
6
Human Exposures, Health Impacts, and Mitigation
This chapter explores chemicals and other pollutants of concern for human exposure and health, as well as ways to reduce exposure and mitigate the impacts of wildland-urban interface (WUI) fires. It addresses all relevant distance scales, from the immediate fire zone, where emergency responders such as firefighters experience direct exposure to heat and high concentrations of fire emissions, to the regional and continental levels, where WUI fire smoke can have an extended impact. The committee has noted where WUI-specific information is available; however, such information is scarce. Therefore, much of the discussion presented in this chapter draws on studies from wildland fires. It is important to note, however, that this chapter is not a comprehensive review of the overall health effects of wildland fire smoke.
This chapter begins by identifying chemicals and other pollutants of concern for human exposure and describing populations who may be more vulnerable to the impacts of WUI fires, and those who experience environmental injustice and health inequities. The next section describes what is known about routes of exposure, followed by a discussion of the acute and chronic health impacts for all near- and far-field populations, with a dedicated section on exposures and impacts for firefighters. The last section explores ways to reduce exposure to WUI fire pollutants, as well as specific interventions for firefighters and affected communities.
Box 6-1 defines key terms that are used throughout this chapter.
CHEMICALS OF CONCERN FOR HUMAN EXPOSURE
Wildland fires are major sources of organic and inorganic gases and aerosols containing ultrafine particles (0.1 μm or less), fine particulate matter (PM2.5), and coarse particulate matter (PM10; EPA, 2021e). Specific composition is dependent on the fire fuel sources, direct emissions, secondary chemical and physical processes, ventilation, and meteorological conditions. A complex mixture of emission gases is present and can include greenhouse gases such as carbon dioxide (CO2) and methane (CH4); photochemically reactive substances such as as nitrogen oxides (NOx), carbon monoxide (CO), and volatile organic compounds (VOCs); and PM of various diameters. These emissions all contribute to available air pollution that can be detrimental to human health and ecosystems. Specific studies of fire-generated smoke have identified numerous hazardous substances including VOCs and semi-VOCs (SVOCs) like benzene, dioxins, furans, flame retardants, plasticizers, polycyclic aromatic hydrocarbons (PAHs), and polychlorinated biphenyls (PCBs), as well as carbon monoxide (CO), hydrogen cyanide (HCN), hydrogen chloride (HCl), nitrogen oxides (NOx), sulfur oxides (SOx), and heavy metals (CARB, 2021). Many of these substances represent known or probable carcinogens, irritants, respiratory sensitizers, or reproductive and developmental toxicants with linkages to cardiovascular impacts and neurological impairments (IARC, 2010). Smoke from WUI and wildland fires consists of complex mixtures of the aforementioned toxicants, which have the potential to interact with each other to modify the toxicity of single compounds (Zeliger, 2003). However, analysis of mixture toxicity and health effects is complicated. Thus, assessing the toxicity of individual constituents is most often used to predict the toxicity of the mixture. Table 6-1 summarizes some examples of key pollutants recognized in fire events along with general health impacts and common routes of exposure.
Research need: A need exists to pioritize WUI-related chemicals of concern, their exposure potentials, and their human health risks, with consideration of vulnerable populations, so that mitigation strategies can be developed.
TABLE 6-1 Examples of Chemical Pollutants Related to WUI Fire Events and Human Exposures
| Group of Pollutants | Common Examples | Routes of Exposure | Potential Health Outcomes | Selected References |
|---|---|---|---|---|
| Asbestos | Fibrous asbestos, chrysotile | Inhalation Ingestion |
Cancer; asbestosis; respiratory irritation; pleural disease | EPA, 2021a; ATSDR, 2016 |
| Asphyxiant gases | Carbon monoxide (CO), carbon dioxide (CO2), hydrogen cyanide (HCN) | Inhalation | Depression of central nervous system and hypoxia; acute respiratory effects | NIOSH, 2011; Gold and Perera, 2021 |
| Dioxins and furans (polychlorinated dibenzo-p-dioxins [PCDDs] and polychlorinated dibenzofurans [PCDFs]) | 2,3,7,8-Tetrachloro-dibenzo-p-dioxin/furan | Inhalation Ingestion Dermal (low penetration into skin by itself, but can cause skin lesions) |
Cancer or predisposition to cancer; reproductive and developmental effects; immune suppression; dermal toxicity; endocrine disruption | CDC, 2017; EPA, 2021b |
| Flame retardants | Tris(1-chloro-2-propyl) phosphate (TCPP), tris(2chloroethyl) phosphate (TCEP), tris isobutylated triphenyl phosphate, methyl phenyl phosphate | Inhalation Ingestion |
Neurotoxicity or neurodevelopmental damage; reproduction and fetal development effects; endocrine and thyroid disruption | ATSDR, 2015; NIEHS, 2021a |
| Inorganic acid gases | Hydrogen chloride (HCl), hydrogen fluoride (HF), phosphoric acid, SOx, NOx | Inhalation | Chemical burns; increased risk of laryngeal and lung cancer | ATSDR, 2002; NCI, 2019 |
| Inorganic and organic metals | Lead, lithium, iron, mercury, methylmercury, nickel, cadmium, palladium chloride | Inhalation Ingestion Dermal |
Neurotoxicity; reproductive and developmental effects, dermal irritation or allergen; respiratory irritation | Goyer, 2004; NIOSH, 2019a |
| Isocyanates | Methyl isocyanate, methylene diphenyl diisocyanate, toluene diisocyanate | Inhalation | Irritation and pulmonary sensitivity | ATSDR, 2014a; NIOSH, 2014 |
| Organic and other gases | Phosgene (COCl2), ammonia (NH3) | Inhalation | Acute effects; pulmonary edema and irritation | EPA, 2021c; CDC, 2018 |
| Ozone (O3) | Inhalation | Acute and chronic respiratory symptoms including coughing and exacerbation of chronic diseases such as bronchitis and asthma; increased risk of pulmonary infections | NEPHT, 2020 | |
| Particulate matter (PM) | PM is often classified by size, where the size is based on the aerodynamic diameter in micrometers (e.g., PM2.5); smaller particles penetrate deeper into the respiratory system | Inhalation Ingestion Dermal |
Cancer; cardiopulmonary toxicant; immunosuppressant; neurotoxicant; reproductive and developmental toxicity | EPA, 2021d; CDC, 2019 |
| Plasticizers | Ortho phthalates including dibutyl phthalate, terephthalates, adipates, benzoates | Inhalation Ingestion |
Endocrine disruptors; reproductive and developmental toxicity | EPA, 2022a; CDC, 2021 |
| Polycyclic aromatic hydrocarbons (PAHs) | Benzo[a]pyrene, benzo[a] anthracene, benzo[b] fluoranthene, chrysene, pyrene, fluoranthene, naphthalene, anthracene | Inhalation Ingestion Dermal |
Cancer; reproductive and developmental (teratogenic) toxicity; kidney and liver damage | CDC, 2022; ATSDR, 2014b |
| Polychlorinated biphenyls (PCBs) | 2-Chlorobiphenyl, 2,2-dichlorobiphenyl, 2,4,5-trichlorobiphenyl; PCBs typically occur as a mixture of PCB congeners (i.e., aroclors) | Inhalation Ingestion Dermal |
Cancer; neurotoxicity; immune suppression; endocrine disruption; reproductive and developmental toxicity; respiratory toxicity | ATSDR, 2000; Ahlborg et al., 1992 |
| Volatile organic compounds (VOCs) | Formaldehyde, acetaldehyde, acrolein, benzene, toluene, ethylbenzene, para-xylene, ortho-xylene, meta-xylene, styrene, naphthalene; complex mixtures of VOCs are classified as total VOCs, and some are not toxic | Inhalation Ingestion |
Cancer; reproductive and developmental toxicity; neurotoxicity; respiratory irritation; odorants | EPA, 2021c |
| Other emission and transformation products that are currently unidentified | Per- or polyfluoroalkyl substances (PFASs), including perfluorooctane sulfate and perfluorooctanoic acid Reactive oxygen species, including peroxides (R-OO-R) and superoxides (O2–) |
Inhalation Ingestion |
Cancer; respiratory and developmental toxicity | NTP, 2016 |
NOTE: Table 6-1 focuses on groups of chemicals with sound available data. The lists are meant as common examples and not meant to be exhaustive. A wide range of VOCs and SVOCs may be present including amines, amides, nitrosamines, trihalomethanes, glycols, and ethers.
VULNERABLE POPULATIONS, HEALTH EQUITY, AND ENVIRONMENTAL JUSTICE
Health is a product of multiple determinants. Social, economic, environmental, and structural factors and their unequal distribution matter more than health care in shaping health disparities (NASEM, 2017). To characterize what is known about human exposure, health impacts, and mitigation strategies for WUI fires, the committee examined individual and structural factors that may affect human health. For the purpose of this report, vulnerable populations are defined as individuals or communities at higher risk of adverse health effects from exposures, such as from greater pollutant exposure concentrations, higher health response to a given level of exposure, or reduced capacity to adapt, including lack of information or resources for personal mitigative strategies to reduce exposure. Another vulnerability is inequity in access to information, such as inequity based on the location of air pollution monitoring networks (Sun et al., 2022), which could result in a differential exposure misclassification that is propagated through human health studies.
A growing number of studies have shown that human health vulnerability to wildland fires can be influenced by several factors such as those related to life stage, location (e.g., at the WUI), socioeconomic status, race/ethnicity, occupation (e.g., outdoor workers), and underlying health conditions (Burke et al., 2021; Chan et al., 2013; Davies et al., 2018; Rudolph et al., 2018). The studies differ in their approaches, especially the methods to assess where and when fire exposures occur, such as for air pollution, and results are not perfectly consistent. For example, a study of wildland fire smoke in Alaska that examined the effects of wildland fire–associated PM2.5 on the general population and different subpopulations to assess vulnerability found that exposure to wildland fire–associated PM2.5 varied between specific Alaskan Native tribes, with the greatest effect levels seen for the Alaskan Athabascan tribe (Woo et al., 2020).
In another study, however, PM2.5 from wildland fire smoke was found to be at higher levels for non-Hispanic whites (Burke et al., 2021). The authors noted that actual differential health impacts were affected by social determinants other than exposure, such as those factors briefly described later in this section. Collectively, studies indicate that some populations may suffer a higher risk of related health outcomes from wildland fires, which is consistent with the broader research on environmental justice and health equity.
At a population level, health disparities (or health inequities) arise from root causes that could be organized in two clusters: (1) intrapersonal, interpersonal, institutional, and systemic mechanisms (sometimes called structural inequities) that organize the distribution of power and resources differentially across lines of race, gender, class, sexual orientation, gender expression, and other dimensions of individual and group identity; and (2) the unequal allocation of power and resources—including goods, services, and societal attention—which manifests itself in unequal social, economic, and environmental conditions, also called the determinants of health.
Health inequities are largely a result of poverty, structural racism, and discrimination (NASEM, 2017). Structural racism refers to the “totality of ways in which societies foster racial discrimination through mutually reinforcing systems of housing, education, employment, earnings, benefits, credit, media, health care, and criminal justice. These patterns and practices in turn reinforce discriminatory beliefs, values, and the distribution of resources” (Bailey et al., 2017, p. 1453). Additionally, structural intersectionality highlights that individual life chances are shaped not by a single status hierarchy but by multiple overlapping systems of oppression such as racism, sexism, and classism (Hardeman et al., 2022; Homan et al., 2021).
The reasons for greater vulnerability for some conditions are multifaceted and based on both historical and current social, cultural, and political factors, including structural racism. As a few examples, baseline health status, nutrition and diet, access to quality health care including language-appropriate providers, occupational opportunities, and ability to adapt (e.g., move residence) can impact one’s health response to environmental conditions. This health response includes not only the more commonly studied physical responses such as respiratory symptoms, but also mental health and well-being impacts that come from such stressors. For instance, building envelope airtightness affects how well ambient air, including smoke, can penetrate indoors, which can result in differential impacts for those in lower-income housing (Chan et al., 2013). Additionally, low-income housing units are less likely to have adequate cooling systems to allow them to keep windows closed during the summer heat when wildland fires and WUI fires are typically occurring (HHS, 2018). They also may not be able to afford to purchase home air cleaners for particle and chemical filtration. The nonprofit Resources for the Future reported that projects to reduce risk to wildland fires are disproportionately located in communities of higher socioeconomic status, of higher education, and with a higher proportion of white residents (Anderson et al., 2020).
Table 6-2 describes vulnerable populations affected by WUI fires. Note that adults may face additional exposure based on occupation and may experience multiple aspects of vulnerability. Environmental injustice in the workplace
TABLE 6-2 Vulnerable Populations at the WUI
| Vulnerable Population | Example Pathways to Vulnerability (vulnerability includes increased exposure, inability to adapt, and health response) | Selected References |
|---|---|---|
| Community- or Life Stage–Based Vulnerability | ||
| Children |
|
Sacks et al., 2011; Vanos, 2015; Perera, 2008; Revi et al., 2014 |
| Older Adults |
|
Rudolph et al., 2018; EPA, 2019; Liu et al., 2017 |
| Pregnant People |
|
EPA, 2009 |
| People with Respiratory and Cardiovascular Disease |
|
Wettstein et al., 2018; DeFlorio-Barker et al., 2019; |
| Tribal Communities |
|
Rudolph et al., 2018; Woo et al., 2020 |
| Communities of Color, and Immigrant, Migrant, and Refugee Communities |
|
Rudolph et al., 2018; Brim et al., 2008; Fussell et al., 2018; Davies et al., 2018; Liu et al., 2017 |
| Low-Income Communities |
|
Rudolph et al., 2018; Reid et al., 2016a; Brim et al., 2008 |
| Rural Communities |
|
Rudolph et al., 2018 |
| Unhoused/Homeless Communities |
|
Rudolph et al., 2018 |
| People with One or More Disabilities |
|
Rudolph et al., 2018 |
| Occupation-Based Vulnerability | ||
| Wildland Firefighters and Emergency Responders (e.g., Emergency Health Care Personnel) |
|
Rothman et al., 1991; Fent et al., 2017; Navarro et al., 2019 |
| Outdoor Workers (e.g., Farmworkers, Construction Workers, Utility Workers) |
|
Austin et al., 2021 |
| Environmental Remediation Workers (e.g., Hazardous and Solid Waste Removal) |
|
EPA, 2019; Fussell et al., 2018 |
| Domestic Workers and Day Laborers |
|
IDEPSCA, 2020 |
Referenced in developing this table:
EPA. 2021g. “Which Populations Experience Greater Risks of Adverse Health Effects Resulting from Wildfire Smoke Exposure?” https://www.epa.gov/wildfire-smoke-course/which-populations-experience-greater-risks-adverse-health-effects-resulting.
American Public Health Association. n.d. “Climate Changes Health: Vulnerable Populations.” https://www.apha.org/topics-and-issues/climate-change/vulnerable-populations.
EPA. 2019. Wildfire Smoke: A Guide for Public Health Officials. EPA-452/R-19-901. Washington, DC: EPA.
occurs as disproportionate exposure to occupational hazards and as vulnerable populations disproportionately working at high-risk jobs, such as wildland firefighting, emergency response, and environmental remediation.
Finding: Vulnerable populations may exhibit a higher risk of adverse health response and exacerbation of ongoing disease, particularly asthma and pulmonary disorders, as a result of WUI smoke exposure.
Research need: More studies are needed on exposure and potential health effects of WUI fires on children and other vulnerable groups.
ROUTES OF EXPOSURE
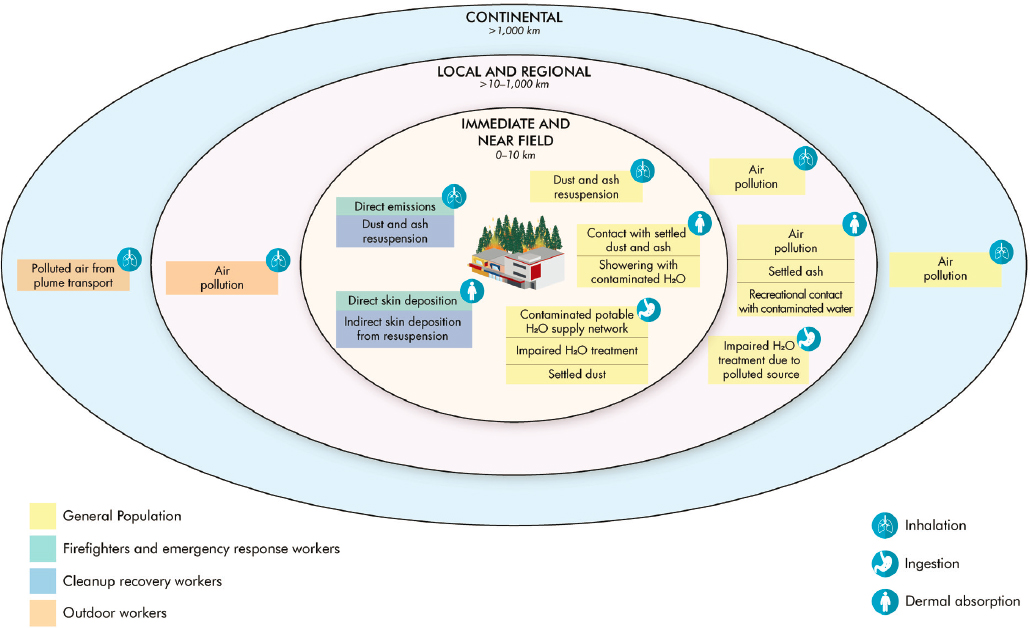
Human exposure to smoke emissions is possible at all spatial scales away from WUI fires (Figure 6-1). As depicted in the figure, the subpopulations that are exposed and the most important pathways and routes of exposure vary across the different WUI zones.
The environmental matrices of immediate concern for health effects of exposure to emissions from a WUI fire to persons in the immediate (<1 km) and near-field (1–10 km) regions include the following:
- Outdoor air contaminated directly from smoke emissions associated with combusted fuels
- Indoor air contaminated via infiltration from outdoors
- Indoor surfaces contaminated by deposition of airborne particulates
- Soil contaminated via ash residue from combusted fuel or deposition from airborne emissions
- Surface water contaminated from ash and aerosol deposition, runoff from contaminated soils, and increased runoff due to reduced land cover
- Drinking water
Air that is polluted by plume transport is the main environmental matrix of concern for populations in the local (10–100 km), regional (100–1,000 km), and continental (>1,000 km) zones. There is also potential for exposure in the local and regional zones via contact with settled dust and ash and contaminated surface water. However, a major difficulty in understanding the extent and the impact of wildland fire is the limitation of ambient monitoring networks that were designed primarily to support environmental regulation. The insufficiency of ambient monitoring networks is amplified for WUI fires, where additional chemical composition information is needed to understand exposure. As expected, the potential interactions of different population subgroups with the contaminated matrices and the patterns of exposure (i.e., intensity, frequency, and duration) will vary and be time dependent relative to the fire event (during vs post fire). These interactions and the potential exposure levels for possible exposure scenarios, when data are available, are discussed in the following subsections.
Inhalation Exposures
This section explores inhalation exposures in the various zones of a WUI fire.
Immediate and Near-Field Inhalation Exposure
Ideally, the general public is evacuated from the immediate and near-field zones during WUI fires; however, complete and timely evacuation is not always possible. In cases of full evacuation, wildland firefighters and other emergency response workers are the most likely population subgroups that will be exposed to air pollution from WUI fires in these zones, while the fire is burning. These firefighters will experience the highest exposure concentration of pollutants because of firefighting duties that involve protecting structures and other properties in urban areas and the consequent proximity to the emission source. A few individuals who do not comply with evacuation orders could also experience elevated exposure levels of air pollutants.
However, data on the personal inhalation exposures of wildland firefighters and other emergency response workers in the immediate and near-field zones during WUI fires have yet to be reported. While such data could be extrapolated from that of wildland fires, burning structures could contribute to increased exposure concentrations and smoke components that are mostly absent in purely vegetative wildland fires (Fent et al., 2018; Jaffe et al., 2020). Also, wildland firefighters, unlike structural firefighters, routinely do not wear any respiratory protection against inhalation exposures, as there is no approved respirator for wildland firefighting. Moreover, they may experience repeated exposures annually and across their careers.
Personal exposure monitoring of wildland firefighters suggests that the exposure concentration of PM2.5 at WUI fires could average hundreds to thousands of micrograms per cubic meter (μg/m3; Cherry et al., 2019). Currently, no regulated occupational standard exists for wildland firefighters that is relevant to such PM exposure, since wildland fire–generated particles have multiple reactive and toxic components. Relatedly, wildland firefighters are specifically excluded from the California Occupational Safety and Health Administration’s standard on
protection of workers from wildland fire smoke when the US Environmental Protection Agency (EPA) Air Quality Index (AQI) for PM2.5 is equal to or higher than 151 (PM2.5 concentration ≥ 55 μg/m3; State of California, n.d.). Nonetheless, the National Wildfire Coordinating Group recommends an occupational exposure limit of 750 μg/m3 for wildland firefighting, which is often exceeded. Moreover, smoke particles from WUI fires are likely to be enriched with metals, asbestos, and other fibrous particles, as well as PAHs, halogenated hydrocarbons, and pesticides, due to burning structures and depending on land use (Carratt et al., 2017; Kohl et al., 2019; Plumlee et al., 2007; Stec, 2017). Radionuclide enrichment of airborne particles is also possible if nuclear facilities are involved, as in the Cerro Grande, New Mexico, fire in 2000 (Eberhart, 2010).
Personal exposure and area concentration data at wildland fires are available only for a limited number of gaseous contaminants, with results indicating that fireline exposure could occasionally exceed the Occupational Safety and Health Administration (OSHA) 8-hour permissible exposure limits of 100 ppb, 1 ppm, and 50 ppm for acrolein, benzene, and carbon monoxide, respectively (Barboni et al., 2010; Miranda et al., 2010; Reinhardt and Ottmar, 2004; Reisen and Brown, 2009). Personal exposure of firefighters at the fireline to benzene, a blood carcinogen, may be even more elevated at WUI fires due to its enrichment in smoke emissions from the combustion of non-biomass WUI fuels (structural materials, vehicles, and furniture), compared to wildland fires (Jaffe et al., 2020). Emissions of hydrogen cyanide, an asphyxiant, and respiratory irritants including hydrogen chloride, nitrogen dioxide, and sulfur dioxide are also enriched in smoke emitted from the combustion of non-biomass WUI fuels versus wildland fires (Jaffe et al., 2020).
Direct measurement of the exposures of other emergency response workers within the immediate and near-field zones during fires has yet to be reported in the literature (Navarro, 2020). However, their inhalation exposures are expected to be less than those experienced by wildland firefighters because they spend less time in proximity to the fireline. The amount inhaled and effective dose of smoke constituents in wildland firefighters are also increased relative to other emergency responders and the public due to the increased breathing (ventilation) rates required during the physically exerting tasks of firefighting (Navarro et al., 2019).
Area measurements of air pollutants within the near-field zone reveal possible exposures of individuals who do not or cannot comply with evacuation orders. PM2.5 concentrations up to an order of magnitude above the National Ambient Air Quality Standard of 35 μg/m3 per day, and considered unhealthy for the general public on the EPA AQI, were measured in this zone during the 2016 Horse River Fire in Alberta, Canada, and the 2018 Camp Fire in California (CARB, 2021; Landis et al., 2018; Tam and Adams, 2019; Wentworth et al., 2018). Elevated concentrations of lead, but below the National Ambient Air Quality Standard of 0.15 μg/m3, were also measured during the Camp Fire. Exceedances of the National Ambient Air Quality Standard for the major gases (nitrogen dioxide, carbon monoxide, sulfur dioxide, and ozone) were not observed in area measurements in either of the aforementioned fires.
Ultimately, the effective exposure of those who do not or cannot evacuate will depend on their activity indoors or outdoors and/or the building ventilation. Since the size of particles in combustion emissions is typically below 1 micrometer (Kleinman et al., 2020; Sparks and Wagner, 2021; Zauscher et al., 2013), the penetrability of particulates together with gaseous contaminants in smoke from the outdoors to the indoor airspace will be high (Xiang et al., 2021). A large portion of wildland fire smoke is PM with a higher proportion of ultrafine particles than typical ambient air pollution. The average PM2.5 infiltration factor (the fraction of outdoor PM2.5 that enters and remains suspended in indoor air) during a period of wildland fire impact ranged between 0.33 and 0.76 for seven homes that were located hundreds of miles away from the fire (Xiang et al., 2021). Infiltration in the near-field zone may be even higher since particle size distribution tends to be smaller in freshly emitted smoke (Kleinman et al., 2020; Zauscher et al., 2013).
Since reentry decisions after an evacuation are made based on monitoring, ambient air concentrations of fire-related pollutants are expected to be of less concern for residents returning to evacuated communities, as observed for the Horse River Fire (Tam and Adams, 2019). In addition, careful debris removal will mitigate the contribution of this removal to air pollution and the exposure of returning residents (DuTeaux, 2019). Nevertheless, inhalation exposure of residents and recovery (cleanup) workers to fire emissions can still occur due to the resuspension of fire ash and dust from surfaces both indoors and outdoors, and offgassing of VOCs adsorbed onto surfaces indoors. Also, inhalation exposure to VOCs from contaminated potable water supply networks is a possibility; elevated concentrations of benzene, toluene, and styrene were measured in the water supply system after
the 2017 Tubbs Fire and 2018 Camp Fire (Proctor et al., 2020). Although these are possible routes to inhalation exposure, the committee chose to focus on the most likely routes to inhalation exposure.
Regional and Continental Inhalation Exposure
Farther away from the fire, the plume dilutes and ages, resulting in different inhalation exposure considerations from those of the near-field region. Concentrations of air pollutants can drop off rapidly away from the fire (O’Neill et al., 2021), but as the plume spreads, it may impact large population centers and thus affect a far greater number of people than in the near-field region (Koman et al., 2019). Numerous examples from the 2020 and 2021 fire seasons show large parts of the western United States experiencing sustained unhealthy air pollutant concentrations, with several days or longer of daily averaged PM2.5 concentrations near 150 μg/m3 (Filonchyk et al., 2022; Zhou et al., 2021). Some of these plumes degraded air quality thousands of kilometers downwind, as was observed on the US East Coast during July of 2021 (NASA EO, 2021). This long-range smoke transport makes wildland fires more than just a regional concern, but a national or international air quality issue (Dreessen et al., 2016). Additionally, local topography can lead to severe smoke episodes outside of the near-field range. Smoke can settle into valleys and remain trapped by smoke-induced inversions, leading to extremely high PM concentrations (Kochanski et al., 2019). An example of this was seen in 1999 in Northern California, where daily PM10 concentrations exceeded 500 μg/m3 (Mott et al., 2002).
Measurements in aging plumes have shown that gas-phase compounds have varying atmospheric lifetimes, and that the species that are important drivers of health effects in the near field may not be as important for far-field exposures. For example, reactive compounds like acrolein rapidly decrease in concentration with aging, while nonreactive compounds like hydrogen cyanide can remain elevated after 3 days of aging (O’Dell et al., 2020). Particle composition also changes, with the rapid formation of tar balls (Adachi et al., 2019) and the oxidation of organic PM constituents (Hodshire et al., 2019) downwind. The fly ash in the plume will also fall out downwind of the fire, but the lifetime of ash in the atmosphere is not well known (Bodi et al., 2014). The extent of ash dispersion may be particularly important for WUI fires since toxic metals can concentrate in the ash (Alexakis, 2020). Many unknowns remain in the aging of smoke from WUI fires (as discussed in Chapter 4) and how those factors could impact the potential health effects in downwind communities.
In addition to the changing chemistry of the plume, mitigation measures taken farther afield may differ from those closer to the fire. Public health messaging efforts may be limited or nonexistent in communities hundreds of kilometers downwind, and therefore fewer people might take mitigating measures to reduce potential exposure, such as staying indoors, operating heating, ventilating, and air-conditioning (HVAC) filtration systems, or using portable air cleaners. The awareness of smoke, either through decreased visibility or by odor, can prompt people to take mitigating actions (Kolbe and Gilchrist, 2009), and the lower concentrations far away from the fire may not meet the threshold for public awareness. Magzamen et al. (2021) observed differential health effects between local and long-range transported smoke with lower incidence of adverse health outcomes being associated with local smoke. Although engagement in mitigation actions and exposure misclassification could have biased the result, the authors hypothesized that aging led to additional oxidant production in the long-range transported smoke that could have increased inflammatory response (Magzamen et al., 2021). The authors’ results highlight the importance of a better understanding of exposures in the far-field range. Identification of compounds that can serve as surrogates for WUI fire exposures (i.e., source tracers) is one of the tools that could support future epidemiological analyses.
Finding: Based on information from wildland fires, smoke inhalation is an exposure route of concern for WUI fires, including at longer distance scales (i.e., regional and continental), with the best available information on particulate matter exposure.
Research need: There is a need to better understand the composition of gas and particulate exposures in WUI fires, and how they differ from wildland fires.
Research need: Assessments of smoke exposure typically rely on outdoor concentrations. A continued understanding of indoor penetration and persistence of smoke during and after fires, and an accounting for the chemical emissions profile of WUI fires, is needed.
Dermal Exposures
Although likely for residents in the near-field zone, dermal exposure is of most concern for wildland firefighters during responses to WUI fires. Evidence from non-WUI fires indicates that dermal absorption contributes significantly to the exposures of wildland firefighters working at fires (Banks et al., 2021; Fent et al., 2017, 2019a,b; Pleil et al., 2014; Stec et al., 2018). Such exposure could occur either through direct deposition on exposed skin, by cross-contamination between the turnout gear and skin, and/or via permeation and penetration through firefighter protective clothing (Kirk and Logan, 2015). Biomonitoring studies have measured increased concentrations of PAHs on the skin, their metabolites in urine, and VOCs (including benzene, toluene, ethylbenzene, xylenes, styrene, and naphthalene) in exhaled breath following training or controlled structure fires. This was true even among structural firefighters who, in addition to fireproof clothing, consistently wore self-contained breathing apparatuses (Banks et al., 2021; Fent et al., 2017, 2019a,b; Pleil et al., 2014; Stec et al., 2018), which essentially eliminate inhalation as an exposure route.
Increased concentrations of PAHs on skin and their metabolites in urine have also been measured among wildland firefighters following work at prescribed fires (Adetona et al., 2017a; Cherry et al., 2021). Furthermore, the potential for dermal exposure is likely higher during wildland firefighting since looser fitting protective clothing with fewer layers is typically worn at wildland fires compared to structure fires. The significance of dermal absorption during wildland firefighting is demonstrated by a more pronounced reduction in urinary concentration of the PAH metabolite, hydroxypyrene, from immediately after a firefighting shift to the following morning among firefighters who followed an enhanced skin hygiene intervention (change to new clothes, washing of firefighting clothes, and showering) immediately post-shift compared to those who did not. Similarly, urinary hydroxypyrene concentration was lower among wildland firefighters who reported having more opportunities for skin hygiene (e.g., wash, shower, and change of clothes) while working at the 2016 Horse River Fire (Cherry et al., 2019).
In addition to PAHs and VOCs, firefighters may also be dermally exposed to higher concentrations of halogenated organics (e.g., PCDD/Fs, PCBs, and flame retardants) at WUI fires. However, no study of dermal exposures of firefighters to these compounds during WUI fires has been reported. Likewise, the committee found no study of dermal exposure of recovery workers to contaminants in WUI fire ash; the committee expects that such exposure can be prevented by the use and cleaning of appropriate protective clothing and personal washing procedures.
While dermal absorption of contaminants in settled indoor dust is a potential exposure pathway for residents returning after WUI fires (Meng, 2018; Shi, 2021), trace metal and PAH concentrations were similar or lower in dust vacuumed from home floors (carpet or hardwood) in the city of Fort McMurray, which was affected by the 2016 Horse River Fire, compared to the typical home in Canada (Kohl et al., 2019). Similar concentrations of PAHs and metals in vacuumed dust were also measured in homes in Fort McMurray neighborhoods irrespective of the severity of fire damage based on the number of burned buildings (Kohl et al., 2019). However, dust samples were collected only once, 14 months after the wildland fire event, rendering comparisons with pre-wildland fire dust concentrations in the same homes impossible.
Appropriate post-fire cleanup procedures and regular home cleaning are expected to reduce concentrations of fire-related smoke contaminants in homes and potential exposures over time. However, it is uncertain that cleanup guidance is consistently issued to returning residents, and the potential increased exposure risk that can result from noncompliance with issued guidance is a source of concern. Moreover, the concentrations of arsenic, chromium, copper, tin, vanadium, and zinc in ash samples collected from burned buildings in Fort McMurray during the fire event were one to two orders of magnitude higher than those measured in the house dust 14 months later. The building ash samples were also enriched in trace metals, but not PAHs, relative to the ash samples collected in burned forests outside of the city during the fire event.
The committee identified no other studies of actual or potential dermal exposures due to indoor dust. Although enrichment of nutrients and metals in fire-impacted surface water and increased concentrations of VOCs and heavy metals in the public water supply have been documented (Burton et al., 2016; Emmerton et al., 2020; Proctor et al., 2020; USGS, 2012), actual dermal exposure via these pathways has yet to be studied. Finally, dermal exposures of outdoor workers and the general population beyond the immediate and near-field zones around fires may be of concern: researchers observed an association between WUI fire–impacted air pollution and clinical visits due to atopic dermatitis and itch in San Francisco, California, which is 280 km away from the areas burned by the 2018 Camp Fire (Fadadu et al., 2021).
Finding: The potential for dermal exposure to smoke constituents among firefighters at WUI fires is demonstrated by dermal exposures of firefighters to PAHs and VOCs at structural and wildland fires.
Research need: Studies are needed to characterize the dermal exposures of emergency and cleanup workers, and residents upon reentry.
Research need: There is a need for research to develop standard procedures for the cleanup of contaminated homes post-fire.
Ingestion
Ingestion of contaminants emitted in fire smoke most likely results from exposure to contaminated water post-fire in the immediate, near-field, local, and regional zones (see Chapter 5). Ingestion can also occur from hand-to-mouth transfer when hands are contaminated with settled dust or surfaces are contaminated with fire by-products. Consistent with wildland fires in general (Rust et al., 2018), studies of WUI fires have observed an increased loading of sediments, carbon, nutrients, and metals into surface waters, because of exposed soil and ash, in storm flows following WUI fires (Burke et al., 2013; Burton et al., 2016; Emmerton et al., 2020; Hohner et al., 2016; Stein et al., 2012; USGS, 2012; Writer et al., 2014). Studies have reported storm-associated elevation of the concentration of dissolved organic carbon in surface or source water above the threshold (5 mg/L; USGS, 2012) set for ideal water treatment; levels below this threshold are more conducive to water treatment and disadvantage the formation of unwanted disinfection by-products (Burton et al., 2016; Hohner et al., 2016; USGS, 2012; Writer et al., 2014). Ash from fires could also reduce the effectiveness of dissolved organic carbon removal by alum coagulation for drinking water treatment (Chen et al., 2020).
Hohner et al. (2016) reported the formation of the disinfection by-products trihalomethanes and haloacetic acids above the EPA maximum concentration limits of 80 and 60 μg/L, respectively, in post-storm water samples at the intake of the Fort Collins, Colorado, drinking water treatment plant downstream of the burned areas of the 2012 Hewlett Gulch and High Park WUI fires. However, the committee found no studies of disinfection by-product concentration in drinking water supply following chlorine or chloramine disinfection in areas affected by fires. The more toxic, but unregulated, bromine-substituted trihalomethanes and haloacetic acids preferentially form in the presence of bromine (Chen et al., 2020; Uzun et al., 2020), which is likely to be more concentrated in WUI fire emissions due to its presence in plastics and household products. Nevertheless, no actual measurements of these compounds in drinking water supplies following WUI fires have been reported.
Evidence indicates that trace metals may be enriched in contaminated stormwater that is associated with fires that involve residences or other structures compared to strictly wildland fires. Burton et al. (2016) and Wolf et al. (2011) reported higher concentrations of trace metals in fire ash and its leachate (water that has percolated through a solid and leached out some of the constituents), respectively, in samples collected from residential areas compared to those from wildlands burned by fires. WUI fire studies measured post-fire concentrations of arsenic, cadmium, and lead in stormwater that were above the EPA primary drinking water standards (10, 5, and 15 μg/L, respectively; Burton et al., 2016; Burke et al., 2013; Murphy et al., 2020; Stein et al., 2012). Arsenic concentrations also exceeded the EPA ambient water quality criteria of 18 μg/L in some studies (Burton et al., 2016; Murphy et al., 2020; Stein et al., 2012). EPA secondary drinking water standards were exceeded in some instances for other metals: aluminum (200 μg/L), iron (300 μg/L), manganese (50 μg/L), and zinc (7.4 mg/L; Burton et al., 2016; Burke et al., 2013; Murphy et al., 2020). Nonetheless, evidence suggests that bioavailability of the metals may be low as they partition preferentially to the particulate phase and are adsorbed efficiently by ash (Cerrato et al., 2016).
Radionuclides may also be mobilized into surface water after WUI fires depending on existing land use (Gallaher and Koch, 2004; Igarashi et al., 2020). Persistent organic pollutants emitted in WUI fires, including PAHs, dioxins, and PCBs, have also been measured in stormwater runoff (Gallaher and Koch, 2004; Stein et al., 2012). Of these measurements, only PCBs following the Cerro Grande Fire were reported to exceed standards, including that for primary drinking water at 500 ng/L and ambient water criteria at 64 pg/L.
Proctor et al. (2020) recently reported potential post-WUI-fire exposures to elevated concentrations of VOCs in drinking water via the contamination of the plumbing network in fire-affected areas during the Tubbs and
Camp Fires (Proctor et al., 2020). They found that maximum concentrations of VOCs in the impacted area, measured in the public drinking water supply of the affected communities, were multiple times the EPA primary drinking water standard for benzene (40,000 vs 5 μg/L), dichloromethane (41 vs 5 μg/L), styrene (460 vs 100 μg/L), toluene (1.4 vs 1.0 mg/L), and vinyl chloride (16 vs 2 μg/L; Proctor et al., 2020). The study suggested that contamination of the drinking water supply could have been caused by the heating/burning of the components of the water supply plumbing network and/or depressurization of the system (Proctor et al., 2020). Although recent laboratory experiments have demonstrated the thermal degradation of plastic pipe products used for drinking water sources with the emission of VOCs and SVOCs (including benzene, toluene, styrene, and phthalates) leaching into the water (Chong et al., 2019; Isaacson et al., 2020), findings similar to those of Proctor et al. (2020) or other measurements of contamination of drinking water by WUI fires have not been reported. More research is needed to better understand potential sources of contamination into drinking water and how community water systems could minimize impacts on public health.
Finally, ingestion of deposited WUI-emitted dust- and ash-borne contaminants on indoor surfaces and crops is possible. However, ingestion of contacted contaminants from surfaces by residents upon reentry into their homes and/or community can be minimized through effective cleanup activities and personal hygiene measures such as frequent hand washing. As previously noted, indoor dust concentrations of PAHs and trace metals in homes in Fort McMurray, Alberta, Canada, were apparently unimpacted by the Horse River Fire when measured 14 months after the fire event (Kohl et al., 2019). Also, information is lacking about potential exposure due to the ingestion of contaminated crops.
Finding: Ingestion exposures can occur through three primary mechanisms: compromise of the water supply network, compromise of water treatment, and hand-to-mouth transfer of contaminated dust.
Research need: Studies that characterize the contamination of the indoor environment, pathways of pollutant exposure to returning residents, and effective mitigation strategies for pollutant removal are needed.
Research need: Research is needed to further characterize the chemicals and health impacts of WUI fire emissions via different routes of exposure, including inhalation, dermal exposure, and ingestion. Affected communities need to be fully engaged in this research to better inform approaches and implementation.
HEALTH IMPACTS
Wildland and WUI fires adversely impact public health as they represent a dramatic source of air, water, and soil pollution in neighboring and even more distant populations. Epidemiological studies estimate that the global mortality burden attributable to landscape fire smoke is approximately 339,000 deaths annually (Johnston et al., 2012). Adverse health effects from fires have been measured hundreds of kilometers away, such as the impacts of the 2018 Camp Fire on California Bay Area residents 240 km downwind (Rooney et al., 2020). They have also been measured well beyond 1,000 km away, such as with the 2016 Horse River Fire, which started near Fort McMurray, Alberta, Canada, and resulted in smoke transport and impacts on air quality more than 4,000 km away in New York City, New York, in the United States (Wu et al., 2018). This section first describes health effects associated with exposure to wildland and WUI fires, in particular WUI fires, as they impact communities and regional populations. It then explores health implications in near-field firefighters and emergency responders, which could include law enforcement, emergency medical technicians, and paramedics, all of whom may be at higher risk due to proximity. The discussion is divided into acute and chronic health conditions and further divided into epidemiological and toxicological findings related to wildland fires and WUI fires. Publications selected for inclusion in this section were based upon a literature search by the authors and the National Academies of Sciences, Engineering, and Medicine, and studies were selected that have clearly described health outcomes in communities and regional populations associated with smoke from wildland fires or WUI fires.
Health effect studies in the general population specific to WUI fires are extremely limited. However, researchers can learn much from the studies that identify health impacts associated with exposure of general populations to wildland fire smoke, as well as the decades of research on outdoor PM that can inform our understanding of the health
effects associated with fire-associated smoke. Key health outcomes from these studies include mortality from heart disease, chronic obstructive pulmonary disease (COPD), and respiratory disease (Malig et al., 2021). Lung cancer has not yet been identified as a health outcome of wildland fires or WUI fires for smoke-exposed community and regional populations; however, the InternationaI Agency for Research on Cancer (IARC, Group 1) and the National Cancer Institute have concluded that exposure to PM in outdoor air is carcinogenic to humans (https://dceg.cancer.gov/research/what-we-study/ambient-outdoor-matter). Moreover, a recent IARC determination that there was sufficient evidence for increased mesothelioma and bladder cancer rates in firefighters, as well as limited evidence for an additional five cancers, demonstrates the need to study these health conditions in regional populations (Demers et al., 2022).
Available data demonstrated elevated risks of emergency room visits during the 2015 wildland fire season in Northern California with specific health outcomes more prevalent, including myocardial infarction, ischemic heart disease, dysrhythmia, heart failure, pulmonary embolism, ischemic stroke, and transient ischemic attack (Wettstein et al., 2018). Studies (reviewed in Reid et al., 2016a) consistently confirm the association between wildland fire smoke exposure and some respiratory health outcomes, with the clearest evidence related to exacerbation of asthma (Gan et al., 2017). In a study by Malig et al. (2021) examining PM2.5 and morbidity during the 2017 northern San Francisco Bay wildland fires, increased PM levels were consistently linked with emergency department visits with asthma, chronic lower respiratory disease, and acute myocardial infarction; increases in acute respiratory infection and decreases in mental health/behavioral hospital visits were observed, but were sensitive to model specifications. In contrast to the preponderance of data demonstrating the association between wildland fires and asthma, the links between wildland fire smoke and both COPD and increased susceptibility to bacterial infections, including those associated with pneumonia, are not as clear (Malig et al., 2021; Reid and Maestas, 2019; Reid et al., 2016a). Studies also suggest that toxicity of PM2.5 from wildland fires is more harmful than equal concentrations of non–wildland fire PM2.5 (Aguilera et al., 2021).
Both current and past research concludes that more studies are needed to fill the gaps on population subgroups that are most vulnerable to the health implications of wildland fire smoke and the far-field respiratory health impacts of these events with high air pollution. As the pulmonary, cardiovascular, cerebrovascular, and reproductive systems appear to be most representative of the health effects associated with wildland fires, diseases associated with those target organs, as well as mental health, will be the focus of this section. In addition to acute and chronic health conditions associated with smoke exposure in the general population, delayed effects (i.e., effects that occur later, after the fire is over) have been observed. Because the committee identified only one study on delayed effects, it is grouped with chronic health studies in the section on “Chronic Conditions and Exacerbation of Disease.” It is important to note that smoke-associated PM is the primary constituent considered among all of the health studies discussed in this report. Also worth noting is the fact that comparing health effects of wildland and WUI fire events across world regions is difficult due to variation in intensity, fuel type, population, PM sources and composition, and other factors (Tinling et al., 2016).
Finding: WUI-specific studies are rare, making it extremely difficult to understand related health effects for this specific, complex type of fire. Most information about acute and chronic health conditions is based on wildland fire studies, because of the greater amount of data available.
Research need: Studies that explicitly define the particular type of fire (i.e., wildland fires vs WUI fires) to which the general population is exposed are needed to clearly delineate and possibly mitigate the types of health conditions that could emerge, as pollutant emissions (as well as toxicant concentrations) between wildland fires and WUI fires can be quite different.
Acute Conditions and Exacerbation of Disease
Epidemiological Studies
Respiratory Effects
A growing body of evidence documents an association between an exacerbation of asthma and wildland fire smoke exposure. For example, a positive association has been observed between hospitalizations, emergency department (ED) visits, and outpatient visits for asthma exacerbation and wildland fire smoke exposure (Gan et al., 2017; Hutchinson
et al., 2018; Malig et al., 2021; Reid et al., 2016a,b). Wildland fire smoke inhalation also increased the risk for asthma morbidity during the 2013 wildland fire season in Oregon (Gan et al., 2020). By contrast, however, Tinling et al. (2016) found only weak associations between wildland fire smoke exposure and asthma.
As discussed by Reid et al. (2016a,b), multiple studies have described a decrease in lung function associated with wildland fire smoke exposure among individuals without asthma or bronchial hyperreactivity. In the Wallow Fire, researchers observed an increased risk of ED visits for some respiratory and cardiovascular conditions during heavy smoke conditions, and risk varied by age and sex. The subpopulation of 65+ years of age was especially at risk for increased ED visits. The majority of epidemiology studies found that wildland fire smoke was associated with an increased risk of respiratory and cardiovascular diseases. In one study, a significantly increased risk of ED visits was identified among the 65+ population for asthma (relative rate [RR] = 1.73, 95% confidence interval [CI] = 1.03–2.93) and for diseases of the veins and lymphatic and circulatory systems (RR = 1.56, 95% CI = 1.00–2.43). For the age group of 20 to 64 years, there was an increase in ED visits for diseases of pulmonary circulation (RR = 2.64, 95% CI = 1.42–4.9) and for cerebrovascular disease (RR = 1.69, 95% CI = 1.03–2.77; Resnick et al., 2015). Additional findings suggest that PM2.5 exposure during wildland fire smoke days is more likely to trigger strong, acute responses such as asthma, bronchitis, and wheezing, compared with non-smoke days, in the older population (DeFlorio-Barker et al., 2019).
Findings from studies examining infection risk associated with exposure to wildland fire smoke are inconsistent. In a study of the impacts of Indonesian wildland fires on air pollution and health in Singapore, clinic visits for acute respiratory infections increased during weeks with high fire levels (as estimated from satellite-derived values of fire radiative power) in 2010–2016 (Sheldon and Sankaran, 2017). Alman et al. (2016) reported a borderline association for combined hospitalizations and ED visits for upper respiratory infections and PM2.5 during wildland fires in 2012 in Colorado. However, the committee found two recent studies with seven different analyses of the association between wildland fire smoke and pneumonia, of which all analyses revealed negative associations except two: (1) The analysis of outpatient presentations (but not hospitalizations or ED visits) by Hutchinson et al. (2018) found a weak relationship with infections. (2) Gan et al. (2017) reported a strong association between pneumonia hospitalizations and wildland fire smoke during the 2012 Washington state fires only when assessing exposure from kriging monitoring data, but not from an aerosol measurement or blended model. A recent study by Zhou et al. (2021) examined the relationship between increased ambient concentrations of PM2.5 from recent California wildland fires and the incidence of COVID-19 infection. The authors concluded that high particulate pollution levels were temporally associated with an increase in the incidence and mortality rates of COVID-19 after adjusting for several time-varying confounding factors such as weather, seasonality, long-term trends, mobility, and population size.
Studies investigating the association between wildland fire smoke and acute bronchitis show mixed findings, with results from a single study using temporal comparisons demonstrating an association for ED visits and outpatient presentations, but not for hospitalizations, among Medi-Cal patients in San Diego (Reid and Maestas, 2019). By contrast, a study of the 2012 Washington state wildland fires found no association between acute bronchitis hospitalizations and wildland fire smoke using three different methods to estimate smoke. In addition, no association was found for combined hospitalizations and ED visits for bronchitis during the 2012 wildland fire season in Colorado.
The null findings associated with pneumonia and bronchitis contrast with previous papers that collectively hinted at an association between wildland fire smoke and pneumonia and bronchitis. Most of the previous studies grouped pneumonia and bronchitis together rather than separating them, as is the norm in the recent studies. One earlier study that did separate pneumonia and bronchitis found a strong association between PM2.5 and pneumonia, but not acute bronchitis, during the 2003 wildland fires in Southern California (Delfino et al., 2008).
Several recent papers investigated the relationship between wildland fire smoke and all respiratory health outcomes grouped together. Studies consistently found strong associations between smoke exposure and hospitalizations, hospitalizations and ED visits combined, ED visits, and outpatient presentations (Reid and Maestas, 2019). However, findings from a few studies reported conflicting results. One of these authors noted that one of the investigations examined smoke transported long-range rather than fresh smoke, which could have a different chemical composition (Magzamen et al., 2021). For more information on smoke plume aging and composition, please see Chapter 3 of this report.
Cardiovascular Effects
A growing number of studies have implicated exposure to wildland fire smoke as a risk factor for cardiovascular disease. Of the 48 wildland fire epidemiological studies that currently exist (as of 2021; Chen et al., 2021), 38 are on cardiovascular morbidity, and most outcomes focus on ED visits and hospitalizations for cardiovascular symptoms and illness. Twenty-five of the 38 studies report a positive association between wildland fire smoke exposure and increased health care for cardiovascular disease (Chen et al., 2021). For example, Haikerwal et al. (2015) demonstrated that PM2.5 exposure was associated with increased risk of out-of-hospital cardiac arrests and ischemic heart disease during the 2006–2007 wildland fires in Victoria, Canada. The evidence indicates that PM2.5 may act as a triggering factor for acute coronary events during wildland fire episodes. In a study by Haikerwal et al. (2015), an interquartile range increase of 9.04 mg/m3 in PM2.5 over a 2-day moving average during the 2006–2007 wildland fire season in Victoria, Australia, was significantly associated with an increase in risk of out-of-hospital cardiac arrests, with the strongest associations observed among men and older adults, and was also associated with an increased risk for ischemic heart disease–related ED visits (2.07 percent) and hospitalizations (1.86 percent), particularly among women and the elderly.
While the preponderance of evidence suggests an association between cardiovascular disease and wildland fire–generated PM, a conclusive link between wildland fire smoke exposure and adverse cardiovascular effects still remains somewhat elusive. However, a recent review by Chen et al. (2021) assessing epidemiological data, controlled clinical exposure studies, and toxicological studies has concluded that wildland fire smoke–associated PM is a risk factor for adverse cardiovascular disease, especially among vulnerable populations. In addition, findings also concluded that young and healthy people may also develop biological responses including systemic inflammation and vascular activation, both associated with increased cardiovascular disease risk. Future epidemiological studies could benefit from improved exposure assessments and the implementation of more sensitive indicators of cardiovascular dysfunction. More data are also needed to accurately define the risk of cardiovascular health effects including common, life-threatening, disabling, and costly clinical outcomes that include myocardial infarction, stroke, heart failure, heart rhythm disturbances, and sudden death.
Reproductive Effects
In 2012, Kessler compared the average birth weight of infants carried in utero during wildland fires with that of infants who were either born before or conceived after the fires. The author also compared birth weights of infants exposed to wildland fire smoke during the first, second, and third trimesters of pregnancy. After adjusting for infant sex, gestational age at birth, and other factors known to influence birth weight, the researcher reported that smoke-exposed infants weighed an average of 6.1 g (0.21 oz) less at birth than unexposed infants. Infants exposed to smoke as fetuses during the second trimester of pregnancy demonstrated the largest average size reduction at 9.7 g (0.34 oz), while those exposed during the third trimester showed an average reduction of 7.0 g (0.24 oz). Alternatively, infants exposed during the first trimester showed an average reduction of 3.3 g (0.11 oz), which was no different from the control. The trends were corroborated by a sensitivity analysis that compared pregnant mothers according to whether the air-pollution monitor nearest their residence recorded high or low PM levels during the wildland fires.
Findings from O’Donnell and Behie (2015), who used data from the Australian Capital Territory and examined the influence of the 2003 Canberra wildland fires on the weight of babies born to mothers living in fire-affected regions, demonstrated heightened responsiveness in the male cohort. While this was not a direct effect of smoke exposure, the authors also showed that elevated maternal stress due to wildland fires acted to accelerate the growth of male fetuses, potentially through an elevation of maternal blood glucose levels. These studies concluded that effects of disaster exposure alter fetal growth patterns in response to maternal signals. However, the direction of the change in birth weight is opposite to that of many earlier studies. While this study has a number of limitations, the findings indicate a risk of macrosomia to exposed male infants that could pose immediate health risks to both mother and child, as well as longer-term health risks to the child.
The work of Abdo et al. (2019) supports these findings, demonstrating that exposure to wildland fire smoke, specifically smoke-associated PM2.5, over the full gestation period and during the second trimester was positively associated with preterm birth, while exposure during the first trimester was associated with decreased birth weight. In a recent systematic review by Amjad et al. (2021), the authors concluded that while some evidence existed that
maternal exposure to wildland fire smoke is associated with birth weight reduction and preterm birth, particularly when exposure occurs late in the pregnancy, based on all data, the association still remains inconclusive, despite strong evidence linking PM2.5 exposure with reduced birth weight (Sun et al., 2016).
Chronic Conditions and Exacerbation of Disease
Epidemiological Studies
Respiratory Effects
Recent data on wildland fires and COPD outcomes have caused doubt about a relationship between them, which previously had been established. Researchers observed strong associations between wildland fire smoke and COPD ED visits, but saw null results for hospitalizations during the 2008 Northern California wildland fires (Reid et al., 2016b). An analysis of the 2012 Washington state fires demonstrated an association between hospitalizations for COPD when using monitoring data or PM2.5 exposures from a model that blended monitoring, aerosol optical depth, and aerosol measurement data, but not from PM2.5 estimates derived from aerosol measurements (Gan et al., 2017). Alman et al. (2016) also reported a strong association between combined hospitalizations and ED visits for COPD and smoke-associated PM2.5 levels during the 2012 Colorado fire season. Analyses using temporal comparisons were null for outpatient visits, ED visits, and hospitalizations (Hutchinson et al., 2018), as were results from two analyses using aerosol measurement–derived PM exposures for ED visits (Haikerwal et al., 2016; Tinling et al., 2016). In a study by Hutchinson et al. (2018) that examined the health care utilization of Medi-Cal recipients during the fall 2007 San Diego wildland fires, which exposed millions of people to wildland fire smoke, young children appeared at highest risk for respiratory problems, especially asthma, which is a cause of particular concern because of the potential for long-term harm to children’s lung development. Regarding delayed effects, a study by Reid et al. (2016a) 10 years after wildland fire smoke exposure found lung function to be reduced among individuals without asthma or bronchial hyperreactivity.
Cardiovascular and Cerebrovascular Effects
Wettstein et al. (2018) conducted population-based epidemiological analyses for daily cardiovascular and cerebrovascular ED visits and wildland fire smoke exposure in 2015 among adults in eight California air basins. Findings from this study revealed elevated risks for individual diagnoses of myocardial infarction, ischemic heart disease, heart failure, dysrhythmia, and pulmonary embolism. The same study also showed that smoke exposure was associated with cerebrovascular ED visits for all adults (ischemic stroke and transient ischemic attack), particularly for those 65+ years. The authors of the study concluded that individuals with underlying cardiovascular disease risk factors may be at greater risk for a cardiovascular or cerebrovascular event during a period of wildland fire smoke exposure.
Mental Health Effects
Mental health is included in this report as recent research has shown that small increases in particulate air pollution are linked to significant rises in depression and anxiety. For example, a recent study (Petrowski et al., 2021) examining nationally representative data of German populations revealed an association between mental health and well-being and particulate air pollution. Moreover, studies have also found an increased rate of post–wildland fire mental health disorders in both adult and pediatric populations, with a number of associated risk factors, the most significant being characteristics of the wildland fire trauma itself. A recent study by To et al. (2021) demonstrated that direct exposure to large-scale fires significantly increased the risk for mental health disorders, particularly for post-traumatic stress disorder, depression, and generalized anxiety, at several follow-up times after the wildland fire, from the subacute phase to years after.
Brown et al. (2019) examined mental health in children following the Fort McMurray fire in Alberta, Canada, and noted a high incidence of post-traumatic stress disorder, depression, anxiety, and alcohol- or substance-abuse disorders. The authors concluded that disasters have a negative impact on the mental health of youth, particularly those who directly experienced fires. However, they also noted the role of resilience on mental health among this group, with lower resilience associated with substantially lower mental health outcomes. A follow-up study by some
of the same authors (Brown et al., 2021) following the Fort McMurray fire not only validated their first study, but showed that mental health issues worsened rather than improved over time. Moreover, the authors observed higher levels of mental health distress among older students, in females compared to male students, and in individuals with a minority gender identity, including transgender and gender-nonconforming individuals. These follow-up findings illustrate that deleterious mental health effects can persist in youth for years following a fire disaster and therefore are critical to discuss in this report.
Controlled Human Exposure Studies
This section discusses controlled human wood-smoke exposure studies, in concert with in vivo animal studies, to complement the wildland fire studies in this report. Controlled human exposure studies complement the cardiovascular mortality and morbidity observations in epidemiology as they offer a chance to examine the associated pathophysiological changes. While wood smoke used for clinical and experimental studies does not entirely reflect smoke from a wildland fire or WUI fire, chamber studies do allow for a better understanding of mechanisms underlying observed health effects. Moreover, low or moderate exercise can be introduced in the study protocols to increase the ventilatory rate to simulate physical activity in the vicinity of a wildland fire.
Most human wood-smoke exposure studies conducted to date have investigated pulmonary function, respiratory inflammation, systemic inflammatory responses, and cardiovascular endpoints or markers related to vascular pathophysiology. In one study (Andersen et al., 2017), 43 subjects participated in various training exercises that included activities to extinguish fires fueled by either wood alone or by wood and household materials (a mattress). They found that firefighting activity was associated with decreased heart rate variability and microvascular function measured as reactive hyperemia index pressure. While no definitive conclusions can be reached in these types of studies due to differences in such factors as wood types and duration of exposure, the overall outcomes support the positive cardiopulmonary findings observed in wildland fire epidemiological studies.
In Vivo Toxicology Studies
While humans best represent themselves for identifying contaminant-associated health effects, studies using animal models provide biological plausibility for the associations revealed in epidemiological studies, as well as provide a mechanistic understanding for such observed effects. Several studies have shown that exposure to wood smoke leads to increased cardiovascular risk in animals (reviewed in Chen et al., 2021). For example, Kim and colleagues (2014) established an in vivo model wherein female CD-1 mice were exposed through oropharyngeal aspiration to 100 mg peat smoke condensate from different combustion stages (smoldering vs near extinguished). Mice exposed to smoke produced during the smoldering stage revealed significantly decreased cardiac function and increased post-ischemic cardiac death in an experimentally induced ischemia model. Animal studies have shown that the toxicity of wood smoke depends on the wood type, as well as the combustion conditions, with wood smoke from smoldering wood producing fewer effects relative to smoke produced by the burning of specific wood types.
In a study by Black et al. (2017), 3-year-old macaque monkeys were housed in outdoor facilities at the California National Primate Research Center and exposed to California wildland fire smoke during pregnancy and in the first 3 years of life. Adolescent monkeys demonstrated reduced lung function and long-term immune alterations dependent on sex. The authors concluded that modulation of peripheral blood cytokine synthesis and altered later-in-life lung function was significantly associated with early-life wildland fire smoke exposure (Black et al., 2017). These results support the findings by Orr et al. (2020) which show that initial smoke exposure can lead to health effects in subsequent years. Overall, in vivo animal studies are challenging to interpret in a clinical context, as exposure dose and duration may be difficult to compare with real-world conditions impacting public health. However, as previously stated, these studies provide plausibility for epidemiological studies demonstrating wildland fire–induced respiratory dysfunction, as well as insight into underlying mechanisms.
Finding: Particulate matter is the primary metric related to health outcomes in almost all existing studies on wildland fire and WUI fire smoke.
Research need: Further studies are critical to understanding whether physiological and psychological chronic health disorders associated with regional exposures among the general public are similar for WUI and wildland fires.
Research need: Additional studies are needed to evaluate the health implications of wildland fire and WUI fire smoke constituents other than PM, including volatile organic compounds, semi-volatile organic compounds, and polycyclic aromatic compounds.
Research need: A need exists to better understand the persistent and delayed effects of smoke exposures, especially for far-field community and regional populations.
Research need: A need exists to better understand the effects of smoke exposures to WUI fire components, which may include biomonitoring studies of general populations and vulnerable subpopulations.
Firefighter Acute Exposures and Effects
Although ongoing research exists on WUI firefighter acute exposures and health effects, the committee found no published studies specific to WUI fires. A limited amount of information is available on acute exposures and health effects for wildland firefighters, with additional data available on structural firefighters from municipal fire departments. Measurement of urinary hydroxylated metabolites of PAHs has been used for the assessment of exposure to combustion products (Fent et al., 2020; Keir et al., 2017). Among PAHs, the known, probable, and possible carcinogens include benzo[a]pyrene, dibenz[a,h]anthracene, chrysene, benzo[a]anthracene, and naphthalene (IARC, 2010). Evaluation of PAH metabolites in urine also provides a biological measure of combined inhalation and dermal exposure.
Wildland Firefighters
Wildland firefighters are exposed to carcinogens including benzene, formaldehyde, and PAHs (Broyles, 2013; Reinhardt and Ottmar, 2004; Ward and Hardy, 1991). More research studies have been published on prescribed burns than on larger campaign fires. Researchers have found urinary PAH metabolites to be elevated in wildland firefighters after a prescribed burn (Adetona et al., 2017a). However, firefighters can minimize their exposures during certain types of prescribed burns by avoiding smoke plumes. For example, in a study of Bureau of Indian Affairs/Fort Apache Agency wildland firefighters before, during, and after conducting pile burns (prescribed fires), despite finding 20 of the 21 PAHs analyzed in area (smoke plume) samples, researchers found only 3 (naphthalene, phenanthrene, and fluorine) of the 16 PAHs analyzed in personal exposures, based on the ability of the firefighters to move away from the smoke, and there were no significant changes in urinary 1-hydroxypyrene concentrations (Robinson et al., 2008). Urinary methoxyphenols have been used to evaluate exposure to wood smoke (Dills et al., 2006). In US wildland firefighters, PAH DNA adducts were associated with diet, but not occupational exposure (Rothman et al., 1993).
Wildland firefighting is known to be associated with acute adverse health effects. Previous studies of wildland firefighters have recorded cross-seasonal changes in lung function (Gaughan et al., 2008; Liu et al., 1991; Rothman et al., 1991), and decreases in lung function have been associated with hours of firefighting activity (Rothman et al., 1991) and continuous exposure to wood smoke (Adetona et al., 2011). Additionally, several studies have measured elevated inflammation and oxidative stress among wildland firefighters after prescribed burns (Adetona et al., 2017b, 2019) and wildland fires (Main et al., 2020). Inflammation and oxidative stress are known risk factors for cancer (Coussens and Werb, 2002; Reuter et al., 2010).
Structural Firefighters
Among structural firefighters, exposure during the overhaul phase (the phase after the main fire has been extinguished, during which firefighters search a fire scene to detect hidden fires or smoldering areas that may rekindle) increased lung inflammation in firefighters wearing multipurpose (high-efficiency particulate, acid gas, and organic vapor) air-purifying respirators, which suggested inadequate protection offered by the air-purifying respirators
(Burgess et al., 2001). Air-purifying respirators can provide protection against many products of combustion at concentrations relevant to overhaul, although formaldehyde may break through under certain conditions, particularly at elevated ambient temperatures (Jones et al., 2015; Staack et al., 2021). Fent et al. (2014) evaluated exposures in structure fires during controlled burns when firefighters wore self-contained breathing apparatus for all phases including overhaul (Fent et al., 2014). Within this study, dermal swabs of skin surfaces that were collected before and after the fires showed that the neck was the most exposed part of the body. The results also showed an increase in urinary PAH metabolites 3 hours after the fire response. Kirk and Logan (2015) also analyzed firefighting ensembles for deposition and off-gassing of contaminants following controlled burns and found VOCs, carbonyl compounds, PAHs, and hydrogen cyanide off-gassing from the gear. They determined that deposition of contaminants on firefighting ensembles is cumulative, and that laundering reduced contamination to pre-exposure levels.
One potential mechanism of acute toxicity following exposures among structural firefighters is activation of the aryl hydrocarbon receptor (Beitel et al., 2020). This activation is reportedly the same toxic mechanism by which dioxin causes cancer, and the aryl hydrocarbon receptor is also a potential target for cancer chemotherapy (Kolluri et al., 2017).
Firefighter Chronic Effects
As with acute exposures and health effects, although there is ongoing research on WUI firefighter chronic health effects, the committee found no published studies specific to WUI fires. Limited information is available on chronic health effects from smoke exposure for wildland firefighters, with additional data available from municipal fire departments. Researchers have linked PAH exposures to a number of cancers, including skin, lung, bladder, and gastrointestinal cancers (Boffetta et al., 1997; Diggs et al., 2011; Rota et al., 2014). Research has identified elevated levels of persistent organic contaminants, such as PCDD/Fs, associated with cancer and other adverse chronic health effects in California firefighters (Shaw et al., 2013).
Wildland Firefighters
A survey study associated the employment duration of wildland firefighters with a history of being diagnosed with hypertension and arrhythmias (Semmens et al., 2016). Wildland firefighters have an estimated increased risk of lung cancer mortality and cardiovascular disease (Navarro et al., 2019). To our knowledge, no epidemiological studies of cancer in wildland firefighters have been published.
Structural Firefighters
Cancer is a leading cause of mortality and morbidity in the municipal fire service. The National Institute for Occupational Safety and Health (NIOSH) study of Philadelphia, Chicago, and San Francisco firefighters demonstrated a 14 percent increase in overall cancer mortality compared to the general population, and specific excesses in lung (10%), gastrointestinal (30–45%), kidney (29%), and mesothelioma (100%) cancer deaths, with similar increases in cancer incidence (Daniels et al., 2014). In Australian volunteer firefighters, prostate cancer was increased compared to the general population, and kidney cancer increased with the number of fire exposures (Glass et al., 2016). Among female firefighters, colorectal cancer increased with the increasing number of fire responses. A study of cancer among firefighters in five Nordic countries found a significant excess risk of prostate cancer and melanoma among those 30–49 years of age, as well as an increase in non-melanoma skin cancer, multiple myeloma, lung adenocarcinoma, and mesothelioma among older firefighters (Pukkala et al., 2014). A previous meta-analysis of 32 studies of cancer in the fire service found an elevated risk for non-Hodgkin’s lymphoma, prostate cancer, and testicular cancer (LeMasters et al., 2006).
Cancer is a multistage process with a latency period between exposure and the onset of disease from as short as 5 to over 30 years (Nadler and Zurbenko, 2014). Previous firefighter studies have shown limited evidence of direct DNA damage (change in DNA sequence) as a result of occupational exposure. A study of structural firefighters in India found increased buccal cell micronuclei compared with controls (Ray et al., 2005). Beyond direct DNA damage, advances in technology have led to a greater appreciation of the role of epigenetic (not involving a change in DNA sequence) contributions to carcinogenesis: epigenetic markers are known to have important roles
in carcinogenesis. Key among these are DNA methylation and miRNA expression, which researchers have shown to be different in incumbent and new-recruit structural firefighters (Jeong et al., 2018; Zhou et al., 2019) and which change over time in new recruits (Jung et al., 2021). Numerous studies have shown how DNA methylation (Dugue et al., 2021; Jaenisch and Bird, 2003; Jones and Laird, 1999; Onwuka et al., 2020; Wang et al., 2010) and miRNA expression (Calin and Croce, 2006; Carter et al., 2017) are associated with cancers.
Finding: Insufficient research exists on acute exposures and acute and chronic health effects in WUI firefighters.
REDUCING EXPOSURE RISKS AND HEALTH EFFECTS
This section focuses primarily on reducing the risk of smoke (inhalation) exposure and its effects. However, dermal and ingestion exposures are also a concern, particularly in the near field, that can be reduced through actions discussed in this section. Mitigation opportunities at a structural level to reduce the incidence of WUI fires, such as adjusting land-use policy, also exist; these are not discussed because the scope of this report is focused on chemistry.
Reducing Near-Field Exposure Risks
This section discusses actions that reduce near-field exposure for the general public in the evacuation zone and for firefighters working in close proximity. While there is a range of individual and community actions (or interventions; e.g., use of portable air cleaners, wearing of N95 masks [see Box 6-2]) to mitigate fire smoke exposure (EPA, 2021f; Xu et al, 2020), there is limited information about the effectiveness of their use during wildland and WUI fires (EPA, 2021f). Information is also lacking about best practices by residents to reduce their exposures upon reentry post-fire. These limitations are underscored by the lack of comprehensive information about fire emissions specific to WUI fires, such as the chemical composition of PM and pollutants that may not be monitored in targeted analyses.
Evacuation
While no data sets systematically track the occurrence of emergency evacuations or other exposure reduction actions for wildland fires (CCST, 2020), data specific to state and fire incidents are available. For example, CCST (2020) noted one study estimated that 1.1 million people were ordered to evacuate during 11 major wildland fires between 2017 and 2019 in California (Wong et al., 2020) with non-compliance to mandatory evacuation orders for three wildland fires in California ranging from 3 to 13 percent of the population (Wong et al., 2020). Similar results
have been observed in other studies. In the western United States, 11–20 percent of survey respondents who resided in areas within or adjacent to perimeters of recent wildland fires and/or were under evacuation orders did not evacuate during the fires (Kuligowski, 2021; Kuligowski et al., 2022; McCaffrey et al., 2018), while a similar 9–10 percent of survey respondents reported an intention to stay and defend property regardless of authorities’ evacuation orders in cases of future wildland fires (Edgeley and Paveglio, 2019; Mozumder et al., 2008; Paveglio et al., 2014; Stasiewicz and Paveglio, 2021).
In a study conducted in New Mexico, 89 percent of survey respondents reported that they would evacuate under mandatory orders compared to 57 percent under voluntary ones (Mozumder et al., 2008). Nonetheless, the implementation of mandatory evacuation orders and the enforcement of penalties for disobeying such orders, if any exist, are inconsistent across the country, and WUI fire–specific data are largely unavailable (Kuligowski, 2021; Mozumder et al., 2008). Even without research, WUI fire evacuation planning can benefit from the availability and use of contemporaneous real-time collection of data about evacuation decisions or progress, such as location data from cellular information (Melendez et al., 2021). But the inadequacy of communication and transport infrastructure or their degradation by wildland fire activities can impair the availability of such data and the evacuation performance (Cova et al., 2011; Kuligowski, 2021). In addition, evacuation is not always the best safety decision, and evacuation that is delayed or made under congested traffic conditions can result in catastrophic unintended consequences including death (Cova et al., 2011; Kuligowski, 2021; Li et al., 2019; McLennan et al., 2018).
Reentry Exposure Risk and Mitigation
Exposure to lingering smoke and ash from a fire after WUI residents are allowed to return to their homes can cause significant health effects. Guidance provided by NIOSH and other agencies provides general information on health and safety hazards for homeowners and environmental remediation workers after the area is declared safe for reentry. According to NIOSH, these activities may pose health and safety hazards that require necessary precautions, and in most cases, it may be more appropriate for professional cleanup and disaster restoration companies, rather than homeowners or volunteers, to conduct this work (NIOSH, 2019b).
Cleanup recovery workers undertake demanding and often dangerous work to remove debris and demolish damaged structures. Many immigrants make up this recovery workforce because of their substantial representation in the formal and informal construction sectors (Eckstein and Peri, 2018). Related research on immigrant experiences with cleanup and reconstruction work illustrates the many risk factors that make these workers vulnerable to hazardous work conditions and exploitation (Vinck et al., 2009). Despite this, specific research on vulnerable populations and workers in WUI fire–affected areas is sparse. One resource that extends education and training to those responding to disaster events is the National Institute of Environmental Health Sciences Worker Training Program, which funds a network of labor organizations, worker centers, and university-based programs (NIEHS, 2021b).
One survey conducted by a community-based organization in Southern California surveyed 195 blue collar workers in the area following the 2018 Woolsey Fire (house cleaners, childcare providers, gardeners, construction workers, and caregivers to the elderly) to learn how their work was shaped by the fire and to document the consequent health, safety, and economic impacts. Some domestic workers reported engaging in fire cleanup tasks, such as cleaning ash and debris that thickly coated furniture inside homes that were adjacent to fully burned structures, and respondents indicated that employers provided little more than simple face masks to carry out dangerous tasks (IDEPSCA, 2020).
Research need: Research is needed to better identify at-risk and vulnerable residents and workers affected by near-field WUI fires, and to identify culturally appropriate opportunities for interventions to reduce adverse health impacts.
Reducing Exposure Risk and Health Effects for Firefighters
Potential mitigation interventions for wildland firefighters are grouped into dermal, inhalation, mixed, and administrative categories (Table 6-3). Dermal interventions include directly removing soot from the skin and more
TABLE 6-3 Potential Interventions to Reduce Exposures and Health Effects in Wildland Firefighters
| Dermal | Take shower after operational period, or use skin wipes when shower not available |
| Carry clean change of clothes for after operational period if not returning to base camp | |
| Prevent contamination of backpack (14-day bag with personal items) contents using sealed, impervious bags | |
| Use improved wildland turnout gear to reduce dermal exposure | |
| Inhalation | Use respiratory protection if you are a vehicle driver / pump operator |
| Provide exposure monitoring equipment to firefighters, when appropriate, to help them identify and avoid inhalation hazards (implement with support of safety officers on incidents and risk management personnel at land agencies) | |
| Change cabin air filters in fire department apparatus | |
| Mixed | Clean tents and sleeping bags after each assignment |
| Implement clean cab protocol | |
| Administrative | Use job rotations to reduce exposures (fire incident management personnel can rotate and reassign crews and resources after completing job tasks associated with higher smoke exposures to job tasks that have lower expected smoke exposures) |
| Allow firefighters to patrol for spots rather than stand stationary on the fireline |
frequently cleaning dirty gear. Wildland firefighting gear is different from municipal turnout gear, being constructed of lighter materials. Many wildland firefighters continue to wear dirty gear for multiple shifts in a row during a campaign fire, although recent changes in some departments encourage cleaning after each shift. The wildland firefighter interventions shown in Table 6-3 may also apply to WUI firefighters.
By early 2022, some US wildland departments expected to have new personal protective equipment with a built-in protective barrier to help reduce skin exposure. They are also working on decontamination protocols for wildland firefighters, focused on dermal post-fire decontamination, and a clean cab protocol for wildland firefighting. Researchers have shown that the use of air-purifying respirators reduces respiratory symptoms in wildland firefighters in Australia (De Vos et al., 2009).
Research need: A need exists for research on the effectiveness of interventions to mitigate WUI firefighter smoke exposures and the associated adverse health effects.
A limited number of published studies are available evaluating exposure reduction interventions in municipal firefighters. A study (Hoppe-Jones et al., 2021) measured urinary PAH metabolites (naphthols, phenanthrols, fluorenols, and 1-hydroxypyrene) in over 140 municipal fire department personnel at a baseline and 2 hours after completing their fireground responses. Contrary to expectations, the exposure was similar in engineers and paramedics at the scene as compared to the fire attack teams, which may be explained by exposure to smoke from the fire and diesel exhaust from fire service vehicles coupled with the nonuse of respiratory protection. Furthermore, the study found that interior responses (as contrasted to exterior responses), smoke odor on the skin after showering, and a lack of recent (greater than 1 month) laundering or changing of hoods were all significantly associated with an increased level of urinary PAH metabolites.
Based on these study findings, the fire department chose to test interventions to reduce fireground exposure, including the use of self-contained breathing apparatuses by engineers, washing procedures for the entry team prior to doffing gear at the fire scene, the isolation of contaminated equipment, and personnel showering and the washing of gear upon return to the station (Burgess et al., 2020). Compared to exposures in the pre-intervention period, the interventions significantly reduced the mean total post-fire urinary PAH metabolite level in engineers (−40.4%, 95% CI = −63.9%, −2.3%) and firefighters (−36.2%, 95% CI = −56.7%, −6.0%).
The potential effectiveness of skin hygiene intervention for the reduction of exposure at wildland fires was also demonstrated by Cherry et al. (2021). They observed that the reduction in urinary 1-hydroxypyrene excretion from immediately post-shift to the following morning among firefighters with confirmed hand PAH contamination was
more than six times higher among those who followed the intervention, including a change of clothes immediately after firefighting and returning to base, washing of firefighting clothes, and showering (Cherry et al., 2021). While reported opportunities for engaging in skin hygiene while deployed to the Fort McMurray WUI fire were associated with reduced urinary 1-hydroxypyrene, samples were collected at least 37 days after deployment, which is potentially longer than the half-life of the biomarker (Cherry et al., 2019).
Reducing Regional Exposures
Communities face a range of potential exposures from air, water, and ash or soil deposition. However, the health effects of smoke inhalation, and ways to mitigate risk, are the most widely studied exposures at this time. Smoke from large fires can spread over thousands of square kilometers, potentially affecting the air breathed by millions of people. While people can take numerous actions to reduce exposure to smoke, a large degree of variability exists in the efficacy of each (Laumbach, 2019; Xu et al., 2020). Table 6-4 lists some interventions.
TABLE 6-4 Potential Interventions to Reduce Exposures and Health Effects in Communities
| Inhalation | Reduce activity level and time outdoors. Follow any state or municipality guidance levels or standards for acceptable exposure to smoke, such as the threshold of 151 mg/m3 or less of PM2.5, as provided in California (by the California Division of Occupational Safety and Health) for outdoor workers. |
| Consider wearing a respirator outdoors, or a properly fitted N95 or P100 mask. Standard dust or surgical masks do not keep out fire smoke. Make sure the mask fits as recommended by the manufacturer. | |
| If you are traveling in a vehicle, close the windows and doors and run the air system in recirculation mode. | |
| Stay indoors with windows and doors closed, and use an HVAC system in recirculation mode, not bringing in any outdoor air. Use the highest rated minimum efficiency reporting value (MERV) filter in the HVAC system, with a MERV 13 recommended. | |
| Use indoor air cleaners (if available) that contain a high-efficiency particulate air (HEPA) filter for fine particle removal. If the option is available, add a charcoal filter for chemical collection. Place air cleaners in primary living and sleeping areas and ensure that the air cleaner has Association of Home Appliance Manufacturers approval with an appropriately sized clean air delivery rate provided. Do not use ozone-generating air cleaners, since ozone is a strong pulmonary irritant. Other air cleaners may release unintentional ozone during operation; thus, select only products that meet California’s Air Cleaner Regulation AB 2276 of not releasing more than 0.05 ppm ozone (CARB, 2008). | |
| If retail air cleaners are not available or are economically prohibitive, consider using a DIY air cleaner consisting of a simple box fan with an attached HVAC filter. Follow assembly and safe operating instructions (Underwriters Laboratories, 2021). | |
| Keep the indoor space clean by wiping all surfaces with an antistatic or damp cloth. Use a HEPA vacuum to clean surfaces and upholstered furniture. | |
| Consider using PM2.5 personal devices or real-time air monitors for measuring indoor levels, so that mitigative strategies including air cleaning/filtration can be used for high PM measurement events. | |
| Reduce PM2.5 generation indoors by limiting the use of chemical cleaners and aerosols, air fresheners, gas cooking, and processes like frying. | |
| Locate indoor “safe air spaces” provided by the community, especially for vulnerable populations. These may include specially prepared spaces like sports arenas, theaters, and shopping malls. | |
| When the outdoor air becomes safer, consider “airing out” your space by opening windows and doors and providing as much air circulation as possible. EPA’s AirNow Fire and Smoke map (https://fire.airnow.gov/) is a source of real-time air quality and fire information that can be used to identify when outdoor air quality has improved. | |
| Dermal/Ingestion | Keep the indoor space clean and reduce indoor dust by using air cleaners and wiping all surfaces with a static-free or damp cloth. If available, use a HEPA vacuum to clean all surfaces including flooring, countertops, shelving, and upholstered furniture. |
| Wash hands frequently, especially those of children who have frequent hand-to-mouth activity. | |
| Consider treatment/filtration of drinking water to remove particles and chemical contamination from fire emissions or thermally degraded water lines. |
Reducing Indoor Exposure
EPA (2021f) describes means of reducing smoke, particularly PM2.5 exposure, and the impacts of interventions; selected text follows:
The primary focus for several actions is reducing indoor PM2.5 concentrations while at home where people spend most of their time. Housing characteristics, such as age of the home and presence and type of HVAC system, influence the infiltration of particles indoors under normal conditions, and also influence the efficacy and availability of these actions for reducing smoke exposures in homes (Davison et al., 2021; EPA, 2020; Joseph et al., 2020). Therefore, housing characteristics of the geographic area impacted by smoke is another important factor, and if variability in the housing stock is not accounted for in some way then estimates of exposure reduction could be under- or overestimated. . . .
EPA (2018) reviewed residential measurement studies that used portable air cleaners and central HVAC system filters to reduce indoor PM2.5 exposures overall, not PM2.5 specific to wildfire smoke. Portable air cleaners were found to substantially reduce indoor concentrations of PM of both indoor and outdoor origin, often reducing indoor PM2.5 concentrations by around 50% on average. . . .
EPA (2018) also noted a few residential measurement studies that showed higher efficiency central HVAC system filters such as those rated minimum efficiency reporting value (MERV) 13 or above can reduce indoor PM2.5 concentrations. Singer et al. (2017) reported a 90% reduction in PM2.5 using HVAC filtration with high efficiency MERV filters in a single test house in California during typical ambient PM2.5 concentrations, which was comparable to running a portable air cleaner in the home. However, results from a recent study by Alavy and Siegel (2020) showed actual in-home effectiveness of HVAC filtration for PM2.5 was much lower (average ~40%) and varied widely across homes even for filters with the same MERV rating depending on the home. Filter performance was strongly linked to home- and system-specific parameters including ventilation rate and system run time.
Of the studies evaluated, Reisen et al. (2019) is the only available residential measurement study that examined the effectiveness of closing windows and doors during a smoke event. However, the study only included four homes in Australia that experienced smoke due to a prescribed fire. Simple infiltration modeling of the measurements showed that remaining indoors with windows and doors closed reduced exposure to peak PM2.5 concentrations by 29 to 76% across the homes and that a tighter house, in terms of reduced ventilation, provided greater protection against particle infiltration. (EPA, 2021f)
Most of the previous research has focused on achieving PM reductions indoors; however, WUI fires may emit a wide variety of chemical compounds, and very little is known about the infiltration of these compounds indoors and effective air cleaning approaches. Recent work by Ye et al. (2021) focused on evaluating VOC air cleaning technologies for a range of compounds. They observed a wide variety of reduction rates across appliances and for different compounds. They also observed that some air cleaners themselves were a source of VOC emissions and in some cases their usage led to the formation of oxidized by-products. Further research is needed to identify air cleaning technology that can be used to mitigate exposure to VOCs and other WUI fire smoke compounds.
Research need: A need exists to identify the air cleaning and exposure reduction approaches that are effective at reducing the concentrations of WUI fire compounds other than particulate matter.
Finally, making spaces with cleaner air available during the day can provide an alternative for people unable to reduce smoke levels in their homes, especially vulnerable populations. Public health official guidance describes opportunities to provide such public “safe air spaces” with cleaner air than outdoors (EPA, 2019). These spaces could include schools, senior centers, libraries, and shopping malls, as long as adequate filtration is used, such as a MERV 13 or higher filter in the HVAC system or an adequately sized portable air cleaner with HEPA filtration. However, information about the efficacy of this type of intervention is not available.
Standards/Guidance for Outdoor Workers and Communities
In addition to the workers who are directly involved with wildland fire management and suppression, workers are engaged in supporting the fire response (e.g., at base camp or evacuation centers) or in cleanup efforts
TABLE 6-5 Occupational Wildland Fire Smoke Standards
| Jurisdiction | Threshold Value or PM2.5 Concentration | Action |
|---|---|---|
| State of California | AQI ≥ 151 (55.5 mg/m3) | Implement engineering and administrative controls; provide respirators for voluntary use |
| AQI ≥ 500 (500.4 mg/m3) | Require respirator use | |
| State of Oregon | AQI ≥ 101 (35.5 mg/m3) | Develop training and communication programs; provide respirators for voluntary use |
| AQI ≥ 201 (150.5 mg/m3) | Implement engineering and administrative controls; require respirator use | |
| AQI ≥ 501 (500.4 mg/m3) | Require respirator use; implement a respiratory protection program | |
| State of Washington | 20.5 mg/m3 | Develop information and hazard communication plan; encourage use of exposure controls |
| 55.5 mg/m3 | Implement engineering and administrative controls; provide respirators for voluntary use at no cost |
SOURCE: Table adapted from EPA, 2022b.
(e.g., demolition crews). Many other workers continue to do their usual non-fire-related outdoor jobs, such as agricultural workers, landscapers, utility workers, and park personnel, during an incident (EPA, 2021e). OSHA is the regulatory entity for employee health and safety, but in about half of US states, an OSHA-approved state program regulates nonfederal workplaces.
Currently, three occupational standards specifically for wildland fire smoke exist in the United States (Table 6-5). On July 18, 2019, the California Safety and Health Standards Board adopted an emergency regulation for a California Division of Occupational Safety and Health standard to protect workers from hazards associated with wildland fire smoke (Navarro, 2020), which was revised and readopted in 2020 (Cal/OSHA, 2020). The State of Washington adopted a temporary rule in July 2021, and Oregon adopted a temporary rule in August 2021 (Oregon DCBS, 2021; State of Washington, 2021). Common features of these three rules include use of threshold AQI or PM2.5 values for smoke exposure reduction actions; exemption of some workplaces, such as workplaces involved in emergency response; use of direct-read PM2.5 monitors for ambient measurements; and stipulations for instrument accuracy and operation. To date, recommended standards and guidelines address particulate emissions (PM2.5) only, and not emissions of chemicals or combustion gases.
Although no specific federal occupational standards for wildland fire smoke exist, federal occupational standards do exist for total dust and specific chemicals like benzene. These standards for toxic and hazardous substances are included in OSHA standard 19CFR1910 and include levels for long- and short-term exposure periods for work/industrial environments. These occupational standards are not applicable in nonindustrial environments or among the general public, for example, in schools, homes, or recreational spaces, where vulnerable populations exist. In these unregulated environments, guidance is often provided by organizations related to healthy buildings and healthy indoor environments. Key sources of such guidance are voluntary ASHRAE Standards (ASHRAE, 2020, n.d.).
Reducing Other Routes of Exposure
While interventions to mitigate dermal exposure to firefighters working at wildland fires have been studied, the committee found no published studies related to mitigation to reduce dermal exposure to contaminants in other outdoor workers, fire recovery (cleanup) workers, and the general population. While there are engineering, administrative, or personal protective equipment controls that are potentially applicable to prevent and mitigate dermal exposure, there is a lack of published empirical evidence in this area. Individual fire incident reports, work-site monitoring data, and information from occupational safety agencies may provide opportunities for future epidemiological research and recommended mitigations to prevent potential exposure and protect worker health.
No published studies are available on specific interventions designed to mitigate ingestion of contaminants related to WUI fires. Ingestion of contaminants emitted in fire smoke is most likely to result from post-fire exposure to contaminated water, either through fire emissions or leached chemicals from thermally degraded components of water systems. Therefore, increased monitoring, reporting, and potential treatment of drinking water for such contaminants has the potential to mitigate this exposure route. Ingestion may also be possible through dust- and ash-borne contaminants at homes or other indoor settings, depending on the scope of the post-fire remediation activities performed. Reducing indoor dust may mitigate potential ingestion of WUI fire–related contaminants.
Health Risk Communication
Risk communication is critical for minimizing harm to residents affected by any disaster. Studies on reducing human smoke exposure for all types of major fires have mostly been conducted through retrospective surveys of communities. Surveys have focused on determining awareness of smoke through health risk communications such as public service announcements and tying those health communication methods to any resulting action by a community or individual (Kolbe and Gilchrist, 2009; Mott et al., 2002; Sugerman et al., 2012). However, risk communication can help only to some extent. For example, while staying indoors is often advised by public health authorities to reduce exposure to regional smoke, staying indoors is not possible for people who have to work or travel outdoors during fire events, and people experiencing homelessness.
Reviews by Xu et al. (2020) and Laumbach (2019) have found that engineering controls such as closing windows and doors or indoor air filtration can be effective (20–80 percent exposure reduction), as can administrative controls such as staying indoors and avoiding outdoor activities (~50 percent exposure reduction). These reviews and studies are limited by not clearly differentiating WUI and non-WUI fires, and by having limited information on the accessibility of exposure reduction actions (e.g., portable air cleaners) for vulnerable populations, such as low-income communities.
Findings on the effectiveness of risk communication concerning fires also vary by study location, population, source of the communication, and levels of language- and culturally appropriate information. For example, if local radio and television broadcast disaster communications only in English, immigrants with limited English proficiency are language isolated. Studies show that Hispanic immigrants, especially those who do not speak or understand English well and who lack legal status, are less likely to be prepared for an emergency event (Burke et al., 2012; Eisenman et al., 2009). Trusted sources of information about health risks may come from community-based organizations and trusted social networks in some areas.
Health care providers also play a critical role in advising patients on actions they can take to reduce exposure related to fires. EPA provides a training endorsed by the Centers for Disease Control and Prevention (https://www.epa.gov/wildfire-smoke-course) for health care providers to better advise their patients on actions they can take before and during a fire to reduce exposure. The training includes information to help providers identify groups at greater risk from particle pollution in fire smoke and information on how to use the AQI to advise patients on how to reduce exposure and protect their health during periods of fire smoke.
CONCLUSION
This chapter on exposures, adverse health effects, and mitigation provides an overview of the human impacts of WUI fires at spatial scales from the immediate up to the continental level. Many chemicals of concern for human health are generated in WUI fires and, through a variety of exposure routes, can be introduced to different populations. Some populations are more vulnerable to the impacts of WUI fire exposure than others, for a variety of reasons discussed here. There is limited information available on health effects that is specific to WUI fire exposure; therefore, the chapter takes an expanded look at what is known about chronic and acute health effects in the general population and for firefighters for the more well-studied cases of wildland fires and structural fires. Finally, the chapter presents some ways to reduce exposures that lead to health effects.
An important common thread runs through the narrative: the need for more research specific to WUI fires. The committee hypothesizes that some conclusions can be drawn from what is known about wildland fires and structural fires.
Still, the complexity and heterogeneity that is characteristic of WUI fires make them difficult yet important to study directly. The committee’s examination of the issues in this chapter led them to identify several findings as well as crucial research needs, which are highlighted throughout and reiterated in Chapter 8.
REFERENCES
Abdo, M., I. Ward, K. O’Dell, B. Ford, J. R. Pierce, E. V. Fischer, and J. L. Crooks. 2019. “Impact of Wildfire Smoke on Adverse Pregnancy Outcomes in Colorado, 2007–2015.” International Journal of Environmental Research and Public Health 19. https://doi.org/10.3390%2Fijerph16193720.
Adachi, K., A. J. Sedlacek III, L. Kleinman, S. R. Springston, J. Wang, D. Chand, J. M. Hubbe, J. E. Shilling, T. B. Onasch, T. Kinase, K. Sakata, Y. Takahashi, and P. R. Buseck. 2019. “Spherical Tarball Particles Form through Rapid Chemical and Physical Changes of Organic Matter in Biomass-Burning Smoke. Proceedings of the National Academy of Sciences 116 (39): 19336–19341. https://doi.org/10.1073/pnas.1900129116.
Adetona, O., D. B. Hall, and L. P. Naeher. 2011. “Lung Function Changes in Wildland Firefighters Working at Prescribed Burns.” Inhalation Toxicology 23 (13). https://doi.org/10.3109/08958378.2011.617790.
Adetona, O., C. D. Simpson, Z. Li, A. Sjodin, A. M. Calafat, and L. P. Naeher. 2017a. “Hydroxylated Polycyclic Aromatic Hydrocarbons as Biomarkers of Exposure to Wood Smoke in Wildland Firefighters.” Journal of Exposure Science and Environmental Epidemiology 27 (1): 78–83. https://doi.org/10.1038/jes.2015.75.
Adetona, A. M., O. Adetona, R. M. Gogal Jr., D. Diaz-Sanchez, S. L. Rathbun, and L. P. Naeher. 2017b. “Impact of Work Task-Related Acute Occupational Smoke Exposures on Select Proinflammatory Immune Parameters in Wildland Firefighters.” Journal of Occupational and Environmental Medicine 59 (7): 679–690. https://doi.org/10.1097/JOM.0000000000001053.
Adetona, A. M., W. K. Martin, S. H. Warren, N. M. Hanley, O. Adetona, J. J. Zhang, C. Simpson, M. Paulsen, S. Rathbun, J. S. Wang, D. M. DeMarini, and L. P. Naeher. 2019. “Urinary Mutagenicity and Other Biomarkers of Occupational Smoke Exposure of Wildland Firefighters and Oxidative Stress.” Inhalation Toxicology 31 (2): 73–87. https://doi.org/10.1080/08958378.2019.1600079.
Aguilera, R., T. Corringham, A. Gershunov, and T. Benmarhnia. 2021. “Wildfire Smoke Impacts Respiratory Health More Than Fine Particles from Other Sources: Observational Evidence from Southern California.” Nature Communications 12 (1): 1493. https://doi.org/10.1038/s41467-021-21708-0.
Ahlborg, U. G., A. Brouwer, M. A. Fingerhut, J. L. Jacobson, S. W. Jacobson, S. W. Kennedy, A. A. F. Kettrup, J. H. Koeman, H. Poiger, C. Rappe, S. H. Safe, R. F. Seegal, T. Jouko, and M. van den Berg. 1992. “Impact of Polychlorinated Dibenzop-dioxins, Dibenzofurans, and Biphenyls on Human and Environmental Health, with Special Emphasis on Application of the Toxic Equivalency Factor Concept.” European Journal of Pharmacology: Environmental Toxicology and Pharmacology 228 (4): 179–199. https://doi.org/10.1016/0926-6917(92)90029-C.
Alavy, M., and J. A. Siegel. 2019. “In-situ Effectiveness of Residential HVAC Filters.” Indoor Air 30 (1): 156–166. https://doi.org/10.1111/ina.12617.
Alexakis, D. E. 2020. “Suburban Areas in Flames: Dispersion of Potentially Toxic Elements from Burned Vegetation and Buildings. Estimation of the Associated Ecological and Human Health Risk.” Environmental Research 183. https://doi.org/10.1016/j.envres.2020.109153.
Alman, B. L., G. Pfister, H. Hao, J. Stowell, X. Hu, Y. Liu, and M. J. Strickland. 2016. “The Association of Wildfire Smoke with Respiratory and Cardiovascular Emergency Department Visits in Colorado in 2012: A Case Crossover Study.” Environmental Health 15. https://doi.org/10.1186/s12940-016-0146-8.
American Public Health Association. n.d. “Climate Changes Health: Vulnerable Populations.” https://www.apha.org/topics-and-issues/climate-change/vulnerable-populations (accessed February 19, 2022).
Amjad, S., D. Chojecki, A. Osornio-Vargas, and M. B. Ospina. 2021. “Wildfire Exposure during Pregnancy and the Risk of Adverse Birth Outcomes: A Systematic Review.” Environment International 156. https://doi.org/10.1016/j.envint.2021.106644.
Andersen, M. H. G., A. T. Saber, P. B. Pedersen, et al. 2017. “Cardiovascular Health Effects Following Exposure of Human Volunteers during Fire Extinction Exercises.” Environmental Health 16 (1): 96. https://doi.org/10.1186/s12940-017-0303-8.
Anderson, S., A. J. Plantinga, and M. Wibbenmeyer. 2020. Inequality in Agency Responsiveness: Evidence from Salient Wildfire Events. Washington, DC: Resources for the Future.
ASHRAE. n.d. Planning Framework for Protecting Commercial Building Occupants from Smoke During Wildfire Events. Atlanta, GA: ASHRAE. https://www.ashrae.org/file%20library/technical%20resources/covid-19/planning-framework-for-protecting-commercial-building-occupants-from-smoke-during-wildfire-events.pdf.
ASHRAE. 2020. ASHRAE 189.1 Standard for the Design of High-Performance Green Buildings Except Low-Rise Residential Buildings. Atlanta, GA: ASHRAE. https://www.epa.gov/smartgrowth/ansiashraeusgbcies-standard-1891-2014-standard-design-high-performance-green-buildings.
ATSDR (US Agency for Toxic Substances and Disease Registry). 2000. Public Health Statement Polychlorinated Biphenyls (PCBS): 1–9. https://www.atsdr.cdc.gov/toxprofiles/tp17.pdf.
ATSDR. 2002. Hydrogen Chloride. https://www.atsdr.cdc.gov/toxfaqs/tfacts173.pdf.
ATSDR. 2014a. Methyl Isocyanate. https://www.atsdr.cdc.gov/toxfaqs/tfacts182.pdf (accessed March 22, 2022).
ATSDR. 2014b. Polycyclic Aromatic Hydrocarbons (PAHs). https://wwwn.cdc.gov/TSP/ToxFAQs/ToxFAQsDetails.aspx?faqid=121&toxid=25 (accessed March 24, 2022).
ATSDR. 2015. Phosphate Ester Flame Retardants. https://wwwn.cdc.gov/TSP/ToxFAQs/ToxFAQsDetails.aspx?faqid=1164&toxid=239 (accessed March 22, 2022).
ATSDR. 2016. Health Effects of Asbestos. https://www.atsdr.cdc.gov/asbestos/health_effects_asbestos.html (accessed March 22, 2022).
Austin, E., E. Kasner, E. Seto, and J. Spector. 2021. “Combined Burden of Heat and Particulate Matter Air Quality in WA Agriculture.” Journal of Agromedicine 26 (1): 18–27. https://doi.org/10.1080/1059924x.2020.1795032.
Bailey, Z. D., N. Krieger, M. Agénor, J. Graves, N. Linos, and M. T. Bassett. 2017. “Structural Racism and Health Inequities in the USA: Evidence and Interventions.” Lancet 389 (10077): 1453–1463. https://doi.org/10.1016/S0140-6736(17)30569-X.
Banks, A. P. W., P. Thai, M. Engelsman, X. Wang, A. F. Osorio, and J. F. Mueller. 2021. “Characterising the Exposure of Australian Firefighters to Polycyclic Aromatic Hydrocarbons Generated in Simulated Compartment Fires.” International Journal of Hygiene and Environmental Health 231. https://doi.org/10.1016/j.ijheh.2020.113637.
Barboni, T., M. Cannac, V. Pasqualini, A. Simeoni, E. Leoni, and N. Chiaramonti. 2010. “Volatile and Semi-volatile Organic Compounds in Smoke Exposure of Firefighters during Prescribed Burning in the Mediterranean Region.” International Journal of Wildland Fire 19 (5). https://doi.org/10.1071/wf08121.
Beitel, S. C., L. M. Flahr, C. Hoppe-Jones, J. L. Burgess, S. R. Littau, J. Gulotta, P. Moore, D. Wallentine, and S. A. Snyder. 2020. “Assessment of the Toxicity of Firefighter Exposures Using the PAH CALUX Bioassay.” Environment International 135: 105207. https://doi.org/10.1016/j.envint.2019.105207.
Black, C., J. E. Gerriets, J. H. Fontaine, R. W. Harper, N. J. Kenyon, F. Tablin, ... and L. A. Miller. 2017. “Early Life Wildfire Smoke Exposure Is Associated with Immune Dysregulation and Lung Function Decrements in Adolescence.” American Journal of Respiratory Cell and Molecular Biology 56 (5): 657–666.
Bodi, M. B., D. A. Martin, V. N. Balfour, C. Santin, S. H. Doerr, P. Pereira, A. Cerda, and J. Mataix-Solera. 2014. “Wildland Fire Ash: Production, Composition and Eco-hydro-geomorphic Effects.” Earth-Science Reviews 130: 103–127. https://doi.org/10.1016/j.earscirev.2013.12.007.
Boffetta, P., N. Jourenkova, and P. Gustavsson. 1997. “Cancer Risk from Occupational and Environmental Exposure to Polycyclic Aromatic Hydrocarbons.” Cancer Causes and Control 8: 444–472. https://doi.org/10.1023/a:1018465507029.
Brim, H., P. Mokarram, F. Naghibalhossaini, and M. Saberi-Firoozi. 2008. “Impact of BRAF, MLH1 on the Incidence of Microsatellite Instability High Colorectal Cancer in Populations Based Study.” Molecular Cancer 7 (68). https://doi.org/10.1186/1476-4598-7-68.
Brown, M. R. G., V. I. O. Agyapong, A. J. Greenshaw, I. Cribben, P. Brett-MacLean, J. Drolet, C. B. McDonald-Harker, J. Omeje, M. Mankowski, S. Noble, D. T. Kitching, and P. H. Silverstone. 2019. “Significant PTSD and Other Mental Health Effects Present 18 Months After the Fort Mcmurray Wildfire: Findings from 3,070 Grades 7–12 Students.” Frontiers in Psychiatry 10. https://doi.org/10.3389/fpsyt.2019.00623.
Brown, M. R. G., H. Pazderka, V. I. O. Agyapong, A. J. Greenshaw, I. Cribben, P. Brett-MacLean, J. Drolet, C. B. McDonald-Harker, J. Omeje, B. Lee, M. Mankowski, S. Noble, D. T. Kitching, and P. H. Silverstone. 2021. “Mental Health Symptoms Unexpectedly Increased in Students Aged 11–19 Years During the 3.5 Years After the 2016 Fort McMurray Wildfire: Findings from 9,376 Survey Responses.” Frontiers in Psychiatry 12. https://doi.org/10.3389%2Ffpsyt.2021.676256.
Broyles, G. A. 2013. Wildland Firefighter Smoke Expsoure Study. Utah State, Logan, Utah. Masters of Natural Resources.
Burgess, J. L., C. Nanson, D. Bolstad-Johnson, R. Gerkin, T. Hysong, R. C. Lantz, D. Sherrill, C. Crutchfield, S. Quan, A. Bernard, and M. Witten. 2001. “Adverse Respiratory Effects Following Overhaul in Firefighters.” Journal of Occupational and Environmental Medicine 43 (5): 467–473. https://doi.org/10.1097/00043764-200105000-00007.
Burgess, J. L., C. Hoppe-Jones, S. C. Griffin, J. J. Zhou, J. J. Gulotta, D. D. Wallentine, P. K. Moore, E. A. Valliere, S. R. Weller, S. C. Beitel, L. M. Flahr, S. R. Littau, D. Dearmon-Moore, J. Zhai, A. M. Jung, F. Garavito, and S. A. Snyder. 2020. “Evaluation of Interventions to Reduce Firefighter Exposures.” Journal of Occupational and Environmental Medicine 62 (4): 279–288. https://doi.org/10.1097/JOM.0000000000001815.
Burke, M., A. Driscoll, S. Heft-Neal, J. Xue, J. Burney, and M. Wara. 2021. “The Changing Risk and Burden of Wildfire in the United States.” Proceedings of the National Academy of Sciences 118 (2).
Burke, M. P., T. S. Hogue, A. M. Kinoshita, J. Barco, C. Wessel, and E. D. Stein. 2013. “Pre- and Post-Fire Pollutant Loads in an Urban Fringe Watershed in Southern California.” Environmental Monitoring and Assessment 185 (12): 10131–10145. https://doi.org/10.1007/s10661-013-3318-9.
Burke, S., J. W. Bethel, and A. F. Britt. 2012. “Assessing Disaster Preparedness among Latino Migrant and Seasonal Farmworkers in Eastern North Carolina.” International Journal of Environmental Research and Public Health 9 (9): 3115–3133. https://doi.org/10.3390/ijerph9093115.
Burton, C. A., T. M. Hoefen, G. S. Plumlee, K. L. Baumberger, A. R. Backlin, E. Gallegos, and R. N. Fisher. 2016. “Trace Elements in Stormflow, Ash, and Burned Soil Following the 2009 Station Fire in Southern California.” PLoS One 11 (5): e0153372. https://doi.org/10.1371/journal.pone.0153372.
CARB (California Air Resources Board). 2008. Evaluation of Ozone Emissions from Portable Indoor Air Cleaners: Electrostatic Precipitators and Ionizers. Sacramento, CA: California Air Resources Board. https://www.arb.ca.gov/research/indoor/esp_report.pdf?_ga=2.88136991.567876424.1668176695-1290726036.1668176695.
CARB. 2021. Camp Fire Air Quality Data Analysis. Sacramento, CA: California Air Resources Board. https://ww2.arb.ca.gov/resources/documents/camp-fire-air-quality-data-analysis.
Cal/OSHA (California Division of Occupational Safety and Health). 2020. “Protection from Wildfire Smoke.” https://www.dir.ca.gov/Title8/5141_1.html.
Calin, G. A., and C. M. Croce. 2006. “MicroRNA-Cancer Connection: The Beginning of a New Tale.” Cancer Research 66 (15): 7390–7394. https://doi.org/10.1158/0008-5472.CAN-06-0800.
Carratt, S. A., C. Flayer, M. Kossack, and J. A. Last. 2017. “Pesticides, wildfire suppression chemicals, and California wildfires: A human health perspective.” Current Topics in Toxicology 13.
Carter, J. V., N. J. Galbraith, D. Yang, J. F. Burton, S. P. Walker, and S. Galandiuk. 2017. “Blood-Based MicroRNAs as Biomarkers for the Diagnosis of Colorectal Cancer: A Systematic Review and Meta-Analysis.” British Journal of Cancer 116 (6): 762–774. https://doi.org/10.1038/bjc.2017.12.
CCST (California Council on Science and Technology). 2020. The Costs of Wildfire in California.
CDC (Centers for Disease Control and Prevention). 2017. Dioxins, Furans and Dioxin-Like Polychlorinated Biphenyls Factsheet. https://www.cdc.gov/biomonitoring/DioxinLikeChemicals_FactSheet.html (accessed March 22, 2022).
CDC. 2018. Facts About Phosgene. https://emergency.cdc.gov/agent/phosgene/basics/facts.asp (accessed March 22, 2022).
CDC. 2019. Particle Pollution. https://www.cdc.gov/air/particulate_matter.html (accessed March 22, 2022).
CDC. 2021. Phthalates Factsheet. https://www.cdc.gov/biomonitoring/Phthalates_FactSheet.html (accessed March 23, 2022).
CDC. 2022. Polycyclic Aromatic Hydrocarbons (PAHs) Factsheet. https://www.cdc.gov/biomonitoring/PAHs_FactSheet.html (accessed March 24, 2022).
Cerrato, J. M., J. M. Blake, C. Hirani, A. L. Clark, A. M. Ali, K. Artyushkova, E. Peterson, and R. J. Bixby. 2016. “Wildfires and Water Chemistry: Effect of Metals Associated with Wood Ash.” Environmental Science: Processes & Impacts 18 (8): 1078–1089. https://doi.org/10.1039/c6em00123h.
Chan, W. R., J. Joh, and M. H. Sherman. 2013. “Analysis of Air Leakage Measurements of US Houses.” Energy and Buildings 66: 616–625. https://doi.org/10.1016/j.enbuild.2013.07.047.
Chen, H., H. Uzun, A. T. Chow, and T. Karanfil. 2020. “Low Water Treatability Efficiency of Wildfire-Induced Dissolved Organic Matter and Disinfection By-product Precursors.” Water Research 184. https://doi.org/10.1016/j.watres.2020.116111.
Chen, H., J. M. Samet, P. A. Bromberg, et al. 2021. “Cardiovascular Health Impacts of Wildfire Smoke Exposure.” Particle and Fibre Toxicology 18: 2. https://doi.org/10.1186/s12989-020-00394-8.
Cherry, N., Y. A. Aklilu, J. Beach, P. Britz-McKibbin, R. Elbourne, J. M. Galarneau, B. Gill, D. Kinniburgh, and X. Zhang. 2019. “Urinary 1-Hydroxypyrene and Skin Contamination in Firefighters Deployed to the Fort McMurray Fire.” Annals of Work Exposures and Health 63 (4): 448–458. https://doi.org/10.1093/annweh/wxz006.
Cherry, N., J. M. Galarneau, D. Kinniburgh, B. Quemerais, S. Tiu, and X. Zhang. 2021. “Exposure and Absorption of PAHs in Wildland Firefighters: A Field Study with Pilot Interventions.” Annals of Work Exposures and Health 65 (2): 148–161. https://doi.org/10.1093/annweh/wxaa064.
Chong, N. S., S. Abdulramoni, D. Patterson, and H. Brown. 2019. “Releases of Fire-Derived Contaminants from Polymer Pipes Made of Polyvinyl Chloride.” Toxics 7 (4). https://doi.org/10.3390/toxics7040057.
Coussens, L., and Z. Werb. 2002. “Inflammation and Cancer.” Nature 420. https://doi.org/10.1038/nature01322.
Cova, T. J., D. M. Theobald, J. B. Norman, and L. K. Siebeneck. 2011. “Mapping Wildfire Evacuation Vulnerability in the Western US: The Limits of Infrastructure. GeoJournal 78 (2): 273–285. https://doi.org/10.1007/s10708-011-9419-5.
Daniels, R. D., T. L. Kubale, J. H. Yiin, M. M. Dahm, T. R. Hales, D. Baris, S. H. Zahm, J. J. Beaumont, K. M. Waters, and L. E. Pinkerton. 2014. “Mortality and Cancer Incidence in a Pooled Cohort of US Firefighters from San Francisco, Chicago and Philadelphia (1950–2009).” Occupational and Environmental Medicine 71 (6): 388–397. https://doi.org/10.1136/oemed-2013-101662.
Davies, I. P., R. D. Haugo, J. C. Robertson, and P. S. Levin. 2018. “The Unequal Vulnerability of Communities of Color to Wildfire.” PLoS One 13 (11): e0205825. https://doi.org/10.1371/journal.pone.0205825.
Davison, G., K. K. Barkjohn, G. S. W. Hagler, A. L. Holder, S. Coefield, C. Noonan, and B. Hassett-Sipple. 2021. “Creating Clean Air Spaces During Wildland Fire Smoke Episodes: Web Summit Summary.” Frontiers in Public Health. https://doi.org/10.3389/fpubh.2021.508971.
De Vos, A. J., A. Cook, B. Devine, P. J. Thompson, and P. Weinstein. 2009. “Effect of Protective Filters on Fire Fighter Respiratory Health: Field Validation during Prescribed Burns.” American Journal of Industrial Medicine 52 (1): 76–87. https://doi.org/10.1002/ajim.20651.
DeFlorio-Barker, S., J. Crooks, J. Reyes, and A. G. Rappold. 2019. “Cardiopulmonary Effects of Fine Particulate Matter Exposure among Older Adults, during Wildfire and Non-Wildfire Periods, in the United States 2008–2010.” Environmental Health Perspectives 127 (3): 37006. https://doi.org/10.1289/EHP3860.
Delfino, R. J., S. Brummel, J. Wu, H. Stern, B. Ostro, M. Lipsett, A. Winer, D. H. Street, L. Zhang, T. Tjoa, and D. L. Gillen. 2008. “The Relationship of Respiratory and Cardiovascular Hospital Admissions to the Southern California Wildfires of 2003.” Occupational and Environmental Medicine 66 (3): 189–197. https://doi.org/10.1186/s12940-016-0146-8.
Demers, P. A., D. M. DeMarini, K. W. Fent, D. C. Glass, J. Hansen, O. Adetona, M. H.G. Andersen, L. E. B. Freeman, A. J. Caban-Martinez, R. D. Daniels, T. R. Driscoll, J. M. Goodrich, J. M. Graber, T. L. Kirkham, K. Kjaerheim, D. Kriebel, A. S. Long, L. C. Main, M. Oliveira, S. Peters, L. R. Teras, E. R. Watkins, J. L. Burgess, A. A. Stec, P. A. White, N. L. DeBono, L. Benbrahim-Tallaa, A. de Conti, F. El Ghissassi, Y. Grosse, L. T. Stayer, E. Suonio, S. Viegas, R. Wedekind, P. Boucheron, B. Hosseini, J. Kim, H. Zahed, H. Mattock, F. Madia, and M. K. Schubauer-Berigan. 2022. “Carcinogenicity of occupational exposure as a firefighter.” The Lancet Oncology 23 (8): 985-986. https://doi.org/10.1016/S1470-2045(22)00390-4.
Diggs, D. L., A. C. Huderson, K. L. Harris, J. N. Myers, L. D. Banks, P. V. Rekhadevi, M. S. Niaz, and A. Ramesh. 2011. “Polycyclic Aromatic Hydrocarbons and Digestive Tract Cancers: A Perspective.” Journal of Environmental Science and Health, Part C: Toxicology and Carcinogenesis 29 (4): 324–357. https://doi.org/10.1080/10590501.2011.629974.
Dills, R., M. Paulsen, J. Ahmad, D. Kalman, F. Elias, and C. Simpson. 2006. “Evaluation of Urinary Methoxyphenols as Biomarkers of Woodsmoke Exposure.” Environmental Science & Technology 40. https://doi.org/10.1021/es051886f.
Dreessen, J., J. Sullivan, and R. Delgado. 2016. “Observations and Impacts of Transported Canadian Wildfire Smoke on Ozone and Aerosol Air Quality in the Maryland Region on June 9–12, 2015.” Journal of the Air & Waste Management Association 66 (9): 842–862. https://doi.org/10.1080/10962247.2016.1161674.
Dugue, P. A., J. K. Bassett, E. M. Wong, J. E. Joo, S. Li, C. Yu, D. F. Schmidt, E. Makalic, N. W. Doo, D. D. Buchanan, A. M. Hodge, D. R. English, J. L. Hopper, G. G. Giles, M. C. Southey, and R. L. Milne. 2021. “Biological Aging Measures Based on Blood DNA Methylation and Risk of Cancer: A Prospective Study.” JNCI Cancer Spectrum 5 (1): pkaa109. https://doi.org/10.1093/jncics/pkaa109.
DuTeaux, S. 2019. Final Report of Air Quality in the Vicinity of Camp Fire Debris Removal. Edited by California Environmental Protection Agency, CalRecycle, and California Governor’s Office of Emergency Services. Sacramento, CA: California Environmental Protection Agency.
Eberhart, C. 2010. Measurements of Air Contaminants during the Cerro Grande Fire at Los Alamos National Laboratory. Los Alamos, NM: Los Alamos National Laboratory.
Eckstein, S., and G. Peri. 2018. “Immigrant Niches and Immigrant Networks in the U.S. Labor Market.” RSF: The Russell Sage Foundation Journal of the Social Sciences 4 (1): 1–17. https://doi.org/10.7758/rsf.2018.4.1.01.
Edgeley, C., and T. B. Paveglio. 2019. “Exploring Influences on Intended Evacuation Behaviors during Wildfire: What Roles for Pre-fire Actions and Event-Based Cues?” International Journal of Disaster Risk Reduction 37. https://doi.org/10.1016/j.ijdrr.2019.101182.
Eisenman, D. P., D. Glik, R. Maranon, L. Gonzales, and S. Asch. 2009. “Developing a Disaster Preparedness Campaign Targeting Low-Income Latino Immigrants: Focus Group Results for Project PREP.” Journal of Health Care for the Poor and Underserved 20 (2): 330–345. https://doi.org/10.1353/hpu.0.0129.
Emmerton, C. A., C. A. Cooke, S. Hustins, U. Silins, M. B. Emelko, T. Lewis, M. K. Kruk, N. Taube, D. Zhu, B. Jackson, M. Stone, J. G. Kerr, and J. F. Orwin. 2020. “Severe Western Canadian Wildfire Affects Water Quality Even at Large Basin Scales.” Water Research 183. https://doi.org/10.1016/j.watres.2020.116071.
EPA (US Environmental Protection Agency). 2009. Integrated Science Assessment (ISA) for Particulate Matter (Final Report, Dec 2009). EPA/600/R-08/139F. Washington, DC: EPA.
EPA. 2018. Residential air cleaners: A technical summary. EPA 402-F-09-002. Washington, DC: EPA.
EPA. 2019. Wildfire Smoke: A Guide for Public Health Officials. EPA-452/R-19-901. Washington, DC: EPA.
EPA. 2020. Wildfires and indoor air quality (IAQ). https://www.epa.gov/indoor-air-quality-iaq/wildfires-and-indoor-air-quality-iaq (accessed February 9, 2021).
EPA. 2021a. Learn About Asbestos. https://www.epa.gov/asbestos/learn-about-asbestos#effects (accessed March 22, 2022).
EPA. 2021b. Learn About Dioxin. https://www.epa.gov/dioxin/learn-about-dioxin (accessed March 22, 2022).
EPA. 2021c. Volatile Organic Compounds’Impact on Indoor Air Quality. https://www.epa.gov/indoor-air-quality-iaq/volatile-organic-compounds-impact-indoor-air-quality (accessed March 22, 2022).
EPA. 2021d. Health and Environmental Effects of Particulate Matter (PM). https://www.epa.gov/pm-pollution/health-and-environmental-effects-particulate-matter-pm (accessed March 22, 2022).
EPA. 2021e. Why Wildfire Smoke Is a Health Concern. https://www.epa.gov/wildfire-smoke-course/why-wildfire-smoke-health-concern (accessed February 19, 2022).
EPA. 2021f. Comparative Assessment of the Impacts of Prescribed Fire versus Wildfire (CAIF): A Case Study in the Western U.S. https://cfpub.epa.gov/ncea/risk/recordisplay.cfm?deid=352824.
EPA. 2021g. “Which Populations Experience Greater Risks of Adverse Health Effects Resulting from Wildfire Smoke Exposure?” https://www.epa.gov/wildfire-smoke-course/which-populations-experience-greater-risks-adverse-health-effects-resulting (accessed February 19, 2022).
EPA. 2022a. Risk Management for Phthalates. https://www.epa.gov/assessing-and-managing-chemicals-under-tsca/risk-management-phthalates (accessed March 23, 2022).
EPA. 2022b. How to Evaluate Air Sensors for Smoke Monitoring Webinar Archive. https://www.epa.gov/research-states/how-evaluate-air-sensors-smoke-monitoring-webinar-archive (accessed March 25, 2022).
Fadadu, R. P., B. Grimes, N. P. Jewell, J. Vargo, A. T. Young, K. Abuabara, J. R. Balmes, and M. L. Wei. 2021. “Association of Wildfire Air Pollution and Health Care Use for Atopic Dermatitis and Itch.” JAMA Dermatology 157 (6): 658–666. https://doi.org/10.1001/jamadermatol.2021.0179.
Fent, K. W., J. Eisenberg, J. Snawder, D. Sammons, J. D. Pleil, M. A. Stiegel, C. Mueller, G. P. Horn, and J. Dalton. 2014. “Systemic Exposure to PAHs and Benzene in Firefighters Suppressing Controlled Structure Fires.” Annals of Occupational Hygiene 58 (7): 830–845. https://doi.org/10.1093/annhyg/meu036.
Fent, K. W., B. Alexander, J. Roberts, S. Robertson, C. Toennis, D. Sammons, S. Bertke, S. Kerber, D. Smith, and G. Horn. 2017. “Contamination of Firefighter Personal Protective Equipment and Skin and the Effectiveness of Decontamination Procedures.” Journal of Occupational and Environmental Hygiene 14 (10): 801–814. https://doi.org/10.1080/15459624.2017.1334904.
Fent, K. W., D. E. Evans, K. Babik, C. Striley, S. Bertke, S. Kerber, D. Smith, and G. P. Horn. 2018. “Airborne Contaminants during Controlled Residential Fires.” Journal of Occupational and Environmental Hygiene 15 (5): 399–412. https://doi.org/10.1080/15459624.2018.1445260.
Fent, K. W., C. Toennis, D. Sammons, S. Robertson, S. Bertke, A. M. Calafat, J. D. Pleil, M. A. Geer Wallace, S. Kerber, D. L. Smith, and G. P. Horn. 2019a. “Firefighters’ and Instructors’ Absorption of PAHs and Benzene during Training Exercises.” International Journal of Hygiene and Environmental Health 222 (7): 991–1000. https://doi.org/10.1016/j.ijheh.2019.06.006.
Fent, K. W., C. Toennis, D. Sammons, S. Robertson, S. Bertke, A. M. Calafat, J. D. Pleil, M. A. G. Wallace, S. Kerber, D. Smith, and G. P. Horn. 2019b. “Firefighters’ Absorption of PAHs and VOCs during Controlled Residential Fires by Job Assignment and Fire Attack Tactic.” Journal of Exposure Science and Environmental Epidemiology 30 (2): 338–349. https://doi.org/10.1038/s41370-019-0145-2.
Fent, K. W., M. LaGuardia, D. Luellen, S. McCormick, A. Mayer, I. Chen, S. Kerber, D. Smith, and G. P. Horn. 2020. “Flame Retardants, Dioxins, and Furans in Air and on Firefighters’ Protective Ensembles during Controlled Residential Firefighting.” Environment International 140. https://doi.org/10.1016/j.envint.2020.105756.
Filonchyk, M., M. P. Peterson, and Dongqi Sun. 2022. “Deterioration of Air Quality Associated with the 2020 US Wildfires.” Science of the Total Environment 826: 154103. https://doi.org/10.1016/j.scitotenv.2022.154103.
Fussell, E., L. Delp, K. Riley, S. Chavez, and A. Valenzuela. 2018. “Implications of Social and Legal Status on Immigrants’ Health in Disaster Zones.” American Journal of Public Health 108 (12). https://doi.org/10.2105/AJPH.2018.304554.
Gallaher, B. M., and R. J. Koch. 2004. Cerro Grande Fire Impacts to Water Quality and Stream Flow near Los Alamos National Laboratory: Results of Four Years of Monitoring. Los Alamos, NM: Los Alamos National Laboratory.
Gan, R. W., B. Ford, W. Lassman, G. Pfister, A. Vaidyanathan, E. Fischer, J. Volckens, J. R. Pierce, and S. Magzamen. 2017. “Comparison of Wildfire Smoke Estimation Methods and Associations with Cardiopulmonary-Related Hospital Admissions.” GeoHealth 1 (3): 122–136. https://doi.org/10.1002/2017GH000073.
Gan, R. W., J. Liu, B. Ford, K. O’Dell, A. Vaidyanathan, A. Wilson, J. Volckens, G. Pfister, E. V. Fischer, J. R. Pierce, and S. Magzamen. 2020. “The association between wildfire smoke exposure and asthma-specific medical care utilization in Oregon during the 2013 wildfire season.” Journal of Exposure Science & Environmental Epidemiology 30: 618–628. https://doi.org/10.1038/s41370-020-0210-x.
Gaughan, D. M., J. M. Cox-Ganser, P. L. Enright, R. M. Castellan, G. R. Wagner, G. R. Hobbs, T. A. Bledsoe, P. D. Siegel, K. Kreiss, and D. N. Weissman. 2008. “Acute Upper and Lower Respiratory Effects in Wildland Firefighters.” Journal of Occupational and Environmental Medicine 50 (9): 1019–1028. https://doi.org/10.1097/JOM.0b013e3181754161.
Glass, D. C., S. Pircher, A. Del Monaco, S. Vander Hoorn, and M. R. Sim. 2016. “Mortality and Cancer Incidence in a Cohort of Male Paid Australian Firefighters.” Occupational and Environmental Medicine 73: 761–771. http://doi.org/10.1136/oemed-2015-103467.
Gold, A., and T. B. Perera. 2021. EMS Asphyxiation and Other Gas and Fire Hazards. Treasure Island, FL: StatPearls Publishing.
Goyer, R. 2004. Issue Paper on the Human Health Effects of Metals. Washington, DC: EPA.
Haikerwal, A., M. Akram, A. Del Monaco, K. Smith, M. R. Sim, M. Meyer, A. M. Tonkin, M. J. Abramson, and M. Dennekamp. 2015. “Impact of Fine Particulate Matter (PM2.5) Exposure during Wildfires on Cardiovascular Health Outcomes.” Journal of the American Heart Association 4 (7). https://doi.org/10.1161/JAHA.114.001653.
Haikerwal, A., M. Akram, M. R. Sim, M. Meyer, M. J. Abramson, and M. Dennekamp. 2016. “Fine Particulate Matter (PM2.5) Exposure during a Prolonged Wildfire Period and Emergency Department Visits for Asthma.” Respirology 21 (1): 88–94. https://doi.org/10.1111/resp.12613.
Hardeman, R. R., P. A. Homan, T. Chantarat, B. A. Davis, and T. H. Brown. 2022. “Improving the Measurement of Structural Racism to Achieve Antiracist Health Policy.” Health Affairs 21 (2). https://doi.org/10.1377/hlthaff.2021.01489.
HHS (US Department of Health and Human Services). 2018. Low Income Home Energy Data for Fiscal Year 2017. https://liheappm.acf.hhs.gov/home-energy-notebooks/ (accessed February 26, 2022).
Hodshire, A. L., A. Akherati, M. J. Alvarado, B. Brown-Steiner, S. H. Jathar, J. L. Jimenez, S. M. Kreidenweis, C. Lonsdale, T. B. Onasch, A. M. Ortega, and J. R. Pierce. 2019. “Aging Effects on Biomass Burning Aerosol Mass and Composition: A Critical Review of Field and Laboratory Studies.” Environmental Science & Technology 53 (17): 10007–10022. https://doi.org/10.1021/acs.est.9b02588.
Hohner, A., K. M. Cawley, J. Oropeza, R. S. Summers, and F. L. Rosario-Ortiz. 2016. “Drinking Water Treatment Response Following a Colorado Wildfire.” Water Research 105: 187–198. https://doi.org/10.1016/j.watres.2016.08.034.
Holm, S. M., M. D. Miller, and J. R. Balmes. 2021. “Health Effects of Wildfire Smoke in Children and Public Health Tools: A Narrative Review.” Journal of Exposure Science and Environmental Epidemiology 31 (1): 1–20. https://doi.org/10.1038/s41370-020-00267-4.
Homan, P., T. H. Brown, and B. King. 2021. “Structural Intersectionality as a New Direction for Health Disparities Research.” Journal of Health and Social Behavior 62 (3): 350–370. https://doi.org/10.1177/00221465211032947.
Hoppe-Jones, C., S. C. Griffin, J. J. Gulotta, D. D. Wallentine, P. K. Moore, S. C. Beitel, L. M. Flahr, J. Zhai, J. J. Zhou, S. R. Littau, D. Dearmon-Moore, A. M. Jung, F. Garavito, S. A. Snyder, and J. L. Burgess. 2021. “Evaluation of Fire-ground Exposures Using Urinary PAH Metabolites.” Journal of Exposure Science and Environmental Epidemiology 31 (5): 913–922. https://doi.org/10.1038/s41370-021-00311-x.
Hutchinson, J. A., J. Vargo, M. Milet, N. H. F. French, M. Billmire, J. Johnson, and S. Hoshiko. 2018. “The San Diego 2007 Wildfires and Medi-Cal Emergency Department Presentations, Inpatient Hospitalizations, and Outpatient Visits: An Observational Study of Smoke Exposure Periods and a Bidirectional Case-Crossover Analysis.” PLoS Medicine https://doi.org/10.1371/journal.pmed.1002601.
IARC (InternationaI Agency for Research on Cancer). 2010. “Some Non-heterocyclic Polycyclic Aromatic Hydrocarbons and Some Related Exposures.” IARC Monographs on the Identification of Carcinogenic Hazards to Humans 92.
IDEPSCA (Instituto de Educacion Popular del Sur de California). 2020. “On the Frontlines: The Role of Domestic Workers and Day Laborers in Confronting Recent Wildfires in Southern California.” https://www.cadomesticworkers.org/news/on-the-frontlines-the-role-of-domestic-workers-and-day-laborers-in-confronting-recent-wildfires-in-california/ (accessed February 23, 2022).
Igarashi, Y., Y. Onda, Y. Wakiyama, A. Konoplev, M. Zheleznyak, H. Lisovyi, G. Laptev, V. Damiyanovich, D. Samoilov, K. Nanba, and S. Kirieiev. 2020. “Impact of Wildfire on 137Cs and 90Sr Wash-Off in Heavily Contaminated Forests in the Chernobyl Exclusion Zone.” Environmental Pollution 259: 113764. https://doi.org/10.1016/j.envpol.2019.113764.
Isaacson, K. P., C. R. Proctor, Q. E. Wang, E. Y. Edwards, Y. Noh, A. D. Shah, and A. J. Whelton. 2020. “Drinking Water Contamination from the Thermal Degradation of Plastics: Implications for Wildfire and Structure Fire Response.” Environmental Science: Water Research & Technology 7 (2): 274–284. https://doi.org/10.1039/d0ew00836b.
Jaenisch, R., and A. Bird. 2003. “Epigenetic Regulation of Gene Expression: How the Genome Integrates Intrinsic and Environmental Signals.” Nature Genetics 33: 245–254. https://doi.org/10.1038/ng1089.
Jaffe, D. A., S. M. O’Neill, N. K. Larkin, A. L. Holder, D. L. Peterson, J. E. Halofsky, and A. G. Rappold. 2020. “Wildfire and Prescribed Burning Impacts on Air Quality in the United States.” Journal of the Air & Waste Management Association 70 (6): 583–615. https://doi.org/10.1080/10962247.2020.1749731.
Jeong, K. S., J. Zhou, S. C. Griffin, E. T. Jacobs, D. Dearmon-Moore, J. Zhai, S. R. Littau, J. Gulotta, P. Moore, W. F. Peate, C. M. Richt, and J. L. Burgess. 2018. “MicroRNA Changes in Firefighters.” Journal of Occupational and Environmental Medicine 60 (5): 469–474. https://doi.org/10.1097/JOM.0000000000001307.
Johnston, F. H., S. B. Henderson, Y. Chen, J. T. Randerson, M. Marlier, R. S. DeFries, P. Kinney, D. M. J. S. Bowman, and M. Brauer. 2012. “Estimated Global Mortality Attributable to Smoke from Landscape Fires.” Environmental Health Perspectives 120 (5). https://doi.org/10.1289/ehp.1104422.
Jones, L., E. A. Lutz, M. Duncan, and J. L. Burgess. 2015. “Respiratory Protection for Firefighters— Evaluation of CBRN Canisters for Use During Overhaul.” Journal of Occupational and Environmental Hygiene 12 (5). https://doi.org/10.1080/15459624.2014.989363.
Jones, P. A., and P. W. Laird. 1999. “Cancer Epigentics Comes of Age.” Nature Genetics 21 (2). https://doi.org/10.1038/5947.
Joseph, G., P. J. Schramm, A. Vaidyanathan, P. Breysse, and B. Goodwin. 2020. Evidence on the Use of Indoor Air Filtration as an Intervention for Wildfire Smoke Pollutant Exposure: A Summary for Health Departments. BRACE technical report series. Atlanta, GA: Centers for Disease Control and Prevention. https://stacks.cdc.gov/view/cdc/108289.
Jung, A. M., J. Zhou, S. C. Beitel, S. R. Littau, J. J. Gulotta, D. D. Wallentine, P. K. Moore, and J. L. Burgess. 2021. “Longitudinal Evaluation of Whole Blood miRNA Expression in Firefighters.” Journal of Exposure Science and Environmental Epidemiology 31 (5): 900–912. https://doi.org/10.1038/s41370-021-00306-8.
Keir, J. L. A., U. S. Akhtar, D. M. J. Matschke, T. L. Kirkham, H. M. Chan, P. Ayotte, P. A. White, and J. M. Blais. 2017. “Elevated Exposures to Polycyclic Aromatic Hydrocarbons and Other Organic Mutagens in Ottawa Firefighters Participating in Emergency, On-Shift Fire Suppression.” Environmental Science & Technology 51 (21): 12745–12755. https://doi.org/10.1021/acs.est.7b02850.
Kessler, R. 2012. “Followup in Southern California: Decreased Birth Weight Following Prenatal Wildfire Smoke Exposure.” Environmental Health Perspectives 120 (9). https://doi.org/10.1289/ehp.120-a362b.
Kim, Y. H., H. Tong, M. Daniels, E. Boykin, Q. T. Krantz, J. McGee, M. Hays, K. Kovalcik, J. A. Dye, and M. I. Gilmour. 2014. “Cardiopulmonary Toxicity of Peat Wildfire Particulate Matter and the Predictive Utility of Precision Cut Lung Slices.” Particle and Fibre Toxicology 11: 29. https://doi.org/10.1186/1743-8977-11-29.
Kirk, K. M., and M. B. Logan. 2015. “Firefighting Instructors’ Exposures to Polycyclic Aromatic Hydrocarbons During Live Fire Training Scenarios.” Journal of Occupational and Environmental Hygiene 12 (4). https://doi.org/10.1080/15459624.2014.955184.
Kleinman, L. I., A. J. Sedlacek III, K. Adachi, P. R. Buseck, S. Collier, M. K. Dubey, A. L. Hodshire, E. Lewis, T. B. Onasch, J. R. Pierce, J. Shilling, S. R. Springston, J. Wang, Q. Zhang, S. Zhou, and R. J. Yokelson. 2020. “Rapid Evolution of Aerosol Particles and Their Optical Properties Downwind of Wildfires in the Western US.” Atmospheric Chemistry and Physics 20 (21): 13319–13341. https://doi.org/10.5194/acp-20-13319-2020.
Kochanski, A. K., D. V. Mallia, M. G. Fearon, J. Mandel, A. H. Souri, and T. Brown. 2019. “Modeling Wildfire Smoke Feedback Mechanisms Using a Coupled Fire-Atmosphere Model with a Radiatively Active Aerosol Scheme.” Journal of Geophysical Research: Atmospheres 124 (16): 9099–9116. https://doi.org/10.1029/2019jd030558.
Kodros, J. K., K. O’Dell, J. M. Samet, C. L’Orange, J. R. Pierce, and J. Volckens. 2021. “Quantifying the Health Benefits of Face Masks and Respirators to Mitigate Exposure to Severe Air Pollution.” GeoHealth 5 (9): e2021GH000482. https://doi.org/10.1029/2021GH000482.
Kohl, L., M. Meng, J. Vera, B. Bergquist, C. A. Cooke, S. Hustins, B. Jackson, C. W. Chow, and A. W. H. Chan. 2019. “Limited Retention of Wildfire-Derived PAHs and Trace Elements in Indoor Environments.” Geophysical Research Letters 46 (1): 383–391. https://doi.org/10.1029/2018gl080473.
Kolbe, A., and K. L. Gilchrist. 2009. An Extreme Bushfire Smoke Pollution Event: Health Impacts and Public Health Challenges. NSW Public Health Bulletin 20. https://doi.org/10.1071/NB08061.
Kolluri, S. K., U. H. Jin, and S. Safe. 2017. “Role of the Aryl Hydrocarbon Receptor in Carcinogenesis and Potential as an Anti-cancer Drug Target.” Archives of Toxicology 91 (7): 2497–2513. https://doi.org/10.1007/s00204-017-1981-2.
Koman, P. D., M. Billmire, K. R. Baker, R. de Majo, F. J. Anderson, S. Hoshiko, B. J. Thelen, and N. H. F. French. 2019. “Mapping Modeled Exposure of Wildland Fire Smoke for Human Health Studies in California.” Atmosphere (Basel) 10 (6). https://doi.org/10.3390/atmos10060308.
Kuligowski, E. 2021. “Evacuation Decision-Making and Behavior in Wildfires: Past Research, Current Challenges and a Future Research Agenda.” Fire Safety Journal 120. https://doi.org/10.1016/j.firesaf.2020.103129.
Kuligowski, E. D., X. Zhao, R. Lovreglio, N. Xu, K. Yang, A. Westbury, D. Nilsson, and N. Brown. 2022. “Modeling Evacuation Decisions in the 2019 Kincade Fire in California.” Safety Science 146. https://doi.org/10.1016/j.ssci.2021.105541.
Landis, M. S., E. S. Edgerton, E. M. White, G. R. Wentworth, A. P. Sullivan, and A. M. Dillner. 2018. “The Impact of the 2016 Fort McMurray Horse River Wildfire on Ambient Air Pollution Levels in the Athabasca Oil Sands Region, Alberta, Canada.” Science of the Total Environment 618: 1665–1676. https://doi.org/10.1016/j.scitotenv.2017.10.008.
Laumbach, R. J. 2019. “Clearing the Air on Personal Interventions to Reduce Exposure to Wildfire Smoke.” Annals of the American Thoracic Society 16 (7): 815–818. https://doi.org/10.1513/AnnalsATS.201812-894PS.
LeMasters, G. K., A. M. Genaidy, P. Succop, J. Deddens, T. Sobeih, H. Barriera-Viruet, K. Dunning, and J. Lockey. 2006. “Cancer Risk Among Firefighters: A Review and Meta-Analysis of 32 Studies.” Journal of Occupational and Environmental Medicine 48 (11): 1189–1202. https://doi.org/10.1097/01.jom.0000246229.68697.90.
Li, D., T. J. Cova, and P. E. Dennison. 2019. “Setting Wildfire Evacuation Triggers by Coupling Fire and Traffic Simulation Models: A Spatiotemporal GIS Approach.” Fire Technology 55 (2): 617–642. https://doi.org/10.1007/s10694-018-0771-6.
Liu, D., I. B. Tager, J. R. Balmes, and R. J. Harrison. 1991. “The Effect of Smoke Inhalation on Lung Function and Airway Responsiveness in Wildland Fire Fighters.” American Review of Respiratory Disease 146 (6). https://doi.org/10.1164/ajrccm/146.6.1469.
Liu, J. C., A. Wilson, L. J. Mickley, K. Ebisu, M. P. Sulprizio, Y. Wang, R. D. Peng, X. Yue, F. Dominici, and M. L. Bell. 2017. “Who Among the Elderly Is Most Vulnerable to Exposure to and Health Risks of Fine Particulate Matter from Wildfire Smoke?” American Journal of Epidemiology 186 (6): 730–735. https://doi.org/10.1093/aje/kwx141.
Magzamen, S., R. W. Gan, J. Liu, K. O’Dell, B. Ford, K. Berg, K. Bol, A. Wilson, E. V. Fischer, and J. R. Pierce. 2021. “Differential Cardiopulmonary Health Impacts of Local and Long-Range Transport of Wildfire Smoke.” GeoHealth 5 (3). https://doi.org/10.1029/2020gh000330.
Main, L. C., A. P. Wolkow, J. L. Tait, P. Della Gatta, J. Raines, R. Snow, and B. Aisbett. 2020. “Firefighter’s Acute Inflammatory Response to Wildfire Suppression.” Journal of Occupational and Environmental Medicine 62 (2): 145–148. https://doi.org/10.1097/JOM.0000000000001775.
Malig, B. J., D. Fairley, D. Pearson, X. Wu, K. Ebisu, and R. Basu. 2021. “Examining Fine Particulate Matter and Cause-Specific Morbidity during the 2017 North San Francisco Bay Wildfires.” Science of the Total Environment 787: 147507. https://doi.org/10.1016/j.scitotenv.2021.147507.
McCaffrey, S., R. Wilson, and A. Konar. 2018. “Should I Stay or Should I Go Now? Or Should I Wait and See? Influences on Wildfire Evacuation Decisions.” Risk Analysis 38 (7): 1390–1404. https://doi.org/10.1111/risa.12944.
McLennan, J., B. Ryan, C. Bearman, and K. Toh. 2018. “Should We Leave Now? Behavioral Factors in Evacuation Under Wildfire Threat.” Fire Technology 55 (2): 487–516. https://doi.org/10.1007/s10694-018-0753-8.
Melendez, B., S. Ghanipoor Machiani, and A. Nara. 2021. “Modelling Traffic during Lilac Wildfire Evacuation Using Cellular Data.” Transportation Research Interdisciplinary Perspectives 9. https://doi.org/10.1016/j.trip.2021.100335.
Meng, M. 2018. Composition of Wildfire-Derived Particulate Matter and Impacts on House Dust after a Major Wildfire. University of Toronto, Toronto, ON. Masters of Applied Science.
Miranda, A. I., V. Martins, P. Cascao, J. H. Amorim, J. Valente, R. Tavares, C. Borrego, O. Tchepel, A. J. Ferreira, C. R. Cordeiro, D. X. Viegas, L. M. Ribeiro, and L. P. Pita. 2010. “Monitoring of Firefighters Exposure to Smoke during Fire Experiments in Portugal.” Environmental International 36 (7): 736–745. https://doi.org/10.1016/j.envint.2010.05.009.
Mott, J. A., P. Meyer, D. Mannino, S. Redd, E. M. Smith, C. Gotway-Crawford, and E. Chase. 2002. “Wildland Forest Fire Smoke: Health Effects and Intervention Evaluation, Hoopa, California, 1999.” Western Journal of Emergency Medicine 176 (3). https://doi.org/10.1136/ewjm.176.3.157.
Mozumder, P., N. Raheem, J. Talberth, and J. Berrens. 2008. “Investigating Intended Evacuation from Wildfires in the Wildland–Urban Interface: Application of a Bivariate Probit Model.” Forest Policy and Economics 10 (6). https://doi.org/10.1016/j.forpol.2008.02.002.
Murphy, S. F., R. B. McCleskey, D. A. Martin, J. M. Holloway, and J. H. Writer. 2020. “Wildfire-Driven Changes in Hydrology Mobilize Arsenic and Metals from Legacy Mine Waste.” Science of the Total Environment 743: 140635. https://doi.org/10.1016/j.scitotenv.2020.140635.
Nadler, D. L., and I. G. Zurbenko. 2014. “Estimating Cancer Latency Times Using a Weibull Model.” Advances in Epidemiology 2014: 1–8. https://doi.org/10.1155/2014/746769.
NASA EO (National Aeronautics and Space Administration Earth Observatory). 2021. Smoke across North America. https://earthobservatory.nasa.gov/images/148610/smoke-across-north-america.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2017. Communities in Action: Pathways to Health Equity. Washington, DC: The National Academies Press. https://doi.org/10.17226/24624.
NASEM. 2022. Communities, Climate Change, and Health Equity: Proceedings of a Workshop–In Brief. Washington, DC: The National Academies Press. https://doi.org/10.17226/26435.
Navarro, K. 2020. “Working in Smoke: Wildfire Impacts on the Health of Firefighters and Outdoor Workers and Mitigation Strategies.” Clinics in Chest Medicine 41 (4): 763–769. https://doi.org/10.1016/j.ccm.2020.08.017.
Navarro, K. M., M. T. Kleinman, C. E. Mackay, T. E. Reinhardt, J. R. Balmes, G. A. Broyles, R. D. Ottmar, L. P. Naher, and J. W. Domitrovich. 2019. “Wildland Firefighter Smoke Exposure and Risk of Lung Cancer and Cardiovascular Disease Mortality.” Environmental Research 173: 462–468. https://doi.org/10.1016/j.envres.2019.03.060.
NCI (National Cancer Institute). 2019. Strong Inorganic Acid Mists Containing Sulfuric Acid. https://www.cancer.gov/about-cancer/causes-prevention/risk/substances/inorganic-acid (accessed March 22, 2022).
NEPHT (National Environmental Public Health Tracking). 2020. Air Quality. https://www.cdc.gov/nceh/tracking/topics/AirQuality.htm#ozone (accessed March 22, 2022).
NIEHS (National Institute of Environmental Health Sciences). 2021a. Flame Retardants. https://www.niehs.nih.gov/health/topics/agents/flame_retardants/index.cfm.
NIEHS. 2021b. About the Worker Training Program (WTP). https://www.niehs.nih.gov/careers/hazmat/about_wetp/index.cfm (accessed March 24, 2022).
NIOSH (National Institute for Occupational Safety and Health). 2011. Sodium Cyanide: Systemic Agent. https://www.cdc.gov/niosh/ershdb/emergencyresponsecard_29750036.html (accessed March 22, 2022).
NIOSH. 2014. Isocyanates. https://www.cdc.gov/niosh/topics/isocyanates/default.html (accessed March 22, 2022).
NIOSH. 2019a. Lead & Other Heavy Metals – Reproductive Health. https://www.cdc.gov/niosh/topics/repro/heavymetals.html (accessed March 22, 2022).
NIOSH. 2019b. Fighting Wildfires – Hazards During Cleanup Work. https://www.cdc.gov/niosh/topics/firefighting/cleanup.html (accessed 2022).
NTP (National Toxicology Program). 2016. NTP Monograph: Immunotoxicity Associated with Exposure to Perfluorooctanoic Acid or Perfluorooctane Sulfonate. https://ntp.niehs.nih.gov/ntp/ohat/pfoa_pfos/pfoa_pfosmonograph_508.pdf.
O’Dell, K., R. S. Hornbrook, W. Permar, E. J. T. Levin, L. A. Garofalo, E. C. Apel, N. J. Blake, A. Jarnot, M. A. Pothier, D. K. Farmer, L. Hu, T. Campos, B. Ford, J. R. Pierce, and E. V. Fischer. 2020. “Hazardous Air Pollutants in Fresh and Aged Western US Wildfire Smoke and Implications for Long-Term Exposure.” Environmental Science & Technology 54 (19): 11838–11847. https://doi.org/10.1021/acs.est.0c04497.
O’Donnell, M. H., and A. M. Behie. 2015. “Effects of Wildfire Disaster Exposure on Male Birth Weight in an Australian Population.” Evolution, Medicine, and Public Health. https://doi.org/10.1093/emph/eov027.
O’Neill, S. M., M. Diao, S. Raffuse, M. Al-Hamdan, M. Barik, Y. Jia, S. Reid, Y. Zou, D. Tong, J. J. West, J. Wilkins, A. Marsha, F. Freedman, J. Vargo, N. K. Larkin, E. Alvarado, and P. Loesche. 2021. “A Multi-analysis Approach for Estimating Regional Health Impacts from the 2017 Northern California Wildfires.” Journal of the Air & Waste Management Association 71 (7): 791–814. https://doi.org/10.1080/10962247.2021.1891994.
Onwuka, J. U., D. Li, Y. Liu, H. Huang, J. Xu, Y. Liu, Y. Zhang, and Y. Zhao. 2020. “A Panel of DNA Methylation Signature from Peripheral Blood May Predict Colorectal Cancer Susceptibility. BMC Cancer 20 (1): 692. https://doi.org/10.1186/s12885-020-07194-5.
Oregon DCBS (Oregon Department of Consumer and Business Services). 2021. Adoption of Temporary Rules to Address Employee Exposure to Wildfire Smoke. https://osha.oregon.gov/OSHARules/adopted/2021/ao9-2021-letter-temp-wildfire-smoke.pdf.
Orr, A., C. A. L. Migliaccio, M. Buford, S. Ballou, and C. T. Migliaccio. 2020. “Sustained Effects on Lung Function in Community Members Following Exposure to Hazardous PM2.5 Levels from Wildfire Smoke.” Toxics 8 (3): 53.
Paveglio, T. B., T. Prato, D. Dalenberg, and T. Venn. 2014. “Understanding Evacuation Preferences and Wildfire Mitigations among Northwest Montana Residents.” International Journal of Wildland Fire 23 (3): 435–444. https://doi.org/10.1071/WF13057.
Perera, F. P. 2008. “Children Are Likely to Suffer Most from Our Fossil Fuel Addiction.” Environmental Health Perspectives 116 (8). https://doi.org/10.1289/ehp.11173.
Petrowski, K., S. Bührer, B. Strauß, O. Decker, and E. Brähler. 2021. “Examining Air Pollution (PM10), Mental Health and Well-Being in a Representative German Sample.” Scientific Reports 11: 18436. https://doi.org/10.1038/s41598-021-93773-w.
Pleil, J. D., M. A. Stiegel, and K. W. Fent. 2014. “Exploratory Breath Analyses for Assessing Toxic Dermal Exposures of Firefighters during Suppression of Structural Burns.” Journal of Breath Research 8 (3). https://doi.org/10.1088/1752-7155/8/3/037107.
Plumlee, G. S., D. A. Martin, T. Hoefen, R. Kokaly, P. Hageman, A. Eckberg, G. P. Meeker, M. Adams, M. Anthony, and P. J. Lamothe. 2007. Preliminary Analytical Results for Ash and Burned Soils from the October 2007 Southern California Wildfires. Report 2007-1407. Reston, VA: United States Geological Survey.
Proctor, C. R., J. Lee, D. Yu, A. D. Shah, and A. J. Whelton. 2020. “Wildfire Caused Widespread Drinking Water Distribution Network Contamination. AWWA Water Science 2 (4). https://doi.org/10.1002/aws2.1183.
Pukkala, E., J. I. Martinsen, E. Weiderpass, K. Kjarheim, E. Lynge, L. Tryggvadottir, P. Sparen, and P. A. Demers. 2014. “Cancer Incidence Among Firefighters: 45 Years of Follow-Up in Five Nordic Countries.” Occupational and Environmental Medicine 71 (6). http://doi.org/10.1136/oemed-2013-101803.
Ray, M. R., C. Basu, S. Mukherjee, S. Roychowdhury, and T. Lahiri. 2005. “Micronucleus Frequencies and Nuclear Anomalies in Exfoliated Buccal Epithelial Cells of Firefighters.” International Journal of Human Genetics 5 (1): 45–48. https://doi.org/10.1080/09723757.2005.11885915.
Reid, C. E., and M. M. Maestas. 2019. “Wildfire Smoke Exposure under Climate Change: Impact on Respiratory Health of Affected Communities.” Current Opinion in Pulmonary Medicine 25 (2). https://doi.org/10.1097/MCP.0000000000000552.
Reid, C. E., M. Brauer, F. H. Johnston, M. Jerrett, J. R. Balmes, and C. T. Elliott. 2016a. “Critical Review of Health Impacts of Wildfire Smoke Exposure.” Environmental Health Perspectives 124 (9): 1334–1343. https://doi.org/10.1289/ehp.1409277.
Reid, C. E., M. Jerrett, I. B. Tager, M. L. Petersen, J. K. Mann, and J. R. Balmes. 2016b. “Differential Respiratory Health Effects from the 2008 Northern California Wildfires: A Spatiotemporal Approach.” Environmental Research 150: 227–235. https://doi.org/10.1016/j.envres.2016.06.012.
Reinhardt, T. E., and R. D. Ottmar. 2004. “Baseline Measurements of Smoke Exposure Among Wildland Firefighters.” Journal of Occupational and Environmental Hygiene 1 (9). https://doi.org/10.1080/15459620490490101.
Reisen, F., and S. K. Brown. 2009. “Australian Firefighters’ Exposure to Air Toxics during Bushfire Burns of Autumn 2005 and 2006.” Environmental International 35 (2): 342–352. https://doi.org/10.1016/j.envint.2008.08.011.
Reisen, F., J. C. Powell, M. Dennekamp, F. H. Johnston, and A. J. Wheeler. 2019. “Is Remaining Indoors an Effective Way of Reducing Exposure to Fine Particulate Matter During Biomass Burning Events?” Journal of the Air & Waste Management Association 69 (5). https://doi.org/10.1080/10962247.2019.1567623.
Resnick, A., B. Woods, H. Krapfl, and B. Toth. 2015. “Health Outcomes Associated with Smoke Exposure in Albuquerque, New Mexico, during the 2011 Wallow Fire.” Journal of Public Health Management and Practice 21: S55–S61. https://doi.org/10.1097/PHH.0000000000000160.
Reuter, S., S. C. Gupta, M. M. Chaturvedi, and B. B. Aggarwal. 2010. “Oxidative Stress, Inflammation, and Cancer: How Are They Linked?” Free Radical Biology and Medicine 49 (11): 1603–1616. https://doi.org/10.1016/j.freeradbiomed.2010.09.006.
Revi, A., D. Satterthwaite, F. Aragón-Durand, et al. 2014. “Towards Transformative Adaptation in Cities: The IPCC’s Fifth Assessment.” Environment and Urbanization 26 (1): 11–28. https://doi.org/10.1177/0956247814523539.
Robinson, M. S., T. R. Anthony, S. R. Littau, P. Herckes, X. Nelson, G. S. Poplin, and J. L. Burgess. 2008. “Occupational PAH Exposures during Prescribed Pile Burns.” Annals of Occupational Hygiene 52 (6): 497–508. https://doi.org/10.1093/annhyg/men027.
Rooney, B., Y. Wang, J. H. Jiang, B. Zhao, Z.-C. Zeng, and J. H. Seinfeld. 2020. “Air Quality Impact of the Northern California Camp Fire of November 2018.” Atmospheric Chemistry and Physics 20 (23): 14597–14616. https://doi.org/10.5194/acp-20-14597-2020.
Rota, M., C. Bosetti, S. Boccia, P. Boffetta, and C. La Vecchia. 2014. “Occupational Exposures to Polycyclic Aromatic Hydrocarbons and Respiratory and Urinary Tract Cancers: An Updated Systematic Review and a Meta-Analysis to 2014.” Archives of Toxicology 88 (8): 1479–1490. https://doi.org/10.1007/s00204-014-1296-5.
Rothman, N., D. P. Ford, M. E. Baser, J. A. Hansen, T. O’Toole, M. S. Tockman, and P. T. Strickland. 1991. “Pulmonary Function and Respiratory Symptoms in Wildland Firefighters.” Journal of Occupational and Environmental Medicine 33 (11). https://doi.org/10.1097/00043764-199111000-00013.
Rothman, N., M. C. Poirier, R. A. Haas, A. Correa-Villasenor, P. Ford, J. A. Hansen, T. O’Toole, and P. T. Strickland. 1993. “Assocation of PAH-DNA Adducts in Peripheral White Blood Cells with Dietary Exposure to Polyaromatic Hydrocarbons.” Environmental Health Perspectives 99: 265–267. https://doi.org/10.1289/ehp.9399265.
Rudolph, L., C. Harrison, L. Buckley, and S. North. 2018. Climate Change, Health, and Equity: A Guide for Local Health Departments. Oakland, CA and Washington, DC: Public Health Institute and American Public Health Association.
Rust, A. J., T. S. Hogue, S. Saxe, and J. McCray. 2018. “Post-fire Water-Quality Response in the Western United States.” International Journal of Wildland Fire 27 (3). https://doi.org/10.1071/wf17115.
Sacks, J. D., L. W. Stanek, T. J. Luben, D. O. Johns, B. J. Buckley, J. S. Brown, and M. Ross. 2011. “Particulate Matter–Induced Health Effects: Who Is Susceptible?” Environmental Health Perspectives 119 (4). https://doi.org/10.1289/ehp.1002255.
Samet, J. M., S. M. Holm, and S. Jayaraman. 2022. “Respiratory Protection for the Nation: A Report from the National Academies of Sciences, Engineering, and Medicine.” Journal of the American Medical Association 327 (11): 1023–1024. https://doi.org/10.1001/jama.2022.1318.
Semmens, E. O., J. Domitrovich, K. Conway, and C. W. Noonan. 2016. “A Cross-Sectional Survey of Occupational History as a Wildland Firefighter and Health.” American Journal of Industrial Medicine 59 (4). https://doi.org/10.1002/ajim.22566.
Shaw, S. D., M. L. Berger, J. H. Harris, S. H. Yun, Q. Wu, C. Liao, A. Blum, A. Stefani, and K. Kannan. 2013. “Persistent Organic Pollutants Including Polychlorinated and Polybrominated Dibenzo-p-Dioxins and Dibenzofurans in Firefighters from Northern California.” Chemosphere 91 (10): 1386–1394. https://doi.org/10.1016/j.chemosphere.2012.12.070.
Sheldon, T. L., and C. Sankaran. 2017. “The Impact of Indonesian Forest Fires on Singaporean Pollution and Health.” American Economic Review 107 (5): 526–529. https://doi.org/10.1257/aer.p20171134.
Shi, Y. L. 2021. Polycyclic Aromatic Hydrocarbons in Settled House Dust. University of Toronto, Toronto, ON. Masters of Applied Science.
Singer, B. C., W. W. Delp, D. R. Black, and I. S. Walker. 2017. “Measured Performance of Filtration and Ventilation Systems for Fine and Ultrafine Particles and Ozone in an Unoccupied Modern California House.” Indoor Air 27: 780–790. https://doi.org/10.1111/ina.12359.
Sparks, T. L., and J. Wagner. 2021. “Composition of Particulate Matter during a Wildfire Smoke Episode in an Urban Area.” Aerosol Science and Technology 55 (6): 734–747. https://doi.org/10.1080/02786826.2021.1895429.
Staack, S. D., S. C. Griffin, V. S. T. Lee, E. A. Lutz, and J. L. Burgess. 2021. “Evaluation of CBRN Respirator Protection in Simulated Fire Overhaul Settings.” Annals of Work Exposures and Health 65 (7): 843–853. https://doi.org/10.1093/annweh/wxab004.
Stasiewicz, A. M., and T. B. Paveglio. 2021. “Preparing for Wildfire Evacuation and Alternatives: Exploring Influences on Residents’ Intended Evacuation Behaviors and Mitigations.” International Journal of Disaster Risk Reduction 58. https://doi.org/10.1016/j.ijdrr.2021.102177.
State of California. n.d. California Code of Regulations, Title 8, Section 5141.1. “Protection from Wildfire Smoke.” https://www.dir.ca.gov/title8/5141_1.html.
State of Washington. 2021. Wildfire Smoke. https://lni.wa.gov/rulemaking-activity/AO21-26/2126CR103EAdoption.pdf.
Stec, A. A. 2017. “Fire Toxicity – The Elephant in the Room?” Fire Safety Journal 91: 79–90.
Stec, A. A., K. E. Dickens, M. Salden, F. E. Hewitt, D. P. Watts, P. E. Houldsworth, and F. L. Martin. 2018. “Occupational Exposure to Polycyclic Aromatic Hydrocarbons and Elevated Cancer Incidence in Firefighters.” Scientific Reports 8 (1): 2476. https://doi.org/10.1038/s41598-018-20616-6.
Stein, E. D., J. S. Brown, T. S. Hogue, M. P. Burke, and A. Kinoshita. 2012. “Stormwater Contaminant Loading Following Southern California Wildfires.” Environmental Toxicology and Chemistry 31 (11): 2625–2638. https://doi.org/10.1002/etc.1994.
Sugerman, D. E., J. M. Keir, D. L. Dee, H. Lipman, S. H. Waterman, M. Ginsberg, and D. B. Fishbein. 2012. “Emergency Health Risk Communication During the 2007 San Diego Wildfires: Comprehension, Compliance, and Recall.” Journal of Health Communication 17 (6): 698–712. https://doi.org/10.1080/10810730.2011.635777.
Sun, X., X. Luo, C. Zhao, B. Zhang, J. Tao, Z. Yang, W. Ma, and T. Liu. 2016. “The Associations between Birth Weight and Exposure to Fine Particulate Matter (PM2.5) and Its Chemical Constituents during Pregnancy: A Meta-Analysis.” Environmental Pollution 211: 38e47. http://doi.org/10.1016/j.envpol.2015.12.022.
Sun, Y., A. Mousavi, S. Masri, and J. Wu. 2022. “Socioeconomic Disparities of Low-Cost Air Quality Sensors in California, 2017–2020.” American Journal of Public Health 112 (3): 434–442. https://doi.org/10.2105/AJPH.2021.306603.
Tam, N., and C. Adams. 2019. Characterization of Air Quality During the 2016 Horse River Wildfire Using Permanent and Portable Monitoring. Edmonton, AB: Government of Alberta, Ministry of Environment and Parks.
Tinling, M. A., J. J. West, W. E. Cascio, V. Kilaru, and A. G. Rappold. 2016. “Repeating Cardiopulmonary Health Effects in Rural North Carolina Population during a Second Large Peat Wildfire.” Environmental Health 15 (12). https://doi.org/10.1186/s12940-016-0093-4.
To, P., E. Eboreime, and V. I. O. Agyapong. 2021. “The Impact of Wildfires on Mental Health: A Scoping Review.” Behavioral Sciences (Basel) 11 (9): 126. https://doi.org/10.3390/bs11090126.
Underwriters Laboratories. 2021. DIY Box Fan Air Cleaner Safety Tips. https://chemicalinsights.org/wp-content/uploads/Box_Fan_Handout_090921.pdf (accessed February 23, 2022).
USGS (United States Geological Survey). 2012. Wildfire Effects on Source-Water Quality—Lessons from Fourmile Canyon Fire, Colorado, and Implications for Drinking-Water Treatment. Reston, VA: United States Geological Survey.
Uzun, H., R. A. Dahlgren, C. Olivares, C. U. Erdem, T. Karanfil, and A. T. Chow. 2020. “Two Years of Post-wildfire Impacts on Dissolved Organic Matter, Nitrogen, and Precursors of Disinfection By-products in California Stream Waters.” Water Research 181: 115891. https://doi.org/10.1016/j.watres.2020.115891.
Vanos, J. K. 2015. “Children’s Health and Vulnerability in Outdoor Microclimates: A Comprehensive Review.” Environment International 76: 1–15. https://doi.org/10.1016/j.envint.2014.11.016.
Vinck, P., P. N. Pham, L. E. Fletcher, and E. Stover. 2009. “Inequalities and Prospects: Ethnicity and Legal Status in the Construction Labor Force After Hurricane Katrina.” Organization & Environment 22 (4): 470–478. https://doi.org/10.1177/1086026609347192.
Wang, L., J. A. Aakre, R. Jiang, R. S. Marks, Y. Wu, J. Chen, S. N. Thibodeau, V. S. Pankratz, and P. Yang. 2010. “Methylation Markers for Small Cell Lung Cancer in Peripheral Blood Leukocyte DNA.” Journal of Thoracic Oncology 5 (6). https://doi.org/10.1097/jto.0b013e3181d6e0b3.
Ward, D. E., and C. C. Hardy. 1991. “Smoke Emissions from Wildland Fires.” Environment International 17 (2–3): 117–134. https://doi.org/10.1016/0160-4120(91)90095-8.
Wentworth, G. R., Y. A. Aklilu, M. S. Landis, and Y. M. Hsu. 2018. “Impacts of a Large Boreal Wildfire on Ground Level Atmospheric Concentrations of PAHs, VOCs and Ozone.” Atmospheric Environment 178: 19–30. https://doi.org/10.1016/j.atmosenv.2018.01.013.
Wettstein, Z. S., S. Hoshiko, J. Fahimi, R. J. Harrison, W. E. Cascio, and A. G. Rappold. 2018. “Cardiovascular and Cerebrovascular Emergency Department Visits Associated with Wildfire Smoke Exposure in California in 2015.” Journal of the American Heart Association 7 (8). https://doi.org/10.1161/JAHA.117.007492.
Wolf, R. E., S. A. Morman, P. L. Hageman, T. M. Hoefen, and G. S. Plumlee. 2011. “Simultaneous Speciation of Arsenic, Selenium, and Chromium: Species Stability, Sample Preservation, and Analysis of Ash and Soil Leachates.” Analytical and Bioanalytical Chemistry 401 (9): 2733–2745. https://doi.org/10.1007/s00216-011-5275-x.
Wong, S. D., J. C. Broader, and S. A. Shaheen. 2020. Review of California Wildfire Evacuations from 2017 to 2019. Berkeley, CA: University of California Institute of Transportation Studies. https://doi.org/10.7922/G29G5K2R.
Woo, S. H. L., J. C. Liu, X. Yue, L. J. Mickley, and M. L. Bell. 2020. “Air Pollution from Wildfires and Human Health Vulnerability in Alaskan Communities under Climate Change.” Environmental Research Letters 15 (9). https://doi.org/10.1088/1748-9326/ab9270.
Writer, J. H., A. Hohner, J. Oropeza, A. Schmidt, K. M. Cawley, and F. L. Rosario-Ortiz. 2014. “Water Treatment Implications after the High Park Wildfire, Colorado.” Journal – American Water Works Association 106 (4): E189–E199. https://doi.org/10.5942/jawwa.2014.106.0055.
Wu, Y., A. Arapi, J. Huang, B. Gross, and F. Moshary. 2018. “Intra-continental Wildfire Smoke Transport and Impact on Local Air Quality Observed by Ground-Based and Satellite Remote Sensing in New York City. Atmospheric Environment 187: 266–281. https://doi.org/10.1016/j.atmosenv.2018.06.006.
Xiang, J., C. Huang, J. Shirai, Y. Liu, N. Carmona, C. Zuidema, E. Austin, T. Gould, T. Larson, and E. Seto. 2021. “Field Measurements of PM2.5 Infiltration Factor and Portable Air Cleaner Effectiveness during Wildfire Episodes in US Residences.” Science of the Total Environment 773. https://doi.org/10.1016/j.scitotenv.2021.145642.
Xu, R., P. Yu, M. J. Abramson, F. H. Johnston, J. M. Samet, M. L. Bell, A. Haines, K. L. Ebi, S. Li, and Y. Guo. 2020. “Special Report: Wildfires, Global Climate Change, and Human Health.” New England Journal of Medicine 383 (22). https://doi.org/10.1056/NEJMsr2028985.
Ye, Q., J. E. Krechmer, J. D. Shutter, V. P. Barber, Y. Li, E. Helstrom, . . . and J. H. Kroll. 2021. “Real-Time Laboratory Measurements of VOC Emissions, Removal Rates, and Byproduct Formation from Consumer-Grade Oxidation-Based Air Cleaners.” Environmental Science & Technology Letters 8 (12): 1020–1025.
Zauscher, M. D., Y. Wang, M. J. K. Moore, C. J. Gaston, and K. A. Prather. 2013. “Air Quality Impact and Physicochemical Aging of Biomass Burning Aerosols during the 2007 San Diego Wildfires.” Environmental Science & Technology 47 (14): 7633–7643. https://doi.org/10.1021/es4004137.
Zeliger, H. I. 2003. “Toxic Effects of Chemical Mixtures.” Archives of Environmental Health: An International Journal 58 (1): 23–29.
Zhou, J., T. G. Jenkins, A. M. Jung, K. S. Jeong, J. Zhai, E. T. Jacobs, S. C. Griffin, D. Dearmon-Moore, S. R. Littau, W. F. Peate, N. A. Ellis, P. Lance, Y. Chen, and J. L. Burgess. 2019. “DNA Methylation among Firefighters.” PLoS One. https://doi.org/10.1371/journal.pone.0214282.
Zhou, X., K. Josey, L. Kamareddine, M. C. Caine, T. Liu, L. J. Mickley, M. Cooper, and F. Dominici. 2021. “Excess of COVID-19 Cases and Deaths Due to Fine Particulate Matter Exposure during the 2020 Wildfires in the United States.” Scientific Advances 7 (33): eabi8789. https://doi.org/10.1126/sciadv.abi8789.








































