
Summary1
Serious vulnerabilities have been present in global medical product supply chains for many years. Some of these have been highlighted by the ongoing COVID-19 pandemic—where shortages of masks and personal protective equipment for health care workers, medical products used to treat COVID-19, and medications to treat related conditions have put the lives of Americans at risk and compromised the U.S. health care system. In response, the U.S. government has urged a “whole-of-government approach to assessing the vulnerabilities in, and strengthening the resilience of, critical supply chains.” Section 3101 of the Coronavirus Aid, Relief, and Economic Security (CARES) Act, signed into law on March 27, 2020, directed the secretary of the U.S. Department of Health and Human Services (HHS) to enter into an agreement with the National Academies of Sciences, Engineering, and Medicine (the National Academies) to establish an ad hoc committee to examine the security and resilience of U.S. medical product supply chains. The full charge to the committee is presented in Chapter 1 of this report.
In many ways, medical product supply chains resemble supply chains of other products. They consist of multiple stages, which are often carried out by different organizations in different parts of the world. However, because medical products are particularly important to human health, medical product supply chains have some unique characteristics, including higher levels of oversight and regulation. To date, the primary emphasis of regulatory oversight in the United States has been product quality, with
___________________
1 This Summary does not include references. Citations for the discussion presented in the Summary appear in the subsequent report chapters.
a secondary focus on cost. But as the COVID-19 pandemic powerfully reminded the nation, supply reliability is also vital to human health. The investment, both financial and human capital, that government and private industry has made in the supply reliability of medical product supply chains has not been sufficient to meet the public health need. In keeping with the committee’s charge, this report focuses specifically on the resilience of medical product supply chains, which is defined as the ability to prevent public health and safety from being compromised by disruptions to supplies of medical products.
Supply shortages of medical products can be the result of many types of events, including production process problems (at the final product level or at any prior level of the supply chain), inadequate or unacceptable quality, natural disasters, disease outbreaks, geopolitical events, and many more. To improve the resilience of medical product supply chains, the risks to such events need to be assessed and strategies identified to reduce those risks. However, because other social needs also demand resources, it is vital to consider cost.
DEFINING SUPPLY CHAIN CRITICAL MEDICAL PRODUCTS
To identify measures that will have the greatest effect on public health and safety per dollar invested, it is important to first determine which medical products warrant attention. The U.S. Food and Drug Administration (FDA) defines essential drugs and devices as those “that are medically necessary to have available at all times.” However, a product that is medically essential under this definition, but already has a highly reliable supply chain, is a poor target for resilience investments. Therefore, the committee defines the term supply chain critical medical products as those that are both medically essential and vulnerable to shortages.
Chapter 5 describes a formal supply chain criticality score that represents risk as the expected patient harm attributable to the disruption of the supply of a given product. This score is given by the product of a measure of medical criticality and a measure of supply risk. By focusing attention on medical products that present the largest expected health risk to the public, this definition encourages cost-effectiveness through measures that protect large numbers of people. However, shortages of some products can present very grave risks to small groups of people. Other products present unlikely but extreme risks. In the interests of equity and national security, the committee advocates for including certain products on the list of supply chain critical medical products beyond those included for reasons of maximizing overall public health and safety. These considerations are discussed in more detail in Chapter 5.
UNDERSTANDING MEDICAL PRODUCT SUPPLY CHAINS
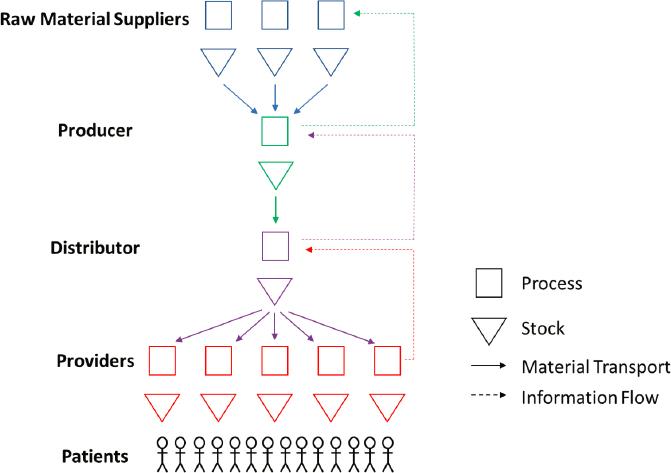
To increase the resilience of medical product supply chains, the causes of the supply disruption risks they face must first be understood. This in turn requires an understanding of the basic structure of medical product supply chains. Chapter 2 provides a high-level overview of medical product supply chains and how they differ depending on the product. These chains are complex, multistage, global systems that involve people, processes, technologies, and policies. Medical product supply chains facilitate the flow of drugs and devices from raw material or component suppliers (e.g., makers of ingredients or subassemblies) to producers (e.g., final assembly plants, fill-and-finish facilities) to distributors (e.g., wholesalers) to providers (e.g., health systems, pharmacies, retailers) and finally to patients (Figure S-1). A variety of stakeholders, including government agencies, raw material suppliers, manufacturers, distributors, group purchasing organizations, health systems, providers, and patients influence the behavior of medical product supply chains.
Medical product supply chains—which for the purpose of this report is an all-encompassing term that includes the supply chains for drugs, biologics, medical devices, and medical equipment—deliver a diverse array of drugs and devices, including the four main categories described in this
report.2 Product types have production processes and supply chains that vary considerably depending on product characteristics. When considering measures to increase supply chain resilience for a specific medical product, these characteristics can be important to consider. But when considering broader public policy measures, it is helpful to group products into classes.
Drugs can be divided into originator and generic products. A generic drug is a medication developed to be equivalent to an already marketed brand-name drug in dosage form, safety, strength, route of administration, quality, performance characteristics, and intended use so that the generic medicine works in the same way and provides the same clinical benefit as the brand-name medicine. In general, margins are much lower on generic drugs than on original drugs. Because this implies that generic drug producers have less financial incentive to protect supply continuity, generics are more prone to routine supply disruptions and quality deviations and are thereby more likely to warrant inclusion on the supply chain critical list. Within the supply chains of both generic and originator drugs, two basic steps occur: (1) the basic production of bulk-drug substances, commonly referred to as active pharmaceutical ingredients (APIs) and pharmaceutical excipients and (2) the pharmaceutical manufacturing of finished dosage form (FDF) drug products. This is important to supply chain risk assessment and remediation because API or incipient production may pose significant risks of shortages but is all but invisible to both buyers and regulators because the producer identity and location for inputs is not generally disclosed by drug manufacturers.
Medical devices are defined by FDA as any object or component used in the diagnosis, treatment, prevention, or cure of medical conditions or diseases, or that affects body structure or function through means other than chemical or metabolic reaction in humans or animals. For regulatory purposes, devices are divided into three classes. Class I medical devices present minimal potential for harm to the user and are often simpler in design than Classes II and III. Class II medical devices present moderate risk of harm to the patient or user. More than 50 percent of FDA-regulated medical devices are considered Class II. Class III medical devices are highly complex devices that also present a high safety risk to the patient and user. These classes
___________________
2 This report does not focus in detail on supply chains for biologics or vaccines given the distinct features in their supply chains. However, as some biologics and vaccines are high-margin, patent-protected pharmaceuticals while others are not, the discussion of profit margins and incentives between originator and generic drugs is still applicable to these medical products. Furthermore, four new reports from the National Academy of Medicine focus on how to prepare for seasonal and pandemic influenza through lessons learned from COVID-19—with one report in particular focusing on globally resilient supply chains for pandemic and seasonal influenza vaccines. These reports can be accessed here: https://nam.edu/four-new-reports-from-the-national-academy-of-medicine-focus-on-how-to-prepare-for-seasonal-and-pandemic-influenza-through-lessons-learned-from-covid-19.
were established primarily to regulate product quality. However, the fact that Class III devices present the highest safety risks does not mean they present the highest supply disruption risk. Complex Class III devices, such as pacemakers, have high margins that motivate producers to protect their supply chains in order to protect their revenue streams. In contrast, less risky Class II devices, such as N95 respirators, have lower margins that lead producers to leave them vulnerable to shortages. As seen in the early months of the COVID-19 pandemic, shortages of relatively simple personal protective equipment (PPE) products can present serious public health risks.
There are two important insights from this overview of medical product supply chains. First, there is no one-size-fits-all strategy for increasing supply chain resilience for all medical products, which implies that a key challenge is to match resilience measures to products in a cost-effective manner. Second, current classification schemes for medical products are sometimes based solely on clinical importance, which implies the need to factor in shortage risks when making decisions about improving the resilience of medical product supply chains.
GLOBALIZATION OF U.S. MEDICAL PRODUCT SUPPLY CHAINS
As has been the case in other industries, the past several decades have been a time of rapid globalization for U.S. medical product supply chains. As described in Chapter 3, medical product companies have increasingly sourced production of products, components, and raw materials from locations around the globe that offer cost-effectiveness, skilled labor, and the necessary infrastructure to support manufacturing and distribution. This globalization has provided benefits to U.S. producers, consumers, investors, and health care providers, such as lower costs, expanded efficiency, and greater resources to invest in innovation in some cases, but also in the form of supply security because of diversification and innovation driven by competition.
However, globalization also has downsides. International production is more difficult to inspect and regulate than domestic production. This has contributed to a rash of quality problems in generic drugs that peaked in 2011 but remains an ongoing source of safety and supply problems. Long, global supply chains spread around the world are also less transparent than short, domestic ones. As a result, purchasers of medical products often do not know where they are produced and almost never know where the ingredients and components they contain are sourced from. Even FDA does not have detailed enough information about global medical product supply chains to enable assessment of vulnerabilities.
These issues have led to widespread calls for the on-shoring of medical product manufacturing. Unfortunately, many calls fail to specify what
on-shoring actually means. Often it seems that the recommendations are to move final assembly to domestic sites without a recognition of the rest of the supply chain. By themselves, such moves will have a limited effect on supply reliability because they leave supplies vulnerable to disruptions in the supply of necessary inputs. Moving all stages of production to the United States would be highly daunting for supply chains with more than a few stages. Even if it were possible, it could significantly increase operating costs.
Consequently, on-shoring is not the panacea it is sometimes presented as. But this does mean that it cannot be part of a cost-effective strategy to improve the resilience of medical product supply chains. To properly determine if and when on-shoring is appropriate, on-shoring proposals need to be vetted financially against alternatives. To facilitate this, and more importantly to identify the components of a cost-effective strategy for medical product supply chains, a framework is needed for systematically enumerating alternatives.
CAUSES OF FAILURES OF MEDICAL PRODUCT SUPPLY CHAINS
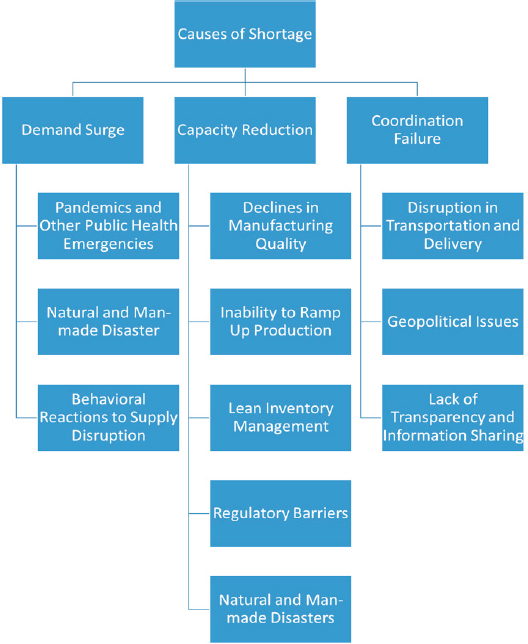
A precursor to creating a framework for resilient medical product supply chains is to describe the mechanisms that lead to supply shortages. To do this, the committee examined how trigger events, including natural disasters, infectious disease outbreaks, or manufacturing process problems, can disrupt medical product supply chains in three primary ways:
- Demand surge: An event drives demand for a medical product well above the normal level for an extended period of time. For example, a major natural disaster, such as a tornado or earthquake, can spike regional demand for certain medical products if these events result in a significant number of casualties requiring medical care. As seen during COVID-19, a pandemic can drive up global demand for many medical products.
- Capacity reduction: One or more production or transport processes are impeded by lack of assets, power, or people. For example, a natural disaster could cause a factory to lose power and halt production or regulatory barriers or manufacturing quality problems could restrict the output of a supplier or producer, and could even eliminate inventory stock if a product is recalled. As seen during the COVID-19 pandemic, production of some products may have decreased because of lockdown measures or the need for workers to quarantine or be on sick leave.
- Coordination failure: Events that prevent supply from being matched to demand can cause shortages of medical products even
- when total supply is sufficient to meet total demand. For example, geopolitical issues or communication system failures during a hurricane or other natural disaster can reduce or obstruct the delivery of emergency supplies to the people that need them.
It is important to note that disruptions can overlap and interact—demand surges and capacity reductions may occur simultaneously, or capacity reductions may precipitate subsequent demand increases and vice versa. Additionally, disruptions do not cause medical product supply chains to shift instantly from the normal conditions to shortages. Because all supply chains contain at least some amount of inventory, and because decision makers will take steps to increase capacity or implement flexible strategies in response to an impending shortage, it will take time for a disruption to turn into a shortage experienced by patients. Chapter 4 describes the different causes of failures of medical product supply chains and provides examples of each (Figure S-2).
FRAMEWORK FOR IMPROVING THE RESILIENCE OF MEDICAL PRODUCT SUPPLY CHAINS
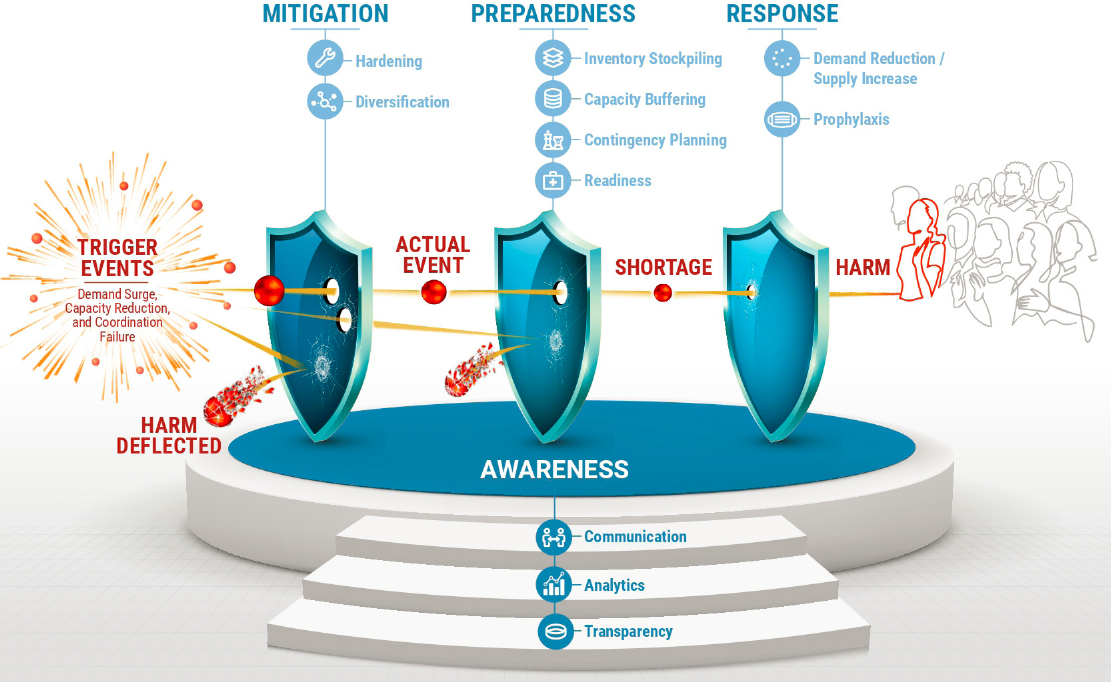
The key challenge of a medical product supply chains resilience framework is to identify the means for preventing trigger events from leading to human harm. As such, the resilience of medical product supply chains is an example of a reliability problem—albeit a complicated and difficult one because there are many resilience options available that fit together in intricate ways. Nevertheless, the basic concepts of system reliability and supply chain management can be invoked to create a framework that systematically categorizes means for providing a desired level of protection for a given medical product. Figure S-3 graphically illustrates such a framework by depicting the path from a potential trigger event (see Figure S-2) to public harm, with successive layers (or shields) of protection in between. In this figure, each shield represents a category of measures to prevent or reduce harm to the public’s health and safety from shortages in medical product supply chains. The options within these categories comprise the building blocks of a resilience strategy for medical product supply chains.
Note that the shields in Figure S-3 are organized chronologically. The awareness category, shown as a foundation for the shields, is a precursor for the other three categories and includes measures that provide the information needed to implement them. The mitigation shield includes measures that reduce (possibly to zero) the extent to which a trigger event results in a supply shortage. The preparedness shield includes measures that reduce (possibly to zero) the extent to which a supply shortage reaches patients or providers. And finally, the response shield reduces (possibly to zero) the extent to which a supply shortage that reaches patients and providers causes harm to health and safety. The framework in Figure S-3 shows the shields deflecting the balls (threats caused by trigger events) to represent full prevention of harm, and also reducing the size of the balls to represent reduction in the magnitude of harm.
In addition to simply enumerating resilience options, overarching insights can be applied to help prioritize options for cost-effectiveness. In the framework of Figure S-3, a cost-effectiveness hierarchy is suggested among the protection shields in order of their timing. That is, in general, using awareness measures to give supply chain actors information to make better decisions is more efficient than using mitigation measures to avoid a shortage, which is more efficient than using preparedness measures to prevent shortages from reaching people, which is more efficient than using response measures to deal with shortage situations after the fact. This implies that a resilience strategy for medical product supply chains should carefully consider the awareness foundation and the early protection shields before thinking about the later shields.
However, the law of diminishing returns from economics implies that the cost-effectiveness of incremental investments in any single resilience measure will decrease as the amount of investment increases. For example, the cost of each additional unit of inventory in a stockpile is the same but the amount of protection provided decreases because the likelihood of needing the extra inventory declines. This suggests that a diversified strategy that uses a balance of different supply chain measures will be more cost-effective than one that relies on a single measure. Therefore, although while the protection shields should be considered in chronological order, it is also important to consider how far to go in each shield and how to fit measures from the different shields together. This process is discussed in Chapter 5 and is used to describe the connections between the committee’s different recommendations in Chapters 6–9.
Finally, it must be acknowledged that shortages in medical product supply chains are in part the result of a market failure. Profit motives of manufacturers and vendors motivate a smaller investment in protection than is optimal from a public health perspective. Basically, firms have an incentive to protect supply continuity at a level that maximizes profits, while society has an incentive to protect supply continuity at a higher level that preserves public health. Consequently, the committee’s recommendations include some necessary regulatory components. However, where possible, the committee’s recommendations call for incentive-based solutions instead of behavior-forcing solutions that tap the power of the market to innovate and compete.
With the framework of Figure S-3 and the above observations, seven recommendations were identified as key to building resilient supply chains for medical products.
AWARENESS
Awareness across the entire medical product supply chain ecosystem requires transparency activities from regulators, suppliers, producers, distributors, and providers. The more transparency stakeholders bring into medical product supply chains, the better positioned they will be to identify vulnerabilities and proactively mitigate, prepare for, and respond to potential disruptions in medical product supply chains. As health system purchasing agents have long known, and the COVID-19 pandemic has made glaringly obvious, it is not always known where key components of the medical products are made or where in the supply chain medical products are. The current practice of keeping medical product supply chains confidential conflicts with public health needs and puts the public’s health at risk. Improving the public’s access to data that is important to their health and well-being is critical. Furthermore, lack of transparency and limited
visibility into medical product supply chains have led to limited empirical evidence for identifying best strategies to address supply chain issues. These limitations also hamper the government’s ability to work effectively with industry and other partners to increase the resilience of medical product supply chains.
Awareness measures can be broken into three categories: (1) transparency activities that make data available, (2) analytics activities that process data into useful information, and (3) communication activities that get the information into the hands of the people responsible for mitigation, preparedness, and response. Over the longer term, efforts should be established to collect, compile, and disseminate medical product supply chain data from these various stakeholders to increase end-to-end awareness to identify and mitigate risks. In the short, immediate term, the committee identifies upstream transparency efforts as a critical first step to increasing the resilience of medical product supply chains. The committee offers two recommendations pivotal to collecting, compiling, and disseminating the data on where and how medical products are made. Recommendation 1 (Public Transparency) addresses the significant gap in the data needed to assess and address risks in medical product supply chains by calling for both quality transparency (via risk-based site selection scores becoming public) and supply chain transparency (via all FDA Establishment Identifier [FEI] location data made public for where products are made).3 These two dimensions of transparency (quality and supply chain) each have different sources. Quality data are currently kept by regulators, but they are not available to the public or manufacturers and distributors. Supply chain data are currently kept by manufacturers, but they are not available to the public or regulators. Recommendation 1 (Public Transparency) also calls for volume and capacity transparency to further assess risks directly related to medical product supply chains and to evaluate strategies for ameliorating these. Transparency is required both from manufacturers and from regulators so the public can be both informed about available medical products and empowered to act upon these data through data analysis and potentially put pressure on regulators and lawmakers. These data will enable the mapping of medical product supply chains, the identification of vulnerabilities such as supply concentrations, and the assessment of what
___________________
3 Making certain data submitted to the FDA transparent to the public may also warrant certain legislative changes. For instance, it might necessitate a statutory amendment in the form of a change to section 301(j) of the FD&C Act (21 U.S.C. § 331(j)), which would be required only to the extent that the data that are proposed to be disclosed outside HHS are deemed as “concerning any method or process which as a trade secret is entitled to protection.” In addition, 18 U.S.C. § 1905 (the Trade Secrets Act) would have to be amended to the extent the disclosed information “concerns or relates to … trade secrets, processes, [or] operations … or to the identity [or] confidential statistical data” of any company, unless disclosure of that information is otherwise “authorized by law.”
medical products are most at risk. Specific data essential to transparency are discussed further in Chapter 6. Without this information, it is nearly impossible to make use of the supply chain resilience framework to identify measures for reducing risks to public health and safety.
Recommendation 1 (Public Transparency). The U.S. Food and Drug Administration (FDA) should take steps to make sourcing, quality, volume, and capacity information publicly available for all medical products approved or cleared for sale in the United States. These steps include the following:
- The manufacturer for a pharmaceutical drug should be required to publicly disclose the manufacturing location, in particular the FDA Establishment Identifier (FEI), the city, and the country, for the finished dosage form (FDF), active pharmaceutical ingredient (API), major excipients, and major packaging and delivery devices for all pharmaceutical drugs sold in the United States. API manufacturers shall be required to publicly disclose the sources of raw materials. This information should be made available on the labels for all pharmaceutical drugs and in a publicly accessible database. The National Drug Code should be associated with the primary FEI (where a majority of the volume is manufactured) in the database.
- FDA should make publicly available their risk-based Site Selection Model scores for all pharmaceutical drug manufacturing facilities that make drugs sold in the United States. FDA should also make public the Office of Pharmaceutical Quality (OPQ) scores. The risk-based Site Selection Model scores for the API and FDF plants (e.g., FEIs) should be made available on the labels for all pharmaceutical drugs and in a publicly accessible database, and the OPQ scores should also be included in this database.
- The manufacturer for a medical device should be required to publicly disclose the manufacturing location, in particular the FEI, the city, and the country, for the primary manufacturing and final assembly steps for all medical devices and major components sold in the United States. This information should be made available on the labels for all medical devices and in a publicly accessible database. The part number should be associated with the primary FEI (where a majority of the volume is manufactured) in the database.
- The risk-based Site Selection Model score for the primary manufacturing and final assembly plants (e.g., FEIs) should be made
- available on the labels for all medical devices and in a publicly accessible database.
- Sourcing and quality information should be provided as part of the pharmaceutical drug or medical device approval or clearance processes and on an ongoing basis in order to retain a license or clearance to sell in the United States.
- Drug volume data reported to FDA, as mandated by the CARES Act, should be made available in a publicly accessible database. This requirement should be expanded to include reporting of capacity, in addition to volume, and should be required for medical devices, in addition to drugs.
- To the extent that amendments to the Trade Secrets Act at 18 U.S.C. § 1905 and to the Food, Drug, and Cosmetic Act at 21 U.S.C. § 331(j) are necessary to permit public disclosure of all the sourcing, quality, volume, and capacity information referenced in this recommendation, Congress should make such amendments.
However, data by themselves are not information. To enable stakeholders to make better decisions, data must be compiled into useful forms and disseminated to those who need it. Merely including supplier identity and location information on labels will not by itself enable health system purchasers to reduce their risk of supply disruptions or enable government officials to determine how and where to spend resources to protect the public health from such disruptions. Therefore, Recommendation 2 (Public Database) calls for the establishment of a publicly accessible database that summarizes supply chain information for medical products. Making the database public allows analyses and compilations to be done by both government actors and third parties. This will facilitate the use of sophisticated technologies, such as artificial intelligence, to process data and evaluate the type and degree of supply chain risks to medical product supplies.
Recommendation 2 (Public Database). The U.S. Food and Drug Administration (FDA), in cooperation with other U.S. government agencies, should establish a publicly accessible database containing the supply chain information acquired for medical products. FDA, in cooperation with other U.S. government agencies, should use the information on medical product supply chains it acquires to
- Understand better the vulnerabilities of medical product supply chains as a whole.
- Perform risk assessments regarding the risks to the total supply of particular medical products in both normal and emergency scenarios.
- Coordinate, conduct, and compile research on the resilience of medical product supply chains, including by funding independent research that uses the established database.
- Track the ways in which increased transparency, and the prediction of potential medical product shortages through data tracking, support improved supply chain resilience and functionality.
- Incentivize the establishment of third-party rating system(s) for risk and quality.
Making this type of supply chain risk information publicly available will produce a host of predictable benefits. For example, a rating system that makes disruption risks visible will enable health system purchasers to factor supply reliability into their purchasing decisions. This in turn would provide an incentive for producers to improve supply chain reliability. Highlighting risks will also enable policy makers to prioritize programs for protecting public health by focusing on areas of greatest vulnerability. Finally, by placing more data into the hands of analysts, this public database creates the potential for new and useful insights. For instance, researchers may detect previously unknown risk predictors that could be used to design new and effective resilience measures for medical product supply chains.
MITIGATION
Mitigation includes actions taken prior to a disruptive event that helps prevent the event altogether or reduce its magnitude. Types of mitigation measures include hardening to reduce the likelihood or magnitude of disruptive events within stages of the system, and diversification to create parallel versions of stages to reduce the risk of catastrophic failure.
Because of a lack of transparency, medical product manufacturers currently have little incentive to harden their supply chains through updated techniques, processes, and controls that promote reliability and quality in medical products. The information that would be available in the public database proposed in Recommendation 2 would provide a key tool for improving the resilience of medical product supply chains. However, this information must be acted upon. A key place where this action is needed is in the purchasing decisions by health systems because a high percentage of medical product shortages, particularly in generic drugs, are encountered during normal times as a result of process disruptions caused by problems with quality. Hence, an important method to reduce the likelihood and magnitude of medical product supply shortages is by inducing health systems to incorporate reliability into their purchasing decisions.
The incentives that health systems have when managing their supply chains are misaligned with the incentives of the suppliers, distributors,
and others participating in medical product supply chains. Health system contracts that focus on price alone can drive competitor products from the market in a “race to the bottom” pricing structure. This can lead to fewer suppliers, which in turn can weaken the resilience of the supply chain as no options are available to fill the void if a quality or manufacturing issue occurs. Health systems can address the “cost only” inertia by explicitly contracting for supply reliability in addition to price. Previous reports have issued recommendations that call for manufacturers to adopt updated manufacturing processes that would improve the quality and reliability of medical products (see Appendix B). Recommendation 3 (Resilience Contracting by Health Systems) builds on these by tasking health systems with actions that, when taken together with manufacturers and suppliers, will help build robust mitigation strategies into critical medical product supply chains.
Recommendation 3 (Resilience Contracting by Health Systems). Health systems should promote a more resilient market for medical products by deliberately incorporating quality and reliability, in addition to price, in their contracting, purchasing, and inventory decisions. When quality ratings for medical products are available, accreditation organizations for health systems should use the ratings of the products sourced by health systems in their evaluations and ratings, as well as the frequency of shortages experienced at a health system that negatively affected patient care. Specifically,
- Health systems should fortify their contracts with medical product suppliers by including failure-to-supply penalties for contracts requiring a committed purchase or purchase volume, preferentially awarding contracts to suppliers that can demonstrate superior quality and reliability, awarding contracts to multiple suppliers of the same medical product, and requiring these same standards in contracts that are negotiated by group purchasing organizations on their behalf.
- Health systems should budget to adequately reward a select groups of products (e.g., low-cost, low-margin, off-patent, small molecule) if guarantees are met for higher quality and assured supply levels.
- Health systems and medical product wholesalers should routinely enter into emergency purchasing agreements for a specified list of emergency supplies or products that guarantees product delivery in the event of an unexpected supply demand or a substantial supply disruption. They should have a good understanding of the supplier’s ability to meet demand, considering commitments to other buyers.
PREPAREDNESS
Preparedness includes actions taken prior to a disruptive event that will reduce the risks to health and safety if the event occurs. These actions can be grouped into four subcategories, two physical and two virtual. Physical preparedness measures include inventory buffering and capacity buffering, in which stock or productive capacity are held in readiness to fill a supply shortfall. Virtual preparedness measures include contingency planning, which establishes plans for dealing with specific scenarios, and readiness, which builds capabilities for dealing with scenarios without specific plans made in advance.
During the COVID-19 crisis, holding inventory in readiness was more complicated in practice than in theory. In the real world, problems with forecasting demand and monitoring stock levels, rotating stock to prevent expiration, and other practical details prevented inventory stockpiles from providing the intended level of protection in an emergency. Furthermore, capacity can be a cost-effective alternative or supplement to inventory as protection against shortages. The committee recommends action related to both stockpiling and capacity buffering. Stockpiling is already part of the national preparedness strategy, primarily in the form of the Strategic National Stockpile. Therefore, Recommendation 4 (Stockpiling) focuses primarily on refining and improving the ways inventory is held as protection against a medical product shortage.
Recommendation 4 (Stockpiling). The Office of the Assistant Secretary for Preparedness and Response should take steps to develop strategies to modernize and optimize inventory stockpiling management for the Strategic National Stockpile (SNS) and beyond to respond to medical product shortages at the national and regional levels. These steps include the following:
- Consider the recommendations provided in the National Academies report, Ensuring the Effectiveness of the Public Health Emergency Medical Countermeasures Enterprise, particularly those that focus on adopting a systems approach to managing the SNS.
- Analyze risk levels of supply chain critical medical products and the viability of other response strategies (e.g., capacity buffering).
- Examine key inventory stockpiling process considerations such as
- Inventory system visibility.
- Mechanisms and thresholds for the use, sharing, deployment, distribution, and allocation of stockpiled inventory in response to shortages (triggered by both emergencies and routine use) and to prevent product expiration.
-
- The risks and benefits of stockpiling ingredients or components as opposed to finished goods.
- The risks and benefits of just-in-time production or inventories in larger reserves.
- Funding levels to meet the required inventory levels and management tasks for the regional and national stockpiles as well as incentives for stakeholders for holding inventory.
- Convene regional and local working groups composed of emergency health planners, clinicians, health care systems, and public health agencies, among others, to discuss and inform expectations for federal SNS support; national and regional stockpile content and pre-deployment positioning; regional supply capabilities and expectations; and roles and responsibilities for key stakeholders.
Recommendation 5 (Capacity Buffering) calls for measures to cultivate contingent capacity that can be brought online to supplement inventory buffers as needed. Such capacity buffering could be the result of direct contracts, such as advance arrangements to have specific manufacturers provide emergency capacity, as the auto manufacturers did during the pandemic by assembling ventilators. It could also be the result of a list of guaranteed “crisis prices” that the government would pay for certain products under specified conditions. This would provide an incentive for firms to find creative ways to deliver pop-up capacity during emergencies. Finally, the federal government should fund research on advanced manufacturing technologies that make it more economical to produce locally and easier to scale up capacity quickly. Both of these would make capacity buffering a more viable preparedness option, and hence would facilitate a partial shift away from expensive inventory and toward cheaper capacity.
As noted earlier, on-shoring is often espoused as a means for increasing the resilience of medical product supply chains via the argument that the more medical products a country produces domestically, the more control it has of supplies during an emergency. By reducing labor costs and promoting flexibility and scalability, the advanced manufacturing technologies advocated in Recommendation 5 (Capacity Buffering) may make on-shoring a good option for some products. Indeed, if technological capabilities permit efficient, small-scale production, then dispersed production in the country of consumption will be the natural market outcome. However, where this is not the case, on-shoring will impose a significant price penalty on an ongoing basis in return for a potentially small advantage during emergencies. If many developed countries pursue on-shoring strategies for many medical products, considerable resources will be spent that could be put to better use addressing other problems.
Therefore, on-shoring should be part of an integrated resilience strategy, rather than the option of choice.
Recommendation 5 (Capacity Buffering). The Office of the Assistant Secretary for Preparedness and Response (ASPR) and the U.S. Food and Drug Administration (FDA) should take steps to cultivate capacity buffering for supply chain critical medical products where such capacity is a cost-effective complement to stockpiling and as protection against long-lasting supply disruptions or demand surges. These steps include
- Government investments in capacity buffering should be aimed at all stages of the supply chain and at major public health emergencies.
- ASPR and FDA should develop and routinely maintain a crisis-prices list of supply chain critical medical products (i.e., medically essential and supply chain vulnerable) and identify which capacity measure is a practical supplement to the stockpiled inventory. Further, ASPR should develop and manage a database to coordinate inventory stockpiling and capacity buffering policies regarding crisis-prices list.
- ASPR and FDA should fund research and development for both advanced pharmaceutical and advanced medical technology manufacturing techniques to help make on-shoring more cost-competitive. By making capacity more easily scalable, these technologies would enable firms to respond to the need for capacity buffers more quickly and cost-effectively.
- ASPR and FDA should create public–private partnerships and support and fund capital and staff investments jointly, to implement these advanced manufacturing approaches to ensure production capacity. These partnerships will provide a great depth and breadth of expertise and can be leveraged for new economic incentives and regulatory clarity.
- ASPR should be responsible for anticipating and assessing public health emergency demand surge for supply chain critical medical products. They should clarify production capacity, identify vulnerabilities in supply chains, and engage producers in developing plans for surge response.
RESPONSE
Response includes actions taken after an event to minimize harm from the shortage and to resolve the shortage. These actions can be subdivided into prophylaxis measures, which protect human health while the shortage persists, and measures to close the supply gap through demand reduction
and/or supply increase. Taken together, response activities seek to return the supply chain to normal (or to a “new normal”) with as little harm as possible to end users and patients. The committee’s recommendations about response include strategies at the global and end user levels to minimize harm from medical product shortages once they occur—both levels of response are needed to ensure the resilience of U.S. medical product supply chains. The key to both levels of response is effective communication and cooperation.
Because many medical product supply chains are global, some response actions must address production and supplies across international borders. The COVID-19 pandemic highlighted the vulnerability of global medical product supply chains to export bans and embargoes. By undermining trust that global medical product supply chains will function when they are needed most, these shortsighted measures promote both “tit-for-tat reciprocity” and “go-it-alone” behaviors that increase our collective vulnerability. The U.S. government must take on the task of better managing and reducing these risks, while maximizing the benefits of globalization. Recommendation 6 (International Treaty) calls for a plurilateral agreement by major exporters of medical products, including the United States, under the World Trade Organization that prohibits export bans on components of critical medical products. Although such an agreement cannot prevent a worldwide shortage from occurring, it can limit the risk to any individual country by “spreading the pain” across the global economy. Furthermore, if such an agreement increases the collective trust in global supply chains during an emergency, then it can be used in conjunction with Recommendation 5 (Capacity Buffering) to promote shared sources of contingent capacity. It is almost certainly more cost-efficient to build virtual capacity capabilities globally than locally. Hence, using the treaty as the basis for collaboration, major medical product exporting countries could further cooperate on providing capacity buffering for medical products likely to be in short supply during global emergencies.
Recommendation 6 (International Treaty). Major exporters of medical products, including the United States, should negotiate a plurilateral treaty under the World Trade Organization that prohibits export bans and restrictions on key components of global medical product supply chains. Any country that violates the terms of this agreement should be subject to sanctions by other signatories of the agreement. Specifically,
- The treaty should provide incentives for countries to uphold commitments and cooperate in the event of a public health crisis.
- The treaty should provide disincentives or sanctions, such as reputational, economic, and legal sanctions, for violating the terms of the agreement.
- Treaty negotiators could consider adding provisions to this treaty that facilitate information sharing, particularly during medical emergencies.
While plurilateral cooperation will help ensure rational distribution of critical medical products among nations during emergencies, distribution of these supplies to end users, such as hospitals, clinicians, pharmacies, and patients, is also vital to protection of public health and safety. Consequently, these end users have important potential roles to play in addressing supply chain disruptions. Second, end users play critical roles in developing and using contingency plans when shortages arise that reduce the effect of shortages on patient and community health. Recommendation 7 (Last-Mile Management) advocates forming a working group of key stakeholders who represent the very end of medical product supply chains, to evaluate and improve the allocation and delivery of medical products during shortages. To protect public health it is vital to be ready to manage this final stage well in an emergency. One way this working group could improve the ability to manage the last mile of medical product supply chains in the next emergency is to collect, standardize, and disseminate best practices from past emergency events. Finally, this working group could lend its combined experience to the development of training and response readiness building programs for medical product shortages within health systems.
Recommendation 7 (Last-Mile Management). The Office of the Assistant Secretary for Preparedness and Response, in collaboration with the Centers for Disease Control and Prevention, should convene a working group of key stakeholders to examine and identify effective last-mile strategies to ensure end users are able to respond in the event of medical product shortages. The working group should
- Determine what information needs to be shared, with whom and in what form, in order for end users to be able to execute resource sharing, supply redistribution, substitution, adaptation, and other strategies for responding to medical product shortages at the local level.
- Develop a standard national ethical framework for allocating scarce medical products, building in previous crisis standards of care work, including attention to equity, efficiency, and additional ethical values.
- Develop and incorporate response plans and training for medical product shortages into public health and health care professional capabilities.
CONCLUDING REMARKS
Taken together, the committee’s seven recommendations will increase the resilience of medical product supply chains by using all four protective shields of the resilience framework (see Box S-1). With proper coordination between them, these will substantially increase the nation’s ability to maintain the supply of medical products and prevent harm during normal and emergency conditions.
__________________






















