
5
Telehealth Access
Jay Shore, University of Colorado, moderated the workshop’s fourth session, which focused on access issues posed by telehealth. The session’s speakers included Ateev Mehrotra, Harvard University; Theresa Cullen, Pima County Public Health; Elizabeth Krupinski, Emory University; and Angela Siefer, National Digital Inclusion Alliance (NDIA).
TELEMEDICINE USE DURING THE PANDEMIC AND THE DIGITAL DIVIDE
Ateev Mehrotra, Harvard University
Ateev Mehrotra, professor in the Department of Health Care Policy at Harvard Medical School, discussed telehealth trends and equity considerations in the context of the COVID-19 pandemic.
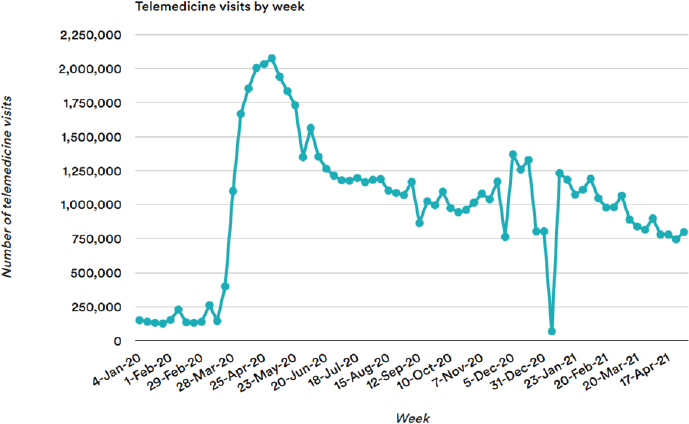
Mehrotra explained that after a steep initial drop in health care visits at the beginning of the COVID-19 pandemic, regulatory and payment changes enabled many patients to access telehealth from anywhere and for nearly any clinical specialty, leading to a surge in telehealth adoption (see Figure 5-1) (Mehrotra et al., 2020, 2021; Patel et al., 2021). One of the most influential changes was the ability to see out-of-state clinicians, which helped hundreds of thousands of Medicare beneficiaries access primary care, mental health services, and specialty care. He noted that many telehealth-only companies emerged or expanded during the pandemic. He added that telehealth expanded into a wide range of modalities, including e-consults, remote patient monitoring, and portal messaging (Patel et al., 2021).
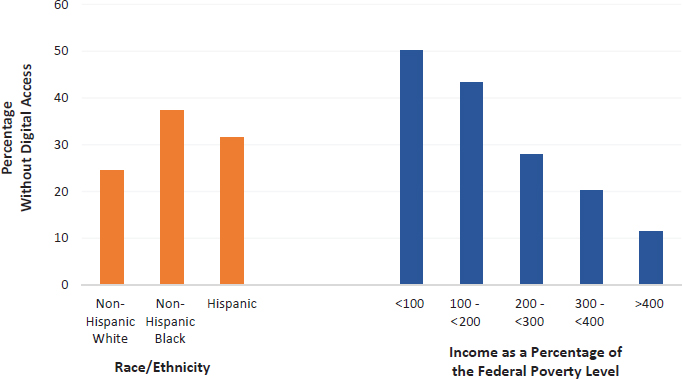
Mehrotra said while it seems that telehealth could improve health care equity by removing structural or socioeconomic barriers many patients face in accessing in-person health care, the evidence on this has been mixed. He noted that patients who face the greatest barriers to care are also the least likely to have the digital tools to access telehealth (Mehrotra and Velasquez, 2020). More than 40 percent of Medicare beneficiaries are people in communities that have historically experienced inequitable access to broadband Internet and digital devices (see Figure 5-2), especially rural enrollees, who used telehealth
SOURCES: From STAT News (https://www.statnews.com). Copyright 2021 Boston Globe Media Partners. All rights reserved. Used under license. Presented by Ateev Mehrotra on March 10, 2022, at The Use of Telehealth for Disability Evaluations in Medicine and Allied Health: A Workshop (Gray et al., 2021).
SOURCES: Presented by Ateev Mehrotra on March 10, 2022, at The Use of Telehealth for Disability Evaluations in Medicine and Allied Health: A Workshop (Roberts and Mehrotra, 2020).
less than their urban counterparts (Patel et al., 2021; Roberts and Mehrotra, 2020). He said these findings suggest that to avoid exacerbating health inequities, it is important to continue offering telehealth via phone, which does not require access to broadband or Internet-enabled devices.
RURAL ACCESS TO TELEHEALTH: CHALLENGES AND SOLUTIONS
Theresa Cullen, Pima County Public Health
Theresa Cullen, public health director for Pima County, Arizona, discussed the challenges and benefits of telehealth for rural communities and shared illustrative examples of rural telehealth programs.
Cullen explained that overall, people living in rural communities have lower socioeconomic status than urban communities, which increases their vulnerability to many health issues and decreases the likelihood that patients will have the tools to access telehealth. She added that patients in rural areas may be less likely to have strong relationships with clinicians, may have less trust in health care, and may be less likely to have stable social support systems.
She noted that despite these challenges, telehealth can bring many benefits for rural communities. Cullen echoed other speakers, noting telehealth can improve health care access, reduce patient costs and travel burdens, increase family engagement, and reduce administrative burdens.
Cullen said it is important to consider patient interest in, access to, and comfort with telehealth tools. She noted that it is also important to recognize that some patients may still prefer in-person visits. It is also important to integrate telehealth into administrative workflows, staff capabilities, and space constraints to avoid impeding service delivery. She explained that greater health equity can be achieved by applying lessons from successful rural health networks, incorporating universal design considerations, health care team mentoring, and clinician and patient tool kits.
Cullen highlighted illustrative examples from Arizona communities. Telehealth has been used for more than 50 years to serve people residing on the large, remote Tohono O’Odham reservation via STARPAHC (Space Technology Applied to Rural Papago Advanced Health Care), a program jointly run by the Indian Health Service, the National Aeronautics and Space Agency (NASA), and the Office of Research and Development (Bashshur, 1980). The program is composed of a network of hospitals, local health centers, and mobile health units staffed by community members with appropriate training and cultural knowledge. Cullen said during COVID-19 surges when large urban hospitals were full, telehealth support proved especially helpful for STARPAHC’s intensive care units. She noted that technology advances have significantly improved telehealth capabilities. She said, as an example, now that smartphones provide high-resolution images, trauma surgeons can often make an initial determination of treatment needs based on photographs.
Cullen said other successful programs include AFHCAN (Alaska Federal Health Care Access Network), which serves people living in Alaska’s most remote areas; ECHO (Extension for Community Healthcare Outcomes), which enables primary care clinicians to treat people with complex diseases in rural areas; and telehealth services offered at Federally Qualified Health Centers.
Cullen noted that some patients may require more than one virtual visit to feel comfortable using telehealth. She said that programs that are best positioned to thrive are those that include mentoring, are culturally responsive, ensure clinicians have an understanding of nonverbal cues, consider patient needs related to age and disability, and have tool kits to help clinicians meet patient needs and overcome reluctance.
DISABILITY EVALUATIONS IN MEDICINE AND ALLIED HEALTH: CHALLENGES AND SOLUTIONS FOR CLINICIANS
Elizabeth Krupinski, Emory University
Elizabeth Krupinski is professor and vice chair of research at Emory University in the departments of radiology, psychology, and bioinformatics; associate director of evaluation for the Arizona Telemedicine Program; and director of the Southwest Telehealth Resource Center. She discussed differences between telehealth visits and in-person visits and the resources available for clinicians to better serve their patients.
Krupinski explained that telehealth visits have obvious differences from in-person visits and require different skills. The human factors, such as touch, vision, smell, hearing, and “gut feeling”—which not only provide important clues about a patient’s health status but also establish patient comfort and satisfaction—are either completely missing or very limited. She also noted that many patients’ homes do not have high-speed Internet, the right devices, or sufficient lighting, and may present distractions.
Krupinski said that despite the clear challenges, nearly every clinical specialty can use telehealth as successfully as in-person visits. Often, the biggest hurdle for clinicians is adapting in-person skills to telehealth visits. She explained that the Health Resources and Services Administration created 12 Telehealth Resource Centers to help clinicians develop or improve telehealth skills. These resource centers compile literature about disability assessments and accommodations, cultural awareness issues, telehealth core competencies, and ethical and legal guidelines (AAMC, 2022). She said they also create patient guides in multiple languages explaining the benefits of telehealth and providing instructions to help address areas of resistance or concern.
DIGITAL INCLUSION AND TELEHEALTH EQUITY
Angela Siefer, National Digital Inclusion Alliance
Angela Siefer is the executive director of the National Digital Inclusion Alliance (NDIA), a national coalition of organizations to increase awareness of the digital divide and advocate for expanded broadband access, Internet-enabled devices, and training and support programs. She discussed the challenges to digital equity and potential solutions.
Siefer explained that digital equity is achieved when all individuals have the capacity to access the technology they need. Digital equity includes affordable, robust broadband Internet service; devices that meet user needs; effective training; quality technical support; and applications and content that enable
self-sufficient participation and collaboration. She noted that achieving digital equity also requires recognizing that the digital divide shifts as new technologies emerge. Siefer said that Internet access is not a binary yes-or-no issue, but rather a spectrum in which not all forms of Internet access are sufficient to enable use of telehealth. Digital equity is not just a rural issue: many urban households lack quality broadband service as well (U.S. Census Bureau, 2019). She noted that some urban areas experience “digital redlining,” with lower broadband infrastructure deployment, maintenance, and upgrade rates that are tied to historical inequities such as real estate redlining.
Siefer explained that in the health context, equitable telehealth requires reliable, accessible, and affordable high-speed Internet; Internet-enabled devices; and digital literacy training. She said that health systems should match their telehealth offerings to patients’ digital readiness and pursue programs and partnerships to help bridge gaps. The Affordable Connectivity Program (ACP), for example, helps consumers acquire Internet access. She explained that partnering with a trusted community organization can also help organizations provide culturally responsive, convenient training to overcome reluctance. She added that the Telehealth Equity Coalition is another organization that helps health professionals and digital equity specialists collaborate on solutions. Siefer described an example of NDIA’s work in which the Telehealth Equity Coalition formed a collaboration with a public library in Texas to create a private area for telehealth appointments, sign patrons up for the ACP, and teach digital literacy skills. She also highlighted other NDIA projects that facilitate telehealth for patients, such as digital navigator programs.
DISCUSSION
Participants discussed the role of social determinants of health and interconnected factors in health care and telehealth delivery, opportunities at the community level, and the future of telehealth.
Interconnected Factors
Speakers discussed the appropriate role of health care entities in providing or supporting services beyond health care, given that many factors influence success in telehealth and health care more broadly. Siefer noted as an example that technology costs still pose a challenge for many patients as the ACP does not cover 100 percent of Internet access or device costs. She added that VA is piloting programs to directly provide its patients with these assets.
Mehrotra agreed that health care is interconnected with other factors. He said that since people with secure housing have better health outcomes, for example, it could be argued that the health care system should provide hous-
ing. Mehrotra noted that there is a reason health care, Internet connectivity, and housing are supported by different agencies and bodies. He suggested that the health care industry should not take direct responsibility for addressing all of these issues but that health care providers should take an active role in helping patients access the resources they need. “Health care should do what health care does well and then refer to the necessary government programs or other programs that exist within the community that focus on that issue,” he said. Mehrotra noted that, following the same logic, it is not the health care industry’s responsibility to pay for all telehealth tools, but if health care costs were reduced, taxpayers could be in a better position to afford those things themselves.
Siefer agreed, adding that while it is not necessarily clinicians’ responsibility to provide all the needed services, they can find creative ways to collaborate with those who do provide services. She said that as an example, Cleveland Clinic is piloting a program for patients to receive digital literacy training from a local organization onsite in the clinic. Shore noted that some insurance companies pay for such services as part of cost-avoidance models, because effective at-home care lowers overall costs. Krupinski added that helping patients access digital resources is similar to the role of the patient navigator, who helps patients understand financial issues and access needed services.
Cullen noted that there is an important distinction between clinical care delivery and public health care models, where there is a responsibility to study and more directly address social determinants of health. She said the innovative programs piloted during the pandemic can help identify solutions to improve telehealth equity, adding that solutions should be developed with particular attention to the needs of patients with disabilities. Siefer agreed, noting that several NDIA organizations provided tablets to help older adults access telehealth during the pandemic because these devices have been found to be much easier for this patient population to use.
Community-Based Approaches
Speakers discussed various community-based approaches for improving telehealth care delivery. Cullen noted that telehealth for home-based care is not new; the examples highlighted in her presentation have been used in rural communities for decades. She added that in addition to health aides, rural communities often have public health nurses who provide at-home care. She noted that VA also provides services via a hub-and-spokes model that brings care directly to patient homes. Mehrotra added that palliative care and life insurance health checks frequently include home health visits, a model that could be adopted for in-home disability assessments.
Krupinski added that there are also many community-level opportunities to help patients access telehealth. Churches, libraries, and community centers can meet technology, space, or training requirements. She noted that medical students and residents, for example, used these spaces in novel ways to expand care services during the pandemic. Siefer added that community-based digital equity coalitions often collaborate with health care clinicians to share resources, leveraging the different strengths and services each can offer.
Considering the Future of Telehealth
Busis asked speakers to comment on future considerations for telehealth modalities. Mehrotra replied that offering nonvideo services is critical. Patients received care by phone for decades before the pandemic, and phone or text-only services increase access and equity and are sufficient to address many clinical issues. However, he noted that telehealth by phone does raise some concerns related to fraud and abuse. He added that there are times when high-quality video assessment is needed, and people living in historically underresourced areas can face barriers to care in these circumstances. Shore commented that while phone-only telehealth can result in somewhat lower quality care, for patients who face barriers to in-person care and lack the tools to access video telehealth, phone-based care can still be superior to the alternative, which in some cases is no care at all.
Krupinski agreed that offering phone-based care is important and pointed out that health care is not one point in time, but multiple encounters over time, which can include a variety of modalities. She noted that if the federal public health emergency ends, many of the regulatory waivers will also end, recreating the patchwork of state telehealth regulations unless lawmakers take action. Arizona is creating legislation that is very supportive of telehealth, but Krupinski noted that one state’s laws cannot address cross-state licensing requirements.
Speakers also drew attention to the needs of particular patient populations. Cullen noted that the pandemic’s disruption to in-person care particularly disadvantaged rural patients, who already experienced a lower quality of care because rural health systems have fewer resources and tools. Shore agreed and added that even people in some urban areas experience a lower quality of care depending on the community’s resources or populations. Krupinski pointed out that age is also an issue and said that many clinicians underestimate what seniors are capable of or interested in related to technology. Cullen noted that the pandemic created opportunities to experiment with telehealth ideas, such as sending tablets and digital hotspots to patients for at-home care. She noted that as more research is published, clinicians can determine how effective those models were in fulfilling the health care system’s responsibility to provide care.








