
6
Looking Forward
More than any other event since the conception and emergence of CSC plans in 2009, the COVID-19 pandemic has tested how well these plans work. Throughout this experience, lessons have been learned that can inform future planning and give jurisdictions who are just now learning about this framework options to leap past much of the experiential learning that had to take place over the past 10 years. In this chapter, speakers highlight the experiences of CSC at the federal level and the potential roles for the federal government going forward. A subsequent panel discussion synthesizes the challenges and opportunities across key areas of CSC, as previously discussed throughout this workshop series: staffing; planning and implementation; and legal, ethical, and equity considerations. The chapter concludes with a reflection on the opportunities for CSC as the COVID-19 pandemic continues and as leaders and responders continue to consider the risk of the emergence of new pathogens.
KEYNOTE PRESENTATIONS
David Christian Hassell, senior science advisor, deputy assistant secretary for preparedness and response, Office of the Assistant Secretary for Preparedness and Response (ASPR) within HHS, recounted his initial encounter with the 2009 CSC set when he arrived at the ASPR office in 2019. However, once COVID-19 emerged, he said, ASPR realized that CSC needed another look given that it would likely play a role as the pandemic unfolded. From the beginning, ASPR has been very concerned about the effect on frontline health workers and has tried to understand the various
needs of different settings. Essentially, ASPR’s goal is to understand how to help clinicians provide the highest benefit to patients, Hassell said.
Richard Hunt, senior medical advisor, National Health Care Preparedness Programs, ASPR, shared some observations after listening to many clinicians throughout the pandemic. “We really didn’t have a lot of experience implementing CSC before,” he said, “but now we have learned quite a bit.” While listening to frontline workers and the general public about their thoughts related to CSC is important, Hunt said, it needs to be paired with the years of work spent on planning and learn from those who have clinical bedside experience with CSC. He added that the implementation of CSC across the country, with or without planning and standards, outlined the challenges that come with CSC. At its core, CSC happens between patients and their health care team. Some providers had little to no awareness of CSC prior to having to make life-or-death decisions for their patients. Moral injury, compassion fatigue, and attacks on clinicians are becoming more prevalent, said Hunt. Many providers are walking away from medicine. He shared an example in Montana where in some regions, 9-1-1 calls via EMS are met with no response (Montana DPHHS et al., 2021).
CSC addresses the times when there are scarce resources available, especially given the health care workforce shortage—which will likely last for years. Hunt pointed out that the health care delivery system in the United States has become diminished in its capability and capacity. He asked how the nation could best address this profound challenge, and how it could support clinicians to deliver the best care possible when they do have to implement CSC without indicators and standards. If there is no room in curriculums and continued learning for CSC, Hunt asked, then how can the federal government best support clinicians either in real-time when they are faced with difficult decisions, or after they have made them and are left with profound mental anguish? Acknowledging the fatigue that many providers feel and how that affects work on CSC, Hunt stated that based on the experience throughout the pandemic, iterative thinking will not work. He concluded that there is a need to be bold and open minded in thinking about changes, and this kind of an opportunity may only come once in a century.
Roles for the Federal Government
Hassell said the more that federal agencies can provide all the CSC tools in advance for clinicians and policy makers at the state and local levels, the better. There is a great deal of focus on the technical and scientific aspects, he explained, but there is also a need to talk about nontechnical aspects, including the administration of programs and education by politicians and bureaucrats. Federal agencies have a role, but they cannot do it
alone, and they need to partner with other organizations to be successful. Hunt added that, being involved in some way with the development of CSC over the years, he has learned that denial is a powerful tool. Nobody wants to do this, he said. Whether it is a clinician at the bedside, hospital leadership, or the general public, no one wants to have these conversations. When working with various jurisdictions and clinicians, the whole idea is “out of sight, out of mind,” he explained. But providing tools and finding areas where the people can engage with state and local officials has more receptivity now compared to before the pandemic. He cautioned not to underestimate how difficult this process is. He also agreed with Hassell that involvement from federal agencies is not a magic bullet solution. Grassroots approaches and clinicians familiar with ethical concepts who embrace the process are critical.
The federal government has been accomplishing a great deal in this area, but it is frustrating that many clinicians have never heard of CSC, said Eric Toner, senior scholar, Center for Health Security, Johns Hopkins University. He wondered what else could be done to address this and get the attention of those who need to hear this. Hunt replied that using whatever levers are available to make this into clinician education training would be valuable. There is extraordinary variability in the awareness of clinicians about CSC, and many just do the “best they can” and do not connect their decisions at all with the concepts and established frameworks of CSC. Hassell added that more input is needed. ASPR has been reaching out to broad groups of stakeholders, but Hassel said he is interested to know what others think the federal government and national academies can do to help support this effort. Toner finished by saying we should think of ways to not only revise guidance but also to better disseminate and foster its adoption.
REFLECTIONS ON CHALLENGES AND OPPORTUNITIES
This section brings together the topics discussed throughout the workshop series. Speakers summarized the targeted discussions and offered either future questions to consider or key lessons to inform planning across the areas of staffing; planning and implementation; and legal, ethical, and equity issues.
Staffing Considerations
Tener Goodwin Veenema, professor of nursing, Johns Hopkins Center for Health Security, reviewed some of the goals of their discussion, including articulating the opportunities highlighted in Chapter 3 to improve the CSC framework and guidance for planning, activation, implementation, evaluation, and monitoring. She acknowledged the challenges ahead when
thinking about not only future staffing needs but also considering the long-term effect on the health care workforce.
First, Veenema recounted some statements and findings discussed in Chapter 3. The moral injury and staff attrition in health care have been profound, she said, with 30 percent considering leaving their profession. She also noted that 60 percent reported experiencing negative effects on their mental health as a result of their work throughout the pandemic. She mentioned the confusion over the difference between moving from contingency mode to crisis mode, and the allocation of scarce resources decisions left to providers at the bedside. She also highlighted the travel nursing industry, which has contributed to many staffing challenges for hospitals and health care centers.
Challenges include obstacles to mobilizing staff, realizing institutions were not very good at predicting staffing needs, and the need for better cross-sector collaboration across the health care disciplines. There was also a loss of team cohesion, she noted, which has a negative effect on efficiency and trust during difficult patient care situations. This is especially amplified when there are new staff or rotating providers who are not familiar with institutional policies and protocols. For a future framework of CSC staffing needs, she offered several ideas, issues, and strategies:
- Use technology more effectively to resolve or alleviate staffing burden issues (allow nursing care delivery to include telenursing and the e-ICU),
- Better data collection,
- Collected data needs to be shared with relevant parties to be more useful,
- Improve collaboration and communication with entities crossing state borders (e.g., load balancing, EMS, e-ICUs), and
- Create a built-in ethical framework for staffing during CSC implementation.
Veenema reiterated some of the immediate, short-term, and long-term strategies that some large integrated health care centers are using (see Figure 3-3). She also noted the inflection point of two concurrent crises happening in November 2021—the Delta variant and its resulting surge of unvaccinated patients coupled with the burnout crisis of the health care workforce. Physicians are closing practices, there has been an increase in suicides and suicidal ideations in health care professionals, and nurses are leaving the workforce, she explained. She asked how best to correct these and build in respite care to give the workforce time to take a breath and build much-needed resilience. She also wondered what could be done to the workforce pipeline to mitigate future shortages.
Gregg Meyers, president of the Community Division and executive vice president of value-based care at Mass General Brigham, addressed the ongoing challenge of trying to preserve the health care workforce and finding the balance between resilience and workforce stressors. Trying to attend to the hierarchy of needs among colleagues includes ensuring our workforce is sufficiently prepared for these events and feels supported, Meyers added. Workers also need to feel recognized and honored for the work they do. He outlined several foundational elements for the future, based on creating a safe and nurturing workplace setting (see Box 3-1).
Meyers also highlighted some of the key administrative considerations in staffing, including the perverse payment structures that finance the nursing and technical workforce, and he wondered how to invest in nursing differently. As many learned, providing childcare turns out to be absolutely essential to responding to a long-term event and keeping people in the workforce. While this previously seemed outside the purview of health care, it is now front and center.
He also noted the suggestion that there should be a federal overarching coordinating body for CSC. He offered that it could be housed within ASPR and could have the scope of authority to mobilize the resources necessary to respond. This body could also provide a pulse check, he said, and be able to assess staffing numbers nationally and provide situational awareness on what is happening around the country. Finally, Meyers said being able to provide virtual care and harness technology in the e-ICU has been such a jump forward. The ability to virtually move staff through time and space is something that has never been done.
Future Changes to Improve Workforce Needs
Mike Wargo, vice president and chief, Enterprise Preparedness and Emergency Operations, HCA Healthcare, highlighted the notion of the cross-sector alliance, but said we need a stronger bond between health care and public health leaders. He suggested reevaluating the health care incident management system and educating health care leaders more on this unified model and how everyday surges are typically managed. He also called for embracing the future workforce—looking to academia and educating future nurses and emergency managers on CSC. He argued that the workforce should be given the opportunity to understand what to expect in hopes of changing the culture, said Wargo. As Meyers mentioned, many current workers are nearing retirement, and the Medical Reserve Corps (MRC), the national network of medical volunteers, should acknowledge that and prepare itself as best as possible. Wargo noted that the MRC had been left to stagnate, but when COVID-19 suddenly emerged, the health care system needed to rely on it. He suggested encouraging those around
the country who are retiring now or in the short term to join the MRC unit closest to them.
Finally, he advocated for a unified mission and vision. Wargo concluded that if a common vision of what crisis looks like was shared, then the community would be able to come together, which would lead to better outcomes. Asha Devereaux, senior medical officer, Sharp Coronado Hospital, also added that outpatient providers and their teams are typically not included in CSC planning. As seen throughout the COVID-19 pandemic, CSC happened in the outpatient world as well. “Whether patients selected to do hospice at home and avoid crowded hospital settings, they will need our support,” she concluded.
Planning and Implementation
Anuj Mehta, assistant professor of medicine, Denver Health and Hospital Authority, reflected on some of the challenges his team identified around planning and implementation, saying when thinking about moving from plans to reality, they considered implementation case studies, workforce preparation challenges, decision-making challenges, and public and stakeholder perceptions. There has been a lot of debate about how to triage patients for ventilators, he said, or guiding decisions about things that cannot be anticipated in a crisis that may evolve over time. The workshop on planning and implementation highlighted that situational awareness should drive decision making relating to CSC development and planning, as well as activation, implementation, evaluation, and monitoring.
Health care is not the best at real-time assessment, he noted, as has been discussed previously, but many things emerged across speakers and conversations that can and should inform future work. He listed key lessons concerning community engagement, coordination and collaboration, and the workforce (Box 6-1).
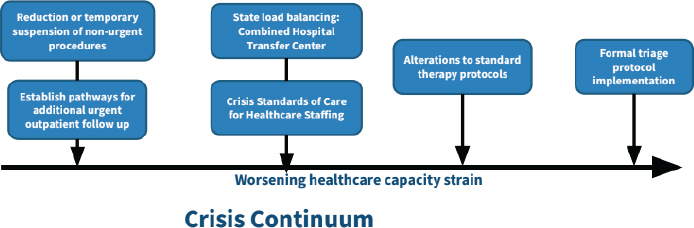
Mehta noted that CSC should not be just triage. Supporting mental health in addition to basic human resources staffing is critical (see Figure 6-1). CSC is a deviation from the standard of care where care to patients is degraded to what would be considered acceptable. He said the line between contingency and crisis is often blurred and that this is where the discomfort arises being a physician. He also suggested considering reducing nonurgent procedures, load balancing, or altering standard therapy—as all of these things may happen before a formal triage protocol for CSC is implemented. This continuum presents a risk to the moral and ethical duties that clinicians have, as well as adding to licensure and liability concerns. He echoed past comments on the importance of presenting this type of event as a continuum related to an ongoing crisis rather than a dichotomous switch that turns on and off.
The scarcity goes beyond discrete devices like ventilators, Mehta continued. Throughout the pandemic, health care systems have experienced shortages of various staff types and shortages of medications, oxygen, or dialysis machines. There are also patients that may be downgraded to a lower level of care than they typically would receive. Now health care is facing shortages across the entire system, he noted, and not just ventilators. Thinking beyond the basic allocation of scarce resources related to types of devices or supplies, he presented a broad framework for CSC, and posited
SOURCE: Anuj Mehta presentation, November 22, 2021.
the following questions to guide a more global framework when deciding how best to allocate scarce resources:
- How likely is a patient to survive without the resource being considered?
- How likely is a patient to not need readmission or reevaluation without the resource considered?
- How likely is a patient to survive even if they do receive the resource being considered?
- Does the patient have realistic access to an alternate care pathway if they are triaged to it (e.g., outpatient care including follow-up, equipment, supplies, and medications)?
While CSC is a continuum, Mehta said, it also involves a host of decision-making points that we may think about today but cannot anticipate what they will be tomorrow. He called for a framework to guide practice both ethically and practically. He concluded that the one key lesson learned is that there will be another crisis, so this is an opportunity to create systems that can perform better next time.
Discussion
Toner asked how the benefits of moving resources from one group to another can be assessed. For example, moving staff members around or cancelling elective procedures to take care of COVID-19 patients has been done, but no one has talked about whether the real effect—benefit or harm—is known. Mehta agreed this is an important question and comes with other key related questions. How do you evaluate this in real time? Are we achieving the benefit we want? Are we identifying patients most
likely to survive? Patients need to be tracked during triage, he said, not just left to wait until the crisis is over. There also needs to be real-time equity evaluations.
Inequities built into the health care system have been exacerbated in this pandemic, Mehta said. Lots of scoring systems have inequities too, he noted, so providers and hospital leaders need to evaluate inequity in all situations where care is being delivered. Those living in rural areas or who have low insurance coverage may be presenting to a hospital much later in their illness progression, and thus have more severe disease because they do not have accessible services. What should we be thinking about regarding how the shifting of resources that occurred affected other patients, both short term and long term, to inform decisions for the next crisis. Where can the health care system actually expand? What are the downstream consequences when the system shrinks back? There is a need to further research these questions to inform the planning for the next crisis, he concluded.
Toner asked who should be involved in making these critical triage decisions. Mehta responded that there are established large-scale frameworks and scores that may be adopted at a state level, but there is a need to consider key stakeholders when doing that. At the ground level in the hospital, he argued for the need to remove this responsibility from the health care providers at the bedside, who are naturally invested in getting their patients the best possible outcome. Having a more objective group of people who have the right expertise and who are also a bit removed from direct care, and who are able to make these decisions, is paramount.
Shandiin Wood, health systems epidemiologist and tribal liaison, New Mexico Department of Health, said that one thing to learn from this experience is the importance of adherence to the plan in a consistent format across different sites, hospitals, and regions within the state. If there is a consistent implementation of a framework adoption, he said, then you have the benefit of looking at intermediate outcomes and fidelity of the adopted plan, which can then provide insight into the long-term effects. This is better than a haphazard adoption of frameworks at different hospitals across the same region, which has happened in many places. He emphasized the need to standardize health and survival outcomes in a given area for people who have gone through that framework.
Legal, Ethical, and Equity Considerations
Jennifer Piatt, deputy director, Network for Public Health Law–Western Region Office, reviewed the webinar discussion dedicated to legal challenges and opportunities pertaining to liability protections in CSC, as well as the incorporation of ethical and equity considerations in the allocation of scarce resources. Piatt said there are two approaches
during CSC implementation. The first involves following the standard of care and evolving with changing circumstances, so the standard of care shifts as needed. But there are distinct concerns in this pathway, she said. It becomes extremely difficult to assess retroactively where a particular standard shifted in a particular location at a particular time. There are lots of different interpretations on that standard; without uniformity, the state, local, and hospital plans all differ.
The second pathway provides enhanced liability protections and may provide more comfort for providers who know that they are supported. But questions for this pathway include duration of the protections and scope of immunity provided. Protections may only last during an emergency declaration, Piatt explained, and may only apply to specific persons or behavior. For example, she reviewed two legal sources for liability protection at the federal level. The CARES Act provides express liability protections for interstate volunteer health care workers, in contrast with the PREP Act, which applies to all covered health care workers against claims of loss in response to a public health emergency. Additional protections can differ at the state level across jurisdictions, resulting in a confusing patchwork of protections at different times for different people or entities.
The second area Piatt highlighted is nondiscrimination in CSC and making difficult decisions lawfully during emergencies. The HHS Office of Civil Rights set up the three categories of red, yellow, and green light scenarios included in triage plans to help guide decisions. She explained that clearly impermissible bases are legally prohibited allocations, which involve categorical exclusions based on protected criteria. She added that the list should be considered as “evolving” as additional evidence arises to illustrate additional disparate effects of other possible allocations bases. CSC plans need to go beyond simply identifying express discrimination and address issues that perpetuate systemic inequities, like SOFA scoring. Planning must be deliberate in addressing disparities, she said.
Monica Peek, professor of medicine, University of Chicago, transitioned to thinking about explicitly ethical issues. The large question with CSC, she said, is can we align multiple different ethical goals? In other words, can we try to prevent harm such as death or illness, as well as loss of caregivers? Can people be treated with equal concern? Can health disparities be mitigated? For those who have been facing structural disadvantages, she asked, how do we as a society take into consideration that their lives have been harmed by policies and procedures that have put them at a disadvantage over time? These people come into health systems with an extra burden of “dis-health” and disease, she noted.
Some research is showing promise for the alignment of these goals. For example, within the ICU, studies have shown that age-aware approaches prevent more deaths and better mitigate racial inequity than SOFA alone
(Raschke et al., 2021). When we think about the distribution of COVID-19 vaccines, Peek said, combining age and SVI is better at preventing harm and mitigating inequity than age alone (Wrigley-Field et al., 2021). She noted the increasing ways being discovered to use these principles in a synergistic fashion to achieve more goals. There are several challenges with mitigation of health disparities. Some categories are not legally allowed to be considered, such as those in the red list, as Piatt had previously noted, but others, while sometimes controversial, can be considered—such as age, vaccination status, SVI, and health metrics.
The previous workshop dedicated to this topic (detailed in Chapter 5) included much discussion around race, but the racial health disparities were amplified and seen the most in news headlines during the COVID-19 pandemic. Peek asked what are the best ways to address those disparities most effectively and comprehensively, and whether this should be done by thinking about individual race, group-level race (including structural disadvantage), or racism. She pondered whether it could be achieved by working exclusively within current legal constraints, or by thinking about a longer historical narrative where there is an understanding that laws were not always just and it has been part of our country’s history to push back against laws that may not be fair—especially for racial and ethnic minorities. Peek suggested the most justice might be found by pushing back against laws and fully capturing racial equity in decision systems for CSC. Solely looking at some of the mechanisms through which structural racism occurs, she said, will make it difficult to develop ways to mitigate health disparities most effectively.
When thinking about scarce resource allocation in the ICU, the resources that come to mind most often are things like ventilators, but as others have mentioned, leaders should be expanding their own mindsets to also think about people, monoclonal antibodies, and other critical resources that may become scarce. She commented that one topic that has been prevalent throughout the webinar series has been the hospital transfer systems and their role in mitigating inequities. That is the most important next frontier in trying to mitigate health inequities—thinking about load balancing at the community level, Peek noted. It is important to consider that small hospitals, often serving communities of color, are most often overrun while tertiary care systems, which primarily serve white communities, have more resources and capacity. She concluded that keeping this in mind when facilitating load balancing can promote equity.
Ethical Reactions to the Pandemic
Matt Wynia, director, Center for Bioethics and Humanities, University of Colorado, said many of the challenges experienced in the pandemic were
expected, but we did not know the extent to which they were going to come into play. For example, the critical importance of load balancing to avoid going into CSC emerged in several locations as a potential preventive measure. Early in the pandemic in New York City, he said, it was more understandable that some hospitals were forced into contingency modes while others nearby had empty beds, as everyone was still figuring things out. But he referred to a story in Texas where just a few months ago a young man died of a curable illness because a hospital bed could not be found. That is completely inexcusable at this point in the pandemic, he argued.
Wynia also commented on the reticence health care institutions had about entering CSC and no longer being able to offer standard services to their population, saying he and his colleagues did expect some of that hesitation. But they did not realize the degree to which hospitals and states would wait and avoid authorizing and activating CSC. By the time organizations actually admit they are at that point, he said, they’ve been there for weeks, if not months. He noted that Colorado had declared CSC for certain things, but many institutions and providers are doing things right now that are quite risky, and doing them without protections.
Finally, he pointed out the irony of CSC documents clearly stating up front that such factors as race, age, and socioeconomic status are not used in allocations and algorithms, but it has become clear during the pandemic that sometimes those do have to be used. For example, early on when authorities were talking about ventilator allocation in several places, the focus was very much on who would die even if they got a ventilator. But thinking about discharge, he said, we now need to consider these types of factors because you cannot ethically discharge someone without insurance coverage or social supports even though they clinically might be the best case to get discharged. Additionally, when age was used for vaccine allocation and distribution there was very little pushback, and elderly people were happy to be first in line. But for other things, like ICU allocation, people were not happy to see age being used as a reason not to receive an ICU bed. So even within our own field, Wynia concluded, there are tensions about how best to use these kinds of criteria.
LOOKING TO THE FUTURE
Suzet McKinney, principal and director of Life Sciences at Sterling Bay, outlined where we can learn and inform planning. Previously, there were a few examples where there were opportunities to gain experience with CSC, such as the Ebola outbreak and certain hurricanes. But at this point, she explained, there has been enough opportunity to do a reevaluation of CSC to ensure all the necessary components of the framework are included and have been informed through our response to COVID-19. There is also
enough evidence and experience at this point to provide recommendations on how to implement the framework. This is a great opportunity to advise others on how to use the framework and how to implement it in the most effective way while also ensuring that health care workers are well trained on indicators and triggers.
Certainly, COVID-19 took us by surprise, McKinney continued, but there were moments throughout the response, especially early on, when we could have anticipated much sooner some of those things that were going to affect our health care systems and ability to implement public health strategies. She amplified Veenema’s previous comments on nurses being a scarce resource and taking that into account more seriously in planning efforts. Another aspect that has been discussed for some time is the need for a toolkit or framework for elected officials. Clearly the scope and size of COVID-19 had officials much more involved than previous emergency responses, McKinney said, but there is now a great impetus for an elected official toolkit at this point.
There is an opportunity to develop a communications framework that integrates messaging at all levels of government so we are providing the most up-to-date and succinct information to the American public, she noted. She also supported the idea of creating a federal coordinating body, which could assist in developing this government communications framework but also could assist in implementing the framework should it become necessary. Finally, she was reminded of the pandemic influenza exercises at the national level that CDC used to conduct with specific jurisdictions to assist them in exercising their plans and measuring effectiveness. There are opportunities at this point to conduct multilevel government and jurisdictional exercises specifically around CSC plans to measure progress at the state and local levels and identify areas for improvement, she concluded.
Wynia highlighted some of the things that he used to worry about before the pandemic and that he now worries about differently. In the aftermath of earlier outbreaks such as SARS in 2003 and Ebola in 2015, he was concerned that politicians would overreact to infectious disease outbreaks and overuse public health police powers to stoke panic or needlessly overreach and be counterproductive. But now he worries about that differently, he explained. Politicians are not doing what they need to be doing right now during the COVID-19 pandemic. So, the role of the public health and medical enterprise in serving as a counterweight to political considerations is different than he anticipated it to be, he said. He stated he originally thought politicians would have to be held back, but instead some had to be pushed forward.
Secondly, he noted the large amount of work done on the “duty to treat” for health professionals and getting them to show up in the face of risk. Wynia stated that early in the pandemic that was not a problem, as
collegiality and volunteerism were at high levels. People did not even need legal protections—they showed up for dangerous and difficult work even when about to retire, he added. But now, Wynia explained, 18 months in, people are burning out and retiring. People can only be stretched so far until they break, he said. So, this conversation for him has changed to how do professionals in the field support frontline workers to maintain their resilience. He is also thinking more about how to encourage members of the public to ask themselves what are their duties as citizens? He believes it possible to have a national consensus on the ethical framework for CSC, as certain questions do get at core actions where there would be wide consensus. But there are numerous implementation challenges that would prove difficult.
Dan Hanfling, vice president, technical staff, In-Q-Tel, offered a few reflections from his experience with CSC over the past decade. He stated that never in a million years did he think that in the greatest health crisis of our time that he would see an erosion of trust in health care workers and public health authorities. He also never anticipated the level of political dysfunction that hampered the country’s ability to put in place what was required for a robust response. With that as context, Hanfling offered a few things about the framework and then suggested some steps to consider going forward, noting the framework was still relevant and aligned with CSC goals and parameters. He recognized that there is a duty to plan and prepare, as well as a duty to steward resources.
Past stakeholders who have worked on these issues over the years all knew that it was always a matter of when, not if, Hanfling said; they knew it was going to happen. He commented on the age of epidemics happening now, with SARS-CoV-2 being the third coronavirus outbreak in 17 years. There are going to be more crises like these, he cautioned. He elaborated on Wynia’s previous point, about engagement at all levels, and thinking about it more ethically, alongside a concept of reciprocity. Looking back on the ethical framework we focused mostly on accountability, Hanfling explained, motivated by the searing testimonials in the aftermath of Hurricane Katrina. There were strong feelings that the government should be accountable to its people at that time, but now it has become clear that people should also be accountable to their communities.
The lack of preparedness clearly relates to liability, he continued. Situational awareness became a critical element early in the process. Load balancing became the operative phrase to get the patients to the right place at the right time with the right resources, but without a national data infrastructure, this was a very difficult task. He called for prioritizing the development of something like that, as technology can be a force multiplier. There is an opportunity to deliver on capabilities like remote patient monitoring, telemedicine, and artificial intelligence, he said, and smarter ways
to deliver care, where just a few years ago these types of assets were only seen in the movies.
As a few final points, Hanfling shared that currently, such quantitative measures as SOFA scoring are unfulfilling, and there is a need to move away from that and identify better and more equitable measures. It also is important to recognize the need for clarity on indicators and triggers and being able to know when a crisis should be declared in terms of altering standards of care. Right now, this happens at the bedside, Hanfling said, but it is important to consider how to shift that decision to the left chronologically, and be able to prevent haphazard decisions from being made on an individual basis. Instead, through good situational awareness, hospital leaders should be able to declare a change of standards across the board prior to things falling apart. In summary, he offered four suggestions CSC work could focus on:
- There should be better and broader coordination and understanding between the bedside and board room. This is an “all of health care entity” requirement, and that divide needs to be bridged.
- Increase buy-in from the political sector. Politicians need to understand what is happening and be active participants in the process.
- Expand provider engagement, which has been an area of underinvestment previously but can be very valuable.
- Effectively address health equity issues. Whether it is COVID-19, masks, or structural racism, it is important as a nation to do better.
This page intentionally left blank.
















