
Mental Health:
Increased Advocacy, Education, Understanding, and Treatment
Since 1970, even as many mental health services shifted from the hospital to the community, scientific advances have greatly improved the treatment of mental health conditions. Mental health services and funding remain inadequate, and stigma continues to surround many mental health conditions, but many more people receive effective mental health care now than in the past.

1979
Grassroots Support for Mental Health
Two mothers fighting for better support for families dealing with mental illness founded the National Alliance on Mental Illness (NAMI) in 1979. Since then, it has become the nation’s largest grassroots mental health organization, with nearly 1,000 local and state affiliates. NAMI and other organizations focused on mental health increase awareness, education, and hope around mental health issues; combat stigma against mental illness; and offer classes and trainings for people living with or affected by mental illness.

1980
Passage of the Mental Health Systems Act
Shortly after Jimmy Carter became president, he created a President’s Commission on Mental Health to examine the serious deficiencies in America’s mental health system. A 1978 report from the commission formed the basis of the 1980 Mental Health Systems Act, which fostered more coherent mental health care through improved community mental health services and coordination of general health care, mental health care, and social support services. Though the federal government’s role in mental health care diminished later in the 1980s, the act signaled a new emphasis on the treatment of mental illness.
1986
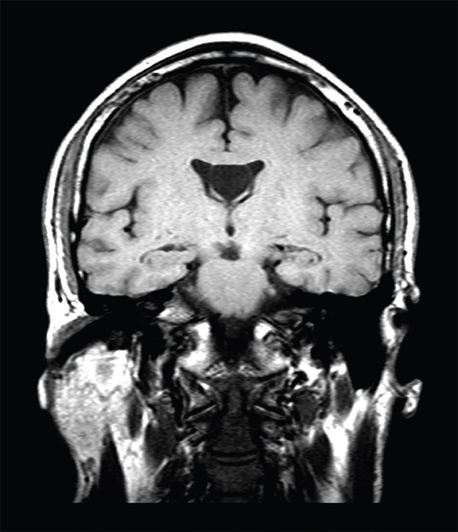
Understanding Schizophrenia Through Brain Imaging
In 1986, magnetic resonance imaging (MRI) of the brains of 38 schizophrenic and 49 control subjects revealed the schizophrenic subjects had smaller frontal lobes, cerebrums, and craniums. The findings suggested that some people with schizophrenia may experience an early developmental defect that impairs the brain’s capacity to grow. Since then, MRI technology has allowed scientists to study the brains of patients with many different mental illnesses, furthering the understanding of their conditions.
1986
Antidepressant Drug Advances
Introduced in 1986, fluoxetine hydrochloride, commonly known as Prozac, was the first major breakthrough for the treatment of depression in nearly 30 years. Prozac was the first of a new class of antidepressant drugs called selective serotonin reuptake inhibitors (SSRIs) that work by preventing the reabsorption of the neurotransmitter serotonin within the brain. The drug revolutionized both the perception and treatment of depression and is still frequently prescribed to treat the 1 in 10 Americans who currently suffer from depression.
2001
The Benefits of Family Psychoeducation
By 2001, more than 30 randomized clinical trials had demonstrated that providing families with education, coping strategies, and problem-solving skills is a valuable treatment for people with mental illness. This family “psychoeducation” can reduce relapse rates and enhance recovery while improving the well-being of participating family members.
2008
Specialty Care for Psychosis
The National Institute of Mental Health launched the Recovery After an Initial Schizophrenia Episode project in 2008 with two studies that examined different aspects of coordinated specialty care treatments for people who were experiencing their first episode of psychosis. Coordinated specialty care is a recovery-oriented program that promotes shared decision-making and features a team of specialists who work with the client to create a personalized treatment plan. Depending on an individual’s needs and preferences, a treatment plan may include psychotherapy, medication management, family education and support, case management, and work or education support. Findings from the studies suggested that this approach is more effective than usual treatments, can be successfully delivered in community practice settings, and is cost effective.
2010
Cognitive Therapy for Depression and Anxiety
Accumulating evidence has supported cognitive therapy as an effective treatment for depressive disorders and anxiety disorders, as reflected in a 2010 recommendation from the American Psychiatric Association. Cognitive therapy generally focuses on short-term, skills-focused treatment aimed at altering inaccurate and maladaptive thoughts to change behaviors and emotions. Specific techniques include identifying inaccurate thinking, examining the evidence for and against automatic thoughts, changing maladaptive thoughts, altering problematic behaviors, and relating to people in more adaptive ways. For patients with depressive disorders, studies have shown that cognitive therapy is generally equivalent in efficacy to pharmacological treatments during the acute phase of treatment and superior to medication in the prevention of relapse. Studies suggest similar effectiveness for patients with anxiety disorders, though additional research is needed to determine how cognitive therapy compares with other treatment methods.

2012
Accelerating Mental Health Care and Research
In 2012, President Barack Obama issued an Executive Order calling for the creation of a National Research Action Plan on posttraumatic stress disorder, other mental health conditions, and traumatic brain injury. Coordinated by the U.S. Departments of Defense, Veterans Affairs, Health and Human Services, and Education, the resulting plan improved mental health services for veterans, service members, and military families through greater investment in research efforts and through rapid translation of research findings into actionable tools for prevention, early diagnosis, and improved treatment.

2014
Mental Health in the Army
Although the suicide rate among U.S. Army soldiers has historically been lower than the rate among the general population, recent years have seen a dramatic increase in Army suicides. In 2014, a comprehensive longitudinal study called the Army Study to Assess Risk and Resilience in Servicemembers tracked 100,000 personnel to shed light on this troubling trend. Nearly half of soldiers who reported suicide attempts had made their first attempt prior to enlistment, suggesting that pre-enlistment mental disorders might be targets for early screening and intervention.

2019
Countering Clinician Burnout
Delivering safe, patient-centered, high-quality, and high-value health care requires a clinical workforce that is functioning at a high level. Unfortunately, clinician burnout is on the rise, largely as the result of dramatic changes that have occurred in the health care system. Regulatory and institutional policies, payer requirements, and intrusive and difficult technologies, among other factors, have contributed to emotional exhaustion, depersonalization, and a low sense of personal accomplishment. As a 2019 report from the National Academy of Medicine (NAM), Taking Action Against Clinician Burnout: A Systems Approach to Professional Well-Being, pointed out, reducing the problem of clinician burnout, stress, anxiety, depression, and suicide will require improving the design and organization of the environments in which clinicians train and work, involving clinicians effectively and meaningfully in the decisions of health care organizations, and supporting well-being throughout clinicians’ education and careers. The NAM created a network of organizations committed to reversing trends in clinician burnout through its Action Collaborative on Clinician Well-Being and Resilience. Its work advances evidence-based, multidisciplinary solutions to improve clinician well-being.

Despite improvements in the diagnosis and treatment of mental illness, past efforts have been far from enough to achieve population-wide mental health. Better evidence-based treatments are needed, and existing evidence-based treatments need to be readily available. Generic programs for mental health must be tailored to individuals and their conditions to ensure human dignity, effectiveness, and the quality of care.




