
7
Sunscreen, Preventive Health Behaviors, and Implications of Changes in Sunscreen Use for Public Health
Sunscreen use is recommended for the protection of human skin from damage due to ultraviolet radiation (UVR) (e.g., CDC, 2021; FDA, 2021a). Other recommended behaviors for sun protection include seeking shade, wearing protective clothing and hats, and reducing outdoor activity during peak UVR hours (CDC, 2021). Together, these behaviors are used to reduce the risk of developing skin cancer and to prevent sunburn and photoaging. Due to the role of sunscreen in sun protection, policies or messaging that reduce the availability or use of certain ingredients raise the question of whether human health impacts may result. This chapter addresses the concern that human sunscreen use behavior and health could be impacted by emerging restrictions on certain UV (ultraviolet) filters or perceptions about the risks sunscreens pose to the aquatic environment.
This chapter first summarizes the key causes and risk factors of skin cancer and other skin damage, and the efficacy of sunscreen for their prevention. It further describes what is known about preventive health behaviors—particularly use of sunscreen—to reduce the damaging effects of UVR exposure, including how usage is driven by consumer preferences or perceived concerns about the environment. Last, based on what is known about human sunscreen usage, the chapter includes an assessment of the potential effects on public health of restricting certain UV filters from use in sunscreens.
UV RADIATION AND SKIN DAMAGE
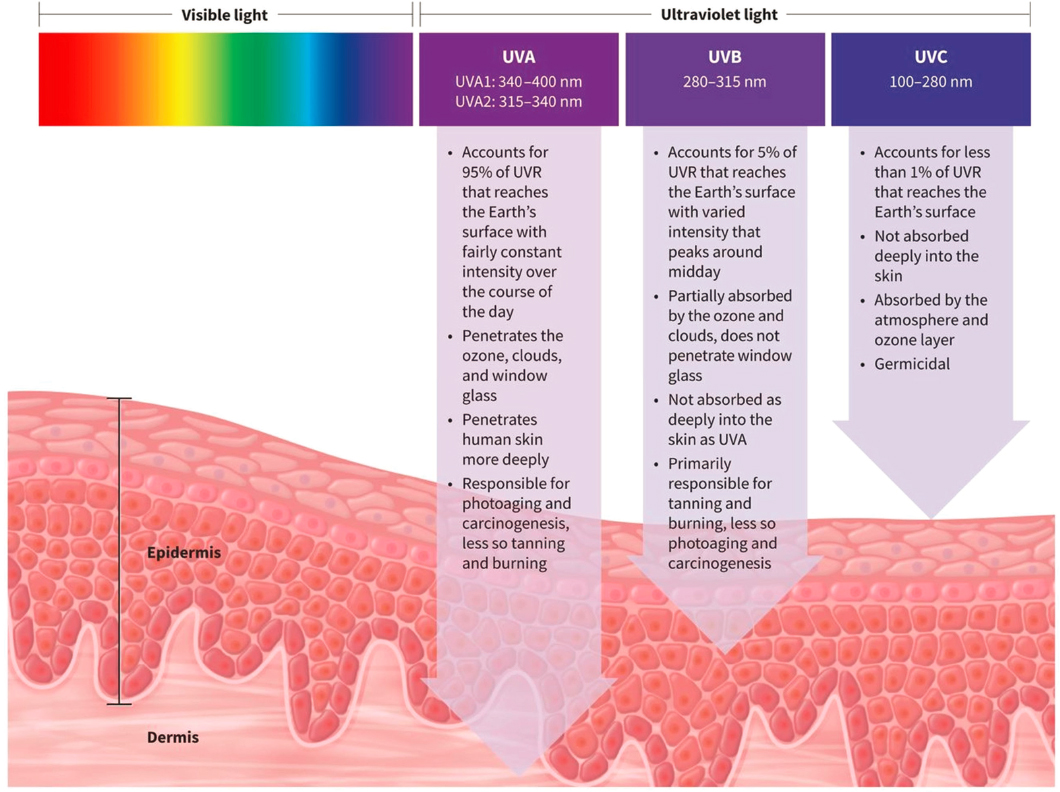
UVR comprises UVA (315–400 nm), UVB (280–315 nm), and UVC (100–280 nm). Naturally occurring UVC does not reach the Earth’s surface. UVA and UVB are both associated with skin cancer, with UVA also being associated with photoaging and UVB being associated with sunburn (Figure 7.1). Evidence related to these human health concerns and UVR is described in the following sections.
Skin Cancer
Skin cancers are the most commonly diagnosed cancers in the United States (CDC, 2021; Guy et al., 2015; NCI, 2021b). An average of 4.9 million U.S. adults were treated for skin cancer each year from 2007 to 2011, with an average annual total cost of treatment of $8.1 billion (Guy et al., 2015). The most common skin cancers are the keratinocyte carcinomas (KC)—basal cell carcinoma (BCC) and squamous cell carcinoma (SCC), which result in significant morbidity and health care utilization (ACS, 2021b). The most deadly skin cancers include melanoma,
Merkel cell carcinoma, and squamous cell carcinomas of the ears and lips. Although melanoma accounts for only about 1 percent of all skin cancers, most skin cancer deaths are from melanoma (Rogers and Coldiron, 2013).
The National Cancer Institute (NCI) estimated that 106,110 new cases of melanoma would be diagnosed in the United States in 2021, and that 7,180 deaths would occur (NCI, 2021a). Melanoma is now the fifth most commonly diagnosed cancer in the United States (excluding KCs), exceeded by breast, prostate, lung, and colorectal cancer (NCI, 2021a). It is a leading cause of cancer and cancer death among young adults (ACS, 2021a). From 2008 to 2017, incidence rates increased about 2 percent per year overall, though rates are stable or decreasing in people under 55 (ACS, 2021b; CDC, 2018). Incidence in 2019 is 6 times as high as it was four decades ago, a disproportionate increase in incidence compared to other preventable cancers (Mayer et al., 2014). The reasons behind the increased incidence are debated and may stem from greater recreational exposure to the sun, increased screening, overdiagnosis, increased longevity, increased use of tanning beds, or environmental factors such as the depletion of the ozone layer (EPA, 2021a; Vaverková et al., 2020; Welch et al., 2021). While the number of people diagnosed with melanoma remains high, mortality rates have been decreasing (NCI, 2021a). A key reason for this is there have been significant advances in treatment, including the introduction of immunotherapy in 2011, along with the fact that the disease may be diagnosed and treated early more often because of routine screening.
Statistics on KCs are harder to track because they are not required to be reported to cancer registries (ACS, 2021a), but diagnoses and treatment can be ascertained through health claims data. A recent estimate is that about 5.4 million new cases of KC were diagnosed in the United States in 2012, affecting 3.3 million individuals (Rogers et al., 2015). BCCs are more common than SCCs, with estimates of their share of KC incidence ranging from 67 percent to 80 percent (The Skin Cancer Foundation, 2021). The management of actinic keratoses—lesions with the potential to progress to squamous cell carcinoma—poses significant health care costs in the United States; in one study performing a billing claims analysis of Medicare Part B data, 35.6 million actinic keratosis lesions were treated in 2015 (Yeung et al., 2018). A report by the American Academy of Dermatology (AAD), Burden of Skin Diseases, indicated that up to 39.5 million Americans presented to medical care for treatment of sun-related skin damage, including actinic keratoses, with associated medical costs of $1.8 billion in 2013 (Lim et al., 2017). The quality-of-life burden of keratinocyte carcinomas, melanoma, and precancerous lesions has not been fully evaluated.
Skin Cancer Causes and Risk Factors
Skin cancer risk is strongly associated with UVR resulting from sun exposure and other sources of UV light, including tanning beds, with clear molecular pathways of UV-induced genetic mutations that can lead to cancer (Ciążyńska et al., 2021; Savoye et al., 2018; Wu et al. 2014a). The role of sunlight as a cause of skin damage has been known for thousands of years, and methods to mitigate this damage dates back to 4000 B.C.E. (Ma and Yoo, 2021). However, the specific role of UVR as a cause of skin cancer was first uncovered over the last 150 years, with an understanding of the role of UVA and UVB and visible light as factors leading to skin damage and, subsequently, skin cancers (Ma and Yoo, 2021). Intermittent intense UVR exposure and sunburns (Gandini et al., 2005; Green et al., 1985, 2011a), and use of tanning beds (Colantonio et al., 2014) play significant roles in the development of cutaneous malignant melanoma. Chronic exposure to UV radiation has been correlated with incidence of BCC and SCC (Chen et al., 2011; Diffey et al., 1979; Downs and Parisi, 2009; Kaskel et al., 2015; Lindgren et al., 1998; Little et al., 2019). Sun exposure during childhood is a particular risk factor for KCs and, to a lesser extent, melanoma development (Green et al., 2011a). More than half of a person’s lifetime UV exposure is estimated to occur before the age of 20 (Cokkinides et al. 2001; Saraiya et al. 2004; Stern et al. 1986).
The increase in skin cancer incidence rates among U.S. young adults in the 1980s and 1990s is partially attributed to use of indoor tanning facilities; this applies especially to adolescent and young adult women who aimed to attain the darker complexions valued in the media (Friedman et al., 2015; Glanz et al., 2019). Their rate of melanoma is much higher than that of young men (NCI, 2021a). Additional studies have identified indoor tanning as a possible explanation for increased skin cancer in other populations as well, including sexual minority men (i.e., those who identify as homosexual, gay, or bisexual) (Mansh et al., 2015). Indoor tanning among high school students decreased between 2009 and 2017 (Holman et al., 2019); however, because the proportion of melanoma attributed to indoor tanning has not been determined, it is not possible to project the impact of reduced indoor tanning use on melanoma rates.
Australia has the highest rates of skin cancer in the world, which is attributed to the phenotypical characteristics of its majority population, such as fair skin, light hair, and inability to tan (Olsen et al., 2019)—as well as Australia’s proximity to the equator, where UVR exposure is more intense year-round (Tabbakh et al., 2019). Overexposure to UVR was identified as a risk factor for melanoma in Australia as early as the 1950s (Holman et al., 1980; Lancaster and Nelson, 1957), with rates doubling by the early 1980s (Little et al., 1980; McCarthy et al., 1980, as reported by Iannacone and Green, 2014). Significant research on melanoma rates and risk factors has been done in Australia, information that is likely applicable to populations with fair skin in other countries, including the United States.
The differential effects of skin pigmentation and ethnicity on skin cancer risk are suggested given that incidence rates for melanomas are higher in white individuals (25.8/100,000) in comparison to Hispanic (4.5/100,000), American Indian/Alaska Native (5.3/100,000), Asian/Pacific Islander (1.2/100,000), and Black populations (0.9/100,000) (U.S. Cancer Statistics, 2021). However, although skin cancers are less common, African Americans often have proportionally lower survival rates from skin cancers than white individuals (Battie, 2013). All individuals, regardless of complexion, are at risk; however, skin cancer prevention behaviors vary according to skin types (Jacobsen
et al., 2016). Using Fitzpatrick’s (1988) classification, individuals who have skin types that tan easily, or skin that is moderately to markedly pigmented, underestimate their risks for skin cancers (Colmenares et al., 2013; Wheat et al., 2013). Racial/ethnic groups with darker skin (higher melanin content) have a lower incidence attributed, in part, to the inherent sun protection provided by melanin (NCI, 2016) However, race and ethnicity are a poor proxy for skin cancer risk. Late-stage melanomas are more prevalent among minority patients and are frequently fatal. Inaccurate perceptions of risk for skin cancers in non-white ethnic groups including Asians and Pacific Islanders can lead to prolonged UV exposures, increased sunburn prevalence, delayed skin cancer diagnoses, and greater risks for death (Higgins et al., 2018).
The question of the contribution of UV exposure to the risk of melanoma in people of color has been examined recently. A systematic review of 13 studies with more than 7,700 cases of melanoma concluded that UV exposure may not be an important risk factor for melanoma in people of color (Lopes et al., 2021). However, the review was limited by the inclusion of studies of moderate to low quality based on evidence ratings for observational studies from the Centre for Evidence-Based Medicine at Oxford. There were problems with limited assessments of UV exposure, inconsistent race classification and assignment of race as a proxy for melanin index or sunburn propensity, and the potential under-powering of the studies to definitively answer the race-UV exposure risk question (Lopes et al., 2021). Similarly, a systematic review of 12 studies conducted between 1990 and 2019 assessed the association of UV exposure with KC in individuals with skin of color, also finding the studies to be of moderate to low quality (Kolitz et al., 2022). The four studies that found positive correlations were on patients receiving phototherapy. The reviewed studies assessing non-phototherapy-related UV exposure found small positive associations, and were conducted in primarily East Asian individuals (studies are lacking among Black and Hispanic individuals and none were performed in the United States). These studies are reflective of the limited inclusion of people of color in studies measuring the influence of UV exposure on skin cancer incidence.
Sunburn
The burden of sunburn (UV-induced burn that appears as reddening, inflammation, and sometimes blistering of skin) to the U.S. health care system has been assessed through prevalence and treatment-seeking behavior. In a recent analysis, approximately one-third of all U.S. adults and over half of U.S. high school students reported getting at least one sunburn per year (Holman et al., 2018a; Kann et al., 2018). Data from 2013 showed that nearly 34,000 people sought treatment for sunburn in an emergency room, resulting in an estimated cost of $11.2 million (Guy et al., 2017). In an analysis of a U.S. commercial insurance database from 2009 to 2018, 186,168 patients with 208,777 encounters for sunburn diagnoses presented for medical treatment, with almost 20 percent presenting to emergency or urgent care settings and most presenting to primary care or dermatology specialty care (Nowakowska et al., 2021). Additionally, as described in the previous section, a history of sunburn correlates with melanoma and keratinocyte carcinoma.
A pooled data analysis of sunburn at 12 beach locations in the United States estimated that 13 percent of beachgoers reported sunburn following a beach visit (DeFlorio-Barker et al., 2020). The analysis found that for those who spent more than five hours in the sun, use of multiple types of photoprotection reduced the rate of sunburn by 55 percent (DeFlorio-Barker et al., 2020). While this is the largest known analysis of sunburn after going to the beach, the data were collected between 2003 and 2009 in only 12 locations, so further updates could be informative.
Photoaging
Photoaging is defined as the cumulative detrimental effects of skin that result from repeated exposure to UVR, including rhytids (e.g., wrinkles), pigmentary spots, and discoloration. Photoaging affects appearance and quality of life, but it may also be associated with increased risk of developing skin cancer. Separating the aesthetic impacts of UVR from its health impacts such as skin cancer may not be possible, though quality of life impact and perceived age associated with photoaging have been reported in the literature (Clatici et al., 2017). Consumer products that claim anti-aging properties have to demonstrate effectiveness and standard methods focus on photoaging (Miller, 2009). For this reason, they typically include UV filters.
Vulnerable Populations with Photosensitive Conditions
Some vulnerable populations are at greater risk for skin cancer due to sun exposure because they are on medications that predispose them to photosensitivity or have an inherited or acquired photosensitive disorder. Photosensitive disorders include phototoxicity (non-immune skin irritation triggered by light activation of a chemical applied to the skin), photoallergy (immune-mediated contact dermatitis in which an allergen must be activated by light to become allergenic), and the worsening or induction of systemic disorders like connective tissue disease (e.g., lupus, dermatomyositis). Those taking photosensitizing medications may be the largest of vulnerable groups, as drugs capable of causing phototoxic reactions include common medications: antibiotics like tetracyclines and sulfonamides, nonsteroidal anti-inflammatory drugs (e.g., ibuprofen), and drugs used to treat diabetes, hypertension, arrhythmia, psychiatric disease, cancer, and fungal infections (FDA, 2015). One example, voriconazole, is an antifungal medication that dramatically accelerates sunburn, photoaging, and rates of KC and melanoma in individuals with altered immune competence (D’Arcy, 2020; Malani and Aronoff, 2008; Miller et al., 2010). The blood pressure medication hydrochlorothiazide has special FDA labeling indicating the small increased risk of cSCC (1 additional case per 16,000 patients taking the medication; FDA, 2020). Approximately 40.6 million prescriptions of this medication were dispensed in the United States in 2018 (Mikulic, 2021).
Certain patients, such as organ transplant recipients who require anti-rejection immunosuppressive medications, have extremely high rates of skin cancer (between 2 and 80 times depending on the cancer type, the level of systemic immunosuppression, and race and ethnicity of the patient), which may be exacerbated by ongoing UV exposure following transplantation (Chundydyal et al., 2021; Gibson et al., 2021; Pritchett et al., 2016; Thet et al., 2021). Malignancy is the second leading cause of death in this population, with overall mortality is 5,308 per 100,000 person-years; skin cancer–specific mortality is 35.27 per 100,000 person-years.
Another group of vulnerable patients is those with inherited or genetic causes of severe sun sensitivity. Patients with xeroderma pigmentosum, a skin disorder associated with mutations in repair pathways for UV-induced DNA damage, have a prevalence of skin cancer of almost 50 percent by age 10 and an average life expectancy of 37 years (Sainsbury et al., 2020; Tamura et al., 2014). Porphyrias, another group of inherited disorders that cause severe photosensitivity, have sensitivity to visible light rather than UV light, specifically Soret and Q bands, necessitating very specific formulations of sunscreen containing tint to protect their health, most commonly those containing iron oxides or pigmentary titanium dioxide (non-nano version) (Lyons et al., 2021).
Photosensitive disorder can be impacted by UVA, UVB, or both (as well as visible light), requiring UV filters that can protect against the full UV spectrum range (Goetze et al., 2015; Macleod and Frain-Bell, 1975; Magnus et al., 1959; Murphy, 2001; Teramura et al., 2018). Additionally, patients can be allergic to individual UV filters, the most common being dibenzoylmethanes (avobenzone), cinnamates, and benzophenones (Heurung et al., 2014; Keyes et al., 2019; Scheuer and Warshaw, 2006), which would require availability of alternative UV filters for photoprotection. These vulnerable populations require almost constant use of sunscreen for basic daily functioning and to reduce the associated risk of skin cancer.
SUNSCREEN EFFICACY, SAFETY, AND USE
Sunscreens are over-the-counter consumer products used for the prevention of skin cancer, sunburn, and photoaging. Regular use of broad-spectrum sunscreen with sun protection factor (SPF) of at least 30 (as recommended by AAD) is part of a regimen of photoprotection that also includes the use of protective clothing, hats, sunglasses, sun avoidance and shade-seeking behaviors. Other cosmetics like makeup or moisturizers with UV filters provide a degree of photoprotection that may supplement sunscreen use (Kim et al., 2021). Modern sunscreen formulations contain a number of UV filters that are approved by FDA for use in over-the-counter preparations for the prevention of sunburn, skin cancer, and photoaging. Chapter 2 of this report describes the UV filters approved for use in the United States. The global sun care products market, of which 79 percent is sun protection products, was $11 billion to $13 billion in 2018–2019 and is expected to reach $16.8 billion to $24.4 billion in value in 2027–2029 (Fortune Business Insights, 2021; Ma and Yoo, 2021).
Efficacy of Sunscreen to Prevent Skin Cancer, Sunburn, and Photoaging
Large randomized control trials have demonstrated that reducing sun exposure through the use of broad spectrum, high SPF sunscreen used as directed reduces sunburn and photoaging (Bakos et al., 2011; Gallagher et al., 2010; Hughes et al., 2013; Pruim and Green, 1999; Young et al., 2017, 2019) and also results in a reduction of melanoma and keratinocyte carcinomas as well as the development of actinic keratoses, lesions considered to be precancerous lesions leading to cSCC (Darlington et al., 2003; Green et al., 1999, 2011b; Mulliken et al., 2012, Naylor et al., 1995; Thompson et al., 1993). Studies have shown that regular sunscreen use is particularly important in vulnerable populations such as children and individuals with lighter skin types (Hall et al., 2001; Stern et al., 1986). Using a decision analysis model that included both household and government perspectives, health economists in Australia concluded that promoting routine sunscreen use in white populations in sunny locations would be a cost-effective, long-term investment for both governments and consumers (Hirst et al., 2012). Modeled estimates indicate that regular use of sunscreen under the age of 18 can reduce skin cancer risks by 50 to 80 percent (Stern et al., 1986). Furthermore, increased regular sunscreen use in the U.S. white population could reduce melanomas by an estimated 11 to 38 percent by 2031 (Olsen et al., 2018).
The Nambour Trial, an influential, randomized controlled trial (RCT) extending over 4.5 years with 8-year follow-up performed by Green et al. (1999) in Australia demonstrated that daily use of SPF16 broad spectrum sunscreen resulted in a decrease of cSCC incidence by 38 percent (876 versus 996 per 100,000; risk ratio 0.88 [0.50–1.56]) and a significantly lower number of SCC tumors in the sunscreen group than in the no daily sunscreen group (1,115 versus 1,832 per 100,000; 0.61 [0.46–0.81]). Although the incidence of BCC also was lower in the sunscreen treatment group, the difference (25 percent) was not statistically significant (2,588 versus 2,509 per 100,000; rate ratio 1.03 [95 percent CI 0.73–1.46]) and the number of BCC tumors was not lower in the sunscreen group. A long-term follow-up of the same trial showed similar evidence for reducing melanoma development (Green et al., 2011b; Figure 7.2) with four years of sunscreen use, specifically reducing the incidence of new
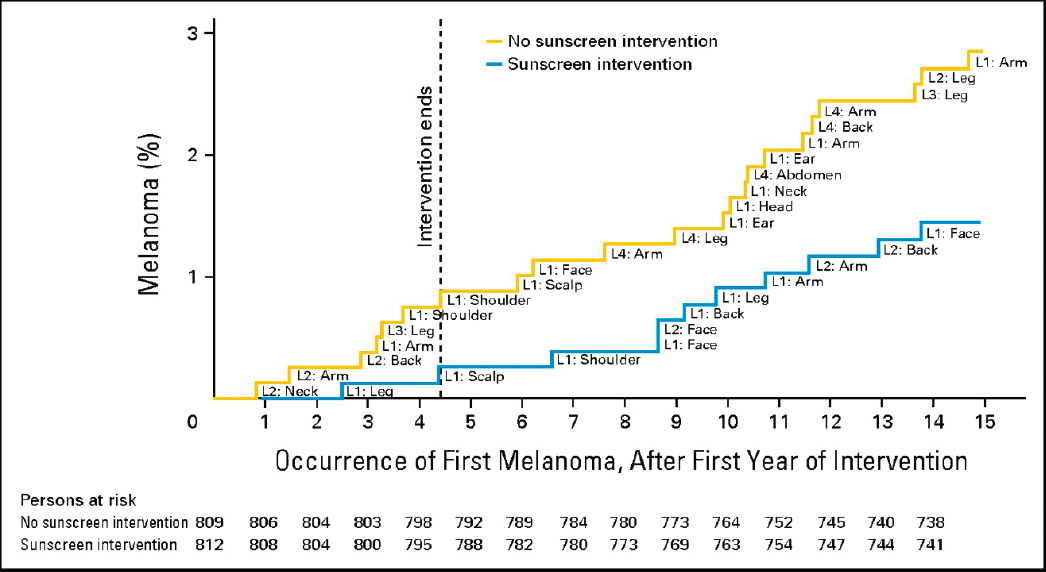
primary melanomas by 50 percent (hazard ratio [HR], 0.50; 95 percent CI, 0.24–1.02; P = 0.051), and a notable reduction in invasive melanoma in the treatment (sunscreen) group (n=3 in active versus 11 in control group; HR, 0.27; 95 percent CI, 0.08–0.97) supporting a role for sunscreen protection. The Nambour Trial was conducted in community settings, not within a restricted clinical environment, hence actual use by the treatment group varied. The median sunscreen use was less than half the amount recommended to achieve the SPF (Neale et al., 2002). However, usage was significantly higher than that of the control group (Green et al., 2011b).
Although the evidence from this trial is considered strong enough to support recommending the use of sunscreen when outdoors in the sun, a limitation of the trial is the relatively homogeneous population studied, in which a majority of participants were white individuals. However, because the trial needed adequate statistical power to evaluate differences in melanoma outcomes, it could only be conducted in Australia, which has very high rates of skin cancer and a population that is approximately 90 percent white (Gimotty and Glanz, 2011). The sunscreen tested in the Nambour Trial was Auscreen Ultrablock Lotion SPF 15-plus (Ross Cosmetics, Melbourne, Australia) containing 8 percent (by weight) of octinoxate and 2 percent (by weight) of avobenzone (Perugini et al., 2019). The additional two arms of this RCT included use of beta-carotene oral supplements versus placebo, which did not yield a clinical benefit.
A prospective population-based cohort study of 143,844 women ages 40 to 75 in Norway found that use of SPF ℹ 15 sunscreen was associated with approximately 30 percent reduced melanoma risk, with over 1.5 million person-years of follow-up and 722 cases of melanoma (Ghiasvand et al., 2016). The findings showed that the estimated population-attributable fraction (PAF) for melanoma associated with use of SPF ℹ 15 sunscreens for women ages 40 to 75 years was 18 percent (95 percent CI, 4 percent to 30 percent), and was 21 percent (95 percent CI, 3 percent to 35 percent) in women with blond/red hair (Ghiasvand et al., 2016). This study included a population-based sample of women followed for up to 21 years, and 99.9 percent of melanomas were morphologically confirmed. The NOWAC (Norwegian Women and Cancer) study examined populations with their real-world use of sunscreen. The NOWAC study differed significantly from the Nambour Trial in Australia because most UV exposure in Norway is intentional rather than incidental, and detailed information on application and type of sunscreen use and other photoprotection behaviors was not available.
The combined evidence from the Nambour Trial and the NOWAC study support the efficacy of broad-spectrum sunscreen for prevention of melanoma. The Nambour Trial also found a significant (38 percent) reduction in cSCC and a 25 percent reduction (though not statistically significant) in BCC. Randomized control trials provide the highest quality of evidence for evaluating clinical treatments (Barton, 2000). However, additional rigorous studies investigating the benefit of higher SPF-rated sunscreens, comparison trials to test the efficacy of different UV filters for prevention of skin cancer, looking at sunscreen use in heterogeneous populations, or the use of sunscreen in conjunction with additional forms of photoprotection have not yet been published and, to the committee’s knowledge, are not under way. A methodological and substantive critique of the Nambour Trial noted that the statistical test that found a reduction in melanoma might be considered borderline under one type of statistical framework (rejecting the null hypothesis), but significant under another often used framework (finding a statistically significant effect for reduced risk of invasive melanoma alone) (Gimotty and Glanz, 2011). The critique concluded that, while sunscreen use alone should not be considered the only strategy for reducing skin cancer, the evidence is strong enough that clinicians, cancer prevention agencies and public health experts should recommend regular use and reapplication of sunscreen for primary prevention in fair-skinned people when they are outdoors (Gimotty and Glanz, 2011).
Safety of Sunscreens for Human Use
In addition to efficacy, it is important to consider the safety of UV filters and sunscreens. As described in Chapter 1, FDA makes determinations about both the effectiveness and the safety of UV filters approved in the monograph process. While the scope of this report is on efficacy, a brief description of current science related to the important matter of sunscreen safety is included here.
FDA requires the submission of safety information from industry to support the designation that an over-the-counter drug is GRASE (generally recognized as safe and effective). FDA has recommended maximal usage trials
(MUsT) that measure absorption through the skin based on advice from the FDA Nonprescription Drug Advisory Committee (FDA, 2016). As part of a MUsT trial, the sunscreen would cover 75 percent of body surface following label instructions for use, and be conducted using at least four formulations for each active ingredient. Absorptions exceeding plasma concentrations of 0.5 ng/mL should pursue further safety studies, according to guidelines. These safety tests were initially requested of sunscreen manufacturers, with the option for manufacturers to defer presentation of results, but the studies have not been reported by industry. As a result, 12 of the monograph ingredients are deemed by FDA to not currently have sufficient information to make GRASE determinations.
In 2019 and 2020, two open-label RCTs done by FDA (Matta et al., 2019, 2020) demonstrated systemic absorption exceeding FDA thresholds for pursuing comprehensive safety studies (plasma concentration > 0.5 ng/mL) for formulations containing oxybenzone, octocrylene, homosalate, octisalate, octinoxate, avobenzone, and ecamsule, under maximal use conditions. Matta et al. (2019) used a single application with plasma measured up to seven days later and Matta et al. (2020) used multiple applications over four days with plasma measured up to 21 days later. Most formulations achieved these plasma levels with just a single application, and some UV filters (homosalate, oxybenzone) showed persistence above the threshold three weeks after the last sunscreen application following multiple applications. Among the tested UV filters, oxybenzone had the highest maximum plasma concentration (258.1 ng/mL) when applied in lotion form over multiple days. These studies only assessed absorption of the UV filters; they did not address effects on human health. Systemic absorption of these UV filters is not an indicator of harm to humans but indicates that further safety studies should be conducted. These were the first studies to clearly demonstrate systemic absorption under recommended sunscreen usage (previously absorption was assumed to be negligible), thus exceeding the FDA threshold requirement for additional safety testing (Adamson and Shinkai, 2020; Califf and Shinkai, 2019). It should be noted that the amount of sunscreen used in the studies (based on directed use) is likely higher than typical use.
The observation of systemic absorption had been recognized as early as 1997 (Hayden et al., 1997) and was suggested to be more widespread in an analysis of urine samples from the 2003–2004 NHANES (National Health and Nutrition Examination Survey) study, which found the presence of oxybenzone in 96.8 percent of participants’ urine (Calafat et al., 2008). Given that no study has found that 90 percent of U.S. adults use sunscreen regularly (see below) (Holman et al., 2015), a possible interpretation of the finding is that multiple sources of oxybenzone contributed to exposure for the study participants (see Chapter 2). Though, as seen in the FDA MUsT trials, oxybenzone can persist for up to three weeks after application so its presence in the body may not require daily use of sunscreen or other products containing the ingredient. A later analysis of the 4,412 participants in the 2003–2006 and 2009–2012 NHANES surveys examined found that the presence of oxybenzone was associated with self-reported frequency of sunscreen use across multiple age groups, sexes, races, and time periods but that the associations were relatively low, from 0.15 to 0.43, and 57 percent of respondents reported never or rarely using sunscreen (Zamoiski et al., 2015).
Concern about the safety of UV filters emerged from in vitro studies of various systems (bacteria, cells, yeast) that indicated or suggested potential mechanisms of action from exposures to various UV filters, at a very wide range of concentrations (Huang et al., 2021). Subsequent in vivo studies of different living organisms (fish, fish embryos, insect larvae, etc.) examined a range of endpoints, also at a very wide range of concentrations. They have studied, and some have found, outcomes/endpoints including neurotoxicity, hormonal changes, gene expression, and even mortality (Huang et al., 2021). Many of the in vitro and in vivo studies have focused on endocrine disruption mechanisms, neurotoxicity, and biomarkers related to cell metabolism. The findings from these studies have led human studies to examine some of the same hypothesized mechanisms and outcomes (Kwon and Choi, 2021).
Human safety studies have mainly examined indicators of UV filter exposure—most often, oxybenzone levels in urine (as well as some other organic UV filters)—rather than actual exposure to UV filters in sunscreen. They have studied hormonal, reproductive, and disease outcomes, mainly in case control studies (Ghazipura et al., 2017; Huang et al., 2021; Suh et al., 2020). Also, because the available studies did not follow people over a long period of time, they could not examine delayed outcomes such as cardiometabolic and cancer risk or persistent fertility problems.
Systematic reviews have synthesized information regarding the safety of UV filters for human health, covering both organic UV filters (Ghazipura et al., 2017; Huang et al., 2021; Ruszkiewicz et al., 2017; Suh et al., 2020),
and titanium dioxide and zinc oxide nanoparticles (Australian Government, 2016; Dréno, 2019). The studies summarized in these reviews have not shown support for elevated systemic levels of organic UV filters associated with adverse effects on male or female fertility, female reproductive hormone levels, adiposity, fetal growth, child’s neurodevelopment, and sexual maturation. These studies have not examined potential mechanisms and have often found different outcomes in subgroups (e.g., males versus females) in humans (Ghazipura et al., 2017; Huang et al., 2021; Suh et al., 2020). Studies have found some associations of organic UV filters with sex-specific birth weight and gestational age, but the effect sizes were modest, and more studies are needed to determine whether these are true associations and have adverse health effects. Reviews of the safety of mineral UV filters in nanoparticle form concluded that there is no evidence of carcinogenicity (Australian Government, 2016; Dréno et al., 2019).
The authors vary in their interpretations of these data, with the majority of reviews and studies conceding that, to date, no levels of toxic effects have been found in humans that outweigh the benefits of these filters in reducing overexposure to UVR. However, the authors all recognize substantial data gaps, including that benefits of UV filters may differ in distinct human populations (individuals with darker skin types who have lower skin cancer risk, and conversely, people with photosensitive conditions).
Guidance for Optimal Sunscreen Use
AAD, the professional organization of dermatologists in the United States, recommends sunscreen use by all persons, including daily use of SPF 30 or higher broad-spectrum products, other photoprotective behaviors, avoidance of tanning bed use, and regular skin examination (AAD, 2021). FDA recommends the use of a broad-spectrum filter with SPF 15 or higher (FDA, 2021a), along with other photoprotection such as clothing, sunglasses, and staying in the shade. The American Cancer Society (ACS) recommendations are similar to those of AAD (Simon, 2020).
Real Life Use: Prevalence of Sunscreen Use and Amount Used
Multiple surveys show that many people do not use sunscreen regularly and that people use less sunscreen than is recommended (Buller et al., 2011; Calderón et al., 2019; Holman et al., 2015; NCI, 2022). Recent surveys show that only about 33.7 percent of adults in the United States routinely (characterized as “always or almost always”) use sunscreen (NCI, 2022). Women are nearly twice as likely to use sunscreen as men (43.6 percent versus 23.4 percent). Routine sunscreen use is highest among non-Hispanic whites at 40.4 percent, 24.7 percent for Hispanic adults, and only 10.9 percent in non-Hispanic Black adults (NCI, 2022). Black and Hispanic adults report lower use of sunscreen and other sun protection behaviors (Calderón et al., 2019; Lunsford et al., 2018). Sunscreen use in Asian Americans was found to be lower in than non-Hispanic whites with 29 percent of Asians reporting consistent use versus 35 percent of whites (Martin et al., 2022). This is relevant because, although overall skin cancer incidence is lower in people of color, having skin cancer is associated with higher rates of morbidity and mortality in those with skin of color (Gloster and Neal, 2006). There has been a significant increase in sunscreen use since 2000 (from about 25 percent to 33 percent), but the sub-group patterns have remained the same. Reported use of any form of photoprotection has increased by about 5 percent since 2000.
As noted above, AAD recommends the use of 1 ounce of sunscreen for the entire adult body and frequent re-application (every two hours or more frequently in circumstances of sweating or water exposure). However, consumers rarely apply sunscreens at recommended thickness (estimated 0.39 to 1.0 mg/cm2 rather than the recommended 2 mg/cm2) or frequency of every two hours (Petersen and Wulf, 2014). Early research noted that photosensitive patients applied inadequate amounts of sunscreen to achieve the recommended thickness (Azurdia et al., 1999). A review of the literature found that “missing areas” and inadequate thickness of application are common ways that people use too little sunscreen (Petersen and Wulf, 2014). One experiment suggested that a second consecutive application might optimize sunscreen use by covering missed areas (Heerford et al., 2018). It should be noted that application of aerosol spray sunscreens is often done poorly and may require special education (Teplitz et al., 2018).
More research is needed to define evidence-based dosages of sunscreen for the clinical benefit of preventing skin cancer and melanoma development. The real-world usage findings that (1) most people do not routinely use
sunscreen when they are outside in the sun, and (2) those who use sunscreen seldom apply sunscreens as recommended in terms of both amount used and timing of re-application have important implications for both expected human health outcomes related to skin protection as well as for generalizing assessments of the impact of UV filters in sunscreen on aquatic environments. Models of the environmental impact of UV filters that rely on currently recommended doses of sunscreen likely overestimate environmental outcomes and would be considered upper bounds.
Use of Sunscreen for Aquatic and Other Outdoor Activities
Participation in aquatic activities (swimming, surfing, snorkeling, etc.) and other outdoor activities is associated with exposure to ultraviolet radiation, often during peak daytime sunlight hours and often for prolonged periods of time. Water-related activities are of particular interest in the context of the committee’s task because they are most likely to be a source of UV filters and other ingredients that go directly into aquatic environments. However, the use of sunscreen for other recreational and occupational outdoor activities—and in routine daily use—can still result in rinse-off in the shower that enters wastewater and aquatic environments, albeit less directly. Here we briefly review UV exposure and the use of sunscreen and other UV protection behaviors related to aquatic activities and other outdoor activities, particularly recreation and sport.
Sunscreen use at the beach has been found to be higher than everyday use. A study using polysulfone dosimeters to measure ambient UVR and observations of beachgoers in Honolulu calculated that most beachgoers spent an average of three hours at the beach and were exposed to five times the UVR dose required to be sunburned (O’Riordan et al., 2008). Of the beachgoers in that study, 73 percent (n = 88) used sunscreen with SPF greater than 30—a much higher proportion than the population as a whole. Sunscreen use was the most often-used solar protection behavior, followed by shirts with sleeves on the beach (62 percent), sunglasses on the beach (59 percent), and hats on the beach (31 percent). Of note, sunscreen total coverage of those wearing sunscreen averaged only 40 percent of body area (O’Riordan et al, 2008). A survey of 756 parents and children in Hawaii reported frequent sunscreen use when going to the beach twice as often as during everyday outdoor activities (80 percent versus 39 percent) (Glanz et al., 1999).
Lifeguards at pools and beaches have high rates of occupational, recreational, and incidental exposure to UV radiation. A study of measured solar UVR exposures of lifeguards in pool settings in four U.S. locations (n =168), using UVR sensitive polysulfone film badges found that 74 percent exceeded threshold limits for occupational exposure, 39 percent received more than four times the limit, and 65 percent had enough UVR exposure to induce sunburn (Gies et al., 2009). Another analysis of the same study showed that lifeguards were measured to have, and also reported, using sunscreen more than adults but less than children at swimming pools (Glanz et al., 2009). They also tend to use sunscreen less regularly later in the summer. Surveys of over 3,000 lifeguards in the United States found that they also report fewer sunburns later in the summer (Hiemstra et al., 2012). The lifeguards, like other outdoor workers, most often used sunscreen and sunglasses for sun protection, and men were more likely to wear hats than women (Gies et al., 2009; Glanz et al., 2007).
Several reports have described high rates of solar UV exposure among individuals who participate in outdoor sports activities (Snyder et al., 2020), and some have found high rates of malignant melanoma in marathon runners (Ambros-Rudolph et al., 2006; Richtig et al., 2008). Outdoor runners have been studied more than most other athletes, and despite their high rates of sun exposure, many have low “skin cancer literacy” or understanding of protective practices (Duarte et al., 2018) and make inadequate use of sunscreen and other protective behaviors (Keeney, 2015; Snyder et al., 2020). One recent controlled crossover trial (Aburto-Corona et al., 2016) found that the use of inorganic sunscreen hindered effective sweating whereas the use of organic sunscreen did not. A survey of more than 4,800 adult skiers and snowboarders at high-altitude ski areas in North America found that only 4.4 percent of respondents fully complied with sunscreen use guidelines (Buller et al., 2011).
Context of Sunscreen Use Among Multiple Behavioral Strategies for Reducing Overexposure to UVR
Multiple strategies are recommended to reduce skin exposure to UV radiation in addition to using sunscreen (Boothby-Shoemaker et al., 2022; Ou-Yang et al., 2017). These include protective clothing, hats, sunglasses, avoidance of outdoor activities during peak hours of sunlight (approximately 10 am to 2 pm), use of personal or group shade devices (umbrellas, tent or shade canopies). 70.8 percent of adults say they use one of three forms of sun protection most of the time when they are outside, but routine practice of each behavior is much lower—for sunscreen (33.7 percent as noted above), protective clothing (38.4 percent), and seeking shade (39.1 percent) (NCI, 2022). Even populations at greater risk from UV radiation—including melanoma survivors, transplant recipients, and those with photosensitive conditions—have inadequate sun protection practices (Biswas et al., 2020; Idorn et al., 2014; Jewett et al., 2020; Sainsbury et al., 2018). Of these behaviors, only sunscreen use has been evaluated in rigorously designed research, but experts recommend the use of multiple behaviors (e.g., FDA, 2021b). Available research shows that the various strategies for protection, sun avoidance, and covering up are usually not used in combination (Bleakley et al., 2018). However, it is important to understand how these other practices contribute to disease prevention, especially if environmental concerns result in a change in sunscreen usage.
Seeking shade is the most commonly used strategy for reducing exposure and harm from UV radiation outdoors. Currently 39 percent of U.S. adults report using this method of sun protection (Holman et al., 2018b; NCI, 2022). This trend of seeking shade has increased steadily since 1991, when only 29 percent of U.S. adults reported using this method (NCI, 2022). Although shade does not confer complete UV protection, studies have shown the ability of this method to reduce total UV exposure while allowing for some UV-induced vitamin D production in the skin (Holman et al., 2018b). Shade and sun-protective fabrics provide some degree of protection against ultraviolet radiation. The provision of shade structures and organization of outdoor activities with attention to shade can reduce UV radiation exposure and may ultimately decrease skin cancer risk (Buller et al., 2017; Fiessler et al., 2018; Gage et al., 2019; Holman et al., 2018b; Parisi and Turnbull, 2014). Deep tree shade blocks up to 95 percent of UV radiation, whereas sun-umbrella shade blocks much less (Saric-Bosanac et al., 2019). In addition to the variation in the characteristics of the shade structure (density of covering, natural versus artificial), the amount of UV reflected from the surrounding environment also varies (Holman et al., 2018b).
Shade protection may be inadequate in certain environments where light can reflect from the surface (Religi et al., 2018). On land, hard, smooth surfaces reflect more than grass and uneven surfaces, with beaches and snow-covered surfaces offering the most opportunity for increased albedo-based, or surface reflectance-based, UV exposures, emphasizing the need for additional protection, including the use of sunscreen in these settings. Light is also reflected by water, increasing potential exposures for boaters and others near the water. For areas of the skin that remain exposed even when in shaded outdoor areas, sunscreen use, hats, or protective clothing may also be required to avoid UV exposure.
Clothing has been used as a sun protection strategy since long before commercial sunscreens became available (Suozzi et al., 2020). Wearing clothing to protect the skin from UV exposures is the second most commonly used strategy in the United States, with 38 percent of adults using this method. Trends in protective clothing use have remained constant in the United States, at around 38 percent since 2005 (NCI, 2022). Although there are specific UV protective clothing items and brands, regular garments with dense weaves can often confer adequate protection. Clothing protective levels are evaluated by an Ultraviolet Protection Factor (UPF) standard measuring UVA and UVB blocking potential of clothing in-vitro (Li et al., 2019a). UPF is a measure of the ratio of average effective UV dose to unprotected skin to the average effective UV dose to skin protected by a fabric in question (Gies, 2007). UPF guidelines recommend levels of UPF 15 to 50+ for adequate protection. The efficacy of protective clothing to reduce or prevent UVR exposures depends on the UV-blocking potential as well as the amount of body coverage provided (Boothby-Shoemaker et al., 2022). One recent study found that currently available UV-protective clothing fabric provided better protection than sunscreen under controlled laboratory conditions (Berry et al., 2022). An observational study at a beach in Honolulu found differences in protective behavior between men and women, with women covering a larger proportion of their upper body than men and wearing hats that were
more protective (broad-brimmed) than men (caps) (Maddock et al., 2007). Overall, hats, sunglasses, shirts, and shade were used by less than 30 percent of beach visitors.
Routine sunscreen may be the only option in settings where unintentional UVR exposures cannot be avoided and the use of barrier protection is not always practical. These settings can include outdoor construction work, fishing, agricultural work, and specific athletic activities, including tennis, track and field events, swimming, and other outdoor aquatic recreation activities (Bens, 2014; HHS, 2014).
Skin Cancer Prevention Strategies and Initiatives
Educational efforts, reminders, ready availability of sunscreen dispensers and shade, and education directed at parents and spouses are examples of prevention strategies that can contribute to better compliance with recommendations for photoprotection (Biswas et al., 2020; Glaser and Tomecki, 2020; Hingle et al., 2014; Sarikaya Solak et al., 2020; Sumen and Oncel, 2021; Walburn et al., 2019, 2020; Weig et al., 2020; Zheng et al., 2021). Both individual strategies such as education and reminders, and environment/policy approaches such as shade structures and provision of free sunscreen are important contributors to improving public health by reducing exposure to UV radiation (Glanz et al., 2004). Policy and environmental change strategies have the potential to be uniquely powerful in that their impact does not rely on persuading individuals to change or on their understanding of detailed features of products (Glanz and Bishop, 2010; Glanz et al., 2004). This section provides an overview of important strategies and initiatives to prevent skin cancer; many do not independently evaluate sunscreen use as a behavior outcome. Evidence-based reviews that focus specifically on sunscreen use are also summarized below.
Beginning in the early 1970s, the high rates of skin cancers seen in Australia led to the implementation of one of the first wide-scale public health measures to change attitudes regarding sun exposure and intentional tanning behaviors. In 1977, the Anti-Cancer Council of Victoria launched one of the best-known public health campaigns for skin cancer prevention: “Slip! Slop! Slap!” The Australian strategy focused on three actions to reduce risks for skin cancers: slip-on UVR-protective clothing, slop on sunscreen, and slap on a hat. The campaign’s strategies have evolved to include multiple environmental, institutional, and behavioral approaches to reduce UVR overexposures that have helped to reduce lifetime risks for skin cancers (Montague et al., 2001). Since the launch of this campaign over 40 years ago in Australia, its wider adoption to address skin cancer prevention led to the current iteration, SunSmart, launched in 1988. The program continues to encourage sun-protective behaviors to minimize the human cost of skin cancer (Iannacone and Green, 2014; Montague et al., 2001; Reintgen et al., 1992).
In 1998, the Centers for Disease Control and Prevention (CDC) launched the national “Choose Your Cover Campaign” (Jorgensen, 2000). This campaign was designed to change social norms regarding sun protection and tanned skin and featured choices for sun protection, including using sunscreen with an SPF 15 or higher, wearing protective clothing, seeking shade, and wearing sunglasses and hats. This campaign was not formally evaluated and no results of its impact have been reported.
The SunWise School Program, developed by the U.S. Environmental Protection Agency (EPA) in 1999, was the first nationwide environmental and health education program for sun safety for children in elementary and middle schools in the United States. The program is modeled after components of Australia’s SunSmart program (Geller et al., 2003). The SunWise School Program’s overall goal was to provide photoprotection education and strategies to the nation’s schools (kindergarten through eighth grade). SunWise is consistent with the CDC guidelines for school programs to prevent skin cancer (Glanz et al., 2002b).
The Community Preventive Services Task Force1 (CPSTF) is an independent, nonfederal, unpaid panel of public health and prevention experts who identify effective public health interventions based on rigorous systematic reviews of peer-reviewed literature. The CPSTF conducted an initial evidence review of interventions to prevent skin cancer by reducing exposure to ultraviolet radiation that was published in 2003–2004 that found sufficient evidence to recommend education and policy approaches to increase sun-protective behaviors determined to be effective when implemented in recreational and tourism settings and in primary schools (Saraiya et al., 2004). However, they found insufficient evidence to determine the effectiveness of such programs when implemented in
___________________
1 See https://www.thecommunityguide.org/task-force/about-community-preventive-services-task-force.
other settings such as childcare centers and occupational settings, as well as community-wide multicomponent interventions and media campaigns alone (Saraiya et al., 2003, 2004). It is worth noting that the evidence for improved sun protection in recreation and tourism settings found improved “covering-up” behavior among adults (Saraiya et al., 2003). However, one large cluster randomized trial in aquatic settings found significant positive changes in children’s use of sunscreen and overall sun-protection, but only improved hat use and overall sun-protection among parents in the study (Glanz et al., 2002a).
An updated review of community-wide interventions to prevent skin cancer, and mass media interventions was reported in 2016 (Sandhu et al., 2016). The review found that multicomponent community-wide interventions resulted in significant increases in use of sunscreen at a median magnitude of 10.8 percentage points, a small decrease in UVR exposure, and a decrease in indoor tanning device use. Though mass media interventions yielded general improvements in UV protection behaviors among children and adults, the effects were not significant across the four included studies.
In addition to the CPSTF evidence reviews, the Cancer Control P.L.A.N.E.T. (Plan, Link, Act, with Evidence-based Tools) web portal includes resources to assist in planning delivery and implementation of evidence-based intervention (EBI) programs (NCI, 2020). Currently, there are 21 research-tested intervention programs designed to reduce the risk for UV damage and skin cancers in a range of settings, including school, workplace, clinical, and home settings. Twenty of these programs suggest using sunscreen as a method to prevent unintentional tanning, particularly in settings where barrier protection is not feasible (Sanchez et al., 2016). Many of the programs were included in the CPSTF evidence reviews, as well.
A series of large, cluster-randomized trials at swimming pools and outdoor recreation programs for children tested educational and environment-policy strategies to increase the use of sun protection practices, including sunscreen, among parents, children and lifeguards. The early studies found that both education and environmental-policy strategies increased solar protection behaviors (Glanz et al., 2001) and that the interventions reduced sunburns among lifeguards (Geller et al., 2001). Another study using targeted, peer-driven communication and social media found that the program reduced sunburns and increased sun protection behaviors among lifeguards (Hall et al., 2008).
Allen and Damian (2022) published the first systematic literature review focusing on studies of behavioral and environmental strategies that reported the endpoint of sunscreen use. Their review of 23 published studies found that education and tailored communications were effective for increasing sunscreen use in high-risk populations (e.g., melanoma survivors, fair-skinned persons). They also found that prompts or reminders, such as when the UV Index is high; and environmental changes such as increasing easy access to sunscreen, were effective for populations when they were outdoors and exposed to UV radiation (Allen and Damian, 2022). These findings are consistent with the systematic reviews and intervention trials in aquatic settings described above.
CORRELATES OF SUNSCREEN USE AND CHANGES IN SUNSCREEN USE
“Sunscreen use” is a complex behavioral concept, and for the purposes of this report it can be described in three distinct categories or dimensions. The first is whether or not to use sunscreen when outdoors in the sun, and how it is used (amount applied, thickness, and re-application). A second relevant behavior category involves correlates of choice of specific types of sunscreen based on the characteristics of the sunscreen (i.e., consumer preferences, and includes people’s understanding of sunscreen labeling and ingredients). A third category—relevant to choice and preference but uniquely relevant to this report—involves attitudes, knowledge and beliefs about the effects of sunscreens on aquatic environments.
Most available research on factors associated with sunscreen use comes from cross-sectional surveys or is based on other observational data, e.g., interviews, ratings of products online, observations. Thus, any inferences from these findings reveal correlates of sunscreen use without strong evidence of a causal relationship (warranting the description of “drivers” or “determinants”). A few controlled experimental studies report on changes in sunscreen use (e.g., Glanz et al., 2013, 2015) and are informative regarding strategies that were found to effect changes in sunscreen usage, mainly focusing on increased use.
Knowledge, Attitudes, Preferences, and Behavior of Consumers
Correlates of Whether or Not People Use Sunscreen
Adults’ sunscreen use in the United States when outdoors in the sun has remained level at about 34 to 38 percent in the past 10 to 15 years (Bleakley et al., 2018; Buller et al., 2011; Glanz et al., 2009; Holman et al., 2015; NCI, 2022). The demographic correlates of sunscreen use were described in a preceding section; females and fairer-skinned individuals are significantly more likely to use sunscreen.
Other factors associated with sunscreen use include more positive attitudes toward sunscreen and its benefits (Buller et al., 2011; Holman et al. 2015; Glanz et al., 1999), as well as knowledge, supportive policies in workplaces and recreation settings (Elliott et al., 2009; Glanz et al., 1999; Walkosz et al., 2008), and occupational sun exposure (Gies et al., 2009; Glanz et al., 2007; Horsham et al., 2014). Sunscreen use is higher at the beach, estimated at about 70 to 80 percent usage as described earlier. Further, one multimethod study in multiple regions of the United States found that swimming pools with very high levels of objectively measured sunscreen use had in place multiple organizational and environmental policies supporting sun safety and sunscreen use (Elliott et al., 2009). Also, a recent longitudinal analysis in Australia found that, over time, sunscreen has been increasing in its role as the “most favored” form of sun protection among adolescents and adults, compared to use of protective clothing and shade (Koch et al., 2017). The findings suggest that it is easier to get people to apply sunscreen than to use other sun protection modalities.
Correlates of Consumers’ Preferences and Choice of Sunscreen
Sunscreen use research and consumer online reviews of sunscreen products indicate that sunscreens with organic UV filters are on average most highly rated, and that sunscreens with inorganic UV filters are on average more expensive and sometimes considered less cosmetically acceptable than their organic UV filter counterparts; however, products of both types can be found among highly rated purchases (Prado et al., 2019a; Xu et al., 2016). Xu et al.’s analysis of online reviews of top selling sunscreen products indicates that consumers are most concerned with cosmetic elegance followed by perceived product effectiveness (Xu et al., 2016). Other features of interest to consumers were skin compatibility, ingredients, other recommendations (e.g., dermatologist recommended or recommended by the Environmental Working Group), and affordability. A more recent analysis of best-selling sunscreens on Amazon—the largest online retailer for sunscreen—found that the majority of best-selling sunscreen products were labeled as broad-spectrum and SPF of at least 30 (92.7 percent), though 27.1 percent were not compliant with AAD guidelines for adequate sun protection (either due to lack of water resistance, SPF lower than 30, and/or no broad-spectrum protection). The presence of organic or inorganic UV filter ingredients was not a determinant of being a best-selling sunscreen (both classes could be found in the best sellers). The study also found that sunscreens with six or more unregulated claims (e.g., “dermatologist recommended,” “natural,” “sport/active”) were highly likely to appear at the top of the best-seller list (Prado et al., 2019a). Of note, while there were many unregulated marketing claims, the label of being “reef-safe” or “reef-friendly” was not noted when the analysis was done, in August 2018. Surveys have also found that many users are unsure of whether their sunscreen provides broad-spectrum protection (Holman et al., 2015).
Recent surveys that asked consumers what is important in their choice of sunscreen have found that the most important qualities reported (in order of priority) are the level of sun protection (defined by SPF), broad-spectrum coverage, the ingredients, the feel of the product on the skin, and the price (Glanz et al., 2022). However, surveys have also found that many users are unsure of whether their sunscreens provide broad-spectrum protection (Holman et al., 2015) and that they are not sure about the main (active) ingredients or UV filters in their preferred sunscreens (Glanz et al., 2022).
A survey of 334 dermatology outpatients showed that fewer than ten percent could correctly answer three questions relevant to FDA-advised sunscreen labeling on sun protection factor, broad spectrum, and water resistance (Prado et al., 2019b). A recent study by Tribby et al. (2021) assessed consumers’ perceptions of the importance of active ingredients in sunscreen and how well they could recall those ingredients when choosing sunscreen products.
Most participants (72 percent) indicated that SPF was the most important sunscreen label information and only 11 percent reported that ingredients were most important. The participants were shown sunscreen bottles with FDA-consistent labels in random order and then asked to recall any active ingredients. Even though the sample (n = 47) was highly educated, only 11 percent could recall any ingredients on the labels they had seen (Tribby et al., 2021).
Attitudes and Knowledge About Sunscreen and Environmental Impacts
There are only a few empirical publications that report on attitudes and knowledge about sunscreen and potential effects on aquatic environments including coral reefs. The first publication on the topic was a master’s thesis by Woodruff (2019) that examined consumers’ willingness to pay more for “coral safe” sunscreen. A convenience sample of 348 adults responded to an online survey and on average, were willing to pay $17 for “coral-safe” sunscreen. There was an association between higher “pro-environment” beliefs and values and the willingness to pay more for sunscreen that they believed would be less damaging to coral reefs (Woodruff, 2019).
Levine (2020) surveyed 1,325 beachgoers in Hawaii (23 percent of whom were Hawaii residents) using a two-minute survey with multiple choice and open-ended questions. Findings showed that the most common reason for choice of sunscreen, based on a closed-ended question, was a higher SPF (42 percent), followed by the sunscreen being “non-toxic” to the environment (25 percent). The author noted the general lack of knowledge of respondents about which chemicals to avoid (Levine, 2020). It is noteworthy that this survey was conducted in fall 2018 and spring 2019, after the Hawaii “sunscreen ban” law was passed but 18 to 22 months before the law went into effect (see below). Also, it is noteworthy that the study provided no information about the validity or reliability of the survey items.
A third publication, by Casas-Beltrán et al. (2021), aimed to estimate the impact of tourist behavior on the discharge of sunscreen contamination in the Mexican Caribbean using surveys, interviews, and mathematical models to estimate “sunscreen pollution.” This study used different terminology than is most often used in the literature, with an emphasis on whether sunscreens were “biodegradable,” though the article did not give a definition of the term biodegradable. Their survey found that 78 percent of visitors believed that conventional sunscreen could cause pollution, and 58 percent that biodegradable sunscreen could also be a pollutant. However, only 10 percent of respondents said they used biodegradable or “ecological” sunscreens (Casas-Beltrán et al., 2021). There was little information about the surveys used, making it difficult to evaluate the measures’ validity.
Consumers concerned with environmental impacts might seek “reef-safe” or other similarly branded or certified products; however, there is no regulatory definition or oversight for what constitutes “reef-safe” that ensures it is scientifically meaningful or accurate. Despite that, these terms are prominently visible on the internet, in advertising, and on labels on sunscreen packaging (Tsatalis et al., 2020). A 2019 analysis of 97 of the most popular sunscreens (those with at least 150 reviews on Amazon) found that 52 (54 percent) were labeled as “reef safe,” and that 48 percent of those labeled as “reef safe” did not meet the criteria identified by NOAA or the legislative bans in Hawaii and Florida (Tsatalis et al., 2020). The use of certifications may also drive the behavior of consumers, with limitations similar to those noted above because there is no regulated or otherwise standardized definition of what makes a sunscreen “reef safe.” Certifications, such as those modeled on the Good Housekeeping Seal of Approval, have the potential to promote consumer trust and promote sales of products (Strach and Russell, 2003).
Media Communication, Advocacy, and Public Awareness
Early research which reported that UV filters caused damage to coral reefs was highly publicized in mass media in newspapers, on the internet, and in TV news and radio interviews (EWG, 2021; Glusac, 2018; NOAA National Ocean Service, 2021; The Ocean Agency, 2021; Ocean Conservancy, 2021; Save the Reef, 2021; Surfrider Foundation, 2021). Thus, the issue drew and continues to draw substantial public attention, making it important to understand the role of the media in communicating science and influencing public awareness and understanding of an issue.
There has been little formal attention to date to the spread of scientific information, and we are aware of no published study that has analyzed media spread of information on the topic of sunscreen use, UV filters, and
aquatic environments. However, recent attention to the complexity, process, and ethics of communicating about science (NASEM, 2017) have increasingly brought such issues to the attention of researchers. The difficulty of scaling up fact-checking (Allen and Damian, 2022) and the ease of sharing information based on limited research (Pennycook, et al., 2021) make it difficult to convey balanced and critical information to the general public or to scientists and health experts. The “stickiness” of early information on a topic of emerging interest (Lee et al., 2021; Wadhwa et al., 2021) creates a challenge for the public to understand and evaluate emerging findings. For example, the use of the terminology of “reef-toxic” sunscreen and “reef-safe” sunscreen have been widely used in public communications, advertising, and as labels on some sunscreen packaging. This is important to note because it creates confusion among consumers, given the lack of a scientific, health professional, or regulatory definition or guidance for identifying or labeling sunscreen products as “reef safe” or “reef friendly.” The complex issues of media communications and public understanding of this topic warrant continuing monitoring and analysis.
Current and Proposed Policies and Regulations to Restrict Sunscreens
Regulations and policies are intended to modify human behavior—both industry behavior (formulation, sales and advertising) and consumer behavior (purchase and use). Table 7.1 describes regulations or policies that have been passed or enacted to date to restrict usages of certain sunscreen ingredients. This provides a starting point for examining what changes in sunscreen usage may look like based on regulatory drivers, though policies may look different in the future. Notably, the regulations have focused on restricting all or some organic ingredients exclusively. All of the regulations/policies reference concerns about aquatic ecosystems, particularly coral reefs. The regulations in places in the United States (Hawaii, Maui, U.S. Virgin Islands) allow for access to sunscreens containing banned ingredients with prescriptions. However, since sunscreens are regulated as over-the-counter drugs, the relevance of allowing their use as prescription products is not clear. At present (July 2022), there are no available data on the monitoring, enforcement, or evaluation of the effects of these policies and regulations on either human sunscreen purchasing or use behavior or on aquatic environments. Anecdotal data indicate limited to no enforcement to date.
POTENTIAL CHANGES TO SUNSCREEN USE AND THE HUMAN HEALTH CONSEQUENCES
This section reviews the potential alternative scenarios to current use and choice of sunscreens, and information pertinent to the likelihood of each scenario happening. As noted earlier in this chapter, behavior and changes in behavior can be driven both by changes in availability of products and by messaging, regardless of availability. For each scenario about possible changes in sunscreen choice and use, this section describes what the resulting human health outcomes may be expected to be. A restriction on certain UV filters may have negative impacts on the use of sunscreen to prevent skin cancer and photoaging if it leads to reduced sunscreen usage (Cassel and Glanz, 2018), or it may have no impact, or even lead to strategies that cause positive impacts on health. The current modest use of sunscreen and other photoprotection measures, perceptions about the ingredients in different sunscreens and their safety for humans and the environment, consumer preferences, and the higher cost of some alternatives may all contribute to changes in skin cancer prevention. Notably, if higher cost is a factor, there may be differences in health outcomes between affluent and disadvantaged populations. However, to date there has been very little research about people’s knowledge and attitudes about these issues and their understanding of the provisions of sunscreen policies, restrictions, or bans (Glanz et al., 2022; Levine, 2020; Woodruff, 2019; Tribby et al., 2021). Neither have there been studies that evaluate the effect of these policies on human health (or on the environment). Available research on sunscreen use behavior, reviewed in this chapter thus far, is the best available guide to predict future behavior.
The assessment of health impacts and the information related to the likelihood of each scenario occurring were informed by the research summarized in this chapter or otherwise referenced in each description. The impact on health outcomes related to preventing skin cancer was based on sunscreen efficacy and not human safety of UV filters, which was not in the committee’s Statement of Task. In all scenarios, the availability of SPF 30+ and
TABLE 7.1 Regulations and Policies to Limit UV Filters Used in Sunscreen
| Location | UV Filters | Prohibitions | Status | Citation |
|---|---|---|---|---|
| U.S. Locations | ||||
| Hawaii | Oxybenzone, octinoxate | Ban of sale within the state of Hawaii without a prescription. Does not apply to online sales. Does not prohibit tourists from bringing banned ingredients. | Passed May 2018; in effect January 1, 2021 | Hawaii SB 2571 |
| Maui County, Hawaii | All organic (“non-mineral”) UV filters | Bans sale, use, or distribution without a prescription. | Passed December 6, 2021; in effect October 1, 2022; enactment pending review by Mayor | Bill No. 135, Ordinance No. 5306; Tanji, 2021 |
| Hawaii 2022 | Ingredients not recognized as GRASE | Bans sale, use, or distribution without a prescription. | SB 2949 deferred indefinitely; SB 3001 deferred to January 1, 2050, HB 1519 deferred to July 1, 2100 | SB 2949 SB 3001 HB 1519 |
| U.S. Virgin Islands | Oxybenzone, octinoxate, octocrylene | Bans sale, distribution, and use without a prescription. | Passed July 20, 2019; in effect March 30, 2020 | Bill No. 33-0043, Act No. 8185 |
| Non-U.S. Locations | ||||
| Palau | Oxybenzone, octinoxate, octocrylene, plus 7 othersa | Bans sale and distribution. Tourists may not bring sunscreens with banned ingredients with them. | Passed in October 2018; in effect January 1, 2020 | Senate Bill 10-135 |
| Thailand | Oxybenzone, octinoxate, 4-methylbenzylidene camphora, and butylparabena | Bans use in national parks. | Announced August 3, 2021 | TAT News, 2021 |
| Aruba | Oxybenzone | Bans the import, manufacture, sale, or free distribution. | Passed November 27, 2019; in effect July 1, 2020 | Landsverordening verbod voor het milieu, Afkondigingsblad van Aruba 2019 no. 67 [National Ordinance prohibiting environmentally harmful products, Bulletin of Aruba 2019 no. 67] |
| Bonaire | Oxybenzone, octinoxate | Bans use. | Passed May 15, 2018; in effect January 1, 2021 | |
| Mexico (various locations in the Yucatan Peninsula) | Non-biodegradable UV filters | Bans of use at individual protected areas. In some cases, no sunscreens at all are permitted. | Various, as early as 1986 in some places | Various, summarized in Casas-Beltran et al. (2021) |
a Ingredients not available in the United States.
broad-spectrum sunscreen was considered to be a basic requirement for prevention of skin cancers, sunburn, and photoaging. Importantly, this evaluation reflects the current state of knowledge and could change as more information becomes available.
The following scenarios are likely to lead to negative effects on health:
- Decreased use of sunscreen with no change to other sun protective behaviors: This scenario would occur if preferred sunscreen ingredient(s) are unavailable, resulting in use of sunscreen at either reduced frequency or in reduced quantities with no compensating behaviors. The likelihood of this scenario is dependent on which ingredients are removed from availability. Notably, some evidence shows that consumers are more likely to have preferences for sunscreens with organic ingredients due to their cosmetic appeal even if they are unaware of the ingredients themselves (Xu et al., 2016). Restrictions on a small number of organic UV filters would have less impact than restrictions on many or all organic UV filters. This assumes broad spectrum, SPF 30+ coverage could still be maintained with those that remain, and some UV filters have fewer replacements than others in regard to the range they protect against, such is the case for avobenzone. Additionally, regardless of ingredients, messaging about environmental impacts may confuse some people to think all sunscreen is harmful to the environment.
- Decreased use of sunscreen with suboptimal increases in other sun protective behaviors: This scenario would occur if preferred sunscreen ingredient(s) are unavailable, resulting in use of sunscreen at either reduced frequency or in reduced quantities but with some compensating behaviors such as covering skin (e.g., clothing, hats) and sun avoidance (e.g., shade, avoiding sun exposure in peak times). Because shade and clothing alone provide only partial protection against UV radiation (Boothby-Shoemaker, 2022; Religi et al., 2018), such coverage would be inadequate. While the overall impact on health is likely to still be negative, it is less so than the scenario where no alternative behaviors are employed. Routine use of protective clothing and shade is not prevalent, with under 40 percent of the population practicing each protective measure on a routine basis (NCI, 2022). The use of skin protection behaviors other than sunscreen is likely to be situation dependent rather than be a complete transition to alternate behaviors (e.g., occupational exposure where shade is unavailable; during athletic events; use of shade on a beach but not when entering the water) (Bens, 2014; HHS, 2014).
- Use of alternative sun protection products with UV filters that do not meet FDA standards: This scenario would occur if people choose to use “natural products” rather than those containing UV filters that remain on the market. These may not provide good quality UVR protection and are inconsistent in quality and thus would be expected to have a negative impact on health. Interest in “natural” sunscreen alternatives, i.e., products not meeting standards set by FDA for marketing as sunscreens, is surprisingly common with inorganic minerals (other than those approved for use), lignin, melanin, silymarin, and other ingredients being incorporated into formulations (He et al., 2021a; Kumar and Jose, 2020; Nery et al., 2021; Solish et al., 2020). A recent study found substantial variability in photoprotection and human safety among these products (Thompson et al., 2021). However, do-it-yourself sunscreen tutorials are widely viewed online (Julian et al., 2020).
These scenarios are likely to lead to no or minimal effects on health:
- Decreased use of sunscreen with optimal practice of other sun protective behaviors: This scenario would occur if preferred sunscreen ingredient(s) are unavailable, resulting in use of sunscreen at either reduced frequency or in reduced quantities with uptake of recommended compensating behaviors such as shade-seeking, use of hats and protective clothing, and sun avoidance. The practice of multiple UV protective behaviors in order to achieve substantial protection against UV radiation depends on individuals making well-informed choices consistently, and also supportive environments. However, some outdoor activities and employments do not lend themselves to use of these alternatives or there is insufficient uptake in these practices. Even among those at highest risk for skin cancer, use of alternatives is suboptimal. The
- marketplace and organizational (e.g., pools, schools, worksites) policies for high-quality provision of shade and scheduling to avoid peak UV exposure hours may be necessary. While these can be found in some locations (Elliott et al., 2009), it is often challenging to enact (Kapelos and Paterson, 2014).
- Obtaining sunscreens with restricted ingredients from elsewhere: This scenario will occur when visitors bring sunscreen with them or when residents import sunscreen from places where any restricted ingredients remain for sale. Policies that only ban sale but not use of certain UV filters would allow for this scenario to occur. Tourists are very likely to bring sunscreen with them to vacation destinations. In May 2021, 80 percent of out-of-state tourists visiting a popular marine snorkeling beach park reported bringing sunscreen with them in their luggage (Cassel and Glanz, in review). Less is known about the likelihood that residents will purchase sunscreen elsewhere.
- Switching to alternate formulations: This scenario would occur when consumers use sunscreens that contain UV filters that have not been restricted. Like the scenario of decreased use, this will also be dependent on which ingredients are removed from availability. If available formulations are cosmetically appealing and provide broad-spectrum protection—two key concerns that drive consumer behavior (Prado et al., 2019a; Xu et al., 2016)—the likelihood of this scenario is higher.
This scenario is likely to lead to positive effects on health:
- Increased use of sunscreen: This scenario may occur if there is a multilevel sunscreen-use campaign that includes provision of free sunscreen at beaches and pools and/or ensures favorable pricing for available sunscreens, and includes consistent, effective communications that educate and motivate people to use sunscreens with the available, unrestricted ingredients. This would include increased rates of adoption of the full suite of sun-protective behaviors, including sunscreen. Based on limited intensity and reach of past skin cancer prevention campaigns, such as the “Choose Your Cover” campaign by CDC, an additional campaign may have some but still limited impact. Some beaches have provided sunscreen to promote use but this has not been widespread.
As noted in several of these scenarios, the likelihood of each occurring—and therefore the resulting human health outcomes—is in part dependent on which UV filters remain available. The ability to produce broad spectrum SPF 30+ that people will actually use (typically requiring a mixture of UV filters) is a key determinant of health outcomes. Coverage across UVA1, UVA2, and UVB wavelengths, and the strength of protection a UV filter provides, will be important in the selection of UV filters that remain on the market. As described in Chapter 2, there are multiple and complex chemical considerations that go into developing an effective sunscreen including its stability, substantivity, and cosmetic appeal or ease of use. It is important to add that the above analysis is based on the current availability of UV filters as active ingredients, and the introduction of new active ingredients and combinations of ingredients through industry innovation and FDA approval may change these outcomes.
FINDINGS AND KNOWLEDGE GAPS
Based on the information reviewed in this chapter, the committee highlights the following areas as key findings from the information as well as gaps in knowledge pertinent to understanding the implications of changing sunscreen availability and usage on human health.
Finding: Exposure to UVR causes sunburn and photoaging in human skin and is a risk factor for the development of skin cancers, both keratinocyte carcinomas and melanomas.
Finding: Consistent use of broad spectrum, SPF 30 sunscreen when outdoors reduces the risk of developing skin cancer (keratinocyte carcinomas and melanomas), photoaging, and sunburn.
Finding: Only about a third of the U.S. population uses sunscreen regularly, though use is higher during outdoor activities and at the beach (between 70 percent and 80 percent). Even when sunscreen is used, dosage (i.e., amount applied and rate of reapplication) usually does not meet recommendations for optimal effectiveness.
Finding: Sunscreen preferences are primarily driven by perceived effectiveness (e.g., SPF) and cosmetic preferences (e.g., skin feel, scents, and appearance on skin). These features can be influenced by UV filters and other ingredients in sunscreen. However, in general, consumers are not knowledgeable about the ingredients in their sunscreens. Some consumers can also be influenced in their choice of sunscreens based on perceived impacts on the environment.
Knowledge Gap: At present, there are no available research findings that definitively evaluate the human behavioral and health outcomes of restricting UV filters in sunscreen in one or more locations, for measuring the impact on human health in the short run, or in populations with different skin cancer risks. The use of natural experiments (as described in Bor, 2016; Craig et al., 2017b) before and after policies are enacted would be the most promising way to assess changes in sunscreen use and the effects on human health, including rates of skin cancer. Such natural experiments could involve comparisons between similar locations with and without regulations/restrictive policies, assessed before and after the policy is put in place, and with varying levels of enforcement of those policies, would be most informative. In addition, risk prediction modeling studies (e.g., Rigotti and Wallace, 2015; Stern et al., 1986; van Dijk et al., 2013) could be designed to address these potential incidence, morbidity, and mortality outcomes related to skin cancers, given potential changes in sunscreen, effectiveness, availability, and use.




















