
5
Saving More Lives and Enhancing Equity with Deceased Donor Organ Allocation Policies
Allocation systems—that is, how patients are prioritized on the waiting list and organs are rated for transplant—differ by organ type. The U.S. Department of Health and Human Services (HHS) Final Rule directs the Organ Procurement and Transplantation Network (OPTN) to design organ allocation policies “to achieve the best use of donated organs.1 Specifically, the OPTN must rank candidates from “most to least medically urgent” while “taking into account…that life-sustaining technology allows alternative approaches.” However, allocation systems differ by organ. Heart, liver, and lung allocation comply with the OPTN regulation and have allocation systems designed specifically on candidate urgency. Donated livers are allocated based on the transplant candidate’s likelihood of dying while on the wait list. Lung allocation is similar, but takes into account a transplant candidate’s likelihood of dying within a year after the transplant (Friedewald et al., 2013). Heart allocation relies on treatment choices as a proxy for medical urgency rather than by calculations coming from a scoring system. The kidney allocation system (KAS) ranks candidates primarily by waiting time.
According to the United Network for Organ Sharing (UNOS),2 several logistical and medical factors must be taken into account before a donated organ can be allocated to a patient. First, an organ needs to match the candidate; waiting list candidates who are incompatible (i.e., because of blood type, organ size, or other medical issues) are removed from consideration for that particular donated organ. Next, the order of eligible candidates is decided using what UNOS calls a match run, which is a rank-order list of candidates for a particular organ. The computed match run is unique for every organ and every donor. The match run also takes into consideration factors that affect the likely success of a transplant, including geographical factors such as transplant hospital locations or organ-specific time constraints that may limit the distance an organ is able to travel and still be viable for transplant (Table 5-1) and organ size (i.e., a pediatric-sized organ is best for a pediatric patient). Matching criteria do
___________________
1 42 C.F.R. §121.8 e-CFR: Title 42: Public Health.
2 For more specific information, see https://unos.org/transplant/how-we-match-organs (accessed October 21, 2021).
TABLE 5-1 Structural Factors and Key Disparities in Organ Allocation
| Organ | Before the Waiting List and Offer Process | Factors Considered in Allocationa | Key Disparities |
|---|---|---|---|
| Kidney | A candidate must undergo evaluation by the transplant team, and given blood tests, diagnostics tests, and a mental health evaluation. The transplant team will review medical history to determine eligibility for transplant, then the candidate is added to the UNOS waiting list.b Average wait time: 3–5 yearsc |
Proceeds through the Kidney Allocation System, which includes estimated 1-year posttransplant survival (EPTS), distance from donor hospital, pediatric status, waiting time, prior living donor, donor/recipient immune system incompatibility (CPRA)d,e Max organ preservation time: 24–36 hours |
Black patients, patients with diabetes, patients with prior solid organ transplantations Driven largely by inequitable access to donors, disparities in wait time vary widely across geographic location |
| Heart | A candidate must be referred by their physician, then be evaluated by the transplant team. The transplant team reviews their medical history to determine eligibility for transplant. A candidate who smokes must also cease smoking and be nicotine free for several months before they are allowed on the waiting list. Candidates are rank ordered for transplant by the treatments they need, and assigned 1 of 6 total adult status levels. Candidates with higher medical urgency (i.e., adult status 1) are prioritized for transplantation. Status levels are based primarily on use and complexity of treatments and devices needed (advanced support therapies), with some consideration of medications and additional heart conditions. Average wait time: 7–10 months |
Medical need; distance from donor hospitalf Max organ preservation time: 4–6 hours |
|
| Lung | A candidate must first be evaluated by a transplant team then given blood tests, diagnostics tests, and a mental health evaluation. Similar to heart transplant, the transplant team also reviews the patient’s medical history to determine eligibility for transplant. A candidate who smokes must also cease smoking and be nicotine free for several months before being allowed on the waiting list.g Once a candidate is deemed eligible, they are added to the UNOS waiting list. Average wait time: a few months to many years depending on lung disease diagnosis |
Lung allocation system, which includes medical urgency and survival benefit; waiting time; distance from donor hospitalh Max organ preservation time: 4–6 hours |
|
| Liver | Candidates must be evaluated by the transplant team, and will be given blood tests, imaging, and physical exams to determine the origin and severity of their liver disease, if any other diseases are affecting them, and estimate their likelihood to survive transplant. Those not eligible for transplant are candidates with a severe infection, current alcohol or drug abuse, serious heart or lung diseases, or cancer (outside the liver). |
Model of End-Stage Liver Disease or Pediatric End-Stage Liver Disease score; medical need; distance from donor hospitalj Max organ preservation time: 8–12 hours |
Adult patients of small size Pediatric patients of color, due to less frequent application for exception points; pediatric patients older than 1 year but less than 2 years old; and potentially pediatric patients aged 12–17k |
| Once a candidate is deemed eligible, they are added to the UNOS waiting list.i Average waiting time: less than 30 days to more than 5 years |
|||
| Intestine | A candidate must undergo evaluation by the transplant team. Candidates are then assigned a status for transplant—1, 2, or inactive. Status 1 candidates are prioritized for transplant. Status-level assignments are based on medical criteria.l |
Time on the waiting list, abnormal liver function, limited access points for intravenous feeding tubes, or presence of other medical indications warranting urgent transplant; blood type identical to or compatible with donor; geographic distance from transplant hospital (priority for within 500 NM then sharin is national)a | |
| VCA | A candidate must undergo evaluation by the transplant team. Candidates are registered on the waiting list by VCA type.m |
Time on the waiting list, blood type compatibility with donor, and geographic distance from the transplant hospital (priority for within 500 NM, then sharing is national). | |
| Pancreas | Candidates must undergo evaluation by the transplant team, and testing to determine their CPRA value. Only candidates diagnosed with diabetes, pancreatic exocrine insufficiency, or that require a pancreas as part of a multiorgan transplant for technical reasons are permitted to enter the waiting list.n | Time on the waiting list, CPRA, distance from the transplant hospital (priority for within 250 NM, then 2,500 NM, then sharing is national). | |
| Multiorgan | Candidates are evaluated by the transplant team according to the policies governing the types of organ transplants they need. | Multiorgan transplant specific policies for heart–lung, liver–kidney, and kidney–pancreas transplants; time on the waiting list, distance from the transplant hospital, and needed medical support without transplant, in line with single-organ transplant policies. | Kidney-alone transplant candidateso |
NOTE: NM = nautical miles; CPRA = calculated panel reactive antibody; VCA = vascularized composite allotransplantation; UNOS = United Network for Organ Sharing. SOURCES:
a https://unos.org/transplant/how-we-match-organs.
b https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/kidney-transplant.
c https://www.kidney.org/atoz/content/transplant-waitlist.
d https://www.srtr.org/transplant-centers/university-of-wisconsin-hospital-and-clinics-wiuw/?organ=kidney&recipientType=adult&donorType=.
e https://www.srtr.org/transplant-centers/university-of-chicago-medical-center-iluc/?organ=kidney&recipientType=adult&donorType=.
f https://www.upmc.com/services/transplant/heart/process/waiting-list.
g https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/lung-transplant.
h https://my.clevelandclinic.org/health/articles/9971-lung-transplant-finding-an-organ-donor.
i https://www.niddk.nih.gov/health-information/liver-disease/liver-transplant/preparing-transplant.
m https://optn.transplant.hrsa.gov/media/4211/bp_202012_programming-vca-allocation-in-unet.pdf.
not consider income, celebrity status, or insurance status in determining allocation priority. The committee is mindful that its charge is to consider all types of solid organ transplants. While each of these organs is considered in this chapter, the majority of this text focuses on kidneys since the vast majority of candidates on any waiting list for any organs are waiting for a kidney transplant.
DISPARITIES EXACERBATED BY ALLOCATION SCORING SYSTEMS
As described in previous chapters, factors contributing to disparity in the waiting list for transplantation include gaps in access to health care, uneven referral rates to specialist providers, and differing education efforts on treatment options and preparation for end-stage disease. These upstream factors are inextricable from the end result of the organ transplantation system and therefore crucial to highlight again.
Chapter 4 of this report discusses disparities in detail as they relate to many aspects of the organ transplantation system. Only a few key inequities are summarized here as fundamental underlying problems plaguing current allocation policies.
Implications of Current Policies Regarding Measurement of Organ Function and Recipient Suitability in Allocation Decisions3
Black organ donors receive a higher Kidney Donor Profile Index (KDPI) score because of the inclusion of race/ethnicity as a term in KDPI calculation (see Table 5-6). Few patients with diabetes or who have had a previous solid organ transplant will meet the current criteria for priority kidney allocation. In addition, because of the known high prevalence of diabetes among black and Hispanic patients, these groups may be less likely to gain the advantages of priority allocation when longevity matching4 patients with a 20 percent estimated posttransplant survival (EPTS) to donated organs with a 20 percent KDPI (Delgado et al., 2021; Freedman et al., 2016; Julian et al., 2017).
Changes to allocation with the new kidney allocation system in 2014 improved allocation by introducing sharing of donor organs at local, regional, and national levels for patients with high calculated panel reactive antibody (CPRA) scores. However, some disparities still exist. Black candidates with a CPRA of 80 percent or more continue to have lower access to transplantation compared with white candidates, whereas Hispanic candidates have similar access as white candidates with the changes. Patients who live in rural areas continue to have lower probability of finding a donor organ, especially if they do not get priority nationally (Kulkarni et al., 2019; Stewart et al., 2018).
There are regional differences in longevity matching, such that areas that do not have very many candidates with a low EPTS may not be able to optimize organs donated with a low KDPI, thus donated kidneys calculated to be least medically complex may go to candidates with a lower estimated survival posttransplant (Husain et al., 2019; Schold et al., 2014). As discussed in the section later in this chapter on survival benefit, it is not clear that this is a disparity with respect to the organ transplantation system overall, but it may affect patient outcomes on an individual or regional level. Waiting list mortality for liver transplant
___________________
3 Much of this section is excerpted or slightly modified from papers commissioned by the committee for this study (Ku, 2021; Lai, 2021). Commissioned papers are in the study’s public access file and are available upon request from the National Academies’ Public Access Records Office (paro@nas.edu).
4 Longevity matching refers to better matching the life span of an organ with the life span of the recipient.
candidates is comparable between patients of different race and ethnic backgrounds, likely driven by the objective measurements used in calculating the Model for End-Stage Liver Disease (MELD) scores.
Women waiting for liver transplants are much more likely to die while on the waiting list than men, likely caused by creatinine measures underestimating kidney function in women that is further exacerbated by serum sodium level calculations (Locke et al., 2020). However, sex differences also play a crucial role in liver diseases, their evolution and outcome, and in liver transplantation in terms of graft survival, metabolic levels, and quality of life after liver transplantation (Rodriquez-Castro et al., 2014). Disparities in access to liver transplants are exacerbated by considerations of body and organ size as well as differences in the etiology of underlying liver disease in addition to the previously mentioned limitations of the MELD score, especially regarding creatinine levels (Axelrod and Pomfret, 2008). Exception points granted to patients diagnosed with hepatocellular carcinoma are also more likely to be given to men, given the disease prevalence. Updated guidance to granting exception points for these patients may address this but has yet to be studied.
Exception points for Pediatric End-Stage Liver Disease (PELD) calculations are frequently requested and granted. However, patients identifying as nonwhite request exception points at lower rates. A National Liver Review Board, introduced in 2019, aims to standardize exception points, but the effects of this board on racial and ethnic disparities is still unknown.
There may also be age-based disparities in PELD calculations. Children older than 1 year but less than 2 years of age have a higher risk of dying while on the waiting list. In addition, children aged 12–17 years are prioritized for transplant using MELD, but MELD was based on blood values in adults and has not been verified for its accuracy in adolescents.
Kidney-alone transplant candidates may be disadvantaged by multiorgan allocation policies, where the “next sequential” candidate who would have received a donated kidney had it not gone to a multiorgan transplant recipient tended to be younger, more highly sensitized, and more likely to identify with a minority group (Westphal et al., 2021).
CURRENT ALLOCATION POLICIES AND SCORING SYSTEMS
Within the context of the structural factors and key disparities described in Table 5-1, each organ has varying policies and procedures governing transplantation. Some of the historical context around these policies is described in Chapter 3. The current policies and procedures working to govern allocation, including relevant factors for prewaiting list, waiting list, and postwaiting list, are described in this section.
Waiting List Management
Organ transplant waiting list management has become increasingly complex across all organ types but especially in the kidney population. Large transplant programs report upward of 1,000 or more kidney patients on their waiting list, underscoring the importance of assessing individual patients for transplant readiness, communication of waiting list status, and patient education. Husain et al. (2018) found that in the years 2008 through 2015, between 14 and 20 percent of deceased donor kidneys that were eventually transplanted were first offered to one or more deceased candidates, contributing to less efficiency in the process of organ offers, and perhaps contributing to organ nonuse.5
___________________
5 The text in this section and throughout the report was modified after release of the report to clarify the findings of the study by Husain et al. (2018).
In late 2011, regulatory changes led to the Social Security Administration (SSA) not including protected state death records in the Death Master File used by the OPTN, among others, to verify patient status. Although changes affected access to the SSA, dialysis units and transplant centers are obligated to report all kidney patient deaths to the U.S. Renal Data System in almost real time. Though death data ultimately are reported via a different mechanism, offers to deceased candidates highlight the lack of patient engagement around organ offers being declined on their behalf by transplant centers (Husain et al., 2018; see Figure 5-1). With national death data available to update the waiting list in a timely fashion, it is perplexing why the OPTN and/or transplant centers choose not to update the waiting list with this information. Understanding that 14 to 20 percent of deceased donor kidneys that were eventually transplanted were first offered to one or more deceased candidates (Husain et al., 2018) is a situation that undermines public trust in the organ transplantation system6. Updating patient data can improve the organ offer process, and make it possible for the right organ to get to the right recipient in a timely manner. A real opportunity exists for better data management of waiting list candidates by transplant centers and the OPTN.
In 2016, the OPTN implemented the 3-year Collaborative Improvement and Innovation Network (COIIN), a study designed to improve the use of kidneys with a KDPI score of greater than 50 percent (Wey et al., 2020). Although COIIN did not have an effect on kidney use, waiting list management was a key focus area of the intervention guide and included referring patients for transplant evaluation, evaluating and selecting candidates for listing, and reevaluating wait-listed candidates. A visual analytics tool that displays information
__________________
6 The text in this section and throughout the report was modified after release of the report to clarify the findings of the study by Husain et al. (2018).
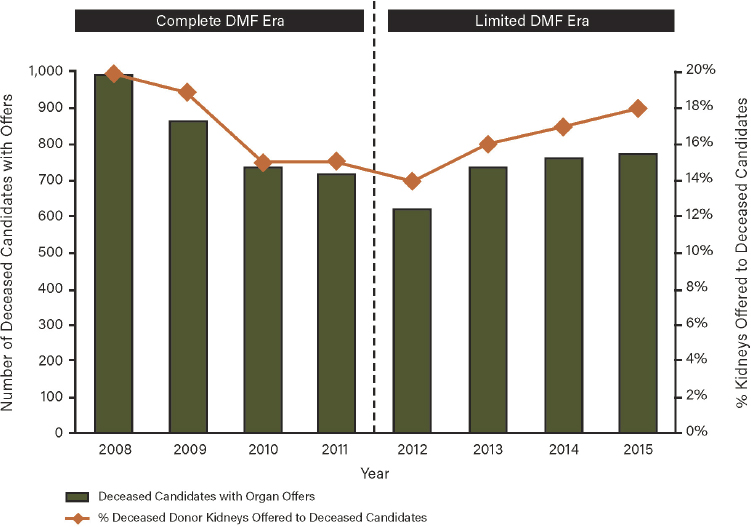
NOTE: DMF = Death Master File.
SOURCE: Husain et al., 2018.
related to the active and inactive status of kidney patients on transplant center waiting lists was launched by UNOS in early 2020 and is available to all kidney transplant programs on its data analytics portal (OPTN, 2021b).
Overview of Efforts to Address Geographic Disparities
Certain organ allocation and distribution policies have been highly debated among the transplantation community over the years. As a recent example, there was a change in 2018 to the adult heart allocation system that was made to improve stratification of waiting list candidates and provide broader access to the most medically urgent cases. Waiting list stratification changed from a three-tiered to six-tiered system. There were concerns that the changes would encourage a different approach to the care of critically ill heart failure patients, and early data suggest that may be the case (Cogswell et al., 2020). Following this change, which went into effect in October 2018, the number of heart transplants increased from 2,954 to 3,032, though this was most likely not related to the change. However, 78 percent of transplants after the change were from the most medically urgent categories (status 1, 2, and 3) versus 68 percent in status 1a (the most urgent before the change) (Goff et al., 2020). In addition, the median distance between the donor and transplant hospital increased from 83 to 216 nautical miles. Six-month posttransplant survival did not change significantly (93.6 percent vs. 92.8 percent). Use of extra corporeal membrane oxygenation was also statistically significantly higher than before the allocation change (1.93 percent vs. 1.06 percent; P < .001). More intra-aortic balloon pumps were also implanted following the change (8.84 percent vs. 3.86 percent; P < .001). It is too early to determine the overall effect of the change, but the challenges point to the complexities in making sweeping changes to the allocation system. One cohort study comparing heart transplant rates before and after the 2018 allocation change found significant variation in heart transplantation rates among centers in the same geographic region and those sharing the same organ procurement organization (OPO)—the largest variation being 27 percent for two transplant centers with the same OPO (Tran et al., 2022). Centers with higher transplant volumes and a greater proportion of candidates with intra-aortic balloon pump had higher transplant rates (Tran et al., 2022).
The evolution of liver allocation and distribution policies is another example of changes that have occurred. It was first developed in 1987 using a points-based system and relied on defined distribution units. Within this system, there was concern that candidates with the highest medical need could be bypassed for candidates with a lower medical need if the individual with the highest need were outside of the service area of the OPO that procured the liver. The OPTN Final Rule in 1998 sought to address some of these geographic disparities in deceased donor organ allocation. Specifically, the Final Rule directs that organ allocation policies not be based on a transplant candidate’s place of residence or listing except to the extent required by other requirements of the Final Rule and that allocation should achieve equitable allocation among patients, including through the distribution of organs over as “broad a geographic area as feasible” under the other allocation policies7. The ensuing controversy prompted Congress to request a study from the Institute of Medicine (IOM) to ascertain the effects of the Final Rule; the IOM committee later issued a report recommending broader sharing of livers (IOM, 1999).
Implementation of the MELD system of allocation in 2002 was intended to better address medical urgency in liver transplantation. A number of distribution efforts related to expanded allocation followed, including the Share 15 policy in 2005, which sought to improve access
___________________
7OPTN Final Rule, 42 C.F.R. §121.8.
for candidates with the highest need by making liver offers to those with a MELD score of 15 or higher at the regional level prior to the local level. The Share 35 policy in 2013 further extended regional and national sharing to candidates with MELD scores over 35 before local candidates with scores under 35. Massie et al. (2015) found that nonuse rates and waiting list mortality both decreased following implementation. However, regional variation in transplant outcomes following implementation of this policy was also noted (Halazun et al., 2016). In 2018, liver distribution policy moved away from the donation service area to acuity circles based on 150, 250, and 500 nautical miles from a donor hospital.8 While implementation was delayed because of legal action, the policy went into effect in February 2020.
In an effort to address geographic disparities more broadly, the OPTN created an ad hoc committee in 2017 focused on the geographic distribution of organs. The committee recommended, and the OPTN board of directors subsequently adopted in 2018, a continuous distribution framework as the best option for future distribution policies and directed its organ-specific committees to move in this direction. Whether these changes to allocation policies will result in the desired corrections to geographic disparities in access to transplant remains to be seen; however, as with any new policy changes, it will be important to monitor implementation efforts for unintended consequences.
Continuous Distribution
Continuous distribution is a framework for allocating and distributing deceased donor organs developed by the OPTN. The framework aims to eliminate fixed geographic boundaries currently used to separate groups of candidates based on distance between donor hospital and transplant hospital. Prior deceased donor organ distribution frameworks have considered patient characteristics in a defined sequence, whereas continuous distribution will create a composite score that considers multiple patient and donor attributes all at once with an overall score that includes medical urgency, posttransplant survival, candidate biology, patient access (such as pediatric or prior living donor), and placement efficiency, defined as efficient use of resources to match, transport, and transplant a donated organ (OPTN, n.d.-a).
The OPTN gives the following illustration on its website to describe some of the differences under a continuous distribution framework (Figure 5-2). Under current classification systems, one factor alone (e.g., distance from donor hospital) can determine the order in which hypothetical transplantation candidates A, B, C, and D receive an organ offer. Taking distance from the donor hospital as the example, candidate C would receive an organ offer first, followed by A, B, and finally D.
Taking this same example in a continuous distribution framework instead, depending on the weight and value of attributes selected by the organ-specific committee and transplant community, candidate B may be the first to receive an organ offer owing to their combination of medical urgency, survival probability, and distance to the donor hospital. Under this hypothetical framework, candidate A would receive the next offer, followed by C and then D.
Conclusion 5-1: Assigning a relatively large weight to the placement efficiency factor (based on potential recipients’ proximity to the donor hospital) in the continuous distribution policy would violate the Final Rule and defeat the goals of the policy, which the OPTN adopted to ensure that organs are allocated fairly and efficiently among patients nationally.
___________________
8 For more information on allocation based on acuity circles, see https://optn.transplant.hrsa.gov/governance/key-initiatives/liver (accessed August 10, 2021).
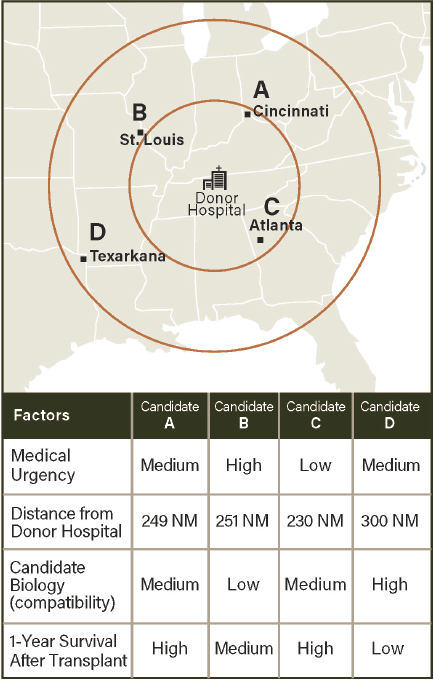
NOTE: NM = nautical mile.
SOURCE: OPTN, n.d.-a.
Organ-specific committees, with input from transplant communities, are identifying and confirming relevant attributes for candidates on the waiting list; prioritizing the attributes and assigning waiting list point values to them; developing, modeling, and analyzing the proposed frameworks; seeking formal public comment on the proposals; incorporating changes proposed in the public comment period as appropriate; and then seeking approval from the OPTN board of directors before implementing the new frameworks (see Chapter 2 for a further description of the OPTN policy-making process).
The continuous distribution for lung transplantation is the furthest along in the process, with the board of directors reviewing it in December 2021 and anticipated implementation in 2023. The kidney and pancreas policy completed its public comment phase at the end of September 2021,9 and it will go to the board of directors in 2022 for review. Continuous distribution policy development for liver and intestine will begin next, anticipated in 2022, followed by heart and vascularized composite allotransplantation (VCA), anticipated in 2023.
___________________
9 To read the public comments on this policy, see https://optn.transplant.hrsa.gov/governance/public-comment/update-on-continuous-distribution-of-kidneys-and-pancreata (accessed November 5, 2021).
Conclusion 5-2: The OPTN is developing the continuous distribution formulas for each organ type consecutively, which pushes full system implementation of the policy additional years into the future and delays achieving an equitable, transparent, and efficient system of organ transplantation in the United States.
Heart Allocation
Heart allocation in adults is determined by clinical observations and medical information, rather than a series of laboratory tests. Heart allocation is prioritized by medical urgency, with the highest priority for transplantation given to candidates who are sickest and using mechanical circulatory support devices for circulation and breathing (Table 5-2). This policy went into effect in 2018, adding additional stratification levels to the previous heart medical urgency statuses for a total of six categories (see Chapter 2). In addition to directing donated hearts to the most medically urgent candidates, the 2018 policy change altered the geographic distribution priorities for transplantation. Following the change, significant increases in regional and national distribution of donated hearts was observed coupled with a higher percentage of transplants going to candidates with a higher urgency status.10 This policy change also appears to have driven a change in strategies for managing patients on the waiting list, such as increased use of extracorporeal membrane oxygenation and temporary use of a ventricular assist device. For example, one study found that the use of temporary percutaneous endovascular mechanical circulatory support was an efficient, safe, and effective intervention for tier 2 candidates until a heart transplant could be received (Clerkin et al., 2022), potentially indicating a change in the heart transplant community’s practices of caring for patients prior to transplantation (Silvestry and Rogers, 2022). Another study compared the use of short-term mechanical circulatory support—an intervention as a bridge to transplant—before and after the 2018 heart allocation changes and found the use of this circulatory support increased and continued to expand following the allocation policy changes (Cascino et al., 2021). However, the increased use of short-term mechanical circulatory support was not consistent across transplant centers. While the allocation change may have had the intended effect of increasing access to transplantation for patients using this mechanical support, there could be variations in equitable access to heart transplantation due to the variations in transplant center behavior (Cascino et al., 2021).
In January 2020, the use of zones for heart and lung distribution was replaced with nautical mile (NM) fixed distance circles from the donor hospital. This change to using nautical
___________________
10 For more detailed information, see https://optn.transplant.hrsa.gov/media/3701/data_report_thoracic_committee_heart_subcommittee_20200227_rpt1_revised_508_compliant.pdf (accessed October 20, 2021).
TABLE 5-2 Heart Allocation System
| Allocation System | Factors and Variables |
|---|---|
| Heart (adult) | Using advanced support therapies, such as implanted medical devices to assist with circulation or breathing Required stay in hospital Experiencing complications from infection or blood clotting Using other support for circulation or breathing Using heart function-stimulating medication Experiencing difficult to control, life-threatening condition Needing one or more other organ transplants |
SOURCE: https://transplantliving.org/organ-facts/heart/heart-faq (accessed October 21, 2021).
miles for thoracic organ distribution was the first step toward a full continuous distribution policy.
Liver Allocation
Liver allocation in adults is determined by either three or four laboratory blood tests (Table 5-3) to calculate a MELD score. The MELD-based liver allocation system improves on the prior allocation system based on Child-Turcotte-Pugh classification and wait time, with advantages in objectivity, simplicity, and use of easily acquired standardized components (see Chapter 3). Similar to MELD, the PELD score is calculated to allocate livers to children aged 12 and younger using similar blood tests plus age and relative growth pattern (Table 5-3) (Lai, 2021).
Lung Allocation
Lung allocation is determined by the lung allocation score (LAS) (UNOS, 2021). The LAS is calculated from a number of factors, from clinical data or laboratory tests, and from daily-living factors like age or how easy it is to perform everyday tasks (Table 5-4). The LAS reflects the seriousness of each candidate’s medical status before transplant, as well as the likelihood of a successful transplant. It also estimates how long a patient will survive follow-
| Allocation Scoring System | Factors and Variables |
|---|---|
| Model for End-Stage Liver Disease (MELD) Liver (adult) | Serum creatinine Bilirubin International Normalized Ratio (INR) for prothrombin time Serum sodium |
| Pediatric End-Stage Liver Disease (PELD) Liver (pediatric) | Albumin Serum bilirubin INR for prothrombin time Growth failure (based on gender, height, and weight) Age at listing |
SOURCE: https://optn.transplant.hrsa.gov/data/allocation-calculators/about-meld-and-peld (accessed January 14, 2022).
| Algorithm | Factors and Variable |
|---|---|
| Lung Allocation Score (LAS) | Age at offer Bilirubin Bilirubin increase of at least 50% Body mass index Cardiac index prior to any exercise Central venous pressure Continuous mechanical ventilation, if candidate is hospitalized Serum creatinine Diabetes Diagnosis of lung ailment Predicted forced vital capacity Functional status Oxygen need to maintain saturation at rest pCO2 pCO2 increase of at least 15% Resting pulmonary artery systolic pressure 6-minute walk distance (with oxygen if needed) |
SOURCE: UNOS, 2021.
ing transplant relative to other patients on the waiting list (UNOS, 2021). Lung will be the first organ fully transitioned to continuous distribution allocation, beginning in early 2023.11
Intestine and VCA Allocation
Intestine and VCA transplants make up relatively small percentages of total annual transplants in the United States. The OPTN policies regulating allocation of these types of transplants are concordantly less complex than they are for many other types of transplants. Allocation for these types of transplants is primarily based on necessary medical support without transplant, clinical judgment or diagnoses, geographic distance from transplant hospitals, and length of time spent on the waiting list.
Additional Policies for Multiorgan Transplant Allocation
The OPTN currently has formal policies regarding allocation to heart–lung, liver–kidney, and kidney–pancreas multiorgan transplant candidates. For heart transplant candidates that also need a lung transplant, the heart is matched first and the lungs come from the same deceased donor. If a lung transplant candidate also needs a heart transplant, the lungs are matched first but the donated heart is first offered to transplant candidates in “allocation classifications 1 through 12.” In June 2021, the OPTN clarified policies surrounding multiorgan allocation to resolve issues with variation in OPO interpretations as to the prioritization of organ offers for the second required organ (kidney or liver), if available, from the same donor to a potential transplant recipient. The updated policy also increased the allocation prioritization for heart and lung multiorgan candidates from 250 to 500 nautical miles, to better align with thoracic allocation policies (OPTN, 2021a,b).
___________________
11https://unos.org/news/new-lung-allocation-policy-approved (accessed January 14, 2022).
Kidney Allocation
Estimating Kidney Function for Waiting List Prioritization12
For a patient to accrue waiting time points on the kidney transplant waiting list, they must either be on dialysis or have an estimated glomerular filtration rate (eGFR) that falls below 20 mL/min; eGFR is determined by serum creatinine, age, gender, and race. Serum creatinine levels in the body vary. In an attempt to account for this variability, eGFR has included race in its calculations. However, as discussed in Chapter 4 of this report, race is not defined by biology but is rather a social construct. Inclusion of race in eGFR has led to disparities in medical practice. For the same serum creatinine, a black patient will be wait-listed later than a patient of any other race or ethnicity, given the adjustment factor that is applied in the Chronic Kidney Disease Epidemiology Collaboration equation inflates the estimated kidney function of black individuals by approximately 16 percent (Ku et al., 2021; Zelnick et al., 2021).
Race and eGFR
The committee acknowledges that the use of race in eGFR is and has been part of a larger debate about the continued use of race-based medicine in health care (AABA, 2021; American Society of Human Genetics, 2020).13 Using race in clinical equations generally, and in transplant clinical equations specifically, poses urgent ethical and scientific challenges. Because the concept of race has no scientific basis, retaining race as a variable in clinical equations is unethical and can reinforce and perpetuate structural racism (Emanuel et al., 2000). Chapters 4 and 5 have explored inequities among racial and ethnic groups throughout the process of organ transplantation, from end-stage organ failure to posttransplant outcomes. As stakeholders in the organ transplantation system move toward a more equitable system that better addresses the needs of minority and underserved populations who have experienced limited access to transplantation and worse transplant outcomes, reevaluating the use of race in eGFR and other clinical equations (e.g., KDPI) is warranted. Indeed, many organizations and groups have been working toward this end, including a National Kidney Foundation/American Society of Nephrology (NKF/ASN) taskforce, the OPTN and Health Resources and Services Administration (HRSA), as well as research supported by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health (NIDDK) (OPTN Minority Affairs and Kidney Transplantation Committees, 2021).
The NKF/ASN taskforce recently examined alternatives to race-based estimations of kidney functions and evaluated the effects of including race in eGFR estimations. After a careful deliberative process, the taskforce concluded that revising the current eGFR calculations to remove race was an immediate first step that could reduce disparity, as well as yielding other
___________________
12 The text in this section was modified after release of the report to clarify that it refers to criteria for waiting list prioritization and not to criteria for registering for the list.
13 In defining race-based medicine, the American Academy of Family Physicians (AAFP) states that “Race is a social construct that is used to group people based on physical characteristics, behavioral patterns, and geographic location. Racial categories are broad, poorly defined, vary by country, and change over time. People who are assigned to the same racial category do not necessarily share the same genetic ancestry; therefore, there are no underlying genetic or biological factors that unite people within the same racial category. By using race as a biological marker for disease states or as a variable in medical diagnosis and treatment, the true health status of a patient may not be accurately assessed, which can lead to racial health disparities. AAFP opposes the use of race as a proxy for biology or genetics in clinical evaluation and management and in research. AAFP encourages clinicians and researchers to investigate alternative indicators to race to stratify medical risk factors for disease states.” https://www.aafp.org/about/policies/all/racebased-medicine.html (accessed November 15, 2021).
medical benefits. For all individuals at high risk of developing chronic kidney disease, the task force recommended widespread use of a new measure that incorporates a blood test for cystatin C along with serum creatinine in the calculation; this would improve the accuracy of estimation over either individual measure without adversely affecting any populations (Delgado et al., 2021). A study funded by the NIDDK based on the Chronic Renal Insufficiency Cohort (CRIC) registry similarly recommended use of cystatin C in calculating eGFR based on analyses of the CRIC data under several conditions (Hsu et al., 2021).
Conclusion 5-3: Use of race in eGFR estimations is one factor leading to systematic underestimation of kidney disease severity in black individuals. This results in health inequities in that black patients have to wait longer for transplants, are sicker than other patients when they get a transplant, and disproportionately die of kidney disease.
Race and KDPI
Given current scientific evidence and the recent advice to remove race from eGFR (Delgado et al., 2021), it is appropriate for the scientific community to continue efforts to develop and refine clinical equations so they do not include race as a variable. Some on the committee wanted to recommend the immediate removal of race from KDPI and other clinical equations because race is a social construct, lacks a biological basis, is not scientifically founded, and perpetuates racialized medicine (Ioannidis et al., 2021). Thus, as an unscientific variable, continuing to use race would be unethical (Emanuel et al., 2000). For these reasons, some on the committee argued race should neither be used in medical practice nor used as a biological proxy and that this committee should recommend the immediate removal of race from KDPI. Others on the committee were hesitant to recommend complete removal of race in these equations because of having insufficient information on the unintended consequences of doing so. Some committee members also felt that the issue was not a particular focus of this committee’s charge and would be better assessed by a properly constituted group of subject matter experts with specific instructions for considering the use of race in KDPI and other clinical equations. Based on the available information the committee believes that to achieve a more equitable organ transplantation system race should be eliminated from any equation or measurement used to determine access to the waiting list or eventual transplant (e.g., KDPI), understanding that doing so might have unintended consequences. The potentiality of such consequences needs to be considered by a group of experts knowledgeable in the multiple dimensions of this matter. The HHS should expeditiously convene such an expert group.
While the organ transplantation system moves toward a vision of non-race-based measures in assessing kidney function, some have suggested that
- Changing practice guidelines will require significant education efforts within health systems and consideration of the increased number of patients that may be classified with chronic kidney disease (Ahmed et al., 2021). The authors suggest further study to better define whether differences in creatinine-based eGFR are based on social or ancestry factors and advocate for increased transparency with patients if race-adjusted eGFR is used.
- There will be many short- and long-term consequences that should be addressed, including access to clinical trials (Delgado et al., 2021), antibiotic dosing (Eneanya et al., 2019), patients being classified with advanced stage kidney disease, and implications for health insurance (Ahmed et al., 2021).
- There may also be a number of benefits including increasing referral rates to special-
- New equations should be developed using scientifically validated variables such as height and weight, while more research should be done to ascertain the potential benefits and harms of eliminating race in eGFR calculations (Eneanya et al., 2019).
- Use a stepped approach that incorporates patient voices and moves toward an evidence-based solution in the long term (Powe, 2020). Variability across institutions may create more confusion and unreliable trends.
ists, reducing disparities in access to a transplant waiting list, and the potential for better management of chronic kidney disease (Powe, 2020).
As highlighted in Chapter 4, black patients experience disproportionate rates of kidney disease compared to white patients yet have less access to specialist care. While black populations make up approximately 13 percent of the U.S. population, adjusted prevalence of end-stage kidney disease was 3.4 times higher than white individuals in 2018 (USRDS, 2020). Black patients with chronic renal insufficiency also progressed through end-stage renal disease at five times the rate of whites with chronic renal insufficiency, which suggests that a refinement of the NKF chronic kidney disease (CKD) classification for stages of CKD may be warranted given the differences in progression among black and white patients (Hsu et al., 2003). Important strategies for slowing CKD progression include hypertension management and albuminuria management. Early referral to nephrologists is associated with improved CKD patient outcomes, but there are known disparities by race in referral (Gander et al., 2018).
Conclusion 5-4: Non-race-based ways of measuring organ function are greatly needed and deserve prioritization by federal agencies to set the standards for what is scientifically and ethically acceptable in determining patient prioritization for the transplant waiting list and eventual transplantation.
Conclusion 5-5: Using race in surveillance approaches for measuring outcomes across populations is useful for identifying the existence and persistence of disparities. However, researchers need to provide the rationale for how and why race is used in any such analysis.
Predialysis Wait Time
In the current allocation system, a transplant candidate’s access to transplantation before beginning dialysis (predialysis) is determined by the time of registration on the waiting list. The U.S. kidney allocation system currently gives priority “waiting time” points for years on dialysis but simultaneously allows unlimited predialysis “waiting time” points to accumulate. This substantially advantages white, educated individuals with private insurance who are able to gain timely access to transplant referral and join the waiting list before beginning dialysis (King et al., 2019; Reese et al., 2021). Black and Hispanic patients are approximately four times less likely to receive a preemptive transplant (Figure 5-3). Furthermore, candidates with longer dialysis time are at a higher risk of death without a transplant (Aufhauser et al., 2018); therefore, transplanting individuals already on dialysis saves more lives than preemptive transplants.
Prior to implementation of the KAS in 2014, transplantation candidates preemptively entered on the waiting list with a qualifying eGFR accrued waiting time from their listing date onward, while candidates wait-listed after starting maintenance dialysis accrued waiting time from their listing date onward.
One of the goals of the KAS was to improve equity in organ allocation for candidates
who were wait-listed after spending years undergoing dialysis. In the current policy, candidates wait-listed after the onset of maintenance dialysis accrue a priority point for each year of prelisting dialysis. However, candidates wait-listed before dialysis onset (preemptive wait-listing) continue to receive a point for each year waiting after reaching the qualifying eGFR of 20 (Harhay et al., 2018).
The revisions to the kidney allocation system also prioritized deceased donor kidney transplantation for candidates with long dialysis durations. Early studies have shown that the KAS has been successful in closing the gap in transplant rates between wait-listed white and minorities. Preemptive transplants have not experienced the same closing of the gap (Figure 5-3). In 2019, 11 percent of all adult deceased donor kidney transplants nationwide were preemptive. White patients received 65 percent, and black patients received only 17 percent of those preemptive kidneys, though the waiting list was made up of 38 percent white and 31 percent black patients (Reese et al., 2021). Also in 2019, 48 percent of wait-listed white patients, but only 22 percent of wait-listed black patients, began to accrue waiting time priority before dialysis (Reese et al., 2021).
A first-come, first-served approach that allows transplant priority to accrue for patients prior to the point of dialysis initiation is not in line with equity (Reese et al., 2021). Patients who already have advantage with both residual kidney function and greater ability to navigate the health system (primarily white, educated, privately insured) get greater access.
It is also the case that black patients with elevated creatinine will have a higher eGFR (thereby making them ineligible for wait-listing) but nonetheless may need kidney transplantation sooner than similar white patients because of rapid disease progression.
Another consideration for preemptive transplant is long-term management of patients who have already received a kidney transplant. It is common for transplant recipients to experience failure of their donated kidney; on average, more than half of transplant recipients experience loss of their donated kidney within 10 years. Emotional effects of this loss notwithstanding, there are also many medical decisions to make to best manage disease including a decision about whether or not to enroll on the waiting list for a new transplant.
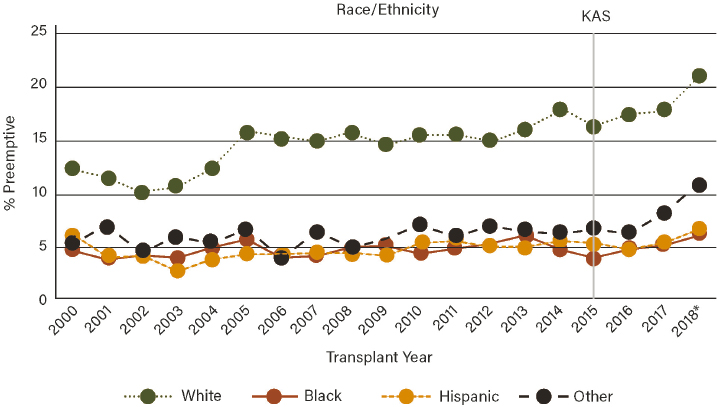
SOURCE: King et al., 2019.
Repeat transplant patients are enrolled on the waiting list at lower rates than would be expected given their and their clinicians’ familiarity with the system. There were about 4,000 patients in 2019 or just under 11 percent of the total waiting list (Davis and Mohan, 2021).
Many countries require that a patient must be on dialysis in order to be added to the waiting list (although different policies may apply to children or multiorgan transplant candidates).14 The criteria to start dialysis for end-stage kidney disease is regulated tightly by the Centers for Medicare & Medicaid Services (CMS) in the United States. It is possible that removing predialysis wait time from the kidney allocation system could reduce structural racism in kidney allocation and save more lives. It would be important that any policy change not ban preemptive deceased donor kidney transplants, but rather represent that these transplants may confer less benefit than transplanting patients with significant dialysis time. For example, preemptive deceased donor transplants could still occur if the candidate had a high enough priority based on the other components in the kidney allocation system. It would also be important that any policy change have no direct effect on candidate listing for planned living donor transplantation by inadvertently disincentivizing or limiting this type of transplantation.
A recommendation to remove waiting time was made in the 1999 Institute of Medicine report Organ Procurement and Transplantation for Liver Allocation under Recommendation 2 and read: “Discontinue use of waiting time as an allocation criterion for patients in statuses 2B and 3.” This recommendation was instrumental in the transition to a MELD-based liver allocation system. Similarly, removing preemptive waiting list time as a factor in kidney allocation policies could (1) improve access for patients on dialysis by making available deceased donor kidneys that were previously going to individuals who had not yet started dialysis; (2) improve equity in access to a transplant for individuals previously disadvantaged; (3) increase living donation as patients previously advantaged by preemptive access to deceased donor kidneys would seek living donation if they wish to receive a preemptive transplant; and (4) align with the intention of some other countries without completely limiting access to the waiting list to only those who have started dialysis as some other countries do. It is important to note that the committee’s recommendation is not to categorically eliminate preemptive transplants with deceased donor kidneys. These preemptive transplants would still be possible if the candidate has accrued a sufficiently high allocation priority via other mechanisms in the kidney allocation system (i.e., high CPRA, proximity to the donor, prior living donor points). It is also important to note that children do not typically tolerate lengthy time on dialysis very well (de Galasso et al., 2020; Verghese, 2017), so a policy change may need to exempt pediatric patients.
Ultimately, national efforts to advance early recognition of kidney disease are needed such that individuals needing a transplant are able to access the waiting list in an equitable manner. All transplant candidates—minorities, individuals without private health insurance, and those with limited access to the health care system—deserve access to transplantation based on their medical need. While this longer-term goal (see Recommendation 1) is advanced, the elimination of predialysis waiting time points is an immediate policy lever to increase equity and efficiency in the transplantation system.
Conclusion 5-6: Although the new kidney allocation system may be narrowing transplant rates between white and ethnic minority populations, a large disadvantage remains in access to preemptive transplants, in large part because of the accumulation of waiting time points for predialysis wait time.
___________________
14 Much of this section is excerpted or slightly modified from a paper commissioned by the committee for this study (Parker et al., 2021). Commissioned papers are in the study’s public access file and are available upon request from the National Academies’ Public Access Records Office (paro@nas.edu).
Conclusion 5-7: The use of a single tool, eGFR, measured at one point in time to determine kidney function and an individual’s eligibility for the waiting list, is inadequate and does not appropriately account for the rapidity with which a patient’s condition is likely to decline and have an urgent need for transplantation.
Conclusion 5-8: Transplant centers can also select one of three eGFR measures to determine kidney function; this can greatly affect an individual’s access to the waiting list and thereby increase the accident of geography.
Wait-Listing and the Kidney Allocation System
In general, the Scientific Registry of Transplant Recipients (SRTR) holds that when considering the distribution of a scarce resource such as donated kidneys, the methods must be derived from and based upon sound ethical principles, including the two key principles of utility and equity (Table 5-5). As previously mentioned, the KAS was implemented in 2014 by the OPTN to address high rates of procured organ nonuse and variability in access to organ transplantation. The KAS also attempts to match the amount of time donated kidneys are expected to function with estimated transplant recipient length of life, in some cases. For instance, kidneys with the longest expected function are allocated to the individuals with the longest expected lifetime—after initial allocation to multiorgan recipients and children—via metrics of EPTS and the KDPI (Table 5-6). The majority of the kidneys are still allocated primarily by length of time on the waiting list. The KAS also assigns additional priority to highly sensitized transplant candidates to give them access to the national donor pool via the CPRA metric (Table 5-6). In 2019, additional changes to the policy were approved to allow kidney distribution based on geographical distance between donor and recipient, as opposed to the previous policy where match sequencing relied on donation service area and the OPTN region.
Within its first year, the KAS reduced age mismatch between donated organs and transplant recipients, and increased transplant access for previously disadvantaged patients, such as highly sensitized candidates or those who had been on dialysis for long periods Wang
TABLE 5-5 Guiding Principles Considered in the Redesigned Kidney Allocation System
| Proposed Goals of the Kidney Allocation System (KAS) | Ethical Principle Addressed |
|---|---|
| More accurately estimate graft and recipient longevity to maximize the potential survival of every transplanted kidney and to provide acceptable levels of access for candidates on the waiting list. | Utility/Equity |
| Promote posttransplant kidney function for candidates with the longest estimated posttransplant survival who are also the most likely to require additional transplants because of early age of ESRD onset. | Utility |
| Minimize loss of potential functioning years of deceased donor kidney grafts through improved matching. | Utility |
| Improve the efficiency of the offering system and organ use through the introduction of a new scale for kidney quality, the Kidney Donor Profile Index. | Utility |
| Reduce differences in transplant access for populations described in the National Organ Transplant Act (e.g., candidates from racial/ethnic minority group, pediatric candidates, and sensitized candidates). | Equity |
SOURCE: https://www.srtr.org/media/1072/friedewald_the_kidney_allocation_system_surg_clin_n_am_2013.pdf (accessed January 20, 2022).
| Algorithm | Factors and Variables |
|---|---|
| Calculated panel reactive antibody (CPRA) | Calculates unacceptable human leukocyte antigens to measure a transplant candidate’s sensitization level and likelihood of the presence or intensity of acute or antibody-mediated rejection. Transplant programs define unacceptable antigens for each transplant candidate, and there is variation in the definition among different transplant centers. |
| Estimated posttransplant survival (EPTS) | EPTS factors include (1) candidate time on dialysis, (2) diabetes diagnosis, (3) prior solid organ transplantation, and (4) age. |
| Kidney Donor Profile Index (KDPI) | Age History of diabetes Height Cause of death Weight Serum creatinine Race or ethnicity Hepatitis C virus (HCV) status, from serological or NAT testing History of hypertension Donation after circulatory death (DCD) status |
SOURCES: https://optn.transplant.hrsa.gov/learn/professional-education/kidney-allocation-system (accessed January 15, 2022); https://optn.transplant.hrsa.gov/resources/allocation-calculators (accessed January 15, 2022); Cecka, 2010.
(et al., 2017). However, despite these accomplishments, rates of kidney nonuse were not reduced. Because there are many more transplant candidates than there are donated organs, the KAS and its underlying principles prioritize allocating kidneys to younger and healthier candidates (Table 5-5).
EPTS and KDPI15
The EPTS score is assigned to all adult candidates on the kidney waiting list as part of the KAS. Its intent is to match high-quality organs to candidate recipients with the best estimated survival following transplant, and it is calculated relative to all candidates on the waiting list (Chopra and Sureshkumar, 2015).
The EPTS is used with the KDPI to introduce the concept of longevity matching into the new allocation system. Only candidates with EPTS scores of 20 percent or less will receive increased priority for offers for kidneys with KDPI scores of 20 percent or less, meaning that in the context of these two calculations, the 20 percent of highest-quality donated kidneys are prioritized to candidates with the longest estimated survival after transplantation. For the remaining 80 percent of kidney allocations, EPTS is not used at all. Independent assessment of how EPTS performs judged it to be a “moderately good tool for discriminating posttransplant survival of adult kidney-only transplant recipients” by testing the algorithm on Australia and New Zealand’s combined dialysis and transplant registry (Clayton et al., 2014). Allocation proceeds by geography and local candidates—even those with an EPTS score exceeding 20 percent—appear on the match list before candidates listed outside the donor service area.
The KDPI score estimates the risk of graft failure, and it is intended to help assess the suitability of donated kidneys for particular patients as well as with longevity matching. KDPI is a scoring system based on 10 donor factors as a screening tool for donor quality and has been shown to be generally predictive of both short- and long-term graft survival, and though it may have other shortcomings it has the advantage of creating a sliding scale of assessment rather than a distinct decision, as with the standard criteria donor/extended criteria donor designations it replaced.
This longevity matching in allocation has two effects: (1) younger and healthier patients on the waiting list are prioritized to receive the kidneys that are expected to survive the longest posttransplant, and (2) medically urgent candidates receive kidneys with lower estimated survival posttransplant, which potentially worsens the patient’s long-term outcomes.
Other countries do not use KDPI as a consideration in their allocation decisions. For example, Alexandre Loupy and colleagues estimated that the U.S. rate of nonuse for procured organs is nearly double the rate in France (Aubert et al., 2019). France tends to use donated kidneys with higher KDPI, largely driven by use of organs from older donors, and transplanted patients still realize significant survival benefit.
Conclusion 5-9: The United States is alone in constructing its allocation policies around a single measure of kidney quality (KDPI), which reduces the number of deceased donor transplants without improving average outcome. This results in fewer total transplants than would occur if these patients had access to donated kidneys that are expected to produce better results. The committee concludes that constructing U.S. allocation policies around KDPI is an inappropriate focal point that does not exist in other countries and may lead to perverse regulatory incentives for U.S. transplant centers to be overly selective and risk averse in the kidneys they choose to transplant. As a result, many opportunities are missed to provide transplantation to a greater number of individuals on the waiting list.
___________________
15 Much of this section is excerpted or slightly modified from a paper commissioned by the committee for this study (Ku, 2021). Commissioned papers are in the study’s public access file and are available upon request from the National Academies’ Public Access Records Office (paro@nas.edu).
SURVIVAL BENEFIT OF TRANSPLANTATION
The survival benefit of transplantation is the counterfactual difference between a patient’s estimated survival with transplantation and without transplantation. Traditionally, the benefit of transplantation has been restricted to posttransplant survival, typically 1-year posttransplant survival. This is a measure of graft survival, and maximizing 1-year graft survival leads to the selection of the healthiest candidates and most viable organs. By contrast, survival benefit measures additional lives saved by comparing the expected waiting list survival to the expected posttransplant survival for a given patient and organ dyad, in a given transplant center. Maximizing survival benefit may lead to the selection of the most medically urgent16 candidates that still have high likelihood of posttransplant survival.
The survival benefit of deceased donor organ transplantation has been quantified in lung (Vock et al., 2017), heart (Parker et al., 2019; Singh et al., 2014), liver (Luo et al., 2018), and kidney (Merion et al., 2005; Pérez-Sáez et al., 2016; Wolfe et al., 1999). The current kidney transplantation system conveys a significant overall 5-year survival benefit of 31.6 percent (50.8 percent survival associated with remaining on the waiting list versus 82.4 percent associated with transplantation). Nevertheless, survival benefit varies widely from 24 to 39 percent owing to variation in candidate characteristics. Similarly, survival benefit varies widely across transplant centers, from 20 to 48 percent for a median KDPI kidney (KDPI = 43 percent) (Parker et al., 2021).
During the course of the committee’s work, the idea of survival benefit was introduced and seemed promising as a way to reduce inequities in the organ transplantation system. However, the committee—being acutely aware and mindful of the extent of the organ transplantation system’s complexity—understands that any change of this magnitude could introduce both intended and unintended effects. The committee is also aware that the policy revision process is a laborious one that involves input from many stakeholders and thoughtful debate. There was disagreement between some on the committee about the degree to which statistical modeling should play a role in changing allocation. Nevertheless, a substantial amount of modeling and further work and testing would need to be done to verify the committee’s impression that this could be a step forward—rather than a rehashing of similar discussions that took place prior to implementation of the KAS in 2014—and also to identify potential unintended consequences that could undermine the intended change.
Further evaluation of survival benefit through simulation and further studies should be undertaken expeditiously. Given the magnitude of potential benefit to patients and possibility to reduce inequity, sufficient evidence should be accrued within the next 3 years to determine whether further incorporating a survival benefit metric into allocation decisions for all organs—but especially kidneys—could be made by that time.
Conclusion 5-10: If transplant centers are ranked based on 1-year survival of transplant recipients, any measure of organ quality will result in organ nonuse based on
___________________
16 According to OPTN policy, a new definition of the medically urgent classification within all kidney allocation categories “creates priority for candidates at imminent risk of death due to an inability, or anticipated inability, to accept dialysis treatment for renal failure” (OPTN, 2020a). While the committee recognizes this as the OPTN definition for medically urgent classification for kidney transplant patients, the committee defines medical urgency in this report differently than the OPTN (Parker et al., 2021). This committee’s definition of medical urgency is “risk of death without receiving an organ transplant.” The committee recognizes that patients in renal failure without any viable dialysis access are certainly the candidates in the most dire need of transplantation. However, the kidney allocation system does not yet clearly allocate organs to the candidates with highest risk of dying without transplantation. Therefore, in order to align kidney allocation with the other organs, throughout the remainder of the report the term medical urgency refers to the “risk of death without receiving an organ transplant” and not the exhaustion of dialysis access options.
the assumption that they will lower a center’s ranking and increase costs. A ranking system is needed that is based on saving lives, not 1-year graft survival, and a reimbursement system is needed that acknowledges the importance of reimbursing transplant centers for the increased costs associated with transplanting lifesaving medically complex organs.
Constructing a Good Survival Benefit Estimator
Survival benefit is not a new concept (Massie et al., 2014). Prior to implementing the KAS, the OPTN and the transplant community considered survival benefit as a basis for kidney organ allocation, but they rejected the idea when the calculation proposed was found to favor younger and healthier candidates in contrast to the HHS Final Rule. However, there may be other ways to estimate survival benefit that are less likely to favor younger, healthier candidates and that could improve the efficiency of kidney allocation. First, by focusing on a finite time interval, it is possible that more medically urgent candidates with high waiting list mortality will derive increased benefit from a transplant relative to remaining on the list than young healthy candidates whose waiting list mortality is more similar to their posttransplant survival. Second, survival benefit is not constant over time; rather, it varies significantly from the short term to the long term, and any improved model would reflect this variation. Third, there is variability in survival benefit among transplant centers (Parker et al., 2019, 2021). A good survival benefit estimator would include adjustment to estimated survival benefit for a given candidate that is specific to the transplant center at which that person is listed. Fourth, a good survival benefit estimator should include detailed candidate characteristics (e.g., age, diabetes, dialysis time, prior transplantation) and donor characteristics (e.g., KDPI or an improved estimator of quality of the donor organ) and allow them to interact in producing a survival benefit estimate. The more detailed the measured characteristics, the better the estimator. A limitation of the current KAS is that many important characteristics of the candidate and donor are not routinely collected (e.g., cardiac risk).
Conclusion 5-11: Better estimators of survival benefit, focusing on saving more lives, are available and would benefit from being reviewed by the SRTR via simulation to determine their operating characteristics relative to the current KAS allocation system.
Conclusion 5-12: The concept of survival benefit, the difference between estimated waiting list and posttransplant survival over a fixed interval of time, focuses on saving more lives relative to the current metric of 1-year graft survival. The use of survival benefit has the potential to improve allocation, center rankings, and share decision making between transplant candidates and transplant teams. The application of a survival benefit is particularly relevant to kidney allocation, where allocation is based largely on histocompatibility and waiting time regardless of medical urgency.
Racial Disparities
As discussed in Chapter 4, disparities research often focuses on differences in care for black and white patients, and other ethnic and racial groups receive less research focus. Racial disparities between black and white patients are discussed here with the understanding that additional research on the effects of allocation changes in other ethnic and racial groups is needed.
Prior to the implementation of the KAS in 2014, dialysis time prior to wait-listing was ignored by the allocation system. In fact, structural racism in health care often prevents black patients from accessing transplant centers for listing in the first place (Gander et al., 2018; Joshi et al., 2013; Peng et al., 2018). Racial disparities in dialysis time at transplant persisted between 2010 and 2020 despite the implementation of the KAS in 2014. In 2013, the median dialysis time at transplant for a white recipient was 2.6 years compared to 4.5 years for black recipients. In 2019, the median dialysis time at transplant for a white recipient was 2.5 years compared to 4.8 years for black recipients (Joshi et al., 2013). The KAS did reduce the race gap in transplant rate (Melanson et al., 2017), likely because of a backlog in minority candidates with very long dialysis times who finally got credit for the years they suffered waiting. The racial disparity in rates of preemptive transplants has continued to increase since the implementation of the KAS. In 2020, the rate was 20 percent for whites and only 7 percent for black patients, a disparity that has only worsened since implementation of the KAS in 2014 (Patzer et al., 2009).
Survival benefit increases with increasing dialysis time. Therefore, minorities who enter the waiting list with almost twice the dialysis time could have a higher likelihood of receiving a kidney offer if allocation is based on survival benefit rather than 1-year posttransplant survival, for which their rates are lower and lead to increased racial disparity because of existing allocation algorithms.
Conclusion 5-13: Black candidates enter the kidney transplant waiting list with double the length of dialysis time than white candidates and as a consequence have increased medical urgency as evidenced by their increased risk of mortality without transplantation. Under the current allocation system, which focuses on 1-year posttransplant survival and waiting list time, the disparity will persist. There is need to understand whether a shift in allocation policy to survival benefit would prioritize those populations currently disadvantaged because of their increased waiting list mortality.
Longevity Matching17
In the KAS, candidates with low scores on the high EPTS measure are given priority for the top 20 percent KDPI kidneys. The KAS was designed in this manner to better match the life span of an organ with the life span of the recipient (i.e., longevity matching). While this policy may extend total graft survival, it may also lower the total number of lives saved by the KAS because healthier transplant candidates receive the higher-quality kidneys. Overall, the top 20 percent EPTS candidates have much lower estimated survival benefit than the top 20 percent most medically urgent candidates. Transplanting the median patient without diabetes after the median amount of dialysis time (3.8 years of dialysis) was associated with 5-year survival benefit of 32 percent compared to only 19 percent for preemptively transplanting the same patient (i.e., dialysis time of 0, see Figure 5-4). This translates to more than 1 life saved for every 10 transplants performed in dialysis recipients compared to preemptive transplant recipients. Figure 5-4 illustrates the survival benefit of transplantation for a 55-year-old recipient without diabetes—transplanted after 3.8 years of dialysis and 848 days of waiting list time—compared to preemptively transplanting the same patient after 433 days of waiting
___________________
17 Much of this section is excerpted or slightly modified from a paper commissioned by the committee for this study (Parker et al., 2021). Commissioned papers are in the study’s public access file and are available upon request from the National Academies’ Public Access Records Office (paro@nas.edu).
list time. The preemptive transplant recipient has higher 5-year posttransplant survival (93 percent vs. 88 percent), but transplantation is significantly less urgent than the recipient on dialysis (survival without transplant 73 percent vs. 56 percent). In combination, this means the patient on dialysis experiences a much greater benefit from transplantation (32 percent) compared to the preemptive recipient (19 percent). This raises important questions regarding the effectiveness of longevity matching.
Furthermore, the top 20 percent most urgent candidates experience a greater benefit from lower KDPI kidneys than the top 20 percent EPTS candidates. For both a 15 percent and 85 percent KDPI kidney, allocation to the top 20 percent most medically urgent candidates produces large increases in survival benefit relative to the longevity matching (top 20 percent EPTS recipients). The difference in 5-year survival benefit between receiving a 15 percent versus an 85 percent KDPI kidney is near zero for the top 20 percent EPTS recipients, but 7 percent greater for the 15 percent KDPI kidney relative to the 85 percent KDPI kidney for the top 20 percent most medically urgent recipients. These data suggest that longevity matching—at least through 5 years posttransplant—is having the opposite of its intended effect. Relative to receiving a high KDPI kidney, lower KDPI kidneys produce greater survival benefit for sicker recipients than they do for the younger and healthier EPTS recipients.
Finally, with respect to the use of KDPI in general, there was a small but statistically significant decrease in posttransplant survival with higher KDPI kidneys. For every 10 percent increase in KDPI, 5-year survival benefit decreased by 1 percent. However, kidneys with a KDPI greater than 85 percent were associated with a 5-year survival benefit of 28 percent, which is still an appreciable benefit of transplantation relative to remaining on the waiting list. In 2019, there were 1,356 transplants performed using donor kidneys with a KDPI of 85 percent or more. If these transplants had not been performed, an estimated 377 candidates would have died within 5 years.
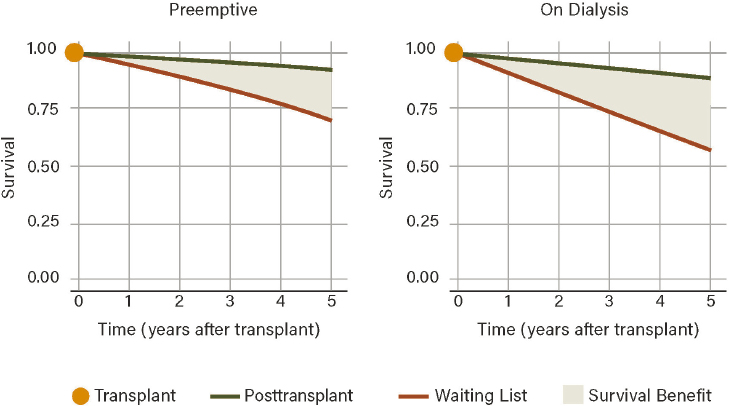
NOTE: Survival benefit of transplantation for a 55-year-old recipient without diabetes transplanted after 3.8 years of dialysis and 848 days of waiting list time (survival benefit = 32%) compared to preemptively transplanting the same patient after 433 days of waiting time (survival benefit = 19%).
SOURCE: Parker et al., 2021.
Conclusion 5-14: The current kidney allocation system includes longevity matching of the highest-quality kidneys (top 20 percent KDPI kidneys) with the healthiest candidates on the transplant waiting list. This policy gives priority for the highest-quality kidneys to younger and healthier patients on the waiting list who are estimated to have the longest survival posttransplantation. While this policy increases overall graft survival, it may save fewer lives than allocating these high-quality kidneys to the most urgent candidates.
Survival Benefit as a Potential Tool for Organ Allocation
In addition to facilitating greater acknowledgement and incorporation of patient preferences in accepting or declining organ offers, survival benefit could potentially be used to inform changes to allocation policy more broadly. CMS and the OPTN regulate transplant program performance primarily through 1-year posttransplant patient and graft survival (Parker et al., 2019; Singh et al., 2014). Focusing on posttransplant survival does not account for health lost while waiting for transplant—which is particularly important for medically urgent candidates who are at higher risk of death or deterioration and who tend to lose health more rapidly—and reduces the efficiency of deceased donor kidney allocation. This regulatory pressure creates an incentive to prioritize the healthiest candidates. This regulation also promotes excess selectivity of donors, leading transplant programs to not use one in five procured deceased donor kidneys recovered for transplantation owing to an incorrect perception of low quality. In contrast, allocation based on survival benefit could prioritize medically urgent patients with decreased waiting list survival. Such an allocation system would actively counter the disparities in access to transplantation that lead to minority candidates entering the waiting list with greater medical urgency.
- also be reviewed to ensure that the best performance possible is achieved and that they are properly validated using data not used to derive the prediction models.
- Modify the MELD scoring system for liver allocation and prioritization or establish an alternative overall prioritization scheme to include a modifier based on body size or muscle mass to overcome the demonstrated disparities observed for patients of smaller size.
- Immediately implement the recommendations of the National Kidney Foundation and American Society of Nephrology joint task force to use the revised equation, which eliminates race, in calculating eGFR for all individuals and to use the revised equation for high-risk individuals that incorporates a blood test for cystatin C along with serum creatinine.
- Require the OPTN to ensure that all laboratories in the transplantation system become capable of conducting validated cystatin C tests within 12 months.
- Resolve the use of race in KDPI and other clinical equations. Within 12 months HHS should make a decision on the continued use of race in KDPI and how best to eliminate race from KDPI and other clinical equations used in organ allocation and access.
- Continue to gather data on factors that may result in disparities in access to, and outcomes of, organ transplantation (e.g., socioeconomic status, place of residence, access to health care, race and ethnicity, presence in patient or family of stressors caused by racism) and use such data to determine whether faster progression to end-stage kidney disease is experienced by patients with any particular factor or combination of factors, and if so whether this evidence should be used to establish a new threshold for listing on the transplant list and for allocation of an organ for transplantation.
MODELING ALLOCATION POLICY CHANGES
The current process for modeling allocation policy begins when the OPTN notices a problem with waiting lists, such as the case study in geographic disparities in liver allocation (Mulligan, 2021). The OPTN takes into account factors such as organ transportation time limits, geographic boundaries of service areas, organ donation rates, transplantation rates, when in their disease patients enter the waiting list, and variation in how likely a patient is to die or be removed from the waiting list for being too sick. The OPTN determines the most pressing underlying problem and requests models of how different policy changes might affect those numbers from the SRTR. The OPTN agrees on practical parameters to restrict the modeling to solutions that are feasible, such as a minimum number of districts in a sharing area to make sure donated livers were not traveling for longer than transportation time limit. With a few options for changing policy, the OPTN conducts community forums to gather feedback on those potential changes from patients, transplant centers, OPOs, and other stakeholders in the transplantation community. IT then iterates the proposed changes with this feedback to update the models and present a “concept document” and a recommendation for proposed changes to the OPTN board of directors.
The SRTR builds and updates simulated allocation models (SAMs) to model alternative organ allocation policies and predicted outcomes for patients on the waiting lists for each organ type. The models also predict patient outcomes following transplant. Currently, the SRTR maintains SAMs for liver, heart and lung together or separately as thoracic organs, and kidney and pancreas. The SAMs “use a variety of allocation rules to determine how organs would be allocated to potential recipients under each rule considered” (SRTR, 2019). The
models include and try to predict variation for factors in organ allocation such as individual accept/reject decisions or estimating life expectancy with or without receiving a transplant. SRTR is developing new simulation software, the Organ Allocation Simulator, that uses more modern coding language, cross-platform compatibility, and built-in parameters for error checking that will make the simulator more accurate and easier to use. As of October 2021, the Organ Allocation Simulator was not yet officially launched or accessible.
The data used to build all of these simulations come from the OPTN database of historical data of patients on the related waiting list over the past year, donated organs that became available in the same time frame, and characteristic organ offer acceptance practices (Snyder, 2021). The OPTN database collects only information on a patient’s name, gender, race/ethnicity (as 1 variable), age, ABO blood group, human leukocyte antigen, status codes, number of previous transplants, and acceptable donor characteristics. No information is collected regarding socioeconomic or patient-centered factors such as health care access, distance to a transplant center, perceived discrimination or trust (see Chapter 4), candidate cardiac risk factors, or information from donors including secondary diseases or conditions other than cause of death.
Other limitations of the current modeling system pertain to behavior change, as reported by Snyder (2021). The simulators do not capture behavior change in response to new allocation policies, nor do they predict behavior change when it comes to accept/reject decisions in the context of the policy change being modeled because of its basis in historical data. For example, in the case of modeling changing geographic boundaries in allocation, the existing models do not account for how the characteristics of eligible donors may change for a given transplant candidate in a revised geographic area. Moreover, the available data do not adequately capture instances when an offered organ is declined in the match run system. Lastly, Snyder highlighted a need for the simulations to model and account for predicted changes in behavior following a policy change, saying,
I often hear from the expert in the field that we know how behavior might change in response to this [new] policy. Can the simulator actually implement that change? We’d like to…develop modules so that the user of the simulator—[SRTR] or any independent researcher—could actually implement those behavior changes as suggested and show the [OPTN] committee how that might work.
The data on which some allocation algorithms are based are not frequently updated. For example, the current KDPI model is derived from deceased donor kidney transplants from 1995 to 2005 (OPTN, 2020b), likely rendering its predictions for transplants in 2021 biased. Even when it is clear an update is necessary, there are multiple-year delays. For example, including sodium significantly improved the accuracy of MELD (Kim et al., 2008). However, MELD was not updated to include this variable until 2016.
Conclusion 5-15: The process and output of modeling allocation policy changes would be improved by
- Addressing current gaps in OPTN data collection, including socioeconomic and patient-centered factors, transplant candidate cardiac risk factors, information about organ donors regarding secondary diseases or conditions, and meaningful justifications for when a donated organ is declined by a transplant team;
- Accounting and allowing for more predictive models that include effects from anticipated behavior changes following allocation policy implementation;
- Including metrics and analyses of the cost and any other associated economic implications of proposed allocation changes; and
- Running randomized controlled trials of major allocation policy changes when possible.
Conclusion 5-16: Equitable and efficient organ allocation in the United States relies on the performance of several multivariable prediction models, such as the KDPI, EPTS, and the MELD. The OPTN infrequently updates these scores, despite their critical role in rank-ordering candidates and donors.
INFORMATION TECHNOLOGY INFRASTRUCTURE OPPORTUNITIES
UNOS, a nonprofit, private voluntary organization, holds the subcontract for the OPTN and has been the sole administrator of the OPTN since the initial contract was awarded by HRSA in 1986 (see Chapter 2). The OPTN is responsible for matching donated organs with potential recipients at the national level. The specific contract ensures that
- the national organ waiting list is maintained,
- the information technology (IT) system operates to match organs with patients,
- system performance is monitored and based on transplant data gathered, and
- organ allocation policies are developed (Proctor, 2019).
Since 1986 there have been open opportunities for other organizations or entities to bid on the OPTN contract. However, the contractual needs of the IT system and the complex infrastructure needed to support the organ donation and transplantation system were significant barriers to some potential bidders. For example, some have argued that the short timeline for response, unreachable requirements for organizational experience for an entity other than UNOS, and overall uncertainty about the transition period for key software systems discouraged innovative approaches to the OPTN and competitive bids outside of UNOS (Gentry and Segev, 2019). In 2020, the Senate Finance Committee questioned UNOS’s presumed ownership of its IT, given funding with taxpayer dollars, and the perception of an incumbency advantage (U.S. Senate Committee on Finance, 2020). In 2021, the House of Representatives Appropriations Committee expressed encouragement for HHS to promote competition for the OPTN contract.18
The perceived risks and challenges to accomplishing the mission of the OPTN contract include
- time considerations (delays in implementing the Final Rule resulted in unforeseen time constraints that would make this contract challenging),
- financial considerations, and
- an unstable legal and regulatory environment (RAND, 1999).
In 2019, under an executive order from the president calling for improvements for those with end-stage kidney failure, HHS issued a request for information (RFI) regarding the OPTN IT infrastructure (HHS, 2019). The RFI established that it was in search of “ideas and
___________________
18Departments of Labor, Health and Human Services, and Education, and Related Agencies Appropriations Bill, 2022. 117th Cong., 1st sess. See pages 63-64 at https://docs.house.gov/meetings/AP/AP00/20210715/113908/HMKP-117-AP00-20210715-SD003.pdf (accessed February 4, 2022).
information about how to improve the national information technology system for matching transplantable organs and managing detailed, confidential medical data on transplant patients and organ donors” (HHS, 2019). In announcing HHS’s RFI on the OPTN technology, then-HHS Secretary Alex Azar said: “The Health Resources and Services Administration will issue a Request for Information about more effective ways in which modern IT systems may be able to manage allocating organs and handling patient and donor data on a national scale. We especially want to hear from entities that are capable of developing a system that is more effective than the one we have today” (HHS, 2019). Additionally, in 2020, an external analysis of UNOS’s technology, endorsed by all five past, bipartisan HHS Chief Technology Officers, concluded that “[UNOS] maintains an antiquated technology and limited technical acumen” (Bloom Works, 2020).
Many years ago, organ donation used to be managed by one man with one voice mail box (Crichton, 2021). In the early 1980s, Don Denny relied on messages left on his voice mail box to coordinate organ donations and matches. Nearly 2,700 transplants were conducted this way over a 4.5-year period (Crichton, 2021). By 1986, shortly after UNOS became incorporated, information technology was beginning to evolve which led to more computerized systems to deal with organ matching. In 2012, a large improvement came in UNOS’ adoption of a mobile application called TransNet, which allowed OPOs to “electronically package and label organs” reducing errors in handwriting and data entry mistakes (Crichton, 2021).
Committee Considerations
The committee considered the limited available evidence on the performance of the OPTN IT infrastructure as well as anecdotal end-user experiences, but gaps remain in the committee’s understanding of any specific enhancements to the IT system that have been made in recent years and generally how well the IT system is supporting the achievement of an equitable, efficient system of organ transplantation. If the IT system is unable to support the goals of the organ transplantation system then change is needed. The committee is aware that previously the OPTN contract was changed to separate out the data analysis function—a role currently implemented successfully through a HRSA contract for the SRTR.
Committee members recognize that potential changes and restructuring of the OPTN IT functions creates risk. The greatest risks are that the government contracts for a new, separate IT infrastructure to perform the organ allocation and other OPTN IT functions currently performed by UNOS, and the new system does not work or does not work properly. Healthcare.gov is a recent example in a long line of similar examples where government contracting for large IT systems resulted in initial failures that took time to overcome. The current organ transplantation IT system performs key functions every hour, and enables the matching of available organs with wait-listed candidates, using complex algorithms associated with transplant allocation for all organ types. The committee recognizes that great care must be taken to ensure the continued, effective lifesaving operations of any system used to perform the IT functions.
Committee members discussed several ways to manage the risks associated with procuring the IT functionality necessary to perform the basic and sophisticated operations of a system such as the OPTN. One of them was to operate the current UNOS IT infrastructure in parallel with the new IT infrastructure over a prescribed period of time in order to ensure that a fallback capability remains available as the new IT infrastructure comes online. It may be necessary to clarify that the National Organ Transplant Act (NOTA) authority would
permit the temporary operations of dual systems as part of potential transitions. Another way to mitigate risk is by contracting for agile system development where key basic IT functions are made operational in a new system; once the first several functions are operational, then additional functions are systematically developed and added over time. This approach ensures that the eventual complete system is functional from day 1 of its full operational status and not subject to catastrophic system development failure. While agile development is an effective way to prevent catastrophic failures associated with new, large IT systems, in the case of the OPTN, the existing IT infrastructure would most likely need to function alongside the agile development of the new one, which would involve funding considerations and potential statutory issues as well.
It may also be necessary for the government to use contracting mechanisms to create a stepped approach to ensuring government ownership and control of the existing IT functionality operated by UNOS. This becomes even more important if the government were to award a new contract to a non-UNOS organization to potentially operate the UNOS system as a backup during the development of a new and improved IT infrastructure.
The committee recognizes that competitive government contracting for IT systems is complex, and there are likely additional or other ways of mitigating risks beyond or instead of those outlined here.
Conclusion 5-17: While a significant amount of data are currently collected about various aspects of the transplantation system, few metrics are well defined, have consistent definitions, or aim to capture the patient experience. Opportunities exist to improve the types of data collected about the transplantation system to prioritize standardized, meaningful, patient-centered data to inform the development of performance measures for OPOs and transplant centers.
Conclusion 5-18: Significant improvements could be needed in the IT infrastructure underpinning the organ transplantation system to improve the efficiency and equity of organ allocation and make the system more user friendly.
- Immediately separate the IT infrastructure components from the remainder of the OPTN contract and institute a new competitive process for an IT services contractor. or
- Incorporate the identified improvements in the next OPTN contract bidding process in 2023. This could include smart approaches to mitigate potential system failure risks, separating the IT infrastructure components from the OPTN contract to address necessary improvements, and keeping the contract intact but with updated expectations for the winning contractor. or
- Pursue an alternative approach that would achieve the same desired outcome.
If HHS determines that separating the IT infrastructure from the current OPTN contract requires a change in the NOTA, then HHS should work with Congress to revise NOTA accordingly.
REFERENCES
AABA (American Association of Biological Anthropologists). 2021. AABA statement on race & racism. https://physanth.org/about/position-statements/aapa-statement-race-and-racism-2019 (accessed December 31, 2021).
Ahmed, S., C. T. Nutt, N. D. Eneanya, P. P. Reese, K. Sivashanker, M. Morse, T. Sequist, and M. L. Mendu. 2021. Examining the potential impact of race multiplier utilization in estimated glomerular filtration rate calculation on African-American care outcomes. Journal of General Internal Medicine 36(2):464-471.
American Society of Human Genetics. 2020. American Society of Human Genetics statement regarding concepts of“good genes” and human genetics. https://www.ashg.org/publications-news/ashg-news/statement-regarding-good-genes-human-genetics (accessed December 31, 2021).
Aubert, O., P. P. Reese, B. Audry, Y. Bouatou, M. Raynaud, D. Viglietti, C. Legendre, D. Glotz, J. P. Empana, X. Jouven, C. Lefaucheur, C. Jacquelinet, and A. Loupy. 2019. Disparities in acceptance of deceased donor kidneys between the United States and France and estimated effects of increased US acceptance. JAMA Internal Medicine 179(10):1365-1374.
Aufhauser, D. D., A. W. Peng, D. R. Murken, S. J. Concors, P. L. Abt, D. Sawinski, R. D. Bloom, P. P. Reese, and M. H. Levine. 2018. Clinical Transplantation 32(6):e13260.
Axelrod, D. A., and E. A. Pomfret. 2008. Race and sex disparities in liver transplantation: Progress toward achieving equal access? JAMA 300:2425-2426.
Bloom Works. 2020. Bloom Works: The costly effects of an outdated organ donation system: Technology recommendations. https://bloomworks.digital/organdonationreform/Technology (accessed February 2, 2022).
Cascino, T. M., J. Stehlik, W. S. Cherikh, Y. Cheng, T. M. F. Watt, A. A. Brescia, M. P. Thompson, J. S. McCullough, M. Zhang, S. Shore, J. R. Golbus, F. D. Pagani, D. S. Likosky, and K. D. Aaronson. 2021. A challenge to equity in transplantation: Increased center-level variation in short-term mechanical circulatory support use in the context of the updated U.S. heart transplant allocation policy. Journal of Heart and Lung Transplantation 41(1):95-103.
Cecka, J. M. 2010. Calculated PRA (CPRA): The new measure of sensitization for transplant candidates. American Journal of Transplantation 10(1):26-29.
Chopra, B., and K. K. Sureshkumar. 2015. Changing organ allocation policy for kidney transplantation in the United States. World Journal of Transplantation 5(2):38-43.
Clayton, P. A., S. P. McDonald, J. J. Snyder, N. Salkowski, and S. J. Chadban. 2014. External validation of the estimated posttransplant survival score for allocation of deceased donor kidneys in the United States. American Journal of Transplantation 14(8):1922-1926.
Clerkin, K. J., O. Salako, J. A. Fried, J. M. Griffin, J. Raikhelkar, R. Jain, S. Restaino, P. C. Colombo, K. Takeda, M. A. Farr, G. Sayer, N. Uriel, and V. K. Topkara. 2022. Impact of temporary percutaneous mechanical circulatory support before transplantation in the 2018 heart allocation system. JACC: Heart Failure 10(1):12-23.
Cogswell, R., R. John, J. D. Estep, S. Duval, R. J. Tedford, F. D. Pagani, C. M. Martin, and M. R. Mehra. 2020. An early investigation of outcomes with the new 2018 donor heart allocation system in the United States. Journal of Heart and Lung Transplantation 39(1):1-4.
Crichton, D. 2021. How technology is transforming organ procurement. https://techcrunch.com/2021/09/22/how-technology-is-transforming-organ-procurement/?guccounter=1 (accessed November 1, 2021).
Davis, S., and S. Mohan. 2021. Managing patients with failing kidney allograft. Clinical Journal of the American Society of Nephrology 17(3):444-451. https://doi.org/10.2215/cjn.14620920.
de Galasso, L., S. Picca, and I. Guzzo. 2020. Dialysis modalities for the management of pediatric acute kidney injury. Pediatric Nephrology (Berlin, Germany) 35(5):753-765.
Delgado, C., M. Baweja, N. R. Burrows, D. C. Crews, N. D. Eneanya, C. A. Gadegbeku, L. A. Inker, M. L. Mendu, W. G. Miller, M. M. Moxey-Mims, G. V. Roberts, W. L. St. Peter, C. Warfield, and N. R. Powe. 2021. Reassessing the inclusion of race in diagnosing kidney diseases: An interim report from the NKF-ASN task force. Journal of the American Society of Nephrology 32(6):1305-1317.
Emanuel, E. J., D. Wendler, and C. Grady. 2000. What makes clinical research ethical? JAMA 283:2701-2711.
Eneanya, N. D., W. Yang, and P. P. Reese. 2019. Reconsidering the consequences of using race to estimate kidney function. JAMA 322(2):113-114.
Freedman, B. I., S. O. Pastan, A. K. Israni, D. Schladt, B. A. Julian, M. D. Gautreaux, V. Hauptfeld, R. A. Bray, H. M. Gebel, A. D. Kirk, R. S. Gaston, J. Rogers, A. C. Farney, G. Orlando, R. J. Stratta, S. Mohan, L. Ma, C. D. Langefeld, D. W. Bowden, P. J. Hicks, and J. Divers. 2016. APOL1 Genotype and kidney transplantation outcomes from deceased African American donors. Transplantation 100(1):194-202.
Friedewald, J. J., C. J. Samana, B. L. Kasiske, A. K. Israni, D. Stewart, W. Cherikh, and R. N. Formica. 2013. The kidney allocation system. Surgical Clinics of North America 93(6):1395-1406.
Gander, J. C., X. Zhang, L. Plantinga, S. Paul, M. Basu, S. O. Pastan, E. Gibney, E. Hartmann, L. Mulloy, C. Zayas, and R. E. Patzer. 2018. Racial disparities in preemptive referral for kidney transplantation in Georgia. Clinical Transplantation 32(9):e13380.
Gentry, S. E., and D. L. Segev. 2019. Restructuring the OPTN contract to achieve policy coherence and infrastructure excellence. American Journal of Transplantation 19(6):1622-1627.
Goff, R. R., K. Uccellini, K. Lindblad, S. Hall, R. Davies, M. Farr, S. Silvestry, and J. G. Rogers. 2020. A change of heart: Preliminary results of the United States 2018 adult heart allocation revision. American Journal of Transplantation 20(10):2781-2790.
Halazun, K. J., A. K. Mathur, A. A. Rana, A. B. Massie, S. Mohan, R. E. Patzer, J. P. Wedd, B. Samstein, R. M. Subramanian, B. D. Campos, and S. J. Knechtle. 2016. One size does not fit all—Regional variation in the impact of the share 35 liver allocation policy. American Journal of Transplantation 16(1):137-142.
Harhay, M. N., M. O. Harhay, K. Ranganna, S. M. Boyle, L. L. Mizrahi, S. Guy, G. E. Malat, G. Xiao, D. J. Reich, and R. E. Patzer. 2018. Association of the kidney allocation system with dialysis exposure before deceased donor kidney transplantation by preemptive wait-listing status. Clinical Transplantation 32(10):e13386.
HHS (U.S. Department of Health and Human Services). 2019. Modern National Resource Allocation System: Request for Information. https://sam.gov/opp/69bd972384b8480283bd2599fc8805a9/view;%20 (accessed October 19, 2021).
Hsu, C.-Y., F. Lin, E. Vittinghoff, and M. G. Shlipak. 2003. Racial differences in the progression from chronic renal insufficiency to end-stage renal disease in the United States. Journal of the American Society of Nephrology 14(11):2902-2907.
Hsu, C.-Y., W. Yang, R. V. Parikh, A. H. Anderson, T. K. Chen, D. L. Cohen, J. He, M. J. Mohanty, J. P. Lash, K. T. Mills, A. N. Muiru, A. Parsa, M. R. Saunders, T. Shafi, R. R. Townsend, S. S. Waikar, J. Wang, M. Wolf, T. C. Tan, H. I. Feldman, and A. S. Go. 2021. Race, genetic ancestry, and estimating kidney function in CKD. New England Journal of Medicine 385(19):1750-1760.
Husain, S. A., F. S. Winterhalter, and S. Mohan. 2018. Kidney transplant offers to deceased candidates. American Journal of Transplantation 18(11):2836-2837.
Husain, S. A., K. L. King, G. K. Dube, D. Tsapepas, D. J. Cohen, L. E. Ratner, and S. Mohan. 2019. Regional disparities in transplantation with deceased donor kidneys with Kidney Donor Profile Index less than 20% among candidates with top 20% estimated post transplant survival. Progress in Transplantation (Aliso Viejo, California), 29(4):354-360.
Ioannidis, J. P., N. R. Powe, and C. Yancy. 2021. Recalibrating the use of race in medical research. JAMA 325(7):623.
IOM (Institute of Medicine). 1999. Organ procurement and transplantation: Assessing current policies and the potential impact. Washington, DC: National Academy Press.
Joshi, S., J. J. Gaynor, S. Bayers, G. Guerra, A. Eldefrawy, Z. Chediak, L. Companioni, J. Sageshima, L. Chen, W. Kupin, D. Roth, A. Mattiazzi, G. W. Burke III, and G. Ciancio. 2013. Disparities among blacks, Hispanics, and whites in time from starting dialysis to kidney transplant waitlisting. Transplantation 95(2):309-318.
Julian, B. A., R. S. Gaston, W. M. Brown, A. Reeves-Daniel, A. K. Israni, D. P. Schladt, S. O. Pastan, S. Mohan, B. I. Freedman, and J. Divers. 2017. Effect of replacing race with apolipoprotein L1 genotype in calculation of kidney donor risk index. American Journal of Transplantation 17(6):1540-1548.
Kim, W. R., S. W. Biggins, W. K. Kremers, R. H. Wiesner, P. S. Kamath, J. T. Benson, E. Edwards, and T. M. Therneau. 2008. Hyponatremia and mortality among patients on the liver-transplant waiting list. New England Journal of Medicine 359(10):1018-1026.
King, K. L., S. A. Husain, Z. Jin, C. Brennan, and S. Mohan. 2019. Trends in disparities in preemptive kidney transplantation in the United States. Clinical Journal of the American Society of Nephrology 14(10):1500-1511.
Ku, E. 2021 (unpublished). Review of algorithms used in kidney allocation—Issues of fairness, equity, and system variation. Paper commissioned by the Committee on a Fairer and More Equitable, Cost-Effective, and Transparent System of Donor Organ Procurement, Allocation, and Distribution, National Academies of Sciences, Engineering, and Medicine, Washington, DC.
Ku, E., C. E. McCulloch, D. B. Adey, L. Li, and K. L. Johansen. 2021. Racial disparities in eligibility for preemptive waitlisting for kidney transplantation and modification of EGFR thresholds to equalize waitlist time. Journal of the American Society of Nephrology 32(3):677-685.
Kulkarni, S., K. Ladin, D. Haakinson, E. Greene, L. Li, and Y. Deng. 2019. Association of racial disparities with access to kidney transplant after the implementation of the New Kidney Allocation System. JAMA Surgery 154(7):618.
Lai, J. C. 2021 (unpublished). Review of algorithms in liver allocation. Paper commissioned by the Committee on a Fairer and More Equitable, Cost-Effective, and Transparent System of Donor Organ Procurement, Allocation, and Distribution, National Academies of Sciences, Engineering, and Medicine, Washington, DC.
Locke, J. E., B. A. Shelton, K. M. Olthoff, E. A. Pomfret, K. A. Forde, D. Sawinski, M. Gray, and N. L. Ascher. 2020. Quantifying sex-based disparities in liver allocation. JAMA Surgery 155(7).
Luo, X., J. Leanza, A. B. Massie, J. M. Garonzik-Wang, C. E. Haugen, S. E. Gentry, S. E. Ottmann, and D. L. Segev. 2018. MELD as a metric for survival benefit of liver transplantation. American Journal of Transplantation 18(5):1231-1237.
Massie, A. B., X. Luo, E. K. Chow, J. L. Alejo, N. M. Desai, and D. L. Segev. 2014. Survival benefit of primary deceased donor transplantation with high-KDPI kidneys. American Journal of Transplantation 14(10):2310-2316.
Massie, A. B., E. K. Chow E, C. E. Wickliffe, X. Luo, S. E. Gentry, D. C. Mulligan, and D. L. Segev. 2015. Early changes in liver distribution following implementation of Share 35. American Journal of Transplantation 15:659-667.
Melanson, T. A., J. M. Hockenberry, L. Plantinga, M. Basu, S. Pastan, S. Mohan, D. H. Howard, and R. E. Patzer. 2017. New kidney allocation system associated with increased rates of transplants among black and hispanic patients. Health Affairs (Project Hope) 36(6):1078-1085.
Merion, R. M., V. B. Ashby, R. A. Wolfe, D. A. Distant, T. E. Hulbert-Shearon, R. A. Metzger, A. O. Ojo, and F. K. Port, F. 2005. Deceased-donor characteristics and the survival benefit of kidney transplantation. JAMA 294(21):2726-2733.
Mulligan, D. 2021. The role of modeling in proposed organ allocation policy changes. Presentation at the February 4-5, 2021 public workshop of the Committee on a Fairer and More Equitable, Cost-Effective, and Transparent System of Donor Organ Procurement, Allocation, and Distribution, National Academies of Sciences, Engineering, and Medicine Virtual Meeting, Washington, DC. https://www.nationalacademies.org/event/02-04-2021/afairer-and-more-equitable-cost-effective-and-transparent-system-of-donor-organ-procurement-allocation-anddistribution-a-virtual-workshop (accessed January 26, 2022).
OPTN (Organ Procurement and Transplantation Network). 2020a. Briefing to the OPTN Board of Directors on addressing medically urgent candidates in the new kidney allocation system. https://optn.transplant.hrsa.gov/media/3813/202006_kidney_medical_urgency_bp.pdf (accessed February 3, 2022).
OPTN. 2020b. A guide to calculating and interpreting the Kidney Donor Profile Index (KDPI). https://optn.transplant.hrsa.gov/media/1512/guide_to_calculating_interpreting_kdpi.pdf (accessed January 2, 2022).
OPTN. 2021a. Clarify multi-organ allocation policy. https://optn.transplant.hrsa.gov/governance/public-comment/clarify-multi-organ-allocation-policy (accessed December 31, 2021).
OPTN. 2021b. OPTN metrics: Waitlist details. https://insights.unos.org/OPTN-metrics (accessed December 13, 2021).
OPTN. n.d.-a. Continuous distribution. https://optn.transplant.hrsa.gov/policies-bylaws/a-closer-look/continuous-distribution (accessed December 13, 2021).
OPTN. n.d.-b https://optn.transplant.hrsa.gov/professionals/by-topic/guidance/kidney-pancreas-allocation-system-frequently-asked-questions/= (accessed January 27, 2022).
OPTN Minority Affairs and Kidney Transplantation Committees. 2021. Reassess inclusion of race in estimated glomerular filtration rate (eGFR) calculation. https://optn.transplant.hrsa.gov/media/pdrel25h/20210819_ki_mac_egfr_meeting_summary.pdf (accessed January 2, 2022).
Parker, W. F., A. S. Anderson, R. D. Gibbons, E. R. Garrity, L. F. Ross, E. S. Huang, and M. M. Churpek. 2019. Association of transplant center with survival benefit among adults undergoing heart transplant in the United States. JAMA 322(18):1789.
Parker, W. F., Y. Becker, and R. D. Gibbons. 2021 (unpublished). Saving more lives with deceased donor kidney transplantation. Paper commissioned by the Committee on a Fairer and More Equitable, Cost-Effective, and Transparent System of Donor Organ Procurement, Allocation, and Distribution, National Academies of Sciences, Engineering, and Medicine, Washington, DC.
Patzer, R. E., S. Amaral, H. Wasse, N. Volkova, D. Kleinbaum, and W. M. McClellan. 2009. Neighborhood poverty and racial disparities in kidney transplant waitlisting. Journal of the American Society of Nephrology 20(6):1333-1340.
Peng, R. B., H. Lee, Z. T. Ke, and M. R. Saunders. 2018. Racial disparities in kidney transplant waitlist appearance in Chicago: Is it race or place? Clinical Transplantation 32(5):e13195.
Pérez-Sáez, M. J., E. Arcos, J. Comas, M. Crespo, J. Lloveras, and J. Pascual. 2016. Survival benefit from kidney transplantation using kidneys from deceased donors aged ≥75 years: A time-dependent analysis. American Journal of Transplantation 16(9):2724-2733.
Powe, N. R. 2020. Black kidney function matters: Use or misuse of race. JAMA 324(8):737-738.
Proctor, G. 2019. HRSA Healthy Grants Workshop. HRSA examined: The Healthcare Systems Bureau. https://www.hrsa.gov/sites/default/files/hrsa/grants/manage/technicalassistance/hsb-2019.pdf (accessed October 18, 2021).
RAND informs government it will not bid on contracts to administer OPTN, SRTR. 1999. The Free Library. https://www.thefreelibrary.com/RAND+informs+government+it+will+not+bid+on+contracts+to+administer...-a058091072 (accessed December 16, 2021).
Reese, P. P., S. Mohan, K. L. King, W. W. Williams, V. S. Potluri, M. N. Harhay, and N. D. Eneanya. 2021. Racial disparities in preemptive waitlisting and deceased donor kidney transplantation: Ethics and solutions. American Journal of Transplantation 21(3):958-967.
Rodríguez-Castro, K. I., E. De Martin, M. Gambato, S. Lazzaro, E. Villa, and P. Burra. 2014. Female gender in the setting of liver transplantation. World Journal of Transplantation 4(4):229-242.
Schold, J. D., L. D. Buccini, P. P. Reese, E. D. Poggio, and D. A. Goldfarb. 2014. Effect of dialysis initiation for preemptively listed candidates in the revised kidney allocation policy. American Journal of Transplantation 14(12):2855-2860.
Silvestry, S. C., and J. G. Rogers. 2022. Rinse, wash, repeat: The evolution of the UNOS heart transplant allocation system. JACC: Heart Failure 10(1):24-26.
Singal, A. K., and P. S. Kamath. 2013. Model for end-stage liver disease. Journal of Clinical and Experimental Hepatology 3(1):50-60.
Singh, T. P., C. E. Milliren, C. S. Almond, and D. Graham. 2014. Survival benefit from transplantation in patients listed for heart transplantation in the United States. Journal of the American College of Cardiology 63(12):1169-1178.
Snyder, J. 2021. Simulated allocation models: Strengths, limitations, and data availability. Presentation at the February 4-5, 2021 public workshop of the Committee on a Fairer and More Equitable, Cost-Effective, and Transparent System of Donor Organ Procurement, Allocation, and Distribution, National Academies of Sciences, Engineering, and Medicine Virtual Meeting, Washington, DC. https://www.nationalacademies.org/event/02-04-2021/a-fairer-and-more-equitable-cost-effective-and-transparent-system-of-donor-organ-procurement-allocation-and-distribution-a-virtual-workshop (accessed January 26, 2022).
SRTR (Scientific Registry of Transplant Recipients). 2019. Simulated allocation models. https://www.srtr.org/requesting-srtr-data/simulated-allocation-models (accessed January 1, 2022).
Stewart, D. E., A. R. Wilk, A. E. Toll, A. M. Harper, R. R. Lehman, A. M. Robinson, S. A. Noreen, E. B. Edwards, and D. K. Klassen. 2018. Measuring and monitoring equity in access to deceased donor kidney transplantation. American Journal of Transplantation 18(8):1924-1935.
Tran, Z. T., R. Hernandez, J. Madrigal, S. T. Kim, A. Verma, D. G. Rabkin, and P. Benharash. 2022. Center-level variation in transplant rates following the heart allocation policy change. JAMA Cardiology. https://doi.org/10.1001/jamacardio.2021.5370.
UNOS. 2021. Lung calculation. https://unos.org/wp-content/uploads/unos/Lung_Calculation.pdf (accessed December 16, 2021).
USRDS (United States Renal Data System). 2020. Annual data report: Epidemiology of kidney disease in the United States. Bethesda, MD: National Institute of Diabetes and Digestive and Kidney Diseases.
U.S. Senate Committee on Finance. 2020. FinalSIGNED - Grassley Wyden to HHS 23Oct2002. https://www.finance.senate.gov/imo/media/doc/FinalSIGNED%20-%20Grassley%20Wyden%20to%20HHS%2023Oct2020.pdf (accessed February 4, 2022).
Verghese, P. S. 2017. Pediatric kidney transplantation: A historical review. Pediatric Research 81(1-2):259-264.
Vock, D. M., M. T. Durheim, W. M. Tsuang, C. A. Finlen-Copeland, A. A. Tsiatis, M. Davidian, M. L. Neely, D. J. Lederer, and S. M. Palmer. 2017. Survival benefit of lung transplantation in the modern era of lung allocation. Annals of the American Thoracic Society 14(2):172-181.
Wang, C. J., J. B Wetmore, and A. K. Israni. 2017. Old versus new: Progress in reaching the goals of the new kidney allocation system. Human Immunology 78(1):9-15.
Westphal, S. G., E. D. Langewisch, A. M. Robinson, A. R. Wilk, J. J. Dong, T. J. Plumb, R. Mullane, S. Merani, A. L. Hoffman, A. Maskin, and C. D. Miles. 2021. The impact of multi-organ transplant allocation priority on waitlisted kidney transplant candidates. American Journal of Transplantation 21(6):2161-2174.
Wey, A., J. Foutz, S. K. Gustafson, R. J. Carrico, K. Sisaithong, H. Tosoc-Haskell, M. McBride, D. Klassen, N. Salkowski, B. L. Kasiske, A. K. Israni, and J. J. Snyder. 2020. The collaborative innovation and improvement network (COIIN): Effect on donor yield, waitlist mortality, transplant rates, and offer acceptance. American Journal of Transplantation 20(4):1076-1086.
Wolfe, R. A., V. B. Ashby, E. L. Milford, A. O. Ojo, R. E. Ettenger, L. Y. C. Agodoa, P. J. Held, and F. K. Port. 1999. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. New England Journal of Medicine 341(23):1725-1730.
Zelnick, L. R., N. Leca, B. Young, and N. Bansal. 2021. Association of the estimated glomerular filtration rate with vs without a coefficient for race with time to eligibility for Kidney Transplant. JAMA Network Open 4(1).
This page intentionally left blank.




































