
2
The U.S. Organ Transplantation System and Opportunities for Improvement
This chapter examines the evolution of organ transplantation policies and systems, highlighting the complexity in the overall system, the benefits of setting ambitious goals for improvement, and challenges and opportunities for improving the efficiency and effectiveness of the Organ Procurement and Transplantation Network (OPTN) policy-making process going forward.
Since solid organ transplantation began in the United States in the 1950s, the systems and policies supporting organ donation, procurement, allocation, and distribution have evolved into a highly complex network of medical organizations and professionals, federal agencies, nonprofit contractors, patients, families, and advocates. This chapter traces the evolution and current status of the nation’s solid organ procurement, allocation, distribution, and transplantation system. The chapter discusses the cost-effectiveness of transplantation; the committee’s recommendations for national performance goals for the system (Recommendation 1); and opportunities to improve the OPTN policy-making process (Recommendation 2).
EVOLUTION OF NATIONAL ORGAN TRANSPLANTATION SYSTEMS, POLICIES, AND OVERSIGHT
After the first successful living donor kidney transplant between identical twin brothers in 1954, kidney transplantation was recognized as a viable medical alternative to dialysis (Tilney, 2003). With dialysis serving as a lifeboat for those awaiting transplantation and the advent of immune suppression agents to prevent organ rejection, kidney transplant operations became more commonplace by the 1960s, but donor organ procurement was primarily hospital based. Since the characteristics of donated organs could not always be matched with patients at a particular hospital, transplant programs typically relied on their informal network to facilitate the sharing of such organs with other programs. This led transplant professionals to establish more formal transplant networks in Los Angeles, Boston, and Richmond (DeVita et al., 1993).
Legislative Milestones
In the late 1960s, improvements in mechanical ventilation and other medical measures that sustained cardiopulmonary function enabled some patients who had experienced respiratory arrest or severe brain injuries to recover. Other patients, whose injuries were more extensive or who experienced a longer period of anoxia before restoration of circulation, could remain unconscious on a ventilator indefinitely. Postmortem examinations of patients in the latter group revealed brain damage inconsistent with their ever regaining consciousness or spontaneous circulatory-respiratory functions. Physicians developed methods of diagnosing when this loss of brain function was permanent and proposed that such patients could be declared dead even while a ventilator and associated medical interventions provided circulation of oxygenated blood (Report of the Ad Hoc Committee, 1968). In the period that followed, experts further elaborated the criteria and methods for determining death based on irreversible loss of brain functions, and the traditional methods of diagnosing death based on loss of circulation were clarified (DeVita et al., 1993; Guidelines for the determination of death, 1981; Halevy and Brody, 1993). Beginning in 1981, most states adopted the Uniform Determination of Death Act, which set forth two standards under which physicians were permitted to apply accepted medical criteria to determine that death had occurred, based either on the loss of circulatory and respiratory functions or on loss of all brain functions, including the brainstem (President’s Commission, 1981). For both sets of criteria, the diagnosis of death requires both the cessation of function and irreversibility (Guidelines for the determination of death, 1981). The use of neurological criteria for the determination of death has gained wide medical, legal, ethical, and public acceptance in the United States, although debates continue (Bernat, 2005; Greer et al., 2020; Laureys, 2005). During the 1970s and 1980s, organ donation in the United States involved almost exclusively brain-based determinations of death. Beginning in the early 1990s, however, protocols were developed for donation after circulatory determination of death (DCDD), and, despite some controversy, this approach has become an increasingly important source of organs from deceased donors (Domínguez-Gil et al., 2021). In some areas of the country, the practice of DCDD never went away; however, the increases in DCDD started with the advent of a 2003 national Organ Donation Breakthrough Collaborative (see Chapters 6 and 7 for greater discussion of procurement of DCDD organs and national quality improvement efforts).
National Organ Transplant Act (NOTA)
In 1983, the growing demand for organ transplantation, controversies regarding the allocation of organs, and concerns about payment for organs prompted members of Congress to propose the creation of a formal, privately administered network to more effectively procure and equitably allocate deceased donor organs. This proposal became the National Organ Transplant Act (NOTA), which was adopted on October 19, 1984. NOTA authorized the creation of the OPTN to regularize and make more efficient and equitable the system for obtaining and distributing organs, based on an improved matching process (see Box 2-1).1 NOTA specified that the OPTN would be operated by a private, nonprofit organization under federal contract. The Act also banned the purchase or sale of human organs for transplantation but allowed transplant professionals, hospitals, transporters, and organ pro-
___________________
1 Organ procurement and transplantation network, 42 U.S.C. §274, https://uscode.house.gov/view.xhtml?req=granuleid%3AUSC-2020-title42-chapter6A-subchapter2-partH&saved=%7CZ3JhbnVsZWlkOlVTQy0yMDIwLXRpdGxlNDItc2VjdGlvbjI3NGU%3D%7C%7C%7C0%7Cfalse%7C2020&edition=2020 (accessed February 4, 2022).
curement organizations (OPOs) to receive compensation for the services they provide (HHS, 2022). NOTA also permits living donors to receive reimbursement for the costs they bear in donating (such as travel, lost income, etc.), and it encourages the honoring of an individual’s documented wishes with respect to organ donation.
The Act also created the U.S. Task Force on Organ Transplantation to examine and report back to Congress on a broad range of issues including the technical, practical, and ethical limitations on sharing organs. In its April 1986 report, the Task Force concluded that “donated cadaveric organs are a national resource,” whose distribution ought not to be based on “accidents of geography.” This means that, to the extent technically feasible, every person in the nation in need of a transplant—not simply those who live in the area where an organ is donated—should be equally considered a potential recipient.2 After the Task Force’s report was submitted, the Secretary issued the OPTN contract to a nonprofit organization, the United Network for Organ Sharing (UNOS), based in Richmond, Virginia.
NOTA has been amended many times since 1984. In 1988 and again in 1990, the original scope of the OPTN’s responsibilities—namely, to assist OPOs in distributing organs that “cannot be placed within [their] service areas”—was broadened, in line with the Task Force’s conclusion, to assist OPOs “in the nationwide distribution of organs equitably among transplant patients.”3
The Omnibus Reconciliation Act of 1986 required all hospitals performing organ transplants to be members of the OPTN and to abide by its rules to receive Medicare and Medicaid payments.4 The Omnibus Health Amendments of 1988 required the OPTN to “establish membership criteria and medical criteria for allocating organs and provide to members of the public an opportunity to comment with respect to such criteria.”5
On September 8, 1994, the Health Resources and Services Administration (HRSA), a unit within the Department of Health and Human Services (HHS), issued a Notice of Proposed Rulemaking for a regulation governing the operation of the OPTN. Although the public comment period was supposed to end in December 1994, the department continued to accept comments on the OPTN’s operations and its policies for allocating organs.6 Two years later, in November 1996, the department officially extended the period for public comment on the proposed rule, due to controversy over revisions in the liver allocation policies being proposed by the OPTN’s board.7 Even after HRSA published the OPTN Final Rule on April 2, 1998,8 Congress twice delayed its going into effect.9 HRSA finally implemented the Final Rule on March 6, 2000.10 The OPTN board is composed of transplant physicians, recipients, candidates, family members, deceased donor families, recipient families, living donors, transplant hospitals, OPO representatives, and members of the public who are organized into various committees that are delegated with policy-making authority. In establishing the OPTN’s regulatory framework, the rule instructs its board of directors to draft policies “based
___________________
2 Organ Transplantation: Issues and Recommendations: Report of the Task Force on Organ Transplantation. Rockville, MD: U.S. Dept. of Health & Human Services, Public Health Service, Health Resources and Services Administration, Office of Organ Transplantation (1986), at 91.
3 Transplant Amendments of 1990, P. L. 101-616, Title II, § 202, now codified at 42 U.S.C. 274(b)(2)(D).
4 P. L. 99-509 (1986).
5 P. L. 100-607 (1988).
6 59 Federal Register 46482 (1994), https://www.govinfo.gov/content/pkg/FR-1994-09-08/html/94-21993-2.htm (accessed February 3, 2022).
7 61 Federal Register 58158 (1996), https://www.govinfo.gov/content/pkg/FR-1996-11-13/pdf/96-29145.pdf (accessed February 3, 2022).
8 63 Federal Register 16296 (1998), https://www.federalregister.gov/documents/1998/04/02/98-8191/organ-procurement-and-transplantation-network (accessed February 3, 2022).
9 Ticket to Work and Work Incentives Act, P. L. 106-170, §413 (1998); 1999 Consolidated Appropriations Act, P. L. 106-113 (1999).
10https://optn.transplant.hrsa.gov/about/final-rule (accessed February 3, 2022).
on sound medical judgment…to achieve the best use of donated organs”11 and gives the board discretion to develop and implement these policies. But, in accordance with congressional enactments, the Final Rule also states that the Secretary of HHS must approve “significant” policies promulgated by the OPTN, such as the allocation rules for each type of organ, before they become federally enforceable.12 OPOs, hospitals, and other entities that are members of the OPTN are expected to adhere voluntarily to the policies and bylaws adopted by the board to govern the OPTN’s internal operations. These internal policies do not go through the process of Secretarial approval and are therefore not deemed to be federal rules.
COMPLEXITY OF THE CURRENT ORGAN TRANSPLANTATION SYSTEM
“We have to make our processes more nimble. I think everyone in this system, no matter who we represent, are all extremely well intentioned. But, when we get it wrong, we have to own it and do better.”
—Jayme Locke, University of Alabama at Birmingham, testimony to the committee during July 15, 2021 public listening session
The current organ transplantation system in the United States is a complex web with multiple entities involved in various aspects of making and implementing policies, gathering data, and providing oversight. This web includes multiple agencies within HHS, including HRSA, the Centers for Medicare & Medicaid Services (CMS), Centers for Disease Control and Prevention, the Food and Drug Administration, and the National Institutes of Health. In addition, NOTA created the OPTN as an independent entity, and HRSA maintains two contracts: the OPTN and the Scientific Registry of Transplant Recipients (SRTR) to support the system (see Figure 2-1).
The OPTN is charged with developing policies for and implementing an equitable system of organ allocation, maintaining the waiting list of potential recipients, and compiling data from U.S. transplant centers. OPOs and transplant centers certified for participation in Medicare are required to participate in the OPTN. The OPTN’s oversight responsibilities include solid organ donation and transplantation from deceased donors, but also include ancillary activities on living organ donation. UNOS, a nonprofit, private voluntary organization, holds the subcontract for the OPTN and has been the sole administrator of the OPTN since the initial contract was awarded by HRSA in 1986.13
Oversight for the OPTN contract is provided by the Division of Transplantation (DoT) in HRSA, part of HHS. DoT also administers the contract for the SRTR that provides analytical support for the OPTN’s evaluation of existing allocation policies and development of new policies. For the past 12 years, the SRTR contract has been held by the Hennepin Healthcare Research Institute’s Chronic Disease Research Group, which uses the data collected by the OPTN to provide HRSA with the OPTN/SRTR Annual Data Report. Section 373 of the Public
___________________
11 Organ Procurement and Transplantation Network Final Rule, 42 C.F.R. §121. The current version of the Final Rule can be viewed at https://www.ecfr.gov/current/title-42/chapter-I/subchapter-K/part-121 (accessed February 3, 2022).
12 Organ Procurement and Transplantation Network Final Rule, 42 C.F.R. § 121. The current version of the Final Rule can be viewed at https://www.ecfr.gov/current/title-42/chapter-I/subchapter-K/part-121 (accessed February 3, 2022).
13 The OPTN board of directors are elected and simultaneously installed as UNOS Corporate Board of Directors Members, resulting in identical board memberships. However, UNOS and the OPTN are not interchangeable: UNOS is a nonprofit corporation; the OPTN is a nongovernmental body, established by law, comprised of volunteers, professionals, and other stakeholders involved in the donation and transplantation system and operated under federal contract.

NOTES: HHS = Department of Health and Human Services; NOTA = National Organ Transplant Act. *United Network for Organ Sharing (UNOS) is the current OPTN contractor. **Hennepin Healthcare Research Institute (HHRI) is the current Scientific Registry of Transplant Recipients (SRTR) contractor. The Health Resources and Services Administration (HRSA) acts as a liaison connecting the overlapping efforts of both contractors.
SOURCE: HRSA. Provided by Frank Holloman, January 31, 2022.
Health Service Act requires the SRTR operator to support ongoing evaluation of the scientific and clinical status of solid organ transplantation. It aims to present its data and analytical results in a way that facilitates their use by all constituencies in the organ transplantation community (SRTR, 2022).
The HHS Advisory Committee on Organ Transplantation (ACOT) has advised the HHS secretary on (1) enhancing organ donation, (2) ensuring that the system of organ transplantation is grounded in the best available medical science, (3) assuring the public that the system is as effective and equitable as possible, and (4) increasing public confidence in the integrity and effectiveness of the transplantation system (HRSA, 2021a). ACOT has been sporadically active since 2004. During the April 2020 ACOT meeting, recommendations were made to the HHS secretary on reexamining impediments to transplants for HIV-positive patients through the HIV Organ Policy Equity (HOPE) Act and improving testing with respect to the microbiological evaluation of organ donors and transplants (HRSA, 2021b).
NATIONAL GOALS TO DRIVE SYSTEMATIC IMPROVEMENT
A range of federal and nonfederal actors oversees the current organ transplantation system, resulting in a complex web of responsibilities and accountabilities across stakeholders. This committee carefully considered opportunities for the federal government to set clear goals for the organ transplantation system in terms of equity and quality. The following section considers the significant successes of national efforts to improve health care quality and patient safety and sets the stage for the committee’s recommendation that HHS should set national performance goals for the U.S. organ transplantation system (Recommendation 1).
Establishing clear goals at an appropriate scale is fundamental to successful quality improvement (Alyesh, 2021). For example, bold goals implemented at the national scale previously resulted in significant national increases in hospital patient safety. The IOM landmark 1999 report, To Err Is Human, estimated that there were between 44,000 and 98,000 deaths annually in U.S. hospitals due to medical errors (IOM, 2000). The report precipitated national, statewide, and organization-specific activities to improve patient safety, including the Institute for Healthcare Improvement 100,000 Lives Campaign, concerted and successful efforts to improve hospital patient safety in the Veterans Hospital Administration, and more.
As part of this growing movement, then HHS Secretary Kathleen Sebelius, together with CMS Administrator Don Berwick and other national leaders, launched the Partnership for Patients initiative in 2010. The partnership was grounded in a bold national goal to reduce preventable harm in all U.S. hospitals by 40 percent by 2014 (CMS, 2011). According to subsequent independent reviews by the Agency for Healthcare Research and Quality (AHRQ), safety improved in U.S. hospitals from the 2010 baseline year through 2014, resulting in 2.1 million fewer harms, an estimated 87,000 deaths prevented, and $19.9 billion in cost savings (AHRQ, 2016). U.S. hospitals achieved a 17 percent reduction in overall harm from the 2010 baseline, which equated to a 39 percent reduction in preventable harm. Based on the success of the initial 4-year Partnership for Patients initiative, CMS has continued to support hospital quality improvement in patient safety through the present.
AHRQ estimates of sustained national reductions in hospital harm rates through 2017 are summarized below in Figure 2-2 (AHRQ, 2016, 2020). The harm rate has gone from 145 harms per thousand discharges in the 2010 baseline year to 86 harms per thousand discharges in 2017. Two values are reported for 2014 to permit comparisons of rates that reflect an adjustment in AHRQ’s standardized methodology for tracking hospital harm.
Bold goals implemented at the national scale also resulted in previous major national improvements in organ donation (Shafer et al., 2006). In April 2003, then HHS Secretary Tommy Thompson joined with national leaders from the Institute for Healthcare Improvement, the American Society for Minority Health and Transplant Professionals, the Association of Organ Procurement Organizations, and others to formally commit to achieving an ambitious target of a 75 percent organ donation rate in the nation’s 500 largest hospitals through a Contract for Results. The goal was established based on data showing that about 15 of the nation’s 200 largest trauma centers had already been able to achieve a donation rate greater than 70 percent (Shafer et al., 2006). These high-performing hospitals constituted 5 percent of the total large trauma centers targeted by the quality improvement initiative. Over the course of the next several years, all 59 of the nation’s OPOs, together with many of their largest hospitals, jointly engaged in a massive quality improvement effort to learn, test, adapt, and spread the best practices of the large trauma centers and OPOs with high donation rates. This effort resulted in major increases in the numbers of the nation’s largest hospitals who achieved the 75 percent donation rate goal and major increases in overall donation rates
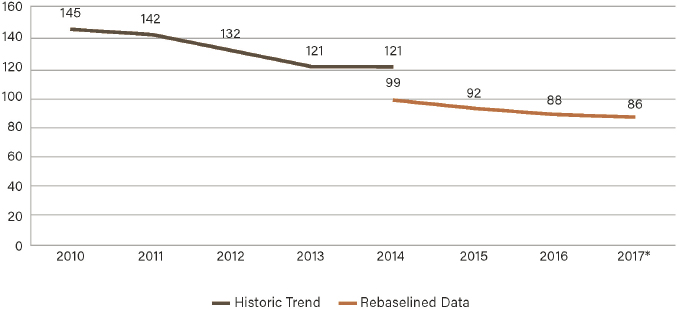
SOURCE: AHRQ, 2020. AHRQ National Scorecard on Hospital-Acquired Conditions: Final Results for 2014 Through 2017.
(Shafer et al., 2006). In 2005, HRSA and HHS formally recognized teams from 184 of the nation’s 500 largest hospitals and their affiliated OPOs who had achieved the 75 percent donation rate (HHS, 2005). In 2006 and 2007, 371 and 392 hospitals were recognized for achieving this rate, respectively. HHS continued various forms of recognition for increased organ donation and transplantation yield through at least 2009.
As part of this same quality improvement effort, in January 2004 HHS set an additional national goal, increasing the proportion of deceased donors whose deaths have been determined based on loss of circulatory function to 10 percent of the total. At that time, only about 4 percent of total deceased donors organs came from DCDD and only a handful of OPOs were implementing the DCDD protocol. The organ donation community of practice (i.e., donor hospitals and OPOs) achieved the 10 percent DCDD threshold in 2007. Growth in DCDD has continued since then: in 2021 approximately 30 percent of all deceased donors came from DCDD donors (4,187 DCDD donors out of the total 13,861 deceased organ donors in 2021) (OPTN, 2022).
Approach to Establishing Ambitious Goals
In all three of the cases outlined above, the goals established by HHS were extremely ambitious, but they were also grounded in the proven practices and outcome levels already achieved by the highest performers in the system. The quality improvement goal on donation was established using the levels of performance achieved by the top 5 to 10 percent of organizations (e.g., 5 percent of the 500 largest trauma centers). After 4 years of intensive quality improvement, nearly 80 percent (392) of the 500 largest trauma hospitals in the nation were recognized by HHS for achieving the 75 percent donation rate target.
The 2003–2004 goal that 10 percent of deceased donors originate with DCDD was achieved in a similar 4-year time frame, representing a more than double increase from the original 4 percent national rate in 2003. At that time, few OPOs were pursuing DCDD donors, and only 6 of the 59 had achieved a rate where 10 percent or more of their deceased donors came from DCDD.14 In both of these organ donation and transplant cases, and in
___________________
14https://optn.transplant.hrsa.gov/data/view-data-reports/national-data (accessed November 5, 2021).
the case of the national patient safety goal of a 40 percent reduction in preventable hospital harm within 4 years, HHS successfully used ambitious time-limited goals to substantially increase the overall performance of the system, based on the proven practices and the levels of achievement of the highest performers in the system.
When establishing ambitious goals of this nature, it is important to be mindful of potential unintended consequences. For example, in establishing a goal to increase the percentage of deceased donors coming from DCDD, it is often useful to incorporate balancing measures to ensure that the total numbers of donors coming from donation after neurological determination of death (DNDD) do not drop as a result of the ambitious DCDD goal. In recommending ambitious goals like those outlined in this report, it is the intention of the committee that the goals be pursued and obtained in ways that represent meaningful progress and true effects that benefit the patients we all serve, not as a result of gaming or manipulation of data (HRSA, 2018).
The goals recommended in this report are as ambitious as each of the prior examples detailed above. Achieving the recommended targets outlined in this report will require commitment, persistence, and focused attention to learning, testing, spread, and improvement of known best practices that are already being used by the highest performers in the system.
Conclusion 2-1: The current organ transplantation system is unduly fragmented and inefficient. The system’s component parts—physicians caring for patients with organ failure, donor hospitals, organ procurement organizations, the OPTN, transplant centers, the SRTR, CMS and other payers, among others—do not operate as a fully integrated system. Likewise, the entities with oversight responsibilities each oversee particular components, but none monitors the performance of the system as a whole in producing predictable, consistent, and equitable results.
Conclusion 2-2: The organ transplantation system could save additional lives and be more equitable if its component parts functioned in a more cohesive fashion and were overseen by a single entity, or by several entities operating in a coordinated fashion with common goals and unified policies and processes. Such alignment of all components and oversight responsibilities would allow the public and Congress to ascertain whether the system is fairly and efficiently maximizing the benefits provided by organ donation and transplantation.
Conclusion 2-3: Since deceased donor organs are a national resource, the fairest way to allocate them to patients on the waiting list is on a national, continuous basis, in accordance with the OPTN Final Rule 2000 as most recently revised by HHS. The committee recognizes that some members of the transplant community feel strongly that deceased donor organs procured in a particular geographic area should be retained for allocation to wait-listed patients in that area.
Conclusion 2-4: By setting ambitious goals in its prior quality improvement initiatives in organ transplantation, HHS has achieved significant progress in increasing the number of successful transplants performed nationally.
Current OPTN Policy Development Process
The OPTN’s current policy development process is lengthy and complex (see Figure 2-3).
Overview of Policy Development Steps
The OPTN’s policy development process begins with a proposal process informed by first gathering information from a variety of sources and stakeholders via the existing OPTN committee structure. UNOS staff leaders and the OPTN committee leadership review proposals and prioritize those that offer the greatest potential benefit for the transplant community, best align with the OPTN’s strategic goals, and are within the legal and regulatory authority of the OPTN. Before proposals are released for public comment, a HRSA review for compliance is conducted. Proposals developed by committees are approved for public comment release following review by HRSA and the OPTN Board or Executive committee,15 after
___________________
15 Before the public comment period is approved, proposals are reviewed by HRSA to determine if the proposal is within the legal, regulatory, and contractual authority of the OPTN and the OPTN Policy Oversight Committee to ensure that the project engages the appropriate stakeholders and provides solutions tailored to the problem, as well as determining whether it imposes any significant fiscal burdens on the transplantation system.

SOURCE: OPTN policy development process explanatory document. https://optn.transplant.hrsa.gov/media/3115/optn-policy-development-process-explanatory-document.pdf (accessed November 18, 2021).
which the arguments and concerns expressed by stakeholders are reviewed to ensure that all relevant constituencies and demographics are well represented. The sponsoring committee reviews the public comments, revises the proposal if needed (which may be subject to another round of public comments), and then votes on whether to send the policy proposal to the Board.16 The Board considers the committees’ recommended policy proposals, and receives input from Board policy groups, which are subgroups of the Board that provide initial review as part of the Board review process, consisting of stakeholders representing transplant programs, OPOs, living donors, donor families, and members with specific policy-relevant competencies. The Board policy group review is an operational process; only the OPTN Board approves policies.
To approve a policy, the Board requires evidence that the proposal addresses the stated problem, complies with NOTA and the Final Rule, and is aligned with the OPTN strategic plan. Rejected proposals are returned to the appropriate committee for further consideration. When the board adopts a policy proposal, it is officially designated as the “OPTN policy.” UNOS staff regularly review the effectiveness and potentially negative effects of implemented policies by collecting and analyzing relevant data, then report their findings to the board and the sponsoring committees. These continuous review activities may result in new projects to further refine a policy. Similarly, the Membership and Professional Standards Committee’s monitoring of member compliance with policies may also lead to new policy projects.
___________________
16 During this time, UNOS staff also prepares an estimate of the resources that the OPTN will need to implement and maintain the new policy, including the costs of monitoring member compliance, as well as a review by subject matter experts of the proposal’s fiscal effect on the OPTN members.
Advantages and Disadvantages of the OPTN Policy Development Approach
The OPTN’s current policy development process has advantages and disadvantages. Its advantages include transparency, collaboration, and centralization. For instance, to ensure ample stakeholder involvement throughout the policy development process, multiple stakeholder individuals and organizations are encouraged to collaborate with the responsible OPTN committee(s) in the development of national transplant policies and medical criteria. During the public comment period feedback is solicited from those closely aligned within the organ transplantation system, and most importantly, the overall public who are outside the system. Following the close of the public comment period, the relevant OPTN committee addresses the issues raised by publishing written responses. Stakeholder and public engagement with the policy-making process is an advantage of the OPTN approach, providing important feedback and direction for policy-making and strengthening public trust in the process. A recent change was made to enhance the role of the Policy Oversight Committee, which is responsible for harmonizing and prioritizing policy-making work and timelines across OPTN committees. Additionally, centralized rulemaking enables OPTN policy makers to focus on a set of predetermined policy objectives.2
The disadvantages of the process relate to its length, complexity, and challenges in implementation. Because the OPTN’s rulemaking process seeks engagement and input from a broad range of passionate stakeholders, the policy process requires multiple committee reviews to avoid possible unintended consequences across the OPTN. Although rare, additional public comment periods may also be necessary if substantial policy revisions are made as a result of public comment. As an operating committee of the OPTN, the Policy Oversight Committee advises the OPTN Board of Directors and Executive Committee in the development of strategic policy priorities, prioritization and coordination of policy and committee projects with broad implications for the OPTN, evaluation of policy and committee proposals prior to public comment, assessment of the impact of proposed policies, and confirmation that the OPTN committees justify proposals in compliance with policy development requirements. The Policy Oversight Committee has helped to avoid situations in which committee projects are placed on hold and started again, sometimes multiple times. The consensus-driven nature of the OPTN policy development process can create slowness and policy implementation challenges can further delay the process, such as when stakeholders are in disagreement about how best to allocate organs and categorize patient prioritization on the waiting list. Recently, this already lengthy process has been further exacerbated by litigation.17
The steps in the OPTN policy-making process are also complex and variable in the time allotted for public comment periods, as well as the overall time taken from committee project approval to OPTN board approval. For example, a federal study of the similarities and differences in the processes the OPTN used to change the liver and lung allocation policies revealed variations in public comment periods for informing the policy development process. The current liver allocation policy included a 25-day public comment period; the 2017 liver allocation policy included two separate 62-day and 64-day public comment periods; and the current lung allocation policy had a retroactive 61-day public comment period (GAO,
___________________
2 Organ Transplantation: Issues and Recommendations: Report of the Task Force on Organ Transplantation. Rockville, MD: U.S. Dept. of Health & Human Services, Public Health Service, Health Resources and Services Administration, Office of Organ Transplantation (1986), at 91.
17 An April 2019 press release posted to the OPTN website explained that “implementation of both the liver and intestinal organ distribution policy based on acuity circles and the National Liver Review Board (NLRB) will be deferred” as a result of a pending federal lawsuit challenging this new OPTN-approved liver distribution policy, which had been under development for years. https://optn.transplant.hrsa.gov/news/liver-distribution-policy-nlrb-implementation-deferred-until-may-14 (accessed April 12, 2022).
2020). Significant variability exists in terms of the average time it takes from committee project approval to final board approval. For example, as presented during the virtual public session of the OPTN’s December 6, 2021, Board meeting,18 between 2009 and 2021 the longest period of policy development was 9.6 years for the revised kidney allocation system in 2013 (see Figure 2-4). A project on liver distribution redesign modeling in 2017 took 6.4 years from committee project approval to board approval. Since 2019, project timelines have shown a downward trend with the 2021 continuous distribution policy for lungs taking 2.6 years. Implementation time for each policy was not included in the presented analysis.
There is limited information and analyses of the overall performance of the policy-making process in meeting the stated goals of the OPTN. Based on the evidence of variability in overall OPTN policy development timelines and challenges in maintaining stakeholder agreement on contentious issues in patient prioritization and organ allocation, the committee believes there is an opportunity for the OPTN to draw on previously untapped external organizations with expertise in managing complex stakeholder involvement through a transparent and collaborative process.
Conclusion 2-5: The OPTN policy-making process includes extensive committee reviews that aim to involve all stakeholders, but the nature of the reviews contributes to variability and a general slowness in policy development and implementation. Identifying and prioritizing strategic objectives through process changes in committee responsibilities and implementing continuous distribution as the uniform policy model have been effective in the last 2 years in decreasing the time for policy approval by the OPTN Board of Directors; however, opportunities for improvement in policy development and implementation timelines exist.
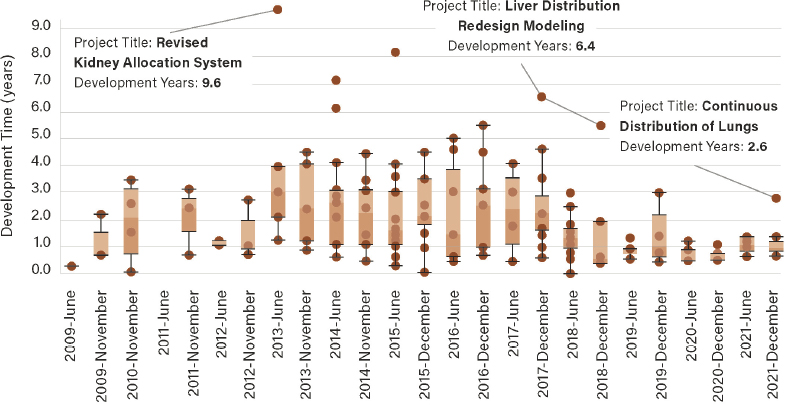
SOURCE: “OPTN Contract Requirement 3.3.2.: Policy Development Process Metrics – Metric 9: Average Time from Committee Project Approval to Board Approval.” OPTN Policy Oversight Committee Chair Report to the OPTN Board of Directors. 6 December 2021. Provided by: Chelsea Haynes, UNOS.
___________________
18https://unos.org/news/optn-board-adopts-new-transplant-program-performance-metrics (accessed January 26, 2022).
Conclusion 2-6: Organizations such as the National Quality Forum (NQF) are skilled in the development and use of timely, multistakeholder, consensus-based developmental processes, like the Measure Applications Partnership (MAP). The work of the NQF MAP is tied to, and guided by, specific regulatory and payment timelines of participating HHS agencies and their associated rulemaking processes. The experience and expertise of the NQF and/or other similar organizations can provide valuable insights to inform improvements in speed and agility, as well as stakeholder engagement and consensus of OPTN policy development work.
DECEASED DONOR ORGAN USE AND ECONOMICS TODAY19
This section briefly summarizes data and trends pertaining to deceased donor organ use that are relevant to the committee’s charge, including statistics on wait-listing (see Table 2-1), deceased organ donation, transplantation, and resource use metrics such as initial hospital length of stay and hospital readmission rates. Although the organ system writ large is greatly affected by living donor donation, this study’s scope is limited to deceased donation after brain death or circulatory death. Living donation has the potential to increase the number of organs available for transplantation, shorten waiting times, improve morbidity, improve quality of life, and address inequity and unfairness in distribution systems (Gruessner and Gruessner, 2018; Humar et al., 2019; Kazley et al., 2019; Levy et al., 2016; Mathur et al.,
___________________
19 This section draws heavily from the 2019 SRTR/OPTN Annual Data Report (released February 2021). The 2019 SRTR/OPTN Annual Data Report includes data from 2008–2019 and was the most recent summary publication available at the time this committee’s report was published. Wherever possible, the committee uses 2021 data on the number of individuals on the waiting list and the number of transplants performed from the OPTN website: https://optn.transplant.hrsa.gov/data (accessed January 26, 2022).
| U.S. waiting list candidates (n) | Living donor organ transplants in 2021 | Deceased donor organ transplants in 2021 | |
|---|---|---|---|
| Kidney | 90,293 | 5,970 | 18,699 |
| Pancreas | 838 | 0 | 143 |
| Liver | 11,489 | 569 | 8,667 |
| Intestine | 201 | 0 | 96 |
| Heart | 3,458 | 0 | 3,817 |
| Lung | 1,055 | 0 | 2,524 |
| Kidney/Pancreas | 1,815 | 0 | 820 |
| Heart/Lung | 35 | N/A | 45 |
SOURCE: OPTN https://optn.transplant.hrsa.gov/data/view-data-reports/national-data (accessed January 25, 2022). U.S. waiting list candidates for each organ as of February 1, 2022. Total waiting list candidates are 106,557; organ totals are less than the sum because of patients in multiple categories. Living donor and deceased donor organ transplants are totals for 2021.
2020; Pena, 2016; UNOS, 2021). Neither tissue transplantation nor vascularized composite allotransplantation were a significant focus of the committee.
The nonuse rates provided for each organ, which are based on the number of organs recovered for transplant but not transplanted, are particularly important in informing efforts to optimize the use of deceased donor organs (Figure 2-5). Over the past decade in the United States, there have been increases in the numbers of both deceased organ donors and deceased donor organ transplants, which reached all-time highs of 13,861 and 41,354 in 2021, respectively (OPTN, 2022). However, the percentage of organs recovered for transplant but not transplanted has continued in an upward trend. For each type of organ, the rates of nonuse also increased in 2019 over 2018 (Figure 2-5). In addition to issues of organ nonuse, some argue that after controlling for the impact of public health crises and trends, organ donation rates have not kept pace with population growth, as they should (Karp et al., 2021).
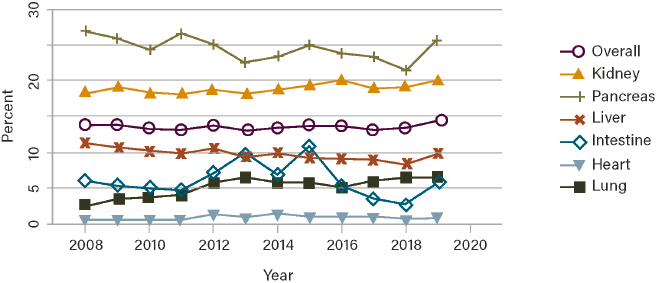
NOTE: Percentages are calculated as the difference between the number of organs recovered and the number of organs transplanted, divided by the number of organs recovered. Pancreata recovered for islet transplant are excluded.
SOURCE: Israni et al., 2021.
Vascularized Composite Allotransplantation
Vascularized composite allotransplantation (VCA) is a form of solid organ transplantation involving the transplantation of multiple structures that may include skin, bone, muscles, blood vessels, nerves, and connective tissue as a functional unit in patients with major tissue loss or injury. A VCA may provide an alternative treatment option when reconstructive surgery is not feasible or effective. VCA transplants are performed to improve functional outcomes and quality of life and thus intend to be life enhancing, and are not considered lifesaving. For example, some recipients received a VCA organ after traumatic injury or limb loss through trauma (e.g., war-related exposure to explosive devices or traffic accidents).
In the United States, the first unilateral upper extremity transplant was performed in 1999. In the past decade, more than 90 individuals have received a VCA (American Society of Transplantation, 2021). HHS redefined VCAs as organs, as opposed to tissue, in 2014, which enabled the OPTN to assume oversight of policies pertaining to authorization for deceased donation, allocation, and distribution of VCA organs. CMS redefining VCA as an organ would allow increased alignment across performance metrics in the transplantation system. VCA transplants include upper extremity, face, uterus, penis, larynx, abdominal wall, and others. Most VCA organs are donated by deceased donors; however, uterus donors may also be living donors.
The field of VCA is growing. The surgical procedures themselves are generally no longer construed as experimental procedures, considering the mastery of microsurgical techniques and immunosuppressive approaches have placed reconstructive surgery at the highest rung in the surgical ladder (Cetrulo et al., 2017; Kaufman et al., 2019). However, the determination of whether VCA is a standard of care is a complex matter. Some countries consider certain forms of VCA as being a standard of care (Kaufman et al., 2019).
In the United States, all transplant programs have traditionally been required to obtain institutional review board (IRB) oversight to perform VCA. However, some VCA programs are no longer functioning under IRB oversight. Currently, VCA costs are covered by transplant programs. Insurance companies do not currently pay for VCA because they view VCA as not being the standard of care. A major challenge to becoming a standard of care is the small number of patients undergoing each type of VCA procedure. Without enough information on long-term functional outcomes among enough recipients to control for demographic and clinical variables, it is unclear whether the procedure is effective and worth the risks (ethically) and resources (financially). Insurance companies are awaiting long-term outcomes data before covering these procedures.
For reasons delineated, the broad scope of the study task and the limited time frame for this study, the committee did not conduct an in-depth analysis of VCA transplantation. The committee considered the implications that increased use of VCA could have on organ donation including some of the challenges that may arise as the public increasingly confronts difficult questions of whether they, as individuals, would approve donation of their organs (e.g., face, uterus, or penis) upon their death. Public opinion is generally supportive of VCA donations from deceased donors (Rodrigue et al., 2017); however, given the limitations of educational materials on VCA (Rasmussen et al., 2020), the transplant community will need to develop efforts to educate the public about how to make informed decisions about donating VCA organs and explain how VCA organs will be procured and used.
Key Use Statistics and Trends by Organ20
The landscape of kidney transplantation in the United States is characterized by promising trends and ongoing challenges. The overall number of kidney transplants has continued to increase over the past 6 years, reaching 24,273 in 2019—more than 70 percent of which were deceased donor organ transplants. However, the number of available donor kidneys is far surpassed by the number of patients awaiting kidney transplant, and the extent of the shortage is far greater than other organs. From 2014 to 2019, only approximately 25 percent of patients on the waiting list received a deceased donor kidney transplant within 5 years, and this varies significantly based on donation service area—from 15.5 to 67.8 percent. In 2019, the nonuse rate for deceased donor kidneys was 20.1 percent overall (Israni et al., 2021). As will be described in Chapter 6, the probability of receiving a deceased donor kidney transplant within 3 years of waiting list placement varies across transplant centers in the United States, with 16-fold variance between centers. Waiting patients at transplant centers with low offer acceptance rates have only a 4 percent chance of getting a transplant within 3 years. Conversely, patients waiting at transplant centers with high offer acceptance rates have a 65 percent chance of getting a transplant within 3 years (King et al., 2020).
Of note, the rate of nonuse of hepatitis C virus (HCV)-positive kidneys has been declining since 2014 and by 2019, the rate was nearly equivalent to that of HCV-antibody-negative kidneys. In terms of resource use, the average length of hospital stay after transplant for kidney recipients was 7.4 days in 2019, a slight decline since 2008. The rate of reported hospital readmission during the first year posttransplant was 48.1 percent in 2018.
More than 1,000 pancreas-alone and kidney-pancreas transplants were performed in 2019—a number that remained relatively stable compared to 2018, as did the number of wait-listed patients awaiting transplant. The number of deceased organ pancreas transplants has increased marginally since the 2014 revision of the Pancreas/Kidney-Pancreas Allocation System. However, a concerning issue is the high rate of nonuse for deceased donor pancreata—25.4 percent in 2019—compared to other organs; this may be related to relatively short pancreas transplant wait times and the current state of the art for pancreas transplantation. For pancreas recipients, the average length of transplant hospitalization in 2019 was 11.5 days and the rate of hospital readmission during the first year posttransplant was almost 62 percent; both of these have declined in recent years.
Almost 8,900 liver transplants were performed in 2019, 94 percent of which were deceased donor transplants. HCV-positive donor organs have continued to increase since 2008, representing 9.7 percent of deceased donor livers in 2019. Both the number of new waiting list registrations and the number of transplants performed have been on the rise, while both the median waiting time for candidates with a Model for End-Stage Liver Disease (MELD) score of 15–34 and the number of transplants performed for patients with exception points decreased.21 The nonuse rate for deceased donor livers was 9.6 percent in 2019 compared to 8.6 percent in 2018, likely driven by an increase in nonused organs from donors aged 55 years or more. For liver recipients, the average length of transplant hospitalization in 2019 was 20.8 days and the rate of hospital readmission during the first year posttransplant
___________________
20 This section reflects information in the 2019 SRTR/OPTN Annual Data Report (https://www.srtr.org/reports/srtroptn-annual-data-report [accessed January 26, 2022]) which was the most recent summary publication available at the time this committee’s report was published.
21 These changes may have been related to the policy changes that took effect in May 2019, which increased waiting list priority for candidates without exception status.
was almost 60 percent among those who received a transplant in 2018; both of these have remained relatively stable since 2008.
Intestine transplants represent the smallest proportion of solid organ transplants performed in the United States.22 Intestine transplantation is a maturing field, and advances in intestine failure therapies have resulted in fewer patients being added to the waiting list for intestine transplant alone or for intestine transplant in combination with other organs. Just 81 deceased donor intestine transplants were performed in 2019. The nonuse rate for deceased donor intestines was relatively low, at about 6 percent. For intestine recipients, average length of transplant hospitalization in 2019 was about 61 days, which has varied substantially over the past decade. The rate of hospital readmission during the first year posttransplant was almost 96 percent among those who received a transplant in 2018—far higher than any other organ.
Around 3,600 heart transplants were performed in 2019—a slight increase over the previous year—but the number of candidates on the waiting list continued to increase.23 The number of donor hearts increased by almost 64 percent between 2008 and 2019, when the number reached an all-time peak. The nonuse rate for deceased donor hearts was less than 1 percent, the lowest of all organs, although this rate has fluctuated over the past decade. For heart recipients, the average length of transplant hospitalization in 2019 was about 49 days, trending upward in recent years. The use of some preoperative devices or days of requiring extracorporeal membrane oxygenation as a bridge to transplantation could account for the lengthier hospital stay for some heart transplant recipients. Heart transplant patients without these interventions have much shorter hospital stays (e.g., less than 10 days). The rate of hospital readmission during the first year posttransplant was just under 40 percent, which was also the lowest rate of all organs.
The number of lung transplants performed each year in the United States is continuing to rise, increasing by 52.3 percent over the past decade and reaching an all-time peak of almost 2,800 transplants in 2019. This trend is likely attributable to increasing numbers of wait-listed candidates as well as the number of donors, which has increased by 62 percent in the last 10 years. The mortality rate for individuals on the lung waiting list decreased 14.6 percent in 2019, which is an important positive trend given the increasingly older and sicker lung candidate population. The nonuse rate for deceased donor lungs was more than 6 percent in 2019. For lung recipients, average length of transplant hospitalization in 2019 was around 34 days, which has generally increased in recent years. The rate of hospital readmission during the first year posttransplant was close to 52 percent.
From 2013 to 2017, 8,246 multiorgan transplants (MOTs) were performed in the United States, with 1,853 occurring in 2017 (OPTN, 2019). The most frequent type of MOT across this 4-year period were kidney–pancreas, kidney–liver, and kidney–heart, respectively. Additionally, the rate of MOT has been increasing over the last 2 decades (OPTN, 2019). MOTs, however, create issues of inequities, given that each combination of organs has its own allocation strategies and prioritization of those awaiting a MOT has not been standardized across the different organs. For example, some organ combinations require a candidate to join a single, combined, or multiple organ waiting lists. Confusion has arisen because of the varying levels of OPO discretion regarding their ability to “choose which MOT combinations get allocated if there are multiple MOT combinations possible from the same donor” (OPTN, 2019). Additionally, across the United States the current prioritization according to Policy
___________________
22 Intestine transplants may be performed alone, with a liver transplant, or as part of a multivisceral transplant including combinations of liver, stomach, pancreas, colon, spleen, and kidney.
23 A new adult heart allocation policy was approved in 2016 and implemented in October 2018; 2019 data may illustrate early effects of this policy.
5.10: Allocation of Multi-Organ Combinations is that a MOT is typically prioritized above single organ transplant at the local level, which can also affect equity differently across the country depending on the volume of MOTs in the differing geographic areas.
Cost-Effectiveness of Transplantation by Organ
This section provides an overview of recent studies that have estimated the cost-effectiveness of kidney, liver, heart, and lung transplantation. It should be noted that even though the OPTN/SRTR’s Annual Data Report releases data suitable for use in cost-effectiveness modeling of solid organ transplantation, up-to-date cost-effectiveness studies are not always available for all organs. Although cost-effectiveness analyses provide important information, they are only one element among others guiding health policy. There is debate about methodological and ethical shortcomings of the “quality-adjusted life year” (QALY), the most typically used measure of health gains in cost-effectiveness assessments of medical interventions (Rand and Kesselheim, 2021).
Cost-Effectiveness of Kidney Transplantation
Kidney transplantation is associated with a significant improvement in patient survival and quality of life across the spectrum of organ quality compared with maintenance dialysis (Axelrod et al., 2018; Massie et al., 2014; Whiting et al., 2000; Wolfe et al., 1999, 2009). Recent estimates (Axelrod et al., 2018) indicate that end-stage kidney disease (ESKD) patients who receive a living donor kidney transplantation (LDKT) or deceased donor kidney transplantation (DDKT) experience significantly longer expected survival than ESKD patients who receive dialysis therapy in terms of derived QALYs: 10 years with dialysis therapy, 4.03 QALYs; LDKT (human leukocyte antigen [HLA]-compatible, well-matched living donor [LD]), 6.34; LDKT (ABO-incompatible LD), 6.12; LDKT (HLA-incompatible LD), 5.47; DDKT (KDPI24 < 85), 6.07; DDKT (Public Health Service [PHS] increased risk), 5.91; DDKT (KDPI > 85), 5.20. Kidney transplants are also the most cost-effective treatment for ESKD,25 although the extent of the cost savings varies by quality of the donor organ.
Axelrod et al. (2018) estimate that from the payer’s (i.e., Medicare’s) perspective, low-to-moderate KDPI (≤ 85) DDKTs are cost saving over 10 years compared to dialysis ($49,017 vs. $72,476 per QALY), as are high-KDPI (> 85%) DDKT compared to dialysis ($63,531 vs. $72,476 per QALY). Despite the additional therapeutic procedures needed to facilitate complex transplants such as ABO-incompatible LDKT, they also represent cost savings ($59,564 per QALY) compared to remaining on dialysis. Compared to DDKT, HLA-compatible LDKT was more cost effective for compatible donors with up to three HLA mismatches ($39,939 per QALY) and for compatible donors with four to six HLA mismatches ($41,016 per QALY). Consistent patterns were found upon repeat analysis using a 20-year time horizon; all transplantation options resulted in cost-effectiveness ratios lower than the commonly cited willingness-to-pay threshold of $100,000 per QALY (Neumann et al., 2016).
___________________
24 For deceased donor kidneys, the Kidney Donor Profile Index (KDPI) provides a measure of organ quality by summarizing the likelihood of graft failure after DDKT.
25 Organ transplantation cost-effectiveness studies typically compare the cost of achieving one additional QALY between alternative treatments. A payer perspective is usually adopted, implying that direct medical care costs are considered. Direct health care cost comparisons, however, underestimate the potential overall societal benefit, which ought to include both the productivity gains from returning to employment and associated tax revenue, which are higher for transplant recipients. Held et al. (2016) estimate that the full value of a transplant to a patient on the waiting list is $937,000.
Cost-Effectiveness of Liver Transplantation
Recent studies found liver transplantation to be cost effective (less than $100,000 per QALY). For instance, Dageforde et al. (2013)26 studied the cost-effectiveness of liver transplantation with DNDD organs and DCDD organs by considering two waiting list strategies: (1) only DNDD organs and (2) both DNDD and DCDD organs (DNDD + DCDD). Over a 10-year horizon, the DNDD + DCDD waiting list strategy was more cost effective (5.6 QALYs; cost of $69,000/QALY) than the DNDD-alone strategy (6.0 QALYs; cost of $61,000/QALY) because of the decreased waiting list mortality and pretransplant morbidity associated with the former strategy.
In the United States, the current practice is for HCV-negative patients only to accept HCV-negative livers. Bethea et al. (2019) compared the cost-effectiveness of this current strategy versus a strategy of accepting any HCV-negative or HCV-positive livers, with recipients of HCV-positive livers receiving preemptive direct-acting antiviral therapy. For patients with a MELD score of 28,27 it was cost effective for them to accept any liver. The incremental cost-effectiveness ratio of accepting any liver versus accepting only HCV-negative livers was $62,600/QALY. Incremental cost-effectiveness ratios of receiving any liver were less than $100,000 for patients with a MELD score of 22 or greater; the strategy was also cost effective for patients with low MELD scores that may not accurately reflect disease severity.
Sarasin et al. (2001) study found that in the United States, LDLT can be cost effective for patients with early hepatocellular carcinoma when waiting times for transplantation exceed 7 months.28 A study using more recent data29 found that over a 10-year period, both LDLT and deceased donor liver transplantation are cost effective compared to no transplant (i.e., medical management of cirrhosis) (Northup et al., 2009). Being on a waiting list with possible deceased donor liver transplant (DDLT) versus being on a waiting list with possible DDLT or LDLT were associated with 4.4 and 4.9 QALYs, respectively. The DDLT or LDLT strategy had an incremental cost-effectiveness ratio of $106,788 over DDLT only.
Cost-Effectiveness of Heart Transplantation
The 2013 OPTN/SRTR Economics Annual Data Report presented a cost-effectiveness analysis of heart transplantation—the most expensive of the major transplants—that compared transplant recipients who had received a ventricular assist device (VAD) procedure with those who had not (Schnitzler et al., 2015). The total expected discounted cost of care from 1 year prior to the transplant through 20 years posttransplant was lower for a patient with a VAD ($505,000) than patients without a VAD ($525,000). However, patients with a VAD gained fewer discounted QALYs (5.53) than patients without a VAD (6.28). Thus, the cost per QALY was greater for patients with a VAD ($91,000) than those without a VAD ($84,000), although both are within the conventional willingness-to-pay threshold (less than $100,000).
___________________
26 The study (Dageforde et al., 2013) adopted a societal perspective, including direct medical costs and indirect cost such as lost earnings and out-of-hospital expenses.
27 The median MELD score at transplant centers in the United States (Bethea et al., 2019).
28 For short waiting times, the gains from LDLT were only marginal and were outweighed by the losses in life-years caused by the donor operation.
29 From the Adult to Adult Living Donor Liver Transplantation Cohort Study.
Cost-Effectiveness of Lung Transplantation
Schnitzler et al. (2014) used Medicare data linked to SRTR data to examine the effect of allocation based on the lung allocation score (LAS) on the cost-effectiveness of a lung transplant compared with medical management of end-stage pulmonary disease, finding that the relative cost-effectiveness of a lung transplant is correlated with LAS. Specifically, incremental cost-effectiveness ratios—measuring additional costs per QALY gained from a transplant—increased with LAS. Even at the highest LAS scores, the cost-effectiveness of lung transplants is within the conventionally cited limits.30
Conclusion 2-7: Transplantation, independent of organ type, is a cost-effective intervention overall. Although SRTR has been releasing current data on pre- and posttransplant costs suitable for cost-effectiveness modeling, there is a need for up-to-date cost-effectiveness analyses for all organs to ensure that current data on effectiveness and costs are taken into account. There is debate about methodological and ethical shortcomings of cost-effectiveness analyses. In particular, cost-effectiveness may fail to capture features relevant to equity. Cost-effectiveness analyses are only one factor among others guiding health care policy choices.
INNOVATION CHALLENGES AND OPPORTUNITIES
Recommendations made in this report could change some of the OPTN’s operations and processes; thus it is important to identify challenges related to innovation and consider how health care systems can evolve to improve. A robust understanding of health care delivery and innovation science can inform the profession with a specific focus on organ donation and transplantation. Nonetheless, it is a daunting task to change a massive and complicated system with multiple elements and complex interactions. With that in mind, the goal is to create a fairer, more equitable, cost-effective, and transparent system of donor organ procurement, allocation, and distribution.
One successful model for health care systems operationalizing and upscaling innovations is the Veterans Health Administration’s Innovation Ecosystem (VHA IE), which is predicated on multiple pillars that are critical to support the development and implementation of the types of health care innovation suggested in this report (Vega and Kizer, 2020).
- The target workforce must have the capacity to adopt and actualize any innovation.
- The organization infrastructure and leadership must be integrated, practice systemness, and be able to develop repeatable procedures for change.
- An engaging and supportive culture of innovation and resulting change is necessary.
- Collaborations with strategic external partnerships are needed.
- The infrastructure must align with financial resources and incentives, obtain clinical and administrative championship, and appropriate allocation of resources to enable change.
As part of this model’s success, the various innovative health care delivery approaches initiated through the model positively affected more than a million caregivers and veterans, with over 25,000 employees participating, and resulted in $40 million in direct cost avoid-
___________________
30 The cost of 1 QALY gained was $46,472 for LAS scores < 35, $73,053 for LAS scores between 35 and 50, and $103,448 for LAS scores > 50.
ance for the system. The success of the VHA IE approach to innovation, program evolution, and change deserves consideration for the OPTN, OPOs, and transplant centers in prioritizing innovation.
Of course, the complexities of the United States organ procurement and transplant enterprise are not the only challenges to innovative practice implementation and change. External pressures from a variety of professional, political, health care, insurance, and patient advocacy groups will likely present opposition to some suggested changes; these entities may also have their own agendas and recommendations.
While it is critical to improve organ recovery and organ use, addressing the organ shortage and improving the available organs for transplantation can be modified greatly through innovation. For example, the HOPE Act has provided increased transplantation opportunities for transplant candidates with HIV who are willing to accept organs from donors identified as HIV positive. Since the HOPE Act became law in 2013, 170 kidneys and 53 liver transplants have taken place (UNOS, 2020). Similarly, the release of direct acting antiviral medications for the curative treatment of HCV in 2014 has facilitated improved use of HCV-antibody-positive and viremic organs to be transplanted into recipients without HCV with curative posttransplant treatment. This has further increased accessibility and use of organs for transplant. Recently, the use of normothermic perfusion has improved use of physiologically stressed organs, most commonly DCDD organs, with improved outcomes.
Ongoing innovation will be needed in the organ transplantation system. Innovations to improve organ availability and accessibility include all aspects of research, including but not limited to
- Developing novel organ sources (e.g., organoids, printed organs, artificial organs, xenotransplantation);
- Rehabilitating organs not currently being transplanted (e.g., defatting of livers);
- Creating novel organ distribution and transport mechanisms (e.g., using drones, transporting kidneys while on a pump);
- Minimizing immunosuppression posttransplant in order to improve posttransplant outcomes;
- Maximizing both deceased and living donation through improving understanding and outreach to diverse communities;
- Conducting patient-centered research to understand patient priorities for the transplantation system;
- Improving education initiatives for providers, potential donors, and potential transplant recipients; and
- Applying health care delivery and implementation science in the field of organ transplantation, specifically in regards to advancing health equity.
REFERENCES
AHRQ (Agency for Healthcare Research on Quality). 2016. Saving lives and saving money: Hospital-acquired conditions update: Final data from national efforts to make care safer, 2010–2014. https://www.ahrq.gov/sites/default/files/wysiwyg/professionals/quality-patient-safety/pfp/2014finalhacreport-cx.pdf (accessed October 15, 2021).
AHRQ. 2020. AHRQ National Scorecard on Hospital-Acquired Conditions: Final results for 2014 through 2017. https://www.ahrq.gov/sites/default/files/wysiwyg/professionals/quality-patient-safety/pfp/Updated-hacreportFInal2017data.pdf (accessed October 15, 2021).
Alyesh, A. Z. 2021 (unpublished). Quality improvement lessons from health care and applications to the United States organ donation and transplantation system. Paper commissioned by the Committee on a Fairer and More Equitable, Cost-Effective, and Transparent System of Donor Organ Procurement, Allocation, and Distribution, National Academies of Sciences, Engineering, and Medicine, Washington, DC.
American Society of Transplantation. 2021. Vascularized composite allotransplantation (VCA) research. https://www.myast.org/public-policy/vascularized-composite-allotransplantation-vca-research (accessed November 16, 2021).
Axelrod, D. A., M. A. Schnitzler, H. Xiao, W. Irish, E. Tuttle-Newhall, S.-H. Chang, B. L. Kasske, T. Alhamad, and K. L. Lentine. 2018. An economic assessment of contemporary kidney transplant practice. American Journal of Transplantation 18(5):1168-1176.
Bernat, J. L. (2005). The concept and practice of brain death. Progress in Brain Research 150:369-379. https://doi.org/10.1016/S0079-6123(05)50026-8.
Bethea, E. D., S. Samur, F. Kanwal, T. Ayer, C. Hur, M. S. Roberts, N. Terrault, R. T. Chung, and J. Chhatwal. 2019. Cost effectiveness of transplanting HCV-infected livers into uninfected recipients with preemptive antiviral therapy. Clinical Gastroenterology and Hepatology 17(4):739-747.
Cetrulo, C. L., Z. Y. Ng, J. M. Winograd, and K. R. Eberlin. 2017. The advent of vascularized composite allotransplantation. Clinics in Plastic Surgery 44(2):425-429. https://doi.org/10.1016/j.cps.2016.12.007.
CMS (Centers for Medicare & Medicaid Services). 2011. Partnership for patients to improve care and lower costs for Americans. https://www.cms.gov/newsroom/press-releases/partnership-patients-improve-care-and-lower-costs-americans (accessed October 28, 2021).
Dageforde, L. A., I. D. Feurer, C. W. Pinson, and D. E. Moore. 2013. Is liver transplantation using organs donated after cardiac death cost-effective or does it decrease waitlist death by increasing recipient death? International Hepato-Pancreato-Biliary Association 15(3):182-189.
DeVita, M. A., J. V. Snyder, and A. Grenvik. 1993. History of organ donation by patients with cardiac death. Kennedy Institute of Ethics Journal 3(2):113-129.
Domínguez-Gil, B., N. Ascher, A. M. Capron, B. Gardiner, A. R. Manara, J. L. Bernat, E. Miñambres, J. M. Singh, R. Porte, J. F. Markmann, K. Dhital, D. Ledoux, C. Fondevila, S. Hosgood, D. Van Raemdonck, S. Keshavjee, J. Dubois, A. McGee, G. V. Henderson, A. K. Glazier, S. G. Tullius, S. D. Shemie, and F. L. Delmonico. 2021. Expanding controlled donation after the circulatory determination of death: Statement from an international collaborative. Intensive Care Medicine 47(3):265-281.
GAO (U.S. Government Accountability Office). 2020. Organ transplants: Changes in allocation policies for donated livers and lungs. https://www.gao.gov/assets/gao-21-70.pdf (accessed January 24, 2022).
Greer, D. M., S. D. Shemie, A. Lewis, S. Torrance, P. Varelas, F. D. Goldenberg, J. L. Bernat, M. Souter, M. A. Topcuoglu, A. W. Alexandrov, M. Baldisseri, T. Bleck, G. Citerio, R. Dawson, A. Hoppe, S. Jacobe, A. Manara, T. A. Nakagawa, T. M. Pope, W. Silvester, D. Thomson, H. Al Rahma, R. Badenes, A. J. Baker, V. Cerny, C. Chang, T. R. Chang, E. Gnedovskaya, M. K. Han, S. Honeybul, E. Jimenez, Y. Kuroda, G. Liu, U. K. Mallick, V. Marquevich, J. Mejia-Mantilla, M. Piradov, S. Quayyum, G. S. Shrestha, Y. Y. Su, S. D. Timmons, J. Teitelbaum, W. Videtta, K. Zirpe, and G. Sung. 2020. Determination of brain death/death by neurologic criteria: The World Brain Death Project. Journal of the American Medical Association 324(11):1078-1097.
Gruessner, R. W. G., and A. C. Gruessner. 2018. Solid-organ transplants from living donors: Cumulative United States experience on 140,156 living donor transplants over 28 years. Transplant Proceedings 50:3025-3035.
Guidelines for the determination of death: Report of the medical consultants on the diagnosis of death to the President’s Commission for the Study of Ethical Problems in Medicine and Biomedical and Behavioral Research. 1981. Journal of the American Medical Association. 246(19):2184-2186.
Halevy, A., and B. A. Brody. 1993. Brain death: Reconciling definitions, criteria, and tests. Annals of Internal Medicine 119:519-525.
Held, P. J., F. McCormic, F. Ojo, and J. P. Roberts. 2016. A cost-benefit analysis of government compensation of kidney donors. American Journal of Transplantation 16(3):877-885.
HHS (U.S. Department of Health and Human Services). 2005. HHS Honors 184 hospitals for increasing their donation rate to 75%. https://www.thefreelibrary.com/HHS+honors+184+hospitals+for+increasing+their+donation+rate+to+75%25.-a0134175445 (accessed October 28, 2021).
HHS. 2022. History & NOTA. https://optn.transplant.hrsa.gov/about/history-nota (accessed February 1, 2022).
HRSA (Health Resources and Services Administration). 2018. White paper on manipulating waitlist priority. https://optn.transplant.hrsa.gov/governance/public-comment/white-paper-on-manipulating-waitlist-priority (accessed November 17, 2021).
HRSA. 2021a. Advisory Committee on Organ Transplantation. https://www.hrsa.gov/advisory-committees/organ-transplantation (accessed November 16, 2021).
HRSA. 2021b. Summary of Advisory Committee on Organ Transplantation (ACOT) consensus recommendations to the secretary of Health and Human Services (HHS). https://www.hrsa.gov/advisory-committees/organtransplantation/recommendations (accessed October 1, 2021).
Humar, A. H., S. Ganesh, D. Jorgensen, A. Tevar, A. Ganoza, M. Milinari, and C. Hughes. 2019. Adult living donor versus deceased donor liver transplant (LDLT versus DDLT) at a single center—Time to change our paradigm for liver transplant. Annals of Surgery 270(3):444-451.
IOM (Institute of Medicine). 2000. To err is human: Building a safer health system. Washington, DC: National Academy Press.
Israni, A. K., D. Zaun, J. D. Rosendale, C. Schaffhausen, W. McKinney, and J. J. Snyder. 2021. OPTN/SRTR 2019 annual data report: Deceased organ donors. American Journal of Transplantation 21(S2):567-604.
Karp, S. J., G. Segal, and D. J. Patil. 2021. Using data to achieve organ procurement organization accountability—reply. JAMA Surgery 156(1):99-100.
Kaufman, C. L., N. Bhutiani, A. Ramirez, H. Y. Tien, M. D. Palazzo, E. Galvis, S. Farner, T. Ozyurekoglu, and C. M. Jones. 2019. Current status of vascularized composite allotransplantation. The American Surgeon 85(6):631-637. https://doi.org/10.1177/000313481908500628.
Kazley, A. S., E. Johnson, L. Holland-Carter, S. Mauer, J. Correll, N. Marlow, K. Chavin, and P. Baliga. 2019. The non-directed living kidney donor: Why donate to strangers? Journal of Renal Care 45(2):102-110.
King, K. L., S. A. Husain, J. D. Schold, R. E. Patzer, P. P. Reese, Z. Jin, L. E. Ratner, D. J. Cohen, S. O. Pastan, and S. Mohan. 2020. Major variation across local transplant centers in probability of kidney transplant for wait-listed patients. Journal of the American Society of Nephrology 31(12):2900-2911.
Laureys, S. 2005. Death, unconsciousness and the brain. Nature Reviews Neuroscience 6:899-909. https://doi.org/10.1038/nrn1789.
Levy, G. A., N. Selzner, and D. R. Grant. 2016. Fostering living donor liver transplantation. Current Opinion in Organ Transplantation 21:224-230.
Massie, A. B., X. Luo, E. K. Chow, J. L. Alejo, N. M. Desai, and D. L. Segev. 2014. Survival benefit of primary deceased donor transplantation with high-KDPI kidneys. American Journal of Transplantation 14(10):2310-2316.
Mathur, A. K., Z. A. Stewart-Lewis, P. H. Warren, M. C. Walters, K. A. Gifford, J. Xing, N. P. Goodrich, R. Bennett, A. Brownson, J. Ellefson, G. Felan, G. Barrett, R. E. Hays, C. Klein-Glover, S. Lagreco, N. Metzler, K. Provencher, E. Walz, K. Warmke, R. M. Merion, and A. O. Ojo. 2020. Best practices to optimize utilization of the National Living Donor Assistance Center for the financial assistance of living organ donors. American Journal of Transplantation 20:25-33.
Neumann, P. J., G. D. Sanders, L. B. Russell, J. E. Siegel, and T. G. Ganiats, eds. 2016. Cost-effectiveness in health and medicine. Oxford University Press.
Northup, P. G., M. M. Abecassis, M. J. Englesbe, J. C. Emond, V. D. Lee, G. J. Stukenborg, L. Tong, C. L. Berg, and Adult-to-Adult Living Donor Liver Transplantation Cohort Study Group. 2009. Addition of adult-to-adult living donation to liver transplant programs improves survival but at an increased cost. Liver Transplantation 15(2):148-162.
OPTN (Organ Procurement and Transplantation Network). 2019. Ethical implications of multi-organ transplants. https://optn.transplant.hrsa.gov/media/2989/ethics_boardreport_201906.pdf (accessed November 18, 2021).
OPTN. 2022. All-time records again set in 2021 for organ transplants, organ donation from deceased donors. https://optn.transplant.hrsa.gov/news/all-time-records-again-set-in-2021-for-organ-transplants-organ-donation-from-deceased-donors (accessed January 26, 2022).
Pena, A. 2016. Wanted: Living organ donor. Transplantation 100(11):2239-2243.
President’s Commission for the Study of Ethical Problems in Medicine and Biomedical and Behavioral Research. 1981. Defining death: A report on the medical, legal and ethical issues in the determination of death. Washington, DC: U.S. Government Printing Office.
Rand, L. Z., and A. S. Kesselheim. 2021. Controversy over using quality-adjusted life-years in cost-effectiveness analyses: A systematic literature review: Systematic literature review examines the controversy over the use of quality-adjusted life-year in cost-effectiveness analyses. Health Affairs 40(9):1402-1410.
Rasmussen, S., J. Uriart, N. Anderson, B. Doby, A. Ferzola, H. Sung, C. Cooney, G. Brandacher, E. Gordon, D. Segev, and M. Hendersen. 2020. Public education materials about vascular composite allotransplantation and donation in the United States: Current scope and limitations. Clinical Transplantation 34(11). https://doi.org/10.1111/ctr.14066.
Report of the Ad Hoc Committee of the Harvard Medical School to Examine the Definition of Brain Death. A definition of irreversible coma. 1968. JAMA. 205(6):337-340. https://doi.org/10.1001/jama.1968.03140320031009.
Rodrigue, J., D. Tomich, A. Flieshman, and A. Glazier. 2017. Vascularized composite allograft donation and transplantation: A survey of public attitudes in the United States. American Journal of Transplantation 17:2687-2695.
Sarasin, F. P., P. E. Majno, J. M. Llovet, J. Bruix, G. Mentha, and A. Hadengue. 2001. Living donor liver transplantation for early hepatocellular carcinoma: A life-expectancy and cost-effectiveness perspective. Hepatology 33(5):1073-1079.
Schnitzler, M., M. Skeans, A. Israni, and M. Valapour. 2014. Incremental cost-effectiveness of lung transplant by lung allocation score: Abstract 1386. Transplantation 98:192.
Schnitzler, M. A., M. A. Skeans, D. A. Axelrod, K. L. Lentine, J. E. Tuttle-Newhall, J. J. Snyder, A. K. Israni, and B. L. Kasiske. 2015. OPTN/SRTR 2013 annual data report: Economics. American Journal of Transplantation 15(S2):1-24.
Shafer, T. J., D. Wagner, J. Chessare, F. A. Zampiello, V. McBride, and J. Perdue. 2006. Organ donation breakthrough collaborative: Increasing organ donation through system redesign. Critical Care Nurse 26(2):33-48.
SRTR (Scientific Registry of Transplant Recipients). 2022. Mission, vision, and values. https://www.srtr.org/about-srtr/mission-vision-and-values (accessed February 1, 2022).
Tilney, N. L. 2003. In transplant: From myth to reality. New Haven, CT: Yale University Press. Pp. 199-216.
UNOS (United Network for Organ Sharing). 2020. HOPE Act impact continues at five-year milestone. https://unos.org/news/in-focus/hope-act-impact-continues-at-five-year-milestone (accessed November 16, 2021).
UNOS. 2021. Living donation. https://unos.org/transplat/living-donation (accessed March 14, 2021).
Vega, R. J., and K. W. Kizer. 2020. VHA’s innovation ecosystem: Operationalizing innovation in health care. NEJM Catalyst 1(6). https://doi.org/10.1056/CAT.20.0263.
Whiting, J. F., R. S. Woodward, E. Y. Zavala, D. S. Cohen, J. E. Martin, G. G. Singer, J. A. Lowell, M. R. First, D. C. Brennan, and M. A. Schnitzler. 2000. Economic cost of expanded criteria donors in cadaveric renal transplantation: Analysis of Medicare payments. Transplantation 70(5):755-760.
Wolfe, R. A., V. B. Ashby, E. L. Milford, A. O. Ojo, R. E. Ettenger, L. Y. C. Agodoa, P. J. Held, and F. K. Port. 1999. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. New England Journal of Medicine 341(23):1725-1730.
Wolfe, R. A., K. P. McCullough, and A. B. Leichtman. 2009. Predictability of survival models for waiting list and transplant patients: Calculating LYFT. American Journal of Transplantation 9(7):1523-1527.
This page intentionally left blank.


























