
2
Understanding Medical Product Supply Chains
Medical product supply chains are complex, global systems that involve people, processes, technologies, and policies. This chapter describes the ways different categories of medical product supply chains are structured and concludes with a brief overview of the various economic and policy spaces in which they operate. Medical product supply chains are designed for efficiency and cost, and do not always consider transparency or resilience. This can have negative consequences for public health and national security as evidenced by the ongoing COVID-19 pandemic as well as persistent medical product shortages that take place every year in the United States. To identify policies for making medical product supply chains more resilient, understanding their characteristics is essential. This background chapter is critical to understanding how to ensure a resilient supply chain as different products, different markets, and different risk profiles require different interventions. The key challenge will be to match interventions to products in a cost-effective manner.
OVERVIEW OF THE MEDICAL PRODUCT SUPPLY CHAIN SYSTEM
This section focuses primarily on the supply chains for (1) drugs, particularly active pharmaceutical ingredients (APIs) and finished dosage form
(FDF) drug products, and (2) medical devices.1 While the general structure of these products’ supply chains is similar (i.e., spanning the path from raw materials to manufacturers to distributor to end user), the details of each are as varied as the products themselves, warranting separate discussions for each. However, the framework presented in Chapter 5 is still flexible enough to be adapted to the assessment and remediation of individual supply chains. What follows will provide a background for how different types of medical product supply chains operate, the economic incentives that promote and support these structures, and finally, the current challenges each presents to building more resilient supply chains.
General Structure of Medical Product Supply Chains
As discussed in Chapter 1, owing to the complexity and interconnectedness of medical product supply chains, there are a variety of stakeholders involved in supply chain operations, including government agencies, raw material suppliers, manufacturers, distributors, group purchasing organizations, health systems, providers, and patients. These stakeholders make the decisions that enable medical product supply chains to facilitate the flow of medical products from raw material or component suppliers (e.g., makers of ingredients, subassemblies) to producers (e.g., final assembly plants, fill-and-finish facilities), to distributors (e.g., wholesalers), to providers (e.g., health systems, pharmacies, retailers), and finally, to patients. To coordinate these steps, the supply chain must transmit demand information upstream to use as guidance for production and transport decisions for the products downstream. An efficient supply chain matches supply with demand in a responsive and cost-efficient manner. As currently structured, medical product supply chains are typically inelastic, meaning that there is demand for products regardless of price (Haninger et al., 2011), leading to a financially imbalanced supply-and-demand setup. See Figure 2-1 for a graphical representation of a typical medical product supply chain under normal well-functioning conditions.
___________________
1 As mentioned in Chapter 1, this report does not focus in detail on supply chains for biologics or vaccines given the distinct features in their supply chains. However, as some biologics and vaccines are high-margin, patent-protected pharmaceuticals while others are not, the discussion of profit margins and incentives between originator and generic drugs is still applicable to these medical products. Furthermore, four new reports from the National Academy of Medicine focus on how to prepare for seasonal and pandemic influenza through lessons learned from COVID-19—with one report in particular focusing on globally resilient supply chains for pandemic and seasonal influenza vaccines. These reports can be accessed here: https://nam.edu/four-new-reports-from-the-national-academy-of-medicine-focus-onhow-to-prepare-for-seasonal-and-pandemic-influenza-through-lessons-learned-from-covid-19.
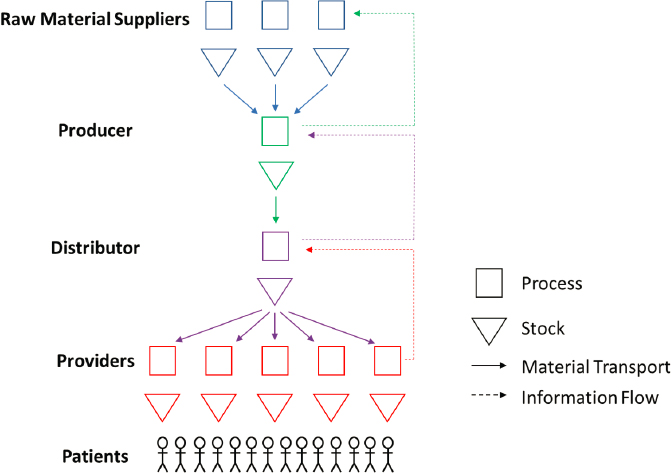
SOURCE: Adapted from NASEM, 2020.
Pharmaceuticals (Originator and Generic)
Pharmaceutical manufacturing starts with the acquisition of raw materials, such as solvents, reagents, and other chemicals. These are combined by a series of reactions and then purified by a process designed to result in the desired APIs, or API intermediates (FDA, 2016). The APIs are then added to various excipients, shaped into a particular configuration, such as a tablet, capsule, or injectable, and apportioned into a particular dose to produce the drug product (FDA, 2012, 2016). Depending on the manufacturer, this process may occur in the same facility that manufactured the APIs or it may be outsourced to other drug manufacturing facilities. Regardless of where FDF production occurs, the timeframe for production, from raw materials to FDF, varies widely (from days to months) as many quality assurance and quality control tests are required before the drug products are deemed safe for distribution (FDA, 2016). To keep production efficiency high, produce less waste, and reduce inventory costs, raw materials are produced only as ordered and many drug manufacturers use just-in-time inventory management and receive the raw materials or APIs only as they need them (Dias et al., 2012; Stevens, 2020; The White House, 2021).
Pharmaceutical manufacturing can additionally be thought of as producing either originator or generic drugs. A generic drug is a medication developed to be the same as an already marketed brand-name drug in dosage
form, safety, strength, route of administration, quality, performance characteristics, and intended use so the generic medicine works in the same way and provides the same clinical benefit as the brand-name medicine (FDA, 2021c). The manufacturing processes for originator and generic drugs are virtually identical, with the supply chains for each differing mainly by location, meaning the two kinds of drugs only differ where they are made or packaged, not how they are made. In the United States, off-patent, generic drugs are the most commonly used prescription pharmaceuticals and are the most frequently dispensed retail prescriptions (Berndt et al., 2017), accounting for 90 percent of all prescriptions filled and 20 percent of all prescription drug spending (AAM, 2021).
The last 3 decades have seen pharmaceutical manufacturing become a global enterprise (see Chapter 3 for further detail). In the United States, this shift toward relying on foreign manufacturing has been motivated mainly by the desire to control costs. This pressure to keep profits high deincentivizes generic drug manufacturers from using the highest-quality materials for production as these come at premium costs (Khan, 2020). Taken together, U.S. pharmaceutical companies were monetarily incentivized to either move their manufacturing offshore or rely on foreign manufacturers for their materials or both.
Medical Devices—Simple (Class I) and Complex (Class II/III)
Medical devices are defined by the U.S. Food and Drug Administration (FDA) as any object or component used in the diagnosis, treatment, prevention, or cure of medical conditions or diseases, or that affects body structure or function through means other than chemical or metabolic reaction in humans or animals (CDRH, 2018).2 This broad definition includes a huge range of products, ranging from tongue depressors to computerized tomography scanners. Unlike pharmaceutical manufacturing, medical device manufacturing is highly varied depending on the product, and a one-process-flow description is not feasible. Furthermore, due to the large array of equipment classified as medical devices, FDA has no single standard to which a specific device must be manufactured. Instead, FDA created a standards guide that all manufacturers must follow, which includes requiring manufactures to develop comprehensive procedures within the FDA framework to produce devices that meet approved safety standards (CDRH, 2018). Approved medical devices are then categorized into one of three classes by these safety standards, according to the safety risks they pose.
___________________
2 The statutory language from the Food, Drug, and Cosmetic Act (FD&C Act) 513(a) specifically distinguishes between the classes by defining medical devices as “as any instrument, apparatus, implement, machine, contrivance, implant, in vitro reagent, or other similar article (including a component of such article) intended for use in the diagnosis, cure, mitigation, treatment, or prevention or disease or other conditions, or intended to affect any structure or function of the body, that does not function primarily through chemical or metabolic reaction.”
Class I medical devices present minimal potential for harm to the user and are often simpler in design than Classes II and III and are considered simple-design devices. Class II medical devices present moderate risk of harm to the patient or user. Most FDA-regulated medical devices are considered Class II (FDA, 2017). Class III medical devices are highly complex devices that also present a high safety risk to the patient or user. These devices usually sustain or support life, are implanted, or present potentially unreasonable risk of illness or injury. These represent 10 percent of medical devices regulated by FDA (FDA, 2017). As devices in Classes II and III are more complex in design than Class I devices, the medical devices that fall into Classes II and III are considered complex-design devices.
These product classifications are useful in protecting patient safety. But they are less helpful in assessing risks or building resilience in supply chains. One reason is that device complexity—simple (Class I) or complex (Class II or III)—does not always correlate with supply chain complexity. There is little similarity between where the devices are made/packaged and how they are made. Furthermore, the complexity of the supply chain for a medical device is not necessarily reflective of the complexity of the design of the device itself and few standards exist for interchangeable parts (e.g., ventilator tubing).3 For instance, a simple, small adhesive bandage has a complex supply chain for production. Band-Aids, simple medical devices, have four components, each with its own raw materials sourcing and manufacturing processes (Lin et al., 2016). Production of the finished product requires the raw materials for each component (plastic strip, absorbent pad, adhesive, and release sheets), and therefore can be halted by the disruption of any of these supplies. Therefore, although supply chains are generally broader (more components) and deeper (more tiers) for complex products that contain more parts than for simple products with fewer parts, this is not always the case. Therefore, the simple/complex classifications will be used in the report as an approximation of supply chain complexity, recognizing that individual characteristics must be considered when assessing or remediating supply risks for specific products. All other things being equal, complex supply chains present greater risks of disruption.
DIFFERENCES IN SUPPLY CHAIN ECONOMICS BY PRODUCT CATEGORY
Supply chain complexity is not the only factor that affects the likelihood of a medical product supply disruption. Management decisions are also important. In low-margin products, which include many but not all generic drugs and simple devices, there is a heavy emphasis on cost control because of price pressures and profitability concerns. Consequently, many drug manufacturers rely on lean practices, such as just-in-time inventory
___________________
3 21 U.S.C. 807.81, when a premarket notification submission is required (amended December 28, 2007).
management, receiving raw materials or APIs only as they need them, to keep production efficiency high, produce less waste, and reduce inventory costs (Dias et al., 2012; Stevens, 2020). However, this makes supply chains more vulnerable to disruption because there is less protective inventory in the system. Although supply chain resilience and supply continuity may also be important considerations, there is variability in the extent to which the industry’s concerns about continuity align with the concerns of customers or society at large. Moreover, the nature of the supply chain economics that shape decisions about investment in resilience and continuity differs by product category.
Producers of low-margin products, like generic drugs and simple medical devices, may have only a modest incentive to ensure supply continuity, even though patients and society may have high demand for and be dependent upon the availability of these products. For companies in the medical product industry—particularly those producing low-volume and low-margin products—lack of market insights about future demand can deter investment to expand manufacturing capacity to prepare for potential supply chain disruption (The PEW Charitable Trusts and ISPE, 2017). High costs can dissuade these same producers from upgrading facilities to comply with FDA current good manufacturing practice requirements, elevating the risk of quality issues that can precipitate shortages (The PEW Charitable Trusts and ISPE, 2017). Finally, cost pressures incentivize companies to shift the manufacturing of low-margin products to lower-cost countries, making quality oversight and assurance more difficult (The PEW Charitable Trusts and ISPE, 2017). This has led to shortages of low-margin products caused by issues at offshore manufacturing facilities. For all of these reasons, low-margin products—and generic drugs in particular—have been much more prone to supply disruptions than products with higher margins have been. It is possible to build just-in-case inventory or other business continuity protections into the supply chains for these products, but when margins are low, the returns on such investments do not justify the costs.
In contrast, for high-margin products—such as originator drugs and complex medical devices—producers are typically incentivized to ensure the continuity of their supply streams because this also protects their valuable revenue streams and market shares. For instance, when a disruption occurs, a company that already has market power will be more likely to maintain its leadership role if it is resilient enough to respond effectively and recover rapidly. Companies in this type of position can justify investment in strengthening their supply chain’s resilience because their strong market role is linked to high-profit margins. Furthermore, companies that avoid disruptions may attract less attention from regulatory authorities (Sheffi and Rice, 2005). However, these incentives are most powerful when markets are competitive. If a producer has a monopoly on a product with few viable substitutes, it may still have an incentive to invest in business
continuity measures to protect its revenue stream, but it will not have the added incentive to protect its market share.
The consequences of these differences in the supply chains of high- and low-margin products become particularly acute in emergencies, because they represent rare situations. From a financial perspective, it is difficult for companies to justify sufficient investment to ensure supply chain resilience and supply continuity in the event of a low-frequency but potentially high-consequence event, such as a large-scale natural or man-made disaster. This is a challenge for producers of products of all margins, but even more so for producers of low-margin products. As a result, rare events can pose serious risks to public health security if they disrupt the supply chains for products that are essential to health but are produced by industries that have limited financial incentives to ensure supply continuity.
Given these differences, an ideal starting point for identifying medical products at risk of shortages, due to capacity failures during normal times or lack of surge capacity to cope with demand surges during emergencies, is to focus on low-margin products. This generally means generic drugs and simple devices. But this is only an approximation, since some generic drugs and simple devices can have high margins. Also, some higher-margin products can have other risk factors, such as a high level of supply chain complexity or a low level of market diversification. Therefore, although the low-margin product categories will be used as partial predictors of supply risk, it also must be noted that there remains the need for more work to highlight medical products most vulnerable to shortages. The existing categories have been designed with quality and safety in mind. New categories can be developed to adapt or extend these to consider reliability. Alternatively, analytic techniques such as machine learning of past shortages can be used to identify product characteristics that predict shortages during normal conditions. Such analytic techniques will be less useful for predicting shortages in major disasters because the rarity of such events limits the data that are available. Therefore, to focus future medical product supply chain resilience efforts, new categories will likely be developed and analytics tools will be used for predicting risks.
POLICY UNDERPINNINGS OF U.S. MEDICAL PRODUCT SUPPLY CHAINS
The current U.S. policy landscape, and those specific to the ongoing COVID-19 pandemic, have significant implications for U.S. medical product supply chains. This section highlights the policies most relevant to medical product supply chains.4
___________________
4 For a summary of existing U.S. legislation governing medical product supply chains and relevant legislation introduced in the 116th Congress see Appendixes A and B, respectively, at https://sgp.fas.org/crs/misc/R46507.pdf.
Federal Food, Drug, and Cosmetic Act
FDA is responsible for ensuring the safety and effectiveness of medical products marketed in the United States, and it plays a critical role in medical product supply chains. Box 2-1 details current tools at FDA’s disposal to address supply chain shortages. The FD&C Act contains a number of statutory requirements relevant to the medical product supply chain. The
FD&C Act has been amended on several occasions to address medical product shortages and other issues related to the medical product supply chain.
For instance, in 2012, the Food and Drug Administration Safety and Innovation Act (FDASIA) amended the FD&C Act, giving FDA new authorities to address global supply chain challenges.5 Among other things, FDASIA amended the FD&C Act to require that manufacturers notify FDA of discontinuance or interruption in the production of certain prescription drugs that are “life-saving, life-sustaining, or intended for use in the prevention or treatment of a debilitating disease or condition.”6 Additionally, FDASIA requires FDA to submit an annual report to Congress on drug shortages. The legislation called for the creation of a task force on drug shortages and set in motion a strategic plan to address drug shortages. FDASIA also introduced provisions aimed at improving the security of the drug supply chain, enumerating new requirements for facility registrations, risk-based facility inspections, and inspection reports. A 2021 study by Lee and colleagues empirically validated that this type of mandate-induced “operational transparency” was strongly associated with faster drug shortage recovery.
Below, some key aspects of this act are summarized in four categories—awareness, mitigation, preparedness, and response—in line with the committee’s medical product supply chains resilience framework as detailed in Chapter 5.
Awareness of Medical Product Shortages
In response to the increasing frequency and threat of medical product shortages, the U.S. Congress passed legislation to improve the federal government’s awareness of shortages. The FD&C Act requires that the secretary of the U.S. Department of Health and Human Services (HHS) publish a list of drugs and devices that are in shortage in the United States.7,8 The FDA defines a drug and/or device shortage as a period of time when the demand or projected demand for the product within the United States exceeds the supply of the product (CDER, 2018). The shortage lists are to include the name of the drug or device, the name of the manufacturer, the reason for the shortage, and the estimated duration of the shortage. Furthermore,
___________________
5 Food and Drug Administration Safety and Innovation Act, Public Law 112-144, 112th Congress (July 9, 2021).
6 Food and Drug Administration Safety and Innovation Act, Public Law 112-144, 112th Congress (July 9, 2021).
7 21 U.S.C. 356e, Drug shortage list (amended March 27, 2020).
8 21 U.S.C. 356j, Discontinuance or interruption in the production of medical devices (amended March 27, 2020).
the HHS secretary is required to submit an annual report to Congress on the number of manufacturers reporting new drug shortages, the number of ongoing drug shortages, and the actions FDA has taken to prevent or alleviate shortages.9
Crucial to the government’s ability to track product shortages is the requirement that manufacturers of drugs and devices that meet certain requirements,10,11 such as being life supporting, life sustaining, or for use during a public health emergency, must notify the HHS secretary if the product will be permanently discontinued or is experiencing a meaningful disruption in its supply. This could be the result of a manufacturing disruption, a demand surge, and/or a mismatch in the location of available supply and demand need. Drug manufacturers are required to disclose reasons and risk factors for the discontinuation or interruption, as well as the sources of the API if that is a reason or risk factor for the interruption. These statutes also give the HHS secretary the authority to distribute nonproprietary information regarding the discontinuance or interruption to relevant groups, including patient organizations, health care providers, and prescribers. Of note, however, is that from 2014 to 2021, FDA has sent noncompliance letters to six different manufacturers who have failed to adequately notify of a discontinuance or interruption (FDA, 2021a), although manufacturers are not subject to fines or other disciplinary actions in cases of noncompliance.
During the COVID-19 pandemic, the FD&C Act was again amended under the Coronavirus Aid, Relief, and Economic Security (CARES) Act to provide more open communication and reporting between manufacturers and HHS. This is covered in more detail in the CARES Act section below.
Mitigation of Medical Product Shortages
In addition to measures to detect and track medical product shortages, the FD&C Act contains provisions to prevent shortages and blunt their effects. One such provision established a drug task force, which was charged with developing and implementing a strategic plan to prevent and mitigate shortages.12 The legislation also calls for the strategic plan to include plans for
___________________
9 21 U.S.C. 356c-1, Annual reporting on drug shortages (amended December 13, 2016).
10 21 U.S.C. 356c, Discontinuance or interruption in the production of life-saving drugs (amended March 27, 2020).
11 Food and Drug Administration Safety and Innovation Act, Public Law 112-144, 112th Congress (July 9, 2021).
12 21 U.S.C. 356d, Coordination; task force and strategic plan (amended July 9, 2012).
- interagency and intra-agency coordination,
- ensuring the consideration of drug shortages in regulatory actions,
- effective communication with external stakeholders,
- the effect of shortages on research and clinical trials, and
- examining the establishment of a qualified manufacturing partner program—a program that would use manufacturers with the capability and capacity to rapidly produce and supply drugs undergoing shortages.
In 2018, the FDA commissioner established the interagency Drug Shortages Task Force to focus more on drug shortages, to identify reasons why some shortages remain a persistent challenge, and to look for holistic solutions to addressing the underlying causes of the shortages (FDA, 2018). This task force produced a report on the root causes and potential solutions to drug shortages in 2019,13 highlighting that on average, the number of ongoing drug shortages has been increasing and are lasting longer (FDA Drug Shortages Task Force, 2020). The task force also promoted several legislative proposals and FDA initiatives to help prevent and mitigate shortages, including improved data sharing and risk management plans.
Preparedness for Medical Product Shortages
The FD&C Act also gives the HHS secretary the authority to prioritize and expedite the review of drug or device applications,14,15 or inspection of the facilities that produce them, when there is or is likely to be a shortage in which such an expedited review or inspection could mitigate or prevent the shortage. The relevant statutes create a system of accountability in requiring that FDA’s annual report to Congress include information on the number of expedited reviews and inspections.16 The annual reports also must contain the names of manufacturers that failed to notify the HHS secretary of interruptions or discontinuations, descriptions of the coordination between FDA and the Drug Enforcement Administration (DEA), and identify instances in which FDA exercised regulatory flexibility to prevent or alleviate shortages.
A provision of the FD&C Act also relegates responsibility to manufacturers of FDF drugs, APIs, or any associated medical device used for
___________________
13 For more information and to read the full report, see https://www.fda.gov/media/131130/download (accessed August 19, 2021).
14 Food and Drug Administration Safety and Innovation Act, Public Law 112-144, 112th Congress (July 9, 2021).
15 For a summary of existing U.S. legislation governing the medical product supply chain and relevant legislation introduced in the 116th Congress see Appendixes A and B, respectively, at https://sgp.fas.org/crs/misc/R46507.pdf.
16 21 U.S.C. 356j, Discontinuance or interruption in the production of medical devices (amended March 27, 2020).
the preparation or administration of the drug to develop and maintain redundancy risk management plans and implement them as necessary.17 The risk management plans are required to identify and evaluate the risks to the supply of the drug for each facility in which the FDF drug or API is manufactured. These plans are subject to inspection by the HHS secretary.
Various federal agencies, such as Departments of Commerce, Defense, Homeland Security, State, and Veterans Affairs, have developed and continue to develop regulations, guidance, standards, and other policy documents that complement the legal requirements regarding the medical product supply chain. These materials provide supply chain stakeholders with additional instruction for their role in the medical product supply chain.
Several gaps exist in the current legislation on medical product supply chains, leaving vulnerabilities unaddressed at the federal level. First, the reporting requirement for drug and device manufacturers focuses on disruptions to manufacturing, excluding downstream disruptions that could also lead to shortages, such as transportation disruptions, or disruptions that distributors detect. The President’s Fiscal Year 2020 budget proposed levying financial penalties on manufacturers that failed to adequately notify FDA of a drug shortage (FDA Drug Shortages Task Force, 2020), but such penalties were not included in the CARES Act. Another notable gap is that, unlike drug manufacturers, device manufacturers are not required to develop risk management plans. Furthermore, the current statute only requires that risk mitigation management plans be available upon inspection. While companies are likely compelled to provide records to FDA to avoid official actions, the CARES Act does not require that manufacturers proactively submit their plans to FDA, which would allow the federal government to have a more comprehensive understanding of risks in the supply chain. FDA does however have the authority to initiate administrative, judicial, or other punitive actions when a firm refuses to provide access to records under the Federal Food, Drug, and Cosmetic Act (FDA, 2014).
Response for Medical Product Shortages
Finally, the FD&C Act provides authority for FDA and HHS to respond in the event of a medical product shortage. These provisions can be generally classified as ones for an expected shortage or those for active, ongoing shortages. The former are discussed in the preceding section.
Under the FDASIA-amended section 506C,18 FDA and HHS can coordinate with the attorney general of DEA to increase production quotas for drugs should the nation experience a shortage of a controlled substance.
___________________
17 Food and Drug Administration Safety and Innovation Act. Public Law 112-144, 112th Congress (July 9, 2021).
18 21 U.S.C. 356c-1, Annual reporting on drug shortages (amended December 13, 2016).
Furthermore, this section releases hospitals from registration requirements as “repackagers” of an FDF drug product, and saves them from some of the laborious nature of bureaucracy, if during response measures to a drug shortage, hospital pharmacies divide the volume of a drug into smaller amounts in order to extend its supply and safely transfer repackaged drugs to other hospitals within the same health system.19 These policies enable medical supply chain resilience through flexibility in response measures.
Coronavirus Aid, Relief, and Economic Security Act
The shortages of medical products precipitated by the COVID-19 pandemic provided renewed urgency for addressing the resilience and transparency of medical product supply chains (Francis et al., 2021). Understanding this urgency, the U.S. government passed the CARES Act in March 2020, which called for the present study on the security of the medical product supply chain, and provided additional requirements for tracking and preventing medical product shortages.20
Due to a lack of transparency between manufacturers and HHS and incomplete reporting under existing regulations, the CARES Act amended the FD&C Act, adding certain API and device manufacturers to the categories of manufacturers that must notify the HHS secretary and Center for Devices and Radiological Health (CDRH) of device and drug shortages (FDA, 2020). It also added requirements for medical product manufacturers to develop risk management plans and annually report the amount of drug produced. The CARES Act also included provisions requiring (1) interagency notification of drug shortages, (2) facility inspection reports be sent to experts on drug shortages within FDA when drugs on the shortage list are produced at a specific facility, and (3) reporting the volume of each listed drug produced by each registered facility.
Defense Production Act
The Defense Production Act (DPA) enacted by Congress in 1950 was a post-World War II law, which gives the president emergency authority to manage U.S. industries and provide essential materials and goods to the government for national defense.21 In response to the COVID-19 pandemic, President Trump used the DPA to address medical product supply shortages, by issuing several executive orders from March through August 2020, allowing numerous federal agencies (i.e., HHS, Homeland Security, Department
___________________
19 21 U.S.C. 356f, Hospital repackaging of drugs in shortage (amended July 9, 2012).
20 Coronavirus Aid, Relief, and Economic Security Act of 2020, Public Law 116-136, 116th Congress (March 27, 2020).
21 Defense Production Act of 1950, Public Law 81-774, 81st Congress (September 8, 1950).
of Commerce, etc.) to use DPA authorities to mitigate supply chain issues (GAO, 2020). These authorities included (1) identifying nationwide priorities and allocations of all health and medical resources needed to respond to COVID-19 within the United States; (2) preventing the hoarding and price gouging of resources such as personal protective equipment and disinfecting and sanitizing products; (3) expanding the production capacity of medical products such as ventilators; (4) providing loans to create, maintain, protect, expand, and restore the domestic industrial base capabilities; and (5) determining the priorities and allocations of essential medicines, medical countermeasures, and critical inputs, including APIs and raw materials (GAO, 2020).
Drug Supply Chain Security Act
The Drug Supply Chain Security Act (DSCSA), which was enacted by Congress in 2013, was intended to protect consumers from exposure to drug products that may be counterfeit, adulterated, or otherwise harmful to patients.22 It lays out steps to create an electronic system to track and trace certain prescription drugs in the United States to help improve detection and removal of potentially dangerous drugs from the drug supply chain. The Partnership for DSCSA Governance, a nonprofit public–private partnership, was established to implement DSCSA traceability requirements over the coming years (FDA, 2021b). As of late 2021, the partnership had released a blueprint23 with requirements and recommendations to meet the DSCSA’s interoperability requirements that will take effect in 2023 (PDG, 2021).
Executive Orders
In addition to legislation on the medical product supply chain, several Presidential Executive Orders regarding the security of the supply chain have been released. These are discussed below.
Executive Order 13944 List of Essential Medicines, Medical Countermeasures, and Critical Inputs—August 6, 2020
The Trump administration released an executive order regarding the security of the medical product supply chain.24 The order directed relevant
___________________
22 Drug Quality and Security Act, Public Law 113-54, 113th Congress (November 27, 2013).
23 For more information and to read the full blueprint, see https://dscsagovernance.org/wpcontent/uploads/2021/07/PDG_Blueprint-v1.0-Final_071221.pdf (accessed October 11, 2021).
24 Exec. Order No. 13944, 85 FR 49929 (August 6, 2020).
executive departments and agencies to identify and promote the procurement of essential medicines, medical countermeasures, and critical inputs from domestic sources, as well as to increase their production domestically. The administration also ordered the FDA commissioner and the director of the Office of Management and Budget to identify and mitigate vulnerabilities in the supply chain for essential medicines, medical countermeasures, and critical inputs. In October 2020, FDA published the list of essential medicines, medical countermeasures, and critical inputs required by the executive order.25
Executive Order 14001 A Sustainable Public Health Supply Chain—January 26, 2021
This executive order from the Biden administration focuses on the “strategy to design, build, and sustain a long-term capability in the United States to manufacture supplies for future pandemics and biological threats.”26 This order directs representatives from various departments and agencies to coordinate with the Assistant to the President for National Security Affairs and Assistant to the President for Domestic Policy to develop a strategy to ensure the functioning of the supply chain in the event of future pandemics or biological threats.
In July 2021, HHS and the Departments of Commerce, Defense, Homeland Security, State, and Veterans Affairs, as well as the White House Office of the COVID-19 Response, released a report in response to Executive Order (EO) 14011 addressing the resilience of the public health supply chain, outlining goals, objectives, and recommendations to improve resilience.27 The recommendations are divided into three goals: (1) to build a diverse, agile public health supply chain and sustain long-term U.S. manufacturing capability for future pandemics; (2) to transform the U.S. government’s ability to monitor and manage the public health supply chain through stockpiles, visibility, and engagement; and (3) to establish standards, systems, and governance to manage supply chains and ensure fair, equitable, and effective allocation of scarce resources. The committee of this National Academies of Sciences, Engineering, and Medicine (the National Academies) report provides recommendations that build upon the above three goals and additionally includes calls for international and global cooperation along with focusing resources at the last mile.
___________________
25 See https://www.fda.gov/about-fda/reports/executive-order-13944-list-essential-medicines-medical-countermeasures-and-critical-inputs (accessed December 20, 2021).
26 Exec. Order No. 14001, 86 FR 7219 (January 21, 2021).
27 For the full report, see https://www.phe.gov/Preparedness/legal/Documents/NationalStrategy-for-Resilient-Public-Health-Supply-Chain.pdf (accessed October 6, 2021).
Executive Order 14017 America’s Supply Chains—February 24, 2021
Another executive order from the Biden administration took a broader approach, outlining the administration’s vision for resilient, diverse, and secure supply chains.28 The order calls for (1) the continuation of reporting to identify risks to the supply chain for drugs and the APIs that compose them, (2) policy recommendations to combat those risks, and (3) a report on the supply chains for the public health and biological preparedness industrial base. Ultimately, the goal of this executive order is to use the aforementioned reports to inform the Assistant to the President for National Security Affairs and the Assistant to the President for Economic Policy to be able to make recommendations regarding actions to make U.S. supply chains stronger and more resilient, such as regular supply chain reviews and international cooperation.
The report published in response to EO 14017 details some of the key risks and vulnerabilities to the pharmaceutical supply chain and offers potential solutions to address those vulnerabilities. The recommendations are divided into six categories: (1) rebuilding our production and innovation capabilities; (2) supporting the development of markets with high road production models, labor standards, and product quality; (3) leveraging the government’s role as a market actor; (4) strengthening international trade rules, including trade enforcement mechanisms; (5) working with allies and partners to decrease vulnerabilities in the global supply chains; and (6) partnering with industry to take immediate action to address existing shortages.
CONCLUDING REMARKS
Medical product supply chains are vital to the nation’s collective health and safety, in ordinary times as well as emergencies. But these supply chains are complex, varied, global, and constantly evolving. To an ever-greater degree, they are distributed enterprises managed by a network of organizations, rather than vertically integrated enterprises within a single entity. Particularly when profit margins are low, the private, profit-driven incentives to invest in supply resilience can differ widely from the public health and safety incentives to protect supplies of critical medical products. These factors all contribute to risks of supply disruptions, as evidenced by routine shortages and shortages during the COVID-19 pandemic.
Several acts of Congress and presidential executive orders have been enacted to address these risks. Although these instruments provide some authority, tools, and infrastructure for building medical product supply chain resilience, there is still much to do to better prepare for the next public health emergency. There have been continual policy fluctuations, and an
___________________
28 Exec. Order No. 14017, 86 FR 11849 (March 1, 2021).
unclear role of the federal government (or federal assets) in a public health emergency—which serve a stunting role in investment in medical product supply chain resilience. Finally, as noted in this chapter, the product classifications used to monitor quality and safety are not ideal for assessing and remediating supply risks. This leads to a lack of clear sense of where resilience measures are needed most. There is also no systematic framework for enumerating, prioritizing, and combining measures into a medical product supply chain resilience strategy. The remainder of this report will focus on these questions in order to inform recommendations that will substantially increase the resilience of medical product supply chains.
REFERENCES
AAM (Association for Accessible Medicines). 2021. 2020 Generic drug & biosimilars access & savings in the U.S. Washington, DC: Association for Accessible Medicines. https://accessiblemeds.org/sites/default/files/2020-09/AAM-2020-Generics-Biosimilars-Access-Savings-Report-US-Web.pdf (accessed October 20, 2021).
Berndt, E. R., R. M. Conti, and S. J. Murphy. 2017. The generic drug user fee amendments: An economic perspective. Journal of Law and the Biosciences 5(1):103-141.
CDER (Center for Drug Evaluation and Research). 2018. Drug shortage management. In Manual of Policies and Procedures (MAPP 4190.1 Rev.3), edited by FDA (U.S. Food and Drug Adminstration). Silver Spring, MD. https://www.fda.gov/media/72447/download (accessed January 12, 2022).
CDRH (Center for Devices and Radiological Health). 2018. Medical device overview. https://www.fda.gov/industry/regulated-products/medical-device-overview#What%20is%20a%20medical%20device (accessed October 14, 2021).
Dias, V., J. D. Quick, and J. R. Rankin. 2012. Ch 23: Inventory management. In MDS-3: Managing access to medicines and health technologies, edited by M. Embrey. Arlington, VA: Management Sciences for Health. https://msh.org/resources/mds-3-managing-access-to-medicines-and-health-technologies/ (accessed December 21, 2021).
FDA (U.S. Food and Drug Adminstration). 2012. Q11 development and manufacture of drug substances, edited by Center for Drug Evaluation and Research. Silver Spring, MD: HHS. https://www.fda.gov/media/80909/download (accessed October 21, 2021).
FDA. 2014. Guidance for industry FDA records access authority under sections 414 and 704 of the federal Food, Drug, and Cosmetic Act. https://www.fda.gov/media/83083/download (accessed December 20, 2021).
FDA. 2016. Q7 good manufacturing practice guidance for active pharmaceutical ingredients guidance for industry. FDA-1995-D-0288 HHS. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/q7-good-manufacturing-practice-guidance-active-pharmaceutical-ingredients-guidance-industry (accessed October 20, 2021).
FDA. 2017. Learn if a medical device has been cleared by FDA for marketing. https://www.fda.gov/medical-devices/consumers-medical-devices/learn-if-medical-device-has-been-cleared-fda-marketing (accessed December 9, 2021, 2021).
FDA. 2018. Statement by FDA commissioner Scott Gottlieb, M.D., on formation of a new drug shortages task force and FDA’s efforts to advance long-term solutions to prevent shortages. HHS. https://www.fda.gov/news-events/press-announcements/statement-fda-commissioner-scott-gottlieb-md-formation-new-drug-shortages-task-force-and-fdas (accessed November 5, 2021).
FDA. 2020. Medical device supply chain notifications during the COVID-19 pandemic. https://www.fda.gov/medical-devices/coronavirus-covid-19-and-medical-devices/medical-device-supply-chain-notifications-during-covid-19-pandemic (accessed October 12, 2021).
FDA. 2021a. Drug shortages: Non-compliance with notification requirement. https://www.fda.gov/drugs/drug-shortages/drug-shortages-non-compliance-notification-requirement (accessed October 11, 2021).
FDA. 2021b. Drug supply chain security act public-private partnership. https://www.fda.gov/drugs/drug-supply-chain-security-act-dscsa/drug-supply-chain-security-act-public-private-partnership (accessed October 12, 2021).
FDA. 2021c. Generic drugs: Questions & answers. https://www.fda.gov/drugs/questions-answers/generic-drugs-questions-answers (accessed October 20, 2021).
FDA Drug Shortages Task Force. 2020. Drug shortages: Root causes and potential solutions. https://www.fda.gov/drugs/drug-shortages/report-drug-shortages-root-causes-and-potential-solutions (accessed December 16, 2021).
Francis, J. R., B. M. Mairose, and E. M. Tichy. 2021. 2020—the year the world was awakened to the importance of supply chain management. Mayo Clinic Proceedings. Innovations, Quality & Outcomes 5(1):187-192.
GAO (Government Accountability Office). 2020. Defense Production Act: Opportunities exist to increase transparency and identify future actions to mitigate medical supply chain issues. https://www.gao.gov/assets/gao-21-108.pdf (accessed October 12, 2021).
Haninger, K., A. Jessup, and K. Koehler. 2011. Economic analysis of the causes of drug shortages, edited by Office of Science and Data Policy and Office of the Assistant Secretary for Planning and Evaluation. Washington, DC: HHS. https://aspe.hhs.gov/reports/economic-analysis-causes-drug-shortages-0 (accessed October 20, 2021).
Khan, R. 2020. Unsustainable low prices causing generic drug market failure leading to supply chain disruptions and shortages. Forbes, July 6. https://www.forbes.com/sites/roomykhan/2020/07/06/unsustainable-low-prices-causing-generic-drug-market-failure-leading-to-supply-chain-disruptions-and-shortages/?sh=2f5c682a74d4 (accessed December 20, 2021).
Lee, J., H. S. H. Lee, H. Shin, V. Krishnan. 2021. Alleviating drug shortages: The role of mandated reporting induced operational transparency. Management Science 67(4):2326-2339. https://doi.org/10.1287/mnsc.2020.3857.
Lin, A., F. Ma, and M. Rees. 2016. Life cycle of an adhesive bandage. http://www.designlife-cycle.com/adhesive-bandage (accessed October 14, 2021).
NAM (National Academy of Medicine). 2021. Four new reports from the National Academy of Medicine focus on how to prepare for seasonal and pandemic influenza through lessons learned from COVID-19. NAM, November 17. https://nam.edu/four-new-reports-from-the-national-academy-of-medicine-focus-on-how-to-prepare-for-seasonal-and-pandemic-influenza-through-lessons-learned-from-covid-19/ (accessed January 11, 2022).
NASEM (National Academies of Sciences, Engineering, and Medicine). 2020. Strengthening post-hurricane supply chain resilience: Observations from hurricanes Harvey, Irma, and Maria. Washington, DC: The National Academies Press.
PDG (Partnership for Drug Supply Chain Security Act [DSCSA] Governance). 2021. Partnership for DSCSA Governance (PDG) foundational blueprint for 2023 interoperability. https://dscsagovernance.org/wp-content/uploads/2021/07/PDG_Blueprint-v1.0-Final_071221.pdf (accessed October 11, 2021).
The PEW Charitable Trust and ISPE. 2017. Drug shortage: An exploration of the relationship between U.S. market forces and sterile injectable pharmaceutical products: Interviews with 10 pharmaceutical companies. PEW and ISPE. https://www.pewtrusts.org/-/media/assets/2017/01/drug_shortages.pdf (accessed October 25, 2021). Sheffi, Y., and J. B. Rice, Jr. 2005. A supply chain view of the resilient enterprise. MIT Sloan Management Review 47(1):41.
Sheffi, Y., and J. B. Rice, Jr. 2005. A supply chain view of the resilient enterprise. MIT Sloan Management Review 47(1):41.
Stevens, C. 2020. What is just-in-time (JIT) inventory management? https://www.business.org/finance/inventory-management/what-is-just-in-time-inventory-management/ (accessed October 21, 2021).
The White House. 2021. Building resilient supply chains, revitalizing American manufacturing, and fostering broad-based growth: 100-day reviews under Executive Order 14017. Washington, DC: Department of Commerce, Department of Energy, Department of Defense, and Department of Health and Human Services. https://www.whitehouse.gov/wp-content/uploads/2021/06/100-day-supply-chain-review-report.pdf (accessed October 20, 2021).
This page intentionally left blank.




















