
Introduction
Many states and localities in the United States have loosened or eliminated COVID-19 mitigation measures, including mask mandates, vaccine requirements, and explicit guidelines for returning to work or school after a COVID-19 diagnosis. As a result, individuals must make their own decisions regarding the risks and benefits of various actions, both for themselves and for those who depend on them (e.g. children, aging parents, employees, customers, and students). Those decisions can have health, social, and economic consequences. To make well-informed decisions, individuals must assess the risks their actions can create and reduce. This report summarizes scientific knowledge regarding how public health officials can support the public in making those individually relevant risk assessments.
That support must reflect the uncertainty of the disease, with its ongoing mutations, and complex connections between reported infections, hospitalizations, and deaths. Early on, those indicators often followed similar, time-sequenced patterns, with increased rates of infection leading to increased hospitalizations and then deaths. Over time, though, as vaccination became available and treatment improved, nationally high rates of reported infections were no longer accompanied by comparably high rates of severe outcomes. Nonetheless, variations in vaccination rates and human behavior (e.g., social distancing, conducting and reporting test results) have made it challenging to generalize research results, and medical research continues to reveal new sources of concern and uncertainty (e.g., long COVID, reinfection). Thus, it has become more difficult to assess risks just as the need for those assessments has fallen on a broader public.
That shift in responsibility reflects a shift in the Centers for Disease Control and Prevention’s (CDC’s) focus from reducing infection and transmission to reducing mortality and strain on the health care system (Centers for Disease Control and Prevention [CDC], 2022a),5 a shift that the agency has attributed to the population immunity provided by high levels of vaccination and previous infection, along with the availability of testing and therapeutics (CDC, 2022a). The CDC’s new framework reflects the position that COVID-19 will not be eradicated, but must be contained.
As a result of this shift in national priorities, policies for reducing transmission and mortality have fallen to state, local, tribal, and territorial officials, and individuals must now assess their own pandemic responses amid differing mitigation measures, regulations, and metrics across states and localities. What should they do when deciding whether to send their children to school, go to an indoor party, visit someone with compromised immunity, or go back to the office? Moreover, individuals often must make these decisions in a politically polarized environment. How individuals perceive risks and the effectiveness of control measures has been found to affect their decisions regarding self-protective behaviors (Garfin et al., 2021; Reinholtz et al., 2021). This rapid expert consultation6 summarizes research examining how individuals understand the risks related to COVID-19 and how public health officials can aid them in increasing that understanding.
__________________
5 The COVID-19 Community Levels framework replaces the Indicators of Community Transmission framework, which had been in place since September 2020, prior to the availability of vaccines. The COVID-19 Community Levels framework focuses on the rate of new cases over the past week, the number of new hospital admissions due to COVID-19, and the percentage of hospital beds occupied by COVID-19 patients, rather than on case counts and test positivity rates.
6 The full statement of task states: “The National Academies of Sciences, Engineering, and Medicine will produce a rapid expert consultation to assist decision makers in communicating about assessing personal and community risks related to COVID-19 to guide individual decision-making. This assessment will take into consideration that many states and localities have started rolling back mitigation measures, leaving individuals to make their own decisions about protective behaviors and risks. Drawing from research on science and risk communication, decision-making, and psychology, this document will identify actionable guidance and strategies that state and local government decision-makers can use in helping individuals assess their own and others’ COVID-19 risk in a context where many mitigation measures are being lifted. This document will be designed to be of practical use to decision makers, but will not recommend specific actions or include other recommendations. It will be reviewed in accordance with institutional guidelines.”
CURRENT CONTEXT OF COVID-19
Daily case counts have ebbed and flowed over the pandemic, largely reflecting the transmission patterns of different variants. Figure 1 shows COVID-19 case counts and trends over time, from January 2020 to June 9, 2022, in the United States as reported to the CDC. On June 9, 2022, there were 95,582 new cases and 205 deaths (CDC, 2022b). These figures are lower than the 1,260,526 cases reported on January 10, 2022, and the 4,215 deaths reported on February 1, 2022, at the height of the omicron surge (CDC, 2022b). The reported numbers of cases vary across the country; as of June 9, 2022, for example, the total case rate per 100,000 population was highest for Hawaii at 80 and lowest for South Dakota at 16 (CDC, 2022b).
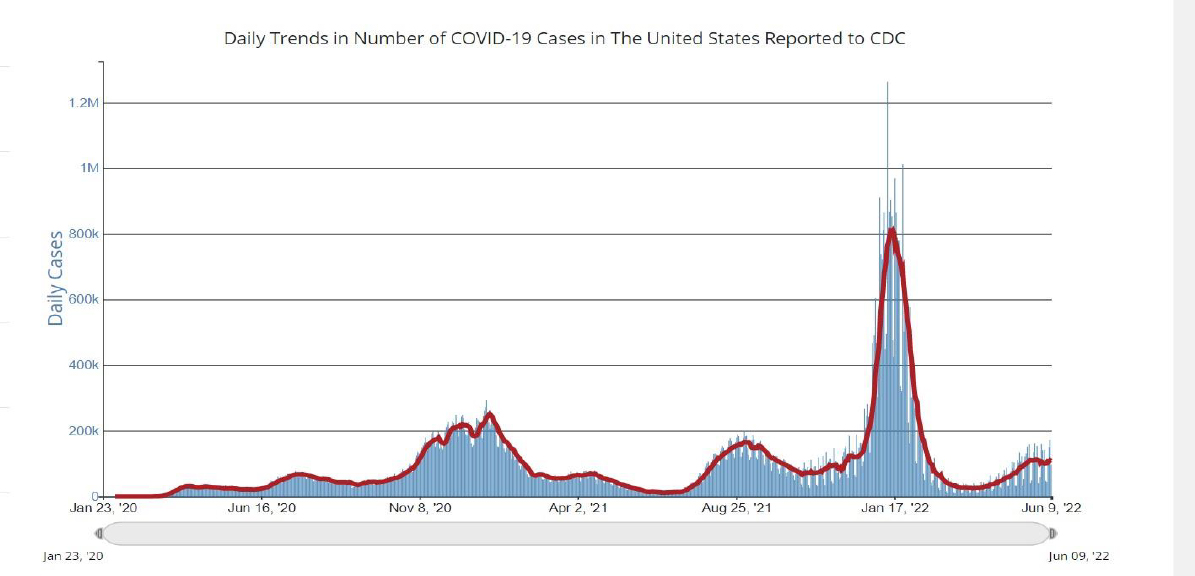
Source: CDC (2022b).
Importantly, the virus continues to have a disproportionate impact on populations long subject to health inequities. As of March 2022, the COVID-19 cumulative crude death rates per 100,000 population were 453 for Native Americans, 347 for Pacific Islanders, and 343 for Blacks, compared with 325 for Whites, 261 for Latinx individuals, and 160 for Asian Americans.7 The CDC data tracker also shows that as of May 26, 2022, 71.5 percent of counties in the United States were classified as having low COVID-19 community levels, with levels classified as medium in 20.7 percent and as high in 7.8 percent (CDC, 2022c). This variation in COVID-19 levels across the country corresponds to differences in the risks facing individuals living in these communities, and thus in the decisions that may be appropriate for them.
Moreover, as the pandemic has evolved, so, too, have the benchmarks used to gauge community transmission, complicating understanding of risk. Individuals must now, for example, recalibrate their risk assessments to reflect the CDC’s shift in focus from the portion of positive lab tests to hospitalizations and available hospital capacity (CDC, 2022d). That shift has meant that some counties previously considered high risk are now considered low risk.
__________________
After interpreting these population-level statistics, individuals must integrate them with other emerging evidence, such as increased reporting of the long-term health8 effects of COVID-19 (Lopez-Leon et al., 2021) and its mental health impacts (NASEM, 2021a; Saltzman et al., 2021). Individuals must also consider nonhealth factors, such as effects on their businesses, workforce participation, and childcare responsibilities (Bartik et al., 2020; NASEM, 2021a,b; Wellenius et al., 2021). All these impacts may vary across groups, as will group members’ resources for managing them.
CONSIDERATIONS FOR SUPPORTING INDIVIDUAL RISK ASSESSMENT
The lifting of many public health restrictions presents a special dilemma for people at high risk of adverse outcomes from COVID-19, such as those who are immunocompromised or who care for people who are. With rare exceptions, individuals must assess their personal risks while having only aggregate statistics and general guidance. In some cases, that guidance has remained constant throughout the pandemic, even as seemingly relevant conditions have changed (e.g., N95 masks are highly effective, droplets are dangerous, ventilation matters). In other cases, the guidance has changed, with varying levels of explanation (e.g., fabric face masks are useful as part of layered protection, fomites are a minor risk, aerosols are a major problem).
Public health officials need to provide individuals with the information required to estimate their own risks and the risks posed by others (e.g., sitting next to unmasked or unvaccinated individuals in meetings, caring for their children or aged parents). Unless officials provide that information in ways that are readily found and used, people will look elsewhere, rendering them vulnerable to mis- and disinformation (Fischhoff, 2020). Studies from early in the pandemic found that communications were uncoordinated, untested, ambiguous, and conflicting, leading to confusion and distrust (Garfin et al., 2021; NASEM, 2020a, 2021c).
The present, new context for the pandemic requires individuals to understand their risk level in different settings, as well as the costs and expected benefits of possible ways to reduce that risk. To that end, they will need to translate general statistics to the specific settings where they live, work, worship, travel, and play, as well as to estimate the support they will receive from their employers, communities, families, and health systems in sustaining their choices and coping with negative health outcomes. Without necessary support from the government, employers, communities, and families, individuals’ decision options may be limited. People with accurate risk perceptions may be forced to act against their own best judgment unless their employers allow needed time off, they have adequate childcare or elder care, they have access to protective measures (vaccines, masks), and they can access appropriate medical treatment.
Assessing personal COVID-19 risks requires translating population risks into personally relevant terms, accommodating such health-related risk factors as obesity, diabetes, chronic obstructive pulmonary disease (COPD), or immunocompromised status (e.g., due to age, cancer treatment); COVID-19 vaccination status; the immunity provided by prior COVID-19 infections; and the behavior of others around them (Joslyn et al., 2021). And they must do so in an often-crowded information environment. They must find the good information in a sea of claims and counterclaims, some of it well-meaning, some of it mis- and disinformation. They must integrate valid information that can use different terms, work off different data sets, address different audiences, and reveal different
__________________
8 There is emerging evidence of potential negative health sequelae following the acute phase of COVID-19 (e.g., recent findings on diabetes and heart problems) and the potential for long COVID, even among people who are up to date in vaccination and healthy (Xie et al., 2022).
uncertainties. The sensitivity of individuals’ decisions to their perceptions of risks, costs, and supports has been documented in many settings, including COVID-19 (Gerace et al., 2022). Without accurate information, individuals cannot make effective decisions, however hard they try and however self-aware they are. Table 1 lists personal, social network, and physical environment risk factors that may be taken into consideration when individuals assess their COVID-19 risk. Some online risk assessment calculators have been developed that ask users for a variety of data on such characteristics as location, type of activity, number of people involved, demographics, preexisting conditions, and lifestyle that can be used to calculate an individual’s relative risk of COVID-19 exposure and infection. However, these risk calculators have yet to be standardized.
Table 1 Risk Factors for COVID-19
| Personal | Social Network | Physical Environment |
|---|---|---|
|
|
|
Previous rapid expert consultations and reports of the National Academies of Sciences, Engineering, and Medicine (NASEM) have provided guidance focused on communicating uncertainty; presenting clear and aligned public health messages; engaging communities in building confidence in COVID-19 vaccines; and ensuring equitable access to testing, therapeutics, and vaccines (NASEM, 2017, 2020a; 2021c,d,e). The NASEM (2020a) report A Framework for Equitable Allocation of COVID-19 Vaccine distinguishes two mutually exclusive but mutually supportive activities: risk communication and health promotion.
Risk communication, the focus of this rapid expert consultation, provides just the facts, including the associated uncertainties, that people need to have when making independent personal decisions and evaluating public policies (NASEM, 2020a). Health promotion seeks to induce specific behaviors, whether overtly (e.g., with persuasion or incentives) or covertly (e.g., with manipulations of choice architecture) (NASEM, 2020a). Risk communication supports health promotion by demonstrating officials’ respect for the public and by creating the mental models needed to understand the rationale for recommended actions (Bruine de Bruin and Bostrom, 2013). Risk communication is undermined by the perception that facts are being spun to manipulate recipients’ behavior.
Individual decisions have always played a key role in the pandemic. That role has grown with the elimination of public mandates and other mitigation measures. People are faced with many decisions—for example, “Should I visit my family?” “Should I get tested before that visit?” “Should I go to a concert?” “Should I wear a mask?” In this new context, people will not only need to assess the
risks, but also to feel personal responsibility for managing them, sometimes supported by social pressures, sometimes not. The science of risk communication studies how to help people assess risks; use those assessments in their decision making; and, where necessary, defend them (Fischhoff, 2013).
THE SCIENCE OF RISK COMMUNICATION
Risk communication has been formally defined by the World Health Organization (WHO) as “the real-time exchange of information, advice and opinions between experts or officials, and people who face a threat (hazard) to their survival, health or economic or social well-being” (World Health Organization, 2020a, para. 1). The science of health risk communication focuses on those goals in the specific context of health-related decisions (DiClemente and Jackson, 2017).
The NASEM (2020a) report Framework for Equitable Allocation of COVID-19 Vaccine emphasizes the need for risk communication to go hand in hand with community engagement. The report also states that those communications need to be “(1) consistent with the evidence, (2) consistent with one another, (3) responsive to public needs, (4) tested for comprehension by members of target audiences, and (5) delivered by trusted sources through effective channels” (NASEM, 2020a, p. 176).
Risk communication research has identified factors that can influence perceptions of risk and hence must be addressed by risk communications. Those factors include the magnitude of the risks, how well they are understood by those exposed to them and by science, how controllable they appear to be, and how much of a feeling of dread they evoke (Slovic, 1987). Failure to address these factors can be seen in the atmosphere of mistrust accompanying the Ebola outbreak in West Africa (Bedrosian, et al., 2016; Transparent Communication in Epidemics, 2014). In contrast, after some initial missteps, U.S. authorities achieved a relatively high level of understanding among the public of the risk posed by that outbreak (Fischhoff et al., 2018).
Risk communication research has also shown the importance of providing information in the form that people need. For example, comparisons of relative risk are inherently incomplete; an action doubling a risk may raise it from 1 in a million to 2 in a million or from 1 in 10 to 1 in 5. Such comparisons are misleading when individuals guess the wrong baseline or erroneously infer that the source would not have used a big number if it were not a big risk.
A rapid scoping review9 of communication during the COVID-19 pandemic found that people receive pandemic-related health risk information from a broad range of formal channels and sources, including television; newspapers; scientific articles and summaries; federal, state, and local government websites; radio; government SMSs; and a web of interpersonal and informal sources, including friends, family, health care professionals, social media, and other online outlets (Berg et al., 2021).
Research on the COVID-19 pandemic has also shown how individuals’ decisions regarding self-protection and vaccine uptake reflect their risk perceptions (Garfin et al., 2021; Reinholtz et al., 2021; Viswanath et al., 2021). For example, people who perceived a greater risk of contracting or dying
__________________
9 A scoping review is a preliminary assessment of the potential size and scope of available research literature. The aim is to identify the nature and extent of research evidence on a topic, usually including ongoing research (Grant and Booth, 2009).
from COVID-19 were more likely to practice social distancing and less likely to engage in risky behaviors, such as dining indoors (Garfin et al., 2021; Reinholtz et al., 2021). Individuals’ personal risk assessments also reflect their beliefs about the effects of others’ behavior, such mask wearing and vaccination (Joslyn et al., 2021).
Box 2, drawing on the science of risk communication, presents strategies for meeting the key challenges facing state, local, and tribal decision makers seeking to encourage sound risk assessment and decision making by individuals in their specific communities. The sections below elaborate on each in turn, providing practical implications and points of access to the supporting research literatures.
Build Trust and Credibility
Officials need to explain how their decisions are made and why they change over time (Smith, 2006). Such transparency demonstrates respect for the public’s right to know and its ability to understand. Officials can prepare the public for expected changes of course that will occur as part of the pandemic and frame official statistics, recommendations, and policies as adaptive rather than erratic.
Such explicit acknowledgment of uncertainty might have reduced the confusion that has plagued communications since the onset of the pandemic. For example, WHO’s initial mask message, on January 29, 2020, was that face masks offered limited protection against the spread of coronavirus for members of the public (WHO, 2020b). Despite emerging evidence to the contrary (e.g., NASEM, 2020b), WHO reiterated the limited value of masks for members of the public in a subsequent message on April 6, 2020 (WHO, 2020c). By some accounts, WHO sought to downplay the value of
masks so they would be reserved for health care workers (Jingnan, 2020). Explaining that motivation would have expressed trust in the public to reserve masks for those with the greatest need. It would have protected WHO from criticism for inconsistency and inaccuracy when masks were later recommended for all. When people trust official health information, public health outcomes can improve (e.g., Quinn et al., 2013).
Such transparency enhances the credibility essential to effective communication (Briñol and Petty, 2009). Credibility increases with the speed and accuracy with which information is provided and the empathy and openness shown for its audience (Agley, 2020; Devine et al., 2021; Reynolds and Quinn, 2008). The goal is “social trust” (Siegrist, 2021) in “those who have the responsibility for making decisions and taking actions related to the management of technology, the environment, medicine, or other realms of public health and safety” (Siegrist, Cvetkovich, and Roth, 2000, p. 354). Research on COVID-19 reinforces the general finding that social trust increases the adoption of mitigation measures (Siegrist and Bearth, 2021).
The actions of officials during the pandemic will naturally be seen in the context of their other actions. That context includes historical legacies of injustices in medical research and services, along with current structural inequities (Evans and Hargittai, 2020), creating a priori distrust that new communications must overcome. The NASEM (2020a) report Framework for Equitable Allocation of COVID-19 Vaccine describes strategies for achieving warranted trust. Foremost among them is partnering with community-serving organizations that can provide trusted channels, tailor messages, and hear community concerns. Emphasizing common values and aligned interests can also help in building trust.
Those recommendations reflect the large body of research showing the value of building trust by engaging credible, trusted people and sources within communities (Balog-Way, McComas, and Besley, 2020; Institute of Medicine, 1999; NASEM, 2008, 2021c,d,e). Research on COVID-19 has found that greater trust in information sources is associated with greater adherence to recommendations (Coroiu et al., 2020; Fridman et al., 2020). A study in Arkansas found that such trusted sources included academic medicine and health science researchers, local health care providers, and public health organizations and leaders (Purvis et al., 2021). A study of U.S. adults found that traditional media (television, radio, and newspapers) were the most trusted sources, followed by government websites and social media (Ali et al., 2020). That study also found that trust varied by gender, age, education level, and political affiliation (Ali et al., 2020). Practical experience from the early COVID-19 outbreak in Lombardy, Italy, showed the importance of using the communication methods that people trusted most (Brivio, Oliveri, and Pravettoni, 2020), which requires knowing the views of each population group.
The trust warranted by an organization’s risk communications depends on its institutional accountability10 mechanisms for ensuring and demonstrating its transparency. The framework proposed in the NASEM (2020a) report A Framework for Equitable Allocation of COVID-19 Vaccine is intended to “not only be equitable, but also [to] be perceived as equitable by audiences who are socioeconomically, culturally, and educationally diverse, and who have distinct historical experiences with the health system” (p. 33). To that end, the report proposes a framework that “can be easily and equally well understood by the diverse audiences that the vaccine allocation mechanism must
__________________
10 Accountability refers to the objective and balanced reporting of an entity’s activities and policies, which represents the entity’s acceptance of responsibility (Rawlins, 2008).
address” and that “distinguishes scientific and ethical judgments in their application” (p. 34).
Had early communications regarding masks reflected such accountability mechanisms, some of the associated controversy and erosion of trust might have been avoided. Had subsequent communications included the evidence supporting the changes in policy, trust might have been slowly regained. Such explanations show health officials’ competence, in tracking the evidence, and their respect for the public, in sharing it. They require sharing uncertainties, avoiding spin, and preparing people for changes. In an open society with multiple information sources, health officials are vulnerable to criticism if they exaggerate risks to motivate action or underplay them to reassure the public (NASEM, 2020a). If officials withhold information, people look for it elsewhere, potentially in less authoritative or beneficent sources (Kovic and Füchslin, 2018).
When asked, members of the public report that they want to know the truth, even if it is bad (Fischhoff et al., 2018; Garfin et al., 2021). One COVID-19-related study found that providing negative information can increase trust (Petersen et al., 2021). Another found that when officials acknowledge uncertainty, they build trust and do not undermine confidence in the information or its source (van der Bles et al., 2020). A study of weather forecasts found that adding numeric expressions of uncertainty “increases trust and gives people a better idea of what to expect in terms of both the range of possible outcomes and the amount of uncertainty in the particular situation, all of which benefit precautionary decisions” (Joslyn and LeClerc, 2013, p. 308). A related study (Grounds and Joslyn, 2018) found that numeric probabilistic forecasts were as useful for individuals with no more than a high school education as for those with a college degree. These authors emphasize the need for preparatory research ensuring that the expression of uncertainty is compatible with both the decisions people face and their cognitive processes (also, Fischhoff and Davis, 2014).
FOSTER AUTONOMY AND EMPOWERMENT
Such user-centered preparatory research is essential for all communications, especially when sharing unfamiliar information with diverse individuals from different backgrounds. Without the feedback that preparatory research provides, officials may mistakenly assume that their audience cannot understand them when they in fact have not made themselves clear. If officials give up on the public, they may undermine its autonomy instead of empowering it to participate in personal and public decision making (Patton, 2008). When officials make a recommendation (e.g., wearing masks, returning to school), they need to explain its rationale and acknowledge individuals’ right to choose.
Research on science and risk communication reveals ways for scientists to earn trust by identifying and overcoming barriers to understanding. It often finds that rigorously developed 898989 messages11 can make potentially abstruse scientific information clear (Joslyn and Demnitz, 2021). The first step is learning how people intuitively think about an issue. Those “mental models” of how things work are acquired over a lifetime of formal and informal science education, personal experience, and input from other sources (Gentner and Stevens, 1983; Johnson-Laird, 1983). Scientific claims that connect with mental models enable people to absorb more information than is achievable with a string of facts while empowering them to explain their beliefs and choices to themselves and others (Bruine de Bruin and Bostrom, 2013).
If people do not understand officials’ messages, they may rightly assume that officials do not understand them. To reduce that risk, messages need to be tested before they are disseminated.
__________________
11 This is a short code that can send SMS and MMS messages to mobile phones.
Researchers have evaluated ways to communicate many topics (as illustrated by references cited in this report). Those evaluations are subjected to the same arduous process required for any peer-reviewed research. In practical settings, though, testing can be as simple as asking a few people, drawn from the target audience, to think aloud as they read successive drafts of a communication. These “concurrent verbal protocols” (Ericsson and Simon, 1994) may reveal passages that seemed clear to the authors but confused the readers, passages that seemed clear to the readers but were not interpreted as intended, missing facts that the authors mistakenly thought went without saying, and tone that was inadvertently inappropriate. Such simple testing may reveal that officials have misinterpreted their public’s ability, opportunity, and motivation to pursue recommended actions (MacFarlane et al., 2021; Michie, Van Stralen, and West, 2011). Such testing can also guide tailoring of communications to audiences varying in their numeracy, statistical, and graphic literacy skills (Galesic and Garcia-Retamero, 2010, 2011). And it can help in selecting among different visual and numerical formats (e.g., icon arrays, natural frequencies) (Trevena et al., 2013).
Fostering empowerment requires attention to a message’s tone and framing as well as its content (Lakoff, 2010). For example, telling people to “calm down” implies that they are in a panic, conveying a lack of confidence in them, even though panic is rare (Jones, 2020; Tierney, 2003; Wessely, 2005). Communications must also recognize the personal values that can lead reasonable people to choose different health behaviors (Nieh et al., 2018). Although often stable, personal values may change or have uncertain implications for responding to novel threats like the COVID-19 pandemic (Daniel et al., 2022).
However excellent their content, communications have little value unless they can be found easily, in the places where people naturally look. For example, websites without proper user testing may, effectively, hide vital information in plain sight. Effective dissemination, too, requires preparatory research and may benefit from community partnerships. A 2007 outbreak of acute hemorrhagic conjunctivitis in Keelung City and Taipei City was controlled through a multifaceted risk communication plan that included interpersonal messages, print, and mobile technology channels (Yen et al., 2009). And Lejano and colleagues (2020) embedded risk communication in a community-building program in a refugee resettlement camp.
HONOR PEOPLE’S EMOTIONS AND PERSONAL STORIES
Emotions can both aid decision making, by directing attention to problems, and undermine it, by clouding judgments (Finucane et al., 2000). Years of research on “fear appeals” has found that “messages that incite fear tend to only be successful in producing a desired behavior when people feel a strong sense of efficacy” (Van Bavel et al., 2020, p. 461). Thus, when decisions are difficult to make and carry out and their outcomes are uncertain, communications need to acknowledge those realities, thereby demonstrating empathy and sympathy for decision makers’ circumstances. That recognition can also reduce outcome bias, which occurs when people judge decisions by how things turned out rather than by how thoughtfully they were made (Baron and Hershey, 1988).
COVID-19 stories that contextualize risks without resorting to fear tactics can help people assess risk by envisioning possible situations and creating mental models for how to behave in those situations. Narratives that acknowledge the challenges individuals face and their capabilities can show empathy, emotion, compassion, and concern (Pfattheicher et al., 2020; Reynolds and Quinn, 2008; Seeger, 2006). Narratives can also address the weariness that many people feel with the prolonged pandemic, including its often poor communications (Guidry et al., 2017). Narratives have been found
effective in other health settings, resulting in better recall and fewer counterarguments (Green, 2006; Leshner et al., 2018; Shaffer et al., 2021), although a challenge with narratives is properly representing the diversity of potential scenarios (Bruine de Bruin et al., 2009). An example of the use of narratives can be seen in cancer research in a randomized controlled trial that compared the impact of a culturally based narrative film and a nonnarrative film. The culturally based narrative film was found to be more effective in increasing cervical cancer–related knowledge, attitudes, and intentions among Mexican Americans than the nonnarrative film (Murphy et al., 2015).
ENCOURAGE PUBLIC ENGAGEMENT
As the COVID-19 pandemic wears on and new threats (e.g., monkeypox) emerge, consistent engagement strategies are needed to avoid overwhelming the public. One such strategy is engaging with trusted, credible community partners who are committed to sustained relationships (Lewandowsky, Ecker, and Cook, 2017). Identifying trusted and credible messengers requires community partnerships and buy-in, which can be achieved through community engagement (NASEM, 2020a). Community engagement is particularly important given the dynamic nature of a pandemic, which means that treatment and mitigation guidance is evolving (NASEM, 2020a). A two-way process between officials and community leaders who are trusted and credible includes: (1) continuous community engagement that entails establishing two-way communication channels and hearing multiple voices; (2) engagement using multiple channels to accommodate those who cannot attend in-person meetings, those who cannot access the internet, those who are incarcerated, and those who speak other languages; (3) timeliness, which requires monitoring and anticipating community needs; and (4) trustworthiness, which involves maintaining transparency and providing information when problems are encountered (NASEM, 2020a).
A second public engagement strategy is acknowledging the public’s contributions and sacrifices in the collective response to the pandemic (Levy, 2020). A third is tailoring communication processes and content to the social contexts of diverse publics, including their group identities, ages, genders, resources, and norms (Airhihenbuwa et al., 2020; Cash et al., 2003). Such tailoring shows awareness of how different communities are affected by the pandemic and can be sensitive to preferred forms of engagement, such as whether people prefer prescriptive guidance; suggested guidance; or none at all, just the facts they need to decide for themselves.
A public engagement strategy also needs to anticipate disagreements in a political and value-laden environment, some of which will challenge the legitimacy of the evidence being communicated (Cairney, 2016; Head, 2007; Lewandowsky et al., 2017; Mulgan, 2005). Health officials can take the initiative by evoking the overarching social norm that guides them: serving all the people. That stance may be easier to maintain when the focus is on empowering individual decisions rather than, as it has been, on encouraging or enforcing mandatory policies. When addressing the risks that people create for others (e.g., not wearing a mask in a crowded environment), communications can evoke the shared responsibility to protect those who cannot protect themselves (Cammett and Lieberman, 2020; Grant and Hofmann, 2011; Schultz et al., 2007). That strategy, which is faithful to the public health mission, may also elicit a sense of togetherness, encouraging people to look beyond differences and build a sense of shared fate and responsibility (Jetten et al., 2020; Van Bavel et al., 2020; van Zomeren, Postmes, and Spears, 2008). A study of 6,000 respondents in 11 countries found that whether people believed “we are all in this together and we all need to come out of it together” predicted whether they reported adhering to COVID-19 mitigation measures (Jetten et al.,
2020).
CONCLUSION
The continuing evolution of the COVID-19 pandemic has seen a shift from societal control to individual decision making. If individuals are to bear that responsibility effectively, they need support in assessing risks and choosing among ways to manage them. Central to that support is clear, accurate, transparent, agile, trustworthy information, delivered by trusted, credible messengers in ways that people can easily access, understand, and use. Research on communication identifies strategies for providing these communications in ways that empower individuals to make sound decisions while fostering trust in the sources of the information. Central to these strategies is listening to people in order to understand their needs, desires, constraints, and resources, and then continuing to listen when revising communications as people respond and circumstances change.
SEAN is interested in your feedback. Was this rapid expert consultation useful? Send comments to sean@nas.edu or (202) 334-3440.











