
2
Organizational Capacity
Organizational capacity (OC) is the ability of an organization to perform work and ensure that its organizational resources are used effectively and efficiently to achieve its goals. In the context of governmental organizations, OC is a multidimensional concept that refers to the organization’s ability to marshal, develop, direct, and control its financial, human, physical, and information resources. OC captures the collective skills, abilities, knowledge, and experiences of an organization.
Various models for conceptualizing OC have been proposed, but almost all include four key features: infrastructure, finances, workforce, and culture (Cox et al., 2018). These four elements, which are evaluated in this chapter, represent the means and mechanisms through which the people and resources in an organization are brought together and utilized to accomplish its work, achieve its goals, and fulfill its mission. Like any organization, OC underpins and shapes the identity and personality of the Centers for Disease Control and Prevention’s (CDC’s) Division of Global Migration and Quarantine (DGMQ). Thus, as the key determinant of the DGMQ’s performance, OC is essential to understanding the organization’s effectiveness, its efficacy, and its ability to execute tactics and strategies aligned with its intentions and purpose.
The DGMQ’s infrastructure is central to its OC and is a key element in protecting public health as people become increasingly mobile within today’s globally interconnected world. Financial management involves the deployment of funds and other assets to achieve organizational goals. More specifically, it entails budget planning, acquiring funds, distribution, and allocation of resources. The domain of workforce and human resources includes per-
sonnel recruitment, retention, training, development, competencies, and performance. Finally, culture encompasses an organization’s values, norms, behaviors, and beliefs. Culture is integral to both individual and collective performance within an organization, as well as its ability to be adaptive and remain relevant. Although culture is difficult to measure, it often serves as the glue that holds an organization together (Cox et al., 2018).
Throughout the extraordinary work environment of the last decade, the DGMQ has continued to evolve in the face of complex challenges stemming from our global interconnectedness, the speed of travel and trade, and the integration of unprecedented societal changes, especially those resulting from the COVID-19 pandemic. Despite the advances made, the DGMQ faces significant challenges that undermine its ability to fulfill its mission. With core funding that has remained inadequate over the last decade, the division is limited in its ability to keep pace with a regular stream of public health emergencies. Persistent understaffing and burnout demonstrate the institutional challenges. The DGMQ must undergo significant changes with its finances, workforces, and culture in order to become a more agile and responsive structure. It must be successful in this formidable and disruptive setting, but achieving this will require absorbing, adapting, and being able to pivot quickly. The pillars of OC are foundational in helping the organization improve its work and performance. Without significant and rapid changes, the DGMQ’s capacity to lead the nation in preparedness and response is severely limited.
Much of the information in this chapter was provided by DGMQ representatives during open public committee meetings. Because detailed information about infrastructure, workforce, finances, and culture is not available from other publicly available sources, these presentations were invaluable in allowing the committee to assess the inner workings of the DGMQ and develop salient conclusions and recommendations. These four critical areas of OC reflect the evidence presented to the committee and, while critical, are not exhaustive. Other aspects of organizational capacity may warrant further exploration.
DGMQ INFRASTRUCTURE
The DGMQ works to maintain public health security by preventing the introduction, transmission, and spread of infectious diseases into the United States within a context of rapid global travel.1 The DGMQ is one of the nine offices and divisions housed within the National Center for Emerging and Zoonotic Infectious Diseases (NCEZID). The NCEZID collaborates with national and global partners to mitigate the impact of infectious
___________________
1 More information about the DGMQ’s work is available from the CDC (2016).
diseases (CDC, 2016). The DGMQ’s primary functions include screening, processing, and evaluating travelers—including immigrants and refugees—entering the country for any public health risks, and providing them with public health information. The DGMQ partners with airlines and cruise lines to identify sick travelers and alert other passengers of potential exposure. The division forwards information to local public health officials to enable individual follow-up and collaborates with these officials to prevent people with certain infectious diseases from traveling and exposing others. The DGMQ is also tasked with regulating the entry of animals, processing animal imports, and restricting animal products harmful to human health. Additionally, the division is responsible for emergency distribution of essential drugs and biologics, such as botulism antitoxin, under CDC investigational new drug (IND) protocols. In addition, the DGMQ periodically distributes investigational drugs of critical public health importance under IND when commercially available drugs are ineffective or have had supply disruptions, such as intravenous artesunate for severe malaria. Quarantine stations began stocking this drug when the CDC received U.S. Food and Drug Administration (FDA) approval to distribute it in 2007 for patients who failed treatment with intravenous quinidine (the only FDA-approved drug for severe malaria), then expanded distribution in 2019 after quinidine was no longer available in the United States (Rosenthal and Tan, 2019).2 This section provides an overview of the composition and function of the DGMQ’s infrastructure, with a particular focus on the Quarantine and Border Health Services Branch (QBHSB) and the network of quarantine stations operated by the DGMQ.
Quarantine Stations and International Field Offices
The United States receives nearly 1 million travelers per day across the nation’s land, air, and sea ports of entry (CDC, 2021d). To prevent the spread of contagious diseases into the United States, the CDC DGMQ operates 20 quarantine stations as of March 2022. Most stations are located within U.S. international airports with the highest volumes of arriving international travelers; two stations are located at U.S.–Mexico land-border crossings, which handle approximately 25 percent of daily legal land crossings. The QBHSB oversees the 18 airport-based quarantine stations, while the San Diego and El Paso land border stations fall under the purview of the United States–Mexico Health Unit. Each station has its own jurisdiction, which includes the various subports such as seaports, land-border crossings, and smaller airports within a geographic area. Collaborating with
___________________
2 This text was modified after release of the report to the study sponsor to provide additional clarity about DGMQ activities under the CDC’s investigational new drug protocols.
other federal agencies, such as Customs and Border Protection (CBP), the quarantine stations cover all (> 300) U.S. ports of entry.3
In addition to those 20 quarantine stations, the DGMQ currently operates three international field offices in Kenya, Mexico, and Thailand (Cetron, 2021).4 The offices in Kenya and Thailand primarily support activities undertaken by the Immigrant, Refugee, and Migrant Health Branch while the Mexico Office supports activities undertaken by the U.S.–Mexico Unit for populations moving back and forth across the U.S.–Mexico border or residing in the border region (Institute of Medicine, 2006).
Structures of Quarantine and Border Health Services Branch and the United States–Mexico Unit
Headquartered in Atlanta, the QBHSB is among the largest branches within the CDC in terms of its number of federal employees and contractors (Brown et al., 2021). As illustrated in Figure 2-1, the branch includes five teams that report directly to the U.S. QBHSB branch chief: (1) the Quarantine Travel Epidemiology Team (QuarTET); (2) the Epidemiology Field Team (eFIT), (3) the Zoonoses Team (ZTeam); (4) the Preparedness and Policy Coordination Team (PPCT); and (5) the Communication, Evaluation, and Training (ComET) Team. In addition to these teams, the QBHSB has a chief medical officer who oversees surveillance and clinical activities, and makes recommendations on overall detection and control strategy. The deputy branch chief supervises the Resource Support Services Team (RSST) and the Operations Team. Branch operations include managing the 18 quarantine stations, which are subdivided into four regions, each of which has a regional officer in charge. The chief medical officer and deputy branch chief report directly to the branch chief.
The QBHSB houses the principal activities related to quarantine station operations. QuarTET supports response to ill travelers. This includes managing implementation of federal public health travel restrictions (Do Not Board and Public Health Lookout).5 QuarTET also facilitates response to exposures to communicable diseases of public health concern during air and maritime travel and coordinates contact investigations with federal, state, tribal, local, and territorial (STLT), and international partners. QuarTET provides guidance, trainings, and standard operating procedures so that staff at quarantine stations can respond appropriately. The eFIT is
___________________
3 See https://www.cbp.gov/border-security/ports-entry#:~:text=Locate%20Port%20Information,of%20entry%20throughout%20the%20country (accessed May 20, 2022).
4 More information about CDC quarantine stations can be found at https://www.cdc.gov/quarantine/quarantine-stations-us.html (accessed February 26, 2022).
5 More information about federal public health travel restrictions is available from https://www.cdc.gov/quarantine/do-not-board-faq.html (accessed February 24, 2022).
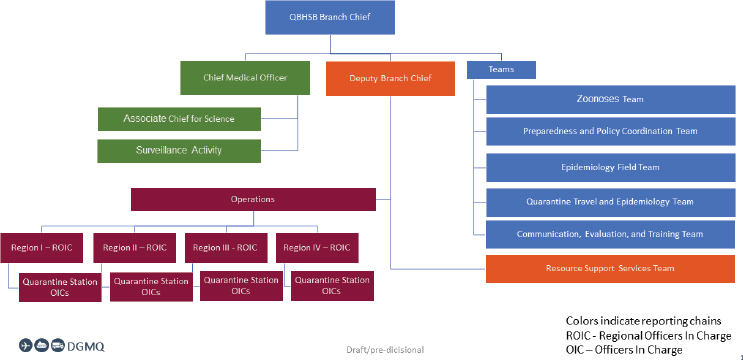
SOURCE: Brown et al., 2021, slide 8.
composed of a cadre of epidemiologists that carry out projects to advance the science and practice of travel and border public health. The ZTeam works to prevent the introduction and spread of diseases from imported live animals, animal products, or human remains by administering, and updating when needed, the CDC’s regulatory authorities and issuing guidance. Recent areas of focus for this team include canines, nonhuman primates, and mink (and mink products). The PPCT is responsible for preparedness planning for hazards and continuity of operations, emergency operations and response management, and preparedness training. The team also analyzes travel data, develops exercises, and facilitates and evaluates the development of After Action and Improvement Plans. Additional focus areas include quarantine station operations support and SharePoint site development and management. The ComET team works to train branch personnel and is responsible for communicating health information through various mechanisms, including posters, handouts, websites, and media responses. The RSST provides logistical support for operations at the quarantine stations.
The United States–Mexico Unit (U.S. MU) oversees the land ports of entry along the 2,000-mile U.S.–Mexico border. General protocols and training are derived from the QBHSB, but adapted for land border–specific environments. The permanent quarantine station staff and surge contractors located in San Diego and El Paso respond remotely to illnesses, exposures, and importations at all land ports of entry on the U.S.–Mexico border. Also housed within the U.S. MU is the Mexico Country Office, the Border Epidemiology Unit focused on strengthening U.S.–Mexico border state surveillance and response, and the Migrant/Communications team
with specific activities for mobile southern border populations. Together, the QBHSB and the U.S. MU manage the quarantine station network with support from the DGMQ’s Office of the Director.
Recent Responses to Disease Threats
The DGMQ is responsible for preventing the importation and spread of a number of disease threats. Daily quarantine station operations include restricting the importation of animals and animal products that may carry disease and containing the importation and spread of pathogens—such as rabies and monkeypox—from animals or vectors. The stations respond to ill travelers who arrive in the United States, along with addressing communicable disease case-patients (e.g., tuberculosis [TB], measles) or outbreaks (e.g., varicella, SARS-CoV-2).6 During outbreaks of infectious diseases of concern in other countries, the division works to protect travelers and contain the importation and spread of pathogens from specific locations or regions into the United States. For example, during the Ebola virus disease epidemic in Western Africa (2014–2016), the DGMQ recommended that Americans avoid nonessential travel to the three countries most affected by the epidemic. Working with airports and federal authorities, the division streamlined response efforts by diverting passengers from countries experiencing outbreaks to five U.S. airports. The division also trained U.S. Customs and Border Protection staff at airports to screen these passengers for symptoms of Ebola or possible exposures (CDC, 2021b). During the Zika virus disease outbreaks in the Americas (2015–2016), the DGMQ focused efforts on traveler education and outreach, especially for pregnant travelers and their partners. Outreach efforts included posted travel notices about preventing the spread of Zika, interactive maps, risk assessment tools, text messaging systems, and extensive airport messaging. Quarantine stations located in areas that were at greater risk of Zika spread, such as the U.S.–Mexico border and Puerto Rico, built partnerships with local governments and community health workers to alert travelers about Zika risk (CDC, 2021b).
Public health emergencies of international concern as declared by the World Health Organization (WHO)7—such as polio and the COVID-19 pandemic—fall under the DGMQ’s purview. In 2009, the CDC (including the DGMQ) collaborated with state and local health departments to stop the spread of the H1N1 influenza pandemic in the United States (CDC,
___________________
6 This paragraph was modified after release of the report to the study sponsor to correctly characterize some of DGMQ’s responsibilities. Similar corrections have been made throughout the report.
7 For more information on public health emergencies of international concern and the CDC, see: https://www.cdc.gov/nndss/about/ihr.html (accessed May 3, 2022).
2021b). In 2020, the CDC began its largest and most complex response to date in addressing the COVID-19 pandemic. The DGMQ’s efforts focused on protecting travelers and other mobile populations and reducing the risk of importing and spreading COVID-19 by way of global travel. Activities included
- taking regulatory actions, such as no-sail orders, quarantine measures for incoming international travelers, mask requirements on public transportation, and a rental eviction moratorium;
- establishing public health guidance for managing infected travelers and travelers potentially coming from countries deemed at greater risk due to high countrywide transmission levels;
- publishing travel guidance and health notices;
- establishing and conducting public health entry screening; and
- providing refugees, immigrants, and migrant workers with culturally and linguistically appropriate resources related to COVID-19.
Additional DGMQ efforts focus on controlling communicable disease outbreaks at immigration detention centers and repatriation locations. For example, the DGMQ issued quarantine orders for U.S. citizens repatriated from Wuhan, China, and cruise ships that were affected by initial outbreaks of COVID-19 in early 2020 (CDC, 2021b). This responsibility has also included responses to COVID-19 outbreaks at U.S. southern border locations. The division also addresses communicable diseases associated with mass migration emergencies, such as the displacement of Afghan refugees in 2021 and 2022 (Roohi, 2022). These actions complement those of the Department of Homeland Security, which establishes entry requirements for incoming travelers at U.S. ports of entry (Department of Homeland Security, 2022).
Infrastructure Challenges and Constraints
The responses to disease threats required thus far in the 21st century reflect the challenges the DGMQ faces in carrying out its mission. The division is involved in frontline activity in the majority of CDC disease threat responses, yet it lacks efficient mechanisms to quickly surge staff. Responsibilities have been increasing with each response, and the DGMQ is dependent on supplemental funding to carry these out, as discussed in the next section. The ability to urgently scale up health screening and data collection at U.S. airports in the immediate response to a newly emerging disease threat is limited, and challenges in gathering, analyzing, reporting, and validating data are at play. There are also challenges in ensuring effective coordination with STLT partners to manage both cases and exposed
passengers when they leave the airport or cruise ship. The division is considering how innovative approaches to data systems or analytical methods might be leveraged to mitigate these scale limitations (see Chapter 4). However, the scope of responsibilities for quarantine stations and the types of partners needed to meet them are broad. Furthermore, interoperability issues between agency and partner data systems pose challenges to unified public health efforts. The DGMQ is one of the few organizational components at the CDC with regulatory responsibilities, which places an added burden on the division and requires unique skill sets such as regulation writing and legal support. Managing movement restrictions of large groups of people—and using federal orders to do so—poses policy, operational, and legal challenges. Thus, the implementation of recommended measures may involve changes to regulations governing the CDC’s and DGMQ’s activities and authorities (see Chapter 6).
High Traveler Volume across Numerous Border Entries
International experts from South Korea, Hong Kong, Canada, Taiwan, Singapore, Australia, and the United Kingdom spoke to the committee regarding their countries’ procedures for screening, isolation, and quarantine of incoming passengers during the COVID-19 pandemic (see Chapter 3). Notable differences between the United States and other nations were apparent. A primary difference is that the volume of incoming passengers to other countries is much lower than the volume arriving in the United States. Moreover, many of the countries represented at the briefings (Taiwan, Australia, Canada) closed their borders to most incoming individuals when the COVID-19 pandemic began, whereas the United States primarily closed its borders to individuals traveling from specified high-risk regions (Hoffman and Poirier, 2022). The number of entry points is also much smaller in these other countries than in the United States and were further restricted during the COVID-19 pandemic. Whereas many countries had few points or only a single point of entry, the United States has approximately 320 land, air, and sea border entry points (Buigut and Maskery, 2021). Also, many of these presenters represented island nations, making access easier to restrict. Effectiveness of entry requirements and containment measures is highly dependent on context, making comparison between countries challenging.
In spite of the large number of U.S. points of entry, only 20 of them contain quarantine stations (CDC, 2021c), resulting in approximately 300 border entry points without any consistent public health service presence on site (CDC, 2021c). These border crossings may have a limited need for public health assistance and are staffed by other federal agencies. The 20 quarantine stations are strategically positioned at border entries with high concentrations of international travelers (See Chapter 1). Approximately 80
percent of all international arrivals enter the United States via an airport with an associated quarantine station (CDC, 2019a).8 However, public health threats can appear at any border entry point, so there is a need to expand the CDC presence to the other ports of entry (Walls, 2021). Therefore, solutions, including enhanced capacity for telehealth, are needed to assure adequate availability of public health services for personnel at all border crossings at all times.
Pandemic-Related Demand Increases
Other challenges relate to pandemic-related demand increases. In recent years, the DGMQ has been active in simultaneous responses, which can prove taxing for staff. For example, from 2020 to 2021, the division addressed Ebola virus disease outbreaks, concerns on the Southwest border due to the large number of persons arriving for immigration into the United States, the evacuation of Afghan refugees, and the COVID-19 pandemic. Screening processes established to address COVID-19 increased demands on the DGMQ. For instance, the number of individuals screened for COVID-19 across 15 designated U.S. airports rose from less than 1,000 on March 11, 2020, to nearly 30,000 by March 14, a mere 3 days later (Buigut and Maskery, 2021; Dollard et al., 2020).
The scale of demands posed by the COVID-19 pandemic is highlighted when comparing it with the Ebola epidemic of 2014 to 2016. The latter involved the screening of more than 38,000 travelers entering the United States in a span of 16 months (Cohen et al., 2016). In contrast, more than 760,000 travelers were screened for COVID-19 at U.S. airports in only 7 months (January–December 2020) (Dollard et al., 2020). Once Ebola data collection efforts began, the CDC was able to share contact data for all travelers with STLT public health agencies who were tasked with monitoring over 99 percent of them, post-arrival. In the first 7 months of the COVID-19 pandemic, contact data for 32 percent of screened travelers could not be shared due to data collection limitations. Many states opted out of receiving data due to the fact that STLT health officials were focused on addressing known COVID-19 cases and contacts rather than screening all travelers, most of which were at low risk of illness or exposure. The monitoring rate for travelers for COVID-19 after arrival is unknown.
The DGMQ is already among the largest and most complex divisions within the CDC and needs to grow. It has a unique set of responsibilities and is one of the few units at the CDC with direct regulatory responsibilities. It is also one of the few CDC components that operates field units,
___________________
8 This text was modified after release of the report to the study sponsor to correctly reflect the percentage and type of travel.
including those with international responsibilities. Other federal agencies, such as the U.S. Department of Agriculture (USDA), have successful overseas preclearance programs that increase work efficiency at U.S. ports. The DGMQ presently has overseas personnel stationed in Kenya, Thailand,9 and Mexico. However, today’s public health emergencies and refugee crises can emerge in almost any part of the world. Developing a more robust overseas presence could enable earlier and more effective response efforts. In addition, a pre-identified and cleared team of experts could be established, allowing them to be deployed when needed if there is an emerging threat from a specific region. While not specifically studied by the committee, there may be merit in redesigning the organization to include a more unified network of quarantine stations and functions.
Maritime Unit
The current structure of the maritime unit poses unique logistical challenges. Prior to the COVID-19 pandemic, two distinct CDC entities addressed maritime public health. The Maritime Activity, housed under the DGMQ, liaised with quarantine stations regarding communicable diseases of public health concern on maritime vessels, developed procedures for quarantine stations, and supervised management of outbreak response on vessels. The Vessel Sanitation Program (VSP), housed under the National Center for Environmental Health, managed cases of gastroenteritis on cruise ships. In April 2020, these entities merged to form a temporary Maritime Unit under the Global Migration Task Force. While the formation of the Maritime Unit has allowed for enhanced cooperation in responding to public health concerns on maritime vessels, challenges have emerged with the transition. As this merging was intended to be a temporary solution, the Maritime Unit is not permanently housed within any division (Tardivel, 2022). As gleaned from stakeholder presentations during committee meetings, there has been a perception among some stakeholders of a lack of communication between the Maritime Unit and the cruise industry, contributing to frustration regarding clarity in regulations and requirements from industry. Establishing a permanent base for the Maritime Unit could allow for improved communications, enhanced recruitment efforts, and greater effectiveness in achieving public health goals.10
___________________
9 Kenya and Thailand were selected as base locations for DGMQ’s Africa and Asia Field Programs (respectively), which oversee medical screening for immigrants and refugees traveling to the United States (see https://www.cdc.gov/ncezid/dgmq/focus-areas/irmh.html; accessed March 10, 2022).
10 See Chapter 3 for additional information on the Maritime Unit, including disease control strategies.
DGMQ’S FINANCIAL LANDSCAPE
Trends in the DGMQ Budget and Allocations (Fiscal Years 2012–2022)
The committee was briefed on trends in budgeting and allocations to the DGMQ and its quarantine stations over the past decade (Damon, 2022).
Baseline Funding
The DGMQ’s aggregated core budget lines—that is, its usual operating budget—supports its mission and programmatic activities. A substantial proportion of the DGMQ’s core funding also supports the salary and benefits for DGMQ permanent staff responsible for executing mission and programmatic activities (Cetron, 2021). The DGMQ’s baseline funding saw little to no increase over the past decade, despite substantial increases in the DGMQ’s responsibilities and the growth of international travel during that period (Cetron, 2021). Between fiscal year (FY) 2012 and FY2022, the DGMQ’s core funding has remained relatively static year over year, except for a small increase in FY2020’s core ceiling (Damon, 2022). Baseline funding has remained between $45–54 million per year, with an average increase each year of just 1 percent. The budgeting and allocation trend remained particularly flat for the salary and benefits for DGMQ permanent employees during that period.
Response Surge Funding
The DGMQ has received supplemental funds to support additional activities required during emergency responses. For instance, surge funding has been implemented during emergencies such as the COVID-19 pandemic. Emergencies that resulted in influxes of supplemental response-specific funding prior to the COVID-19 pandemic include the Ebola virus disease epidemic (Western Africa) (FY2014–FY2016) and the Zika virus disease epidemic in the Americas (FY2016–FY2017) (Damon, 2022). Thus, individual public health response supplemental funds have shaped the DGMQ’s budgetary trends over the past decade. Between FY2012 and FY2022, the DGMQ’s total budget fluctuation year over year has been strongly response driven, with a significant driver of the DGMQ’s current operating budget being its near-constant state of emergency response (see Figure 2-2). There is a need for an accessible central emergency fund that can be readily accessed in the event of emergencies to prevent delays in financing critical response elements (see Chapter 6). Surge funding has been a lifeline to the DGMQ and its ability to address emergencies. However,
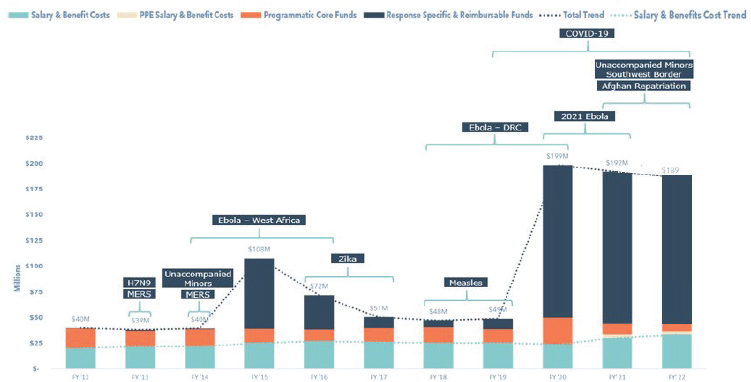
NOTE: The budget is largely response driven, with a notable increase for fiscal year 2020–2022.
SOURCE: Damon, 2022, slide 79.
whether funding will be allocated, the amount of funding, and its timing are uncertain in the early phases of the response. The funds often come late in a response and because surge funding is temporary, there are limitations in how it can be used; usually only temporary or contractual personnel can be brought on board and supported using these funds.
Added Responsibilities and Activities
Each new public health emergency brings additional responsibilities for the DGMQ, placing further strain on its infrastructure, finances, and workforce. To support this expanded work, the DGMQ allocates a larger percentage of its core operational funding to support salary and benefits. This requirement decreases the remaining funding within the core budget to conduct mission and programmatic activities. Although the salary and benefits proportion of core funding has increased year over year between FY2012 and FY2022, baseline funding has remained static (Damon, 2022). For FY2021 and FY2022, 2-year limited COVID-19 funding is being used to support the salary and benefits for 24 permanent positions provided to the DGMQ in the agency’s FY2021 Enterprise Hiring Plan. Once the limited COVID-19 funding ends, other funds will need to be used to support these full-time equivalents (FTEs).
With the COVID-19 pandemic response (FY2020–FY2022), the DGMQ has executed close to $200 million annually (discussed in further detail in the next section). The DGMQ projects that the long-term impacts
of the pandemic will include an expanded DGMQ work portfolio that includes regulatory actions taken to mitigate the burden of COVID-19. The result is a new permanent staffing requirement to support expanded regulatory and programmatic work and increased programmatic costs to sustain mission activities. In light of this, leadership within the DGMQ and the CDC supported a congressional appropriation request to increase the DGMQ core funding by $30 million (Damon, 2022). The FY2022 appropriation ultimately included an $8 million increase to the DGMQ’s core funding. However, this anticipated core funding increase in budget comes almost 3 years into the pandemic and remains a critical need that has not been addressed swiftly enough.
High-Level Overview of the DGMQ Budget: Fiscal Year 2021 and 2022
The committee was provided with a high-level overview of the DGMQ’s budget for FY2021 and FY2022, including funding streams in aggregate—reflecting both proposed and anticipated increases—as well as categories in which funding is spent, and program spending power at current core funding levels (Damon, 2022).
Funding Streams
The DGMQ’s two major funding streams include core funding and supplemental response allocations. The division received almost $192.1 million in total obligated funding in FY2021, with a reduction to $189.7 million proposed for FY2022. Core funding had nearly $45.1 million obligated in FY2021, with a 1.5 percent increase planned for FY2022, bringing the total core funding to about $45.8 million. The FY2022 President’s Budget request proposed $30 million increase to the DGMQ’s core budget will be critical to sustain its mission and programmatic activities. As previously described, significant DGMQ activities are funded through response supplemental funding lines. The DGMQ supplemental response allocations had about $146.4 million obligated in FY2021 and $143.3 million planned for FY2022. The CDC has proposed an $8 million increase in response allocations for FY2022 (Damon, 2022).
Spending Categories
Of the almost $192.1 million in total funding (including supplemental funds) obligated to the DGMQ in FY2021, virtually all of the funds went to three categories: contracts (61 percent), grants and cooperative agreements (21 percent), and salary and benefits (17 percent). For FY2022, there is a planned salary and benefits increase of 15 percent to support infrastruc-
ture priority positions. However, the DGMQ’s core funding increase is just 1.5 percent from FY2021 to FY2022, so the planned salary and benefits increase of 15 percent will require a decrease in the DGMQ’s mission and program spending from core funding.
DGMQ spending on grants, cooperative agreements, and contracts will remain fairly constant in FY2022 relative to FY2021. Grants and cooperative agreements may increase by $2.4 million (a 6 percent increase). However, grants and cooperative agreements are primarily supported through supplemental funding. They also reflect the DGMQ’s partnership engagements and collaborations to support public health interventions and improve the effectiveness of interventions. The spending on contracts will stay largely the same between FY2021 and FY2022, with a slight decrease in contracts of $9.4 million (8 percent decline) (Damon, 2022). This reflects the DGMQ operating infrastructure required to execute both mission and programmatic activities as well as response-related work.
Spending Power
DGMQ program spending power at current core funding levels is directly impacted by the need for increased staffing to sustain its mission and programmatic activities. In FY2021, 65 percent of the core funding ceiling ($45.1 million) was spent on salary and benefits, leaving 35 percent of that funding to cover all operational and programmatic costs, including mission and regulatory activities. Based on the planned core funding ceiling for FY2022 ($45.8 million) and given the planned increase to salary and benefits, about 74 percent of funding will be spent on salary and benefits, leaving just 26 percent to sustain operational, mission, and regulatory activities.
Hypothetical Financing Scenarios for Fiscal 2023
The committee heard two hypothetical financing scenarios for FY2023. If the DGMQ’s needs are not prioritized financially, the staffing footprint required to facilitate its preparedness for public health emergencies and to fill all authorized positions would leave no funds remaining for program and mission work.
Specifically, for FY2023, core funding projected at current levels will be about $46.4 million—all of which will need to be spent on salary and benefits, leaving no core funding for programmatic, mission, and regulatory efforts and nonpersonnel operational costs. If the proposed $30 million FY2022 increase to core funding is realized, however, the core ceiling will increase to about $76 million. This will enable 67 percent of core funding to cover salary and benefits, with 33 percent for programmatic, mission,
and regulatory work. Although the anticipated increase to its core funding would allow the DGMQ to hire to its approved staffing level, it would merely be able to sustain—but not grow—its programmatic and mission work.
These two hypothetical scenarios are untenable. Therefore, it is clear that the DGMQ requires additional funding. A permanent income stream beyond congressional funding could be one means of achieving this. Baseline core funding has been flat for years and has left permanent staffing underfilled. The reliance on surge funding in crises is unsustainable for meeting consistent staffing requirements. The establishment of a “no year” emergency response fund, with sufficient funds to cover crisis activities and increased surge staff needs, would obviate the wait for annual congressional appropriations and supplemental appropriations in crisis situations.
Potential Funding Streams
Currently, the DGMQ does not have sufficient core funding to support its personnel and programs. Increased core funding is needed to sustain programmatic activities so the organization does not have to rely solely on emergency funding that is only made available at some point after the start of an emergency (see Chapter 6). The DGMQ could explore sources of funding in addition to the standard congressional appropriation to support its core personnel and activities. For instance, the DGMQ could explore whether user fees—from industries that receive direct benefit from DGMQ activities and regulatory oversight such as the maritime and aviation industry—could provide a sustainable source of funding. The CDC’s VSP, in which cruise industries pay user fees to have their vessels inspected, sets precedent for this arrangement (CDC, 2019b). User fee charges could be tied to objective criteria such as the number of passengers per year. A caveat is the potential for a conflict of interest on the part of the DGMQ, as it would be paid by the industries being regulated. Although this practice is somewhat controversial, other federal agencies have successfully implemented similar strategies (FDA, 2022). The division is in need of other more reliable funding streams besides its traditional appropriations and surge funding. The committee is aware that there may be barriers to establishing user fee authority; however, in other agencies, user fee programs have been transformative in improving staffing and program performance. Since the DGMQ performs an array of critical, direct services at the border that support regulated industries and the public, there is an adequate basis for such a funding mechanism. There is also a need for better human resources (HR), thereby allowing for more nimble hiring of personnel to fulfill surge needs. Current staff are now absorbing the workload of the vacant unfilled positions, contributing to substantial levels of burnout.
WORKFORCE
Over the past decade, the DGMQ has been operating in emergency response mode more often than not. Therefore, operating in response mode has become the de facto normal operational state and tempo, not be viewed as unusual or the exception. However, both its number of FTE employees and its level of core funding have remained nearly unchanging despite the escalating size of the DGMQ’s suite of responsibilities. Currently, surge responses to emergencies are being managed as individual, time-limited occurrences. They are supported by temporary funding and large numbers of temporary personnel and staff. This short-term solution does not effectively address the division’s long-term needs. It is imperative that the DGMQ, including its quarantine stations, be appropriately staffed to fulfill its mission and execute its responsibilities.
Trends in DGMQ Staffing Requirements and Levels
Within the DGMQ, the number of permanent, FTE employees has remained static for years (Damon, 2022). However, between FY2019 and FY2022, the response to the COVID-19 pandemic has generated a substantial increase in staffing needs. To meet these needs, the DGMQ has used term-limited federal appointees (TERM NTE), training program appointments, and contractors. Note that all federally appointed employees worked full time and that TERM NTE only indicates the distinction between term-limited and permanent employees. To meet mission and regulatory requirements, this increase in staffing has involved slow upscaling through resource-intensive recruitment and hiring, as well as the use of contract mechanisms (Figure 2-3).
Evaluation of DGMQ Staffing Composition: 2019–2022
The committee was provided with a high-level overview of the evolution of the DGMQ’s total staffing composition—including both permanent and nonpermanent staff types—between FY2015 and FY2022 (Damon, 2022). Nonpermanent staff types include malaria-funded TERM NTE positions (hired prior to the COVID-19 response for expanded distribution of intravenous artesunate under the CDC’s investigational new drug protocol), COVID-19–funded TERM NTE positions, contractors, fellows, students, and guest researchers. Authorized permanent staffing levels11 remained relatively static from FY2015 to FY2019, maintaining approximately 180 FTE
___________________
11 The authorized permanent staffing level does not represent an occupancy rate. Although authorized, not all permanent positions were filled during these fiscal years.
positions. By FY2019, the number of approved positions in the DGMQ increased to 223 FTE positions, however, the DGMQ did not have the core funding to fill and maintain this permanent staffing footprint. Thus, the DGMQ has compensated with an enhanced footprint of TERM NTEs, contractors, fellows, and other nonpermanent employee types.
Between FY2019 and FY2022, there was a marked escalation in overall staffing resources. In FY2022, the number of approved FTE staff positions in the DGMQ increased to 331 (Damon, 2022). This was catalyzed by (1) multiple ongoing responses, (2) expanding regulatory requirements, and (3) increasing mission activities inclusive of response efforts. With a continued lack of core funding, the DGMQ has continued with an enhanced nonpermanent staffing footprint.
The escalation in overall staffing from FY2019 to FY2022 was also driven by increases in temporary staffing to support the response to the COVID-19 pandemic. During that period, the number of authorized TERM NTE positions increased almost seven-fold, from 17 to 115. During the same period, the staffing ceiling for contractors and fellows spiked 32-fold from 24 to 770 positions. By FY2022, the DGMQ had an unprecedented number of positions for TERM NTEs, contractors, fellows, and other employee types. Thus, the overall volume of temporary staffing dwarfed the volume of permanent staffing by roughly four-fold in FY2022. Positions held by TERM NTEs, contractors, and fellows have increased from 41 in 2019 to 885 in 2022 to support the DGMQ’s response, mission, and program requirements (Damon, 2022).
For over a decade, the DGMQ has had a chronic deficit in baseline funds (see previous section). This deficit has not permitted the division to keep pace with its growing responsibilities and work effectively in an era of unprecedented infectious disease emergencies. The DGMQ’s non-emergency workload has concurrently grown due to significant increases in international travel and trade, migration, and population relocations. The division is in the unenviable position of determining whether to use funds to support personnel or programmatic activities, as there is not enough funding to do both. The DGMQ has received additional FTEs. But if they use their funds to support these FTEs, there will be no remaining funds to support program activities. This is analogous to a “fool’s choice” as both are imperative to fulfill their mission.
Current DGMQ Staffing, Occupancy, and Turnover Rates
The division has more than 1,100 permanent and nonpermanent positions currently staffed, although this number is consistently in flux. Nonpermanent staff currently comprise a significant proportion (77 percent) of the total staff.
Occupancy and turnover rates among DGMQ staff remain major ongoing concerns. In FY2019, the DGMQ’s average occupancy rate for FTE positions was about 82 percent, which declined to 77 percent in FY2022 (Damon, 2022). The volume of staff leaving DGMQ has also increased sharply in recent years. In FY2021, the DGMQ saw significant turnover of 44 FTE staff lost; although they were able to maintain staffing at a level near that of 2020 by bringing on 44 new staff, there was no net gain (Damon, 2022). From 2019 to 2021, there was an increase in the turnover of employees leaving the DGMQ by approximately two-fold (Damon, 2022). Most departures were among staff in the general schedule (GS)-9 and GS-11 (mid-level) categories, with a noticeable shift toward those staff leaving the agency entirely rather than staying within the CDC. The committee did not explore staffing trends across the CDC but, if similar, the CDC may benefit from an agencywide approach to rebuilding the workforce.
Quarantine and Border Health Services Branch Staffing Levels
Based on FY2022 staffing levels, the QBHSB is the fourth-largest branch at the CDC in terms of the number of federal staff—including FTE and TERM NTE staff—and the second-largest branch at the CDC if contractors are included (Brown et al., 2021). Figure 2-3 illustrates the overall trends in total staffing for QBHSB between 2008 and 2022, including both authorized and filled positions for FTE staff, TERM NTE staff, contractors, students, training programs, and deployers (the CDC and the Department of Health and Human Services [HHS] staff that are deployed to assist in the DGMQ work). Spikes in the numbers of nonpermanent staff—particularly contractors—correlate directly with major response efforts, including the influenza A (H1N1) pandemic (2009), the Ebola virus disease epidemic in West Africa (2014–2016), the Zika virus disease epidemic (2015–2016), the expansion of distribution of the intraveinous artesunate for severe malaria (2019), and the COVID-19 pandemic (2019–2022).
As of November 2021, there are currently 252 approved positions within the DGMQ’s QBHSB, including 108 approved FTE positions and 144 TERM NTE positions (Brown et al., 2021). The overall vacancy rate for both FTE and TERM NTE staff is about 42 percent (November 2021), with 146 of 252 total approved positions filled (Brown et al., 2021). The vacancy rates are widely variable (0–60 percent) across the five in-house teams that report directly to the QBHSB branch chief: ZTeam, 60 percent vacancy rate (4/10 approved positions filled); QuarTET, 50 percent (17/34); PPCT, 30 percent (7/10); eFiT, 29 percent (5/7); ComET, 0 percent (7/7). Additionally, nearly half of the QBHSB Operations Team (the quarantine stations) positions are currently vacant (86/160), but almost all of the ap-
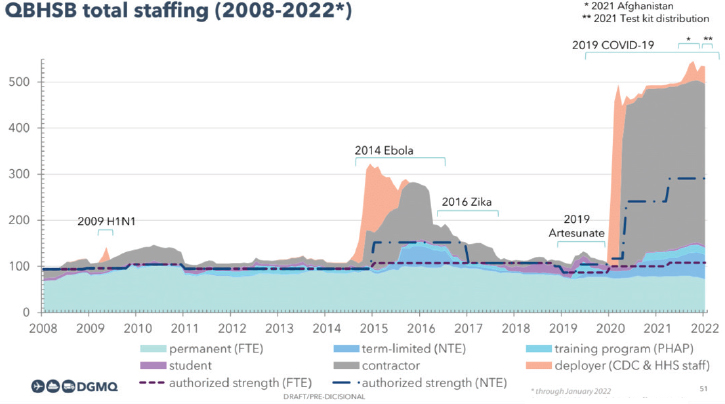
NOTES: CDC = Centers for Disease Control and Prevention; FTE = full-time equivalent (permanent staff); HHS = Department of Health and Human Services; NTE = temporary federal appointees; PHAP = Public Health Associate Program.
SOURCE: Alvarado-Ramy, 2022, slide 51; based on data from QBHSB consolidated staffing records.
proved positions at QBHSB Headquarters are filled (10/11) and most of the Resource Support Services Team positions are filled (10/13).
Quarantine Station Staffing Levels
As of March 2022, the DGMQ operates 20 designated quarantine stations (18 airports and 2 land border crossings) (CDC, 2022). As conveyed by discussions with DGMQ representatives during committee meetings, the number of positions at each of the quarantine stations is determined by multiple factors: (1) volume of arriving international travelers, immigrants, and refugees; (2) cargo volume (especially for primate, canine, and other CDC-regulated importations); (3) geographic coverage and risk factors specific to the jurisdiction of quarantine station (including the number and types of ports of entry within the jurisdiction and number of arrivals from high-risk geographic areas); (4) number of responses occurring at a given time; and (5) the availability of cross-station coverage for surges in operations (CDC, 2021a).
Among the 18 quarantine stations located at international airports in the network, there are currently 160 approved positions—the majority of which are TERM NTE positions. The number of total approved positions at each quarantine station varies widely, from 4 each at the Anchorage and
Philadelphia stations, to 16 at the New York station located in John F. Kennedy airport (Brown et al., 2021). Overall, only 86 (54 percent) of these approved positions were occupied as of November 2021, representing a total vacancy rate of 46 percent (Brown et al., 2021). The vacancies are most glaring for the TERM NTE appointments, of which just 41 of 104 positions (39 percent) are occupied, versus 45 of 56 (80 percent) FTE positions.
Like the number of positions, the vacancy rates vary widely across the network of quarantine stations, from 25 to 75 percent as of November 2021 (Brown et al., 2021). Vacancy rates at some of the larger stations are noteworthy: San Francisco Quarantine Station (67 percent), Atlanta Quarantine Station (60 percent), Los Angeles Quarantine Station (40 percent), and New York Quarantine Station (44 percent). The lowest vacancy rates are at the Philadelphia Quarantine Station (25 percent), Chicago Quarantine Station (31 percent), and Washington, DC Quarantine Station (33 percent). The current staff per station currently ranges between 1 and 9 individuals, which contrasts sharply with the range in the number of approved positions across the stations (4–16 positions).
Workforce Challenges
The DGMQ’s primary workforce-related challenges include lack of sufficient funding to support adequate staffing, understaffing of permanent and temporary positions, and high rates of vacancy and turnover.
Funding Challenges
As previously described, the DGMQ received a substantial increase to its permanent staffing footprint in FY2022. Unfortunately, the division has not received a commensurate increase to its core funding to sustain the expansion to the staffing ceiling and maintain program activities. Thus, the increase in the DGMQ’s permanent staffing ceiling represents a driver for the decreased spend power of the DGMQ’s core budget. Moreover, the regular budget process has not provided a sufficiently sustainable source of funding for permanent staff. Instead, there have been periodic infusions of emergency funding which cannot be used to support long-term, permanent staff (see Figure 2-2).
The committee was provided with a breakdown of how authorized staffing ceilings within the DGMQ were funded in FY2019 versus FY2022 (Damon, 2022). During FY2019 all 223 authorized FTE positions were supported by core funding. In FY2022, the same number of FTE positions were also funded by the core, despite the authorization of an additional 108 permanent positions. Of those additional positions, 91 have a response supplemental temporary source of funding to support the position through the end of that fiscal year, while 17 do not have an identified source of
funding.12 In FY2019, all 17 TERM NTE positions were supported by core funding; in FY2022, all 115 temporary positions were supported by supplemental response funding. The 24 positions for contractors and fellows were entirely core funded in FY2019. In FY2022, 735 of the 770 positions for contractors and fellows were funded by response supplemental funding lines, while 35 were supported by core funding.
Challenges in Recruiting and Retaining Permanent Staff
The DGMQ currently relies heavily on TERM NTE staff, contractors, and fellows—as opposed to permanent staff—in order to execute its responsibilities, but this is inadequate and inefficient for operating with and sustaining long-term effectiveness. Required competencies, including skill sets and qualifications, within these nonpermanent categories of personnel may be limited or not appropriately aligned to the position or job requirements they are expected to perform. In addition, term positions are established using emergency funds, which means the positions are dissolved once the emergency is over unless alternative funding and positions are identified. This is not a sustainable model for a functional organization. This manner of staffing in the DGMQ not only affects the division’s efficiency and functionality but can also undermine employee morale. An additional inefficiency of temporary personnel is high turnover, resulting in the loss of acquired organizational knowledge. Temporary personnel and contractors may also not be as committed to the culture and success of the organization as permanent personnel would likely be. Thus, understaffing of permanent positions is a major concern for the DGMQ. While TERM NTE staff are important for filling the current gaps resulting from high turnover of FTE employees, the long-term stability and effectiveness of the DGMQ requires a steady FTE workforce.
There are likely multiple reasons for the dramatic split between permanent and nonpermanent staff. In addition to the funding issues described in the previous section, representatives of the DGMQ reported a range of challenges associated with recruiting and retaining permanent staff, including greater demands and consequent strain on human resource time (e.g., onboarding, badging, medical clearances) (Damon, 2022). The work required for contracting—including maintaining contracts and the administrative hurdles involved in filling other types of positions—is significant and time consuming. Furthermore, the training requirements and requisite oversight given to nonpermanent, temporary employees can cause inefficiency and increased demands on individual entities or the entire division. These requirements are incredibly challenging during emergency responses.
___________________
12 Few of those unfunded positions are critical to the DGMQ sustainable infrastructure support for program and mission funds, so the DGMQ will align core programming dollars to funding these staffing needs.
Response Surge Staffing Challenges
Over the years, a continuing challenge for the DGMQ has been the need to staff surge responses with the right number of personnel, with the appropriate skill sets, in a timely manner. This challenge is underpinned by a host of issues (Roohi, 2022). For example, quickly hiring and onboarding new staff is difficult due to human resource constraints and challenging federal hiring procedures. During larger responses in particular—for example, emergencies such as the COVID-19 pandemic—there are competing staff needs of other CDC response components and task forces. Similar issues relate to non-CDC personnel—for example, Public Health Service surge staffing requires mission prioritization and approval from the U.S. Public Health Service Headquarters, given the substantial needs that also exist in other agencies.
When surge staff are identified, additional issues relate to the provision of national security clearance and badging requirements for physical access to restricted areas at U.S. ports, further impeding the speed of response capacity. Moreover, there are potential delays related to onboarding and administrative processes for arranging travel and medical clearance prior to domestic and international deployments. Skill set issues and training resource requirements can pose further barriers, especially when response needs are time sensitive. In the current and previous responses, the DGMQ onboarded a small number of CDC retirees on a temporary basis; however, this is not a sustainable solution due to the length of time involved in this process and the relatively small number of interested retirees. The DGMQ has also attempted to utilize nonfederal volunteer surge staff, but this gave rise to similar issues around security and medical clearance requirements, badging requirements, and access to IT systems.
Quarantine Station Staffing Challenges
Staffing of quarantine stations is also associated with a specific set of challenges. For instance, many tasks performed by quarantine station staff are largely administrative and do not require technical skills (such as medical training), while others—such as evaluating passengers for quarantinable diseases—require medical skills. In the past, the quarantine stations were staffed by well-trained public health administrators (i.e., quarantine officers). In recent years, however, the DGMQ has prioritized staffing quarantine stations with medical officers to facilitate screening needs. There may be opportunities to accomplish these screening needs by implementing technological solutions such as telemedicine (see Chapter 4) that could both reduce the workload on overburdened staff and minimize the need for positions requiring certain skill sets that may be more difficult to fill. In addition, medical
professionals such as emergency medical technicians or nurse practitioners could be available on-site with doctors available remotely as needed.
Other challenges pertain to the operational hours and shift work at quarantine stations. Presently, many quarantine stations operate in a single daytime shift (i.e., 9:00 AM–5:00 PM) with varying degrees of after-hours coverage and on-call response. Based on experience during the response to the COVID-19 pandemic and other recent emergencies, a single shift does not adequately meet the necessary operational needs that are demanded. The arrival of passengers, cargo, and animals through designated U.S. ports of entry can occur at any time during a 24-hour day. This often requires staff members to work extended hours, to conduct public health consults remotely from home, or to return to the station during designated nonworking periods. This consistent occurrence during continuous high operational tempo inevitably leads to decreased morale, employee burnout, and increased turnover rates.
The Need for Competent Employees
The skills that workers need can change over the course of a few years (World Economic Forum, 2016). This is especially true for the DGMQ that operates in complex networks and relationships, needs significant technological advances and digital talent, works in a globally interconnected structure, and works as a regulator in the midst of the larger CDC that is almost entirely nonregulatory. Organizations in today’s rapidly changing and complex environment need to “upskill” their workforce. Upskilling is a professional development strategy to augment the knowledge, skills, and competencies that help employees advance their careers and become more productive. It is a key tool to recruit, retain, and develop workers for organizational growth (Vroman and Danko, 2022). Some of the key skills recommended include collaboration, communication, creativity, critical thinking, cultural sensitivity, adaptation, transdisciplinary abilities, and ability to work across professions and organizations (Davies et al., 2011). Hiring and developing employees with pertinent skills is a key part of planning for its future workforce.
Challenges Related to Vacancy and Turnover Rates
As described, high vacancy and turnover rates across DGMQ staffing pose substantial challenges. Among the many reasons for vacancies and turnover are burnout, lack of adequate staff, and consequent overburdening of existing staff, especially increased overtime demands. Notably, early-mid career personnel—for example, GS-9 and GS-11 categories—tend to leave their positions at the DGMQ more frequently, which represents a loss of
future leaders in the pipeline. Not only are many leaving the DGMQ, but they are increasingly leaving the CDC altogether—a significant challenge to be addressed, due to its consequences for both existing bench strength and the potential future of the DGMQ public health workforce.
The DGMQ staff have worked huge amounts of overtime hours to meet the needs and demands of recent major response efforts, which raises concerns of staff burnout and the DGMQ’s ability to maintain mission-critical or regulatory work. Between 2019 and 2020, there was a drastic increase in the number of overtime hours worked, of 2,428 percent, which was aligned with COVID-19 spikes (Damon, 2022).13 An initial very high peak of overtime work occurred in January 2020, reflecting the efforts to establish entry screening and support repatriation quarantine and isolation. Another peak occurred in July 2020. During this time, other staffing sources (e.g., U.S. Public Health Service Commissioned Corps Headquarters deployments) supported the DGMQ response, along with the CDC Emergency Operations Center (EOC) responders and deployers. An interagency agreement with the Department of Homeland Security Countering Weapons of Mass Destruction Office (CWMD) was also established to support screening, and other contract mechanisms were established for surge staffing. Although the steep increase in overtime hours worked moderated compared to the beginning of the pandemic, the number still remained higher than the baseline. Throughout late 2020 and into 2021, smaller peaks in overtime hours occurred with each successive wave of COVID-19 due to emerging variants of interest or concern in the United States.
At quarantine stations in particular, high turnover and vacancies made it difficult to conduct outbreak responses (Council of State and Territorial Epidemiologists, 2021). Overtime hours have seen an especially significant increase among more experienced workers—that is, those with higher GS levels (Damon, 2022).
The quarantine station network plays a critical role in the frontline protection of our borders from the introduction of communicable diseases. Excessive vacancies within the quarantine station network and the inability to retain skilled and experienced staff jeopardize the ability of the DGMQ to accomplish its core mission of protecting the United States from the introduction of communicable diseases. Thus, the appropriate staffing of authorized positions within the individual quarantine stations is a critical necessity that needs to remain a priority for the DGMQ.
___________________
13 A caveat is that this percentage does not represent the additional efforts of certain staff types that are compensated differently (e.g., not eligible for overtime).
Potential Solutions to Workforce Challenges
The committee identified a range of potential solutions to the DGMQ’s workforce challenges previously outlined. These include developing strategies to ensure adequate staffing, implementing changes to quarantine station operations, leveraging technology and telemedicine, and providing training opportunities. Among the primary needs is a standing “reserve force” of personnel that are able to be deployed at the outset of an emergency. In order to be ready when needed, this force would need to be in place before the emergency begins. Personnel need to be recruited, vetted by HR, and have received all necessary credentials so that the force is in place before an emergency occurs, saving precious time and effort in the response. Such a reserve corps would need to be composed of individuals that have critically needed skill sets to meet DGMQ emergency operational needs and who could immediately fill unoccupied temporary positions. These positions could be filled by federal employees, including from the CDC, or other contracted staff that are prepared to be deployed as soon as the need arises. The armed forces or HHS National Health Service Corps might serve as a model for innovative recruitment strategies; they support tuition and provide stipends for students in exchange for a commitment to serve for a specified period of time.
Developing Strategies to Ensure Adequate Staffing
- The DGMQ can explore a range of options to ensure adequate staffing, including the following: Explore the CRMD CDC PHI fellowship program14 and the Public Health Associate Program15 as a means of recruiting.
- Partner with local jurisdictions to hire or assign staff to work in the quarantine stations.
- Develop MOUs (Memoranda of Understanding) with other HHS agencies or the Public Health Service (PHS) to assign or detail their personnel to the quarantine stations.
- Develop MOUs with other federal agencies (e.g., Department of Homeland Security, Department of Transportation, Department of Defense) to assign or designate their personnel to work in the quarantine stations. The MOUs should better delineate the roles and responsibilities of the DGMQ versus its agency partners.
- Establish division-specific HR services to address challenges related
___________________
14 More information on the CDC PHI fellowship program can be found at: https://phi-cdcfellows.org (accessed March 15, 2022).
15 More information on the Public Health Associate Program can be found at: https://www.cdc.gov/phap/index.html (accessed March 15, 2022).
- to routine HR processes to expedite training and clearance to onboard surges of staff.
Implementing Changes to Quarantine Station Operations
The DGMQ leadership has expressed the division’s willingness to establish a goal that enables all quarantine stations to remain operational daily, utilizing two personnel shifts to provide 24-hour coverage. This change appears necessary and an appropriate common standard to implement across the network based on recent response requirements. However, the current high number of vacancies, which varies between quarantine stations, and the high number of TERM NTE positions will make this standard challenging—if not impossible—to meet for the entire network. Furthermore, if required, this will create more significant challenges to meet the demand of adding additional quarantine stations to the network.
A comprehensive plan needs to be developed to allocate the appropriate number of personnel required to fully operate two personnel shifts daily at each quarantine station and to conduct 24-hour operations during surges to DGMQ response requirements. This plan will need to focus on developing an increased number of permanent positions over the heavily reliant temporary positions; it should also include a thorough evaluation of the requirements to determine the requisite number of positions, competencies, job series, and grades needed at each station. Additionally, such a plan could also consider the use of available technologies that could reduce or eliminate some of the staff tasks and requirements currently being performed and minimize the need for extended hours and extra shifts. The development of a model prototype quarantine station could be beneficial. The design of a new maritime station—and perhaps additional air and/or land stations—could integrate personnel changes resulting from technology advances and collaboration with other federal organizations. Once new operating procedures and methods have been refined, the model could be scaled and used in other stations.
Leveraging Technology and Telemedicine
The DGMQ has an opportunity to also explore opportunities to leverage technology and telemedicine to alleviate the burden of responsibilities on its staff or potentially obviate the need for onsite medical officers. The COVID-19 pandemic has demonstrated the viability and value of telemedicine and digital support tools in preserving health care resources during an emergency response (Shen et al., 2021). For example, Mayo Clinic—the largest U.S. health care system—reported a 78 percent decrease in in-person health care visits from mid-March to mid-April 2020 and a 10,880 percent
increase in video appointments during that same time frame (Marin, 2020). Now established in many countries, telemedicine platforms enable direct interactions between health care providers conducting consultations and their patients for health care visits. Moreover, teletechnology is available that can remotely collect data—such as blood pressure, heart rate, body temperature, recordings of the heart and lungs, and imaging of the ears, mouth, and skin—and transmit it to the health care provider in real time.
In briefings to the committee, quarantine authorities from other countries presented information about the implementation of various digital tools. These include electronic vaccination information and burner phones used to inform incoming passengers of public health risks and requirements. These tools offer benefits such as facilitating follow-up activities, avoiding issues associated with distribution of information in paper-based formats, and eliminating the need to manually enter information.16 In planning to integrate telemedicine and digital technology, the DGMQ could consider
- contracting or utilizing a local private medical consultant or group;
- staffing a quarantine station with other medical professionals (e.g., nurses, physician assistants, nurse practitioners) with telemedicine backup within the DGMQ or elsewhere at the CDC;
- establishing a telemedicine agreement with a local clinic, hospital, or academic medical center; and
- establishing a telemedicine agreement with a national telemedicine service.
Providing Training Opportunities
To enhance workforce development opportunities for its staff and improve staff retention, strategies could be implemented to support training and education, as well as promoting staff wellness (Benenson, 2007). Once the staffing plan has been developed and appropriate skills and competencies have been identified, training and experiential learning needs can be determined for each job series.
The DGMQ already offers robust internal training opportunities for its staff that could be enhanced and expanded (Damon, 2022). For example, the DGMQ offers an internal Training and Transformational Leadership Upskilling Series, where it works to bring topics of broad interest into the division training series and strategizes to offer these opportunities to personnel at strategic times to increase attendance. The 2021 DGMQ Training Series was implemented to “(1) provide staff with requested trainings on priority topics, (2) offer opportunities and resources for DGMQ staff to add
___________________
16 For further information on digital tools and technology in DGMQ, see Chapter 4.
knowledge and develop new skills for improving resiliency and institutional processes, and (3) create a more sustainable preparedness and response workforce infrastructure to address DGMQ’s evolving needs in global migration and quarantine” (Damon, 2022). In 2021, the DGMQ Training Series had almost 1,000 attendees. The DGMQ’s 2021 Transformational Leadership Upskilling Workshop—which had almost 500 attendees—was designed to develop future leaders and to invest in promoting leadership skills at all levels (Damon, 2022). It also contributes to building the DGMQ’s public health workforce pipeline. Transformational leadership theory is used as a foundation to help staff become dynamic team members and leaders.
The CDC has developed a series of training programs aimed at advancing employee careers, reimaging organizational goals, and fostering employee well-being. CDC University, an internal training program, provides courses and pathways for enhanced competencies within an employee’s job series or discipline. Courses are offered both in-person and virtually. CDC University’s Compassion Institute was established with the goal of promoting compassion as a key component of its programs and activities in order to advance societal well-being through the organization. The DGMQ helped create and pilot CDC University’s “Caring from the Inside Out” Training Initiative, which focuses on employee well-being, including sessions on mitigating stress and burnout and practicing self-care. Trained facilitators guide these 6-week sessions to provide participants with resources to improve work and home life (Damon, 2022).
In addition to the professional development trainings previously listed, the QBHSB provides robust routine and response-specific training to its staff. Upon joining the branch, staff received training plans with 20–40 operational courses tailored to their specific role. Courses usually have quizzes that must be completed to finish the course, and most courses must be repeated every 1–2 years to ensure staff are refreshed on content. The branch also creates partner training materials for station staff to use during their onsite trainings of port and public health partners. The branch also created and maintains a robust train-the-trainer program for CBP staff at the Federal Law Enforcement Training Center (FLETC) in Glynco, GA—where new CBP officers receive their basic training, including training in supporting CDC quarantine station operations. Through training a cadre of 10–20 FLETC trainers to deliver the CDC module 60+ times a year, the DGMQ empowers the CBP to partner in training and saves a significant amount of staff time and resources in traveling to the FLETC to deliver training. The CDC also augments CBP training at ports of entry (POE) through developing and delivering just-in-time trainings as needed on response operations (e.g., COVID-19 testing and vaccination requirements before boarding, COVID-19 public health risk assessments, etc.).
In addition to in-house training activities, the DGMQ could partner
with academic institutions—including schools of public health and administration—to supplement and expand training activities. Partnering with schools of public health and administration could help to develop a pipeline of well-trained students that could fill positions within the division, including at the quarantine stations. Participation could be encouraged by providing potential incentives for graduates to work at the CDC, including loan repayment programs or scholarships. Students could also undertake experiential training while in school as interns or in other roles.
CULTURE
An organization’s culture is defined by its system of collective beliefs, values, norms, behaviors, and artefacts (Cox et al., 2018). Culture represents an organization’s “DNA” and helps to determine its actions and relationships. It is interwoven into the DGMQ’s staffing issues and chronic underresourcing. Without an in-depth culture audit, the committee was limited in assessing this dimension of the DGMQ. However, there are a number of challenges that may be contributing to a culture at the DGMQ that limits its organizational capacity. These include structural constraints (e.g., inadequate financial and human resources), chronic vacancy rates, large amounts of overtime, diminished work-life balance, potential burnout and some industry relationships that may shape new norms and reflect a changing value system.
An organization’s climate is different from its culture and describes the shared perception of people about an organization’s policies, procedures, rewards, and personnel system. As such, the current difficulties in recruitment and retention may be critical climate issues and represent how others perceive the division. Other important culture considerations include ensuring that the DGMQ is a learning organization with an emphasis on continuous improvement and integration of knowledge; its ability to adapt, pivot, and be innovative; its commitment to diversity, equity, and inclusion; its levels of wellness and resilience; and its tolerance toward risk and transformational change.
The committee noted that the DGMQ recently instituted a Transformational Leadership training program with the Compassion Institute, designed to help staff become effective team members and dynamic leaders. The division has also established other internal training projects that are positive steps. However, more needs to be done. The DGMQ needs to invest further in leadership development and succession planning. Additional attention is needed in health, wellness, and resilience to address burnout, and work–life balance. The DGMQ needs to foster a supportive and diverse work environment to nurture a climate that maximizes its capacity to achieve the division’s goals and to protect employees from experiencing any negative or long-term effects.

SOURCE: Damon, 2022, slide 97.
The DGMQ is currently exploring opportunities to support and enhance its workforce culture, with a focus on four key areas: workplace environment, strategy, leadership, and workload (see Figure 2-4) (Damon, 2022). Within the domain of workplace environment, efforts are focused on (1) crystallizing and defining the culture of the DGMQ; (2) supporting diversity, equity, inclusion, and belonging efforts; (3) fostering greater collaboration; and (4) increasing accountability. Strategy efforts involve strategic planning, increasing innovation, focusing on sustainability, and sharing the division’s priorities and metrics. Efforts to enhance leadership include empowering and supporting leadership, treating staff well, and building trust. In the focus area of addressing workload, opportunities include (1) addressing work-life balance challenges, (2) exploring ways to reduce the unequal burnout of headquarters and field staff, (3) cross-training staff, and (4) reducing the constant sense of urgency.
CONCLUSIONS AND RECOMMENDATIONS
The current level of funding and personnel for the Quarantine Station Program of the DGMQ is inadequate and is preventing the organization from effectively and efficiently carrying out its many responsibilities and activities. The continuous challenge of emergencies and pandemics over the last decade have stretched the DGMQ’s capacity and ability to respond to global disease threats.
The committee’s assessment of the agency’s organizational capacity finds that it is designed to operate in a past era—before the last decade’s unprecedented and profound health events. The DGMQ has had to leap from crisis to crisis by trying to use surge funds, temporary workers, and contract workers to meet these profound challenges. Unfortunately, operat-
ing in persistent emergency mode with inadequate staff and other resources has become the norm. Even after the COVID-19 pandemic has subsided, it is highly unlikely that the organization will ever return to “normal.” New outbreaks and emergencies are the new normal, and the surge requirements seen over the last decade are not an aberration. Thus, now is an inflection point for the DGMQ that calls into question how it works, what it works on, with whom it works, when it works, and if it will ever have sufficient resources and a modern infrastructure to carry out its mandate and meet present and future public health challenges. The status quo is not an acceptable strategy.
The committee acknowledges that the DGMQ has implemented a number of successful changes and actions since the report on the agency 15 years ago (Institute of Medicine, 2006). The addition of quarantine stations and increased capacity for testing and tracing mark needed progress. Although mostly successful in the past, however, the DGMQ needs to confront and change many of its legacy programs, systems, and behaviors as it faces a more uncertain and complex future. Changing trends in global travel have vastly outpaced institutional changes within the DGMQ. The division’s current structure, including its finances and staffing, is drastically underprepared to meet demands of the modern global context. It is clear that the current limitations on funding and personnel are inadequate for the DGMQ’s quarantine stations to effectively carry out their responsibilities and mission.
There is an opportunity to redesign quarantine stations, adopting new technologies and innovations (digital and diagnostic platforms), altering workload and operational hours, incorporating telehealth, working smarter, and creating a network of modern quarantine stations for the future. The organization needs a contemporary personnel plan and culture audit that resolves key issues such as high vacancy rates, excessive overtime work, a preponderance of temporary and contract employees, burnout, turnover (especially in younger employees who represent the leaders of the future), skills and competencies compatible with the changing needs of their jobs, an innovative and exciting recruiting plan, and tools and programs to ensure resiliency. The committee notes that standalone organizations—including entities with a “Center” designation—are better able to manage finances and personnel in addition to allowing for more senior positions to facilitate recruitment, retention, and professional advancement opportunities.
The committee’s findings and conclusions are not a reflection of the many outstanding people of the DGMQ, but rather a reflection of its difficult times and how the organization needs to realign itself to meet contemporary needs and technological advances. In today’s context, any organization that cannot rethink and reimage is unlikely to be successful.
Conclusions
Conclusion 2-1: Due to its critical role in ensuring national health security, the DGMQ may benefit from a more prominent position in the CDC’s organizational structure.
Conclusion 2-2: The DGMQ has a broad range of responsibilities that extend beyond its primary scope, such as the distribution of drugs.
Conclusion 2-3: Data management systems to track travelers could facilitate disease detection, surveillance, and contact tracing.
Conclusion 2-4: Additional engagement of aviation and maritime industries could assist in communicable disease control.
Conclusion 2-5: Current base funding is not commensurate with current DGMQ responsibilities. Cycles of surge funding do not support a sustainable, proactive system that is ready to be deployed as soon as a public health emergency is identified. Recalibration of the DGMQ’s baseline funding would help the division meet the challenges of today’s expansive border health landscape and heightened threats of novel infectious disease outbreaks, thus enabling the DGMQ to meet its growing responsibilities and to be better prepared for a complex, uncertain, and demanding future.
Conclusion 2-6: A pandemic fund that explicitly mentions the DGMQ as a recipient could allow the DGMQ to nimbly access funds during crises while awaiting legislative appropriation. Emergency/pandemic funds that are readily accessible and of sufficient amounts are needed to enable the DGMQ to respond to the next emergency more quickly and effectively than its current capability.
Conclusion 2-7: Identifying pathogens for prioritization would be valuable to focus efforts and response possibilities. The DGMQ could consider appropriate prioritization schematics in generating responses and targeting resources.17
Conclusion 2-8: The DGMQ is currently not appropriately staffed and therefore cannot effectively discharge its responsibilities and ac-
___________________
17 In 2021, a workshop was held to prioritize pathogens in the U.S.–Mexico border region that are of concern to U.S. federal and state partners (see https://www.cdc.gov/usmexicohealth/pdf/onehealth-southernus-508.pdf). Conducting further pathogen prioritization relevant to all ports of entry would be beneficial.
complish its mission. Staff currently work extended hours and take on extra shifts, leading to staff burnout and turnover.
Conclusion 2-9: The DGMQ’s heavy reliance on nonpermanent staff, such as fellows and contractors, is an inefficient way to operate and to accomplish its range of critical activities. This reliance on nonpermanent staff is likely to affect the functioning of the division, its workplace culture, and the morale of the permanent staff.
Conclusion 2-10: The availability of modern technologies could influence the requisite skill sets of personnel assigned to quarantine stations. While medical consultation is clearly needed for the quarantine stations to fulfill their responsibilities, options that do not rely on on-site medical officers to reduce the work burden may be viable. Establishing a telemedicine agreement with national telemedicine service
Conclusion 2-11: If the DGMQ gained designation as a Center, it would be eligible to gain more support staff and be eligible for higher-level grades and positions which would help with staff retention. It would also result in more readily available funding.
Recommendations
Recommendation 2-1: The U.S. Department of Health and Human Services (HHS), especially including the Centers for Disease Control and Prevention (CDC), should ensure that the Division of Global Migration and Quarantine (DGMQ) has the necessary financial and personnel resources, an effective organizational structure, and optimal infrastructure to effectively meet its responsibilities, execute its growing volume of work, and achieve its mission.
To implement this recommendation, the DGMQ needs to specifically act and resolve the following issues:
-
Organizational restructuring
- Strong consideration should be given to restructuring the DGMQ to become a standalone unit with a direct reporting line to the CDC director.
-
Finances
- HHS should make a special agreement with the DGMQ to enable the DGMQ to utilize readily accessible funding in future emergencies. The process of acquiring and utilizing surge funds should be streamlined to facilitate greater flex-
-
- ibility during both their acquisition and during the draw-down period post-emergency.
- The CDC should explore, along with the administration and Congress, the development of a user fee program to ensure that the division has a consistent and dependable source of revenue to cover the costs of operating the quarantine stations.
-
Workforce
- The DGMQ should develop and implement a comprehensive and contemporary personnel plan to address multiple issues of recruitment, retention, skills development, vacancy rates, burnout, and excessive reliance on contract and temporary staff. This plan should also include a commitment to diversity, equity, and inclusion, and to critical training needs and upskilling to prepare staff to successfully work in a dynamic, rapidly changing, and demanding environment and to stay abreast of evolving technologies. The plan should address the need for all quarantine stations to operate on a two-shift standard.
-
The DGMQ should develop and launch innovative strategies to support its critical recruitment needs.
- The organization should work with academic entities, such as universities and schools of public health, medicine, and law to develop a pipeline of future employees. Creative incentives and a streamlined human resources (HR) process should be used to facilitate the recruitment of graduates.
- The DGMQ should design, develop, and implement a “Ready Reserve Corps”: a well-trained, experienced, and agile group of personnel with essential competencies who are preapproved and cleared, and thus could be immediately available to rapidly meet personnel needs of the organization during emergencies. This group should be paid a stipend to serve, be on standby status, and engage in training and practice exercises.
- DGMQ should leverage opportunities presented through the CDC director’s diversity, equity, and inclusion initiatives while undergoing the division’s workforce study.
-
Culture
The DGMQ should assess its organizational culture and climate in association with the personnel and development plan to ensure that the division’s values positively support its mission. This assessment should include a focus on diversity, equity, and inclusion. Corrective actions should be initiated if findings suggest that an adjustment is needed.
Recommendation 2-2: The Division of Global Migration and Quarantine (DGMQ) should create an effective and innovative quarantine-station model that matches the expanding and changing needs of a global, mobile world and augments its work in a progressively challenging infectious disease environment.
To achieve this recommendation, the DGMQ needs to implement these specific steps:
- Develop criteria to determine whether a quarantine station should be added, deleted, or upgraded, and adjust the current number of stations accordingly. If a new station is deemed necessary, conduct a business plan during preplanning to determine (1) the optimal number of staff to support a two-shift standard, (2) requisite staff competencies, (3) necessary support staff, and (4) capacity for routine round-the-clock coverage during emergencies if needed. If a new station is deemed necessary, conduct a business plan during preplanning to (5) determine whether the new site could have multiple uses and (6) identify potential partners that the new site could engage between and during emergencies. Finally, (7) adopt appropriate advanced technology including telemedicine options.
- The maritime unit should be permanently housed within the DGMQ so that it can address the unique needs of the cruise industry and maritime-traveling public to enhance collaboration and disease control activities in maritime settings. The maritime quarantine station should have transparent operations and strong partnerships with regulated parties and other relevant entities.
- Develop a more robust program for preclearance of passengers, immigrants, and animals, including collaborative actions with other pertinent agencies and organizations. The emphasis would be on upstream locations outside of the United States to ease workload at entry sites.
- Redesign post-entry follow-ups in partnership with local and state agencies, and other federal agencies, in which resources and responsibilities are better shared and modern technology is used for communications, tracking, and surveillance.
REFERENCES
Alvarado-Ramy, F. 2022. Quarantine and Border Health Services Branch: CDC, DGMQ. Presentation to the National Academies of Sciences, Engineering, and Medicine Committee on Analysis to Enhance the Effectiveness of the Federal Quarantine Station Network.
Benenson, G. 2007. CDC’s quarantine branch: Building partnerships and enhancing workforce development. Paper presented at 135st APHA Annual Meeting and Exposition.
Brown, C., F. Alvarado-Ramy, and A. Klevos. 2021. To screen or not to screen? There’s more to border health than interventions at our borders: CDC. Presentation to the National Academies of Sciences, Engineering, and Medicine Committee on Analysis to Enhance the Effectiveness of the Federal Quarantine Station Network.
Buigut, J., and B. A. Maskery. 2021. CDC’s Division of Global Migration and Quarantine: National Academy of Sciences DGMQ overview and COVID-19 regulatory activities: CDC. Presentation to the National Academies of Sciences, Engineering, and Medicine Committee on Analysis to Enhance the Effectiveness of the Federal Quarantine Station Network.
CDC (Centers for Disease Control and Prevention). 2016. Division and office overviews. National Center for Emerging and Zoonotic Infectious Diseases (NCEZID). https://www.cdc.gov/ncezid/who-we-are/ncezid-divisions/index.html (accessed May 3, 2022).
CDC. 2019a. How CDC’s quarantine stations welcome new arrivals to the United States and protect the health of U.S. communities. Atlanta, Georgia: Centers for Disease Control and Prevention. https://www.cdc.gov/ncezid/dgmq/feature-stories/quarantine-stations-arrivals.html (accessed February 18, 2022).
CDC. 2019b. About the Vessel Sanitation Program. https://www.cdc.gov/nceh/vsp/desc/about-vsp.htm (accessed April 27, 2022).
CDC. 2021a. Laws and regulations. Division of Global Migration and Quarantine (DGMQ). https://www.cdc.gov/ncezid/dgmq/laws-and-regulations.html (accessed May 18, 2022).
CDC. 2021b. Emergency response. Division of Global Migration and Quarantine (DGMQ). https://www.cdc.gov/ncezid/dgmq/emergency-response.html (accessed February 18, 2022).
CDC. 2021c. Quarantine and border health services. Division of Global Migration and Quarantine (DGMQ). https://www.cdc.gov/ncezid/dgmq/focus-areas/quarantine.html (accessed February 28, 2022).
CDC. 2021d. Who we are. Division of Global Migration and Quarantine (DGMQ). https://www.cdc.gov/ncezid/dgmq/who-we-are.html (accessed February 25, 2022).
CDC. 2022. U.S. quarantine stations. https://www.cdc.gov/quarantine/quarantine-stations-us.html (accessed February 16, 2022).
Cetron, M. 2021. DGMQ’s evolution since the 2006 NASEM report: Quarantine stations at ports of entry: Protecting the public’s health: CDC. Presentation to the National Academies of Sciences, Engineering, and Medicine Committee on Analysis to Enhance the Effectiveness of the Federal Quarantine Station Network.
Cohen, N. J., C. M. Brown, F. Alvarado-Ramy, H. Bair-Brake, G. A. Benenson, T. H. Chen, A. J. Demma, N. K. Holton, K. S. Kohl, A. W. Lee, D. McAdam, N. Pesik, S. Roohi, C. L. Smith, S. H. Waterman, and M. S. Cetron. 2016. Travel and border health measures to prevent the international spread of ebola. MMWR: Morbidity and Mortality Weekly Report 65(3):57-67.
Council of State and Territorial Epidemiologists. 2021. Evaluation of jurisdictional & federal public health responses to past & current outbreaks & implementation of CSTE protocol for health department notification to CDC quarantine stations of infectious persons with recent travel. Atlanta, Georgia: U.S. Council of State and Territorial Epidemiologists.
Cox, K., S. Jolly, S. Van Der Staaij, and C. Van Stolk. 2018. Understanding the drivers of organisational capacity. Santa Monica, California: RAND Corporation. https://doi.org/10.7249/RR2189.
Damon, J. 2022. Review of budget and staffing—DGMQ funding, staffing, and turnover data 2019–2021: CDC. Presentation to the National Academies of Sciences, Engineering, and Medicine Committee on Analysis to Enhance the Effectiveness of the Federal Quarantine Station Network.
Davies, A., D. Fidler, and M. Gorbis. 2011. Future work skills 2020. Palo Alto, California: Institute for the Future.
Department of Homeland Security. 2022. DHS responds: Coronavirus (COVID-19). https://www.dhs.gov/coronavirus (accessed May 2, 2022).
Dollard, P., I. Griffin, A. Berro, N. J. Cohen, K. Singler, Y. Haber, C. de la Motte Hurst, A. Stolp, S. Atti, L. Hausman, C. E. Shockey, S. Roohi, C. M. Brown, L. D. Rotz, M. S. Cetron, CDC COVID-19 Port of Entry Team, and F. Alvarado-Ramy. 2020. Risk assessment and management of COVID-19 among travelers arriving at designated U.S. airports, January 17–September 13, 2020. MMWR: Morbidity and Mortality Weekly Report 69(45):1681-1685. http://dx.doi.org/10.15585/mmwr.mm6945a4.
FDA (U.S. Food and Drug Administration). 2022. FDA user fee programs. https://www.fda.gov/industry/fda-user-fee-programs (accessed March 16, 2022).
Hoffman, S. J., and M. J. P. Poirier. 2022. The law, epidemiology and politics of COVID-19 national border closures: Global Strategy Lab. Presentation to the National Academies of Sciences, Engineering, and Medicine Committee on Analysis to Enhance the Effectiveness of the Federal Quarantine Station Network.
Institute of Medicine. 2006. Quarantine stations at ports of entry: Protecting the public’s health. Washington, DC: The National Academies Press.
Marin, A. 2020. Telemedicine takes center stage in the era of COVID-19. Science November 6.
Roohi, S. 2022. Role of global migration task force (GMTF) in CDC Incident Management Structure (IMS): U.S. Centers for Disease Control and Prevention, Division of Global Migration and Quarantine. Presentation to the National Academies of Sciences, Engineering, and Medicine Committee on Analysis to Enhance the Effectiveness of the Federal Quarantine Station Network.
Rosenthal, P. J., and K. R. Tan. 2019. Expanded availability of intravenous artesunate for the treatment of severe malaria in the United States. The American Journal of Tropical Medicine and Hygiene 100(6):1295-1296. https://doi.org/10.4269/ajtmh.19-0230.
Shen, Y. T., L. Chen, W. W. Yue, and H. X. Xu. 2021. Digital technology-based telemedicine for the COVID-19 pandemic. Frontiers in Medicine 8:646506. https://doi.org/10.3389/fmed.2021.646506.
Tardivel, K. M. D. 2022. Maritime Unit: CDC. Presentation to the National Academies of Sciences, Engineering, and Medicine Committee on Analysis to Enhance the Effectiveness of the Federal Quarantine Station Network.
Vroman, S. R., and T. Danko. 2022. How to build a successful upskilling program. Harvard Business Review January 18. https://hbr.org/2022/01/how-to-build-a-successful-upskilling-program (accessed May 18, 2022).
Walls, T. M. 2021. Federal quarantine: The issue with limited CDC presence at ports of entry. Journal of Biosecurity, Biosafety and Biodefense Law 12(1):175-191. https://doi.org/10.1515/jbbbl-2021-2009.
World Economic Forum. 2016. The future of jobs: Employment, skills, and workforce strategy for the fourth industrial revolution. Geneva, Switzerland: World Economic Forum.
This page intentionally left blank.






































