
The first (April 2021) workshop began with an introductory session that provided a foundation for the workshop series. Camara Phyllis Jones, senior fellow at the Satcher Health Leadership Institute and Cardiovascular Research Institute and adjunct associate professor at Morehouse School of Medicine, presented an allegory for understanding racism, discussed the adoption of a broader perspective for comprehending the obesity epidemic, provided an analogy to illustrate levels of health intervention, and offered a perspective on commonalities between race and weight status and between racism denial and the obesity epidemic.
Jones began by sharing a story she developed to illustrate racism’s existence, titled “Dual Reality: A Restaurant Saga.” Based on an experience she had as a first-year medical student, Jones’s story began with a group of hungry medical students venturing into town for a meal after a long day of studying. She and her friends had entered a restaurant, sat down and ordered food, and begun eating when she noticed a sign in the restaurant that caused her to have a startling revelation about racism. The sign read “Open,” she explained, and she commented that she could have thought no more about it and assumed that other hungry people could enter the restaurant and order food as she and her friends had done. But because she was aware of the two-sided nature of such signs, she continued, she realized that the restaurant was now closed to anyone on the other side of the sign, who despite their hunger would not be able to enter and eat.
Jones described that moment as critical to shaping her understanding that racism structures “open/closed” signs in our society, which she
characterized as a “dual reality.” Those sitting inside the restaurant and eating, she elaborated, look up and see the “Open” sign and are potentially unaware that the opposite side of the sign has a different message. Jones asserted that it is difficult for people to recognize a system of inequity that privileges them, whereas individuals on the outside clearly see the “closed” sign and are keenly aware of the two-sided nature of the system as they look through the window and see others inside. For example, she went on, it is difficult for White Americans to recognize White privilege and racism, and difficult for all Americans to recognize American privilege in the global context.
Jones extended the allegory, explaining that people inside the restaurant may wonder whether the two-sided sign (i.e., racism) really exists. It is difficult to know the answer to this question when one can see only “Open,” she suggested, asserting that it is a privilege not to have to know. But when those inside recognize the two-sided nature of the sign, they can no longer wonder why those outside do not enter and sit down to eat. Knowledge of the existence of the two-sided sign (i.e., naming racism) is not scary, but empowering. Such knowledge does not compel those inside the restaurant to act, she clarified, but it does equip them for action if they care about those on the other side of the sign. As an example, she explained that the people inside could inform the restaurant owner about those outside and suggest that they be allowed to enter, or pass food out through the window, or even try to tear down the sign or break down the door.
Jones expressed feeling encouraged that more people who are “born inside the restaurant” have a sense of the two-sided nature of the sign compared with a year ago. More people are saying the word “racism,” as well as recognizing the terms “structural racism” and “systemic racism.” She cautioned against proclaiming these terms but failing to act, thereby slipping back into what she called a staunchly held societal “racism denial.” Naming racism is essential but insufficient, and she urged the audience not only to understand that racism is the sign creating a dual or multifaceted reality, but also to recognize that the sign corresponds to a locked door that must be broken down. “If we start acting, we will not forget why we are acting,” Jones declared as she concluded her story.
Jones moved on to further characterize racism and link it to the obesity epidemic, weight status, and discrimination. She described racism as “a system of structuring opportunity and assigning value based on the social interpretation of how one looks (i.e., what society calls ‘race’), that (1) unfairly disadvantages some individuals and communities, (2) unfairly advantages other individuals and communities, and (3) saps the strength of the whole society through the waste of human resources” (Jones, 2002). With regard to her second named impact of racism, Jones suggested that the issue of “unearned White privilege” is scarcely discussed in the United States
because it makes some people, particularly those living as White, uncomfortable. She urged leaning into such discomfort, proposing that “the edge of our comfort is actually our growing edge.” She also urged society to raise awareness of her third named impact of racism, such as through media storytelling and dinner table conversations, to instill a societal sense of urgency around dismantling the system of racism and replacing it with a system in which all people can know and develop to their full potential.
According to Jones, her definition of racism can be generalized to define any system of structured inequity. She cited sexism as an example, characterizing it as a system of structuring opportunity by assigning value based on gender, and having the same three impacts described in her definition of racism. Many axes of inequity operate in society and intersect in individuals and communities, Jones said, giving the examples of ethnicity, Indigenous status, and colonial history; weight status; labor roles and social class markers; nationality, language, and immigration status; sexual orientation, gender identity, and gender expression; disability status; geography; age; religion; and incarceration history. These axes are risk markers for how opportunity is structured and value is assigned, she claimed, and some are also risk factors in the progression to poor health (Jones, 2014).
Shifting to discuss obesity and weight perception, Jones stated that the U.S. obesity epidemic has traditionally been characterized as a binary classification of individuals on either side of the body mass index (BMI) cut point for obesity. Overweight and obesity are considered characteristics of “high-risk” individuals, she maintained, but suggested that understanding distributions of BMI as characteristics of populations—given that shifts in the population distribution of body mass drive the obesity epidemic—would illuminate what action is needed.
Such a shift in perspective has implications for intervention strategies, Jones continued, and she contrasted “high-risk” strategies with population-based strategies. The former involve urging individuals to avoid weight gain or lose weight by focusing on diet and physical activity, with success being dependent on perception of weight, motivation, and availability of healthful resources. The latter strategies, on the other hand, are aimed at shifting the distribution of body mass at the population level toward lower values via policy and environmental changes that target the types of food and activity opportunities available in such settings as neighborhoods, schools, and workplaces, where success is influenced by leadership and political will.
Jones elaborated on intervention strategies by offering a cliff analogy to explain levels of health intervention. Imagine that a person “fell off the cliff of good health,” she began, and was met by an ambulance at the bottom to whisk them to medical care. If society were concerned about others who might encounter the cliff (i.e., if it cared about population or community health), it might consider what supports to put in place in addition to the
ambulances at the bottom. Jones outlined potential support strategies, along with their limitations: a net between the edge of the cliff and the ground below, although some people might still fall through holes in the net; a trampoline halfway down the cliff, although those who landed on it might end up bouncing up and down, unable to get back to the top of the cliff; and a fence at the edge of the cliff to prevent falls, although it would have to be strong enough to resist heavy pressure from the population. A fourth support strategy, she suggested, would be to move the population away from the cliff’s edge. Jones likened the ambulance to acute medical care and tertiary prevention, the net and trampoline to safety net programs and secondary prevention, the fence to primary prevention, and shifting the population away from the edge to addressing social determinants of health and the contexts of peoples’ lives that push or position them into a high-risk area (Figure 2-1).
Jones pointed out a critical limitation of the cliff analogy, which is its failure to address how health disparities arise. She offered three explanations for the existence of health disparities, which she explained may
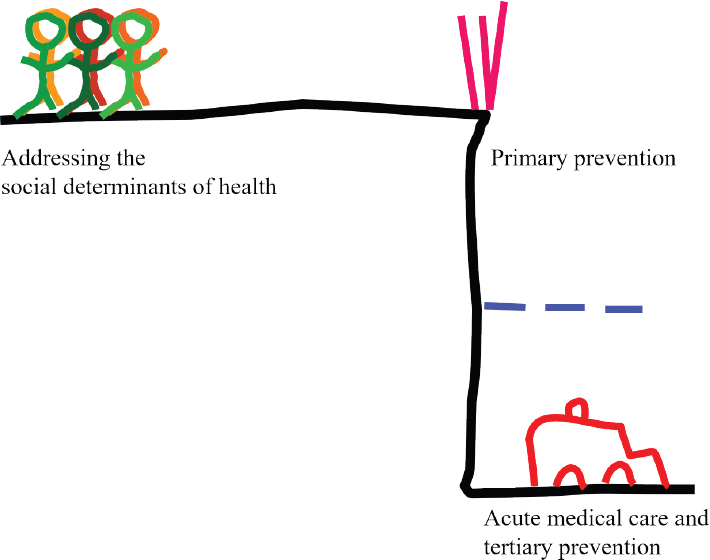
SOURCE: Presented by Camara Phyllis Jones, April 8, 2021; Jones et al., 2009. Reprinted with permission of Johns Hopkins University Press.
manifest according to such characteristics as racial/ethnic identity, weight status, region, or immigration status. One explanation is differences in the quality of care received in the health system; a second is differences in access to health care, including preventive and curative services; and a third is differences in life opportunities, exposures, and stresses that result in differences in underlying health status (Byrd and Clayton, 2001; IOM, 2003; Phelan et al., 2010). Returning to the cliff analogy, she pointed out that these three explanations indicate that the cliff is three- (rather than two-) dimensional, and that some parts of the cliff might have slow or misdirected ambulances at the bottom, as well as insufficient or missing nets or fences. These limitations, Jones continued, are representative of differences in quality of care and in access to care, respectively. At those parts of the cliff, she added, the population is usually pushed closer to the edge, which she likened to differences in opportunities and exposures (Figure 2-2).
Taking a step back, Jones explained that the analogy of a three-dimensional cliff prompts such questions as how it became three-dimensional,
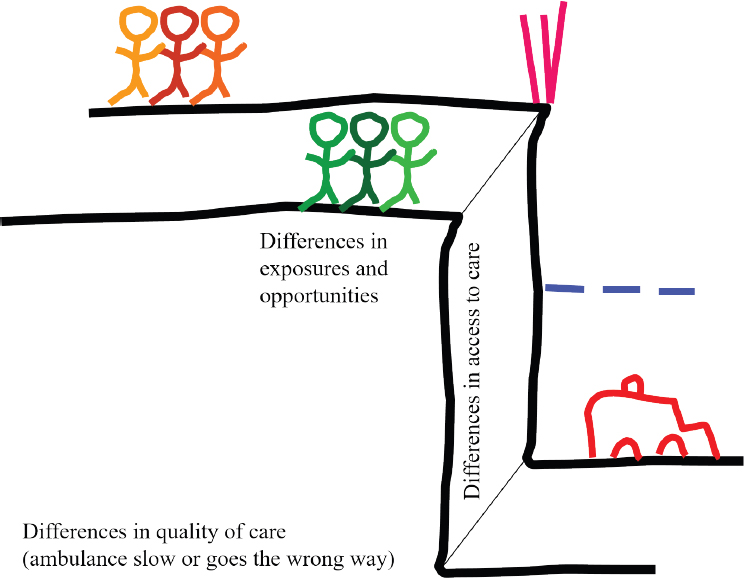
SOURCE: Presented by Camara Phyllis Jones, April 8, 2021; Jones et al., 2009. Reprinted with permission of Johns Hopkins University Press.
why differences in resources exist along the cliff face, and why differences exist in the populations that are found at different points along the cliff (Jones et al., 2009). When these questions come to the forefront, she said, it stimulates conversations about systems of power that can lead to differential circumstances. She termed these systems of power “social determinants of equity” (or inequity) or “systems of structured inequity.” According to Jones, such systems include racism, sexism, heterosexism, capitalism, and all of the systems associated with weight bias and discrimination.
Next, Jones expanded the cliff analogy to explain three dimensions of health intervention. The dimension along the cliff’s edge is where preventive and curative health services, such as the ambulance, net, and fence, are displayed. If this dimension is the only focus, she cautioned, even a universal health care system may be overwhelmed by the need to serve everyone. Jones urged moving into a second dimension of health intervention—addressing such social determinants of health as adverse neighborhood conditions and poverty—to move people away from the cliff’s edge. Failure to recognize that the cliff is three-dimensional, she warned, risks moving only some of the population away from the edge and thereby exacerbating health disparities. Jones emphasized the importance of acknowledging and addressing the three-dimensional nature of the cliff. Doing so, she suggested, leads to the third dimension of health intervention: addressing social determinants of equity.
The cliff analogy and the framework it creates raise three questions, Jones continued. First is why such a large proportion of U.S. health care expenditures goes toward acute medical care and tertiary prevention. The most cynical and apparent answer, she suggested, is that a great deal of money is made on medical treatments and devices, pharmaceuticals, and other such products and services. The more profound answer, however, is that the United States is too narrowly focused on the individual and does not recognize people’s health problems until they have already occurred. This narrow focus prevents recognition of the proximity of populations to the cliff’s edge as a health problem, Jones asserted, noting that such metrics as income inequality and social cohesion are not used as health measures.
Jones went on to raise the second question: why certain populations are so close to the edge of the cliff—why they engage in non–health-promoting behaviors. This focus on individual behaviors, she proposed, renders systems and structures either invisible or seemingly irrelevant.
The third question, Jones continued, is why a problem exists with the three-dimensional cliff. In her view, individuals may ask this question if they are in relatively privileged positions and lack a strong sense of urgency to help disadvantaged populations with whom they rarely come into contact. Jones shared her belief that this point of view reflects an endorsement of the “myth of meritocracy.” She acknowledged that most people who have
“made it” have indeed worked hard, but she suggested that this is not a universal truth: that not everyone who has “made it” has worked hard, and some who have worked hard “will never make it” because the playing field is uneven, a situation perpetuated by systems of structural inequity. According to Jones, denying the existence of an uneven playing field; reasoning that lack of hard work is why people have not “made it”; and talking about diversity, equity, inclusion, cultural competence, disparities, and other similar terms without naming racism are different ways of denying racism’s existence.
To conclude her presentation, Jones recapped what she perceives as four commonalities between denial of racism and the obesity epidemic: (1) a narrow focus on the individual that leads to (2) ignorance of systems and structures that contribute to the problem, and therefore (3) “invisibilizing” of solutions that would address those structures, leading to (4) indifference and inaction in the face of need.
After her presentation, Jones answered a question from Pronk about defining health equity in the context of obesity. She provided a three-part definition that she said encompasses what health equity is, how it can be achieved, and how it relates to health disparities. According to Jones, health equity is not an outcome but a process by which society pursues assurance of the conditions for optimal health for all people. She stressed that achieving health equity requires valuing all individuals and populations equally, recognizing and rectifying historical injustices, and providing resources according to need. She closed by asserting that health disparities will be eliminated when health equity is achieved.








