
Health Information Technology
Health information technology (HIT) systems designed to facilitate health care delivery, management, and payment have become pervasive throughout the U.S. health care system. One of the more common forms of HIT is the electronic health record (EHR),1 which has a wide array of uses, ranging from clinical support functions, digital prescriptions, and automated medication dispensing, to functions related to billing, reimbursement, and administration, to patient safety and quality improvement (Alexander and Madsen, 2018; Cherry et al., 2011; Kruse et al., 2017; Rantz et al., 2010a; Scott et al., 2017; Shiells et al., 2019). The capabilities of HIT in effectively promoting patient safety, enhancing the effectiveness of patient care delivery, facilitating the management of chronic conditions, and improving the efficiency of health care professionals are particularly important in nursing home settings, given the characteristics of the patient population. Nursing home residents typically have complex conditions, take multiple medications, and frequently undergo transitions in care (e.g., visits to the emergency department and hospital admissions) (Vest et al., 2019). Moreover, a nursing home resident’s stay tends to be extended rather
___________________
1 Although the terms “electronic health record” (EHR) and “electronic medical record” (EMR) are often used interchangeably, they are not the same. EMRs are the traditional patient medical chart in digital rather than paper format and are typically tied to one organization. EMRs enable providers to track data over time, identify patients for preventive visits and screenings, monitor patients, and improve health care quality. EHRs go beyond EMRs in their capacity to collect and store information from all the clinicians providing care to the patient (including laboratories and specialists). Importantly, all authorized clinicians involved in a patient’s care can access the information in an EHR (ONC, 2019a). For more information, see https://www.healthit.gov/faq/what-are-differences-between-electronic-medical-records-electronic-health-records-and-personal (accessed December 1, 2021).
than episodic, with care typically lasting years rather than weeks or months. This requires more extensive ongoing communication, care coordination activities, and different HIT reporting mechanisms that can support the clinical staff in identifying, monitoring, and responding to changes in a resident’s condition over an extended period of time (Rantz et al., 2010a,b). Effective integration of HIT into care delivery has the potential to improve communication and data sharing for treatment referrals, allow providers to securely share data in real time, and provide better and more efficient care to beneficiaries (MACPAC, 2021).
Used appropriately, EHRs have the potential to prevent medical errors, expedite team decisions, reduce health care costs, increase administrative efficiencies, decrease paperwork, promote patient safety, and expand access to health care in nursing home settings (Bjarnadottir et al., 2017; Kruse et al., 2017; Lee, 2015; ONC, 2019b). Thus, members of the nursing home interdisciplinary care team, with appropriate training (DiAngi et al., 2019; Longhurst et al., 2019; Pantaleoni et al., 2015), can call upon the multiple functions of EHRs to improve the overall quality of care for nursing home residents (Spinelli-Moraski and Richards, 2013).
Other health technologies such as telehealth, videoconferencing, and personal monitoring devices are also effective tools in nursing home settings. The importance of these technologies became evident during the COVID-19 pandemic when measures such as locking down nursing home facilities to protect vulnerable residents from infection limited access to in-person clinical services as well as residents’ contact with friends and family members (Whitelaw et al., 2020). Thus, health technologies that serve dual roles as alternatives to face-to-face clinical visits as well as tools to mitigate the negative health outcomes of social isolation and loneliness have a key role to play in improving the quality of care and quality of life of nursing home residents.
This chapter of the report explores the role of HIT systems in nursing home settings, beginning with a brief background on the introduction and use of HIT in nursing homes. The discussion then turns to an examination of how HIT aligns with and supports the components of the committee’s conceptual model for high-quality nursing home care. From there, the chapter explores HIT’s role in facilitating and operationalizing the components of the committee’s model of high-quality care in nursing homes as it relates to quality measurement and improvement (Chapter 3), resident care planning (Chapter 4), and workforce productivity (Chapter 5). The discussion in this chapter will also include a review of HIT’s impact on advancing patient safety and will touch on issues related to the nursing home physical environment (Chapter 6) as well as HIT’s role in value-based payment (Chapter 7). The chapter concludes with a discussion of the use of other HIT applications, such as telehealth, during the COVID-19 pandemic.
EVOLUTION OF HEALTH INFORMATION TECHNOLOGY IN NURSING HOMES
The evidence base supporting the role of HIT systems in improving the quality of care in nursing homes has been steadily evolving over the past three decades. As discussed in Chapter 2, the Institute of Medicine2(IOM) 1986 report Improving the Quality of Care in Nursing Homes outlined many urgently needed measures to improve the quality of care in nursing homes. The committee’s extensive reform plan reflected the recognition of the significance of HIT systems for monitoring and sustaining quality in nursing home care. The report recommended developing large national datasets derived from standardized resident assessments (IOM, 1986). This recommendation led to the creation of the Minimum Data Set (MDS), a standardized instrument used in every U.S. nursing home to assess the condition of residents. As discussed in Chapter 4 and explored further below, the MDS was designed for three key purposes: to collect data to describe each resident’s condition and create individualized resident care plans, generate quality indicators to evaluate nursing homes and guide improvement efforts, and serve a reimbursement role. Notably, MDS data are also used to develop publicly reported quality measures (Rahman and Applebaum, 2009).
Subsequent IOM reports focused on the key role of HIT in improving health care quality, with a call for the widespread use of computerized patient records systems to replace paper-based patient health records within 10 years (IOM, 1991). The 2000 IOM report, To Err Is Human: Building a Safer Health System, shone a bright light on the safety issues affecting all types of health care delivery systems and promoted technology as a solution (IOM, 2000). That report recommended that all health care organizations implement computerized capabilities—such as computerized drug order entry systems—that could improve the safety of health care delivery. A subsequent IOM report also emphasized the importance of using HIT systems in long-term care facilities for clinical assessment, quality monitoring, and reimbursement (IOM, 2001a).
The steadily growing evidence base supporting the key role of HIT systems in clinical assessment, health care safety, and quality monitoring and improvement provided support for the enactment of a number of legislative actions to promote the widespread adoption of HIT throughout the health care system (see Box 9-1). The first of such legislation, the Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009, authorized $35 billion to support health care providers such as hospitals, acute care, and ambulatory care providers to implement EHRs.
___________________
2 As of March 2016, the Health and Medicine Division of the National Academies of Sciences, Engineering and Medicine (NASEM) continues the consensus studies and convening activities previously carried out by the Institute of Medicine (IOM). The IOM name is used to refer to reports issued prior to July 2015.
Notably, nursing homes were not included among the group of health care providers eligible to participate in CMS’ EHR Incentive Program,7 which was renamed Promoting Interoperability Programs8 (Adler-Milstein et al., 2016; Gold and McLaughlin, 2016). As a result, nursing homes have
___________________
3 American Recovery and Reinvestment Act of 2009, Public Law 111-5; 111th Cong., 1st sess. (February 17, 2009).
4 Improving Medicare Post-Acute Care Transformation (IMPACT) Act of 2014, Public Law 113-185; 113th Cong., 2nd sess. (October 6, 2014).
5 Medicare Access and CHIP Reauthorization Act of 2015, Public Law 114-10; 114th Cong., 1st sess. (April 16, 2015).
6 21st Century Cures Act of 2016, Public Law 114-255; 114th Cong., 2nd sess. (December 13, 2016).
7 American Recovery and Reinvestment Act of 2009, Public Law 111-5; 111th Cong., 1st sess. (February 17, 2009).
8 See https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms (accessed October 27, 2021).
not benefited from the significant financial support for EHR adoption that has been provided to other sectors of the health care system (Alexander et al., 2019a, 2020a; Kistler et al., 2021; MACPAC, 2021; ONC, 2021b; Walker et al., 2016).
Bolstered by federal financial incentives and other factors, EHRs have been adopted at a steadily increasing rate across all sectors of the health care system over the past decade. The level of EHR adoption among all nonfederal acute care hospitals was 96 percent in 2016 (ONC, 2017a), while nearly 90 percent of office-based physicians used an EMR or EHR as of 2019 (CDC, 2021a). In contrast, an Office of the National Coordinator for Health Information Technology survey estimated that as of 2016 less than two-thirds of all nursing homes had adopted an EHR (Alvarado et al., 2017). By 2019, a survey of nearly 600 nursing homes indicated the nationwide prevalence of EHR adoption among nursing homes to be 84 percent (Vest et al., 2019). Nursing homes that have not implemented EHRs continue to rely on inefficient paper-based, rather than electronic, exchange of health information. The urgency of the need for accurate, efficient exchange of health information has been underscored by the COVID-19 pandemic and its devastating effect on nursing home residents (Alexander et al., 2022).
Even those nursing homes that have an EHR in place are not necessarily taking advantage of the full benefits of EHR adoption. A lack of interoperability, or the inability to electronically share health information between different HITs such as hospital and nursing home EHRs, is a key barrier to the full and effective use of EHRs. Only a small share of the 600 nursing homes surveyed in the study referenced above indicated that they were able to perform the key functions associated with the benefits of interoperability, namely sending, receiving, searching, and integrating patients’ electronic health information across care settings. As the study authors point out, “without engagement in interoperability, EHRs risk becoming just another data silo” (Vest et al., 2019). This finding aligns with earlier research that nursing homes have not taken full advantage of their investments in health information technology (Alexander et al., 2017a). Thus, it is important not only for nursing homes to adopt HIT but also for them to ensure that HIT is used to its full capacity to foster the seamless exchange of health information to support quality care for nursing home residents.
ROLE OF HIT IN QUALITY CARE IN NURSING HOMES
As discussed in Chapter 1, the committee’s conceptual model for quality care in nursing homes (depicted in Figure 9-1) includes such key components as effective, timely, and equitable care; responsive and caring communication and collaboration; and an empowered staff that is knowledgeable, consistent, compassionate, and engages in team-based
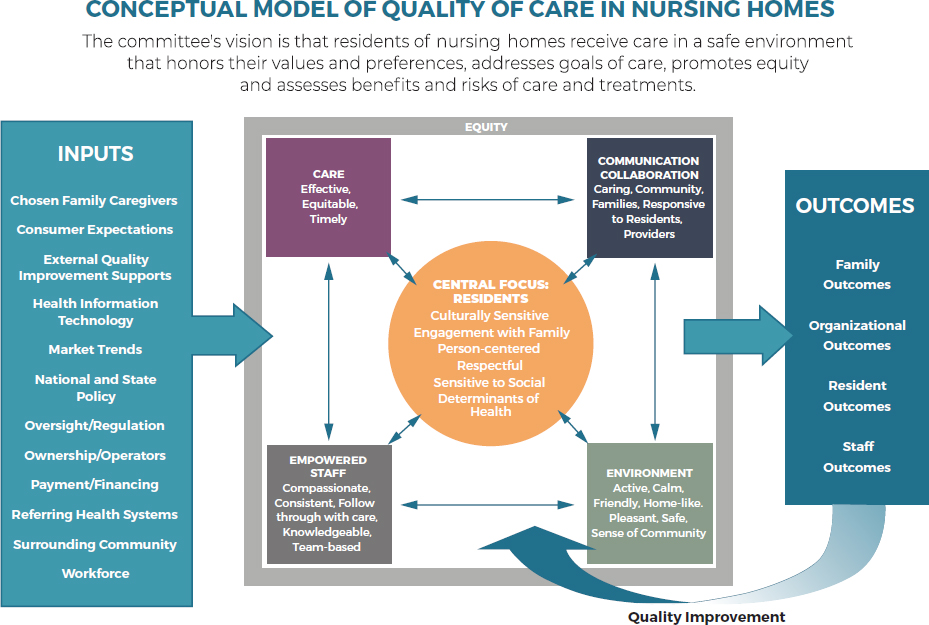
follow-through with care—all centered on providing person-centered, culturally sensitive, respectful care. As will be discussed below, HIT facilitates effective operationalization of the model’s components and, in so doing, is key to delivering quality, person-centered care in nursing homes.
The implementation of HIT in nursing homes, if done well, holds the potential to yield benefits for nursing home residents, their families, and the people who care for them. Effective use of HIT can improve the quality of care and quality of life of nursing home residents, reduce medical errors, increase the efficiency of nursing home staff, provide the data needed to drive quality improvement and quality assurance efforts, and increase person-centered care. A number of barriers to successfully implementing EHRs and other HIT systems to their full capacity in nursing homes exist, calling for greater attention to address those challenges.
Use of HIT to Support Quality Measurement
The MDS was first fully implemented nationwide in 1991 as part of the federally required process for the clinical assessment of all residents in Medicare- and Medicaid-certified nursing homes. Described as “a powerful tool for implementing standardized assessment and for facilitating care
management in nursing homes” (CMS, 2021a), the MDS enables an extensive evaluation of nursing homes, both on a facility level as well as on the level of individual resident’s characteristics such as their medical, social, and functional status (Wu et al., 2009). The required MDS information also provides data for quality measurement and improvement purposes (AHRQ, 2018a). The MDS has been updated periodically since it was first introduced, with the most recent version, MDS 3.0, released in 2010.
Although concerns have been raised about the accuracy and completeness of the MDS (Rahman and Applebaum, 2009; Wu et al., 2009), it is a key resource within the broader portfolio of data sources critical to the quality of care in nursing homes. The MDS data collected during resident assessments include information about the resident’s health and functioning and about changes in resident status. Importantly, this standardized data collection enables nursing homes to monitor the quality of resident care, and MDS data were critical to the development of quality indicators (Rantz and Connolly, 2004; Saliba and Buchanan, 2012) (see Chapter 3). The MDS provides the basis for the National Quality Forum–endorsed nursing home measures (AHRQ, 2018b).
EHRs can facilitate the effective, efficient, and accurate collection of data on nursing home residents required as part of the MDS process (Rantz et al., 2011). Indeed, the MDS serves as the basis for most commercially available EHRs for nursing home use. Effective EHR implementation can lead to quality improvement as reflected in lower deficiency scores, fewer medication errors and adverse drug reactions, improved compliance with practice guidelines, and improved resident outcomes regarding activities of daily living, among other quality measures (Alexander and Madsen, 2021; ONC, 2019b; Rantz et al., 2010a; Silow-Carroll et al., 2012). EHR implementation also has been found to contribute to improving other quality measures, such as increased vaccination rates, in nursing home settings (Bjarnadottir et al., 2017).
HIT and Quality Improvement
Given its capacity to facilitate communication between health care providers and advance patient safety across all health care settings, including nursing homes, HIT is viewed as an effective tool for improving the quality of care. Studies have explored the role of HIT in quality improvement related to patient safety, error reduction, improved communication, avoidable hospitalization, medication management, and health equity.
Harm reduction is particularly important in the nursing home setting, given that one in five Medicare beneficiaries experiences an adverse event within 35 days of admission to a nursing home. Moreover, nearly 60 percent of adverse events are preventable episodes associated with substandard
treatment, inadequate monitoring, and delays in giving or failure to give necessary care (OIG, 2014). Adverse events are defined as harm or injury resulting from medical care (including the failure to provide needed care). Examples of adverse events include falls with injury, pressure injuries, health-care–acquired infections, and adverse drug events (Kapoor et al., 2019). Such events result, in part, from missing or inadequate information about functional, mental, and behavioral status in the communications carried out at the point of nursing home admission or discharge to a nursing home (Adler-Milstein et al., 2021). Ensuring that nursing home HIT systems are linked to the broader health care system could help address such information shortcomings (King et al., 2013; Popejoy et al., 2014; Vogelsmeier, 2014).
HIT is also associated with improved communication and the documentation of risk assessments for falls, a key area of patient safety in nursing homes (discussed in Chapter 6). For example, HIT systems have been used to facilitate the collection of longitudinal data on older adults by embedding sensors in their living spaces to detect small changes in gait speed and stride length over time. These measures are used to compare older adults who had a fall versus those who did not. Studies have shown that individuals that have cumulative changes in gait speed over time (3 weeks) have a 4.2 times greater likelihood of falling than those who have not experienced changes in their gait speed (Phillips et al., 2017). More research is needed to better understand the ways in which such data can most effectively be used by the interdisciplinary team to develop successful fall-prevention strategies for older adults (Dowding et al., 2012).
HIT has also been instrumental in another area of patient safety: that of risk assessment concerning the prevention of pressure ulcers, another prevalent condition among nursing home residents (discussed in Chapter 4). HIT has been used to improve communication about evidence-based pressure ulcer prevention strategies. One study of more than 200 nursing assistants in 16 nursing homes, for example, found that sophisticated HIT systems improved the nursing assistants’ ability to pass clinical information on to other staff members, enhanced their ability to keep track of resident needs, and improved their access to clinical information overall (Alexander, 2015). Although this one study revealed a positive impact, other studies about EHR implementations and interventions using EHR data in nursing homes have demonstrated mixed impacts of technology on pressure ulcer outcomes (Dendere et al., 2021).
HIT has also shown significant promise in reducing avoidable hospitalizations and their associated costs by targeting ineffective and insufficient communication that can lead to unnecessary transfers of nursing home residents to hospitals (Ashcraft and Owen, 2017). One study of communication strategies used to reduce avoidable hospitalizations identified
improvement strategies in a range of areas, including appointment scheduling, laboratory specimen drawing and results reporting, pharmacy orders and reconciliation, communication related to social work discharge planning, and tracing admission and preadmission data (Alexander et al., 2015). In each situation, nursing home staff suggested that HIT systems would improve data use efficiency and workflow and reduce the possibility of human error–associated information transfer. The study found that when nursing homes implemented these strategies, the average hospital transfer rates declined from nearly 2.5 per 1,000 resident days in 2014 to less than 2 per 1,000 resident days in 2018 (Vogelsmeier et al., 2021).
Another example of the ways in which the effective use of EHRs can advance patient safety in nursing homes is in the area of medication management. Polypharmacy, defined as the regular use of five or more medications (discussed further in Chapter 6), provides one example of how data integration is closely linked to patient safety. Structured EHR data, when integrated with computerized physician order entry and electronic prescribing, can enable decision-support functions that can promote compliance with guidelines and alert clinicians to potential medication interactions or allergies (Krüger et al., 2011). One study, for example, found that an electronic clinical decision-support system identified 57 to 73 percent of potentially inappropriate prescribing (depending on the criteria used) in seniors with multiple conditions (Rogero-Blanco et al., 2020). A review of 20 studies concluded that EHR-enabled clinical decision-support systems were effective in reducing potentially inappropriate prescribing in hospitals, though the results in nursing home settings were mixed (Scott et al., 2018).
In addition to HIT’s potential role in advancing patient safety, it is also important to consider the role of HIT in advancing equity—another key domain of health care quality (IOM, 2001b; Lee, 2015; NASEM, 2021; NORC, 2010). As discussed in Chapter 2, the COVID-19 pandemic had a disproportionate impact on racial and ethnic minorities, both in the community (CDC, 2021b) and in nursing home settings (Gorges and Konetzka, 2021). HIT can support critical data collection and record demographic information such as race, ethnicity, and language preferences (Wyatt et al., 2016). The lack of data on race and ethnicity served as a barrier to developing targeted response efforts to the COVID-19 pandemic (Artiga et al., 2020).
Health information technology builds organizational capacity, which in turn enables nursing home staff to better identify resident care needs and track and manage care delivery processes; it also optimizes the nursing home staff’s ability to access information important for making decisions about care delivery (Alexander, 2015). However, more evidence is needed, particularly in nursing home settings, on the specific effects of information
systems components on quality measurement and quality reporting. The first step in this process would be to create sustained regular reporting mechanisms linking nursing home HIT adoption trends as a measure of quality improvement and HIT’s influence on resident, family, staff, and organizational outcomes.
HIT and Care Planning
As discussed in Chapter 4, the resident care plan developed through the use of the MDS is central to the delivery of high-quality, person-centered care in nursing homes. By providing more holistic views of individual residents, including their past as well as current needs, standardized electronic documentation of resident information advances person-centered care (Zhang et al., 2012). Studies have shown that EHRs, with some customization, have the ability to increase fidelity to person-centered care plans, which is an important component of achieving person-centered care (Stanhope and Matthews, 2019).
Given the “information intensive” nature of health care (Shiells et al., 2019), documenting resident conditions is very time consuming for nursing home staff. The use of traditional, paper-based documentation is viewed as outdated, incomplete, inconsistent, and difficult to update, and it increases the opportunity for errors and may have a negative impact on the quality of care provided. EHRs, for their part, may be used for assessment and care planning with the associated benefits of effective chronic care management, improvement in quality of care, and ability to provide person-centered care (Shiells et al., 2019). Studies have shown that nursing home staff have positive views on the use of electronic documentation for care planning (Zhang et al., 2012) and that they have found templates that provide prompts to staff to identify potential problems to be particularly useful (Cherry et al., 2011). Research has provided a robust evidence base showing that EHRs can improve the accuracy and accessibility of resident documentation and contribute to a positive impact on the quality of care (Cherry et al., 2008; Kruse et al., 2017; Meehan, 2017).
Moreover, a proactive person-centered longitudinal plan of care is critical to care coordination (Dykes et al., 2014). The EHR designs most likely to advance person-centered care and care coordination would include specialized data formats whose precise form would depend on whether a person was a receiver or sender of information. This is particularly important when patient information is shared between nursing homes and hospitals during transitions of care because nursing homes often collect very specific and unique types of clinical data related to patient outcomes, while hospitals may not. Moreover, nursing home residents have very specific care needs related to chronic health conditions and care management. Without attending to specific physical as well as cognitive care needs, the individual
may be at risk for rapid decline in function, and it is often very difficult or impossible for them to return to their former level of functional/mental abilities. While many common data elements in EHRs, such as code status, are represented across different health care settings, some unique fields (e.g., the activities of daily living collected by nursing homes) can create information gaps when one health care provider collects data, but another one does not. These differences could be addressed with an increased focus on standardizing HIT systems across the continuum of care so that the most useful data could be collected continuously and exchanged seamlessly between settings (ONC, 2017b; Skrocki, 2013; Suter et al., 2009).
Resident transitions between the nursing home and the hospital settings have been found to have missing, inaccurate, or conflicting information, which contributes to the risk of rehospitalization and inappropriate care for residents (King et al., 2013) as discussed in Chapter 6. Research highlights the importance of high-quality communication among health care professionals, including the effective use of EHRs to facilitate care transitions (Scott et al., 2017).
Advance Care Planning
As discussed, the care plan is instrumental in the delivery of person-centered care to nursing home residents. The pandemic amplified the importance of one element of care planning—advance care planning (ACP)—as nursing home residents are extremely vulnerable to contracting the life-threatening virus. ACP, a key component of end-of-life care, is associated with promoting person-centered care that reflects an individual’s values, preferences, and beliefs, preventing unwanted care as well as reducing unnecessary hospitalizations (see Chapter 4). Individual preferences for end-of-life care are captured in written documents such as advance directives. Having a complete advance care plan in place that is accessible to clinicians is essential to the provision of care that aligns with the individual resident’s preferences, values, and goals of care. The absence of an accurate advance care plan renders residents vulnerable to receiving treatment that may be aggressive and does not reflect the resident’s preferences.
Studies suggest that the use of EHRs could address challenges related to documenting advance directives and thereby provide benefits for patients, families, and providers (Lemon et al., 2019). Ideally, the EHR would include electronic triggers to prompt clinicians to have goals-of-care conversations with patients and their families. In addition, EHRs would provide templates to guide the clinician through the conversation, and would generate data for quality improvement and reporting. Most importantly, given that people transition between care settings across the lifespan, using an EHR for documenting advance directives would ensure easy access to the necessary documentation to help ensure that patients receive care that is aligned with their preferences (Lamas et al., 2018).
HIT and the Workforce
HIT has the potential to improve staff efficiency with an associated positive impact on resident outcomes. One study, for example, found that 6 months after implementation of an EHR, nurses were able to spend significantly more time engaging with patients in their rooms and in purposeful interactions and less time at the nurses’ station (Gomes et al., 2016). Using health information technology to capture resident health information in real time at the bedside can also reduce staff fatigue and the burden of relying on short-term memory, while also improving patient safety by enhancing the accuracy of the patient information (McAllen et al., 2018). Many nursing homes, however, only have computers located at central nursing stations and not close to residents’ rooms. To take full advantage of real-time patient data collection in the EHR, mobile charting platforms are required, including tablets or point-of-care mobile workstations (Edelman et al., 2020).
Using the full capabilities of an EHR can improve the collection and documentation of patient assessment information. Ideally, the collection and recording of patient data and information should occur as close as possible to the provision of patient care, which in the nursing home setting is often at the bedside. (Rantz et al., 2011). Such real-time data entry has been shown to improve patient care, allowing for quicker results of laboratory tests and medication orders and providing more decision-making support to the clinicians (Alotaibi and Federico, 2017; Kruse et al., 2015). One study identified improvements in range of motion and reduction of high-risk pressure sores associated with the implementation of a bedside EMR with the capability of prompting staff to provide necessary care (Rantz et al., 2010a). Moreover, such improved care leads to greater patient satisfaction. Finally, real-time data entry can reduce the duplication of documentation and, in doing so, contribute to clinicians’ overall efficiency (Classen et al., 2018; Gliklich et al., 2014).
Studies highlight the central role of training and education as predictors of positive workforce experience with EHRs, and emphasize that health care professionals who are not trained to use the EHR appropriately are unlikely to realize any gains in efficiency, nor will they be able to use the EHR to improve the quality of care. Research highlights not only EHR training in general, but specifically the need for initial, follow-up, and ongoing training for nursing home staff on using the EHR appropriately and to the full range of its capabilities. Additional training may have to be targeted to those nursing home staff who might lack general computer experience or who are not adept at using technology for documentation purposes (Cherry et al., 2008; Kruse et al., 2015).
Satisfaction with EHRs—on the part of clinicians as well as residents and their families—is a critically important factor in successful EHR adoption
and use. If an EHR system is not easy to use or is perceived as making more work for nursing home staff rather than decreasing their workload, it will not be used to its full potential (Staggers et al., 2018). Moreover, poor EHR usability can lead to errors, which can potentially have a negative impact on patient safety (Gardner et al., 2018; Howe et al., 2018).
HIT usability needs to be assessed in terms of HIT’s impact on resident, family, staff, and organizational outcomes as well as in terms of advancing equity and reducing disparities in nursing home care. Priority areas include the fit of the technology to tasks conducted by nursing home staff, user satisfaction, perceived workflows, and perceptions of system integration among processes of care. These issues are part of a growing area of research addressing the effect of clinician burden and burnout (Alexander and Ballou, 2018; Gardner et al., 2018; Zsenits et al., 2019).
HIT and Value-Based Payment
As discussed further in Chapter 7, the Centers for Medicare & Medicaid Services (CMS) continues to promote value-based programs as a way of advancing high-quality care and lowering health care costs. Launched in 2018, the Skilled Nursing Facility Value-Based Purchasing (SNF VBP) program awards or penalizes facilities for the quality of care provided to Medicare beneficiaries (see discussion in Chapter 7) (CMS, 2021b). Under this program, facilities are evaluated and receive incentives for improvements and achievements in hospital readmission measures, with additional measures expected to be introduced in the future. In a recent study, researchers reported that most U.S. skilled facilities were penalized nearly 1 percent of their Medicare payments in year 1 of the SNF VBP (Qi et al., 2020). Among the facilities more likely to be penalized were those that were small, for profit, and with low staffing levels. Additionally, homes located in low-income zip codes and with a high proportion of frail residents were likely to be penalized (Qi et al., 2020).
Research on nursing home responses to performance-based accountability measures, including the adoption of quality improvement changes, indicates that the strongest correlation between quality improvement changes was the implementation of EHRs and other HIT, such as clinical decision-support tools, to help frontline staff improve care delivery (Shetty et al., 2020). Another favorable care improvement approach includes incorporating standardized protocols into care delivery, which is often facilitated by electronic means (Hughes, 2008; Skrocki, 2013). Finally, the exchange of information with community providers was another strategy adopted by skilled nursing facilities to improve their performance levels (Adler-Milstein et al., 2021; Rahman et al., 2018).
Interoperability and Health Information Exchange
Many nursing homes lack the core competence or resources to make the most effective use of EHRs and other forms of HIT beyond using them for billing and reporting purposes. Moreover, getting information from other health care providers, such as hospitals, primary care providers, and clinical laboratories, into the EHR in a readily usable form remains a challenge. EHRs are typically facility specific, located within hospitals, physician practices, and pharmacies, but they are generally not interconnected to enable the seamless flow of health information across various health care settings. This lack of connectivity is a particular problem for the care of nursing home residents. Nursing home residents often have multiple complex medical conditions, which require effective care coordination to ensure safety and quality of care as the individual transitions among different health care settings (Brownell et al., 2014; Carroll et al., 2020; Grabowski et al., 2007; Jung et al., 2016; Lee, 2015; Mor et al., 2010; Rantz et al., 2010a,b; Unruh et al., 2013a,b; Wang et al., 2011).
Interoperability and health information exchange (HIE) are often used interchangeably but are two distinct components involved in advancing the HIT ecosystem to the point where there is efficient and effective collaboration and coordination of care among health care providers and across settings of care. HIE allows patients as well as health care providers to access and share medical information electronically in a secure manner (ONC, 2019d). Interoperability is defined as the ability of two or more HIT systems to not only exchange information, but to be able to use the information that has been exchanged. While HIE is necessary, it is, in and of itself, not sufficient for interoperability.9
Among the approximately two-thirds of nursing homes that had EHRs in 2017, less than 20 percent were capable of integrating patient health information from other health care organizations (Henry et al., 2018). The absence of this capability is a significant barrier to the real-time exchange of patient information (Powell and Alexander, 2021). Some nursing homes, however, have adopted HIT systems with the capability of supporting HIE (Adler-Milstein et al, 2021; Alexander et al., 2019b). These tend to be larger urban nursing homes with 100 beds or more and with higher staffing levels as well as those affiliated with a chain of nursing homes (Zhang et al., 2016).
Research has identified enhanced communication, increased effectiveness of care, and patient safety as being among the benefits of HIE implementation, and workflow integration has been shown to be a key facilitator of HIE (Kruse et al., 2018). A key barrier is that laboratory results and
___________________
9 See https://www.healthit.gov/buzz-blog/meaningful-use/interoperability-health-information-exchange-setting-record-straight (accessed January 26, 2022).
hospital discharge records are often transferred, if at all, as PDF files that are difficult for clinical staff to use and impossible to track (Alper et al., 2021; Kruse et al., 2018). Reaching the full potential of an interoperable data exchange could improve both the quality of care and the safety of residents (Kruse et al., 2018).
The use of HIE to improve and support communication and care delivery, together with full-time embedded advanced practice registered nurses and a focus on early-illness detection and end-of-life care, were the three key elements of the Missouri Quality Initiative, a CMMI demonstration project whose goal was to reduce avoidable hospitalizations among nursing home residents (discussed in Chapter 3). The 8-year effort resulted in a 40 percent decrease in hospitalizations (for any reason) and a nearly 60 percent decrease in potentially avoidable hospitalizations. HIE facilitated staff access to detailed resident health information, enabling staff members to monitor patient progress more effectively and to identify signs of possible problems, which helped to reduce avoidable hospitalizations (Ingber et al., 2017; Rantz et al., 2017a).
Policy Measures to Advance the Use of HIT
Recognizing that significant shortcomings exist related to HIT infrastructure, data flow, security, and interoperability among health systems, CMS has sought to use policy measures to encourage the use of EHRs for the exchange of clinical information between health care settings. For example, the Interoperability and Patient Access final rule went into effect in July 2021; it requires hospitals with certain EHR capabilities to send admission, discharge, and transfer data to other providers (CMS, 2021c). This rule aims to advance interoperability through application programming interfaces (APIs)10 to facilitate and expand access to health information.
CMS is collaborating with the Office of the National Coordinator for Health Information to establish a Trusted Exchange Framework and Common Agreement11 to develop a nationwide network that supports the use of technology to streamline processes of care and payment (HHS, 2022). Additionally, CMS is working with standards-based organizations
___________________
10 “The CMS regulations include policies which require or encourage payers to implement Application Programming Interfaces (APIs) to improve the electronic exchange of health care data—sharing information with patients or exchanging information between a payer and provider or between two payers. APIs can connect to mobile apps or to a provider electronic health record (EHR) or practice management system to enable a more seamless method of exchanging information” (CMS, 2021c).
11 See https://www.healthit.gov/topic/interoperability/trusted-exchange-framework-and-common-agreement-tefca (accessed January 26, 2022).
(i.e., HL7) using Fast Healthcare Interoperability Resources,12 to promote transparency and exchange among providers, payers, and patients, which could enable important discussions about cost and the value of care among these stakeholders.
The inclusion of EHR-based clinical quality measures for nursing homes in Medicare’s Meaningful Measures Initiative13 serves as an impetus for nursing homes to use the EHR to its full capability, while the 21st Century Cures Act focuses on advancing HIE capabilities14 provided additional policy support (Vest et al., 2019). As nursing homes increasingly use new measures to assess HIT adoption and interoperability, such information can be made publicly available in Care Compare (Adler-Milstein et al., 2020a; Bjarnadottir et al., 2017; Enyioha et al., 2021; Kistler et al., 2021; Kruse et al., 2017; Powell et al., 2021; Vest et al., 2019).
CHALLENGES OF HIT ADOPTION AND USE IN NURSING HOMES
The adoption, implementation, and effective use of EHRs in nursing home settings face significant challenges. Key barriers include cost, adequate staff training, clinician burden and workload, the interoperability of information systems, and disparities in uptake and infrastructure (Alexander et al., 2017b,c; Zhang et al., 2016).
Financial Barriers
Studies have demonstrated that there are significant costs associated with the adoption of HIT such as EHRs (Kruse et al., 2015; Rantz et al., 2010a). Moreover, it is important to consider that it is not only the initial cost of adopting an EHR—regular maintenance and required technology infrastructure upgrades also represent a considerable expense for nursing homes (Filipova, 2013; Holup et al., 2013; Kruse et al., 2015; Phillips et al., 2010; Resnick et al., 2009). As noted above, nursing homes were not eligible for the federally funded incentives to help cover the costs of EHR adoption. This ineligibility for financial support is critical, as costs represent a key barrier to EHR adoption in nursing homes (Abramson et
___________________
12 See https://www.healthit.gov/topic/standards-technology/standards/fhir-fact-sheets (accessed January 26, 2022).
13 For more information see https://www.cms.gov/Medicare/Quality-Initiatives-PatientAssessment-Instruments/QualityInitiativesGenInfo/MMF/General-info-Sub-Page (accessed December 1, 2021).
14 For more information, see https://www.federalregister.gov/documents/2020/05/01/2020-07419/21st-century-cures-act-interoperability-information-blocking-and-the-onc-healthit-certification (accessed December 1, 2021).
al., 2014; Cherry et al., 2008; Vest et al., 2019; Wang and Biedermann, 2012).
If incentives are offered to high-performing nursing homes to encourage the adoption of quality improvement strategies involving EHRs, these funds might potentially serve to offset the costs of EHR implementation. However, lower-performing nursing homes that do not receive any incentives may experience wider disparities in resident outcomes due to the inability to fund similar quality improvement strategies (Bjarnadottir et al., 2017; Kruse et al., 2015).
Clinician Burden
Another challenge to broader adoption of HIT in nursing homes is the impact of EHR use on the workforce. Issues that shape the impact of EHRs on nursing home staff and their ability to develop, implement, and monitor resident care plans include the management of documentation, the time consumed using the EHR, and effect of EHR use on productivity (e.g., time spent with patients). These elements have been identified as important factors in clinician burden and burnout related to the use of EHRs (Adler-Milstein et al., 2020b; Alexander and Ballou, 2018).
One example of clinician burden is the phenomenon known as EHR alert fatigue. The structured format of an EHR enables developers and administrators who oversee EHR implementation to add various clinical decision-support tools that can recommend specific actions or warn the EHR user of a potential issue using an electronic alert. Alerts can be very beneficial, helping busy clinicians to identify potential changes in a patient’s condition (e.g., a laboratory value that is out of bounds) that need to be addressed. This is particularly important given the prevalence of polypharmacy among nursing home residents.
However, while alerts can improve care processes, alerts can be burdensome and lead to clinicians ignoring them—for example, nearly one in four medication orders generate an alert (Saiyed et al., 2017). In fact, alert override can become a habitual behavior, rendering clinical decision-support systems significantly less useful (Ancker et al., 2017; Baysari et al., 2017). Given the scope of this problem, researchers have developed processes for better managing alerts to increase their effectiveness and reduce alert burden. One approach uses targeted deactivation of low-quality or low-effectiveness alerts (Simpao et al., 2015), while another approach is to make alerts silent to start, compile data on alert performance, and use that information to inform alert implementation decisions (Saiyed et al., 2017). Some investigators have suggested developing adaptive clinical decision-support tools that learn from a clinician’s behavior and filter alerts accordingly (Lee et al., 2014). Ethical
frameworks have been proposed to guide the development and implementation of these and other types of EHR capabilities to articulate the appropriate use of these systems, and incorporate processes for monitoring data quality and ensuring the security of patient data (Evans and Whicher, 2018).
Although HIT has the potential to improve staff productivity and workflow, such improvements can be offset by duplicative efforts such as staff using paper documentation in addition to use of the EHR. Other factors that impede HIT use by nursing home staff include the lack of embedded decision support and the lack of standardized language. A number of studies have identified workarounds used by staff, which are associated with errors in documentation as well as in clinical care (Hudak and Sharkey, 2007; Vogelsmeier et al., 2008). Other barriers include the lack of appropriate HIT expertise within the nursing home staff as well as the designation of HIT management to staff members who have other roles and training outside the scope and experience of managing a HIT system (Alexander et al., 2020b).
HIT that is designed well and takes into account the human factor is thought to build upon organizational capacity by enabling nursing home staff to better identify resident care needs, to track and manage care delivery processes, and to access needed information for making decisions about care delivery (Alexander, 2015; Alexander and Staggers, 2009). Research is increasingly focused on the importance of human-centered designs to address the low rates of clinician satisfaction with HIT and the perception on the part of clinicians that technology should help to manage their workload, not add to it (Carayon and Hoonakker, 2019).
Lack of Standardized Language
An additional challenge is the variation in the language used to document care practices between health care organizations. Variations in content and formatting affect the utility of resident’s medical records, and various studies have concluded that medical records do not accurately reflect the patient’s condition or care provided, which makes it more difficult to evaluate health care services (Skrocki, 2013). One way to improve the ability of EHRs to improve care is to design systems that reap the benefits of standardization in terms of more accurate, precise, and up-to-date information transfer among all members of the interdisciplinary team. A standardized language across the continuum of care will enable the continuous retrieval and analysis of documentation over time and across care settings to improve quality, support evidence-based practice, and achieve desired outcomes (Keenan et al., 2008; Lundberg et al., 2008).
Training
Research has identified insufficient staff training as one key HIT implementation challenge. Nursing homes have not made sufficient investments in staff training in all aspects of EHR adoption and use, nor has training been ongoing after the initial adoption of the EHR (Cherry et al., 2008; Ko et al., 2018; Kruse et al., 2015, 2017; Longhurst et al., 2019; Vest et al., 2019). Studies have found staff dissatisfaction related to the limited amount of time devoted to HIT training (Fossum et al., 2011; Meehan, 2017). Staff describe situations in which they received one single training session, the duration of which ranged from 30 minutes to an all-day session, with single training sessions of a half hour or less for certified nursing assistants or personal care aides (Ko et al., 2018). One study did show staff satisfaction with training in which the staff in the study received multiple days of training (Yu et al., 2008). Researchers have emphasized the need for policy makers and health systems to make incentives and other funds available to support HIT training and technology infrastructure in nursing homes (Ko et al., 2018).
Interoperability
The ability of nursing homes to share patient data about residents as they transition from the hospital to post-acute care settings is critical to the health care professionals who are responsible for care coordination and post-acute care. Estimates indicate that, overall, only half of all EHR systems are capable of transferring medical records to other EHR systems (Kistler et al., 2021; Powell et al., 2021; Vest et al., 2019). One study of nearly 800 acute-care hospitals, for example, found that fewer than half of the hospitals had an EHR portal through which long-term care facilities could access hospital information. Moreover, less than half of all hospitals had a portal through which hospitals could send information electronically to long-term care facilities (Adler-Milstein et al., 2020a). Other studies have pointed to shortcomings related to the information-sharing capabilities of EHRs. One study, for example, examined information sharing among nearly 500 nursing homes paired with hospitals. The study found that key information on residents’ functional, mental, and behavioral status as well as on the identification of the specific individual to contact at the hospital with follow-up questions was often missing, delayed (often arriving after the patient), and difficult to use (Adler-Milstein et al., 2021).
Interoperability is a challenge for the entire health care system, one that the HITECH Act and the 21st Century Cures Act of 202015 have attempted to address. These two initiatives have had limited success, however, because
___________________
15 21st Century Cures Act of 2020, Public Law 114-255 (December 13, 2016).
of technical, policy, governance, and funding issues; the proprietary policies of EHR vendors; and security and privacy concerns (Adler-Milstein and Pfeifer, 2017; Powell et al., 2021; Ratwani et al., 2018). Incomplete and inconsistent information in EHRs from multiple sources, inconsistent language use in EHRs, organizational resistance to sharing data, the high cost of hiring specialists to manage interoperability, information that is not shared in a timely manner, and inadequate investment in preparation, infrastructure, and training are significant barriers to achieving meaningful interoperability (Adler-Milstein et al., 2021).
Disparities in HIT Adoption
Another challenge is related to the uneven levels of HIT adoption across nursing homes. Studies exploring the use of HIT in rural and urban nursing homes, for example, have found that nursing homes in larger, more populated areas are more likely to have more extensive HIT capabilities, use, and integration than nursing homes in less populated regions of the country (Alexander et al., 2017b, 2020c). In addition to geographic location, other nursing home characteristics that have an impact on HIT development, implementation, and use include size, staffing ratios, payer mix, and financial model (Kistler et al., 2021).
HIT adoption by nursing homes in urban areas has enabled the improved integration of clinical data into laboratory and pharmacy systems. Lower rates of HIT adoption in nursing homes in rural areas, in contrast, might lead to greater disparities in care delivery, leaving rural nursing home residents increasingly vulnerable to poor outcomes. One analysis, for example, found that 60 percent of resident care systems in rural nursing homes are not at all able to interface with external entities’ computerized systems, including those found in clinics, clinical laboratories, hospitals, and other nursing homes, reducing those nursing homes’ capacity for health data sharing (Powell et al., 2021). Qualitative interviews conducted with administrators from these nursing home facilities identified privacy and security concerns, transparency and control, fear of lawsuits, and organizational factors as key barriers slowing the uptake of technology (Powell et al., 2021). Identifying HIT adoption standards across nursing homes may help reduce HIT inequities and disparities both within and across facilities (Kistler et al., 2021).
Infrastructure
HIT, including EHRs and virtual telehealth applications, is a resource that can enhance access to health care services and improve equity, but only if adequate infrastructure (e.g., high-speed broadband access) and resources (e.g., knowledgeable staff) are available to support the use of
the technology. However, nursing homes in rural areas of the country face numerous inequities in access to these HIT resources compared with their urban counterparts. These differences can lead to negative health outcomes. For example, older adults who live in nursing homes in urban areas have better access to specialized health care providers than those in rural areas. Recent studies have shown that HIT can support health systems in advancing health equity (Brewer et al., 2020), with at least one research team developing a digital health equity framework (Crawford and Serhal, 2020).
Limited Internet access, lack of wireless connectivity, and poor integration of HIT systems are major issues reported in studies. Poor Internet connectivity and wireless “dead zones” throughout a nursing home are identified as major barriers to the successful use of HIT (Alexander et al., 2007; Meehan, 2017). A study of nearly 900 nursing home clinicians found that while nearly 90 percent of those surveyed reported having used EHRs, only 72 percent indicated that their facilities had a wireless network (Enyioha et al., 2021). In the absence of wireless networks, nursing home staff may develop temporary approaches known as workarounds16 to bypass inefficiencies. Such workarounds can involve a range of actions that might present temporary “fixes” to workflow obstacles, but they may result in negative consequences in terms of resident safety and quality of care, which in turn can lead to poor outcomes for residents (Kandaswamy et al., 2021).
HIT AND THE COVID-19 PANDEMIC
Nursing homes used health information technology during the COVID-19 pandemic in a number of ways, including to enhance the surveillance of outbreaks and the responses to those outbreaks.17 The Centers for Disease Control and Prevention (CDC), for example, implemented the National Healthcare Safety Network to support the nation’s COVID-19 response. This mandatory electronic reporting and surveillance system enabled long-term care facilities to assess and report COVID-19 impacts, including statistics related to rates of positivity and mortality (CDC et al., 2021; ODPHP, 2022). Results are made available in an electronic dashboard.
___________________
16 EHR workarounds are defined as “behaviors that may differ from organizationally prescribed or intended procedures. They circumvent or temporarily ‘fix’ an evident or perceived workflow hindrance in order to meet a goal or to achieve it more readily” (Debono and Braithwaite, 2015, p. 27; see also Boonstra et al., 2021; Debono et al., 2013). Workarounds in the EHR context “can involve skipping prescribed steps, entering data that should be entered by others, or registering activities later in the EHR system rather than letting the system guide these activities” (Boonstra et al., 2021, p. 2; see also Azad and King, 2008; Blijleven et al., 2017).
17 See https://www.cdc.gov/nhsn/index.html (accessed January 26, 2022).
EHRs contain many important data elements that can support an effective response to a viral outbreak (Atreja et al., 2008; Kukafka et al., 2007). Nursing home staff with EHR capabilities used their EHRs to monitor resident symptoms and vital signs and developed electronic dashboards to track and report resident and staff COVID infections (Andersen et al., 2021). Staff also used telehealth and other technologies, as discussed below.
Telehealth
Telehealth (defined in Box 9-2 below) has been used across all sectors of the health care system, including nursing homes, for decades (Grabowski and O’Malley, 2014; Hui et al., 2001; IOM, 1996). In many ways, nursing homes represent ideal settings for the use of telehealth services. Although the medical needs of residents have grown increasingly complex over time,
nursing home clinicians may be on site at the nursing home on an intermittent basis, creating challenges that can contribute to misdiagnoses, delayed diagnoses, overuse of emergency department visits, and avoidable hospitalizations (Driessen et al., 2016, 2018a).
Research has shown telehealth in nursing home settings to have a variety of potential benefits, such as expanding access to care, addressing gaps in coverage, reducing the burden on staff, improving resident outcomes, and achieving cost savings. Studies have also found clinicians, residents, and family members agree about the benefits of telehealth for patient care (Edelman et al., 2020; Groom et al., 2021). These results build on earlier studies that found benefits of telehealth—in terms of both clinical efficacy as well as cost savings—for the delivery of certain specialty services, such as dermatology, geriatrics, and psychiatry, to nursing home residents (Wade et al., 2010). The potential benefits and challenges of telehealth use for nursing home residents, families, and clinicians are summarized in Table 9-1.
The use of telehealth as a viable modality for health care delivery accelerated dramatically after March 2020, when CMS, under a public health emergency waiver, removed existing barriers to telehealth services.18 This policy change, which enabled nursing homes and other health care providers to be reimbursed for telehealth visits at the same rate as a
TABLE 9-1 Potential Benefits and Challenges Associated with Telehealth Use in Nursing Homes
| Potential benefits of adopting telehealth | Potential challenges to adopting telehealth |
|---|---|
| Enable residents to avoid exposure to infectious disease, and to avoid the stress associated with transportation to and from appointments outside of a facility Improve access to care/providers Improve efficiency for clinicians (e.g., less time spent traveling to nursing homes) Improve communication between nursing home staff and providers Provide opportunities for early intervention Provide opportunities to include family in care of the resident Reduce hospital readmissions |
Greater difficulty building the resident–provider relationship Variability in implementation, use, and integration of different software/platforms/devices used for telehealth visits Lack of available, integrated, and interoperable data Delays in follow-up care of nursing home residents Increased burden for nursing home staff |
SOURCE: Powell and Alexander, 2021.
___________________
18 For more information, see https://www.cms.gov/About-CMS/Agency-Information/Emergency/EPRO/Current-Emergencies/Current-Emergencies-page (accessed November 23, 2021).
face-to-face visit (CMS, 2020), was implemented to facilitate the provision of care remotely while simultaneously keeping nursing home residents, staff, and clinicians safe through social distancing. Regulations had previously limited the reimbursement for telehealth services to rural nursing homes as originating sites of care. In addition, CMS developed a telehealth toolkit to provide guidance to health care facilities in the use of telehealth19 (CMS, 2020; Gillespie et al., 2020). Telehealth was found to be a critical tool to assist nursing homes to provide high-quality care in the context of an underresourced workforce spread thin by the heightened challenges of caring for vulnerable older adults during the pandemic (Jen et al., 2021), though there were challenges arising from limited workforce and resident training.
Research has found that virtual care reduced stress for residents and increased access to services, but that it also worsened social isolation and caused confusion among some patients (Powell and Alexander, 2021; Seifert et al., 2020).
However, telehealth allowed the provision of remote clinical care by both primary care physicians and specialists (Jen et al., 2021; Powell and Alexander, 2021), which enabled nursing home staff to preserve limited supplies such as personal protective equipment (PPE) (Edelman et al., 2020) (as discussed further in Chapter 6).
Significant variation exists in the use of telehealth services by nursing homes. A study based on survey results of a random sample of over 700 nursing homes found that 79 percent of nursing homes reported partial implementation of telehealth, 16 percent reported no telehealth use, and only 5 percent reported the maximum use of telehealth.20 Though telehealth use did not vary by ownership type, the use was lower for nursing homes in rural areas. Overall, the majority of nursing home administrators reported low use of telehealth relative to other health care settings, despite the supportive policy environment (Alexander et al., 2020c). One study found that geriatric, psychiatric, and palliative care telemedicine consults were the most common in nursing homes during the COVID-19 pandemic (Groom et al., 2021). A 2018 survey found that the providers showing the highest level of interest in telemedicine consults for nursing home residents were in the areas of dermatology, geriatric psychiatry, and infectious disease (Driessen et al., 2018b).
Despite the relatively limited overall use of telehealth, the study found
___________________
19 For the toolkit, see https://www.cms.gov/files/document/general-telemedicine-toolkit.pdf (accessed November 8, 2021).
20 Nursing home respondents completed surveys between January 2019 and August 2020, which, according to the study authors, provides a comparison of pre- and post-telehealth expansion use (Alexander et al., 2020c).
that compared with the pre-expansion period (prior to March 6, 2020), nursing homes were more likely to use telehealth for a number of discrete tasks. For example, nursing homes were more than 11 times more likely to use telehealth for evaluating residents and making pre-transfer arrangements and more than four times more likely to use telehealth for second opinions and consultations in the post-expansion period, compared with the pre-expansion period. The study also found that nursing homes were nearly three times more likely to use telehealth to access radiology results and for reporting activities (Alexander et al., 2020c).
Given the potential of telehealth to reduce social isolation and preserve limited PPE in the early phases of the pandemic as well as to enhance clinical decision making and medication order entry, the low rates of telehealth use are viewed as a missed opportunity to improve the quality and safety of care in nursing homes (Alexander et al., 2020c). The limited use of telehealth in nursing home settings may be due to factors such as inadequate infrastructure, limited scientific evidence on the effectiveness of telehealth interventions to improve outcomes, concerns about the discontinuation of policies supporting telehealth billing, insufficient training and support, and the competence of workforce (Alexander et al., 2020c; Ko et al., 2018).
HIT to Counter Social Isolation
The restrictions imposed by nursing homes in response to the COVID-19 pandemic intensified feelings of social isolation and loneliness among nursing home residents who were unable to see friends and family members for long periods of time. Research has documented the negative impact of social isolation and loneliness on residents’ health, well-being, and quality of life (Kemp, 2020; Ruopp, 2020; Simard and Volicer, 2020). The known health impacts include cognitive decline, depression, and anxiety (NASEM, 2020). The longer-term impacts of social isolation for nursing home residents can also include rapid functional decline, pressure injuries due to limited mobility, dehydration and malnutrition, and a sense of hopelessness. Measures taken during the pandemic to protect residents and staff by limiting outside visitors were particularly severe for residents with dementia, as their cognitive impairments made it extremely difficult to understand significant changes in their routines, including not having regular visitors (Edelman et al., 2020).
Given the serious health risks associated with social isolation and loneliness, it is critical to understand the potential of various health technology applications and ways to facilitate their use in nursing home settings to ensure residents remain connected with family and friends. While some research suggests that socially assistive robots may be helpful to address social isolation in nursing homes (Bemelmans et al., 2012), the applications
do not necessarily have to involve complicated technologies. One program developed during the pandemic, for example, arranged weekly phone conversations between medical school student volunteers and older adults in nursing homes. Initial reports highlight the program’s potential as an effective intervention to increase social connection among nursing home residents during the pandemic (van Dyck et al., 2020). For a resident’s perspective on the impact of visitation restrictions in nursing homes as a result of the COVID-19 pandemic, see Box 9-3.
Other interventions involve applications that are more complex. The use of video technology, for example, is particularly helpful to nursing home residents with hearing impairments who compensate for their limited or lack of hearing by lip reading and using visual cues. Relying on such movements is not possible when the individual speaking to them is wearing a mask, but video connection renders a mask unnecessary. Other options include video-enabled rounding of nursing home residents who may require reminders to eat or drink or who are in need of company while eating their meal (Edelman et al., 2020).
OTHER HIT CONSIDERATIONS FOR QUALITY IMPROVEMENT
As discussed in Chapter 4, the committee based its approach to exploring needs-based care in the nursing home setting on a combination of models, including Maslow’s hierarchy of needs. Interestingly, HIT can support an individual nursing home resident’s progression through each level of Maslow’s hierarchy from basic needs to self-actualization. For example, warmth and comfort in an older person’s residence are basic needs at the physical and physiological level that innovative HIT devices can address.
Smart wearable sensors, for instance, can detect body temperature fluctuations and send an electronic message to a caregiver in situations when a nursing home resident has an abnormal temperature (Chan et al., 2012).
In the higher levels of Maslow’s model, networking innovations such as social robots, which respond to touch sensations, may help address issues of isolation and loneliness in older adults living alone (Alonso-Martín et al., 2017). Devices that support greater freedom of choice and mobility within the community may help older adults remain independent and maintain a greater sense of self-esteem. For example, global positioning systems can support autonomy, independence, and safety for older adults with dementia by providing information about their location to caregivers (Øderud et al., 2015). These technological innovations, many of which are newly available or still in development, represent important opportunities to enhance the quality of care and improve the quality of life of nursing home residents.
Assistive Health Technologies
Various assistive technologies, such as remote monitoring systems and interactive therapeutic robots, are increasingly being used in nursing home settings to improve quality of care and quality of life (Birks et al., 2016; McGlynn et al., 2014; Moyle et al., 2017a,b).
Use of Remote Monitoring and Robotic Technology
Applications that support remote monitoring technology have begun to change the landscape of long-term care delivery and improve nursing home resident outcomes. Remote monitoring systems use devices that can connect to the Internet (e.g., using wireless connectivity), allow objects to move around independently, and monitor and capture medical and other health data from patients and electronically transmit this information to health care providers for assessment (Adler-Milstein et al., 2021). Such information sharing is leading to new relationships and the strengthening of existing ones among multiple stakeholders, with the ultimate goals being to enhance and sustain quality improvement initiatives, align financial incentives to reduce costs, and improve care coordination activities (Carroll et al., 2020).
Other sophisticated remote monitoring innovations can improve nursing home resident safety and alert staff to medically significant physiologic changes. For example, radar and other sensing devices are able to
- Assist in detecting falls by nursing home residents,
- Provide automatic alerting mechanisms with early notifications sent to nursing home staff when a resident is alone in a room (Su et al., 2018),
- Detect change in activities of daily living and mobility resulting from worsening heart conditions, detected by wearable or non-wearable sensors (Despins et al., 2020), and
- Detect early changes in health status triggered by data from sensors, such as those that detect blood pressure change, heart rate, and respiratory rate, embedded in the residents’ living environment (Rantz et al., 2012, 2017b; Su et al., 2019).
Robotic therapy provides an additional option for the use of technology in nursing home settings and may potentially represent an innovative approach to providing care to the large and growing share of nursing home residents diagnosed with dementia. A systematic review and meta-analysis of robotic therapy research on adults with dementia found that such therapy significantly decreased agitation and increased social interaction, though it did not have a significant effect on depression, anxiety, cognitive status, or quality of life (Ong et al., 2021).
Robots can also be used to help older adults maintain independence by assisting with health monitoring tasks (e.g., taking blood pressure and providing medication reminders), instrumental tasks (e.g., housekeeping) (Louie et al., 2014), and the manipulation of objects (e.g., retrieving belongings) (Gerling et al., 2016; Grönvall and Verdezoto, 2013; Lee and Dey, 2011). Other types of robots can assist staff with tasks such as lifting patients and delivering necessary care equipment and can also alert the staff of emergencies (Purtill, 2019). There is also recent interest in the potential for robots to provide social connection and support to the decreasing workforce (Girling, 2021; Philipson, 2021; Purtill, 2019).
Regardless of how promising these and other future innovations might be for the nursing home setting, developers and implementers of assistive technologies need to consider the impact of these innovations on clinician workflow, burden, and satisfaction. Moreover, it is critically important to evaluate on a systematic basis the effect of these tools on nursing home residents’ quality of life, comfort, and satisfaction, including concerns for privacy and the loss of human connection (Gerling et al., 2016; Girling, 2021).
Implementing HIT in nursing homes, if done well, has the potential to yield extensive benefits for nursing home residents, their families, and the people who care for them. Effective use of HIT can improve the quality of care and quality of life of nursing home residents, reduce medical errors, increase the efficiency of nursing home staff, and provide the data needed to drive quality improvement and quality assurance efforts, and increase person-centered care. While there are a number of barriers to successfully implementing EHRs and other HIT systems in nursing homes, research has identified potential approaches to addressing those barriers. As the demand for long-term care services increases with the aging of the population, it
becomes ever more critical to identify the most appropriate uses of HIT and provide the training and support to use HIT to address the needs of older adults and other individuals who receive care in nursing homes.
KEY FINDINGS AND CONCLUSIONS
- Health information technology (HIT) in the nursing home setting plays a key role in enabling the components of the committee’s conceptual model by
- promoting person-centered care,
- improving documentation for the resident’s care plan,
- facilitating communication between health care providers across settings of care,
- improving the safety of health care delivery (e.g., by reducing harmful errors),
- supporting the delivery of personal health care services and managing chronic conditions, and
- monitoring and sustaining quality.
- The long-term care sector has a different model of care delivery than acute care. A nursing home resident’s length of stay is typically much longer than that of a patient in acute care, which requires extensive ongoing communication, care coordination activities, and different HIT reporting mechanisms to support, maintain and improve the resident’s physical and mental functioning over time.
- HIT implementation in nursing homes, if done well, has the potential to yield far-reaching benefits for nursing home residents, their families, and the people who care for them.
- Nursing homes have not had the financial support granted to other health care providers, given their ineligibility to participate in the federal EHR incentive program.
- The adoption, implementation, and effective use of EHRs in nursing home settings face significant challenges, including cost, adequate staff training, clinician burden and workload, the interoperability of information systems, and existing nursing home infrastructure.
- Health technologies such as telehealth, videoconferencing, and personal monitoring devices are also effective tools in nursing home settings.
- Other health technology innovations to improve care in nursing homes include wireless remote monitoring devices that can collect data about residents (e.g., humanoid robots), as well as radar and other sensing devices.
REFERENCES
Abramson, E. L., S. McGinnis, J. Moore, R. Kaushal, and HITEC Investigators. 2014. A statewide assessment of electronic health record adoption and health information exchange among nursing homes. Health Services Research 49(1 Pt 2):361–372.
Adler-Milstein, J., and E. Pfeifer. 2017. Information blocking: Is it occurring and what policy strategies can address it? Milbank Quarterly 95(1):117–135.
Adler-Milstein, J., S. C. Lin, and A. K. Jha. 2016. The number of health information exchange efforts is declining, leaving the viability of broad clinical data exchange uncertain. Health Affairs 35(7):1278–1285.
Adler-Milstein, J., K. Raphael, A. Bonner, L. Pelton, and T. Fulmer. 2020a. Hospital adoption of electronic health record functions to support age-friendly care: Results from a national survey. Journal of the American Medical Informatics Association 27(8):1206–1213.
Adler-Milstein, J., W. Zhao, R. Willard-Grace, M. Knox, and K. Grumbach. 2020b. Electronic health records and burnout: Time spent on the electronic health record after hours and message volume associated with exhaustion but not with cynicism among primary care clinicians. Journal of the American Medical Informatics Association 27(4):531-538.
Adler-Milstein, J., K. Raphael, T. A. O’Malley, and D. A. Cross. 2021. Information sharing practices between U.S. hospitals and skilled nursing facilities to support care transitions. JAMA Network Open 4(1):e2033980.
AHRQ (Agency for Healthcare Research and Quality). 2018a. Data sources for health care quality measures. https://www.ahrq.gov/talkingquality/measures/understand/index.html (accessed January 26, 2022).
AHRQ. 2018b. Major nursing home quality measurement sets. https://www.ahrq.gov/talkingquality/measures/setting/long-term-care/nursing-home/measurement-sets.html (accessed January 26, 2022).
Alexander, A. G., and K. A. Ballou. 2018. Work–life balance, burnout, and the electronic health record. American Journal of Medicine 131(8):857–858.
Alexander, G. L. 2015. Nurse assistant communication strategies about pressure ulcers in nursing homes. Western Journal of Nursing Research 37(7):984–1004.
Alexander, G. L., and R. Madsen. 2018. A national report of nursing home quality and information technology: Two-year trends. Journal of Nursing Care Quality 33(3):200–207.
Alexander, G. L., and R. W. Madsen. 2021. A report of information technology and health deficiencies in U.S. nursing homes. Journal of Patient Safety 17(6):e483–e489.
Alexander, G., and N. Staggers. 2009. A systematic review of the designs of clinical technology: Findings and recommendations for future research. Advances in Nursing Science 32(3):252–279.
Alexander, G. L., M. Rantz, M. Flesner, M. Diekemper, and C. Siem. 2007. Clinical information systems in nursing homes: An evaluation of initial implementation strategies. Computers Informatics Nursing 25(4):189–197.
Alexander, G. L., M. Rantz, C. Galambos, A. Vogelsmeier, M. Flesner, L. Popejoy, J. Mueller, S. Shumate, and M. Elvin. 2015. Preparing nursing homes for the future of health information exchange. Applied Clinical Informatics 6(2):248–266.
Alexander, G. L., R. W. Madsen, E. L. Miller, M. K. Schaumberg, A. E. Holm, R. L. Alexander, K. K. Wise, M. L. Dougherty, and B. Gugerty. 2017a. A national report of nursing home information technology: Year 1 results. Journal of the American Medical Informatics Association 24(1):67–73.
Alexander, G. L., R. Madsen, and M. Newton. 2017b. Analyzing change in nursing home information technology sophistication: A 2-year survey. Journal of Gerontological Nursing 43(1):17–21.
Alexander, G. L., D. Madsen, E. L. Miller, D. S. Wakefield, K. Wise, and R. L. Alexander. 2017c. The state of nursing home information technology sophistication in rural and nonrural U.S. markets. Journal of Rural Health 33(3):266–274.
Alexander, G. L., K. Powell, C. B. Deroche, L. Popejoy, A. S. M. Mosa, R. Koopman, L. Pettit, and M. Dougherty. 2019a. Building consensus toward a national nursing home information technology maturity model. Journal of the American Medical Informatics Association 26(6):495–505.
Alexander, G. L., R. Madsen, C. B. Deroche, R. Alexander, and E. Miller. 2019b. Ternary trends in nursing home information technology and quality measures in the United States. Journal of Applied Gerontology 39(10):1134–1143.
Alexander, G. L., C. Deroche, K. Powell, A. S. M. Mosa, L. Popejoy, and R. Koopman. 2020a. Forecasting content and stage in a nursing home information technology maturity instrument using a Delphi method. Journal of Medical Systems 44(3):60.
Alexander, G. L., A. Georgiou, J. Siette, R. Madsen, A. Livingstone, J. Westbrook, and C. Deroche. 2020b. Exploring information technology (IT) sophistication in New South Wales residential aged care facilities. Australian Health Review 44(2):288–296.
Alexander, G. L., K. R. Powell, and C. B. Deroche. 2020c. An evaluation of telehealth expansion in U.S. nursing homes. Journal of the American Medical Informatics Association 28(2):342–348.
Alexander, G. L., C. Galambos, M. Rantz, S. Shumate, A. Vogelsmeier, L. Popejoy, and C. Crecelius. 2022. Value propositions for health information exchange toward improving nursing home hospital readmission rates. Journal of Gerontological Nursing 48(1):15–20.
Alonso-Martín, F., J. J. Gamboa-Montero, J. C. Castillo, Á. Castro-González, and M. Á. Salichs. 2017. Detecting and classifying human touches in a social robot through acoustic sensing and machine learning. Sensors 17(5):1138.
Alotaibi, Y. K., and F. Federico. 2017. The impact of health information technology on patient safety. Saudi Medical Journal 38(12):1173–1180.
Alper, E., T. A. O’Malley, and J. Greenwald. 2021. Hospital discharge and readmission. https://www.uptodate.com/contents/hospital-discharge-and-readmission (accessed January 26, 2022).
Alvarado, C. S., K. Zook, and H. JaWanna. 2017. Electronic health record adoption and interoperability among U.S. skilled nursing facilities in 2016. Washington DC: Office of National Coordinator.
Ancker, J. S., A. Edwards, S. Nosal, D. Hauser, E. Mauer, R. Kaushal, and the HITEC Investigators. 2017. Effects of workload, work complexity, and repeated alerts on alert fatigue in a clinical decision support system. BMC Medical Informatics and Decision Making 17(1):36.
Andersen, L. E., L. Tripp, J. F. Perz, N. D. Stone, A. H. Viall, S. M. Ling, and L. A. Fleisher. 2021. Protecting nursing home residents from COVID-19: Federal strike team findings and lessons learned. NEJM Catalyst: Innovations in Care Delivery 2(3), June 28. https://catalyst.nejm.org/doi/full/10.1056/CAT.21.0144 (accessed January 28, 2022).
Artiga, S., B. Corallo, and O. Pham. 2020. Racial disparities in COVID-19: Key findings from available data and analysis. https://www.kff.org/report-section/racial-disparities-in-covid-19-key-findings-from-available-data-and-analysis-issue-brief (accessed November 10, 2021).
Ashcraft, A. S., and D. C. Owen. 2017. Comparison of standardized and customized SBAR communication tools to prevent nursing home resident transfer. Applied Nursing Research 38:64–69.
Atreja, A., S. M. Gordon, D. A. Pollock, R. N. Olmsted, and P. J. Brennan. 2008. Opportunities and challenges in utilizing electronic health records for infection surveillance, prevention, and control. American Journal of Infection Control 36(3 Suppl):S37–S46.
Azad, B., and N. King. 2008. Enacting computer workaround practices within a medication dispensing system. European Journal of Information Systems 17(3):264–278.
Baysari, M. T., A. Tariq, R. O. Day, and J. I. Westbrook. 2017. Alert override as a habitual behavior—A new perspective on a persistent problem. Journal of the American Medical Informatics Association 24(2):409–412.
Bemelmans, R., G. J. Gelderblom, P. Jonker, and L. de Witte. 2012. Socially assistive robots in elderly care: A systematic review into effects and effectiveness. Journal of the American Medical Directors Association 13(2):114–120.e111.
Birks, M., M. Bodak, J. Barlas, J. Harwood, and M. Pether. 2016. Robotic seals as therapeutic tools in an aged care facility: A qualitative study. Journal of Aging Research 2016:8569602.
Bjarnadottir, R. I., C. T. A. Herzig, J. L. Travers, N. G. Castle, and P. W. Stone. 2017. Implementation of electronic health records in U.S. nursing homes. Computers, Informatics, Nursing 35(8):417–424.
Blijleven, V., K. Koelemeijer, M. Wetzels, and M. Jaspers. 2017. Workarounds emerging from electronic health record system usage: Consequences for patient safety, effectiveness of care, and efficiency of care. JMIR Human Factors 4(4):e27.
Boonstra, A., T. L. Jonker, M. A. G. van Offenbeek, and J. F. J. Vos. 2021. Persisting workarounds in electronic health record system use: Types, risks and benefits. BMC Medical Informatics and Decision Making 21(1):183.
Brewer, L. C., K. L. Fortuna, C. Jones, R. Walker, S. N. Hayes, C. A. Patten, and L. A. Cooper. 2020. Back to the future: Achieving health equity through health informatics and digital health. JMIR mHealth and uHealth 8(1):e14512.
Brownell, J., J. Wang, A. Smith, C. Stephens, and R. Y. Hsia. 2014. Trends in emergency department visits for ambulatory care sensitive conditions by elderly nursing home residents, 2001 to 2010. JAMA Internal Medicine 174(1):156–158.
Carayon, P., and P. Hoonakker. 2019. Human factors and usability for health information technology: Old and new challenges. Yearbook of Medical Informatics 28(1):71–77.
Carroll, N. W., L. R. Hearld, and R. Joseph. 2020. Hospital ownership of postacute care providers and the cost of care. Health Care Management Review 45(4):E35–E44.
CDC (Centers for Disease Control and Prevention). 2021a. Electronic medical records/electronic health records (EMRs/EHRs). https://www.cdc.gov/nchs/fastats/electronic-medical-records.htm (accessed November 30, 2021).
CDC. 2021b. Health equity considerations and racial and ethnic minority groups. https://www.cdc.gov/coronavirus/2019-ncov/community/health-equity/race-ethnicity.html (accessed November 10, 2021).
CDC, National Center for Emerging and Zoonotic Infectious Diseases (NCEZID), and Division of Healthcare Quality Promotion (DHQP). 2021. National Healthcare Safety Network (NHSN): Nursing home COVID-19 data dashboard. https://www.cdc.gov/nhsn/covid19/ltc-report-overview.html (accessed January 26, 2022).
Chan, M., D. Estève, J. Y. Fourniols, C. Escriba, and E. Campo. 2012. Smart wearable systems: Current status and future challenges. Artificial Intelligence in Medicine 56(3):137–156.
Cherry, B., M. Carter, D. Owen, and C. Lockhart. 2008. Factors affecting electronic health record adoption in long-term care facilities. Journal for Healthcare Quality 30(2):37–47.
Cherry, B. J., E. W. Ford, and L. T. Peterson. 2011. Experiences with electronic health records: Early adopters in long-term care facilities. Health Care Management Review 36(3):265–274.
Classen, D., M. Li, S. Miller, and D. Ladner. 2018. An electronic health record–based real-time analytics program for patient safety surveillance and improvement. Health Affairs 37(11):1805–1812.
CMS (Centers for Medicare & Medicaid Services). 2020. Long-term care nursing homes telehealth and telemedicine tool kit. https://www.cms.gov/files/document/covid-19-nursing-home-telehealth-toolkit.pdf (accessed November 22, 2021).
CMS. 2021a. Minimum data set (MDS) 3.0 for nursing homes and swing bed providers. https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/NursingHomeQualityInits/NHQIMDS30 (accessed January 26, 2022).
CMS. 2021b. The Skilled Nursing Facility Value-Based Purchasing (SNF VBP) program. https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/SNF-VBP/SNF-VBP-Page (accessed January 26, 2022).
CMS. 2021c. Policies and technology for interoperability and burden reduction. https://www.cms.gov/Regulations-and-Guidance/Guidance/Interoperability/index (accessed January 26, 2022).
CMS. 2022. Quality payment program overview. https://qpp.cms.gov/about/qpp-overview (accessed February 17, 2022).
Crawford, A., and E. Serhal. 2020. Digital health equity and COVID-19: The innovation curve cannot reinforce the social gradient of health. Journal of Medical Internet Research 22(6):e19361.
Debono, D., and J. Braithwaite. 2015. Workarounds in nursing practice in acute care: A case of a health care arms race? In R. L. Wears, E. Hollnagel, and J. Braithwaite (eds.), Resilient health care, vol. 2. New York: Routledge. Pp. 23–38.
Debono, D. S., D. Greenfield, J. F. Travaglia, J. C. Long, D. Black, J. Johnson, and J. Braithwaite. 2013. Nurses’ workarounds in acute healthcare settings: A scoping review. BMC Health Services Research 13(1):175.
Dendere, R., M. Samadbeik, and M. Janda. 2021. The impact on health outcomes of implementing electronic health records to support the care of older people in residential aged care: A scoping review. International Journal of Medical Informatics 151:104471.
Despins, L. A., G. Guidoboni, M. Skubic, L. Sala, M. Enayati, M. Popescu, and C. B. Deroche. 2020. Using sensor signals in the early detection of heart failure: A case study. Journal of Gerontological Nursing 46(7):41–46.
DiAngi, Y. T., L. A. Stevens, B. Halpern-Felsher, N. M. Pageler, and T. C. Lee. 2019. Electronic health record (EHR) training program identifies a new tool to quantify the EHR time burden and improves providers’ perceived control over their workload in the EHR. JAMIA Open 2(2):222–230.
Dowding, D. W., M. Turley, and T. Garrido. 2012. The impact of an electronic health record on nurse sensitive patient outcomes: An interrupted time series analysis. Journal of the American Medical Informatics Association 19(4):615–620.
Driessen, J., A. Bonhomme, W. Chang, D. A. Nace, D. Kavalieratos, S. Perera, and S. M. Handler. 2016. Nursing home provider perceptions of telemedicine for reducing potentially avoidable hospitalizations. Journal of the American Medical Directors Association 17(6):519–524.
Driessen, J., N. G. Castle, and S. M. Handler. 2018a. Perceived benefits, barriers, and drivers of telemedicine from the perspective of skilled nursing facility administrative staff stakeholders. Journal of Applied Gerontology 37(1):110–120.
Driessen, J., W. Chang, P. Patel, R. M. Wright, K. Ernst, and S. M. Handler. 2018b. Nursing home provider perceptions of telemedicine for providing specialty consults. Telemedicine Journal and e-Health 24(7):510–516.
Dykes, P. C., L. Samal, M. Donahue, J. O. Greenberg, A. C. Hurley, O. Hasan, T. A. O’Malley, A. K. Venkatesh, L. A. Volk, and D. W. Bates. 2014. A patient-centered longitudinal care plan: Vision versus reality. Journal of the American Medical Informatics Association 21(6):1082–1090.
Edelman, L. S., E. S. McConnell, S. M. Kennerly, J. Alderden, S. D. Horn, and T. L. Yap. 2020. Mitigating the effects of a pandemic: Facilitating improved nursing home care delivery through technology. JMIR Aging 3(1):e20110.
Enyioha, C., S. Khairat, and C. E. Kistler. 2021. Adoption of electronic health records by practices of nursing home providers and wi-fi availability in nursing homes. Journal of the American Medical Directors Association 22(2):475–476.
Evans, E. L., and D. Whicher. 2018. What should oversight of clinical decision support systems look like? AMA Journal of Ethics 20(9):E857–E863.
Filipova, A. A. 2013. Electronic health records use and barriers and benefits to use in skilled nursing facilities. Computers, Informatics, Nursing 31(7):305–318.
Fossum, M., M. Ehnfors, A. Fruhling, and A. Ehrenberg. 2011. An evaluation of the usability of a computerized decision support system for nursing homes. Applied Clinical Informatics 2(04):420–436.
Gardner, R. L., E. Cooper, J. Haskell, D. A. Harris, S. Poplau, P. J. Kroth, and M. Linzer. 2018. Physician stress and burnout: The impact of health information technology. Journal of the American Medical Informatics Association 26(2):106–114.
Gerling, K., D. Hebesberger, C. Dondrup, T. Körtner, and M. Hanheide. 2016. Robot deployment in long-term care: Case study on using a mobile robot to support physiotherapy. Zeitschrift fur Gerontologie und Geriatrie 49(4):288–297.
Gillespie, S. M., S. M. Handler, and A. Bardakh. 2020. Innovation through regulation: COVID-19 and the evolving utility of telemedicine. Journal of the American Medical Directors Association 21(8):1007–1009.
Girling, R. 2021. Can care robots improve quality of life as we age? Forbes, January 18. https://www.forbes.com/sites/robgirling/2021/01/18/can-care-robots-improve-quality-of-life-as-we-age/ (accessed October 20, 2021).
Gliklich, R. E., N. A. Dreyer, and M. B. Leavy. 2014. AHRQ methods for effective health care. In Registries for evaluating patient outcomes: A user’s guide. Rockville, MD: Effective Health Care Program, Agency for Healthcare Research and Quality.
Gold, M., and C. McLaughlin. 2016. Assessing HITECH implementation and lessons: 5 years later. Milbank Quarterly 94(3):654–687.
Gomes, M., P. Hash, L. Orsolini, A. Watkins, and A. Mazzoccoli. 2016. Connecting professional practice and technology at the bedside: Nurses’ beliefs about using an electronic health record and their ability to incorporate professional and patient-centered nursing activities in patient care. Computers, Informatics, Nursing 34(12):578–586.
Gorges, R. J., and R. T. Konetzka. 2021. Factors associated with racial differences in deaths among nursing home residents with COVID-19 infection in the US. JAMA Network Open 4(2):1–10.
Grabowski, D., J. O’Malley, and N. Barhydt. 2007. The costs and potential savings associated with nursing home hospitalizations. Health Affairs (Project Hope) 26:1753–1761.
Grabowski, D. C., and A. J. O’Malley. 2014. Use of telemedicine can reduce hospitalizations of nursing home residents and generate savings for Medicare. Health Affairs 33(2):244–250.
Grönvall, E., and N. Verdezoto. 2013. Understanding challenges and opportunities of preventive blood pressure self-monitoring at home. Paper read at Proceedings of the 31st European Conference on Cognitive Ergonomics. https://dl.acm.org/doi/10.1145/2501907.2501962 (accessed November 22, 2021).
Groom, L. L., M. M. McCarthy, A. W. Stimpfel, and A. A. Brody. 2021. Telemedicine and telehealth in nursing homes: An integrative review. Journal of the American Medical Directors Association 22(9):1784–1801.
Henry, J., Y. Pylypchuk, and V. Patel. 2018. Electronic health record adoption and interoperability among U.S. skilled nursing facilities and home health agencies in 2017. The Office of the National Coordinator for Health Information Technology U.S. Department of Health and Human Services, https://www.healthit.gov/sites/default/files/page/2018-11/Electronic-Health-Record-Adoption-and-Interoperability-among-U.S.-Skilled-Nursing-Facilities-and-Home-Health-Agencies-in-2017.pdf (accessed November 10, 2021).
HHS (U.S. Department of Health and Human Services). 2022. ONC completes critical 21st Century Cures Act requirement, publishes the Trusted Exchange Framework and the Common Agreement for health information networks. https://www.hhs.gov/about/news/2022/01/18/onc-completes-critical-21st-century-cures-act-requirement-publishes-trusted-exchange-framework-common-agreement-health-information-networks.html (accessed January 26, 2022).
Holup, A. A., D. Dobbs, H. Meng, and K. Hyer. 2013. Facility characteristics associated with the use of electronic health records in residential care facilities. Journal of the American Medical Informatics Association 20(4):787–791.
Howe, J. L., K. T. Adams, A. Z. Hettinger, and R. M. Ratwani. 2018. Electronic health record usability issues and potential contribution to patient harm. JAMA 319(12):1276–1278.
Hudak, S., and S. Sharkey. 2007. Health information technology: Are long term care providers ready? Oakland, CA: California HealthCare Foundation.
Hughes, R. G. 2008. Chapter 44. Tools and strategies for quality improvement and patient safety. In R. Hughes (ed.), Patient safety and quality: An evidence-based handbook for nurses. Rockville, MD: Agency for Healthcare Research and Quality. Pp. 3-1–3-39.
Hui, E., J. Woo, M. Hjelm, Y. T. Zhang, and H. T. Tsui. 2001. Telemedicine: A pilot study in nursing home residents. Gerontology 47(2):82–87.
Ingber, M. J., Z. Feng, G. Khatutsky, J. M. Wang, L. E. Bercaw, N. T. Zheng, A. Vadnais, N. M. Coomer, and M. Segelman. 2017. Initiative to reduce avoidable hospitalizations among nursing facility residents shows promising results. Health Affairs (Millwood) 36(3):441–450.
IOM (Institute of Medicine). 1986. Improving the quality of care in nursing homes. Washington, DC: National Academy Press.
IOM. 1991. Computer-based patient record: An essential technology for health care. Washington, DC: National Academy Press.
IOM. 1996. Telemedicine: A guide to assessing telecommunications for health care. Washington, DC: National Academy Press.
IOM. 2000. To err is human: Building a safer health system. Washington, DC: National Academy Press.
IOM. 2001a. Improving the quality of long-term care. Washington, DC: National Academy Press.
IOM. 2001b. Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academy Press.
Jen, S. P., A. Bui, and S. D. Leonard. 2021. Maximizing efficiency of telemedicine in the skilled nursing facility during the coronavirus disease 2019 pandemic. Journal of the American Medical Directors Association 22(6):1146–1148.e1142.
Jung, H.-Y., A. N. Trivedi, D. C. Grabowski, and V. Mor. 2016. Does more therapy in skilled nursing facilities lead to better outcomes in patients with hip fracture? Physical Therapy 96(1):81–89.
Kandaswamy, S., Z. Pruitt, S. Kazi, J. Marquard, S. Owens, D. J. Hoffman, R. M. Ratwani, and A. Z. Hettinger. 2021. Clinician perceptions on the use of free-text communication orders. Applied Clinical Informatics 12(03):484–494.
Kapoor, A., T. Field, S. Handler, K. Fisher, C. Saphirak, S. Crawford, H. Fouayzi, F. Johnson, A. Spenard, N. Zhang, and J. H. Gurwitz. 2019. Adverse events in long-term care residents transitioning from hospital back to nursing home. JAMA Internal Medicine 179(9):1254–1261.
Keenan, G. M., E. Yakel, D. Tschannen, and M. Mandeville. 2008. Chapter 49. Documentation and the nurse care planning process. In R. Hughes (ed.), Patient safety and quality: An evidence-based handbook for nurses. Rockville, MD: Agency for Healthcare Research and Quality. Pp. 3-175–3-206.
Kemp, C. L. 2020. #Morethanavisitor: Families as “essential” care partners during COVID-19. The Gerontologist 61(2):145–151.
King, B. J., A. L. Gilmore-Bykovskyi, R. A. Roiland, B. E. Polnaszek, B. J. Bowers, and A. J. H. Kind. 2013. The consequences of poor communication during transitions from hospital to skilled nursing facility: A qualitative study. Journal of the American Geriatrics Society 61(7):1095–1102.
Kistler, C. E., S. Zimmerman, and S. Khairat. 2021. Health information technology challenges and innovations in long-term care. Journal of the American Medical Directors Association 22(5):981–983.
Ko, M., L. Wagner, and J. Spetz. 2018. Nursing home implementation of health information technology: Review of the literature finds inadequate investment in preparation, infrastructure, and training. Inquiry 55:46958018778902.
Krüger, K., L. Strand, J. T. Geitung, G. E. Eide, and A. Grimsmo. 2011. Can electronic tools help improve nursing home quality? ISRN Nursing 2011:208142.
Kruse, C. S., M. Mileski, V. Alaytsev, E. Carol, and A. Williams. 2015. Adoption factors associated with electronic health record among long-term care facilities: A systematic review. BMJ Open 5(1):e006615.
Kruse, C. S., M. Mileski, A. G. Vijaykumar, S. V. Viswanathan, U. Suskandla, and Y. Chidambaram. 2017. Impact of electronic health records on long-term care facilities: Systematic review. JMIR Medical Informatics 5(3):e35.
Kruse, C. S., G. Marquez, D. Nelson, and O. Palomares. 2018. The use of health information exchange to augment patient handoff in long-term care: A systematic review. Applied Clinical Informatics 9(4):752–771.
Kukafka, R., J. S. Ancker, C. Chan, J. Chelico, S. Khan, S. Mortoti, K. Natarajan, K. Presley, and K. Stephens. 2007. Redesigning electronic health record systems to support public health. Journal of Biomedical Informatics 40(4):398–409.
Lamas, D., N. Panariello, N. Henrich, B. Hammes, L. C. Hanson, D. E. Meier, N. Guinn, J. Corrigan, S. Hubber, H. Luetke-Stahlman, and S. Block. 2018. Advance care planning documentation in electronic health records: Current challenges and recommendations for change. Journal of Palliative Medicine 21(4):522–528.
Lee, E. K., T.-L. Wu, T. Senior, and J. Jose. 2014. Medical alert management: A real-time adaptive decision support tool to reduce alert fatigue. AMIA Symposium 2014:845–854.
Lee, J. 2015. The impact of health information technology on disparity of process of care. International Journal for Equity in Health 14:34. https://doi.org/10.1186/s12939-015-0161-3.
Lee, M. L., and A. K. Dey. 2011. Reflecting on pills and phone use: Supporting awareness of functional abilities for older adults. Paper read at Proceedings of the SIGCHI Conference on Human Factors in Computing Systems. http://www.cs.cmu.edu/~mllee/docs/Lee2011Reflecting_on_Pills_and_Phone_Use-CHI2011.pdf (accessed November 22, 2021).
Lemon, C., M. De Ridder, and M. Khadra. 2019. Do electronic medical records improve advance directive documentation? A systematic review. American Journal of Hospice and Palliative Care 36(3):255–263.
Longhurst, C. A., T. Davis, A. Maneker, H. C. Eschenroeder, Jr., R. Dunscombe, G. Reynolds, B. Clay, T. Moran, D. B. Graham, S. M. Dean, J. Adler-Milstein, and C. Arch. 2019. Local investment in training drives electronic health record user satisfaction. Applied Clinical Informatics 10(2):331–335.
Louie, W. G., J. Li, T. Vaquero, and G. Nejat. 2014. A focus group study on the design considerations and impressions of a socially assistive robot for long-term care. Paper read at the 23rd IEEE International Symposium on Robot and Human Interactive Communication, August 25–29, 2014.
Lundberg, C. B., J. J. Warren, J. Brokel, G. M. Bulechek, H. K. Butcher, J. M. Dochterman, M. Johnson, M. Maas, K. S. Martin, S. Moorhead, C. Spisla, E. Swanson, and S. Giarrizzo-Wilson. 2008. Selecting a standardized terminology for the electronic health record that reveals the impact of nursing on patient care. Online Journal of Nursing Informatics 12(2).
MACPAC (Medicaid and Children’s Health Insurance Program Payment and Access Commission). 2021. Integrating clinical care through greater use of electronic health records for behavioral health. In June 2021 report to Congress on Medicaid and CHIP. Washington, DC: Medicaid and CHIP Payment and Access Commission.
McAllen, E. R., Jr., K. Stephens, B. Swanson-Biearman, K. Kerr, and K. Whiteman. 2018. Moving shift report to the bedside: An evidence-based quality improvement project. Online Journal of Issues in Nursing 23(2). https://doi.org/10.3912/OJIN.Vol23No02PPT22.
McGlynn, S., B. Snook, S. Kemple, T. L. Mitzner, and W. A. Rogers. 2014. Therapeutic robots for older adults: Investigating the potential of paro. Paper presented at Proceedings of the 2014 ACM/IEEE International Conference on Human-Robot Interaction, Bielefeld, Germany. https://doi.org/10.1145/2559636.2559846 (accessed November 22, 2021).
Meehan, R. 2017. Electronic health records in long-term care: Staff perspectives. Journal of Applied Gerontology 36(10):1175–1196.
Mor, V., O. Intrator, Z. Feng, and D. C. Grabowski. 2010. The revolving door of rehospitalization from skilled nursing facilities. Health Affairs (Project Hope) 29(1):57–64.
Moyle, W., C. J. Jones, J. E. Murfield, L. Thalib, E. R. A. Beattie, D. K. H. Shum, S. T. O’Dwyer, M. C. Mervin, and B. M. Draper. 2017a. Use of a robotic seal as a therapeutic tool to improve dementia symptoms: A cluster-randomized controlled trial. Journal of the American Medical Directors Association 18(9):766–773.
Moyle, W., U. Arnautovska, T. Ownsworth, and C. Jones. 2017b. Potential of telepresence robots to enhance social connectedness in older adults with dementia: An integrative review of feasibility. International Psychogeriatrics 29(12):1951–1964.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2020. Social isolation and loneliness in older adults: Opportunities for the health care system. Washington, DC: The National Academies Press.
NASEM. 2021. The future of nursing 2020–2030: Charting a path to achieve health equity. Washington, DC: The National Academies Press.
NORC (NORC at the University of Chicago). 2010. Briefing paper: Understanding the impact of health IT in underserved communities and those with health disparities. Bethesda, MD: NORC at the University of Chicago.
Øderud, T., B. Landmark, S. Eriksen, A. B. Fossberg, S. Aketun, M. Omland, K. G. Hem, E. Østensen, and D. Ausen. 2015. Persons with dementia and their caregivers using GPS. Studies in Health Technology and Informatics 217:212–221.
ODPHP (Office of Disease Prevention and Health Promotion, U.S. Department of Health and Human Services). 2022. National healthcare safety network (NHSN). https://health.gov/healthypeople/objectives-and-data/data-sources-and-methods/data-sources/national-healthcare-safety-network-nhsn (accessed February 17, 2022).
OIG (Office of the Inspector General). 2014. Adverse events in skilled nursing facilities: National incidence among Medicare beneficiaries. Washington DC: Office of the Inspector General, U.S. Department of Health and Human Services.
ONC (Office of the National Coordinator for Health Information Technology). 2017a. Non-federal acute care hospital electronic health record adoption. Health IT Quick-Stat #47. https://www.healthit.gov/data/quickstats/non-federal-acute-care-hospital-electronic-health-record-adoption (accessed November 30, 2021).
ONC. 2017b. Improve care coordination. https://www.healthit.gov/topic/health-it-and-health-information-exchange-basics/improve-care-coordination (accessed January 26, 2022).
ONC. 2019a. What are the differences between electronic medical records, electronic health records, and personal health records? https://www.healthit.gov/faq/what-are-differences-between-electronic-medical-records-electronic-health-records-and-personal (accessed December 1, 2021).
ONC. 2019b. Improved diagnostics & patient outcomes. https://www.healthit.gov/topic/health-it-and-health-information-exchange-basics/improved-diagnostics-patient-outcomes (accessed November 10, 2021).
ONC. 2019c. Meaningful use and the shift to the merit-based incentive payment system. https://www.healthit.gov/topic/meaningful-use-and-macra/meaningful-use (accessed October 29, 2021).
ONC. 2019d. Health information exchange. https://www.healthit.gov/topic/health-it-and-health-information-exchange-basics/health-information-exchange#:~:text=Read%20the%20Roadmap-,What%20is%20HIE%3F,a%20patient’s%20medical%20information%20electronically (accessed February 17, 2022).
ONC. 2019e. What is telehealth? How is telehealth different from telemedicine? https://www.healthit.gov/faq/what-telehealth-how-telehealth-different-telemedicine (accessed November 22, 2021).
ONC. 2020. Telemedicine and telehealth. https://www.healthit.gov/topic/health-it-health-care-settings/telemedicine-and-telehealth (accessed November 10, 2021).
ONC. 2021a. ONC’s Cures Act final rule. https://www.healthit.gov/curesrule (accessed October 29, 2021).
ONC. 2021b. Health IT legislation. https://www.healthit.gov/topic/laws-regulation-and-policy/health-it-legislation (accessed June 4, 2021).
Ong, Y. C., A. Tang, and W. Tam. 2021. Effectiveness of robot therapy in the management of behavioural and psychological symptoms for individuals with dementia: A systematic review and meta-analysis. Journal of Psychiatric Research 140:381–394.
Pantaleoni, J. L., L. A. Stevens, E. S. Mailes, B. A. Goad, and C. A. Longhurst. 2015. Successful physician training program for large scale EMR implementation. Applied Clinical Informatics 6(1):80–95.
Phillips, K., C. Wheeler, J. Campbell, and A. Coustasse. 2010. Electronic medical records in long-term care. Journal of Hospital Marketing & Public Relations 20(2):131–142.
Phillips, L. J., C. B. DeRoche, M. Rantz, G. L. Alexander, M. Skubic, L. Despins, C. Abbott, B. H. Harris, C. Galambos, and R. J. Koopman. 2017. Using embedded sensors in independent living to predict gait changes and falls. Western Journal of Nursing Research 39(1):78–94.
Philipson, A. 2021. Robots could one day work alongside human caregivers. https://medcitynews.com/2021/06/robots-could-one-day-work-alongside-human-caregivers (accessed October 20, 2021).
Popejoy, L., C. Galambos, and A. Vogelsmeier. 2014. Hospital to nursing home transition challenges: Perceptions of nursing home staff. Journal of Nursing Care Quality 29(2):103–109.
Powell, K. R., and G. L. Alexander. 2021. Consequences of rapid telehealth expansion in nursing homes: Promise and pitfalls. Applied Clinical Informatics 12(4):933–943.
Powell, K. R., C. B. Deroche, and G. L. Alexander. 2021. Health data sharing in U.S. nursing homes: A mixed methods study. Journal of the American Medical Directors Association 22(5):1052–1059.
Purtill, C. 2019. Stop me if you’ve heard this one: A robot and a team of Irish scientists walk into a senior living home. https://time.com/longform/senior-care-robot (accessed October 20, 2021).
Qi, A. C., A. A. Luke, C. Crecelius, and K. E. Joynt Maddox. 2020. Performance and penalties in year 1 of the skilled nursing facility value-based purchasing program. Journal of the American Geriatrics Society 68(4):826–834.
Rahman, A. N., and R. A. Applebaum. 2009. The nursing home Minimum Data Set assessment instrument: Manifest functions and unintended consequences—past, present, and future. The Gerontologist 49(6):727–735.
Rahman, M., E. A. Gadbois, D. A. Tyler, and V. Mor. 2018. Hospital-skilled nursing facility collaboration: A mixed-methods approach to understanding the effect of linkage strategies. Health Services Research 53(6):4808–4828.
Rantz, M. J., and R. P. Connolly. 2004. Measuring nursing care quality and using large data sets in non-acute care settings: State of the science. Nursing Outlook 52(1):23–37.
Rantz, M. J., L. Hicks, G. F. Petroski, R. W. Madsen, G. Alexander, C. Galambos, V. Conn, J. Scott-Cawiezell, M. Zwygart-Stauffacher, and L. Greenwald. 2010a. Cost, staffing and quality impact of bedside electronic medical record (EMR) in nursing homes. Journal of the American Medical Directors Association 11(7):485–493.
Rantz, M. J., M. Skubic, G. Alexander, M. A. Aud, B. J. Wakefield, C. Galambos, R. J. Koopman, and S. J. Miller. 2010b. Improving nurse care coordination with technology. Computers, Informatics, Nursing 28(6):325–332.
Rantz, M. J., G. Alexander, C. Galambos, M. K. Flesner, A. Vogelsmeier, L. Hicks, J. Scott-Cawiezell, M. Zwygart-Stauffacher, and L. Greenwald. 2011. The use of bedside electronic medical record to improve quality of care in nursing facilities: A qualitative analysis. Computers, Informatics, Nursing 29(3):149–156.
Rantz, M. J., M. Skubic, R. J. Koopman, G. L. Alexander, L. Phillips, K. Musterman, J. Back, M. A. Aud, C. Galambos, R. D. Guevara, and S. J. Miller. 2012. Automated technology to speed recognition of signs of illness in older adults. Journal of Gerontological Nursing 38(4):18–23.
Rantz, M. J., L. Popejoy, A. Vogelsmeier, C. Galambos, G. Alexander, M. Flesner, C. Crecelius, B. Ge, and G. Petroski. 2017a. Successfully reducing hospitalizations of nursing home residents: Results of the Missouri quality initiative. Journal of the American Medical Directors Association 18(11):960–966.
Rantz, M., L. J. Phillips, C. Galambos, K. Lane, G. L. Alexander, L. Despins, R. J. Koopman, M. Skubic, L. Hicks, S. Miller, A. Craver, B. H. Harris, and C. B. Deroche. 2017b. Randomized trial of intelligent sensor system for early illness alerts in senior housing. Journal of the American Medical Directors Association 18(10):860–870.
Ratwani, R. M., E. Savage, A. Will, A. Fong, D. Karavite, N. Muthu, A. J. Rivera, C. Gibson, D. Asmonga, B. Moscovitch, R. Grundmeier, and J. Rising. 2018. Identifying electronic health record usability and safety challenges in pediatric settings. Health Affairs 37(11):1752–1759.
Resnick, H. E., B. B. Manard, R. I. Stone, and M. Alwan. 2009. Use of electronic information systems in nursing homes: United States, 2004. Journal of the American Medical Informatics Association 16(2):179–186.
Rogero-Blanco, E., J. A. Lopez-Rodriguez, T. Sanz-Cuesta, M. Aza-Pascual-Salcedo, M. J. Bujalance-Zafra, I. Cura-Gonzalez, and P. A. P. G. Multi. 2020. Use of an electronic clinical decision support system in primary care to assess inappropriate polypharmacy in young seniors with multimorbidity: Observational, descriptive, cross-sectional study. JMIR Medical Informatics 8(3):e14130.
Ruopp, M. D. 2020. Overcoming the challenge of family separation from nursing home residents during COVID-19. Journal of the American Medical Directors Association 21(7):984–985.
Saiyed, S. M., P. J. Greco, G. Fernandes, and D. C. Kaelber. 2017. Optimizing drug-dose alerts using commercial software throughout an integrated health care system. Journal of the American Medical Informatics Association 24(6):1149–1154.
Saliba, D., and J. L. Buchanan. 2012. Making the investment count: Revision of the Minimum Data Set for nursing homes, MDS 3.0. Journal of the American Medical Directors Association 13(7):602–610.
Scott, A. M., J. Li, S. Oyewole-Eletu, H. Q. Nguyen, B. Gass, K. B. Hirschman, S. Mitchell, S. M. Hudson, and M. V. Williams. 2017. Understanding facilitators and barriers to care transitions: Insights from Project ACHIEVE site visits. Joint Commission Journal on Quality and Patient Safety 43(9):433–447.
Scott, I. A., P. I. Pillans, M. Barras, and C. Morris. 2018. Using EMR-enabled computerized decision support systems to reduce prescribing of potentially inappropriate medications: A narrative review. Therapeutic Advances in Drug Safety 9(9):559–573.
Seifert, A., J. A. Batsis, and A. C. Smith. 2020. Telemedicine in long-term care facilities during and beyond COVID-19: Challenges caused by the digital divide. Frontiers in Public Health 8:601595.
Shetty, K. D., A. A. Tolpadi, M. W. Robbins, E. A. Taylor, K. N. Campbell, and C. L. Damberg. 2020. Nursing home responses to performance-based accountability: Results of a national survey. Journal of the American Geriatrics Society 68(9):1979–1987.
Shiells, K., I. Holmerova, M. Steffl, and O. Stepankova. 2019. Electronic patient records as a tool to facilitate care provision in nursing homes: An integrative review. Informatics for Health and Social Care 44(3):262–277.
Silow-Carroll, S., J. N. Edwards, and D. Rodin. 2012. Using electronic health records to improve quality and efficiency: The experiences of leading hospitals. Issue Brief (Commonwealth Fund) 17:1–40.
Simard, J., and L. Volicer. 2020. Loneliness and isolation in long-term care and the COVID-19 pandemic. Journal of the American Medical Directors Association 21(7):966–967.
Simpao, A. F., L. M. Ahumada, B. R. Desai, C. P. Bonafide, J. A. Gálvez, M. A. Rehman, A. F. Jawad, K. L. Palma, and E. D. Shelov. 2015. Optimization of drug–drug interaction alert rules in a pediatric hospital’s electronic health record system using a visual analytics dashboard. Journal of American Medical Informatics Association 22(2):361–369.
Skrocki, M. 2013. Standardization needs for effective interoperability, https://scholarworks.wmich.edu/ichita_transactions/32/ (accessed January 26, 2022).
Spinelli-Moraski, C., and K. Richards. 2013. Health information technology in nursing homes: Why and how? Research in Gerontological Nursing 6(3):150–151.
Staggers, N., B. L. Elias, E. Makar, and G. L. Alexander. 2018. The imperative of solving nurses’ usability problems with health information technology. Journal of Nursing Administration 48(4):191–196.
Stanhope, V., and E. B. Matthews. 2019. Delivering person-centered care with an electronic health record. BMC Medical Informatics and Decision Making 19(1):168.
Su, B. Y., K. C. Ho, M. Rantz, and M. Skubic. 2018. Radar placement for fall detection: Signature and performance. Journal of Ambient Intelligence and Smart Environments 10:21–34.
Su, B. Y., M. Enayati, K. C. Ho, M. Skubic, L. Despins, J. Keller, M. Popescu, G. Guidoboni, and M. Rantz. 2019. Monitoring the relative blood pressure using a hydraulic bed sensor system. IEEE Transactions on Biomedical Engineering 66(3):740–748.
Suter, E., N. D. Oelke, C. E. Adair, and G. D. Armitage. 2009. Ten key principles for successful health systems integration. Healthcare Quarterly (Toronto, Ont.) 13(Spec No):16–23.
Unruh, M. A., D. C. Grabowski, A. N. Trivedi, and V. Mor. 2013a. Medicaid bed-hold policies and hospitalization of long-stay nursing home residents. Health Services Research 48(5):1617–1633.
Unruh, M. A., A. N. Trivedi, D. C. Grabowski, and V. Mor. 2013b. Does reducing length of stay increase rehospitalization of Medicare fee-for-service beneficiaries discharged to skilled nursing facilities? Journal of the American Geriatrics Society 61(9):1443–1448.
van Dyck, L. I., K. M. Wilkins, J. Ouellet, G. M. Ouellet, and M. L. Conroy. 2020. Combating heightened social isolation of nursing home elders: The Telephone Outreach in the COVID-19 Outbreak Program. American Journal of Geriatric Psychiatry 28(9):989–992.
Vest, J. R., H. Y. Jung, K. Wiley, Jr., H. Kooreman, L. Pettit, and M. A. Unruh. 2019. Adoption of health information technology among U.S. nursing facilities. Journal of the American Medical Directors Association 20(8):995–1000.e1004.
Vogelsmeier, A. 2014. Identifying medication order discrepancies during medication reconciliation: Perceptions of nursing home leaders and staff. Journal of Nursing Management 22(3):362–372.
Vogelsmeier, A. A., J. R. B. Halbesleben, and J. R. Scott-Cawiezell. 2008. Technology implementation and workarounds in the nursing home. Journal of the American Medical Informatics Association 15(1):114–119.
Vogelsmeier, A., L. Popejoy, K. Canada, C. Galambos, G. Petroski, C. Crecelius, G. L. Alexander, and M. Rantz. 2021. Results of the Missouri Quality Initiative in sustaining changes in nursing home care: Six-year trends of reducing hospitalizations of nursing home residents. Journal of Nutrition, Health and Aging 25(1):5–12.
Wade, V. A., J. Karnon, A. G. Elshaug, and J. E. Hiller. 2010. A systematic review of economic analyses of telehealth services using real time video communication. BMC Health Services Research 10(1):233.
Walker, D., A. Mora, M. M. Demosthenidy, N. Menachemi, and M. L. Diana. 2016. Meaningful use of EHRs among hospitals ineligible for incentives lags behind that of other hospitals, 2009–13. Health Affairs 35(3):495–501.
Wang, H. E., M. N. Shah, R. M. Allman, and M. Kilgore. 2011. Emergency department visits by nursing home residents in the United States. Journal of the American Geriatrics Society 59(10):1864–1872.
Wang, T., and S. Biedermann. 2012. Adoption and utilization of electronic health record systems by long-term care facilities in Texas. Perspectives in Health Information Management 9(Spring). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3329211 (accessed November 23, 2021)..
Whitelaw, S., M. A. Mamas, E. Topol, and H. G. C. Van Spall. 2020. Applications of digital technology in COVID-19 pandemic planning and response. The Lancet Digital Health 2(8):e435–e440.
Wu, N., V. Mor, and J. Roy. 2009. Resident, nursing home, and state factors affecting the reliability of minimum data set quality measures. American Journal of Medical Quality 24(3):229-240.
Wyatt, R., M. Laderman, L. Botwinick, K. Mate, and J. Whittington. 2016. Achieving health equity: A guide for health care organizations. Cambridge, MA: Institute for Healthcare Improvement.
Yu, P., D. Hailey, and H. Li. 2008. Caregivers’ acceptance of electronic documentation in nursing homes. Journal of Telemedicine and Telecare 14(5):261-265.
Zhang, N., S. F. Lu, B. Xu, B. Wu, R. Rodriguez-Monguio, and J. Gurwitz. 2016. Health information technologies: Which nursing homes adopted them? Journal of the American Medical Directors Association 17(5):441–447.
Zhang, Y., P. Yu, and J. Shen. 2012. The benefits of introducing electronic health records in residential aged care facilities: A multiple case study. International Journal of Medical Informatics 81(10):690–704.
Zsenits, B., J. Alcantara, and R. Mayo. 2019. Impact of HIT on burnout remains unknown—for now. Journal of the American Medical Informatics Association 26(10):1156–1157.










































