
4
Confronting and Eliminating Inequities in the Organ Transplantation System
The preceding chapter established that a trustworthy organ transplantation system must adhere to ethical principles and have transparent processes and results. The committee concluded that the principle of justice is central for the system’s success, and that one essential measure of justice is the equity1 of the system’s processes and patient outcomes. This chapter presents evidence that factors such as patients’ race, ethnicity, socioeconomic circumstances, and similar attributes do affect the way patients are treated at multiple points along the transplantation journey, from referral for evaluation at a transplant center to the speed with which a transplant occurs. Not surprisingly, the differences in the way that various patient populations are treated result in marked disparities2 in the outcomes they experience, ranging from longer, better lives for some and early deaths for others. Further, existing data-gathering practices leave gaps concerning processes and outcomes for other groups, such as women, the elderly, and people with disabilities or hereditary disorders. Additionally, there are major gaps in our knowledge about those with failing organs who never enter the transplant pathway in the first place, but who would otherwise be eligible or interested in receiving a transplant. These gaps in data, along with the complex way diverse factors—socioeconomic, racial and ethnic, federal and state policies, various features of health systems, and individual-level characteristics—interact makes it difficult to describe the true scope of the disparities in transplantation. Nonetheless, the existence of such disparities is undeniable.
___________________
1 Health equity is the “attainment of the highest level of health for all people. Achieving health equity requires valuing everyone equally with focused and ongoing societal efforts to address avoidable inequalities, historical and contemporary injustices, and the elimination of health and health care disparities” (HHS, 2021b).
2 As discussed in Chapter 1, the committee adopted the following definition for health disparities in the context of this report: “a particular type of health difference that is closely linked with social, economic, and/or environmental disadvantage. Health disparities adversely affect groups of people who have systematically experienced greater obstacles to health based on their racial or ethnic group; religion; socioeconomic status; gender; age; mental health; cognitive, sensory, or physical disability; sexual orientation or gender identity; geographic location; or other characteristics historically linked to discrimination or exclusion” (HHS, 2021a).
Structural problems in society, including injustices in the provision and financing of health care, lie behind the disparities associated with chronic disease care and the health care system more broadly; these also affect processes and outcomes in organ transplantation. However, some of the causes for disparities are specific to the current system of organ transplantation, which are discussed further in this chapter. Organizations working on organ transplantation have multiple aims, such as increasing the number and quality of deceased donor organs and advancing scientific knowledge about, and techniques to prevent, the rejection of organs by transplant recipients’ immune system. These aims affect organizations’ interactions with transplant candidates, health care providers and researchers, and the public and its elected representatives. When equity is not one of the key aims, instances of inequitable treatment are less likely to be noticed, much less to become a focus for the organization’s efforts to improve the system. For example, the object of principal concern for the Organ Procurement and Transplantation Network (OPTN) has been individuals who are on the waiting lists for each type of organ—that is, patients who have been referred to and evaluated and accepted by a transplant center—rather than all patients diagnosed with organ failure. Although more data are needed concerning patients who are not referred for evaluation, enough is known to conclude that members of groups that experience subordination and exclusion in many aspects of their lives are more heavily represented among patients diagnosed with organ failure than on transplant waiting lists. Further study is needed to understand how and why such disparities occur, but the evidence examined in this chapter makes clear the harmful effects of the disparities in terms of the greater likelihood for some populations of not being listed for a needed transplant and of dying prematurely.
The transplantation system’s commitment to justice does not mean that the principle of justice always takes priority over all other objectives. As Chapter 3 explained, the various values being sought—not only justice but also respect for the choices of organ donors and recipients, minimizing harm, and maximizing benefits, especially for the least well off—can sometimes pull in different directions. This tension is explored further in Chapter 5 in the assessment of alternative allocation policies. A just organ transplantation system could resolve this conflict between maximizing utility and acting fairly by adopting one policy or the other or some combination of the two. In contrast, when the transplantation system produces glaringly worse results for certain groups of patients—especially those defined by perceived race, ethnicity, sex, religion, socioeconomic status, disability status, geographic location of residence, or the like—a just system would seek the roots of such inequities and take whatever steps are needed to remove them because the benefits experienced by historically favored groups do not justify the imposition of harm on the victims of transplant disparities.
The Statement of Task for the study, found in Box 1-2, has specific charges to the committee for considering equity and fairness throughout the procurement, allocation, and distribution processes. Specifically, the committee was asked to consider whether measures could be taken to reduce inequities in organ allocation affecting socioeconomically disadvantaged populations. This chapter details what is currently known about inequities in access to organ transplants in the United States as well as related aspects including referral to specialists, access to the transplant waiting list, and posttransplant outcomes, and it proposes a recommendation for addressing root causes of inequities in the transplantation system. Other issues examined in this chapter include structural challenges and data gaps that contribute to health inequities in the organ transplantation system in the United States.
PRIORITIZING HEALTH EQUITY IN THE TRANSPLANTATION SYSTEM—WHY IS THIS IMPORTANT?
The National Organ Transplant Act of 1984 created the Task Force on Organ Transplantation charged with, among other duties, providing recommendations for ensuring equitable
access to and allocation of donated organs. Ensuring equity in transplantation requires recognizing inequities that persist across the transplantation system. Removing inequities is vital for creating a system that ensures that all people who need care achieve their best possible health outcomes. Addressing disparities within the system is also vital for building a trustworthy and transparent system (discussed further in Chapter 3). For too long, acknowledgments of individual-level health disparities have taken priority over attention to structural and systemic solutions to inequities (the definitions used by the committee throughout this report can be found in Box 1-3). By not addressing the structures that perpetuate inequities, the system has not adapted to care for patients who may experience more barriers to receiving an organ transplant.
As the focus on promoting health care and social equity in the larger national discussion increases, it is important that the transplantation community commit to working toward equity in both stated policies and practices. Recent years have seen more attention directed toward issues of equity in organ transplantation. For example, the OPTN’s strategic plan for 2018–2021 again included providing equity in access to transplant as a strategic goal, and the 2021–2024 strategic plan includes the same goal with a specific initiative focused on identifying and addressing ethnic, socioeconomic status, and geographic disparities.3 Some professional groups in the transplant community have also more recently included equity as strategic initiatives or explicit goals, though this is not consistent across the community. When equity is not one of the key aims, instances of inequitable treatment may not be noticed, much less become a focus for the organization’s efforts to improve the system. While equity has been a long-standing goal of the transplantation system as a whole, stated goals and intentions have not always matched the actions of the stakeholders within the system and translated into change for communities who have been disadvantaged by policies and practices (including racial and ethnic minorities, individuals with disabilities, and the poor). As a result, achieving equity has not been realized.
Current practices of the organ transplantation system lie downstream from earlier, and often times compounding issues, in the health care system (e.g., unequal access to primary care physicians, chronic disease inequities, uneven referral to specialists). However, stakeholders within the organ transplantation system can take many actions to improve equity, including increasing access to the waiting list. Dialysis providers and others caring for patients with end-stage organ failure can establish more systematic referral pathways to transplant centers. Transplant centers can improve their inclusiveness and approaches to the evaluation and listing of referred patients. Organ procurement organizations (OPOs) can promote training and efforts to better meet the needs of minority donor families. Stakeholders within the system need to be held accountable for working to eliminate inequities in organ transplantation, and should be incentivized to do so. The system should also be nimble enough to move quickly in identifying and mitigating unintended consequences that may arise as new policies are implemented. The committee’s conclusions and recommendation that follow describe the current state of inequities in transplantation and identify actions that should be taken as the organ transplantation system works to eliminate inequities.
Conclusion 4-1: Although equity in access and allocation has been a proclaimed principle of the organ transplantation system for decades, and appears in federal regulations directing allocation policy, equity has, until recently, been absent as a stated goal or vision in the strategic plans of many organizations working in organ transplantation. While the stated priorities and plans of organizations involved in
___________________
3 For information on the OPTN Strategic Plan (2021–2024) see https://optn.transplant.hrsa.gov/media/2546/optn_unos_strategic_plan.pdf (accessed January 26, 2022).
the transplantation system may now include equity, current policies and practices do not always reflect this commitment to equity.
STRIVING FOR HEALTH EQUITY AND FAIRNESS IN ORGAN TRANSPLANTATION
“As a medical and scientific community, it is time for our actions to move beyond describing and acknowledging inequities. Rather, we must commit to enacting solutions that rectify inequity through multidimensional approaches that address fundamental causes.”
—Boulware and Mohottige, 2021, p. 816
Presented by Kimberly Jacob Arriola, Emory University, testimony to the committee during February 5, 2021 public workshop
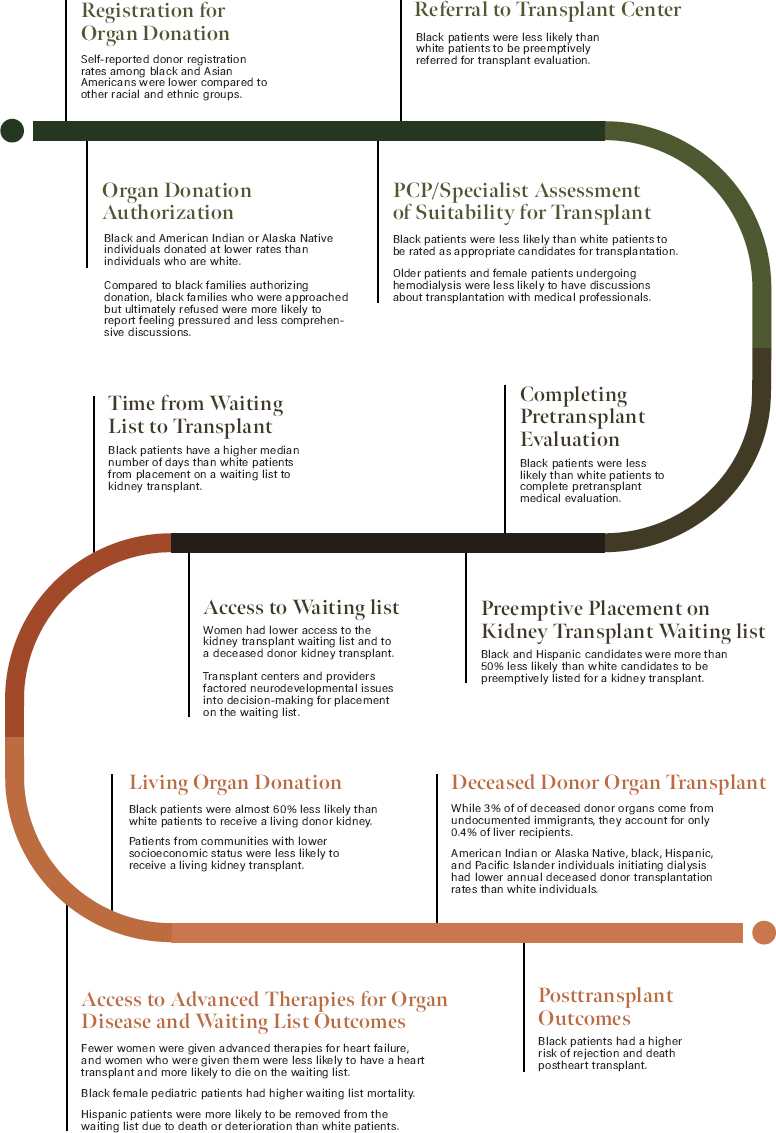
It is well documented that various populations in the United States experience health disparities at specific steps along the pathway to an organ transplant. Table 4-1 and Figure 4-1 provide a sampling of data on health disparities in the context of organ donation and transplantation and the groups that are advantaged and disadvantaged as a result. The committee wanted to highlight these areas of health disparities at various points in the organ donation and transplantation pathway. The committee’s overall goal was to use a broader lens and bring attention to structural causes of inequities that drive these disparities in the transplantation system and propose solutions to further health equity.
Conclusion 4-2: The current organ transplantation system in the United States is demonstrably inequitable. Certain groups of patients (e.g., racial and ethnic minority populations, lower socioeconomic status, female gender, older patients, individuals with intellectual and developmental disabilities, or inheritable diseases such as cystic fibrosis) receive organ transplants at a disproportionately lower rate and in some cases after longer wait times than other patients with comparable need.
Inequities Among Racial and Ethnic Groups
Flawed assumptions about trends according to race pervade the clinical literature on organ transplantation and undermine efforts to understand and address inequities in access to transplantation (Harding et al., 2021). Moreover, much transplant research, following U.S. government and National Institutes of Health requirements, fails to disaggregate data, and instead uses categorical race descriptors (e.g., black, Latino, Hispanic, Asian, white, Alaska Native, American Indian, nonblack) that conflate the categories of race and ethnicity and preclude meaningful comparisons across and within diverse ethnic groups (see Box 4-1). As highlighted in Table 4-1, much of the existing data on disparities in organ transplantation focus on race and ethnicity in kidney transplantation, mainly between black and white populations.
Limitations of the Literature
While most research has focused on black patients, a major limitation of the extant literature on disparities in transplantation is that relatively little attention has focused on Latinx and Hispanic patients, American Indian patients, Asian, or ethnic groups within European American patients. Another limitation of the literature is that authors do not provide definitions of race or ethnicity and do not disaggregate groups for refined analysis (Boyd et al., 2020; Fontanarosa and Bauchner, 2018); in some cases, this is attributable to small sample sizes.
TABLE 4-1 Data on Health Disparities Related to Steps in the Organ Donation and Transplant Pathway
| Step in the Organ Donation and Transplant Pathway | Organ | Adult vs. Pediatric | Population(s) Affected | Key Outcomes |
|---|---|---|---|---|
| Registration for organ donation | n/a | n/a | Black, Asian American |
|
| Organ donation authorization | n/a | n/a | Black, American Indian/Alaska Native |
|
| Primary care physician/specialist assessment of suitability for transplanta | Kidney | Adult | Black |
|
| Kidney | Adult | Patients over age 65, women |
|
|
| Referral to transplant centera | Kidney | Adult | Black |
|
| Completing pretransplant evaluationa | Kidney | Adult | Black |
|
| Preemptive placement on transplant waiting list | Kidney | Adult | Black, Hispanic |
|
| Step in the Organ Donation and Transplant Pathway | Organ | Adult vs. Pediatric | Population(s) Affected | Key Outcomes |
|---|---|---|---|---|
| Access to the waiting list | Kidney | Adult | Women |
|
| All organs | Pediatric | Individuals with an intellectual disability |
|
|
| Time from waiting list to transplant | Kidney | Adult | Black |
|
| Access to advanced therapies for organ disease and waiting list outcomes | Heart | Adult | Women, black |
|
| Heart | Pediatric | Female, black |
|
|
| Liver | Adult | Hispanic |
|
|
| Living organ donationb | Kidney | Adult | Black |
|
| Kidney | Adult | Lower socioeconomic status (SES), black |
|
|
| Deceased donor organ transplant | Liver | Adult | Undocumented immigrants |
|
| Kidney | Adult | American Indian or Alaska Native, black, Pacific Islander, Hispanic |
|
|
| Kidney | Adult | Lower SES |
|
|
| Heart | Adult | Lower SES (inadequate funds or health insurance) |
|
|
| Liver | Adult | Women |
|
|
| Posttransplant outcomes | Heart | Adult | Black |
|
| Kidney | Pediatric | Uninsured or underinsured |
|
NOTES: The data displayed in this table do not reflect all disparities in the U.S. organ transplantation system but rather a sampling of the scientific literature reviewed by the committee. SES = socioeconomic status; SVI = Social Vulnerability Index; CF-LVAD = continuous flow left ventricular assist device; OPTN = Organ Procurement and Transplantation Network.
a The steps highlighted in this section occur prior to a patient being placed on a transplant waiting list and therefore fall outside of the scope of the OPTN’s data collection. Disparities that occur within these steps affect downstream access to transplantation and are noted here as measures contributing to the overall equity or inequity of the transplantation system.
b Although the Statement of Task for this consensus study is focused on deceased donor organ transplants, the health disparities related to living donation are critical and have an effect on the overall transplantation system and therefore are highlighted above.
c The Centers for Disease Control and Prevention Social Vulnerability Index (SVI) uses U.S. census data to determine which communities may be more vulnerable based on social factors.
NOTE: PCP = primary care physician.
SOURCE: See full list of references in Table 4-1.
The categories Latinx and Hispanic, for example, comprise myriad cultural and ethnic groups that should be compared (e.g., Mexican Latinx share some common cultural patterns but also differ culturally from Cuban Latinx). As a result, categories are analyzed as a homogeneous group of people, despite considerable cultural variation. All groups need to be analyzed, and conceptions of racial and ethnic groups need to be better understood. For example, associated health needs exist within the categorization of racial and ethnic minority populations and studying these groups separately may help illuminate differences in outcomes.
Conclusion 4-3: The absence of U.S. Department of Health and Human Services (HHS) requirements to collect disaggregated data by race and ethnicity, gender/sex, age, and language in organ donation and transplantation research precludes efforts to fully understand inequities in organ transplantation. Data gaps further compound challenges in provider decision making and preclude institutional priority setting for redressing inequities.
Geographic Disparities
In the Statement of Task, the committee was asked to consider whether deceased donor organs should be allocated to specific individuals based on need rather than groups of individuals defined by geography. Geographic disparities in organ transplantation occur for a number of reasons, including variation in OPO procedures, transplant center behavior, the number of potential organ donors and donation rates, and listing criteria. Where a potential organ transplant candidate is listed for a transplant is cited as one of the highest contributing factors associated with unintended disparities in access across multiple organ types including kidney, liver, heart, and lung (UNOS, 2021). Each organ has a specific framework for distribution among potential candidates based on various factors (e.g., medical urgency, blood type), and these policies also take into consideration cold ischemic times for various organs (e.g., heart and lung have shorter times while pancreas and kidney have longer times).4 Because of the role geographic location plays in access to organ transplantation, there have been a number of efforts and actions to address geographic variation in transplant access, which are discussed further in Chapter 5 on equity in allocation. The committee also explores areas for improving procurement, acceptance, and use of deceased donor organs in Chapter 6.
Individuals with Intellectual Disabilities
“So long as the decision making of medical practitioners at the evaluation stage has little to no oversight or guidance applied to it and so long as discriminatory attitudes exist, so too [will] these barriers to transplantation exist.”
— Kelly Israel, Autistic Self Advocacy Network, testimony to the committee during
July 15, 2021 public listening session
Organ transplantation for individuals with intellectual disabilities (IDs) is a controversial issue among some transplant providers, and carries varying degrees of importance in listing decisions based on the type of organ being transplanted and the severity of the disability. Prior to the 1990s, having an ID was considered by many transplant professionals as a contraindication for being listed for an organ transplant. In some cases, such as Down syndrome, there may be concerns related to immunological factors conveying potentially higher risks of infection or congenital heart disease. In other cases, reasons for contraindication include the patient potentially not understanding the procedure and assumption of a patient’s lack of adherence to a strict posttransplant medication regimen required for transplant recipients. Lack of data remains a significant challenge for understanding the full breadth of disparities in access to transplantation for individuals with disabilities.
Legal protections for individuals with disabilities exist within the Americans with Disabilities Act, the Affordable Care Act (ACA), and the Rehabilitation Act. These protections specify that qualified individuals with disabilities cannot be excluded from programs receiving federal funding and that those programs should provide reasonable accommodations for individuals with disabilities.5 However, many individuals with ID still face challenges in referral for evaluation and access to a transplant waiting list. In recent years, a number of
___________________
4Cold ischemic time refers to the time between when an organ is cross-clamped after being removed from the donor and when the organ is warmed with the recipient’s blood.
5 Americans with Disabilities Act of 1990 (42 U.S.C. §12182), Affordable Care Act of 2010 (42 U.S.C. §18116), Rehabilitation Act of 1973 (29 U.S.C. §794).
states have passed laws attempting to ban discrimination in organ transplantation based on an individual’s ID, and other states are considering legislation. Discrimination in the context of individuals with ID is also under consideration for further action at the federal level (HHS, 2021c). Whether these laws and actions will have an effect on access remains to be seen.
Disparities in Provider Referrals and Evaluation
Disparities in provider referral and evaluation contribute to unequal access to a waiting list for individuals with ID, and downstream, to an organ transplant. Dobbels (2014) notes that there is a lack of data on the number of individuals with ID who are found to be ineligible for transplant following an evaluation as well as the number of individuals never referred. A 2004 survey of 205 individuals and family members of those with disabilities found that about one-third of individuals for whom referral was suggested were never evaluated for an organ transplant (National Work Group on Disability and Transplantation, 2004). Provider bias may also play a role in how quality of life is assessed for individuals with ID, and ultimately, how likely they are to receive a referral for transplant or placement on the waiting list following an evaluation. For example, a systematic review by Pelleboer-Gunnink et al. (2017) found that stigmatizing attitudes regarding ID were present among mainstream health professionals.
Surveys of transplant centers and programs indicate that there is wide variability in listing decisions based on psychosocial and cognitive characteristics (Levenson and Olbrisch, 1993; Richards et al., 2009; Secunda et al., 2013; Wall et al., 2020). Because transplant programs can place varying levels of importance on cognitive characteristics and other factors, individuals with ID may experience different levels of disparities from one center to another, and transparency may be lacking for patients. During the committee’s public listening session in July 2021, advocates suggested several paths forward including formalizing rules, providing individualized assessment for patients (rather than policies that consider ID as an absolute or relative contraindication for transplantation), and recognizing that some patients may need additional support in posttransplant care.
Heart, Kidney, and Liver Transplantation and Intellectual Disabilities
Heart transplantation is one area where ID has been—and to some extent remains—controversial for providers in making decisions about listing a patient for transplant. In 2006, the International Society for Heart and Lung Transplantation (ISHLT) guidelines recommended that ID be regarded as a relative contraindication to transplantation (Mehra et al., 2006). The guidelines noted, however, the limited data on the validity of psychosocial evaluation for predicting outcomes and indicated that there may be wide variability in evaluation across centers. ISHLT updated its guidelines in 2016 and recommended that lack of adequate social support to achieve compliance could be considered a relative contraindication to heart transplant, but it recommended against heart transplant for individuals with severe cognitive-behavioral disabilities (Mehra et al., 2016). A survey by Richards et al. (2009) found that pediatric heart transplant programs tended to factor neurodevelopmental issues into the decision-making process for listing to a higher degree than kidney or liver programs with 71 percent of programs indicating that they would “always” or “usually” consider a candidate’s neurodevelopmental status in their decision versus 30 percent and 33 percent for kidney and liver, respectively. Attitudes may be shifting to a small degree; of those programs considering severe ID as an absolute contraindication, 37.2 percent were heart, 44.4 percent were lung, 22.4 percent were liver, and 11.8 percent were kidney transplant programs (Wall et al., 2020). While outcomes data related to heart transplantation for individuals with ID are
very limited, some studies indicate that outcomes for individuals with ID and those without ID may be similar (Samelson-Jones et al., 2012; Wightman et al., 2017).
In contrast to heart transplantation, kidney transplantation occurs more frequently in individuals with ID. This is likely attributable in part to the greater prevalence of kidney transplants in relation to other organ transplants as well as the potential for living donors. Studies have found that outcomes in this population are generally similar to patients without ID (Ohta et al., 2006; Wightman et al., 2014), though some note that long-term survival rates may be lower (Galante et al., 2010).
Data on liver transplantation in individuals with ID are limited. Wightman et al. (2016) found similar short-term graft and patient survival outcomes between pediatric patients with and without ID, but noted the need for research on long-term outcomes. A provider survey on medical and psychosocial characteristics of liver transplant recipients found that 30 percent of respondents had formal institutional policies characterizing cognitive disability as a contraindication to listing (Secunda et al., 2013). Transplant centers varied in how they viewed cognitive disability, with 42.6 percent considering moderate disability not to be a contraindication, 49.2 percent considering it a relative contraindication, and 8.2 percent considering it an absolute contraindication.
Inequitable Access to Transplants for Undocumented Immigrants
Approximately 10.7 million undocumented immigrants live in the United States as of 2016,6 equivalent to about 3 percent of the population (Pew Research Center, 2019). Undocumented immigrants experience disparities in gaining access to deceased donor organ transplantation. While approximately 3 percent of deceased donor organs come from undocumented immigrants, disproportionately fewer undocumented immigrants (0.4 percent) receive organ transplants (Glazier et al., 2014; Lee and Terrault, 2020). Both the National NOTA and the OPTN policy state that medical need alone should determine deceased donor organ allocation and a candidate’s citizenship or residency status in the United States should not be taken into consideration (OPTN, 2021). While undocumented immigrants may be eligible to receive an organ transplant, most states do not have funding mechanisms to support necessary posttransplant care (Ackah et al., 2019). Barriers to equitable access extend well beyond funding mechanisms, raising questions about policy and ethics.
Kidney-Specific Issues
The exact prevalence of undocumented immigrants with end-stage kidney disease (ESKD), or kidney failure, is unknown primarily because data on this population are not collected as part of the U.S. Renal Data System (Rodriguez et al., 2020). A recent estimate indicated that approximately 5,500 to 8,857 undocumented immigrants live with ESKD in the United States (Rodriguez et al., 2020). Undocumented immigrants with ESKD have been living in the United States on average for more than 5 years at the time of their diagnosis, and many continue to work despite their illness (Cervantes et al., 2017). Unlike U.S. citizens, undocumented immigrants with ESKD are not eligible for coverage of scheduled hemodi-
___________________
6 An undocumented immigrant in this context refers to a person who is not a citizen of the United States, but resides in the United States (Yu and Wightman, 2021).
alysis through Medicare and are not eligible for accessing insurance through the ACA.7 However, select state-level governments in the United States provide coverage for scheduled maintenance dialysis through Emergency Medicaid programs (Berger et al., 2020).8 In the states that do not provide this option undocumented immigrants with ESKD must rely on emergency-only hemodialysis when their condition becomes life threatening. Emergency-only hemodialysis results in adverse health outcomes for patients, decreased quality of life, and stress on the health care system and providers (Berger et al., 2020). Recent efforts at a North Texas safety-net hospital to place undocumented immigrants with ESKD on scheduled dialysis resulted in greater survival benefit for the patients and also proved beneficial for the dialysis unit, the emergency department, and the hospital system (Berger et al., 2020).9 Local nonprofit organizations may offer financial and placement assistance for undocumented immigrants requiring dialysis. However, these support structures are sporadic and do not cover the costs associated with kidney transplantation (cost will be discussed further in Chapter 6).
Conclusion 4-4: Coverage of costs for scheduled dialysis for undocumented immigrants with end-stage kidney disease varies by state and results in disparities in the care available to patients. Emergency-only dialysis increases strain on hospital systems, providers, and patients.
DATA CHALLENGES RELATED TO ASSESSING AND ASSURING EQUITY
Assessing and promoting health equity in the organ transplantation system requires access to a wide range of timely and accurate data, including information related to the social determinants of health (Dover and Belon, 2019). Currently, the OPTN database collects the following information about patients on the transplant waiting list:
- Name
- Gender
- Race/ethnicity
- Age
- ABO blood group10
- Patient human leukocyte antigens (HLAs)11
- Patient status codes (for heart and liver)
- Number of previous transplants
- Acceptable donor characteristics12
___________________
7 Hemodialysis is the process of cleaning the blood of individuals whose kidneys are not functioning properly. In the context of ESKD, maintenance dialysis is important for disease management and can cost thousands of dollars out of pocket if insurance coverage is unavailable.
8 Emergency Medicaid provides temporary coverage for emergency treatment for individuals who qualify for Medicaid but are not eligible based on immigration status.
9 Safety-net hospitals provide health care and health services to individuals who are uninsured or are insured through Medicaid.
10 ABO blood group refers to the system by which blood type is categorized based on markers present on the surface of red blood cells (into A, B, O, or AB). The system is used to match the blood type of the donor and the recipient.
11 HLAs are molecules present on most cells in the body that are involved in the body’s immune response. HLA testing occurs prior to an organ transplant to determine whether the donor and recipient tissues match.
12 Acceptable donor characteristics are things like body size and comorbidities.
When a patient is added to the waiting list, the transplant candidate registration form gathers information on the candidate’s primary source of income, highest level of education, and employment status (OPTN, 2020). However, this pool of currently available data is not complete enough to assess the socioeconomic status of transplant candidates as there is a lack of granular information on socioeconomic and patient-centered factors, including measures of annual household income, household size, access to safe housing, job opportunities, health care access, distance to a transplant center, the patient’s social networks, and neighborhood segregation. A noted gap in existing research, the influence of these social determinants of health on disparities in organ transplantation (Wesselman et al., 2021),13 could be used to further explore the effects of waiting list time on subpopulations. Recently, the OPTN Minority Affairs Committee proposed efforts to collect additional socioeconomic information related to disparities in access to kidney transplantation, though this effort is still in progress.14
Gaps in Data Present a Systems Issue
As previously noted, it is difficult to properly assess equitable referral and evaluation for organ transplantation because of a lack of national surveillance data. The U.S. Renal Data System allows for studies of these aspects related to kidney transplants, but such a nationwide data collection system does not exist for other organ transplants such as liver, heart, and lung. The absence of such data creates a systems issue—specifically around referral and admissions data. The system cannot adequately capture information on social determinants of health and may also miss capturing the medical and social needs of patients in the transplantation system. Without these data, patients may get labeled as noncompliant, which can lead to poorer access to transplantation and thereby poorer outcomes. In February 2021, the OPTN announced a feasibility study that would evaluate data collection related to the social determinants of health.15 The feasibility project will look at potentially collecting aggregated third-party data to better understand how social determinants of health affect transplantation.
Gaps in data and the evidence base more broadly make it difficult for providers to make decisions, especially regarding vulnerable populations such as those with intellectual disability. As previously noted, these populations experience uneven access to referral and transplantation. To overcome some of these data gaps within the transplantation system, more patient-reported data are needed. This may include data related to education, perceived discrimination, perceived racism, distrust of the health care system, physical infrastructure and environmental factors, and access to pharmacies. Furthermore, information on the social determinants of health are needed at the time of transplant evaluation as well as follow-up data on transplant and outcomes.
In June 2021, the OPTN developed an equity dashboard with the goal of increasing transparency in access to transplantation.16 The dashboard uses an access to transplant score
___________________
13 According to the Centers for Disease Control and Prevention, the social determinants of health are “conditions in the places where people live, learn, work, and play that affect a wide range of health risks and outcomes” (CDC, 2021).
14 For information on the Minority Affairs Committee proposal see https://optn.transplant.hrsa.gov/media/3811/202006_mac_ses_bp.pdf (accessed November 12, 2021). Public comments on the proposal raised several concerns related to implementation, including patient privacy, potential for data misuse, and the challenges in verifying socioeconomic data.
15 For more information on the OPTN effort to collect data on the social determinants of health see https://unos.org/news/sdoh-data-collection (accessed September 12, 2021).
16 For more information on the OPTN Equity in Access to Transplant dashboard see https://insights.unos.org/equity-in-access (accessed September 9, 2021).
derived from a Cox proportional hazards regression model measuring 15 patient characteristics such as biological (e.g., blood type, calculated panel reactive antibodies), sociocultural (e.g., ethnicity), health insurance type, and environmental (e.g., donor service area where the patient is listed). These factors are derived more broadly from the National Institute on Minority Health and Disparities Research Framework. Together, this total score is meant to convey how likely it is that a candidate on a transplant waiting list will receive a deceased donor heart, lung, kidney, or liver transplant. A major challenge to measuring equity in transplant using data collected by the OPTN—including data presented in the equity dashboard—is the lack of data regarding the referral process and steps prior to initiating evaluation. Another limitation is that the dashboard identifies a patient’s gender as part of the patient characteristics collected; however, it does not separate this information from the patient’s sex. Additionally, the dashboard does not identify where disparities may be occurring along the pathway to a transplant after a patient initiates a transplant evaluation because the OPTN does not have access to data on individuals starting an evaluation up to the point of placement on the waiting list (becoming a “candidate”). Consequently, little is known about where individuals are most likely to fall off the path to completing evaluation, and where disparities in falling off occur. Complicating matters in tracking the evaluation process is that transplant centers vary in the order in which tests are done in the evaluation process. Opportunities to address some of the data challenges will be discussed further in Chapter 6.
Conclusion 4-5: It is well established that inequities arise in access to referrals, evaluation, and the waiting list for organ transplant, yet little is known where along the trajectory in that process disparities are most likely to arise, especially for vulnerable populations. There is a need to expand federal oversight to include the steps involved in identifying patients as needing a transplant before patients are added to the waiting list. Because current OPTN oversight begins only when a patient is added to the waiting list, measures and actions to advance equity throughout the system will be hampered until these earlier steps in the patients’ process of gaining access to transplantation are addressed as part of the transplantation system and a source for evaluating progress in achieving equity.
Implicit Bias
Implicit bias, defined as “an unconscious favoritism toward or prejudice against people of a certain race, gender, or group that influences one’s own actions or perceptions,” has long-standing effects on health accessibility and outcomes (NASEM, 2021, p. 1). Implicit bias spans social and structural determinants of health and is often included in considerations of socioeconomic status, race/ethnicity, gender, and disability, among a host of other factors. The computer-based Implicit Association Test (IAT), first introduced in 1998, has been used to delve into the implicit biases of physicians, documenting racial and ethnic disparities in treatment and quality. The IAT can be a useful tool to help people reflect upon their implicit biases, though studies continue to assess its validity for effectively identifying implicit cognition (Meissner et al., 2019; Schimmack, 2021; Vianello and Bar-Anan, 2021). Though physicians’ explicit (self-reported) attitudes regarding preferential treatment of patients based on race and attitudes regarding stereotypes about the cooperativeness of patients based on race have not been statistically significant, detection of physicians’ implicit biases by the IAT show strong associations with their decisions to provide treatment (Green et al., 2007; Hall et al., 2015). Implicit attitudes may also play a role in organ donation since explicit attitudes regarding altruism toward others are likely to be subject to biases in how the donor feels they
may be perceived (Joshi and Stevens, 2017). The role that implicit bias can play in patient referral will be explored further in the next section.
STRUCTURAL BARRIERS TO EQUITY IN THE PATHWAY TO AN ORGAN TRANSPLANT
Delays in Referral to Specialists
Delays in referrals to specialists for patients with end-stage organ failure are among the many structural barriers to equity in the pathway to an organ transplant (Anees et al., 2018; Prakash et al., 2010; Suarez et al., 2018). Delayed or late referral poses adverse consequences for patients in need of kidney, heart, liver, and lung transplants. Delayed referral is further compounded by disparities in access to primary care, which can create downstream issues in accessing necessary specialist care (Brown et al., 2016; Sabounchi et al., 2018; Tung et al., 2019).
Patient-, provider-, and system-level factors contribute to these disparities. Patient-level factors include a lack of knowledge and awareness of transplantation. In the case of kidney disease, a patient may be unaware of having kidney disease given that symptoms may not appear until advanced stages of disease. Some patients may also maintain negative attitudes and beliefs about transplantation and face socioeconomic and psychosocial challenges that preclude them from being referred or placed on the waiting list (Dageforde et al., 2015; Martin, 2014; Patzer et al., 2012; Schold et al., 2011). Provider-related factors include late referrals, which may be caused by a lack of knowledge about kidney disease and when to refer patients, and lack of bilingual or bicultural providers. In addition, evidence suggests that providers from low-wait-listing dialysis centers are unaware of the disparity in wait-listing black patients in the United States (Kim et al., 2018), and that nephrologists experience challenges building trust with ethnic minorities (Hanson et al., 2016). Similarly, providers from transplant programs may lack awareness of disparities in access to living donor transplantation at their own institution (Gordon et al., 2020). System-level factors include difficulty facilitating communication among providers across the complex health care systems for chronic care patients and the lack of culturally sensitive approaches to delivering patient education (Waterman et al., 2010).
Kidney
Nearly 20 to 50 percent of chronic kidney disease patients start dialysis without a prior clinical exam by a nephrologist (Levin, 2000). A systematic literature review found that for patients with chronic kidney disease, late referral to nephrologists is associated with patient demographics, clinical factors, patient and provider attitudes, and health system characteristics. Patient demographic factors associated with late referral include older age, being a member of an ethnic or racial minority group, having less education, and being uninsured. Clinical factors include the presence of multiple comorbidities and the insensitivity of serum creatinine as a screening tool to identify patients with early-stage renal disease (Levin, 2000).17 One study found that nondiabetic kidney disease and Charlson comorbidity index were significantly associated with late referral;18 the authors recommended that physicians
___________________
17 Serum creatinine is a laboratory measure used to assess kidney functioning. Higher levels of creatinine (a waste product) in the blood indicates impaired kidney functioning.
18Charlson comorbidity index is a method for predicting patient mortality based on a number of comorbid conditions.
pay special attention to patients with nondiabetic kidney disease and those with multiple comorbidities (Navaneethan et al., 2007). Physician and patient attitudes surrounding chronic kidney disease as a silent disease and the need for treatment influence the initiation of dialysis (Ghahramani et al., 2011, 2014; Gordon and Sehgal, 2000; Hanson et al., 2016; Levin, 2000). A study looking at nephrologist perceptions related to referring patients for kidney transplant found that the most commonly stated exclusionary factor was inadequate social support followed by the patient’s limited understanding of the transplant process (Bartolomeo et al., 2019). Health system characteristics that contribute to delayed referral include lack of communication between primary care physicians and nephrologists (Navaneethan et al., 2008), as well as geographic factors (Ghahramani et al., 2014).
Late referral can contribute to increased morbidity, mortality, and resource use, as well as reduced quality of life and missed windows of opportunity for preemptive transplantation (Levin, 2000; Reese et al., 2021a). A systematic review of late referral for chronic kidney disease recommended that primary care physicians and nephrologists engage in comprehensive efforts to educate patients and physicians about the effects of delaying referral (Navaneethan et al., 2008). Patients who are referred to specialist nephrology care later in the course of renal disease when their need for dialysis is imminent tend to have poor outcomes (Levin, 2000), while a study of decline in kidney function before and after nephrology referral confirmed that early detection, specialist referral, and intervention have benefits for kidney and patient survival (Jones et al., 2006). After referral to a nephrologist, patients’ decline of glomerular filtration rate slowed significantly,19 which was also associated with better likelihood of survival. Thus, tools are needed to enhance early identification of renal insufficiency,20 along with interventions to delay progression of renal insufficiency and prepare patients for renal replacement therapy (Levin, 2000).
Preemptive Kidney Transplantation
Obtaining a kidney transplant before initiating maintenance dialysis is referred to as preemptive transplantation, and it confers longer patient survival than transplantation following dialysis initiation. However, disparities arise in preemptive referral to kidney transplantation with black patients having a 37 percent lower chance of being preemptively referred for transplant evaluation than white patients (odds ratio = 0.63 [95% confidence interval: 0.55, 0.71]) (Gander et al., 2018). Similarly, preemptive kidney transplantation occurs at significantly lower rates among patients with less than a high school education and Medicaid beneficiaries (King et al., 2019). Patients who are white, had greater health literacy, and had private health insurance have been shown to have greater access to preemptive transplantation (Grams et al., 2013; Patzer et al., 2013; Purnell and Crews, 2019; Taylor et al., 2016). Factors that affected preemptive transplantation included patient’s cardiovascular disease, social deprivation, and renal units’ characteristics (Kutner et al., 2012; Patzer et al., 2013). An additional challenge in preemptive kidney transplantation are the available data regarding dialysis tolerance among patients from racial and ethnic minorities, which may contribute to delays. A number of studies have shown that racial and ethnic minority dialysis patients have greater survival (Eisenstein et al., 2009; Rhee et al., 2014), though others note that there
___________________
19 Glomerular filtration rate, or GFR, is a measurement of how well the kidneys filter blood. It is used to estimate how well the kidneys are functioning with lower rates indicating reduced functioning.
20 Renal insufficiency refers to poor functioning of the kidneys; over time, this may result in the need for dialysis or transplant.
may be other contributing factors to survival advantage, such as age, that should be further studied to inform provider decision making (Johns et al., 2014; Kucirka et al., 2011).
Policy changes to the U.S. kidney allocation system have not addressed preemptive transplantation in an effort to mitigate disparities, thereby enabling such disparities to persist (Reese et al., 2021b). Researchers have suggested strategies to remediate disparities including (1) educating primary care physicians to refer patients before they reach an estimated glomerular flow rate (eGFR) of 20 or less; (2) incentivizing transplant centers to add potential candidates to the waiting list quickly; (3) implementing kidney allocation system changes (e.g., standardizing the GFR estimation to foster fairness through the use of a single standard to all patients); and (4) educating patients regarding preemptive transplantation and offering patient navigators (Reese et al., 2021b).
Heart
A qualitative study of health care providers evaluated the association of gender and race with allocation of advanced heart failure therapies using clinical vignettes. The study found evidence of bias linked to gender and race in clinicians’ decision-making process for offering advanced therapies—which was particularly evident in the case of black female patients, who tended to be judged more harshly in terms of appearance and adequacy of social support—although no association between gender and race was found in the final recommendation for allocation. However, the authors concluded that this bias could contribute to delayed allocation (Breathett et al., 2020). As one minority clinician, when presented with a patient vignette of a black female patient, observed:
It’s a shame that this lady was only diagnosed 2 years ago. I mean I get angry about that. I mean particularly being a [minority] provider, I see that many patients that are referred to me regardless of their race tend to be referred late from a heart failure standpoint. I find that my minority patients, particularly my African American patients, are referred even later.…Many times it’s because their symptoms were going unrecognized by the people that were taking care of them…or their symptoms weren’t believed.…They tell me many stories, and I’m hoping that this isn’t the case for her but unfortunately if you see it enough times…it starts to dishearten you (Breathett et al., 2020, p. 7).
Delays in seeking treatment among heart failure patients (i.e., not recognizing symptoms or seeking care late into symptom onset) can compound delays in referrals to specialists, and delays in seeking treatment have been found to be significantly high (Evangelista et al., 2000). These effects could potentially be mitigated by the promotion of early symptom recognition and management among patients and families.
Liver
Similar disparities in timely referrals have been observed among patients who need liver transplantation evaluation. Late referral to liver specialists has been identified as a major factor contributing to disproportionately low rates of liver transplantation among black individuals, despite the higher prevalence of end-stage liver disease among this racial group compared to others (Mustian et al., 2019). The same study found that black patients tend to be referred for evaluation for a transplant with more advanced disease, as evidenced by their higher median Model for End-Stage Liver Disease (MELD) score at listing. A study evaluating disparities in transplant referral patterns for alcohol-related liver disease found that gastroenterologists and transplant hepatologists were significantly more
likely to refer higher-risk patients than primary care physicians (Loy et al., 2020). This suggests that there is a disparity in the referral of patients with alcohol-related liver disease based on whether the patient has access to specialty care. A retrospective evaluation of the OPTN registrants examined ethnicity and insurance-specific disparities in MELD scores at the time of waiting list registration. They found that among black patients, higher MELD scores at listing did not translate to higher waiting list mortality. However, patients with Medicare, Medicaid, or who were uninsured had significantly higher waiting list mortality than privately insured patients (Robinson et al., 2021).
Patient Evaluation and Access to a Transplant Waiting List
Racial and ethnic groups are disproportionately less likely to be referred for transplant evaluation and to complete transplant evaluation to be placed on the transplant waiting list as compared to non-Hispanic whites (Epstein et al., 2000; Harding et al., 2017; Mucsi et al., 2017; Patzer et al., 2012; Weng et al., 2005; Wolfe et al., 1999). Specifically, black and Hispanic patients have a significantly longer time from starting dialysis to being placed on the waiting list than whites. However, effects remained only partially significant after controlling for socioeconomic status factors (i.e., Medicare insurance among patients over age 64 and zip code poverty levels) (Joshi et al., 2013). Disparities for black patients in access to the waiting list also persisted after controlling for social determinants of health (i.e., knowledge of transplantation, psychosocial factors, and cultural factors) (Ng et al., 2020). Moreover, black patients in poor neighborhoods are significantly less likely to be put on the waiting list than whites in nonpoor neighborhoods indicating that neighborhood racial composition and neighborhood poverty were related to racial disparities in access to the waiting list for black patients (Peng et al., 2018).
Conclusion 4-6: Based on available information, the committee does not find justifiable reasons for the demonstrable disparities between organ transplant rates for persons who would benefit from organ transplants and the burden of disease in many populations. Disproportionately fewer racial and ethnic minority patients receive organ transplants than are represented on the transplant waiting list. These inequities undermine the trust necessary for the organ transplantation system to function optimally.
IMPROVING QUALITY AND HEALTH EQUITY ACROSS THE ENTIRE ORGAN TRANSPLANTATION SYSTEM
Explanation of the Proposed Framework
The committee looked at previous work on health equity as they sought to propose a framework that infuses equity, value, and transparency throughout the organ transplantation system and the points along the care pathway (Figure 4-2). The principle of health equity as a component of quality in a health care system was central. One source, Crossing the Quality Chasm: A New Health System for the 21st Century, described urgent changes needed in the U.S. health care delivery system to improve care for all Americans. The report established six aims for improving key dimensions in the health care system: safety, effectiveness, patient centeredness, timeliness, efficiency, and equity (IOM, 2001a). Further, the report called upon all health care constituencies to adopt these shared aims with the goal of improving the quality of care within the overall health system.
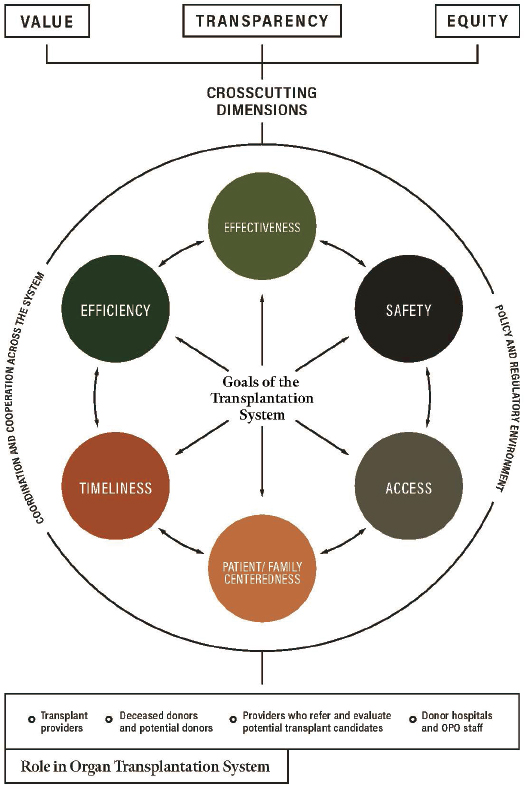
SOURCE: Adapted from IOM, 2010.
Equity as a crosscutting component of system performance and quality health care was further defined in Envisioning the National Health Care Quality Report (IOM, 2001b). The report described a two-dimensional conceptual framework in which the first dimension captures components related to quality (safety, effectiveness, patient centeredness, and timeliness) and the second dimension captures the consumer perspective on patient needs (staying healthy, improving health, living with illness or disability, coping with the end of life). Within the framework, measures of equity are meant to fit in the cells corresponding to the quality component and health care need being addressed. The Future Directions for the National Healthcare Quality and Disparities Reports built on the reports Envisioning the National Health Care Quality Report and Crossing the Quality Chasm to include access and efficiency as quality care components in its conceptual framework for categorizing health care quality and disparities (IOM, 2010). The framework also included care coordination and health systems infrastructure as foundational components supporting the performance
measurement of the other quality components. An additional dimension was included to show the crosscutting nature of equity and value, achievable with improvements in both the quality components and foundational components.
The goal of the committee in building upon prior frameworks and developing Figure 4-2 was not to be prescriptive to the stakeholders within the organ transplantation system but rather to provide a framing for how stakeholders can discuss equity. The committee added a crosscutting dimension of transparency to highlight how the quality components can increase the overall transparency of the system in addition to equity and value. The framework may serve as a heuristic tool or decision aid to help shape future policies by promoting better access to granular data. To that end, the committee considered this framework in developing recommendations, including the dashboard of metrics (see Chapter 7). In the framework, equity is not meant to be a single activity or value; it is foundational. Given the complexity of the organ transplantation system, a framework may also serve as a means of bringing more awareness around the interconnected nature of the system to the various components and stakeholders. All stakeholders within the organ transplantation system are responsible for, and accountable to, ensuring the system is equitable.
EVIDENCE-BASED INTERVENTIONS FOR IMPROVING HEALTH EQUITY IN THE ORGAN TRANSPLANTATION SYSTEM
A number of evidence-based interventions have been developed to reduce disparities and increase access to kidney transplantation, improve organ donation rates, and increase access to living donor kidney transplantation. These interventions include the use of patient navigators as well as a range of culturally targeted educational interventions delivered online, through mass media, or in person at transplant centers, patients’ homes, or community-based venues. The appropriateness of culturally targeted efforts in organ donation authorization has been a subject of much research. As previously discussed, despite improvements in organ donation authorization rates among black and Asian individuals, some challenges remain. For example, data suggest that black families may not be approached regarding organ donation requests in the same manner (or as frequently) as white families and may not view those interactions as favorably (Siminoff et al., 2003). Data from a study by Bodenheimer et al. (2012) looking at organ donation authorization in liver transplantation suggest that racial concordance between the donor and the coordinator may play a role in authorization rates and the authors highlighted the importance of adequate coordinator training to overcome barriers, though they also suggest more study is needed.
Patient Navigators
The effect of patient navigators on reducing racial disparities in access to transplantation has been inconclusive. Patient navigators helped patients complete transplant candidate steps to be placed on the waiting list, as well as helping patients gain greater access to living donor kidney transplantation (LDKT) (Marlow et al., 2016; Sullivan et al., 2012). However, navigators did not affect the completion of transplant evaluation and did help patients to get on the waiting list, but not until after the first 500 days after starting evaluation for transplant (Basu et al., 2018).
Culturally Targeted Interventions
Project ACTS: About Choices in Transplantation and Sharing is a culturally sensitive, family-focused intervention designed to improve readiness for organ and tissue donation
among African American adults, particularly in the southeastern United States. A study evaluated the effectiveness of Project ACTS and found that the intervention was an effective tool for encouraging family discussion of deceased donation intentions among African Americans (Arriola et al., 2010). The authors concluded that OPOs, civic organizations, churches, and public health departments can use this intervention to improve organ donation intention rates among target populations. Furthermore, they concluded that intervention material could be adapted to suit the cultural needs of other populations.
A culturally tailored and linguistically congruent Hispanic Kidney Transplant Program (HKTP) at Northwestern Medicine was implemented at two other transplant programs designed to increase living donor kidney transplantation among Hispanic and Latinx patients. The HKTP comprises 16 components that redress disparities at the patient, provider, and organizational levels (Gordon et al., 2018). Through a hybrid type 2 clinical trial design, the study evaluated both the effectiveness of the HKTP intervention and the effectiveness of the intervention implementation (Gordon et al., 2021). The study found that the HKTP intervention effectively increased LDKT in Hispanic patients, compared to whites, at one intervention site that implemented the intervention with greater fidelity, in comparison to pre- and postassessments at two matched control sites. Intervention site 1 improved the Hispanic LDKT rate by 47 percent (from 20.3 percent at pre-HKTP to 29.8 percent at post-HKTP).
A study evaluated the effectiveness of interventions designed to remove barriers to living donor kidney transplantation for black patients, who receive this type of transplantation less frequently than patients of other racial groups (Rodrigue et al., 2014). Patients were randomized to one of the following three groups, in which health educators delivered interventions to (1) patients and their guests in the patient’s home, (2) clusters of patients and guests in transplant centers, or (3) individual patients alone in transplant centers. The study found that patients who received house calls were more likely than those who had visits at transplant centers to have at least one donor inquiry and evaluation. Patients who received house calls had greater knowledge, fewer concerns, and greater willingness to talk about living donation 6 weeks after the intervention. The authors emphasized the importance of including the patient’s social network in live donor kidney transplantation education to reduce racial disparities in live donor transplantation rates.
A mobile, customized patient education tool was developed to provide animated patient education and show individualized risk-adjusted outcomes for kidney transplant candidates following transplant. A study examined the effectiveness of this mobile, iOS-based application among a diverse group of renal transplant candidates (Axelrod et al., 2017). Most participants reported that the tool improved their knowledge and was culturally appropriate to their own race or ethnicity. Furthermore, patients scored higher on a transplant knowledge test after using the application—regardless of their health literacy level—and expressed more interest in living and deceased donor kidney transplantation.
A randomized controlled trial was conducted to test the effectiveness of a bilingual website about living kidney donation and transplantation that was culturally targeted for Hispanics and Latinos, who are disproportionately affected by kidney disease and receive disproportionately fewer LDKTs than whites (Gordon et al., 2016a,b). Compared to participants who only received routine transplant education sessions, those who were also exposed to the website had greater increases in their knowledge scores that persisted at a 3-week follow-up. These results underscore the potential benefit of supplementing transplant education using culturally tailored educational tools.
In 2010, a Spanish language mass media campaign on living organ donation attitudes and behavioral interventions was conducted among Hispanics in the southwestern United
States using an intervention community and a control community (Alvaro et al., 2010). This evaluation revealed a posttest increase in intentions related to living organ donation in the intervention group that was not observed in the control group. Moreover, those in the intervention community who were exposed to the campaign had more positive donation intentions than individuals in the same community who were not exposed to the campaign.
A religiously tailored and ethically balanced educational intervention was designed to increase living organ donation intent among Muslim Americans (Padela et al., 2020). An evaluation of this intervention found that participants in the educational intervention were more likely to donate a kidney; they were also more likely to encourage a loved one, coworker, or fellow mosque member with end-stage kidney disease to seek a living kidney donor.
Improving Implementation of Evidence-Based Interventions
Despite the availability and effectiveness of evidence-based interventions aimed at increasing organ transplantation equity, these approaches have not been widely adopted within the organ transplantation system. For example, OPOs are responsible for discussing organ donation with a potential donor’s next of kin. However, despite the importance of high-quality, positive interactions between OPO staff and the family members of a potential donor, there are no national standards for how to train OPO staff on communication skills in compassion and cultural sensitivity. One study across eight geographically distinct areas of the United States found meaningful variations in the way OPO staff communicated with family decision makers about organ donation, suggesting that “OPO staff were missing opportunities to increase the supply of available deceased donor organs…and equalize some of the regional variations in donation, conversion, and transplantation rates” (Traino et al., 2017, p. 7).
Implementation research shows that evidence-based interventions often take years to be adopted into practice; furthermore, these gaps in translation of interventions are not well understood, which can impede investment decisions for those attempting to implement interventions (Morris et al., 2011). Implementation science, which examines methods for promoting the adoption of evidence-based policies and practices in health care and public health, reveals that many factors influence the uptake of evidence-based interventions into practice. These factors pertain to the institution or organization in which an intervention is implemented, the nature of the intervention itself, and the attitudes about the intervention held by the stakeholders involved in implementing the intervention (Damschroder et al., 2009). In the context of implementing an intervention to increase Hispanics’ access to transplantation and LDKT, barriers emerged including awareness of the disparity, concerns about focusing on reducing disparities for one minority group and not others in need, misperceptions about patients’ payer mix, and the lack of patient disaggregated data by racial and ethnic background (Gordon et al., 2020). There is a need for more implementation science research, and implementation scientists need to be part of the effort to adopt effective interventions in the transplantation system.
Conclusion 4-7: Evidence-based interventions have been developed to reduce disparities and increase access to transplantation. Nonetheless, such interventions are rarely implemented into practice. Despite the availability of these interventions, dialysis centers, donor hospitals, transplant centers, OPOs, and others have not implemented the interventions to help resolve inequities in access to transplant referral, evaluation, and care.
- HHS should require and support work with OPOs to increase the diversity of their workforce to better meet the needs of donor families.
REFERENCES
Ackah, R. L., R. R. Sigireddi, and B. V. R. Murthy. 2019. Is organ retransplantation among undocumented immigrants in the United States just? AMA Journal of Ethics 21(1):E17-E25.
Ahearn, P., K. L. Johansen, J. C. Tan, C. E. McCulloch, B. A. Grimes, and E. Ku. 2021. Sex disparity in deceased-donor kidney transplant access by cause of kidney disease. Clinical Journal of the American Society of Nephrology 16(2):241-250.
Alvaro, E. M., J. T. Siegel, W. D. Crano, and A. Dominick. 2010. A mass mediated intervention on Hispanic live kidney donation. Journal of Health Communication 15(4):374-387.
Anees, M., Y. Hussain, M. Ibrahim, I. Ilahi, S. Ahmad, K. I. Asif, and A. Jameel. 2018. Outcome of chronic kidney disease patients on the basis of referral to nephrologist: A one-year follow-up study. Journal of the College of Physicians and Surgeons of Pakistan 27(4):304-307.
Arriola, K., D. H. Robinson, N. J. Thompson, and J. P. Perryman. 2010. Project ACTS: An intervention to increase organ and tissue donation intentions among African Americans. Health Education & Behavior 37(2):264-274.
Axelrod, D. A., N. Dzebisashvili, M. A. Schnitzler, P. R. Salvalaggio, D. L. Segev, S. E. Gentry, J. Tuttle-Newhall, and K. L. Lentine. 2010. The interplay of socioeconomic status, distance to center, and interdonor service area travel on kidney transplant access and outcomes. Clinical Journal of the American Society of Nephrology 5(12):2276-2288.
Axelrod, D. A., C. S. Kynard-Amerson, D. Wojciechowski, M. Jacobs, K. L. Lentine, M. Schnitzler, J. D. Peipert, and A. D. Waterman. 2017. Cultural competency of a mobile, customized patient education tool for improving potential kidney transplant recipients’ knowledge and decision-making. Clinical Transplantation 31(5). https://doi.org/10.1111/ctr.12944.
Bartolomeo, K., A. Tandon Gandhir, M. Lipinski, J. Romeu, and N. Ghahramani. 2019. Factors considered by nephrologists in excluding patients from kidney transplant referral. International Journal of Organ Transplantation Medicine 10(3):101-107.
Basu, M., L. Petgrave-Nelson, K. D. Smith, J. P. Perryman, K. Clark, S. O. Pastan, T. C. Pearson, C. P. Larsen, S. Paul, and R. E. Patzer. 2018. Transplant center patient navigator and access to transplantation among high-risk population: A randomized, controlled trial. Clinical Journal of the American Society of Nephrology 13(4):620-627.
Berger, J. R., H. Quinones, and M. A. Vazquez. 2020. Dialysis for undocumented immigrants: Challenges and solutions. Kidney360 1(6):549-552.
Bhimani, S., G. Boyle, W. Liu, S. Worley, E. Saarel, and S. Admani. 2020. Gender and racial disparities in pediatric heart transplantation in the current era: A UNOS registry analysis. Journal of Heart and Lung Transplantation 39(4):S461-S462.
Bodenheimer, H. C., Jr., J. M. Okun, W. Tajik, J. Obadia, N. Icitovic, P. Friedmann, E. Marquez, and M. J. Goldstein. 2012. The impact of race on organ donation authorization discussed in the context of liver transplantation. Transactions of the American Clinical and Climatological Association 123:64-78.
Bonham, V. L., E. D. Green, and E. J. Pérez-Stable. 2018. Examining how race, ethnicity, and ancestry data are used in biomedical research. Journal of the American Medical Association 320(15):1533-1534.
Boulware, L. E., and D. Mohottige. 2021. The seen and the unseen: Race and social inequities affecting kidney care. Clinical Journal of the American Society of Nephrology 16(5):815-817.
Boyd, R., E. Lindo, L. Weeks, and M. McLemore. 2020. On racism: A new standard for publishing on racial health inequities. Health Affairs. https://www.healthaffairs.org/do/10.1377/hblog20200630.939347/full (accessed December 11, 2021).
Breathett, K., E. Yee, N. Pool, M. Hebdon, J. D. Crist, R. H. Yee, S. M. Knapp, S. Solola, L. Luy, K. Herrera-Theut, L. Zabala, J. Stone, M. M. McEwen, E. Calhoun, and N. K. Sweitzer. 2020. Association of gender and race with allocation of advanced heart failure therapies. JAMA Network Open 3(7):e2011044.
Brown, E. J., D. Polsky, C. M. Barbu, J. W. Seymour, and D. Grande. 2016. Racial disparities in geographic access to primary care in Philadelphia. Health Affairs 35(8):1374-1381.
CDC (Centers for Disease Control and Prevention). 2021. About social determinants of health. https://www.cdc.gov/socialdeterminants/about.html (accessed September 12, 2021).
Center for Health Progress. 2017. Race is a social construct. https://centerforhealthprogress.org/blog/race-social-construct (accessed October 19, 2021).
Cervantes, L., S. Fischer, N. Berlinger, M. Zabalaga, C. Camacho, S. Linas, and D. Ortega. 2017. The illness experience of undocumented immigrants with end-stage renal disease. JAMA Internal Medicine 177(4):529-535.
Dageforde, L. A., A. Box, I. D. Feurer, and K. L. Cavanaugh. 2015. Understanding patient barriers to kidney transplant evaluation. Transplantation 99(7):1463-1469.
Damschroder, L. J., D. C. Aron, R. E. Keith, S. R. Kirsh, J. A. Alexander, and J. C. Lowery. 2009. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implementation Science 4(50).
Darden, M., G. Parker, E. Anderson, and J. F. Buell. 2021. Persistent sex disparity in liver transplantation rates. Surgery 169(3):694-699.
DeFilippis, E. M., L. K. Truby, A. R. Garan, R. C. Givens, K. Takeda, H. Takayama, Y. Naka, J. H. Haythe, M. A. Farr, and V. K. Topkara. 2019. Sex-related differences in use and outcomes of left ventricular assist devices as bridge to transplantation. Journals of the American College of Cardiology: Heart Failure 7(3):250-257.
Dobbels, F. 2014. Intellectual disability in pediatric transplantation: Pitfalls and opportunities. Pediatric Transplantation 18(7):658-660.
Dover, D. C., and A. P. Belon. 2019. The health equity measurement framework: A comprehensive model to measure social inequities in health. International Journal for Equity in Health 18(36).
Eisenstein, E. L., J. L. Sun, K. J. Anstrom, J. A. Stafford, L. A. Szczech, L. H. Muhlbaier, and D. B. Mark. 2009. Do income level and race influence survival in patients receiving hemodialysis? American Journal of Medicine 122(2):170-180.
Epstein, A. M., J. Z. Ayanian, J. H. Keogh, S. J. Noonan, N. Armistead, P. D. Cleary, J. S. Weissman, J. A. DavidKasdan, D. Carlson, J. Fuller, D. Marsh, and R. M. Conti. 2000. Racial disparities in access to renal transplantation—clinically appropriate or due to underuse or overuse? New England Journal of Medicine 343(21):1537-1544.
Epstein, S. 2007. Inclusion: The politics of difference in medical research. Chicago, IL: University of Chicago Press.
Evangelista, L. S., K. Dracup, and L. V. Doering. 2000. Treatment-seeking delays in heart failure patients. Journal of Heart and Lung Transplantation 19(10):932-938.
Fontanarosa, P. B., and H. Bauchner. 2018. Race, ancestry, and medical research. JAMA 320(15):1539-1540.
Galante, N. Z., G. A. Dib, and J. O. Medina-Pestana. 2010. Severe intellectual disability does not preclude renal transplantation. Nephrology, Dialysis, Transplantation 25(8):2753-2757.
Gander, J. C., X. Zhang, L. Plantinga, S. Paul, M. Basu, S. O. Pastan, E. Gibney, E. Hartmann, L. Mulloy, C. Zayas, and R. E. Patzer. 2018. Racial disparities in preemptive referral for kidney transplantation in Georgia. Clinical Transplantation 32(9):e13380.
Geronimus, A. T. 2013. Deep integration: Letting the epigenome out of the bottle without losing sight of the structural origins of population health. American Journal of Public Health 103(Suppl 1):S56-563.
Ghahramani, N., Z. Y. Karparvar, M. Ghahramani, and P. Shrivastava. 2011. Nephrologists’ perceptions of renal transplant as treatment of choice for end-stage renal disease, preemptive transplant, and transplanting older patients: An international survey. Experimental and Clinical Transplantation 9(4):223-229.
Ghahramani, N., A. Sanati-Mehrizy, and C. Wang. 2014. Perceptions of patient candidacy for kidney transplant in the United States: A qualitative study comparing rural and urban nephrologists. Experimental and Clinical Transplantation 12(1):9-14.
Glazier, A. K., G. M. Danovitch, and F. L. Delmonico. 2014. Organ transplantation for nonresidents of the United States: A policy for transparency. American Journal of Transplantation 14(8):1740-1743.
Gordon, E. J., and A. R. Sehgal. 2000. Patient-nephrologist discussions about kidney transplantation as a treatment option. Advances in Renal Replacement Therapy 7(2):177-183.
Gordon, E. J., J. Feinglass, P. Carney, K. Vera, M. Olivero, A. Black, K. O’Connor, J. MacLean, S. Nichols, J. Sageshima, L. Preczewski, and J. C. Caicedo. 2016a. A culturally targeted website for Hispanics/Latinos about living kidney donation and transplantation: A randomized controlled trial of increased knowledge. Transplantation 100(5):1149-1160.
Gordon, E. J., J. Feinglass, P. Carney, K. Vera, M. Olivero, A. Black, K. G. O’Connor, J. M. Baumgart, and J. C. Caicedo. 2016b. A website intervention to increase knowledge about living kidney donation and transplantation among Hispanic/Latino dialysis patients. Progress in Transplantation 26(1):82-91.
Gordon, E. J., J. Lee, R. H. Kang, J. C. Caicedo, J. L. Holl, D. P. Ladner, and M. D. Shumate. 2018. A complex culturally targeted intervention to reduce Hispanic disparities in living kidney donor transplantation: An effectiveness-implementation hybrid study protocol. BMC Health Services Research 18(1):368.
Gordon, E. J., E. Romo, D. Amórtegui, A. Rodas, N. Anderson, J. Uriarte, G. McNatt, J. C. Caicedo, D. P. Ladner, and M. Shumate. 2020. Implementing culturally competent transplant care and implications for reducing health disparities: A prospective qualitative study. Health Expectations 23(6):1450-1465.
Gordon, E. J., J. Uriarte, J. Lee, R. Kang, M. Shumate, R. Ruiz, A. Mather, D. Ladner, and J. C. Caicedo. 2021. Effectiveness of a culturally competent care intervention in reducing disparities in Hispanic live donor kidney transplantation: A hybrid trial. American Journal of Transplantation 22(2):474-488. https://doi.org/10.1111/ajt.16857.
Grams, M. E., B. P. Chen, J. Coresh, and D. L. Segev. 2013. Preemptive deceased donor kidney transplantation: Considerations of equity and utility. Clinical Journal of the American Society of Nephrology 8(4):575-582.
Green, A. R., D. R. Carney, D. J. Pallin, L. H. Ngo, K. L. Raymond, L. I. Iezzoni, and M. R. Banaji. 2007. Implicit bias among physicians and its prediction of thrombolysis decisions for black and white patients. Journal of General Internal Medicine 22(9):1231-1238.
Hall, W. J., M. V. Chapman, K. M. Lee, Y. M. Merino, T. W. Thomas, B. K. Payne, E. Eng, S. H. Day, and T. CoyneBeasley. 2015. Implicit racial/ethnic bias among health care professionals and its influence on health care outcomes: A systematic review. American Journal of Public Health 105(12).
Hall, Y. N., A. I. Choi, P. Xu, A. M. O’Hare, and G. M. Chertow. 2011. Racial ethnic differences in rates and determinants of deceased donor kidney transplantation. Journal of the American Society of Nephrology 22(4):743-751.
Hanson, C. S., S. J. Chadban, J. R. Chapman, J. C. Craig, G. Wong, and A. Tong. 2016. Nephrologists’ perspectives on recipient eligibility and access to living kidney donor transplantation. Transplantation 100(4):943-953.
Harding, J. L., A. Perez, and R. E. Patzer. 2021. Nonmedical barriers to early steps in kidney transplantation among underrepresented groups in the United States. Current Opinion in Organ Transplantation 26(5):501-507.
Harding, K., T. B. Mersha, P.-T. Pham, A. D. Waterman, F. J. Webb, J. A. Vassalotti, and S. B. Nicholas. 2017. Health disparities in kidney transplantation for African Americans. American Journal of Nephrology 46:165-175.
HHS (U.S. Department of Health and Human Services). Health Resources and Services Administration, Healthcare Systems Bureau. 2019. 2019 National Survey of Organ Donation Attitudes and Practices: Report of findings. Rockville, MD: U.S. Department of Health and Human Services. https://www.organdonor.gov/sites/default/files/organ-donor/professional/grants-research/nsodap-organ-donation-survey-2019.pdf (accessed August 24, 2021).
HHS. 2021a. Healthy people 2020. https://www.healthypeople.gov/2020/about/foundation-health-measures/Disparities (accessed November 18, 2021).
HHS. 2021b. Healthy people 2030. https://health.gov/our-work/healthy-people/healthy-people-2030/questions-answers (accessed November 18, 2021).
HHS. 2021c. Request for Information. 45 CFR Part 84. Discrimination on the basis of disability in critical Health and Human Services programs or activities. https://www.hhs.gov/sites/default/files/504-rfi.pdf (accessed September 8, 2021).
IOM (Institute of Medicine). 2001a. Crossing the quality chasm: A new health system for the 21st century. Washington, DC: The National Academy Press.
IOM. 2001b. Envisioning the national health care quality report. Washington, DC: The National Academy Press.
IOM. 2010. Future directions for the National Healthcare Quality and Disparities Reports. Washington, DC: The National Academies Press.
Johns, T. S., M. M. Estrella, D. C. Crews, L. J. Appel, C. A. Anderson, P. L. Ephraim, C. Cook, and L. E. Boulware. 2014. Neighborhood socioeconomic status, race, and mortality in young adult dialysis patients. Journal of the American Society of Nephrology 25(11):2649-2657.
Jones, C., P. Roderick, S. Harris, and M. Rogerson. 2006. Decline in kidney function before and after nephrology referral and the effect on survival in moderate to advanced chronic kidney disease. Nephrology, Dialysis, Transplantation 21(8):2133-2143.
Joshi, M. S., and C. Stevens. 2017. Implicit attitudes to organ donor registration: Altruism and distaste. Health Psychology and Behavioral Medicine 5(1):14-28.
Joshi, S., J. J. Gaynor, S. Bayers, G. Guerra, A. Eldefrawy, Z. Chediak, L. Companioni, J. Sageshima, L. Chen, W. Kupin, D. Roth, A. Mattiazzi, G. W. Burke, III, and G. Ciancio. 2013. Disparities among blacks, Hispanics, and whites in time from starting dialysis to kidney transplant waitlisting. Transplantation 95(2):309-318.
Kernodle, A. B., W. Zhang, J. D. Motter, B. Doby, L. Liyanage, J. Garonzik-Wang, K. R. Jackson, B. J. Boyarsky, A. B. Massie, T. S. Purnell, and D. L. Segev. 2021. Examination of racial and ethnic differences in deceased organ donation ratio over time in the US. JAMA Surgery 156(4):e207083.
Killian, A. C., B. Shelton, P. MacLennan, M. C. McLeod, A. Carter, R. Reed, H. Qu, B. Orandi, V. Kumar, C. Sawinski, and J. E. Locke. 2021. Evaluation of community-level vulnerability and racial disparities in living donor kidney transplant. JAMA Surgery 156(12):1120-1129.
Kim, J. J., M. Basu, L. Plantinga, S. O. Pastan, S. Mohan, K. Smith, T. Melanson, C. Escoffery, and R. E. Patzer. 2018. Awareness of racial disparities in kidney transplantation among health care providers in dialysis facilities. Clinical Journal of the American Society of Nephrology 13(5):772-781.
King, K. L., S. A. Husain, Z. Jin, C. Brennan, and S. Mohan. 2019. Trends in disparities in preemptive kidney transplantation in the United States. Clinical Journal of the American Society of Nephrology 14(10):1500-1511.
King, L. P., L. A. Siminoff, D. M. Meyer, C. W. Yancy, W. S. Ring, T. W. Mayo, and M. H. Drazner. 2005. Health insurance and cardiac transplantation: A call for reform. Journal of the American College of Cardiology 45:1388–1391.
Kucirka, L. M., M. E. Grams, J. Lessler, E. C. Hall, N. James, A. B. Massie, R. A. Montgomery, and D. L. Segev. 2011. Association of race and age with survival among patients undergoing dialysis. JAMA 306(6):620-626.
Kutner, N. G., R. Zhang, Y. Huang, and K. L. Johansen. 2012. Impact of race on predialysis discussions and kidney transplant preemptive wait-listing. American Journal of Nephrology 35(4):305-311.
Lee, B. P., and N. A. Terrault. 2020. Liver transplantation in unauthorized immigrants in the United States. Hepatology 71(5):1802-1812.
Levenson, J. L., and M. E. Olbrisch. 1993. Psychosocial evaluation of organ transplant candidates: A comparative survey of process, criteria, and outcomes in heart, liver, and kidney transplantation. Psychosomatics 34(4):314-323.
Levin, A. 2000. Consequences of late referral on patient outcomes. Nephrology Dialysis Transplantation, 15(Suppl 3):8-13.
Loy, V. M., A. Rzepczynski, C. Joyce, S. Bello, and A. Lu. 2020. Disparity in transplant referral patterns for alcohol-related liver disease based on physician-dependent variables. Transplantation Proceedings 52(3):900-904.
Marlow, N. M., A. S. Kazley, K. D. Chavin, K. N. Simpson, W. Balliet, and P. K. Baliga. 2016. A patient navigator and education program for increasing potential living donors: A comparative observational study. Clinical Transplantation 30(5):619-627.
Martin, P. 2014. Living donor kidney transplantation: Preferences and concerns amongst patients waiting for transplantation in New Zealand. Journal of Health Services Research & Policy 19(3):138-144.
McEnhill, M. E., J. L. Brennan, E. Winnicki, M. M. Lee, M. Tavakol, A. M. Posselt, P. G. Stock, and A. A. Portale. 2016. Effect of immigration status on outcomes in pediatric kidney transplant recipients. American Journal of Transplantation 16(6):1827-1833.
Mehra, M., J. Kobashigawa, R. Starling, S. Russell, P. Uber, J. Parameshwar, P. Mohacsi, S. Augustine, K. Aaronson, and M. Barr. 2006. Listing criteria for Heart transplantation: International Society for Heart and Lung Transplantation guidelines for the care of cardiac transplant candidates—2006. Journal of Heart and Lung Transplantation 25(9):1024-1042.
Mehra, M. R., C. E. Canter, M. M. Hannan, M. J. Semigran, P. A. Uber, D. A. Baran, L. Danziger-Isakov, J. K. Kirklin, R. Kirk, S. S. Kushwaha, L. H. Lund, L. Potena, H. J. Ross, D. O. Taylor, E. Verschuuren, A. Zuckermann, and International Society for Heart Lung Transplantation, Infectious Diseases, Pediatric and Heart Failure and Transplantation Councils. 2016. The 2016 International Society for Heart Lung Transplantation listing criteria for heart transplantation: A 10-year update. Journal of Heart and Lung Transplantation 35(1):1-23.
Meissner, F., L. A. Grigutsch, N. Koranyi, F. Müller, and K. Rothermund. 2019. Predicting behavior with implicit measures: Disillusioning findings, reasonable explanations, and sophisticated solutions. Frontiers in Psychology 10:2483.
Morris, A. A., E. P. Kransdorf, B. L. Coleman, and M. Colvin. 2016. Racial and ethnic disparities in outcomes after heart transplantation: A systematic review of contributing factors and future directions to close the outcomes gap. Journal of Heart and Lung Transplantation 35(8):953-961.
Morris, Z. S., S. Wooding, and J. Grant. 2011. The answer is 17 years, what is the question: Understanding time lags in translational research. Journal of the Royal Society of Medicine 104(12):510-520.
Mucsi, I., A. Bansal, O. Famure, Y. Li, M. Mitchell, A. D. Waterman, M. Novak, and S. J. Kim. 2017. Ethnic background is a potential barrier to living donor kidney transplantation in Canada: A single-center retrospective cohort study. Transplantation 101(4):e142-e151.
Mulligan, C. J. 2021. Systemic racism can get under our skin and into our genes. American Journal of Physical Anthropology 175:399-405.
Mustian, M. N., B. A. Shelton, P. A. MacLennan, R. D. Reed, J. A. White, D. E. Eckhoff, J. E. Locke, R. M. Allman, and S. H. Gray. 2019. Ethnic and age disparities in outcomes among liver transplant waitlist candidates. Transplantation 103(7):1425-1432.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2021. The science of implicit bias: Implications for law and policy: Proceedings of a workshop-in brief. Washington, DC: The National Academies Press. https://doi.org/10.17226/26191.
National Work Group on Disability and Transplantation. 2004. Summary report of the individual and family disability survey, March 11, 2004.
Navaneethan, S. D., S. Nigwekar, M. Sengodan, E. Anand, S. Kadam, V. Jeevanantham, M. Grieff, and W. Choudhry. 2007. Referral to nephrologists for chronic kidney disease care: Is non-diabetic kidney disease ignored? Nephron Clinical Practice 106(3):c113-c118.
Navaneethan, S. D., S. Aloudat, and S. Singh. 2008. A systematic review of patient and health system characteristics associated with late referral in chronic kidney disease. BMC Nephrology 9(3).
Ng, Y. H., V. S. Pankratz, Y. Leyva, C. G. Ford, J. R. Pleis, K. Kendall, E. Croswell, M. A. Dew, R. Shapiro, G. E. Switzer, M. L. Unruh, and L. Myaskovsky. 2020. Does racial disparity in kidney transplant waitlisting persist after accounting for social determinants of health? Transplantation 104(7):1445-1455.
Nissaisorakarn, P., X. Huiling, M. D. Doshi, N. Singh, K. L. Lentine, and S. E. Rosas. 2021. Eliminating racial disparities in kidney transplantation. Clinical Transplantation 35(8):e14397.
Ohta, T., O. Motoyama, K. Takahashi, M. Hattori, S. Shishido, N. Wada, Y. Gotoh, T. Yanagihara, A. Hasegawa, and T. Sakano. 2006. Kidney transplantation in pediatric recipients with mental retardation: Clinical results of a multicenter experience in Japan. American Journal of Kidney Diseases 47(3):518-527.
OPTN (Organ Procurement and Transplantation Network). 2020. Briefing to the OPTN board of directors on data collection to assess socioeconomic status and access to transplant. https://optn.transplant.hrsa.gov/media/3811/202006_mac_ses_bp.pdf (accessed September 9, 2021).
OPTN. 2021. Policies. https://optn.transplant.hrsa.gov/media/1200/optn_policies.pdf (accessed September 9, 2021).
Padela, A. I., R. Duivenbode, M. R. Saunders, M. Quinn, and E. Koh. 2020. The impact of religiously tailored and ethically balanced education on intention for living organ donation among Muslim Americans. Clinical Transplantation 34(12):e14111.
Patzer, R. E., J. P. Perryman, J. D. Schrager, S. Pastan, S. Amaral, J. A. Gazmararian, M. Klein, N. Kutner, and W. M. McClellan. 2012. The role of race and poverty on steps to kidney transplantation in the southeastern United States. American Journal of Transplantation 12(2):358-368.
Patzer, R. E., B. A. Sayed, N. Kutner, W. M. McClellan, and S. Amaral. 2013. Racial and ethnic differences in pediatric access to preemptive kidney transplantation in the United States. American Journal of Transplantation 13(7):1769-1781.
Pelleboer-Gunnink, H. A., W. Van Oorsouw, J. Van Weeghel, and P. Embregts. 2017. Mainstream health professionals’ stigmatising attitudes towards people with intellectual disabilities: A systematic review. Journal of Intellectual Disability Research 61(5):411-434.
Peng, R. B., H. Lee, Z. T. Ke, and M. R. Saunders. 2018. Racial disparities in kidney transplant waitlist appearance in Chicago: Is it race or place? Clinical Transplantation 32(5):e13195.
Pew Research Center. 2019. U.S. unauthorized immigrant population estimates by state, 2016. https://www.pewresearch.org/hispanic/interactives/u-s-unauthorized-immigrants-by-state (accessed September 2, 2021).
Popejoy, A. B., K. R. Crooks, S. M. Fullerton, L. A. Hindorff, G. W. Hooker, B. A. Koenig, N. Pino, E. M. Ramos, D. I. Ritter, H. Wand, M. W. Wright, M. Yudell, J. Y. Zou, S. E. Plon, C. D. Bustamante, and K. E. Ormond, Clinical Genome Resource (ClinGen) Ancestry and Diversity Working Group. 2020. Clinical genetics lacks standard definitions and protocols for the collection and use of diversity measures. American Journal of Human Genetics 107(1):72-82.
Prakash, S., R. A. Rodriguez, P. C. Austin, R. Saskin, A. Fernandez, L. M. Moist, and A. M. O’Hare. 2010. Racial composition of residential areas associates with access to Pre-ESRD nephrology care. Journal of the American Society of Nephrology 21(7):1192-1199.
Purnell, T. S., and D. C. Crews. 2019. Persistent disparities in preemptive kidney transplantation. Clinical Journal of the American Society of Nephrology 14(10):1430-1431.
Reese, P. P., O. Aubert, M. Naesens, E. Huang, V. Potluri, D. Kuypers, A. Bouquegneau, G. Divard, M. Raynaud, Y. Bouatou, A. Vo, D. Glotz, C. Legendre, C. Lefaucheur, S. Jordan, J. P. Empana, X. Jouven, and A. Loupy. 2021a. Assessment of the utility of kidney histology as a basis for discarding organs in the United States: A comparison of international transplant practices and outcomes. Journal of the American Society of Nephrology 32(2):397-409.
Reese, P. P., S. Mohan, K. L. King, W. W. Williams, V. S. Potluri, M. N. Harhay, and N. D. Eneanya. 2021b. Racial disparities in preemptive waitlisting and deceased donor kidney transplantation: Ethics and solutions. American Journal of Transplantation 21(3):958-967.
Rhee, C. M., P. Lertdumrongluk, E. Streja, J. Park, H. Moradi, W. L. Lau, K. C. Norris, A. R. Nissenson, A. N. Amin, C. P. Kovesdy, and K. Kalantar-Zadeh. 2014. Impact of age, race and ethnicity on dialysis patient survival and kidney transplantation disparities. American Journal of Nephrology 39(3):183-194.
Richards, C. T., L. M. Crawley, and D. Magnus. 2009. Use of neurodevelopmental delay in pediatric solid organ transplant listing decisions: Inconsistencies in standards across major pediatric transplant centers. Pediatric Transplantation 13(7):843-850.
Robinson, A., G. Hirode, and R. J. Wong. 2021. Ethnicity and insurance-specific disparities in the model for end-stage liver disease score at time of liver transplant waitlist registration and its impact on mortality. Journal of Clinical and Experimental Hepatology 11(2):188-194.
Rodrigue, J. R., M. J. Paek, O. Egbuna, A. D. Waterman, J. D. Schold, M. Pavlakis, and D. A. Mandelbrot. 2014. Making house calls increases living donor inquiries and evaluations for blacks on the kidney transplant waiting list. Transplantation 98(9):979-986.
Rodriguez, R., L. Cervantes, and R. Raghavan. 2020. Estimating the prevalence of undocumented immigrants with end-stage renal disease in the United States. Clinical Nephrology 93(1):108-112.
Sabounchi, N., N. Sharareh, F. Irshaidat, and S. Atav. 2018. Spatial dynamics of access to primary care for the Medicaid population. Health Systems 9(1):64-75.
Salter, M., M. A. McAdams-Demarco, A. Law, R. J. Kamil, L. A. Meoni, B. G. Jaar, S. M. Sozio, W. H. L. Kao, R. S. Parekh, and D. L. Segev. 2014. Age and sex disparities in discussions about kidney transplantation in adults undergoing dialysis. Journal of the American Geriatrics Society 62(5):843-849.
Samelson-Jones, E., D. M. Mancini, and P. A. Shapiro. 2012. Cardiac transplantation in adult patients with mental retardation: Do outcomes support consensus guidelines? Psychosomatics 53(2):133-138.
Schimmack, U. 2021. The Implicit Association Test: A method in search of a construct. Perspectives on Psychological Science 16(2):396-414.
Schold, J. D., J. A. Gregg, J. S. Harman, A. G. Hall, P. R. Patton, and H. U. Meier-Kriesche. 2011. Barriers to evaluation and wait listing for kidney transplantation. Clinical Journal of the American Society of Nephrology 6(7):1760-1767.
Secunda, K., E. J. Gordon, M. W. Sohn, L. A. Shinkunas, L. C. Kaldjian, M. D. Voigt, and J. Levitsky. 2013. National survey of provider opinions on controversial characteristics of liver transplant candidates. Liver Transplantation 19(4):395-403.
Siminoff, L. A., R. H. Lawrence, and R. M. Arnold. 2003. Comparison of black and white families’ experiences and perceptions regarding organ donation requests. Critical Care Medicine 31(1):146-151.
Siminoff, L. A., G. P. Alolod, H. M. Gardiner, R. D. Hasz, P. A. Mulvania, and M. Wilson-Genderson. 2020. A comparison of the content and quality of organ donation discussions with African American families who authorize and refuse donation. Journal of Racial and Ethnic Health Disparities 8:485-493.
Suarez, J., J. B. Cohen, V. Potluri, W. Yang, D. E. Kaplan, M. Serper, S. P. Shah, and P. P. Reese. 2018. Racial disparities in nephrology consultation and disease progression among veterans with CKD: An observational cohort study. Journal of the American Society of Nephrology 29(10):2563-2573.
Sullivan, C., J. B. Leon, S. S. Sayre, M. Marbury, M. Ivers, J. A. Pencak, K. A. Bodziak, D. E. Hricik, E. J. Morrison, J. M. Albert, S. D. Navaneethan, C. M. Reyes, and A. R. Sehgal. 2012. Impact of navigators on completion of steps in the kidney transplant process: A randomized, controlled trial. Clinical Journal of the American Society of Nephrology 7(10):1639-1645.
Taylor, D. M., J. A. Bradley, C. Bradley, H. Draper, R. Johnson, W. Metcalfe, G. Oniscu, M. Robb, C. Tomson, C. Watson, R. Ravanan, P. Roderick, and ATTOM Investigators. 2016. Limited health literacy in advanced kidney disease. Kidney International 90(3):685-695.
Thuluvath, P. J., W. Amjad, and T. Zhang. 2020. Liver transplant waitlist removal, transplantation rates and posttransplant survival in Hispanics. PLoS ONE 15(12):e0244744
Traino, H. M., A. J. Molisani, and L. A. Siminoff. 2017. Regional differences in communication process and outcomes of requests for solid organ donation. American Journal of Transplantation 17(6):1620-1627.
Tung, E. L., D. A. Hampton, M. Kolak, S. O. Rogers, J. P. Yang, and M. E. Peek. 2019. Race/ethnicity and geographic access to urban trauma care. JAMA Network Open 2(3).
UNOS (United Network for Organ Sharing). 2021. Equity in access to transplant. https://insights.unos.org/equity-in-access (accessed August 10, 2021).
USRDS (United States Renal Data System). 2020. Annual data report: Epidemiology of kidney disease in the United States. Bethesda, MD: National Institute of Diabetes and Digestive and Kidney Diseases.
Vianello, M., and Y. Bar-Anan. 2021. Can the Implicit Association Test measure automatic judgment? The validation continues. Perspectives on Psychological Science 16(2):415-421.
Vyas, D. A., L. G. Eisenstein, and D. S. Jones. 2020. Hidden in plain sight—reconsidering the use of race correction in clinical algorithms. New England Journal of Medicine 383(9):874-882.
Wall, A., G. H. Lee, J. Maldonado, and D. Magnus. 2020. Genetic disease and intellectual disability as contraindications to transplant listing in the United States: A survey of heart, kidney, liver, and lung transplant programs. Pediatric Transplantation 24(7):e13837.
Waterman, A. D., J. R. Rodrigue, T. S. Purnell, K. Ladin, and L. E. Boulware. 2010. Addressing racial and ethnic disparities in live donor kidney transplantation: Priorities for research and intervention. Seminars in Nephrology 30(1):90-98.
Waterman, A. D., J. D. Peipert, S. S. Hyland, M. S. McCabe, E. A. Schenk, and J. Liu. 2013. Modifiable patient characteristics and racial disparities in evaluation completion and living donor transplant. Clinical Journal of the American Society of Nephrology 8(6):995-1002.
Weng, F. L., M. M. Joffe, H. I. Feldman, and K. C. Mange. 2005. Rates of completion of the medical evaluation for renal transplantation. American Journal of Kidney Diseases 46(4):734-745.
Wesselman, H., C. G. Ford, Y. Leyva, X. Li, C. H. Chang, M. A. Dew, K. Kendall, E. Croswell, J. R. Pleis, Y. H. Ng, M. L. Unruh, R. Shapiro, and L. Myaskovsky. 2021. Social determinants of health and race disparities in kidney transplant. Clinical Journal of the American Society of Nephrology 16(2):262-274.
Wightman, A., B. Young, M. Bradford, A. Dick, P. Healey, R. McDonald, and J. Smith. 2014. Prevalence and outcomes of renal transplantation in children with intellectual disability. Pediatric Transplantation 18(7):714-719.
Wightman, A., E. Hsu, Q. Zhao, and J. Smith. 2016. Prevalence and outcomes of liver transplantation in children with intellectual disability. Journal of Pediatric Gastroenterology and Nutrition 62(6):808-812.
Wightman, A., H. L. Bartlett, Q. Zhao, and J. M. Smith. 2017. Prevalence and outcomes of heart transplantation in children with intellectual disability. Pediatric Transplantation 21(2). https://doi.org/10.1111/petr.12839.
Wolfe, R. A., V. B. Ashby, E. L. Milford, A. O. Ojo, R. E. Ettenger, L. Y. Agodoa, P. J. Held, and F. K. Port. 1999. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. New England Journal of Medicine 341(23):1725-1730.
Yu, E., and A. Wightman. 2021. Pediatric kidney transplant in undocumented immigrants: An American perspective. Pediatric Transplant 25(1):e13788.
Yudell, M., D. Roberts, R. DeSalle, S. Tishkoff, 70 signatories. 2020. NIH must confront the use of race in science. Science 369(6509):1313-1314.
This page intentionally left blank.
































