
Appendix D
Commissioned Economic Analysis
The committee commissioned one white paper to further their understanding in the economic considerations for enhancing the resilience of medical product supply chains: Ellis, P. 2021. Where There’s a Will: Economic Considerations in Reforming America’s Medical Product Supply Chains. Paper commissioned by the Committee on Security of America’s Medical Product Supply Chain.
WHERE THERE’S A WILL: ECONOMIC CONSIDERATIONS IN REFORMING AMERICA’S MEDICAL PRODUCT SUPPLY CHAINS
Philip Ellis, Ph.D.
Consultant to the Committee
November 10, 2021
EXECUTIVE SUMMARY
- For a range of reasons, it is useful to distinguish rather sharply between the issues raised by the shortages of personal protective equipment (PPE) and other supplies that arose during the COVID-19 pandemic, and the issues involved in the persistent supply problems for generic drugs. Simply put, they have different causes, involve different orders of magnitude, and will likely require different solutions.
- Another very important distinction to draw is between the desired level of supply that is needed and the location of the production facilities used to generate that supply. In short, total supply can be increased and supply chains can be made more robust by either domestic or foreign production, so increasing the level of supply does not require moving production to the United States. In general, foreign production will be the less expensive option.
- To help size up the problem, total purchases of PPE in the United States during 2019 were about $5 billion. But PPE use rose 10-fold or more in 2020, and would have increased further except for the PPE shortages that emerged. N95 masks are a useful example, with their use increasing from about 50 million in 2019 to about 600 million in 2020. Firm figures are harder to come by for the generic drugs involved in ongoing shortages, but total demand for these at preshortage prices is probably in the range of $700 million to $1 billion per year; sterile injectable drugs account for a substantial share of the shortage problem. It is worth noting that these are often produced in this country.
- In effect, the benefits of having ample medical supplies can be seen in the cost of not having them. Credible estimates indicate that the lack of adequate PPE in 2020 may have caused between 1,000 and 2,000 deaths from COVID-19 nationwide among health care staff and other essential workers, imposing costs of $5 billion to $10 billion. Other costs, such as those for avoidable hospitalizations, are much smaller, around $300 million. These figures likely understate the costs of PPE shortages. Drug shortages also impose costs but the effects are often harder to quantify.
- Although estimates vary widely, domestically produced PPE and generic drugs would probably cost 20 to 50 percent more than supplies produced abroad. At nonpandemic levels of demand for PPE, that would increase total spending in the United States by $1 billion to $2.5 billion per year. To provide pandemic-level quantities of supplies, spending might have to rise from $50 billion, a 10-fold increase in quantities at prepandemic prices, to between $60 billion and $75 billion when purchased domestically. The incremental cost of domestic production in this scenario could be as much as $10 billion to $25 billion per year, or $5 billion to $12.5 billion for a 6-month supply.
- Maintaining the capacity to meet pandemic levels of demand from domestic suppliers would also seem to present daunting challenges since it is not economical for producers to maintain that capacity absent extensive subsidies or other federal interventions. These same issues arise regarding the option to have a domestic surge capacity that is available to make a substantial contribution to out
- put in a pandemic. It is also worth remembering that a pandemic that strikes the United States could significantly inhibit domestic production, as could a natural disaster.
- One conclusion I draw is that pandemic-level demand for medical supplies would be met most efficiently by stockpiling large quantities of these supplies. That approach should provide more certainty that the supplies will be available when needed, and will allow those products to be purchased at prices close to nonpandemic levels from less expensive foreign suppliers. Models exist for rotating supplies through storage so that the stockpiled supplies do not become stale or ineffective.
- To address the ongoing problems with shortages of generic drugs, hospitals are already incurring costs because of inefficient workarounds and patchwork efforts undertaken at the last minute. Those costs have been credibly estimated at about $360 million per year, which is about 35 to 50 percent of the annual costs of the shortage of the drugs themselves. It follows that purchasers should be willing to pay prices that are 35 to 50 percent higher in order to ensure a reliable supply of these drugs.
- However, most hospitals and other purchasers have shown, by revealed preference, that they are largely unwilling to pay the extra costs involved in producing more reliable supplies. The federal government will most likely need to take steps to change that behavior, but the optimal approach is unclear, partly owing to limited data.
- To bring about changes in medical product supply chains more generally, the federal government would need to take steps that actually change the incentives facing suppliers and purchasers, through some combination of subsidies for preferred activities or outcomes, penalties for the opposite, or regulations designed to achieve those goals, which in turn will often impose costs on suppliers, purchasers, or both.
- The federal government can also facilitate changes in medical product supply chains by generating more information about the ultimate sources of production for many items, the quality of those products, and the status of existing stockpiles across the country, but by themselves, those steps will not incentivize changes in medical product supply chains.
- Absent such steps, purchasers will gravitate back toward the cheapest sources of supply that provide prepandemic levels of quality and reliability. If that were to happen, our country would be back in the same boat when the next pandemic occurs, which is a matter of when, not if. However, these problems are tractable and another truism also applies: where there is a will, there is a way.
INTRODUCTION
The COVID-19 pandemic has stressed the U.S. health care system in many ways, not least in its ability to provide the medical supplies needed to treat and care for patients in hospitals, doctors’ offices, and other settings. Policy makers understandably want to address those problems so that the country is better prepared for the next pandemic, whenever it happens, and for other unexpected events. That focus has also drawn more attention to long-standing problems with the supply of various drugs, mostly generic, which are usually made overseas. A general goal is to make the medical product supply chains that yield those products more reliable and secure.
In both cases, the basic options under discussion include moving more production of medical supplies to domestic sources, an approach known as on-shoring production, or at least creating more capacity to surge domestic production in a crisis. Other primary options are stockpiling more supplies to address shortages when they arise, or continuing to rely on global medical product supply chains but work to make them more robust and less vulnerable to disruption. Still other options may yet emerge in the debate.
When considering the available options, the field of economics, which at root is the study of how scarce resources are allocated, has much to contribute. Each of the options will have its own costs and benefits, and choices among them will often involve trade-offs that policy makers might prefer to avoid confronting. Some costs are easier to identify, such as federal subsidy payments to cover the added costs of buying more reliable supplies or of stockpiling supplies. Other costs are harder to observe, such as those stemming from regulations of suppliers or purchasers that raise their costs, but those are economic costs nonetheless. The goal of this analysis is to spell out as well as possible the key costs, benefits, and trade-offs among the basic options available for making America’s medical product supply chains more reliable and secure with quantitative information, if possible.
Economics also tells us that, in general, market forces provide powerful incentives that must be understood and harnessed in the pursuit of policy goals, and not simply ignored. In particular, it stands to reason that current procurement practices are roughly optimal for private buyers and sellers in light of the objectives they have, the incentives they face, and the information available to them. However, those choices may not be socially optimal because buyers and sellers may not take into account costs their actions impose on others or benefits that accrue to others, such as health improvements or reductions in risks to the overall economy or national security. Another lesson from economics is that the last increments of risk reduction are likely to be the most expensive, and that people generally do accept some risks in their daily lives, so seeking to reduce risks is more feasible than trying to eliminate them.
Perhaps the central point economists make is that changing behavior will require changes in the incentives that buyers and sellers face and improving the information available to them, with the incentives being the most important factor. In general, economists would also argue for using market mechanisms to the greatest extent feasible, so that producers can devise the most efficient means of meeting the objectives, whatever they may be. But this statement is not an endorsement of laissez-faire economics; that is, some set of government interventions is needed if we hope to avoid ending up with roughly the same medical product supply chains that we had before the COVID-19 pandemic.
The remainder of this analysis proceeds as follows: the next section reviews key background points about the shortages and supply problems that have emerged both in the COVID-19 pandemic and before it. I then examine the benefits that are likely to accrue from having more reliable medical supplies, benefits that would be common to all of the options, to the extent they achieve that goal. Next, I turn to consider in greater detail the four options mentioned above for changing medical product supply chains, including any quantitative information that is available to help think about the costs of the options and the trade-offs among them. Finally, I examine the economics surrounding the options that policy makers could employ to bring about desired changes in medical product supply chains, including regulations, subsidies, and penalties, as well as improvements in information.
BACKGROUND: THE PROBLEM
The COVID-19 pandemic has highlighted two broad types of problems or challenges with the country’s supply chains for medical goods:
- First and foremost, the demand for some products that was needed to address the pandemic itself soared, just as the supply of those products fell because of pandemic-related shutdowns of economic activity around the globe and the associated disruptions of international trade. Shortages of PPE were perhaps the most obvious examples of the gap between demand and supply, but basic and needed drugs such as antibiotics were also scarce.
- Second, the pandemic also shed new light on ongoing problems with certain supplies which both predated that outbreak and are likely to continue into the future unless new policies are implemented to address them. The most notable cases involve generic drugs, some of which are key components of chemotherapy treatments for cancer patients.
In many but not all cases, the problems have involved products that are primarily made overseas. Most of the world, for example, relies heavily on China for supplies of many types of PPE; by some estimates, about 70 percent of U.S. masks and more than half of all its PPE come from China.1 Most generic drugs are made abroad as well, although important information about their production is simply not available. Before exploring the options for addressing these concerns, it is first necessary to review the problem or problems these options are supposed to solve in order to arrive at an accurate diagnosis. The recent experience with COVID-19 and PPE is fairly familiar, and can be reviewed briefly, whereas the background on shortages of generic drugs is longer and more complex.
A. PPE Shortages and the COVID-19 Pandemic
The pandemic highlighted an important characteristic of current medical product supply chains—a high reliance on foreign producers, especially China. This focus arose in part because the pandemic started in China, so shutdowns of production there had global consequences. But China and other countries also started to hoard their own supplies, in ways both overt and subtle. As a result, just when the demand for PPE started to spike, supplies were actually becoming scarce. This is not to suggest, however, that domestic production of PPE would have prevented the shortages that arose, which were driven more by a sharp increase in demand than by the limits on foreign supplies.
In the ensuing months, shortages worsened, prices for PPE spiked, bidding wars broke out, and the environment was chaotic. Reports abounded of medical personnel reusing their masks and gowns, or even turning to makeshift substitutes, including garbage bags.2 The Associated Press found that no imports of N95 masks had arrived anywhere in the United States during the month of March 2020.3
Rather quickly, the federal government relaxed regulations around PPE use and reuse, and also made it easier to use telehealth as an alternative to in-person visits in order to reduce the need for PPE. The federal government
___________________
1 See page 15 of Congressional Research Service, COVID-19: China Medical Supply Chains and Broader Trade Issues (updated December 23, 2020), https://crsreports.congress.gov/product/pdf/R/R46304; and “Chinese Share Among Selected U.S. Imports of Medical Supplies and Equipment in 2019,” Statista (July 20, 2020), https://www.statista.com/statistics/1122414/select-us-imports-from-china-medical-supplies-under-tariff-exclusions/.
2 Susan Glaser, “How Did the United States End Up with Nurses Wearing Garbage Bags?” The New Yorker (April 9, 2020). https://www.newyorker.com/news/letter-from-trumps-washington/the-coronavirus-and-how-the-united-states-ended-up-with-nurses-wearing-garbage-bags.
3 Juliet Linderman and Martha Mendoza, “First N95 Medical Mask Imports Finally Reaching US,” Associated Press (March 31, 2020). https://apnews.com/article/health-global-trade-asia-ca-state-wire-virus-outbreak-1d5aff5e3a3970fac857e3ae01e9d321.
also established a “control tower” within the Department of Health and Human Services (HHS). This entity worked with the major U.S. wholesalers through which nearly all PPE are purchased to establish daily monitoring of the demand for—and supply of—these supplies. By the summer of 2020, Chinese supplies had become broadly available again.4 However, shortages of PPE in the United States persisted for the remainder of 2020 and seem to have extended well into 2021.5
In considering the options for dealing more effectively with future pandemics, data on the amount of spending involved are crucial. Some information is available to help size up the U.S. market for PPE and for some specific products, but it is sparse. For N95 masks, publicly available estimates of their use in 2020 vary quite widely, but more reliable information seems to come from the Defense Department, which through its Defense Logistics Agency effectively provided oversight for the market once the pandemic got going. According to those reports, the United States had been using about 50 million N95 masks per year prior to the pandemic, but use soared to about 47 million per month in the spring of 2020.6 On an annual basis, that would amount to about 560 million masks. This figure is likely to understate what the demand was in the pandemic because it reflects only the units that were actually sold and delivered at the higher prices which prevailed at the time, not the amounts that hospitals and other purchasers would have wanted to use at the more moderate prices that would have been charged if supplies had been more plentiful.
What were those prices? Public reports on pricing also vary but tend to indicate that N95 masks were going for about $1 each before the pandemic. Thus, total spending in the United States on N95 masks prepandemic was about $50 million. During the pandemic, however, prices reportedly rose to about $7 or $8 per mask. At those prices, 560 million masks would have cost about $4 billion, an 80-fold increase in spending.7
More broadly, estimates indicate that total worldwide spending on PPE prior to the pandemic was on the order of $13 billion. The United States
___________________
4 Ken Roberts, “China More Dominant Than Ever In Covid-Related ‘PPE’ — And U.S. Flags,” Forbes (September 19, 2020). https://www.forbes.com/sites/kenroberts/2020/09/19/china-more-dominant-than-ever-in-covid-related-ppe---and-us-flags/?sh=8f5df4f17f71.
5 Andrew Jacobs, “Health Care Workers Still Face Daunting Shortages of Masks and Other P.P.E.,” The New York Times (December 20, 2020). https://www.nytimes.com/2020/12/20/health/covid-ppe-shortages.html.
6 See Jared Serbu, “Pentagon Says it Needs Billions to Repay Contractors for Employee Leave,” Federal News Network (June 11, 2020). https://federalnewsnetwork.com/defense-main/2020/06/pentagon-says-it-needs-billions-to-repay-contractors-for-employee-leave/.
7 Data on PPE prices and spending in this paragraph and the next one drawn from this report: 2020 HIDA Personal Protective Equipment Market Report, Health Industry Distributors Association (December 2020). https://www.hida.org/distribution/research/market-reports/PPE-Market-Report.aspx.
represents about 40 percent of global spending on all medical care, which would imply that total U.S. spending on PPE was about $5 billion in 2019. Of that total, hospitals spent about $2 billion and doctors’ offices and other entities spent about $3 billion. Ideally, more precise figures would be available, but for the time being, these data may have to suffice.
B. Ongoing Problems with Supplies of Generic Drugs
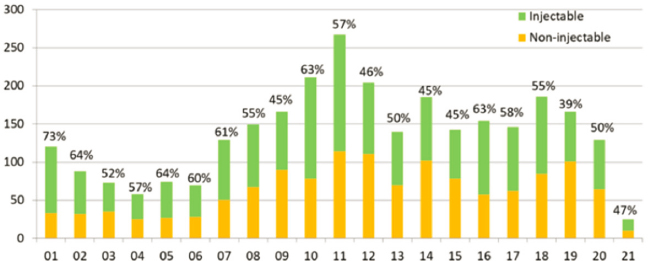
A second set of issues arises around the ongoing problems with medical product supply chains, ones that predated the COVID-19 pandemic and are likely to continue afterwards unless they are addressed in a new way. Those problems primarily involve generic drugs, particularly sterile, injectable drugs. As Figure 1 shows, the number of new drug shortages has generally been higher since 2006, with the average number more than doubling from 81 over the 2001–2006 period to 173 over the 2007–2019 period.8 The figure also shows that a substantial share of the new shortages in any year involve sterile injectable drugs, even though those drugs constitute a small share of total drug spending.
Observers have identified several factors that contribute to these shortages. Generic drugs generally have very thin profit margins, meaning that producers do not suffer extensive losses during a shortage, and so have limited incentives to avoid them. Indeed, establishing robust supply lines would be more costly, and thus would put a company at a cost disadvantage against its competitors. To minimize costs, production processes for generic drugs are typically very lean, with little margin for error or unexpected events. By contrast, brand-name drugs with patent protection gener-
___________________
8 Data and figure drawn from American Society of Health-System Pharmacists, “Drug Shortages Statistics,” available at https://www.ashp.org/drug-shortages/shortage-resources/drug-shortages-statistics.
ally have high margins on their unit sales, giving their manufacturers strong incentives to avoid shortages in order to continue making those sales.
Roughly 90 percent of prescriptions filled in the United States are for generic drugs, so these pills account for the vast majority of drug production. As Table 1 shows, the production of both active pharmaceutical ingredients (APIs) and final dosage forms (FDFs) for the U.S. market is usually done overseas. APIs are the key ingredients of drugs, which are then combined with other ingredients and shaped into pills or other forms to be used by patients. An important limitation of those figures, however, is that the U.S. Food and Drug Administration (FDA) has information on where facilities are located, but not on how much is produced at each facility. With that proviso in mind, the United States, Canada, and the European Union collectively account for 43 percent of the facilities for production of APIs and 59 percent of the facilities for production of FDFs.9
The same FDA report found the following:
the number of ongoing drug shortages has recently been increasing after declining from a peak in 2011, and drug shortages have been lasting longer, in some cases more than 8 years. FDA analyzed 163 drugs that went into shortage in the 5-year period between 2013 and 2017. Of the 163 drugs in the sample, 63 percent (103) were drugs administered by injection (sterile injectables) and 67 percent (109) were drugs that have a generic version on the market.10
Table 1 Regional Distribution of Facilities Manufacturing Finished Dosage Forms and Active Pharmaceutical Ingredients in 2018
| County/Region | Active Pharmaceutical Ingredient | Final Dosage Form |
|---|---|---|
| U.S. | 12% | 37% |
| Canada | 0% | 4% |
| European Union | 31% | 18% |
| China | 14% | 8% |
| India | 31% | 24% |
| Latin America | 2% | 0% |
| Rest of World | 11% | 10% |
| TOTAL | 100% | 100% |
___________________
9 Data in this paragraph and Table 1 drawn from Food and Drug Administration, Drug Shortages: Root Causes and Potential Solutions (October 2019; updated February 2020). https://www.fda.gov/drugs/drug-shortages/report-drug-shortages-root-causes-and-potential-solutions.
10 See page 5 of FDA, Drug Shortages: Root Causes and Potential Solutions.
To an economist, the idea that a true economic shortage could continue for several years, much less 8 years, is hard to believe.11 One would expect that prices would rise and that existing producers would thus have incentives to resume production and that other companies would find it attractive to start making the product that’s in short supply. If the drug is essential for care, demand for the drug should be “inelastic,” meaning that purchasers should be willing to pay substantially higher prices in order to bring the quantity supplied close to the preshortage level. As economists say, the cure for high prices is high prices.
But according to FDA’s own analysis, that typically does not happen for prescription drugs. Specifically, the agency conducted a study of drugs in shortage and found the following:
- Only 18 percent had a sustained price increase (i.e., an increase of 50 percent or more that began during the shortage and lasted for 6 months).
- Only 42 percent had significant production increases; either new suppliers were entering the market or existing suppliers were increasing production during the shortage to restore at least 50 percent of the unavailable quantity.
- Only 30 percent had the quantity of the drug sold restored to at least 100 percent of its amount prior to the shortage (i.e., after 12 months of being in shortage, or at the end of the shortage if it had already been resolved within 12 months).12
These findings would seem to indicate rather modest responses to the shortages, in contrast to the price spikes and production increases that might have been expected. One possible explanation is that doctors and hospitals are able to use other drugs instead when one is in short supply. Certainly, some efforts in that regard go on, and by some estimates those activities costs hospitals about $360 million per year.13 But in other cases,
___________________
11 The term shortage can be defined in various ways, and is typically meant to describe a situation in which the quantity demanded exceeds the quantity supplied. This definition is adequate, so long as the quantity demanded truly reflects the most that buyers are willing to pay and not just an abstract expression that buyers would like more supplies, but not if they cost more. For economists, a more precise definition of a shortage is that buyers are willing to pay more than the current cost of production for an item but are unable to purchase that item. If buyers would like to have more, but are not willing to pay more for it, then the correct term is scarcity.
12 See pages 36-37 of FDA, Drug Shortages: Root Causes and Potential Solutions.
13 Alex Kacik, “Drug Shortages Drain at Least $359M from Health Systems,” Modern Healthcare (June 26, 2019). https://www.modernhealthcare.com/finance/drug-shortages-drain-least-359m-health-systems.
treatments must be delayed. Data on the extent of those substitutions and delays would be quite useful.
The FDA report itself concludes that, taken together, “these findings lead to the hypothesis that drugs that go into shortage are products that companies may not have a strong financial incentive to market or to produce using mature manufacturing quality management.” This finding simply begs the question of why producers lack these financial incentives, and why the drugs go into shortage in the first place. The report states that the market does not foster a reliable supply of generic drugs. But markets are simply made up of people and companies, the buyers and suppliers, and reflect their choices and preferences. To quote Shakespeare, “the fault, dear Brutus, is not in our stars, but in ourselves.” For these reasons, I find it difficult to avoid the conclusion that markets do not reward these things because most of the providers that purchase the drugs involved are not actually willing to pay much more for those drugs, at least not enough to cover what it would cost to produce the drugs with substantially fewer quality problems and supply disruptions.
Certainly, there are ways of changing the incentives for drug makers, if the requisite willingness to pay more on the part of buyers exists. An HHS report on drug shortages from 2011 stated the following:
Private organizations that purchase drugs and vaccines…can help alleviate future shortages by strengthening the failure-to-supply requirements in their contracts in exchange for increases in price. Such contract changes are likely to lead manufacturers to invest in extra capacity of both production lines and API.14
Evidently, that approach has gained little traction.
Alternatively, an intermediary company could come forth to serve as a reliable supplier and take on the responsibility of establishing more reliable lines of supply. Such a company was formed in 2018, called Civica Rx, with funding from some major hospitals and health systems as well as three health-focused foundations, which provided about 30 percent of the start-up funding.15 The company’s stated focus is on making generic drugs generally and sterile injectable drugs particularly. To date, that company has been approved to market about 40 different drugs. Precise information on their prices and sales is not available, although industry sources indicate
___________________
14 Office of the Assistant Secretary for Planning and Evaluation (ASPE), “Economic Analysis of the Causes of Drug Shortages” (October 2011). https://aspe.hhs.gov/sites/default/files/migrated_legacy_files//57791/ib.pdf.
15 The Editorial Board, “Pharma Disrupter: Nonprofit Drugmaker Targets Supply, Costs,” Pittsburgh Post-Gazette (January 13, 2019). https://www.post-gazette.com/opinion/editorials/2019/01/13/Pharma-disrupter-Nonprofit-drugmaker-targets-supply-costs/stories/201901130087.
that Civica Rx’s products are more expensive than those of traditional suppliers of generic drugs. While a promising development, it remains to be seen how well or sustained these efforts or similar initiatives will succeed at reducing shortages.
More broadly, some information is available to try to size up the markets for generic drugs during shortages and for generic sterile injectable drugs; this information should be helpful in thinking about the costs of addressing the supply problems. The HHS report cited above indicates that drugs in shortage typically account for about one-half of 1 percent of all drugs, but did not indicate how much was typically spent on those drugs prior to the shortage. However, if we focus on generic drugs and assume that generic drugs in shortage accounted for the same share of spending as they do for all drugs, we can derive some rough figures. On the basis of my own analysis, I estimate that total outpatient spending in 2019 on all generic drugs (including physician-administered drugs) was about $135 billion. One-half of 1 percent of that amount would be less than $1 billion, or to provide a more precise point estimate, $675 million in that year.
As for sterile injectables that are available in generic form, Medicare enrollees used about $725 million worth of these drugs in 2019. Since Medicare accounts for about 25 or 30 percent of health care spending in the United States, a reasonable extrapolation is that total spending in the United States on these drugs was three to four times Medicare’s spending, between $2 billion and $3 billion. Reports have not been clear on what percentage of sterile injectables are in shortage at any one time, but if that were 10 percent then preshortage spending on those drugs would have been around $200 million or $300 million per year, or roughly half of all spending on generic drugs in shortage.
It is worth noting that some additional use of drugs occurs in an inpatient setting, but this spending is difficult to identify because it is generally included in a broader bundled payment to the hospital. At the same time, physician-administered drugs, including those for chemotherapy, are typically given in an outpatient setting and providers receive a separate payment for those drugs that usually exceeds their acquisition cost, at least on average. As a result, more data are available for such spending. These arrangements also mean that hospitals are often not required to finance any extra costs for drugs in shortage out of a fixed payment per admission.
THE BENEFITS OF MORE RELIABLE MEDICAL PRODUCT SUPPLY CHAINS
As we consider the benefits of different options for improving the reliability and security of America’s medical product supply chains, it is useful and important to distinguish between benefits that may be unique to each
of those options on the one hand and benefits associated with improved supply chains generally on the other. The first category is discussed in the next section, where we examine these distinct options. Here we review the benefits that are likely to stem from any of the options. The costs of the options can then be evaluated relative to those benefits, taking into account the likelihood that the option, with sufficient funding in the cost column, will achieve the desired goals.
Some of the benefits of having reliable and robust medical product supply chains will be difficult to quantify. In particular, there may be benefits to national security that stem from being less dependent on or beholden to a given country, but such benefits are inherently hard to measure. Even so, it can be useful to quantify those benefits that can be quantified so an assessment can be made about whether the intangible benefits are likely to be large enough to warrant the costs involved. Even some tangible benefits can be hard to quantify. As discussed above, the COVID-19 pandemic gave rise to shortages of PPE as well as many key drugs, including antibiotics. Because some data were available regarding PPE, I focused on that case rather than the pandemic-related shortages of drugs.
In the case of PPE, the benefits of having reliable supplies were amply illustrated in the spring of 2020 when the opposite occurred, and demand for PPE greatly outstripped supply. Focusing on items such as masks, gloves, and gowns, and their use by health care workers and other essential personnel, one can envision the following principal risks that arose as a result of inadequate supplies:
- Greater risk of transmitting the virus to hospital patients who were not admitted with COVID-19, increasing their risk of developing a serious case and risk of death
- Greater risk of transmitting the virus among hospital staff, which not only poses health risks for those people but also makes them more likely to miss work, which in turn reduces the capacity of the health care system to exacerbate bottlenecks in patient care
- Greater perception of risk among the general public about seeking medical care, which may lead them to forego other necessary services. For example, a particularly troubling statistic from early in the pandemic was that the number of emergency room visits for strokes or heart attacks declined by roughly 40 percent.16 There is no reason to believe those underlying medical events happened less often.
___________________
16 Lenny Bernstein and Frances Stead Sellers, “Patients with Heart Attacks, Strokes and Even Appendicitis Vanish from Hospitals,” The Washington Post (April 19, 2020). https://www.washingtonpost.com/health/patients-with-heart-attacks-strokes-and-even-appendicitis-vanishfrom-hospitals/2020/04/19/9ca3ef24-7eb4-11ea-9040-68981f488eed_story.html.
A study from 2020 provides some data with which to quantify some of the benefits. The government of California tracked COVID-19 infections and deaths among health care workers, allowing some calculations to be made regarding the effect of limited PPE supplies, which I then extrapolated to the country as a whole.17 Specifically, I applied the ratios from California to national data about the pandemic through the end of November 2020, which roughly corresponds to the period in which PPE supplies were most constrained. The figures indicate that about 600,000 cases of COVID-19 occurred among health care workers nationwide over that period, resulting in roughly 3,000 deaths.18
The authors of the study estimated that about one-third of those cases could have been prevented if PPE had been readily available. Thus, about 200,000 cases of COVID-19 among health care workers could arguably have been avoided, along with about 1,000 deaths. If the analysis were extended to other essential workers, who also lacked for supplies of PPE, those figures would roughly double to about 400,000 avoidable cases of COVID-19 and 2,000 avoidable deaths. Even if ample supplies of PPE would have prevented only half as many cases and deaths as the authors estimated, the effect would be substantial. Assuming that a statistical life for working-age people is worth $5 million, or about $125,000 per year, the cost to society of 1,000 deaths would be $5 billion and the cost of 2,000 deaths would be $10 billion.
In addition to avoiding deaths among essential workers, substantial costs for pandemic-induced hospitalizations also could have been averted with proper supplies of PPE. Based on the study of California cited above, I estimate that through November 2020 there were about 10,000 hospitalizations nationwide among health care workers and other essential workers that could have been avoided with plentiful supplies of PPE. In making that calculation, I estimated that the COVID-19 hospitalization rate among non-elderly adults was about 2.5 percent. Estimates of the average costs of hospitalizations for COVID-19 vary, but several analyses point to an average cost of about $20,000 per admission.19 Using that figure yields an estimated national cost of about $200 million for avoidable hospitalizations among health care workers and other essential workers. Even if the actual number
___________________
17 William Dow, Kevin Lee, and Laurel Lucia, Economic and Health Benefits of a PPE Stockpile (August 12, 2020). https://laborcenter.berkeley.edu/economic-and-healthbenefits-of-a-ppe-stockpile/.
18 See also https://www.theguardian.com/us-news/ng-interactive/2020/aug/11/lost-on-thefrontline-covid-19-coronavirus-us-healthcare-workers-deaths-database.
19 See Krutika Aminand Cynthia Cox,“Unvaccinated COVID-19 Hospitalizations Cost Billions of Dollars,” Peterson-KFF Health System Tracker (September 14, 2021), https://www.healthsystemtracker.org/brief/unvaccinated-covid-patients-cost-the-u-s-health-system-billions-of-dollars/; and FAIR Health, Key Characteristics of COVID-19 Patients (July 14,2020), https://www.fairhealth.org/article/fourth-covid-19-study-from-fair-health-examines-patient-characteristics.
were half of that estimate, the costs are considerable. And that analysis does not take into account the effect on hospital patients stemming from the spread of the coronavirus that is attributable to a supply shortage of PPE.
Less information is available to quantify the overall costs of ongoing supply problems involving generic drugs and the benefits of avoiding those problems, but some data points do exist. One study of a shortage of norepinephrine found that hospital death rates from septic shock increased by about 10 percent, or 3.7 percentage points, as a result.20 The 2019 FDA report on drug shortages noted that affected patients “may experience treatment delays, receive alternative treatments that are not as effective or well tolerated, or may have to forgo treatment” and cited several specific examples. As noted earlier, a recent study estimated that costs to hospitals dealing with drug shortages were about $360 million per year.
These benefits would stem from any approach that achieves the objective of having reliable medical product supply chains, or at least, those that are substantially more reliable than the current arrangements. As a result, the key question in evaluating the options for strengthening these medical product supply chains is not what the benefits will be, but what are the chances that the option in question will yield the desired increase in reliability. Perhaps a better way to frame the issue is to say that each of the options below has some probability of making the supply chains “substantially” more reliable. The expected benefits of each option are, in the simplest terms, the benefits of that increase in reliability times the probability of achieving that increase via the option. Then those expected benefits can be weighed against the expected costs.
CHANGING MEDICAL PRODUCT SUPPLY CHAINS: A MENU OF OPTIONS AND TRADE-OFFS
The country has a number of options or approaches that it could pursue to improve the security and reliability of its medical product supply chains. At least for analytic purposes, it is useful to distinguish between the direct changes to the supply chains and the policies that are designed to bring about or encourage those changes. This section focuses on the direct changes. The subsequent section focuses on policy options to support those changes, which could include
- subsidies for purchasing supplies that have a more robust supply chain and penalties for failing to do so;
___________________
20 Emily Vail and others, “Association Between US Norepinephrine Shortage and Mortality Among Patients with Septic Shock,” Journal of the American Medical Association, vol. 317, no. 14 (April 11, 2017). https://jamanetwork.com/journals/jama/fullarticle/2612912.
- temporary or permanent changes in regulations affecting the supply of, demand for, and price of these products; and
- improvements to the information available to purchasers as well as suppliers.
However, I will defer discussion of these measures until the changes that they would be designed to encourage are examined more fully.
Direct changes to the supply chains can be arrayed on something of a continuum, as follows:
- On-shoring of production;
- Creating or arranging for domestic surge capacity;
- Stockpiling supplies; and
- Making global medical product supply chains more diverse and robust.
The differences across those options largely involve how much production capacity or supply would be shifted to domestic locations. On-shoring would obviously involve the highest shift of production locations, though even within that broad approach, there are a range of options regarding the extent to which medical product supply chains are made domestic. For example, on-shoring could occur only for the final assembly of supplies or could instead encompass all or most stages of the production process. At the other end of the spectrum, steps could be taken to make medical product supply chains more robust without moving any additional production capacity or supplies on-shore, for example, by spreading capacity across more global locations to limit the risk of specific bottlenecks or disruptions. The second and third options represent something of a middle ground, with steady levels of supply being provided largely as they have been, but with added measures taken to ensure that supplies are available domestically in case of a disruption or shortage.
Those options are not mutually exclusive; indeed, even for a given product, a combination of approaches could be used. For example, the United States could increase its stockpile of N95 masks at the same time that it takes steps to diversify its ongoing sources of supply. And depending on the particular mix of costs and benefits involved, different approaches may be more appropriate for different types of supplies. For example, some prescription drugs may expire or lose effectiveness rapidly enough that stockpiling would be useful only on a limited basis, if at all, while others may require raw materials or other input that would not be feasible to produce domestically. As a general rule, it may be best to think of all the real policy options as involving a combination of approaches in order to have a comprehensive approach for improving the robustness of medical
product supply chains. Or, as the saying goes, don’t put all of your eggs in one basket.
Another very important distinction to emphasize is to distinguish between the desired level of supply that is needed and the location of the production facilities that are used to generate that supply. Just because policy makers may conclude that more capacity is needed to produce more supplies in response to a pandemic-style spike in demand, it does not mean that such capacity has to be created domestically. In principle, global medical product supply chains could be made more diverse, primarily to guard against supply shocks, and at the same time more extensive, primarily to accommodate demand shocks.
Ideally, the choice of approaches used, and the particular policy levers employed to pursue those approaches, would be informed by a careful consideration of the costs and benefits involved. Some benefits, such as increased national security, may be difficult or impossible to quantify in any precise way. Potentially, those intangible benefits could still be compared to the economic effect that can be quantified to allow policy makers to make informed decisions about whether the net benefits of a given option are likely to be sufficient or not. Unfortunately, it has proven difficult to develop even rudimentary estimates of many of the costs or benefits involved because of the lack of data.
A. On-Shoring Production
The economic debate about on-shoring can essentially be reduced to two key questions. First, how much more would it cost to produce medical supplies domestically? Second, to what extent would on-shoring actually solve the problem of supply disruptions or shortages? Both sets of information are crucial for determining whether the costs of on-shoring will outweigh the benefits, but unfortunately very little information is publicly available about how costs compare between domestic and foreign production, or about the quantitative increase in reliability that would come from on-shoring. Obviously, the answers will depend mainly on the nature of the product itself, and on the extent of the production process that is brought on shore.
Costs of On-Shoring.
The stages of the production process will vary by the type of product being produced, but a useful distinction can be seen in the process for making prescription drugs. In that process, the API may be produced in one location, but inactive ingredients may come from other sources, which are then combined into FDFs that have a particular shape, color, strength, form, and dosage. That latter step is sometimes referred to as the fill-and-finish stage of the production process.
Clearly the costs of any on-shoring efforts would depend on whether the entire production process, including the supply of raw materials, would be
made domestic, but distressingly little information is available about the cost of the production of medical supplies, much less how these costs break down by stage. Naturally, it would be less costly to on-shore the fill-and-finish stage of production, but at the same time concerns about relying on foreign suppliers would be addressed only modestly by such a step; disruptions in the supply of APIs or other inputs could still create shortages. These issues would also be relevant for any proposals to require or encourage U.S. purchasers to “Buy American” because a reasonably precise definition would have to be established for what counts as domestic production of these medical supplies.
One limited exception to the rule of data scarcity about production costs for medical supplies concerns N95 masks, where at least some data are available. Discussions with industry experts indicate that domestically produced N95 masks might need to be priced only 20 to 30 percent higher than masks produced in China to be profitable. A recent press report also indicated that production costs for N95 masks are about 25 cents, on average, in China, but can be more than double that amount in the United States.21 Despite indicating a wide range of possibilities, these two data points may actually be compatible, since masks produced in China will have additional costs for transportation to the United States that would make the aggregate costs of supply less disparate between the two countries than their respective costs of production might indicate.
Another helpful data point was provided in the Biden administration’s recent report on building resilient medical product supply chains. The report, citing an FDA study from 2011, indicated that the production of APIs in India could reduce costs by 30 to 40 percent compared with production costs in the United States or Europe.22 In other words, production of APIs in the United States would cost about 50 percent more than production in India. This explains why the production of most of these supplies has shifted overseas, given that purchasers seem to value low prices for medical supplies and have evidently found their associated levels of quality and reliability to be acceptable at those prices.
A related point worth noting about the economics of on-shoring is that the cost figures suggest a smaller role for differences in labor costs across the counties than might be anticipated. The Biden administration’s report also noted, citing a 2009 study by the World Bank, that overall labor costs in China and India are about 8 and 10 percent, respectively, of labor costs
___________________
21 Monika Evstatieva, “U.S. Companies Shifted to Make N95 Respirators During COVID. Now, They’re Struggling,” National Public Radio (June 25, 2021). https://www.npr.org/2021/06/25/1009858893/u-s-companies-shifted-to-make-n95-respirators-during-covidnow-theyre-struggling.
22 See page 215 of Building Resilient Supply Chains, Revitalizing American Manufacturing, And Fostering Broad-Based Growth (June 2021). https://www.whitehouse.gov/wp-content/uploads/2021/06/100-day-supply-chain-review-report.pdf.
in typical Western countries.23 Therefore, U.S. labor costs are about 10 times higher than those in China and India. U.S. production costs, on the other hand, at least for some products, are only two times higher, perhaps less. What accounts for the difference? Presumably, the manufacturing process in the United States uses much less labor and much more capital and equipment, including robots and other forms of automation. That inference makes perfect sense from an economic perspective, with U.S.-based production methods substituting relatively cheap machines for relatively expensive workers.
How much would those subsidies cost? As indicated above, the United States typically buys about 50 million N95 masks per year, at a total cost of about $50 million. Hypothetically, a 50 percent increase in those costs would raise spending on N95 masks by about $25 million per year. To subsidize the extra costs of pandemic-type levels of demand would necessarily be more expensive. Covering the added expenses for domestic production of 500 million masks would cost $250 million if the average incremental cost was 50 cents per mask. If that added cost were $1 per mask (a doubling of the price) and 1 billion masks were needed, then subsidies would run to $1 billion. An increase in average costs of 50 percent at nonpandemic levels of demand would thus increase nationwide spending on PPE by about $2.5 billion per year, with $1 billion attributable to hospitals and $1.5 billion to other purchasers.
Another point concerning on-shoring indicates that its costs are probably too high to be sustainable without some form of government subsidies. The economics of such subsidies are discussed in more detail in the next section. This inference is based on developments with the N95 mask, when the Defense Department contracted in mid-2020 to quickly increase domestic production to roughly one billion units per year. Companies responded and built capacity accordingly, but now that the total demand for masks has dropped and foreign supplies are available again, these very companies are having to lay off workers and close down production lines.24 Absent federal financial support or other interventions that make it optimal for purchasers to obtain most or all of their supplies from domestic sources, the United States is likely headed back to the same situation that existed prior to the pandemic in fairly short order regarding medical supplies.
Some argue that new production methods, such as continuous production processes, will make domestic production more competitive or
___________________
23 See pages 214-215 of Building Resilient Supply Chains. I have assumed that the underlying analysis controlled for average differences across the countries in skill levels – that is, in the mix of jobs.
24 Timoth Aeppel, “America’s Mask Makers Face Post-Pandemic Meltdown,” Reuters (May 11, 2021). https://www.reuters.com/business/healthcare-pharmaceuticals/americasmask-makers-face-post-pandemic-meltdown-2021-05-11/.
perhaps even less costly than foreign production. While that is theoretically possible, it would generally be more efficient to let the market work out the best way to produce a given quantity of medical supplies, given the incentives for such production. In my opinion, federal efforts to invest in specific new production technologies that are aimed at making domestic manufacturing more competitive are probably misguided, or are, at the least, an inefficient use of federal resources. As economist Larry Summers reportedly observed in 2011 when he was serving as the head of President Obama’s National Economic Council, the government is generally not a very good venture capitalist.25
Benefits of On-Shoring.
The second key consideration regarding onshoring is to determine what the benefits would be. In particular, the central question is whether and to what extent on-shoring would actually solve the supply problems that exist, either with the ongoing issues concerning generic drugs or future pandemic-style spikes in demand and drops in supply.
An important point on this dimension was contained in the Biden administration’s recent report highlighting the fact that domestic production is by no means a panacea. The report noted that the majority of drug shortages over the past decade have been for sterile injectable drugs, a relatively small subset of drugs. Furthermore, the report acknowledged that the problem “is not necessarily an issue of foreign manufacturing because much of the infrastructure for sterile injectable manufacturing is located in the United States owing to the high costs of transporting liquids that often require climate control.”26 In other words, natural disasters, pandemics, and other surprises can also disrupt a domestic medical product supply chain. Supply disruptions have happened often with sterile injectable drugs even though their production has been completed on shore.
Moreover, on-shoring may be a solution that is poorly suited in the case of a pandemic that is acutely affecting the United States, since that same pandemic could easily cause workforce or supply disruptions for domestic manufacturers just as domestic demand for medical supplies is increasing. By itself, on-shoring can create many of the same risks of having “all of your eggs in one basket” as exists currently by relying so extensively on China for many medical supplies. In that light, I will analyze other options for changing medical product supply chains.
___________________
25 Roberta Rampton and Mark Hosenball, “In Solyndra Note, Summers Said Feds ‘Crappy’ Investor,” Reuters (October 3, 2011). https://www.reuters.com/article/us-solyndra/in-solyndra-note-summers-said-feds-crappy-investor-idUSTRE7925C520111003.
26 See page 223 of Building Resilient Supply Chains.
B. Creating Domestic Surge Capacity
An alternative to on-shoring all production of various medical supplies is to create surge capacity to produce them domestically only when a shortage or disruption arises. A historical analogy for this approach would be its role as “arsenal of democracy” that the United States played during World War II, with arms production ramping up over several years from practically nothing to high levels of output. In principle, this approach would be less expensive than on-shoring all production because typical levels of demand would still be met using lower-cost foreign sources of supply. The option to create or rely on surge capacity located in other countries is discussed below in the section on diversifying global medical product supply chains. Just how feasible a strategy it is, particularly if demand jumps 10-fold or more during a pandemic, and how costly it would be are unclear.
In economic terms, the two key questions about this option are first, how to maintain surge capacity during times of normal demand, and second, how to be confident that the surge capacity can actually surge when it is needed. On the second point, a further question is whether enough of the right types of labor and equipment would be available for a production surge. Some observers have noted that in the lead-up to World War II, the United States still had substantial numbers of workers who were unemployed or underemployed stemming from the Great Depression who could be put to work on defense production. Indeed, it was the wartime production surge that finally brought the Great Depression to an end. In the case of a pandemic, such an army of the unemployed may not be available. Also, the amount of labor needed to produce PPE would probably be limited as well, but as we saw in 2020, many workers of various skill levels became unemployed during the pandemic and might be available to make PPE.
Rather than wondering whether surge capacity can arise, a better way to frame that issue is to ask: how long would it take for any surge capacity to be available, given the need to assemble the necessary inputs, and how much could policy initiatives affect that timing? Experience from the COVID-19 pandemic sheds some light on those questions. A number of companies were able to start producing masks and other PPE within a few months of the pandemic’s outbreak. In some cases, that added production was timely enough to help ameliorate the shortage, but in other cases the companies were not able to bring their capacity online in substantial amounts until other sources had largely filled the gap.
Importantly, one of the factors that helps bring forth surge capacity is the increase in prices that typically stems from a shortage. As noted above, prices for N95 masks grew from about $1 each to about $8 each at the peak of the shortage. But that phenomenon means that items bought during the surge will typically be substantially more expensive than items bought when demand is at normal levels. To a certain extent, surge capacity will
occur naturally, at least for PPE. As prices rise, more companies will find it economically feasible to enter into production or they will shift existing production lines that make similar products as that of PPE. We have seen this to a certain extent during the COVID-19 pandemic. For drugs, however, the requirements for FDA approval of production facilities, intended to ensure that the drugs those facilities produce are safe, makes it very difficult to enter the market during a shortage or shift production from other types of drugs to those in that are in shortage.
A policy option to encourage or force such shifts is the Defense Production Act (DPA), which essentially allows the federal government to commandeer production facilities in times of national emergency.27 According to many press reports, the Trump administration was somewhat reluctant to invoke the DPA, often preferring to work out voluntary arrangements with the appropriate firms. Even so, the threat of temporary nationalization presumably encouraged those companies to show flexibility. These experiences also suggest that at least 3 months, and more likely 6 to 9 months, may be needed to ramp up production of PPE by domestic sources.
In any event, all of these issues lead back to the central question of how to foster or support enough surge capacity in times of normal demand when that capacity is not needed. The closer to being ready these facilities are, the less time would be needed to ramp up production when needed, despite the higher the costs of maintaining that surge capacity in the interim. As an example, one option would be for companies to maintain excess capacity and run their plants at, say, 50 percent of their potential output. That would help to ensure that output could be expanded quickly when necessary.28 However, this would obviously be costly, so producers would need to be paid extra to do so, roughly double, in this case. Even then, the question of how they would obtain twice the raw materials they would normally use in order to double their output would remain. If output were to increase 10-fold, the economics of maintaining surge capacity would become more daunting still. The same issues arise when considering surge capacity in locations overseas, but at a lower level of spending because production costs are lower overseas.
___________________
27 The Defense Production Act became law in 1950. Rather famously, President Truman’s effort in 1952 to seize control of domestic steel mills during the Korean War was rebuffed by the Supreme Court. See Steve Hendrix, “Truman Declared an Emergency When He Felt Thwarted. Trump Should Know: It Didn’t End Well,” The Washington Post (January 11, 2019). https://www.washingtonpost.com/history/2019/01/08/truman-declared-an-emergency-when-he-felt-thwarted-trump-should-know-it-didnt-end-well/.
28 The United States and most other countries essentially do this with their militaries, maintaining much larger forces than are needed on a routine basis so as to have the ability to respond quickly to a crisis.
C. Stockpiling Supplies
Rather than maintaining surplus production capacity that could be surged, an obvious alternative would be to maintain actual surplus supplies that could be drawn upon in a shortage, particularly a large-scale one induced by a future pandemic. An analogy would be like saving for a rainy day, or perhaps a bird in the hand being worth two in the bush. A major advantage of this approach is that PPE and other supplies could be purchased from existing suppliers at roughly nonpandemic price levels. The obvious downsides of this approach, from an economic perspective, are the storage costs that have to be incurred in the interim, and the risk that the amounts stockpiled will either be too large, implying a waste of some resources, or too small, necessitating a surge in production or other measures. Even in these cases, however, addressing a given shortage would be easier than it would be in the absence of such a stockpile.
Background on Stockpiling.
The federal government had already established a Strategic National Stockpile (SNS) containing PPE, certain drugs, and other supplies deemed essential. However, those stockpiles were drained early in the pandemic, and some of the products it contained were found to be ineffective or expired.29 New targets have been set for the SNS, and these figures, along with the stockpiled inventories at recent points, are shown in Table 2. For reasons that are not clear, the most recent data on the contents of the stockpile that were available as of this writing is from May 21, 2021, nearly 6 months ago.30
TABLE 2 PPE in the Strategic National Stockpile (Millions of Items)
| Product | Inventory on 2/26/21 | Inventory on 5/21/21 | Planned 90-day Inventory | 5/21/21 as Percent of Planned |
|---|---|---|---|---|
| Surgical/Exam Gloves | 227 | 516 | 4,500 | 11.5% |
| N95 Respirators | 307 | 424 | 300 | 141.3% |
| Surgical/Face Masks | 411 | 273 | 400 | 68.3% |
| Surgical Gowns & Coveralls | 66 | 17 | 265 | 6.4% |
| Goggles & Face Shields | 18 | 20 | 18 | 111.1% |
___________________
29 Nick Miroff, “Protective Gear in National Stockpile is Nearly Depleted, DHS Officials Say,” The Seattle Times (April 1, 2020). https://www.seattletimes.com/nation-world/protective-gear-in-national-stockpile-is-nearly-depleted-dhs-officials-say/.
30 See https://www.phe.gov/about/sns/COVID/Pages/personal-protective-equipment.aspx.
As the table shows, the SNS held more than the target amount of certain PPE items, particularly N95 masks, but far less than other targets, particularly for surgical gowns. Also, SNS holdings increased between February and May for some items and decreased for others. The budget to operate and maintain the SNS in 2020 and 2021 was about $700 million per year; the Biden administration has requested about $900 million for 2022.31 Those budgetary figures do not include any additional appropriations that may have been provided through pandemic-related legislation in 2020 or 2021.
The target amounts for the SNS have been described as “90-day inventories,” but I was not able to determine how these targets were set, and in particular, what use rate was assumed in setting those targets. The target of 300 million N95 masks corresponds to annual usage of 1.2 billion masks, which is in the range of the quantity that would probably have been demanded in 2020, absent major supply constraints. But that target appears to have been set as early as February 2020, before the pandemic really began in earnest.
One important consideration regarding the federal government’s decisions about the extent of stockpiling is that state and local governments as well as medical providers themselves are likely to increase their stockpiles of PPE, at least for some period of time. Data on these activities are also hard to come by, but a survey by the National Governors Association in 2020 found that 9 out of 12 states surveyed indicated that they planned to increase their stockpiles, and 5 of those states intended to maintain a 90-day level of supply.32 Importantly, those levels of supply would be based on use rates observed in the pandemic. Another source indicated that 18 states aimed to maintain at least a 90-day supply of PPE, and another 10 states aimed to maintain at least a 30-day supply.33 Unfortunately, information was not available about the use rates used to develop the 90-day requirement for the level of those supplies.
Costs of Stockpiling.
As stated previously, finding data on the costs involved in stockpiling PPE and other key medical supplies was difficult. Nevertheless, there are a few available data points that may be informative.
The first one is the budget of the SNS itself. As indicated above, the budget to maintain a 90-day supply of PPE at pandemic-level use rates is about $900 million per year. This implies that doubling the size of the SNS to hold a 6-month supply would cost roughly $1 billion per year, or
___________________
31 Additional information about the SNS budget is here: https://www.phe.gov/about/aspr/Pages/Budget.aspx.
32 National Governors Association, Strategies to Address the Need for Personal Protective Equipment as States Gradually Reopen (July 28, 2020). https://www.nga.org/center/publications/ppe-reopening-covid19/.
33 See page 17 of the 2020 HIDA Personal Protective Equipment Market Report.
perhaps less, to the extent that the existing budget would reflect some fixed costs of simply having an SNS in the first place. Another data point comes from England, where press reports indicate that PPE storage is costing the government about £1 million per day.34 Conversion to dollars and adjusting for the fact that the U.S. population is about five times larger, that translates into $2.5 billion per year in storage costs.
A third and somewhat more obscure data point comes from Taiwan, which, like many countries, has also maintained a stockpile of PPE and other supplies prior to the COVID pandemic. About 10 years ago, Taiwan adopted a replacement model for its reserves of supplies, in which the oldest stock is sold off on a continuing basis, thus keeping the stockpiled supplies fresh. According to one analysis of that model,
The Taiwan CDC adopted a more economical and efficient way to refresh the stockpile, in which it pays the private contractors only a service fee instead of new products’ purchase cost. The service fee includes the manual and the computational process the contractors need to refresh the stockpile, which is less than the original purchasing cost, because the contractors could further sell the replaced stockpile to domestic institutions through the joint e-purchasing platform or to other countries through their own channels of distribution.35
Specifically, the authors estimated that the service fee for surgical masks was only 27 percent of the purchase price for those items; for N95 respirators, the fee was 46 percent of the purchase price, and for surgical gowns, it was 34 percent of the original price.
A final economic consideration regarding the option to stockpile PPE and other supplies is that the costs of that option will largely be the same regardless of whether the federal government maintains the stockpile itself or imposes stockpiling requirements on states or on health care providers. While there could be some economies of scale that make federal control of the stockpile advantageous, as with the SNS model, there could also be some advantages to local control of stockpiles and associated innovations in stockpile management. At the same time, a stockpile that is federally controlled could more easily be directed to areas of the country where the need for supplies is most acute. From an economic standpoint, a combination of local and national stockpiles would be ideal, and the most efficient.
___________________
34 Katherine Rushton, Sophie Barnes, and Laura Donnelly, “Government Paying £1M a Day to Store Mountain of PPE,” The Telegraph (November 22, 2020). https://www.telegraph.co.uk/news/2020/11/22/government-paying-1m-day-store-mountain-ppe-nhs-staff-still/.
35 Yu-Ju Chen and others, “Stockpile Model of Personal Protective Equipment in Taiwan,” Health Security, vol. 15, no. 2 (April 2017). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5404251/.
C. Diversifying Global Medical Product Supply Chains
Probably the least expensive option for expanding the capacity and improving the reliability of medical product supply chains is to continue purchasing supplies from other countries, while diversifying the specific sources used in order to reduce the risk that a single disaster, breakdown, or political event could disrupt supplies. However, keeping track of these medical product supply chains to ensure they remain robust under various scenarios may be challenging. In principle, treaties or other agreements could be reached in advance so countries do not hoard supplies in a future pandemic, but these agreements could be difficult to enforce, and the parties may prefer to violate the agreements first and deal with the consequences afterwards.
Costs of Diversification.
It is obvious that purchasing PPE and other medical supplies from foreign suppliers is less expensive than purchasing from domestic producers, which is why most PPE presently comes from abroad, where labor costs are lower. At the same time, diversifying medical product supply chains so supplies come from a broader set of companies, countries, or regions will cost somewhat more than current supplies; if it did not cost more, the supply chain would probably be more diversified already. In other words, the current suppliers and their supply chains are probably the least expensive sources of medical supplies at the quality and reliability levels observed today. If we were to want more suppliers or higher-quality supplies, or both, it would necessitate an increase in prices of at least a few percentage points. Unfortunately, data on the costs of such options are unavailable to me.
A related consideration is how to monitor the resiliency of medical product supply chains and to assess the costs of that monitoring. My understanding is that FDA has the theoretical obligation or right to inspect foreign production facilities used to make products bound for the U.S. market. In practice, however, the costs and challenges of sending inspectors abroad have proven to a barrier, so those inspections have been few and far between. Apparently, FDA cannot or does not hire local workers to carry out such inspections; the reason why is not clear. One option is simply to increase funding for those activities. As discussed in the next section, however, other options include having FDA move away from its focus on approving production facilities and instead focus on testing the products that are imported for quality, which will encourage producers to take steps to improve the quality and reliability of their supplies.
The Role of International Agreements.
Another set of steps that could be taken to help improve the reliability of global medical product supply chains would be to establish agreements or treaties to help govern activities in the next pandemic and to manage ongoing medical product supply
chains. Such agreements could include penalties that would raise the cost of hoarding supplies by allowing importers to apply tariffs. These pacts could also provide a structure for managing global production chains in an emergency.
However, arranging for international cooperation is easier said than done. Nations are essentially autonomous, acting largely in their perceived self-interest, and the ties between the developed countries that mostly buy medical supplies and the developing countries that mostly make them are weak. In a crisis, or when they perceive their national interests to be at odds with the interests of the larger group, nations have a strong tendency to put their own interests first, ahead of any treaty obligations that would obligate them to cooperate.
This challenge has been discussed extensively in other contexts, particularly in the area of international relations and security studies. Robert Jervis, a professor of political science at Columbia University, began his classic article entitled “Cooperation Under the Security Dilemma” in the following way:
The lack of an international sovereign not only permits wars to occur, but also makes it difficult for states that are satisfied with the status quo to arrive at goals that they recognize as being in their common interest. Because there are no institutions or authorities that can make and enforce international laws, the policies of cooperation that will bring mutual rewards if others cooperate may bring disaster if they do not. Because states are aware of this, anarchy encourages behavior that leaves all concerned worse off than they could be, even in the extreme case in which all states would like to freeze the status quo.36
While Jervis was focused on a situation in which nations wanted to maintain the status quo—peace—with a focus on nuclear arms control, the same issues arise when trying to cooperate to improve upon the status quo with respect to global medical product supply chains.
For their part, economists will recognize these concerns as practical examples of the “prisoners’ dilemma” scenario. In this scenario, two prisoners have been arrested for a crime they committed together. The prisoners involved would be better off if they could cooperate with each other and say nothing to the police. But each prisoner is tempted to cheat on the other by turning state’s evidence in order to gain a short-term advantage or to hedge against cheating by the other prisoner. The equilibrium result is that they both fink on each other; a poor outcome, from the prisoners’
___________________
36 Robert Jervis, “Cooperation Under the Security Dilemma,” World Politics, vol. 30, no. 2 (January 1978). http://www.sfu.ca/~kawasaki/Jervis%20Cooperation.pdf.
perspective, with a longer sentence for both than they would have achieved if they had both stayed silent. In some versions, the prisoners are unable to communicate, but the same basic result holds if they are unable to credibly commit to keeping mum.
Of course, such situations are not hopeless, as shown by the substantial number and scope of international agreements, particularly regarding trade. In general, game theorists have shown that repeated interactions tend to increase the odds of cooperative outcomes. Even so, disputes can go unresolved for many years, as evident in many long-standing disagreements between China and other countries regarding unfair trading practices, currency manipulation, and the protection of intellectual property rights. Simply put, pandemics that may occur years apart could be too infrequent to prevent countries from focusing heavily on the crisis that is at hand and ignoring concerns about dealing with the next crisis at some future point; that is, myopia would prevail. In any event, agreements related to medical product supply chains are likely to take many years to hammer out.
D. Quantifying Some Comparisons Across Options
Although data limitations make it difficult to quantify many of the trade-offs between these options, some useful calculations can still be made. In particular, it is feasible to illustrate some of the break-even points that exist as well as the sensitivity of those findings to different values of the key economic factors involved. Probably the most useful cases to illustrate are those involving the country’s preparedness for similar COVID-19 global pandemic. If the medical product supply chains were able to handle that set of circumstances, they would almost certainly be able to address less cataclysmic events such as natural disasters or regional health crises.
A specific question of interest is whether and under what circumstances it may be less expensive to stockpile supplies that are made abroad than to move production on shore. In the case of N95 masks, the information cited above indicates that domestic production would be about 50 percent more expensive. Stockpiling would allow the supplies themselves to be purchased at lower prices, but would also incur some ongoing costs for storage. Industry sources suggest that such costs are about 15 percent of the value of the inventory being stockpiled.
Now let us consider the costs of procuring a 6-month supply of N95 masks via on-shoring or stockpiling, that is, a 6-month supply to satisfy pandemic-type levels of demand. In the absence of major supply constraints, or equivalently at prices close to the prepandemic average price of $1 per mask, usage might be about 100 million masks per month, or 1.2 billion per year. A 6-month supply would be 600 million N95 masks, or double the current target level for the SNS. The cost of domestic production would be
- $1.50 per mask * 50 million masks = $75 million per year
- $1.50 per mask * 600 million masks = $900 million
- $Z = Annual cost of maintaining domestic surge capacity for 600 million masks
The first expression captures that annual cost of meeting nonpandemic demand levels at domestic prices; the second is the cost of buying the masks needed when the pandemic hits; the third term reflects the annual cost of maintaining domestic surge capacity so that supplies can be ramped up from 50 million per year to 100 million per month when the next pandemic hits.
If instead, masks were purchased from foreign sources and stockpiled, the three corresponding terms would be as follows, with the third term here representing storage costs:
- $1.00 per mask * 50 million masks = $50 million per year
- $1.00 per mask * 600 million masks = $600 million
- $1.00 per mask * 600 million masks * 15 percent = $90 million per year
Taking the differences between these three components yields expression (7) below, which captures the added costs (if any) of domestic production. The relative costs depend on how many years it will be until the next pandemic occurs, which is hard to predict. That unknown is represented by the variable X. The relative costs also depend on what $Z equals and how it compares to the annual costs of maintaining the stockpile.
- $25 million * X + $300 million + ($Z million – $90 million) * X
If $Z happened to equal $90 million, then expression 7 would always be positive, meaning that on-shoring would never be cheaper than stockpiling. Indeed, the expression would be positive for all values of X so long as $Z was greater than or equal to $65 million. Alternatively, if $Z was equal to $5 million, the added costs of domestic production would simplify to this:
- $300 million – $60 million * X
In this case, on-shoring would be cheaper than stockpiling if the stockpile had to be maintained for more than 5 years. If $Z were $45 million, or half of the annual costs of maintain the stockpile, then stockpiling would be cheaper as long as X is less than 15 years.
More generally, Figure 2 below shows the points at which on-shoring and stockpiling would have the same costs as a function of $Z and X. In
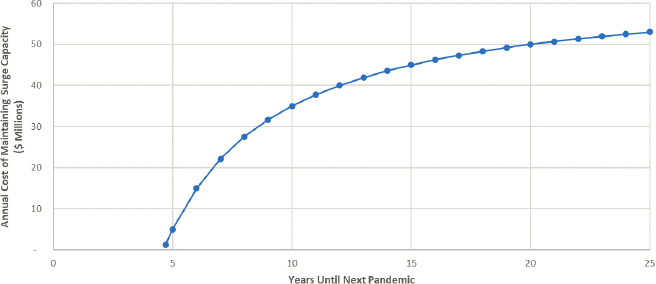
Above the Line, Stockpiling Is Cheaper
this analysis, I have maintained the assumption that domestic production involves a 50 percent price premium. Above the blue line, stockpiling is the cheaper option, which happens when the next pandemic is expected to occur sooner, or when the annual costs of maintaining domestic surge capacity rise.
The same approach can be used to assess how sensitive the results are to other assumptions or estimates. In Figure 3 below, I hold X equal to 10 years and examine how the break-even points vary as a function of $Z and the domestic price premium. Here, the relationship is linear, with stockpiling being less costly when the domestic price premium is higher or the annual costs of maintaining domestic surge capacity increase.
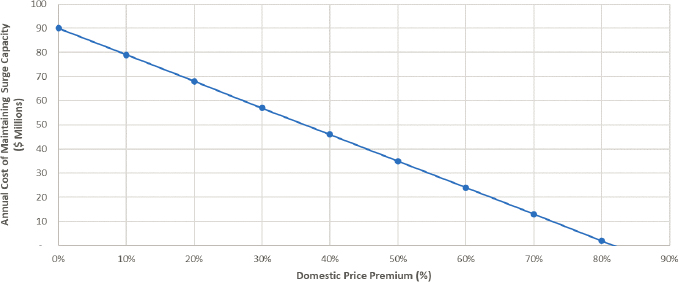
Above the Line, Stockpiling Is Cheaper
POLICY OPTIONS TO SPUR CHANGES IN MEDICAL PRODUCT SUPPLY CHAINS
In general, where the elements of medical product supply chains are located and how they operate are up to the private companies and organizations that produce and purchase these products. These private actors make choices in light of the incentives they face and the goals they seek to achieve. In order to change how medical product supply chains work, federal policies will have to influence those choices through some combination of regulations, subsidies, and penalties. In some cases, the distinction between subsidies and penalties on the one hand, and regulations on the other, can become blurred. Private actors may also lack the information they need to make the choices that achieve their goals and ideally, to also produce outcomes that are better for society as a whole. Thus, another role for government may be to improve the information available to them that concerns the medical product supply chains.
A. Improving Information
As noted throughout this analysis, the issues involved in supplying PPE and other materials during a pandemic and the issues involved in addressing ongoing problems with the supply of generic drugs are often sufficiently distinct as to warrant different solutions. Such is the case regarding the information that would be helpful in bringing about more reliable and secure medical product supply chains. Potentially, this information could be used in structuring subsidies for favorable actions or actors and penalties for the unfavorable ones, which would indeed provide incentives to improve behavior. However, in and of itself, the provision of information generally does not incentivize action.
Information on Pandemic-Related Supplies.
One problem that quickly became evident at the start of the COVID-19 pandemic is that no clear and comprehensive picture was available regarding the status of PPE supplies and the demand for them, as expressed in orders. In the United States, the vast majority of those supplies are purchased from one of five large distributors. Rather quickly, HHS was able to establish agreements with those companies to receive continuous updates about their holdings and the orders and supplies that they had received. This repository of information was known, at least informally, as the “control tower.”
Because the infrastructure for such a control tower can be difficult to erect at the onset of a pandemic, or may at least take up precious time, it makes sense to continue that activity after the COVID-19 pandemic subsides. How much it would cost to maintain that capability, however, and
under what terms the companies involved would agree to do so, are not clear.
Information on Generic Drug Production.
A prominent proposal in the recent FDA report on drug shortages was to improve the information available to purchasers about where and how the drugs they buy are made. Specifically, the report recommended “the development of a system to measure and rate the quality management maturity of individual manufacturing facilities based on specific objective indicators. The rating system would evaluate the robustness of a manufacturing facility’s quality system” and could help identify manufacturers that maintain a robust medical product supply chain. Currently, purchasers and other observers have noted that they lack “line of sight” into where the drugs they buy are made, and do not have an easy way of assessing their quality. Toward that end, simply rating individual facilities might be insufficient; instead, a more fulsome assessment of the reliability of entire medical product supply chains may be necessary. The costs of establishing such a system, however, are hard to estimate.
Such a step would probably be helpful in improving the reliability of medical product supply chains, particularly for generic drugs. It is worth noting, however, that consumers often have little information about where or how the products they buy are made except for perhaps a “made in” label. Clearly, drugs are not average consumer goods and problems with their quality would cause substantial harm. Therefore, one might expect drug purchasers to be hypervigilant about product quality as a result. Although individual hospitals might well find it challenging to establish their own quality-control systems, additional private actors could fill the gap if there was indeed a willingness to pay the costs of these activities. Automobiles are another complex product with important safety dimensions. For these, the Insurance Institute for Highway Safety (IIHS) provides crash test information that is summarized in a user-friendly way, while J.D. Power and Associates provides quality awards.37 The apparent lack of such mechanisms for generic drugs again suggests that there is not a sufficient willingness to pay for that information on the part of drug purchasers.
B. Relaxing or Strengthening Regulations
The choices of private actors that affect the structure and performance of medical product supply chains are themselves influenced by a wide range of regulations, many but not all of which are set at the federal level. In some cases, policy makers could seek to improve the reliability of sup-
___________________
37 The federal government also provides crash test results, but the IIHS assessments may be more useful to consumers.
plies by relaxing certain safety regulations. For example, FDA could make it easier for new suppliers to enter a market if a drug shortage has arisen, or regulations governing reuse of PPE could be relaxed. These approaches, however, run the risk of reducing safety for patients and care providers, as well as generating additional adverse outcomes.
In other cases, policy makers may seek to impose more extensive regulations on suppliers or purchasers than those that exist today, but such approaches also tend to raise costs for suppliers and purchasers. For example, federal programs like Medicare and Medicaid could require providers to obtain their supplies from companies that can demonstrate they have robust supply chains, or FDA could even require such a demonstration as a condition of selling generic drugs in the U.S. market. In addition to regulations primarily affecting the supply or demand of medical products, federal and state regulations for price or payment rates for items under Medicare or Medicaid also have a ripple effect on medical product supply chains, and may need to be reconsidered in light of efforts to improve reliability.
Regulations Primarily Affecting Demand.
The most obvious examples of regulations affecting the demand for medical supplies may be the ones governing how often PPE must be changed in the course of treatment. In general, the rule of “one patient, one unit” had applied to PPE prior to the pandemic. However, because of the PPE shortages that arose, FDA relaxed some of its regulations temporarily, and CDC issued guidance indicating that prolonged use or reuse of certain PPE should be allowed as needed to address shortages.38
Concerns about the effects of relaxing regulations on safety and disease transmission are certainly warranted, but in a crisis the alternatives may be worse. Even with time to plan in advance for what to do in another pandemic, the option of relaxing these regulations is still worth considering because its costs could also be less than those for other approaches. I presented some estimates above about the costs of relaxing those rules, particularly in terms of excess lives lost. But those estimates are based on limited information. A more extensive analysis of the risks involved and any excess transmissions that may have been caused by the emergency use authorizations related to COVID-19 should be undertaken as part of a broader assessment of the competing risks posed by all of the options for improving the reliability of medical product supply chains.
Regulations Primarily Affecting Supply.
FDA regulations affect the supply of drugs in many ways. First and foremost is the requirement for drugs to have approval as being safe and effective, without which they cannot be supplied at all. FDA then regulates drug production processes in several
___________________
38 Centers for Disease Control and Prevention, “Summary for Healthcare Facilities: Strategies for Optimizing the Supply of PPE During Shortages” (updated Dec. 29, 2020). https://www.cdc.gov/coronavirus/2019-ncov/hcp/ppe-strategy/strategies-optimize-ppe-shortages.html.
ways. As part of the application for a new drug, FDA assesses whether the manufacturing methods will be adequate to assure the drug’s identity, strength, quality, and purity. Additionally, FDA seeks to ensure product integrity on a continuing basis “through product and facility registration; inspections; chain of custody documentation; and technologies to protect against counterfeit, diverted, subpotent, adulterated, misbranded, and expired drugs.”39 As a part of this process, FDA has established a set of Current Good Manufacturing Practices that drug makers are required to follow.
To an outside observer, it is somewhat surprising that FDA puts so much emphasis on what might be called process measure of quality, rather than on outcome measures. The agency requires some sampling and testing of in-process materials and drug products, and it does try to track adverse outcomes among patients through postmarket surveillance programs, but arguably a better approach would be to test the finished products extensively for purity and potency. To a certain extent, FDA’s focus on production processes may be from the historical legacy of predecessor agencies going back to the early 1900s, for which “ensuring product integrity was the key task.” Granted, the costs of testing a sufficient sample of each of the products under its purview may be greater than the costs of overseeing production processes, but the results might also be better. Both the costs of testing and the risks of shifting from one regulatory regime to another could be limited in two ways: one, if such testing were used as an added measure rather than a substitute measure, at least initially, and two, if the initial focus of the testing program was narrowed to the types or categories of drugs that have had repeated quality problems or shortages, such as generic sterile injectables.
Some observers argue for going further. In a recent piece, Dr. Rena Conti and Dr. Fiona Scott Morton, two widely recognized experts on prescription drugs, argue that drug companies should be required to report detailed information about their medical product supply chains in order to “receive annual approval to sell into the U.S. market, which would create a strong incentive for manufacturers to comply in a timely fashion.”40 Furthermore, they propose a new office should be created within the Department of Health and Human Services, but outside of FDA, that would be charged with analyzing and improving the reliability of pharmaceutical supply chains. Among the reasons they cite are that “FDA has been the agency responsible for supply chain disruptions for over a decade, includ-
___________________
39 This discussion is drawn in part from Congressional Research Service, How FDA Approves Drugs and Regulates Their Safety and Effectiveness (May 8, 2018). https://sgp.fas.org/crs/misc/R41983.pdf.
40 Rena M. Conti and Fiona Scott Morton, “Building a Resilient Rx Drug Supply: A New HHS Office and Other Steps,” Health Affairs Blog (August 27, 2021). https://www.healthaffairs.org/do/10.1377/hblog20210824.559824/full/.
ing the sale of substandard products into the U.S. market that have harmed Americans.”41
Regulations Governing Prices.
While regulations affecting the demand for—or supply of—medical products obviously influence their prices as well, some federal regulations affect the prices of those goods more directly. In particular, recent studies indicate that laws and regulations reducing the payment rates for generic drugs under Medicare and Medicaid have played a role in causing shortages of these drugs. While the specifics differ, it stands to reason that a reduction in revenue for generic drug makers would put pressure on them to adopt lower-cost production methods and to use supply lines that are more vulnerable to disruptions, or at least to limit their investments in robust medical product supply chains.
Under Medicaid, the most relevant regulation may be one that was enacted recently. Medicaid has long required drug manufacturers to pay rebates on original, brand-name drugs when their prices rise faster than the general rate of inflation. Legislation enacted in 2015 extends that same requirement to generic drugs. While the desire to reduce spending on Medicaid is understandable, that requirement means that any price spikes stemming from a generic drug shortage will have to be rebated to that program.42 As a result, generic drug makers gain less from a given price increase, and would therefore not increase supply as much, nor would they have to raise prices higher to bring supply and demand into alignment. Shortages are somewhat more difficult to address, and since Medicaid accounts for about one-eighth of all domestic spending on generic drugs, the effect may be substantial.
A similar trend has been observed for a price reduction in Medicare, and in that case the magnitude of the effect could be quantified. Specifically, a study looked at the effect of substantial reductions in Medicare’s payment
___________________
41 Having worked for the federal government for 2 decades, and having studied its operations, I respectfully disagree with their proposal to create a new agency outside of FDA that has overlapping responsibilities with it. I agree with their diagnosis that FDA has been slow to change and has not been effective enough in responding to ongoing shortages of drugs, but I believe that establishing a new center within FDA focused on issues involved in drug production, including the reliability of medical product supply chains, is more likely to succeed. That success is by no means guaranteed, however, and determined leadership over a period of many years will be needed to make a new center, and a new approach, take hold. (FDA’s organizational chart is at https://www.fda.gov/about-fda/fda-organization-charts/fda-overview-organization-chart).
42 See Richard Manning and Fred Selck, Penalizing Generic Drugs with the CPI Rebate Will Reduce Competition and Increase the Likelihood of Drug Shortages (Bates-White Economic Consulting: September 12, 2017). https://www.accessiblemeds.org/sites/default/files/2017-09/Bates-White-White-Paper-ReportCPI-Penalty-09-12-2017.pdf.
rates for physician-administered drugs that were implemented in 2005.43 The resulting reductions in prices averaged about 50 percent. That change in policy was quite understandable, since by all accounts Medicare had previously been paying much higher prices, based on the drugs’ list prices, than private insurers had paid. Nevertheless, a payment cut is a payment cut, and the study’s authors estimated that this cut could account for a 25 percent increase in the expected number of shortage days per year for generic drugs. This change may have been an important factor behind the rise in shortages that has been observed over the past 15 years.
C. Providing Subsidies or Imposing Penalties
If it chose to do so, the federal government could subsidize the higher costs of domestically produced PPE or the higher cost of maintaining robust supply lines for generic drugs in a wide variety of ways:
- Medicare and Medicaid payments to hospitals could be increased to reward hospitals that purchase PPE domestically or that maintain robust supply lines.
- Tax credits or deductions could be used to reward companies that make improvements to their supply chain’s reliability and security.
- The federal government could set up a program of direct outlays of subsidies to accomplish the same goals.
In each of these endeavors, the two key challenges will be defining what activities qualify for subsidies and determining the subsidy rate. Inevitably there will be some perverse compliance and some “buying out the base,” a term budget analysts use when referring to payments to people or organizations for complying with program requirements when they would have complied anyway, without a payment.
Even so, economists often recommend providing subsidies or imposing penalties as a means of changing the behavior of private actors in a relatively efficient way. Examples include subsidies for clean forms of energy use, free vaccinations for communicable diseases, and “sin” taxes on cigarettes and alcohol. In general, the goals of such approaches include having private actors internalize the benefits or costs that their actions impose on others, as well as those which they might ordinarily fail to consider, plus yielding too much activity that can cause external harm and too little activity that could provide external benefits. Such policies effectively lower
___________________
43 Ali Yurukoglu, Eli Liebman, and David B. Ridley, “The Role of Government Reimbursement in Drug Shortages,” American Economic Journal: Economic Policy, vol. 9, no. 2 (May 2017). https://www.jstor.org/stable/26156409. See also: https://www.nber.org/system/files/working_papers/w17987/w17987.pdf.
the price of favored activities and raise the price of unfavored ones. The resulting quantities that are supplied depend on how responsive buyers and sellers are to the changes in prices.
Instead of adjusting prices, an alternative approach is to limit the quantity that can be produced of a product that is known to have had adverse effects. For example, certain forms of pollution are capped, with tradeable permits issued that allow polluters to buy and sell emission rights in a way that helps minimize the cost of achieving a given reduction in pollution. As a result, the market price of polluting will settle at the level needed to limit pollution to the prescribed amount. It might seem that imposing a tax on pollution and limiting the quantity of allowed pollution would be equally effective, but an important article in the field of regulatory economics found that in the face of uncertainty between optimal price and optimal quantity, the more efficient approach is to regulate the one which is less uncertain.44
How do these rather abstract considerations apply to medical product supply chains? In the case of PPE, the federal government could increase domestic production, either by subsidizing domestically produced items, or by ordering a certain quantity of domestically produced goods. If the government was omniscient, it could choose either target with equal precision. But in reality, we have only a rough idea of how much PPE we might need in a future pandemic, and an even rougher idea of what sort of subsidy domestic producers would need in order to be competitive with foreign sources of supply, nor do we know how much these domestic producers would supply.
We, as a polity, may be more certain about the quantity of PPE that we want rather than the price we should pay to get that quantity. In other words, setting a subsidy for PPE may require more trial and error than specifying an amount to stockpile and purchasing that amount, at whatever price emerges. Likewise, with generic drugs, we may have a better idea of what quantities we want to maintain in the event of a supply disruption than we do about the subsidies needed to yield the desired increase in reliability and reduction in shortages.
__________________
___________________
44 Martin L. Weitzman, “Price vs. Quantities,” Review of Economic Studies, vol. 41, no. 4 (October 1974). https://scholar.harvard.edu/weitzman/publications/prices-vs-quantities.
This page intentionally left blank.






































