
Proceedings of a Workshop
OVERVIEW OF THE WORKSHOP1
Reducing suicide-related mortality is a global imperative declared by the World Health Organization (WHO, 2014). The persistent trends in suicide necessitate action among mental health care providers and payers, researchers, and community leaders. The suicide prevention movement has been gaining momentum as organizations, advocates, and others have increasingly collaborated on effective strategies. Health care settings provide an important opportunity for suicide intervention and prevention, but they cannot yet fully manage suicide risk because of a lack of training, knowledge gaps, and reimbursement challenges. School, workplace, and community-based interventions can help reduce the incidence of suicidal behavior, as can better access to care and reduced access to lethal means of suicide (Hogg et al., 2021; National Action Alliance for Suicide Prevention, 2017; Pistone et al., 2019).
To better understand the strategies to improve access to effective interventions to prevent suicide, the Forum on Mental Health and Substance Use Disorders at the National Academies of Sciences, Engineering, and Medicine hosted a two-part virtual public workshop, Strategies and Interventions to
___________________
1 The planning committee’s role was limited to planning the workshop, and the Proceedings of a Workshop was prepared by the workshop rapporteurs as a factual summary of what occurred at the workshop. Statements, recommendations, and opinions expressed are those of individual presenters and participants, and are not necessarily endorsed or verified by the National Academies of Sciences, Engineering, and Medicine, and they should not be construed as reflecting any group consensus.
Reduce Suicide, on June 22, 2021, and July 28, 2021. The presentations and discussions during the first webinar on June 22 examined the scope of the public health problem, discussed the implementation of effective approaches for suicide prevention care, and addressed the known barriers to health care access. The second webinar on July 28 focused on building 9-8-8, the new nationwide emergency number designated to the National Suicide Prevention Lifeline, and participants discussed current crisis systems, gaps, challenges, and needs for marginalized populations. Appendix A contains the workshop Statement of Task, and Appendix B contains the workshop agendas, respectively.2Appendix C contains biographical sketches of the speakers and the moderators of the workshop. The objectives of the workshop were to discuss:
- The scope of the public health problem, with a focus on data regarding suicidal ideation, suicide attempts, and death by suicide;
- What is known about the effectiveness of approaches and interventions to reduce harm and prevent risk of suicide;
- Policy opportunities to support, improve, and implement early interventions to increase access and quality of care for individuals at risk of suicide; and
- Areas where further evidence or attention is needed to improve the quality of care available across the continuum for suicide prevention.
This Proceedings of a Workshop summarizes the presentations and discussions. The speakers, panelists, and workshop participants presented a broad range of views and ideas. Box 1 presents an overview of observations and suggestions from individual presentations and discussions and are discussed throughout the proceedings.
SUICIDE TRENDS IN U.S. SUBGROUPS
To provide context for the workshop, Jeffrey A. Bridge,3 director of the Center for Suicide Prevention and Research at Nationwide Children’s Hospital, and Crystal L. Barksdale, acting deputy director and chief of Minority Mental Health Research for the Office for Disparities Research and Workforce
___________________
2 For additional information, see https://www.nationalacademies.org/event/06-10-2021/integrating-serious-illness-care-into-primary-care-delivery-a-workshop-first-webinar (accessed October 25, 2021) and https://www.nationalacademies.org/event/10-26-2020/integrating-serious-illness-care-into-primary-care-delivery-a-workshop#sectionEventMaterials (accessed October 25, 2021).
3 Complete titles and affiliations for all speakers are available in Appendix C.
Diversity at the National Institute of Mental Health (NIMH), presented some of the data on suicide rates for various populations in the United States.
Overall, suicide was the 10th leading cause of death in the United States in 2019, accounting for 47,500 deaths, said Bridge. Death by suicide spans all age groups, he explained, and it is the second leading cause of death among individuals ages 10 through 34. Data from the National Vital Statistics System show that age-adjusted suicide rates in the United States increased for both males and females from 1999 through 2019 (see Figure 1), with an overall increase of 35.2 percent (Hedegaard et al., 2021). There is a gender paradox regarding suicide and suicidal behavior in that suicide rates for males have remained four times higher than for women over that time span, while the rate of suicide attempts by young females is three to four times higher than by young males.
Suicide rates have shown to be persistent. Between 1999 and 2007, there was a decline among U.S. youth ages 10 to 19 years old, but since then, suicide rates increased by 88 percent between 2007 and 2018 (see Figure 2). Even accounting for a drop in suicides in 2019, the increase from 2007 would be approximately 80 percent. Broken down by gender, suicide rates for both females and males fell between 1999 and 2007, by 16 percent and 20 percent respectively, while from 2007 to 2018 the suicide rate among females in the 10- to 19-year-old population increased by 147 percent, compared to 75 percent in males in the same age group (see Figure 3). The larger increase among females contributed to a narrowing of the gender gap in this age range (Ruch et al., 2019), said Bridge.
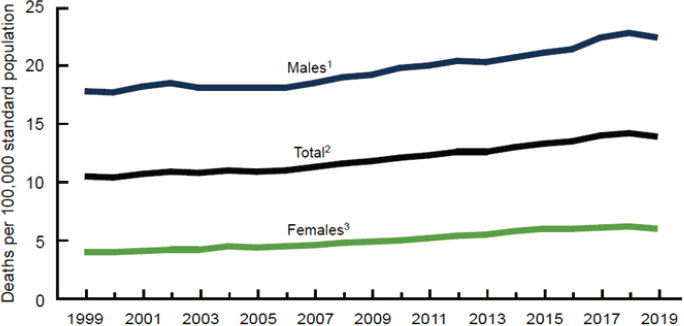
SOURCES: Presented by Jeffrey A. Bridge on June 22, 2021, at the workshop on Strategies and Interventions to Reduce Suicide; Hedegaard et al., 2021.
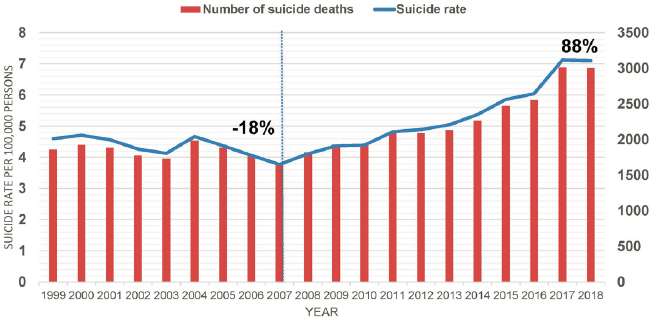
SOURCES: Presented by Jeffrey A. Bridge on June 22, 2021, at the workshop on Strategies and Interventions to Reduce Suicide. Data from CDC, 2021a.
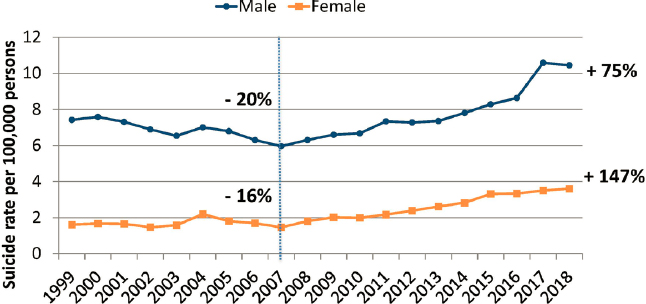
SOURCES: Presented by Jeffrey A. Bridge on June 22, 2021, at the workshop on Strategies and Interventions to Reduce Suicide. Data from CDC, 2021a.
There are racial differences in U.S. suicide rates, Bridge continued, with suicide rates among White individuals across the life span being higher than among every other racial subgroup (see Figure 4). However, from 1999 to 2019, suicide rates among American Indian and Alaska Natives children and adolescents were significantly higher than among any other racial subgroup in the United States (see Figure 4). Moreover, suicide rates among children and adolescents ages 10–19 years were approximately 35 percent higher among American Indian and Alaska Native females compared to both Black and Asian and Pacific Islander males in the same age group, said Bridge. Parsing the data by ethnicity shows that suicide rates across all ages, including among
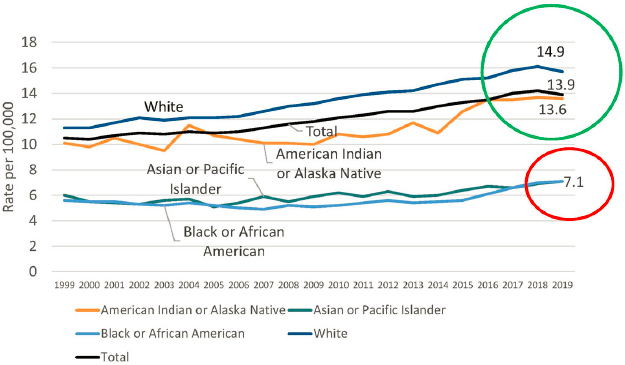
SOURCES: Presented by Jeffrey A. Bridge on June 22, 2021, at the workshop on Strategies and Interventions to Reduce Suicide; Ramchand et al., 2021.
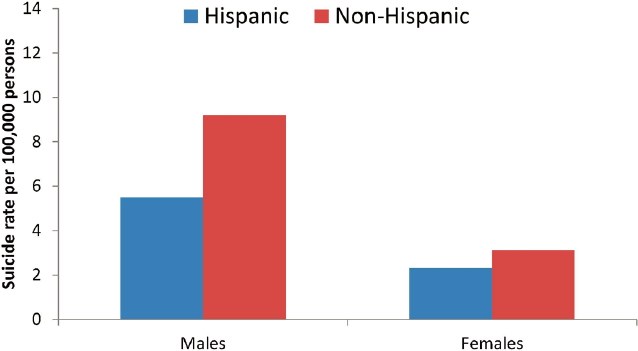
individuals ages 10 to 19 years old, are higher among non-Hispanic individuals, though the gap between non-Hispanic and Hispanic females ages 10 to 19 years old is small (see Figure 5).
Bridge described the geographic urban versus rural differences in suicide rates in the United States, as seen in Figure 6. He noted that while there would be some variation in the data over the past 20 years, the states with the highest suicide rates have remained unchanged. While there has been no published
SOURCES: Presented by Jeffrey A. Bridge on June 22, 2021, at the workshop on Strategies and Interventions to Reduce Suicide; CDC, 2021a.

SOURCES: Presented by Jeffrey A. Bridge on June 22, 2021, at the workshop on Strategies and Interventions to Reduce Suicide; CDC, 2021a.
research examining the causes for these differences, people have proposed several explanations. One might be that higher suicide rates in the western United States are tied to a higher density of firearms among the population. Another explanation could be disparities in access to health care. “In my mind, it would be a good study to do to begin to understand the contributors to this geographic variation in suicide in the United States,” said Bridge.
In 2015, Bridge and his team began looking at trends in suicide among children 5 to 11 years old in the United States and found that there was no trend overall. However, when his team stratified the data by race, they saw two divergent patterns. Among White children, and particularly 5- to 11-year-old boys, there was a significant decrease in the suicide rate from 2001 to 2015, while among Black children the opposite was true (Bridge et al., 2015, 2018). Extending the age range, Bridge and his team found that around age 13, the suicide rate among Black youth began to decrease relative to the rates among White youth, a decline that continued throughout adolescence (Bridge et al., 2015) (see Figure 7). He noted that suicide was the 16th leading cause of death among Black youth and the 12th leading cause of death among White youth in 1999, and by 2018 it had become the 7th leading cause of death for both Black and White youth.
Regarding nonfatal suicidal behavior, researchers have found that there was a decline in suicidal thoughts and behaviors across racial and ethnic groups
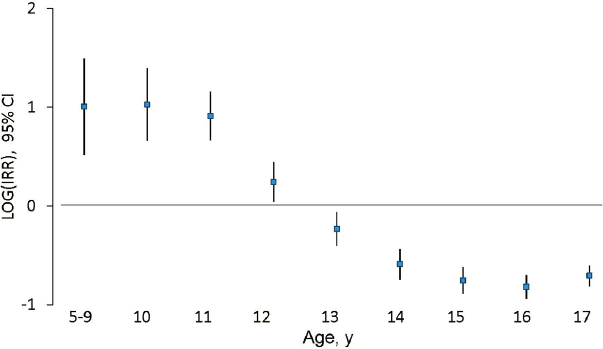
NOTES: Blue squares indicate the estimated LOG of the age-specific IRR, vertical lines indicate 95% CI, and reference group is White youth. CIs of 95% that do not include zero are considered statistically significant. CI = confidence interval; IRR = incidence rate ratio; LOG = natural logarithm; y = years.
SOURCES: Presented by Jeffrey A. Bridge on June 22, 2021, at the workshop on Strategies and Interventions to Reduce Suicide; Bridge et al., 2018.
between 1991 and 2017 (Lindsey et al., 2019). However, when the researchers looked specifically at Black adolescents, there was a significant linear trend increase in the suicide attempt rate for both Black boys and Black girls. In particular, said Bridge, there was an increase for Black males in suicide attempts requiring medical treatment (CDC, 2019; Lindsey et al., 2019).
In preteens, suicide rates for both males and females are well under 1 per 100,000 persons through age 9 but begin to accelerate through adolescence (see Figure 8). For children ages 5 through 12, suicide deaths have increased by 280 percent since their low in 2008 (CDC, 2021a). One study found that 43.1 percent of suicide attempt and suicide ideation (SA/SI) visits were among children 5 to 11 years old (Burstein et al., 2019; Mishara and Stijelja, 2020). “This is a trajectory we do not want to see,” said Bridge. Rates of youth ages 5 to 12 presenting to emergency care settings for self-harm have increased about 5-fold between 2001 and 2019 (CDC, 2021a). Bridge noted that the COVID-19 pandemic has exacerbated this situation to such a degree that Colorado Children’s Hospital has declared a state of emergency because of the rising number of young people presenting to the emergency department with suicidal thoughts or behaviors (Children’s Hospital Colorado, 2021).
In recent years, the National Violent Death Reporting System has begun capturing information about gender identity and sexual orientation, which will make it possible going forward to understand at a regional or national level some
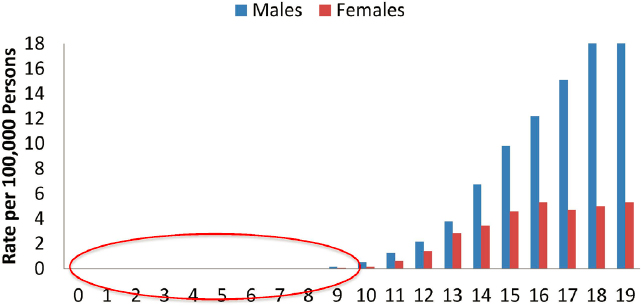
SOURCES: Presented by Jeffrey A. Bridge on June 22, 2021, at the workshop on Strategies and Interventions to Reduce Suicide; CDC, 2021a.
of the factors associated with suicide by sexual orientation, or gender identity status (CDC, 2021b; Ream, 2020), which Bridge called a positive step forward. Data from the Centers for Disease Control and Prevention (CDC) Youth Risk Behavior Survey show that students identifying as lesbian, gay, or bisexual have the highest rates of thinking about, planning, and attempting suicide (CDC, 2019). The rates for those who identify as “not sure” and who may be questioning their sexual identity are also higher than for heterosexual students (see Figure 9). The same pattern exists for students who identify as having a same sex partner compared to those with an opposite sex partner only, added Bridge.
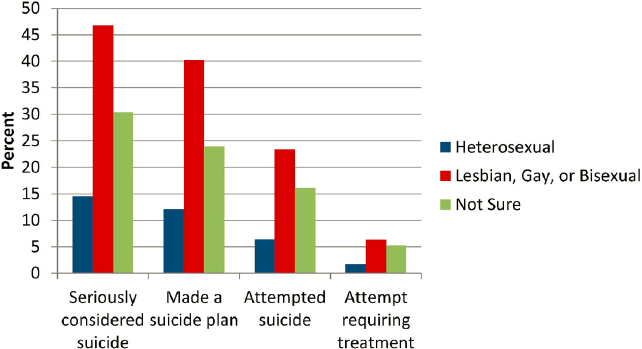
SOURCES: Presented by Jeffrey A. Bridge on June 22, 2021, at the workshop on Strategies and Interventions to Reduce Suicide. Data from CDC, 2019.
A divergent pattern was found between Black and White individuals between 2017 and 2020. When comparing the rates of death by suicide during two periods—March through May 2017 and March through May 2020—the rates for Blacks increased by 94.1 percent but decreased for Whites by 45.1 percent (Bray et al., 2021), though Bridge cautioned that the absolute numbers of deaths by suicide were small. In 2020, another study that examined suicidal ideation, anxiety symptoms, substance use, trauma, and stress-related symptoms found that there were disproportionate adverse mental health outcomes for younger adults, racial and ethnic minorities, essential workers, and unpaid adult caregivers (Czeisler et al., 2020).
At the same time of the COVID-19 pandemic, the United States was experiencing large public protests, particularly the racial awakening typified by the Black Lives Matter movement.4 Bridge mentions these events due to the outsized effect on Black children and adolescents and highlights the need for culturally sensitive adaptations of effective interventions to address the problem of suicide among Black youth. As an example, Bridge described a promising intervention developed by researchers at DePaul University who adapted an existing cognitive-behavioral, group-based preventive intervention that aims to enhance adaptive coping skills and reduce suicidal ideation (Robinson et al., 2021). The adapted 15-session intervention incorporates strategies that counter stressors associated with systemic racism that burdens Black adolescents. The results look promising, Bridge noted, with the adolescents being favorable and receptive to this intervention, thus showing that it is feasible to implement.
Barksdale then discussed the current status of suicide prevention and use of mental health services among U.S. subpopulations. She began by explaining that NIMH is the lead federal agency for research on mental health disorders, supporting more than 3,000 research grants and contracts at universities and other institutions across the United States and abroad. In addition, NIMH’s intramural program supports approximately 600 scientists.
Mental health care services, said Barksdale, are a critical component of suicide prevention efforts, and those services addressing suicide prevention can occur in a variety of settings, including crisis centers, health centers, clinics, in the home, and other locations specific to the population. For example older adults may use services at rehabilitation centers or nursing homes, and children and adolescents may be primarily served in schools. In fact, she added, suicide prevention requires the active engagement of multiple systems working in coordination across multiple settings, she said. Integrating suicide prevention into the delivery of mental health care services has been found to help prevent suicides (While et al., 2012), and this fosters a comprehensive
___________________
4 See https://blacklivesmatter.com (accessed October 25, 2021).
approach to care by encouraging increased collaboration between and coordination of services among care providers.
However, individuals at risk for suicide—and particularly youth and historically minoritized populations—often do not seek mental health services (Hom and Stanley, 2021). This reality affects suicide prevention outcomes and exacerbates disparities in suicidal behavior and suicide prevention. For this reason, Barksdale noted, it is important to understand help-seeking behaviors in order to promote effective suicide prevention efforts and answer questions such as whether a person has or has not considered mental health care, whether they have sought advice from family and friends about getting care, and what their experience with the care they have received has been and if it helped them get better. “Overall, we want to provide and make available culturally and linguistically appropriate mental health care services that meet the needs of individuals at risk, and then encourage individuals to see these services as an option to address their needs,” said Barksdale.
Turning to the subject of mental health services used by specific subpopulations, she said research suggests that across racial and ethnic groups, service use among youth at elevated risk for suicide is consistently below 50 percent (Michelmore and Hindley, 2012) and that only half of the youth (56.1 percent) discharged from inpatient care received a follow-up mental health visit within 7 days (Fontanella et al., 2015). In addition, non-Hispanic Black and other racially and ethnically diverse youth are less likely than non-Hispanic White youth to receive follow-up care from mental health care after psychiatric hospitalization (Merikangas et al., 2011). Moreover, context and settings are critical for youth populations, as racially and ethnically diverse youth are more likely to access mental health care services in school settings compared with community settings or community clinics (Cummings et al., 2010; Jaycox et al., 2010). This is particularly noteworthy in the context of the COVID-19 pandemic, said Barksdale, because these youth could not attend school in person and as a result have not been able to access their usual source of mental health care.
The reasons why racially and ethnically diverse groups may not be using or are underutilizing mental health services vary, but some of the most cited reasons include stigma surrounding seeking help (Eylem et al., 2020), structural inequalities in the mental health care service system (Nazroo et al., 2020; Williams, 2018), and limited knowledge of and access to resources (McGuire and Miranda, 2008). Other reasons include the limited availability of culturally and linguistically competent or culturally appropriate services and limited mental health literacy. For individuals living in rural areas, research suggests that individuals at elevated risk of suicide are less likely than those living in urban communities to have received mental health treatment (Cantrell et al., 2012; Fontanella et al., 2015), and they are more likely to use a firearm in sui-
cide attempts (Searles et al., 2014). Barksdale said multiple factors contribute to rural populations underutilizing mental health services, including a shortage of mental health care providers, the lengthy distance to care providers, low mental health literacy, low perceived need, concerns about confidentiality, and stigma. Even when individuals living in rural areas do seek care, they do so later, often with more serious symptoms, and requiring more intensive treatments than their urban counterparts, said Barksdale.
Regarding mental health services use among sexual and gender minorities, research suggests that lesbian, gay, bisexual, transgender, queer and/or questioning, intersex, and asexual (LGBTQIA+) adults and youth, and particularly those who identify as transgender or gender diverse, are less likely to seek general community mental health services than non-LGBTQIA+ individuals (Craig et al., 2019) and they experience higher risk of suicide ideation (Oransky et al., 2019; Russon et al., 2021). Even when LGBTQIA+ individuals do access such services, they often report a high level of dissatisfaction with the services they receive. Transgender individuals, for example, have significantly different experiences in accessing care, specifically in terms of being denied care and experiencing discrimination. Reasons for underutilization by LGBTQIA+ individuals, said Barksdale, include a lack of family support and lack of support to seek services, concerns about privacy and disclosure, stigma, and a lack of available services that are affirming toward LGBTQIA+ individuals.
Turning to opportunities and next steps, Barksdale highlighted CDC’s social-ecological model of suicide prevention that accounts for the complex interplay between individual, relationship, community, and societal factors.5 This four-tier framework organizes risk and protective factors that can illustrate how one level might influence others and then inform corresponding multilevel intervention and prevention strategies that she believes are critical to addressing the complex issue of suicide prevention.
There are certainly opportunities to improve data collection, said Barksdale, particularly epidemiologic data on minoritized youth and intersectional populations. There are also opportunities to improve the ability to identify individuals, especially minoritized youth, who are at risk of completing a suicide attempt. In addition, more information and research are needed on the best approaches to prevent suicide, particularly among minoritized youth, and ensuring these approaches are both developmentally appropriate and culturally relevant. Barksdale concluded her remarks with a list of research opportunities available at NIMH detailed in Box 2.
___________________
5 Additional information is available at https://www.cdc.gov/violenceprevention/about/social-ecologicalmodel.html (accessed October 25, 2021).
OPPORTUNITIES IN HEALTH CARE TO REDUCE SUICIDE RISK
Following the two presentations, Holly C. Wilcox, professor at the Johns Hopkins Bloomberg School of Public Health, and Richard McKeon, chief of the Suicide Prevention Branch at the Substance Abuse and Mental Health Services Administration (SAMHSA), joined Bridge and Barksdale to answer questions from the workshop participants and to offer a few comments of their own. Jane Pearson, special advisor to the director on suicide research at NIMH, served as the discussion moderator.
Wilcox emphasized the pressing need to have layered suicide prevention approaches that include policies and protocols for workflow; training; developmentally timed, layered, evidence-based practices; coordination across systems of care; and better use of data for action. She also reiterated Barks-
dale’s point that there are many barriers to engaging youth and adults in the traditional array of mental health services. “We lose people along each link in the chain of care,” said Wilcox, who noted that there is some promise in leveraging technology to overcome some of those barriers to care. Wilcox also highlighted the importance of focusing more effort upstream to prevent crises from happening in the first place.
McKeon raised the issue that the Garrett Lee Smith Campus Suicide Prevention Grant Program,6 which SAMHSA funds, is limited by law to the 10–24 age group. This is unfortunate, he said, because research has shown there is a sustained effect after consecutive years of programming, so starting that programming at a younger age might lead to an even larger positive effect on suicide rates in future years. The other implication of that finding is that suicide prevention programming cannot be “one and done.” He also noted that the impact of Garrett Lee Smith grants was greater in rural communities than in other communities, though not in frontier communities (Walrath et al., 2015).
The second point McKeon made was that people at risk for suicide who have made suicide attempts are not getting the mental health care they need. “We have to be aware that there are many people at risk who are just not getting into our care systems, and we need to be able to pay better attention to them,” said McKeon.
The first question for the panelists asked about when data from 2020 will be available. Bridge replied that national mortality data are available about 1 year later, so 2020 data should be available around December 2021. Bridge also noted that CDC has developed a system that provides provisional mortality estimates on a quarterly basis, which does allow for rapid surveillance of the issues.
In response to a question about the role of religious culture and suicide, Pearson asked Barksdale to comment on the religious settings in which some subgroups would potentially feel more or less comfortable. Barksdale replied that there have been several studies that included religion and religious settings as a source of care, which have shown that some individuals prefer to seek help from their religious care provider or their source of religion and have done so quite well (Harris et al., 2021; Hays and Lincoln, 2017), while other individuals have seen that as a source of stigma (Misra et al., 2021). “I think it depends on the cultural relevance of the help-seeking source,” said Barksdale. Understanding help-seeking preferences is important, and there has been work on that subject, as well as on engaging religious institutions around mental health and suicide prevention.
___________________
6 See https://www.samhsa.gov/newsroom/press-announcements/202106251130 (accessed October 25, 2021).
Responding to a question about the role that schools can play in suicide prevention, Wilcox said that schools can be an important component of upstream interventions. “If we can reach youth early, well in advance of a small issue becoming a big problem, we will make tremendous strides in reducing suicidal behavior,” she said. Schools, however, cannot do this alone, and care transitions are absolutely critical between settings that can screen for suicide risk and settings that can intervene. Having a defined pathway for referrals into treatment would make it easier for schools and other screening settings to be part of an integrated system of care.
When asked about the role the 9-1-1 emergency call system can play in suicide prevention, McKeon said the issue is whether suicidal thoughts should always be considered an immediate emergency, and whether the response to such an emergency would be to use whatever means possible to get someone to the emergency department. “There is reason to think that is not the most effective system,” said McKeon McKeon, adding “To the extent to which we can make emergency departments less central as part of a comprehensive suicide prevention response, I think there are many significant advantages to that, simultaneous with trying to improve care in the emergency department and, very importantly, improve follow-up afterward.”
Based on a cohort study, explained McKeon, research has shown that people who made suicide attempts and who were seen in the emergency department had a 56-fold higher rate of death by suicide over the next 12 months, compared to general population patients who also visited the emergency department in the same 1-year period (Goldman-Mellor et al., 2019).
EXPERIENCES IN IMPLEMENTING SUICIDE PREVENTION CARE IN FEDERAL HEALTH CARE SETTINGS
Assessment and Management of Those at Risk for Suicide
Lisa Brenner, professor at the University of Colorado School of Medicine and director of the U.S. Department of Veterans Affairs (VA) Rocky Mountain Mental Illness Research, Education, and Clinical Center (MIRECC), discussed clinical practice guidelines and the role they can play in suicide prevention. The VA issued its clinical practice guidelines in 20197 to incorporate the significant leap in knowledge that had taken place over the 6 years since the VA released its previous guidelines. The VA developed the guidelines through a process of assembling multidisciplinary experts who developed 12 key questions, having an independent third party conduct a systematic review
___________________
7 See https://www.healthquality.va.gov/guidelines/MH/srb (accessed October 25, 2021).
of the evidence relevant to those questions, and using a model of that looks at population, intervention, comparison or control, outcome, and time period, known as the PICOTS framework (Riva et al., 2012), to develop 22 recommendations that would put the best evidence into clinical practice. She noted that in many cases, sufficient research has yet to be conducted, highlighting an opportunity to engage in continued rigorous efforts to evaluate practices as a means of augmenting the existing evidence base.
As an example, one question the experts posed aimed to identify the most effective treatment approaches for patients identified as being most at risk for attempting suicide, particularly with regard to who was at risk and where and when to deliver an intervention. Brenner noted that this question highlighted an important point, which is that most of the research relevant to this question did not include minority populations and thus the findings may not hold for individuals from different backgrounds, different sexual orientations, gender identities, and different histories.
Of the 22 recommendations, 5 pertain to screening and evaluation, 12 to risk management and treatment, and 5 to other care management modalities including population- and community-based interventions. Brenner noted that each recommendation has a “strength” notation that indicates how strong the evidence is in favor or against a specific clinical practice. As an example, she cited one of the screening and evaluation recommendations that states,
We recommend an assessment of risk factors as part of a comprehensive evaluation of suicide risk, including but not limited to current suicidal ideation, prior suicide attempt(s), current psychiatric conditions (e.g., mood disorders, substance use disorders) or symptoms (e.g., hopelessness, insomnia, agitation), prior psychiatric hospitalization, recent biopsychosocial stressors, and the availability of firearms.
Brenner noted that the evidence is strong for this recommendation. She added that in many cases, these recommendations line up with requirements for accrediting bodies.
The risk management and treatment recommendations include four pertaining to nonpharmacologic treatment, three to pharmacologic treatment and post-acute care, and two to technology-based treatment modalities. Brenner also noted that nonpharmacologic interventions include one for which the evidence is strong—using interventions based on cognitive behavioral therapy that are focused on suicide prevention for patients with a recent history of self-directed violence to reduce incidents of future self-directed violence—and three for which the supporting evidence is weak—offering dialectical behavioral therapy to individuals with borderline personality disorder and recent self-directed violence; offering psychotherapies based on problem solving to three specific groups of patients, and completing a crisis response plan for individuals with suicidal ideation or a lifetime history of suicide attempts. While the evidence supporting the use of these plans is weak, the VA highly
recommends that clinicians engage in this type of activity, which is also an accreditation requirement. Brenner said that the VA clinical practice guideline website contains a variety of resources for each recommendation, as well as three clinical algorithms for clinicians.8
PROMOTING LETHAL MEANS SAFETY AMONG VETERANS: OPPORTUNITIES AND CHALLENGES
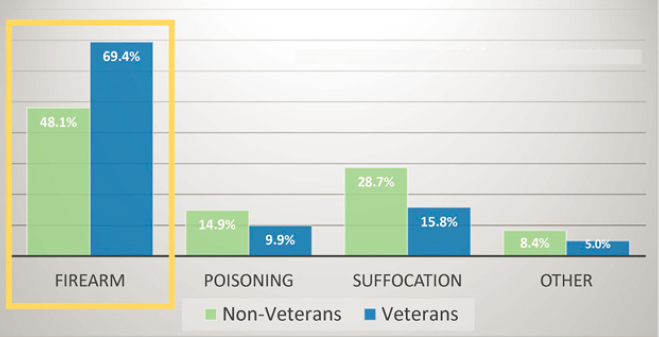
Lethal means safety is an intentional, voluntary practice to reduce access to lethal methods of suicide in order to reduce suicide risk, explained Joseph Simonetti, a physician and suicide prevention researcher at the VA Rocky Mountain MIRECC. This can be accomplished using a cable lock to secure a firearm, storing a firearm or ammunition outside of the home, or keeping medications in a secure lockbox stored away from those in a household who are at risk of suicide. Reduced access to lethal methods is one of the evidence-based methods for reducing suicide rates at the population level, said Simonetti. For that reason, the VA clinical practice guidelines, as well as various medical and public health professional societies, promote lethal means safety counseling or firearm safety counseling for individuals with elevated suicide risk. He added that in the VA, discussing how to reduce access to firearms is a key focus of lethal means safety counseling because 70 percent of veterans who die by suicide do so with a firearm (see Figure 10).
SOURCE: Presented by Joseph Simonetti on June 22, 2021, at the workshop on Strategies and Interventions to Reduce Suicide; VA, 2019.
___________________
8 Additional information is available at https://www.healthquality.va.gov/guidelines/MH/srb (accessed October 25, 2021).
In practice, VA clinicians provide lethal means safety counseling as part of a safety plan, which is developed for patients with identified suicide risk. In addition, the VA now has an effort under way to provide standalone firearm safety counseling for patients with other identified injury risk factors. Simonetti explained that the VA is now supporting clinicians in providing firearm safety counseling across a wide array of clinical settings and different scenarios, and it has begun developing training resources for individuals in the firearm retail industry to parallel the VA’s counseling efforts. At the same time, he added, the VA’s research portfolio related to firearm injury prevention in general and suicide prevention specifically has expanded to ensure the VA is delivering high-quality and evidence-based interventions to its at-risk patients.
Simonetti suggested that one reason the VA has been able to establish itself as a leader in this field is its preexisting infrastructure and expertise in suicide prevention that is centrally coordinated. “That means we are able to rapidly disseminate resources to the field and reach a broad number of clinicians, and thus a large number of patients, through most of our efforts,” said Simonetti. Another reason why the VA has been able to move forward with this effort is that there is a high level of acceptability throughout the VA system for having these types of conversations in clinical spaces. For example, the 2019 National Firearms Survey (Simonetti et al., 2021) shows that between 80 and 90 percent of those who live in U.S. households with firearms agree that clinicians should initiate firearm safety discussions when someone is at risk of suicide. In addition, there is widespread recognition that veterans are at elevated risk of suicide (Nelson et al., 2017). During a 2021 interview, when asked about discussing firearm safety with clinicians, one veteran told Simonetti that it was not bothersome that information came from clinicians because he trusts them, and while it seemed that this was nobody’s business but his, he recognized that too many veterans are dying by suicide and so this went beyond his personal beliefs (Newell et al., 2021).
That being said, Simonetti noted there are a few important challenges to address to realize the full potential of lethal means safety counseling. First, lethal means safety counseling is not a single intervention; rather, it needs to be provided across many different settings and through different messengers delivering different messages to a heterogeneous mix of at-risk populations. In addition, researchers are challenged to develop and disseminate interventions that are effective, feasible, and tailored to these different audiences and settings.
Another challenge, he noted, is related to efforts to move suicide prevention interventions upstream. “This is critical because we know that many of our patients who go on to die by suicide are not engaged in specialty mental health treatment or safety planning,” he said. Moving upstream by shifting the responsibilities for these tasks to clinical spaces that may be less accustomed to
mental health treatment or suicide prevention generally is likely to require a shift in clinical practice for many clinicians and perhaps even a shift in clinical culture. “It is one thing to provide a psychologist with better tools to deliver firearm safety counseling,” Simonetti, continuing,
It may be a whole different challenge to begin thinking about how we facilitate the delivery of these discussions in medical and surgical subspecialty settings, for example, that do not consider suicide prevention within their clinical purview or wheelhouse.
Moving upstream will also require evidence that these interventions will remain acceptable and effective in the upstream setting. Simonetti notes that one thing that research has made clear is that while in general there is a high level of acceptability in terms of discussing lethal means safety, clinical context matters (Dobscha et al., 2021; Richards et al., 2021; Simonetti et al., 2020). Simply put, patients want to know why they are being asked about their firearms, said Simonetti.
In his final remarks, he noted that media reporting has suggested that firearm sales have surged, marked by purchases from different demographic groups and those who have different ownership motives, including individuals who have a wide range of prior training and experience with respect to firearm safety. The result, said Simonetti, is that these new gun purchasers may also have different firearm safety behaviors (Lyons et al., 2021). One study even found that individuals who purchased firearms for the first time during the COVID-19 pandemic were more likely to have suicidal ideation than other firearm owners (Anestis et al., 2021). “It is unclear whether the past year has spawned these unique risk populations that we know very little about in terms of both their suicide risk and their firearm safety behaviors,” he said. Indeed, he added, much of the research in the qualitative and survey literature has focused on understanding the perspectives of the population that is familiar with firearms and how that population tends to have different perspectives and experiences from those that do not own or experience firearms regularly.
What is needed, he said, is research to understand the perspectives of people who own and/or live with firearms based on other characteristics such as gender or experiences with racial discrimination or trauma. Otherwise, said Simonetti, public health will continue to be at a disadvantage in trying to explain why suicide risk and rates may differ and be on different trajectories among specific populations. “That limits our ability to think about how we should be tailoring our approaches,” he noted in closing. “This is work we desperately need to pursue if we are going to develop and eventually disseminate patient-centered interventions related to firearm safety and lethal means safety.”
SUICIDE PREVENTION AND CARE PROGRAM
Pamela End of Horn, the national suicide prevention consultant to the Indian Health Service’s (IHS’s) Office of Clinical and Preventive Services, discussed IHS’s efforts to work with national and local tribal communities on suicide prevention. Suicide, she noted, is a significant issue to Indian country—suicide is the eighth leading cause of death among all American Indian and Alaska Native communities across all ages—and it is one that can take over entire communities. The Suicide Prevention and Care program, she explained, operates in conjunction with programs in mental health and substance use disorders and with the IHS Telebehavioral Health Center of Excellence9 to provide programs to tribal communities and tribal nations that focus on behavioral health care and suicide prevention.10
IHS, explained End of Horn, is a health care system, but, unlike the VA, it is more of a set of systems than one system in that it has federal partners, tribal partners, and local partners. Noting that the focus of IHS is on upstream models of care, she explained:
We work to empower local tribal communities to take what we can provide them in regard to program offering, funding, information, evidence-based practices, best practice models, and help them implement them at the local level.
Regarding suicide prevention and care, she and her colleagues are engaged in the Ask Suicide-Screening Questions (ASQ) Toolkit pilot project (Horowitz et al., 2013; LeCloux et al., 2020), the IHS Substance Abuse Suicide Prevention Program,11 and the Zero Suicide Initiative (Layman et al., 2021; Stapelberg et al., 2021), as well as developing the IHS community crisis response guidelines for addressing suicide behavior-related crises.12
The Zero Suicide model, explained End of Horn, is a comprehensive approach to suicide care that aims to reduce the risk of suicide for all individuals seen in health care systems (detailed in Box 3). Zero Suicide represents a bold commitment to patient safety, she said, holds the belief that the entire health system has the responsibility for preventing suicide deaths for patients under care. Zero Suicide promotes the use of seven elements to improve patient safety—lead, train, identify, engage, treat, transition, and improve—as being essential to improving patient safety. She noted that most of the Zero Suicide pilot sites are located in the U.S. Southwest, with three in Navajo
___________________
9 See https://www.ihs.gov/telebehavioral (accessed October 25, 2021).
10 See https://www.ihs.gov/telebehavioral (accessed October 25, 2021).
11 See https://www.ihs.gov/sasp/aboutsasp (accessed October 25, 2021).
12 See https://www.ihs.gov/suicideprevention/communityguidelines (accessed October 25, 2021).
areas, one each in Phoenix, Albuquerque, and Oklahoma City, as well as two in the north in Bemidji, Minnesota, and Billings, Montana. This wide swath of sites requires adapting how the model is implemented to reflect local cultures.
The pilot program, said End of Horn, established cooperative agreements with the tribal governments so that she and her colleagues could work closely with the tribes to understand how best to apply the model, how it works in different cultures, and what the tribes needed to do within their health systems to improve care and prevent suicides. The pilot program ended in 2021. She noted that while the COVID-19 pandemic created significant challenges to the program, particularly with regard to in-person to health care facilities, it also made the tribes realize that they can implement this type of model within the community and within their schools. One site, for example, established a COVID-19 hotline that people could call if they were feeling overwhelmed or suicidal and needed to gain access to resources. “It helped the community find a cohesive response to the issue of the pandemic and the reality that they were facing in regard to what was happening at the local level,” she said. The new perspective that the local sites have gained from the COVID-19 pandemic is something that she hopes to maintain.
The pilot program has also encountered a number of challenges, including high staff turnover and having to invest in retraining, as well as the need to have staff dedicated to case management and follow up. Other challenges have included establishing and maintaining participation with primary care, a lack of collaboration with community health facilities following inpatient discharge, a lack of data-sharing agreements that hinders assessment and continuous improvement activities, and the difficulty of retrofitting electronic health records (EHRs) to embed screening, assessment, and tracking tools.
Going forward, said End of Horn, she and her colleagues plan to use crisis lines to assist with follow-up contacts and use case managers to conduct continual tracking of patients in care pathways. They also plan to improve EHR functionality by adding alerts and establishing data-sharing agreements.
IMPROVING SUICIDE PREVENTION: ADDRESSING KNOWN BARRIERS TO HEALTH CARE ACCESS
Ursula Whiteside, chief executive officer at NowMattersNow.org and clinical faculty member at the University of Washington, introduced the next session by referring participants to the 2018 report from the National Action Alliance for Suicide Prevention, Recommended Standard Care for People with Suicide Risk,13 which aims to help health systems better identify and support people who are at increased risk of suicide. In particular, she said, the report addresses some of the barriers that people at risk of suicide face in accessing care. “People with lived experience have all sorts of reasons for not reaching out for care or for having poor experiences when they do,” she said.
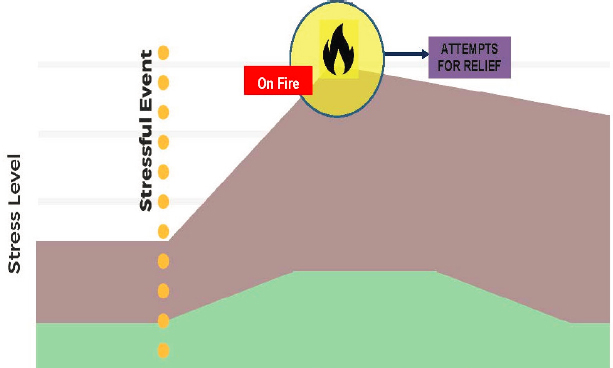
Whiteside referred to a treatment called dialectical behavior therapy,14 a form of cognitive behavior therapy that her team uses to understand the history and biology that informs where people are on a day-to-day level in terms of their stress. On a given day, for example, some people are more emotionally reactive than others based on different adverse life experiences, such as trauma or systemic injustice. “We think about this as being on fire emotionally, and the adverse experience may explain why people do things that they would not necessarily do otherwise” said Whiteside. She asked the workshop participants to consider this model (see Figure 11) of emotional dysregulation when thinking about a person during a crisis, adding that this model can also help family members and friends have a better understanding of what someone at risk of suicide may be experiencing.
Language matters, emphasized Whiteside. Based on feedback received from those who have had a personal experience related to suicide, health care
___________________
13 The report is available for free at https://theactionalliance.org/sites/default/files/action_alliance_recommended_standard_care_final.pdf (accessed October 26, 2021).
14 Additional information is available at https://behavioraltech.org/resources/faqs/dialectical-behavior-therapy-dbt (accessed October 26, 2021).
SOURCE: Presented and created by Ursula Whiteside on June 22, 2021, at the workshop on Strategies and Interventions to Reduce Suicide.
providers and others should choose compassionate and accurate language when discussing suicide. Language should shift from using the term “committed suicide” to “died by suicide or died of suicide,” and from “dealing with” suicidal patients to “working with” them. Similarly, she said, it is important to be thoughtful in describing behavior and not adding an interpretation, which means eliminating the use of phrases such as “manipulative,” “attention seeking,” “suicidal gesture,” and “cry for help.”
Whiteside noted that in the work she does, she is guided by a team of people with lived experience. The biggest take-home message they have is that all the interventions in the world may not help if the health care provider panics, does not show that they are with the individual in that moment of crisis, and cannot figure out a way to offer hope. “This is not in an ‘It is going to be okay, I have all the answers’ manner, but in a way that conveys they will help that person in crisis get through the next 5 minutes.”
IMPROVING SUICIDE PREVENTION: ADDRESSING KNOWN BARRIERS TO HEALTH CARE ACCESS FOR LGBTQIA+ PEOPLE IN INSTITUTIONAL SETTINGS
With almost 2.1 million people, New Mexico is a culturally rich, mostly rural, economically challenged majority-minority state, explained Cathleen Willging, center director and senior research scientist at the Pacific Institute for Research and Evaluation’s Southwest Center. Suicide is a lead-
ing cause of death, she continued, with the state experiencing higher rates of suicide than the U.S. average for the last quarter of the century. Rates of suicidal behaviors for LGBTQIA+ adults and youth far exceed those for heterosexual and cisgender New Mexicans (Whiteside, 2019; Whiteside and Green, 2021).
In 2019, more than 19 percent of sexual minority adults and 22 percent of gender minority adults in New Mexico had reportedly considered attempting to die by suicide (Personal communication from C. Whiteside to C. Willging, 2021), while 40 percent of LGBTQIA+ high school students had considered attempting to die by suicide, 34 percent developed a plan to do so, and 25 percent making an attempt in the past year (Ivey-Stephenson et al., 2020; Whiteside, 2019). These disparities in suicidal thoughts and behaviors, said Willging, are linked to exposure to structurally based stressors, such as discrimination, associated with being part of a socially stigmatized group, as opposed to being LGBTQIA+ in and of itself.
Willging noted that New Mexico is underserved medically, with most services concentrated in Albuquerque, while all or parts of 33 counties, accounting for 50 percent of the state’s population, are designated primary care and health professional shortage areas (Avery et al., 2018). Some 60 percent of the state’s residents live in mental health professional shortage areas, and in addition, the state’s behavioral health system is fragmented and fragile, a situation exacerbated by the forced closure of community mental health centers in 2013 that created mental health care deserts throughout the state (Willging and Trott, 2018). This closure was caused by a political controversy that resulted in the New Mexico’s Department of Health and Human Services removing Medicaid payments to 15 mental health providers after an audit reported credible evidence of fraud (Terrell, 2019). As a result, primary care clinics in the state are struggling to increase their service delivery capacity because there are few places to which they can refer patients, and appointments and waiting lists for services are long throughout the state of New Mexico. Furthermore, most practices have yet to try tailoring services to LGBTQIA+ patients.
Schools are another de facto source of support, Willging added, though there are less than 80 school-based health centers for New Mexico’s 89 school districts and 867 schools (LESC, 2021a,b; LFC, 2021). Of the 89 school districts, 18 have less than one full-time school nurse, with more than one-third of the school-based nurses serving multiple campuses (Shattuck et al., 2021). In 2009, said Willging, 40 percent of the state’s high school-based nurses provided emergency management for a suicidal student, a figure that increased to 75 percent in 2019 (Ramos et al., 2013; Shattuck et al., 2021).
Willging explained that her remarks draw from two studies shaped by implementation science.15 The first study was a randomized cluster trial initiated in 2016 that used implementation science to enable the uptake of evidence-informed practices to make high schools safer and more supportive of LGBTQIA+ students, thereby reducing their risk for suicidal behavior (Green et al., 2018; Shattuck et al., 2020; Willging et al., 2016).16 The second study used a mixed method research design to assess factors affecting access to quality primary care for LGBTQIA+ patients, focusing on clinical preparedness, implementation climates, and readiness for LGBTQIA+-centered care in clinical settings (Willging et al., 2020).17
Social institutions such as health systems and schools perpetuate cultural values of heteronormativity and cisgenderism that can harm the health of LGBTQIA+ people from youth into adulthood, said Willging, “the attitudes, language, and behaviors of health and school professionals can engender hostile climates, marginalizing LGBTQIA+ people and making them feel disconnected.” Experiences of discrimination in these settings, such as the biased enforcement of rules that disproportionately target LGBTQIA+ youth and students of color, combined with the social pressures of being part of a minoritized group, contribute to school pushout and a domino effect of other negative consequences that can heighten a young person’s risk for suicide as they age, she explained. Furthermore, when LGBTQIA+ people experience discrimination in health care settings, they may delay or avoid getting the care they need.
Willging noted that staff in health systems and schools commonly state that they treat everyone the same to signify that they do not discriminate, yet such attitudes may reduce the motivation to educate themselves and support evidence-informed policies and practices that might benefit the physical and mental health of LGBTQIA+ people. In addition, a pervasive lack of education among health and school professionals contributes to the invisibility of LGBTQIA+ people in institutional settings and low awareness of their unique mental health needs.
Several barriers thwart access to needed supports in schools, said Willging. To start, the paucity of school-based health care professionals creates hardships
___________________
15 Implementation science is the scientific study of methods and strategies that facilitate the uptake of evidence-based practice and research into regular use by practitioners and policymakers. More information can be found at https://impsciuw.org/implementation-science/learn/implementation-science-overview (accessed November 29, 2021).
16 Additional information is available at https://southwest.pire.org/project/implementing-school-nursing-strategies-to-reduce-lgbtq-adolescent-suicide (accessed October 26, 2021).
17 Additional information is available at https://southwest.pire.org/project/enhancing-primary-care-services-for-diverse-sexual-and-gender-minority-populations (accessed October 26, 2021).
in identifying or responding to any student with suicidal behaviors. Moreover, school staff are often unsure as to whether community-based care providers are LGBTQIA+ competent or accepting. In addition, the professional development of school staff on suicide prevention and intervention occurs infrequently, is seldom reinforced through follow-up training, and typically is not a priority for school leadership unless it is student or community initiated. She added that because of high turnover rates across schools, many staff are unlikely to receive even basic training to address suicide.
Willging et al. (2016) has found that school staff often cite low mental health literacy and insufficient engagement among parents and guardians as major challenges in making sure students experiencing suicidal behaviors get support. In addition, stigma about having their children identified as having mental health concerns or as queer creates further resistance among parents to seek needed services and support. In the same way, primary care providers point to the difficulties of delivering private, confidential care to at-risk LGBTQIA+ youth without accepting families.
In addition to the challenges of accessing needed services in schools, Willging said there are additional barriers to addressing the needs of LGBTQIA+ people at risk for suicide. The primary care providers and staff she and her colleagues have talked to make it clear that clinics could be doing more to engage in outreach and to advertise their services to LGBTQIA+ people to pull patients in for care. They report not knowing much about LGBTQIA+ resources outside their clinics, including where to get training or where to refer patients with mental health concerns, such as LGBTQIA+ support groups. One reason outreach is not happening, she noted, is that administrators are not seeing a need to engage in those types of activities. “LGBTQIA+ people remain off the radar, and the demand for LGBTQIA+-responsive services is deemed low,” said Willging. “Not having electronic medical records setup to collect and use data on the gender identities and sexual orientations of patients, or staff prepared to ask appropriate questions to get this information, likely contributes to perceptions of low demand.”
Worse yet, during Willging’s research, she found that administrators in some places do not want to create LGBTQIA+-responsive services because they do not want to make non-LGBTQIA+ patients resentful or uncomfortable. Having to care for patients of varying ages and cultural backgrounds also makes it hard to justify innovating services for LGBTQIA+ people, said Willging. This contributes to the siloing of expertise in which only a minority of staff may possess the knowledge and skills necessary to work with LGBTQIA+ patients, particularly with respect to gender affirming care.
One major finding from her two studies is that people do not know what they do not know. “Until they started taking part in our studies, many folks we talked to had not given much attention to LGBTQIA+ issues in their
workplace, so they did not have a reason to prioritize or invest in inclusive services or supports,” said Willging. “Because these issues are on the periphery of their radar screens, if at all, preparedness to intervene appropriately to reduce negative health and mental health outcomes for LGBTQIA+ people is minimal.” On the other hand, her research showed that through professional development, it is possible to make substantial inroads toward enabling people working in these institutional settings to become more involved and to initiate the processes of organizational change.
In terms of what institutions can do to reduce access barriers and health disparities for LGBTQIA+ individuals, there are evidence-informed practices available. Schools, for example, can establish safe spaces and social groups on campus that promote school connectedness among LGBTQIA+ students, a major protective factor against suicidal behaviors. Schools can also adopt inclusive curricula that do not neglect LGBTQIA+ health concerns and that foster mental health literacy. They can also vet community health care providers and confirm they are knowledgeable about and provide supportive care for LGBTQIA+ people. In fact, she and her colleagues have collaborated with schools to organize LGBTQIA+ 101 trainings for local care providers, attracting them by offering free continuing education credits.
Primary care clinics can do more as well, particularly in terms of creating a welcoming environment. Steps they can take include increasing outreach efforts in the communities they serve, transitioning to gender-neutral restrooms, and displaying artwork and educational materials that signify their support. Clinics can also start collecting and using data on gender identity and sexual orientation as part of routine clinical care and make it possible for staff to understand and address disparities affecting LGBTQIA+ patients. In addition, primary care clinics have a responsibility to ensure, through targeted workforce development, that LGBTQIA+ patients receive care in keeping with national recommendations and best practices.
Willging said that everyone working in schools and primary care should be expected to—and empowered to—become familiar with basic approaches to cultural competency when interacting with LGBTQIA+ people. They also need to be proficient in using common LGBTQIA+ terminology, as well as supporting and enforcing antidiscrimination policies as a means of guarding against marginalizing LGBTQIA+ people. Finally, she added, by forging connections with LGBTQIA+ communities, such as with advocacy organizations, schools and clinics will find eager collaborators willing to make these things possible.
There are, however, social factors, pragmatic considerations, and leadership issues that can get in the way of introducing innovations that support populations such as LGBTQIA+ people that experience health disparities and increased risk for suicide. For example, being from a small socially conservative
community where stigma surrounding mental health and LGBTQIA+ issues abounds can make staff less likely to get visibly engaged as change champions. Time constraints, being overworked, and lack of resources can also get in the way of implementing LGBTQIA+-inclusive practices in schools and clinics. So, too, can misalignment among different leaders within an organization. In one case, Willging shared, school nurse leaders were eagerly awaiting the receipt of implementation support for suicide prevention, but their principals unilaterally withdrew from Willging’s school study based on their personal beliefs that LGBTQIA+ students did not warrant special intervention. Leaders may also deprioritize LGBTQIA+-directed initiatives for less problematic reasons, as their time and energy are often devoted to ensuring that schools and clinics comply with the many state and federal mandates governing education and health care delivery.
While institutions need to change and foster suicide prevention and intervention for populations with health disparities, Willging said that society cannot demand change without investing in the institutions and people who work within them to do things differently. Professional development that cultivates knowledge and reflection on the social causes of ill health and understanding of the reasons behind inadequate or fragmented support is critical, she said, adding that it cannot be done in a single training. Willging briefly noted that while focusing on health risk behaviors at the individual level is useful for professional development, it can also reinforce stigma and stereotypes when it is not paired with attention to structural and systemic processes that exacerbate inequities for minoritized social groups. In that respect, adopting a structural competency framework to organize professional development can be useful by enhancing awareness of upstream factors such as stigma and discrimination that abet marginalization and give way to disproportionate risks for suicidal behaviors. Such a framework can also enhance the case for larger-order, focused interventions directed at changing implementation environments, overcoming institutional inertia, and doing something about adverse health outcomes for particular social groups.
Making a pitch for using implementation science to overcome barriers, Willging said there are conceptual frameworks to guide change processes and promote access to suicide prevention and intervention in institutional settings. Two frameworks she mentioned were the Consolidated Framework for Implementation Research (Damschroder et al., 2009) and the Exploration, Preparation, Implementation, and Sustainment framework (Aarons et al., 2011). These frameworks focus on multiple stages and levels of influence during change processes, encouraging initial and ongoing assessment of factors at the outer context, including the broader system environment, policy, funding, and community stigma, as well as inner context factors, or characteristics internal
to a school or clinic, such as staff and leader attitudes and behaviors. They also offer roadmaps for crafting climates conducive to successful implementation.
Implementation science also offers tools to increase the uptake of new programs or practices. Two strategies for promoting stakeholder engagement and building capacity among diverse stakeholders to wrestle with health disparities include the dynamic adaptation process (Aarons et al., 2012) and implementation facilitation (Ritchie et al., 2020). As a final comment, Willging said that implementation science is about addressing messy but important problems, including health disparities and structural incompetence. She said,
Addressing such problems is complex and takes time, but [it] is essential to carrying out evidence-based suicide prevention and intervention in schools, clinics, and other institutional settings, and for reducing high rates of suicidal behaviors for health disparity populations.
RISK ID: THE VA SUICIDE RISK IDENTIFICATION STRATEGY
One way to improve the availability of suicide prevention services is by upstream screening and evaluation, which the VA has been striving to implement throughout its health care system, not just in mental health specialty care, said Brenner. The VA’s Suicide Risk Identification Strategy program (Risk ID) is a national, standardized process for suicide risk screening and evaluation using high-quality, evidence-based tools and practices to facilitate and encourage fidelity to best screening and evaluation practices. “This is the largest effort that has been undertaken in any health care system in the United States,” she said, adding that the VA has screened about 6 million people using Risk ID, including many who would not have been seen in a specialty clinic.
Risk ID outlines a clear process for who should be screened and evaluated, when screening or evaluation should occur, and how screening or evaluation should be conducted and documented. It includes a universal requirement that every veteran will be screened by an appropriate staff member. Specific clinical settings in which the veteran is known to be at risk have additional screening and evaluation requirements (see Table 1), said Brenner, who added that Risk ID is also indicated when a new behavioral health concern is evident. By including these different clinical settings, the VA now has many more health care providers who understand that suicide prevention is part of their daily business and that they are responsible for it in their screening and treatment situations. She also noted that the process of screening and evaluation has evolved over time with new evidence and that the VA expects it will continue to evolve as the program continues to gather data.
The two-step Risk ID process uses the Columbia-Suicide Severity Rating Scale (C-SSRS), a validated, evidence-supported questionnaire available in 103
TABLE 1 Minimum Screening Requirements by Setting for Risk ID
| Setting | Requirements (in addition to Annual Screening) |
| Emergency Department and Urgent Care Centers | C-SSRS Screener at each encounter (is embedded in the National Emergency Department/Urgent Care RN Triage note) |
| Outpatient Mental Health | C-SSRS Screener during intake evaluation; as clinically indicated thereafter |
| Sleep Clinic | C-SSRS Screener at referral or intake; C-SSRS Screener must be completed during intake evaluation if > 30 days from referral; as clinically indicated thereafter |
| Pain Clinic | C-SSRS Screener at referral or intake; C-SSRS Screener must be completed during intake evaluation if > 30 days from referral; as clinically indicated thereafter |
| Opioid Treatment Program | C-SSRS Screener during intake evaluation; as clinically indicated thereafter. In cases of administrative discharge, CSRE within 24 hours before discharge if the patient can be reached. |
| Mental Health Residential Rehabilitation Treatment Program | C-SSRS Screener within 24 hours of admission and CSRE during the first week of admission; updated CSRE within a week before discharge and C-SSRS within 24 hours before discharge |
| Community Living Center | C-SSRS Screener within 24 hours of admission and within 24 hours before discharge |
| Inpatient Mental Health | C-SSRS Screener within 24 hours of admission and within 24 hours before discharge |
| Inpatient Medical/Surgical | C-SSRS Screener within 24 hours of admission and within 24 hours before discharge |
| Inpatient & Residential Rehabilitation | C-SSRS Screener within 24 hours of admission and within 24 hours before discharge |
NOTE: C-SSRS = Columbia-Suicide Severity Rating Scale; CSRE = VA Comprehensive Suicide Risk Evaluation.
SOURCE: Presented by Lisa Brenner on June 22, 2021, at the workshop on Strategies and Interventions to Reduce Suicide.
different languages.18 A positive C-SSRS score requires the timely completion of the VA Comprehensive Suicide Risk Evaluation (CSRE), which would be on the same day in the ambulatory care setting and with 24 hours in inpatient or residential settings. The CSRE is designed to inform clinical impressions about acute and chronic risk and associated disposition, thereby allowing clinicians to match the risk level with an appropriate treatment.
To support staff that may not be accustomed to conducting suicide risk screening, VA has developed a number of additional trainings, laminated
___________________
18 The C-SSRS questionnaire and additional information is available at https://suicidepreventionlifeline.org/wp-content/uploads/2016/09/Suicide-Risk-Assessment-C-SSRSLifeline-Version-2014.pdf (accessed November 5, 2021).
screening materials, and dashboards that clinicians can review to see how well they are doing. Risk ID includes a technical support email address and call center as well. “We are trying to support care providers in different settings and in different types of care and implement this as a whole-of-enterprise process,” said Brenner. The dashboard, for example, helps clinicians identify who they are missing and why, which not only helps improve overall levels of practice, but also provides information on workflows and practice settings that can help local clinics improve their operations.
One of the initial assessments of Risk ID demonstrated that instituting a universal screening plan is possible with commitment and technical assistance (Bahraini et al., 2020). This study also showed that the risk level of veterans seen in the emergency department was higher than for those seen in an ambulatory care setting, which was not unexpected, said Brenner. The VA has begun collecting initial data regarding race, ethnicity, and other factors that should help the VA ensure that individuals from different backgrounds are receiving screening and evaluation though missing data limits the VA’s ability to assess for health disparities by race (GAO, 2019).
Brenner’s hope is that the VA will implement more evidence-based practices, conduct more systematic screening, and generate more data that will enable the system to do a better job of meeting the needs of all veterans equitably. As a closing comment, she said that the VA has a free consultation service available for clinicians treating veterans in community care settings.19
SUICIDE PREVENTION: BARRIERS TO CARE AMONG BLACK YOUTH AND FAMILIES
Between 1991 and 2017, 18.8 percent of U.S. high school–aged youth thought about suicide and 14.7 percent had formed a suicide plan (Lindsey et al., 2019), said Michael Lindsey, executive director of New York University’s McSilver Institute for Poverty Policy and Research. Over the same period, he noted, suicide attempts for Black youth rose by 73 percent while falling for every other racial and ethnic group. Similarly, the rate of injury related to a suicide attempt for Black youth increased by 120 percent over that time. These increases occurred even while thinking about and planning suicide had actually decreased among Black youth over that period, which led Lindsey to wonder if Black youth might be going straight to a suicide attempt.
To explore that possibility, Lindsey and his collaborators used an ideation to action framework (Klonsky and May, 2015) to look at whether there are
___________________
19 See https://www.ptsd.va.gov/professional/consult/index.asp (accessed October 26, 2021).
distinctions based on race in terms of which youth are engaging in different types of nonfatal suicide behaviors. He noted that many studies examine outcomes related to suicides by comparing youth who have engaged in suicide behavior compared to non-suicidal youth, whereas this study looks within the group of youth who have engaged in suicide behavior to see if there are any distinctions. The main finding from this study was that compared to youth of all other racial and ethnic groups, Black youth had higher odds of having an attempt only and no preceding thoughts or plans. “In terms of screening and prevention, this is scary when you think that the common warning signs we look for in terms of suicidal behavior might not be as apparent for Black youth,” said Lindsey. In fact, he added, a recent study found that there is a higher rate of suicide misclassification for Black adolescents who died compared to their White counterparts (Ali et al., 2021).
Turning to the subject of barriers to care, Lindsey noted that large scale epidemiologic studies have shown that Black youth, relative to White youth, underuse specialty mental health care and receive less treatment for mood disorders (Costello et al., 2014). Research has also found that fewer than 50 percent of youth who access mental health treatment do so following an emergency department visit (Bridge et al., 2012; Rhodes et al., 2018).
In terms of barriers to care, Lindsey addressed two broad factors. Factor one, he said relates to the stigma associated with mental illness and service use and the primacy of family support. Qualitative studies he has conducted have found that Black youth prefer to take their problems, concerns, and cares to family members first, and in many cases, the family members then tell them not to take their problems outside of the family. Often, said Lindsey, Black youth who present with a mental health struggle are seen by their family members—and even educators—as simply being lazy, and therefore, are not likely to seek care for the child. In addition, there is a distrust of health care providers because of concern they will not understand a Black person’s unique experiences and provide messages discordant with lived, contextual experiences or that the provider will misdiagnose or misclassify presenting symptoms.
The results of these attitudes are seen in a study Lindsey and his colleagues conducted in Baltimore. There, they found that about half of a sample of 465 ninth graders had identified mental health needs, but only 20 percent of those students received services, even when those services were available at their schools (Lindsey et al., 2010). All this, said Lindsey, argues for developing different types of interventions and strategies to employ when working with Black families, interventions that can overcome stigma and perceptual barriers to treatment. He noted that those Black youth who did access services reported that they had positive or supportive family networks.
The other broad factor that acts as a barrier to seeking care is the common misinterpretation of presenting symptoms in schools. For example it is well-
established that youth with depression are likely to exhibit irritability, anger, and other kinds of negative behaviors as a manifestation of their depression. Lindsey said that because of implicit bias, a Black student exhibiting those behaviors is more likely to be suspended or expelled from school compared to a White student. In fact, Black students, boys, and children with disabilities are often overrepresented with regard to disproportionate discipline in school (GAO, 2018).
He noted another study showing that school children living in lower socioeconomic areas displayed the highest level of behavioral problems at the end of the month, which was associated with the family running out of Supplemental Nutrition Assistance Program benefits (Gennetian et al., 2016). The same group of investigators found that income instability also predicted student expulsions and suspensions (Gennetian et al., 2015). “Often, it seems to be the case that schools do not do that next level of inquiry about what kind of presenting issues or concerns that kid is bringing to the school, which in this instance is perhaps hunger,” said Lindsey.
One important policy issue, Lindsey explained, has to do with the fact that fewer than 10 states across the nation require social and emotional learning standards from pre-kindergarten through 12th grade. Lindsey said,
I think that it would be incredibly important for kids to understand how to process their emotions, how to reconcile interpersonal challenges that they have with others in a way that allows them to be able to understand their emotional processing, and then perhaps be at a place to ask for help as they need it.
The biggest policy action that could reduce or eliminate a barrier to care, he said, would be for every school to have available mental health care providers at a level proportionate to the number of children in a school. “What we find, particularly in communities of color, is that there is not a provider available at school, or if there is a provider, they are there only 1 day a week,” he noted. This is why Lindsey and his colleagues, as well as members of Congress, have been advocating for the federal government to pay more attention to this issue (Coleman and Congressional Black Caucus, 2019) which led to the U.S. House of Representatives passing the Pursuing Equity in Mental Health Act in May 2021 by a margin of 349 to 74.
SUICIDE PREVENTION: STIGMA AND THE COVID-19 PANDEMIC
Session moderator Erin Bagalman, director of the Division of Behavioral Health Policy in the Office of the Assistant Secretary for Planning and Evaluation at the U.S. Department of Health and Human Services (HHS), opened the panel discussion by asking Willging to comment on suicide prevention in
the context of the COVID-19 pandemic. Willging replied that she and her colleagues surveyed 379 self-identified LGBTQIA+ youth in New Mexico and found that during the pandemic 41 percent did not feel safe in the own homes because of their sexual orientations or gender expression.
In addition, over 83 percent felt sad or hopeless during the summer of 2020, 46 percent considered suicide during those early months of the pandemic, close to 33 percent made a plan for suicide, and 12 percent attempted suicide. She noted that during the pandemic, schools lost track of those kids who might be at risk, which left those youth without a de facto surveillance system. Limited broadband access in New Mexico has aggravated some of the mental health needs for these children and adolescents. “Even finding a private space to engage online with a mental health specialist was challenging for many youth, and we had several reports of youth telling us their parents were actively discouraging them from getting mental health support,” said Willging. Another issue was that schools and teachers were so focused on making adjustments to conducting online instruction during the pandemic that suicide prevention and initiatives to support LGBTQIA+ youth were deprioritized.
Bagalman then asked End of Horn to comment on suicide prevention in the context of the racial tensions and civil unrest demonstrated in 2020 and 2021. End of Horn replied that the Black Lives Matter movement served as a wake-up call for many Native scholars to talk about how colonization, colonialism, and White supremacy have affect tribal nations, not only in terms of racial disparities but in terms of the high mortality and morbidity rates and the high rates of disease burdens. This awakening brought to the forefront the issue of how to contextualize suicide prevention without using colonial language to meet the unique needs of the Native population.
Simonetti noted that the pandemic, racial justice demonstrations, and other recent events have placed different stressors on different households, and people have interpreted these stressors in different ways. He said two primary concerns are the spike of firearm violence in many major cities in the country that has led to a “wholesale sense of urgency,” and the increase in firearm purchases at a time when families have been clustered together under high-stress conditions. One question is whether this period will represent a short-lived change or if firearm ownership has changed for a large proportion of the country.
Brenner commented that she appreciated Lindsey noting that food insecurity and other factors not normally associated with suicide can, in fact, be suicide risk factors. Food insecurity and other financial challenges are risk factors for veterans, she noted, and the COVID-19 pandemic has introduced huge economic stresses into many families that have not experienced them before. It will be important, she said, to monitor how this confluence of stressors will play out over time. Lindsey agreed that it is time to consider
some of the larger contextual factors and the role they play beyond traditional psychiatric symptoms in leading to engagement in suicidal behaviors.
Bagalman asked the panelists for their ideas on how to change the stigma, especially in the Black community, in order to address mental health as an illness rather than from a negative perspective. Lindsey replied with exemplar of a freestanding mental health clinic located in a church-associated facility that provides free services to all. As he noted, faith communities can play a critical role in combating stigma. Another opportunity is to revisit what is happening in schools with regard to so-called zero-tolerance policies and to instead provide the kinds of behavioral health supports that children need, including working with families to provide education about psychological issues. In fact, the whole idea of providing services in nontraditional settings can be used to combat stigma, he said.
Both Whiteside and Brenner commented on the importance of getting health care providers out of their offices to meet people where they are most comfortable receiving services, whether that be in their churches or at the firing range. Brenner noted the importance of getting unlikely partners to engage with the mental health community. Simonetti agreed and said that is happening in the firearm community. “Engaging those stakeholders provides a great opportunity for outreach and to build credibility in communities where we might not necessarily carry with us the most credibility,” said Simonetti.
LEVELS OF PROGRESS TOWARD PREVENTION
Michael Hogan, principal at Hogan Health Solutions, concluded day one of the workshop with some of the key themes he observed throughout the day. “Suicide remains a major issue and despite some trends that may be positive … it remains a major issue and a major cause of unnecessary loss of life,” says Hogan. But he also emphasized the progress that the VA has accomplished within its health care system, and he said it could serve as an example of what could be done in other health care contexts.
Hogan noted some positive changes in the expectations of accrediting organizations, including the Joint Commission and the Commission on Accreditation of Rehabilitation Facilities. However, he said it is time to provide consistent federal funding, such as a block grant rather than a competitive grant, for the Garrett Lee Smith Campus Suicide Prevention Grant Program.
When it comes to caring for people who are actively contemplating suicide, says Hogan, it is clear that connection and collaboration are crucial, that isolation is poisonous, and that directly dealing with thoughts and impulses from suicide is necessary and effective. “It is high time to bring those things, as we have in the VA, across the rest of our health care system,” said Hogan. He noted that the nation is slowly beginning to evolve attitudes about race, and there is slow but remarkable progress with respect to attitudes about gender,
and in understanding that both culture and gender are pivotal when it comes to suicidality.
Hogan concluded by saying that upstream suicide prevention efforts are important, but they are massively under-resourced. “We cannot pretend that we can achieve what needs to be done until we make a change,” he said. The national movement to turn on 9-8-8 as a single emergency phone number next year for people in a mental health crisis can possibly be a turning point, “but it is only a beginning step and we have to do much more, especially upstream.”
BUILDING 9-8-8: AN OPPORTUNITY TO BUILD INCLUSIVE CARE STRUCTURES
Through legislation, 9-8-8 has been designated the new nationwide emergency number to the National Suicide Prevention Lifeline.20 By July 2022, Americans will be able to quickly connect with crisis counselors for easier access to life-saving resources. The second webinar of this workshop considered opportunities to build inclusive care and the implications of the 9-8-8 expansion initiative including the gaps, challenges, and needs for marginalized and vulnerable populations.
Mary Roary, director of the Office of Behavioral Health Equity at SAMHSA, opened the day by acknowledging that every 40 seconds, someone dies by suicide. After 40 seconds of silence in memory of those who have died by suicide, she reiterated the key themes that emerged during the first webinar on June 22, 2021, which were the importance of cultural competency, health equity, and addressing the barriers to suicide prevention, such as the lack of access to health care services and health care provider shortages, that are exacerbated by COVID-19 and the ongoing civil unrest. Roary noted that sustainability needs to be built into planning for suicide prevention programs and that there is a need for an extended research focus that targets traditionally under-resourced and marginalized groups such as American Indians and Alaska Natives, members of the LGBTQIA+ community, Black youth, military veterans, and people who are homeless.
IMPROVING CARE COORDINATION WITHIN CRISIS SERVICES
Mary Ann Nihart, associate director of patient care services and nurse executive for the San Francisco Veterans Affairs Healthcare System, recounted
___________________
20 See https://www.congress.gov/bill/116th-congress/senate-bill/2661/all-info (accessed October 26, 2021).
two tragic incidents that occurred in two communities on the California coast, one was rated one of the 100 safest cities in America. Two young people who were having an acute mental health episode ended up dying at the hands of law enforcement when their parents and siblings called the police asking for help. Christine Goias called 9-1-1 seeking help for her son, Errol Chang, who was in the midst of a psychotic episode at his father’s home. Police and the media arrived shortly after the call and spent 6 hours talking and working with Errol to get him out of the house. Errol’s father disclosed there were weapons in the home and based on an established memorandum of understanding in the county, police were obligated to then call in the Special Weapons and Tactics (SWAT) team. The SWAT team engaged in repetitive communication and pointed weapons at the house and an individual experiencing paranoia. After 6 hours of communicating with the police, Errol was killed by specialized law enforcement agents 20 minutes after the SWAT team arrived. This happens to hundreds of families every year, Nihart stressed. Just 3 months later and 11 miles down the road, an 18-year-old woman with a developmental disability was refusing to take her medications. Her family called the police for help. The encounter with the county sheriff ended in the same result. There is an unsettling acceptance when individuals who have a mental illness and are experiencing a mental health crisis are killed, Nihart said.
In California, Jeannine Loucks, a psychiatric mental health clinical nurse specialist, collaborated with several organizations, she took all of the trainings that police received to prepare for these kinds of emergencies, modify the interventions, and created a series of videos that are now available to every police department in the country through the Orange County Mental Health Association. Nihart’s community was able to acquire a psychological emergency response team that goes out with the police and gives families options on how to deal with their loved ones. “Imagine what could have happened in these two cases if 9-8-8 existed,” said Nihart. “Imagine how we could help so differently, and imagine that this tragedy may not have had to occur at all.”
THE 9-8-8 LIFELINE: POTENTIAL AND IMPLICATIONS FOR CRISIS RESPONSE
The Community Mental Health Services Framework
In communities today, dialing 9-1-1 typically provides one of three options: police, emergency medical services, or fire, but as Anita Everett, director of the Center for Mental Health Services at SAMHSA, explained, 9-1-1 systems for the most part are not setup to respond to mental health emergencies or to provide behavioral health services, even though a large proportion of 9-1-1 calls relate to mental health emergencies. In recognition
of that fact Congress passed the National Suicide Hotline Designation Act of 2020, known colloquially as the 9-8-8 Act. As a result, in 2022, dialing 9-8-8 from any phone line (mobile phone, landline, or Voice over Internet Protocol line), will connect the caller with the National Suicide Prevention Lifeline.
Everett said that SAMHSA’s Center for Mental Health Services, in its efforts to lower the national suicide rate, is working in four main areas. The first is to bring crisis response services into the twenty-first century so the entire mental health system is more responsive to the needs of individuals. Other components of SAMHSA’s community mental health services framework include expanding the Zero Suicide program that was discussed on the first day of the workshop; enhancing suicide management skills among practicing health professionals; and providing more actionable data to local governments and health services organizations.
Regarding the first of those initiatives, Everett said that twenty-first century crisis services have three key components: a call, the mobile response for those who need it, and a place to go or someone to talk to, depending on the situation. Everett focused her discussion on the “someone to talk to” component.
Richard McKeon elaborated on how the 9-8-8 system will work. As Everett mentioned, the 9-8-8 system will build on the structure of the National Suicide Prevention Lifeline, which since 2005 has used the number 1-800-273-TALK (1-800-273-8255). Unlike 9-1-1 calls, 9-8-8 calls will all be directed to this national structure instead of being dispatched locally, said McKeon. Upon reaching 9-8-8, callers will hear a recorded message telling them to “press 1” if they are calling about a veteran or service member, which will then connect them to the veterans crisis line, or “press 2” if they need to be connected to a crisis counselor who is fluent in Spanish. Otherwise, the call will be distributed to one of the 184 local crisis centers located in every one of the 50 states as well as the territory of Guam. If the call is not answered within the first couple of minutes, it will go to a backup center; this is a feature that is not part of that the 9-1-1 system. McKeon added that the lifeline also has a small text chat service.
By July 2022 every phone system will need to make 9-8-8 operational, stated McKeon. Currently, most mobile phone systems have made 9-8-8 operational, but most landline systems have not, and the Federal Communications Commission (FCC) is proposing regulations to enable universal texting to 9-8-8. McKeon emphasized that this is a once-in-a-generation opportunity to improve mental health crisis services in America, both by expanding access to and awareness of connecting to 9-8-8, but also by being able to link to a more coordinated system that can connect people to the appropriate crisis intervention services. As part of this expansion, the Biden administration’s budget released in May 2021 called for quadrupling funding for the National Suicide Prevention Lifeline to $102 million (SAMHSA, 2021).
McKeon added that SAMHSA is also working on the development of a comprehensive roadmap for 9-8-8 implementation, including providing more guidance for crisis centers and the states. The agency is also working to make sure that tribal communities are included and are able to receive the same crisis services. He concluded his remarks by noting that coordination between 9-8-8 and 9-1-1 will be important, as will educating the public about the differences between the two systems and when to call 9-8-8 versus 9-1-1.
Effectiveness of National Crisis Lines
National crisis lines were first highlighted in the 2012 Surgeon General’s report National Strategy for Suicide Prevention: Goals and Objectives for Action (Office of the Surgeon General and National Action Alliance for Suicide Prevention, 2012), and they continued to have a prominent place in 2021 in the Surgeon General’s Call to Action to Implement the National Strategy for Suicide Prevention (U.S. Surgeon General and National Action Alliance for Suicide Prevention, 2021), said Madelyn S. Gould, Irving Phillips Professor of Epidemiology in Psychiatry at the Columbia University Vagelos School of Physicians and Surgeons. However, she added, when the first national strategy was published in 2001, suicide crisis lines were not part of the strategy because the evidence for crisis line effectiveness was considered insufficient at the time.
What did happen in 2001, though, was SAMHSA’s funding of a national network of local certified call centers that eventually became the National Suicide Prevention Lifeline. Equally important, SAMHSA has since funded continuous studies to evaluate the effectiveness of these crisis lines. “What has been unique to these evaluations and the relationship with SAMHSA and the lifeline is that these evaluation findings have been used to shape best practice standards across the network, with implementation of new standards then leading to additional evaluation studies” said Gould.
Prior to the lifeline evaluation, there was a pervasive impression that callers to crisis hotlines were not actually in a suicidal crisis, said Gould, but one of the major findings from 20 years of evaluation was to dispel this myth by demonstrating that individuals who are seriously contemplating suicide do call telephone crisis services (Gould et al., 2018; Kalafat et al., 2007). In addition, what Gould and her collaborators found in their first evaluation was that callers’ suicide risk—the caller’s intent to die, for example—was reduced significantly from the beginning to the end of the call (Gould et al., 2007). “So our original studies did show this reduction in suicide risk during the call,” said Gould. Other evaluations have also found that counselors at lifeline centers are more likely to inquire about current suicidal ideation, recent ideation, and past attempts, and that callers are more likely to experience reduced distress at lifeline centers in comparison to some centers that were not part
of the network. However, there is still room for improvement, less than half of National Suicide Prevention Lifeline centers inquire about recent suicide ideation or suicide attempts, suggesting a persistent problem among suicide (Ramchand et al., 2017).
She and her colleagues then started focusing on callers who were at imminent risk of suicide and found that crisis counselors were able to engage in collaboration with the callers to decide on an intervention in 76.4 percent of at-risk calls (Gould et al., 2016). “When you call the Lifeline, even if you are at an imminent-risk of suicide, the crisis counselors can collaborate,” Gould explained. “They know how to collaborate with someone who is at imminent risk.” For 19.1 percent of calls, the counselors did have to send emergency services, but they did so in collaboration with the caller (Gould et al., 2016). In 24.3 percent of imminent risk calls, she added, the counselors did have to send emergency services without the caller’s collaboration (Gould et al., 2016), so overall, about 43 percent of imminent risk calls involve emergency services. In the collaborative interventions not involving emergency services, collaboration entailed involving a third party—a friend or family member—to eliminate access to lethal means (Gould et al., 2016).
Evaluation studies focused on types of interventions that can be carried out with third-party callers to protect the people who are at imminent risk. Such studies have shown that crisis counselors are able to provide a large range of interventions that can supplement, and at times replace, replace calling 9-1-1 (Gould et al., 2021b). Gould and her team have also done evaluation studies showing that follow-up calls from the crisis center do reduce suicidal individuals’ perceived risk of future suicidal behavior (Gould et al., 2018).
To increase access to crisis services, lifeline services now have evolved to include not only telephone access but also crisis chat capability. Her team’s evaluation of crisis chat functions found that almost 84 percent of people who chat report either current or recent suicidal ideation on a pre-chat survey, which is markedly higher than the estimated 23 percent of lifeline callers who are experiencing suicidal behavior on the day of or the day before their call (Gould et al., 2021a). Two-thirds of those individuals who used the chat function reported that the chat was helpful and that they were significantly and substantially less distressed at the end of the chat intervention than they were at the beginning, said Gould.
She said the time is now ripe for 9-8-8 because of the positive results of these evaluations. Gould also offered a number of suggested evaluations of the 9-8-8 system going forward. The questions to address include:
- To what extent is imminent risk reduced during the course of the crisis intervention without needing additional services?
- How often are 9-1-1 or police called by Lifeline crisis centers?
- How often are mobile crisis teams and stabilization units used?
- To what extent is information shared among Lifeline crisis centers, 9-1-1, emergency departments, and other crisis and emergency services?
- What outcomes emerge after different types of dispatch and information sharing?
- Do dispatch and outcomes vary for different ethnic, racial, and gender groups?
Veterans Crisis Line 9-8-8 Expansion Initiative and Implications
Lisa Kearney, director of the Veterans Crisis Line at the VA, spoke about the crisis line’s current call volume and how the VA is preparing for the national rollout of the 9-8-8 system, particularly with regard to what happens after the call, text, or chat. The crisis line, she said, has fielded more than 5.4 million calls and 204,000 texts, engaged in more than 630,000 chats, and made more than 975,000 referrals since it opened in 2007. In fiscal year 2021, the crisis line has been answering around 2,000 calls per day, making more than 400 referrals per day on average, and dispatching emergency services just over 96 times per day on average. Compared to fiscal year 2020, average daily referrals and emergency dispatch calls are up by 14.6 percent and 20.0 percent, respectively.
VA has started two initiatives that align with preparing for 9-8-8. The Caring Letters initiative, said Kearney, is an evidence-based intervention for suicide prevention in which individuals who are in crisis have a follow-up letter sent at intervals to connect them with resources and provide them information about support they can receive (Reger et al., 2019). This program has been shown to help reduce the rate of suicide death, attempts, and ideation, and it has been added to the VA/U.S. Department of Defense clinical practice guidelines for addressing suicide risk. The Caring Letters initiative is now focused on expanding critical crisis intervention work to help veterans continue to feel supported and engaged, and the goal is to reach more than 90,000 veterans annually with nine letters over the course of a year after their call to the crisis line. Launched in June 2020, the crisis line has mailed more than 530,000 caring letters to more than 100,000 veterans. The VA is currently evaluating how effective this new program is at reducing suicide deaths, attempts, and ideation among veterans.
The second initiative, which the VA launched in June 2021, is the Peer Support Outreach whose mission is to provide support, hope, and recovery-oriented services to veterans who are identified as at increased risk for suicide. Kearney explained that this program provides care via phone and text messaging services to veterans who originally called the crisis line. VA peer specialists, who are veterans in recovery, staff the call center with supervision by licensed
independent care providers. The goal is to support the veteran while he or she engages in follow-up care, either in the community or within the VA health system. “This is not just about getting people help within the moment of crisis, but getting them care, resources, and support afterwards to help them engage in follow-up,” said Kearney.
Ongoing evaluation at the Peer Support Outreach Call Center has shown a 5-fold reduction in distress for callers at the end of the call than at the beginning, and callers are more likely to have less suicidal ideation at end of the call than the beginning. Callers were 91 percent less likely to have suicidal urgency at the end of the call compared to at the beginning, and 83 percent of callers reported feeling better following their call (Rasmussen et al., 2017). In addition, said Kearney, veterans were more likely to engage in care after receiving a responder referral (Britton et al., 2013).
Regarding the expected effects of the 9-8-8 rollout, Kearney said that the increased ease of accessing services should lead to increased call volumes and an increased need for collaboration and coordination after the call with services both internal and external to the VA. At a minimum, 9-8-8 has the potential to serve as a single point of entry into the care system for veterans, service members, and their families. She noted that the VA is preparing to expand its clinical operations and is currently increasing its quality assurance monitoring and beefing up its information technology infrastructure. In short, the VA expects 9-8-8 to increase access to the full continuum of care; this is driving the VA to consider how to shape and direct demand for mental health services to maximize capacity. As a final comment, she reminded everyone that while some carriers have already implemented 9-8-8, many have not, and individuals who subscribe to carriers that have not yet implemented it should still call 1-800-273-8255 and press 1 to reach the veterans crisis line, connect to chat at https://www.veteranscrisisline.net/get-help/chat, or connect via text at 838-255. These will remain active even after full activation of 9-8-8.
9-8-8 ROLLOUT: PRIVACY, CONFIDENTIALITY, AND EQUITY CONSIDERATIONS
The 9-8-8 Workforce and Culturally and Linguistically Appropriate Services
Sue Ann O’Brien, chief executive officer at Behavioral Health Link, said the advent of 9-8-8 will be transformational in helping people who are in a behavioral health crisis and getting them connected to care. Behavioral Health Link, she explained, operates Georgia’s crisis and access line, which at the time
of the workshop was on track to answer more than 250,000 calls in 2021, as well as texts and chats.
O’Brien noted that the key to success with the 9-8-8 rollout will be providing callers with access to the full continuum of care so they receive the care that is right for them. “The predictions are that the call volume will drastically increase with the ease of the three-digit number, and that is a great thing in terms of accessibility and [it is hoped] decreased stigma, but we will have to have those other services in place,” she said. She added that if the full range of options is not available, the result will be a continued overreliance on 9-1-1, with individuals ending up in jail, the emergency department, or the morgue. “These adverse outcomes are exponentially more likely for people of color,” said O’Brien.
Ensuring a sufficient workforce to meet the expected increase in demand will be an essential component for providing access to the full spectrum of care, and building that workforce cannot rely solely on licensed clinicians because they are already in short supply. Moreover, the majority of the behavioral health workforce in the United States is approximately 85 percent White according to some estimates, while the number of non-White residents is approaching half of the U.S. population, with about 57 million people speaking a language other than English in their homes. These demographics got O’Brien thinking about the National Standards for Culturally and Linguistically Appropriate Services (CLAS) that HHS released in 2000 and updated in 2013. The National Standards for CLAS, she reminded the audience, are a set of 15 recommendations for health care agencies that was intended to advance health equity and to eliminate health care disparities in health care organizations.
One of the recommendations is to have a workforce that proportionately represents the population being served (HHS, 2013), which O’Brien said is an issue that many organizations, including hers, have been looking at, especially with the recent and ongoing civil unrest and attention to racial injustice. In Atlanta, where Blacks account for 51 percent of the population, her call center workforce is 77 percent Black. However, the population outside of Atlanta is more than 60 percent White, which can make it difficult for callers to connect with trained call center staff because of cultural and life experience differences as well, she said. “I think what is needed is more of an emphasis on cultural humility,” said O’Brien, who defined cultural humility as the ability to maintain an interpersonal stance that is open to the aspects of cultural identity most important to the person. “If we cannot bridge that divide, it might indeed be a matter of life and death,” she said. “It is imperative that we leverage a well-trained, diverse, and even nonclinical workforce, including peer support specialists, if we are truly going to address the equity issue head-on.”
PATIENT-CENTERED CARE CONSIDERATIONS IN CRISIS SERVICES FOR AMERICAN INDIAN/ALASKA NATIVE PEOPLE
The IHS provides health care to 2.2 million American Indians and Alaska Natives living in 37 states, including Alaska, with an intentional focus on the culture of each of the more than 500 unique tribal communities with which IHS works, said End of Horn. IHS approaches equity within health care—providing needed health care, when it is needed, and how it is needed—from a perspective of humanization in health care. What this entails, said End of Horn, is the use of a person-centered approach that asserts the intrinsic dignity of all human beings through the adoption of core values that include honesty and integrity, caring compassion, altruism, empathy, and respect for others (Velasco Bueno and La Calle, 2020).
Patient-centered care, explained End of Horn, focuses on accepting, assessing, and identifying patients from their perspective, as well as understanding what the patient needs and empowering them to go where they want to go to address their needs (Cheraghi et al., 2017). Factors that play a role in implementing patient-centered care include open visitation policies; communication; a focus on the well-being of the patient; having the presence and participation of relatives; care for the health care professional; prevention, management and monitoring; having humanized architecture and infrastructure, and providing appropriate end-of-life care (Velasco Bueno and La Calle, 2020).
In many tribal communities, the act of sharing stories is seen as medicine, said End of Horn. Patient-centered care in that context requires the health care provider to listen to the individual as they share what is happening to them and what they are experiencing; this can involve a translator for those individuals who feel more comfortable telling their story in their native language. “Including family, communication, relationship building, being open to cultural influences, and providing traditional treatment options allows Western medicine to meet the needs of Native people,” she said (Sylliboy and Hovey, 2020).
Providing culturally humble, aware, and appropriate care comes down to building capacity, said End of Horn. Building capacity, she explained, is a fundamental component to the community-level development of outcomes that use the community’s resources to address problems and issues. Building capacity requires including strong representation of the Native community in creating community-based interventions and education and developing networks throughout the community (Smith-Morris and Epstein, 2014). Intensive outreach, as well as implementing services in equal partnership with the community, are essential for success, she emphasized.
BUILDING EQUITY INTO THE FRONT END OF 9-8-8
Victor Armstrong, director of the Division of Mental Health, Developmental Disabilities, and Substance Abuse Services in the North Carolina Department of Health and Human Services, said the 9-8-8 rollout is a tremendous opportunity to create a system where equity is the foundation rather than an afterthought. He noted equity is not just about race, culture, and ethnicity. Armstrong said,
The lens of equity is about the intersectionality of race, culture, and ethnicity, in addition to living with mental health challenges. It is about being Black and living with a serious mental illness. It is about being Latino and living with intellectual disability resulting from traumatic brain injury. It is about being Native American and living with a substance use disorder. It is about being an Asian trans-person struggling with an anxiety disorder exacerbated by the discrimination that often accompanies mental illness, the hatred that is perpetrated toward trans Americans, and the increasing rates of violence toward Asian Americans.
Armstrong contends that the very construct of the current U.S. mental health care system is flawed, beginning with its response to individuals experiencing mental health emergencies. The current system, he said, was not built from the perspective of individuals with lived health experiences, nor was it designed to address their mental health needs. “I would argue that our current system is not designed to protect and nurture the individual experiencing the mental health emergency, but to protect the rest of us from the individual experiencing the mental health emergency, and that is wrong,” said Armstrong. “The introduction of 9-8-8 will provide us an opportunity to mitigate those challenges and to correct that wrong.” Because many people of color do not have access to outpatient services or crisis services in the communities where they live, their introduction to the mental health care system often ends up being in the back of a police car or in an acute care emergency department when they are in a state of crisis, and “that is not conducive to good clinical outcomes, nor is it likely to foster a positive relationship with the mental health system,” said Armstrong. Research indicates that Black adults more likely to report psychological stressors than their White counterparts (SAMHSA, 2020; Williams, 2018), but they are less likely to enter treatment and more likely to terminate treatment prematurely (Williams, 2018), said Armstrong.
He explained that suicide itself is not a disease, but rather the worst possible outcome of a combination of many complex factors. That being the case, there are opportunities to intervene with person-centered approaches before a person reaches the point of suicidality. Suicide prevention, however, should be about more than detaining someone when they are in crisis. Assessing risk
at the individual level or the community level, said Armstrong, involves considering not only risk factors but also protective factors.
In addition, without understanding or acknowledging the effect of cultural beliefs, including stigma; the relationships with law enforcement; or the effect of structural racism on an individual’s life and their perception of their place in America, an intervention may become another traumatic experience that the individual will have to carry. On the other hand, he added, building cultural humility in the system via 9-8-8 will increase the likelihood that individuals receive care in their communities and that they receive care that accounts for the intersectionality of race, ethnicity, culture, and sexual identity.
Systemic racism and bias, both explicit and implicit, are multilayered and seep into every crevice of society, including law enforcement, schools, and health care, and the mental health system is not immune, said Armstrong, adding,
But we know that inequity exists, and it is our moral responsibility to address those inequities by leaning into equity in every decision that we make as clinicians, policy makers, or simply as change agents. Either lean into creating a more equitable system or perpetuate inequity.
Armstrong pointed out that according to the Washington Post Police Shooting Database, 6,697 people have been shot and killed by a police officer in the line of duty since January 1, 2015. Nearly one-fourth were Black and almost 97 percent of those were Black males (The Washington Post, 2021). People in mental health crisis are at high risk of death during a police interaction, with 23 percent of people killed by police identified as having a mental illness. He cited those figures not to impugn officers but to suggest that there is a flaw in the system, one that puts Black individuals who are having a mental health crisis, whether a psychotic episode or suicidality, at high risk of a negative outcome.
However, 9-8-8 can be the spark that dismantles racism in a mental health response system and become a building block in creating a system that is more equitable, said Armstrong. It can do so by supporting the creation of more mental health resources in communities of color and underserved communities. Those resources, he noted, can include mobile crisis care, facility-based crisis care, peer respite, and others designed to divert individuals away from emergency departments and jails. Armstrong said,
We can create more community-based resources that provide access to upstream treatment rather than continuing in the crisis response mode that we have existed in for the past several decades, and we can seize the opportunity to build a workforce that mirrors the populations served.
While Blacks comprise roughly 13 percent of America’s population, only about 4 percent of American psychologists are Black, and only about 2 percent of America’s psychiatrists are Black, Armstrong noted.
There is a ready-made but under used workforce of individuals from a broad range of racial, ethnic, and cultural groups with lived mental health experience, said Armstrong. In North Carolina, there are approximately 4,000 trained peer specialists, though only some 1,600 are gainfully employed. “We need to utilize the peer workforce, pay them a living wage, and build them into our crisis continuum to respond to individuals experiencing mental health emergencies at a time when they most need someone who understands their immediate challenges,” adding
We can increase the percent of historically marginalized populations receiving behavioral health services by building and earning trust between historically marginalized communities, behavioral health care providers, and funders as we bring them to the table in planning our 9-8-8 model.
It is possible, he stated, to reimagine the nation’s approach to mental health and build an equitable mental health care system. The challenge is to seize the opportunity afforded by the 9-8-8 rollout to work with community partners and community media to:
- create grassroots messaging to educate communities, combat stigma, and address concerns about receiving mental health treatment;
- use expertise and care providers of color who have traditionally served historically marginalized communities, often without access to government grants and contracts; and
- engage them in the planning, giving voice to those with lived experience.
Indeed, without paying attention to the intersectionality of clinical expertise and the voice of historically marginalized individuals, any approach will be ill advised, ill informed, and ill fated, said Armstrong. Listening only to the opinions of intellectuals, the desires of legislators, and the needs of the majority would create a system that might work for 80 percent of the U.S. population but not address the needs of 80 percent of the Black, Latinx, or Native American population, he added. “If you have not lived the life experience of those you seek to assist and do not have decision makers with that life experience at the table, you cannot fully understand the challenges and address the need, no matter how well intentioned you may be,” said Armstrong.
Historically marginalized communities, whether marginalized because of race, ethnicity, or diagnosis, are not looking to be rescued, nor are they looking for a handout, he noted. Rather, historically marginalized communities are looking for a collaborative partner who will value their expertise and life experience. “Those living with mental health challenges, those struggling with addictions, and those living with intellectual disabilities or traumatic
brain injuries are themselves a historically marginalized population, and they are looking for an opportunity to have their voices be heard” said Armstrong.
In closing, Armstrong reiterated that implementing the 9-8-8 system creates an opportunity to build a more equitable and responsive system, one that is not only evidence based and evidence informed but informed by the community and individuals’ lived experiences. “My life experience tells me that if we do not build equity into 9-8-8 on the front end, the most powerless and vulnerable among us will not receive equity, justice, or access to the mental health resources they need and deserve,” he said.
BUILDING CULTURAL COMPETENCE WITHIN CRISIS SERVICES
A Potential Framework for Developing Culturally Responsive and Personalized Evidence-Based Mental Health Interventions for Culturally Diverse Populations
May Yeh, associate professor of psychology at San Diego State University, described the PersIn Approach to developing personalized, evidence-based interventions for culturally diverse populations (McCabe et al., 2020). This approach entails three steps. The first step is the identification of factors and dimensions upon which personalization for culturally diverse populations might need to occur. This is a critical step, said Yeh, because individual health care providers may not be aware of the different cultural dimensions that might affect care for any given person. In their work, she and colleagues accomplished this step by finding factors or dimensions that have published research showing a relationship to clinically meaningful outcomes, have variability across cultural groups, and can be addressed through personalization.
In the case of suicide prevention, clinically meaningful outcomes might relate to service use, engagement with the intervention, or a reduction in suicide-related ideation or behavior. The types of cultural factors that may be relevant, said Yeh, may vary based upon the clinically relevant outcome. For example, when considering barriers to using mental health services, stigma may be a stronger barrier in certain cultural groups, while mistrust of care providers or lack of access—or knowledge of—services may be a more important barrier for another.
She also noted that when assessing risk and protective factors for suicidal behavior, Joyce Chu and colleagues indicate that it may be important to account for cultural factors such as family conflict, social discord, acculturative stress, minority stress, cultural sanctions related to suicide, and idioms of distress (Chu et al., 2020). Ascertaining clinically and culturally relevant dimen-
sions may require further research, literature review, and consultation with experts, community members, and leaders or other stakeholders, added Yeh.
The second step of the PersIn framework focuses on finding ways to briefly assess the components identified in the first step, recognizing that that groups are heterogeneous. It may be, for example, that certain factors are more salient for some individuals within a group or may apply to others outside of that group. In addition, people may affiliate with more than one cultural group. “Developing assessments for the specific dimensions or factors allows us to broaden the ability of the intervention to respond to different groups while also individualizing the treatment protocol to the specific person,” said Yeh. Results of this brief assessment, she explained, gives care providers a sense of the factors that may be especially important to address with a particular individual before they begin the intervention.
In the third step, tools or modifications are developed to address the dimensions or factors identified in the first step. For example, one tool might be developed to address a potential risk factor of family conflict, while another tool may be constructed to address minority-related stress. As she explained, developing these tools for the array of possibilities gives care providers a toolbox containing what they may need to address important factors. There is also a need to train care providers in effective use of these tools.
Once the personalized intervention is developed, it is used as follows: the brief assessment can be given before the intervention begins, and the tools or modifications are triggered and then implemented to personalize intervention. The goal, said Yeh, is to provide a culturally responsive intervention that takes into account important cultural dimensions while making it possible to standardize the use of the tools and personalize the intervention to an individual when implemented.
BEYOND CULTURAL COMPETENCY
Culture is a value-laden term, with values themselves being a reflection of culture, said End of Horn. She noted that anthropologically, there is no set definition of culture, but there are three aspects to the concept: a group of people who “belong together” by value of some shared features, a systemic organizer of psychological systems of individual persons, and how the person and environment are interrelated (Valsiner, 2003). In other words, culture is not just systemic beliefs, practices, or knowledge, but rather culture is what belongs to a group of people and to what those people belong. This conceptualization of culture says not to lump all American Indians and Alaska Natives into one group because that takes away from the individuality and uniqueness of each tribal nation, said End of Horn.
Cultural competency is not a clinical skill, said End of Horn. Rather, it is an opportunity for individuals to learn about local customs and local perspectives, to build networks, and to incorporate those elements and aspects into the care that is provided and allow the care to be responsive to the community needs and political patterns, especially when talking about tribal nations. Tribal nations change often with regard to administration and political pattern, she said, and so providing services that are understanding of that and responsive to that will go to where the patient is, deliver what they need, and provide equitable health care (Smith-Morris and Epstein, 2014). “I cannot stress this enough: you have to go to the community and become part of that community in order to provide services,” said End of Horn, adding
This is not something that the community should be coming to you for. You should be going to the community, inviting them in, building bridges, and working to understand their reality and then incorporating that within the services that you’re providing, because no one person is going to be able to provide that.
In closing, emphasized that she is just one person from just one of the 500 federally recognized tribes and 100 more state-recognized tribes, each of which has different realities. “So please consider going beyond cultural competency and see it as an opportunity,” said End of Horn.
WORKING IN DIVERSE COMMUNITIES
Jennifer Battle, director of access with the Harris Center for Mental Health and Intellectual/Developmental Disabilities, began her comments by saying that she wishes she could have specific training for every single community represented, not just in Harris County but the entire state of Texas, but the likelihood of that happening is slim. As a result, the focus on cultural humility is key if the 9-8-8 call centers are going to be able to work collaboratively with the numerous communities throughout the state and be able to connect callers with support in their specific community.
Harris County, home to Houston, has almost 5 million people, with 69 percent of the residents identifying as coming from a community of color. More than 145 languages are spoken, and almost half of the county’s residents either speak a language other than English or are bilingual. “That’s exciting as a community but terrifying from a call center perspective,” said Battle.
One topic of discussion regarding health equity has been around how to handle calls from a non-native English speaker and where the responsibility of the 9-8-8 system morphs into the community’s responsibility to provide language assistance. The discussions have also raised the possibility of training the people who provide translation services to serve in the call centers because
they may not have expertise or understanding around mental health issues or suicide prevention.
Battle encouraged audience members who are not involved in their 9-8-8 planning grant process to reach out to their local crisis centers so they can find out what is going on and see if there is anything they can do to lend their expertise and voice to that process, especially if their work has a strong equity focus. She then noted that conversations at the state level have focused on suicide prevention as a form of social justice work, saying
The more that we can create a life worth living for people, the more that people are going to reach out for the care that they need when they need it, and hopefully trust us enough to be able to be the folks that they reach out to.
As a final comment, she reiterated the call to involve local communities in whatever plans are being made, as well as to reach out to local call centers and support them however possible.
LATINX YOUTH AND THE UNDOCUMENTED
Thomas Chávez, associate professor in counseling psychology at the University of New Mexico, noted that the Latinx population is the second largest racial or ethnic group in the United States, representing about 60.6 million people, 80 percent of whom are U.S. citizens. The Latinx community includes many diverse groups, with most immigrants coming from Colombia, Guatemala, and Honduras, followed by El Salvador, Cuba, and the Dominican Republic. The smallest immigrant Latinx group comes from Mexico, he added.
One theory about Latinx well-being centers on acculturation, where the longer an immigrant stays and aligns with U.S. values and health systems, the poorer their health outcomes are. Chávez said the measure of acculturation should take into consideration affective, cognitive, and behavioral dimensions to understand its effect on health. It is also important, he said, to consider the sociological systems that affect well-being, such as whether the individual came to the United States as a child or whether they migrated as an adolescent or young adult. Another contextual feature is the diversity of the destination culture; migrating to an area with less diversity makes it more likely that the individual will experience stress. In particular, Chávez explained, there are two types of acculturative stress, including the pressure to assimilate as well as stress resulting from discrimination. Youth also experience the complex developmental stressors typical for adolescence, as well as bullying that often coincides with anti-immigrant sentiments that may be present in a particular region. Such stresses may contribute to internalizing and externalizing behaviors.
Chávez said there are lower rates of death by suicide in the Latinx population compared to other ethnic and racial groups (Ramchand et al., 2021),
though Latino youth are more likely to report suicidal ideation and attempts than their non-Hispanic peers (Limas and Vaughn, 2018; Silva and Van Orden, 2018). Latina groups report elevated rates of experiencing violence and oppression related to their gender, particularly in regard to cultural expressions that are in discord with their acculturation (Zayas and Pilat, 2008), said Chávez. In fact, Latina adolescents are more likely to attempt suicide when they have poor psychosocial functioning and family crisis. Suicide rates among LGBTQIA+ Latinx youth are also elevated even after accounting for depression and substance use (Boyas et al., 2019).
Understanding the Latinx population has been limited to theoretical perspectives and has not considered their unique experiences, said Chávez. Critical race theory, a methodology for helping investigators maintain consciousness of racialized constructs and historical sociopolitical mechanisms, can help investigators and practitioners understand such experiences (Ford and Airhihenbuwa, 2010).
LatCrit, or Latino critical theory, allows investigators to examine how multiple forms of oppression can intersect with the lives of people of color and how interactions manifest in day-to-day experiences unique to the Latinx community, such as immigration status, language, ethnicity, and culture (Bernal, 2002). Another useful theory, UndocuCrit or Undocumented critical theory, offers a critical approach for analyzing how racist immigrant practices, policies, and rhetoric function to spread fear among populations of undocumented immigrants (Aguilar, 2018).
For example, his team has used critical race theory to inform a study in which they found that Latinx young adults and their families avoided health care institutions for fear of being reported to immigration officials and were constantly stressed because of financial and emotional issues connected to the lack of health insurance and having to pay for care out of pocket. This population, he noted, largely depends on community health clinics for all their health care needs and only seek emergency services when faced with a life or death situation. This study also identified risk factors for suicidal behaviors that included exposure to violence and trauma, acculturation of absent family systems, social and linguistic isolation, economic stress, and family conflict. Protective factors included the values of familism, personalism, and respect; parental interventions, highlighting and promoting biculturalism and bilingualism, and expanding social networks (Chávez et al., 2021).
Chávez suggested focusing suicide prevention efforts on social media campaigns to reduce stigma of mental health and substance use disorders and to promote safety, as well as enforcing nondiscrimination laws, guaranteeing universal coverage for all youth, implementing trauma-informed policies, keeping families together, and promoting community resiliency. He emphasized the
need to promote mental health from a young age and to include antibullying training. In addition, he noted the importance of evidence-based practices for Latinx behavioral health and the creation of partnerships among family, community, and schools to promote resilience and heal trauma.
BUILDING CULTURAL COMPETENCE WITHIN CRISIS SERVICES
Xinzhi Zhang, chief of health inequities and the global health branch of the National Heart, Lung, and Blood Institute, noted that suicide is the leading cause of death among Asian American adolescents (Murphy et al., 2021). A number of factors are contributing to this rise, said Zhang, including family conflict, intergenerational differences, lack of English proficiency, self-image and identity issues, bullying, discrimination because of Asian names, and academic pressures.
To counter these factors, the U.S. Public Health Service, SAMHSA, the National Institute on Minority Health and Health Disparities, and the Asian American Health Initiative in Montgomery County, Maryland, started a Healthy Mind Initiative that is reaching out to different Asian communities to increase awareness and promote suicide prevention among Asian adolescents. This initiative relies on individuals from the various communities who speak the language and understand the specific culture. He noted that getting that type of community engagement involvement will be critical for implementing 9-8-8 initiatives.
Zhang concluded his comments with an example of the type of program that has come out of this initiative. In 2019, students 16 to 18 years old competed in a national essay contest to speak up about mental health (NIMH, 2021). The “This is My Story” competition received more than 200 essays from 34 states and Puerto Rico, with 10 receiving awards and 2 receiving honorable mentions. A second competition is in the works, said Zhang.
9-8-8, HEALTH EQUITY, AND FAITH WITHIN THE BLACK COMMUNITY
Brandon Johnson, public health advisor to SAMHSA’s Center for Mental Health Services, discussed how 9-8-8 can be used to improve outcomes for Black youth, who have twice the suicide rate of White youth and among whom those rates have been increasing at an alarming rate, as Lindsey discussed during the first webinar. The rollout of the 9-8-8 system, said Johnson, could address health equity issues by increasing access to mobile crisis teams for Black families, which in turn could save lives by avoiding engagement with
law enforcement. He noted, too, that local crisis centers often have information on local mental health resources and community supports. Connecting Black and Brown families with culturally appropriate resources increases the likelihood for engagement and would benefit youth specifically if equipped with resources designed to meet their needs.
It is important as well to remember the family. “As we talk about young Black children between the ages of 5 and 12, we are talking about a family unit,” said Johnson, adding,
Often, it will be the parents reaching out to 9-8-8 asking for resources, wanting to know what they can do for their youth, and as we know, there has been structural racism and systemic racism that has made it more difficult for Black families to thrive.
It is also critical to have resources dedicated to the specific social determinants of health that make it more difficult for a family to access various services. There is also the need to have resources for LGBTQIA+ youth, youth who are experiencing homelessness, those in foster care, and others.
Johnson said that 9-8-8 creates the opportunity to address the specific needs of various populations, to use the available data, and create resources that are timely and relevant. Moreover, by emphasizing cultural humility, it should be possible to understand those aspects of the lived experience that may be driving suicidal behavior but may not have been accounted for and attended to in the past.
As co-leader of the Faith Communities Task Force, which leads the National Action Alliance for Suicide Prevention’s efforts to engage faith communities in suicide prevention, Johnson said that a focus on faith communities can:
- help integrate and coordinate suicide prevention activities across multiple sectors and settings,
- increase knowledge about the factors that offer protection from suicidal behaviors and that promote wellness and recovery, and
- provide care and support to individuals affected by suicide deaths and attempts to promote healing and implement community strategies to help prevent further suicides.
Involving faith communities in suicide prevention efforts can also help people get connected to services and coordinate their care, as well as help educate individuals about mental health and how it can affect them. “As we engage with faith communities, we understand that the communities oftentimes are already doing this type of work in promoting hope and healing, as well as making linkages to services and instilling in individuals an increased sense of purpose,” said Johnson.
As 9-8-8 rolls out, he said it will be important to reach out to faith leaders, engage with them, and help them understand the potential benefits it can bring to their communities so they can in turn convey that information to their communities. Engaging faith communities in these conversations can normalize the conversation about mental health and remove some of the stigma around accessing mental health services.
Toward that end, Johnson and his colleagues will be working with faith communities to help them if they want to develop specific dissemination materials for the rollout of 9-8-8. He noted that the faith communities he has engaged with are eager to be helpful and want to know how to best support individuals to lead their best lives possible. The task force is also creating dialogs and holding informational sessions and webinars with faith leaders across the country to answer questions and be available for individuals to ask what they can do to help.
A HISTORIC FIRST: SPECIALIZED SERVICES IN 9-8-8 FOR LGBTQIA+ YOUTH
LGBTQIA+ youth are at high risk of suicidal ideation, said Sam Brinton (they/them), vice president of advocacy and government affairs at the Trevor Project. Data collected by the National Survey on LGBTQIA+ Youth Mental Health show that 42 percent of LGBTQIA+ youth overall seriously considered suicide in the past year, but Brinton noted that there were differences in suicide risk among different populations of LGBTQIA+ youth. While 12 percent of White LGBTQIA+ youth attempted suicide, 31 percent of Native and Indigenous LGBTQIA+ youth, 21 percent of Black and multiracial LGBTQIA+ youth, and 18 percent of Latinx LGBTQIA+ youth attempted suicide in the past year.
Brinton also noted that 94 percent of LGBTQIA+ youth said that recent policies had negatively affected their mental health. But Brinton said 9-8-8 is a tremendous advance because the legislation requires an implementation plan for what are called “specialized services” for high-risk populations, including LGBTQIA+ youth, as well as minority and rural populations. Brinton also noted that when the legislation passed both houses of Congress by unanimous vote, it was the first and only time an LGBTQIA+-inclusive bill passed without a single no vote.
ENSURING 9-8-8 SERVES ALL
Tracie Schneider, Deaf Services Coordinator for the Arkansas Department of Health and Human Services, said the 9-8-8 initiative will neither be truly inclusive nor fully accessible unless text message and direct video call acceptance capabilities are integrated into the rollout. Currently, she said, people
with disabilities have to deal with multiple phone numbers—a text number, a teletypewriter (TTY) number, a speech-to-speech number, and others—to reach crisis services, so one important goal of the 9-8-8 rollout is to make sure that everyone has only one number to remember and that it responds to text or video calls without any extra steps.
As it is now envisioned, a Deaf person who primarily uses American Sign Language (ASL) would have to access the 9-8-8 crisis line through what is called a video relay service, which uses either standalone equipment or smartphone/desktop apps to place a call using an interpreter over a broadband connection. “If I am trying to call 9-8-8, I have to facilitate that through an interpreter because texting to 9-8-8 is not available,” said Schneider. The same is true, she said, for direct video calling that would automatically direct the call to someone who knows ASL. Not only would direct video call acceptance be linguistically affirming, but it would also be culturally appropriate as well, she noted.
INCLUDING SCHOOLS IN THE CRISIS RESPONSE SYSTEM
Sharon Hoover, professor and co-director of the National Center for School Mental Health at the University of Maryland School of Medicine, said it is imperative for the nation to build a universal system for behavioral health promotion and early identification and intervention to minimize crises while simultaneously addressing the failings of the current crisis response system for children. Such a system for children should include schools because one of the most central tenets to creative, accessible, and equitable systems of crisis care and behavioral health care is to meet people where they are.
Hoover noted that an increasing number of schools are installing what many are referring to as comprehensive school mental health systems, which are partnerships between the education and behavioral health sectors to support a full continuum of mental health supports and services, including mental health promotion and treatment. These comprehensive school mental health systems, she explained, provide a full array of supports that can include promoting positive mental health for all students, providing prevention interventions for those students who are most at risk for developing mental health conditions or mental health challenges, and providing early intervention services for those students who may screen positive for mental health concerns. She added that when treatment is provided in school settings, young people are far more likely to not only be identified early but to initiate and complete care.
The new National Center for Safe Supportive Schools,21 funded by SAMHSA, focuses on three areas: developing comprehensive school mental
___________________
21 Additional information is available at https://www.ncs3.org (accessed November 5, 2021).
health systems, implementing culturally responsive and equitable policies, and supporting trauma-informed, healing-centered practices.
Hoover said,
It is increasingly evident to educators and to the mental health field that for all students to feel safe and supported in schools and to support their behavioral health and well-being, we must not only put mental health supports and services in place, but also ensure that all of our approaches are culturally responsive, antiracist, and equitable, and that they are delivered through a trauma-informed and healing-centered approach.
An essential component of comprehensive school mental health systems is crisis prevention and response. In fact, said Hoover, implementing comprehensive, multitiered systems of mental health support in schools has been demonstrated to reduce emotional and behavioral health crises (Bohnenkamp et al., 2021; Kase et al., 2017; SAMHSA and CMS, 2019; Stephan et al., 2015). Her team, for example, recently finished a 5-year implementation and study of crisis prevention and response that included peer training for students from various social groups in each school who were trained in conflict management and bullying prevention, as well as online virtual simulation technology to train teachers on how to support students experiencing psychological distress, as well as clear referral, assessment, and coordination processes and a structured process for post-crisis prevention. Positive outcomes from this program included 56 percent fewer suspensions in the intervention schools, 76 percent fewer office referrals, and more on-site crisis response as opposed to off-site referrals to emergency departments or law enforcement (Bohnenkamp et al., 2021). As a final comment, she urged everyone to keep children, adolescents, and young adults in mind as the nation rolls out its 9-8-8 system.
DISCUSSION: HEALTH EQUITY AND 9-8-8
Pearson posed a question from the audience asking if calls to 9-8-8 are actually free and if it is accessible to people in Canada. McKeon replied that all calls to 9-8-8 are toll free, with the cost absorbed by SAMHSA’s lifeline grant program. Geographically, 9-8-8 will be accessible across all 50 states and all U.S. territories, but not in Canada. The Public Health Agency of Canada and the Mental Health Commission of Canada have been in contact with SAMHSA with regard to developing a similar system for Canada. Pearson noted that the U.S. 9-8-8 system is modeled after the United Kingdom’s system, and McKeon added that some—North Dakota, Connecticut, Maryland, Colorado, and Georgia—have their own three-digit crisis lines in operation. Presumably, those will continue to operate, but discussions about what will happen to those systems going forward are important, says McKeon.
Pearson commented that while it is important to have these crisis services in place, the best outcome would be to have fewer crises. She then asked the panelists for their suggestions regarding upstream interventions. McKeon responded that there needs to be an increased awareness that intervening with someone in crisis is different from what needs to be done to prevent someone from becoming suicidal in the first place. In his view, there are three levels of intervention strategies: those that can help prevent people from becoming suicidal, those that can prevent individuals who are having suicidal thoughts from progressing to an acute suicidal crisis, and those such as 9-8-8 that can help someone at imminent risk.
Brinton said that the message needs to be promoted by encouraging people to call 9-8-8 during a very bad day, saying,
If we are doing our job as a nation, then … we can answer that phone or that text message quickly and efficiently and let you know that we are spending time with you, that you are not alone. That is the major preventive activity in this work.
Brinton noted that not every state legislature has passed legislation on 9-8-8 implementation yet, but they emphasized that every school should have a suicide prevention policy and that every teacher, faith community leader, and mental health professional should know about 9-8-8 and spread the word about it so that calling it becomes a normalized process.
REFLECTIONS: OPPORTUNITIES TO BUILD INCLUSIVE CARE STRUCTURES
To conclude the workshop, Barbara Limandri, a psychiatric nurse with the American Psychiatric Nurses Association and professor emerita at Linfield University, and David Covington, chief executive officer and president of RI International and a partner with Behavioral Health Link, offered their thoughts and reflections. Limandri first commented that 9-8-8 is a long overdue community intervention for suicide prevention that will make it easier to ask for help. However, she added that 9-8-8 is not a cure-all. “We still have to reduce stigma,” she said.
Limandri noted that suicide is the equivalent of a heart attack in terms of an emergency, and that while it took a few decades, cardiopulmonary resuscitation (CPR) is now a community intervention. In her mind, suicide prevention is mental health CPR, and everyone needs to be trained in the basics. The good news, she said, is that robust research on suicide intervention and prevention shows that the skills for suicide prevention are simple: asking the question, “Are you thinking of killing yourself?”; listening to the
response without judgment; and then connecting that person to those who can help them. This skill, called QPR, or question, persuade, and refer, should be taught to everyone along with CPR, Limandri said.
What the public needs to recognize, she said, is that suicide prevention is effective. “Suicidal thinking and behaviors are a transient state of extreme impulsivity and lack of perspective,” said Limandri. “Having someone else step in and be a source of hope and perspective can be an immense improvement in the struggle for the person with suicidal thinking and behaviors.” What this comes down to, she said, is seeing each person in their setting and culture and taking care of them. She also pointed out that family, friends, and neighbors are the most essential first responders in a suicide crisis, not the mental health professional. Limandri said, “We get them after they are in the crisis, after they have made an attempt, but it is the neighbor, the family member that is hearing it first, and they do not know what to do.” However, they can learn those skills in the same way that community members learn CPR she added. As a final comment, she called for a systemic approach to suicide prevention. “I think the COVID pandemic has taught us that our health care system and our mental health care system are broken, and we need to improve on that as well,” said Limandri. She also posted two resources for suicide prevention training:
- Psychiatric-Mental Health Nurse Essential Competencies for Assessment and Management of Individuals at Risk for Suicide (https://www.apna.org/i4a/pages/index.cfm?pageid=5684)
- Question, Persuade, and Refer (https://qprinstitute.com)
Covington noted that the ideal crisis system for mental health, addiction, and suicidal behavior may seem like a fanciful dream, but the United States created the 9-1-1 system to respond to emergencies, just as it is about to do for the 9-8-8 system and mental health emergencies. Currently, however, a common experience for a person on their worst day is that they perceive what happens as punishment, not care or support. They are detained, delayed, and denied care, and they spend time in hospital emergency departments—and some people who are having a mental health crisis end up handcuffed in the back of a police vehicle.
Nonetheless, the combination of the pressure from the COVID-19 pandemic on hospitals, discussions of race inequity, a reconsideration of the role of law enforcement in this process, and the galvanizing promise of 9-8-8 provides an opportunity to create something different for everyone in crisis, but particularly for people of color and the LGBTQIA+ community. “This is an amazing day and once-in-a-lifetime opportunity to transform mental health care,” said Covington.
REFERENCES
Aarons, G. A., M. Hurlburt, and S. M. Horwitz. 2011. Advancing a conceptual model of evidence-based practice implementation in public service sectors. Administration and Policy in Mental Health and Mental Health Services Research 38(1):4-23.
Aarons, G. A., A. E. Green, L. A. Palinkas, S. Self-Brown, D. J. Whitaker, J. R. Lutzker, J. F. Silovsky, D. B. Hecht, and M. J. Chaffin. 2012. Dynamic adaptation process to implement an evidence-based child maltreatment intervention. Implementation Science 7(1):32.
Aguilar, C. 2018. Undocumented critical theory. Cultural Studies ↔ Critical Methodologies 19(3):152-160.
Ali, B., I. R. H. Rockett, T. R. Miller, and J. B. Leonardo. 2021. Racial/ethnic differences in preceding circumstances of suicide and potential suicide misclassification among US adolescents. Journal of Racial and Ethnic Health Disparities. https://doi.org/10.1007/s40615-020-00957-7.
Anestis, M. D., A. E. Bond, S. E. Daruwala, S. L. Bandel, and C. J. Bryan. 2021. Suicidal ideation among individuals who have purchased firearms during COVID-19. American Journal of Preventive Medicine 60(3):311-317.
Avery, A., M. Landen, T. Massaro, C. Novak, D. Sanchez, and A. Sandoval. 2018. 2020–2022 new mexico state health improvement plan. Santa Fe, NM: New Mexico Department of Health.
Bahraini, N., L. A. Brenner, C. Barry, T. Hostetter, J. Keusch, E. P. Post, C. Kessler, C. Smith, and B. B. Matarazzo. 2020. Assessment of rates of suicide risk screening and prevalence of positive screening results among us veterans after implementation of the Veterans Affairs suicide risk identification strategy. JAMA Network Open 3(10):e2022531.
Bernal, D. D. 2002. Critical race theory, latino critical theory, and critical raced-gendered epistemologies: Recognizing students of color as holders and creators of knowledge. Qualitative Inquiry 8(1):105-126.
Bohnenkamp, J. H., C. M. Schaeffer, R. Siegal, T. Beason, M. Smith-Millman, and S. Hoover. 2021. Impact of a school-based, multi-tiered emotional and behavioral health crisis intervention on school safety and discipline. Prevention Science 22(4):492-503.
Boyas, J. F., T. Villarreal-Otálora, L. R. Alvarez-Hernandez, and M. Fatehi. 2019. Suicide ideation, planning, and attempts: The case of the Latinx LBG youth. Health Promotion Perspectives 9(3):198-206.
Bray, M. J. C., N. O. Daneshvari, I. Radhakrishnan, J. Cubbage, M. Eagle, P. Southall, and P. S. Nestadt. 2021. Racial differences in statewide suicide mortality trends in Maryland during the coronavirus disease 2019 (COVID-19) pandemic. JAMA Psychiatry 78(4):444-447.
Bridge, J. A., S. C. Marcus, and M. Olfson. 2012. Outpatient care of young people after emergency treatment of deliberate self-harm. Journal of the American Academy of Child and Adolescent Psychiatry 51(2):213-222.
Bridge, J. A., L. Asti, L. M. Horowitz, J. B. Greenhouse, C. A. Fontanella, A. H. Sheftall, K. J. Kelleher, and J. V. Campo. 2015. Suicide trends among elementary school-aged children in the United States from 1993 to 2012. JAMA Pediatrics 169(7):673-677.
Bridge, J. A., L. M. Horowitz, C. A. Fontanella, A. H. Sheftall, J. Greenhouse, K. J. Kelleher, and J. V. Campo. 2018. Age-related racial disparity in suicide rates among US youths from 2001 through 2015. JAMA Pediatrics 172(7):697-699.
Britton, P., R. Bossarte, C. Thompson, J. Kemp, and K. Conner. 2013. Influences on call outcomes among veteran callers to the national veterans crisis line. Suicide & Life-Threatening Behavior 43.
Burstein, B., H. Agostino, and B. Greenfield. 2019. Suicidal attempts and ideation among children and adolescents in US emergency departments, 2007–2015. JAMA Pediatrics 173(6):598-600.
Cantrell, C., S. Valley-Gray, and R. E. Cash. 2012. Suicide in rural areas: Risk factors and prevention. In Rural mental health: Issues, policies, and best practices, edited by K. B. Smalley, J. C. Warren, and J. P. Rainer. New York: Springer. Pp. 213-228.
CDC (Centers for Disease Control and Prevention). 2019. Youth risk behavior survey: Data summary & trends report 2009–2019. https://www.cdc.gov/healthyyouth/data/yrbs/pdf/YRBSDataSummaryTrendsReport2019-508.pdf (accessed November 4, 2021).
CDC. 2021a. National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS). https://www.cdc.gov/injury/wisqars (accessed November 16, 2021).
CDC. 2021b. National Violent Death Reporting System (NVDRS), violence prevention. https://www.cdc.gov/violenceprevention/datasources/nvdrs/index.html (accessed November 4, 2021).
Chávez, T., S. Vences, Y. Ruiz, J. Navarro, F. Rodriguez, and I. Aranda. 2021. Critical incidences in U.S. health care systems experienced by undocumented young adults. Health Equity 5:569-576.
Cheraghi, M. A., M. Esmaeili, and M. Salsali. 2017. Seeking humanizing care in patient-centered care process: A grounded theory study. Holistic Nursing Practice 31(6):359-368.
Children’s Hospital Colorado. 2021. Children’s Hospital Colorado declares a state of emergency for youth mental health. https://www.childrenscolorado.org/about/news/2021/may2021/youth-mental-health-state-of-emergency (accessed November 4, 2021).
Chu, J., B. Maruyama, H. Batchelder, P. Goldblum, B. Bongar, and R. E. Wickham. 2020. Cultural pathways for suicidal ideation and behaviors. Cultural Diversity & Ethnic Minority Psychology 26(3):367-377. https://doi.org/10.1037/cdp0000307 (accessed November 16, 2021).
Coleman, B. W., and Congressional Black Caucus Emergency Taskforce on Black Youth Suicide and Mental Health. 2019. Ring the alarm: The crisis of Black youth suicide in America. Washington, DC: Congressional Black Caucus Emergency Taskforce on Black Youth Suicide and Mental Health.
Costello, E. J., J. P. He, N. A. Sampson, R. C. Kessler, and K. R. Merikangas. 2014. Services for adolescents with psychiatric disorders: 12-month data from the National Comorbidity Survey-Adolescent. Psychiatric Services 65(3):359-366.
Craig, S. L., L. B. McInroy, A. D. Eaton, G. Iacono, V. W. Y. Leung, A. Austin, and C. Dobinson. 2019. An affirmative coping skills intervention to improve the mental and sexual health of sexual and gender minority youth (Project Youth Affirm): Protocol for an implementation study. JMIR Research Protocols 8(6):e13462.
Cummings, J. R., N. A. Ponce, and V. M. Mays. 2010. Comparing racial/ethnic differences in mental health service use among high-need subpopulations across clinical and school-based settings. Journal of Adolescent Health 46(6):603-606.
Czeisler, M., R. I. Lane, E. Petrosky, J. F. Wiley, A. Christensen, R. Njai, M. D. Weaver, R. Robbins, E. R. Facer-Childs, L. K. Barger, C. A. Czeisler, M. E. Howard, and S. M. W. Rajaratnam. 2020. Mental health, substance use, and suicidal ideation during the COVID-19 pandemic—United States, June 24–30, 2020. Morbidity and Mortality Weekly Report 69(32):1049-1057.
Damschroder, L. J., D. C. Aron, R. E. Keith, S. R. Kirsh, J. A. Alexander, and J. C. Lowery. 2009. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implementation Science 4(1):50.
Dobscha, S. K., K. D. Clark, S. Newell, E. A. Kenyon, E. Karras, J. A. Simonetti, and M. Gerrity. 2021. Strategies for discussing firearms storage safety in primary care: Veteran perspectives. Journal of General Internal Medicine 36(6):1492-1502.
Eylem, O., L. de Wit, A. van Straten, L. Steubl, Z. Melissourgaki, G. T. Danışman, R. de Vries, A. J. F. M. Kerkhof, K. Bhui, and P. Cuijpers. 2020. Stigma for common mental disorders in racial minorities and majorities a systematic review and meta-analysis. BMC Public Health 20(1):879.
Fontanella, C. A., D. L. Hiance-Steelesmith, G. S. Phillips, J. A. Bridge, N. Lester, H. A. Sweeney, and J. V. Campo. 2015. Widening rural-urban disparities in youth suicides, United States, 1996–2010. JAMA Pediatrics 169(5):466-473.
Ford, C. L., and C. O. Airhihenbuwa. 2010. Critical race theory, race equity, and public health: Toward antiracism praxis. American Journal of Public Health 100(Suppl 1):S30-S35.
GAO (U.S. Government Accountability Office). 2018. Discipline disparities for Black studnets, boys, and students with disabilities. Washington, DC: GAO. https://www.gao.gov/assets/gao-18-258.pdf (accessed November 4, 2021).
GAO. 2019. Opportunities exist for VA to better identify and address racial and ethnic disparities. Washington, DC: GAO.
Gennetian, L. A., S. Wolf, H. D. Hill, and P. A. Morris. 2015. Intrayear household income dynamics and adolescent school behavior. Demography 52(2):455-483. https://doi.org/10.1007/s13524-015-0370-9.
Gennetian, L., R. Seshadri, N. Hess, A. Winn, and R. Goerge. 2016. Supplemental Nutrition Assistance Program (SNAP) benefit cycles and student disciplinary infractions. Social Service Review 90:403-433.
Goldman-Mellor, S., M. Olfson, C. Lidon-Moyano, and M. Schoenbaum. 2019. Association of suicide and other mortality with emergency department presentation. JAMA Network Open 2(12):e1917571.
Gould, M., J. Kalafat, J. Harrismunfakh, and M. Kleinman. 2007. An evaluation of crisis hotline outcomes part 2: Suicidal callers. Suicide and Life-Threatening Behavior 37:338-352.
Gould, M. S., A. M. Lake, J. L. Munfakh, H. Galfalvy, M. Kleinman, C. Williams, A. Glass, and R. McKeon. 2016. Helping callers to the National Suicide Prevention Lifeline who are at imminent risk of suicide: Evaluation of caller risk profiles and interventions implemented. Suicide and Life-Threatening Behavior 46(2):172-190.
Gould, M. S., A. M. Lake, H. Galfalvy, M. Kleinman, J. L. Munfakh, J. Wright, and R. McKeon. 2018. Follow-up with callers to the National Suicide Prevention Lifeline: Evaluation of callers’ perceptions of care. Suicide and Life-Threatening Behavior 48(1):75-86.
Gould, M. S., S. Chowdhury, A. M. Lake, H. Galfalvy, M. Kleinman, M. Kuchuk, and R. McKeon. 2021a. National Suicide Prevention Lifeline crisis chat interventions: Evaluation of chatters’ perceptions of effectiveness. Suicide and Life-Threatening Behavior. http://doi.org/10.1111/sltb.12795 (accessed November 16, 2021).
Gould, M. S., A. M. Lake, M. Kleinman, H. Galfalvy, and R. McKeon. 2021b. Third-party callers to the National Suicide Prevention Lifeline: Seeking assistance on behalf of people at imminent risk of suicide. Suicide and Life-Threatening Behavior. http://doi.org/10.1111/sltb.12769 (accessed November 16, 2021).
Green, A. E., C. E. Willging, M. M. Ramos, D. Shattuck, and L. Gunderson. 2018. Factors impacting implementation of evidence-based strategies to create safe and supportive schools for sexual and gender minority students. Journal of Adolescent Health 63(5):643-648.
Harris, J., E. Wahesh, M. Barrow, and J. Fripp. 2021. Demographics, stigma, and religious coping and Christian African Americans’ help seeking. Counseling and Values 66:73-91.
Hays, K., and K. D. Lincoln. 2017. Mental health help-seeking profiles among African Americans: Exploring the influence of religion. Race and Social Problems 9(2):127-138.
Hedegaard, H., S. C. Curtin, and M. Warner. 2021. Suicide mortality in the United States, 1999–2019. Hyattsville, MD: National Center for Health Statistics.
HHS (U.S. Department of Health and Human Services). 2013. National standards for culturally and linguistically appropriate services in health and health care: A blueprint for advancing and sustaining CLAS policy and practice. https://thinkculturalhealth.hhs.gov/assets/pdfs/EnhancedCLASStandardsBlueprint.pdf (accessed November 16, 2021).
Hogg, B., J. C. Medina, I. Gardoki-Souto, I. Serbanescu, A. Moreno-Alcázar, A. Cerga-Pashoja, E. Coppens, M. D. Tóth, N. Fanaj, B. A. Greiner, C. Holland, K. Kõlves, M. Maxwell, G. Qirjako, L. de Winter, U. Hegerl, V. Pérez-Sola, E. Arensman, and B. L. Amann. 2021. Workplace interventions to reduce depression and anxiety in small and medium-sized enterprises: A systematic review. Journal of Affective Disorders 290:378-386.
Hom, M. A., and I. H. Stanley. 2021. Considerations in the assessment of help-seeking and mental health service use in suicide prevention research. Suicide and Life-Threatening Behavior 51(1):47-54.
Horowitz, L. M., D. Snyder, E. Ludi, D. L. Rosenstein, J. Kohn-Godbout, L. Lee, T. Cartledge, A. Farrar, and M. Pao. 2013. Ask suicide-screening questions to everyone in medical settings: The asQ’em Quality Improvement Project. Psychosomatics 54(3):239-247.
Ivey-Stephenson, A. Z., Z. Demisssie, A. E. Crosby, D. M. Stone, E. Gaylor, N. Wilkins, R. Lowry, and M. Brown. 2020. Suicidal ideation and behaviors among high school students—Youth Risk Behavior Survey, United States, 2019. Morbidity and Mortality Weekly Report 69(1):47-59.
Jaycox, L. H., J. A. Cohen, A. P. Mannarino, D. W. Walker, A. K. Langley, K. L. Gegenheimer, M. Scott, and M. Schonlau. 2010. Children’s mental health care following Hurricane Katrina: A field trial of trauma-focused psychotherapies. Journal of Trauma and Stress 23(2):223-231.
Kalafat, J., M. Gould, J. Munfakh, and M. Kleinman. 2007. An evaluation of crisis hotline outcomes part 1: Nonsuicidal crisis callers. Suicide and Life-Threatening Behavior 37:322-337.
Kase, C., S. Hoover, G. Boyd, K. D. West, J. Dubenitz, P. A. Trivedi, H. J. Peterson, and B. D. Stein. 2017. Educational outcomes associated with school behavioral health interventions: A review of the literature. Journal of School Health 87(7):554-562.
Klonsky, E. D., and A. May. 2015. The three-step theory (3st): A new theory of suicide rooted in the “ideation-to-action” framework. International Journal of Cognitive Therapy 8:114-129.
Layman, D. M., J. Kammer, E. Leckman-Westin, M. Hogan, J. Goldstein Grumet, C. D. Labouliere, B. Stanley, J. Carruthers, and M. Finnerty. 2021. The relationship between suicidal behaviors and zero suicide organizational best practices in outpatient mental health clinics. Psychiatric Services https://ps.psychiatryonline.org/doi/10.1176/appi.ps.202000525 (accessed November 16, 2021).
LeCloux, M. A., M. Weimer, S. L. Culp, K. Bjorkgren, S. Service, and J. V. Campo. 2020. The feasibility and impact of a suicide risk screening program in rural adult primary care: A pilot test of the ask suicide-screening questions toolkit. Psychosomatics 61(6):698-706.
LESC (Legislative Education Study Committee). 2021a. School-based health care. Legislative Education Study Committee Bill Analysis, 55th Legislature, 1st Session, 2021. https://www.nmlegis.gov/Sessions/21%20Regular/LESCAnalysis/SM015.PDF (accessed November 5, 2021).
LESC. 2021b. Full-time school nurse. Legislative Education Study Committee Bill Analysis. 55th Legislature, 1st Session, 2021. https://www.nmlegis.gov/Sessions/21%20Regular/LESCAnalysis/SB0031.PDF (accessed November 5, 2021).
LFC (Legislative Finance Committee). 2021. Full-time nurse in every school, HB 32. Fiscal Impact Report. https://nmlegis.gov/Sessions/19%20Regular/bills/house/HB0476.pdf (accessed November 5, 2021).
Limas, E. A., and E. L. Vaughan. 2018. Associations between substance use disorders and suicidal ideation: An investigation of latino emerging adults. Emerging Adulthood 7(1):21-30.
Lindsey, M. A., C. L. Barksdale, S. F. Lambert, and N. S. Ialongo. 2010. Social network influences on service use among urban, African American youth with mental health problems. Journal of Adolescent Health 47(4):367-373.
Lindsey, M. A., A. H. Sheftall, Y. Xiao, and S. Joe. 2019. Trends of suicidal behaviors among high school students in the United States: 1991–2017. Pediatrics 144(5):e20191187.
Lyons, V. H., M. J. Haviland, D. Azrael, A. Adhia, M. A. Bellenger, A. Ellyson, A. Rowhani-Rahbar, and F. P. Rivara. 2021. Firearm purchasing and storage during the COVID-19 pandemic. Injury Prevention 27(1):87-92.
McCabe, K. M., M. Yeh, and A. A. Zerr. 2020. Personalizing behavioral parent training interventions to improve treatment engagement and outcomes for culturally diverse families. Psychological Research and Behavior Management 13:41-53.
McGuire, T. G., and J. Miranda. 2008. New evidence regarding racial and ethnic disparities in mental health: Policy implications. Health Affairs (Project Hope) 27(2):393-403.
Merikangas, K. R., J. P. He, M. Burstein, J. Swendsen, S. Avenevoli, B. Case, K. Georgiades, L. Heaton, S. Swanson, and M. Olfson. 2011. Service utilization for lifetime mental disorders in U.S. adolescents: Results of the National Comorbidity Survey-Adolescent Supplement (NCS-A). Journal of the American Academy of Child and Adolescent Psychiatry 50(1):32-45.
Michelmore, L., and P. Hindley. 2012. Help-seeking for suicidal thoughts and self-harm in young people: A systematic review. Suicide and Life-Threatening Behavior 42(5):507-524.
Mishara, B. L., and S. Stijelja. 2020. Trends in US suicide deaths, 1999 to 2017, in the context of suicide prevention legislation. JAMA Pediatrics 174(5):499-500.
Misra, S., V. W. Jackson, J. Chong, K. Choe, C. Tay, J. Wong, and L. H. Yang. 2021. Systematic review of cultural aspects of stigma and mental illness among racial and ethnic minority groups in the United States: Implications for interventions. American Journal of Community Psychology https://doi.org/10.1002/ajcp.12516 (accessed November 16, 2021).
Murphy, S. L., J. Xu, K. D. Kochanek, E. Arias, and B. Tejada-Vera. 2021. Deaths: Final data for 2018. National Vital Statistics Reports 69(13). https://www.cdc.gov/nchs/data/nvsr/nvsr69/nvsr69-13-508.pdf (accessed November 29, 2021).
National Action Alliance for Suicide Prevention: Transforming Communities-Community-Based Suicide Prevention Priority Group. 2017. Transforming communities: Key elements for the implementation of comprehensive community-based suicide prevention. Washington, DC: National Action Alliance for Suicide Prevention.
Nazroo, J. Y., K. S. Bhui, and J. Rhodes. 2020. Where next for understanding race/ethnic inequalities in severe mental illness? Structural, interpersonal and institutional racism. Sociology of Health & Illness 42(2):262-276.
Nelson, H. D., L. M. Denneson, A. R. Low, B. W. Bauer, M. O’Neil, D. Kansagara, and A. R. Teo. 2017. Suicide risk assessment and prevention: A systematic review focusing on veterans. Psychiatric Services 68(10):1003-1015.
Newell, S., E. Kenyon, K. D. Clark, V. Elliott, A. Rynerson, M. S. Gerrity, E. Karras, J. A. Simonetti, and S. K. Dobscha. 2021. Veterans are agreeable to discussions about firearms safety in primary care. Journal of the American Board of Family Medicine 34(2):338.
NIMH (National Institute of Mental Health). 2021. NIH Announces Winners of High School Mental Health Essay Contest. https://www.nimh.nih.gov/news/sciencenews/2019/nih-announces-winners-of-high-school-mental-health-essay-contest (accessed November 16, 2021).
Office of the Surgeon General and National Action Alliance for Suicide Prevention. 2012. 2012 national strategy for suicide prevention: Goals and objectives for action. Washington, DC: HHS.
Oransky, M., E. Z. Burke, and J. Steever. 2019. An interdisciplinary model for meeting the mental health needs of transgender adolescents and young adults: The Mount Sinai Adolescent Health Center approach. Cognitive and Behavioral Practice 26(4):603-616.
Pistone, I., U. Beckman, E. Eriksson, H. Lagerlöf, and M. Sager. 2019. The effects of educational interventions on suicide: A systematic review and meta-analysis. International Journal of Social Psychiatry 65(5):399-412.
Ramchand, R., L. Jaycox, P. Ebener, M. L. Gilbert, D. Barnes-Proby, and P. Goutam. 2017. Characteristics and proximal outcomes of calls made to suicide crisis hotlines in California. Crisis 38(1):26-35.
Ramchand, R., J. A. Gordon, and J. L. Pearson. 2021. Trends in suicide rates by race and ethnicity in the united states. JAMA Network Open 4(5):e2111563.
Ramos, M. M., C. Greenberg, R. Sapien, J. Bauer-Creegan, B. Hine, and C. Geary. 2013. Behavioral health emergencies managed by school nurses working with adolescents. Journal of School Health 83(10):712-717.
Rasmussen, K. A., D. A. King, M. S. Gould, W. Cross, W. Tang, K. Kaukeinen, X. Tu, and K. L. Knox. 2017. Concerns of older veteran callers to the veterans crisis line. Suicide and Life-Threatening Behavior 47(4):387-397.
Ream, G. L. 2020. An investigation of the LGBTQ+ youth suicide disparity using national violent death reporting system narrative data. Journal of Adolescent Health 66(4):470-477.
Reger, M. A., H. M. Gebhardt, J. M. Lee, B. A. Ammerman, R. P. Tucker, B. B. Matarazzo, A. E. Wood, and D. A. Ruskin. 2019. Veteran preferences for the caring contacts suicide prevention intervention. Suicide and Life-Threatening Behavior 49(5):1439-1451.
Rhodes, A. E., M. Sinyor, M. H. Boyle, J. A. Bridge, L. Y. Katz, J. Bethell, A. S. Newton, A. Cheung, K. Bennett, P. S. Links, L. Tonmyr, and R. Skinner. 2018. Emergency department presentations and youth suicide: A case-control study. Canadian Journal of Psychiatry 64(2):88-97.
Richards, J. E., S. D. Hohl, C. D. Segal, D. C. Grossman, A. K. Lee, U. Whiteside, C. Luce, E. J. Ludman, G. Simon, R. B. Penfold, and E. C. Williams. 2021. “What will happen if I say yes?” perspectives on a standardized firearm access question among adults with depressive symptoms. Psychiatric Services 72(8):898-904.
Ritchie, M. J., K. M. Dollar, C. J. Miller, J. L. Smith, K. A. Oliver, B. Kim, S. L. Connolly, E. Woodward, T. Ochoa-Olmos, S. Day, J. A. Lindsay, and J. E. Kirchner. 2020. Using implementation facilitation to improve healthcare (version 3). Washington, DC: Veterans Health Administration.
Riva, J. J., K. M. Malik, S. J. Burnie, A. R. Endicott, and J. W. Busse. 2012. What is your research question? An introduction to the PICOT format for clinicians. Journal of the Canadian Chiropractic Association 56(3):167-171.
Robinson, W. L., C. R. Whipple, L. A. Jason, and C. E. Flack. 2021. African American adolescent suicidal ideation and behavior: The role of racism and prevention. Journal of Community Psychology 49(5):1282-1295.
Ruch, D. A., A. H. Sheftall, P. Schlagbaum, J. Rausch, J. V. Campo, and J. A. Bridge. 2019. Trends in suicide among youth aged 10 to 19 years in the United States, 1975 to 2016. JAMA Network Open 2(5):e193886.
Russon, J., R. Washington, A. Machado, L. Smithee, and J. Dellinger. 2021. Suicide among LGBTQIA+ youth: A review of the treatment literature. Aggression and Violent Behavior 101578.
SAMHSA (Substance Abuse and Mental Health Services Administration). 2020. Serious psychological distress in the past year among adults 18 years of age and over, percentage, 2019. Results from the 2019 National Survey on Drug Use and Health: Mental Health Detailed Tables. Table 10.43B. Rockville, MD: SAMHSA.
SAMHSA. 2021. SAMHSA awards Vibrant Emotional Health the grant to administer 988 dialing code for the National Suicide Prevention Lifeline. SAMHSA News Release. https://www.samhsa.gov/newsroom/press-announcements/202106161430 (accessed November 4, 2021).
SAMHSA and CMS (Centers for Medicare & Medicaid Services). 2019. Guidance to states and school systems on addressing mental health and substance use issues in schools. In Joint Informational Bulletin. Washington, DC: SAMHSA and CMS.
Searles, V. B., M. A. Valley, H. Hedegaard, and M. E. Betz. 2014. Suicides in urban and rural counties in the United States, 2006–2008. Crisis 35(1):18-26.
Shattuck, D., J. L. Hall, A. Green, C. Greenberg, L. Peñaloza, M. Ramos, and C. Willging. 2020. Recruitment of schools for intervention research to reduce health disparities for sexual and gender minority students. Journal of School Nursing 36(4):258-264.
Shattuck, D., R. Sebastian, M. Ramos, and K. Zamarin. 2021. Behavioral health emergencies managed by school nurses. Paper presented at National Association of School Nurses 2021 Virtual, Transforming Student Health: School Nurses Leading the Way.
Silva, C., and K. A. Van Orden. 2018. Suicide among hispanics in the United States. Current Opinion in Psychology 22:44-49.
Simonetti, J. A., B. Dorsey Holliman, R. Holliday, L. A. Brenner, and L. L. Monteith. 2020. Correction: Firearm-related experiences and perceptions among United States male veterans: A qualitative interview study. PLOS ONE 15(4):e0231493.
Simonetti, J., D. Azrael, W. Zhang, and M. Miller. 2021. Normative beliefs among veteran firearm owners regarding when clinicians should discuss firearm safety with patients: Results from the 2019 National Firearms Survey. Paper presented at U.S. Department of Veterans Affairs/U.S. Department of Defense National Suicide Prevention Conference.
Smith-Morris, C., and J. Epstein. 2014. Beyond cultural competency: Skill, reflexivity, and structure in successful tribal health care. American Indian Culture and Research Journal 38:29-48.
Stapelberg, N. J. C., J. Sveticic, I. Hughes, A. Almeida-Crasto, T. Gaee-Atefi, N. Gill, D. Grice, R. Krishnaiah, L. Lindsay, C. Patist, H. V. Engelen, S. Walker, M. Welch, S. Woerwag-Mehta, and K. Turner. 2021. Efficacy of the zero suicide framework in reducing recurrent suicide attempts: Cross-sectional and time-to-recurrent-event analyses. British Journal of Psychiatry 219(2):427-436.
Stephan, S. H., G. Sugai, N. Lever, and E. Connors. 2015. Strategies for integrating mental health into schools via a multitiered system of support. Child and Adolescent Psychiatric Clinics of North America 24(2):211-231.
Sylliboy, J. R., and R. B. Hovey. 2020. Humanizing Indigenous peoples’ engagement in health care. Canadian Medical Association Journal 192(3):E70.
Terrell, S. 2019. Film explores 2013 behavioral health shakeup in New Mexico. AP News. https://apnews.com/article/08a5ed186c424b01a1cae3b95fd679bb (accessed November 5, 2021).
U.S. Surgeon General and National Action Alliance for Suicide Prevention. 2021. The Surgeon General’s call to action to implement the National Strategy for Suicide Prevention. Washington, DC: HHS. https://www.hhs.gov/sites/default/files/sprc-call-to-action.pdf (accessed November 4, 2021).
VA (U.S. Department of Veterans Affairs). 2019. National veteran suicide prevention annual report. Washington, DC: VA.
Valsiner, J. 2003. Culture and its transfer: Ways of creating general knowledge through the study of cultural particulars. Online Readings in Psychology and Culture 2(1).
Velasco Bueno, J. M., and G. H. La Calle. 2020. Humanizing intensive care: From theory to practice. Critical Care Nursing Clinics of North America 32(2):135-147.
Walrath, C., L. G. Garraza, H. Reid, D. B. Goldston, and R. McKeon. 2015. Impact of the Garrett Lee Smith Youth Suicide Prevention Program on suicide mortality. American Journal of Public Health 105(5):986-993.
The Washington Post. 2021. Washington Post police shooting database. https://www.washingtonpost.com/graphics/investigations/police-shootings-database (accessed November 4, 2021).
While, D., H. Bickley, A. Roscoe, K. Windfuhr, S. Rahman, J. Shaw, L. Appleby, and N. Kapur. 2012. Implementation of mental health service recommendations in England and Wales and suicide rates, 1997–2006: A cross-sectional and before-and-after observational study. Lancet 379(9820):1005-1012.
Whiteside, C. 2019. Health behaviors and conditions of adult New Mexicans, results from the New Mexico Behavioral Risk Factor Surveillance System (BRFSS) 2019 annual report. Santa Fe, NM: New Mexico Department of Health.
Whiteside, C., and D. Green. 2021. Sexual orientation and gender identity: Data from the youth risk and resiliency survey and behavioral risk factor surveillance system. Santa Fe, NM: New Mexico Department of Health.
WHO (World Health Organization). 2014. Preventing suicide: A global imperative. Geneva, Switzerland: WHO Press.
Willging, C. E., and E. M. Trott. 2018. Outsourcing responsibility: State stewardship of behavioral health care services. In Unequal coverage: The experience of health care reform in the United States, edited by J. Mulligan and H. Castaneda. New York: New York University Press. Pp. 231-253.
Willging, C. E., A. E. Green, and M. M. Ramos. 2016. Implementing school nursing strategies to reduce LGBTQ adolescent suicide: A randomized cluster trial study protocol. Implementation Science 11(1):145.
Willging, C., M. Kano, A. E. Green, R. Sturm, M. Sklar, S. Davies, and K. Eckstrand. 2020. Enhancing primary care services for diverse sexual and gender minority populations: A developmental study protocol. BMJ Open 10(2):e032787.
Williams, D. R. 2018. Stress and the mental health of populations of color: Advancing our understanding of race-related stressors. Journal of Health and Social Behavior 59(4):466-485.
Zayas, L. H., and Pilat, A. M. 2008. Suicidal behavior in Latinas: explanatory cultural factors and implications for intervention. Suicide & Life-Threatening Behavior 38(3):334-342.










































































