
8
Preparedness Measures for Resilient Medical Product Supply Chains
As described in the previous two chapters, awareness and mitigation measures can reduce the size and prevalence of supply disruptions. They are practical and cost-effective strategies for avoiding shortages caused by routine process control problems. However, major supply disruptions and demand surges caused by natural disasters, pandemics, or biological threats are much more difficult to avoid. Manufacturing problems will constrain supply, emergencies will spike demand, and all manner of events—predictable and unpredictable—will lead to imbalances of supply and demand for critical medical products. Therefore, to address these, a balanced supply chain resilience strategy must also contain preparedness measures that shield the public from harm when these events occur.
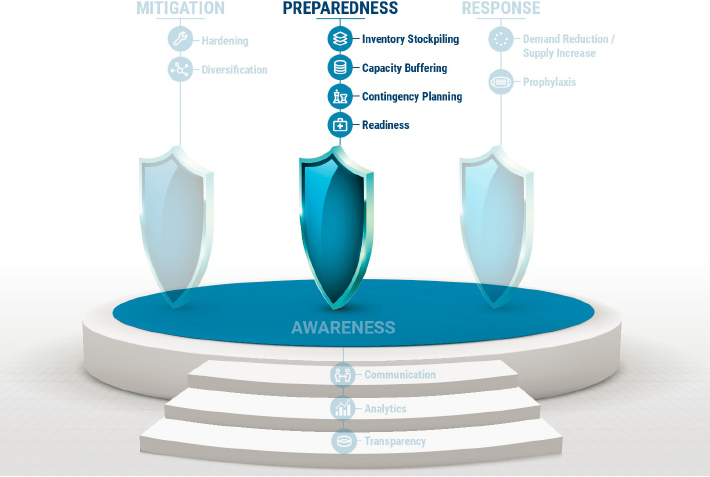
Preparedness includes actions taken prior to a disruptive event that will reduce the negative effects on health and safety if the event occurs. As described in the medical product supply chain resilience framework in Chapter 5, preparedness measures can be grouped into four subcategories, two physical and two virtual (Figure 8-1). Physical preparedness measures include inventory stockpiling and capacity buffering, in which stock or productive capacity are held to fill a supply shortfall. Virtual preparedness measures include contingency planning, which establishes plans for dealing with specific scenarios, and readiness, which builds capabilities for dealing with scenarios without specific plans made in advance. Each of these categories is vital to an integrated resiliency strategy. Additionally, in the discussion that follows, the committee covers how the measures in the different categories can be complementary, and their selection as preparedness measures must consider this complementarity.
Some of the preparedness measures the committee recommends represent market interventions by the government. Medical product supply chains need these interventions because, as discussed in Chapter 4, medical product supply chains are typically optimized for routine conditions, with regular lead times and predictable levels of variability in demand and supply. Producers of medical products achieve this by taking steps to ensure supply can regularly meet demand, and thereby protect their revenue streams. Producers also control costs with various measures including lean production and supply chain practices. Lean medical supply chains are effective in serving patients and producing profits under routine conditions but are often ill equipped to respond to disruptions that are outside of the normal variability in supply or demand (HIDA, 2020). As the committee noted in Chapter 4, products with low profit margins are particularly likely to have supply chains that are vulnerable to failures in emergency situations because manufacturers lack any financial incentives to build in protections. When this is the case, outside interventions are needed to induce preparedness measures that meet the public need for public health and safety, rather than only the private sector’s incentives to maximize profits.
Box 8-1 provides an overview of how to set a protection target for a given product and how to select and combine preparedness measures to achieve it. More details on this process are given in Chapter 5. In this
chapter, the committee elaborates on this process in discussing the issues of execution and coordination within each preparedness category. These discussions provide the motive and inform the two preparedness recommendations that focus on inventory stockpiling and capacity buffering.
INVENTORY STOCKPILING
The most basic form of inventory stockpiling is holding physical stock in a state of readiness in preparation for a supply shortfall. Manufacturers, distributors, and health care systems all hold inventories of drugs and devices as protection against normal variations in supply and demand. However, these inventories are typically inadequate to protect against an unusual disruption of supply or an unanticipated surge in demand. Therefore, the federal government holds additional physical stock of critical medical products known as medical countermeasures (MCMs) in the Strategic National Stockpile (SNS). In theory, this is an excellent protection measure. With a reasonable estimate of the protection volume Xi for a given product i, then a stock level of Xi is one way to provide the appropriate amount of protection (see Box 8-1). However, it is not the only option, and other forms of preparedness should be considered to find the right balance of measures to improve resilience. Furthermore, there are real-world issues with holding inventory that this chapter will evaluate.
Holding inventory is more complicated in practice than in theory. In reality, problems with forecasting demand, monitoring stock levels, rotating stock to prevent expiration, and other practical details can prevent inventory stockpiles from providing the intended level of protection in an emergency. For example, a recent analysis of the SNS noted that the lack of transparency into medical product supply chains caused a lack of strategic forecasting leading up to the coronavirus disease (COVID-19) pandemic. This analysis also found that a lack of technology to monitor demand further hindered setting appropriate stock levels. Such problems led to inadequate supplies in the SNS, including for personal protective equipment (PPE), which had been depleted during the H1N1 pandemic and was not adequately restocked before the COVID-19 pandemic struck (Klein, 2020; Reinhard and Brown, 2020).
The SNS and other public inventories can improve the effectiveness of their stocks by applying evidence-based approaches to managing their inventories. For example, calculating optimal inventory levels can prevent hoarding and overstock. These calculations take into account the demand rate, order lead time, setup cost, proportional order cost, and inventory holding cost to determine the optimal amount of inventory to have on hand (Nahmias and Olsen, 2021). Using such data-driven models can help provide cost-effective protection against shortages, discourage hoarding, and respond to normal variations in supply and demand. In addition, strategic stockpiling helps to buffer the system against variations outside the normal range of routine disruptions discussed earlier.
The Public Health Emergency Medical Countermeasures Enterprise (PHEMCE) develops the SNS Annual Review. These reviews provide policy guidance to the Office of the Assistant Secretary for Preparedness and
Response (ASPR) and the SNS for budget formulation and procurement of MCMs. Innovations in how the SNS is maintained are a major lever of PHEMCE, and a recently released National Academies report and a recent White House report both call for a root cause assessment of SNS lessons learned from COVID-19 and other past public health emergencies (DoD et al., 2021; NASEM, 2021a). While the SNS’s budget is limited by the funds it receives from Congress, a recent National Academies report on examining PHEMCE highlighted multiple options, including public–private partnerships, that could be implemented to improve national preparedness and response. Specifically, these options could assist with “key stockpiling decisions [including] what, how much, where, and how to stock; how to allocate limited resources; and how to resupply” (NASEM, 2021a).
Vendor-Managed Inventory and Consignment Inventory
Decentralization is a common industry approach for dealing with some of the complexities of inventory management. Rather than a single actor (e.g., the health system or the retailer) making all inventory management decisions and incurring the cost of inventory holding, stocking decisions and partial related costs are relegated to other actors—suppliers—with superior knowledge and experience with specific products. Two approaches for this type of decentralization are vendor-managed inventory (VMI), in which suppliers are responsible for controlling inventory levels, and consignment inventory (CI), in which suppliers own and maintain physical stock (Lakra and Bedi, 2014).
An example of VMI is Walmart’s policy of allowing suppliers to manage inventories in its warehouses (Greenspan, 2019). Suppliers make use of stock level, point-of-sale data from Walmart, and their experience base (e.g., knowledge of demand seasonality) to calculate the appropriate volume of warehouse stock levels.
To use VMI, the product supplier, such as a medical device or drug manufacturer, takes full responsibility for maintaining an agreed-upon inventory level of the product or its components at the end user’s location (e.g., hospital or pharmacy). For example, a hospital seeks to ensure that a given medical product is always in stock. Under a VMI model, the supplier would determine a reorder point that would provide sufficient stock to ensure this level of service, as well as an efficient replenishment quantity that would balance the costs of shipping and holding inventory. Each time the reorder point is reached, the vendor is notified and ships the replenishment quantity to the hospital. With the correct systems in place to monitor the hospital’s consumption, such as the vendor being on site checking supply levels or the hospital regularly sending usage reports to the vendor, patterns can be identified, and the product stock levels can be adjusted as needed.
A VMI model can help end users in health care achieve improved patient care and service, reduced demand uncertainty, and reduced inventory costs. However, since VMI systems rely on the vendor/supplier to keep track of the actual number products or units in stock, health systems have a reduced visibility of future inventory, leading to an increased risk of a shortage within a health system and a decreased resilience of the supply chain. Therefore, prior to using a VMI approach, a careful risk assessment must be done to determine how the health system will handle an emergency response situation.
Consignment inventory (CI) is another useful tool to improve the management of medical product inventories. An example of CI is Amazon’s use of drop shipping, in which online orders are filled from stocks owned and held by suppliers (Amazon, 2021). Under a CI system, a supplier maintains an end user’s promised inventory either at the supplier’s site or some other location. The end user purchases the inventory only when they use it. The government and health care systems could use a CI approach to free up working capital, reduce overall supply expenses, and keep products that are expensive and difficult to acquire at the ready. However, a major drawback for end users with a CI system is the lack of direct management, oversight, control, and transparency over inventory; products may become misplaced, damaged, expired, or go to competing nearby facilities. This can lead to increased costs associated with expired or unusable products. Furthermore, a particular unit of product can be promised to several customers without any of them really knowing how many units are being stored against what kind of risk. These problems can become particularly acute during emergencies that cause a sudden surge in demand, resulting in a lower than planned level of protection. For either a VMI or CI model to work between suppliers and end users, it is critical for there to be trust between parties, an understanding of performance capability, clear and frequent communication, and transparency (Sumrit, 2020).
Options for the Strategic National Stockpile
Health systems can make use of VMI and CI to manage inventory effectively during normal routine conditions. While stockpiling is already part of the national preparedness strategy, primarily in the form of the SNS, the exclusive authority vested in that federal function is problematic (Fitzpatrick, 2020; NASEM, 2021a). To make the SNS more effective than it was during COVID-19, the SNS can model how health systems manage inventory. The SNS must refine and improve the ways it holds its inventory as protection against a supply shortage or demand surge. In particular, one problem in the SNS that VMI or CI could address is product expiration. While all drugs and medical devices have expiration dates set by the manufacturer, their
actual shelf life, if stored properly, can be much longer (AMA, 2001; Lyon et al., 2006). A federal initiative called the Shelf Life Extension Program was developed in the 1980s to defer and reduce the replacement costs of federal stockpiles of critical medical products by extending useful shelf lives through periodic U.S. Food and Drug Administration (FDA) stability testing and strict environmental controls (Khan et al., 2014; Lyon et al., 2006). Yet, replenishing stockpile products postexpiration is challenging since this can occur long after the events that necessitated their use passed. During the interim, public and political support for large government expenditures to store medical products that may never get used can wane. This was the case after the response to the H1N1 influenza pandemic in 2009. During H1N1, the SNS distributed large quantities of emergency medical supplies, but Congress never appropriated funding to replace the items used in that effort (Quinn, 2020; Rule, 2020). Therefore, when states and other agencies began requesting assistance from the SNS in March 2020 for response to COVID-19, the medical products remaining from the H1N1 response were deemed past their shelf life and unable to be used (Lieb and Dil, 2020; Rule, 2020). The lack of local control and oversight of government-held stockpiles was a serious impediment to flexible responses to the pandemic.
Using VMI or CI strategies where inventory is located adjacent to a manufacturing facility or distribution warehouse would shift rotation and expiration date problems to vendors with detailed product knowledge. This would be particularly valuable for short shelf life products where frequent rotation is necessary. Under a VMI or CI system, new stock would be delivered to the warehouse, spend a specified amount of time in stock, and be shipped out through normal supply channels in first in, first out fashion. This would provide protection for a duration equal to the amount of time the product is kept in stock and would eliminate the excess material handling due to shipping product in and out of a separate SNS facility to manage expiration dates. It would also vastly simplify the SNS management duties of the government.
Note that VMI and CI systems that put responsibility for stocking and rotation in the hands of individual vendors with detailed knowledge of their products will benefit the SNS regardless of whether the stock is owned by the government and held in public facilities (VMI) or owned and stocked by vendors (CI). However, because vendors lack profit incentives to maintain these stocks, accountability measures are still needed. The logical way to achieve this is for the government to pay vendors for the cost of stockpiling products and to monitor vendor performance, perhaps via periodic audits. Unlike the Walmart and Amazon examples where retailers can evaluate suppliers on their ongoing performance, emergency scenarios occur rarely by definition. Therefore, waiting for an emergency to evaluate a stockpile is too late. It must also be stressed that there is no one-size-fits-all strategy.
The key is to analyze product and/or supply chain risk with respect to the medical product supply chain resilience framework (see Figure 8-1) and decide on the most appropriate protection level and strategy.
An additional measure for effective stockpiling would be to push more responsibility for inventory management to the state and local levels. Local health officials and health systems have much better knowledge about inventory usage patterns, distribution plans to rotate stock, and how to align communications and activities needed to make VMI more robust. This gives them the advantageous position to forecast emergency demand, to monitor stock levels, and to allocate and release inventory regionally. These same local officials would also serve as powerful advocates for the replenishment of critical stocks, which might prevent failures to rebuild stockpiles after an emergency, as happened with PPE and other products after the H1N1 pandemic (Quinn, 2020; Rule, 2020). Therefore, a reasonable strategy for the SNS and the National Stockpiling Strategy is to have a national program with regional stockpiles and national guidelines, similar to what is currently in place. However, some central planning, funding/incentives, and oversight must be retained because independent planning will overlook opportunities for resource sharing, such as shipping ventilators from one region to another as relative needs shift during an event.
Without information, VMI, CI, and regional stockpiles cannot function. To manage stockpile inventories, stakeholders—hospitals, health departments, first responders, suppliers—need information about surges in demand and remaining supplies. To evaluate the inventory implications of disruptions, planners need information about prevention and mitigation measures, such as mask reuse and resource sharing. For example, if crisis standards call for N95 masks to be reused X times instead of once, then total demand will be 1/X the forecast of uses during the emergency. Finally, stakeholders need inventory data about what medical products are available and where. Because such information has national security concerns, technology is needed to preserve security while providing transparency. The use of blockchain as a data synchronizer,1 as well as predictive analytics, have been proposed as ways to help forecast demand more effectively and therefore inform stockpiling practices (Bhaskar et al., 2020).
CAPACITY BUFFERING
Economically, capacity buffering can be a cost-effective alternative or supplement to inventory buffering when protecting against shortages. Inventory buffers require the production and storage of products in advance.
___________________
1 Blockchain is a shared, fixed ledger that facilitates the process of recording transactions and tracking assets in a network. Assets can be tangible or intangible. Tracking and trading on a blockchain network can reduce risks and costs for all network members.
This is advantageous during sudden shortages as inventory is immediately available. However, inventory stockpiles simultaneously incur both the fixed and variable costs of manufacturing (i.e., facilities/equipment and material/labor, respectively), along with the costs of storage. Capacity buffers, alternatively, rely on having the production capability prepared and manufacture the products only if the additional supply is needed. See Box 8-2 for an example of capacity buffering in action.
While this necessitates lead time to activate the capacity and to produce the needed products, with the fixed-cost investments up front, the overall cost between fixed and variable manufacturing is split (Huang et al., 2016). See Chapter 5 for an additional discussion on the economics of inventory stockpiling and capacity buffering.
It is important to note that, as described in Chapter 5, any strategy for creating capacity will only work if sufficient supplies of ingredients and components are also available. This implies that capacity buffers are needed at all stages of the supply chain or that there are adequate inventory stockpiles of ingredients or components. The latter option is what many firms do via assemble-to-order strategies. For example, Dell Computer stocks components such as central processing units, memory chips, keyboards, screens, and power supplies, and puts them together to configure specific computers for customers. This type of assemble-to-order strategy allows Dell to be responsive to customers while vastly reducing the cost of the inventory they carry (CFI, 2021).
The combination of technology advances, which make final assembly cost competitive in the United States, and an assemble-to-order strategy could facilitate on-shoring (see Box 8-3). For example, suppose advanced manufacturing makes the fill-and-finish stage of production for a given drug cost competitive in the United States, but active pharmaceutical ingredient
production remains highly uncompetitive. On-shoring the final step would provide little ability to sustain or ramp up production during an emergency if components are in short supply. But if these critical inputs are stockpiled (perhaps using VMI or CI), on-shored final assembly could be beneficial since it could protect against disruption of imported supplies.
Market Incentives
While useful, the medical product supply chain resilience framework has its limitations. Inventory stockpiles and capacity buffers are an important part of a balanced supply chain resilience strategy. But these are not simple levers that can be engaged directly. Although the government
can purchase and stockpile supplies of critical medical products, doing this effectively requires regional coordination, engagement of end users, and public–private cooperation, as described earlier and addressed later in Recommendation 4 (Stockpiling). Capacity buffering is even more nuanced because direct government control is problematic, and capacity usually needs to be virtual to be cost-effective.
Although the federal government could set up its own manufacturing facilities to produce needed critical medical products, it would be enormously expensive to hold such capacity idle in anticipation of an emergency. The federal government could also enter selected markets by establishing production facilities to produce generic drugs and simple medical devices. But this fundamental change in the role of government and the workings of the health care system is beyond the scope of this study. Therefore, the most practical approach is to consider options for creating capacity buffers within the current market for drugs and medical devices.
A basic obstacle to the resilience of medical product supply chains is that profit motives of manufacturers and vendors motivate a smaller investment in protection than is optimal from a public health perspective. The gap between privately optimal and publicly optimal investment is most acute where margins are low but medical needs are high. For example, an inexpensive generic drug that is essential to health does not warrant significant private investment to protect revenue streams but does warrant significant public investment to protect health.
On the inventory side, the gap can be bridged with public investment in stockpiles; however, capacity will require a more subtle approach. Ideally, this approach should create incentives for the private sector to create additional capacity buffering but be flexible enough to allow manufacturers or hospitals to find the most efficient ways to do this. As such, incentives should focus on the ends (i.e., production of emergency supplies when needed) rather than the means (i.e., who produces what and how).
A mechanism for inducing more investment for capacity buffering by private firms is to pay for it in the form of “crisis prices.” These could be set via auctions in which the federal government takes bids to deliver supplies of specific medical products to supplement stockpile inventories. This is similar to what the government does when the Defense Production Act (DPA) is invoked (FEMA, 2020; Scott, 2020). However, holding open auctions would open the door to innovative entrepreneurs with novel ways of creating capacity buffers. Also, to give firms incentives to make time or money investments to be ready to bid in these auctions, the government should publish, in advance, a list of products eligible for crisis prices, along with information about the events that would trigger an auction. Finally, to prevent fraud, the U.S. government should devise rules, similar to those enacted by other governments like Germany, to prevent firms from inducing or exacerbating a supply shortage only to profit from it (Reese and Chance, 2021).
Determining which products should be included on the crisis-prices list for auctions will require an assessment of risk levels (where risk score is defined as the product of the medically essential score and the disruption likelihood level), as described in Chapter 5. Determining the likelihood of a disruption needs to take into consideration business continuity measures included in firms’ risk management plans. This focus should be on high-risk products. But risk alone is not enough to determine which products need increased capacity buffering. A list of products for inclusion on the crisis-prices list with stockpiling policies needs to be constructed. For example, a product for which stockpiling is relatively inexpensive might be best covered entirely by inventory and not included on the list at all. Another product for which stockpiling is expensive might need only enough inventory to cover the anticipated lead time to ramp up capacity.
BUT BUFFER FLEXIBILITY
As discussed in Chapter 5, flexibility makes inventory stockpiling and capacity buffering more effective. For example, resource sharing is a form of inventory flexibility that can significantly reduce the cost of achieving a given level of protection (Song and Song, 2009; Van Mieghem, 2007). Regional inventory stockpiles are inflexible if they can only be used to satisfy demand within the region. If cross-regional sharing is allowed, the stockpiles become flexible because they can satisfy demand in multiple regions. This type of flexibility is valuable when demand can be high in one region and low in another (i.e., regional demand is independent or negatively correlated). A concrete example during the COVID-19 pandemic was the case of ventilators, where there was considerable talk (but much less action) about shifting units between regions because surges of intensive care unit patients occurred at different times in different regions. On a global scale, sharing materials and products across regions is an important element of buffering the capacity of global medical product supply chains. Products with geographically diversified2 supply chains can be transshipped from low-demand regions to high-demand regions.
Another form of inventory flexibility is substitution. For example, if drug A can be substituted for drug B, then drug A can be used to satisfy two different types of demand. As such, a stockpile of drug A can serve as protection against shortages of both drugs A and B. However, unlike inventory sharing across regions, where the main costs are likely to be transportation and administration, the main cost in substitution could be a decline in clinical effectiveness. Therefore, finding ways to make substitute
___________________
2 Note that diversification elevates supply chain protection through both mitigation and preparedness measures prior to and during an event, respectively. Awareness of supply chain diversification is also a vital precursor to understanding the measures for promoting flexibility through diversification.
drugs and devices safely and effectively in advance of an emergency can enhance the flexibility of these products and hence their utility in protecting the public against medical supply shortages.
How to make inventory flexible so it can be used in resource sharing schemes depends on the situation. In some cases, such as the ventilator scenario, it might only require ensuring that the shared items are suitable for all participating health systems (i.e., standards are consistent) and articulating rules for sharing. In other cases, it may also require product modifications. For example, in nonmedical applications, manufacturers design appliances with universal plugs or adapters to make them compatible with the electrical standards of different countries so they can redirect supplies from one country to another to match demand. Because medical products are licensed independently in different countries, this type of flexibility to share supplies across borders may be limited. However, FDA can issue emergency use orders to allow use of medical products approved by other countries, as it did during the COVID-19 pandemic for KN95 masks from China.
As with inventory, flexibility in capacity can take various forms. One of the simplest is cross-training, which makes human capacity flexible so it can shift from producing one product or service to another. Cross-trained workers can be used in medical production facilities to facilitate ramping up capacity for a product with increased demand (e.g., due to an emergency or disruption).
Although labor flexibility can enable use of existing idle capacity (e.g., an unused night shift), further expansion of capacity will also require equipment/manufacturing flexibility. Flexible manufacturing, which makes use of computer and numerically controlled tools and other equipment that can perform multiple functions, along with cross-trained operators, is common in many industries. But in pharmaceutical manufacturing, new technologies such as additive manufacturing,3 modular manufacturing, single-use manufacturing, and continuous manufacturing4 are widely touted but still
___________________
3 Blockchain technology may facilitate additive manufacturing, an advanced manufacturing technique. Blockchain can verify the authenticity of additive manufacturing product designs when these designs are being shared by a disperse network of global manufacturers (Kurpjuweit et al., 2019). Moreover, blockchain ledgers increase the transparency of the supply chain in a way that meaningfully promotes quality. Quality and identity assessments, performance metrics, input materials, and product ownership can all be logged and tracked across the life cycle of the product—from starting material to delivery of the final product to health care centers (Bhaskar et al., 2020; Kurpjuweit et al., 2019). This technology, if applied correctly, can help reduce the entrance of fraudulent and substandard medical products into the market and protect consumers.
4 This method of drug manufacturing involves moving pharmaceuticals nonstop within the same facility, eliminating hold times between steps. Material is fed through an assembly line of fully integrated components. This method saves time, reduces the likelihood for human error, and can respond more nimbly to market changes. It can also run for a longer period of time, which may reduce the likelihood of drug shortages (FDA, 2017a).
sparsely used methods for increasing flexibility and scalability.5 As such, measures that promote the development and use of these advanced manufacturing technologies could help medical product facilities adjust production to meet needs during an emergency. In turn, the ability of such facilities to generate surge capacity more quickly will reduce the amount of inventory that will be needed in stockpiles as protection against a disruption. A 2021 National Academies report on innovation in pharmaceutical manufacturing recommended several actions that the Center for Drug Evaluation and Research (CDER) could implement to improve the uptake of innovative manufacturing technologies (NASEM, 2021b). These included increasing institutional awareness of and expertise in innovative technologies, new mechanisms to approve innovations to existing products, and expanded opportunities for external engagement on the issue.
A number of public–private partnerships have been established to support the development of advanced manufacturing technologies and address their barriers to uptake (FDA, 2021). Manufacturing USA and America Makes are two examples of public–private partnerships that bring together academia, industry, and government to accelerate the innovation and uptake of advanced manufacturing technologies.6, 7 FDA has also taken several steps to promote the implementation of advanced manufacturing. These steps include funding extramural research projects in various aspects of advanced manufacturing, issuing grants to academic institutions and nonprofits to study advanced manufacturing and recommend improvements, and establishing the Additive Manufacturing of Medical Products research facility to improve FDA’s technical and regulatory infrastructure. FDA also established the Emerging Technology Program to facilitate industry’s adoption of advanced manufacturing, allowing industry to work collaboratively with regulators in addressing potential technical and regulatory barriers (FDA, 2019). In an effort to lower the regulatory barriers that manufacturers face when updating production processes, facilities, and equipment, FDA updated its guidance on the required information on postapproval manufacturing changes in annual reports for drug and biologics in 2014 and 2017, respectively, so changes with minor risk to product quality could be made without prior authorization (FDA, 2014, 2017b).
___________________
5 Modular manufacturing is done in a large area with no fixed equipment, allowing for a facility to be broken down into functional building blocks or modules in order to simplify, standardize, verify, and reuse designs as well as actual modules in different implementations (Riley, 2016). Single-use manufacturing uses disposable tools to reduce the risk of product contamination and improve operational efficiency by eliminating the need to sterilize instruments between batches (Parrish, 2018). Continuous manufacturing is done from end to end on a single, uninterrupted production line (Siemens, 2021).
6 For more information, see https://www.manufacturingusa.com/pages/how-we-work (accessed October 20, 2021).
7 For more information, see https://www.americamakes.us/ (accessed October 20, 2021).
Another flexible use of capacity is “pop-up capacity,” in which new players enter a market to address an emergency shortage. Additionally, pop-up capacity can be used for more routine but not necessarily constant public health emergencies. For instance, during flu season, distilleries in hard-hit areas could be incentivized to produce hand sanitizer, or local businesses accustomed to serving a large volume of customers daily, like a bank or fast-food restaurant, can partner with the local health department to host vaccine clinics (CDPH, 2021; Kaur, 2020).
CONTINGENCY PLANNING AND READINESS
As described in Chapter 5, contingency planning involves mapping out a course of action for responding to a specific scenario, while readiness involves actions that improve the ability to respond to a category of scenarios once the details of the event become known. In contrast to the physical buffers of inventory and capacity, contingency planning and readiness are virtual protections. But they are important parts of the preparedness picture nonetheless because they do not incur the ongoing costs associated with physical assets. As such, they are essential for addressing rare events for which these costs cannot be justified.
Contingency planning can address many factors that influence supply chain resilience, including inventory and capacity. An illustrative example from the COVID-19 pandemic is ventilator production. In April 2020, the DPA was invoked to compel Ford, General Motors, Medtronic, and others to produce ventilators, although most of them had already begun ramping up production (Clark, 2020; Dzhanova, 2020; Vazquez, 2020). Without advance preparation, the auto companies were only able to produce simpler transport ventilators, rather than the intensive care unit ventilators doctors preferred (Bergin, 2020). Furthermore, the on-the-fly supply chain coordination resulted in shortages that led to delays. Despite the good intentions and heroic efforts by medical device and other manufacturers, it seems that they could have ramped up ventilator production more quickly and accurately with some advance planning in place. Additionally, contingency planning and readiness measures can be combined with physical buffering to create capacity on an as-needed basis that could be activated in times of emergency. One approach is “warm basing.” This transitional state between the physical and virtual preparedness measures allows for a production facility to remain in a state of partial readiness, with either the physical supplies or trained staff ready to go when the need arises.
A contingency plan that specifies the triggers, mechanisms, and responsibilities of various actors for implementing resource sharing would be one way to promote inventory flexibility. Examples of contingency planning include crisis standards of care (CSC) planning for health systems. Resources on CSC and substitution can be found in Box 8-4.
Readiness measures can be thought of as organizational preparations at multiple levels (i.e., top-down, bottom-up) allowing for flexibility, dynamic control, and adaptive management during disruptive events (Ivanov and Sokolov, 2012). For these measures to work, partners and stakeholders must be preemptively identified and prepared to act when needed. This is critical to supply chain preparedness.
RECOMMENDATIONS
The COVID-19 crisis served as a stark reminder that holding inventory in stockpiles is more complicated in practice than in theory. In real-world settings, problems with forecasting demand, monitoring stock levels, rotating stock to prevent expiration, and other practical details can prevent inventory stockpiles from providing the intended level of protection in an emergency. Furthermore, as described above, capacity buffering can be a cost-effective alternative or supplement to inventory as protection against shortages. Finally, contingency plans and readiness activities can provide additional levels of protection for rare events that are too costly to buffer with physical inventory and capacity.
Therefore, the committee recommends action related to both inventory stockpiling and capacity buffering. Stockpiling is already part of the national preparedness strategy, primarily in the form of the SNS. Recommendation 4 (Stockpiling) is substantially about refining and improving the ways inventory is held as protection against medical product shortages. Recommenda-
tion 5 (Capacity Buffering) complements these steps by advocating measures to develop capacity that can be brought online to supplement inventory stockpiles as needed. Such capacity buffering could be the result of direct contracts, such as advance arrangements to have specific manufacturers provide emergency capacity, as the auto manufacturers did during the pandemic by assembling ventilators. Capacity buffers could also be the result of a list of guaranteed crisis prices that the government would pay for certain products under specified conditions. This would provide incentives for firms to find creative ways to deliver pop-up capacity during emergencies. Finally, the federal government should fund research on advanced manufacturing technologies that make it more economical to locally produce goods and easier to scale up capacity quickly. Both of these would make capacity buffering a more viable preparedness option and hence would facilitate a partial shift away from expensive inventory and toward cheaper capacity.
As noted earlier, on-shoring is often promoted as a means for building medical supply chain resilience via the argument that the more medical products a country produces domestically, the more control it has of supplies during an emergency. By reducing labor costs and promoting flexibility and scalability, the advanced manufacturing technologies advocated in Recommendation 5 (Capacity Buffering) may make on-shoring a good option for some products. Indeed, if technological capabilities permit efficient, small-scale production, then dispersed production in the country of consumption will be the natural market outcome. However, where this is not the case, on-shoring will impose a significant price penalty on an ongoing basis in return for a potentially small advantage during rare emergencies. If many high-income countries pursue on-shoring strategies for many medical products, considerable resources will be spent that could be put to better use addressing other problems. Therefore, on-shoring should be part of an integrated resilience strategy, rather than the option of choice.
Recommendation 4 (Stockpiling). The Office of the Assistant Secretary for Preparedness and Response should take steps to develop strategies to modernize and optimize inventory stockpiling management for the Strategic National Stockpile (SNS) and beyond to respond to medical product shortages at the national and regional levels. These steps include
- Consider the recommendations provided in National Academies report, Ensuring the Effectiveness of the Public Health Emergency Medical Countermeasures Enterprise, particularly those that focus on adopting a systems approach to managing the SNS.
- Analyze risk levels of supply chain critical medical products and the viability of other response strategies (e.g., capacity buffering).
- Examine key inventory stockpiling process considerations such as
- Inventory system visibility.
-
- Mechanisms and thresholds for the use, sharing, deployment, distribution, and allocation of stockpiled inventory in response to shortages (triggered by both emergencies and routine use) and to prevent product expiration.
- The risks and benefits of stockpiling ingredients or components as opposed to finished goods.
- The risks and benefits of just-in-time production or inventories in larger reserves.
- Funding levels to meet the required inventory levels and management tasks for the regional and national stockpiles as well as incentives for stakeholders for holding inventory.
- Convene regional and local working groups composed of emergency health planners, clinicians, health care systems, and public health agencies, among others, to discuss and inform expectations for federal SNS support; national and regional stockpile content and pre-deployment positioning; regional supply capabilities and expectations; and roles and responsibilities for key stakeholders.
Recommendation 5 (Capacity Buffering). The Office of the Assistant Secretary for Preparedness and Response (ASPR) and the U.S. Food and Drug Administration (FDA) should take steps to cultivate capacity buffering for supply chain critical medical products where such capacity is a cost-effective complement to stockpiling and as protection against long-lasting supply disruptions or demand surges. These steps include
- Government investments in capacity buffering should be aimed at all stages of the supply chain and at major public health emergencies.
- ASPR and FDA should develop and routinely maintain a crisis-prices list of supply chain critical medical products (i.e., medically essential and supply chain vulnerable) and identify which capacity measure is a practical supplement to the stockpiled inventory. Further, ASPR should develop and manage a database to coordinate inventory stockpiling and capacity buffering policies regarding the crisis-prices list.
- ASPR and FDA should fund research and development for both advanced pharmaceutical and advanced medical technology manufacturing techniques to help make on-shoring more cost-competitive. By making capacity more easily scalable, these technologies would enable firms to respond to the need for capacity buffers more quickly and cost-effectively.
- ASPR and FDA should create public–private partnerships and support and fund capital and staff investments jointly, to imple
- ment these advanced manufacturing approaches to ensure production capacity. These partnerships will provide a great depth and breadth of expertise and can be leveraged for new economic incentives and regulatory clarity.
- ASPR should be responsible for anticipating and assessing public health emergency demand surge for supply chain critical medical products. They should clarify production capacity, identify vulnerabilities in supply chains, and engage producers in developing plans for surge response.
REFERENCES
AMA (American Medical Association). 2001. Pharmaceutical expiration dates. Paper read at American Medical Association Annual Meeting, June 17-21, Chicago, IL.
Amazon. 2021. Fulfillment by Amazon. https://sell.amazon.com/fulfillment-by-amazon (accessed November 1, 2021).
ASPR_TRACIE (Assistant Secretary for Preparedness and Response_Technical Resources, Assistance Center, and Information Exchange). 2022. Topic collection: COVID-19 crisis standards of care resources. https://asprtracie.hhs.gov/technical-resources/112/covid-19-crisis-standards-of-care-resources/99#plans-tools-and-templates (accessed January 20, 2022).
Bergin, T. 2020. The U.S. has spent billions stockpiling ventilators, but many won’t save critically ill COVID-19 patients. Reuters, December 2. https://www.reuters.com/article/us-health-coronavirus-ventilators-insigh/the-u-s-has-spent-billions-stockpiling-ventilators-but-many-wont-save-critically-ill-covid-19-patients-idUSKBN28C1N6 (accessed October 14, 2021).
Bhaskar, S., J. Tan, M. L. Bogers, T. Minssen, H. Badaruddin, S. Israeli-Korn, and H. Chesbrough. 2020. At the epicenter of COVID-19: The tragic failure of the global supply chain for medical supplies. Frontiers in Public Health 8:821.
CDPH (California Department of Public Health). 2021. California partners with McDdonald’s franchisees across the state for COVID-19 vaccine pop-up clinics. Sacramento, CA. https://www.cdph.ca.gov/Programs/OPA/Pages/NR21-198.aspx (accessed November 3, 2021).
CFI (Corporate Finance Institute). 2021. Assemble-to-order. CFI. https://corporatefinanceinstitute.com/resources/knowledge/strategy/assemble-to-order/#:~:text=Dell%20Technologies%20follows%20an%20assemble-to-order%20business%20model%20for,the%20PC%20is%20assembled%20and%20shipped%20for%20delivery (accessed December 8, 2021).
Clark, D. 2020. Trump invokes Defense Production Act to force GM to make ventilators for coronavirus fight. NBC, March 27. https://www.nbcnews.com/politics/donald-trump/trump-invokes-defense-production-act-force-gm-make-ventilators-coronavirus-n1170746 (accessed December 8, 2021).
DoD (U.S. Department of Defense), HHS (U.S. Department of Health and Human Services), DHS (U.S. Department of Homeland Security), and VA (U.S. Department of Veterans Affairs). 2021. National strategy for a resilient public health supply chain, edited by Department of Health and Human Services, Department of Defense, Department of Homeland Security, Department of Commerce, Department of State, Department of Veterans Affairs, and The White House Office of the COVID-19 Response. Washington, DC. https://www.phe.gov/Preparedness/legal/Documents/National-Strategy-for-Resilient-Public-Health-Supply-Chain.pdf (accessed October 29, 2021).
Dzhanova, Y. 2020. Trump compelled these companies to make critical supplies, but most of them were already doing it. CNBC, April 3. https://www.cnbc.com/2020/04/03/coronavirus-trump-used-defense-production-act-on-these-companies-so-far.html (accessed December 8, 2021).
FDA (U.S. Food and Drug Administration). 2014. Guidance for industry: CMC postapproval manufacturing changes to be documented in annual reports. https://www.fda.gov/media/79182/download (accessed October 14, 2021).
FDA. 2017a. Modernizing the way drugs are made: A transition to continuous manufacturing. https://www.fda.gov/drugs/news-events-human-drugs/modernizing-way-drugs-are-madetransition-continuous-manufacturing (accessed October 18, 2021).
FDA. 2017b. Guidance for industry: CMC postapproval manufacturing changes for specified biological products to be documented in annual reports. https://www.fda.gov/media/106935/download (accessed October 14, 2021).
FDA. 2019. Emerging technology program. https://www.fda.gov/about-fda/center-drug-evaluation-and-research-cder/emerging-technology-program (accessed October 20, 2021).
FDA. 2021. Advanced manufacturing. https://www.fda.gov/emergency-preparedness-and-response/mcm-issues/advanced-manufacturing (accessed October 19, 2021).
FEMA (Federal Emergency Management Agency). 2020. Applying the Defense Production Act. https://www.fema.gov/press-release/20210420/applying-defense-production-act (accessed December 8, 2021).
Fitzpatrick, S. 2020. Why the Strategic National Stockpile isn’t meant to solve a crisis like coronavirus. NBC, March 28. https://www.nbcnews.com/health/health-care/why-strategic-national-stockpile-isn-t-meant-solve-crisis-coronavirus-n1170376 (accessed January 20, 2022).
Greenspan, R. 2019. Walmart’s inventory management. Panmore Institute. http://panmore.com/walmart-inventory-management (accessed December 8, 2021).
Gruley, B., and R. Clough. 2020. How 3M plans to make more than a billion masks by end of year. https://www.bloomberg.com/news/features/2020-03-25/3m-doubled-production-of-n95-face-masks-to-fight-coronavirus?utm_campaign=news&utm_medium=bd&utm_source=applenews (accessed November 4, 2021).
HIDA (Health Industry Distributors Association). 2020. Building a more robust supply chain: A public-private framework to create a pandemic response infrastructure. https://www.hida.org/distribution/advocacy/COVID19/White-Paper-Building-A-More-Robust-Supply-Chain.aspx?utm_source=blueprint-page&utm_medium=web&utm_campaign=medical-supplies-last-mile (accessed December 16, 2021).
Huang, L., J.-S. Song, and J. Tong. 2016. Supply chain planning for random demand surges: Reactive capacity and safety stock. Manufacturing & Service Operations Management 18(4):509-524.
IOM (Institute of Medicine). 2009. Guidence for establishing crisis standards of care for use in disaster situations: A letter report. Washington, DC: The National Academies Press.
Ivanov, D., and B. Sokolov. 2012. Structure dynamics control approach to supply chain planning and adaptation. International Journal of Production Research 50(21):6133-6149.
Kaur, H. 2020. Distilleries are making hand sanitizer with their in-house alcohol and giving it out for free to combat coronavirus. CNN, March 19. https://edition.cnn.com/2020/03/16/us/distilleries-hand-sanitizer-coronavirus-trnd/index.html (accessed November 3, 2021).
Khan, S. R., R. Kona, P. J. Faustino, A. Gupta, J. S. Taylor, D. A. Porter, and M. Khan. 2014. United States Food and Drug Administration and Department of Defense shelf-life extension program of pharmaceutical products: Progress and promise. Journal of Pharmaceutical Sciences 103(5):1331-1336.
Klein, P. 2020. America’s medical supply crisis (PBS Frontline Season 2020: Ep. 6). https://www.pbs.org/wgbh/frontline/film/americas-medical-supply-crisis/ (accessed November 3, 2021).
Kurpjuweit, S., C. Schmidt, M. Klöckner, and S. Wagner. 2019. Blockchain in additive manufacturing and its impact on supply chains. Journal of Business Logistics 42.
Lakra, P., and P. Bedi. 2014. Topic: The comparative study of consignment and vendor managed inventory with special reference of cost structure. International Journal of Advancements in Research & Technology 3(3):142-146.
Lieb, D. A., and C. Dil. 2020. Review: State stockpiles were depleted before the virus. The Mercury News, April 23. https://www.mercurynews.com/2020/04/23/review-state-stockpiles-were-depleted-before-the-virus/ (accessed October 14, 2021).
Lyon, R. C., J. S. Taylor, D. A. Porter, H. R. Prasanna, and A. S. Hussain. 2006. Stability profiles of drug products extended beyond labeled expiration dates. Journal of Pharmaceutical Sciences 95(7):1549-1560.
Nahmias, S., and T. L. Olsen. 2021. Production and operations analytics. 8th ed. Long Grove, IL: Waveland Press.
NAM (National Academy of Medicine). 2022. Crisis standards of care for the COVID-19 pandemic. https://nam.edu/112920-crisis-standards-of-care-resources/ (accessed January 20, 2022).
NASEM (National Academies of Science, Engineering, and Medicine). 2021a. Ensuring an effective public health emergency medical countermeasures enterprise. Washington, DC: The National Academies Press.
NASEM. 2021b. Innovations in pharmaceutical manufacturing on the horizon: Technical challenges, regulatory issues, and recommendations. Washington, DC: The National Academies Press.
Parrish, M. 2018. Product focus: Single-use technologies. Pharma Manufacturing. https://www.pharmamanufacturing.com/articles/2018/product-focus-single-use-technologies (accessed November 2, 2021).
Quinn, M. 2020. What you need to know about the strategic national stockpile. CBS, April 7. https://www.cbsnews.com/news/q-a-with-greg-burel-former-director-of-the-strategic-national-stockpile/ (accessed October 14, 2021).
Reese, U., and C. Chance. 2021. Pricing and reimbursement laws and regulations: Germany. In Global Legal Insights (GLI): Pricing and Reimbursement 2021. 4th ed., edited by G. Castle. London, UK: Covington & Burling LLP. https://www.globallegalinsights.com/practice-areas/pricing-and-reimbursement-laws-and-regulations/germany (accessed January 11, 2022).
Reinhard, B., and E. Brown. 2020. Face masks in national stockpile have not been substantially replenished since 2009. The Washington Post, March 10. https://www.washingtonpost.com/investigations/face-masks-in-national-stockpile-have-not-been-substantially-replenished-since-2009/2020/03/10/57e57316-60c9-11ea-8baf-519cedb6ccd9_story.html (accessed November 3, 2021).
Riley, S. 2016. Modular manufacturing. Pharmaceutical Processing World. https://www.pharmaceuticalprocessingworld.com/modular-manufacturing (accessed November 2, 2021).
Rule, T. 2020. Toward a more strategic national stockpile. Europe PMC, SSRN. doi: 10.2139/ssrn.3662799.
Scott, R. E. 2020. Defense Production Act urgently needed for critical medical gear. The Hill, March 26. https://thehill.com/opinion/healthcare/489430-defense-production-act-urgently-needed-for-critical-medical-gear#:~:text=to%20use%20the%20Defense%20Production%20Act%20%28DPA%29%20to,of%20medical%20supplies%20is%20a%20job%20for%20governors (accessed December 8, 2021).
Siemens. 2021. Continuous manufacturing. https://new.siemens.com/global/en/markets/pharma-industry/continuous-manufacturing.html (accessed November 2, 2021).
Song, H. U. A., and Y.-F. Song. 2009. Impact of inventory management flexibility on service flexibility and performance: Evidence from mainland Chinese firms. Transportation Journal 48(3):7-19.
Sumrit, D. 2020. Supplier selection for vendor-managed inventory in healthcare using fuzzy multi-criteria decision-making approach. Decision Science Letters 9(2):233-256.
Van Mieghem, J. A. 2007. Risk mitigation in newsvendor networks: Resource diversification, flexibility, sharing, and hedging. Management Science 53(8):1269-1288.
Vazquez, M. 2020. Trump invokes Defense Production Act for ventilator equipment and N95 masks. CNN, April 2. https://www.cnn.com/2020/04/02/politics/defense-production-act-ventilator-supplies/index.html (accessed December 8, 2021).
This page intentionally left blank.
























