
Proceedings of a Workshop
WORKSHOP OVERVIEW1
The COVID-19 pandemic has created a time fraught with uncertainty and fear, but also a time of action, said Nancy Davidson, president and executive director of the Seattle Cancer Care Alliance and senior vice president, director, and professor in the Clinical Research Division at the Fred Hutchinson Cancer Center. As the SARS-CoV-2 virus swept through communities across the globe, health systems, clinicians, and the clinical research community took actions to protect patients, their families, and their clinical teams; to ensure continuity of cancer care amid an ongoing public health crisis; and to continue the important work of conducting clinical cancer research. To facilitate these efforts, health care regulators and payers rapidly made adjustments to help adapt cancer care and cancer research to meet the evolving needs across the health care and research enterprises. Pharmaceutical companies shifted their priorities to develop vaccines and therapeutics for COVID-19, while adapting their ongoing drug development operations to advance progress in oncology care and other disease areas.
___________________
1 The planning committee’s role was limited to planning the workshop, and this Proceedings of a Workshop was prepared by the workshop rapporteurs as a factual summary of what occurred at the workshop. Statements, recommendations, and opinions expressed are those of the individual presenters and participants, and are not necessarily endorsed or verified by the National Academies of Sciences, Engineering, and Medicine, and they should not be construed as reflecting any group consensus.
This workshop, Innovation in Cancer Care and Cancer Research in the Context of the COVID-19 Pandemic, was organized by the National Cancer Policy Forum of the National Academies of Sciences, Engineering, and Medicine. Held virtually on July 26–27, 2021, the workshop provided an opportunity to examine the short- and long-term responses to the pandemic, and to consider lessons learned from this experience in order to improve the delivery of high-quality cancer care and the conduct of cancer clinical trials in the post-pandemic era. Richard Schilsky, professor emeritus at the University of Chicago, said the pandemic could have long-lasting implications for cancer research and care, and noted that the pandemic illustrated the critical need for “flexibility, collaboration, communication, use of telehealth, cooperation, building trust in communities, and paying attention to the importance of the social determinants of health to achieve equitable care and research. All of these things are essential for us to improve our health care system, improve the way in which we deliver care, improve access to high-quality cancer care
for all people, and to make our research as accessible and efficient as possible,” Schilsky said. Samir Khleif, professor of oncology and director of the Center of Immunology and Immunotherapy at Georgetown University, agreed, noting that the oncology field should capitalize on this current sense of urgency to advance priorities for improved care.
This Proceedings of a Workshop summarizes the issues discussed at the workshop and highlights observations and suggestions from individual participants, which are discussed throughout the Proceedings and summarized in Boxes 1 and 2, respectively. The workshop included presentations and discussions on clinical practice changes—such as increased use of telehealth—and adaptations to clinical trial design and conduct that were implemented at the start of the pandemic and continued to evolve as the pandemic progressed. Workshop participants also discussed their suggestions to retain and build on the beneficial changes that have occurred, as well as the policy, practice, and research challenges that still need to be overcome to spur progress in the
delivery of high-quality, equitable cancer care and cancer research. Appendix A includes the Statement of Task for the workshop, and the agenda is provided in Appendix B. The workshop webcast and speaker presentations are available online.2
CANCER CARE DELIVERY DURING THE COVID-19 PANDEMIC
The COVID-19 pandemic affected health care systems globally and resulted in care disruptions for many patients, said Shonta Chambers, executive vice president of Health Equity Initiatives and Community Engagement at the Patient Advocate Foundation. During the pandemic, health care staff and resources were diverted to care for the surge of individuals diagnosed with COVID-19, and some aspects of in-person health care were suspended to prevent further transmission of the SARS-CoV-2 virus. In some cases, this resulted in delays, cancellations, and modifications to the delivery of cancer care, including cancer screening as well as cancer treatment (e.g., surgery, radiation therapy, and chemotherapy) (ACS, 2020; Mitchell, 2020; Schrag et al., 2020).
As described in the next sections, several workshop speakers discussed how members of the cancer community—including clinicians, administrators, payers, and professional organizations—responded to the crisis and made adaptations to the delivery of oncology care. Also, a number of speakers said the rapid and widespread adoption of telehealth was among the most dramatic changes in cancer care during the COVID-19 pandemic. As health care systems and clinical trials restricted in-person visits to protect patients and staff, many adopted video or audio calls for live, virtual clinician–patient encounters, as well as in-home health monitoring tools and technologies for asynchronous interactions.
Adapting Oncology Care Practices
Randall Oyer, medical director of the Ann B. Barshinger Cancer Institute at Penn Medicine Lancaster General Health and past president of the Association of Community Cancer Centers, discussed community oncology practice efforts to uphold their important role of providing high-quality, patient-driven care during the pandemic. Oyer said he helped establish a Community
___________________
2 See https://www.nationalacademies.org/event/07-26-2021/cancer-care-and-cancer-research-in-the-context-of-the-covid-19-pandemic-a-workshop-on-lessons-learned (accessed December 15, 2021).
Oncology COVID-19 Collaborative within his local area, with the goals of (1) preserving hospital resources to care for individuals diagnosed with COVID-19; (2) providing emergency back-up cancer care capacity for smaller oncology practices; and (3) creating the communication channels to share information, resources, and approaches to cancer care during the pandemic. The Collaborative invited local oncology clinicians and practice administrators to participate in weekly conference calls and adopted the Penn Medicine principles for cancer care in the context of the COVID-19 pandemic.3 Participants discussed ethical challenges to cancer care delivery, tested strategies for practice operations and oncology care, extended outreach to community partners caring for vulnerable populations (e.g., nursing homes, extended care facilities, and prisons), and held case discussion conferences to support safe, equitable care for patients.
Nationally, Oyer noted that the Association of Community Cancer Centers created a community-focused national educational initiative for cancer care during the COVID-19 pandemic that offered webcasts, podcasts, and a peer forum to share up-to-date information on topics such as infection control measures, risk stratification for patients with cancer during the pandemic, COVID-19 testing strategies, staffing and care coordination, and modifications to cancer treatment protocols.
Steven Pergam, associate professor in the Vaccine and Infectious Diseases Division at the Fred Hutchinson Cancer Center and medical director of infection prevention at the Seattle Cancer Care Alliance, provided a health system perspective on cancer care delivery during the pandemic. Because Seattle had some of the first patients diagnosed with community-acquired COVID-19 in the United States, Pergam said adapting to changing circumstances quickly became a top priority. He noted that cancer centers were already well positioned to protect their patient populations, who are vulnerable to severe illness from respiratory infections. Cancer center staff are well trained and focused on infection prevention; cancer centers have policies in place to avoid having ill staff members coming into work; patients and caregivers are well educated about the risks of community exposures to infectious disease; and many patients who were most vulnerable to infection were already taking measures to limit exposure in their daily lives. He added that cancer centers are well connected—through professional societies and multi-institutional collaborations—which enabled early sharing of policies, procedures, and experiences.
___________________
3 These general principles were put forward as very broad guidelines used at Penn Medicine. The principles include (1) When possible, the standard of care should be delivered. (2) Priority should be given to patients with potentially curable disease. (3) Patients who are receiving end-of-life care should receive their care at home via telehealth visits. (4) The age of a patient, as well as any comorbidities, should be considered in delivering their care.
Planning for a surge of COVID-19 inpatient admissions required changes to cancer care delivery, Pergam said. For example, because fewer intensive care unit beds were available for patients receiving cancer therapy, his cancer center prioritized bone marrow transplantations and CAR-T therapy for patients who were at highest risk of disease progression, and delayed these procedures for individuals with stable disease. COVID-19 modeling data were used to prepare for worst case scenarios, and although accuracy of modeling predictions varied, he said they effectively predicted peaks and enabled health care institutions to prepare for surges.
Pergam emphasized that cancer center staff needed to be flexible and take on a variety of roles in response to the rapidly changing environment. In addition, the cancer center built offsite testing capacity for patients and staff, created an app-based COVID-19 screening process, increased pre-visit patient communication and virtual symptom monitoring, and used social media to disseminate information to patients, families, and caregivers (Ueda Oshima et al., 2021; Woodfield et al., 2021).
Karen Knudsen, chief executive officer of the American Cancer Society and the American Cancer Society Cancer Action Network,4 discussed strategies employed by the Sidney Kimmel Cancer Center at Jefferson Health in response to the pandemic; she was serving as the enterprise director when the pandemic began. She noted that Jefferson Health serves a diverse and densely populated area with a high cancer burden; this population also faced a very high COVID-19 infection rate.
Knudsen said that during the first peak of the pandemic, from March to June 2020, Sidney Kimmel Cancer Center created a command center for rapid communication among the cancer center leadership, emphasizing evidence-based decision making and inclusion of infectious disease expertise. Knudsen noted that surgical oncology procedures and clinical trials with curative intent were considered “essential” and allowed to continue. The use of telehealth—which was in place prior to the pandemic—was escalated, and the cancer center provided backup oncology care capacity if community practices were unable to deliver care. Knudsen said that in the lull that followed from July to September 2020, staff were able to use the time to prepare for the next peak, ramp up mental health care services for patients and staff, and initiate new oncology clinical trials. When the second peak began, the team resumed daily incident command communication. Knudsen noted that based on lessons learned during the first peak, staff were able to improve their ability to help patients navigate through the complex care challenges posed by COVID-19. Knudsen highlighted four key lessons learned from their experiences during
___________________
4 Knudsen is the former executive vice president of oncology services and enterprise director of the Sidney Kimmel Cancer Center at Jefferson Health.
the pandemic: (1) prepare oncology teams by supporting competency development in emerging technologies (e.g., telehealth); (2) increase use of rapid communication platforms for care teams across different geographic settings; (3) include key participants in cancer policy decision making (e.g., infectious disease expertise); and (4) develop emergency plans within the local geographic area, including community oncology practices and community advocates.
Telehealth in Cancer Care Delivery
Inga Lennes, senior vice president of ambulatory care and patient experience at Massachusetts General Hospital and the Massachusetts General Physicians Organization, said that scaling virtual care across such a large enterprise required careful deliberation about practice operations, platform and technology optimization, as well as policy and regulatory considerations, which will be critical to sustaining virtual care in the future. Efforts to improve practice operations included standardizing workflows, facilitating scheduling, and making adjustments when best practices are identified, Lennes said. Because Massachusetts General Hospital serves many patients who live outside of the state, the scheduling technology platform also needed to build in decision trees to help schedulers pair these patients with appropriately licensed clinicians.
Lennes said Massachusetts General Hospital is prioritizing health equity in its implementation of telehealth services. She said the enterprise dashboard for virtual care prominently features statistics on access to virtual care by race and ethnicity, helping the organization to monitor patients’ virtual and in-person experiences and to address identified disparities. In addition, the institution implemented a number of interventions aimed at improving health equity, such as employing digital access coordinators, offering multiple language options, and loaning devices to patients to enable telehealth connections. Lennes noted that researchers are examining the effectiveness of these and other interventions, the optimal deployment of virtual care, patient acceptance of virtual care modalities, and the impact of virtual care on condition-specific research.
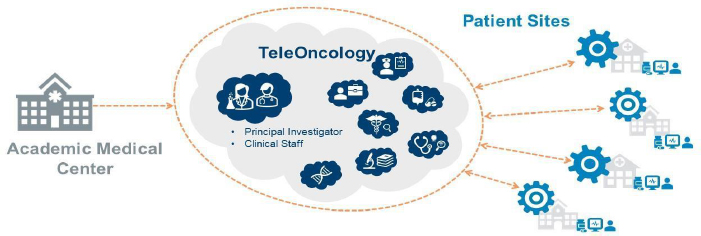
Michael Kelley, professor of medicine at Duke University Medical Center and national program director for oncology at the Department of Veterans Affairs (VA), discussed the use of telehealth within the VA health system. Just prior to the pandemic, the VA had launched its TeleOncology Service, which “seeks to realign the supply and demand for oncologists with a primary goal to improve access to care for veterans with cancer, including improving timeliness of cancer care.” He said that oncology telehealth visits increased dramatically during the pandemic. The TeleOncology Service consists of a central virtual hub, which includes access to specialized expertise, and “spokes,” community sites of care that offer patients with cancer more conveniently located access to cancer care (see Figure 1).

NOTE: NCI = National Cancer Institute, PET = positron emission tomography.
SOURCE: Kelley presentation, July 26, 2021.
Shelley Fuld Nasso, chief executive officer of the National Coalition for Cancer Survivorship (NCCS), discussed results from NCCS surveys that asked cancer survivors for their experiences with care delivery during the pandemic. First, Fuld Nasso said that the Telehealth Project solicited input from 29 patients on their experience using telehealth via focus groups in May and June 2020. While some participants reported that telehealth visits offered more convenience, lower costs, and fewer barriers, others mentioned downsides, such as technology burdens and concerns about patient privacy.5 A subsequent survey, the annual State of Cancer Survivorship, was a nationally representative survey of more than 1,000 cancer survivors, which was complemented by in-depth interviews with a smaller group of cancer survivors (NCCS, 2021). Preliminary results show that respondents were generally satisfied with their cancer care and believed the pandemic did not greatly impact their care. Most had a favorable view of telehealth visits overall, though in-person appointments were preferred for most situations, with the strongest preference for in-person visits for first time visits and physical therapy. The only types of appointments in which respondents preferred telehealth were counseling and education, medication management, and sharing test results.
Payment Policies and Coverage Adjustments
Lee Fleisher, chief medical officer and director of the Center for Clinical Standards and Quality at the Centers for Medicare & Medicaid Services
___________________
5 See https://canceradvocacy.org/wp-content/uploads/NCCS-Telehealth-Project-Executive-Summary-2114.pdf (accessed November 2, 2021).
(CMS), discussed CMS actions to provide broad payment coverage for telehealth during the COVID-19 public health emergency, as well as the agency’s role in ensuring the delivery of high-quality health care—both in person and via telehealth—in the future. During the pandemic, he said CMS provided payment parity for virtual and in-person visits, but whether this will continue after the public health emergency is over is still being considered and may require statutory changes. Fleisher said the key issue for telehealth is understanding the contexts in which it is most appropriate, including whether video- or audio-based telehealth modalities achieve equivalent patient outcomes, and how telehealth affects access to care and disparities in patient outcomes.
Lara Strawbridge, director of the Division of Ambulatory Payment Models at the Center for Medicare & Medicaid Innovation (CMMI) at CMS, said that CMS made significant adjustments to payment policies to ensure patient access to care during the public health emergency resulting from the pandemic (see Table 1). For example, CMS launched the Hospital Without Walls and the Acute Hospital at Home programs, which provide broad regulatory flexibility to enable hospitals to provide services in locations beyond their existing walls (CMS, 2020a).
Strawbridge noted that CMMI also recognized the need for flexibility for its alternative payment models, and prioritized adjustments to financial methodologies, quality reporting, and model time lines (CMS, 2020b). Strawbridge said that changes to the Oncology Care Model focused on continuing value-based payment, minimizing financial risks to oncology practices, and reducing reporting burdens so clinicians could focus on patient needs and safety, especially if staff were diverted from administrative duties during the pandemic (CMS, 2020c). Strawbridge said that CMS is carefully evaluating the outcomes from these experiences, and noted that there is enthusiasm within the health care sector for continuing flexibilities for telehealth and in-home services. She added that CMS is also evaluating how altered care patterns and delayed cancer screenings will affect patient outcomes and post-pandemic cancer care delivery.
Bhuvana Sagar, a national medical executive at Cigna, said there was a dramatic decrease in the use of cancer screening during the early months of the pandemic. Sagar said Cigna responded by sending reminders to undergo screening, at-home screening kits for colorectal cancer, and patient education resources for tobacco cessation. Although screening rates were still lower than the prior year, she said rates began to improve in the latter part of 2020. Sagar said the incidence of new cancer diagnoses was lower in 2020 compared with 2019, but increased in the first 5 months of 2021: “We did not see any significant increase in [the diagnosis of] advanced-stage cancer so far, but we are monitoring [those] data as well.”
| Telehealth | People with Medicare could access telehealth services from their home. |
| Care by Phone | Patients could consult with a doctor, nurse practitioner, psychologist, and other clinicians with Medicare payment. |
| Rapidly Expand Health Care Workforce | A physician who had to self-quarantine could be recruited to provide care virtually, or oversee care delivered by other clinicians through interactive video/audio conferencing. Medicare paid for clinicians licensed in one state to provide care in a different state if they were needed. Health systems could provide care options that use population management strategies such as triaging based on COVID status or clinical status, employing physicians, nurses, and other staff to better manage high patient volumes. Clinicians who were not fully employed during the emergency were enabled to provide care in other areas. |
| Making the Most Use of Community Health Care Resources | Hospitals could transfer patients to different types of care units and facilities to keep patients safe and free up beds. |
| COVID-only Care Centers | During the public health emergency, hospitals and dialysis centers could set up COVID-only centers to help reduce virus transmission to others. |
| Expanding Hospital Capacity | Community resources such as hotels, convention centers, and surgery centers could be converted for hospital care. |
| Patients Over Paperwork | Administrative burdens were reduced dramatically and permitted frontline care providers to triage patients and coordinate care, despite high volume and extraordinary system stresses. By extending quality reporting deadlines and suspending medical necessity documentation, time was freed up to focus on patients. For example, documentation requirements for prior authorization were temporarily suspended. Additionally, regulatory changes provided temporary relief from many audit and quality reporting requirements so that care providers, health care facilities, Medicare Advantage health plans, Part D prescription drug plans, and states could focus on providing needed care to Medicare and Medicaid beneficiaries affected by COVID-19. |
SOURCES: Strawbridge presentation, July 26, 2021; https://www.cms.gov/files/document/covid-flexibilities-overview-graphic.pdf (accessed November 1, 2021).
She noted that Cigna informed its members of the expanded offerings for virtual care. Virtual visits for oncology care spiked during April and May, 2020, but she said they have leveled off. “We know that for oncology care, not all visits can or should be virtual. We need to continue to evolve and build effective models to determine who would be appropriate [to receive] virtual care going forward,” Sagar said.
Cigna’s strategic goals for 2021 include a focus on advancing health equity, Sagar said. For example, Cigna launched a new initiative to reimburse clinicians for conducting screening for the social determinants of health and for providing appropriate referrals to address the identified needs (Cigna, 2020).
Organizational Collaboration and Communication
Although the pandemic created enormous stresses for patients and clinicians, cancer-related professional organizations showed remarkable agility in responding to the rapidly evolving challenges and in seizing opportunities for collaboration and learning, said Lawrence Shulman, professor of medicine and deputy director for Clinical Services at the University of Pennsylvania’s Abramson Cancer Center. For example, he said that an ad hoc coalition of national cancer organizations—including the Commission on Cancer, National Accreditation Program for Breast Centers, American College of Radiology, American Society of Breast Surgeons, and National Comprehensive Cancer Network (NCCN)—rapidly came together in late March 2020 to produce recommendations for prioritization, treatment, and triage of patients with breast cancer during the pandemic (Dietz et al., 2020).
In addition, Shulman said that U.S. and international cancer centers, health systems, and hospitals quickly formed the COVID-19 and Cancer Consortium, whose goal is to collect data about patients with cancer who have been diagnosed with COVID-19 (Warner et al., 2020). NCCN created a COVID-19 task force to discuss and disseminate information related to the delivery of cancer care during the pandemic (e.g., patient and health care staff safety). Later in the pandemic, NCCN’s COVID-19 Vaccination Advisory Committee issued vaccination guidance for patients with cancer (Cinar et al., 2020; NCCN, 2021).
Shulman and Oyer noted that the COVID-19 pandemic enabled organizations that typically operate as competitors to work as collaborators with a joint mission to serve their communities using open communication and shared decision making. Knudsen noted that these partnerships enabled rapid communication about best practices for patient and health care staff safety and also fostered new collaborations.
Shulman said it will be important to preserve the powerful multidisciplinary collaborations that grew out of the pandemic, and continue rapid
information sharing to avoid the refragmentation of U.S. cancer care. “We should think about what we’ve learned, what we were able to do when the chips were down, and what we can do going forward. People’s lives are on the line if we don’t move things forward appropriately and safely, but as quickly as possible,” said Shulman.
Robert Winn, director of the Virginia Commonwealth University Massey Cancer Center and professor of pulmonary disease and critical care medicine at Virginia Commonwealth University, emphasized that the inclusion of community voices is critical to effectively respond to the public health emergency created by the pandemic. “The reality is people don’t really care how much you know until they know that you care,” Winn said, and stressed that the onus is on cancer centers and health care organizations to earn community trust, which requires the establishment of long-term, sustained relationships with communities.
Fuld Nasso said that from a patient advocacy perspective, it was heartening to see collaborations among clinicians, health systems, and payers to improve policies for patient care. Knudsen and Shulman added that while the relationships between clinicians and payers can often feel adversarial, it felt more collaborative during the pandemic.
COVID-19 and Social Determinants of Health
Many speakers noted that racial and ethnic minority populations and people with low socioeconomic status have been disproportionately affected by the COVID-19 pandemic (Balogun et al., 2020; Boserup et al., 2020; Lopez et al., 2021). Many individuals who are at increased risk of exposure to the virus are also at increased risk of developing cancer. In addition, patients with cancer are at an increased risk of poor outcomes from COVID-19 (Giannakoulis et al., 2020; Sun et al., 2021). Winn said it is clear that certain populations are bearing a disproportionate burden, and the primary drivers of these disparities are largely socioeconomic. Winn said that growing awareness of these persistent disparities coincided with nationwide protests about the systems and structures that contribute to racial injustice and disparities in America. “It has become clear that the social determinants of health that exist now cannot be separated from the history that created some of these structures and policies,” said Winn.
Chambers said that while the disproportionate impact of the COVID-19 pandemic drew widespread attention, most stories failed to report on the role of broader, unaddressed social risk factors—such as food insecurity and inadequate access to quality education and employment—that make some individuals more vulnerable to COVID-19 and also create enormous barriers to accessing care (Frankel and Tony, 2020; Hauck et al., 2020; Johnson and Buford, 2020; Oxley
et al., 2020). Chambers quoted Camara Phyllis Jones, who said, “We can reduce health disparities and better connect people to high-quality medical care, but to really make a difference, we need to address the social determinants of health and equity that protect some people and push others off the cliff” (Jones, 2021). Winn emphasized that cancer centers have a critical role to play to address the broad structural policies and issues that impact the social determinants of health.
Loretta Christensen, chief medical officer of the Indian Health Service (IHS) and a member of the Navajo Nation, said the social determinants of health have contributed to poor health outcomes among American Indian and Alaska Native populations. She said these social determinants of health were exacerbated during the COVID-19 pandemic, as many families already lacked access to running water and utilities; had poor cellular service; faced unmet transportation needs along with poor road infrastructure; had inadequate access to nutritious, affordable foods; and lacked opportunities for education. Many Tribal members do not have broadband Internet access, which she said has been particularly challenging for the delivery of telehealth during the pandemic.
There is also a lack of access to specialty expertise and culturally appropriate care, which has been problematic for the delivery of cancer care. Christensen added that Tribal communities continue to have distrust in the government due to their experiences with historical trauma. IHS and community leaders “spent a great deal of time during the COVID-19 pandemic trying to heal that so we could proceed with the [acceptance and uptake of] vaccines. I think by the numbers you can see we did a really excellent job, very much depending on the family community commitment that our Tribal members have to get vaccinated to protect their people,” she said.
Christensen said patients with cancer who are served by IHS would benefit from improved access to telehealth, satellite clinics, collaborative agreements with larger cancer centers for treatment, investment in culturally appropriate patient education, and increased support for community-based cancer screenings.
ADVANCING CANCER CARE DELIVERY IN A POST-PANDEMIC ERA
Many workshop participants discussed potential opportunities to improve care delivery and clinical cancer research in the post-pandemic era. Some speakers stressed the importance of improving patient access to care by enhancing the use of telehealth and other digital tools, redesigning payment models, and ensuring cancer center–level expertise is accessible to patients and clinicians in rural and underserved settings of care.
Lori Pierce, president of the American Society of Clinical Oncology (ASCO), and professor of radiation oncology and vice provost for academic
and faculty affairs at the University of Michigan, urged the cancer community to make the successful adaptations permanent in order to advance cancer care and patient outcomes, and to better position health care for the next public health emergency. She said the COVID-19 pandemic exposed and exacerbated existing barriers in access to high-quality, affordable cancer care, as well as a number of challenges in delivering oncology care, conducting clinical research, and ensuring clinician well-being (ASCO, 2021a). Pierce said the ASCO Road to Recovery Report recommends ways for clinical cancer researchers to increase trial access, efficiency, and flexibility. In addition, it encourages policy makers, payers, and clinicians to collaborate to improve care access and equity, enhance support for oncology practices in underserved communities, and protect patient safety (Pennell et al., 2021). Similarly, the 2020 Cancer Disparities Progress Report from the American Association for Cancer Research highlights how the pandemic exacerbated some health disparities despite expanded coverage under the Patient Protection and Affordable Care Act (AACR, 2020; Chen et al., 2021).
The report urges continued data collection to determine how, for example, screening delays during the pandemic affected underserved populations, especially in states without expanded Medicaid coverage (KFF, 2021; The Commonwealth Fund, 2021). “Cancer outcomes could be dramatically improved if we consistently apply what we already know and scale the lessons that we have already learned,” Pierce said. She added that existing interventions that have reduced racial disparities in cancer outcomes should be continued and scaled (Grubbs et al., 2013) and that the expanded use of telehealth should be made permanent.
Pierce said ASCO encourages community-based, real-world interventions that incorporate an understanding of the social determinants of health, and has developed Telemedicine Standards to improve access to cancer care and cancer clinical trials for vulnerable populations (Patel et al., 2020). Pierce stressed that implementation of post-pandemic interventions need to be carefully designed so they do not further exacerbate existing health disparities or contribute to clinicians’ administrative burdens.
The Future of Telehealth in Cancer Care
Several workshop speakers shared their experiences with telehealth that worked well during the pandemic. David Spigel, chief scientific officer at the Sarah Cannon Research Institute and medical oncologist at Tennessee Oncology, said their palliative care team found telehealth visits to be very effective because they were well received by patients and their families, and also faster and easier to conduct. William Dahut, scientific director for clinical research at the National Cancer Institute (NCI) Center for Cancer Research, said the
National Institutes of Health’s (NIH’s) Clinical Center’s telehealth service worked well. He noted that staff members practiced telehealth technology with patients beforehand to ensure no technical challenges were encountered. He suggested that this best practice could be applied in the context of routine care, as well as in the context of participation in a clinical trial.
Virtual visits also made it possible for long-distance family members to participate in patient appointments, said Larissa Nekhlyudov, professor of medicine at Harvard Medical School, internist with Brigham and Women’s Hospital, and clinical director for Internal Medicine for Cancer Survivors at the Dana-Farber Cancer Institute. She said that virtual engagement has worked particularly well for multi-person visits where everyone is virtual and caregivers or family members can participate more easily.
She said virtual encounters can also be useful for health professional education. Shulman emphasized that telehealth is not ideal for initial visits with patients experiencing their first cancer diagnosis, but he said they did enable consultations with patients who lived far away and were considering traveling for their care.
Robin Zon, medical oncologist and past president of Michiana Hematology Oncology, PC, discussed ASCO policy positions on telehealth in oncology (ASCO, 2020a,b, 2021b; Pennell et al., 2021). She said the ASCO Expert Panel on Telehealth, which she co-chairs, is developing recommendations for optimal strategies for telehealth in oncology, including issues such as when it is preferable to see patients in person versus via telehealth; implementation considerations for telehealth in the oncology setting; roles for advanced-practice providers and allied health professionals; virtual multidisciplinary cancer conferences; and the use of telehealth in cancer clinical trials. Zon said ASCO recommends that state and federal policy makers provide adequate and ongoing reimbursement for all modalities of telehealth, and that state and federal governments promote universal access to high-speed broadband by expanding digital infrastructure. ASCO has also urged federal and state governments to promote health equity by encouraging the use of telemedicine in all care settings, including safety net and rural settings of care.
Zon added that ASCO has asked medical liability insurers to include telemedicine- and data security–related risks in their policies, and that physicians need to verify that their medical liability plans provide coverage for provision of telemedicine services. Zon explained that prior to the pandemic, telehealth visits conducted across state lines typically required a clinician to be licensed in multiple states, which can pose barriers to patient access. These rules were relaxed in response to the public health emergency, but the use of trans-state telehealth may be limited again. She said that cross-state licensure could address this barrier going forward, and that ASCO supports state and federal policy action to permit the practice of telehealth across state lines,
with a provision requiring the doctor–patient relationship to be established prior to the provision of any telemedicine service, and advocates for all states to participate in the voluntary Interstate Medical Licensure Compact.6 Kelley also suggested that the VA’s cross-state licensure is a good model to consider.
Fleisher added that as states end their public health emergency declarations, multiple CMS flexibilities will be affected, including the ability to conduct telehealth across state lines. However, he said some value-based payment models are not bound by the CMS fee-for-service rules; as a result, he posited that the viability for continuing telehealth will likely depend on state rules.
Zon said patient preferences should drive decisions about the use of telehealth, as long as telehealth provides high-quality care (e.g., provides effective management of adverse events) and is not disruptive to clinical workflows (e.g., does not increase no-show rates). Nekhlyudov agreed that telehealth needs to incorporate patient priorities and perspectives. Fleisher suggested that the design of telehealth services should incorporate multidisciplinary perspectives, including diagnostic specialists who may be consulted about a patient’s cancer diagnosis, as well as nurses, physician assistants, and other health care professionals who assist with care communication and coordination. Knudsen added that hybrid telehealth approaches can be helpful if a specialist is not at one site full-time, or to relieve the logistical and economic challenges associated with running multidisciplinary clinics. Dahut and Zon both shared that their facilities and others already use this approach, offering virtual meetings to convene pathologists, radiologists, oncologists, and other clinicians, along with patients and their families.
Davidson also noted that she used telehealth successfully for multidisciplinary visits, and that this was especially appreciated by older patients who wanted to avoid in-person visits, although the inability to perform physical examinations during virtual appointments is a key drawback. Paul Jacobsen, associate director of the NCI Healthcare Delivery Research Program, pointed out that this model has been used successfully to provide mental health care, where a centrally located psychiatrist works with multiple clinicians to manage medications and monitor treatment adherence.
Lennes suggested that equipping patients with wearable technologies and conducting both telehealth and in-person visits could offer exciting opportunities to improve patient care and outcomes. She shared that Mass General is considering adding local hubs or kiosks in their community to improve access to virtual care. Kelley added that the VA is also considering the creation of telehealth “pods” located in veteran service organizations and large nationwide stores to serve rural patients. He said that effective practices built around patient preferences and convenience can help to overcome existing
___________________
6 See https://www.imlcc.org (accessed November 2, 2021).
barriers and meet the shared interests of clinicians, patients, and regulators. “The future looks bright, I think, in terms of moving medicine into a different environment,” Kelley said.
Michael McNeely, director of the Health Resources and Services Administration’s (HRSA’s) Office for the Advancement of Telehealth within the Federal Office of Rural Health Policy, said telehealth offers many benefits for patients, clinicians, and payers by providing much-needed access to care for rural and underserved populations, reducing care disruptions during public health emergencies, and serving as a cost-effective alternative to traditional in-person care delivery. However, key challenges to facilitating broader uptake include limited access to broadband, ongoing uncertainty regarding payment coverage for telehealth, as well as issues with licensure, credentialing, and prescribing across state lines. He added that many of the flexibilities that payers and states adopted during the pandemic are temporary and vary by state, such as lifting geographic practice restrictions, expanding services eligible for telehealth, and allowing audio-only calls.
As the use of telehealth grows, McNeely said HRSA will continue to monitor regulatory changes, build strong federal partnerships, and collaborate with research programs and government agencies to advance the field. Currently, HRSA funds several programs that intersect with telehealth and cancer care: the Telehealth Technology-Enabled Learning Program7 connects cancer specialists with clinicians who are caring for patients with complex disease; Telehealth Centers of Excellence8 study telehealth research and practice; and Telehealth Resource Centers9 provide technical assistance, education, and clinician resources. In addition, the Licensure Portability Program10 works to reduce regulatory barriers to interstate telehealth. McNeely said resources for patients and clinicians with telehealth questions can be found online at www.telehealth.hhs.gov.
Jacobsen discussed research initiatives to advance the use of telehealth across the cancer care continuum. He said telehealth has the potential to address longstanding challenges in cancer care delivery, such as improving access to care among underserved populations (e.g., patients with low incomes or those who live in rural areas).
___________________
7 See https://www.hrsa.gov/grants/find-funding/hrsa-21-107 (accessed November 2, 2021).
8 See https://www.hrsa.gov/grants/find-funding/hrsa-21-030 (accessed November 2, 2021).
9 See https://www.hrsa.gov/rural-health/telehealth/telehealth-resource-centers-trcs (accessed November 2, 2021).
10 See https://www.hrsa.gov/grants/find-funding/hrsa-19-019 (accessed November 2, 2021).
Comments received from a July 2020 NCI request for information on the scientific gaps and research needs related to the delivery of cancer-related care via telehealth11 suggested there are three priority areas for investigation: (1) approaches to integrate telehealth into cancer care; (2) development and dissemination of best practices for telehealth; and (3) the impact on health equity and access (NCI, 2021a). NCI conducted a grant portfolio analysis and identified 21 grants with a synchronous patient–clinician communication component, but none focusing on telehealth for routine cancer care, in the way it has been adopted during the pandemic. Jacobsen said that research is needed to identify which contexts are best suited for telehealth in oncology; to evaluate innovative approaches combining synchronous and asynchronous communication; to assess telehealth interventions that aim to reduce disparities and improve access to care; and to identify telehealth models that are scalable, sustainable, and suitable for improving patient outcomes and the delivery of high-quality, efficient cancer care. To encourage research in these areas, NCI launched two funding opportunities. First, the Centers on Telehealth Research for Cancer-Related Care will be established to provide the research infrastructure for testing telehealth approaches in real-world settings of care, to promote dissemination of effective models of telehealth, and to advance a national cancer-focused telehealth research agenda in the context of a changing health care environment (NCI, 2021b). NCI has also issued a Notice of Special Interest for Telehealth in Cancer Care that encourages a wide range of submissions, including studies that focus on populations that experience inequities in access to care and have worse cancer outcomes compared with the general population (NCI, 2021c).
Addressing Disparities in Access Through Telehealth
A number of speakers said that telehealth can remove barriers to cancer care. Zon said that audio-only telehealth services were critical for individuals who lacked reliable Internet access—and proved particularly helpful for serving rural patients or those with transportation barriers to receiving care. Lennes agreed that audio-only services are important for increasing patient access, especially among underserved populations, and suggested that payment parity for these interactions should be continued. Zon added that she has been inspired by the creative solutions that school districts have applied during the pandemic, such as installing hot spots for students to access educational materials.
Kelley said that patients served by the VA system face similar technology barriers, adding that inadequate access to technology affects not only health
___________________
11 See https://healthcaredelivery.cancer.gov/media/stakeholder-input.html (accessed November 2, 2021).
care, but many aspects of their lives. To address this issue, the VA has loaned devices to patients. Lennes said that loaning out devices was also successful at Mass General, but emphasized that new telehealth initiatives require new infrastructure, staff training, and interpretation services.
Karen Winkfield, executive director of the Meharry-Vanderbilt Alliance and an Ingram Professor of Cancer Research at the Vanderbilt University Medical Center, agreed that continuing telehealth will require more comprehensive solutions to address the digital divide. Knudsen and Kelley agreed, and noted that health care organizations have had to devote significant staff time to teaching patients how to use their smartphones for telehealth. Kelley noted that these challenges can be partly addressed by improving the usability of telehealth platforms. As an example, Lennes said that Mass General enabled telehealth service delivery via patient portals for those who had problems with the web interface.
Making Cancer Care More Equitable
Marcella Nunez-Smith, chair of the Presidential COVID-19 Health Equity Task Force, senior advisor to the White House COVID-19 Response Team, and associate dean for Health Equity Research and founding director of the Equity Research and Innovation Center at the Yale School of Medicine, discussed strategies for ensuring equity in cancer care. She said the COVID-19 pandemic broadly brought to light the fundamental, long-ignored structural inequities in health care and society. “When it comes to health inequities, a person’s zip code is a stronger predictor of health than their genetic code,” Nunez-Smith said. She explained that these health disparities will not be easy to solve, but building resilience into recovery, engaging communities, and committing to an antiracist, multipronged, equitable strategy can enhance access to clinical trials, prioritize representation in health care and health care leadership, and improve health outcomes for all populations.
Nunez-Smith said strategies to achieve these goals must be rooted in deep community engagement, strong partnerships, and an acknowledgment of the harms of structural racism, both in medicine and in society. Vital steps are to elevate patient voices and to study equity with rigor, representation, and antiracism within these strategies, she said, emphasizing that interventions are needed to eliminate the unacceptable variation in health outcomes. She said that data collection, which substantially improved during the pandemic, is still incomplete, especially for medically underserved populations. Nunez-Smith said the time has come for the cancer community to not merely report on patterns of inequity, but drive transformative change for patients based on sociodemographic, disaggregated, intersectional data that incorporates other factors that shape biological health, such as environmental justice and eco-
nomic policies. She urged clinicians to anticipate post-pandemic health access barriers such as time constraints due to child care and employment, transportation needs, or limited English proficiency. However, she cautioned that any modification—such as increased use of telehealth—without an intentional focus on equity could create cascading, negative consequences for populations that are already experiencing health care inequities.
Winkfield said it is critical to acknowledge the past, be intentional about changing the future, and understand the importance of representation to ameliorate racism, not just in oncology but across society (Chapman et al., 2020). She added that health care workforce diversity needs to be a top priority so that patients see themselves in their clinicians and clinicians benefit from the diversity of perspectives that can spur innovation and equity (Atcheson, 2018; Deville et al., 2020; Herring, 2009; Siker et al., 2020).
Christopher Lathan, chief clinical access and equity officer at the Dana-Farber Cancer Institute, associate medical director of the Dana-Farber Cancer Institute Network, and assistant professor of medicine at Harvard Medical School, discussed opportunities for academic cancer centers and the NCI to improve health equity. Lathan said that advancements in precision medicine have not reached all populations equally. Despite incremental improvements, recent data suggest that racial and ethnic minority populations are still less likely to get comprehensive molecular testing (Campbell et al., 2017) or participate in clinical trials. To address these ongoing challenges, Lathan stressed that cancer centers and NCI need to work together to encourage new interventions to promote health equity (Bruno et al., 2021; Doykos et al., 2021; Robert et al., 2021).
Lathan said that patients with the greatest disease burden tend to have the most needs and the fewest resources. For many of these patients, a cancer diagnosis leads to a complex struggle with clinicians, payers, and employers. He argued that the surprising flexibility and resourcefulness of cancer centers demonstrated during the pandemic can be put to use to better serve vulnerable patients. He suggested that cancer centers should foster meaningful community engagement to develop trusted, durable, mutually beneficial relationships that will enable measurable interventions, community-focused navigation, and transdisciplinary research focused on underserved populations. Because access to care is so closely tied to patient outcomes, a sustained community presence will also require infrastructure that is open to the community, dismantles care barriers, and elevates the status of health equity research and the people who conduct that work. He emphasized that cancer centers need to identify adequate resources in order to deliver care closer to where patients live.
As described in the next sections, some speakers suggested that researchers and clinicians need to reliably collect information on the social determinants of health, and that clinicians should act on this data as an integral part of
providing optimal care. Winn and Chambers urged improved integration of social care into health care to systemically address persistent disparities. Chambers stressed that such a path does not necessarily require new infrastructure, but rather an intentional reframing of routine interactions and processes (e.g., patient intake and patient reporting), along with a mechanism to link patients to relevant services as needed. Some speakers emphasized the need for adequate research funding to study interventions that address the social determinants of health.
Payment and Policy Opportunities to Advance Health Equity
Winkfield said there is an opportunity to develop payment models and policies that support best practices to address disparities in health outcomes. The pandemic showed that rapid adoption and payer support for care innovation is possible; she urged policy makers to step in to declare that everyone’s health—including the health of underserved communities—matters, and to ensure that successful changes made during the pandemic be sustained. For example, she suggested that cancer centers should be required to provide care to patients with Medicaid insurance to receive federal funding.
Lathan agreed, stressing the importance of advocating for policies to benefit the most vulnerable populations to support intentional, innovative work to achieve health equity. Chambers added that direct or indirect messaging about who a cancer center serves—and who it does not serve—affects relationships with communities. To overcome systemic exclusion and structural racism, Winkfield noted, there needs to be an acknowledgment that historical policies have created contemporary inequities.
Improving Coordination, Communication, and Patient Navigation
Several workshop participants called for the continuation of adaptations made in response to the pandemic that were helpful to patients, such as enhanced care navigation, team-based care, care coordination, and distributed care closer to home. Lathan noted that integrating patient navigation, education, and outreach is an example of low-hanging fruit that can benefit communities. Winkfield agreed, adding that expanding patient navigation staff, perhaps to include trusted community members, and ensuring reimbursement for patient navigation would improve care access, clinical trial enrollment, and patient satisfaction. Pierce said allowing all health care team members to work at the top of their scope of practice would also facilitate improved team-based care.
Chambers said the definition of “a health care team” needs to be expanded to include community members, social workers, and others in a position to
help address the social determinants of health. Christensen noted that IHS relies on community health representatives, pharmacists, and health aides to communicate and engage with patients. She urged that these valuable services, desperately needed in understaffed areas, be appropriately reimbursed because, as the pandemic showed, bringing care closer to patients is possible and beneficial.
Improving Community Engagement
Winn said that cancer centers are often distant from the communities they serve, both geographically and culturally. This lack of true community connection and engagement, along with inadequate health care access, structural inequities, racism, and bias, contribute to disparities in cancer care delivery and health outcomes.
Chambers and Winkfield agreed that cancer centers historically have not meaningfully engaged with the communities they serve. Chambers suggested that for cancer centers to better engage with communities, cancer centers need to provide community members with decision-making influence and power, appreciate the value community members ring, and be willing to learn from them. Winkfield suggested that NCI could play an important role in advancing meaningful community engagement by adding requirements for community engagement to its funding agreements. For example, she said NCI’s Comprehensive Cancer Centers Program has the opportunity to prioritize bidirectional communication and elevate the status of community expertise and the role of community resources in improving patient outcomes. Some participants suggested funding agencies should require specific features and metrics of community engagement to ensure that funded projects create meaningful, sustained, and effective engagement that builds trust and improves community outcomes. Lathan called for financial support for community partners that already serve community needs.
Winn asked how cancer centers can balance community needs with business objectives. Lathan responded that cancer centers need to be more transparent in their budgeting decisions, and that some research funding should be reserved for community initiatives, adding that unfunded mandates could present an added burden for community cancer centers.
Sagar suggested that community oncology practices could share data to identify “hotspots” where resources can be directed. Raising awareness of common issues can lead to opportunities to improve community oncology workflows and health care access, especially for underserved groups. For example, Cigna worked with trusted community centers and hospitals in Memphis to ensure that cancer screening notifications came from known, trusted community members, which resulted in improved screening rates. Pierce agreed,
citing recent work that has brought constituents together through intentional actions, such as creating a meaningful advisory board and patient-centered procedures (Guerra et al., 2021).
Christensen noted that payers are generally not incentivized to build relationships with Tribal communities because they are small, isolated populations. To run a successful community engagement program requires being embedded in the community, being willing to learn about the community’s culture and expertise, and becoming trusted leaders. “We have 574 Tribes, each with their own nuance, but the first thing is community trust, and you can’t do that in your granite buildings of cancer centers,” she said. “You have to do that out in the rural areas and become part of those communities.”
CLINICAL CANCER RESEARCH DURING THE COVID-19 PANDEMIC
As the COVID-19 pandemic swept across the world, cancer clinical trials were severely disrupted (van Dorn, 2020). Many speakers noted that ongoing clinical trials needed to pause or change course in order to protect patients and health care staff from infection with SARS-CoV-2 to ensure the integrity of the research results obtained during the pandemic, and because resources needed to be diverted to respond to the public health crisis.
Many clinical trial investigators made adaptations to clinical trial design, including protocol amendments and decentralized approaches to allow for home medication delivery and remote monitoring. Patient advocate Jane Perlmutter said the COVID-19 pandemic has provided a window of opportunity to rethink how cancer research should be undertaken. Prior to the pandemic, clinical trials were conducted primarily in academic settings of care and designed to answer questions of interest to clinical investigators; however, she said there is increasing interest in experimenting with more distributed trial designs that answer treatment-related questions that are important to patients.
Adapting Clinical Cancer Research
Mia Levy, the Sheba Foundation Director at Rush University Cancer Center and system vice president of Cancer Services at Rush System for Health,12 described three overarching phases of clinical cancer research during the pandemic: (1) a period of temporary shutdowns and shifting of priorities and resources; (2) an adaptation phase; and (3) a solidification phase for new practices. She said that in the early days of the pandemic, in-person clinical services
___________________
12 In August 2021, Levy became Chief Medical Officer of Foundation Medicine.
shifted to virtual formats, and diagnostic and procedural services were prioritized for emergency cases only. Levy said there were patient safety concerns for individuals enrolled in active treatment clinical trials due to the lack of ancillary services available, and as clinical and research staff pivoted to COVID-19 care. Many trial start-up activities were paused, and the focus shifted to rapid start-up for COVID-19-related studies. New accruals slowed, and Rush prioritized cancer therapeutic trials when it was the best treatment option for patients who lacked alternative options for standard-of-care treatment, Levy said.
After this initial phase, clinical trial research began to adapt with a longer term view, Levy said. Many in-person activities were converted to virtual activities (e.g., informed consent, receipt of investigational drug, assessment of patient safety and study adherence). Although these adaptations were challenging, and in many cases created new barriers to clinical trial entry and required time-intensive approval from an Institutional Review Board (IRB), Levy said that overall, they were successful.
Work is ongoing to solidify certain adaptations, such as electronic informed consent and virtual visits, Levy said she noted that optimal workflows or best practices for some clinical trial procedures, such as auditing, have not yet been identified. Another major challenge moving forward is a workforce shortage for clinical cancer research, which Levy speculated will negatively affect patient enrollment in clinical trials.
The pandemic illustrated that “rapid change is possible in clinical research,” which had not previously been demonstrated, given the historically slow-moving, heavily regulated nature of clinical research, Levy said. Going forward, she suggested that the cancer research community could learn additional lessons from the quick activation of COVID-19 therapeutic trials.
Use of Telehealth in Clinical Cancer Research
Spigel characterized the benefits and drawbacks of using telehealth in clinical research. Key benefits included (1) speedier processes for clinical trial selection and activation, due in part to virtual planning sessions that eliminated the need for in-person meetings; (2) the ability to more quickly identify and screen potential patients for clinical trial eligibility and faster enrollment; (3) the transition to remote clinical trial oversight; and (4) increased engagement of colleagues involved in clinical research across the United States. Spigel also described negative experiences with using remote technologies to advance clinical research, including the times when technology failed to work as expected, and the fatigue of remote interactions: “A big surprise has been the fatigue involved with these meetings and conferences that used to be in-person but now are remote, which can be draining if you’re doing it time and time again every day.” In spite of these limitations, Spigel concluded that the
use of telehealth in clinical research improves patient access to clinical trials and enables patients to remain closer to home while participating in clinical trials, reducing the costs for travel.
Kelley explained that the VA TeleOncology Service also serves as a model for initiating decentralized, VA-sponsored cancer clinical trials. The TeleOncology hub provides an interface between academic medical centers and distributed patient sites (see Figure 2). Kelley said that telehealth has the potential to improve clinical cancer research because it can help to lower costs, increase patient recruitment and retention rates, improve diversity, generate more data from integrated digital tools, and improve the applicability of research by involving participants who are more representative of the general population (Khozin and Coravos, 2019). Two trials are currently using TeleOncology, one for patients with cutaneous squamous cell carcinoma and one for patients with metastatic prostate cancer or metastatic non-small cell lung cancer (Migden et al., 2020). However, Kelley noted that some trials may be unsuitable for decentralization, such as those requiring biopsies or frequent laboratory testing, product registration trials, or trials that do not qualify for a Food and Drug Administration (FDA) waiver to be decentralized (Khozin and Coravos, 2019).
Dahut discussed NIH’s Clinical Center’s experiences with telehealth. He noted that every patient at the Clinical Center is enrolled in a research study. During the pandemic, the Clinical Center saw telehealth visits surge for all conditions, including cancer care. In terms of lessons learned from this experience, Dahut suggested that research protocols need to be amended to minimize the frequency of in-person visits at the Clinical Center, decrease requirements for physical examinations, and when scientifically feasible, compress laboratory testing across fewer patient visits. To support clinical trial participation while minimizing travel, he suggested improving processes for shipping investigational therapies to patients’ homes and facilitating the ability for patients to use clinical or research labs outside of the Clinical Center, and
SOURCE: Kelley presentation, July 26, 2021.
working closely with those labs, IRBs, and trial sponsors to ensure compliance and quality. Dahut noted that although the Clinical Center covers transportation costs and provides a stipend for housing, the burden of traveling to the Clinical Center may disproportionately hinder certain groups from participating in clinical trials. He said telehealth has the potential to lessen these burdens and improve equity. They are also looking into opportunities to make changes to trial designs and correlative laboratory and biopsy schedules to improve patient access to these clinical trials.
Leonard Sacks, associate director of clinical methodology in the Office of Medical Policy at FDA’s Center for Drug Evaluation and Research (CDER), said the pandemic placed ongoing cancer clinical trials in peril because of concerns about patient safety, increased reliance on technologies that not everyone could access, disrupted supply chains, and difficulty in obtaining needed lab tests. Sacks noted that FDA issued guidance to assist trial sponsors in ensuring the safety of trial participants, maintaining regulatory compliance, and minimizing risks to trial integrity during the COVID-19 emergency (FDA, 2021).
The pandemic illustrated a number of advantages to remote data acquisition approaches, including increased convenience for patients participating in research; improved access to trials for patients in remote locations; and opportunities for more continuous or frequent data collection using sensors, smart watches, or tablets in real-world settings. However, Sacks said it will be important to develop specifications for technologies to ensure the quality and reliability of data from digital health technologies used in different settings.
Adjustments to Federal Policies and Guidelines for Cancer Research
James Doroshow, director of the Division of Cancer Treatment and Diagnosis and deputy director for clinical and translational research at NCI, discussed the impacts of the pandemic on NCI-supported clinical trials. Doroshow said that within NCI’s National Clinical Trials Network,13 accrual to therapeutic cancer trials dropped sharply in February and March 2020, and that patient accrual took 6 months to return to 2019 levels. He added that accrual to clinical trials at NCI-designated cancer centers was still down; while accrual to early-phase trials has largely recovered, Phase 2 and Phase 3 trial accruals were still below 2019 levels (see Figure 3).
Early on, Doroshow said the pandemic created significant roadblocks to clinical trial accrual, such as the requirement for in-person visits to obtain informed consent, to receive an investigational therapy, and to assess patient
___________________
13 See https://www.cancer.gov/research/infrastructure/clinical-trials/nctn (accessed November 9, 2021).
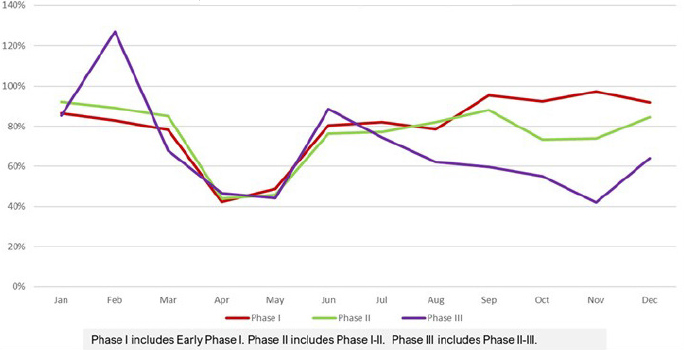
NOTES: Red = Phase 1; green = Phase 2; purple = Phase 3. The 2020 accrual is shown as a percentage of the 2019 accrual. Excludes industry-sponsored trials.
SOURCE: Doroshow presentation, July 26, 2021.
safety and adherence to the treatment protocol. In addition, many trials require the exclusive use of specified imaging and laboratory facilities, which patients were not able to access. There are also regulatory requirements to collect information on low-grade adverse events in trials, despite the potential for limited clinical relevance to study endpoints. In addition, clinical research personnel, facilities, and resources were redirected to the clinical care of patients with COVID-19, which further limited patient access to clinical cancer trials. Doroshow said NCI rapidly instituted changes to overcome these issues, including the use of practices for obtaining informed consent electronically, delivering oral investigational agents to patients’ homes, initiating virtual trial audits, conducting study visits via telemedicine, allowing decentralized testing for required lab and imaging studies, and limiting the impact of minor study deviations on trial conduct and evaluation. He added that NCI is carrying out a retrospective analysis of how the changes have impacted data quality, start-up times, and other measures. Although more study is needed, he speculated that many of the changes implemented during the pandemic are likely to represent improvements. Doroshow said that NCI is in the process of developing the NCI Clinical Trials 2030 Strategic Plan, with a focus on streamlining clinical trials, distributing clinical trial activities, and improving patient access to clinical trials, especially among underrepresented and underserved populations.
Sundeep Agrawal, acting team lead for genitourinary malignancies at CDER and clinical lead of Project Renewal at the Oncology Center of Excellence (OCE) at FDA, spoke about FDA’s regulatory work during the pan-
demic to ensure that clinical research could continue without jeopardizing patient safety or compromising trial integrity. Agrawal said FDA’s COVID-19 guidance for clinical trials14 prioritizes the safety of participants and provides guidance on common issues that clinical trial investigators faced, such as instituting remote monitoring, amending protocols to limit infection risks, and documenting contingency measures (FDA, 2021). Agrawal noted that FDA’s guidance document encourages trial sponsors to contact FDA to discuss protocol modifications related to efficacy endpoints, as well as when they are considering changes to data management or statistical analysis plans. For example, altering timing of imaging assessment could lead to inaccurate interpretation of progression-free survival (Panageas et al., 2007). He stressed that OCE is dedicated to working with all members of the cancer community to generate insights to advance trial modifications that can facilitate decentralized clinical trials.
Industry-Sponsored Clinical Trials
Dietmar Berger, chief medical officer and global head of development at Sanofi, spoke on behalf of TransCelerate.15 He highlighted the pandemic had a catalyzing effect on the pharmaceutical industry because it forced a reconsideration of opportunities to improve clinical trial conduct, not only during the crisis of the pandemic, but also in the future. TransCelerate’s sponsor organizations convened the Modernization of Clinical Trial Conduct Initiative, which identified several key challenges to advancing progress in clinical trial conduct: (1) a lack of global harmonization of regulatory policy; (2) gaps in clinical trial connectivity and integration; (3) variability in privacy laws and ethical considerations; (4) inadequate understanding of patient preferences and burdens related to participation in clinical research; and (5) the need for culture change in clinical research to advance progress (TransCelerate BioPharma, 2020). The group recommended adopting more flexible protocols, prospectively discussing use of digital data collection tools with regulatory agencies, ensuring trial sponsors are able to accept data from planned sources, focusing data collection efforts on the most critical and pertinent information, and prioritizing training for study teams, trial sites, and patients. While there is still a need for global regulatory harmonization, he said the pandemic has made it clear that collaboration across the cancer ecosystem can effectively modernize clinical trials without compromising their integrity. Berger said
___________________
14 See https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/covid-19-related-guidance-documents-industry-fda-staff-and-other-stakeholders (accessed on November 1, 2021).
15 See https://www.transceleratebiopharmainc.com (accessed November 1, 2021).
recent audits of changes made at Sanofi to modernize clinical trials during the pandemic have not found any reductions in quality. He added that their emphasis on patient-centeredness has contributed to the enrollment of more diverse patient populations in their clinical trials.
Kald Abdallah, senior vice president and therapeutic area head of Oncology Medical Affairs at Bristol Myers Squibb (BMS), said that during the pandemic, BMS’s priorities were to protect the safety of patients and personnel at BMS and clinical trial sites, to ensure scientific integrity, and to ensure continued compliance with regulatory obligations. He said the pandemic presented an unprecedented challenge. The company employed a solid, data-driven, and iterative cycle of information gathering and decision making to adapt operations and ensure regulatory compliance and measurement of the long-term impact. He said the pandemic did slow recruitment for BMS clinical trials, with some studies needing to be completely halted. However, BMS made a number of changes to the conduct of their clinical trials, including leveraging new technologies for remote monitoring, encouraging patient–investigator virtual visits when data could be collected by telephone or video call, exploring central monitoring capabilities and virtual site inspections to minimize nonessential travel, allowing trial participants to visit alternative clinical centers, and direct-to-patient shipments of investigational drugs. These adaptations protected patients while sustaining research, Abdallah said.
Fareed Melhem, senior vice president and head of Acorn AI Labs at Medidata, said the company, which works with a large swath of industry-sponsored trials, found that at its peak, enrollment in clinical trials declined 50 to 80 percent, with a greater than 30 percent increase in missed visits for ongoing clinical trials (see Figure 4). In April and May 2020, the data verification rate was approximately zero (Medidata Solutions, 2020). Most sponsors undertook swift, significant changes to keep patients and personnel safe and to keep trials going. Today, the majority of clinical trials have still not returned to 2019 accrual levels,
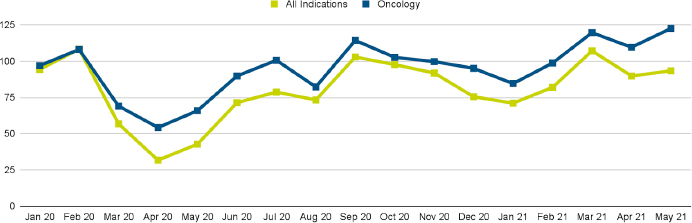
NOTE: Green = all indications; blue = oncology.
SOURCE: Melhem presentation, July 26, 2021.
but Melhem said oncology trials have outperformed others, which he attributed to public health education campaigns and the rapid changes implemented by industry, regulators, investigators, and site coordinators.
While data and technology have long played a role in clinical trials, Melhem said the COVID-19 pandemic brought a rapid, unprecedented industry-wide adoption of a number of tools and approaches. First, data analytics were leveraged to enable study coordinators to assess and adjust in real time to risks as circumstances evolved. Second, new ways to collect and analyze data were adopted, such as decentralized trials, telehealth, and external control arms.16 Finally, risk-based approaches were used to maintain data quality when monitors were unable to be onsite. The adoption of these methods—deployed out of necessity during the pandemic—can provide useful lessons for industry to build on and scale further going forward, Melhem said.
Remaining Challenges in the Conduct of Cancer Clinical Trials
Despite an overall sense of optimism that pandemic-related changes can improve cancer clinical trials in the long run, several speakers identified a number of remaining challenges in clinical trial modernization. While recognizing that it may be too soon to tell, given the ongoing larger societal shifts, Antoni Ribas, professor of medicine, surgery, and molecular and medical pharmacology, and director of the Tumor Immunology Program in the Jonsson Comprehensive Cancer Center at the University of California, Los Angeles, said the biggest challenge he sees is ensuring the capacity of the clinical research workforce. Berger noted that launching new studies has been harder during the pandemic, and pointed out that some adaptations for specialized trial sites were required. Levy said that some sponsors are pushing back against enrolling patients in clinical trials at satellite sites, even though patients are requesting more convenient locations for clinical trial participation. Perlmutter noted that this was a concern before the pandemic and suggested that patient convenience should be prioritized in future FDA guidance and in policy recommendations from ASCO. Schilsky urged clinicians to articulate what they want to learn, and then select the best trial design for that goal. He stressed the importance of reexamining tedious procedures, and discarding them if they do not demonstrate value in terms of ensuring patient safety or promoting trial integrity.
Berger emphasized that a major barrier to progress is the lack of global regulatory harmonization, which results in a patchwork of regulatory requirements for cancer clinical trials that could limit the adoption of innovations.
___________________
16 An external control arm “consists of patients who are not part of the same randomized study as the group receiving the investigational agent.” See https://www.fda.gov/downloads/guidances/ucm073139.pdf (accessed November 1, 2021).
Berger added that countries have experienced the pandemic very differently, with regulatory agencies providing contradictory feedback. He said that FDA has been more forward-thinking than some other regulatory agencies, and consequently, a global approach can require a more conservative course.
Data access and quality were important before the pandemic, but Ribas noted that rapid changes to the conduct of clinical trials brought these issues into even greater prominence. Levy agreed, and added that the pandemic has provided the motivation to enable greater access to patients’ full medical information. However, available technologies to help facilitate this access are often not robust enough or compatible with existing systems, and working with multiple vendors to piece together multiple streams of information is challenging. In particular, she said her institution has grappled with a 2-year limitation on the accessibility of certain medical records, which poses a hindrance to clinical trials that require longer-term recordkeeping for auditing purposes. Identifying better auditing workflows could bring large benefits to the clinical trial ecosystem, she said.
Melhem said the influx of technology products in this area can be confusing, and it will take time to identify the optimal platforms, identify best practices, and scale solutions. Capturing data during clinical trials via a combination of sensors, electronic health records (EHRs), and patient-reported outcomes could provide a promising way forward, he suggested.
ADVANCING CLINICAL CANCER RESEARCH IN A POST-PANDEMIC ERA
Clinical cancer research involves a complex array of regulatory requirements to safeguard clinical research participants and ensure data quality, but a number of speakers said that regulatory bodies and clinical investigators were successful in adapting swiftly to accommodate COVID-19-related constraints while maintaining high-quality standards and advancing research.
Use of Real-World Data for Evidence Generation
Elizabeth Garrett-Mayer, director of the Division of Biostatistics and Research Data Governance at ASCO’s Center for Research and Analytics, said that early in the pandemic, ASCO established a registry of patients diagnosed with both cancer and COVID-19 to inform evidence-based care in this context. This registry was rapidly developed, included a variety of eligibility criteria, had limited elements of data collection, and did not use direct identifiers, so patient consent was not required. Many real-world data registries are populated from EHRs, although Garrett-Mayer noted that EHRs often miss key data regarding COVID-19 diagnosis or comorbidities. This could
contribute to issues with data quality, completeness, and representativeness of the population. To counter concerns about data quality for studies using real-world data, she suggested that researchers need to develop rigorous plans for how they will use the data, define the relevant patient population and study endpoints, and take steps to control for bias and account for missing data. She added that real-world studies conducted with appropriate rigor have already yielded promising oncology insights and can play an important role in informing evidence-based care (Mileham et al., 2021).
Garrett-Mayer pointed to the need for data capture tools that allow multiple clinicians to extract relevant and reliable data from EHRs. Oncology EHRs, for example, focus on cancer treatments, but oncology outcomes can also be influenced by other conditions, such as COVID-19. Paul Kluetz, deputy director of FDA OCE, said that to advance evidence generation and decision making from real-world data, FDA has created an oncology-specific, real-world evidence program that aims to develop consistent terminology; standardize quality metrics for data from various sources; advance real-world endpoints, such as response rate, which are especially important in single-arm cohorts; and support collaborations with the broader cancer community and data ecosystems to improve data quality and interoperability (FDA OCE, 2021b). He said FDA’s Evidence Accelerator17 is capitalizing on the unprecedented speed researchers have gained in characterizing new treatments and outcomes to study evidence generation with real-world data. The challenge, he said, is that some real-world data methodologies cannot be used to assess causality of specific interventions.
Robert Califf, head of Clinical Policy and Strategy at Verily Life Sciences and Google Health, pointed to a recent study that found it was possible to make valid causal inferences from real-world data (Franklin et al., 2021). He speculated that the future will bring increased emphasis on the comparative effectiveness of different treatment options. He said experiences during the COVID-19 pandemic demonstrated that observational data are not rigorous enough to determine the efficacy of new treatments because patient datasets are incomplete, biased, and non-standardized. Multidimensional computational analyses, combined with clinical information within EHRs, may eventually enable a more complex understanding of treatment effectiveness. Califf also emphasized that to make progress, all of these challenges need be addressed in concert, noting that the traditional culture of research can be an obstacle to progress. He added that reduced life expectancy in the United States, which was already declining before the pandemic and is driven partly by enormous health disparities, points to the challenge of translating evidence generation into effective clinical practice (Woolf et al., 2021).
___________________
17 See https://evidenceaccelerator.org (accessed October 11, 2021).
Donna Rivera, associate director for pharmacoepidemiology at FDA OCE, said there is growing interest in alternative methods of evidence generation, which provides an opportunity to rethink the design of cancer clinical studies. She stressed that it will take a collaborative effort to advance data quality and interoperability to harness real-world data in a patient-centric way. While there are barriers, such as a lack of foundational definitions, methods, data characterization and quality, and understanding of biases, she noted that FDA OCE is open to novel study design and evidence generation strategies to improve patient care and outcomes.
The Future Role of Telehealth and Other Modifications in Cancer Clinical Trials
Several speakers suggested that the expanded use of telehealth has been a positive development in cancer clinical trials and suggested further expansion of its use after the pandemic as part of a broader move toward decentralization of cancer clinical trials. Douglas Lowy, principal deputy director of NCI, stressed that NCI is prioritizing collaborative efforts to implement these beneficial modifications to cancer clinical trials. He said the oncology community agrees on many of the principles, and he is optimistic that we will see significant improvements in cancer trials.
Several speakers said the increased adoption of telehealth, at-home services, and remote monitoring approaches in clinical trials during the pandemic were well-received by many trial participants, investigators, regulators, and funders. Lowy said it is imperative to make beneficial clinical trial modifications permanent where feasible. Many of these modifications have shortened the time needed to develop and initiate clinical trials, and have brought trials closer to where patients live, which in turn has made participation in clinical trials much more accessible for patients in underserved areas. Lowy noted that despite the disruptions the pandemic caused, NCI clinical trials did not see a decrease in enrollment among racial and ethnic minority populations. Clinical investigators in NCI’s Experimental Therapeutics Clinical Trials Network for early clinical trials highlighted the benefits of working with local health care staff to provide continuity of care for patients on clinical trials, using telehealth for study visits, shipping experimental oral drugs directly to patients, and using virtual approaches for informed consent and auditing (NCI Division of Cancer Treatment and Diagnosis, 2019). Lowy also urged the continued use and standardization of modifications that improved clinical trial operational efficiency; reduced costs and minimized required data elements and testing; enabled rapid review of clinical trial documents; and added new infrastructure to facilitate data capture from EHRs. He also suggested that study endpoints should be simplified, and that regulatory bodies enable investigators to stop
collecting minor protocol deviations or adverse events that do not affect patient safety. To create more inclusive trials, he added that clinical investigators should strive to increase trial sites for underserved groups and reevaluate overly stringent exclusion criteria that hinder patient enrollment.
Adapting Clinical Trial Designs
Kluetz discussed how trial modifications made during the pandemic have the potential to accelerate evidence generation for cancer therapies, while also improving patient access to clinical research and reducing drug development time and costs. Many modifications hold promise to reduce the burden to patients, and Kluetz noted that trial modifications during the pandemic have accelerated the enthusiasm for use of digital health technologies, patient-generated data, trial decentralization, and the potential for prospective randomized pragmatic trials using real-world clinical data sources. He suggested future efforts need to focus on maximizing data quality, creating best practices for the study modifications that benefit patients most, and determining how these data can best inform regulatory decision making.
Sources of evidence are expanding, and there is a blurring of lines between traditional prospective clinical trials and data generated from routine clinical care, said Kluetz (see Figure 5). Kluetz noted that steps must be taken to better understand the strengths and limitations of remote assessments in
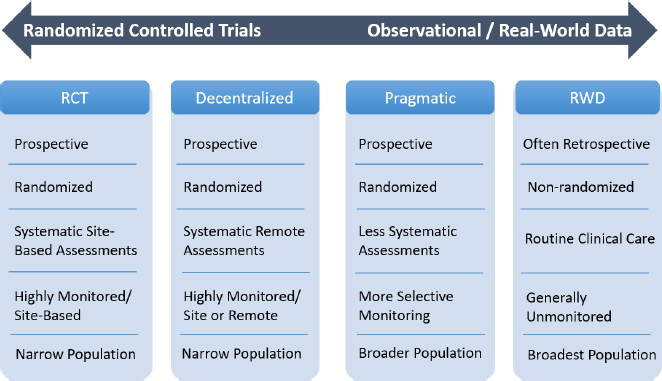
NOTE: RCT = randomized controlled trial; RWD = real-world data.
SOURCE: Kluetz presentation, July 27, 2021.
decentralized trials, and OCE is working with the cancer drug development community to determine how COVID-19 modifications like telemedicine or remote imaging might affect data quality. OCE is interested in ways to flag datasets to identify remote versus trial site assessments as one way to assist in the review of datasets submitted to FDA to facilitate its understanding and use of decentralized trials (FDA OCE, 2021a). Kluetz also noted that overall, there will be much to learn about how modifications made in response to the pandemic affected cancer trial data quality or integrity, what new options for clinical research exist, and how to prioritize what is most meaningful for patients.
Schilsky noted that all trials have or could have some form of decentralization. He stressed that some of the centralized protocols in clinical trials are unnecessary. For example, given the widespread use of digital imaging, scans could be performed at multiple locations with centralized interpretation of digital images. Doroshow agreed, noting that there have already been studies proving that decentralization can work (NCI, 2021d).18 Schilsky also noted another study demonstrating that it is possible to eliminate reporting of low-level adverse events in trials without missing clinically meaningful safety signals (Kaiser et al., 2010).
Derek Angus, chief innovation officer and executive vice president of the University of Pittsburgh Medical Center, associate vice chancellor for Healthcare Innovation, and professor at the University of Pittsburgh Schools of the Health Sciences, discussed the use of adaptive platform trials (APTs). APTs are a type of randomized controlled trial (RCT) that blends aspects of master protocol design19 with adaptive features, such as rules that preferentially assign interventions that demonstrate improved performance in earlier stages of the trial, or rules that trigger the addition or termination of a study arm (Adaptive Platform Trials Coalition, 2019). Angus said that three notable examples of APTs include RECOVERY,20 REMAP-CAP,21 and a “multiplatform” RCT composed of ATTACC,22 ACTIV-4,23 and REMAP-CAP. Angus said within 12 months, these trials enrolled more than 50,000 patients and generated
___________________
18 See https://www.tapur.org (accessed October 11, 2021).
19 Master protocol trials include one overarching protocol under which multiple interventions can be evaluated (Woodcock and LaVange, 2017).
20 See https://www.clinicaltrials.gov/ct2/show/NCT04381936 (accessed November 9, 2021).
21 See https://www.clinicaltrials.gov/ct2/show/NCT02735707 (accessed October 11, 2021).
22 See https://www.clinicaltrials.gov/ct2/show/NCT04372589 (accessed November 9, 2021).
23 See https://www.clinicaltrials.gov/ct2/show/NCT04505774 (accessed November 9, 2021).
high-profile findings that underpinned the vast majority of current COVID-19 treatment guidelines promulgated by the World Health Organization (Adaptive Platform Trials Coalition, 2019; Woodcock and LaVange, 2017). Notable features of these trials included the following: (1) the master protocols were amended to accommodate new study questions; (2) they had open-label control arms and used primary endpoints that were chosen to minimize bias; and (3) they prioritized ease of use and clinician acceptability (e.g., simple trial entry criteria with lean data collection).
Angus said the trials have encountered some criticisms due to lack of familiarity with the methods for statistical analysis and the open label design. Coordinating centers also struggled to keep up with the management of these trials, which involved rapid enrollment and the continual need to incorporate protocol updates. In addition, Angus said there was a somewhat unexpected load on the central architecture for trials, including managing the work of trial steering committees, data coordinating centers, analytic cores, and data safety and monitoring boards. Nevertheless, the successes of APTs during the pandemic have demonstrated that these approaches can work and likely will have an important role in the post-pandemic clinical research landscape, including in oncology.
Angus said that health care systems need better incentives and more streamlined processes to participate in clinical research. He suggested using a “trial-independent” incentive structure that could take on features of the Clinical Research Network Hospital Payment System of the United Kingdom’s National Institute for Health Research (many of the successful COVID-19 APTs were conducted in the United Kingdom). He added that clinical research needs to move toward “federated data solutions” that employ a common data model and use coordinating centers to specify data needs, but draw data from multiple sources, including EHRs (Heimbigner and McLeod, 1985). He also suggested critically reevaluating traditional RCT methodologies and embracing trial designs that foster patient engagement and enrollment.
Lessons from the Development of COVID-19 Vaccines
Randall Hyer, senior vice president of global medical affairs at Moderna, spoke about the Moderna COVID-19 vaccine development process and its relevance to cancer research. He said vaccine development was propelled forward by an overarching sense of urgency during the pandemic. Hyer also attributed the speed of COVID-19 vaccine development and emergency use authorization by FDA to rapid information flow, decision making, and risk management; transparency and collaboration; straightforward purchase agreements; and an emphasis on ensuring diversity of the participants enrolled in the trial (Baden et al., 2021; Moderna, 2021).
From this successful vaccine development program, Hyer said Moderna learned that three things are possible:
- Fast, agile, rapidly scalable clinical trial designs are possible if they fill unmet clinical needs;
- Close collaboration among industry, academia, and regulators is possible; and
- Enrollment of diverse participants in urgent clinical studies is feasible.
Finally, Hyer noted that due to the pandemic, the public is now much more informed about clinical trial research. This has the potential to benefit future oncology research, if this familiarity encourages more people to participate in clinical trials.
Melhem and Berger pointed to the important role of scaling to sustain lasting change. Many of the changes to clinical trials were made quickly, in the context of a public health emergency. They were not necessarily designed to work at scale. However, Melhem said many of the technology-based changes could scale easily and he expressed optimism that they could become permanent. Berger said that as alternative approaches become feasible, it will be important to demonstrate the benefits of selected approaches while ensuring continued trial integrity and data quality.
Assessing the Positives and Negatives of Research Modifications
Several speakers discussed which trial adaptations made in response to the COVID-19 pandemic, if made permanent, would have potential to improve the future of cancer clinical research and evidence generation. Kluetz said changes enacted during the pandemic showed that decentralizing aspects of clinical trials in oncology is feasible, and that it is now up to clinical investigators, patients, trial sponsors, and regulatory bodies to prioritize which modifications provide the most efficiency and benefit to patients with protecting patient safety and data integrity (Flaherty et al., 2021). However, he noted that some aspects of modernizing cancer clinical trials that occurred during the pandemic—such as rapid trial start-up—were a welcome change but largely outside of regulatory control. Hyer suggested focusing on speed and agility, collaboration, and inclusivity. Lowy agreed and said speed and flexibility—while maintaining appropriate trial integrity and rigor—will have a large impact, as long as clinical investigators are vigilant in ensuring that adaptations do not inadvertently exacerbate existing disparities. Lowy suggested that a key priority would be to improve patient access to clinical trials, and ensure faster and more equitable enrollment.
Califf stressed that rigorous research methods are still essential during a public health emergency (London and Kimmelman, 2020), but he cautioned
that it is important to understand which changes worked well—such as alterations to contracts and liability—and which were not sustainable, such as the emergency payment model. He suggested that examining where clinical trial modifications succeeded and failed can create a better system. He said decentralization and digitization of clinical trials were significant and successful changes, but it is imperative to identify best practices and standards for their use, especially with an eye toward ensuring patient access. Researchers also established innovative uses of EHR data and methods for data interoperability during the pandemic, but long-standing issues around data governance, data integration, data privacy, and technology disparities still need to be addressed.
Califf suggested that FDA-approved hybrid designs for at-home assessments of outcomes or safety should be incorporated into frameworks where front-line clinicians can bypass traditional clinical trial procedures. He stressed that randomization is still critically important for therapeutic evaluation, although even randomization cannot eliminate the possibility of deriving incorrect conclusions from poorly designed research trials. Meta-organization of studies and questions accelerated collaboration during the pandemic, but many trials were too small, ended early, and provided little evidence to advance knowledge. Information dissemination was rapid, but rapid communication can also run the risk of propagating errors or false claims, he said.
Califf expressed his admiration for the innovative ways oncology researchers adapted to the pandemic and noted that the improving survival rates for many cancers are a testament to the strength of oncology research. He added that oncology has already made progress by working to establish a common understanding of research terms and goals among oncologists and the academic research community, but that more work is needed. For example, a shared definition of “safe” could help streamline data collection in trials. “If we can take up these efforts and work together on what’s effective and what is not, it could really make a huge difference in fueling much faster generation of knowledge,” he said.
REFLECTIONS
In the final session, workshop speakers reflected on key messages from the workshop. The COVID-19 pandemic has had a significant impact on cancer care and cancer research. Access to cancer treatment was interrupted, cancer screenings were delayed, and many clinical trials were paused to develop new protocols to help keep patients and staff safe from the spread of the virus. Health care staff and resources were also diverted to care for the surge of patients with COVID-19. The disproportionate impacts of the pandemic on marginalized communities amplified existing health disparities and highlighted the urgent need to improve equity in cancer care and clinical trials.
Populations most susceptible to COVID-19 also experience a heavier cancer burden due to longstanding structural inequities.
But amid all the challenges the COVID-19 pandemic posed for cancer research and care, some positive changes also emerged. Health care providers developed new collaborations to share information and resources and to develop protocols and best practices for infection control and patient care. Clinicians and payers collaborated in new ways to rapidly implement telehealth solutions to enable continuity of care and to expand patient navigation and care coordination. New efficiencies in conducting clinical trials emerged, including rapid trial initiation, electronic consent, rapid approval of protocol changes, and increased use of remote assessments and community sites. Increased adoption of decentralized trial designs and telehealth technologies enabled many trials to increase enrollment diversity; novel study designs expanded data collection and opened opportunities to tap new sources; and new strategies were implemented to support data management, integrity, and quality. Regulatory bodies released guidance to industry clarifying that many trial modifications necessary to facilitate decentralization are acceptable, opening the door to unprecedented patient-centered processes that modernized trial conduct during the COVID-19 pandemic.
Many discussions at the workshop revolved around several themes: flexibility and agility, collaboration, equity, access, trust, and urgency. Underlying all of these themes is a sense that the oncology community should not simply revert to the way things operated before the pandemic. Instead, participants urged a rethinking of structures, processes, and assumptions in cancer research and care to make permanent those changes that are most beneficial to improve patient health outcomes. In closing remarks, Schilsky stressed the importance of maintaining and building on the adaptations that have shown to be beneficial to advance cancer care delivery and clinical cancer research. He urged continued attention to the themes and suggestions raised at the workshop in order to speed progress toward better cancer care and research in the post-pandemic era. He also emphasized that “We have to not only talk about what needs to be done; we have to own it. All of you are leaders in your organizations and you and your colleagues have to take responsibility for moving as many of these recommendations forward as possible, recognizing the complexity of many of them.” Echoing these sentiments, Winn concluded, “When we ourselves decide to actually roll up our sleeves and get busy, we can do great things.”
REFERENCES
AACR (American Association for Cancer Research). 2020. AACR cancer disparities progress report. https://cancerprogressreport.aacr.org/disparities (accessed October 11, 2021).
ACS (American Cancer Society). 2020. COVID-19 pandemic impact on cancer patients and survivors. https://www.fightcancer.org/sites/default/files/National%20Documents/Survivor%20Views.COVID19%20Polling%20Memo.Final_.pdf (accessed October 20, 2021).
Adaptive Platform Trials Coalition. 2019. Adaptive platform trials: Definition, design, conduct and reporting considerations. Nature Reviews Drug Discovery 18(10):797–807.
ASCO (American Society of Clinical Oncology). 2020a. ASCO interim position statement: Telemedicine in cancer care. https://www.asco.org/sites/new-www.asco.org/files/content-files/advocacy-and-policy/documents/2020-ASCO-Interim-Position-Statement-Telemedicine-FINAL.pdf (accessed October 11, 2021).
ASCO. 2020b. ASCO special report: A guide to cancer care delivery during the COVID-19 pandemic. https://www.asco.org/sites/new-www.asco.org/files/content-files/2020-ASCO-Guide-Cancer-COVID19.pdf (accessed October 11, 2021).
ASCO. 2021a. ASCO oncology clinician well-being task force roadmap. https://practice.asco.org/sites/default/files/drupalfiles/2021-01/Final-Roadmap-Graphic.pdf (accessed October 11, 2021).
ASCO. 2021b. Telemedicine flexibilities, including permission to cross state lines, should continue after COVID-19. https://www.asco.org/news-initiatives/policy-news-analysis/telemedicine-flexibilities-including-permission-cross-state (accessed October 11, 2021).
Atcheson, S. 2018. Embracing diversity and fostering inclusion is good for your business. Forbes. https://www.forbes.com/sites/shereeatcheson/2018/09/25/embracing-diversity-and-fostering-inclusion-is-good-for-your-business/?sh=10c3577572b1 (accessed November 23, 2021).
Baden, L. R., H. M. El Sahly, B. Essink, K. Kotloff, S. Frey, R. Novak, D. Diemert, S. A. Spector, N. Rouphael, C. B. Creech, J. McGettigan, S. Khetan, N. Segall, J. Solis, A. Brosz, C. Fierro, H. Schwartz, K. Neuzil, L. Corey, P. Gilbert, H. Janes, D. Follmann, M. Marovich, J. Mascola, L. Polakowski, J. Ledgerwood, B. S. Graham, H. Bennett, R. Pajon, C. Knightly, B. Leav, W. Deng, H. Zhou, S. Han, M. Ivarsson, J. Miller, T. Zaks, and C. S. Group. 2021. Efficacy and safety of the MRNA-1273 SARS-COV-2 vaccine. New England Journal of Medicine 384(5):403–416.
Balogun, O. D., V. J. Bea, and E. Phillips. 2020. Disparities in cancer outcomes due to COVID-19, a tale of 2 cities. JAMA Oncology 6(10):1531–1532.
Boserup, B., M. McKenney, and A. Elkbuli. 2020. Disproportionate impact of COVID-19 pandemic on racial and ethnic minorities. The American Surgeon 86(12):1615–1622.
Bruno, D. S., L. M. Hess, X. Li, E. W. Su, Y. E. Zhu, and M. Patel. 2021. Racial disparities in biomarker testing and clinical trial enrollment in non-small cell lung cancer (NSCLC). Journal of Clinical Oncology 39(15 Suppl):9005.
Campbell, J. D., C. Lathan, L. Sholl, M. Ducar, M. Vega, A. Sunkavalli, L. Lin, M. Hanna, L. Schubert, A. Thorner, N. Faris, D. R. Williams, R. U. Osarogiagbon, P. van Hummelen, M. Meyerson, and L. MacConaill. 2017. Comparison of prevalence and types of mutations in lung cancers among Black and white populations. JAMA Oncology 3(6):801–809.
Chapman, C. H., D. Gabeau, C. C. Pinnix, C. Deville, Jr., I. C. Gibbs, and K. M. Winkfield. 2020. Why racial justice matters in radiation oncology. Advances in Radiation Oncology 5(5):783–790.
Chen, R. C., K. Haynes, S. Du, J. Barron, and A. J. Katz. 2021. Association of cancer screening deficit in the United States with the COVID-19 pandemic. JAMA Oncology 7(6):878–884.
Cigna. 2020. Cigna takes action to combat systemic racism and improve equity and equality. https://newsroom.cigna.com/cigna-takes-action-to-combat-systemic-racism-and-improve-equity-and-equality (accessed November 23, 2021).
Cinar, P., T. Kubal, A. Freifeld, A. Mishra, L. Shulman, J. Bachman, R. Fonseca, H. Uronis, D. Klemanski, K. Slusser, M. Lunning, and C. Liu. 2020. Safety at the time of the COVID-19 pandemic: How to keep our oncology patients and healthcare workers safe. Journal of the National Comprehensive Cancer Network 1–6. https://pubmed.ncbi.nlm.nih.gov/32294617 (accessed November 23, 2021).
CMS (Centers for Medicare & Medicaid Services). 2020a. CMS announces comprehensive strategy to enhance hospital capacity amid COVID-19 surge. https://www.cms.gov/newsroom/press-releases/cms-announces-comprehensive-strategy-enhance-hospital-capacity-amid-covid-19-surge (accessed September 24, 2021).
CMS. 2020b. CMS innovation center models COVID-19 related adjustments. https://www.cms.gov/files/document/covid-innovation-model-flexibilities.pdf (accessed September 24, 2021).
CMS. 2020c. Flexibilities overview graphic. https://www.cms.gov/files/document/covid-flexibilities-overview-graphic.pdf (accessed September 24, 2021).
Deville, C., Jr., I. Cruickshank, Jr., C. H. Chapman, W. T. Hwang, R. Wyse, A. A. Ahmed, K. M. Winkfield, C. R. Thomas, Jr., and I. C. Gibbs. 2020. I can’t breathe: The continued disproportionate exclusion of Black physicians in the United States radiation oncology workforce. International Journal of Radiation Oncology-Biology-Physics 108(4):856–863.
Dietz, J. R., M. S. Moran, S. J. Isakoff, S. H. Kurtzman, S. C. Willey, H. J. Burstein, R. J. Bleicher, J. A. Lyons, T. Sarantou, P. L. Baron, R. E. Stevens, S. K. Boolbol, B. O. Anderson, L. N. Shulman, W. J. Gradishar, D. L. Monticciolo, D. M. Plecha, H. Nelson, and K. A. Yao. 2020. Recommendations for prioritization, treatment, and triage of breast cancer patients during the COVID-19 pandemic. The COVID-19 pandemic breast cancer consortium. Breast Cancer Research and Treatment 181(3):487–497.
Doykos, P. M., M. S. Chen, Jr., K. Watson, V. Henderson, M. L. Baskin, S. Downer, L. A. Smith, N. Bhavaraju, S. Dina, and C. S. Lathan. 2021. Special convening and listening session on health equity and community outreach and engagement at National Cancer Institute-designated comprehensive cancer centers. Health Equity 5(1):84–90.
FDA (Food and Drug Administration). 2021. FDA guidance on conduct of clinical trials of medical products during the COVID-19 public health emergency. FDA-2020-D-1106-0002. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/fda-guidance-conduct-clinical-trials-medical-products-during-covid-19-public-health-emergency (accessed September 24, 2021).
FDA OCE (Oncology Center of Excellence). 2021a. Advancing oncology decentralized trials: Learning from COVID-19 trial datasets. https://www.fda.gov/about-fda/oncology-center-excellence/advancing-oncology-decentralized-trials (accessed October 11, 2021).
FDA OCE. 2021b. Oncology real world evidence program: Fostering regulatory science and collaboration to translate real world data into real world evidence. https://www.fda.gov/about-fda/oncology-center-excellence/oncology-real-world-evidence-program (accessed October 11, 2021).
Flaherty, K. T., J. H. Doroshow, S. Galbraith, A. Ribas, P. G. Kluetz, R. Pazdur, and M. R. Theoret. 2021. Rethinking cancer clinical trial conduct induced by COVID-19: An academic center, industry, government, and regulatory agency perspective. Cancer Discovery 11(8):1881–1885.
Frankel, T. C., and R. Tony. 2020. Historic financial decline hits doctors, dentists and hospitals—despite COVID-19—threatening overall economy. The Washington Post. https://www.washingtonpost.com/business/2020/05/04/financial-distress-among-doctors-hospitals-despite-covid-19-weighs-heavily-economy (accessed November 23, 2021).
Franklin, J. M., E. Patorno, R. J. Desai, R. J. Glynn, D. Martin, K. Quinto, A. Pawar, L. G. Bessette, H. Lee, E. M. Garry, N. Gautam, and S. Schneeweiss. 2021. Emulating randomized clinical trials with nonrandomized real-world evidence studies: First results from the RCT duplicate initiative. Circulation 143(10):1002–1013.
Giannakoulis, V. G., E. Papoutsi, and I. I. Siempos. 2020. Effect of cancer on clinical outcomes of patients with COVID-19: A meta-analysis of patient data. JCO Global Oncology 6:799–808.
Grubbs, S. S., B. N. Polite, J. Carney, Jr., W. Bowser, J. Rogers, N. Katurakes, P. Hess, and E. D. Paskett. 2013. Eliminating racial disparities in colorectal cancer in the real world: It took a village. Journal of Clinical Oncology 31(16):1928–1930.
Guerra, C. E., V. Sallee, W.-T. Hwang, B. Bryant, A. L. Washington, S. U. Takvorian, R. Schnoll, K. Glanz, R. B. Cohen, K. L. Nathanson, and R. H. Vonderheide. 2021. Accrual of Black participants to cancer clinical trials following a five-year prospective initiative of community outreach and engagement. Journal of Clinical Oncology 39(15 Suppl):100.
Hauck, G., M. Nichols, M. Marini, and A. Pantazi. 2020. Coronavirus spares one neighborhood but ravages the next. Race and class spell the difference. USA Today. https://www.usatoday.com/in-depth/news/nation/2020/05/02/coronavirus-impact-black-minority-white-neighborhoods-chicago-detroit/3042630001 (accessed November 23, 2021).
Heimbigner, D., and D. McLeod. 1985. A federated architecture for information management. ACM Transactions on Information Systems 3(3):253–278.
Herring, C. 2009. Does diversity pay?: Race, gender, and the business case for diversity. American Sociological Review 74(2):208–224.
Johnson, A., and T. Buford. 2020. Early data shows African Americans have contracted and died of coronavirus at an alarming rate. ProPublica. https://www.propublica.org/article/early-data-shows-african-americans-have-contracted-and-died-of-coronavirus-at-an-alarming-rate (accessed November 23, 2021).
Jones, C. 2021. Dr. Camara Jones explains the cliff of good health. https://www.urban.org/policy-centers/cross-center-initiatives/social-determinants-health/projects/dr-camara-jones-explains-cliff-good-health (accessed October 11, 2021).
Kaiser, L. D., A. S. Melemed, A. J. Preston, H. A. C. Ross, D. Niedzwiecki, G. A. Fyfe, J. M. Gough, W. D. Bushnell, C. L. Stephens, M. K. Mace, and J. S. Abrams. 2010. Optimizing collection of adverse event data in cancer clinical trials supporting supplemental indications. Journal of Clinical Oncology 28(34):5046–5053.
KFF (Kaiser Family Foundation). 2021. Status of state action on the Medicaid expansion decision. https://www.kff.org/health-reform/state-indicator/state-activity-around-expanding-medicaid-under-the-affordable-care-act (accessed October 11, 2021).
Khozin, S., and A. Coravos. 2019. Decentralized trials in the age of real-world evidence and inclusivity in clinical investigations. Clinical Pharmacology & Therapeutics 106(1):25–27.
London, A. J., and J. Kimmelman. 2020. Against pandemic research exceptionalism. Science 368(6490):476–477.
Lopez, L., L. H. Hart, and M. H. Katz. 2021. Racial and ethnic health disparities related to COVID-19. JAMA 325(8):719–720.
Medidata Solutions, Inc. 2020. COVID-19 and clinical trials: The Medidata perspective release 8.0. https://www.medidata.com/wp-content/uploads/2021/06/COVID19-Response8.0_Clinical-Trials_2020824_v1-1.pdf (accessed September 24, 2020).
Migden, M. R., S. Chandra, G. Rabinowits, C. I. Chen, J. Desai, A. Seluzhytsky, M. Sasane, B. Campanelli, Z. Chen, M. L. Freeman, S. F. Ibrahim, N. I. Khushalani, M. Andria, and E. Ruiz. 2020. CASE (CemiplimAB-rwlc Survivorship and Epidemiology) study in advanced cutaneous squamous cell carcinoma. Future Oncology 16(4):11–19.
Mileham, K. F., S. S. Bruinooge, C. Aggarwal, A. L. Patrick, C. Davis, D. Mesenhowski, A. I. Spira, E. J. Clayton, D. M. Waterhouse, S. Moore, A.-R. Jazieh, R. C. Chen, M. Kaltenbaugh, J. H. Williams, R. L. Schilsky, and L. Garrett-Mayer. 2021. Mortality risk for patients undergoing cancer treatment who acquire SARS-COV-2: ASCO registry. Journal of Clinical Oncology 39(15 Suppl):6509.
Mitchell, E. P. 2020. Declines in cancer screening during COVID-19 pandemic. Journal of the National Medical Association 112(6):563–564.
Moderna. 2021. Moderna COVID-19 vaccine. https://www.modernatx.com/covid19vaccine-eua (accessed October 11, 2021).
NCCN (National Comprehensive Cancer Network). 2021. Recommendations of the National Comprehensive Cancer Network® (NCCN®) COVID-19 vaccination advisory committee. https://www.nccn.org/docs/default-source/covid-19/2021_covid-19_vaccination_guidance_v4-0.pdf?sfvrsn=b483da2b_70 (accessed September 24, 2021).
NCCS (National Coalition for Cancer Survivorship). 2021. State of survivorship survey: 2021. https://canceradvocacy.org/wp-content/uploads/NCCS-2021-Survivorship-Survey-Full-Report-Final.pdf (accessed November 23, 2021).
NCI (National Cancer Institute). 2021a. Findings from an NCI Request for Information (RFI): Stakeholder input on scientific gaps and research needs related to delivery of cancer-related care via telehealth. https://healthcaredelivery.cancer.gov/media/stakeholder-input.html (accessed October 8, 2021).
NCI. 2021b. Pre-application webinar for RFA-CA-21-029, centers on telehealth research for cancer-related care (P50 clinical trial required). https://healthcaredelivery.cancer.gov/media/telehealth-research.html (accessed October 8, 2021).
NCI. 2021c. Notice of Special Interest (NOSI): Telehealth in cancer care. https://grants.nih.gov/grants/guide/notice-files/NOT-CA-21-043.html (accessed October 8, 2021).
NCI. 2021d. NCI-MATCH trial (Molecular Analysis for Therapy Choice). https://www.cancer.gov/about-cancer/treatment/clinical-trials/nci-supported/nci-match (accessed October 11, 2021).
NCI Division of Cancer Treatment and Diagnosis. 2019. CTEP cancer therapy evaluation program. https://ctep.cancer.gov/initiativesprograms/etctn.htm (accessed October 11, 2021).
Oxley, T. J., J. Mocco, S. Majidi, C. P. Kellner, H. Shoirah, I. P. Singh, R. A. De Leacy, T. Shigematsu, T. R. Ladner, K. A. Yaeger, M. Skliut, J. Weinberger, N. S. Dangayach, J. B. Bederson, S. Tuhrim, and J. T. Fifi. 2020. Large-vessel stroke as a presenting feature of COVID-19 in the young. New England Journal of Medicine 382(20):e60.
Panageas, K. S., L. Ben-Porat, M. N. Dickler, P. B. Chapman, and D. Schrag. 2007. When you look matters: The effect of assessment schedule on progression-free survival. Journal of the National Cancer Institute 99(6):428–432.
Patel, M. I., A. M. Lopez, W. Blackstock, K. Reeder-Hayes, E. A. Moushey, J. Phillips, and W. Tap. 2020. Cancer disparities and health equity: A policy statement from the American Society of Clinical Oncology. Journal of Clinical Oncology 38(29):3439–3448.
Pennell, N. A., M. Dillmon, L. A. Levit, E. A. Moushey, A. S. Alva, S. Blau, T. L. Cannon, N. R. Dickson, M. Diehn, M. Gonen, M. M. Gonzalez, J. O. Hensold, L. J. Hinyard, T. King, S. C. Lindsey, A. Magnuson, J. Marron, B. L. McAneny, T. M. McDonnell, K. F. Mileham, S. F. Nasso, G. S. Nowakowski, K. R. Oettel, M. I. Patel, D. A. Patt, J. Perlmutter, T. A. Pickard, G. Rodriguez, A. R. Rosenberg, B. Russo, C. Szczepanek, C. B. Smith, P. Srivastava, E. Teplinsky, R. Thota, T. A. Traina, R. Zon, B. Bourbeau, S. S. Bruinooge, S. Foster, S. Grubbs, K. Hagerty, P. Hurley, D. Kamin, J. Phillips, C. Schenkel, R. L. Schilsky, and H. A. Burris, 3rd. 2021. American Society of Clinical Oncology road to recovery report: Learning from the COVID-19 experience to improve clinical research and cancer care. Journal of Clinical Oncology 39(2):155–169.
Robert, N. J., E. D. Nwokeji, J. L. Espirito, L. Chen, M. Karhade, M. C. Evangelist, A. I. Spira, M. A. Neubauer, S. A. Bullock, and R. L. Coleman. 2021. Biomarker tissue journey among patients (pts) with untreated metastatic non-small cell lung cancer (mNSCLC) in the U.S. Oncology Network community practices. Journal of Clinical Oncology 39(15 Suppl):9004.
Schrag, D., D. L. Hershman, and E. Basch. 2020. Oncology practice during the COVID-19 pandemic. JAMA 323(20):2005–2006.
Siker, M. L., C. Deville, Jr., G. Suneja, and K. Winkfield. 2020. Lessons from COVID-19: Addressing health equity in cancer care. International Journal of Radiation Oncology-Biology-Physics 108(2):475–478.
Sun, L., S. Surya, A. N. Le, H. Desai, A. Doucette, P. Gabriel, M. D. Ritchie, D. Rader, I. Maillard, and E. Bange. 2021. Rates of COVID-19-related outcomes in cancer compared with noncancer patients. JNCI Cancer Spectrum 5(1):pkaa120.
The Commonwealth Fund. 2021. Status of Medicaid expansion and work requirement waivers. https://www.commonwealthfund.org/publications/maps-and-interactives/2021/jul/status-medicaid-expansion-and-work-requirement-waivers (accessed October 11, 2021).
TransCelerate BioPharma, Inc. 2020. Beyond COVID-19: Modernizing clinical trial conduct. http://transceleratebiopharmainc.com/wp-content/uploads/2020/07/TransCelerate_Beyond-COVID19_Modernizing-Clinical-Trial-Conduct_July-2020.pdf (accessed September 24, 2021).
Ueda Oshima, M., B. M. Sandmaier, E. Petersdorf, M. E. Flowers, G. R. Hill, S. J. Lee, F. R. Appelbaum, P. A. Carpenter, K. S. Baker, L. Connelly-Smith, A. McCool, S. Elgar, S. A. Pergam, C. Liu, F. M. Stewart, and M. Mielcarek. 2021. Blood and marrow transplantation during the emerging COVID-19 pandemic: The Seattle approach. Bone Marrow Transplant 56(2):305–313.
van Dorn, A. 2020. COVID-19 and readjusting clinical trials. The Lancet 396(10250):523–524.
Warner, J. L., S. Rubinstein, P. Grivas, T. K. Choueiri, N. M. Kuderer, D. Shah, D. R. Rivera, S. Gupta, M. A. Bilen, T. R. Halfdanarson, D. B. Doroshow, F. Wehbe, S. Shah, Y. Shyr, G. Lopes, C. Painter, G. H. Lyman, M. A. Thompson, S. Peters, and B. I. Rini. 2020. Clinical impact of COVID-19 on patients with cancer: Data from the COVID-19 and cancer consortium (CCC19). Journal of Clinical Oncology 38(18 Suppl):LBA110. https://ascopubs.org/doi/abs/10.1200/JCO.2020.38.18_suppl.LBA110 (accessed November 23, 2021).
Woodcock, J., and L. M. LaVange. 2017. Master protocols to study multiple therapies, multiple diseases, or both. New England Journal of Medicine 377(1):62–70.
Woodfield, M. C., S. A. Pergam, and P. D. Shah. 2021. Cocooning against COVID-19: The argument for vaccinating caregivers of patients with cancer. Cancer 127(16):2861–2863.
Woolf, S. H., R. K. Masters, and L. Y. Aron. 2021. Effect of the COVID-19 pandemic in 2020 on life expectancy across populations in the USA and other high income countries: Simulations of provisional mortality data. BMJ 373:n1343.
This page intentionally left blank.
















































