
2
Why Diverse Representation in Clinical Research Matters and the Current State of Representation within the Clinical Research Ecosystem
The analysis draws substantially from research papers by Dr. Bryan Tysinger, Ph.D. and Jakub P. Hlávka, Ph.D. which were commissioned for this study. The full research papers can be found in Appendix A and Appendix B.
In this chapter, the first section details how lack of representation risks undermining the overall goals of clinical research and the costs of maintaining the status quo. The next section describes the current status of clinical research representation with a focus on women and racial/ethnic minority populations. The chapter ends with a description of the clinical research ecosystem with a focus on the processes that might address diverse representativeness.
LACK OF REPRESENTATION IN CLINICAL RESEARCH THREATENS THE OVERARCHING GOALS OF CLINICAL RESEARCH
While inclusion of women and historically excluded groups in clinical research has long been viewed as a worthy aim, what are the consequences of failure to achieve this aim? As the overarching goal of the U.S. investment in biomedical research is to improve the health and well-being of the entire U.S. population, the committee identified seven potential threats to this goal posed by lack of representation in clinical research.
- Lack of representation compromises generalizability of clinical research findings to the U.S. population. Over the latter half of the 20th century, randomized controlled trials (RCTs) came to be regarded by the
-
medical community as the gold standard in evidence-based medicine to determine the safety and efficacy of investigational medical therapies. Initially, the results from these RCTs were largely considered to be generalizable to all patient populations (Bothwell et al., 2016). Over the past few decades, growing evidence has surfaced to challenge that assumption (Sirugo et al., 2019). Specifically, research has demonstrated that many groups underrepresented and excluded in clinical research can have distinct disease presentations or health circumstances that affect how they will respond to an investigational drug or therapy (Beglinger, 2008; Crawley et al., 2003; Garcia et al., 2016; Ramamoorthy et al., 2015). Such differences contribute to variable therapeutic responses and necessitate targeted efficacy and safety evaluation (see Box 2-1). For instance, it appears that men are more likely to respond to tricyclic antidepressants and women to selective serotonin reuptake inhibitors as treatment for depression (Baca et al., 2004; Bano et al., 2004; Kornstein et al., 2000). Reduced renal and hepatic clearance in older adults increases the risk of harms from drugs such as anticoagulants and psychotropic agents (Maixner et al., 1999; Shepherd et al., 1977; Soejima et al., 2022).
Representation by self-identified race and ethnicity is important to generalizability of study findings, but interpretation requires clarity of thought. Racial categories are socially constructed and do not have a biological basis, as is noted at the outset of this report. Some genetic factors that may result in heterogeneity in drug response may be more common in certain ancestral populations, which may be associated with self-identified race and ethnicity, as is the case for classes of medications that have narrow therapeutic window such as anti-coagulants (Box 2-1) or efavirenz (Cummins et al., 2015; Torgensen et al., 2019). In these cases, studies with participants diverse by self-identified race may allow for the identification of specific genotypes important for understanding heterogeneity in drug response. Self-identified race and ethnicity may also be associated with lived experiences that themselves result in specific biological manifestations that are not genetic in origin. For example, the lived experience of structural and interpersonal racism, lower socioeconomic status, and lower educational attainment all appear to be associated with elevations in blood pressure and cardiovascular risk (Hamad et al., 2019, 2020; King et al., 2021; Krieger and Sidney, 2011). Non-genetic factors may affect each population differently and also are subject to epigenetic effects that may vary across populations. Therefore, these analyses are complex and demand nuanced analyses with detailed and high-quality measures on genetic and non-genetic factors, and interpretation of population-specific data in clinical trials. Ensuring diverse participation in scientific studies allow for exploration of all of these factors and their interactions and is critical to the interpretations that allow for generalizability of findings to the population.
-
Threats to generalizability exist for all studies, not just clinical trials of new therapeutics. For example, implementation of evidence-based practice in community settings may be limited because the practice sites may be substantially different from those included in clinical research studies. Clinical research is often performed in well-resourced tertiary care sites in large urban centers, and may have limited applicability to community sites, less well-resourced safety net settings, and rural settings. Genetic and genomic studies that form the basis for “precision medicine” are increasingly recognized to be built on data from mostly populations of European descent (Martin et al., 2019; Sirugo et al., 2019). Tools such as polygenic risk scores that may help to identify risk and target therapeutic agents more selectively are recognized to be substantially less effective in populations with different genetic ancestry (Martin et al., 2019).
- Lack of representation costs hundreds of billions of dollars. It is important to also quantify the potential economic benefits of greater inclusion in clinical trials. The committee commissioned a study using
-
the Future Elderly Model (FEM), a model developed over more than two decades with funding from the National Institutes of Health, MacArthur Foundation, Centers for Medicare & Medicaid Services (CMS), and Department of Labor (see Boxes 2-2 and 2-3).
For the committee’s report, the model follows a representative cohort of Americans over time, generating snapshots of their health, functional status, and medical spending. Health is measured based on a set of self-reported chronic diseases such as diabetes, hypertension, heart disease, cancer, and other conditions. At any point in time, a person’s health and functional status is translated into a disability-adjusted life-year and assigned a monetary value ($150,000 per disability-adjusted life-year). In this way, the model captures both how long a person will live, and the years of disability-free life they will experience over their lifetime. (See Appendix A for more detail.)
Using this model, the committee estimated the social costs of health disparities for groups that have historically been underrepresented in clinical trials and in clinical research. The presumption is that disparities in three outcomes could potentially have been mitigated if clinical trials had been more inclusive: quantity of life (measured by life expectancy), quality of life (measured by disability-free life), and working life (measured by years in the labor force) (see Box 2-1). To quantify the potential benefits of more diverse representation, the committee identified six historically underrepresented groups with sufficient sample size to support the analysis. Throughout, non-Hispanic white men served as the reference group due to their historical inclusion and representation in clinical trials. Self-reported non-Hispanic Black men, Hispanic/Latinx men, non-Hispanic white women, non-Hispanic Black women, and Hispanic/Latinx women all potentially benefit from narrowing the differential impact of disease on the outcomes of interest (see Table 2-1).
The committee then considered potential benefits of reducing disparities in three key chronic diseases: diabetes, heart disease, and hypertension. In aggregate, the committee found when using the FEM that health disparities in diabetes will cost society more than $5 trillion through 2050—including mortality, morbidity, and loss of work. Heart disease would cost more than $6 trillion, and hypertension even more.
What accounts for these differences? Much of it has to do with the shorter life expectancy for Black and Latinx populations with these diseases. The United States has seen dramatic changes in population health over the last century—driving an increase in life expectancy and productivity. As a result, many people have enjoyed greater overall wealth, much of which was previously sapped by illness, disability, and premature death. However, these gains have been uneven (Jamison et al., 2013).
-
Understanding these consequences requires a broader measure of welfare (Clark, 2013). Returns on social investments are usually measured by economic capacity—particularly gross domestic product in national income accounts. However, such accounts only measure the extent of market activities in an economy. They do not account for other valuable nonmarket activities, of which health is likely the most important (Becker et al., 2005).
The committee’s approach measures how health investments could more broadly contribute to social value. These methods have been used to assess progress internationally as well. It does so by measuring the benefits of reducing disparities—which translates into both longer and healthier lives. These methods, which quantify the health improvements in terms of dollars, allow us to compare compressed inequality to other economic outcomes (Goldman et al., 2009; Goldman et al., 2013; Lowsky et al., 2014; Olshansky et al., 2009; Olshansky et al., 2012).
All told, health disparities incur a substantial economic toll on the U.S. society. Of course, better representation in clinical research will not completely alleviate these disparities—after all, they have many interconnected and interdependent causes. However, to the extent that representation in clinical research may improve generalizability of scientific findings across a range of clinical studies for these important health states, drive new discoveries and increase innovation, improve access, and increase trust, representative clinical research may play a role in alleviating these inequities. Even if only 1 percent of these health disparities could be al-
TABLE 2-1 Adjusted Relative Risks for Key Parameters of Interest with 95% Confidence Intervals
| Diabetes | Heart Disease | Hypertension | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mortality | Disability | Work | Mortality | Disability | Work | Mortality | Disability | Work | |
| White males | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Black males | 1.10 [1.02, 1.18] | 1.12 [1.07, 1.16] | 0.89 [0.85, 0.92] | 1.14 [1.07, 1.22] | 1.23 [1.18, 1.27] | 0.86 [0.83, 0.90] | 1.10 [1.02, 1.19] | 1.17 [1.13, 1.22] | 0.95 [0.93, 0.98] |
| Hispanic males | 1.11 [1.02, 1.20] | 1.12 [1.07, 1.16] | 0.91 [0.88, 0.94] | 1.15 [1.07, 1.23] | 1.22 [1.18, 1.27] | 0.89 [0.86, 0.92] | 1.11 [1.03, 1.20] | 1.17 [1.12, 1.21] | 0.96 [0.94, 0.98] |
| White females | 1.10 [1.02, 1.19] | 1.11 [1.07, 1.16] | 0.89 [0.85, 0.92] | 1.14 [1.07, 1.21] | 1.21 [1.17, 1.26] | 0.86 [0.82, 0.90] | 1.10 [1.02, 1.18] | 1.16 [1.12, 1.20] | 0.95 [0.92, 0.98] |
| Black females | 1.11 [1.02, 1.20] | 1.10 [1.06, 1.14] | 0.88 [0.85, 0.92] | 1.15 [1.07, 1.23] | 1.19 [1.15, 1.22] | 0.86 [0.83, 0.90] | 1.11 [1.03, 1.20] | 1.15 [1.11, 1.19] | 0.95 [0.93, 0.98] |
| Hispanic females | 1.11 [1.02, 1.21] | 1.10 [1.06, 1.14] | 0.88 [0.85, 0.92] | 1.15 [1.07, 1.23] | 1.18 [1.15, 1.22] | 0.86 [0.82, 0.90] | 1.11 [1.03, 1.20] | 1.14 [1.11, 1.18] | 0.95 [0.92, 0.98] |
NOTE: Adjusted relative risks for the key parameters of interest (the underrepresented group and disease interaction term) are shown here. The reference group, non-Hispanic white males, will always have values of 1.0. Relative to white males, being in an underrepresented group and having diabetes is associated with an increase in mortality of 10 to 11 percent, an increase in disability of 10 to 12 percent, and a decrease in workforce participation of 9 to 12 percent. Heart disease is associated with a mortality increase of 14 to 15 percent, an increase in disability of 19 to 23 percent, and a decrease in workforce participation of 11 to 14 percent. Hypertension is associated with an increase in mortality of 10 to 11 percent, an increase in disability of 14 to 17 percent, and a decrease in workforce participation of 4 to 5 percent.
-
leviated by better representation in clinical research—like the warfarin example in Box 2-1—the analysis shows it would result in more than $40 billion in gains for diabetes and $60 billion for heart disease alone.
These findings suggest that even modest reductions in health disparities as a result of better representation in clinical trials for diabetes and heart disease would result in billions of dollars of savings to U.S. society. Expanding this estimate by alleviating the health disparity more fully, adding other diseases like Alzheimer’s disease or cancer, or computing across future cohorts would only add to the potential benefits of better representation.
- Lack of representation may hinder innovation. Diversity in study participants allows for greater exploration of variation in the overall effectiveness of a particular intervention. Exploring “heterogeneity of treatment effects” may be necessary not only to understand variation that affects safety and effectiveness of an intervention in the populations that have been underrepresented in studies but also to identify new biological processes that may, in turn, lead to new discoveries important for all populations. For example, the discovery of proprotein convertase subtilisin/kexin type 9 (PCSK9) has transformed the understanding of cholesterol homeostasis and led to development of important therapeutics for prevention and treatment of atherosclerotic cardiovascular disease (Warden et al., 2020). PCSK9 was discovered while examining differences in cholesterol metabolism in the Atherosclerotic Risk in Communities (ARIC) Study that was specifically designed to investigate variation in cardiovascular risk factors, medical care, and disease by self-reported race, gender, and location (Cohen et al., 2006; UNC, 2022). Researchers found that 2 percent of Black subjects in the ARIC cohort had one of two mutations in PCSK9 that are associated with a 40 percent reduction in low-density lipoprotein, or LDL, cholesterol. These mutations are rare among white people, and therefore, PCSK9 may not have been a target for exploration had diversity not been present in the ARIC study.
-
Lack of representation may compound low accrual that causes many trials to fail. According to an analysis by GlobalData (2021), low accrual was the cause for stopping 55 percent of all Phase I–IV clinical trials that were terminated, suspended, or discontinued during 2008–2017 (and for which a reason was given). Improving participation of underrepresented groups would be one way to increase enrollment. Thus, increasing enrollment of underrepresented populations would help solve the number one problem that causes clinical trials to fail, while also helping to ensure clinical data that are more representative of the whole population that could benefit from a studied intervention.
Moreover, improving representation in a way that increases the overall numbers of people who enroll in studies would reduce inefficiency and
-
waste caused by premature study termination. When a study fails to accrue, we often learn little or nothing about the investigational intervention, yet human and monetary resources have been sunk into designing, launching, and maintaining the study.
-
Lack of representation may lead to lack of access to effective medical interventions. Approval and indications for new therapeutics are often restricted to the demographics of the populations included in the clinical studies. Lack of representation may thus impede access to a specific therapeutic agent. For example, when Gilead Sciences Inc. sought Food and Drug Administration (FDA) approval for use of its HIV drug Descovy (emtricitabine/tenofovir alafenamide) as pre-exposure prophylaxis (PrEP), the company included only cisgender men and transgender women in its Phase III PrEP study, and presented the FDA with an extrapolation of data from two Phase I pharmacokinetic studies to support approval of the drug for cisgender women. As a result, the label explicitly excludes from the PrEP indication “individuals at risk of HIV-1 from receptive vaginal sex because effectiveness in this population has not been evaluated” (FDA, n.d.). This exclusion is included in direct-to-consumer advertising for the drug, which notes that Descovy for PrEP is not for use in people assigned female at birth.
Guideline-making bodies that synthesize various lines of evidence are often limited in making evidence-based recommendations that apply to all populations when the evidence base on specific populations does not exist; when these recommendations are tied to insurance coverage, these gaps may affect reimbursement of, and therefore access to, health care. For example, the U.S. Preventive Services Task Force (USPSTF) makes evidence-based recommendations for clinical preventive services, and its top-tier recommendations are linked to first-dollar insurance coverage from commercial payers under the Patient Protection and Affordable Care Act (P.L. 111-148). Lack of representative studies on screening for cancer or cardiometabolic disease may lead to recommendations that fail to consider earlier ages or lower biomarker thresholds to start screening that might be warranted in some populations (e.g., lower BMI [body mass index] or earlier age to start diabetes screening in Asian, Black, or Latinx populations; earlier age to start screening for lung, colorectal, breast, or prostate cancer in some populations). For example, in the 2021 USPSTF Report to Congress, the USPSTF was not “able to make a separate, specific recommendation on colorectal cancer screening in Black adults” because of “limited available empirical evidence” despite Black adults having the highest rates of incidence and mortality from colorectal cancer compared with other racial/ethnic groups (USPSTF, 2021). Although other national guideline organizations have historically recommended that Black adults begin screening at an earlier age, the task force recommends all adults start screening at age 45 due to lack of studies that report findings by race.
-
Clinical trials are a significant, and sometimes the only point of access for the most cutting-edge therapies for advanced disease (e.g., immunotherapy for cancer treatment). Lack of inclusion in clinical trials for advanced therapeutics may result in lack of access to these life-saving interventions.
- Lack of representation may undermine trust. Distrust of the clinical research enterprise and medical establishment rooted in historical and contemporary abuse has been documented as a barrier to participation in clinical studies among some populations. More contemporary work has focused on the importance of the research and medical enterprise working to regain trust and become more trustworthy partners (Alsan and Eichmeyer, 2021; Lucero et al., 2020; Wilkins, 2018). Efforts to overcome barriers to participation in scientific studies and working to create more representative and inclusive research environments may work to increase trust in science and medicine. Studies of vaccine hesitancy for influenza vaccines in Black populations found that knowledge and trust in the process of vaccine development and testing was associated with a higher degree of vaccine uptake (Quinn et al., 2018). Studies have also shown similar trust issues with the SAR-CoV-2 vaccine. Although COVID-19 vaccine trials were some of the most historically diverse trials, one study found that Black participants did not trust that the vaccine results were generalizable to them, contributing to vaccine hesitancy (Bazan and Akgün, 2021). Further, the lack of inclusion of pregnant people in the clinical trials of the SAR-CoV-2 vaccines led to lack of clarity on the use of these vaccines in pregnant people and may have contributed to vaccine hesitancy, even as subsequent data emerged on the importance of preventing COVID-19 infection during pregnancy (Rubin, 2021).
-
Lack of representation compounds health disparities in the populations currently underrepresented in clinical trials and clinical research. Healthy People 2020 defines a health disparity as “a particular type of health difference that is closely linked with social, economic, and/or environmental disadvantage. Health disparities adversely affect groups of people who have systematically experienced greater obstacles to health based on their racial or ethnic group; religion; socioeconomic status; gender; age; mental health; cognitive, sensory, or physical disability; sexual orientation or gender identity; geographic location; or other characteristics historically linked to discrimination or exclusion.” Health disparities are pervasive and prevent us from achieving health equity, defined as the “attainment of the highest level of health for all people. Achieving health equity requires valuing everyone equally with focused and ongoing societal efforts to address avoidable inequalities, historical and contemporary injustices, and the elimination of health and health care disparities” (CDC, 2020).
While achieving health equity and reducing health disparities requires far more than just equitable representation in clinical research, failure to
-
achieve equity on this dimension leaves health disparities unaddressed and reinforces inequities.
For example, prostate cancer is the most common cancer in U.S. men. Disparities in prostate cancer incidence and outcomes are particularly prominent. Black men in the United States have a 1.5 times greater chance of developing prostate cancer and are 2.2 times more likely to die from the disease than white men; roughly 30 percent of all prostate cancer deaths in the United States are in Black men. While the nature of these disparities is complex, the fact that Black men make up less than 3 percent of the participants in clinical trials of this common cancer may directly contribute to disparities via the threats listed above (Borno et al., 2019).
CLINICAL TRIALS PRODUCTION PROCESS
Several stakeholders are involved in the process of diversifying trials. While all of these are outlined in sections throughout this report, the committee thought it was helpful to detail the various stakeholders and processes in one place, for the ease of the reader (see Figure 2-1).
To begin from the ideation stage, investigators, whether in industry or academic medical centers, are often the ones developing research questions. However, working with community organizations and community partners helps build relationships, ensures that the research resources align with local needs, and helps to recruit and retain study participants in the research. The research itself is funded by federal sponsors (the National Institutes of Health [NIH], Centers for Disease Control and Prevention [CDC], Veterans Administration, Department of Defense, and Agency for Healthcare Research and Quality), nongovernmental organizations (academic institutions, patient advocacy groups, and philanthropic organizations), and industry (pharmaceutical, biotechnology, and medical device companies), and the priorities of these funders heavily influence the research that is done.
The study design process is heavily influenced by access to health care and clinical research, as well as the location of where the study itself is completed. Study participants are recruited and selected through word of mouth and social networks, through their primary care physician, and through contract research organizations. Recruitment of participants is highly dependent on where the study itself is taking place and the populations that access care at those sites. For example, federally qualified health centers are more likely to serve uninsured and impoverished families than other sites, such as academic medical centers and private practitioners. The committee would also like to note that while this report largely focuses on clinical trials and clinical research in the United States, many trials are completed overseas. In 2010, the FDA completed a report on the extent to which data submitted to the FDA was from foreign clinical trials. It found that 80 percent of approved applications for drugs and biologics contained data from clinical trials and that over half of clinical trial subjects and sites were located outside of the United States (HHS, 2010).
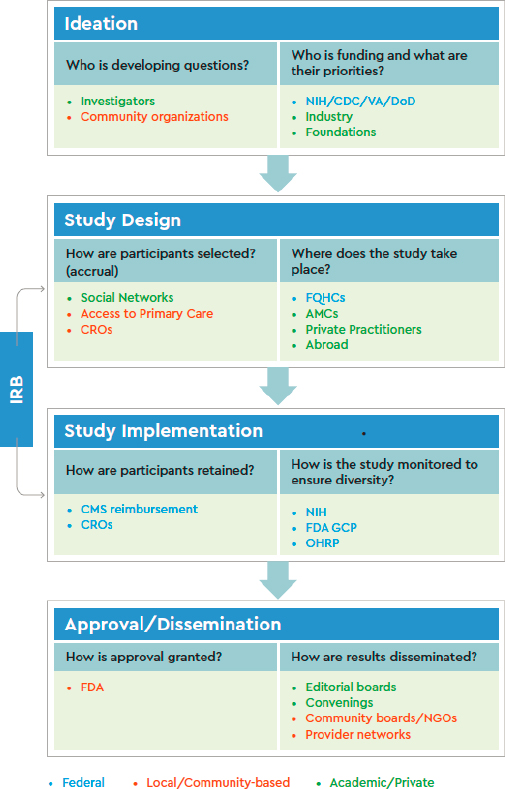
The study implementation phase is heavily influenced by insurance coverage and regulatory bodies. Federal agencies, such as the FDA, have the authority to ensure that trials are diverse and representative. Offices such as the Office for Human Research Protections do not oversee individual studies, but have the authority to revoke assurance within an institution if it is out of compliance with the Common Rule (45 CFR 46). If the NIH funds the study, it also has monitoring authority, along with private sponsors of trials. Participants are often retained assuming the cost of their participation and related costs are reimbursed by the CMS. Institutional review boards (IRBs) are also heavily influential in this stage, although they also influence the study design process as well.
Lastly, the approval and dissemination phase influences the diversity of trials. If investigators would like to submit for drug or biologic approval to the FDA, they have to submit the trial design and trial population. Even if they are not seeking FDA approval, medical journals and editorial boards and scientific conferences ultimately decide what information is published and disseminate results to the public. Ultimately, health-care purchases and payers (e.g., Medicare, private insurers, and individual patients) are primary consumers of clinical trial results, since this informs coverage and health decisions for individuals.
CURRENT STATUS OF CLINICAL TRIAL AND CLINICAL RESEARCH PARTICIPATION: LITTLE CHANGE OVER TIME
In the past three decades, diversity in clinical trials has become an important policy priority advanced by federal agencies such as the NIH Office of Research on Women’s Health, the FDA Office of Women’s Health and the Society for Women’s Health Research, and later by the FDA Office of Minority Health and Health Equity (FDA, 2011a) (see Chapter 3 for extensive analysis of the policy landscape). Despite the increased focus on the lack of women and historically underrepresented populations in U.S.-based clinical trials and research, research participants remain mostly white and male (Coakley et al., 2012; Wissing et al., 2014; Nature Medicine, 2018). Although contemporary reviews have shown increases in participation of women, and more modest increases in participation of racial and ethnic minority population groups and older populations, substantial and significant underrepresentation remains, particularly within certain medical disciplines and diseases, including cardiology, oncology, Alzheimer’s Disease, and HIV/AIDS (Chen et al., 2014; Tahhan et al., 2018; Huamani et al., 2019; Ashford et al., 2020; Tahhan et al., 2020; Reihl et al., 2021). Further, even though women’s representation in trials has increased, knowledge gaps remain, especially regarding treatment during pregnancy and while lactating (Geller et al., 2011; Scott et al., 2018; Vitale et al., 2017). It is also not clear from available data whether increases in women’s representation in clinical trials, writ large, is being driven by clinical study of diseases and conditions that disproportionately affect women.
An FDA summary report of clinical trials of drugs conducted between 2015 and 2019 shows that non-Hispanic white populations compose 78 percent of participants enrolled in U.S. trial sites (FDA, 2020a), though they comprise 61 percent of the country’s population (Ortman and Guarneri, 2009). Although it is not the focus of this report, it is important to note that there are additional issues of underrepresentation for age, such as for children and older adults, where issues of informed consent remain a barrier (Committee on Drugs, 2014; Zulman et al., 2011). The continued lack of representation is seen across numerous fields of medical research: different studies have found that racial and ethnic minority population groups and women remain underrepresented in oncology (Chen et al., 2014; Reihl et al., 2021), cardiovascular (Kim et al., 2008), ophthalmology (Berkowitz et al.,
2021), and surgical trials (Kalliainen et al., 2018). Further, when clinical trials do include underrepresented populations, subgroup-specific analyses and results are oftentimes missing or poorly executed (Assmann et al., 2000; Wang et al., 2007).
Transparency and Accountability in Participation
In 2015 the FDA published its first Drug Trial Snapshots, reporting on the demographic characteristics of participants in studies that resulted in product approvals the same year. The Snapshots made clear the extent to which underrepresented and excluded populations were underrepresented in trials for products that may eventually be prescribed or used in their medical care. In response to this and other recent documentation of the homogeneity of clinical trial participants, bioethicists, scientists, and funders have turned their attention to issues of transparency and accountability (Bierer, 2020; Hudson et al., 2016).
The National Institutes of Health aimed to improve transparency in the entire research enterprise by establishing a systematic process for tracking research studies from application through dissemination of results. The process includes the following key elements: requiring Good Clinical Practice training for investigators and staff; requiring investigators to submit clinical trial applications to trial-specific funding opportunity announcements (FOAs), which require more detailed descriptions of trial design, recruitment, and retention, and analyses plans compared with more generic parent FOAs; requiring more specific notices of award, which describe principal investigator responsibilities for publication of results and data sharing, where applicable; establishing a single IRB requirement to prevent delays in study implementation; and requiring clinical trial registration and summary results with financial penalties for failure to comply (Hudson et al., 2016).
To get a more up-to-date picture of who is participating in clinical trials, the committee commissioned research to analyze two different data sets for the trends in participant inclusion by sex and race/ethnicity in clinical trials (see Appendix B for full analysis). The first, the FDA Drug Trial Snapshots data, includes demographic data on trials from all approved drugs between 2014 and May 1, 2021 (FDA, 2021b). The second is demographic data on all NIH-funded clinical research and Phase III clinical trials from each institute and center at the NIH, from 2013 to 2018 for which data are available. The results of the literature review, as well as the commissioned analyses, are reviewed below for gender and race/ethnicity.
Although improving representation of women and historically excluded groups has been a priority at the NIH and FDA and other federal agencies, the committee noted that limited systematic reporting on the state of participation in clinical trials and clinical research is accessible in the public domain. For example, although the NIH now reports clinical trial enrollment in NIH-sponsored trials by research, condition, and disease categories (starting in 2018), there are only data available for 2018 at the time of the writing of this report, which did not allow the
committee to do a longitudinal assessment of enrollment in clinical trials (NIH, 2022). Additionally, although data sets can be downloaded from ClinicalTrials. gov, the committee faced challenges with the consistency of the data reporting and could not extract demographic data from the database in a reliable fashion. The committee spoke to researchers who have published on demographic data of trials in a specific disease area using ClinicalTrials.gov, and they faced similar issues, requiring researchers to manually insert the data from ClinicalTrials.gov into their own database using a subset of trials (Ludmir et al., 2019). Since the committee was looking at trial participation across all disease areas and over time, manually entering these data would not have been possible. To do the analysis in this report, staff searched through individual NIH institutes’ biennial and triennial reports and manually entered the reported data for each from 2013 to 2018. Although this gave an idea of demographic trends over time for individual institutes, there were inconsistencies in the way the data were reported, particularly for reporting ethnicity and gaps for certain years, making the data difficult to analyze and very labor intensive. Further, several analyses have shown discrepancies between self-reported and electronic health record responses to race and ethnicity data particularly for participants who do not identify as white (Azar et al., 2012; Boehmer et al., 2002). Inaccurate reporting of race and ethnicity data impedes the ability to examine health inequities driven by the social construction of race. Therefore, enrolling participants using self-reported race and ethnicity and not guessing based on presentation is a more reliable way of reporting race and ethnicity in these databases, yet it is unknown how race or ethnicity was determined in reporting to ClinicalTrials.gov. Thus, the success of efforts to improve representation in clinical trials and clinical research is difficult to fully evaluate.
Gender Diversity in Clinical Trials
Despite the regulatory efforts to increase gender diversity in trial enrollment, evidence from the 1990s and early 2000s suggested relative underrepresentation of women and racial and ethnic minority population groups in clinical trials (Cotton, 1990; Harris and Douglas, 2000; Mak et al., 2007; Murthy et al., 2004), which persisted until 2016, when women surpassed men in their participation in clinical trials (FDA, 2020a). However, the overwhelming majority of women participating in clinical trials in the United States are white women (78 percent between 2015 and 2019), and trials routinely exclude pregnant and lactating individuals from participating (FDA, 2019).
Status of Women’s Participation in Clinical Trials
The slow progress is particularly significant given that sex differences are observed in response to some drugs, including the prevalence of adverse events (Anderson, 2005; FDA, 2011a). Recent work has confirmed the challenge of
enrolling women in some therapeutic areas: in stroke clinical trials, for instance, women have been underrepresented even after incidence and prevalence of the disease is taken into account (Carcel and Reeves, 2021), with highest underrepresentation reported in secondary prevention trials (10 percent in one study) (Strong et al., 2020).
Other data do suggest improvements in some areas. For example, somewhat optimistic results were described in a subset of trials studied by Eshera et al. (2015): in studies of drugs approved between 2010 and 2012, just 45 percent of trial participants in small molecule trials were women, but women represented 65 percent of participants in biologic trials. The authors concluded that 82 percent of trials had a study population representative of the sex distribution in the intended patient population, but that racial and ethnic minority population groups still had lower participation rates than would be representative (with 77 percent of participants white, population average 72 percent).
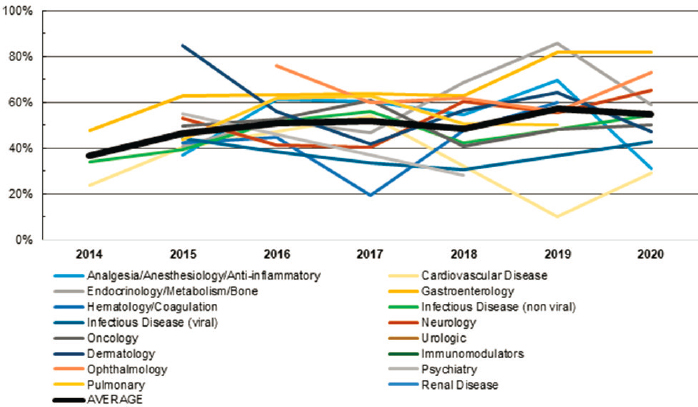
In the commissioned analysis, among drugs that have been approved by the FDA in recent years, the committee found that women represented an average of 51 percent of participants between 2014 and 2021, ranging from 37 percent in 2014 to 54.8 percent in 2020 (data for 2021 are partial only). However, women’s representation varies greatly by disease type. Prior to 2021, women represented greater than 50 percent of trial participants over at least 5 years in the areas of ophthalmology, gastroenterology, and endocrinology/metabolism/bone. However, women represent less than 50 percent of trial participants over at least 5 years in the areas of cardiovascular disease and infectious disease (see Figure 2-2). It is important to note that the participation of women may be driven by diseases and conditions that disproportionately affect women, such as osteoporosis and irritable bowel syndrome. While the committee did not examine clinical trial enrollment by specific disease burden, it is important to note that matching disease burden with trial representation is ideal, and therefore, 50 percent may not be the accurate threshold by which to measure women’s participation in clinical trials and clinical research.
The committee also found similarly positive trends in clinical research participation of women in NIH-sponsored trials. The committee found that participation of women has been steadily increasing from 2013 to 2018 for which data are available (no data were reported in 2015, but reporting requirements changed in FY 2016, resulting in an increase in participants reported across NIH institutes and centers). Across all NIH institutes and centers, mean representation of women in clinical research was 44.3 percent in 2013, 47.2 percent in 2014, 54.1 percent in 2016, 47.9 percent in 2017, and 52.4 percent in 2018 (on average 22.1 million participants were included in NIH-funded trials during each of these annual reporting periods).
As shown in Figure 2-3, among the top 10 largest institutes/centers by research enrollment (which represent 89.7 percent of enrollment across all institutes/centers), women make up at least 50 percent of participants in clinical
SOURCE: Analysis of FDA Drug Trials Snapshots as of May 2021.
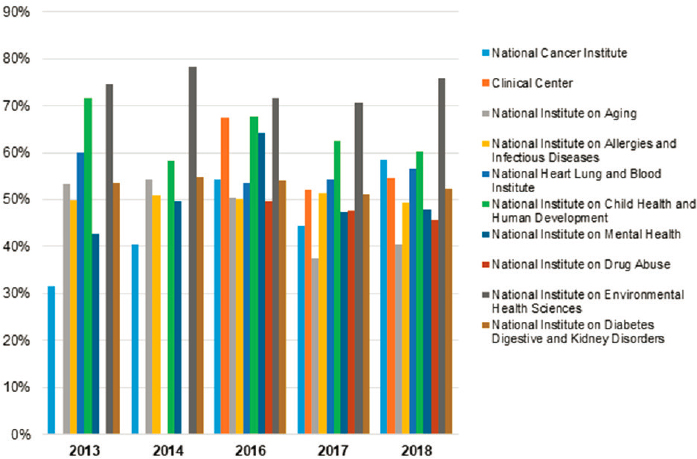
research supported by the National Institute of Environmental Health Sciences, the National Institute of Diabetes and Digestive and Kidney Diseases, and the National Institute of Child Health and Human Development across all years of reporting, and at least 50 percent of participants in at least 3 years of reporting in clinical research supported by the National Institute on Aging, the Clinical Center, the National Institute of Allergy and Infectious Diseases, and the National Heart, Lung, and Blood Institute. Across all 5 years of reporting, women never exceeded 50 percent of participants in clinical research supported by the National Institute on Minority Health and Health Disparities, the National Institute on Alcohol Abuse and Alcoholism, and the National Library of Medicine. Thus, representation of women, particularly white women, has improved in clinical research over the past decade; however, the evidence specifically on pregnant and lactating individuals, sexual- and gender-minority populations, and racial and ethnic subgroups of women is lacking (see the Racial and Ethnic Diversity in Clinical Trials section).1
Participation of Pregnant and Lactating Individuals in Clinical Trials
Nearly 4 million persons in the United States give birth every year, and 3 out of 4 gestational parents start out breastfeeding (Hamilton et al., 2021; HHS, 2022b). During pregnancy and lactation, greater than 90 percent of these individuals take at least one medication, either to treat pregnancy-related complications or to treat ongoing medical issues (NIH, 2018b). However, pregnant and lactating persons are often excluded from clinical trials and clinical research that could help them and provide better clarity on the risks and benefits of taking prescribed medications during pregnancy or while lactating. Very few drugs are approved for use during pregnancy, and most drug labels have little data on pregnancy to inform prescribing decisions (Blehar et al., 2013).
Despite federal initiatives to address this problem, pregnant and lactating individuals remain drastically underrepresented in clinical trials (Blehar et al., 2013). In a study of six clinical trial registries, just 0.32 percent of all active registered trials were focused on pregnant individuals (Scaffidi et al., 2017). Additionally, in a review of 338 Phase 3 and 4 NIH-funded actively recruiting studies in ClinicalTrials.gov, 68 percent explicitly excluded pregnant women and 47.3 percent excluded lactating women (Spong and Bianchi, 2018). Another review found that of 558 industry-sponsored studies, only 1 percent were designed for pregnant women and 95 percent excluded pregnant women (Shields and Lyerly, 2013).
One of the main reasons driving the continued lack of trials on pregnant and lactating individuals is the health risk posed to the survival of pregnant individu-
___________________
1 Unfortunately, the data the committee used for this analysis were not disaggregated by sex and race/ethnicity, so an analysis on the status of the participation of racial and ethnic subgroups of women broken down by different racial and ethnic groups is not included.
als and their offspring. This is exacerbated by the highly publicized cases where drug trials ended with tragic results, such as with thalidomide. Following some of these trials, policies were passed in 1977 that effectively excluded pregnant women from clinical trials (Becker, 2021). The FDA walked back this broad ban in the 1990s, largely thanks to AIDS activists in the 1990s, who argued the policy effectively limited their access to life-saving drugs (Brick-Hezeau, 2019). However, pregnant individuals are still largely excluded from clinical trials beyond preclinical safety assessments (NIH, 2019). The potential risk to fetuses and legal consequences of injury to children who were exposed in utero present ethical and legal considerations for industry. In addition to safety concerns, physiologic changes that occur during pregnancy and while lactating can affect drug metabolism, leading to increased complexity in a clinical trial.
A recent example of the complexity of clinical trial design with pregnant and lactating persons is the COVID-19 vaccine trials, which excluded pregnant and lactating individuals from participating. Pregnant and lactating individuals were excluded from initial COVID-19 vaccine trials for safety concerns and because including them could have complicated and potentially delayed the use of vaccines for the broader population (Szabo, 2022). In addition, because little information on the use of mRNA vaccines in pregnant and lactating individuals existed, the FDA required drug companies to complete developmental and reproductive toxicity studies before testing in pregnant people (FDA, 2011b). These initial toxicity studies take 5 to 6 months to complete, meaning they were not completed for COVID-19 vaccine trials until late 2020.
However, the exclusion of pregnant and lactating persons from COVID-19 trials was made without any evidence suggesting that vaccines are teratogenic and without any evidence that they are transmitted to breast milk, leaving many without the necessary data to make an informed decision (Van Spall, 2021). This has led to the spread of misinformation on the impacts of COVID-19 vaccines on pregnancy and vaccine hesitancy for a high-risk group (Skirrow et al., 2022).
To address this continued challenge, the 21st Century Cures Act (P.L. 144-255) established the Task Force on Research Specific to Pregnant Women and Lactating Women (PRGLAC). PRGLAC was charged with “providing advice and guidance to the Secretary of Health and Human Services on activities related to identifying and addressing gaps in knowledge and research on safe and effective therapies for pregnant women and lactating women.” The PRGLAC report, issued in 2018, includes a list of recommendations to address this issue (see Box 2-4) (NIH, 2018b). Since the report was published, the NIH has proposed an implementation plan for carrying out all of the recommendations in the report and calls on multiple stakeholders, including government, industry, clinicians, and women, to each do their part in carrying out these implementation steps (Byrne et al., 2020).
The committee recognizes that the inclusion of pregnant and lactating individuals in such trials may require special considerations, including medical
clearance of the participants, specialized informed consent, and accelerated completion of reproductive safety and toxicology data on the drug or device under study. While acknowledging the extra steps that are required, examples such as COVID-19 vaccine trials highlight the clinical and scientific grounds where such inclusion can be essential and lifesaving.
Participation of Sex, Sexual and Gender Minority Populations in Clinical Trials and Clinical Research
Sex, sexual and gender minority (SGM) populations experience significant health disparities compared with their cisgender, heterosexual peers, including higher rates of cardiovascular disease, myocardial infarction, some cancers, and HIV. They are more likely to experience violence and trauma, and they report greater anxiety, depression, and suicidality (NASEM, 2020b); which may contribute to alterations in physiology, neurobiology, and immunity (van der Kolk, 2014). Additionally, there are unique considerations related to the biological effects of gender-affirming care and medical or surgical interventions that need to be explored (Jones et al., 2020).). Given the known health disparities and biological considerations, it is important for SGM populations to be included in clinical trials and clinical research.
The committee’s search of the literature did not find much on the status of SGM participation in clinical trials and clinical research.2 There is a literature base on the barriers and facilitators to SGM participation in clinical trials and research, but the committee could find only one analysis on the participation of SGM populations in clinical trials. In a manual analysis of ClinicalTrials.gov by Chen et al. (2019), researchers found a clear increase in transgender-recruiting trials over time, from zero reported trials in 2013, gradually increasing each year up to nearly 70 in 2018.
Part of the reason the analysis of SGM individuals in clinical trials is unknown is because clinical trial registries, such as ClinicalTrials.gov, define Male, Female, and All as structured information for the gender requirement entry and do not collect information about sexual orientation. To specify further that the trial is recruiting SGM individuals, that information is included in the inclusion criteria section (Chen et al., 2019). Due to the lack of routinely collected data on SGM in research, the NIH SGM research working group has in its strategic plan to (1) expand the knowledge base of SGM health and well-being through NIH-supported research; (2) remove barriers to planning, conducting, and reporting NIH-supported research about SGM health and well-being; (3) strengthen the
___________________
2 The committee uses the NIH’s definition of sexual and gender minority (SGM), which as utilized includes lesbian, gay, bisexual, and transgender people (LGBT) as well as those whose sexual orientation, gender identity and expressions, or reproductive development varies from traditional, societal, cultural, or physiological norms.
community of researchers and scholars who conduct research relevant to SGM health and well-being; and (4) evaluate progress on advancing SGM research.
Some research initiatives have focused specifically on SGM populations due to the lack of research data in this population. One such initiative is PRIDEnet, which enrolled 13,244 SGM people and for which researchers can propose studies on data from PRIDE, or request new studies with PRIDE participants (PCORI, 2019).
The NIH 2021–2025 strategic plan to advance research on the health and well-being of SGM populations reports that SGM are a health-disparities population, proposes to provide support of new investigators to build a strong SGM workforce, and will increase projects related to SGM health (NIH, 2021b). That being said, in many cases, sexual orientation and gender identity data are not collected in research, and when they are collected they are not always done so in a standardized way.
Racial and Ethnic Diversity in Clinical Trials
Numerous studies have highlighted the lack of diversity by race and ethnicity and the lack of reporting of these demographic characteristics. Here, the committee highlights several specific studies that provide illustrative evidence of underrepresentation of specific groups in clinical trials in the past two decades.
A 2004 analysis of cancer clinical trials found that Hispanic and Black patients were 28 percent and 29 percent, respectively, less likely to be enrolled than white patients after adjustment for disease incidence, age, and other factors. The difference was largest in lung cancer, where Black patients were 39 percent and Hispanic patients were 53 percent less likely to be enrolled than white patients.
A recent study of 230 vaccine trials from 2011 to 2020 indicated that white participants tend to be overrepresented, while Black and other racial or ethnic minority participants tended to be underrepresented. The enrollment of Asian individuals was perhaps approximate to the U.S. Census estimates (Flores et al., 2021). A report on the diversity of mRNA vaccine trials for COVID-19 by the Kaiser Family Foundation has found a relatively higher share of white participants in both trials compared with the U.S. population, resulting in relative underrepresentation of Black and Asian participants. However, the participation of Hispanic adults exceeded the share of Hispanic adults in the U.S. population (Artiga et al., 2021). These results, however, originated from trial sites within (76.7 percent) and outside of the United States (notably Europe and Latin America), which may explain some of the relative overrepresentation of white and Hispanic participants.
Even recently completed trials have failed to include enrollment consistent with the distribution of disease across the population—a Phase 2 trial of crenezumab in Alzheimer’s disease with 360 participants across 83 sites in 6 countries reported 97.5 percent of participants being white, and only 2.8 percent
of all participants being Hispanic, for example (Genetech Inc., 2020). However, African Americans are about two times more likely than white Americans to develop Alzheimer’s disease and other dementias, and Hispanics are about one and half times as likely as white Americans to develop Alzheimer’s disease and other dementias (AIM, 2020).
In the commissioned analysis of the FDA Drug Trials Snapshots data, the committee found that among approved drugs, participation of white patients has ranged from 84 percent in 2014 to 73.7 percent in 2020, indicating a relatively consistent decrease in the share of white participants in trials resulting in FDA approval during this period (2021 data are yet incomplete). However, the increasing inclusion of data from international trial sites in FDA drug approvals means that this trend may not represent increases in U.S.-residing racial and ethnic minority population groups. Similarly, these data do not speak to whether the demographic distribution in a trial is reflective of the demographic distribution of those affected by the condition being studied.
NIH reporting on ethnicity and race are not always consistent (see Table 2-2), but results show a relatively stable trend of proportion of participants across racial and ethnic groups in clinical trials with the weighted average of white participants among the top 10 institutes ranging from 51.8 percent in 2013 to 60.6 percent in 2018 (this trend mirrors that of all NIH-sponsored trials, as shown in Figure 2-2). Interpretation of these data is limited because the demographic characteristics of the condition or disease under study is not included.
TABLE 2-2 Demographics of Participants in Trials Supported by NIH Centers and Institutes
| 2013 (%) | 2014 (%) | 2016 (%) | 2017 (%) | 2018 (%) | |
|---|---|---|---|---|---|
| Female | 44.3 | 47.2 | 54.1 | 47.9 | 52.4 |
| American Indian | 2.1 | 1.3 | 0.8 | 0.7 | 1.0 |
| Asian | 15.1 | 17.2 | 8.4 | 26.4 | 7.8 |
| Black/African American | 12.2 | 14.3 | 10.0 | 10.8 | 13.5 |
| Native Hawaiian/Pacific Islander | 0.3 | 0.3 | 0.6 | 0.1 | 0.2 |
| White | 52.9 | 49.5 | 49.6 | 49.9 | 60.0 |
| More than 1 race | 1.1 | 1.1 | 2.0 | 1.9 | 2.3 |
| Unknown race | 1.1 | 1.1 | 2.0 | 1.9 | 2.3 |
| Hispanic | 9.8 | 8.1 | 10.8 | 6.7 | 8.5 |
| Non-Hispanic | 86.1 | 89.6 | 62.6 | 81.8 | 76.2 |
| Unknown ethnicity | 4.1 | 2.3 | 22.4 | 9.8 | 12.0 |
| Sum of all races | 84.7 | 84.8 | 73.5 | 91.8 | 87.2 |
| Sum of all ethnicities | 100.0 | 100.0 | 95.8 | 98.3 | 96.7 |
NOTE: The full analysis is available in Appendix B.
To examine the breakdown of race and ethnicity by center, the committee examined clinical research participation for each reported racial and ethnic group sponsored by the top 10 largest NIH institutes. The data on participation were collected, aggregated, and analyzed from biennial and triennial reports provided by each of these institutes. Overall, it appears that demographic trends in NIH-funded clinical research have not changed much over the years (see Appendix B for details). However, these trends can vary widely by institute. For example, the National Institute of Allergy and Infectious Diseases reported participation of African American/Black greater than 25 percent in all years examined, while the National Cancer Institute reported just 10.5 percent at most.
























