, notable disparities exist between patients who could benefit and those who are placed on a transplant waiting list based on race, ethnicity, gender, age, socioeconomic status, geographic place of residence and location of the transplant center visited, intellectual ability, and immigration status. For instance, black patients are significantly less likely than white patients to be referred for transplant evaluation and then wait longer for a transplant once listed. Disparities and inequities in transplantation are discussed throughout the report and in detail in Chapter 4.
Whenever a system is created to allocate a scarce resource that cannot be left to market distribution, favoritism and discrimination among the decision makers can produce inequities. In the case of the shortage of organs donated for transplantation, the resulting concerns seem to be exacerbated by deficiencies in public understanding of organ donation, allocation, and transplantation, which is not surprising given the complexity of the transplanta-
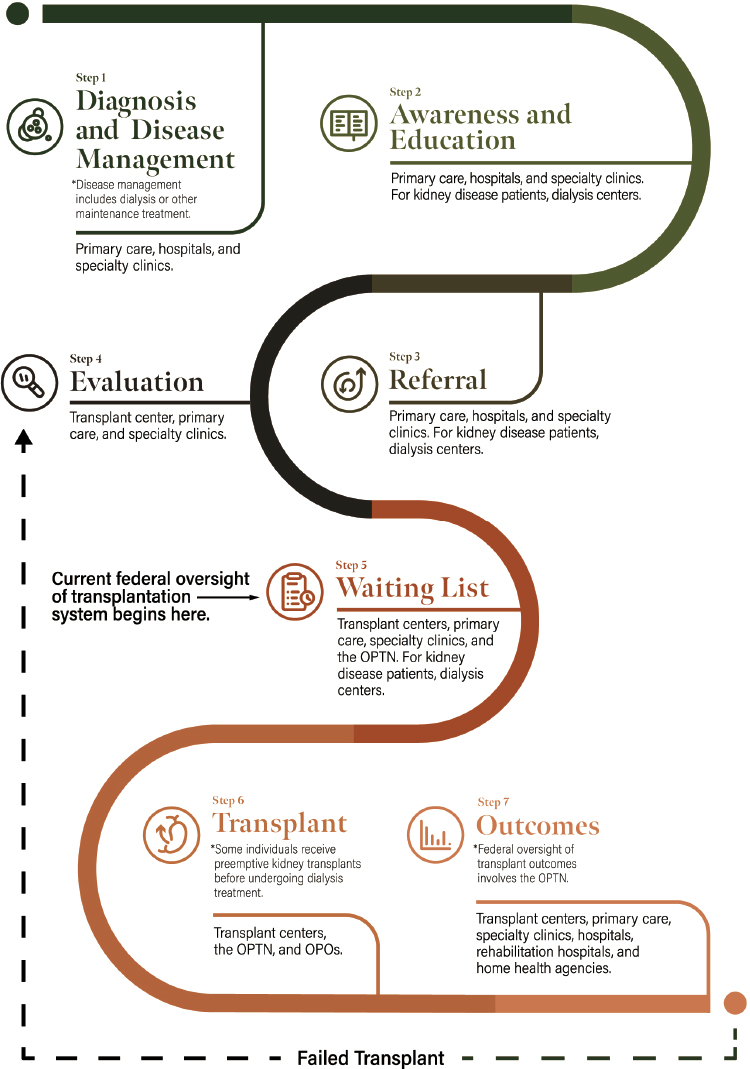
NOTE: OPTN = Organ Procurement and Transplantation Network; OPO = organ procurement organization.
tion system and the sources on which members of the public mostly rely for information. Respondents in the 2019 National Survey of Organ Donation Attitudes and Practices4 reported learning about organ donation primarily through news coverage (51.5 percent), their Department of Motor Vehicles5 (46.5 percent), discussion with family (43.3 percent), discussion with a friend (42.0 percent), movie or TV show (42.0 percent), social media (40.9 percent), and advertisement on TV (40.1 percent). Medical professionals accounted for 29.5 percent and donation organizations accounted for 25.7 percent of the public’s source of information (HHS, 2019). The survey also revealed that only 46.6 percent of respondents had heard, read, or seen information about organ donation or transplantation in the past year (HHS, 2019). The proportion of the public exposed to such information has dropped over time, by nearly 10 percent from 2012 (56.0 percent), and by nearly 18 percent from 2005 (63.3 percent). Since public support for organ donation is essential for the transplantation system to work, the survey’s conclusion that roughly half the respondents believe that wealth and race affect access to a transplant (as reported in Box 1-1) indicate that steps need to be taken to increase the system’s transparency and trustworthiness, a topic to which this report turns in Chapter 3.
___________________
4 For more information about the 2019 National Survey of Organ Donation Attitudes and Practices, see https://www.organdonor.gov/professionals/grants-research/research-reports (accessed August 24, 2021).
5 The organ donation statute in most states provides that people should be offered the opportunity, when obtaining or renewing their driver’s license, to express their willingness to be a deceased organ donor, to be indicated by a statement or sticker on their license.
STUDY CHARGE
This study was mandated by the U.S. Congress in the Consolidated Appropriations Act of 2020.6 Specifically, the National Academies of Sciences, Engineering, and Medicine (the National Academies) was asked to examine and recommend improvements to research, policies, and activities related to deceased donor organ procurement, allocation, and distribution. The congressional language requested that the report include
(1) identification of the current challenges involved in modeling proposed organ allocation policy changes and recommendations to improve modeling; (2) recommendations about how costs should be factored into the modeling of organ allocation policy changes; (3) a review of the scoring systems (e.g., CPRA, EPTS, KDPI, LAS, MELD)7 or other factors that determine organ allocation and patient prioritization and recommendations to assure fair and equitable practices are established, including reducing inequities affecting socioeconomically disadvantaged patient populations; (4) recommendations to update the Organ Procurement and Transplantation Network’s (OPTN’s) policies and processes to ensure that organ allocation decisions take into account the viewpoints of expert OPTN committees; and (5) such other issues as may be identified.8
At the direction of Congress, the National Institutes of Health (NIH) via the National Institute of Allergy and Infectious Diseases sponsored and funded this study. The Statement of Task from NIH, found in Box 1-2, directs the committee to examine the economic (costs), ethical, policy, regulatory, and operational issues related to organ allocation policy decisions involving a range of deceased donor organs. This study follows a history of work conducted by the Institute of Medicine (IOM) and the National Academies, which began some 3 decades
___________________
6 The complete congressional language requesting this consensus study can be found in Division A of the Joint Explanatory Statement that accompanied H.R. 1865, the Further Consolidated Appropriations Act, 2020 (P.L. 116-94) on PDF page 82 here: https://www.appropriations.senate.gov/imo/media/doc/HR%201865%20-%20SOM%20FY20.pdf (accessed February 22, 2022).
7 CPRA = calculated panel reactive antibody; EPTS = estimated posttransplant survival; KDPI = Kidney Donor Profile Index; LAS = lung allocation score; MELD = Model for End-Stage Liver Disease.
8 H.R. 1865, the Further Consolidated Appropriations Act, 2020 (P.L. 116-94). https://www.appropriations.senate.gov/imo/media/doc/HR%201865%20-%20SOM%20FY20.pdf (accessed February 22, 2022).
ago and remains relevant today. Brief summaries of previous IOM and National Academies studies on organ transplantation are in Appendix B.
THE NATIONAL ACADEMIES STUDY PROCESS
A Statement of Task guides each National Academies study and determines what kinds of expertise are needed on a committee. A committee writes a report to answer as thoroughly as possible the questions posed in the Statement of Task.
Committee Formation
Members of the committee that conducted this study9 were selected from among more than 200 persons nominated during the committee-formation phase of the study. Individuals appointed to the committee were chosen for their individual expertise and the relevance of their experience and knowledge to the Statement of Task, not their affiliation with any institution. All committee members volunteer their time to serve on a study committee. Areas of expertise represented on the committee included health care system management, bioethics, population health, anthropology, transplant surgery, organ procurement, organ allocation, management science, economics, biostatistics, and law and regulation. Biographies of committee members are in Appendix C.
Public Input and Committee Deliberations
Members of the public were invited to provide oral or written statements and information to the committee. Virtual public meetings were held in December 2020 and February, April, and July 2021 and included time for members of the public to provide comments to the committee. Public meeting agendas are in Appendix A. Recordings of the public sessions are archived on the study website.10
Written comments to the committee could be submitted at any point during the study process. Comments and information could be delivered to National Academies staff via the study email address and through the feedback form linked on the study website. More than 100 comments and documents were submitted to the committee, and the committee listened to or read all of them. Public submissions of comments, articles, or written testimony for the committee’s consideration are available upon request from the National Academies’ Public Access Records Office (paro@nas.edu). To address the Statement of Task, the committee considered information presented during public meetings. Committee members frequently requested
___________________
9 Every National Academies committee is provisional until the appointed members have had an opportunity to discuss as a group their points of view and any potential conflicts of interest related to the Statement of Task. During this discussion they also determine whether the committee is missing expertise that may be necessary to answer questions in the Statement of Task. As part of their discussion, committee members consider any comments submitted by the public about the committee’s composition. The discussion takes place during the first meeting of the committee. The committee is provisional until the National Academies determines that the committee has the necessary balance and composition to address the Statement of Task, and that committee members are free of unavoidable financial conflicts of interest, transparent about their relevant relationships and publications, and independent from the sponsors of the committee’s work. For more information about the National Academies study process, including definitions and procedures related to composition, balance, and conflict of interest, visit https://www.nationalacademies.org/about/our-study-process (accessed January 24, 2022).
10 The study website includes recordings of public sessions. Visit https://www.nationalacademies.org/our-work/a-fairer-and-more-equitable-cost-effective-and-transparent-system-of-donor-organ-procurement-allocation-anddistribution#sectionPastEvents (accessed January 24, 2022).
additional data or documentation from invited speakers or public commenters following their presentations. The committee also reviewed statements and articles that were submitted or referred to by speakers and thoroughly consulted the peer-reviewed scientific literature. The committee took seriously the information and passion conveyed by stakeholders throughout this study process, and some of the public comments are quoted in this report. To address the study charge, the committee deliberated virtually from December 2020 to February 2022, holding 17 closed session committee meetings in addition to the public sessions mentioned above. The committee reviewed the scientific literature on the issues identified in the Statement of Task and also commissioned seven white papers. The commissioned papers explore such topics as the use of standardized performance metrics and quality improvement in organ transplantation, algorithms used in kidney and liver allocation, challenges and opportunities in OPTN policy making, solutions to financial and policy barriers to increasing deceased donor transplantation, and the use of survival benefit in deceased donor kidney transplantation. The commissioned papers are in the study’s public access file and are available upon request from the National Academies’ Public Access Records Office (paro@nas.edu).
Report Review Process
The concluding phase of a National Academies study is the report review process. When a draft report is complete, it is submitted to the National Academies’ Report Review Committee (RRC). The RRC recruits a diverse and critical group of reviewers who have expertise complementary to that of the committee to ensure that critical gaps and misinformation are identified (see the Reviewers section on p. vii). The reviewers are anonymous to the committee during the review process, and their comments remain anonymous after the report is published. Reviewers are asked to assess how well a report addresses a study’s Statement of Task to ensure that the report addressed the full Statement of Task but did not go beyond it, and are asked to assess whether the report includes evidence, analysis, and arguments to support the conclusions and recommendations.11 The committee must consider and respond to, but not necessarily agree with, all reviewers’ comments in a detailed “response to review” that is examined by independent report review monitors responsible for ensuring that the report review criteria have been satisfied before the report is finalized. When the RRC decides that the committee has adequately and appropriately addressed the reviewer’s comments, the report is ready to be released to the public and to the sponsor.
COMMITTEE APPROACH AND INTERPRETATION OF THE STATEMENT OF TASK
This study charge is broad and asks the study committee to address multiple longtime, vexing issues and challenges in organ procurement, allocation, and distribution. While the study charge was limited to procurement, allocation, and distribution of deceased donor organs, some of the committee’s recommendations may also affect living donors and living donation policies. The committee was not asked to explore issues in tissue procurement and use.
The study charge emphasizes the importance of issues of fairness, equity, cost-effectiveness, and transparency of the organ transplantation system, concerns that were central to the committee’s deliberations (see Box 1-3 for some key definitions and concepts). During the
___________________
11 More information on the National Academies study process and report review process can be found on these pages: https://www.nationalacademies.org/about/our-study-process; https://www.nationalacademies.org/about/institutional-policies-and-procedures/guidelines-for-the-review-of-reports (accessed February 4, 2022).
committee’s work, there were a number of activities and changes in the organ donation and transplantation system. For instance, the Centers for Medicare & Medicaid Services issued a new performance metric for OPOs. There was heightened congressional scrutiny of OPOs as well as the United Network for Organ Sharing (UNOS), the nonprofit government contractor implementing the transplantation system known as the Organ Procurement and Transplantation Network. Throughout the course of this study, UNOS, as the OPTN, continued to refine allocation policies governing how deceased donor organs are prioritized among patients on the waiting list as well as other policies related to performance metrics for transplant centers.
The committee was mindful that OPOs and UNOS were under scrutiny by Congress12 and others,13 and that some of these issues have become contentious among organ transplantation stakeholders who are tasked with working together.14 Congressional scrutiny largely involves issues that this committee was not charged with addressing, nor constituted to address. The committee closely examined challenges and opportunities in deceased donor organ procurement and the variations in performance across OPOs, but some of the OPO issues that have attracted the most congressional and media attention are quite different from those this committee was tasked with addressing. For example, in addition to scrutiny of OPOs, there have been calls to formally reorganize the federal oversight responsibilities of the OPTN by moving or refocusing the current Division of Transplantation within the Health Resources and Services Administration to a new office of the Assistant Secretary of the U.S. Department of Health and Human Services.15 The committee did not interpret its charge to include a request for recommendations on restructuring or reorganizing federal offices with oversight responsibilities for the organ transplantation system, and during the course of its work the committee did not find evidence demonstrating superiority of any particular organizational oversight structure.
The organ transplantation system has realized many amazing, lifesaving achievements in recent decades. Posttransplant outcomes remain positive and most patients see significant improvements in quality of life following transplant. In 2021, there were 41,354 transplants performed—an increase of 5.9 percent over 2020 (OPTN, 2022). Transplantation is also a multidisciplinary field, drawing on the expertise of many passionate individuals in multiple medical specialties, social work, nutrition, case management, pharmacy, surgery, primary care, nursing, home health, rehabilitation, and organ procurement. The context of this report, as requested by the study sponsor, is to discuss specific opportunities to improve the organ transplantation system. The report is written from the perspective that while much has been achieved, significant opportunities remain to improve the availability of and access to deceased donor organs for individuals needing a transplant. In some cases, the committee’s recommendations may include areas where the OPTN or others are currently working to address. It is the committee’s hope that even if some of these issues are already being consid-
___________________
12Oversight subcommittee expands investigation into fraud, waste, and abuse in organ transplant industry. May 27, 2021: https://oversight.house.gov/news/press-releases/oversight-subcommittee-expands-investigation-into-fraudwaste-and-abuse-in-organ; Grassley, Wyden Subpoena the United Network for Organ Sharing as part of continued investigation into U.S. organ transplant system. February 4, 2021: https://www.finance.senate.gov/ranking-membersnews/grassley-wyden-subpoena-the-united-network-for-organ-sharing-as-part-of-continued-investigation-into-usorgan-transplant-system (accessed January 26, 2022).
13 Bloom Works: The Costly Effects of an Outdated Organ Donation System: Summary of Findings. https://bloomworks.digital/organdonationreform/Introduction (accessed January 26, 2022).
14As thousands wait for transplants, medical centers fight to keep livers close to home. May 14, 2019. https://www.npr.org/sections/health-shots/2019/05/14/723371270/new-liver-donation-system-takes-effect-despite-ongoinglawsuit (accessed January 26, 2022).
15 For more information see https://www.healthaffairs.org/do/10.1377/forefront.20201211.229975/full (accessed February 11, 2022).
ered, that these recommendations will draw heightened attention and urgency to undertaking efforts to improve equity and fairness in the organ transplantation system.
This National Academies committee approached the Statement of Task from a systems perspective in reviewing opportunities to improve deceased donor organ procurement, allocation, and organ distribution for the benefit of patients. As this report will describe, an individual engages with the organ transplantation system and the relevant oversight systems such as the OPTN when initiating evaluation for an organ transplant. However, the upstream components—identifying patients who could benefit from transplantation, referring such patients to a transplant center for evaluating patients for their transplant suitability, and adding their names to the organ transplant waiting list—are of critical importance to ensuring that the organ transplantation system is fair and equitable.
The committee was acutely aware that the transplantation system exists within a broader health care system that falls short on delivering equitable access to care (IOM, 2013). Individuals at a disadvantage in receiving health care services in general are likely to be disadvantaged in seeking an organ transplant. The organ transplantation system may be unable to solve issues of inequity in the larger health care system, but these larger issues cannot be an excuse for those in the organ transplantation system to turn their focus away from the need to provide equitable access to the opportunity for transplantation, as well as equitable allocation of deceased donor organs among those on the waiting list. In fact, an opportunity exists for the organ transplantation system to become an example of how to manifest equity in the delivery of care and allocation of a scarce resource. The committee discusses the concepts of fairness, equity, and justice in greater detail in Chapter 3 and throughout the report. While the committee acknowledges the achievements of the organ transplantation system and the complexity of changing policies in this area to avoid unintended consequences, the committee believes the system can be fairer and more equitable.
An additional complexity and context for this study is the role of the opioid epidemic in transplantation and how much increases in organ donation over the last decade are directly attributed to the increase in opioid deaths or other factors (e.g., changes in allocation policy
or efforts of OPOs). The drug overdose epidemic has increased deaths resulting in organ donations as these deceased individuals typically are younger and have limited medical comorbidities that would preclude them from being donors. The number of donors who died from drug overdose increased from 29 to 848, an increase of 2,924 percent, between 1994 and 2016 (Weiner et al., 2017). In 2013, there were an estimated 514 kidney donations from persons who died from drug intoxication and in 2018 this number more than doubled to 1,313 donations (Maghen et al., 2019). Disagreement exists in the transplantation system as to the degree to which the increase in deceased organ donation can be attributed to the opioid epidemic. Some authors suggest the data are indisputable that the increase in donors is due almost wholly to the opioid epidemic (Goldberg and Lynch, 2019), while others are equally passionate that this assertion is unsupported by the data given challenges in accurately categorizing “drug-related” deaths (Cmunt et al., 2020; Stewart et al., 2020). This committee was not tasked with parsing the impact of opioid overdose deaths, car accidents, or homicides on the transplantation system, though the committee recognizes that such public health trends do impact the organ donation system and affect the absolute number of potential organ donors. The committee believes that the most important takeaway is the need for the organ transplantation system to be prepared and at its most high functioning state to handle changes in the number of deaths in the United States as a result of tragedies such as the opioid epidemic or positive changes in laws related to helmet use or vehicle safety.
WHY IS THIS STUDY NEEDED?
The foundation of the organ transplantation system is the gift of organ donation from both living and deceased donors. Every day, individuals and families throughout the United States face the critical decision to donate organs—often in moments that coincide with the loss of a loved one—for the sole purpose of saving the life of another person who is usually unknown to the donor. This study is undertaken with the goal of helping to better facilitate the transition of this valuable lifesaving resource from one person to another and to highlight the importance and challenges of doing so.
A continuous challenge for the organ transplantation system is that the number of organs transplanted each year falls below the number of patients on the waiting list, which therefore grows longer each year. For example, the more than 106,000 persons on organ transplant waiting lists in 2021 were more than double the number of transplants performed that year.
OVERVIEW OF CHALLENGES
To address its broad charge and identify opportunities for improving deceased donor organ procurement, allocation, and organ distribution—and ultimately, downstream effects on mortality—the committee focused on three key issues that exist within the transplantation system: (1) problems of inequity in access, (2) variation and inefficiency in system performance, and (3) underuse of donated organs. In the face of these challenges, it is important to understand that organ transplantation and donation spans a complex system comprising clinics and hospitals, highly specialized transplant centers, OPOs, nonprofit government contractors, and federal oversight agencies, all of which are supported by an equally complex web of dedicated and passionate professionals. Given the complexity of the transplantation system, many of these challenges are interconnected and have the potential to benefit or harm other components within the system. However, the committee believes that for the transplantation system to be truly successful, all of these challenges must be examined within the context of known inequities and disparities.
Challenges of Inequity in Access
The deceased donor organ procurement and transplantation system has long-standing problems of inequity in access to the organ transplant waiting list and eventual transplantation. Getting onto the waiting list (i.e., being listed) is the metaphorical gateway to gaining access to a lifesaving organ transplant. This gate may be especially hard to open for many persons who would benefit from organ transplantation, particularly persons who are racial or ethnic minorities, of lower socioeconomic status, live in rural areas, or have an intellectual disability.
One of the stated aims of the OPTN is to promote equitable access to transplantation and organ allocation; however, after examining the literature, the committee found stark health disparities in organ transplantation rates for certain subsets of the American population but also limited data on disparities for racial and ethnic groups other than those for black and white persons. Disparities are evident at different points along the complicated pathway to an organ transplant and are caused by different structural and other barriers (see Table 4-1 in Chapter 4 for a summary of key data related to health disparities in organ donation and transplantation). Illustrative of some disparities, black persons are three times more likely to develop kidney failure than whites in the United States, but they are significantly less likely to receive lifesaving kidney transplants (Saran et al., 2017). Relatively fewer black patients are referred, evaluated, and added to a transplant waiting list, and fewer living kidney donations are available to black patients compared to white patients (Gander et al., 2018; Waterman et al., 2013). The evidence of disparate access to organ transplants is not limited to black persons who need kidney transplants. As another example, women are less likely to receive a liver transplant than men, regardless of other factors including race, geography, education, body mass index, and weight (Allen et al., 2018; Darden et al., 2021).
The committee found that a rigorous and comprehensive assessment of inequities in the current transplantation system is challenging because of a lack of patient-centered data, especially for individuals not yet listed but in need of a transplant, persons with intellectual disabilities, pediatric patients, and undocumented immigrants. Reliable data on the number of patients who enter the transplant pathway (e.g., patients who might benefit from referral and transplant evaluation) are particularly lacking, and there are few—if any—ways to properly assess the effect of socioeconomic status on transplant access.
Confronting and rectifying the issues related to health inequities in organ transplantation in the United States will require a systemwide approach to prioritize equity, rethink incentive structures for the transplantation system, and collect disaggregated data to inform research on inequities and disparities. The committee’s assessment of and proposed approach to this set of issues is discussed in Chapter 4.
Variation and Inefficiency in System Performance
The performance of the component parts of the organ transplantation system is neither predictable nor consistent across the United States, especially for OPOs and transplant centers. Identifying key areas of variation in the procurement and use of deceased donor organs provides opportunities for developing and implementing quality improvement tools and standardized performance measures to reduce variation in the system. The committee focused on three critical areas of variation in system performance that affect the availability of deceased donor organs for those on transplant waiting lists: (1) the procurement of medically complex organs, in particular donation after circulatory determination of death (DCDD), (2) the acceptance rates of offered organs, and (3) nonuse of procured organs.
The percentage of total deceased donors that originate from DCDD varies widely, ranging from approximately 11 percent to nearly 53 percent of deceased donor organs (see Figure 6-3 and associated discussion in Chapter 6). Similar variability occurs in organ offer acceptance rates across transplant centers. Among 65 transplant centers, acceptance of lung transplants varied from 9 percent to 67 percent (Mulvihill et al., 2020). This marked variability significantly affects which patients may receive a transplant on the basis of which transplant center they use. Rates of nonuse of donated organs also vary widely and are important to address because—like acceptance rates—they can advantage or disadvantage patients on the waiting list. Nonuse rates vary because of factors such as the practices of specific transplant centers and transplant teams, geographic variation in organ availability, patients’ access to transplant centers, and the lack of standard donor acceptance criteria.
Underuse of Donated Organs
While waiting lists remain long and many listed individuals die while awaiting an organ every day, too many donated organs that are procured and offered to patients at transplant centers are not accepted—leaving thousands of potentially lifesaving donated organs unused every year. While estimates vary, approximately 20 percent of organs procured from deceased donors are not used (i.e., the organs are not transplanted into individuals on the waiting list). The committee agreed that this issue of unused organs represents a critical need for system improvement. Evidence indicates that many, if not a large majority, of unused organs could be successfully transplanted and benefit patients. This problem is much more prominent in the United States than in many other countries. For example, the overall nonuse rate in the United States is twice that in France. In the United States, on average, patients who die waiting for a kidney had offers for 16 kidneys that were ultimately transplanted into other patients, indicating that many transplant centers refuse viable kidney offers on behalf of those on the waiting list (Husain et al., 2019).
REFERENCES
Allen, A. M., J. K. Heimbach, J. J. Larson, K. C. Mara, W. R. Kim, P. S. Kamath, and T. M. Therneau. 2018. Reduced access to liver transplantation in women: Role of height, MELD exception scores, and renal function underestimation. Transplantation 102(10):1710-1716.
Arcaya, M. C., A. L. Arcaya, and S. V. Submarinian. 2015. Inequalities in health: Definitions, concepts, and theories. Global Health Action 8:10. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4481045 (accessed December 21, 2021).
Cmunt, K., G. Danovitch, F. Delmonico, F. Fynn-Thompson, A. Glazier, J. Grandas, S. Gunderson, M. Jendrisak, H. K. Johnson, S. Kulkarni, G. Lipowitz, K. Meyer, D. Mulligan, H. Nathan, T. Mone, M. Moritz, K. O’Connor, W. Payne, M. Souter, and R. P. Wood. 2020. Deceased donors: Defining drug-related deaths. Clinical Transplantation 34(3):e13800.
Darden, M., G. Parker, E. Anderson, and J. F. Buell. 2021. Persistent sex disparity in liver transplantation rates. Surgery 169(3):694-699.
Gander, J. C., X. Zhang, L. Plantinga, S. Paul, M. Basu, S. O. Pastan, E. Gibney, E. Hartmann, L. Mulloy, C. Zayas, and R. E. Patzer. 2018. Racial disparities in preemptive referral for kidney transplantation in Georgia. Clinical Transplantation 32(9):e13380.
Goldberg, D., and R. Lynch. 2019. Improvements in organ donation: Riding the coattails of a national tragedy. Clinical Transplantation 34(1). https://doi.org/10.1111/ctr.13755 (accessed January 24, 2022).
HHS (U.S. Department of Health and Human Services). Health Resources and Services Administration, Healthcare Systems Bureau. 2019. 2019 National Survey of Organ Donation Attitudes and Practices: Report of findings. Rockville, MD: U.S. Department of Health and Human Services. https://www.organdonor.gov/sites/default/files/organ-donor/professional/grants-research/nsodap-organ-donation-survey-2019.pdf (accessed August 24, 2021).
HHS. 2021. Healthy People 2030 questions and answers. https://health.gov/our-work/healthy-people/healthypeople-2030/questions-answers (accessed December 17, 2021).
HHS. n.d. Healthy People 2020. https://www.healthypeople.gov/2020/about/foundation-health-measures/Disparities (accessed December 17, 2021).
HRSA (Health Resources and Services Administration). 2021a. Organ donation statistics. https://www.organdonor.gov/learn/organ-donation-statistics (accessed December 17, 2021).
HRSA. 2021b. Patients on the waiting list vs. transplants performed by organ (2020). https://www.organdonor.gov/learn/organ-donation-statistics/detailed-description#fig1 (accessed December 17, 2021).
Husain, S. A., K. L. King, S. Pastan, R. E. Patzer, D. J. Cohen, J. Radhakrishnan, and S. Mohan. 2019. Association between declined offers of deceased donor kidney allograft and outcomes in kidney transplant candidates. JAMA Network Open 2(8):e1910312.
IOM (Institute of Medicine). 2013. Best care at lower cost: The path to continuously learning health care in America. Washington, DC: The National Academies Press. https://doi.org/10.17226/13444.
Maghen, A., T. D. Mone, and J. Veale. 2019. The kidney transplant waiting list and the opioid crisis. New England Journal of Medicine 380(23):2273-2274.
Mulvihill, M. S., H. J. Lee, J. Weber, A. Y. Choi, M. L. Cox, B. A. Yerokun, M. A. Bishawi, J. Klapper, M. Kuchibhatla, and M. G. Hartwig. 2020. Variability in donor organ offer acceptance and lung transplantation survival. The Journal of Heart and Lung Transplantation 39(4):353-362.
OPTN (Organ Procurement and Transplantation Network). 2022. All-time records again set in 2021 for organ transplants, organ donation from deceased donors. https://optn.transplant.hrsa.gov/news/all-time-records-again-set-in-2021-for-organ-transplants-organ-donation-from-deceased-donors (accessed January 20, 2022).
Saran, R., B. Robinson, K. C. Abbott, L. Y. Agodoa, P. Albertus, J. Ayanian, R. Balkrishnan, J. Bragg-Gresham, J. Cao, J. L. Chen, E. Cope, S. Dharmarajan, X. Dietrich, A. Eckard, P. W. Eggers, C. Gaber, D. Gillen, D. Gipson, H. Gu, S. M. Hailpern, Y. N. Hall, Y. Han, K. He, H. Hebert, M. Helmuth, W. Herman, M. Heung, D. Hutton, S. J. Jacobsen, N. Ji, Y. Jin, K. Kalantar-Zadeh, A. Kapke, R. Katz, C. P. Kovesdy, V. Kurtz, D. Lavalee, Y. Li, Y. Lu, K. McCullough, M. Z. Molnar, M. Montez-Rath, H. Morgenstern, Q. Mu, P. Mukhopadhyay, B. Nallamothu, D. V. Nguyen, K. C. Norris, A. M. O’Hare, Y. Obi, J. Pearson, R. Pisoni, B. Plattner, F. K. Port, P. Potukuchi, P. Rao, K. Ratkowiak, V. Ravel, D. Ray, C. M. Rhee, D. E. Schaubel, D. T. Selewski, S. Shaw, J. Shi, M. Shieu, J. J. Sim, P. Song, M. Soohoo, D. Steffick, E. Streja, M. K. Tamura, F. Tentori, A. Tilea, L. Tong, M. Turf, D. Wang, M. Wang, K. Woodside, A. Wyncott, X. Xin, W. Zang, L. Zepel, S. Zhang, H. Zho, R. A. Hirth, and V. Shahinian. 2017. US Renal Data System 2016 annual data report: Epidemiology of kidney disease in the United States. American Journal of Kidney Diseases 69(3 Suppl 1):A7-A8.
Stewart, D., A. Zehner, D. Klassen, and J. Rosendale. 2020. The drug overdose epidemic does not explain all of the rise in deceased donation. Clinical Transplantation 34(5):e13858.
Waterman, A. D., J. D. Peipert, S. S. Hyland, M. S. McCabe, E. A. Schenk, and J. Liu. 2013. Modifiable patient characteristics and racial disparities in evaluation completion and living donor transplant. Clinical Journal of the American Society of Nephrology 8(6):995-1002.
Weiner, S. G., S. M. Malek, and C. N. Price. 2017. The opioid crisis and its consequences. Transplantation 101(4):678-681.
















