10
HEALTH SYSTEM TRANSFORMATION: COMMON PRIORITIES ACROSS SECTORS
INTRODUCTION
“[T]he influenza pandemic that erupted in 1918 was the first great collision between nature and modern science. It was the first great collision between a natural force and a society that included individuals who refused to either submit to that force or to simply call upon divine intervention to save themselves from it, individuals who instead were determined to confront this force directly, with a developing technology and with their minds.”
—John Barry, “The Great Influenza”
In the century following the 1918 influenza pandemic, nature and modern science have collided repeatedly, from the global efforts to eradicate diseases such as smallpox and polio to the devastation and eventual pharmaceutical control of HIV/AIDS and in the past two decades, the emergence and mitigation of pathogens such as SARS, H1N1, Ebola, Zika, and MERS-CoV. During each public health emergency, individuals, families, and communities displayed resilience and led advocacy efforts for improvements in access, outcomes, and equity of care; clinicians cared for the ill; health departments detected and monitored health threats and implemented population-level interventions to inform, educate, and protect the populations in their jurisdictions; and innovators developed new tools for diagnosis, treatment, and prevention. In the aftermath of each crisis, policymakers and leaders in health and health care sectors proposed
steps to improve readiness for future outbreaks, but have found it difficult to sustain preparedness in practice. For example, while the United States ranked first in the world for pandemic preparedness in the 2019 Global Health Security Index, it has faced humbling challenges addressing health system needs during the COVID-19 pandemic (Cameron et al., 2019).
America’s readiness to respond to infectious disease outbreaks following the centennial of the “Great Influenza” was put to the test in the final month of 2019, when global news outlets first reported a “mysterious viral pneumonia” in Wuhan, China (Wee and Wang, 2020). The first U.S. case of COVID-19 infection was confirmed on January 20, 2020, and the Secretary of Health and Human Services officially declared a public health emergency on January 27, 2020, which activated new authorities for regulators and financial resources to aid health departments to detect and contain pathogens (HHS, 2020; Holshue et al., 2020). Still, the government response was slow. Over the following weeks, SARS-CoV-2 (the virus that causes COVID-19) began to spread rapidly across the world, with reports from other countries detailing the virus’s toll on individual and population health, the strain it was already placing on health systems, and the need for public health restrictions with a scale and scope unprecedented in the modern era.
Infections began increasing exponentially in the U.S. in March 2020, with the number of confirmed COVID-19 cases rising from less than 50 to nearly 200,000 over the course of the month (JHU, 2020). Elected officials issued stay-at-home orders, leading to the closure of schools, offices, and retail businesses (Bosman and McKinley, 2020). Hospitals and clinicians struggled to care for the growing volume of patients, which soon outpaced the inpatient capacity of health systems in early epicenters such as New York City and required the rationing of limited supplies and services, known as crisis standards of care. In the U.S., a lack of access to accurate and rapid diagnostic tests, longstanding shortages in staffing, fragmented data systems, a weak digital infrastructure, and inadequate funding limited health department efforts to trace the disease’s spread and control the outbreak (Christopher et al., 2021; HHS OASH, 2016). For individuals, families, and communities, misinformation campaigns on social media obscured or criticized credible information sources, creating confusion and mistrust. Alongside months of inadequate access to essential health care resources, individuals, families, and communities were also excluded from problem solving and decision-making about standards of care, closures in their communities, and other critical safeguards. Health systems experienced shortages of essential medical supplies such as personal protective equipment (PPE), especially during the early stages of the pandemic, leaving health care providers and the general public even more vulnerable (Arangdad and Godfrey, 2021).
Across the first year of the pandemic, over 3,600 health care workers’ deaths were attributed to COVID-19 (KHN and The Guardian, 2021). Meanwhile, at the policy level, a breakdown in coordination between federal, state, and local governments, the politicization of public health guidance, and widespread misinformation fostered uneven approaches to lockdowns and re-openings, and further fractured public trust.
As COVID-19 infections surpassed one million cases in the U.S. by the end of April 2020, the federal government announced the creation of multiple public-private partnerships, including Operation Warp Speed, to accelerate the development of diagnostics, therapeutics, and vaccines for SARS-CoV-2 (Trump White House, 2020). While the research and development (R&D) of medical countermeasures is typically a years-long process, R&D teams were able to successfully accelerate study timelines to a matter of months—while maintaining accepted standards of methodological rigor—thanks to substantial financial investments in clinical research as well as collaborations between academia, industry, and government. By the end of 2020, the Food and Drug Administration (FDA) had authorized hundreds of diagnostics, multiple therapeutics, and even the first COVID-19 vaccines to receive Emergency Use Authorizations (EUAs) (FDA, 2020a). These achievements were remarkable, but the potential global benefits of these innovations have been influenced by limited vaccine availability in many countries, as well as by widely varying personal decisions fueled by the politicization of public health and the spread of misinformation, even in the most economically developed countries.
The damage done by the pandemic has been devastating and disruptive. By April 2022, the SARS-CoV-2 virus had infected over 80 million Americans and taken the lives of more than 950,000—with over 6 million deaths globally (CDC, 2022a; WHO, 2022). The pandemic has disproportionately affected older people, people of color, and individuals from low-income backgrounds, with COVID-19 exposing and exacerbating longstanding inequities in social determinants of health and population health in the U.S. (CDC, 2021a and CDC, 2021b). Indeed, economic inequality, structural racism, and inadequate access to health care were rooted deeply in communities across the U.S. long before the identification of COVID-19, which only increased the susceptibility of under-resourced populations to infection, hospitalization, and fatality from the disease (Maani and Galea, 2020).
Consequently, the pandemic revealed the best and worst of American health care: a system powered by remarkable capabilities for care provision and scientific developments, but too often facing structures, incentives, and data gaps that limit the capacity of evidence-based outreach and population health interventions to address the health priorities of individuals, families, and communities. To better

understand the different facets of the pandemic response and identify opportunities for long-term transformation, a systems-level approach that accounts for the wide range of individuals, institutions, and issue areas comprising the U.S. health system is required.
To this end, the National Academy of Medicine (NAM) convened leaders from nine stakeholder sectors of the health and health care system to assess the impact and experiences within their sectors during the pandemic (see Figure 10-1):
- Patients, Families, and Communities1;
- Clinicians and Professional Societies;
- Care Systems;
- Digital Health;
- Public Health;
- Health Care Payers;
- Health Product Manufacturers and Innovators;
- Biomedical Research; and
- Quality, Safety, and Standards Organizations.
The resulting series of sector-specific impact assessments highlighted unique but interrelated contributions and challenges as each sector worked to respond to COVID-19. Management, financial considerations, incentive structures, governance, accountability, and regulatory dynamics vary from sector to sector, leading to a tendency across sectors—and even within sectors—to operate within siloes. This is largely the cause of the fragmented response observed throughout the COVID-19 public health emergency. Still, strong efforts to forge collaboration
___________________
1 To encompass all people (including those not served in a medical setting), this group is referred to as “individuals, families, and communities” throughout the remainder of this chapter.
and progress in policy and program activities during the pandemic illustrate the value and need for system-wide transformation toward a health system that supports collaboration on common, cross-cutting issues in health, health care, and biomedical science.
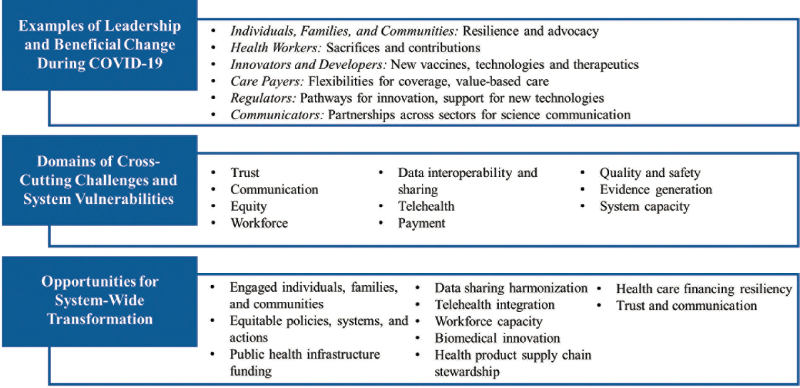
This concluding chapter of the NAM’s pandemic assessment summarizes the common experiences of the different sectors by highlighting examples of beneficial changes prompted by the pandemic (e.g., adjustments to payment and regulation) and examining the cross-cutting challenges and vulnerabilities exposed by COVID-19 (e.g., trust, workforce, technology, capacity). The final section of this chapter explores the cross-cutting opportunities for near- and long-term system-wide transformation, using the NAM’s framework for a continuously learning health system (as outlined in the 2013 IOM publication Best Care at Lower Cost) to foster effectiveness, efficiency, equity, and continuous learning for the future of American health care (IOM, 2013). An overview of this chapter’s findings is summarized in Figure 10-2.
To be successful, these priority actions and opportunities must be underpinned by the critical components of trust, equity, and authentic relationships. Meaningful change will require all individuals to be able to recognize their own interests, perspectives, and culture at the center of their experiences throughout the health system and across the continuum of care. These foundational principles are the basis for transformative action across the themes presented and discussed in this chapter:
- Centering health system actions and accountability on individuals, families, and communities;
- Committing to the pursuit of equity as core to health system performance;
- Securing the public health infrastructure for 21st century population health challenges;
- Building a robust and integrated digital health and data sharing infrastructure;
- Integrating telehealth into payment and delivery systems;
- Investing in workforce capacity and readiness;
- Streamlining innovation pathways for biomedical science;
- Strengthening stewardship of the health product supply chain;
- Restructuring health care payments to focus on outcomes and population health; and
- Fostering communication and collaboration across sectors and stakeholders.
EXAMPLES OF LEADERSHIP AND ADVANCES DURING COVID-19
While the American health system often struggled during the COVID-19 pandemic—a result of both structural issues and underinvestment in pandemic preparedness and foundational and functional public health capabilities—stakeholders across the system took bold steps to respond to COVID-19 that may provide momentum for future system-wide transformation.
Throughout the pandemic, health care and public health workers across the country met the needs of their communities and called attention to the importance of preparedness, often suffering great personal costs to respond to the crisis. At the same time, actions by regulators, payers, and health systems have catalyzed telehealth utilization, and new investments and public-private partnerships have accelerated the development of new medical countermeasures for COVID-19. This section presents some of the ways in which individuals and organizations across the health system have contributed to the many developments, innovations, and advances that have helped America and the world arrive in 2022 with safe vaccines, therapeutic options, and a better understanding of disease control and prevention. Figure 10-3 illustrates examples of leadership and advances made for:
- Individuals, families, and communities;
- Health workers;
- Innovators/developers of health products and technologies;
- Care payers;
- Regulators; and
- Communicators.
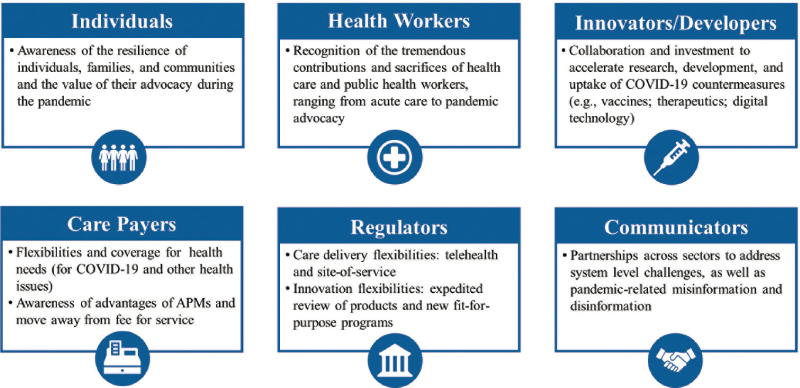
Individuals, Families, and Communities: Resilience and Empowerment
Although individuals and families are best positioned at the center of the health care system, their perspectives and voices are often absent from decision-making, system design, and policy considerations. This reality has substantial downstream consequences for health equity and outcomes. The sequelae of these system failures have been apparent during COVID-19, which has impacted individuals, families, and communities in myriad ways, from the direct harm of infection to the collateral impact on mental health, non-COVID-19 illnesses, and economic and social instability. All of these concerns have been amplified for communities of color, low-income populations, women, and other groups that are economically or socially marginalized.
For individuals and families navigating the system, U.S. health care often feels fragmented, contributing to a sense that it is inadequate and slow. These sentiments were exacerbated by the unique set of obstacles that COVID-19 raised. As evidenced in the chapter on patients, families, and communities (Chapter 1), COVID-19 has unmistakably devastated many communities across America. Although the consequences of the pandemic will reverberate for many years, they should be recognized alongside the many positive community responses and leadership from individuals and families displayed on matters including care, financing, and data and evidence generation.
Individuals, families, and communities have displayed remarkable commitment and resilience in the face of adversity throughout the pandemic. Many have
leveraged their voices against the shortcomings in health system responses, advocating for better access to essential health care resources such as PPE or COVID-19 testing sites, amplifying authoritative public health information, and fighting to ensure that research and innovation for COVID-19 centered on individuals (e.g., spotlighting the effects of “long COVID”, highlighting racial disparities in clinical trials).
Health Workers: Contributions and Sacrifices
Clinicians, including a broad range of direct care providers and allied health professionals, represent the backbone of the American health system. From the outset of the pandemic, health care and public health workers rose to the occasion, working long hours and taking on significant personal risks to care for patients with COVID-19 and other critical illnesses. The health care workforce’s leadership and service has elicited broad public support, from the salute to health care and public health workers that began in New York City and spread nationwide to the significant increase in applications to health professions schools (Murphy, 2020; Newman, 2020).
While health care workers’ commitment to patient care during COVID-19 embodies the essence of their professional oaths and the legacy of service during previous infectious disease outbreaks (e.g., influenza, HIV/AIDS), their contributions to the pandemic response have come at a significant cost. The chapter of this Special Publication focused on clinicians and professional societies (Chapter 2) details how preexisting gaps in the workforce created issues for clinical capacity during COVID-19, and how shortages of PPE and other medical supplies left health care workers exposed to infection, resulting in thousands of cases of clinician infections and deaths (KHN and the Guardian, 2021). The recognition of individual contributions and sacrifices must be understood, therefore, in the context of systemic shortcomings and their consequences on the physical, emotional, and moral well-being of health care professionals (further described in the “Workforce” sub-section of “Cross-Cutting Challenges for COVID-19”).
Innovators/Developers: New Health Products and Technologies for Pandemic Mitigation
Advances in Research and Development
Although significant research has been dedicated to understanding related coronaviruses over the past decades, SARS-CoV-2 emerged in 2019 as a novel pathogen. At the outset of the pandemic, health professionals faced the historical
reality that the development of new medical products—particularly therapeutics and vaccines—can span a decade and cost more than one billion dollars to develop and test (Gouglas et al., 2018). Two chapters of this pandemic assessment—on biomedical research (Chapter 8) and on health product manufacturers and innovators (Chapter 7)—detail how the academic, public, private, and nonprofit sectors engaged in remarkable collaboration to accelerate the development of medical countermeasures for COVID-19. Programs such as the Rapid Acceleration of Diagnostics (RADx) initiative and Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) public-private partnership, both organized by the National Institutes of Health (NIH), are examples of the kind of system-wide initiatives that helped streamline development processes and timelines (e.g., by developing master protocols and organizing data sharing) (Collins and Stoffels, 2020; NIH, 2021; Tromberg et al., 2020).
Biomedical research professionals and health product manufacturers and innovators worked across the globe to adapt clinical trials amidst the unique circumstances and priorities of the pandemic era. In addition to navigating restrictions related to travel, quarantining, and enhanced safety precautions, researchers, manufacturers, and innovators sought to address ongoing racial diversity concerns by appropriately and sustainably enhancing the representation of people of color as clinical trial participants and investigators (FDA 2020b; LaFraniere et al., 2020; Nephew, 2021; NIH, 2020; North et al., 2020). A number of tools have been used to improve cost reduction, efficiency, timeliness, generalizability, and synergy among clinical trials worldwide, including innovative trial design and implementation methodologies (e.g., flexibilities for trial duration, sample size modifications, platform trials, utilization of incidence prediction data to aid in clinical trial site placement and diverse recruitment, in-person/remote interactions during trials) and supportive approaches to data collection and analysis (e.g., tokenization of data, connecting trial data with electronic health records) (FDA, 2020b; Hahn et al., 2020; Kunz et al., 2020; Normand, 2021; Van Dorn, 2020). Regulatory authorities should consider the continued use of such flexibilities to benefit clinical trials where feasible (EMA, 2020; FDA, 2020d; Meyer et al., 2020).
There have been many examples of accelerated scientific innovation during the pandemic. One lasting legacy will be the successful design, testing, evaluation, and distribution of vaccines for COVID-19 in an extraordinarily short time without compromising the safety or quality of vaccine development (WHO, 2021). Under challenging financial, operational, and technical circumstances, leaders across the global health system successfully worked together to focus resources for COVID-19 vaccines, and, by December 2020, two vaccines received EUAs from the FDA (FDA, 2022a; FDA, 2020c). Yet challenges surrounding access, vaccine
refrigeration and storage, and trust slowed vaccine rollout and required significant and ongoing mitigation strategies. As of April 2022, the FDA has fully approved two vaccines and provided an EUA for one other, but equitable vaccine access and vaccine hesitancy still hamper vaccine uptake in the U.S. and abroad at the time of publication (FDA, 2022b; Gill and Ruta, 2022; Saelee, 2022).
Despite these barriers, innovative immunization tools and strategies throughout the pandemic enabled over 255 million Americans to receive at least one dose of a vaccine, over 215 million Americans to be fully vaccinated, and over 100 million Americans to receive at least one vaccine booster as of the time of writing (CDC, 2022b). Continued advancements in biomedical research will need to address the obstacles to research and development faced along the way (e.g., workforce shortages, health system research capacity, trial disruptions due to investigational site access restrictions, diverse participant recruitment issues, and other racial disparities) (Chastain et al., 2020; FDA, 2020d; Helfand et al., 2020; Nephew, 2021; North et al., 2020). Meanwhile, it is important to recognize the history of investments and discovery leading to the scientific achievements achieved during COVID-19. The pace of vaccine development and other medical product milestones realized during the pandemic were unprecedented. These achievements were possible only because of decades of basic science research. At the same time, it is important to recognize that individuals across the world still face many limitations in terms of access and delivery for these same vaccines and therapeutics (Frisch et al., 2021; Johnson, 2021).
Advances in Digital Technology
From artificial intelligence to telemedicine, a number of facets of digital innovation have offered bright spots in the U.S. pandemic response. As the risk of disease transmission made in-person engagement and care infeasible, the rapid deployment of a diverse telemedicine toolkit ensured that essential services could still be provided. These tools were prone to geographic and population-level disparities in the form of the nation’s “digital divide,” but, as a whole, remote patient monitoring, mobile health tools, and synchronous/asynchronous care were essential to preventing care gaps across the U.S. (Maliha et al., 2021; Perrin et al., 2020). The accelerated uptake and use of digital platforms has supported case investigation, contact tracing, and other essential functions of state and local public health throughout the COVID-19 public health emergency (CDC, 2019; Gunasekeran, 2021). Also key has been the implementation of artificial intelligence, helping to manage an often overwhelming amount of data and empowering significant tools for pandemic response (e.g., intelligent chatbots, accelerated therapeutic development, life-saving decision support systems) (Brothers, 2020; Lyons, 2020; Magrabi et al., 2019). While these tools still have
much to gain from a refreshed digital infrastructure and improvements to data interoperability, they demonstrate the remarkable benefits that digital solutions can provide for health system effectiveness, efficiency, equity, and continuous learning (AHA, 2019; Llupia et al., 2020; Peiffer-Smadja et al., 2020).
Care Payers: COVID-19 Insights for Payment Reform
There are a number of shortcomings to the system of reimbursement for health services in the U.S.: the misalignment of financial incentives contributes to unnecessary and low-value service utilization, and information gaps and opaque access and coverage processes can delay access to care (Leavitt et al., 2016; Shrank et al., 2019). However, as COVID-19 disrupted care delivery across the health system, payers and policymakers took rapid action to adjust payment policies, yielding insights for future coverage flexibilities and payment models.
Flexibilities and Coverage for Health Needs During the Pandemic
The passage of emergency pandemic relief legislation included provisions to guarantee that insurers would cover many components of COVID-19 diagnosis and treatment (Keith, 2020). Regulators and clinicians worked together to develop codes for new pandemic-related health products (e.g., COVID-19 tests) and services (e.g., updates to Medicare Severity-Diagnosis Related Groups for inpatient COVID-19 care) (CMS, 2020a; Federal Register, 2020). To support service continuity for non-COVID-19 medical needs (e.g., chronic disease management), payers introduced temporary payment policies for telehealth and other site-of-service adjustments. Beyond these changes to reimbursement, health plans also introduced new financial and administrative flexibilities, ranging from premium deferrals to waivers of prior authorization and cost-sharing policies (AHIP, 2020).
While many of these policies and programs will terminate at the eventual expiration of the public health emergency, the pandemic-era reimbursement and coverage flexibilities suggest opportunities for improving the efficiency and equity of health care payments in the future. For example, simplifying and clarifying the processes of prior authorization and cost sharing may be further explored to improve access and experiences (Gaines et al., 2020).
The federal Medicaid program and the Health Insurance Marketplaces played a critical role in protecting Americans’ access to health insurance and health care during the public health emergency and related economic downturn despite the fact that millions of people across the nation lost their jobs and their employer-sponsored insurance, Medicaid and Health Insurance Marketplace enrollment increases provided an effective stopgap for continued coverage (CMS, 2021; HMA, 2020).
Support for Alternative Payment Models
COVID-19 highlighted a number of limitations inherent in traditional fee-for-service approaches to health care payments with respect to service coordination, data linkage, and population health (Shrank et al., 2021). As chronicled in the chapters of this Special Publication on care systems (Chapter 3) and clinicians and professional societies (Chapter 2), the cancellation and delay of both nonemergent procedures and a range of outpatient health services threatened the financial stability of care delivery organizations, ranging from primary care practices to academic medical centers (Khullar et al., 2020a; Rubin, 2020). Federal relief payments to providers, reimbursement flexibilities for telehealth, and the rebound in volumes for some specialties have partially alleviated this impact, but many providers continue to express concerns about the short- and long-term financial outlook for community practices and hospitals.
The financial impacts of the pandemic have not been evenly distributed across the health system. Clinicians reimbursed under alternative payment models (APMs)—where reimbursement is typically delinked from service volume—reported greater financial stability and operational flexibility during the first year of the pandemic (i.e., primary care providers in capitated, risk-adjusted arrangements have been better insulated from the financial consequences of office closures and were often more prepared to transition to virtual care models) (Ikram et al., 2020; Koller and Shih, 2020; Roiland et al., 2020). Likewise, hospitals reimbursed under global budgets (i.e., provided with a prospectively set, fixed amount of funding to care for specified populations over a time period) have been better positioned to weather the declines in procedure volume and adapt to meet the needs of COVID-19 (Fried et al., 2020). In general, health care systems with substantial levels of premium income from their own health plans have generally fared better during the pandemic (Bannow, 2020).
Amidst the dysfunctionality of fee-for-service payment structures, federal provider relief initiatives such as the Coronavirus Aid, Relief, and Economic Security (CARES) Act helped to mitigate severe financial losses, keep critical care avenues open, and enhance providers’ abilities to adapt to the circumstances of the pandemic (Kaufman Hall, 2021; Socker et al., 2020). Although criteria and distribution systems for these relief avenues may not have been optimally efficient and equitable, they have given many systems the stability, resources, and flexibilities needed to pivot toward more resilient, innovative, and person-centered approaches to health financing and payment.
Payment reform alone is not a panacea for resolving the country’s many health system inefficiencies. Uptake of APMs was lagging prior to the pandemic—with many APMs still including components of traditional fee-for-service models—and it is not clear how well current “value based” models achieve savings and outcome
improvements (Frakt, 2019; HCPLAN, 2019). As COVID-19 has renewed calls to improve the resiliency of health financing, however, payers, providers, and policymakers may be encouraged to accelerate the transition away from existing traditional fee-for-service patterns across the system and take up more sustainable approaches to reimbursement (Gondi and Chokshi, 2020).
Regulators: Pandemic-Era Flexibilities
The exigency of the pandemic led policymakers to issue temporary policies and flexibilities to increase the accessibility of health services, fill capacity needs for COVID-19, and accelerate the development of timely medical products. Select examples of beneficial changes that cut across different facets of the health care system are described below.
Regulatory Flexibilities for Care Delivery
Policymakers took several steps to shore up the capacity of care systems and delivery organizations so as to concentrate inpatient resources for COVID-19 patients while maintaining continuity in non-COVID-19 care where possible. For example, regulatory flexibilities for clinician licensing and scope of practice helped to fill capacity gaps in short-staffed hospitals in outbreak epicenters (Hentze, 2020). Likewise, flexibilities for telehealth (e.g., waivers of originating site requirements, use of consumer-facing platforms such as FaceTime and Skype) and site-of-service programs (e.g., support for Acute Hospital Care at Home) helped to shift the locus of care delivery away from overburdened hospitals and ensure access to many types of non-COVID-19 health services, at the same time protecting individuals from COVID-19 infection and spread (CMS, 2020b; CMS, 2020c).
The pandemic highlighted the value of more flexible and accessible care models, and the evolution of individual preferences after exposure to new care modalities and experiences during COVID-19 may provide opportunities and demand for new, person-centered innovations in care delivery. Potential long-term extensions of such flexibilities require consideration of additional issues such as patient privacy on virtual care modalities.
Regulatory Flexibilities for Medical Innovation
In response to public and industry demand to expedite pandemic response capacity, regulators issued temporary policies and developed fit-for-purpose programs to work with manufacturers to accelerate the development of diagnostics, therapeutics, vaccines, medical devices, and PPE to mitigate and treat COVID-19. For example, as demand for testing outpaced the capacity of the nation’s public
laboratory network, especially given staffing shortages, the FDA issued policies aimed at expanding testing at commercial laboratories and allowed for validated COVID-19 diagnostics to be used prior to the completion of EUA requests (FDA, 2020c). Likewise, the FDA instituted numerous flexibilities to support adaptation to the pandemic environment, including allowing vaccine, medical device, and therapeutic developers to conduct clinical trials amidst COVID-19 restrictions (e.g., through rapid changes to study protocols, use of telehealth) and supporting digital health efforts (e.g., expanded use for home-based care) and other technologies. Beyond such policies, initiatives such as the Coronavirus Treatment Acceleration Program aimed to streamline the review of Investigational New Drug Applications and the initiation of new clinical trials (Hahn et al., 2020).
While in some cases, such policies encountered roadblocks and required iteration (e.g., regarding the validation of COVID-19 diagnostics), the steps taken by regulators overall enabled significant progress for product development and may provide lessons for accelerating medical innovation for other public health needs (Vandenberg et al., 2020).
Communicators: Communication and Collaboration to Address System-Level Challenges
Despite the fragmentation of the nation’s health system, individuals and systems collaborated in a variety of ways to address broader impacts of the pandemic. Examples include:
- Public-private partnerships to develop medical countermeasures;
- Regional collaboratives between health systems and health departments to organize supply chains and clinical capacity;
- Collaboration between industry and public health to accelerate, increase, and improve testing and contact tracing;
- Coordination among health systems and communities to ensure that individuals and families affected by COVID-19 received a comprehensive level of care (encompassing clinical services, food banks, resources for treatment, and temporary housing for individuals with COVID-19 to protect family members); and
- Partnerships such as NIH’s National COVID Cohort Collaborative (N3C) to foster collaborations to combine clinical data from various sources.
One prominent example of collaboration was a focus on communication across the health system and with the general public about existing and evolving data on COVID-19 infection, illness, and prevention. The pandemic has been exacerbated by what some have termed an “infodemic;” misinformation, disinformation, and
gaps in data (e.g., on race and ethnicity) have undermined public trust, weakened compliance with public health best practices, and limited the potential impact that interventions can have in producing equitable outcomes at a state, local, and national level (Christopher et al., 2021; WHO, 2020; Xiang and Lehmann, 2021). To improve the collection and exchange of authoritative and trusted information, partnerships were formed between sectors at multiple levels of the health system. For example, social media platforms worked to verify clinician accounts to identify them as trusted messengers for the lay public (Lunden, 2020). Likewise, partnerships between internet search engines and public health authorities served to filter and route individuals to evidence-based resources for public health (e.g., around best practices for quarantine and self-isolation) (Pichai, 2020).
Each of these initiatives was COVID-19-specific, but the new collaborations formed during the pandemic provide a useful foundation for advancing health and science communication as an essential service of public health. They also improve outreach to specific populations and help to promote health literacy across the country.
CROSS-CUTTING CHALLENGES AND SYSTEM VULNERABILITIES
Although every part of the health delivery system faced unique difficulties during COVID-19, many of the barriers to effective pandemic response cut across the health system and are the result of broader social and political trends, as well as of longstanding neglect and underinvestment in the nation’s health system. The pandemic’s disparate impact on under-resourced populations, in turn, has critical implications for the entire health system, including on diversity concerns in clinical trials and vaccine hesitancy along demographic, educational, and ideological lines that stem from misinformation and long-standing structural barriers such as racism (Agarwal et al., 2021; KFF, 2022b; Okoro et al., 2021).
Meanwhile, clinicians and professional societies, care systems, and health product manufacturers and innovators have struggled with system capacity—from supply chains to clinical workflows. Gaps in preparedness (rooted in pre-pandemic decisions) have been a common challenge, ranging from the reliance on critical supplies sourced in other parts of the world (experienced by health product manufacturers, innovators, and care systems) to funding cuts to initiatives such as the Hospital Preparedness Program and the Public Health Emergency Preparedness Program (experienced by state and local public health and care systems). All sectors of the nation’s health system experienced challenges related to trust, communication, equity, workforce, data interoperability and sharing, telehealth, payment, quality and safety, evidence generation, and system capacity. Table 10-1 notes representative examples of these challenges, followed by elaboration.
TABLE 10-1 | Select Examples of Cross-Cutting Challenges and Experiences of Sectors for COVID-19
| Domain | Cross-Cutting Challenge | Sector Example |
|---|---|---|
| Trust | Mistrust of health-related messages due to politicization of expertise among scientists and health professionals. | State and Local Public Health and Patients, Families, and Communities: Lay public engaged with misinformation and incorrect data; lack of clarity surrounding trusted information sources. |
| Communication | Lack of engagement with and clear communication of best practices – especially with underresourced populations; gaps in alignment across the government and with the private sector. | Biomedical Research and Patients, Families, and Communities: Populations facing structural barriers and historical legacies of injustice demonstrated hesitancy toward novel biomedical research and vaccines. |
| Equity | Disparate impact of COVID-19 on under-resourced populations; systemic underinvestment in population health; and lack of data on individuals’ race, ethnicity, and language. | Patients, Families, and Communities and State and Local Public Health: Increased risk and prevalence of COVID-19 transmission and infection in communities that have been economically/socially marginalized. |
| Workforce | Underinvestment in workforce development, with issues ranging from workplace well-being to education and training. | State and Local Public Health, Care Systems, and Clinicians and Professional Societies: Health professional shortages, gaps in the public health workforce, and gaps in health IT skills relative to the volume/nature of intensive care and public health interventions needed, exacerbated by high levels of burnout and occupational distress. |
| Data Interoperability and Sharing | Limited within- and between-system compatibility and interoperability; lack of effective data standardization, platform consistency, and community accessibility. | State and Local Public Health, Care Systems, Health Product Manufacturers and Innovators, and Patients, Families, and Communities: Challenges exchanging data between health departments, health systems, manufacturers, and communities. |
| Telehealth | Limited broadband access and infrastructure to support increased use of telehealth among all populations and more established links between home care and health care, as well as challenges with payment parity | Clinicians and Professional Societies and Health Care Payers: Gaps in coverage and reimbursement for both COVID-19 and non-COVID-19 services. |
| Domain | Cross-Cutting Challenge | Sector Example |
|---|---|---|
| Payment | System fragilities associated with fee-for-service models; increased out-of-pocket costs for patients. | Health Care Payers and Care Systems: Financial distress for health systems under fee-for-service models. |
| Quality and Safety | Barriers to translating evidence to decision-making and poor health and safety outcomes for specific populations. | Clinicians and Professional Societies and Quality, Safety, and Standards Organizations: Development and dissemination of crisis standards of care for COVID-19. |
| Evidence Generation | Lack of agile and rapid clinical trial infrastructure, underinvestment in basic science, and gaps in evidence translation and population diversity. | Health and Biomedical Research, Clinicians and Professional Societies, and Health Product Manufacturers and Innovators: Ethical tensions between the desire to care for critically ill patients and the need for randomized clinical trials of new therapeutics. |
| System Capacity | Uneven distribution of capacity and insufficient supply chain redundancies. | Care Systems and Health Product Manufacturers and Innovators: Shortages of personal protective equipment, essential medicines, and other medical products. |
Trust
In marked contrast with citizens in other high income countries, Americans’ trust in the health system was already low prior to COVID-19. In a 2011-2013 survey, only 58% of Americans agreed that doctors in their country could be trusted, compared to peers such as Switzerland (83%), Denmark (79%), and the Netherlands (78%) (Blendon et al., 2014). Real issues around the high cost of medical care in the United States and the growing out-of-pocket burden for consumers (e.g., “surprise billing” for services presumed covered by insurance; shifting liability for drugs/medical products) have led individuals, families, and communities to increasingly mistrust clinicians, health care payers, and care systems (Gupta et al., 2020; Kearney et al., 2021).
During the pandemic, this low level of trust persisted: the percentage of survey respondents expressing either “a great deal” or “quite a lot” of confidence in the U.S. medical system declined from 51% in 2020 to 44% in 2021 (Gallup, 2020). As detailed in the chapter of this Special Publication focused on patients, families, and communities (Chapter 1), fragmentation and opacity in the U.S. health system—especially surrounding pandemic guidance, messaging, and response—further
eroded public trust. In addition, the larger trend of polarization in American politics seems to have infiltrated the health system during the pandemic, with surveys revealing stark divides in Americans’ perceptions of pandemic response policies based on their political affiliation (Rothwell and Desai, 2020). This polarization can potentially damage the credibility of key messengers across the health care system and, in turn, limit the efficacy of the policies they put forward.
Distrust also accentuated the disparate impact of the pandemic on communities of color. Alongside gaps in effective engagement and communication, historical legacies of injustice and unethical experiments contributed to higher rates of vaccine hesitancy among Black communities (Okoro et al., 2021).
The issue of trust has significant implications for the entire American health system both during and beyond the pandemic. In the context of COVID-19, gaps in trust have undermined the efficacy of pandemic response policies (e.g., adherence to public health restrictions such as mask-wearing) and exacerbated occupational distress among the health care and public health workforce (e.g., threats against public health leaders, rumors of unethical/profit-seeking behavior among some clinicians) (Baker, 2020). These barriers to trust may inhibit efforts to build and sustain authentic partnerships between communities, public health providers, and health care entities seeking to address inequities in care. Repairing trust in the health system will require multi-level engagement and collaboration from each segment of the U.S. health system, including strengthening community-level relationships and instituting macro-level policy changes and actions that address deeper, systemic issues of equity and integrity entrenched across the health system (Khullar et al., 2020b). The “Principles of Trustworthiness,” developed by the Association of American Medical Colleges, has the potential to serve as a useful tool in this regard (AAMC, 2022).
Communication
Barriers to effective communication during the pandemic are deeply related to these challenges of trust, especially as it surrounds audience alignment and the challenge of conveying nuanced, consistent, and evidence-based information. Throughout the pandemic, a lack of engagement with under-resourced communities has limited the reach of communication strategies with many communities and stymied hopes of increasing equity and effectiveness. Similarly, gaps in communication within and across government have compounded existing pandemic response difficulties. Moving past these will require new communication strategies centered on clarity, coordination, and the equitable engagement of all stakeholder groups.
Lack of Engagement with Under-Resourced Communities and Populations
The health system has struggled to effectively engage with and communicate best practices to the public, particularly with communities and populations that have been economically or socially marginalized. Many of these communities have suffered the brunt of the pandemic’s impact. The persistence of misinformation and perceived distrust of the health system—in particular because of historical systemic injustices—represent a significant challenge, even though numerous examples of effective and equitable communication (e.g., translating materials into multiple languages, using a variety of media platforms, collaborating with reputable public health figures, engaging trusted sources of information in the community) exist across the health care system.
One visible challenge has been the underrepresentation of low income, racial and ethnic minority, and other under-resourced groups in public and private clinical trials and studies (Chastain et al., 2020; Helfand et al., 2020). Health care product manufacturers and innovators made strong efforts to address this, and are now focusing on increasing representation of under-resourced groups (e.g., in registrational Phase 3 programs) beyond the pandemic.
Additionally, the need to provide tailored and effective messaging and authentic engagement to understand the concerns, anxieties, and access needs of individuals, families, and communities has had consequences beyond clinical trials, as evidenced by the manifestation and persistence of vaccine hesitancy in populations experiencing disadvantages because of structural economic and social factors (KFF, 2022b). As pediatric vaccines have become approved and available, vaccine hesitancy continues to limit the full potential of comprehensive pandemic mitigation (Suran, 2021). These issues are not unique to the pandemic, however, and will have consequences for population health far beyond COVID-19 (Dawes, 2020; Gee and Ford, 2011). They require new strategies to build and sustain authentic relationships; develop person, family, and community centered communication; and address the legacy of racism as a source of inequity throughout the health system.
Gaps in Communication Within and Across Government
Obstacles to an effective pandemic response have resulted from a lack of alignment across local, state, and federal governments, coupled with fragmentation within the U.S. health system. Communication difficulties, particularly surrounding misinformation on issues ranging from public health guidance (e.g., policies around mask-wearing, criteria for lockdowns and re-openings) to the procurement of medical supplies (e.g., accessing the Strategic National Stockpile),
have further contributed to the challenges in achieving nationwide alignment on key pandemic mitigation strategies.
The nation’s public health system could serve as a case study to illustrate the issues of alignment. Governance of public health varies widely across the U.S., with some states operating centralized models and others relying on more decentralized approaches (ASTHO, 2012). This lack of alignment resulted in protocols that varied by individual public health departments and offices, creating a lack of coordination, both between health departments and between public health and the public. This confusion compounded the pressure of the pandemic, hindering outbreak control efforts and further diminishing Americans’ trust in health institutions and systems.
Equity
Individual experiences paint a stark picture of the disproportionate impact of the pandemic on communities that have been economically and socially marginalized, underscoring the need for health care and public health systems to center actions and strategies on the needs of the individuals, families, and communities they serve. A lack of focus on equity—in terms of data collection, program design, and power sharing—has been a major driver of the disparities observed throughout the pandemic and the decades that preceded it (Christopher et al., 2021; NASEM, 2019a; Servick, 2020).
People of color are nearly twice as likely to be infected by SARS-CoV-2, more than three times as likely to be hospitalized following SARS-CoV-2 infection, and exhibit mortality rates nearly three times higher than those of White individuals. Compounding these trends are substantial access limitations faced by underresourced populations; unfortunately, the populations most disproportionately affected by the pandemic often have the most difficulty accessing critical services. Yet, the inequities of the pandemic extend beyond the direct health impact of infection. For under-resourced populations, the economic instability inflicted by COVID-19 has exacerbated existing issues (e.g., stable housing and food insecurity), and added to an existing mental health burden. The underinvestment in population health fueling these trends highlights the need for the U.S. health system to dedicate attention and resources toward the social drivers of health alongside the myriad other gaps exposed by the COVID-19 pandemic.
Access Limitations for Under-Resourced Populations
While under-resourced populations are more likely to be affected by COVID-19, they are also more likely to experience difficulties accessing diagnostics and services and supports across the continuum of care. For example, research has revealed major racial and ethnic gaps in access to COVID-19 testing across the
country, with the supply of testing sites often inversely proportional to individual demand (Kim et al., 2020). Likewise, equity and access challenges emerged throughout allocation methodologies for medical supplies such as ventilators (which were later amended), distribution plans for new COVID-19 therapeutics such as remdesivir, and the appropriation of relief funds (Cunningham, 2020; Grogan et al., 2021; Kiptanui et al., 2021; Schmidt et al., 2021).
Furthermore, when COVID-19 vaccines became available in the U.S., low-income individuals—a population at greater risk of exposure and severe illness compared to those with higher incomes—often struggled to access appointments due to structural barriers (e.g., registration difficulties, lack of transportation) (Goodnough and Hoffman, 2021; Hughes et al., 2021). While such examples are specific to COVID-19, they represent only the latest manifestation of longstanding inequities in access to and distribution of health services in the U.S.
Underinvestment in Lifespan-Oriented Population Health
COVID-19 also exacerbated the shortcomings in how the U.S. health system supports meaningful health and well-being outcomes in individuals, families, and communities throughout their lives. Unfortunately, these shortcomings begin with pediatric populations. While children infected with COVID-19 have been less likely to experience severe illness than older populations, the pandemic has had a significant strain on their well-being (CDC, 2021b). Pandemic-era disruptions to educational and social activities and their impact on typical developmental trajectories have been a major concern for families; distressingly, emergency department visits related to mental health increased by 24% for children and 31% for adolescents (Kwai and Peltier, 2021; Leeb et al., 2020). Combined with delays of routine health services such as well visits and a pervasive context of marginalization based on race, geographic placement, and economic status, it has become increasingly clear that efforts to support population health and well-being must begin with equitable and comprehensive pediatric care (AAP, 2020; Santoli et al., 2020).
The experience of older adults throughout the pandemic has demonstrated the necessity of extending this life stage approach to the aging population as well. Adults aged 65 and above experience a markedly higher risk of COVID-19 hospitalization and death than younger individuals (CDC, 2021c). This can be partially attributed to comparatively high rates of chronic illnesses among this population, but nursing home representation is also an important source of disparities, accounting for nearly one-third of COVID-19 deaths and posing major issues related to loneliness and isolation for residents and family members navigating visitation restrictions (CDC, 2021d; CDC, 2021e; NASEM, 2022; The New York Times, 2021). In addition to the toll of the SARS-CoV-2 virus itself, the prolonged isolation of residents of long-term care facilities is associated with
severe consequences for health and well-being (e.g., functional decline; despair; suicidality; nutritional issues) (Abassi, 2020; NASEM 2022; Perissinotto, 2012). While the visitation policies contributing to these issues have been modified over the pandemic’s course, future efforts to respond to public health emergencies must better reflect the lived experiences and priorities of long-term care residents and their families.
A life stage, population-centered approach may have mitigated these disparate outcomes by engaging wraparound, holistic strategies to prevent chronic disease, maintain mobility, and provide home- and community-based care in lieu of institutional care (Horwitz et al., 2020; NASEM, 2017; NASEM, 2019a). Likewise, increased attention toward the needs of long-term care relative to patient priorities and well-being could have helped to improve the pandemic experience for facility residents (NASEM, 2022). Instead, severe disparities for older adults pervaded the pandemic, exacerbated by the uneven distribution of chronic diseases and quality of care along racial, geographical, and economic lines (CDC, 2021d; CDC, 2021e; Gebeloff et al., 2020; Hege et al., 2021). Epidemiological data indicate that chronic conditions such as cancer, cardiovascular disease, and obesity elevate the likelihood of severe illness following COVID-19 infection (CDC, 2021c). The burden of such diseases is unevenly distributed in the U.S. among older adults, communities of color, and low-income individuals, creating the preconditions for the inequitable impact of the pandemic on these populations, especially when income, age, and race and ethnicity intersect.
For the millions of Americans caught in the health-poverty trap (i.e., poor health deriving from a state of poverty which is, in turn, further perpetuated by poor health), the morbidity and mortality associated directly and indirectly with COVID-19 is just the latest example of population health disparities (Maani and Galea, 2020). U.S. health care spending as a percentage of GDP has long outpaced expenditures in other high-income countries, but disparities in health outcomes and the number of preventable deaths along racial, ethnic, and economic strata remain entrenched, in part due to America’s chronic inequities in resource distribution (Tikkanen and Abrams, 2020). For the U.S. to improve its preparedness for public health emergencies after COVID-19, policymakers need to take action to address the fundamental health-related and social needs of communities across the country.
Workforce
The health workforce has been a key driver of the successes experienced by the U.S. health system across the pandemic, with individual dedication, bravery, and innovation present in each facet of the COVID-19 response. At the system
level, however, a marked underinvestment in recruitment, education, and training for both clinicians and public health workers has resulted in substantial capacity and skill deficits relative to modern needs. Across the pandemic, this has been compounded by the pervasive burden of clinician burnout and occupational distress, contributing to high staff turnover and a concerning dearth of employee well-being. Meeting the realities of the pandemic to reduce both gaps in capacity and the rising rates of occupational distress will be key to successfully addressing population health needs of the future.
Underinvestment in Recruitment, Education, and Training
Capacity gaps have been evident across the health care system throughout the pandemic, particularly in terms of the public health and clinician workforce. Even as the responsibilities of public health and the complexity of 21st century public health priorities have expanded in recent years, health departments have lost tens of thousands of jobs over the past decade, with much of the remaining workforce lacking appropriate training and capacity (Bogaert et al., 2019; ASTHO, 2020). Likewise, the availability of clinical services is unevenly distributed in the U.S., with millions of Americans living in so-called Health Professional Shortage Areas (KFF, 2022a). Experts have long called attention to the gaps in the critical care workforce; these have been further strained during the pandemic due to the high volume of patients requiring intensive care. In addition, there is a need to fill skill gaps in informatics and data science to assure the integrity of the information infrastructure (Halpern et al., 2013; Lopez, 2020; Stechmiller, 2002). The long-term care workforce faces similar shortages, with the pandemic calling attention to the adverse effects of high turnover and low staffing on mortality rates, hospitalization rates, and emergency department visits for residents of nursing facilities (Ochieng et al., 2022).
As the pandemic evolves, concerns of “long COVID” and pandemic-related mental health issues in the general public will create further difficulties for clinicians, professional societies, and individuals who work for care systems, exacerbated by workforce gaps in specialties such as long-term care and mental health. Across the health care system, attention to workforce development also highlights the persistent lack of diversity in educational institutions and training programs for health professions; health care leaders must prioritize diversity and inclusion at all levels of recruitment, education, promotion, and training.
Burden of Occupational Distress
Increased individual and population health needs due to the COVID-19 pandemic, coupled with the shortages in clinical capacity described above, have
put tremendous occupational distress on the health care workforce, particularly for clinicians. Previous studies have documented the high rates of occupational distress—of which burnout is a prominent example—among clinicians, including the NAM’s 2019 consensus study on clinician well-being (NASEM, 2019b). Burnout and occupational distress lead to depression, depersonalization, and possibly suicidal ideation for clinicians, as well as decreased patient satisfaction (NASEM, 2019b). COVID-19 magnified all of the existing pressures on the health care workforce, dislocating clinicians from professional support networks, families, and friends due to physical distancing measures and increasing the physical, emotional, and psychological toll brought on by caring for large volumes of acutely ill patients (Shanafelt et al., 2020). Furthermore, issues surrounding distrust, politicization of public health interventions, and false conceptions of unethical or profit-seeking motives by some clinicians have exacerbated moral injury across the health care workforce. Multi-sector health system leaders and policymakers will need to take steps to bolster the morale of the nation’s health care and public health workers and commit to meaningful improvements in workplace wellness to reinvigorate workers as efforts are made to end the COVID-19 pandemic (Dzau et al., 2020).
Data Interoperability and Sharing
Data availability has been a limiting factor for various facets of the pandemic response, including disease surveillance, surge planning, clinical trial reporting, and health product manufacturing and innovation. The problems can be partially attributed to the fragmentation within the American health system, with individuals and institutions at all levels challenged by infrastructure gaps that prevent seamless data exchange, combined with economic and other incentives that work against data sharing and collaboration. Yet another challenge is presented by unstandardized data, with missing and heterogeneously presented data obscuring the information needed to make effective clinical decisions and assess population needs. If the nation hopes to create a seamless digital infrastructure for health system optimization, it will be critical to fix these issues.
Digital infrastructure capacity remains highly variable across the health system, creating significant barriers to collaboration and digital optimization. While American hospitals and office practices have largely transitioned to using electronic health records since the 2009 passage of the Health Information Technology for Economic and Clinical Health Act, digital progress lags in public health, where decades of underinvestment have left health departments underresourced. Although programs such as the Centers for Disease Control and Prevention’s “Digital Bridge” initiative have helped improve the ability of health
departments to exchange data, challenges remain: many health departments still rely on outdated tools such as fax machines and require external collaborators to develop tools such as disease surveillance dashboards (Lumpkin and Wiesenthal, 2020). Similar gaps exist in long-term care, where lagging electronic health record adoption and a lack of interoperable digital infrastructure limit the benefits that facility residents might accrue from a more coordinated system of care (NASEM, 2022).
These gaps in infrastructure contribute to gaps in coordination. Interoperability, or the digital compatibility of different systems with one another to support processes such as data exchange, continues to be a problem both within and between health systems. Barriers to data sharing have led to misalignment between policymakers, health systems, and health departments on issues including transmission of clinical data, the reporting of testing rates, planning for bed capacity, and supply chain issues (Miri and O’Neill, 2020). Indeed, supply chain challenges provide well-established examples of these barriers. Early in the pandemic, the absence of a centralized data structure to identify and distribute needed supplies created the conditions by which states engaged in bidding wars for medical devices (Weixel, 2020). The size of the U.S. medical device industry (roughly 5,300-5,600 companies of various sizes) (MEDPAC, 2017), combined with the decentralized information and decision structures of the U.S. health system (e.g., between delivery organizations, and jurisdictions) has complicated efforts to make scaled, data-driven decisions on device manufacturing and distribution needs. A universally interoperable digital data infrastructure would greatly improve cross-system communication and coordination.
In addition, data structure has often limited the functionality of data use: throughout the pandemic, data fields were often not standardized, with the resulting heterogeneity in reported information providing an incomplete picture for decision-makers across the health system. Missing data elements have particular consequences for health equity, as gaps in reporting on race, ethnicity, and other demographic characteristics obscure the disproportionate impact of COVID-19 on populations that have been marginalized (Krieger et al., 2020).
Telehealth
The expanded use of telehealth has certainly been a helpful development during COVID-19, enabling many individuals to continue accessing an array of health services despite office closures. At the same time, the increased utilization of virtual care modalities has highlighted potential access barriers for different populations. For example, surveys of Medicare beneficiaries indicate variation in access to video health care visits for low-income individuals and people of color
(Roberts and Mehrotra, 2020). Likewise, evidence from New York City indicates disparities in telehealth use for Black individuals (Chunara et al., 2020; Weber et al., 2020). While additional research is needed to further characterize the scope and components of the “digital divide” in health care, these trends, coupled with existing limitations in broadband access and infrastructure, represent concerns that need to be addressed to ensure that telehealth does not recreate the existing disparities observed in in-person care.
In addition to questions of access, payers, clinicians, and health systems have struggled to navigate the evolving reimbursement environment for telehealth. New regulatory flexibilities for payment parity provided clinicians with a financial lifeline during COVID-19; in the near and long-term future, it will be important to develop guardrails for fraud and abuse and adjust payment rates for the expanding suite of home-based health services.
Payment
The “stress test” of the COVID-19 pandemic has revealed inefficient and ineffective practices across the health system. In the domain of health care payers, a major example of this has been the demonstrated system fragilities associated with traditional fee-for-service health care payment structures. U.S. health care is largely oriented to a structure for health payments that incentivizes the provision of higher-cost secondary and tertiary care services over preventive services. Throughout the pandemic, this structure has not supported fluid, collaborative responses between public health and medical care. Similarly, with reward systems skewed toward the higher-revenue, non-emergency, in-person services that were substantially halted during COVID-19, the resulting disruptions to care delivery had significant financial consequences for hospitals, medical practices, and other actors across the health system. As an additional challenge, the cost of COVID-19-related care and the reduction in employer-sponsored health insurance coverage following pandemic-induced layoffs (although somewhat mitigated by Medicaid/insurance marketplace enrollment) spotlights concerns regarding the affordability and accessibility of health services in America (CMS, 2021). It is critical to understand these issues in order to address the concerns of individuals, families, and communities, and to ensure that health system incentives align with better care and resiliency in both typical and emergent situations.
System Fragilities Associated with Traditional Fee-for-Service
The majority of clinicians in the U.S. continue to be reimbursed under traditional fee-for-service arrangements and, as a result, experienced significant disruptions to their revenue streams following the cancellation of non-emergent
procedures and in-person office visits at the beginning of COVID-19. While financial relief and the rebound in health care utilization have helped alleviate this financial impact, the experience has renewed discussion about the fragility of volume-based reimbursement systems (Gondi and Chokshi, 2020). Beyond questions of financial stability, the incentives inherent to entirely volume-based fee-for-service approaches are often misaligned with health outcomes, reinforce the fragmentation of care delivery, and contribute to the continued utilization of low-value health services. As evidence emerges about the contrasting financial experience of providers in APMs compared to those in traditional fee-for-service arrangements, clinicians, payers, and care systems must evaluate opportunities in order to learn from the COVID-19 experience to improve the financial resiliency of the health system.
Spotlight on Affordability and Accessibility
COVID-19 has come at a high cost to Americans, with issues including significant variation in charges for diagnostic tests, and the high price of inpatient care compounded by the prevalence of “surprise billing” for COVID-19 testing and treatment (Curley, 2020; Kliff, 2021). Congressional action sought to expand coverage for COVID-19-related services and limit financial risk for U.S. residents, but such policies have not had universal penetration (e.g., for self-insured health insurance plans), creating potential financial complications (Eisenberg et al., 2020). Indeed, awareness of the potential for high costs and surprise billing may have led individuals to defer necessary COVID-19 diagnostics or treatments, building on existing trends of delaying care due to untenable costs (e.g., in primary care) (Huff, 2020).
Insecurity has been further heightened by the substantial impact of the pandemic on health care coverage rates. While enrollment increases in Medicaid and the health insurance marketplace established by the Affordable Care Act did substantially offset the pandemic’s effect on employer- sponsored coverage, the fluctuation in coverage rates created short-term actuarial uncertainty for payers, illustrating the stark vulnerabilities that recession events can have on health service access (Agarwal and Sommers, 2020; CMS, 2021).
Quality and Safety
The pandemic has renewed awareness of the substantial variation in care quality and patient safety across the American health system. For example, issues surrounding infection control, staffing, and safety protocols in long-term care facilities—all of which predate COVID-19—have been acutely apparent during the pandemic. Likewise, the multiple touchpoints and handoffs for COVID-19
patients, from acute care to rehabilitation, illustrate the need to improve care transitions, especially for older adults. These issues, coupled with measurement and reporting difficulties during the pandemic, highlight the importance of coordination among standards organizations, professional societies, health systems, and others to ensure patient safety both at baseline and in emergency situations.
Quality Gaps in Long-Term Care Facilities
Long-term care facilities and other congregate settings, such as prisons, have often been COVID-19 hot spots, experiencing disproportionately high rates of infection, hospitalization, and mortality. Yet many of the basic operational difficulties (e.g., staffing shortages and turnover, gaps in PPE) and quality issues (e.g., around infection control planning, resident crowding) that hindered the pandemic response were preexisting concerns for long-term care facilities (McGarry et al., 2020). Many are the longstanding product of fragmentation across health system sectors and financing streams, with the pandemic underscoring the level of coverage and payment misalignment across Medicare and Medicaid; gaps in quality standards for staffing requirements; a lack of prompt, seamless, and robust communication between caretakers and family members; and considerations related to public transparency (Grabowski, 2020; Hado and Feinberg, 2020; NASEM, 2022). In order to address the major quality and safety concerns that currently face long-term care facilities, it will be critical to understand and place strategic attention on the full magnitude of the improvements needed (e.g., workforce dynamics, financing, oversight, communication).
Other issues relate to the capacity of the system and workforce, with high occupancy rates and a bias toward institutional care stretching the capacity of long-term care facilities and raising severe quality and safety issues. Furthermore, from an oversight perspective, while initiatives such as Nursing Home Compare have elevated quality issues (for nursing homes specifically), gaps in metric design and scope, coupled with attention and accountability gaps surrounding racial and socioeconomic disparities in long-term care, call for a more robust regulatory framework for long-term care in America (Konetzka et al., 2020).
Challenges Associated with Care Transitions
COVID-19 infections affect the full spectrum of care delivery, encompassing laboratory networks and outpatient diagnostics, inpatient triage and admission, inpatient discharge, and outpatient rehabilitation. As such, shortcomings associated with care transitions for COVID-19 patients have illustrated how health care system fragmentation can negatively impact service quality and safety.
For example, many hospitalized COVID-19 patients require physical rehabilitation services following their recovery from intensive care. While
hospitals have increasingly invested in in-house rehabilitation services and referrals to protect patients from post-ICU syndrome, gaps in care coordination (as well as staffing bandwidth and clinical capacity) have imposed hurdles for COVID-19 patients as they recover (Grabowski and Maddox, 2020). Likewise, reduced capacity, workforce burdens, and significant quality and safety concerns at institutional rehabilitation facilities have caused many individuals to turn to home health services, but home health providers face their own staffing and operational difficulties, and exhibit variability in service offerings and quality (Falvey et al., 2020; Tyler et al., 2021). Together, these examples illustrate the need to increase coordination and reduce fragmentation to improve accessibility and outcomes across the spectrum of care delivery.
Evidence Generation
As SARS-CoV-2 was a novel virus, researchers, clinicians, industry, and publishers across the globe collaborated to rapidly identify and disseminate insights to inform diagnosis and treatment. Even as researchers worked to launch new, large-scale studies, however, they encountered roadblocks ranging from the bureaucratic to the competitive to matters of capacity. The pandemic revealed gaps in clinical trial infrastructure surrounding trial recruitment and enrollment, trial design, and data infrastructure and sharing; all of these could be leveraged to strengthen evidence generation on a global basis. Accessibility and diversity proved challenging as well, with under-resourced communities and older age groups underrepresented in clinical trials, despite being the groups most affected by COVID-19. Overcoming these issues is altogether necessary to ensure that equity, efficiency, and effectiveness is embedded in future capacity for research, product development, and continuous learning within the health system.
Gaps in Clinical Trials Infrastructure
Throughout the COVID-19 pandemic, the large number of interventions requiring timely safety and effectiveness evaluations by large-scale clinical trials have revealed multiple opportunities to improve the nation’s clinical trial architecture. Some of these opportunities for improvement include: efforts to manage enrollment in trials with the same products and research aims; continued commitments toward rigorous study designs and safeguards to produce high quality evidence; attempts to bring the trial to the patient and other methods to ease the burden of trial participation; robust data sharing mechanisms among companies pursuing the same disease with different mechanisms; and preparation of and considerations surrounding ethical dilemmas for clinicians delivering placebo treatments (Herper and Riglin, 2020; Bauchner and Fontanarosa, 2020).
Another set of key opportunities for clinical trial improvement focuses on data infrastructure. Throughout the pandemic, the lack of universal patient identifiers or consistent data sharing practices and capabilities has resulted in a clinical trial IT infrastructure that limits the full potential of evidence generation in the U.S. health system (Couzin-Frankel, 2021; Gottlieb, 2021; Maxmen, 2020; North et al., 2020).
Efforts to address these points throughout the COVID-19 pandemic have provided excellent examples that U.S. clinical trials can scale and implement to enhance resiliency across the pandemic and beyond (Gottlieb and McClellan, 2020). Initiatives such as NIH ACTIV and studies surrounding remdesivir leveraged existing clinical trial networks and public-private partnerships, streamlining the clinical trial process to ensure that funding, resources, and support were mobilized, coordinated, and focused around the products with the greatest degrees of scientific evidence for success (Beigel et al., 2021; Couzin-Frankel, 2021; NIH, 2021). Similarly, the mobilization of the nation’s historic and well-established network of NIH-supported Vaccine and Treatment Evaluation Units (VTEUs), alongside other NIH- and CDC-supported clinical trial networks, provided a nationwide platform for large-scale clinical trials to rapidly evaluate the safety and efficacy of COVID-19 therapies and vaccines. Indeed, over 4,400 interventional studies for COVID-19 were registered on ClinicalTrials.gov as of April 2022 (NLM, 2022). International analogues are of great interest as well, with examples such as the United Kingdom’s RECOVERY Platform providing insights into ways the U.S. could implement and enhance “platform” trial designs (Normand, 2021).
Embracing opportunities for improvement and implementing and scaling examples of success will be critical to advance evidence generation beyond the COVID-19 pandemic. If complemented with a robust national clinical trial infrastructure that improves trial recruitment and enrollment processes, leverages innovative trial designs where relevant, and fosters a secure and interoperable data infrastructure, innovative models can improve the readiness and responsiveness of clinical research in the U.S. at a scale previously unimagined (Gottlieb and McClellan, 2020).
Accessibility and Diversity
Gaps in racial/ethnic representation in clinical trials must be addressed, given that populations bearing the majority of the disease burden are less likely to be represented in studies of potential interventions (e.g., older adults, people of color), possibly due to issues related to distrust, cost, and limited accessibility (Chastain et al., 2020). This issue manifested during the pandemic, from varying degrees of racial and ethnic disproportionality in COVID-19 vaccine trials to the underrepresentation of older adults in studies of COVID-19 therapeutics (Artiga,
et al., 2021; Khalil et al., 2022; Helfand et al., 2020). Leaders of Operation Warp Speed worked to improve the representation of racial and ethnic populations during the vaccine development process, yet diversifying clinical trials in general will require engagement across health system sectors, outreach to build trust among under-resourced communities, and vigilance toward diversity and inclusion in clinical research (LaFraniere et al., 2020).
Gaps in Public Health Research Infrastructure
A foundational role of federal, state, and local public health departments is to provide ongoing assessment and evaluation of disease surveillance and monitoring, as well as of health care capacity and the effectiveness of local, regional, and national responses. Throughout the pandemic, the public health sector’s capacity for generating evidence in these fields proved to be limited, due to a chronic neglect in support and maintenance of public health infrastructure, resulting in shortfalls in capacity, variations in capability, and historically siloed governance and operational structures (IOM, 2012; IOM, 2002; IOM, 1988).
In the decades prior to the pandemic, state and local public health departments have resorted to piecemeal funding approaches (e.g., grants and categorical vehicles). This approach left them without the resources they need to fully fulfill their foundational roles (HHS OASH, 2016). As a result, when COVID-19 reached the U.S., there was not enough laboratory testing equipment or staffing, which contributed to shortcomings in rapid disease detection, surveillance, monitoring, and mitigation throughout the pandemic’s course. Outdated and insufficient public health data systems and technological infrastructure compounded these weaknesses, inhibiting efforts to report or exchange evidence in real time and reducing the amount of relevant information immediately available to decision makers and the public (Christopher et al., 2021; Kliff and Sanger-Katz, 2020). To ensure that state and local public health can generate and share the evidence needed to meet 21st century public health needs in the decades to come, it is critical to optimize this infrastructure atop a more robust and resilient financial structure.
System Capacity
As COVID-19 caseloads grew exponentially in the spring of 2020, it became evident that the U.S. health care system would face significant difficulties with regard to pandemic-mitigation capacity. Public health preparedness—or its lack—was a prominent example of these shortcomings, with chronic underinvestment and funding cuts over the course of decades resulting in major workforce gaps, outdated data infrastructure for disease surveillance, and under-resourced preparedness and response programs. Supply chain shortages provide another example of a capacity
gap in need of improvement: the everyday efficiencies that were built into the system over time to optimize administrative and operational processes were challenged by the protracted public health emergency. It is important to recognize these issues in order to ensure that the state of system capacity observed throughout the COVID-19 pandemic improves in advance of future public health crises.
Public Health Preparedness
Funding for public health emergencies in the U.S. has generally followed a “boom and bust” pattern, with temporary infusions of capital during and immediately after a crisis, followed by a gradual erosion of baseline and supplementary funding streams (Murthy et al., 2017). For example, gradual cuts to the Public Health Emergency Preparedness program and the Hospital Preparedness Program over time, coupled with a general decline in public investment in health care infrastructure, have caused system-wide challenges for pandemic response, especially in regards to overcoming barriers to coordination and communication throughout the ongoing public health emergency. To enhance public health preparedness, it is critical to bolster both the Public Health Emergency Preparedness program and the Hospital Preparedness program, as well as the programs that aid the development and acquisition of medical countermeasures (e.g., the Special Reserve Fund, Strategic National Stockpile, and Biomedical Advanced Research and Development Authority [BARDA]). Programs that strengthen the basic science undergirding product development, medical innovation, and disaster preparedness are also key (Cohen and Wu, 2020; Farberman et al., 2020).
Despite the fact that lawmakers eventually appropriated emergency funds to support the public health response, the resources were primarily directed to one-off measures (e.g., procuring supplies, supporting the temporary hiring of contact tracers) and have not sufficiently addressed longstanding systemic inadequacies in the public health and broader health system infrastructure (e.g., massive workforce gaps, outdated data systems). As policymakers plan for the post-COVID-19 future, they must not only restore funding to budget line items explicitly dedicated to emergency preparedness, but also recognize that public health capabilities, workforce, and infrastructure must be sufficiently resourced even in non-crisis times (Farberman et al., 2020).
Supply Chain Shortages
Established business practices for non-crisis situations emphasized the value of efficient supply chains based on “just-in-time” production. However, as demonstrated by events such as the spike in demand for tests that followed
the 2021-2022 surge of COVID-19 variants, it is apparent that the existing configuration of the supply chain can be improved to keep pace with the pandemic-level demand for supplies and health services (Stolberg and LaFraniere, 2021). Some challenges are structural in nature; the supply chains for many medical products are largely international, with limited domestic manufacturing capacity for specific high-need medical products (e.g., respirators, swabs, laboratory reagents). Other issues have surrounded delays in replenishing the Strategic National Stockpile following previous public health emergencies, existing shortages of many essential and acute care medicines (e.g., dexamethasone), and infrastructure gaps for monitoring and tracking medical supplies.
Although public-private partnerships and federal investment helped to alleviate shortages of many types of medical supplies and equipment (e.g., ventilators), other shortages have persisted throughout the pandemic, impacting individuals, providers, and health systems alike. Supply production and purchasing will naturally scale back as the pandemic recedes, but issues with producing, coordinating, tracking, and procuring medical supplies during COVID-19 should prompt discussions, formal agreements, and changes to protocols to ensure that the medical supply chain is more resilient at baseline and has built-in flexibility for future crises.
OPPORTUNITIES FOR SYSTEM-WIDE TRANSFORMATION
While the pandemic was not the genesis of the issues identified in its course, it has put them in stark relief. Leaders from across the health care delivery system agree that COVID-19 can, and must, be a catalyst for system-wide change. In order to maintain momentum for transformation, however, it is essential to build on the new ways of working that the pandemic allowed (e.g., partnerships, breaking down siloes), implement the ethos of a learning health system (e.g., by integrating evidence development and application), and strengthen the foundation of trust upon which the transformed system will stand.
This section synthesizes the cross-cutting opportunities for health system-wide transformation, all based upon the critical components of trust and equity. Transformation will depend on the ability of individuals to recognize their own interests, perspectives, and culture at the center of their experiences with the health system, informed by authentic and trusting relationships across an equitable continuum of care. This process builds further trust, which will be critical to empowering transformational action in the following ways:
- Centering health system actions and accountability on individuals, families, and communities;
- Committing to the pursuit of equity as core to health system performance;
- Securing the public health infrastructure for 21st century population health challenges;
- Building a robust and integrated digital health and data sharing infrastructure;
- Integrating telehealth into payment and delivery systems;
- Investing in workforce capacity and readiness;
- Streamlining innovation pathways for biomedical science;
- Strengthening stewardship of the health product supply chain;
- Restructuring health care payments to focus on outcomes and population health; and
- Fostering communication and collaboration across sectors and stakeholders.
Centering Health System Actions and Accountability on Individuals, Families, and Communities
As the U.S. health care system has changed over the past half century, it has largely excluded the perspectives of individuals, families, and communities in the development of its dominant policies, programs, and practices. COVID-19 illustrated the consequences of this approach to health system design, on issues including access to care, representation considerations in biomedical research and public health data, and a lack of meaningful program success and accountability measures. The entire health system must have the shared imperative to center individuals, families, and communities, at all points across an individual’s life. This includes on matters ranging from the design of facilities to the development of therapeutic protocols, the creation of access and linkage strategies, operations evaluation, health data sharing, and the use of continuous improvement initiatives. COVID-19 provides an opportunity to build on the work of biomedical research organizations to advance person-centered drug development, and the growth in virtual care delivery modalities during the pandemic points to the need for quality, safety, and standards organizations to develop new person-centered outcomes measures. Furthermore, efforts to equitably redesign the built environment of care systems create avenues to engage individuals, families, and communities in developing more inclusive spaces that align with both individual and population-level needs (e.g., implementing digital infrastructure in long-term care facilities that enhances connection and communication between patients, families, and caregivers).
It is critically important for this engagement to be meaningfully integrated, and meaningfully accountable to individuals, families, and communities as opposed to a box-checking exercise at the end of improvement process cycles. Many existing
governance, engagement, and accountability models exist (e.g., patient advisory boards), but COVID-19 provides the opportunity for health care system leaders to think creatively about how to actively and continuously engage and better integrate individuals, families, and their communities to build a more inclusive and impactful health system for all. As a starting point, leaders should consider modifying care delivery to allow individuals to decide where and how to access care. Innovations and adaptations highlighted in the chapters of this Special Publication, such as expanded use of telehealth, Hospital at Home, and home- and community-based services, are all examples of person-centered strategies worthy of further exploration. The development of data systems oriented to individual needs and goals will allow these innovations to reach their full potential. Leaders should ensure that these systems embrace and enhance engagement, accessibility, and inclusivity to benefit the individuals, families, and communities served, and focus attention on accountability measures that center on their needs and preferences.
Box 10-1 presents considerations for centering health system actions and accountability on individuals, families, and communities.
Committing to the Pursuit of Equity as Core to Health System Performance
If people are at the center of the health system, then equity must be the core criterion for system performance. Some level of inequity in health and health care outcomes has been omnipresent across the globe for as long as health care has been provided to individuals. Leaders aiming to improve the performance of
the health system must strive to understand these inequities by investing in data systems and processes that assess the level of equity achieved and track progress toward improving it (Christopher et al., 2021). Once tracked, the resulting data must be applied to accountability metrics that are structured to focus health system attention toward sustained equity improvements for individuals, families, and communities across their lifespans.
The factors leading to health inequities are complex, ranging from the economic to the cultural; in America, the additional dimension of prolonged structural racism and its sequelae presents an especially difficult—and compelling—fundamental challenge. Because of the pervasive nature of structural racism, solutions to ameliorate this historic injustice require leadership at every level and across all domains of society and economy. The American health system is no exception, and, indeed, offers special vantage points from which to catalyze change. From the perspective of public health, targeting and resourcing population health interventions can work to eliminate the health disparities experienced by communities of color; the clinician workforce may pursue increased numbers of Black, Latinx/Latino(a)/Hispanic, Asian and Pacific Islander, and Indigenous health professionals; the biomedical research sector may seek to increase the numbers of those currently underrepresented in clinical trials and of the personnel conducting those trials. While the form of initiatives may vary, the goal will remain the same: more equitable access, quality, experiences, and outcomes for the health of individuals and populations alike.
For equity to be the core index of health system performance, all stakeholders must collaborate across the health system to assess existing barriers and develop and enact policies, practices, and commitments required to combat many years of structural racism. It will be critical to ensure that existing inequities are not built anew into emerging initiatives by incorporating the lived experiences of the individuals, families, and communities who have borne the impact of these disparities for decades.
To ensure that the appropriate strategy is paired with the system level actions necessary for progress, it is also critical to establish or update funding and payment models to support seamless service links—between medical and social services, home and community care, clinician training, care system capabilities, fundamental public health and safety infrastructure, and the data and information infrastructure, which are all necessary in order to identify individual and community health problems at the earliest possible point. Most of all, there must be collaboration across the health system to ensure that the equity embedded in the performance of each sector builds to the benefit of equity throughout society.
Box 10-2 presents considerations for leaders to advance health equity.
Securing the Public Health Infrastructure for 21st Century Population Health Challenges
For many communities across America, the shortcomings in the response to COVID-19 only serve to illuminate fundamental gaps in the country’s public health infrastructure. Numerous reports from the Institute of Medicine have documented how public health’s chronic funding gaps, variable capabilities, and siloed governance and operational structures have hindered its ability to deliver on the mission of achieving health for all (IOM, 2012; IOM, 2002; IOM, 1988). Upgrades to governmental public health infrastructure are needed to ensure that health departments across America have the necessary resources to fund a baseline set of services. The Public Health Infrastructure Fund provides policymakers with a guide for restructuring resource allocation to ensure that all Americans have access to the essential services of public health (DeSalvo et al., 2019).
Yet upgrading public health infrastructure requires more than just resources; it must also include a more fundamental restructuring of the system overall, as well as its financing. The federal government has developed a roadmap, Public Health 3.0, for modernizing public health and addressing the upstream drivers of health. To realize Public Health 3.0’s vision, health departments should re-organize funding that currently exists in categorical vehicles and grant-based cycles (HHS OASH, 2016); a sizable effort is needed to transform what is currently a network of often very small and inefficient units into a more practical size and number of functionally integrated units.
The movement toward more flexible and ongoing funding models for public health would strengthen the ability of health departments to respond to public health emergencies, address community-specific needs, and scale pandemic-era collaborations with care systems, digital health leaders and companies, and health care payers—as well as with other partners—to address 21st century population health challenges.
An immediate cross-cutting opportunity for collaboration is the transformation of public health data systems, where siloed reporting and a reliance on outdated infrastructure such as fax machines have severely hindered the response to COVID-19 (Christopher et al., 2021; Kliff and Sanger-Katz, 2020). As policymakers and system leaders work to modernize these systems, they should leverage collaborations to ensure that data systems are interoperable, connected to health information exchanges across state borders, and incorporate lessons from the federal government’s implementation of the Health Information Technology for Economic and Clinical Health Act of 2009 (Gold and McLaughlin, 2016).
By transforming public health financing and data systems, leaders can build capacity for enhanced partnerships at local, state, and federal levels that bridge medical and population health-oriented interventions. Improved interdependencies between health, medical, and social service programs across jurisdictions (e.g., partnerships between health departments and state Medicaid programs) will augment the capacity of health departments to provide locally tailored interventions that center on individuals, families, and communities.
Box 10-3 presents considerations for improving public health infrastructure to address 21st century population health challenges.
Building a Robust and Integrated Digital Health and Data Sharing Infrastructure
The impact of shortfalls in data planning, structure, coordination, interoperability, and use is deep and wide across the health system. One of the important developments of the COVID-19 response, however, has been the increased use of digital technologies and data sharing across the health system. Throughout the pandemic, telehealth has been used to deliver care, enhance the functionality of remote monitoring devices, facilitate online pharmacy refills, and support virtual clinical trial monitoring. Innovative data sharing initiatives such as the FDA Evidence Accelerator have also served as “a forum for stakeholders across the health care spectrum to share real-world data and to generate ideas on how to deal with COVID-19” (Reagan Udall Foundation for the FDA and Friends of Cancer Research, 2022).
Despite these achievements, a number of barriers prevent better sharing and response to the troves of data generated by technologies to improve care, bolster emergency preparedness, accelerate product development, and empower quality improvement for care delivery and public health response. If the task for policymakers in the decade preceding COVID-19 was “wiring” the health system, the challenge facing leaders in the decade following the pandemic will be “harmonizing” the health system. This includes ensuring that infrastructure (e.g., outdated information systems in use throughout nursing homes and public health departments) keeps up with data collection practices, as well as developing the sharing capabilities needed to achieve health system transformation and continuously improve care quality, while simultaneously appropriately respecting and protecting individual privacy.
This call to action for harmonization cuts across all aspects of the health care system. In the field of medical device manufacturing and distribution, a centralized “dashboard” (providing visibility as to what products are needed and where they are needed most) may have been able to facilitate data-driven manufacturing and distribution decisions. Likewise, the use of real-world evidence in developing COVID-19 diagnostics and treatments, measuring quality of care, and making decisions about medical products was hampered by a lack of harmonization (Naidoo et al., 2021; Berger et al., 2017). Harmonized efforts to develop frameworks and platforms for defining how such evidence should be generated ahead of study initiation (e.g., master protocols), infrastructure for collecting and sharing information in a safe and secure manner, and processes that align with system-wide consensus on best practices for data use in policy and programmatic decisions (such as those outlined in the NAM’s collection of Special Publications focused on advancing the Learning Health System
[https://nam.edu/publications-of-the-leadership-consortium/]) would help real-world evidence to reach its full potential (Greene et al., 2021; NAM, 2021).
At a foundational level, the harmonization of data sharing and digital health infrastructure would align with the ethos of a learning health system by ensuring that “evidence development and application flow seamlessly and continuously in the course of care” (NAM, 2021). During crisis situations such as COVID-19, this alignment would ensure that the right information is collected and is available to the right entities at the right time. In addition to driving substantive improvements in quality, safety, and accountability for both care delivery and public health response, and harmonization would also better position the health system to respond to emerging threats, coordinate emergency response by gathering syndromic surveillance data, assess trends, and analyze intervention efficacy in near real time. Indeed, preparedness for future emergencies would be enhanced with standardized data sharing practices, aligned privacy and data security standards, and interoperable digital health infrastructure across the entirety of the health system. This would allow for accelerated development, collection, calculation, and analysis of new metrics.
Box 10-4 presents considerations for building a robust and integrated digital health and data sharing infrastructure.
Integrating Telehealth into Payment and Delivery Systems
While virtual care delivery platforms predate the pandemic, COVID-19 has, without question, served as a forcing function for telehealth to achieve significant
penetration across the health system. The question facing the health system now is not whether telehealth is here to stay, but rather how telehealth tools and approaches can be used both confidently and comfortably by clinicians, individuals, families, and communities. As these virtual care platforms evolve, leaders must also reconsider how virtual care is delivered, reimbursed, and regulated.
These questions will require careful consideration from policymakers and coordinated approaches by leaders across the health system, who must take care to ensure that telehealth does not recreate existing inefficiencies (e.g., unnecessary utilization and spending) and inequities (e.g., the digital divide). One particular area of focus for clinicians and professional societies, care systems, and health care payers is reimbursement. Policymakers could consider using alternative payment models as the vehicle for adapting current regulatory flexibilities for telehealth following the conclusion of the public health emergency (Navathe and Liao, 2020). These reimbursement arrangements could create natural disincentives to fraud and waste, and align incentives to drive the integration of virtual and in-person care into a holistic delivery experience for all.
Box 10-5 offers considerations for integrating telehealth into payment and delivery systems.
Investing in Workforce Capacity and Readiness
As the U.S. works toward pandemic recovery, the workforce challenges of coping with COVID-19 will not easily recede. In fact, apart from the dramatically inequitable burden of COVID-19 infection and mortality that certain populations carried, one of the most stark lessons of the pandemic was the burden it placed
on the health system workforce at the frontline and beyond. Workforce capacity shortfalls served to magnify already extreme levels of inequities, moral injury, and burnout.
Shortages have been experienced across all aspects of the health workforce, including among clinicians, emergency personnel, facility intake personnel, public health professionals, community health workers, social service workers, epidemiologists, laboratorians, data analysts, IT experts, supply personnel, public health workers, long-term care/nursing home staff and others. Alongside the shortages of personnel in certain categories, Black individuals have been disproportionally underrepresented in the clinician workforce as a whole, and especially so in backup and surge personnel. Enhanced workforce planning could have helped the health system to reduce fatalities by empowering it to fulfill all necessary pandemic response functions, effectively engage with communities that have been made vulnerable, prepare for surges, mitigate outbreaks in institutional care settings, and facilitate information sharing.
Another workforce challenge that has been growing over recent years (but experienced an acute increase during the pandemic) is burnout. In a survey of nearly 21,000 U.S. clinicians, nearly half of respondents reported experiencing burnout during the pandemic, exacerbating endemic patterns of occupational distress within the clinical workforce (Prasad et al., 2021). The health and wellbeing of the health care workforce was identified as an important need in many of the previous chapters in this Special Publication. The NAM’s 2019 consensus study on the topic presents a systems approach to addressing clinician burnout and promoting professional well-being (NASEM, 2019b). There are numerous opportunities to act across the health care system and address this issue, from streamlining quality reporting to reducing the amount of time dedicated to “desktop medicine.”
The ongoing pandemic experience exposes many priority areas for strengthening the workforce pipeline, including ensuring adequate numbers of critical care clinicians and long-term care personnel, as well as making coordinated investments in education and training across the health care and public health workforce. Meeting these shortfalls will require active collaboration to ensure high quality standards for staffing and adequate reimbursement for the workforce.
As is the case for each of the priority areas in this section, workforce investments should be deployed through the lens of equity, with a focus on correcting the longstanding gaps in representation at all levels of the profession, from trainees to senior leadership.
Box 10-6 presents considerations for investing in workforce capacity and readiness.
Streamlining Innovation Pathways for Biomedical Science
While non-pharmaceutical interventions and prevention measures played an important role in slowing the spread of COVID-19, the rapid development of a portfolio of medical countermeasures—in particular, COVID-19 vaccines and therapeutics—has been critical to driving reductions in morbidity and mortality, especially in the U.S. The pandemic has shown the vital importance of a robust private and public research enterprise dedicated to the public’s health. This enterprise has been supported during COVID-19 by a combination of substantial capital investment, innovative and often unprecedented public-private partnerships, and streamlined regulatory processes. Coordination across the health care system will enable this innovation ecosystem to be harnessed for both existing population health threats (e.g., chronic diseases) and future public health emergencies.
Biomedical advancements require investments in the fundamental science and scientific tools necessary to foster idea generation and innovative practice. This includes improved representation in clinical trials, including communities of color, low-income populations, and older individuals. As research begins to move downstream through clinical and regulatory processes, policymakers and product manufacturers must work together to ensure the careful translation of research findings for public release. The FDA’s 2020 guidance document provides a valuable reference point for the field in ensuring appropriately health literate communications (FDA, 2020b).
COVID-19 has also highlighted the key role of regulation, reimbursement, and communication in advancing biomedical innovation. For example, concerns
around safety and study rigor and the consequences for public confidence illustrate the importance of robust processes for oversight, transparency, and ongoing communication during the R&D process. There are varying levels of public knowledge surrounding the values and processes of the scientific profession, so developing these policies effectively requires that communication and investments in public engagement and scientific education be appropriately tailored (Oreskes, 2019). Doing so can help to facilitate aligned analyses, communication, and expectations around evidence in advance of product development for public health emergencies.
Similarly, clear regulatory pathways for emerging technologies and partnerships between health care payers and health product manufacturers and innovators during emergencies can remove barriers to access. Aligned payment strategies and reimbursement approaches for emerging therapeutics and technologies, streamlined regulatory pathways, and clear communication on the processes will enhance both public confidence and biomedical innovation during future public health crises.
Collaboration across the health system will be critical to addressing each of these issues. For example, alignment between digital health, biomedical research, and health care payers can foster improvements in evidence generation practices to inform product development and future coverage and payment policies. Likewise, partnerships between leaders from patient and family advocacy, communities, care systems, and health product manufacturers and innovators can help identify and fill gaps in representation.
Box 10-7 presents considerations for streamlining pathways for biomedical science.
Strengthening Stewardship of the Health Product Supply Chain
Collaboration to advance new innovations must be paired with partnerships to ensure equitable access to existing products both during inter-pandemic periods and during emergency situations. COVID-19 has exposed supply chain vulnerabilities that must be given high priority for correction. These vulnerabilities carry impacts across the health care system: PPE shortages impact the health care workforce and the American public, the availability of essential medications affects care systems’ ability to serve their patients, and manufacturing capacity affects the global rollout of vaccines. As some of the supply chain shortfalls experienced so acutely in the early phases of the pandemic have begun to be corrected, others are now appearing. For example, the surge in demand for COVID-19 home test kits in response to the omicron variant has resulted in supply shortfalls in many areas.
A more resilient supply chain requires stewardship to identify and mitigate risks, sustainable funding to modernize manufacturing capacity, and informed regulatory elements that align with preparedness aims. Such improvements would benefit all sectors of the health system, improving both the efficiency of day-to-day operations and system-wide preparedness for future emergencies. While the U.S. possesses existing stockpiles and procurement procedures, it would be useful to extend oversight mechanisms to include critical medical products (e.g., devices, consumables) and encompass the entirety of the product life cycle. Collaboration across health system sectors and with policymakers can advance a generational restructuring of the national health care supply chain to ensure the availability of “ever warm” manufacturing capacity and stockpiling.
Modernization of the supply chain requires prioritizing resiliency through new investments in supplies, sourcing, manufacturing, and monitoring of supplies and technology. For example, the FDA has identified COVID-19 as a call to action to advance new manufacturing technologies, practices, and monitoring to improve preparedness for public health emergencies (Hahn and Shah, 2021). Federal leadership and funding can help replenish national stockpiles and incentivize the development of manufacturing capacity that stands prepared to respond and can be rapidly activated in the case of demand.
Box 10-8 presents considerations for enhancing stewardship of the health product supply chain.
Restructuring Health Care Payments to Focus on Outcomes and Population Health
COVID-19 has renewed the impetus to transition away from payment models based purely on volume of service, and move toward those that increasingly reward
the most impactful outcomes. However, the first decade of the value-based care movement has revealed that the sustainable transformation of payment and delivery systems requires collaboration, creativity, and determination across the health care system. With the pandemic experience as a guide, ineffective approaches to paying for health (such as traditional fee-for-service models) should be transformed to reflect non-traditional models (such as re-designed fee-for-service models and others) that improve the effectiveness, efficiency, and equitability of care. Ideally, these payment structures should incentivize the scaling of collaborative activities seen throughout the pandemic, including partnerships between decision-makers from digital health and quality, safety, and standards organizations to drive delivery innovation; and efforts by payers, clinicians, and professional societies to support the transition to new reimbursement arrangements. Continued progress toward value-based payment will require funding for new models, investments in value-based prospective payments, guidance from regulators about the long-term status of pandemic-era reimbursement flexibilities (e.g., telehealth, Hospital at Home), and leadership from payers on foundational questions related to benefit design and administrative processes (e.g., prior authorization).
The pandemic is also a reminder that payment reform is not an end in itself and cannot occur in isolation. Rather, the realignment of financial incentives provides opportunities to drive transformation across the health system. An era of future cross-sector development could include the use of payment reforms to advance public health functions, for example, developing incentive mechanisms for collective action during public health emergencies, changing
reimbursement to improve reporting of laboratory test results and syndromic surveillance, improving clinical trial recruitment, and incentivizing data sharing for research entities (Kadakia et al., 2021; McClellan et al., 2020). Likewise, payers can use the framework of value-based payment to build on pandemic-era pilots geared at addressing individuals’ non-medical needs. As the Accountable Health Communities example demonstrates, these models exemplify the kinds of strategic partnerships envisioned by Public Health 3.0 and illustrate how cross-sector payment reforms can drive meaningful change (HHS OASH, 2016).
Box 10-9 presents considerations for restructuring health care payments to focus on outcomes and population health.
Fostering Communication and Collaboration Across Sectors and Stakeholders
For too long, health and health care in America has been characterized by fragmentation. Each of the opportunities identified above is intended to cut across the health care system, building on the new and collaborative ways of working together that were forged during the pandemic in order to advance system-wide transformation. Improving communication across the health system is intrinsic to this process. With so many sources of information about the dynamics in play, clear and close communication processes and patterns will accelerate the forging, reinforcement, and continual assessment of high priority public messages, allowing for effective messaging and increased trust between and among response partners.
A core lesson from COVID-19 has been that communication tools and strategies must reinforce clear and concise messages to the public, key stakeholders, and partners. To meet this need, communications should be tailored to target audiences. This can be achieved by co-designing messages and strategies by representative stakeholders and structuring communications so as to engage appropriate, targeted messaging strategies and language. Transparency is key–especially surrounding any limits to a message’s contents or generalizability.
New scholarship and collaborative projects sponsored by federal agencies and private and voluntary organizations have sought to provide further guidance on the critical component of communication, especially as it relates to collaboration. As an example, the Public Health Reaching Across Sectors (PHRASES) project led by the de Beaumont Foundation is focused on improving public health’s ability to communicate with other parts of the health care system to advance population health (Castrucci et al., 2020). The pandemic has required extensive communication between care systems and public health, public health and digital health, health payers and product manufacturers, biomedical research, and individuals, families, and communities; it has become evident that persistent and deliberate efforts are required to reduce the structural barriers to such open and continuous communication. Clear communication between partnerships must become the “new normal” in order for health system operations to emerge stronger from the COVID-19 pandemic, although this will not be easy to achieve.
Many aspects of the COVID-19 response, such as the organization of community testing sites and coordination of vaccination campaigns, have relied on collaboration with trusted messengers to reach different audiences. These types of partnerships cannot be transactional, one-off occurrences during emergency situations. Authentic relationships with trusted messengers require sustained engagement over time, and are one of the preconditions for centering the health system on individuals, families, and communities. To augment these strategies and further foster trust, the health system must develop inter-organizational approaches for communication that directly counter misinformation, and are transparent as to sources and resources. By investing in a shared commitment to improve communication and authentic collaboration, the entire health system can be better positioned to work together for transformational change. Box 10-10 presents considerations for fostering communication and collaboration across sectors and stakeholders.
CONCLUSION
Reflecting on the 1918 influenza pandemic, the historian John Barry notes that “the disease has survived in memory more than in any literature.” This is
a shortcoming for future preparedness, for “memory dies with people” (Barry, 2004). To avoid repeating the generational amnesia surrounding the 1918 influenza pandemic, as leaders convened by the NAM from nine sectors of the health delivery system, we are committed to applying the lessons learned from our assessments of the impact of COVID-19, and to doing all we can to foster the actions necessary for health system transformation that enhances the health prospects for present and future generations.
As this chapter makes clear, two narrative threads define the pandemic: a recognition of remarkable responses and advances brought on by the urgency of COVID-19, tempered by the sobering reality of long-standing structural failings and inequities that the pandemic both exposed and exacerbated. The road forward sits at the intersection of these threads, and we must harness the momentum for change to build a more resilient health system. Each chapter of this NAM Special Publication has chronicled the experiences and opportunities relevant to individual health and varying health care sectors, but converting these aspirations into action will require strong collaboration across the system.
This summative chapter underscores the common themes from the individual impact assessments and illustrates the opportunities for partnership. Examples of leadership and change abound: the sacrifices and contributions of health care and public health workers, the development of innovative new biomedical products, the rise of unprecedented flexibilities for reimbursement and regulation, and collaborations across previously unbridgeable siloes to develop a rapid and successful pandemic response. Individual sectors, however, also continue to
encounter a number of common challenges, from issues with data sharing and system capacity to foundational gaps in trust, communication, and health equity. Taken together, these elements frame the opportunities for near- and long-term system-wide transformation. Moving forward, we must center health system incentives and accountability on the outcomes most important to individuals and populations, foster a health manufacturing and supply chain that is ever improving in preparedness and responsiveness, and advance progress toward eliminating health inequities.
The societally disruptive, intense, and too often tragic experiences with the pandemic offer an unprecedented opportunity to build coalitions, embrace aspirational goals, and implement lasting change. Through this Special Publication, its authors are pleased to answer the NAM’s call. As health system leaders and stakeholders, we present an unvarnished picture of the U.S. health system’s successes and failures—and, most importantly, its opportunities—revealed throughout the COVID-19 pandemic to date. We urge others throughout the nation to join with us in working toward the imperative that stands before us, as individuals and as leaders: to emerge stronger by applying what we have learned to build a system committed to the relentless pursuit of equity, efficiency, effectiveness, and continuous learning—and to achieve better health for all.
REFERENCES
Abassi, J. 2020. Social Isolation–the Other COVID-19 Threat in Nursing Homes. JAMA 324(7):619-620. https://doi.org/10.1001/jama.2020.13484.
Agarwal, R., M. Dugas, J. Ramaprasad, and G. Gao. 2021. Socioeconomic Privilege and Political Ideology are Associated with Racial Disparity in COVID-19 Vaccination. PMAS 118(33):e2107873118. https://doi.org/10.1073/pnas.2107873118.
Agarwal, S., and B. D. Sommers. 2020. Insurance Coverage after Job Loss—The Importance of the ACA during the COVID-Associated Recession. New England Journal of Medicine 383(17):1603-1606. https://doi.org/10.1056/NEJMp2023312.
AHIP. 2020. Health Insurance Providers Respond to Coronavirus (COVID-19). Available at: https://www.ahip.org/health-insurance-providers-respond-to-coronavirus-covid-19/ (accessed December 23, 2020).
American Academy of Pediatrics (AAP). 2020. Guidance on Providing Pediatric Well-Care During COVID-19. Available at: https://services.aap.org/en/pages/2019-novel-coronavirus-covid-19-infections/clinical-guidance/guidance-on-providing-pediatric-well-care-during-covid-19/ (accessed March 14, 2022).
Association of American Medical Colleges (AAMC). 2022. The Principles of Trustworthiness. Available at: https://www.aamchealthjustice.org/resources/trustworthiness-toolkit (accessed January 29, 2022).
American Hospital Association (AHA). 2019. Sharing Data, Saving Lives: The Hospital Agenda for Interoperability. Available at: https://www.aha.org/system/files/2019-01/Report01_18_19-Sharing-Data-Saving-Lives_FINAL.pdf (accessed March 14, 2022).
Arangdad, S. R., and A. B. Godfrey. 2021. Understanding the Challenges of Providing Personal Protective Equipment in the United States During COVID-19. Eighteenth Annual Acquisition Research Symposium. May 11-13, 2021. Available at: https://dair.nps.edu/bitstream/123456789/4371/1/SYMAM-21-064.pdf (accessed May 6, 2022).
Artiga, S., J. Kates, J. Michaud, and L. Hill. 2021. Racial Diversity within COVID-19 Vaccine Clinical Trials: Key Questions and Answers. Available at: https://www.kff.org/racial-equity-and-health-policy/issue-brief/racial-diversity-within-covid-19-vaccine-clinical-trials-key-questions-and-answers/ (accessed April 28, 2022).
Association of State and Territorial Health Officials (ASTHO). 2020. New Data on State Health Agencies Shows Shrinking Workforce and Decreased Funding Leading up to the COVID-19 Pandemic. Available at: https://www.astho.org/Press-Room/New-Data-on-State-Health-Agencies-Shows-Shrinking-Workforce-and-Decreased-Funding-Leading-up-to-the-COVID-19-Pandemic/09-24-20/ (accessed October 29, 2020).
ASTHO. 2012. State and Local Health Department Governance Classification System. Available at: https://astho.org/Research/Data-and-Analysis/State-and-Local-Governance-Classification-Tree/ (accessed December 23, 2020).
Baker, D. W. 2020. Trust in Health Care in the Time of COVID-19. JAMA 324(23): 2373-2375. https://doi.org/10.1001/jama.2020.23343.
Bannow, T. 2020. System-owned Health Plans Provide Financial Buffer Against Pandemic. August 1, Modern Healthcare. Available at: https://www.modernhealthcare.com/finance/system-owned-health-plans-provide-financial-buffer-against-pandemic (accessed December 29, 2021).
Barry, J. M. 2004. The Great Influenza: The Story of the Deadliest Pandemic in History. New York: Penguin Books.
Bauchner, H., and P. B. Fontanarosa. 2020. Randomized Clinical Trials and COVID-19: Managing Expectations. JAMA 323(22): 2262-2263. https://doi.org/10.1001/jama.2020.8115.
Beigel, J. H., K. M. Tomashek, L. E. Dodd, A. K. Mehta, B. S. Zingman, A. C. Kalil, E. Hohmann, H. Y. Chu, A. Luetkemeyer, S. Kline, D. Lopez de Castilla,
R. W. Finberg, K. Dierberg, V. Tapson, L. Hseih, T. F. Patterson, R. Paredes, D. A. Sweeney, W. R. Short, G. Touloumi, D. C. Lye, N. Ohmagari, M. Oh, G. M. Ruiz-Palacios, T. Benfield, G. Fatkenheuer, M. G. Kortepeter, R. L. Atmar, C. B. Creech, J. Lundgren, A. G. Babiker, S. Pett, J. D. Neaton, T. H. Burgess, T. Bonnett, M. Green, M. Makowski, A. Osinusi, S. Nayak, H. C. Lane, and the ACCT-1 Study Group Members. 2020. Remdesivir for the Treatment of COVID-19—Final Report. New England Journal of Medicine 383(19):1813-1826. https://doi.org/10.1056/NEJMoa2007764.
Blendon, R. J., J. M. Benson, and J. O. Hero. 2014. Public Trust in Physicians — U.S. Medicine in International Perspective. New England Journal of Medicine 371(17):1570-1572. https://doi.org/10.1056/NEJMp1407373.
Berger, M. L., H. Sox, R. J. Willke, D. L. Brixner, H. Eichler, W. Goettsch, D. Madigan, A. Makady, S. Schneeweiss, R. Tarricone, S. V. Wang, J. Watkins, and C. D. Mullins. 2017. Good Practices for Real-World Data Studies of Treatment and/or Comparative Effectiveness: Recommendations from the Joint ISPOR-ISPE Special Task Force on Real-World Evidence in Health Care Decision Making. Pharmacoepidemiology & Drug Safety 26(9):1003-1039. https://doi.org/10.1002/pds.4297.
Bogaert, K., B. C. Castrucci, E. Gould, K. Sellers, J. P. Leider, C. Whang, and V. Whitten. 2019. The Public Health Workforce Interests and Needs Survey (PH WINS 2017): An Expanded Perspective on the State Health Agency Workforce. Journal of Public Health Management & Practice 25:S16-S25. https://doi.org/10.1097/PHH.0000000000000932.
Bosman, J., and J. McKinley. 2020. One in Five Americans Ordered to Stay Home in Coronavirus Crackdown. March 20, The New York Times. Available at: https://www.nytimes.com/2020/03/20/us/ny-ca-stay-home-order.html (accessed December 22, 2020).
Brothers, W. 2020. A Timeline of COVID-19 Vaccine Development. Available at: https://www.biospace.com/article/a-timeline-of-covid-19-vaccine-development/ (accessed March 14, 2022).
Cameron, E. E., J. B. Nuzzo, J. A. Bell, M. Nalabandian, J. O’Brien, A. League, S. Ravi, D. Meyer, M. Snyder, L. Mullen, and L. Warmbrod. 2019. Global Health Security Index: Building Collective Action and Accountability. Available at: https://www.ghsindex.org/wp-content/uploads/2019/10/2019-Global-Health-Security-Index.pdf (accessed January 7, 2022).
Castrucci, B. C., R. J. Katz, and N. Kendall-Taylor. 2020. Misunderstood: How Public Health’s Inability to Communicate Keeps Communities Unhealthy. Available at: https://www.healthaffairs.org/do/10.1377/forefront.20201006.514216 (accessed January 7, 2022).
Centers for Disease Control and Prevention (CDC). 2022a. United States COVID-19 Cases, Deaths, and Laboratory Testing (NAATs) by State, Territory, and Jurisdiction. Available at: https://covid.cdc.gov/covid-data-tracker/#cases_casesper100klast7days (accessed April 28, 2022).
CDC. 2022b. COVID-19 Vaccinations in the United States. Available at: https://covid.cdc.gov/covid-data-tracker/#vaccinations (accessed April 28, 2022).
CDC. 2021a. Risk for COVID-19 Infection, Hospitalization, and Death by Race/Ethnicity. Available at: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html (accessed August 13, 2021).
CDC. 2021b. Risk for COVID-19 Infection, Hospitalization, and Death by Age Group. Available at: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-age.html (accessed August 13, 2021).
CDC. 2021c. People with Certain Medical Conditions. Available at: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html (accessed December 23, 2020).
CDC. 2021d. Older Adults. Available at: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/older-adults.html (accessed May 14, 2021).
CDC. 2021e. Chronic Diseases in America. Available at: https://www.cdc.gov/chronicdisease/resources/infographic/chronic-diseases.htm (accessed February 13, 2021).
CDC. 2019. Digital Contact Tracing Tools. Available at: https://www.cdc.gov/coronavirus/2019-ncov/php/contact-tracing/contact-tracing-plan/digital-contact-tracing-tools.html (accessed February 3, 2021).
Centers for Medicare & Medicaid Services (CMS). 2021. National Health Spending in 2020 Increases due to Impact of COVID-19 Pandemic. Available at: https://www.cms.gov/newsroom/press-releases/national-health-spending-2020-increases-due-impact-covid-19-pandemic (accessed January 29, 2022).
CMS. 2020a. CMS Develops Additional Code for Coronavirus Lab Tests. Available at: https://www.cms.gov/newsroom/press-releases/cms-develops-additional-code-coronavirus-lab-tests (accessed December 23, 2020).
CMS. 2020b. Physicians and Other Clinicians: CMS Flexibilities to Fight COVID-19. Available at: https://www.ttuhsc.edu/compliance/documents/billing_documents/covid-19-physicians-and-practitioners_april30.pdf (accessed January 7, 2020).
CMS. 2020c. CMS Announces Comprehensive Strategy to Enhance Hospital Capacity Amid COVID-19 Surge. Available at: https://www.cms.gov/newsroom/press-releases/cms-announces-comprehensive-strategy-enhance-hospital-capacity-amid-covid-19-surge (accessed December 23, 2020).
Chastain, D. B., S. P. Osae, A. F. Henao-Martinez, C. Franco-Paredes, J. S. Chastain, and H. N. Young. 2020. Racial Disproportionality in COVID Clinical Trials. New England Journal of Medicine 383(9):e59(1)-e59(3). https://doi.org/10.1056/NEJMp2021971.
Chunara, R., Y. Zhao. J. Chen, K. Lawrence, P. A. Testa, O. Nov, and D. M. Mann. 2021. Telemedicine and Healthcare Disparities: A Cohort Study in a Large Healthcare System in New York City During COVID-19. Journal of the American Medical Informatics Association 28(1):33-41. https://doi.org/10.1093/jamia/ocaa217.
Christopher, G. C., E. Zimmerman, A. Chandra, and L. T. Martin, Editors. 2021. Charting a Course for an Equity-Centered Data System: Recommendations from the National Commission to Transform Public Health Data Systems. Available at: https://www.rwjf.org/en/library/research/2021/10/charting-a-course-for-an-equity-centered-data-system.html (accessed January 6, 2022).
Cohen, A. J., and M. H. Wu. 2020. A Closer Look: The Coronavirus Pandemic and US Federal Investment in Science. Available at: https://www.gspublishing.com/content/research/en/reports/2020/04/29/67c9cada-68a2-48af-b25c-0f5416c0c0c8.html#authors (accessed January 5, 2022).
Collins, F. S., and P. Stoffels. 2020. Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV): An Unprecedented Partnership for Unprecedented Times. JAMA 323(24):2455-2457. https://doi.org/10.1001/jama.2020.8920.
Couzin-Frankel, J. 2021. How Pandemic Pressure is Re-Engineering Clinical Trials. December 8, Science. Available at: https://www.science.org/content/article/how-pandemic-pressure-re-engineering-clinical-trials (accessed January 5, 2022).
Cunningham, P. W. 2020. Medicaid Providers Had to Wait Weeks for Coronavirus Relief Dollars. June 12, The Washington Post. Available at: https://www.washingtonpost.com/news/powerpost/paloma/the-health-202/2020/06/12/the-health-202-medicaid-providers-had-to-wait-weeks-for-coronavirus-relief-dollars/5ee255c188e0fa32f82388f9/ (accessed December 23, 2020).
Curley, B. 2020. Surprise Medical Bills Rising During COVID-19: What to Do If You Get One. December 2, Healthline. Available at: https://www.healthline.com/health-news/surprise-medical-bills-rising-during-covid-19-what-to-do-if-you-get-one (accessed January 30, 2022).
Dawes, D. 2020. Political Determinants of Health. Baltimore: Johns Hopkins University Press.
DeSalvo, K. B., A. Parekh, G. W. Hoagland, A. Dilley, S. Kaiman, M. Hines, and J. Levi. 2019. Developing a Financing System to Support Public Health
Infrastructure. American Journal of Public Health 109(10):1358-1361. https://doi.org/10.2105/AJPH.2019.305214.
Dzau, V. J., D. Kirch, and T. Nasca. 2020. Preventing a Parallel Pandemic—A National Strategy to Protect Clinicians’ Well-Being. New England Journal of Medicine 383(6):513-515. https://doi.org/10.1056/NEJMp2011027.
Eisenberg, M. D., C. L. Barry, C. L. Schilling, and A. Kennedy-Hendricks. 2020. Financial Risk for COVID-19–like Respiratory Hospitalizations in Consumer-Directed Health Plans. American Journal of Preventive Medicine 59(3)445-448. https://doi.org/10.1016/j.amepre.2020.05.008.
European Medicines Agency (EMA). 2020. Points to Consider on Implications of Coronavirus Disease (COVID-19) on Methodological Aspects of Ongoing Clinical Trials. Available at: https://www.ema.europa.eu/en/documents/scientific-guideline/points-consider-implications-coronavirus-disease-covid-19-methodological-aspects-ongoing-clinical_en-0.pdf (accessed January 7, 2022).
Falvey, J. R., T. E. Murphy, T. M. Gill, J. E. Stevens-Lapsley, and L. E. Ferrante. 2020. Home Health Rehabilitation Utilization Among Medicare Beneficiaries Following Critical Illness. Journal of the American Geriatrics Society 68(7):1512-1519. https://doi.org/10.1111/jgs.16412.
Farberman, R. K., M. McKillop, D. A. Lieberman, D. Delgado, C. Thomas, J. Cunningham, and K. McIntyre. 2020. The Impact of Chronic Underfunding on America’s Public Health System: Trends, Risks, and Recommendations, 2020. Available at: https://www.tfah.org/wp-content/uploads/2020/04/TFAH2020PublicHealthFunding.pdf (accessed November 19, 2020).
Federal Register. 2020. Additionally Policy and Regulatory Revisions in Response to the COVID-19 Public Health Emergency. 85 Fed. Reg. 71142 (November 6, 2020). Available at: https://www.federalregister.gov/documents/2020/11/06/2020-24332/additional-policy-and-regulatory-revisions-in-response-to-the-covid-19-public-health-emergency (accessed May 6, 2022).
Frakt, A. 2019. ‘Value’ of CareWas a Big Goal. How Did It Work Out? September 23, The New York Times. Available at: https://www.nytimes.com/2019/09/23/upshot/medicare-health-value-costs.html (accessed December 23, 2020).
Fried, J. E., D. T. Liebers, and E. T. Roberts. 2020. Sustaining Rural Hospitals After COVID-19: The Case for Global Budgets. JAMA 324(2):137-138. https://doi.org/10.1001/jama.2020.9744.
Frisch, M. F., K. W. Scott, and A. Binagwaho. 2021. An Implementation Research Approach to Re-orient Health Supply Chains Toward an Equity Agenda in the COVID-19 Era. Annals of Global Health 87(1):42, 1-6. http://doi.org/10.5334/aogh.3209.
U.S. Food and Drug Administration (FDA). 2022a. Emergency Use Authorization. Available at: https://www.fda.gov/emergency-preparedness-and-response/mcm-legal-regulatory-and-policy-framework/emergency-use-authorization#coviddrugs (accessed April 28, 2022).
FDA. 2022b. COVID-19 Vaccines. Available at: https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/covid-19-vaccines#authorized-vaccines (accessed April 28, 2022).
FDA. 2020a. Coronavirus (COVID-19) Update: December 21, 2020. Available at: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-december-21-2020 (accessed December 23, 2020).
FDA. 2020b. Enhancing the Diversity of ClinicalTrial Populations — Eligibility Criteria, Enrollment Practices, and Trial Designs Guidance for Industry. Available at: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/enhancing-diversity-clinical-trial-populations-eligibility-criteria-enrollment-practices-and-trial (accessed June 8, 2021).
FDA. 2020c. Coronavirus (COVID-19) Update: FDA Issues New Policy to Help Expedite Availability of Diagnostics. Available at: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-issues-new-policy-help-expedite-availability-diagnostics (accessed December 23, 2020).
FDA. 2020d. Statistical Considerations for Clinical Trials During the COVID-19 Public Health Emergency: Guidance for Industry. Available at: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/statistical-considerations-clinical-trials-during-covid-19-public-health-emergency-guidance-industry (accessed March 3, 2021).
Gaines, M. E., A. D. Auleta, and D. M. Berwick. 2020. Changing the Game of Prior Authorization: The Patient Perspective. JAMA 328(8):705-706. https://doi.org/10.1001/jama.2020.0070.
Gallup. 2022. Confidence in Institutions. Available at: https://news.gallup.com/poll/1597/confidence-institutions.aspx (accessed January 29, 2022).
Gebeloff, R., D. Ivory, M. Richtel, M. Smith, K. Yourish, S. Dance, J. Fortiér, E. Yu, and M. Parker. 2020. The Striking Racial Divide in How COVID-19 Has Hit Nursing Homes. September 10, The New York Times. Available at: https://www.nytimes.com/article/coronavirus-nursing-homes-racial-disparity.html (accessed June 1, 2021).
Gee, G. C., and C. L. Ford. 2011. Structural Racism and Health Inequities: Old Issues, New Directions. Du Bois Review: Social Science Research on Race 8(1): 115-132. https://doi.org/10.1017/S1742058X11000130.
Gill, I., and M. Ruta. 2022. Why Global Vaccine Equity is the Prescription for a Full Recovery. Available at: https://www.brookings.edu/blog/future-development/2022/02/11/why-global-vaccine-equity-is-the-prescription-for-a-full-recovery/
development/2022/02/11/why-global-vaccine-equity-is-the-prescription-for-a-full-recovery/ (accessed April 28, 2022).
Gold, M., and C. McLaughlin. 2016. Assessing HITECH Implementation and Lessons: 5 Years Later. The Milbank Quarterly 94(3):654-687. https://dx.doi.org/10.1111%2F1468-0009.12214.
Gondi, S., and D. A. Chokshi. 2020. Financial Stability as a Goal of Payment Reform—A Lesson from COVID-19. JAMA 324(16):1596-1597. https://doi.org/10.1001/jama.2020.18343.
Goodnough, A. and J. Hoffman. 2021. The Wealthy Are Getting More Vaccinations, Even in Poorer Neighborhoods. February 2, The New York Times. Available at: https://www.nytimes.com/2021/02/02/health/white-people-covid-vaccines-minorities.html (accessed June 2, 2021).
Gottlieb, S. 2021. The Need for a US National Clinical Trial Infrastructure in a Public Health Crisis. Available at: https://jamanetwork.com/journals/jama-health-forum/fullarticle/2783677 (accessed January 6, 2022).
Gottlieb, S., and M. McClellan. 2020. Rules for Clinical Trials in a Pandemic. June 21, The Wall Street Journal. Available at: https://www.wsj.com/articles/rules-for-clinical-trials-in-a-pandemic-11592770800 (accessed December 23, 2020).
Gouglas, D., T. T. Le, K. Henderson, A. Klaoudis, T. Danielsen, N. C. Hammersland, J. M. Robinson, P. M. Heaton, and J. A. Røttingen. 2018. Estimating the Cost of Vaccine Development Against Epidemic Infectious Diseases: A Cost Minimisation Study. Lancet Global Health 6(12)e1386-e1396. https://doi.org/10.1016/S2214-109X(18)30346-2.
Grabowski, D. C. 2020. Strengthening Nursing Home Policy for the Postpandemic World: How Can We Improve Residents’ Health Outcomes and Experiences? Available at: https://www.commonwealthfund.org/publications/issue-briefs/2020/aug/strengthening-nursing-home-policy-postpandemic-world (accessed December 23, 2020).
Grabowski, D. C., and K. E. J. Maddox. 2020. Postacute Care Preparedness for COVID-19. JAMA 323(20):2007-2008. https://doi.org/10.1001/jama.2020.4686.
Greene, S., M. Ahmed, P. S. Chua, and C. Grossman, Editors. 2021. Sharing Health Data:The Why, the Will, and the Way Forward. NAM Special Publication. Washington, DC: National Academy of Medicine.
Grogan, C. M., Y. Lin, and M. K. Gusmano. 2021. Health Equity and the Allocation of COVID-19 Provider Relief Funds. American Journal of Public Health 111(4): 628-631. https://doi.org/10.2105/AJPH.2020.306127.
Gunasekeran, D. V., R. M. W. W. Tseng, Y. Tham, and T. Y. Wong. 2021. Applications of Digital Health for Public Health Responses to COVID-19: A Systematic Scoping Review of Artificial Intelligence, Telehealth and Related Technologies. NPJ Digital Medicine 40(2021). https://doi.org/10.1038/s41746-021-00412-9.
Gupta, R., L. Binder, and C. Moriates. 2020. Rebuilding Trust and Relationships in Medical Centers: A Focus on Health Care Affordability. JAMA 324(23)2361-2362. https://doi.org/10.1001/jama.2020.14933.
Hado, E., and L. F. Feinberg. 2020. Amid the COVID-19 Pandemic, Meaningful Communication between Family Caregivers and Residents of Long-Term Care Facilities is Imperative. Journal of Aging & Social Policy 32(4-5):410-415. https://doi.org/10.1080/08959420.2020.1765684.
Hahn, S. M., and A. Shah. 2021. Investing in Advanced Manufacturing to Support Public Health Preparedness. Available at: https://www.fda.gov/news-events/fda-voices/investing-advanced-manufacturing-support-public-health-preparedness (accessed June 8, 2021).
Hahn, S. M., P. Cavazzoni, and P. Marks. 2020. An Update and Behind the Scenes: FDA’s Coronavirus Treatment Acceleration Program. Available at: https://www.fda.gov/news-events/fda-voices/update-and-behind-scenes-fdas-coronavirus-treatment-acceleration-program (accessed December 23, 2020).
Halpern, N. A., S. M. Pastores, J. M. Oropello, and V. Kvetan. 2013. Critical Care Medicine in the United States: Addressing the Intensivist Shortage and Image of the Specialty. Critical Care Medicine 41(12):2754-2761. https://doi.org/10.1097/CCM.0b013e318298a6fb.
Health Care Payment Learning & Action Network (HCPLAN). 2019. APM Measurement Effort. Available at: https://hcp-lan.org/workproducts/apm-infographic-2019.pdf (accessed December 23, 2020).
Health Management Associates (HMA). 2020. COVID-19 Impact on Medicaid, Marketplace, and the Uninsured: May 2020 Update. Available at: https://www.healthmanagement.com/wp-content/uploads/HMA-Updated-Estimates-of-COVID-Impact-on-Health-Insurance-Coverage-May-2020.pdf (accessed January 29, 2022).
Hege, A., S. Lane, T. Spaulding, M. Sugg, and L. S. Iyer. 2021. County-Level Social Determinants of Health and COVID-19 in Nursing Homes, United States, June 1, 2020—January 31, 2021. Public Health Reports 137(1):137-148. https://doi.org/10.1177/00333549211053666.
Helfand, B. K. I., M. Webb, S. L. Gartaganis, L. Fuller, C. S. Kwon, and S. K. Inouye. 2020. The Exclusion of Older Persons from Vaccine and Treatment Trials for Coronavirus Disease 2019—Missing the Target. JAMA Internal Medicine 180(11):1546-1549. https://doi.org/10.1001/jamainternmed.2020.5084.
Hentze, I. 2020. COVID-19: Occupational Licensing During Public Emergencies. Available at: https://www.ncsl.org/research/labor-and-employment/covid-19-occupational-licensing-in-public-emergencies.aspx (accessed December 23, 2020).
Herper, M., and E. Riglin. 2020. Data Show Panic and Disorganization Dominate the Study of COVID-19 Drugs. July 6, STAT. Available at: https://www.statnews.com/2020/07/06/data-show-panic-and-disorganization-dominate-the-study-of-covid-19-drugs/ (accessed December 23, 2020).
Holshue, M. L., C. DeBolt, S. Lindquist, K. H. Lofy, J. Wiesman, H. Bruce, C. Spitters, K. Ericson, S. Wilkerson, A. Tural, G. Diaz, A. Cohn, L. Fox, A. Patel, S. I. Gerber, L. Kim, S. Tong, X. Lu, S. Lindstorm, M. A. Pallansch, W. C. Weldon, H. M. Biggs, T. M. Uyeki, and S. K. Pillai. 2020. First Case of 2019 Novel Coronavirus in the United States. New England Journal of Medicine 382(10): 929-936. https://doi.org/10.1056/NEJMoa2001191.
Horwitz, L. I., C. Chang, H. N. Arcilla, and J. R. Knickman. 2020. Quantifying Health Systems’ Investment in Social Determinants of Health, By Sector, 2017–19. Health Affairs 39(2):192-198. https://doi.org/10.1377/hlthaff.2019.01246.
Huff, C. 2020. COVID-19: Americans Afraid to Seek Treatment Because of the Steep Cost of Their High Deductible Insurance Plans. BMJ 371(m3860). https://doi.org/10.1136/bmj.m3860.
Hughes, M. M., A. Wang, M. K. Grossman, E. Pun, A. Whiteman, L. Deng, E. Hallisey, J. D. Sharpe, E. N. Ussery, S. Stokley, T. Musial, D. L. Weller, B. P. Murthy, L. Reynolds, L. Gibbs-Scharf, L. Harris, M. D. Ritchey, and R. L. Toblin. 2021. County-Level COVID-19 Vaccination Coverage and Social Vulnerability – United States, December 14, 2020—March 1, 2021. CDC Morbidity and Mortality Weekly Report 70(12):431-436. https://doi.org/10.15585/mmwr.mm7012e1.
Ikram, U., S. Gallani, J. F. Figueroa, and T. W. Feeley. 2020. Protecting Vulnerable Older Patients During the Pandemic. NEJM Catalyst. https://catalyst.nejm.org/doi/full/10.1056/CAT.20.0404.
International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH). 2019. ICH E9 Statistical Principals for Clinical Trials. Available at: https://www.ema.europa.eu/en/ich-e9-statistical-principles-clinical-trials (accessed August 18, 2020).
Institute of Medicine (IOM). 2013. Best Care at Lower Cost:The Path to Continuously Learning Health Care in America. Washington, DC: The National Academies Press. https://doi.org/10.17226/13444.
IOM. 2012. For the Public’s Health: Investing in a Healthier Future. Washington, DC: National Academies Press. https://doi.org/10.17226/13268.
IOM. 2002. The Future of the Public’s Health in the 21st Century. Washington, DC: The National Academies Press. https://doi.org/10.17226/10548.
IOM. 1988. The Future of Public Health. Washington, DC: The National Academies Press. https://doi.org/10.17226/1091.
Johnson, C. Y. 2021. Serendipity and Foresight Prepared the World to Fight the Coronavirus. October 1, The Washington Post. Available at: https://www.washingtonpost.com/health/2021/10/01/barney-graham-covid-vaccines/ (accessed January 6, 2022).
Johns Hopkins University & Medicine (JHU). 2022. Coronavirus Resource Center. Available at: https://coronavirus.jhu.edu/us-map (accessed December 22, 2020).
Kadakia, K. T., A. L. Beckman, and A. S. Kesselheim. 2021. Redeploying COVID-19 Payment Reforms for Biomedical Innovation: A New Opportunity for the Value Movement. NEJM Catalyst. https://catalyst.nejm.org/doi/full/10.1056/CAT.20.0617.
Kaiser Family Foundation (KFF). 2022a. Primary Care Health Professional Shortage Areas. Available at: https://www.kff.org/other/state-indicator/primary-care-health-professional-shortage-areas-hpsas/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D (accessed November 30, 2020).
KFF. 2022b. Does the Public Want to Get a COVID-19 Vaccine? When? Available at: https://www.kff.org/coronavirus-covid-19/dashboard/kff-covid-19-vaccine-monitor-dashboard/ (accessed December 23, 2020).
Kaiser Health News (KHN), The Guardian. 2021. Lost on the Frontline: Explore the Database. April 7, Kaiser Health News. Available at: https://khn.org/news/lost-on-the-frontline-explore-the-database/ (accessed June 7, 2021).
Kaufman Hall. 2021. National Hospital Flash Report: January 2021. Available at: https://www.kaufmanhall.com/sites/default/files/2021-01/nationalhospitalflashreport_jan.-2021_final.pdf (accessed March 13, 2022).
Kearney, A., L. Hamel, M. Stokes, and M. Brodie. 2021. Americans’ Challenges with Health Care Costs. Available at: https://www.kff.org/health-costs/issue-brief/americans-challenges-with-health-care-costs/ (accessed April 26, 2022).
Keith, K. 2020. New Guidance To Implement COVID-19 Coverage Requirements And More. Available at: https://www.healthaffairs.org/do/10.1377/forefront.20200413.78972/full/ (accessed January 7, 2020).
Khalil, L., M. Leary, N. Rouphael, I. Ofotokun, P. A. Rebolledo, and Z. Wiley. 2022. Racial and Ethnic Diversity in SARS-CoV-2 Vaccine Clinical Trials Conducted in the United States. Vaccines 10(2):290. https://dx.doi.org/10.3390%2Fvaccines10020290.
Khullar, D., A. M. Bond, and W. L. Schpero. 2020a. COVID-19 and the Financial Health of US Hospitals. JAMA 323(21):2127-2128. https://doi.org/10.1001/jama.2020.6269.
Khullar, D., G. Darien, and D. L. Ness. 2020b. Patient Consumerism, Healing Relationships, and Rebuilding Trust in Health Care. JAMA 324(23):2359-2360. https://doi.org/10.1001/jama.2020.12938.
Kim, S. R., M. Vann, L. Bronner, G. Manthey. 2020. Which Cities Have the Biggest Racial Gaps in COVID-19 Testing Access? Available at: https://fivethirtyeight.com/features/white-neighborhoods-have-more-access-to-covid-19-testing-sites/ (accessed December 23, 2020).
Kiptanui, Z., S. Ghosh, S. Ali, K. Desai, and I. Harris. 2021. Transparency, Health Equity, and Strategies in State-Based Protocols for Remdesivir Allocation and Use. PLoS ONE 16(10):e0257648. https://doi.org/10.1371/journal.pone.0257648.
Kliff, S. 2021. How to Avoid a Surprise Bill for Your Coronavirus Test. August 18, The New York Times. Available at: https://www.nytimes.com/2021/08/18/upshot/coronavirus-test-bill-cost.html (accessed on January 30, 2022).
Kliff, S., and M. Sanger-Katz. 2020. Bottleneck for U.S. Coronavirus Response: The Fax Machine. July 13, The New York Times. Available at: https://www.nytimes.com/2020/07/13/upshot/coronavirus-response-fax-machines.html (accessed January 11, 2022).
Koller, C. F., and A. Shih. 2020. Payer Actions Can Help Sustain Primary Care During and After COVID-19. Available at: https://www.milbank.org/2020/04/payer-actions-can-help-sustain-primary-care-during-and-after-covid-19/ (accessed December 23, 2020).
Konetzka, R. T., K. Yan, and R. M. Werner. 2020. Two Decades of Nursing Home Compare: What Have We Learned? Medical Care Research and Review 78(4):295-310. https://doi.org/10.1177/1077558720931652.
Krieger, N., C. Testa, W. P. Hanage, and J. T. Chen. 2020. US Racial and Ethnic Data for COVID-19 Cases: Still Missing in Action. The Lancet 396(10261):7-13. https://doi.org/10.1016/S0140-6736(20)32220-0.
Kunz, C. U., S. Jörgens, F. Bretz, N. Stallard, K. Van Lancker, D. Xi, S. Zohar, C. Gerlinger and T. Friede. 2020. Clinical trials impacted by the COVID-19 pandemic: Adaptive designs to the rescue? Statistics in Biopharmaceutical Research 12(4):461-477. https://doi.org/10.1080/19466315.2020.1799857.
Kwai, I., and E. Peltier. 2021. ‘What’s the Point?’ Young People’s Despair Deepens as COVID-19 Crisis Drags On. February 14, The New York Times. Available at: https://www.nytimes.com/2021/02/14/world/europe/youth-mental-healthcovid.html (accessed June 1, 2021).
LaFraniere, S., K. Thomas, N. Weiland, D. Gelles, S. G. Stolberg, and D. Grady. 2020. Politics, Science, and the Remarkable Race for a Coronavirus Vaccine. November 21, The New York Times. Available at: https://www.nytimes.com/2020/11/21/us/politics/coronavirus-vaccine.html (accessed December 23, 2020).
Leavitt, M. O., M. McClellan, S. D. DeVore, E. Fisher, R. J. Gilfillan, H. S. Lieber, R. Merkin, J. Rideout, and K. J. Thiry. 2016. Competencies and Tools to Shift
Payments from Volume to Value: A Vital Direction for Health and Health Care. NAM Perspectives. Discussion Paper. https://doi.org/10.31478/201609o.
Leeb, R. T., R. H. Bitsko, L. Radhakrishnan, P. Martinez, R. Njai, and K. M. Holland. 2020. Mental Health–Related Emergency Department Visits Among Children Aged <18 Years During the COVID-19 Pandemic — United States, January 1–October 17, 2020. Morbidity and Mortality Weekly Report 69(45):1675-1680. https://www.cdc.gov/mmwr/volumes/69/wr/pdfs/mm6945a3-H.pdf.
Lopez, E. 2020. The Critical Care Workforce and COVID-19: A State by State Analysis. Available at: https://www.kff.org/coronavirus-covid-19/issue-brief/the-critical-care-workforce-and-covid-19-a-state-by-state-analysis/ (accessed January 30, 2022).
Llupia, A., A. Garcia-Basteiro, and J. Puig. 2020. Still Using MS Excel? Implementation of the WHO Go. Data Software for the COVID-19 Contact Tracing. Health Science Reports 3(2):e164. https://doi.org/10.1002/hsr2.164.
Lumpkin, J. R., and A. Wiesenthal. 2020. A Digital Bridge to Real-Time COVID-19 Data. Available at: https://www.healthaffairs.org/do/10.1377/forefront.20200729.517619/full/ (accessed January 10, 2022).
Lunden, I. 2020. Twitter Prioritizes Blue-Check Verifications to Confirm Experts on COVID-19 and the Novel Coronavirus. Available at: https://techcrunch.com/2020/03/21/twitter-prioritizes-blue-check-verifications-to-confirm-experts-on-covid-19-and-the-novel-coronavirus/ (accessed December 23, 2020).
Lyons, K. 2020. CDC Uses Microsoft Healthcare Chatbot Service to Create Coronavirus Symptom Checker. March 21, The Verge. Available at: https://www.theverge.com/2020/3/21/21189227/cdc-microsoft-chatbot-coronavirus-symptom-checker (accessed February 2, 2021).
Maani, N., and S. Galea. 2020. COVID-19 and Underinvestment in the Health of the US Population. The Milbank Quarterly 98(2):239-249. https://doi.org/10.1111/1468-0009.12462.
Magrabi, F., E. Ammenwerth, J. B. McNair, N. F. D. Keizer, H. Hyppönen, P. Nykänen, M. Rigby, P. Scott, T. Vehko, Z. S. Wong, and A. Georgiou. 2019. Artificial Intelligence in Clinical Decision Support: Challenges for Evaluating AI and Practical Implications. Thieme Medical Publishers 28(01):128-134. https://doi.org/10.1055/s-0039-1677903.
Maliha, G., M. Adelberg, and K. H. Chaiyachati. 2021. Minding the Access Gap: Addressing Both the Digital and Transportation Divides to Improve Outcomes. Available at: https://doi.org/10.1377/forefront.20211105.682777 (accessed March 14, 2022).
Maxmen, A. 2020. Why the United States Is Having a Coronavirus Data Crisis. August 26, Nature. Available at: https://www.nature.com/articles/d41586-020-02478-z (accessed January 10, 2022).
McClellan, M., F. Mostashari, and T. Barker. 2020. Health Care Payment to Support COVID-19 Detection and Containment. Available at: https://healthpolicy.duke.edu/sites/default/files/2020-06/health_care_payment_to_support_covid-19_detection_and_containment_final.pdf (accessed June 8, 2021).
McGarry, B. E., D. C. Grabowski, and M. L. Barnett. 2020. Severe Staffing and Personal Protective Equipment Shortages Faced by Nursing Homes During the COVID-19 Pandemic. Health Affairs 39(10):1812-1821. https://doi.org/10.1377/hlthaff.2020.01269.
Medicare Payment Advisory Commission (MEDPAC). 2017. An Overview of the Medical Device Industry. Available at: http://www.medpac.gov/docs/default-source/reports/jun17_ch7.pdf (accessed August 18, 2020).
Meyer, R. D., B. Ratitch, M. Wolbers, O. Marchenko, H. Quan, D. Li, C. Fletcher, X. Li, D. Wright, Y. Shentu, S. Englert, W. Shen, J. Dey, T. Liu, M. Zhou, N. Bohidar, P. Zhao, and M. Hale. 2020. Statistical Issues and Recommendations for Clinical Trials Conducted During the COVID-19 Pandemic. Statistics in Biopharmaceutical Research 12(4): 399-411. https://doi.org/10.1080/19466315.2020.1779122.
Miri, A. and D. P. O’Neill. 2020. Accelerating Data Infrastructure for COVID-19 Surveillance and Management. Available at: https://www.healthaffairs.org/do/10.1377/forefront.20200413.644614/full/ (accessed January 10, 2022).
Murphy, B. 2020. Applications To Medical School Up Big. Is It The “Fauci Effect”? Available at: https://www.ama-assn.org/residents-students/preparing-medical-school/applications-medical-school-big-it-fauci-effect (accessed December 23, 2020).
Murthy, B. P., N. M. Molinari, T. T. LeBlanc, S. J. Vagi, and R. N. Avchen. 2017. Progress in Public Health Emergency Preparedness—United States, 2001–2016. American Journal of Public Health 107(S2):S180-S185. https://doi.org/10.2105/AJPH.2017.304038.
Naidoo, P., C. Bouharati, V. Rambiritch, N. Jose, S. Karamchand, R. Chilton, and R. Leisegang. 2021. Real-world Evidence and Product Development: Opportunities, Challenges and Risk Mitigation. Wiener Klinische Wochenschrift 133:840-846. https://doi.org/10.1007/s00508-021-01851-w.
National Academy of Medicine (NAM). 2021. The Learning Health System Series. Available at: https://nam.edu/programs/value-science-driven-health-care/learning-health-system-series/ (accessed June 8, 2021).
National Academies of Sciences, Engineering, and Medicine (NASEM). 2022. The National Imperative to Improve Nursing Home Quality: Honoring our Commitment to Residents, Families, and Staff. Washington, DC: The National Academies Press. https://doi.org/10.17226/26526.
NASEM. 2019a. Integrating Social Care into the Delivery of Health Care: Moving Upstream to Improve the Nation’s Health. Washington, DC: The National Academies Press. https://doi.org/10.17226/25467.
NASEM. 2019b. Taking Action Against Clinician Burnout: A Systems Approach to Professional Well-Being. Washington, DC: The National Academies Press. https://doi.org/10.17226/25521.
NASEM. 2017. Communities in Action: Pathways to Health Equity. Washington, DC: The National Academies Press. https://doi.org/10.17226/24624.
National Institutes of Health (NIH). 2021. COVID-19 Therapeutics Prioritized for Testing in Clinical Trials. Available at: https://www.nih.gov/research-training/medical-research-initiatives/activ/covid-19-therapeutics-prioritized-testing-clinical-trials (accessed January 5, 2022).
NIH. 2020. NIH Community Engagement Alliance (CEAL). Available at: https://covid19community.nih.gov/ (accessed March 9, 2022).
National Library of Medicine (NLM). 2022. Clinical Trials.gov – Search Results: Interventional Studies | COVID-19. Available at: https://clinicaltrials.gov/ct2/results?cond=COVID-19&age_v=&gndr=&type=Intr&rslt=&Search=Apply (accessed April 28, 2022).
Navathe, A. S., and J. M. Liao. 2020. After COVID-19, a Payment Policy Reboot: Three Lessons from the Pandemic on How to Improve Value-Based Payment. Available at: https://www.healthaffairs.org/do/10.1377/forefront.20200805.905205/full/ (accessed January 10, 2020).
Nephew, L. D. 2021. Accountability in Clinical Trial Diversity: The Buck Stops Where? EClinicalMedicine 36(2021):100906. https://doi.org/10.1016/j.eclinm.2021.100906.
Newman, A. 2020. What N. Y. C. Sounds Like Every Night At 7. April 10, The New York Times. Available at: https://www.nytimes.com/interactive/2020/04/10/nyregion/nyc-7pm-cheer-thank-you-coronavirus.html (accessed December 23, 2020).
Normand, S. T. 2021. The RECOVERY Platform. New England Journal of Medicine 384(8):757-758. https://doi.org/10.1056/NEJMe2025674.
North, C. M., M. L. Dougan, and C. A. Sacks. 2020. Improving Clinical Trial Enrollment – In the COVID-19 Era and Beyond. New England Journal of Medicine 383(15):1406-1408. https://doi.org/10.1056/NEJMp2019989.
Ochieng, N., P. Chidambaram, and M. Musumeci. 2022. Nursing Facility Staffing Shortages During the COVID-19 Pandemic. Available at: https://www.kff.org/coronavirus-covid-19/issue-brief/nursing-facility-staffing-shortages-during-the-covid-19-pandemic/ (accessed April 29, 2022).
Okoro, O., J. Kennedy, G. Simmons, E. C. Vosen, K. Allen, D. Singer, D. Scott, and R. Roberts. 2021. Exploring the Scope and Dimensions of Vaccine Hesitancy
and Resistance to Enhance COVID-19 Vaccination in Black Communities. Journal of Racial and Ethnic Health Disparities (2021). https://doi.org/10.1007/s40615-021-01150-0.
Oreskes, N. 2019. Science Isn’t Always Perfect—But We Should Still Trust It. October 24, Time. Available at: https://time.com/5709691/why-trust-science/ (accessed January 11, 2022).
Peiffer-Smadja, N., R. Maatoug, F. X. Lescure, E. D’Ortenzio, J. Pineau, and J. R. King. 2020. Machine Learning for COVID-19 Needs Global Collaboration and Data-Sharing. Nature Machine Intelligence 2(6):293–294. https://doi.org/10.1038/s42256-020-0181-6.
Perissinotto, C. M., I. S. Cenzer, and K. E. Covinsky. 2012. Loneliness in Older Persons:A Predictor of Functional Decline and Death. Archives of Internal Medicine 172(14):1078-1084. https://doi.org/10.1001/archinternmed.2012.1993.
Perrin, P. B., B. S. Pierce, and T. R. Elliott. 2020. COVID-19 and Telemedicine: A Revolution in Healthcare Delivery is at Hand. Health Science Reports 3(2):e166. https://doi.org/10.1002/hsr2.166.
Pichai, S. 2020. Coronavirus: How We’re Helping. Available at: https://blog.google/inside-google/company-announcements/coronavirus-covid19-response/ (accessed August 20, 2021).
Prasad, K., C. McLoughlin, M. Stillman, S. Poplau, E. Goelz, S. Taylor, N. Nankivil, R. Brown, M. Linzer, K. Cappeluci, M. Barbouche, and C. A. Sinsky. 2021. Prevalence and Correlates of Stress and Burnout Among U.S. Healthcare Workers During the COVID-19 Pandemic:A National Cross-Sectional Survey Study. EClinicalMedicine 35. https://doi.org/10.1016/j.eclinm.2021.100879.
Reagan-Udall Foundation for the FDA, Friends of Cancer Research. 2022. COVID-19 Evidence Accelerator. Available at: https://evidenceaccelerator.org/ (accessed January 5, 2022).
Roberts, E. T., and A. Mehrotra. 2020. Assessment of Disparities in Digital Access Among Medicare Beneficiaries and Implications for Telemedicine. JAMA Internal Medicine 180(10):1386-1389. https://doi.org/10.1001/jamainternmed.2020.2666.
Roiland, R., M. Japinga, E. Singletary, I. Sharma, J. Gonzalez-Smith, G. Wang, J. Jacobs, W. Bleser, R. Saunders, and M. McClellan. 2020. Value-Based Care in the COVID-19 Era: Enabling Health Care Response and Resilience. Available at: https://healthpolicy.duke.edu/sites/default/files/2020-07/best_practices_brief_final.pdf (accessed December 23, 2020).
Rothwell, J., and S. Desai. 2020. How Misinformation is Distorting COVID Policies and Behaviors. Available at: https://www.brookings.edu/research/how-misinformation-is-distorting-covid-policies-and-behaviors/ (accessed February 20, 2021).
Rubin, R. 2020. COVID-19’s Crushing Effects on Medical Practices, Some of Which Might Not Survive. JAMA 324(4):321-323. https://doi.org/10.1001/jama.2020.11254.
Saelee, R., E. Zell, B. P. Murthy, P. Castro-Roman, H. Fast, L. Meng, L. Shaw, L. Gibbs-Scharf, T. Chorba, L. Q. Harris, and N. Murthy. 2022. Disparities in COVID-19 Vaccination Coverage Between Urban and Rural Counties – United States, December 14, 2020–January 31, 2022. Morbidity and Mortality Weekly Report 71(9):335-340. http://dx.doi.org/10.15585/mmwr.mm7109a2.
Santoli, J. M., M. C. Lindley, M. B. DeSilva, E. O. Kharbanda, M. F. Daley, L. Galloway, J. Gee, M. Glover, B. Herring, Y. Kang, P. Lucas, C. Noblit, J. Tropper, T. Vogt, and E. Weintraub. 2020. Effects of the COVID-19 Pandemic on Routine Pediatric Vaccine Ordering and Administration. Morbidity and Mortality Weekly Report 69(19):591-593. http://dx.doi.org/10.15585/mmwr.mm6919e2.
Schmidt, H., D. E. Roberts, and N. D. Eneanya. 2021. Rationing, Racism and Justice: Advancing the Debate around ‘Colourblind’ COVID-19 Ventilator Allocation. Journal of Medical Ethics 2021:1-5. https://doi.org/10.1136/medethics-2020-106856.
Servick, K. 2020. ‘Huge Hole’ in COVID-19 Testing Data Makes It Harder to Study Racial Disparities. July 10, ScienceInsider. Available at: https://www.sciencemag.org/news/2020/07/huge-hole-covid-19-testing-data-makes-it-harder-study-racial-disparities (accessed March 14, 2022).
Shanafelt, T., J. Ripp, and M. Trockel. 2020. Understanding and Addressing Sources of Anxiety Among Health Care Professionals During the COVID-19 Pandemic. JAMA 323(21):2133-2134. https://doi.org/10.1001/jama.2020.5893.
Shrank, W. H., N. DeParle, S. Gottlieb, S. H. Jain, P. Orszag, B. W. Powers, and G. R. Wilensky. 2021. Health Costs and Financing: Challenges and Strategies for a New Administration. Health Affairs 40(2)235-242. https://doi.org/10.1377/hlthaff.2020.01560.
Shrank, W. H., T. L. Rogstad, and N. Parekh. 2019. Waste in the US Health Care System: Estimated Costs and Potential for Savings. JAMA 322(15):1501-1509. https://doi.org/10.1001/jama.2019.13978.
Stechmiller, J. K. 2002. The Nursing Shortage in Acute and Critical Care Settings. AACN Advanced Critical Care 13(4):577-584. https://doi.org/10.1097/00044067-200211000-00011.
Stolberg, S. G., and S. LaFraniere. 2021. With Omicron, U.S. Testing Capacity Faces Intense Pressure. December 17, The New York Times. Available at: https://www.nytimes.com/2021/12/17/us/politics/us-covid-tests-omicron.html (accessed January 6, 2022).
Socker, E., A. Spratt, and M. E. Miller. 2020. Distributing Provider Financial Aid to Create a More Efficient, Equitable System. Available at: https://doi.org/10.1377/forefront.20201006.416650 (accessed March 14, 2022).
Suran, M. 2021. Why Parents Still Hesitate to Vaccinate Their Children Against COVID-19. JAMA 327(1):23-25. https://doi.org/10.1001/jama.2021.21625.
The New York Times. 2021. Nearly One-Third of U.S. Coronavirus Deaths Are Linked to Nursing Homes. June 1, The New York Times. Available at: https://www.nytimes.com/interactive/2020/us/coronavirus-nursing-homes.html (accessed March 14, 2022).
Tikkanen, R., and M. K. Abrams. 2020. U.S. Health Care from a Global Perspective, 2019: Higher Spending, Worse Outcomes? Available at: https://www.commonwealthfund.org/publications/issue-briefs/2020/jan/us-health-care-global-perspective-2019 (accessed December 23, 2020).
Tromberg, B. J., T. A. Schwetz, E. J. Pérez-Stable, R. J. Hodes, R. P. Woychik, R. A. Bright, R. L. Fleurence, and F. S. Collins. 2020. Rapid Scaling Up of COVID-19 Diagnostic Testing in the United States — The NIH RADx Initiative. New England Journal of Medicine 383(11):1071-1077. https://doi.org/10.1056/NEJMsr2022263.
Trump White House. 2020. Remarks by President Trump on Vaccine Development. Available at: https://trumpwhitehouse.archives.gov/briefings-statements/remarks-president-trump-vaccine-development/ (accessed December 22, 2020).
Tyler, D., M. Hunter, N. Mulmule, and K. Porter. 2021. COVID-19 Intensifies Home Care Workforce Challenges. Available at: https://aspe.hhs.gov/reports/covid-19-intensifies-home-care-workforce-challenges (accessed January 30, 2022).
U.S. Department of Health and Human Services (HHS). 2020. Determination that a Public Health Emergency Exists. Available at: https://www.phe.gov/emergency/news/healthactions/phe/Pages/2019-nCoV.aspx (accessed January 10, 2022).
U.S. Department of Health and Human Services Office of the Assistant Secretary for Health (HHS OASH). 2016. Public Health 3.0: A Call to Action to Create a 21st Century Public Health Infrastructure. Available at: https://www.healthypeople.gov/sites/default/files/Public-Health-3.0-White-Paper.pdf (accessed June 8, 2021).
Van Dorn, A. 2020. COVID-19 and Readjusting Clinical Trials. The Lancet 396(10250): 523-524. https://doi.org/10.1016/S0140-6736(20)31787-6.
Vandenberg, O., D. Martiny, O. Rochas, A. van Belkum, and Z. Kozlakidis. 2020. Considerations for Diagnostic COVID-19 Tests. Nature Reviews Microbiology 19: 171-183. https://doi.org/10.1038/s41579-020-00461-z.
Weber, E., S. J. Miller, V. Astha, T. Janevic, and E. Benn. 2020. Characteristics of Telehealth Users in NYC for COVID-Related Care During the Coronavirus
Pandemic. Journal of the Medical Informatics Association 27(12):1949-1954. https://doi.org/10.1093/jamia/ocaa216.
Wee, S. L., and V. Wang. 2020. China Grapples With Mystery Pneumonia-Like Illness. January 6, The New York Times. Available at: https://www.nytimes.com/2020/01/06/world/asia/china-SARS-pneumonialike.html (accessed December 22, 2020).
Weixel, N. 2020. Shortage of Medical Gear Sparks Bidding War Among States. March 30, The Hill. Available at: https://thehill.com/homenews/state-watch/490263-shortage-of-medical-gear-sparks-bidding-war-among-states (accessed January 11, 2022).
World Health Organization (WHO). 2022. WHO Coronavirus (COVID-19) Dashboard. Available at: https://covid19.who.int/ (accessed April 28, 2022).
WHO. 2021. Statement for Healthcare Professionals: How COVID-19 Vaccines are Regulated for Safety and Effectiveness. Available at: https://www.who.int/news/item/11-06-2021-statement-for-healthcare-professionals-how-covid-19-vaccines-are-regulated-for-safety-and-effectiveness (accessed April 28, 2022).
WHO. 2020. Managing the COVID-19 Infodemic: Promoting Healthy Behaviours and Mitigating the Harm from Misinformation and Disinformation. Available at: https://www.who.int/news/item/23-09-2020-managing-the-covid-19-infodemic-promoting-healthy-behaviours-and-mitigating-the-harm-from-misinformation-and-disinformation (accessed December 23, 2020).
Xiang, D., and L. S. Lehmann. 2021. Confronting the Misinformation Pandemic. Health Policy and Technology 10(3). https://doi.org/10.1016/j.hlpt.2021.100520.
AUTHOR INFORMATION
Amy Abernethy, MD, PhD, is President of Clinical Research Business at Verily. Jeffrey Balser, MD, PhD, is President and CEO of Vanderbilt University Medical Center. Carolyn Clancy, MD, is the Assistant Undersecretary for Health, Discovery, Education and Affiliate Networks (DEAN) at the Department of Veterans Affairs. Karen DeSalvo, MD, MPH, MSc, is adjunct Professor of Medicine and Population Health at Dell Medical School, The University of Texas at Austin and former Acting Assistant Secretary for Health and National Coordinator for Health Information Technology. Kate Goodrich, MD, MHS, is the Senior Vice President for Enterprise Clinical Management at Humana. Robert Hughes, PhD, is former President and CEO at the Missouri Foundation for Health. Frederick Isasi, JD, MPH, is president and CEO at Families USA. Peter Lee, PhD, is Corporate Vice President of Research and Incubations at Microsoft. James Madara, MD, is CEO and Executive Vice President at the
American Medical Association. Mathai Mammen, MD, PhD, is Executive Vice President, Pharmaceuticals R&D, Johnson & Johnson. Mark McClellan, MD, PhD, is Robert J. Margolis Professor of Business, Medicine, and Policy and Director of the Duke-Margolis Center for Health Policy at Duke University. Suzanne Miyamoto, PhD, RN, is CEO at the American Academy of Nursing. Vasant Narasimhan, MD, MPP, is Chief Executive Officer of Novartis. Mary Naylor, PhD, RN, is director at the NewCourtland Center for Transitions and Health at the University of Pennsylvania School of Nursing. Rahul Rajkumar, MD, JD, is COO of Care Solutions at Optum. Jaewon Ryu, MD, JD, is President and CEO of Geisinger. David Skorton, MD, is president and CEO at the Association of American Medical Colleges.
ACKNOWLEDGMENTS
The co-authors would like to acknowledge Nakela Cook, MD, MPH, Patient-Centered Outcomes Research Institute (PCORI), and Michael Lauer, MD, National Institutes of Health (NIH) Office of Extramural Research for their suggestions and contributions, as well as the following individuals for their comments and edits: Laura Adams, MS, National Academy of Medicine; Mahnoor Ahmed, MEng, National Academy of Medicine; Ayodola Anise, MHS, National Academy of Medicine; Laurie Burns, PhD, Janssen at Johnson & Johnson; Michael Cocchiola, MPA, National Academy of Medicine; Kushal Kadakia, MSc, MSt, Harvard Medical School; Jennifer Lee, MD, MPH, National Academy of Medicine; Joseph McGowan, MA, Novartis; Anaeze Offodile, MD, MPH, MD Anderson Cancer Center; and Asia Williams, MPH, National Academy of Medicine.
This paper benefited from the thoughtful input of Julie Morita, Robert Wood Johnson Foundation; and Kara Odom Walker, Nemours Children’s Health.
CONFLICT OF INTEREST DISCLOSURES
Amy Abernethy discloses receiving personal fees from Flatiron Health (Roche Group), AthenaHealth, SignalPath, and CareDx no later than January 2019. Jeffrey Balser discloses that he receives compensation as a member of the board of Varian Medical Systems and is an unpaid member of the board for the Center for Medical Interoperability. Mathai Mammen discloses that his employer received funding from the U.S. government to develop a COVID-19 vaccine; that his employer collaborated with BCG; that his employer’s COVID-19 vaccine has received Emergency Use Authorization in the U.S., European Union, and
other countries; and that Johnson & Johnson is a multi-faceted company that has pharmaceutical, consumer, and medical devices businesses. Mark McClellan discloses that he is an independent director on the boards of Johnson & Johnson, Cigna, Alignment Healthcare, and PrognomIQ; co-chairs the Guiding Committee for the Health Care Payment Learning and Action Network; and receives fees for serving as an advisor for Arsenal Capital Partners, Blackstone Life Sciences, and MITRE. Vasant Narasimhan discloses that his employer is currently undertaking an internal drug discovery program toward a pan-Coronavirus Mpro inhibitor; that his employer has an option and license agreement to develop, manufacture and commercialize two Molecular Partners’ anti-COVID-19 DARPin® candidates; and that his employer has initial agreements with Pfizer-BioNTech and CureVac to manufacture their COVID-19 vaccines, and with Roche for the production of the API for Actemra/RoActemra®. Rahul Rajkumar discloses that he is an advisor to Google Ventures and holds shares in OM1, Advantia Health, and PicassoMD.
NAM LEADERSHIP CONSORTIUM STAFF
J. Michael McGinnis, Executive Director and NAM Senior Scholar
Ayodola Anise, Deputy Director
Mahnoor (Noor) Ahmed, Associate Program Officer
Laura Adams, Special Advisor
Peak Sen Chua, Consultant
Sarah Greene, Special Advisor
Amanda Hunt, Senior Program Officer
Annie Murff, Senior Program Assistant
Asia Williams, Associate Program Officer