
Care Delivery
Nursing homes play a critical role in the continuum of care within the U.S. health care system, providing essential services ranging from assistance with basic needs to care for people with complex medical conditions to end-of-life care. The intensity of the medical condition and the associated care needs are as varied as each individual nursing home resident and require a broad range of resources and skills among nursing home staff (Harrington et al., 2018; Zweig et al., 2011). As discussed in Chapter 5, a diverse workforce—physicians, physician assistants, nurses, nursing assistants, nurse practitioners, social workers, activity personnel, rehabilitation specialists, dietary staff, and others—delivers the wide range of care in the nursing home setting. While the committee recognizes that care delivery is inextricably linked to those who provide the care, this chapter focuses specifically on the types of care provided to nursing home residents. Chapter 5 details the characteristics of the nursing home workforce, including challenges related to staffing, training, and retention.
Care provided by nursing homes is among the most heavily regulated sectors of the U.S. health care system (Koren, 2010). To be certified—and thus be eligible for Medicare and Medicaid payments—nursing homes are required by federal regulations1 to provide “the necessary care and services to attain or maintain the highest practicable physical, mental, and psychosocial well-being in accordance with the comprehensive assessment and plan of care,”2 and to “promote each resident’s quality of life.”3 The broad
___________________
1 The Nursing Home Reform Act incorporated into the Omnibus Budget Reconciliation Act (OBRA) of 1987 contained a sweeping set of reforms aimed at improving the quality of care in nursing homes.
2 CMS Requirements for Long-Term Care Facilities—Quality of Life, 42 CFR § 483.24 (2016).
3 CMS Requirements for Long-Term Care Facilities—Admission, transfer, and discharge rights, 42 CFR § 483.15 (2016).
range of services that nursing homes are required by law to provide are shown in Box S-1 in the Summary chapter of this report.
To meet the extensive statutory requirements nursing homes must discover and address each resident’s individualized needs.4 As Koren observed more than a decade ago, the nursing home reform measures contained in the Omnibus Budget Reconciliation Act of 1987 (OBRA 87) made nursing homes “the only sector of the entire health care industry to have an explicit statutory requirement for what is now known as ‘patient-centered care’” (Koren, 2010). The committee’s conceptual model sees comprehensive, person-centered, equitable care as the central characteristic of high-quality care in the nursing home setting. Such person-centered care requires, at a minimum, knowledge of the range and types of needs of nursing home residents and an assessment and care planning model that identifies, prioritizes, and addresses those needs.
NEEDS-BASED CARE FOR NURSING HOME RESIDENTS
The committee’s conceptual model (Chapter 1) specifies care that meets the individual needs of each resident as the central focus of nursing homes. It is useful, therefore, to identify and categorize the various needs of nursing home residents—both individually and collectively—and the ways that quality care should address those needs. The work of Abraham Maslow, who developed an overall model of human needs (Figure 4-1), provides one starting point for understanding those needs. Maslow’s model includes a five-category hierarchy, with each higher level depending on first satisfying the needs in the levels below. The most basic level includes physiological needs such as food, water, and rest; the second level involves safety and security; the third encompasses social needs such as friendship and intimate relationships; the fourth level addresses self-esteem needs that support self-worth and a feeling of accomplishment; and the fifth level entails self-actualization and achieving one’s full potential (Maslow, 1943, 1954).5
Maslow’s hierarchy of needs has been applied multiple times in health care settings (Abraham, 2011; Bayoumi, 2012; Nydén et al., 2003; Zalenski and Raspa, 2006), and the field of nursing has found the model particularly useful in promoting culture change and developing patient care plans (Reitman, 2010). Maslow’s hierarchy has also been used in hospice and palliative care to guide efforts to provide effective and meaningful care to
___________________
4 CMS Requirements for Long-Term Care Facilities—Quality of Life, 42 CFR § 483.24 (2016).
5 Maslow’s hierarchy is a visual representation of a theory put forth by psychologist Abraham Maslow in his 1943 paper for Psychological Review, “A Theory of Human Motivation.” Maslow’s concepts were more fully developed in his 1954 book, Motivation and Personality.
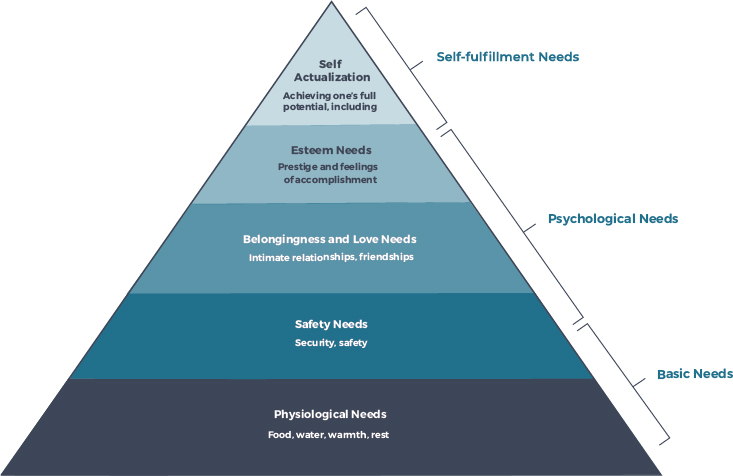
SOURCE: Maslow, 1943; Maslow, 1954.
patients at the end of life (Zalenski and Raspa, 2006). Maslow’s perspective provides an important conceptual framework for understanding the range of needs of nursing home residents and how comprehensive care can be delivered to meet those needs (Jackson et al., 2014).
Another lens with which to consider the range of needs of nursing home residents is provided by the Centers for Medicare & Medicaid Services (CMS) Resident Assessment Instrument (RAI)–Minimum Data Set (MDS). Introduced in the early 1990s as part of implementing OBRA 1987, the RAI–MDS is a standardized, needs-based resident assessment designed to inform care planning (Morris et al., 1990). CMS issued the most recent MDS 3.0 in 2010 (CMS, 2020b). All federally certified nursing homes are required to complete the full RAI–MDS upon an individual’s admission to the nursing home and again on an annual basis. In addition, nursing homes must update a portion of the MDS quarterly and also after any significant change in the condition of a resident. Current needs-related domains covered by the MDS include basic functional activities (activities of daily living [ADLs] and continence), diagnosis-related medical care needs, symptoms (e.g., pain, shortness of breath), perception and communication (hearing, speech, vision), cognitive health and related assistance needs, nutrition (including swallowing/intake issues), and the maintenance of skin integrity.
Other MDS components are more treatment related and include medications, special treatments, procedures, and restraint use.6
A third perspective on identifying and categorizing the various needs of nursing home residents is provided by using quality-of-life measures applicable to nursing home residents. These measures include domains of quality such as physical comfort, functional competence, privacy, autonomy, dignity, meaningful activity, enjoyment, individuality, relationships, security and order, and spiritual well-being (Cutler and Kane, 2006; Travers et al., 2022).
Bringing these three frameworks together provides an overarching structure for understanding the full range of needs of nursing home residents as well as the types of care required to address those needs. The committee contends that planning and providing needs-based quality care in the nursing home setting should address, at minimum, the key elements outlined in the three frameworks (summarized in Table 4-1). The discussion in this chapter features all of the domains listed in Table 4-1, except safety and security. Key areas related to resident safety and security such as falls, medication management, resident abuse, and protecting the health and safety of residents and staff during a public emergency are all discussed in Chapter 6.
ASSESSING THE NEEDS OF NURSING HOME RESIDENTS
Federal regulation and advocacy efforts represent two of the more important factors that have pushed nursing home care delivery to meet residents’ individualized needs. As noted above, federal regulations play a major role in shaping the delivery of nursing home care in the United States. Since first getting involved in nursing home care with the passage of the Social Security Act of 1935 (IOM, 1986), the federal government has revised its regulations and standards for nursing homes multiple times in response to studies and reports describing deficiencies in care (IOM, 1986, 2001). The most current regulations are codified in the 2016 update of the consolidated Medicare and Medicaid requirements for participation for long-term care facilities.7
Nursing home advocacy groups have also led efforts to improve nursing home care. In 1997, several of these organizations coalesced under the umbrella of the Pioneer Network, whose work led to what is known as the culture change movement. The culture change movement is a broad-based
___________________
6 The current 45-page MDS 3.0 is available at https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/NursingHomeQualityInits/Downloads/Archive-Draft-of-the-MDS-30-Nursing-Home-Comprehensive-NC-Version-1140.pdf (accessed October 21, 2021).
7 CMS Requirements for Long-Term Care Facilities—Quality of Life, 42 CFR Part 483, Subpart B (2016).
TABLE 4-1 The Needs of Nursing Home Residents
| Domain* | Key Need Areas within Each Domain |
|---|---|
| Physiological Needs | Physical comfort; nutrition and hydration, warmth, sleep, personal hygiene (ADLs/continence); access to sunlight and fresh air; preservation of skin integrity; symptom management (e.g., pain, constipation, shortness of breath) |
| Safety and Security | Freedom from injury; provision of privacy; protection from development of and/or worsening of illness, including infection; security of personal possessions; freedom from noxious stimuli (e.g., noise, glare, odor); management of diagnosis-related medical issues and symptoms (including some aspects of rehabilitation); comfort with and sense of security regarding staff; certain aspects of support for mood and behavioral needs and expressions |
| Social | Companionship, affection, touch, family and other relationships, sense of inclusion, maximizing sensory perception and communication abilities, sexuality, support of cognitive needs |
| Self-Esteem | Functional competence, autonomy; dignity; self-expression; support for personal preferences, including customary routines, food and activity preferences, and engagement in activities that incur risk such as use of tobacco and alcohol; ability to initiate and engage in activities that are meaningful to the individual and that help maintain their identity; certain aspects of support for mood and behavioral needs and expressions |
| Achievement of Full Potential/Optimal Quality of Life | Enjoyment; participation in expressive/creative activities; maximization of physical, mental, and psychological function through ongoing opportunities, stimulation, and rehabilitation; absence or minimization of displeasure, anxiety, or boredom; opportunity for creation of legacies and life review; opportunity to express one’s spirituality and participate in religious and spiritual practices. |
SOURCE: Adapted from Bennett, 1980.
NOTE: * All domains are crucial to maximize quality of life; typically satisfying the first few areas listed in the table (physiological needs, safety, and security) is a prerequisite for satisfying the other areas (self-esteem and achievement of optimal quality of life).
effort to transform nursing homes from impersonal medical institutions into person-centered homes offering resident-directed long-term care services and supports, with the ultimate goal being the creation of vibrant communities of older adults and the people who care for and support them (Koren, 2010; Mitty, 2005; Pioneer Network, 2021; White-Chu et al., 2009). In order to achieve that goal, the culture change movement promotes a set of core principles (Box 4-1), many of which CMS has incorporated into its revised requirements for nursing homes requirements of participation.8
___________________
8 For the full CMS Requirements of Participation, see https://www.cms.gov/Regulations-and-Guidance/Legislation/CFCsAndCoPs/LTC (accessed October 21, 2021).
Early culture change efforts have included state-level efforts such as the development of the Promoting Excellent Alternatives in Kansas (PEAK) initiative that enabled the state to promote culture change through the survey process. State coalitions were formed in Arkansas and in other states such as Missouri, where a culture change coordinator was added to the survey agency to promote culture change adoption. These state-level efforts were incorporated into revisions of CMS’s Interpretive Guidelines for nursing home surveyors, which featured a greater focus on resident choice and autonomy (Beck et al., 2014; Doll et al., 2017; Grabowski et al., 2014a,b).
One large-scale study evaluated the impact of culture change on the quality of care of nursing home residents. The study found that the adoption of culture change was associated with a nearly 15 percent decline in survey deficiencies related to health care. The researchers interpreted these results as indicating that culture change has the potential to improve nursing home resident care outcomes (Grabowski et al., 2014b). Importantly, research reveals that a nursing home’s ability to implement culture change practices depends on the availability of financial and staff resources and that, as a result, nursing homes that are more heavily dependent on Medicaid financing may find it much more challenging to implement culture change practices (Miller et al., 2014; Shield et al., 2014). Such resource-limited nursing homes will likely require extra support, such as specialized training and assistance from experts from “high-performing nursing homes” (Chisholm et al., 2018).
A family member’s perspective of culture change in the nursing home setting was provided to the committee during its first public webinar by Kathy Bradley, the founder and chief executive officer of Our Mother’s Voice (see Box 4-2).
In addition to these various culture change initiatives, individual facilities and groups of facilities owned by the same organization or company have developed specific programs to deliver high-quality, resident-directed care in nursing home settings (Avila Institute, 2017; CAPC, 2008; Mead, 2013).9
Key Role of the Care Plan
The culture change movement counts resident-directed, person-centered care among its core tenets. In the nursing home setting, the care plan figures prominently in the provision of such care to residents. CMS requires that nursing homes develop and implement a comprehensive care plan for each person admitted to a nursing home either for post-acute care (“short-stay”) or long-term care (“long-stay”). The care plan must be based on a comprehensive assessment, developed using the MDS, of the resident’s goals and preferences, needs, and strengths. The comprehensive care plan is to include measurable goals and a timeframe in which the resident’s physical and mental health and psychosocial needs are met. Framed by federal and state regulations and guided by culture change principles, these care plans
___________________
9 An example of a culture change tool is the Artifacts of Culture Change 2.0. This is a recently updated self-assessment tool for nursing homes to determine the extent to which they have implemented culture change practices. For more information, see https://www.pioneernetwork.net/wp-content/uploads/2021/02/Artifacts_2.0_NH_Form_030521.pdf (accessed November 3, 2021).
are intended to address the residents’ full range of needs and can shape the quality of care and the quality of life for nursing home residents (Dellefield et al., 2015; Lepore et al., 2018).
A care plan is integral to assessing a resident’s individual needs, as discussed in the previous section of this chapter, and presents a plan to support each resident’s care, interests, strengths, and preferences. Residents and family members are expected to be involved in the development of the care plan to ensure that accurate and complete information is included.10 While the care planning process is focused on the individual resident, it is a shared effort in which the resident’s chosen family members are viewed as “co-creators” of the resident’s care plan (Chen et al., 2016; Scales et al., 2019). Ideally, the care plan should contain detailed documentation of “what matters” to the resident—defined as “knowing and aligning care with and older adult’s health outcome goals and care preferences.” Providing care that reflects “what matters” to the older adult is a key component of the age-friendly health system framework, and is compatible with—and facilitates—the provision of person-centered care (Adams-Wendling et al., 2008; Edelman et al., 2021; Koren, 2010). The comprehensive care plan is essential to ensure appropriate and adequate care delivery and improved resident health outcomes (Rantz et al., 2004). Health information technology, such as the use of an effective electronic health record, can play a key role in facilitating the nursing home resident care plan process, discussed in Chapter 9.
CMS 2016 regulatory updates require nursing homes to give residents the chance to become more directly engaged—or, as the revised regulation state, residents are to be the locus of control—in their own care planning. Residents work with nursing home staff to ensure that their goals and preferences are reflected in the plan and that, importantly, the plan is revised as the residents’ needs and preferences change over time (Lepore et al., 2018).
In addition, the updated guidelines specify that an interdisciplinary team (detailed in Box 4-3) that includes the attending physician, a registered nurse with responsibility for the resident, a nursing assistant with responsibility for the resident, a member of the nutrition services staff, and others who would provide care to the resident must prepare, implement, review, and revise the care plan as appropriate.11 In the case of services that the facility does not provide directly (e.g., laboratory, dialysis, dental, specialized behavioral health, pharmacy, hospice), the facility is responsible for managing those contracts and coordinating the associated services.12 Specific roles and functions of the individual care team members are discussed further in Chapter 5.
___________________
10 For more information, see https://theconsumervoice.org/uploads/files/issues/assessment__care_planning-final.pdf (accessed November 22, 2021).
11 CMS Requirements for Long-Term Care Facilities—Comprehensive Person-Centered Care Planning, 42 CFR §483.21 (2016).
12 Ibid.
The updated regulations specify that meetings of the interdisciplinary care team take place on a quarterly basis and include input from residents and their families. In addition, the care plan should be reviewed in the event of a significant change in a resident’s status. These changes are detailed by CMS in the Long-Term Care Resident Assessment Instrument User’s Manual.13 The MDS assessment of residents’ needs and the development and implementation of the care plan by the interdisciplinary care team are essential to providing high-quality, age-friendly care to nursing home residents (Edelman et al., 2021). Effective leadership at the RN level is critical to ensuring the accurate translation and integration of the care plan into nursing home operations (Dellefield, 2006; Forbes-Thompson et al., 2006). Taken as a whole, the updated care planning regulations help to advance nursing home care toward the goal of person-centered care (Lepore et al., 2018).
___________________
13 See MDS 3.0 RAI Manual v1.17.1 Replacement Manual Pages and Change Tables, October 2019 (cms.gov).
Continuing to Improve Care Assessment and Planning
Given its central role in identifying residents’ needs and developing an approach to address those needs, the resident care planning process is foundational to the provision of high-quality care in nursing homes. However, many nursing homes are not meeting care plan requirements. According to an analysis by the Department of Health and Human Services (HHS) Office of the Inspector General (OIG), the failure to develop comprehensive care plans represented the fifth most common nursing home deficiency type14 cited by state survey agencies over the period 2013 to 2017. Such care plan deficiencies represented slightly less than 10 percent of the total top 10 deficiencies over that time period (OIG, 2019). Previous OIG inspections found that for more than one-quarter of resident stays, the nursing home did not develop care plans that met federal requirements (OIG, 2013).
In general, the care assessment and planning process has weaknesses in three key areas that warrant improvement. First, care plans often focus on basic physiologic, safety, and security needs, such as nutrition, personal hygiene, skin integrity, falls, and infection. While meeting these needs is important and contributes to quality of life, an overemphasis on those needs can detract from addressing equally critical social, self-esteem, and quality-of-life needs (Calkins and Brush, 2016). For example, nursing homes rarely address the need for affection and physical connection, including sexual needs (Roelofs et al., 2015), and even when they do, their focus is generally on the safety and protection of vulnerable persons.
Second, opportunities to engage in creative expression are limited, as are meaning-making activities such as reminiscence therapy, which involves the use of photographs or music to evoke memories or generate conversation (Woods et al., 2018), or dignity therapy, which is an approach to help patients as they face the end of life (Cuevas et al., 2021) by focusing on psychosocial or existential distress (Allen et al., 2014; Goddard et al., 2013; Hall et al., 2013). In addition residents may also have limited volunteer opportunities that can promote social interaction and self-esteem. Finally, addressing needs for spiritual and existential care in nursing homes is uneven and limited despite the importance of these concerns for many nursing home residents (Morley and Sanford, 2014).
Other challenges involve residents’ rights related to choice and autonomy. Personal choice and autonomy are key components of self-esteem (see Table 4-1). The resident’s right to self-determination was enacted into law as part of the Nursing Home Reform Law of 1987,15 and as noted earlier,
___________________
14 A nursing home’s failure to meet a federal participation requirement is defined as a deficiency. Examples of deficiencies include a nursing home’s failure to adhere to proper infection control measures and to provide necessary care and services (OIG, 2019).
15 Nursing Home Reform Law of 1987, Public Law 100-203, 42 USC 1395i-3, 100th Cong., 1st Sess., (December 22, 1987).
updated CMS guidance reinforces and strengthens the rights of residents to exercise maximal choice and autonomy (Beck et al., 2014; Doll et al., 2017; Grabowski et al., 2014a). Despite the significant positive associations among residents’ choice, sense of autonomy, and quality of life (Bhattacharyya et al., 2021; McCabe et al., 2021), residents often report limited choice and autonomy (Moilanen et al., 2021). Furthermore, observational studies of staff interactions with residents reveal that resident daily choices such as food, ambulation, and socializing often are curtailed, sometimes without staff awareness of the restrictions they impose (Bhattacharyya et al., 2021). Reasons for these limitations are multifactorial and include staff concerns about causing harm to residents; staff knowledge, attitudes, and habits; lack of time to offer choices; and fear of survey deficiencies, complaints, and legal action (Bekkema et al., 2021; Calkins and Brush, 2016).
Respecting resident autonomy is particularly challenging in situations where preferences clash with best clinical practices, safety, and the rights of other residents (Calkins and Brush, 2016; Sherwin and Winsby, 2011). These potential conflicts can be as seemingly mundane as keeping the volume on the TV too high because of hearing loss, thereby disturbing one’s roommate or others in nearby rooms. These potential conflicts can, however, include more serious issues such as a resident’s refusal to be vaccinated against the COVID-19 virus, for example, which could put other residents, staff, and families at risk. Another common dilemma is the resident’s desire to ambulate independently, which may increase the chance of falling. A recent, poignant example is the imposition of visitation restrictions during the COVID-19 pandemic; residents’ rights and need to socialize were severely curtailed to limit the spread of infection. Very often, mitigating risk is prioritized over residents’ autonomy in nursing homes.
Efforts to address these issues have focused on using structured, shared decision-making approaches to balance autonomy and risk, although the nursing home sector has not adopted these approaches widely (Behrens et al., 2018; Calkins and Brush, 2016). Making progress toward honoring residents’ choices will likely also require a recalibration and re-interpretation of quality indicators such as fall rates (Brauner et al., 2018; Davila et al., 2021).
Identifying and Addressing Unmet Needs
Unmet health care needs can be viewed as the gap between the care and services necessary to address a specific health issue or condition and the actual care that an individual receives (Herr et al., 2014). Research examining unmet needs from the perspective of nursing home residents is relatively rare; what is available focuses on the absence of care itself and on clinical outcomes that can result from inadequate care. Among the health outcomes most often attributed to inadequate care in nursing homes are
avoidable hospitalizations, pressure ulcers, falls, infections, pain, malnutrition, and a higher risk of mortality and lower quality of life (Kalánková et al., 2020; Ogletree et al., 2020). Studies conducted in nursing homes in the United States and Europe indicate that the unmet needs that nursing home residents identify most commonly include timely assistance with ADLs (including mobility), meaningful daytime activities, sensory (vision, hearing) and communication issues, and accommodation for disabilities (Freedman and Spillman, 2014; Tobis et al., 2018; van den Brink et al., 2018). These unmet needs reflect a neglect of physical care, which is a serious ethical and clinical violation (Kalánková et al., 2020). Psychosocial needs (e.g., companionship, relief from distress) are ranked highly in most studies of unmet needs among nursing home residents, with residents having suffered even greater neglect with lockdowns and isolation during the COVID-19 pandemic (Kemp, 2021; Ruopp, 2020; Simard and Volicer, 2020). Addressing unmet needs is critical to residents’ well-being and quality of life.
Residents with higher levels of disability tend to identify both more reported needs and more unmet needs. In contrast, persons with cognitive impairment report fewer needs and fewer unmet needs, which is not surprising since an awareness of need and the ability to communicate need verbally can be impaired in these individuals (Duan et al., 2020; van den Brink et al., 2018). There are two caveats to these findings; first, nursing home residents may hesitate to speak up when asked by staff about unmet needs, and second, persons in settings with fewer resources may identify fewer unmet needs, believing that expressing these needs is futile. As a result, it is important to include perspectives and sources beyond residents to identify gaps in care and unmet needs (Duan et al., 2020).
Certain subpopulations of nursing home residents appear to have particularly high levels of unmet needs. The key characteristics of these subpopulations include racial or ethnic minorities, individuals who lack fluency in English, individuals with moderate or advanced cognitive impairment, and those with aphasia or other communication challenges (Berridge and Mor, 2018; Cooper et al., 2018; Kalánková et al., 2020). In addition, certain facility factors appear to be associated with higher levels of unmet needs, including a large share of residents being on Medicaid; higher resident-to-staff ratios; poor-quality nursing leadership or high leadership turnover, or both; and high proportions of contracted staff relative to employed staff (Castle and Engberg, 2007; Mor et al., 2004). (See Chapter 5 for more discussion on issues related to employed and contracted nursing home staff.)
Subpopulations that may have high levels of unmet needs include residents who do not speak English and are in nursing homes that do not have staff members who speak their native language or English-speaking residents in homes where staff have limited English proficiency. Addressing language
barriers between residents and staff takes on greater importance as residents’ diversity increases, as discussed in Chapter 2. Language barriers and associated miscommunication can negatively impact health outcomes and lead to lower patient and staff satisfaction and care that is not aligned with an individual’s preferences (Al Shamsi et al., 2020; Forsgren et al., 2016). Nursing homes are required by law to communicate medical information to residents in their native language.16 A range of approaches can be used to address language barriers in health care settings, including professional interpreters (which increases costs), family members or friends as interpreters, or online translation tools (Al Shamsi et al., 2020).17
Despite the best intentions and efforts on the part of nursing home staff, however, some unmet needs will always exist. For example, some things that residents may want are either too detrimental to their wellbeing, such as smoking, refusing medications, or not bathing, or pose a risk to others in a congregate setting. Furthermore, nursing home staff will always have more things that they could be doing for residents than are possible, considering the realities of not being able to provide one-on-one care and not having all possible skills and techniques available in all nursing homes at all times. A key role of members of the nursing home leadership team is to help identify and prioritize the care needs of each individual resident. Box 4-4 provides a family member’s perspective on identifying and addressing unmet needs.
___________________
16 CMS Requirements for Long-Term Care Facilities—Resident Rights, 42 CFR § 483.10 (c)(1) (2016).
17 One example is SEIU 1199’s Training and Employment Fund’s English for Speakers of Other Languages program (see: https://www.1199seiubenefits.org/esol) (accessed April 22, 2022).
PROVIDING CARE TO ADDRESS RESIDENTS’ NEEDS
As discussed in the previous section of this chapter, the care plan documents the needs and preferences of each individual nursing home resident and serves to guide the provision of necessary health care services. The wide range of services to address the varied needs of nursing home residents are discussed in the sections that follow, organized according to Maslow’s hierarchy of needs.
Physiological Care
This section examines the first level of Maslow’s hierarchy—basic needs—exploring the ways in which nursing homes provide for the varied physiological care needs of nursing home residents. Nursing homes provide care to two different groups of people who have distinct physiological care needs: short-stay individuals who require post-acute care after a hospital stay of at least 3 days,18 and long-stay residents who have a more diverse range of care needs. The broad diversity of clinical needs of nursing home patients combined with their vulnerability to adverse outcomes complicates the challenge of providing quality care in the nursing home setting (Yurkofsky and Ouslander, 2021).
Nursing homes serve as a place for recuperation that provides post-hospitalization therapies and supports. Twenty percent of all hospitalized Medicare beneficiaries are discharged to skilled nursing facilities for post-acute care (MedPAC, 2021). These short-stay patients receive physical, occupational, and speech therapy as required to make the gains in function necessary to be discharged from the nursing home (Yurkofsky and Ouslander, 2021).
As discussed further in Chapter 7, a new reimbursement method known as the patient-driven payment model (PDPM) took effect in late 2019, replacing the previous system based on resource utilization groups. The PDPM approach to payment, which is based on the complexity of patient care rather than minutes of therapy provided, has resulted in a decrease in the volume of therapy services provided in nursing homes (McGarry et al., 2021).
Long-stay residents tend to need assistance with ADLs, and to have high rates of medically complex conditions that often require multiple medications and skilled nursing care (Fashaw et al., 2020; Katz et al., 2021). The most common of the complex conditions faced by nursing home residents include Alzheimer’s and related dementias (47.8 percent of residents), diabetes (32 percent), heart disease (38.1 percent), and hypertension (71.5 percent) (Harris-Kojetin et al., 2019).
___________________
18 The medically necessary inpatient hospital stay of 3 consecutive days or more (CMS, 2019a) requirement was waived during the COVID-19 pandemic (CMS, 2021a).
Assistance with ADLs
Many nursing home residents require assistance with routine but essential ADLs such as eating, bathing, and mobility (Table 4-2). A person’s ability to accomplish these activities independently determines his or her functional status and serves as a predictor of nursing home admission (Edemekong et al., 2021). Federal regulations require that nursing homes maintain the resident’s condition or prevent or slow further deterioration of a resident’s ability to perform these activities (CMS, 2019b) and that they provide the necessary services to enable residents to maintain good nutrition, grooming, and personal oral hygiene if they need assistance with those tasks. As noted in Chapter 2, most residents require assistance with one or more ADLs (Harris-Kojetin et al., 2019).
Ambulating
Nursing home residents face ambulatory challenges ranging from difficulty walking to an inability to get out of bed by oneself. Nearly two-thirds of nursing home residents depend on a wheelchair or require extensive support from others to move around. According to data available from CMS,19 an average of 3.7 percent of nursing home residents in 2016 were either in a bed or a recliner for 22 or more hours per day. More than one-fifth of nursing home residents suffered from contractures, which are limitations on the full range of motion of any joint resulting from deformity, lack of use, or pain (Harrington et al., 2018).
TABLE 4-2 Activities of Daily Living (ADLs)
| ADL Category | Description |
|---|---|
| Ambulating | The extent of an individual’s ability to move from one position to another and walk independently. |
| Feeding | The ability of a person to feed oneself. |
| Dressing | The ability to select appropriate clothes and to put the clothes on. |
| Personal hygiene | The ability to bathe and groom oneself and to maintain dental hygiene, nail and hair care. |
| Continence | The ability to control bladder and bowel function. |
| Toileting | The ability to get to and from the toilet, using it appropriately and cleaning oneself. |
SOURCE: Edemekong et al., 2021.
___________________
19 CMS has a national database of all data elements collected by state survey agencies during the annual Medicare and Medicaid certification inspection. The Online Survey, Certification and Reporting System (OSCAR) and the Certification and Survey Provider Enhanced Reporting (CASPER) system capture state-level nursing home information on characteristics of nursing home facilities, residents, staffing, and deficiencies.
Pressure injury
A lack of mobility presents a danger to nursing home residents as it can result in pressure injuries (previously referred to as pressure ulcers and informally known as bedsores), localized damage to the skin and/or underlying tissue that results from pressure, friction, or a lack of proper blood flow when an individual remains in bed or in one position for long periods of time (Bhattacharya and Mishra, 2015; Mäki-Turja-Rostedt et al., 2018). Pressure injuries cause pain and create a vicious cycle in which the pain leads to reduced mobility, which leads to more pressure injuries and even more pain, and so on; at the same time, the reduced mobility and pressure injuries also heighten the resident’s risk for infection and mortality. Both short- and long-term nursing home residents are at risk for pressure injuries due to factors such as a lack of mobility after surgery, cognitive impairment, incontinence, hip fracture, and strokes (Harrington et al., 2018). Other factors that increase the risk for pressure injuries include more severe illnesses upon admission, history of recent pressure injuries, nutritional challenges, and use of positioning equipment or catheters (Horn et al., 2004, 2010). Pressure injuries are considered among the most common medical errors across inpatient and outpatient settings in the United States (Van Den Bos et al., 2011).
Pressure injury is an important indicator of quality in the nursing home setting. More than 8 percent of active nursing home residents20 had one or more unhealed pressure ulcers as of Q2 in 2021 according to MDS 3.0 frequency reports (CMS, 2021b). More than 75 percent of residents received special skin care to prevent or reduce such injuries (Harrington et al., 2018). Nursing homes are required to document all interventions to address pressure injury, including the use of devices to relieve pressure, protocols related to positioning and turning, and any wound treatments. Nursing home care team members have a key role to play in the identification of risk factors for pressure injury and in bringing in physical and occupational therapists, dieticians, and wound care specialists to implement care interventions (Yurkofsky and Ouslander, 2021). Specifically, research indicates that higher RN staffing hours per resident and higher nurse aide staffing hours per resident (certified nursing assistants or licensed practical nurses) were associated with fewer pressure ulcers (Castle and Anderson, 2011; Horn et al., 2004, 2005).
Nutrition and hydration
CMS regulations require nursing homes to provide each resident with adequate food and liquids to maintain proper nutrition and hydration. Ensuring that each individual resident’s eating needs are met
___________________
20 “An active resident is a resident whose most recent assessment transaction is not a discharge and whose most recent transaction has a target date (assessment reference date for an assessment record or entry date for an entry record) less than 150 days old” (CMS, 2021b).
is challenging in the nursing home setting, given the large share of residents with eating difficulties and the variation in residents’ degrees of dependency, preferences, and routines (Liu et al., 2014).
Dehydration
In addition to nutritional challenges, nursing home residents are particularly vulnerable to dehydration because of age-related physiological changes, such as deteriorating kidney function, a reduced ability to sense thirst, and reduced muscle mass (which limits the amount of water that is typically stored in muscles). The risk of dehydration is especially acute for nursing home residents with cognitive impairments that make it difficult for them to communicate that they are thirsty, with conditions that reduce appetite and fluid intake, or with physical impairments that prevent them from obtaining sufficient fluids. Certain medications such as diuretics also increase the risk of dehydration. Interventions including offering fluids to residents on a regular basis have resulted in a lower prevalence of dehydration in nursing homes (Greene et al., 2019; Yurkofsky and Ouslander, 2021).
Weight loss
The MDS quarterly reassessment process includes assessing for weight loss, which CMS views as a quality indicator for nursing home care. Cases in which a resident’s weight changes 5 percent over a 30-day period or 10 percent over a 6-month period require nursing homes to review care plans. Research shows that an unintentional weight loss of 5 percent is associated with a significantly increased risk of mortality (Sullivan et al., 2004; Yurkofsky and Ouslander, 2021). Approximately 6 percent of active nursing home residents had weight loss (not physician prescribed) as of Q2 in 2021 according to MDS 3.0 frequency reports (CMS, 2021b).
Many nursing home residents face difficulties maintaining adequate nutrition and hydration. This is particularly true for individuals admitted to nursing homes after a hospital stay, where they may have been designated “nothing by mouth” or have been on a restricted diet, either because of surgery or the need to conduct imaging studies. Another factor is the difficulty of aligning food offerings in institutional settings such as nursing homes with each resident’s individual preferences. Conditions such as gastrointestinal disorders, delirium, and pain can affect a resident’s nutritional status and ability to maintain weight, as can a terminal illness, depression, medication side effects, and a chronic illness that affects appetite, chewing, swallowing, or digesting (Ahmed and Haboubi, 2010; Pilgrim et al., 2015; Wells and Dumbrell, 2006). Weight loss and reduced food intake commonly occur as people near the end of life (Agarwal, 2021; Pilgrim et al., 2015).
The multiple conditions and complex care regimens of nursing home residents make the clinical management of nutritional needs extremely challenging for those providing care for nursing home residents (Liu et al., 2014; Palese et al., 2018). Research has identified a number of factors that
are critical to ensuring adequate nutritional care in the nursing home setting, including assessing the barriers to adequate nutrition; reducing risk factors; attending to specialized diets, altering food presentation, providing supplements when appropriate; being aware of the importance of psychosocial and environmental issues; and considering the role of medication both as a cause and therapeutic adjunct (Sloane et al., 2008). Given that a key issue for many nursing home residents is adequate nutritional intake, groups such as the American Diabetes Association have recommended minimizing the use of restrictive diets (Munshi et al., 2016).
Other nutritional and weight loss–related interventions in the nursing home setting include involving speech and occupational therapists and behavioral health clinicians to address the factors driving weight loss, which can range from the problems listed above to ill-fitting dentures. For example, for residents who have difficulty handling utensils as a result of reduced dexterity resulting from stroke, arthritis, or a fracture, nursing homes can provide special utensils with easier-to-grasp handles, while speech and occupational therapists can target difficulties swallowing. Moreover, registered dieticians can conduct nutritional assessments and specify dietary options, including providing nutritional supplements for residents facing weight loss (Yurkofsky and Ouslander, 2021).
Meeting residents’ nutritional needs
Meeting nursing home residents’ nutritional needs often requires the provision of feeding assistance to those who cannot feed themselves (Batchelor-Murphy et al., 2019; Kilgore, 2014; Yurkofsky and Ouslander, 2021). Federal regulations mandate that each residents’ nutritional needs and related care preferences be met with sufficient staff, including a qualified dietitian or other clinically qualified nutrition professional and support staff, which may also include feeding assistants.21 Studies have found, however, that many nursing homes do not have sufficient staff to meet resident needs (Simmons and Bertrand, 2013; Simmons and Schnelle, 2004, 2006; Simmons et al., 2008). Weight loss and dehydration have been found to be associated with inadequate nursing care and lack of assistance with eating and drinking (Simmons and Schnelle, 2004, 2006; Simmons et al., 2008).
Nutritional challenges were further complicated by the COVID-19 pandemic, which disrupted communal dining and exacerbated existing staff shortages. Moreover, poor nutrition was found to increase older adults’ risk of contracting COVID-19 as well as other chronic conditions (Keser et al., 2021).
___________________
21 CMS Requirements for Long-Term Care Facilities—Food and nutrition services, 42 CFR § 483.60 (2016).
Continence and toileting
The most common needs of nursing home residents are related to bladder or bowel incontinence. One study found that nearly 65 percent of residents had bladder incontinence and nearly 45 percent had bowel continence in 2016 (Harrington et al., 2018). Bladder or urinary incontinence is associated with increased risks of hospitalization, urinary tract infections, and pressure injuries, and it has a significant effect on quality of life. CMS uses the development of urinary incontinence as a quality indicator for long-term nursing home residents (Dubeau et al., 2006; Yurkofsky and Ouslander, 2021), and at least one analysis found associations between urinary incontinence and poorer self-reported quality of life in the domains of dignity, autonomy, and mood (Xu and Kane, 2013).
Interventions include developing toileting schedules and prompted voiding, which both require staff assistance to review the care plan and schedule, and also conducting regular check-ins with residents on their continence needs and abilities. Other interventions include exercises to improve mobility and control, dietary interventions such as increasing fluid and fiber intake, and supplementary interventions such as using laxatives or stool softeners (Leung and Schnelle, 2008). Regular review of all interventions is particularly important to maintain residents’ safety (e.g., preventing from falls) and dignity, as continence care often goes beyond social norms of privacy and touch (Ostaszkiewicz et al., 2020). One study found that using an improved assessment tool reduced the rate of incontinence among nursing home residents without a toileting plan from 79 to 38 percent (Morgan et al., 2008). Use of clinical guidelines, standardized assessments, and regulatory enforcement as well as leveraging organizational culture change practices have been identified as ways to enable nursing homes to meet residents’ continence and toileting needs (Lyons, 2010).
Post-Acute and Rehabilitation Care
Nursing homes provide rehabilitation services for two different groups of individuals—short-stay patients and long-term nursing home residents, with each having different care and rehabilitation needs. Approximately 1.5 million Medicare fee-for-service beneficiaries received such services in the nursing home setting in 2019 (MedPAC, 2021).
Short-stay patients
Some patients require intensive rehabilitation services after surgery, an illness, or injury (MedPAC, 2020). Most nursing homes provide post-acute care, recuperation, and rehabilitation services, such as the continuation of intravenous antibiotics or a course of physical, occupational, or speech therapy. Nearly one-third of nursing home admissions in 2016 involved post-acute or rehabilitation services (Harrington et al., 2018). Medicare covers post-acute care in nursing home facilities, and ensures
skilled services are covered to maintain a resident’s condition or prevent or slow a decline or deterioration of the resident’s condition (CMS, 2021c). Post-acute care in a skilled nursing facility is designed to be short term, a “bridge to home” (Flint et al., 2019).
Patients are most commonly referred to nursing homes for post-acute care for septicemia (sepsis), joint replacement, heart failure and shock, hip and femur procedures, and pneumonia (MedPAC, 2020). These patients are expected to make gains in function from continuing medical therapy and rehabilitation services, most often a combination of physical therapy focused on mobility (including wheelchair mobility), occupational therapy focused on self-care issues such as dressing and feeding, and speech therapy focused on eating, swallowing, and communication problems (Yurkofsky and Ouslander, 2021).
Rehabilitation care can either be active, involving the resident engaging in physical exercise, for example, or passive, involving the use of ultrasound or whole-body vibration. Rehabilitation care in the nursing home setting can be provided by a nurse, physiotherapist, kinesiologist, rehabilitation aide, or fitness instructor in a small group (up to six people) or on an individual basis (McArthur et al., 2015). As noted above, the new PDPM payment system has reduced the amount of therapy provided to nursing home residents.
In an effort to monitor the quality of rehabilitation care provided in the nursing home setting, CMS added new quality measures for short-stay patients to Nursing Home Compare in 2016. Previous star ratings did not distinguish between the quality of care for short-stay and for long-stay nursing home residents. The ratings for the quality of care for short-stay rehabilitation services include measures related to emergency room visits and rehospitalizations, control of pain and treatment of pressure injuries, and independent movement as an element of recovery (Graham, 2019). The new measures are important indicators of nursing home quality. Whereas discharge from nursing homes to the community after a short-term stay has been identified as a critical sign of person-centered care, rehospitalizations and transfers from nursing homes to emergency departments are viewed as potential signs of inappropriate or inadequate nursing home care that leave residents vulnerable to adverse health events while in the hospital. By providing additional information, these new measures enhance the nursing home five-star composite ranking. An early analysis of the measures revealed an association between improved performance on the new measures and nursing home characteristics such as fewer deficiencies, higher staffing and more skilled staffing, nonprofit ownership, and lower proportion of Medicaid residents. The study’s authors emphasized the importance of better understanding of these measures, in light of CMS’s plans to include the measure on rehospitalizations in the value-based purchasing program for nursing homes, discussed further in Chapter 7 (Saliba et al., 2018).
Long-stay patients
Although the goal for short-term post-acute care patients is to regain functional independence, for long-term residents, the goal is to maintain functional abilities to maintain the best quality of life (Graham, 2019). A wide range of physical rehabilitation services are available in the nursing home setting to help residents maintain mobility, strength, and balance, or focus on a specific ADL.
In 2011, patient advocates filed a lawsuit, Jimmo v. Sebelius, arguing that Medicare was denying coverage for therapy based on a patient’s lack of improvement or progress. The Jimmo settlement agreement specified that coverage of therapy services is not determined by the “presence or absence of a beneficiary’s potential for improvement or restoration, but rather on the beneficiary’s need for skilled care.” The agreement clarified that rehabilitative care may be necessary to improve or maintain an individual’s current condition or to prevent further deterioration. The agreement also provided that the Medicare benefit policy manual must include these clarifications (CMS, 2019b, 2021b).
Restorative Care for Long-Stay Residents
Nursing homes also provide restorative care programs to respond to the federal regulations to provide each resident with the “necessary care and services to attain or maintain the highest level of physical, mental, and psychosocial well-being in accordance with the comprehensive assessment and plan of care.”22
Restorative care can be defined as an approach to care that focuses on evaluating residents’ functional capabilities in areas such as walking, range of motion, bed mobility, dressing, eating, swallowing, and communicating. Restorative care reimbursed by Medicare is typically provided to residents who need to maintain functional gains after completing physical, occupational, or speech therapy, or for residents who experience a decrease in function. One study found that although 66 percent of nursing homes provided restorative care programs, less than one-third of long-stay nursing home residents participated in such programs. The study recommended considering implementing restorative care programs as a “philosophy of integrated care” rather than as discrete activities. Proponents of this approach emphasize the importance of training all nursing home staff to integrate activities that promote function and physical activity into all resident interactions (Talley et al., 2015).
___________________
22 CMS Requirements for Long-Term Care Facilities—Quality of Care, 42 CFR § 483.25 (2016).
Pain and Symptom Management
Given that a significant share of nursing home residents have multiple chronic conditions, the management of pain and symptoms is a critical element of care that nursing homes deliver to their residents. Many nursing home residents experience pain, and the appropriate management of pain is critical to their quality of life. Studies that revealed extensive under-treatment or lack of treatment of pain in nursing homes led CMS to enact policy changes that included strengthening nursing home guidance on pain for surveyors in 2009 as well as enhanced measures of pain in MDS 3.0 (Yurkofsky and Ouslander, 2021).
A large share of all nursing home residents—up to 80 percent—experience persistent pain, such as that related to arthritis (Hunnicutt et al., 2017a; Nakashima et al., 2019). Others experience acute pain caused by a new medical or surgical condition, including post-operative pain. Finally, pain at the end of life is common among nursing home residents (Andersson et al., 2018; Teno et al., 2018). The provision of palliative care and hospice care in the nursing home setting is discussed in greater detail later in this chapter.
A study of more than 1.3 million long-stay nursing home residents from 2011 to 2012 found that nearly 39 percent experienced at least some pain and that nearly 20 percent had persistent pain. Of the residents with persistent pain, 6.4 percent received no pharmacologic pain management, and more than 30 percent were undertreated (received no scheduled analgesics for their pain). The study also revealed race and ethnicity disparities as higher rates of untreated and undertreated pain as non-Hispanic Black, Hispanic, and other race/ethnicity residents had higher rates of untreated and undertreated pain compared to White residents. The study concluded that although the prevalence of untreated pain had declined since the enactment of the policy changes and enhanced guidance referred to above, the overall prevalence of pain among nursing home residents is still high. The study called for further research on promoting equity in pain management as well improving overall pain management practices in nursing homes (Hunnicutt et al., 2017b).
Another study examined nursing home residents who required staff to assess their pain because of their inability to do so themselves. The study found that staff documented pain and its treatment less frequently in non-Hispanic Black residents and Hispanic residents than in non-Hispanic White residents. Researchers called for further study to further elucidate differential pain expression, explicit bias, and implicit bias. An enhanced understanding of these factors will enable the design of specific interventions to lessen existing disparities in pain management and treatment (Morrison et al., 2021).The awareness of factors related to differential expression of pain is particularly important in providing care for nursing home residents
with dementia. Research indicates that 60 to 80 percent of nursing home residents with dementia experience pain on a regular basis (Corbett et al., 2012). It is challenging, however, to effectively assess and manage pain in residents with dementia given difficulty these residents typically have communicating about their pain to nursing home staff. As a result, residents with dementia often express pain through behavioral symptoms, such as agitation or wandering, which can then lead to mismanagement of pain (Achterberg et al., 2019). Improved understanding of the factors associated with differential expression of pain among nursing home residents will facilitate the development of specific interventions to lessen existing disparities in pain management and treatment (Morrison et al., 2021).
Oral Health Care
Oral health has a significant effect on an individual’s physiological and social well-being. Poor oral health is associated with pain, reduced function, malnutrition, and a range of medical conditions including cardiovascular disease, pulmonary health issues, and aspirational pneumonia. In addition, research has identified associations between diabetes and periodontal disease, tooth loss, and oral cancer as well as an increased risk of cognitive impairment and dementia with gingivitis, dental caries, or tooth loss (Porter et al., 2015; Sifuentes and LaPane, 2020; Zimmerman et al., 2017). Moreover, symptoms related to poor oral health care, such as bad breath and altered speech, can affect self-esteem and quality of life (Hoben et al., 2016; Maramaldi et al., 2018). Key risk factors for poor oral health among nursing home residents include having Alzheimer’s or other forms of dementia, receiving hospice care, and having a longer length of stay (Zimmerman et al., 2017).
Because of the critical role that oral health plays in overall health, federal regulations require nursing homes to provide services that enable residents to maintain good oral hygiene.23 Specifically, regulations require nursing homes to
- Conduct an oral health assessment of each resident upon admission and quarterly and annually thereafter and record the information in the MDS;
- Meet residents’ routine and emergency dental service needs using outside services;
- Make appointments for residents requesting dental care and arrange for transportation;
___________________
23 CMS Requirements for Long-Term Care Facilities—Resident Assessment, 42 CFR § 483.20 (2016).
- Apply for dental service reimbursement; and
- Refer residents with lost or damaged dentures within 3 days.
Nonetheless, fewer than one in five nursing home residents receive daily assistance with oral health care, such as tooth brushing. Moreover, only 15 percent have very good or better oral hygiene (Coleman and Watson, 2006; Sifuentes and Lapane, 2020; Zimmerman et al., 2017).
One reason for this deficiency may be that the responsibility for conducting an oral health assessment typically falls on certified nursing assistants (CNAs), many of whom lack specific oral health training (Sifuentes and Lapane, 2020). Another reason may be that while nursing homes are required to conduct oral health assessments, they are not required to provide routine dental services for all residents. Medicaid is the primary payer for the large majority of long-stay nursing home residents; consequently nursing homes provide routine dental services only if the Medicaid plan of the particular state in which the nursing home is located covers such routine dental services. Given the high cost of dental health care services, Medicaid beneficiaries are typically unable to afford to pay out of pocket for such care. Compounding the problem is that many states have responded to fiscal pressures by trimming or eliminating Medicaid dental coverage. Additionally, even in states with Medicaid dental coverage, beneficiaries often face great difficulty locating dental providers who accept Medicaid, given that only 20 percent of all dentists participate in the Medicaid program (Northridge et al., 2020).
Providing oral health care in the nursing home setting
Assistance with daily oral health care for nursing home residents is typically the responsibility of the CNAs, who do not receive necessary training to provide oral health care assistance and typically face significant competing demands on their time. Additional challenges include staff perceptions that oral health care is not a priority, staff hesitancy or unwillingness to perform the tasks, and resident resistance to staff assistance with their oral care. Further complicating the delivering of oral health care services to nursing home residents is the increasing prevalence among current nursing home residents of dental prostheses and bridges that require complex care to maintain. As noted earlier, a large share of nursing home residents have some form of dementia and typically require assistance with basic oral care, while at the same time often making it challenging to staff to provide such care. As a result, oral care practices in nursing homes tend to be of poor quality, characterized by insufficient or improper tooth brushing. For example, one study (Coleman and Watson, 2006) revealed that, on average, CNAs brush residents’ teeth for 16 seconds, a significantly shorter timespan than the American Dental Association’s recommended 2 minutes of brushing (Hoben et al., 2016; Porter et al., 2015; Sloane et al., 2013; Zimmerman et al., 2020).
Another important element of high-quality daily oral care is providing and using appropriate supplies. Toothbrushes should have soft bristles, be replaced every 3 months, and be stored in a manner that allows them to dry and that prevents infection. For individuals who have difficulty swallowing, toothpaste can cause choking, so for many residents an alcohol-free rinse is preferable. Cleaning between the teeth can be done safely with an interdental brush, which also should be changed every 3 months. Given the importance of infection control, steps such as hand washing, the use of gloves and mask by the care provider, and using an antimicrobial rinse with alcohol for cleaning toothbrushes and interdental brushes are critical (Sloane et al., 2013).
Innovative approach to improving oral health care
Given the importance of good oral health care to overall health outcomes and quality of life, and the high level of unmet need, researchers have developed some promising practices to improve the oral health care of nursing home residents. Interventions have included developing comprehensive oral health training programs for CNAs and other nursing home staff members, and the identification of a staff member as the oral health specialist (VanArsdall and Aalboe, 2016).
One evidence-based, person-centered care approach, Mouth Care Without a Battle (MCWB), trains nursing home staff to provide oral health care to residents with dementia who typically resist assistance with oral health care. Nursing homes that participated in a MCWB staff training program reduced the incidence of pneumonia in their facilities by 26 to 31 percent during the first year of the program, though that effect faded in the second year of the intervention. Sustaining the benefits of this approach may require the support of dedicated oral care aides to ensure that the nursing home staff continues to follow best practices (Zimmerman et al., 2020).
Among the interventions to improve oral health care in nursing home settings are efforts to enable effective mouth care in nursing home residents with dementia. Residents with dementia tend to exhibit care-resistant behaviors (CRBs) that put them at risk for inadequate mouth care and potential illnesses. Managing Oral Hygiene Using Threat Reduction, a nonpharmacologic, relationship-based intervention, has been shown to be effective in managing CRB during mouth care, resulting in higher rates of completing oral care activities for residents with dementia in a randomized study with a control group (Jablonski et al., 2018).
Hearing and Vision Care
Hearing and vision impairments, common among nursing home residents, can diminish the quality of life for nursing home residents and are associated with falls, social isolation, depression, problems with memory, and cognitive impairment (McCreedy et al., 2018; Williams et al., 2020;
Yurkofsky and Ouslander, 2021). These impairments can also hinder a resident’s ability to communicate effectively, particularly if staff members do not face a resident when they are speaking to them or block facial cues by covering their face with their hands or a mask (Andrusjak et al., 2020; McCreedy et al., 2018).
Some hearing and vision impairments can be reversed through cataract surgery, the use of hearing aids or glasses, or regularly checking for impacted earwax (Yurkofsky and Ouslander, 2021). Research has shown that these relatively simple corrective measures improve quality of life and reduce depression and psychological distress among nursing home residents (Owsley et al., 2007a,b). However, most nursing home residents’ sensory impairments go undetected for a variety of reasons, including the limited availability of evidence-based guidance or training for staff members, staff members’ inability to both identify and manage residents’ impairments, and the assumption that hearing and vision loss is a normal part of aging. Moreover, staff or family may mistake sensory loss as evidence of cognitive decline among residents with dementia. A lack of partnership with external hearing and vision services and inadequate insurance coverage can be additional barriers to providing hearing and visual care (Andrusjak et al., 2020).
Estimates suggest that between 67 and 86 percent of adults who could benefit from hearing aids are not using them (Bainbridge and Ramachandran, 2014; Chien and Lin, 2012; NASEM, 2016). The high cost of hearing aids—typically $2,000 per ear—is a significant barrier (McCreedy et al., 2018; Strom, 2014). Medicare covers 80 percent of the cost of a hearing evaluation but does not provide coverage for hearing aids, while Medicaid pays for some of the cost of hearing aids but only in 31 states. Even then, reimbursement rates are typically low (McCreedy et al., 2018; NASEM, 2016; Weber, 2021; Yurkofsky and Ouslander, 2021).
The 2017 Over-the-Counter (OTC) Hearing Aid Act24 created a class of wearable hearing devices for people with mild to moderate hearing loss. The Food and Drug Administration (FDA) will regulate these hearing aids as medical devices and is expected to issue guidelines for this new category by mid-2022. As an alternative to hearing aids available from audiologists or other hearing specialists, OTC hearing aids will be available for purchase in stores and online (NIDCD, 2021). While the availability of a new class of hearing aids may make such aids more affordable, it may also create additional barriers to accessibility. For example, by separating assessments for hearing aids from health care encounters, people who are unable to afford services may struggle to access care or use their hearing aids without counseling for proper fit and adjustments (Willink et al., 2019).
___________________
24 Over-the-Counter Hearing Aid Act of 2017, S. 670, 115th Cong., 1st Sess., Congressional Record, no. 163 (March 21, 2017).
Even if a nursing home identifies a resident as having a hearing or vision impairment, additional barriers exist to managing these impairments. Residents may have limited dexterity or some other limitation that makes it difficult to manage their own hearing aids or glasses, they may feel that the assistive devices would be of no use to them, or they may be put off by the discomfort of wearing an assistive device that has not been properly fitted. Residents can lose or misplace their hearing aids and glasses, batteries for hearing aids may die without being noticed, and residents may refrain from using them because of perceived stigma. Moreover, residents with dementia may be unable to advocate effectively for help with hearing or vision problems (Andrusjak et al., 2020). Finally, the nursing home environment itself can play a large role, given that nursing homes can be noisy, poorly insulated, or poorly lit, creating additional challenges for residents with sensory impairments (McCreedy et al., 2018).
Current Challenges in Physiological Care Quality
Ensuring that nursing home residents’ basic physiological care needs are met is critically important to providing person-centered care and to maintaining or improving a resident’s quality of life. Resident needs such as toileting, repositioning, mobility, and feeding assistance “represent a care activity that is both time-consuming and required multiple times per day for a substantial proportion of LTC residents” (Simmons et al., 2013, p. 152). Inadequate attention to residents’ basic care needs can endanger their health and well-being and can lead to residents’ feelings of distress, helplessness, and dissatisfaction as well as family members’ concerns about further physical decline of the resident (see Box 4-5 for a family member’s note to
the committee on their initial expectations of physiological care in nursing homes). For example, insufficient attention paid to granting residents preferred food choices might lead to undernutrition and weight loss. Similarly, providing residents with insufficient liquids might lead to dehydration, bladder infections, and potential hospitalization (Basinska et al., 2021).
However, it is important to recognize that meeting one physiological need can create tensions with another. For example, helping nursing home residents remain mobile is important, as is keeping them safe from harm. Given that older adults tend to have health problems that affect their balance, increasing mobility can raise the risk of falls. Thus it is imperative that nursing homes ensure smooth and unobstructed walkways and proper lighting and also consider the impact of medications and health conditions that can influence an individual’s balance as discussed further in Chapter 6 (Alzheimer’s Association, 2009; Pioneer Network, 2016).
CMS regulations require nursing homes to monitor processes and outcomes of care.25 The quality of nursing home care is a central focus of the survey process and of public reporting. Quality measurement and quality assurance programs in nursing homes are discussed in greater detail in Chapters 3 and 8 of this report. Despite regulatory oversight, significant gaps remain in the quality of physiological care delivered in the nursing home setting (see Box 4-6). Such shortcomings in care delivery exist due to a variety of factors, including inadequately prepared staff (Stone and Harahan, 2010), hierarchical structures that impede cohesive team building and functioning (Forbes-Thompson et al., 2006), and inadequate staffing and high staff and leadership turnover (Castle and Lin, 2010; Castle et al., 2007; Collier and Harrington, 2008), all of which impair the strong staff–resident relationships that are critical to providing quality care (see Chapter 5 for a complete discussion on workforce issues).
Other factors associated with poorer quality care include care that is not aligned with evidence-based best practices (Ersek and Jablonski, 2014); poor care coordination resulting from inadequate health information technology support (Alexander and Madsen, 2021; Alexander et al., 2020a; Vest et al., 2019) (see Chapter 9 for more detailed discussion of health information technology); infrequent visits and limited involvement of medical directors and primary care providers; regulations that incentivize certain types of care (e.g., rehabilitation) that are not aligned with residents’ goals and preferences (Carpenter, 2020; Flint et al., 2019); and insufficient resources to provide ready access to ancillary services such as laboratory tests and intravenous therapy (Cantor et al., 2020). Moreover, low-quality communication between nursing homes and hospitals such as missing, incomplete,
___________________
25 CMS Requirements for Long-Term Care Facilities—Quality assurance and performance improvement, 42 CFR § 483.75 (2016).
and inaccurate information has been identified as a significant risk factor for negative patient outcomes related to care transitions (Gillespie et al., 2010; King et al., 2013; Scott et al., 2017; Terrell and Miller, 2006).
Behavioral Health Care
Moving beyond the physiological needs discussed in the previous section, the next category in Maslow’s hierarchy is psychological needs. These include needs ranging from companionship and relationships, a sense of inclusion, and support of an individual’s cognitive needs. In terms of the life of a nursing home resident, this also includes dignity, autonomy, the ability to engage in meaningful activities, and attention to behavioral health needs.
Two different but overlapping elements of behavioral health are important to the optimal mental health and well-being of nursing home residents (Keyes, 2002). The first element reflects the objective presence of mental
disorders, which for nursing home residents can be existing diagnoses, undiagnosed conditions, or conditions that emerge during a resident’s stay. The second element reflects the subjective state of social well-being, which for nursing home residents includes the resident’s ability to cope and their level of functioning (Keyes, 2002).
Environment and services each play a key role in achieving optimal mental health since available resources, environmental demands, and supports can all affect mental well-being (Niclasen et al., 2019). Limited research suggests that the regular presence of behavioral health staff (either on staff or contracted) and the use of interdisciplinary teams enable effective behavioral health care by addressing medical, psychosocial, and environmental issues together (Bartels et al., 2002). However, there is limited evidence in this area, and further research is needed to identify effective service arrangements and the best composition of staff to provide adequate behavioral health care in nursing homes.
Behavioral health or mental health services are traditionally provided within the nursing home facility by physicians, nursing staff, social workers, and activities personnel (Jester et al., 2020). Alternatively, nursing homes may arrange for contracted behavioral health specialists to either provide care in the facility or in the community. The latter would involve transporting residents to and from appointments in the community (Bartels et al., 2002). The primary models of contracted mental health services include psychiatrist-centered, nurse-centered, and multidisciplinary team models.
Regulatory Requirements
The Behavioral Health Services section26 of the Code of Federal Regulations stipulates that each nursing home resident receive and be provided behavioral health care and services in order that the resident be able to attain and maintain the highest practicable physical, mental, and psychosocial well-being. As outlined in the regulations, behavioral health care starts with a comprehensive resident assessment, which forms the basis for the development of a treatment plan that addresses identified mental health needs. Nursing home facilities are expected to have sufficient staff to enable the provision of direct services while attending to the optimal well-being of residents. The regulations further stipulate that nursing homes must provide residents with mental and psychosocial disorders with the appropriate care to attain the highest well-being possible, emphasizing that using nonpharmacological interventions is a preferred approach. Treatment is to include rehabilitation services and medically related social services. These services can be
___________________
26 CMS Requirements for Long-Term Care Facilities—Behavioral health services, 42 CFR § 483.40 (2016).
provided through internal sources using nursing home staff and consultants or through qualified, Medicaid- and Medicare-approved external providers.
OBRA 87 enacted requirements for nursing homes to perform preadmission screening and annual resident reviews (PASRRs) in order to both identify and assess persons with mental illness and developmental disabilities, to ensure that mentally ill persons are not inappropriately admitted to nursing homes, and to make sure that the nursing home setting is the best placement option for the resident.27 Through the PASRR process, residents with mental illnesses placed in nursing homes are expected to receive appropriate mental health services for their diagnoses.28 Persons with developmental disabilities are expected to receive appropriate habilitation services to promote optimal functioning.29
OBRA 87 also emphasized the importance of a person-centered care approach to providing behavioral health services to nursing home residents (CMS, 2017). Toward that end, the regulations introduced new F-tags30 that focus on mental health supports and services, specifically in the areas of services that nursing homes made available and offered to the resident, sufficient and competent staff, and behavioral health training for staff. The deficiency categories most closely associated with behavioral health are resident behavior and facility practices, quality of life, and quality of care. In addition, OBRA 87 requires nursing homes to identify the resources needed to care for residents with behavioral health issues, to conduct competency assessments to identify staff ability to provide behavioral health services, and to provide training to increase staff competency.31
___________________
27 Omnibus Budget Reconciliation Act of 1987, Public Law 100-203; 42 USC 1396r, §1919, 100th Cong., 1st Sess., (December 22, 1987).
28 Omnibus Budget Reconciliation Act of 1987, Public Law 100-203; 42 USC 1396r, §1919 – subparagraph B, 100th Cong., 1st Sess., (December 22, 1987).
29 Omnibus Budget Reconciliation Act of 1987, Public Law 100-203; 42 USC 1395i-3, §1919, 100th Cong., 1st Sess., (December 22, 1987).
30 F-tags are cited when there is noncompliance that is not actual harm but results in minimal discomfort to the resident or has the potential to cause harm. These are very common citations in nursing home surveys. See https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/GuidanceforLawsAndRegulations/Downloads/List-of-Revised-FTags.pdf (accessed October 21, 2021).
31 The Social Security Act prohibits federal Medicaid payments to institutions for mental diseases (IMD), defined as “hospital, nursing facility, or other institution of more than 16 beds that is primarily engaged in providing diagnosis, treatment, or care of persons with mental diseases, including medical attention, nursing care, and related services” (MACPAC, 2019, p. xii). Because of the broad definition, it is difficult to determine which facility in a state qualifies as an IMD, leading to great variation and resource allocation by state (MACPAC, 2019, 2020, 2022). This lack of definitional specificity may also serve as a significant barrier to nursing home residents obtaining necessary behavioral health services.
Current State of Behavioral Health Services in Nursing Homes
The widespread closing and downsizing of inpatient psychiatric hospitals, which began in the 1950s and continued for decades in various phases (Koyanagi, 2007; Pan, 2013), combined with inadequate community resources for mental health services, resulted in nursing homes becoming a main setting to care for persons with persistent serious mental illness (SMI). CMS uses a broad definition of SMI to include a diagnosis of schizophrenia, schizoaffective disorder, schizophrenium disorder, delusional disorder, psychotic mood disorders, and anxiety disorders but not a primary diagnosis of depression or Alzheimer’s disease and related dementias (ADRD).32
Approximately 4 out of 10 long-stay nursing home residents that are Medicaid beneficiaries under the age of 65 have an SMI diagnosis; for those 65 or older, the prevalence is 2 out of 10 (Nelson and Bowblis, 2017). The share of residents diagnosed with schizophrenia or bipolar disorder nearly doubled, from 6.5 percent in 2000 to 12.4 percent in 2017 (Laws et al., 2021). The prevalence of schizophrenia in people aged 65 and over in the general population is 0.1 to 0.5 percent (Rosenberg et al., 2009). Concerns have been raised about nursing home residents with dementia being diagnosed inappropriately with schizophrenia (discussed below and in Chapter 6).
Studies estimate that a disproportionately large share (60 to 90 percent) of nursing home residents have any mental health diagnosis (Brennan and Soohoo, 2019; Burns and Taube, Fullerton et al., 2009; Grabowski et al., 2009, 2010; Orth et al., 2019; Rahman et al., 2013; Smyer et al., 1994; Tariot et al., 1993). Trend analyses indicate that the proportion of residents admitted with mental illness is higher than the proportion with dementia (Aschbrenner et al., 2010; Fullerton et al., 2009; Grabowski et al., 2010). Among individuals with mental illness, individuals diagnosed with schizophrenia or bipolar disorder are more likely to be admitted to a nursing home during the 3-year period following their diagnosis, and older persons with depression are also at an increased risk of being placed in a nursing home (Fullerton et al., 2009). These individuals have a range of complex care needs that present significant challenges for nursing homes (Laws et al., 2021).
Much of the data related to behavioral health conditions of nursing home residents date back more than a decade. More up-to-date prevalence data would likely be higher, reflecting an increase in resident acuity and the proportion of nursing home admissions of residents with mental health conditions (Temkin-Greener et al., 2018a).
___________________
32 See https://www.govinfo.gov/content/pkg/CFR-2009-title42-vol5/pdf/CFR-2009-title42vol5-sec483-100.pdf (accessed February 14, 2022).
Current Challenges
Nursing home use of PASRRs, which was designed to improve access to behavioral health care, has had mixed results, with some conditions, such as schizophrenia, identified more successfully than other conditions, such as depression (Crick et al., 2020). The number of residents with mental health needs in nursing homes is increasing (Temkin-Greener et al., 2018a), and many residents are not having their needs met (Rivera et al., 2020). These unmet needs33 occur more acutely in certain subpopulations of nursing home residents. For example, nursing homes often overlook the mental health needs of racial and ethnic minorities, who are less likely to receive treatment after an SMI diagnosis (Bailey et al., 2009). Research points to a lack of culturally sensitive assessments and treatment practices as factors contributing to the disparities in care and unmet needs minority populations in nursing homes experience (Fashaw-Walters et al., 2021; Li et al., 2019).
Historically, nursing home care and staffing have primarily focused on the physical health care needs of residents, managing their chronic conditions and maintaining their functional ability. While OBRA 87 was enacted to provide protections for nursing home residents with mental illnesses and developmental disabilities, the treatment of psychiatric conditions and behavioral health conditions in nursing home settings still requires significant improvement (Li, 2010). One of the many aims of the nursing home reforms contained in OBRA 87 was to decrease inappropriate use of medications. In some cases, however, medication use has increased, with little effort made to provide nonpharmacologic approaches to care (Crick et al., 2020). Research has identified numerous barriers to providing nonpharmacologic approaches, including insufficient reimbursement to support care from specialized mental health care teams, inadequate staffing levels and staff training, time pressures, and lack of leadership, among other factors (Crick et al., 2020).
Current funding structures serve as barriers to mental health assessment follow-ups and nonpharmacologic approaches to care (Crick et al., 2020), as these approaches can be resource intensive. Providing high-quality care to residents with SMI requires more direct-care hours, specialized staff training, and services from mental health providers external to nursing home facilities (McGarry et al., 2019), but public payments for residents with SMI do not adequately cover the costs of treating those residents (Rahman et al., 2013). Nursing homes report difficulties in accessing mental health specialists willing to provide services in the nursing home, while
___________________
33 Unmet needs are defined here as neglect of care necessary for ADLs. Negative consequences of unmet needs include the resident missing meals, not having appropriate toileting care which results in wetting or soiling clothes, medication error, or not receiving needed assistance in order to walk around (Rivera et al., 2020; Xiang et al., 2017).
the costs to transport residents to external treatment sources may exceed Medicaid coverage in some states (Crick et al., 2020).
Attempts to improve the quality of behavioral health care through regulations have, in many cases, proved to be unsuccessful (Crick et al., 2020), and lower reimbursement rates for SMI care do not encourage quality care (Rahman et al., 2013). In fact, facilities with higher populations of residents requiring SMI care are associated with lower nursing home quality (Rahman et al., 2013) and lower care quality (McGarry et al., 2019). For example, one study of over 14,000 nursing home facilities found that those with greater proportions of residents with SMI also had lower direct-care staffing hours, more residents who were Medicaid beneficiaries, and lower scores on Nursing Home Compare star ratings (Jester et al., 2020) and were more likely to be for-profit facilities.
Eligibility for Medicaid coverage is based on income status as well as disability (including psychiatric disability). There is an increased prevalence of mental illness in high-Medicaid facilities. Moreover, nursing homes with a majority of Medicaid residents are associated with higher rates of psychiatric hospitalization (Becker et al., 2009) and greater rates of antipsychotic medication prescription (Hughes et al., 2000).
Research on access to behavioral health services suggests that there are disparities in access to high-quality nursing homes (Temkin-Greener et al., 2018a). These disparities may be a result of social stigma, nursing home reluctance to accept patients who require medications (which may lower facility quality scores), nursing homes’ concerns about their ability to deal with behavioral problems, and the geographical distribution of five-star nursing homes. Research indicates that inadequate access to behavioral health services occurs in both lower and higher star-rated facilities and in both for-profit and nonprofit nursing homes. Moreover, access to such services is not necessarily affected by for-profit status (Orth et al., 2019). Nursing homes located in urban areas, facilities with higher RN staffing and lower turnover, and facilities with more psychiatrically trained physicians were less likely to report inadequate infrastructure to connect residents to behavioral health services (Orth et al., 2019).
A survey of nursing homes identified a number of key challenges to delivering behavioral health care services, including
- lack of staff training (47 percent),
- inability to adequately meet resident’s behavioral health needs (33.3 percent),
- inadequate coordination between the facility and community providers (31.8 percent), and
- lack of adequate infrastructure to make referrals and transport residents to services outside the facility (26.2 percent) (Orth et al., 2019).
Of those facilities surveyed, 40 percent viewed PASRRs as hindering admission screening and causing admission delays, and more than 60 percent expressed concerns about the perceived difficulty in accessing psychiatric support after nursing home admission (Orth et al., 2019).
Several studies have identified the challenges of training staff in behavioral health and providing quality care as key challenges for nursing homes (Orth et al., 2019; Roberts et al., 2020). Staff behavioral health education was less problematic in facilities that had dedicated Alzheimer’s units, lower turnover of registered nurses, and more psychiatrically trained registered nurses and social workers. Facilities with lower registered nurse turnover and more psychiatrically trained registered nurses were less likely to report inadequate coordination with community providers and being unable to meet resident needs (Orth et al., 2019). Facilities with lower registered nurse turnover, higher registered nurse staffing, and more psychiatrically trained physicians were less likely to report inadequate facility infrastructure (Orth et al., 2019). In a secondary analysis of national data, facilities with social service departments staffed by individuals with higher professional qualifications were associated with improved care through reducing residents’ behavioral health symptoms and avoiding the use of antipsychotics (Roberts et al., 2020).
Promising Practices/Innovative Models to Address Behavioral Health Needs
A number of interventions have been found to be effective in treating behavioral health conditions such as depression in the nursing home environment. One systematic review identified cognitive behavioral therapies, reminiscence activities, interventions aimed at reducing social isolation, and exercise-based interventions as having some impact on decreasing depression in cognitively intact nursing home residents (Simning and Simons, 2017). Another study found decreases in depression and increases in quality of life among residents who participated in a 10-week physical activity program (Lok et al., 2017).
Interventions to reduce loneliness linked to depression have also produced positive results in long-term care settings (NASEM, 2020). One systematic review suggests that the interventions that are more successful at reducing loneliness are the ones that do not require high amounts of physical activity and mobility (Quan et al., 2020). Those interventions for which the strongest results have been reported include reminiscence therapy, laughter, and horticultural therapy34 (Quan et al., 2020).
___________________
34 Horticultural therapy refers to the use of flowers, plants, and horticultural activities for treatment. Such therapy has been shown to help individuals learn new skills, adjust to functional loss, and experience hopeful and nurturing feelings, with positive impacts on physical, psychosocial, and cognitive functions such as improving body coordination, encouraging social activity, and improving mood (Chen and Ji, 2015).
Videoconferencing interventions, PARO robot35 interaction, logotherapy,36 and pet therapy produced more modest results (Quan et al., 2020).
Other studies have reported success at improving the cognitive functioning of nursing home residents. A systematic review of multimodal, nonpharmacologic interventions for cognitive function in older people with dementia concluded that sessions combining exercise, cognitive training, ADL practice, and activity interventions improved global function, executive function, and memory in persons with dementia when the sessions were at least 30 minutes long and done at least three times a week for at least 8 weeks (Yorozuya et al., 2019). One randomized controlled trial using animal-assisted activities reduced depressive symptomatology and increased the quality of life for persons with cognitive impairment (Olsen et al., 2016).
Research on well-being provides some guidance for developing optimal environments for supporting mental health care. For example, one systematic review of the well-being of long-term care residents with chronic mental illness provided broad recommendations for care, including the development of environments that provide nonstigmatizing specialized care that is accepting and supportive (van der Wolf et al., 2019). Given the lack of evidence of effective treatment approaches, the authors concluded that additional research should be conducted in this area, with attention paid to the well-being of residents.
Use of telehealth for behavioral health care
As discussed elsewhere in this report, the COVID-19 pandemic had a particularly deleterious impact in the nursing home setting. This was true not only in terms of morbidity and mortality, but also in terms of residents’ mental and behavioral health. In an effort to protect nursing home residents and staff from contracting the coronavirus, nursing homes quickly restricted access to their facilities and curtailed resident activities. While these measures were put in place to provide for the health and safety of residents and staff, the unintended consequence was a significant increase in social isolation and loneliness, depression, and anxiety among residents (also discussed in Chapter 9 of this report) (Mo and Shi, 2020; Rodney et al., 2021). Typically, all residents facing behavioral health challenges rely on visits with family members and personal contact and interaction with other residents and members of the community for various reasons including socialization,
___________________
35 A PARO robot is a baby harp seal robot used in nursing homes, which has a calming effect on and elicits emotional responses in patients.
36 Logotherapy, from the Greek word logos, or “meaning,” is a form of therapy oriented around helping individuals find meaning in their future.
support, and personal care (Gaugler, 2005). The absence of such coping mechanisms increased the complexity of residents’ behavioral health challenges (Nash et al., 2021). Given nursing homes’ extremely limited resources such as psychologists that specialize in geriatric populations, behavioral telehealth offers one way to expand access to such necessary, but limited, expertise (Friedrich, 2021). The use of health information technology (HIT) including telehealth in nursing homes is discussed further in Chapter 9.
Remote monitoring and robotics
Remote monitoring technology is another innovation that has the potential to improve care delivery and outcomes for nursing home residents. This technology includes devices that can connect remotely to the Internet, which, in the case of mobile devices, makes it possible for the devices to move around independently and collect data about residents. For example, robots can move independently and transmit real-time images to nursing home staff and also open a voice connection between the resident and the remote caregivers to improve communication (Bäck et al., 2012).
In one study, researchers examined the use of assistive robots for the care of nursing home residents with dementia experiencing depression and agitation. In particular, the intervention included a robot device described as being the size of a baby harp seal with a swiveling head, moving legs and tail, and microphones that make authentic sounds like a harp seal; the robot intervention resulted in improved depression and less agitation over time (Jøranson et al., 2015).
It is critical to understand that however useful these and other future innovations might be, the developers and implementers of remote monitoring tools need to always consider the impact of these innovations on resident satisfaction as well as on clinician workflow, burden, and satisfaction (Alexander et al., 2020b).
Research indicates that residents with behavioral health disorders (e.g., schizophrenia, psychosis, bipolar, depression/anxiety, personality disorder, and substance use) are less likely to be admitted to high-quality nursing home facilities than residents without those disorders (Temkin-Greener et al., 2018a). Lower-quality facilities typically have fewer resources available to staff and residents, such as HIT, to help support care delivery during times when in-person access is extremely limited, such as during the pandemic (Alexander et al., 2017). The use of HIT, such as certified electronic health record technology, has been shown to improve communication and clinical integration among behavioral health and all other providers (MACPAC, 2021). The myriad issues related to HIT adoption, implementation, and use in nursing home settings are discussed in Chapter 9.
Care for People with Alzheimer’s Disease and Related Dementias
An estimated 48 percent of nursing home residents—59 percent of long-stay and 37 percent of short-stay (post-acute) residents—have a diagnosis of dementia (Harris-Kojetin et al., 2019). These figures for dementia diagnosis are likely underestimates, as studies have demonstrated that when specialists such as neurologists, psychiatrists, and neuropsychologists conduct assessments in long-term care settings, they identify many undiagnosed cases of dementia (Magaziner et al., 2000; Zimmerman et al., 2007).
Alzheimer’s disease, the most common dementia, begins subtly, passes through mild cognitive impairment, and progresses to mild, moderate, and finally severe dementia, with the course generally lasting a decade or more. Often, the later stages of the disease, which require 24-hour supervision and assistance with most or all ADLs, result in nursing home placement. A variety of other progressive dementias exist, such as frontotemporal dementia, Lewy body dementia, vascular dementia, and dementia associated with Parkinson’s disease. These conditions vary in their presentation, rate of progression, and care needs but share many of Alzheimer’s disease’s effects on cognitive function (Alzheimer’s Association, 2021a,b).
Available research indicates that the key element of dementia care practice should be a focus on the individual’s condition, needs, and desires. That focus should be based on knowing the person; recognizing and accepting the person’s reality; identifying and supporting opportunities for meaningful engagement; building and nurturing authentic caring relationships; creating and maintaining a supportive community for individuals, family, and staff; and evaluating care practices regularly, using evaluation data to guide appropriate changes in care and policy (Fazio et al., 2018).
Most of the principles of quality care for nursing home residents apply equally to persons with cognitive impairment and to those without. However, providing care for persons with cognitive impairment, including persons with ADRD, raises a number of specific issues. For example, managing Alzheimer’s disease and related cognitive disorders largely involves addressing behavioral symptoms such as wandering, resistance to care, repetitive mannerisms, repetitive vocalization, and aggression. Studies show that these behavioral symptoms are often expressions of unmet needs, such as loneliness, boredom, discomfort, anxiety, or pain (Cohen-Mansfield et al., 2015). In this context, a key goal of care should be to identify and meet these needs using individualized approaches and, as first-line methods, nonpharmacological tools and methods (Gaugler et al., 2014). A study found that a diagnosis of cognitive dysfunction upon admission to a nursing home is a stronger predictor of outcome than a diagnosis of dementia. This highlights the need to individualize decisions regarding the risks and benefits of nursing home care for those individuals with cognitive impairment (Burke et al., 2021).
It is also important to recognize that for a person with advanced dementia, the sensory experiences of the present are very important, since awareness of the meaning or future implications of such activities as waiting for a meal, positioning in a bed or chair, or receipt of hygiene care are often not understood. Furthermore, the inexorable progression of virtually all ADRD diagnoses places more importance on the experiences of today, something that is also true of many other nursing residents. These factors combine to make addressing unmet needs, creating pleasant events, and attending to day-to-day quality of life critical outcomes of interest in the care of persons with ADRD (Gaugler et al., 2014; Kitwood, 1997; Logsdon et al., 2002). It is important to note that measuring day-to-day quality of life is challenging and that this key outcome is vastly underrepresented in CMS “quality indicators,” which focus largely on medical outcomes (Burke and Werner, 2019).
In addition, persons with dementia underreport new symptoms or needs and therefore tend to receive less attention, have more undetected symptoms (e.g., constipation), and receive fewer treatments (e.g., medication for pain) than other residents. Decision making is also difficult, which creates challenges for the current model of shared decision making, particularly if family members are relatively uninvolved or are unaware of the relevant values and preferences of the person with dementia (Miller et al., 2016b). As ADRD progresses, cognitive impairment advances, limiting the person’s ability to participate in decision making. Consequently, formal procedures to facilitate early discussion with family and health care professionals about care goals and advance care planning (see Box 4-8 below) are important, as studies have demonstrated that such planning improves end-of-life outcomes (Wendrich-van Dael et al., 2020).
Antipsychotic medications have been used to treat nursing home residents with behavioral and psychological symptoms of dementia, but FDA warnings about the danger of such medications for people with dementia have led to increased efforts to limit their use (also discussed in Chapter 6). CMS launched the National Partnership to Improve Dementia Care in 201237 to reduce potentially inappropriate use of antipsychotics by reorienting nursing homes toward nonpharmacologic person-centered care, including music and exercise programs (Lucas and Bowblis, 2017). Through the initiative, CMS, in partnership with federal and state agencies, nursing homes, advocacy groups and caregivers, working in concert with state-based coalitions, aims to advance best practices to promote person-centered care and improve the quality of life for residents with dementia (Fashaw-Walters et al., 2021; Lucas and Bowblis, 2017).
___________________
37 See https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/SurveyCertificationGenInfo/National-Partnership-to-Improve-Dementia-Care-in-Nursing-Homes (accessed February 9, 2022).
Although the rates of antipsychotic medication use for dementia care in nursing homes declined overall between 2012 and 2019, significant variation exists across states (Rosenthal et al., 2022). Recent research has revealed unintended consequences of the National Partnership’s efforts. For example, an initial examination has shown that rates of schizophrenia, as documented in residents’ MDS assessments, increased after implementation of the Partnership and are higher for Black residents with ADRD than non-Black residents. Such disparities in diagnoses raise concerns that nursing homes are reporting schizophrenia diagnoses in an effort to bypass the Partnership’s goal of reducing antipsychotic medication use. Disparities in schizophrenia diagnoses could be due to a number of factors, including differences in quality of care for Black residents compared to non-Black residents, perceptions of nursing home staff regarding the management of challenging behaviors, or structural racism (Fashaw-Walters et al., 2021).
The U.S. Alzheimer’s Association published a comprehensive set of dementia care practice recommendations and a series of supporting papers (Fazio et al., 2018), which can help inform a greater focus on dementia care in nursing home practice, training, and regulation (Alzheimer’s Association, 2018).38 Additional research has identified shortcomings in the current evidence base on initiatives designed to improve care for people with ADRD in nursing homes, including an overrepresentation of short-term studies with small sample sizes, making it challenging to determine which interventions are effective. Further research is needed on interventions at the community level (care protocols, dementia villages), policy level (paid family leave policies, payment policies, and transportation policies), and societal level (public awareness campaigns). A balance of short-term and long-term studies is needed, as well as including assessments of interventions in real-world settings where people receive care, including the home and long-term care facilities (NASEM, 2021).
Psychosocial Care
The committee’s conceptual model of quality care in nursing homes considers meeting residents’ psychological and social needs—situated in the mid-range of Maslow’s hierarchy—as a critical component of comprehensive person-centered care. The psychosocial needs of older adults incorporate physical, psychological, intellectual, and social dimensions of care. Nursing homes organize these care services to enhance their residents’ mental, social, and emotional well-being; improve outcomes related to their quality of life and quality of care and to resident rights; and support the
___________________
38 For the full recommendations, see https://www.alz.org/media/documents/alzheimers-dementia-care-practice-recommendations.pdf (accessed October 21, 2021).
residents’ family members and other loved ones. Social services, activities, and nursing departments within the nursing home typically deliver these services, which are augmented by consultants and contractual services that require specialized training or expertise, such as psychiatric services and music and art programs. Research has shown that an interdisciplinary team perspective produces better outcomes (Simons et al., 2012a,b), as the team is trained to address psychological, social, and environmental factors that affect care and quality of life (Simons et al., 2012a).
Providing effective individualized care requires a knowledge of residents’ psychosocial preferences (Carpenter et al., 2000). According to one systematic review, nursing home residents identified nine factors important to them that influenced their idea of quality care: staffing levels, staff attitudes, continuity of care, daily routine, environment, decision making/choice, dignity, activities, and attention to culture and spirituality (Gilbert et al., 2021; see also Travers et al., 2021). Research on older adults living in the community has identified preferences for care, trade-offs between freedom and safety, family/friend involvement, privacy issues, avoiding pain, participation in events, and daily routine as areas in which preferences correlate with a better quality of life (Degenholtz et al., 1997). Other studies emphasize preferences in the areas of social contact, growth and leisure activities, personal choice/control, the use of assistive devices, and care and caregivers as being important to an enhanced quality of life (Carpenter et al., 2000). Honoring the choices of nursing home residents is associated with an improved quality of life. Processes such as the initial and ongoing assessment of psychosocial preferences of residents as well as the documentation and communication of these preferences with the interdisciplinary team are central to meeting the needs of residents for optimal delivery of person-centered care.
Regulatory Requirements
The Code of Federal Regulations section on behavioral health services39 mandates that a nursing home provide psychosocial care as detailed in its comprehensive assessment and plan of care. Including the resident, significant others, and members of the interdisciplinary team responsible for psychosocial care is key to developing and reviewing the assessment and plan-of-care document. The regulations also outline a process through which the care plan should address psychosocial care needs and specify that nursing homes must employ qualified staff to provide the services that meet these needs.
As discussed earlier, regulations require Medicare- and Medicaid-certified nursing homes to conduct patient care surveys as part of the
___________________
39 CMS Requirements for Long-Term Care Facilities—Behavioral health services, 42 CFR § 483.40 (2016).
certification process.40 Two areas of assessment pertinent to psychosocial needs are (1) activities and social participation and (2) medical, nursing, and rehabilitative care. A nursing home that fails to meet one or more federal requirements is cited for a deficiency by surveyors. The deficiency categories most closely associated with psychosocial care needs include resident rights; admission, transfer, and discharge rights; resident behavior and facility practices; and quality of life and quality of care.
Although psychosocial care needs are part of the federal requirements, the regulations place a greater emphasis on medical indicators of high-quality care. While physical health indicators are clearly an important area of focus for quality improvement, psychosocial indicators such as enhancing social engagement, supporting self-worth and resident dignity, and addressing the psychological and spiritual needs of the residents are important elements of nursing home care and should be an integral component of the survey process and quality improvement initiatives (Bowen and Zimmerman, 2009).
Current Status
A growing body of evidence suggests that it is important to provide a variety of services and activities to address the psychosocial care needs of nursing home residents, including attending to spiritual needs, counseling, and other psychosocial support services (Johnston and Narayanasamy, 2016; Koenig, 2012; Lok et al., 2017; Olsen et al., 2016; Zhang et al., 2020). However, despite the importance of these services to person-centered care and resident quality of life, the current emphasis on nursing home care in the United States aligns with a medical model of care, with a limited focus on social care.
Research supports the role of a stronger emphasis on psychosocial care in order to ensure a more person-centered approach to nursing home care. As noted above, nursing home residents cite factors related to dignity, activities, and attention to culture and spirituality as being critical to quality care (Gilbert et al., 2021). An emphasis on improving the performance and outcomes of these factors may strengthen the responsiveness of nursing homes to resident concerns.
Wellness, physical activities, and art activities are vital for health, functional mobility, and performing ADLs. Research suggests that physical activity can protect against and lessen ADL disability, improve cognition and quality of life for residents and those with dementia, and improve mental health (de Souto Barreto et al., 2016). One intervention, Function-Focused Care, engages residents with moderate to severe cognitive impairment in physical activities and functional tasks using motivational and individualized techniques. It has the potential to improve older adults’ psychosocial
___________________
40 CMS Requirements for Long-Term Care Facilities—Survey frequency, 42 CFR §488.308 (a) and (b) (2016).
and physical well-being, increase physical activity, and reduce risk of hospitalization and falls (Galik et al., 2013, 2015; Resnick et al., 2016).
There is also evidence that wellness interventions such as tai chi and yoga in nursing homes can improve the quality of life among residents (Saravanakumar et al., 2018), and some evidence suggests that ADL training combined with physical exercise can improve well-being in nursing home residents with moderately severe dementia (Henskens et al., 2018). Studies have also shown that art interventions in nursing homes can improve the quality of life for dementia patients (Schneider, 2018), promote person-centered care among nursing home residents (Vaartio-Rajalin et al., 2021), reduce depression and improve the self-esteem of residents (Ching-Teng et al., 2019), and promote overall resident well-being (Curtis et al., 2018).
Research has identified a number of other areas that require improvement, including an emphasis on stronger staffing requirements to deliver psychosocial care (Bern-Klug et al., 2010; Simons et al., 2012a,b), acquiring outcome data that link care provision with improved quality of care (Bowen and Zimmerman, 2008), and better definition of the processes of psychosocial care in nursing homes (Simons et al., 2012b). Factors associated with the quality of psychosocial care include staffing and payer source; in particular, it has been shown that increases in qualified social service staffing produce higher-quality psychosocial care (Zhang et al., 2008; Zimmerman et al., 2005).
Current Challenges
The Agency for Healthcare Research and Quality conducted an environmental scan of nursing homes and found evidence of omissions in psychosocial care which led to severe adverse events such as avoidable hospitalizations, cognitive decline, death (all-cause and suicide), loneliness, and poor resident-centered care (Ogletree et al., 2020). In addition, several studies have documented omissions in psychosocial care, particularly in the areas of addressing emotional and mental health needs, listening to the resident, and honoring care preferences (Hirst, 2002; Poghosyan et al., 2017; Recio-Saucedo et al., 2018). Other studies have reported serious omissions in psychosocial care leading to loss of dignity, abuse, and neglect of the resident (Hirst, 2002; Malmedal et al., 2009; Nåden et al., 2013). One study reported that nursing home staff limit social care more than ADL care (Zúñiga et al., 2016). An earlier report by the HHS OIG on psychosocial services provided to nursing home residents found that only slightly more than half of Medicare beneficiaries received all the psychosocial services identified in their care plans during their nursing home stay, while 41 percent received some, but not all of the psychosocial services identified in their care plans. Five percent of beneficiaries did not receive any of the psychosocial services identified in their care plans (OIG, 2003).
Promising Practices
While psychosocial care in nursing homes has improved over the years (IOM, 2001), it is still evolving. Notable changes and new models of care strongly support implementing a person-centered care approach. For example, the meaningful activity movement requires nursing homes to employ the elements of active participation, activity content related to past roles and interests of the participants, and activities that meet the needs of identity and belonging for all activity offerings (Genoe and Dupuis, 2012). Promising programs such as MemPics, designed to promote meaningful activity for people with mild to moderate dementia using cognitive stimulation (Mansbach et al., 2017), have been tested in the nursing home setting with positive results. The Preference Match Tracker is a tool to identify activity preferences which can be used to document and track individual recreation preferences and activities. Such preferences can be incorporated in the assessment and care planning process to improve the quality of care and quality of life for residents (Van Haitsma et al., 2016).
Videoconferencing for remote health care provision, counseling, and the delivery of specialized activities such as music therapy (Groom et al., 2021; Newbould et al., 2017) and for counseling family and significant others (Gaugler et al., 2020) is proving to be a promising approach for improving psychosocial care. Several studies have established the feasibility of using such methods for assessment, health care management, clinical support, and diagnosis (Alexander et al., 2020a; Groom et al., 2021; Hale et al., 2018; LeadingAge CAST, 2013). Delivering care through videoconferencing may increase access to specialized services and increase access to care for those living in rural areas. Both staff members and residents report satisfaction with providing services though videoconferencing.
Using care preference tools, such as The Conversation Project, in nursing home settings is one approach to honoring resident choices in care (Galambos et al., 2021). New methods for care planning, such as the adoption of a person-directed care planning process (Lepore et al., 2018), can provide a structure for honoring resident choices. When nursing homes use these tools along with other preference assessment instruments, broadly and consistently, they will strengthen a person-centered approach to providing care for their residents.
Another way for nursing homes to improve the psychosocial well-being of their residents and staff is through the establishment of resident and family councils. Every nursing home resident has the right to form or participate in a resident and family council, and the nursing home must provide space for the group to meet and must listen to the complaints and recommendations provided by the council.41 These councils are described in Box 4-7.
___________________
41 For more information from CMS, see https://downloads.cms.gov/medicare/your_resident_rights_and_protections_section.pdf (accessed November 16, 2021).
Palliative Care and End-of-Life Care
Palliative care focuses on persons with serious, life-limiting illnesses and is characterized by openly discussing illness trajectories and identifying, documenting, and honoring patient- and family-directed goals that guide health care; aggressively preventing, promptly identifying, and effectively treating illness-related symptoms; and identifying psycho-spiritual needs and therapeutic approaches to mitigate suffering (National Consensus Project for Quality Palliative Care, 2018). Palliative care is appropriate for patients throughout the illness trajectory, including, but not solely, at the end of life, and individuals can receive palliative care alongside disease-focused treatments. Despite the need for palliative care services, access to this type of care often is limited in the nursing home setting.
Hospice care is palliative by nature, but it focuses specifically on individuals with terminal illness—usually those with the prognosis of 6 months or less. For these individuals, the goals of care focus on comfort (NHPCO, 2019).
Palliative and end-of-life care are critical components of high-quality nursing home care (Ersek et al., 2014), given that the majority of nursing home residents have multiple chronic illnesses which result in distressing symptoms and marked impairments in ADLs (Boscart et al., 2020; CMS, 2015). Indeed, older adults receiving end-of-life care in nursing homes have high symptom burdens and other needs that make them eligible for palliative care or hospice services (Esteban-Burgos et al., 2021; Stephens et al., 2018). Most hospice care in the United States is funded by Medicare under a specific benefit (NHPCO, 2020).
Nursing homes are the venue of death for approximately 25 percent of Medicare beneficiaries and an estimated 43.5 percent of fee-for-service beneficiaries. In addition, 33.2 percent of Medicare Advantage enrollees had a nursing home stay in the last 90 days of life (Teno et al., 2018). The share of Medicare beneficiaries who die in hospice care increased from 22 percent in 2000 to more than 50 percent in 2019 (MedPAC, 2021; Sheingold et al., 2015). Medicare’s hospice benefit paid for services provided to more than 1.6 million beneficiaries in 2019 (MedPAC, 2021).
Nursing homes rely on one of three common models for delivering palliative care in their facilities: hospice, external palliative care consultation, or internal, facility-based services (Ersek et al., 2014).
Hospice care
Hospice is the most common and well-established approach for delivering palliative care in U.S. nursing homes. CMS extended the Medicare hospice benefit to nursing homes in 1989, and by 2004, 78 percent of nursing homes reported a contract with a hospice agency (Miller and Han, 2008). Approximately one-quarter of deaths among Medicare beneficiaries occurs in a nursing home (Teno et al., 2018).
In order to be eligible, nursing home residents must meet standard hospice admission criteria, including a period of life expectancy of 6 months or less should the terminal illness run its usual course accompanied by a decision that aggressive “curative” treatments would not be pursued (CMS, 2020c). In nursing homes, the Medicare hospice benefit covers the costs of the hospice agency to oversee the individual’s care plan, as well as the costs of all medical supplies and medications related to the individual’s terminal condition. The benefit also covers supplemental support, as needed, from hospice interdisciplinary team members, including chaplains, social workers, and home health aides, as well as bereavement services for up to 1 year following the patient’s death. While providing hospice care, the facility continues to deliver 24-hour nursing care and supportive services for the resident. The Medicare hospice benefit does not provide the resident’s payment for room and board, leaving other sources such as Medicaid or out-of-pocket payments to cover those expenses (CMS, 2020a).
Research comparing end-of-life care for residents with and without hospice has shown that hospice care is associated with better psychosocial support, bereavement care, and pain management (Miller et al., 2002; Stevenson and Bramson, 2009). Hospice enrollment is also associated with fewer hospitalizations and lower health care costs for nursing home residents at the end of life (Gozalo and Miller, 2007; Miller et al., 2012; Stevenson and Bramson, 2009).
Despite the strengths of the hospice model, it has its limitations. For example, many nursing home residents have a life-limiting illness with an uncertain trajectory, which can make it difficult to determine hospice eligibility. Some nursing home administrators believe that hospice involvement does not improve end-of-life care for residents and may complicate the coordination of care (Hanson et al., 2005; Rice et al., 2004). In that vein, successful collaboration between hospice agencies and nursing homes requires a commitment to ensuring excellent communication, including soliciting input from and sharing information with nursing home staff and responding to concerns voiced by nursing home staff and administrators (Ersek et al., 2022; Miller, 2010).
Perverse financial incentives are a major barrier to nursing home hospice enrollment, at least among individuals entering the facility from the hospital and who are eligible for the Medicare skilled nursing facility benefit. Only in rare instances can patients access the Medicare skilled nursing facility and Medicare hospice benefit concurrently (e.g., in circumstances where there are unrelated diagnoses for each benefit). Reimbursement to nursing homes for the Medicare hospice benefit is much lower than for the skilled nursing facility benefit, meaning that facilities prioritize skilled nursing facility care over hospice stays, even when individuals’ care needs are more palliative than
rehabilitative (Hanson and Ersek, 2010). Similarly, these same financial incentives lead families to choose the skilled nursing facility benefit because the skilled nursing facility payment covers all costs in the facility including room and board, unlike the Medicare hospice benefit (Flint et al., 2019). Hospice interdisciplinary team members can supplement the nursing home workforce, which can improve care (Gage et al., 2016; Hwang et al., 2014). Issues related to the inappropriate use of hospice and poor-quality care, particularly for nursing home residents, have increased over the past decade (Chiedi, 2018; MedPAC, 2020; OIG, 2018). Policy makers have paid particular attention to the increase in hospice use in nursing homes, expressing concern that for-profit hospice agencies were aggressively targeting more profitable, long-stay patients (Chiedi, 2018). An investigation by HHS OIG found that hospices do not always provide the services that residents need, such as for pain management, and that in many cases poor-quality care was provided. OIG also cited communication and information gaps that prevented residents and their families and caregivers from making informed decisions about their care. Furthermore, the investigation identified cases of inappropriate billing for higher levels of care than needed and a number of fraud schemes. The current payment system for hospice care creates incentives for hospices to seek out beneficiaries who do not have complex care needs. Hospice is paid on a per diem basis for each day an individual is in hospice, regardless of the quantity or quality of services provided (Chiedi, 2018).
Another trend that raises questions is the growing proportion of nursing homes and hospice agencies that are owned by the same company, coupled with the increasing proportion of nursing home residents receiving hospice services from these providers (Canavan et al., 2013; Stevenson et al., 2020). Co-ownership represents a potential conflict of interest in that residents may be referred to hospice inappropriately to bolster revenue for the hospice agency that is co-owned by the nursing home (usually a for-profit corporation). In addition, co-ownership may limit consumer choice if the nursing home or hospice does not inform residents and family decision makers that they can choose which hospice they want to receive care from. There may also be pressure from the corporate entity for nursing homes to limit contracts with outside hospice agencies (Ersek et al., 2022; Stevenson and Bramson, 2009; Stevenson et al., 2020).
Palliative care consultants
In the second model of end-of-life care, nursing homes contract with external palliative care consultation teams to provide specialized, onsite palliative care services. Consultation teams can be an extension of existing hospital-based teams, outpatient or hospice teams, or independent practitioners. Depending on the team and its resources, consultations focus on symptom management, advance care planning (Box 4-8), or assisting with prognostication or hospice entry. Staff or leadership identify
the need for a consultation, which the resident’s primary care provider then requests. The consultant bills under Medicare Part B, and thus the nursing home does not incur any costs for these services.
A nationally representative study found that 34 percent of nursing homes reported having an arrangement with external specialty palliative care consultants (Schwartz et al., 2019). Nursing homes that had these arrangements were 40 percent more likely to perform above the median on an end-of-life culture change index compared with those without any external or internal palliative care services. Other studies have found that external palliative care consultation is associated with better end-of-life outcomes, such as fewer emergency department visits and hospitalizations in the last months of life and lower likelihood of late admission to hospice (i.e., less than 3 days before death) (Miller et al., 2016a, 2017).
One challenge with this model is the need for consulting practitioners to understand the nursing home environment and to recognize that certain interventions used in other settings may not be used in nursing home settings. Certain palliative care medications, for instance, are not included in nursing home formularies. Moreover, there may be significant limitations in nursing home settings in terms of the ability to administer and titrate pain medication such as intravenous opioids. Another challenge is that implementing consultants’ recommendations depends on the primary care provider’s and nursing home staff’s willingness to accept and implement palliative care recommendations (CAPC, 2008). More broadly, some have pointed to the relatively low reimbursement of these Part B services as a major barrier to their broader use (IOM, 2015).
Facility-based palliative care programs
The third model for palliative care delivery in nursing homes is through facility-based programs (Ersek and Wilson, 2003). This model, sometimes referred to as primary palliative care, is promising in that it does not solely rely on access to specialists, it eliminates the challenges of joint management among multiple organizations, and it provides flexibility in how individual facilities implement such teams (Carlson et al., 2011). Furthermore, this model places the expertise and authority with the nursing home itself, which is responsible and held accountable for residents’ quality of care (Huskamp et al., 2010a). In a 2004 survey, 27 percent of nursing homes reported having a special program or specially trained staff for hospice or palliative/end-of-life care (Miller and Han, 2008). In a 2016 survey, some 40 percent of nursing homes’ directors of nursing reported having a palliative care program; however, the study sample was small and not representative of all U.S. nursing homes (Lester et al., 2016).
Although growing numbers of facilities indicate that they have implemented internal palliative care services, the composition, scope, and
activities of these programs are not well characterized. Generally, they encompass one or more of the following features:
- Implementing specific policies related to palliative care (e.g., the identification of residents who might benefit from this approach);
- Regular, robust advance care planning;
- Standardized symptom assessment and management;
- Training the staff to increase their palliative care knowledge and skills; or
- Creating interdisciplinary palliative care teams and establishing specialty palliative care units (Carpenter et al., 2020; Ersek et al., 2014).
However, there is great variability between programs and no assurances that the care provided by a particular nursing home meets commonly accepted palliative care standards. Moreover, there are no nationally recognized and agreed-upon standards and quality measures for nursing home–based palliative care services, although some efforts have been made to identify such guidelines (Temkin-Greener et al., 2015).
Several studies have examined the benefits of nursing home–based palliative care services. One study found a decrease in the use of unnecessary medications following admission of residents to a nursing home–based palliative care unit (Suhrie et al., 2009). Research has shown that specialized dementia “comfort care” units are associated with higher staff satisfaction, less observed resident discomfort, and lower costs than standard nursing
home care (Kovach et al., 1996). A systematic review of facility-based palliative care programs (Carpenter et al., 2020) found that overall, study quality was generally low and that the results of the different studies were mixed, with some evidence that facility-based palliative care teams can decrease rehospitalizations of patients at skilled nursing facilities (Berkowitz et al., 2011), reduce emergency department visits (Comart et al., 2013), decrease agitation and pain (Chapman and Toseland, 2007), and demonstrate cost savings (Teo et al., 2014). Evidence for enhanced symptom assessment, documentation, and management and engagement in advance care planning was weak (Strumpf et al., 2004). Given the weakness of the evidence, the study’s authors concluded that further research is needed to determine the effectiveness of facility-based palliative care programs (Carpenter et al., 2020).
A major barrier to developing internal nursing home palliative care services is the required financial and human resources. The need to train staff and the additional time necessary to deliver high-quality palliative care are other barriers. High turnover among staff and leadership at nursing homes also threaten the long-term viability of facility-based palliative care teams and programs (Meier et al., 2010). As noted, the evidence base for this model is particularly weak, and little is known about the most effective components and approaches for implementing and sustaining facility-based palliative care and hospice services. Moreover, there are limited financial incentives to provide high-quality palliative care, since the highest reimbursement rates are for post-acute, skilled care (Carlson et al., 2011; Ersek and Carpenter, 2013; Ersek et al., 2014; National Consensus Project for Quality Palliative Care, 2018). Specific measures added to Care Compare would support improved monitoring of the quality of palliative care services provided in nursing home settings (see Chapter 3).
Challenges to Providing Quality, Equitable End-of-Life Care to Nursing Home Residents
There is a wide variation in palliative care services provided by nursing homes (Tark et al., 2020b). In addition to the barriers and limiting factors outlined above, an overarching challenge to providing quality end-of-life care in nursing homes is the pervasive disparities in care. A systematic review (Estrada et al., 2021) revealed that racial and ethnic minority residents had lower rates of completion of advance directives, were more likely to be hospitalized at the end of life, and reported higher levels of pain and less use of hospice care at the end of life than White residents (Araw et al., 2014; Cai et al., 2016; Frahm et al., 2012, 2015; Huskamp et al., 2010b; Lage et al., 2020; Lepore et al., 2011; Monroe and Carter, 2010; Tjia et al., 2018; Zheng et al., 2011).
The review pointed out that the majority of the studies relied on data that were more than 10 years old and thus do not accurately reflect the current diversity of nursing home populations. The review also concluded that more culturally competent research is needed to explore not only the experiences of racial and ethnic minorities at the end of life, but also to characterize the specific barriers to high-quality end-of-life care in nursing homes faced by racial and ethnic minority residents (Estrada et al., 2021). The disproportionate impact of the COVID-19 pandemic on nursing home residents in general, and on racial and ethnic minorities in particular, calls for palliative care interventions. As Rosa and colleagues (2021) explain:
Palliative care health equity frameworks promote assessment of the social and moral determinants of health as well as systemic injustices to tailor services to the individual, context, and culture at hand.
This is also relevant for other minority populations in nursing homes, such as LGBTQ+ residents who could benefit from “inclusive palliative care practices that foster trust, transparency and value-concordant care delivery” (Rosa et al., 2021).
MODELS OF CARE DELIVERY
This chapter has provided an overview of the wide-ranging needs of nursing home residents and the associated complexity of the care challenges faced by nursing homes in addressing those needs. Research on best practices related to clinical, behavioral, and psychosocial care delivery in nursing homes is relatively scarce, however (Andrusjak et al., 2020; Carpenter et al., 2020; Ersek and Jablonski, 2014; NASEM, 2021; van der Wolf et al., 2019). A robust evidence base on specific models of care delivery that could serve as the most effective approach to providing high-quality person-centered care to all nursing home residents, while ensuring equitable care, has yet to be developed.
Moreover, nursing homes are often not well connected to the communities in which they are located, nor to the broader health care system (Lane and McGrady, 2016; Orth et al., 2019). Research that examines models of care that strengthen ties to the broader community and all sectors of the broader health care system is needed to improve these connections. Finally, research on care delivery needs to focus on the specific factors that affect care directly, such as optimal staffing, physical environment, financing and payment, technology, leadership, and organizational policy. Once research has successfully identified the most effective care models, that research should be translated into practice by launching demonstration projects, designed with an eye toward sustainability, to test specific models in nursing home settings.
KEY FINDINGS AND CONCLUSIONS
- The intensity of care needs is as varied as each individual nursing home resident and requires a broad range of resources and staffing.
- The care plan is critical to the identification of residents’ needs, goals, and care preferences and documenting and communicating these preferences with the interdisciplinary team are central to person-centered care.
- Despite their key role, many nursing homes are not meeting care plan requirements.
- Nursing homes are required by law to provide a range of services including medical, nursing, mental and behavioral health, psychosocial care, oral health, among other services, but many residents are not receiving adequate care.
- Despite regulatory oversight and industry reforms, the care for nursing home residents often falls short due to several factors:
- Delivery of care by inadequately trained staff,
- Hierarchical structures that impede cohesive team building and functioning,
- Inadequate staffing and high staff and leadership turnover,
- Providing care that is not aligned with evidence-based best practices,
- Need to provide care to meet the complex and evolving needs of residents,
- The lack of health information technology support for care coordination,
- Infrequent visits and limited involvement of medical directors and primary care providers, and
- Regulations that incentivize care that is not aligned with the residents’ goals and preferences.
- The lack of culturally sensitive assessments and treatment practices contribute to disparities in care and unmet needs experienced by minority populations.
- Psychosocial needs are highly ranked in most studies of unmet needs among nursing home residents.
- The number of residents with mental health needs is increasing, and the mental health needs of many residents remain unmet.
- Further research is needed to identify effective service arrangements and the requisite composition of staff to provide adequate behavioral health care in nursing homes.
- Inadequate access to behavioral health services occurs in both lower- and higher-rated facilities. Moreover, access to such services is not necessarily affected by for-profit status or the size of the facility. Some of the most commonly cited reasons for inadequate access include a lack of staff education, inadequate staffing, and inadequate infrastructure.
- Additional research needs to be conducted on the development of environments that provide nonstigmatizing specialized care that is accepting and supportive of individuals with behavioral health needs, with special attention paid to the well-being of residents.
- Dementia care practice needs to focus on the individual’s condition, needs, and desires, based on knowing the person, recognizing and accepting the person’s reality, identifying and supporting opportunities for meaningful engagement, building and nurturing authentic caring relationships, and creating and maintaining a supportive community for individuals, family, and staff.
- There is great variability among palliative care programs in nursing homes.
- There are no nationally recognized and agreed-upon standards and quality measures for nursing home–based palliative care services.
- Barriers to the development and viability of facility-based palliative care include
- Lack of financial and human resources,
- The need for staff training,
- Additional time needed to deliver such care, and
- High turnover of staff and leadership.
- The evidence base for best practices for behavioral and psychosocial care and palliative care delivery in nursing home settings is particularly weak, and little is known about the most effective components and approaches for implementing and sustaining facility-based services.
- Research is needed to identify specific models of high-quality nursing home care, which would then inform demonstration projects to test the effectiveness of care models in nursing homes.
REFERENCES
Abraham, S. 2011. Fall prevention conceptual framework. Health Care Manager 30(2): 179–184.
Achterberg, W., S. Lautenbacher, B. Husebo, A. Erdal, and K. Herr. 2019. Pain in dementia. Pain Reports 5(1):e803.
Adams-Wendling, L., U. Piamjariyakul, M. Bott, and R. L. Taunton. 2008. Strategies for translating the resident care plan into daily practice. Journal of Gerontological Nursing 34(8):50–56.
Agarwal, K. 2021. Failure to thrive in older adults: Management. https://www.uptodate.com/contents/failure-to-thrive-in-older-adults-management (accessed January 20, 2022).
Ahmed, T., and N. Haboubi. 2010. Assessment and management of nutrition in older people and its importance to health. Clinical Interventions in Aging 5:207–216.
Al Shamsi, H., A. G. Almutairi, S. Al Mashrafi, and T. Al Kalbani. 2020. Implications of language barriers for healthcare: A systematic review. Oman Medical Hournal 35(2):e122.
Alexander, G. L., and R. W. Madsen. 2021. A report of information technology and health deficiencies in U.S. nursing homes. Journal of Patient Safety 17(6):e483–e489.
Alexander, G. L., R. W. Madsen, E. L. Miller, D. S. Wakefield, K. K. Wise, and R. L. Alexander. 2017. The state of nursing home information technology sophistication in rural and nonrural U.S. markets. Journal of Rural Health 33(3):266–274.
Alexander, G. L., K. R. Powell, and C. B. Deroche. 2020a. An evaluation of telehealth expansion in U.S. nursing homes. Journal of the American Medical Informatics Association 28(2):342–348.
Alexander, G. L., C. Deroche, K. Powell, A. S. M. Mosa, L. Popejoy, and R. Koopman. 2020b. Forecasting content and stage in a nursing home information technology maturity instrument using a Delphi method. Journal of Medical Systems 44(3):60.
Allen, R. S., G. M. Harris, L. D. Burgio, C. B. Azuero, L. A. Miller, H. J. Shin, M. K. Eichorst, E. L. Csikai, J. DeCoster, L. L. Dunn, E. Kvale, and P. Parmelee. 2014. Can senior volunteers deliver reminiscence and creative activity interventions? Results of the Legacy Intervention Family Enactment randomized controlled trial. Journal of Pain and Symptom Management 48(4):590–601.
Alzheimer’s Association. 2009. Dementia care practice recommendations for assisted living residences and nursing homes. Chicago, IL: Alzheimer’s Association.
Alzheimer’s Association. 2018. Dementia care practice recommendations. https://www.alz.org/professionals/professional-providers/dementia_care_practice_recommendations (accessed October 21, 2021).
Alzheimer’s Association. 2021a. 2021 Alzheimer’s disease facts and figures: Special report—Race, ethnicity and Alzheimer’s in America. Chicago, IL: Alzheimer’s Association.
Alzheimer’s Association. 2021b. Types of dementia. https://www.alz.org/alzheimers-dementia/what-is-dementia/types-of-dementia (accessed November 4, 2021).
Andersson, S., K. Årestedt, O. Lindqvist, C.-J. Fürst, and M. Brännström. 2018. Factors associated with symptom relief in end-of-life care in residential care homes: A national register-based study. Journal of Pain and Symptom Management 55(5):1304–1312.
Andrusjak, W., A. Barbosa, and G. Mountain. 2020. Identifying and managing hearing and vision loss in older people in care homes: A scoping review of the evidence. The Gerontologist 60(3):e155–e168.
Araw, A. C., A. M. Araw, R. Pekmezaris, C. N. Nouryan, C. Sison, B. Tommasulo, and G. P. Wolf-Klein. 2014. Medical orders for life-sustaining treatment: Is it time yet? Palliative & Supportive Care 12(2):101–105.
Aschbrenner, K., D. C. Grabowski, S. Cai, S. J. Bartels, and V. Mor. 2011. Nursing home admissions and long-stay conversions among persons with and without serious mental illness. Journal of Aging & Social Policy 23(3):286–304.
Avila Institute of Gerontology. 2017. Palliative care: Implementation guide book. https://static1.squarespace.com/static/59dd966ee45a7c496fd4d1be/t/5db20e165e4b5f0984b5efd3/1571950106099/Palliative-Care-Implementation-Guide-0917-1.pdf (accessed August 23, 2021).
Bäck, I., J. Kallio, S. Perälä, and K. Mäkelä. 2012. Remote monitoring of nursing home residents using a humanoid robot. Journal of Telemedicine and Telecare 18(6):357–361.
Bailey, R. K., H. L. Blackmon, and F. L. Stevens. 2009. Major depressive disorder in the African American population: Meeting the challenges of stigma, misdiagnosis, and treatment disparities. JAMA 101(11):1084–1089.
Bainbridge, K. E., and V. Ramachandran. 2014. Hearing aid use among older U.S. adults; the National Health and Nutrition Examination Survey, 2005–2006 and 2009–2010. Ear and Hearing 35(3):289–294.
Bartels, S. J., G. S. Moak, and A. R. Dums. 2002. Mental health services in nursing homes: Models of mental health services in nursing homes: A review of the literature. Psychiatric Services 53(11):1390–1396.
Basinska, K., P. Kunzler-Heule, R. A. Guerbaai, F. Zuniga, M. Simon, N. I. H. Wellens, C. Serdaly, and D. Nicca. 2021. Residents’ and relatives’ experiences of acute situations: A qualitative study to inform a care model. The Gerontologist 61(7):1041–1052.
Batchelor-Murphy, M., S. M. Kennerly, S. D. Horn, R. Barrett, N. Bergstrom, L. Boss, and T. L. Yap. 2019. Impact of cognition and handfeeding assistance on nutritional intake for nursing home residents. Journal of Nutrition in Gerontology and Geriatrics 38(3):262–276.
Bayoumi, M. 2012. Identification of the needs of haemodialysis patients using the concept of Maslow’s hierarchy of needs. Journal of Renal Care 38(1):43–49.
Beck, C., K. J. Gately, S. Lubin, P. Moody, and C. Beverly. 2014. Building a state coalition for nursing home excellence. The Gerontologist 54(Suppl 1):S87–S97.
Becker, M., R. Andel, T. Boaz, and T. Howell. 2009. The association of individual and facility characteristics with psychiatric hospitalization among nursing home residents. International Journal of Geriatric Psychiatry 24(3):261–268.
Behrens, L., K. Van Haitsma, J. Brush, M. Boltz, D. Volpe, and A. M. Kolanowski. 2018. Negotiating risky preferences in nursing homes: A case study of the Rothschild person-centered care planning approach. Journal of Gerontological Nursing 44(8):11–17.
Bekkema, N., A. Niemeijer, B. Frederiks, and C. de Schipper. 2021. Exploring restrictive measures using action research: A participative observational study by nursing staff in nursing homes. Journal of Advanced Nursing 77(6):2785–2795.
Bender, M., K. N. Huang, and J. Raetz. 2021. Advance care planning during the COVID-19 pandemic. Journal of the American Board of Family Medicine 34(Suppl):S16–S20.
Bennett, C. 1980. Nursing home life: What it is and what it could be, 1st ed. New York: Tiresias Press, Inc.
Berkowitz, R. E., R. N. Jones, R. Rieder, M. Bryan, R. Schreiber, S. Verney, and M. K. Paasche-Orlow. 2011. Improving disposition outcomes for patients in a geriatric skilled nursing facility. Journal of the American Geriatrics Society 59(6):1130–1136.
Bern-Klug, M., K. W. Kramer, P. Sharr, and I. Cruz. 2010. Nursing home social services directors’ opinions about the number of residents they can serve. Journal of Aging and Social Policy 22(1):33–52.
Berridge, C., and V. Mor. 2018. Disparities in the prevalence of unmet needs and their consequences among black and white older adults. Journal of Aging and Health 30(9):1427–1449.
Bhattacharya, S., and R. K. Mishra. 2015. Pressure ulcers: Current understanding and newer modalities of treatment. Indian Journal of Plastic Surgery: Official Publication of the Association of Plastic Surgeons of India 48(1):4–16.
Bhattacharyya, K. K., V. Molinari, and K. Hyer. 2021. Self-reported satisfaction of older adult residents in nursing homes: Development of a conceptual framework. The Gerontologist. https://doi.org/10.1093/geront/gnab061.
Boscart, V., L. E. Crutchlow, L. Sheiban Taucar, K. Johnson, M. Heyer, M. Davey, A. P. Costa, and G. Heckman. 2020. Chronic disease management models in nursing homes: A scoping review. BMJ Open 10(2):e032316.
Bowen, S. E., and S. Zimmerman. 2008. Understanding and improving psychosocial services in long-term care. Health Care Financing Review 30(2):1–4.
Brauner, D., R. M. Werner, T. P. Shippee, J. Cursio, H. Sharma, and R. T. Konetzka. 2018. Does Nursing Home Compare reflect patient safety in nursing homes? Health Affairs (Project Hope) 37(11):1770–1778.
Brennan, P. L., and S. SooHoo. 2019. Effects of mental health disorders on nursing home residents’ nine-month pain trajectories. Pain Medicine 21(3):488–500.
Burke, R. E., and R. M. Werner. 2019. Quality measurement and nursing homes: Measuring what matters. BMJ Quality & Safety 28(7):520–523.
Burke, R. E., Y. Xu, and A. Z. Ritter. 2021. Outcomes of post-acute care in skilled nursing facilities in Medicare beneficiaries with and without a diagnosis of dementia. Journal of the American Geriatrics Society 69(10):2899–2907.
Burns, B. J., and C. A. Taube. 1990. Mental health services in general medical care and in nursing homes. In B. S. Fogel, A. Furino, and G. L. Gottlieb (eds.), Mental health policy for older Americans: Protecting minds at risk. Arlington, VA: American Psychiatric Association. Pp. 63–84.
Cai, S., S. C. Miller, and D. B. Mukamel. 2016. Racial differences in hospitalizations of dying Medicare–Medicaid dually eligible nursing home residents. Journal of the American Geriatrics Society 64(9):1798–1805.
Calkins, M., and J. Brush. 2016. Honoring individual choice in long-term residential communities when it involves risk: A person-centered approach. Journal of Gerontological Nursing 42(8):12–17.
Canavan, M. E., M. D. Aldridge Carlson, H. L. Sipsma, and E. H. Bradley. 2013. Hospice for nursing home residents: Does ownership type matter? Journal of Palliative Medicine 16(10):1221–1226.
Cantor, M., C. Liu, M. Wong, J. Chiang, D. Polakoff, and J. Dave. 2020. Reducing COVID-19 deaths in nursing homes: Call to action. https://www.healthaffairs.org/do/10.1377/hblog20200522.474405/full (accessed February 25, 2021).
CAPC (Center to Advance Palliative Care). 2008. Improving palliative care in nursing homes. New York: CAPC. https://www.capc.org (accessed April 26, 2021).
Carlson, M. D. A., B. Lim, and D. E. Meier. 2011. Strategies and innovative models for delivering palliative care in nursing homes. Journal of the American Medical Directors Association 12(2):91–98.
Carpenter, B. D., K. Van Haitsma, K. Ruckdeschel, and M. P. Lawton. 2000. The psychosocial preferences of older adults: A pilot examination of content and structure. The Gerontologist 40(3):335–348.
Carpenter, J. G. 2020. Forced to choose: When Medicare policy disrupts end-of-life care. Journal of Aging and Social Policy 1–8.
Carpenter, J. G., K. Lam, A. Z. Ritter, and M. Ersek. 2020. A systematic review of nursing home palliative care interventions: Characteristics and outcomes. Journal of the American Medical Directors Association 21(5):583–596.e2.
Castle, N. G., and R. A. Anderson. 2011. Caregiver staffing in nursing homes and their influence on quality of care: Using dynamic panel estimation methods. Medical Care 49(6):545–552.
Castle, N. G., and J. Engberg. 2007. The influence of staffing characteristics on quality of care in nursing homes. Health Services Research 42(5):1822–1847.
Castle, N. G., and M. Lin. 2010. Top management turnover and quality in nursing homes. Health Care Management Review 35(2):161–174.
Castle, N. G., J. Engberg, and A. Men. 2007. Nursing home staff turnover: Impact on nursing home compare quality measures. The Gerontologist 47(5):650–661.
Chapman, D. G., and R. W. Toseland. 2007. Effectiveness of advanced illness care teams for nursing home residents with dementia. Social Work 52(4):321–329.
Chen, J., C. D. Mullins, P. Novak, and S. B. Thomas. 2016. Personalized strategies to activate and empower patients in health care and reduce health disparities. Health Education & Behavior 43(1):25–34.
Chen, Y.-M., and J.-Y. Ji. 2015. Effects of horticultural therapy on psychosocial health in older nursing home residents: A preliminary study. Journal of Nursing Research 23(3):167–171.
Chiedi, J. M. 2018. Vulnerabilities in the Medicare hospice program affect quality care and program integrity: An OIG portfolio. https://oig.hhs.gov/oei/reports/oei-02-16-00570.asp (accessed February 25, 2021).
Chien, W., and F. R. Lin. 2012. Prevalence of hearing aid use among older adults in the United States. Archives of Internal Medicine 172(3):292–293.
Ching-Teng, Y., Y. Ya-Ping, and C. Yu-Chia. 2019. Positive effects of art therapy on depression and self-esteem of older adults in nursing homes. Social Work in Health Care 58(3):324–338.
Chisholm, L., N. J. Zhang, K. Hyer, R. Pradhan, L. Unruh, and F.-C. Lin. 2018. Culture change in nursing homes: What is the role of nursing home resources? Inquiry 55:46958018787043.
CMS (Centers for Medicare & Medicaid Services). 2012. Memorandum: F tag 155—Advance directives—Advance copy. https://www.cms.gov/medicare/provider-enrollment-and-certification/surveycertificationgeninfo/downloads/survey-and-cert-letter-12-47.pdf (accessed February 25, 2021).
CMS. 2015. Nursing home data compendium. Baltimore, MD: Centers for Medicare & Medicaid Services.
CMS. 2017. State operations manual appendix PP—Guidance to surveyors for long term care facilities. https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/GuidanceforLawsAndRegulations/Downloads/Appendix-PP-State-Operations-Manual.pdf (accessed March 26, 2021).
CMS. 2019a. Medicare coverage of skilled nursing facility care. https://www.medicare.gov/Pubs/pdf/10153-Medicare-Skilled-Nursing-Facility-Care.pdf (accessed April 29, 2021).
CMS. 2019b. Jimmo settlement. https://www.cms.gov/Center/Special-Topic/Jimmo-Center (accessed April 26, 2021).
CMS. 2020a. Medicare benefit policy manual, Chapter 9—Coverage of hospice services under hospital insurance. https://www.cms.gov/Regulations-and-guidance/Guidance/Manuals/Downloads/bp102c09.pdf (accessed January 7, 2021).
CMS. 2020b. Minimum Data Set (MDS) 3.0 for nursing homes and swing bed providers. https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/NursingHomeQualityInits/NHQIMDS30 (accessed January 23, 2021).
CMS. 2020c. Medicare hospice benefits. https://www.medicare.gov/Pubs/pdf/02154-medicare-hospice-benefits.pdf (accessed September 21, 2021).
CMS. 2021a. COVID-19 emergency declaration blanket waivers for health care providers. https://www.cms.gov/files/document/covid-19-emergency-declaration-waivers.pdf (accessed January 12, 2022).
CMS. 2021b. MDS 3.0 frequency report. https://www.cms.gov/Research-Statistics-Data-and-Systems/Computer-Data-and-Systems/Minimum-Data-Set-3-0-Public-Reports/MinimumData-Set-3-0-Frequency-Report (accessed February 15, 2022).
CMS. 2021c. Frequently asked questions (FAQS) regarding Jimmo settlement agreement. https://www.cms.gov/Center/Special-Topic/Jimmo-Settlement/FAQs (accessed January 24, 2022).
Cohen-Mansfield, J., M. Dakheel-Ali, M. S. Marx, K. Thein, and N. G. Regier. 2015. Which unmet needs contribute to behavior problems in persons with advanced dementia? Psychiatry Research 228(1):59–64.
Coleman, P., and N. M. Watson. 2006. Oral care provided by certified nursing assistants in nursing homes. Journal of the American Geriatrics Society 54(1):138–143.
Collier, E., and C. Harrington. 2008. Staffing characteristics, turnover rates, and quality of resident care in nursing facilities. Research in Gerontological Nursing 1(3):157–170.
Comart, J., A. Mahler, R. Schreiber, C. Rockett, R. N. Jones, and J. N. Morris. 2013. Palliative care for long-term care residents: Effect on clinical outcomes. The Gerontologist 53(5):874–880.
Cooper, C., P. Rapaport, S. Robertson, L. Marston, J. Barber, M. Manela, and G. Livingston. 2018. Relationship between speaking English as a second language and agitation in people with dementia living in care homes: Results from the MARQUE (Managing Agitation and Raising Quality of Life) English national care home survey. International Journal of Geriatric Psychiatry 33(3):504–509.
Corbett, A., B. Husebo, M. Malcangio, A. Staniland, J. Cohen-Mansfield, D. Aarsland, and C. Ballard. 2012. Assessment and treatment of pain in people with dementia. Nature Reviews Neurology 8(5):264–274.
Crick, M., R. Devey-Burry, J. Hu, D. E. Angus, and C. Backman. 2020. The role of regulation in the care of older people with depression living in long-term care: A systematic scoping review. BMC Geriatrics 20(1):273.
Cuevas, P. E., P. Davidson, J. Mejilla, and T. Rodney. 2021. Dignity therapy for end-of-life care patients: A literature review. Journal of Patient Experience 8:2374373521996951.
Curry, L. C., C. Walker, M. O. Hogstel, and M. B. Walker. 2007. A study of family councils in nursing homes. Geriatric Nursing 28(4):245–253.
Curtis, A., L. Gibson, M. O’Brien, and B. Roe. 2018. Systematic review of the impact of arts for health activities on health, wellbeing and quality of life of older people living in care homes. Dementia 17(6):645–669.
Cutler, L. J., and R. A. Kane. 2006. As great as all outdoors. Journal of Housing for the Elderly 19(3–4):29–48.
Davila, H., T. P. Shippee, Y. S. Park, D. Brauner, R. M. Werner, and R. T. Konetzka. 2021. Inside the black box of improving on nursing home quality measures. Medical Care Research and Review 78(6):758–770.
de Souto Barreto, P., J. E. Morley, W. Chodzko-Zajko, H. P. K, E. Weening-Djiksterhuis, L. Rodriguez-Mañas, M. Barbagallo, E. Rosendahl, A. Sinclair, F. Landi, M. Izquierdo, B. Vellas, and Y. Rolland. 2016. Recommendations on physical activity and exercise for older adults living in long-term care facilities: A taskforce report. Journal of the American Medical Directors Association 17(5):381–392.
Degenholtz, H., R. A. Kane, and H. Q. Kivnick. 1997. Care-related preferences and values of elderly community-based LTC consumers: Can case managers learn what’s important to clients? The Gerontologist 37(6):767–776.
Dellefield, M. E. 2006. Interdisciplinary care planning and the written care plan in nursing homes: A critical review. The Gerontologist 46(1):128–133.
Dellefield, M., N. Castle, K. McGilton, and K. Spilsbury. 2015. The relationship between registered nurses and nursing home quality: An integrative review (2008–2014). Nursing Economics 33(2):95–108.
Devitt, M., and B. Checkoway. 1982. Participation in nursing home resident councils: Promise and practice. The Gerontologist 22(1):49–53.
Doll, G. A., L. J. Cornelison, H. Rath, and M. L. Syme. 2017. Actualizing culture change: The Promoting Excellent Alternatives in Kansas nursing homes (PEAK 2.0) program. Psychological Services 14(3):307–315.
Duan, Y., T. P. Shippee, W. Ng, O. Akosionu, M. Woodhouse, H. Chu, J. S. Ahluwalia, J. E. Gaugler, B. A. Virnig, and J. R. Bowblis. 2020. Unmet and unimportant preferences among nursing home residents: What are key resident and facility factors? Journal of the American Medical Directors Association 21(11):1712–1717.
Dubeau, C. E., S. E. Simon, and J. N. Morris. 2006. The effect of urinary incontinence on quality of life in older nursing home residents. Journal of the American Geriatrics Society 54(9):1325–1333.
Edelman, L. S., J. Drost, R. P. Moone, K. Owens, G. L. Towsley, G. Tucker-Roghi, and J. E. Morley. 2021. Editorial: Applying the age-friendly health system framework to long-term care settings. Journal of Nutrition, Health, and Aging 25(2):141–145.
Edemekong, P. F., D. L. Bomgaars, S. Sukumaran, and S. B. Levy. 2021. Activities of daily living. In StatPearls. Treasure Island, FL: StatPearls Publishing.
Ersek, M., and J. G. Carpenter. 2013. Geriatric palliative care in long-term care settings with a focus on nursing homes. Journal of Palliative Medicine 16(10):1180–1187.
Ersek, M., and A. Jablonski. 2014. A mixed-methods approach to investigating the adoption of evidence-based pain practices in nursing homes. Journal of Gerontological Nursing 40(7):52–60.
Ersek, M., and S. A. Wilson. 2003. The challenges and opportunities in providing end-of-life care in nursing homes. Journal of Palliative Medicine 6(1):45–57.
Ersek, M., J. Sefcik, and D. Stevenson. 2014. Palliative care in nursing homes. In A. S. Kelley and D. E. Meier (eds.), Meeting the needs of older adults with serious illness: Clinical, public health, and policy perspectives. New York: Humana Press. Pp. 73–90.
Ersek, M., K. T. Unroe, J. G. Carpenter, J. G. Cagle, C. E. Stephens, and D. G. Stevenson. 2022. High-quality nursing home and palliative care—one and the same. Journal of the American Medical Directors Association 23(2):247–252.
Esteban-Burgos, A. A., M. J. Lozano-Terrón, D. Puente-Fernandez, C. Hueso-Montoro, R. Montoya-Juárez, and M. P. García-Caro. 2021. A new approach to the identification of palliative care needs and advanced chronic patients among nursing home residents. International Journal of Environmental Research and Public Health 18(6):3171.
Estrada, L. V., M. Agarwal, and P. W. Stone. 2021. Racial/ethnic disparities in nursing home end-of-life care: A systematic review. Journal of the American Medical Directors Association 22(2):279–290.e271.
Fashaw, S. A., K. S. Thomas, E. McCreedy, and V. Mor. 2020. Thirty-year trends in nursing home composition and quality since the passage of the Omnibus Reconciliation Act. Journal of the American Medical Directors Association 21(2):233–239.
Fashaw-Walters, S. A., E. McCreedy, J. P. W. Bynum, K. S. Thomas, and T. I. Shireman. 2021. Disproportionate increases in schizophrenia diagnoses among black nursing home residents with ADRD. Journal of the American Geriatrics Society 69(12):3623–3630.
Fazio, S., D. Pace, K. Maslow, S. Zimmerman, and B. Kallmyer. 2018. Alzheimer’s Association dementia care practice recommendations. The Gerontologist 58(Suppl 1):S1–S9.
Flint, L. A., D. J. David, and A. K. Smith. 2019. Rehabbed to death. New England Journal of Medicine 380(5):408–409.
Forbes-Thompson, S., B. Gajewski, J. Scott-Cawiezell, and N. Dunton. 2006. An exploration of nursing home organizational processes. Western Journal of Nursing Research 28(8):935–954.
Forsgren, E., C. Skott, L. Hartelius, and C. Saldert. 2016. Communicative barriers and resources in nursing homes from the enrolled nurses’ perspective: A qualitative interview study. International Journal of Nursing Studies 54:112–121.
Frahm, K. A., L. M. Brown, and K. Hyer. 2012. Racial disparities in end-of-life planning and services for deceased nursing home residents. Journal of the American Medical Directors Association 13(9):819.e7–819.e11.
Frahm, K. A., L. M. Brown, and K. Hyer. 2015. Racial disparities in receipt of hospice services among nursing home residents. American Journal of Hospice and Palliative Medicine 32(2):233–237.
Freedman, V. A., and B. C. Spillman. 2014. The residential continuum from home to nursing home: Size, characteristics and unmet needs of older adults. Journals of Gerontology, Series B: Psycholocial Sciences 69(Suppl 1):S42–S50.
Freeman, I. C. 1997. Nursing home politics at the state level and implications for quality: The Minnesota example. Generations 21(4):44–48.
Friedrich, S. L. 2021. Behavioral telemedicine can improve geriatric mental health. https://www.mcknights.com/marketplace/marketplace-experts/behavioral-telemedicine-can-improve-geriatric-mental-health (accessed October 26, 2021).
Fullerton, C. A., T. G. McGuire, Z. Feng, V. Mor, and D. C. Grabowski. 2009. Trends in mental health admissions to nursing homes, 1999–2005. Psychiatric Services 60(7):965–971.
Gage, L. A., K. Washington, D. P. Oliver, R. Kruse, A. Lewis, and G. Demiris. 2016. Family members’ experience with hospice in nursing homes. American Journal of Hospice & Palliative Care 33(4):354–362.
Galambos, C., J. Starr, M. J. Rantz, and G. F. Petroski. 2016. Analysis of advance directive documentation to support palliative care activities in nursing homes. Health & Social Work 41(4):228–234.
Galambos, C., M. Rantz, L. Popejoy, B. Ge, and G. Petroski. 2021. Advance directives in the nursing home setting: An initiative to increase completion and reduce potentially avoidable hospitalizations. Journal of Social Work in End-of-Life & Palliative Care 17(1):19–34.
Galik, E., B. Resnick, M. Hammersla, and J. Brightwater. 2013. Optimizing function and physical activity among nursing home residents with dementia: Testing the impact of function-focused care. The Gerontologist 54(6):930–943.
Galik, E., B. Resnick, N. Lerner, M. Hammersla, and A. L. Gruber-Baldini. 2015. Function focused care for assisted living residents with dementia. The Gerontologist 55(Suppl 1):S13–S26.
Gaugler, J. E. 2005. Family involvement in residential long-term care: A synthesis and critical review. Aging & Mental Health 9(2):105–118.
Gaugler, J. E., F. Yu, H. W. Davila, and T. Shippee. 2014. Alzheimer’s disease and nursing homes. Health Affairs (Millwood) 33(4):650–657.
Gaugler, J. E., T. L. Statz, R. W. Birkeland, K. W. Louwagie, C. M. Peterson, R. Zmora, A. Emery, H. R. McCarron, K. Hepburn, C. J. Whitlatch, M. S. Mittelman, and D. L. Roth. 2020. The residential care transition module: A single-blinded randomized controlled evaluation of a telehealth support intervention for family caregivers of persons with dementia living in residential long-term care. BMC Geriatrics 20(1):133.
Gaur, S., N. Pandya, G. Dumyati, D. A. Nace, K. Pandya, and R. L. P. Jump. 2020. A structured tool for communication and care planning in the era of the COVID-19 pandemic. Journal of the American Medical Directors Association 21(7):943–947.
Genoe, M. R., and S. L. Dupuis. 2014. The role of leisure within the dementia context. Dementia 13(1):33–58.
Gilbert, A. S., S. M. Garratt, L. Kosowicz, J. Ostaszkiewicz, and B. Dow. 2021. Aged care residents’ perspectives on quality of care in care homes: A systematic review of qualitative evidence. Research on Aging 43(7–8):294–310.
Gillespie, S. M., L. J. Gleason, J. Karuza, and M. N. Shah. 2010. Health care providers’ opinions on communication between nursing homes and emergency departments. Journal of the American Medical Directors Association 11(3):204–210.
Goddard, C., P. Speck, P. Martin, and S. Hall. 2013. Dignity therapy for older people in care homes: A qualitative study of the views of residents and recipients of “generativity” documents. Journal of Advanced Nursing 69(1):122–132.
Goossens, B., A. Sevenants, A. Declercq, and C. Van Audenhove. 2020. Shared decision-making in advance care planning for persons with dementia in nursing homes: A cross-sectional study. BMC Geriatrics 20(1):381.
Gozalo, P. L., and S. C. Miller. 2007. Hospice enrollment and evaluation of its causal effect on hospitalization of dying nursing home patients. Health Services Research 42(2):587–610.
Grabowski, D. C., K. A. Aschbrenner, Z. Feng, and V. Mor. 2009. Mental illness in nursing homes: Variations across states. Health Affairs (Millwood) 28(3):689–700.
Grabowski, D. C., K. A. Aschbrenner, V. F. Rome, and S. J. Bartels. 2010. Quality of mental health care for nursing home residents: A literature review. Medical Care Research and Review 67(6):627–656.
Grabowski, D. C., A. Elliot, B. Leitzell, L. W. Cohen, and S. Zimmerman. 2014a. Who are the innovators? Nursing homes implementing culture change. The Gerontologist 54(Suppl 1): S65–S75.
Grabowski, D. C., A. J. O’Malley, C. C. Afendulis, D. J. Caudry, A. Elliot, and S. Zimmerman. 2014b. Culture change and nursing home quality of care. The Gerontologist 54(Suppl 1): S35–S45.
Graham, J. 2019. How to find and use new federal ratings for rehab services at nursing homes. https://khn.org/news/how-to-find-and-use-new-federal-ratings-for-rehab-services-at-nursing-homes (accessed April 26, 2021).
Greene, C., J. Wilson, A. Tingle, and H. Loveday. 2019. Practical solutions for optimising hydration in care home residents. Nursing Times 115(9):30–33.
Groom, L. L., M. M. McCarthy, A. W. Stimpfel, and A. A. Brody. 2021. Telemedicine and telehealth in nursing homes: An integrative review. Journal of the American Medical Directors Association 22(9):1784–1801.
Hado, E., and L. Friss Feinberg. 2020. Amid the COVID-19 pandemic, meaningful communication between family caregivers and residents of long-term care facilities is imperative. Journal of Aging and Social Policy 32(4–5):410–415.
Hale, A., L. M. Haverhals, C. Manheim, and C. Levy. 2018. Vet Connect: A quality improvement program to provide telehealth subspecialty care for veterans residing in VA-contracted community nursing homes. Geriatrics 3(3):57.
Hall, S., C. Goddard, P. Speck, and I. J. Higginson. 2013. “It makes me feel that I’m still relevant”: A qualitative study of the views of nursing home residents on dignity therapy and taking part in a phase II randomised controlled trial of a palliative care psychotherapy. Palliative Medicine 27(4):358–366.
Hanson, L. C., and M. Ersek. 2010. Meeting palliative care needs in post-acute care settings: “To help them live until they die.” In S. J. McPhee, M. A. Winker, M. W. Rabow, S. Z. Pantilat, and A. J. Markowitz (eds.), Care at the close of life: Evidence and experience. New York: McGraw-Hill. Pp. 513–521.
Hanson, L. C., S. Sengupta, and M. Slubicki. 2005. Access to nursing home hospice: Perspectives of nursing home and hospice administrators. Journal of Palliative Medicine 8(6):1207–1213.
Harrington, C., H. Carrillo, R. Garfield, and E. Squires. 2018. Nursing facilities, staffing, residents and facility deficiencies, 2009 through 2016. https://www.kff.org/medicaid/report/nursing-facilities-staffing-residents-and-facility-deficiencies-2009-through-2016 (accessed October 22, 2020).
Harris-Kojetin, L., M. Sengupta, J. P. Lendon, V. Rome, R. Valverde, and C. Caffrey. 2019. Long-term care providers and services users in the United States, 2015–2016. https://www.cdc.gov/nchs/data/series/sr_03/sr03_43-508.pdf (accessed April 26, 2021).
Henskens, M., I. M. Nauta, M. C. A. van Eekeren, and E. J. A. Scherder. 2018. Effects of physical activity in nursing home residents with dementia: A randomized controlled trial. Dementia and Geriatric Cognitive Disorders 46(1–2):60–80.
Herr, M., J.-J. Arvieu, P. Aegerter, J.-M. Robine, and J. Ankri. 2014. Unmet health care needs of older people: Prevalence and predictors in a French cross-sectional survey. European Journal of Public Health 24(5):808–813.
Hickman, S. E., and R. Critser. 2018. National standards and state variation in physician orders for life-sustaining treatment forms. Journal of Palliative Medicine 21(7):978–986.
Hickman, S. E., C. A. Nelson, A. H. Moss, S. W. Tolle, N. A. Perrin, and B. J. Hammes. 2011. The consistency between treatments provided to nursing facility residents and orders on the physician orders for life-sustaining treatment form. Journal of the American Geriatrics Society 59(11):2091–2099.
Hickman, S. E., B. J. Hammes, A. M. Torke, R. L. Sudore, and G. A. Sachs. 2017. The quality of physician orders for life-sustaining treatment decisions: A pilot study. Journal of Palliative Medicine 20(2):155–162.
Hickman, S. E., A. M. Torke, G. A. Sachs, R. L. Sudore, Q. Tang, G. Bakoyannis, N. H. Smith, A. L. Myers, and B. J. Hammes. 2020. Do life-sustaining treatment orders match patient and surrogate preferences? The role of POLST. Journal of General Internal Medicine 36(2):413–421.
Hickman, S. E., K. Steinberg, J. Carney, and H. D. Lum. 2021. POLST is more than a code status order form: Suggestions for appropriate POLST use in long-term care. Journal of the American Medical Directors Association 22(8):1672–1677.
Hirst, S. P. 2002. Defining resident abuse within the culture of long-term care institutions. Clinical Nursing Research 11(3):267–284.
Hoben, M., H. Hu, T. Xiong, A. Kent, N. Kobagi, and M. N. Yoon. 2016. Barriers and facilitators in providing oral health care to nursing home residents, from the perspective of care aides—A systematic review protocol. Systematic Reviews 5:53.
Horn, S. D., S. A. Bender, M. L. Ferguson, R. J. Smout, N. Bergstrom, G. Taler, A. S. Cook, S. S. Sharkey, and A. C. Voss. 2004. The national pressure ulcer long-term care study: Pressure ulcer development in long-term care residents. Journal of the American Geriatrics Society 52(3):359–367.
Horn, S. D., P. Buerhaus, N. Bergstrom, and R. J. Smout. 2005. RN staffing time and outcomes of long-stay nursing home residents: Pressure ulcers and other adverse outcomes are less likely as RNs spend more time on direct patient care. American Journal of Nursing 105(11):58–70; quiz 71.
Horn, S. D., S. S. Sharkey, S. Hudak, R. J. Smout, C. C. Quinn, B. Yody, and I. Fleshner. 2010. Beyond CMS quality measure adjustments: Identifying key resident and nursing home facility factors associated with quality measures. Journal of the American Medical Directors Association 11(7):500–505.
Hughes, C. M., K. L. Lapane, and V. Mor. 2000. Influence of facility characteristics on use of antipsychotic medications in nursing homes. Medical Care 38(12):1164–1173.
Hunnicutt, J. N., J. Tjia, and K. L. Lapane. 2017a. Hospice use and pain management in elderly nursing home residents with cancer. Journal of Pain and Symptom Management 53(3):561–570.
Hunnicutt, J. N., C. M. Ulbricht, J. Tjia, and K. L. Lapane. 2017b. Pain and pharmacologic pain management in long-stay nursing home residents. Pain 158(6):1091–1099.
Huskamp, H. A., D. G. Stevenson, M. E. Chernew, and J. P. Newhouse. 2010a. A new Medicare end-of-life benefit for nursing home residents. Health Affairs 29(1):130–135.
Huskamp, H. A., D. G. Stevenson, D. C. Grabowski, E. Brennan, and N. L. Keating. 2010b. Long and short hospice stays among nursing home residents at the end of life. Journal of Palliative Medicine 13(8):957–964.
Hwang, D., J. M. Teno, M. Clark, R. Shield, C. Williams, D. Casarett, and C. Spence. 2014. Family perceptions of quality of hospice care in the nursing home. Journal of Pain and Symptom Management 48(6):1100–1107.
IOM (Institute of Medicine). 1986. Improving the quality of care in nursing homes. Washington, DC: National Academy Press.
IOM. 2001. Improving the quality of long-term care. Washington, DC: National Academy Press.
IOM. 2015. Dying in America: Improving quality and honoring individual preferences near the end of life. Washington, DC: The National Academies Press.
Jablonski, R. A., A. M. Kolanowski, A. Azuero, V. Winstead, C. Jones-Townsend, and M. L. Geisinger. 2018. Randomised clinical trial: Efficacy of strategies to provide oral hygiene activities to nursing home residents with dementia who resist mouth care. Gerodontology 35(4):365–375.
Jackson, J. C., M. J. Santoro, T. M. Ely, L. Boehm, A. L. Kiehl, L. S. Anderson, and E. W. Ely. 2014. Improving patient care through the prism of psychology: Application of Maslow’s hierarchy to sedation, delirium, and early mobility in the intensive care unit. Journal of Critical Care 29(3):438–444.
Jester, D. J., K. Hyer, and J. R. Bowblis. 2020. Quality concerns in nursing homes that serve large proportions of residents with serious mental illness. The Gerontologist 60(7):1312–1321.
Johnston, B., and M. Narayanasamy. 2016. Exploring psychosocial interventions for people with dementia that enhance personhood and relate to legacy—An integrative review. BMC Geriatrics 16(1):77.
Jones, A. L., A. J. Moss, and L. D. Harris-Kojetin. 2011. Use of advance directives in long-term care populations. NCHS Data Brief (54):1–8.
Jøranson, N., I. Pedersen, A. M. M. Rokstad, and C. Ihlebæk. 2015. Effects on symptoms of agitation and depression in persons with dementia participating in robot-assisted activity: A cluster-randomized controlled trial. Journal of the American Medical Directors Association 16(10):867–873.
Kalánková, D., M. Stolt, P. A. Scott, E. Papastavrou, and R. Suhonen. 2020. Unmet care needs of older people: A scoping review. Nursing Ethics 28(2):149–178.
Katz, P. R., K. Ryskina, D. Saliba, A. Costa, H. Y. Jung, L. M. Wagner, M. A. Unruh, B. J. Smith, A. Moser, J. Spetz, S. Feldman, and J. Karuza. 2021. Medical care delivery in U.S. nursing homes: Current and future practice. The Gerontologist 61(4):595–604.
Kemp, C. L. 2021. #MoreThanAVisitor: Families as “essential” care partners during COVID-19. The Gerontologist 61(2):145–151.
Keser, I., S. Cvijetić, A. Ilić, I. Colić Barić, D. Boschiero, and J. Z. Ilich. 2021. Assessment of body composition and dietary intake in nursing-home residents: Could lessons learned from the COVID-19 pandemic be used to prevent future casualties in older individuals? Nutrients 13(5):1510.
Keyes, C. L. M. 2002. The mental health continuum: From languishing to flourishing in life. Journal of Health and Social Behavior 43(2):207–222.
Kilgore, C. 2014. An all-hands-on-deck approach to mealtime. Caring for the Ages 15(11):12.
Kim, H., C. Bradway, S. E. Hickman, and M. Ersek. 2019. Exploring provider-surrogate communication during POLST discussions for individuals with advanced dementia. Aging & Mental Health 23(6):781–791.
King, B. J., A. L. Gilmore-Bykovskyi, R. A. Roiland, B. E. Polnaszek, B. J. Bowers, and A. J. Kind. 2013. The consequences of poor communication during transitions from hospital to skilled nursing facility: A qualitative study. Journal of the American Geriatrics Society 61(7):1095–1102.
Kitwood, T. M. 1997. Dementia reconsidered: The person comes first. Philadelphia: Open University Press.
Koenig, H. G. 2012. Religion, spirituality, and health: The research and clinical implications. ISRN Psychiatry 2012:278730.
Koren, M. J. 2010. Person-centered care for nursing home residents: The culture change movement. Health Affairs (Millwood) 29(2):312–317.
Kovach, C. R., S. A. Wilson, and P. E. Noonan. 1996. The effects of hospice interventions on behaviors, discomfort, and physical complications of end stage dementia nursing home residents. American Journal of Alzheimer’s Disease 11(4):7–15.
Koyanagi, C. 2007. Learning from history: Deinstitutionalization of people with mental illness as precursor to long-term care reform. https://www.kff.org/wp-content/uploads/2013/01/7684.pdf (accessed November 18, 2021).
Lage, D. E., C. DuMontier, Y. Lee, R. D. Nipp, S. L. Mitchell, J. S. Temel, A. El-Jawahri, and S. D. Berry. 2020. Potentially burdensome end-of-life transitions among nursing home residents with poor-prognosis cancer. Cancer 126(6):1322–1329.
Lane, S. J., and E. McGrady. 2016. Nursing home self-assessment of implementation of emergency preparedness standards. Prehospital and Disaster Medicine 31(4):422–431.
Laws, M. B., A. Beeman, S. Haigh, I. B. Wilson, and R. R. Shield. 2021. Prevalence of serious mental illness and under 65 population in nursing homes continues to grow. Journal of the American Medical Directors Association S1525-8610(21):00941-00945. Online ahead of print. https://doi.org/10.1016/j.jamda.2021.10.020.
LeadingAge CAST (Center for Aging Services Technologies). 2013. Telehealth and remote patient monitoring for long-term and post-acute care: A primer and provider selection guide. https://mtelehealth.com/pdf/studies/Telehealth_and_Remote_Patient_Monitoring_(RPM)_for_Long-Term_and_Post-Acute_Care_-_A_Primer_and_Provider_Selection_Guide_2013.pdf (accessed April 26, 2021).
Lepore, M. J., S. C. Miller, and P. Gozalo. 2011. Hospice use among urban black and white U.S. nursing home decedents in 2006. The Gerontologist 51(2):251–260.
Lepore, M., K. Scales, R. A. Anderson, K. Porter, T. Thach, E. McConnell, and K. Corazzini. 2018. Person-directed care planning in nursing homes: A scoping review. International Journal of Older People Nursing 13(4):e12212.
Lester, P. E., R. G. Stefanacci, and M. Feuerman. 2016. Prevalence and description of palliative care in U.S. nursing homes: A descriptive study. American Journal of Hospice and Palliative Medicine 33(2):171–177.
Leung, F. W., and J. F. Schnelle. 2008. Urinary and fecal incontinence in nursing home residents. Gastroenterology Clinics of North America 37(3):697-707, x. doi:10.1016/j. gtc.2008.06.005.
Li, Y. 2010. Provision of mental health services in U.S. nursing homes, 1995–2004. Psychiatric Services 61(4):349–355.
Li, Y., X. Cai, C. Harrington, M. Hasselberg, Y. Conwell, X. Cen, and H. Temkin-Greener. 2019. Racial and ethnic differences in the prevalence of depressive symptoms among U.S. nursing home residents. Journal of Aging & Social Policy 31(1):30–48.
Liu, W., J. Cheon, and S. A. Thomas. 2014. Interventions on mealtime difficulties in older adults with dementia: A systematic review. International Journal of Nursing Studies 51(1):14–27.
Logsdon, R. G., L. E. Gibbons, S. M. McCurry, and L. Teri. 2002. Assessing quality of life in older adults with cognitive impairment. Psychosomatic Medicine 64(3):510–519.
Lok, N., S. Lok, and M. Canbaz. 2017. The effect of physical activity on depressive symptoms and quality of life among elderly nursing home residents: Randomized controlled trial. Archives of Gerontology and Geriatrics 70:92–98.
Lucas, J. A., and J. R. Bowblis. 2017. CMS strategies to reduce antipsychotic drug use in nursing home patients with dementia show some progress. Health Affairs 36(7):1299–1308.
Lyons, S. S. 2010. How do people make continence care happen? An analysis of organizational culture in two nursing homes. The Gerontologist 50(3):327–339.
MACPAC (Medicaid and CHIP Payment and Access Commission). 2019. Report to Congress on oversight of institutions for mental diseases. Washington, DC: Medicaid and CHIP Payment and Access Commission.
MACPAC. 2020. MACPAC releases report to Congress on oversight of institutions for mental diseases. https://www.macpac.gov/wp-content/uploads/2020/01/MACPAC-Releases-Report-to-Congress-on-Oversight-of-Institutions-for-Mental-Diseases.pdf (accessed February 3, 2022).
MACPAC. 2021. Integrating clinical care through greater use of electronic health records for behavioral health. Chapter 4 in June 2021 report to Congress on Medicaid and CHIP. Washington, DC: Medicaid and CHIP Payment and Access Commission.
MACPAC. 2022. Payment for services in institutions for mental diseases (IMDs). https://www.macpac.gov/subtopic/payment-for-services-in-institutions-for-mental-diseases-imds/ (accessed February 3, 2022, 2022).
Magaziner, J., P. German, S. I. Zimmerman, J. R. Hebel, L. Burton, A. L. Gruber-Baldini, C. May, and S. Kittner. 2000. The prevalence of dementia in a statewide sample of new nursing home admissions aged 65 and older: Diagnosis by expert panel. Epidemiology of dementia in nursing homes research group. The Gerontologist 40(6):663–672.
Mäki-Turja-Rostedt, S., M. Stolt, H. Leino-Kilpi, and E. Haavisto. 2018. Preventive interventions for pressure ulcers in long-term older people care facilities: A systematic review. Journal of Clinical Nursing 28(13–14):2420–2442.
Malmedal, W., R. Hammervold, and B. I. Saveman. 2009. To report or not report? Attitudes held by Norwegian nursing home staff on reporting inadequate care carried out by colleagues. Scandinavian Journal of Public Health 37(7):744–750.
Mansbach, W. E., R. A. Mace, K. M. Clark, and I. M. Firth. 2017. Meaningful activity for long-term care residents with dementia: A comparison of activities and raters. The Gerontologist 57(3):461–468.
Maramaldi, P., T. Cadet, S. L. Burke, M. LeCloux, E. White, E. Kalenderian, and T. Kinnunen. 2018. Oral health and cancer screening in long-term care nursing facilities: Motivation and opportunity as intervention targets. Gerodontology 35(4):407–416.
Maslow, A. H. 1943. A theory of human motivation. Psychological Review 50(4):370–396.
Maslow, A. H. 1954. Motivation and personality. New York: Harper and Row.
McArthur, C., J. Gibbs, A. Papaioannou, J. Hirdes, J. Milligan, K. Berg, and L. Giangregorio. 2015. Scoping review of physical rehabilitation interventions in long-term care: Protocol for tools, models of delivery, outcomes and quality indicators. BMJ Open 5(6):e007528.
McCabe, M., J. Byers, L. Busija, D. Mellor, M. Bennett, and E. Beattie. 2021. How important are choice, autonomy, and relationships in predicting the quality of life of nursing home residents? Journal of Applied Gerontology 40(12):1743–1750.
McCreedy, E. M., B. E. Weinstein, J. Chodosh, and J. Blustein. 2018. Hearing loss: Why does it matter for nursing homes? Journal of the American Medical Directors Association 19(4):323–327.
McGarry, B. E., N. R. Joyce, T. G. McGuire, S. L. Mitchell, S. J. Bartels, and D. C. Grabowski. 2019. Association between high proportions of seriously mentally ill nursing home residents and the quality of resident care. Journal of the American Geriatrics Society 67(11):2346–2352.
McGarry, B. E., E. M. White, L. J. Resnik, M. Rahman, and D. C. Grabowski. 2021. Medicare’s new patient driven payment model resulted in reductions in therapy staffing in skilled nursing facilities. Health Affairs 40(3):392–399.
Mead, R. 2013. The sense of an ending. https://www.newyorker.com/magazine/2013/05/20/the-sense-of-an-ending-2 (accessed April 26, 2021).
MedPAC (Medicare Payment Advisory Commission). 2020. March 2020 report to the Congress: Medicare payment policy. Washington, DC: Medicare Payment Advisory Commission. Original edition, Chapter 12.
MedPAC. 2021. March 2021 report to the Congress: Medicare payment policy. Washington, DC: Medicare Payment Advisory Commission.
Meier, D. E., B. Lim, and M. D. Carlson. 2010. Raising the standard: Palliative care in nursing homes. Health Affairs (Millwood) 29(1):136–140.
Miller, L. M., C. J. Whitlatch, and K. S. Lyons. 2016b. Shared decision making in dementia: A review of patient and family carer involvement. Dementia 15(5):1141–1157.
Miller, S. C. 2010. A model for successful nursing home–hospice partnerships. Journal of Palliative Medicine 13(5):525–533.
Miller, S. C., and B. Han. 2008. End-of-life care in U.S. nursing homes: Nursing homes with special programs and trained staff for hospice or palliative/end-of-life care. Journal of Palliative Medicine 11:866–877.
Miller, S. C., V. Mor, N. Wu, P. Gozalo, and K. Lapane. 2002. Does receipt of hospice care in nursing homes improve the management of pain at the end of life? Journal of the American Geriatrics Society 50(3):507–515.
Miller, S. C., J. C. Lima, J. Looze, and S. L. Mitchell. 2012. Dying in U.S. nursing homes with advanced dementia: How does health care use differ for residents with, versus without, end-of-life Medicare skilled nursing facility care? Journal of Palliative Medicine 15(1):43–50.
Miller, S. C., N. Cohen, J. C. Lima, and V. Mor. 2014. Medicaid capital reimbursement policy and environmental artifacts of nursing home culture change. Gerontologist 54(Suppl 1): S76–S86.
Miller, S. C., J. C. Lima, O. Intrator, E. Martin, J. Bull, and L. C. Hanson. 2016a. Palliative care consultations in nursing homes and reductions in acute care use and potentially burdensome end-of-life transitions. Journal of the American Geriatrics Society 64(11):2280–2287.
Miller, S. C., J. C. Lima, O. Intrator, E. Martin, J. Bull, and L. C. Hanson. 2017. Specialty palliative care consultations for nursing home residents with dementia. Journal of Pain and Symptom Management 54(1):9–16.e15.
Miller, S. C., W. J. Scott, M. Ersek, C. Levy, R. Hogikyan, V. S. Periyakoil, J. G. Carpenter, J. Cohen, and M. B. Foglia. 2020. Honoring veterans’ preferences: The association between comfort care goals and care received at the end of life. Journal of Pain and Symptom Management 61(4):743-754.e1.
Mitchell, S. L., A. E. Volandes, R. Gutman, P. L. Gozalo, J. A. Ogarek, L. Loomer, E. M. McCreedy, R. Zhai, and V. Mor. 2020. Advance care planning video intervention among long-stay nursing home residents: A pragmatic cluster randomized clinical trial. JAMA Internal Medicine 180(8):1070–1078.
Mitty, E. L. 2005. Culture change in nursing homes: An ethical perspective. https://www.hmpgloballearningnetwork.com/site/altc/article/3870 (accessed September 30, 2021).
Mo, S., and J. Shi. 2020. The psychological consequences of the COVID-19 on residents and staff in nursing homes. Work, Aging and Retirement 6(4):254–259.
Moilanen, T., M. Kangasniemi, O. Papinaho, M. Mynttinen, H. Siipi, S. Suominen, and R. Suhonen. 2021. Older people’s perceived autonomy in residential care: An integrative review. Nursing Ethics 28(3):414–434.
Monroe, T. B., and M. A. Carter. 2010. A retrospective pilot study of African-American and Caucasian nursing home residents with dementia who died from cancer. Journal of Pain and Symptom Management 40(4):e1.
Mor, V., J. Zinn, J. Angelelli, J. M. Teno, and S. C. Miller. 2004. Driven to tiers: Socioeconomic and racial disparities in the quality of nursing home care. The Milbank Quarterly 82(2):227–256.
Morgan, C., N. Endozoa, C. Paradiso, M. McNamara, and M. McGuire. 2008. Enhanced toileting program decreases incontinence in long term care. Joint Commission Journal on Quality Patient Safety 34(4):206–208.
Morley, J. E., and A. M. Sanford. 2014. The god card: Spirituality in the nursing home. Journal of the American Medical Directors Association 15(8):533–535.
Morris, J. N., C. Hawes, B. E. Fries, C. D. Phillips, V. Mor, S. Katz, K. Murphy, M. L. Drugovich, and A. S. Friedlob. 1990. Designing the national Resident Assessment Instrument for nursing homes. The Gerontologist 30(3):293–307.
Morrison, R., B. Jesdale, C. Dube, S. Forrester, A. Nunes, C. Bova, and K. L. Lapane. 2021. Racial/ethnic differences in staff-assessed pain behaviors among newly admitted nursing home residents. Journal of Pain and Symptom Management 61(3):438-448.e3.
Munshi, M. N., H. Florez, E. S. Huang, R. R. Kalyani, M. Mupanomunda, N. Pandya, C. S. Swift, T. H. Taveira, and L. B. Haas. 2016. Management of diabetes in long-term care and skilled nursing facilities: A position statement of the American Diabetes Association. Diabetes Care 39(2):308–318.
Nåden, D., A. Rehnsfeldt, M.-B. Råholm, L. Lindwall, S. Caspari, T. Aasgaard, Å. Slettebø, B. Sæteren, B. Høy, B. Lillestø, A. K. T. Heggestad, and V. Lohne. 2013. Aspects of indignity in nursing home residences as experienced by family caregivers. Nursing Ethics 20(7):748–761.
Nakashima, T., Y. Young, and W.-H. Hsu. 2019. Do nursing home residents with dementia receive pain interventions? American Journal of Alzheimer’s Disease & Other Dementias 34(3):193–198.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2016. Hearing health care for adults: Priorities for improving access and affordability. Washington, DC: The National Academies Press.
NASEM. 2020. Social isolation and loneliness in older adults: Opportunities for the health care system. Washington, DC: The National Academies Press.
NASEM. 2021. Meeting the challenge of caring for persons living with dementia and their care partners and caregivers: A way forward. Washington, DC: The National Academies Press.
Nash, W. A., L. M. Harris, K. E. Heller, and B. D. Mitchell. 2021. “We are saving their bodies and destroying their souls”: Family caregivers’ experiences of formal care setting visitation restrictions during the COVID-19 pandemic. Journal of Aging & Social Policy 33(4–5):398–413.
National Consensus Project for Quality Palliative Care. 2018. Clinical practice guidelines for quality palliative care. 4th ed. Richmond, VA: National Coalition for Hospice and Palliative Care.
National Consumer Voice. 2021. Resident council center. https://theconsumervoice.org/issues/recipients/nursing-home-residents/resident-council-center#resident_council_rights (accessed May 17, 2021).
Nelson, M., and J. R. Bowblis. 2017. A new group of long-stay Medicaid nursing home residents: The unexpected trend of those under age 65 using nursing homes in Ohio. https://sc.lib.miamioh.edu/bitstream/handle/2374.MIA/6176/Nelson-A-New-Group-Medicaid-10-09-2017.pdf (accessed February 15, 2022).
Nemiroff, L., E. G. Marshall, J. L. Jensen, B. Clarke, and M. K. Andrew. 2019. Adherence to “No transfer to hospital” advance directives among nursing home residents. Journal of the American Medical Directors Association 20(11):1373–1381.
Newbould, L., G. Mountain, M. S. Hawley, and S. Ariss. 2017. Videoconferencing for health care provision for older adults in care homes: A review of the research evidence. International Journal of Telemedicine and Applications 2017:5785613.
NHPCO (National Hospice and Palliative Care Organization). 2019. Palliative care or hospice? https://www.nhpco.org/wp-content/uploads/2019/04/PalliativeCare_VS_Hospice.pdf (accessed December 28, 2020).
NHPCO. 2020. Hospice facts & figures. https://www.nhpco.org/hospice-care-overview/hospice-facts-figures (accessed September 21, 2021).
NIA (National Institute on Aging). 2018. Advance care planning: Health care directives. https://www.nia.nih.gov/health/advance-care-planning-health-care-directives (accessed October 26, 2021).
Niclasen, J., L. Lund, C. Obel, and L. Larsen. 2019. Mental health interventions among older adults: A systematic review. Scandinavian Journal of Public Health 47(2):240–250.
NIDCD (National Institute on Deafness and Other Communication Disorders). 2021. Over-the-counter hearing aids. https://www.nidcd.nih.gov/health/over-counter-hearing-aids (accessed November 3, 2021).
Northridge, M. E., A. Kumar, and R. Kaur. 2020. Disparities in access to oral health care. Annual Review of Public Health 41:513–535.
Nydén, K., M. Petersson, and M. Nyström. 2003. Unsatisfied basic needs of older patients in emergency care environments—Obstacles to an active role in decision making. Journal of Clinical Nursing 12(2):268–274.
Ogletree, A. M., R. Mangrum, Y. Harris, D. R. Gifford, R. Barry, L. Bergofsky, and D. Perfetto. 2020. Omissions of care in nursing home settings: A narrative review. Journal of the American Medical Directors Association 21(5):604–614.
OIG (Office of the Inspector General). 2003. Psychosocial services in skilled nursing facilities. Washington, DC: HHS Office of the Inspector General.
OIG. 2013. Skilled nursing facilities often fail to meet care planning and discharge planning requirements. Washington, DC: HHS Office of the Inspector General.
OIG. 2018. Vulnerabilities in the Medicare hospice program affect quality care and program integrity: An OIG portfolio. Washington, DC: HHS Office of the Inspector General.
OIG. 2019. Trends in deficiencies at nursing homes show that improvements are needed to ensure the health and safety of residents. Washington, DC: HHS Office of the Inspector General.
Olsen, C., I. Pedersen, A. Bergland, M. J. Enders-Slegers, G. Patil, and C. Ihlebaek. 2016. Effect of animal-assisted interventions on depression, agitation and quality of life in nursing home residents suffering from cognitive impairment or dementia: A cluster randomized controlled trial. International Journal of Geriatric Psychiatry 31(12):1312–1321.
Orth, J., Y. Li, A. Simning, and H. Temkin-Greener. 2019. Providing behavioral health services in nursing homes is difficult: Findings from a national survey. Journal of the American Geriatrics Society 67(8):1713–1717.
Ostaszkiewicz, J., V. Dickson-Swift, A. Hutchinson, and A. Wagg. 2020. A concept analysis of dignity-protective continence care for care dependent older people in long-term care settings. BMC Geriatrics 20(1):266.
Owsley, C., G. McGwin, Jr., K. Scilley, G. C. Meek, D. Seker, and A. Dyer. 2007a. Effect of refractive error correction on health-related quality of life and depression in older nursing home residents. Archives of Ophthalmology 125(11):1471–1477.
Owsley, C., G. McGwin, Jr., K. Scilley, G. C. Meek, D. Seker, and A. Dyer. 2007b. Impact of cataract surgery on health-related quality of life in nursing home residents. British Journal of Ophthalmology 91(10):1359–1363.
Palese, A., V. Bressan, T. Kasa, M. Meri, M. Hayter, and R. Watson. 2018. Interventions maintaining eating independence in nursing home residents: A multicentre qualitative study. BMC Geriatrics 18(1):292.
Pan, D. 2013. Timeline: Deinstitutionalization and its consequences. https://www.motherjones.com/politics/2013/04/timeline-mental-health-america (accessed November 18, 2021).
Pilgrim, A. L., S. M. Robinson, A. A. Sayer, and H. C. Roberts. 2015. An overview of appetite decline in older people. Nursing Older People 27(5):29–35.
Pioneer Network. 2016. Lighting: Partner in quality care environments. https://www.pioneernetwork.net/wp-content/uploads/2016/10/Lighting-A-Partner-in-Quality-Care-Environments-Symposium-Paper-3.pdf (accessed October 26, 2021).
Pioneer Network. 2021. Artifacts of culture change 2.0: Nursing homes. https://www.pioneernetwork.net/wp-content/uploads/2021/02/Artifacts_2.0_NH_Form_030521.pdf (accessed June 7, 2021).
Poghosyan, L., A. A. Norful, E. Fleck, J. M. Bruzzese, A. Talsma, and A. Nannini. 2017. Primary care providers’ perspectives on errors of omission. Journal of the American Board of Family Medicine 30(6):733–742.
Porter, J., A. Ntouva, A. Read, M. Murdoch, D. Ola, and G. Tsakos. 2015. The impact of oral health on the quality of life of nursing home residents. Health and Quality of Life Outcomes 13:102.
Quan, N. G., M. C. Lohman, N. V. Resciniti, and D. B. Friedman. 2020. A systematic review of interventions for loneliness among older adults living in long-term care facilities. Aging & Mental Health 24(12):1945–1955.
Rahman, M., D. C. Grabowski, O. Intrator, S. Cai, and V. Mor. 2013. Serious mental illness and nursing home quality of care. Health Services Research 48(4):1279–1298.
Rantz, M. J., L. Hicks, V. Grando, G. F. Petroski, R. W. Madsen, D. R. Mehr, V. Conn, M. Zwygart-Staffacher, J. Scott, M. Flesner, J. Bostick, R. Porter, and M. Maas. 2004. Nursing home quality, cost, staffing, and staff mix. The Gerontologist 44(1):24–38.
Recio-Saucedo, A., C. Dall’Ora, A. Maruotti, J. Ball, J. Briggs, P. Meredith, O. C. Redfern, C. Kovacs, D. Prytherch, G. B. Smith, and P. Griffiths. 2018. What impact does nursing care left undone have on patient outcomes? Review of the literature. Journal of Clinical Nursing 27(11–12):2248–2259.
Reitman, N. C. 2010. Care at home of the patient with advanced multiple sclerosis: Part 2. Home Healthcare Now 28(5):270–275.
Resnick, B., E. Galik, E. Vigne, and A. P. Carew. 2016. Dissemination and implementation of function focused care for assisted living. Health Education & Behavior 43(3):296–304.
Rice, K. N., E. A. Coleman, R. Fish, C. Levy, and J. S. Kutner. 2004. Factors influencing models of end-of-life care in nursing homes: Results of a survey of nursing home administrators. Journal of Palliative Medicine 7(5):668–675.
Rivera, E., K. B. Hirschman, and M. D. Naylor. 2020. Reported needs and depressive symptoms among older adults entering long-term services and supports. Innovation in Aging 4(3):igaa021.
Roberts, A. R., A. C. Smith, and J. R. Bowblis. 2020. Nursing home social services and postacute care: Does more qualified staff improve behavioral symptoms and reduce antipsychotic drug use? Journal of the American Medical Directors Association 21(3):388–394.
Rodney, T., N. Josiah, and D.-L. Baptiste. 2021. Loneliness in the time of COVID-19: Impact on older adults. Journal of Advanced Nursing 77(9):e24–e26.
Roelofs, T. S., K. G. Luijkx, and P. J. Embregts. 2015. Intimacy and sexuality of nursing home residents with dementia: A systematic review. International Psychogeriatrics 27(3):367–384.
Rosa, W. E., B. R. Ferrell, and D. J. Mason. 2021. Integration of palliative care into all serious illness care as a human right. JAMA Health Forum 2(4):e211099.
Rosenberg, I., D. Woo, and D. Roane. 2009. The aging patient with chronic schizophrenia. https://www.hmpgloballearningnetwork.com/site/altc/articles/aging-patient-chronic-schizophrenia (accessed February 15, 2022).
Rosenthal, M., J. Poling, A. Wec, E. Connolly, B. Angell, and S. Crystal. 2022. “Medication is just one piece of the whole puzzle”: How nursing homes change their use of antipsychotic medications. Journal of Applied Gerontology 41(1):62–72.
Ruopp, M. D. 2020. Overcoming the challenge of family separation from nursing home residents during COVID-19. Journal of the American Medical Directors Association 21(7):984–985.
Saliba, D., D. L. Weimer, Y. Shi, and D. B. Mukamel. 2018. Examination of the new short-stay nursing home quality measures: Rehospitalizations, emergency department visits, and successful returns to the community. INQUIRY: The Journal of Health Care Organization, Provision, and Financing 55:0046958018786816.
Saravanakumar, P., I. J. Higgins, P. J. Van Der Riet, and D. Sibbritt. 2018. Tai chi and yoga in residential aged care: Perspectives of participants: A qualitative study. Journal of Clinical Nursing 27(23–24):4390–4399.
Scales, K., M. Lepore, R. A. Anderson, E. S. McConnell, Y. Song, B. Kang, K. Porter, T. Thach, and K. N. Corazzini. 2019. Person-directed care planning in nursing homes: Resident, family, and staff perspectives. Journal of Applied Gerontology 38(2):183–206.
Schneider, J. 2018. The arts as a medium for care and self-care in dementia: Arguments and evidence. International Journal of Environmental Research and Public Health 15(6):1151.
Schwartz, M. L., J. C. Lima, M. A. Clark, and S. C. Miller. 2019. End-of-life culture change practices in U.S. nursing homes in 2016/2017. Journal of Pain and Symptom Management 57(3):525–534.
Scott, A. M., J. Li, S. Oyewole-Eletu, H. Q. Nguyen, B. Gass, K. B. Hirschman, S. Mitchell, S. M. Hudson, and M. V. Williams. 2017. Understanding facilitators and barriers to care transitions: Insights from project achieve site visits. Joint Commission Journal on Quality and Patient Safety 43(9):433–447.
Sheingold, S., S. Bogasky, and S. Stearns. 2015. Medicare’s hospice benefit: Revising the payment system to better reflect visit intensity. Washington, DC: HHS Office of the Assistant Secretary for Planning and Evaluation.
Sherwin, S., and M. Winsby. 2011. A relational perspective on autonomy for older adults residing in nursing homes. Health Expectations 14(2):182–190.
Shield, R. R., J. Looze, D. Tyler, M. Lepore, and S. C. Miller. 2014. Why and how do nursing homes implement culture change practices? Insights from qualitative interviews in a mixed methods study. Journal of Applied Gerontology 33(6):737–763.
Sifuentes, A. M. F., and K. L. Lapane. 2020. Oral health in nursing homes: What we know and what we need to know. Journal of Nursing Home Research 6:1–5.
Simard, J., and L. Volicer. 2020. Loneliness and isolation in long-term care and the COVID-19 pandemic. Journal of the American Medical Directors Association 21(7):966–967.
Simmons, S. F., and R. M. Bertrand. 2010. Enhancing the quality of nursing home dining assistance: New regulations and practice implications. Paper presented at Creating Home in the Nursing Home II Symposium.
Simmons, S. F., and J. F. Schnelle. 2004. Individualized feeding assistance care for nursing home residents: Staffing requirements to implement two interventions. Journals of Gerontology: Series A 59(9):M966–M973.
Simmons, S. F., and J. F. Schnelle. 2006. Feeding assistance needs of long-stay nursing home residents and staff time to provide care. Journal of the American Geriatrics Society 54(6):919–924.
Simmons, S. F., E. Keeler, X. Zhuo, K. A. Hickey, H.-W. Sato, and J. F. Schnelle. 2008. Prevention of unintentional weight loss in nursing home residents: A controlled trial of feeding assistance. Journal of the American Geriatrics Society 56(8):1466–1473.
Simmons, S. F., D. W. Durkin, A. N. Rahman, L. Choi, L. Beuscher, and J. F. Schnelle. 2013. Resident characteristics related to the lack of morning care provision in long-term care. The Gerontologist 53(1):151–161.
Simning, A., and K. V. Simons. 2017. Treatment of depression in nursing home residents without significant cognitive impairment: A systematic review. International Psychogeriatrics 29(2):209–226.
Simons, K., R. P. Connolly, R. Bonifas, P. D. Allen, K. Bailey, D. Downes, and C. Galambos. 2012a. Psychosocial assessment of nursing home residents via MDS 3.0: Recommendations for social service training, staffing, and roles in interdisciplinary care. Journal of the American Medical Directors Association 13(2):190.e9-190.e15.
Simons, K., M. Bern-Klug, and S. An. 2012b. Envisioning quality psychosocial care in nursing homes: The role of social work. Journal of the American Medical Directors Association 13(9):800–805.
Sloane, P. D., J. Ivey, M. Helton, A. L. Barrick, and A. Cerna. 2008. Nutritional issues in long-term care. Journal of the American Medical Directors Association 9(7):476–485.
Sloane, P. D., S. Zimmerman, X. Chen, A. L. Barrick, P. Poole, D. Reed, M. Mitchell, and L. W. Cohen. 2013. Effect of a person-centered mouth care intervention on care processes and outcomes in three nursing homes. Journal of the American Geriatrics Society 61(7):1158–1163.
Smyer, M. A., D. G. Shea, and A. Streit. 1994. The provision and use of mental health services in nursing homes: Results from the National Medical Expenditure Survey. American Journal of Public Health 84(2):284–287.
Stephens, C. E., L. J. Hunt, N. Bui, E. Halifax, C. S. Ritchie, and S. J. Lee. 2018. Palliative care eligibility, symptom burden, and quality of life ratings in nursing home residents. JAMA Internal Medicine 178(1):141–142.
Stevenson, D. G., and J. S. Bramson. 2009. Hospice care in the nursing home setting: A review of the literature. Journal of Pain and Symptom Management 38(3):440–451.
Stevenson, D. G., N. Sinclair, S. Zhang, L. M. Meneades, and H. A. Huskamp. 2020. Trends in contracting and common ownership between hospice agencies and nursing homes. Medical Care 58(4):329–335.
Stone, R., and M. F. Harahan. 2010. Improving the long-term care workforce serving older adults. Health Affairs (Millwood) 29(1):109–115.
Strom, K. E. 2014. HR 2013 hearing aid dispenser survey: Dispensing in the age of internet and big box retailers. https://www.hearingreview.com/hearing-products/hearing-aids/ite/hr-2013-hearing-aid-dispenser-survey-dispensing-age-internet-big-box-retailers-comparison-present-past-key-business-indicators-dispensing-offices (accessed October 26, 2021).
Strumpf, N. E., H. Tuch, D. Stillman, P. Parrish, and N. Morrison. 2004. Implementing palliative care in the nursing home. Annals of Long-Term Care 12:35–41.
Suhrie, E. M., J. T. Hanlon, E. J. Jaffe, M. A. Sevick, C. M. Ruby, and S. L. Aspinall. 2009. Impact of a geriatric nursing home palliative care service on unnecessary medication prescribing. American Journal of Geriatric Pharmacotherapy 7(1):20–25.
Sullivan, D. H., L. E. Johnson, M. M. Bopp, and P. K. Roberson. 2004. Prognostic significance of monthly weight fluctuations among older nursing home residents. Journals of Gerontology: Series A 59(6):M633–M639.
Talley, K. M., J. F. Wyman, K. Savik, R. L. Kane, C. Mueller, and H. Zhao. 2015. Restorative care’s effect on activities of daily living dependency in long-stay nursing home residents. The Gerontologist 55(Suppl 1):S88–S98.
Tariot, P. N., C. A. Podgorski, L. Blazina, and A. Leibovici. 1993. Mental disorders in the nursing home: Another perspective. American Journal of Psychiatry 150(7):1063–1069.
Tark, A., J. Song, J. Parajuli, S. Chae, and P. W. Stone. 2020a. Are we getting what we really want? A systematic review of concordance between physician orders for life-sustaining treatment (POLST) documentation and subsequent care delivered at end-of-life. American Journal of Hospice and Palliative Care 38(9):1142–1158.
Tark, A., L. V. Estrada, M. E. Tresgallo, D. D. Quigley, P. W. Stone, and M. Agarwal. 2020b. Palliative care and infection management at end of life in nursing homes: A descriptive survey. Palliative Medicine 34(5):580–588.
Tarzian, A. J., and N. B. Cheevers. 2017. Maryland’s medical orders for life-sustaining treatment form use: Reports of a statewide survey. Journal of Palliative Medicine 20(9):939–945.
Temkin-Greener, H., S. Ladwig, T. Caprio, S. Norton, T. Quill, T. Olsan, X. Cai, and D. B. Mukamel. 2015. Developing palliative care practice guidelines and standards for nursing home-based palliative care teams: A Delphi study. Journal of the American Medical Directors Association 16(1):86.e1–86.e867.
Temkin-Greener, H., L. Campbell, X. Cai, M. J. Hasselberg, and Y. Li. 2018. Are post-acute patients with behavioral health disorders admitted to lower-quality nursing homes? American Journal of Geriatric Psychiatry 26(6):643–654.
Teno, J. M., P. Gozalo, A. N. Trivedi, J. Bunker, J. Lima, J. Ogarek, and V. Mor. 2018. Site of death, place of care, and health care transitions among U.S. Medicare beneficiaries, 2000–2015. JAMA 320(3):264–271.
Teo, W. S., A. G. Raj, W. S. Tan, C. W. Ng, B. H. Heng, and I. Y. Leong. 2014. Economic impact analysis of an end-of-life programme for nursing home residents. Palliative Medicine 28(5):430–437.
Terrell, K. M., and D. K. Miller. 2006. Challenges in transitional care between nursing homes and emergency departments. Journal of the American Medical Directors Association 7(8):499–505.
Tjia, J., M. Dharmawardene, and J. L. Givens. 2018. Advance directives among nursing home residents with mild, moderate, and advanced dementia. Journal of Palliative Medicine 21(1):16–21.
Tobis, S., K. Wieczorowska-Tobis, D. Talarska, M. Pawlaczyk, and A. Suwalska. 2018. Needs of older adults living in long-term care institutions: An observational study using Camberwell assessment of need for the elderly. Clinical Interventions in Aging 13:2389–2395.
Travers, J. L., K. B. Hirschman, and M. D. Naylor. 2022. Older adults’ goals and expectations when using long-term services and supports. Journal of Applied Gerontology 41(3):709-717.
Vaartio-Rajalin, H., R. Santamäki-Fischer, P. Jokisalo, and L. Fagerström. 2021. Art making and expressive art therapy in adult health and nursing care: A scoping review. International Journal of Nursing Sciences 8(1):102–119.
VanArsdall, P. S., and J. Aalboe. 2016. Improving the oral health of long term care facility residents. https://decisionsindentistry.com/article/improving-oral-health-long-term-care-facility-residents/ (accessed February 1, 2022).
Van Den Bos, J., K. Rustagi, T. Gray, M. Halford, E. Ziemkiewicz, and J. Shreve. 2011. The $17.1 billion problem: The annual cost of measurable medical errors. Health Affairs 30(4):596–603.
van den Brink, A. M. A., D. L. Gerritsen, M. M. H. de Valk, A. T. Mulder, R. C. Oude Voshaar, and R. Koopmans. 2018. What do nursing home residents with mental–physical multimorbidity need and who actually knows this? A cross-sectional cohort study. International Journal of Nursing Studies 81:89–97.
van der Wolf, E., S. A. H. van Hooren, W. Waterink, and L. Lechner. 2019. Well-being in elderly long-term care residents with chronic mental disorder: A systematic review. Aging and Mental Health 23(3):287–296.
Van Haitsma, K., K. M. Abbott, A. R. Heid, A. Spector, K. Eshraghi, C. Duntzee, S. Humes, V. Crumbie, S. D. Crespy, and M. Van Valkenburgh-Schultz. 2016. Honoring nursing home resident preferences for recreational activities to advance person-centered care. Annals of Long-Term Care 24(2):25–33.
Vest, J. R., H. Y. Jung, K. Wiley, Jr., H. Kooreman, L. Pettit, and M. A. Unruh. 2019. Adoption of health information technology among U.S. nursing facilities. Journal of the American Medical Directors Association 20(8):995–1000.
Weber, P. C. 2021. Hearing amplification in adults. https://www.uptodate.com/contents/hearing-amplification-in-adults (accessed October 26, 2021).
Wells, J. L., and A. C. Dumbrell. 2006. Nutrition and aging: Assessment and treatment of compromised nutritional status in frail elderly patients. Clinical Interventions in Aging 1(1):67–79.
Wendrich-van Dael, A., F. Bunn, J. Lynch, L. Pivodic, L. Van den Block, and C. Goodman. 2020. Advance care planning for people living with dementia: An umbrella review of effectiveness and experiences. International Journal of Nursing Studies 107:103576.
White-Chu, E. F., W. J. Graves, S. M. Godfrey, A. Bonner, and P. Sloane. 2009. Beyond the medical model: The culture change revolution in long-term care. Journal of the American Medical Directors Association 10(6):370–378.
Williams, N., N. A. Phillips, W. Wittich, J. L. Campos, P. Mick, J. B. Orange, M. K. PichoraFuller, M. Y. Savundranayagam, and D. M. Guthrie. 2020. Hearing and cognitive impairments increase the risk of long-term care admissions. Innovation in Aging 4(2):igz053.
Willink, A., N. S. Reed, and F. R. Lin. 2019. Access to hearing care services among older Medicare beneficiaries using hearing aids. Health Affairs 38(1):124–131.
Woods, B., L. O’Philbin, E. M. Farrell, A. E. Spector, and M. Orrell. 2018. Reminiscence therapy for dementia. Cochrane Database of Systematic Reviews 3(3):CD001120.
Xiang, X., R. An, and A. Heinemann. 2017. Depression and unmet needs for assistance with daily activities among community-dwelling older adults. The Gerontologist 58(3):428–437.
Xu, D., and R. L. Kane. 2013. Effect of urinary incontinence on older nursing home residents’ self-reported quality of life. Journal of the American Geriatrics Society 61(9):1473–1481.
Ye, P., L. Fry, and J. D. Champion. 2021. Changes in advance care planning for nursing home residents during the COVID-19 pandemic. Journal of the American Medical Directors Association 22(1):209–214.
Yorozuya, K., Y. Kubo, N. Tomiyama, S. Yamane, and H. Hanaoka. 2019. A systematic review of multimodal non-pharmacological interventions for cognitive function in older people with dementia in nursing homes. Dementia and Geriatric Cognitive Disorders 48(1–2):1–16.
Yurkofsky, M., and J. G. Ouslander. 2021. Medical care in skilled nursing facilities (SNFs) in the United States. https://www.uptodate.com/contents/medical-care-in-skilled-nursing-facilities-snfs-in-the-united-states (accessed July 16, 2021).
Zalenski, R. J., and R. Raspa. 2006. Maslow’s hierarchy of needs: A framework for achieving human potential in hospice. Journal of Palliative Medicine 9(5):1120–1127.
Zhang, N. J., D. Gammonley, S. C. Paek, and K. Frahm. 2008. Facility service environments, staffing, and psychosocial care in nursing homes. Health Care Financing Review 30(2):5–17.
Zhang, Y., H. Xiao, and B. Yong. 2020. Interventions for improving psychosocial adjustment in nursing home residents: A network meta-analysis. Innovation in Aging 4(Suppl 1):279.
Zheng, N. T., D. B. Mukamel, T. Caprio, S. Cai, and H. Temkin-Greener. 2011. Racial disparities in in-hospital death and hospice use among nursing home residents at the end-of-life. Medical Care 49(11):992.
Zimmerman, S., P. D. Sloane, C. S. Williams, P. S. Reed, J. S. Preisser, J. K. Eckert, M. Boustani, and D. Dobbs. 2005. Dementia care and quality of life in assisted living and nursing homes. The Gerontologist 45(1):133–146.
Zimmerman, S., P. D. Sloane, C. S. Williams, D. Dobbs, R. Ellajosyula, A. Braaten, M. F. Rupnow, and D. I. Kaufer. 2007. Residential care/assisted living staff may detect undiagnosed dementia using the Minimum Data Set cognition scale. Journal of the American Geriatrics Society 55(9):1349–1355.
Zimmerman, S., S. Austin, L. Cohen, D. Reed, P. Poole, K. Ward, and P. D. Sloane. 2017. Readily identifiable risk factors of nursing home residents’ oral hygiene: Dementia, hospice, and length of stay. Journal of the American Geriatrics Society 65(11):2516–2521.
Zimmerman, S., P. D. Sloane, K. Ward, C. J. Wretman, S. C. Stearns, P. Poole, and J. S. Preisser. 2020. Effectiveness of a mouth care program provided by nursing home staff vs. standard care on reducing pneumonia incidence: A cluster randomized trial. JAMA Network Open 3(6):e204321.
Zúñiga, F., M. Schubert, J. P. H. Hamers, M. Simon, R. Schwendimann, S. Engberg, and D. Ausserhofer. 2016. Evidence on the validity and reliability of the German, French and Italian nursing home version of the Basel extent of rationing of nursing care instrument. Journal of Advanced Nursing 72(8):1948–1963.
Zweig, S. C., L. L. Popejoy, D. Parker-Oliver, and S. E. Meadows. 2011. The physician’s role in patients’ nursing home care: “She’s a very courageous and lovely woman. I enjoy caring for her.” JAMA 306(13):1468–1478.












































































