
Proceedings of a Workshop
WORKSHOP OVERVIEW1
Indigenous communities experience higher risks for suicide and self-harm compared to the general U.S. population, with suicide as the second-leading cause of death among Indigenous children and young adults in North America. In some Indigenous communities, death by suicide has reached epidemic proportions with an increase from 21.5 per 100,000 in 2015 (Leavitt et al., 2018) to 23.9 per 100,000 in 2020 (Ehlman, 2022). These rates are typically derived by combining small and distinct Indigenous populations with different suicide prevalence, thus obscuring factors that may protect specific communities or make them more vulnerable. To reduce this tragic trend, it is essential for prevention and intervention efforts to build on scientific evidence, cultural and local knowledge, and the best community, family, and institutional practices to reduce risk and increase protection.
The Forum on Mental Health and Substance Use Disorders and the Forum for Children’s Well-Being of the National Academies of Sciences, Engineering, and Medicine hosted a three-part virtual public workshop on
___________________
1 This workshop was organized by an independent planning committee, whose role was limited to identification of topics and speakers. This Proceedings of a Workshop was prepared by the rapporteurs as a factual summary of the presentations and discussions that took place at the workshop. Statements, recommendations, and opinions expressed are those of individual presenters and participants and are not endorsed or verified by the National Academies of Sciences, Engineering, and Medicine, and they should not be construed as reflecting any group consensus.
April 22, 2022, May 13, 2022, and June 10, 2022. The workshop featured subject matter experts who examined suicide risk and protective factors in Indigenous populations, discussed culturally appropriate and effective suicide prevention policies and programs, explored existing data systems and how data can be used for tracking suicide rates, and considered gaps and challenges in providing the continuum of services needed for substance use and mental health disorders in multiple health care settings across Indigenous communities.
The April 22, 2022, webinar provided an overview of suicide trends and suicide prevention efforts among Indigenous communities.2 Webinar participants discussed the differences between and among groups and tribes geographically, culturally, and linguistically. Additionally, participants discussed how cultural knowledge, practices, and ceremonies contribute unique strengths and serve as protective factors that act in parallel with behavioral health intervention and suicide prevention programs. The May 13, 2022, webinar focused on evidenced-based practices and interventions currently used across Indigenous populations to prevent suicide. The June 10, 2022, webinar focused on the current challenges, gaps, and opportunities for action to decrease suicide rates in Indigenous communities. Webinar participants discussed data surveillance within Indigenous communities and suggested opportunities to implement culturally appropriate upstream interventions to prevent suicide.
In his opening remarks, William Beardslee, director of the Baer Prevention Initiatives, chairman emeritus of the Department of Psychiatry at Children’s Hospital Boston, and Gardner Monks Professor of Child Psychiatry at Harvard Medical School, said that Indigenous populations, specifically Native youth, die by suicide at disproportionately higher rates compared to the rest of the U.S. population. Although federal and tribal governments have implemented multidisciplinary suicide prevention programs to include education and training for clinicians and patients, suicide rates continue to increase.
Elizabeth Fowler, a member of the Comanche Nation with descendancy from the Eastern Band of Cherokee Indians, and acting director of the Indian Health Service (IHS), discussed the importance of the workshop and the
___________________
2 This proceedings uses the term Indigenous communities to refer to all American Indians and Alaska Natives, which includes 574 tribal nations, state recognized tribes, and urban American Indian and Alaska Native communities. Although these populations are unique and can be distinguished geographically and culturally, for this proceedings they are considered under the single term Indigenous communities. The National Academies acknowledges that Indigenous communities also include other communities across North, Central, and South America, including Native Hawaiians in the United States. However, for the purpose of this workshop, we focused on American Indians and Alaska Natives.
urgency to improve suicide prevention in Indigenous communities. Fowler said that the mission of the IHS is to provide federal health services to American Indians and Alaska Natives (AI/AN);3 to raise the physical, mental, social, and spiritual health of Indigenous people to the highest level; and to ensure that comprehensive, culturally appropriate personal and public health services are available and accessible to Indigenous communities. The IHS provides comprehensive primary health care and disease prevention, including suicide prevention, to approximately 2.6 million Indigenous people in approximately 574 federally recognized tribes in 37 states (IHS, 2022).
The IHS has published a strategic plan that lays out goals and objectives for preventing suicide in Indigenous communities. Box 1 summarizes the eight goals of the National Suicide Prevention Strategic Plan to prevent suicide in Indigenous communities. The plan highlights multiple disciplines, perspectives, and resources to create a system in which individuals, families, schools, and communities can access services.
Fowler said that Indigenous communities have historically faced significant social disadvantages and poor health compared with the general population. She said that these inequities are due to continued disparities in social determinants of health, such as food supply, housing, and education. The impact of colonization, historical trauma, and forced relocation contribute to increased substance abuse and worsened health outcomes (Gone and Trimble, 2012; Hartmann and Gone, 2016). “In these settings, suicide remains a devastating and all too frequent event, and there are interrelated factors contributing to increased suicide risk,” Fowler said. She emphasized that proactive and coordinated responses from the public sector, as well as local and tribal communities and programs, are needed to reduce the tragedy of suicide, addressing it as a public health concern that affects everyone across the United States and worldwide.
This Proceedings of a Workshop summarizes the presentations and discussions that took place during the three webinars. It highlights individual participants’ suggestions to reduce suicide rates and to advance suicide prevention efforts across Indigenous communities. These suggestions are discussed throughout the proceedings and summarized in Box 2. Appendix A includes the Statement of Task for the workshop. The webinar agendas are provided in Appendix B. Speaker presentations and the workshop webcast have been archived online.4
___________________
3 See https://www.ihs.gov/aboutihs/overview/ (accessed August 21, 2022).
4 See https://www.nationalacademies.org/our-work/suicide-prevention-in-indigenous-communities-a-workshop (accessed August 21, 2022).
DISPARITIES IN SUICIDE MORTALITY TRENDS
Asha Ivey-Stephenson, a senior behavioral scientist and epidemiologist at the National Center for Injury Prevention and Control, Division of Injury Prevention on the suicide prevention team at the Centers for Disease Control and Prevention (CDC), discussed the trends in suicide rates in the United States and ongoing work by the CDC in tribal suicide prevention.
Ivey-Stephenson said that suicide is a serious public health problem and requires urgent attention. According to recent data from the National Vital Statistics System,5 the overall suicide rate increased 30 percent between 2000 and 2020. In 2020, suicide was the twelfth-leading cause of death in the United States across all age groups, with nearly 46,000 lives lost to suicide (NCIPC, 2020). Suicide was the second-leading cause of death among individuals between the ages of 10–14 and 25–34, the third-leading cause of death among individuals between the ages of 15–24, and the fourth-leading cause of death among individuals between the ages of 35–44 (NCIPC, 2022). In the same year, 12.2 million adults reported thoughts of suicide, 3.2 million made a plan, and 1.2 million reported an attempt (NIMH, 2022). Among youth during the COVID-19 pandemic, from January to June 2021, 20 percent of high school students reported serious thoughts of suicide, 15 percent made a plan, and 9 percent reported an attempt.6
Ivey-Stephenson said that among non-Hispanic Indigenous people, suicide is the leading cause of death in the 10–24 age group, the second-leading cause of death among those in the 15–24 age group, and the third-leading cause of death among those in the 25–34 age group (NIMH, 2022; see Figure 1).
Ivey-Stephenson shared data of an analysis that compared descriptive characteristics and circumstances precipitating suicide among non-Hispanic Indigenous people compared to non-Hispanic Whites across the 18 states that were included in the National Violent Death Reporting System, between the years 2003 and 2014. This prior work concluded that when compared to non-Hispanic White people, non-Hispanic Indigenous people who died by suicide were younger, lived in more rural areas, were more likely to have a friend or family member who had also died by suicide, and were more likely to use alcohol (Leavitt et al., 2018). An update of the analysis is currently ongoing to compare descriptive characteristics and precipitating circumstances of suicide among all Indigenous people compared to non-Indigenous suicides across 32 states during 2015–2019. She noted that one preliminary takeaway
___________________
5 The National Vital Statistics System provides the most complete data on births and deaths in the United States. See https://www.cdc.gov/nchs/nvss/index.htm (accessed August 2, 2022).
6 See https://www.cdc.gov/healthyyouth/data/abes/tables/index.htm (accessed August 2, 2022).
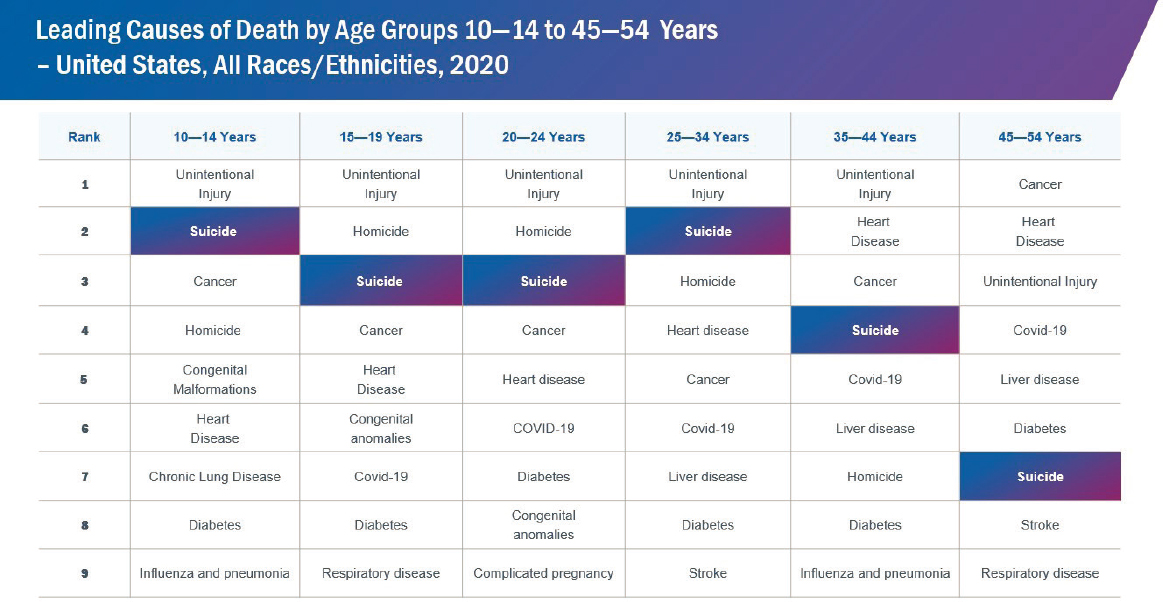
SOURCE: Ivey-Stephenson presentation, 2022
from the ongoing analysis is that Indigenous suicide is preceded by a number of factors where prevention can be targeted, and certain factors may warrant increased and culturally tailored prevention efforts among this population.
Ivey-Stephenson also discussed a recent report on the changes in firearm homicide and firearm suicide rates from 2019 to 2020, coinciding with the emergence of the COVID-19 pandemic (Kegler et al., 2022). The report revealed that from 2019 to 2020, gun-related homicides increased from 14,392 to 19,350, representing nearly a 35 percent increase, the highest firearm homicide rate in more than 25 years. The largest increases in firearm homicide rates were among Black males aged 10–24 and 25–44 years and among Indigenous males aged 25–44 years. Also, the results revealed that in 2020, counties with the highest poverty levels had firearm homicide rates 4.5 times as high as firearm suicide rates, and 1.3 times as high as counties with the lowest poverty rates (Kegler et al., 2022). “There is a substantial need for additional research to expand the evidence base for programs, policies, and practices that effectively reduce firearm injuries and deaths, and that address inequities in risk for violence and suicide,” Ivey-Stephenson said.
In conclusion, Ivey-Stephenson said the CDC is working with tribes to reduce risk and increase protective factors to prevent suicide among Indigenous communities (NCIPC, 2022). For example, she discussed the Tribal Public Health Capacity Building and Quality Improvement Cooperative Agreement,7 funded by the CDC’s National Center for Injury Prevention and Control. She said that the project seeks to increase capacity to adapt, implement, and evaluate suicide prevention programs to reduce suicide-related morbidity and mortality (CDC, 2021).
Emily Haozous, a Chiricahua Fort Sill Apache, registered nurse, and research scientist at the Pacific Institute for Research and Evaluation, discussed premature mortality trends and the racial disparities in premature mortality. Haozous said that Indigenous people continue to experience the effects of colonization and intergenerational and historical trauma that give rise to health disparities and disproportionately high rates of suicide. She added that the health disparities were made more evident during the COVID-19 pandemic, noting that Indigenous people disproportionately experienced substantially greater rates of COVID-19 mortality compared with other racial and ethnic groups (a topic of discussion in Box 3).
Haozous shared a set of analyses on premature mortality—caused by factors including suicide and alcohol use—estimated from national datasets from the U.S. National Center for Health Statistics, Statistics Canada, the
___________________
7 See https://www.cdc.gov/tribal/cooperative-agreements/tribal-capacity-buildingOT18-1803.html (accessed August 21, 2022).
UK Office of National Statistics, the U.S. Census, and CDC WONDER8 (Khan et al., 2018; Spillane et al., 2020). Haozous said that even with “racial misclassification,” Indigenous people were shown to die at disproportionately higher rates than other demographics (Spillane et al., 2020). She said that a study that examined and projected premature mortality rates by race predicted that the premature mortality rates within Indigenous populations will be substantially higher compared to other races by 2030 (Best et al., 2018). The current estimates on premature deaths of Indigenous people may be under-reported because the deceased are least likely to be identified accurately on death certificates (Freemantle et al., 2015; Kalweit et al., 2021). She suggested that it would be essential to create data systems that crosslink vital statistics data to improve the quality of data and build a better sense of health equity.
Intergenerational Trauma and Indigenous Suicides
Donald Warne, an Oglala Lakota, associate dean of diversity, equity, and inclusion, director of the Indians into Medicine and Public Health Programs, and professor of family and community medicine at the School of Medicine and Health Sciences at the University of North Dakota, discussed how suicide prevention should also be considered wellness promotion because of the adverse health outcomes associated with the impact of intergenerational trauma. Warne said that it is critically important to understand the impact of loss of territory, loss of resources, and intergenerational trauma, as well as intergenerational poverty, when looking at interventions in Indigenous populations (Warne and Lajimodiere, 2015; see Figure 2). He explained that historical trauma and other stressors experienced by Indigenous people over their lifetime can significantly increase the risk of depression, anxiety, and posttraumatic stress disorder (PTSD), leading to self-medication with substances that increase the risk of suicidality (Warne et al., 2017). “The impact of adverse childhood experiences (ACEs) is pervasive, not only in mental health but also in physical health, leading to disparities in chronic diseases, which in turn impact life potential,” Warned stressed.
Additionally, there are social conditions and local contexts that place Indigenous communities at greater risk for exposure to ACEs, which can result in disrupted neurodevelopment and subsequent social, emotional, and cognitive impairment that in turn lead to adoption of health risk behaviors, early onset of disease and disability, and social problems and early death, such as from suicide (Felitti et al., 1998, 2019). Warne said that compared to other populations in which suicide rates increase with advancing age, for
___________________
8 CDC WONDER is an online database for research and analysis of public health data, available to the public at https://wonder.cdc.gov/ (accessed August 21, 2022).
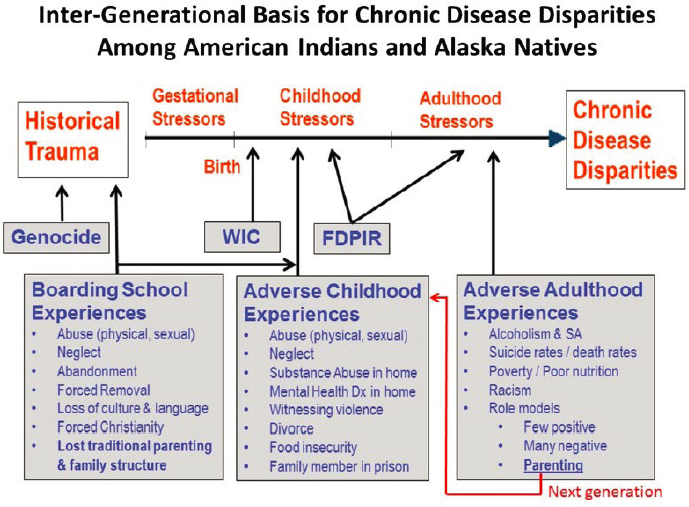
NOTE: FDPIR = Food Distribution Program on Indian Reservations; SA = substance abuse; WIC = Supplemental Nutrition Program for Women, Infants, and Children.
SOURCES: Warne presentation, April 22, 2022; Warne and Lajimodiere, 2015.
Indigenous communities, there is a peak of suicidality in the teen years and early adulthood, strongly suggesting the necessity to intervene early to prevent or reduce ACEs. For example, he shared findings from an analysis to assess the prevalence of ACEs and their association with behavioral health in Indigenous and non-Indigenous populations in South Dakota (Warne et al., 2017). The analysis included the validated ACE questionnaire in a statewide health survey of 16,001 households. The researchers found that compared with non-Indigenous communities, Indigenous people displayed a higher prevalence of ACEs, including abuse, neglect, and household dysfunction, and had a higher total number of ACEs. For both Indigenous communities and non-Indigenous communities, having six or more ACEs significantly increased the odds for depression, anxiety, PTSD, severe alcohol misuse, and smoking compared with individuals with no ACEs (Warne et al., 2017).
Whether it is historical trauma or ACEs, all of these conditions impact the spiritual, mental, physical, and emotional components of the individual, Warne emphasized. He said that that much of the past work has been focused on healing psychological and emotional trauma based on deep-rooted cultural
and spiritual connectedness to land, place, and Earth, but many land-based healing modalities are no longer available due to colonization and the loss of traditional territories. Warne suggested that it would be helpful to address and understand the impact of spiritual trauma, which also increases suicidality. He noted that healing the effects of spiritual trauma through cultural practices and ceremonies, and relearning or expanding Indigenous language, are underestimated and undervalued in the current scientific approach (Stringer, 2018). He said that current interventions have not yet yielded the desired results, and suggested a focus on more open-minded medical systems and research institutions that understand that one size does not fit all and acknowledge that culturally based interventions are necessary to address challenges. Warne emphasized that Indigenous language, traditional ceremonies, and cultural connectedness are foundational for recovering from trauma and promoting wellness in Indigenous populations (see Box 4).
SUICIDE PREVENTION ACROSS INDIGENOUS POPULATIONS
Joseph Gone, a member of the Aaniiih-Gros Ventre tribe, professor of anthropology and of global health and social medicine, and the director of the Harvard University Native American Program, discussed the rationale for evidence-based practice and the evidence base for mainstream and Indigenous suicide interventions, and reflected on strategies to reduce Indigenous suicide.
Rationale for Evidence-Based Practice
Gone said that the need for mental health treatments eclipses the availability (Levinson, 2011; WHO, 2022), and that tough decisions about how to allocate those scarce resources must be made. He continued that most current mental health interventions have not been vigorously evaluated in scientific terms. Gone said that this is partly because clinician practice deviates from the structured interventions developed for mental health conditions. Gone mentioned that the rationale for evidence-based practice emerges from a commitment to provide health care services that are likely to help people without causing them harm. He cautioned that certain interventions, although developed with good intent, may actually harm individuals.
Gone explained how evidence-based practices are developed in mental health services. Evidence-based practice in psychology has been defined as the combination of the best research evidence, client values and preferences for treatments and interventions, and clinician expertise in delivering treatments and interventions (Kazdin, 2008). He said that these are interventions that first originate in tightly controlled efficacy trials to try to establish cause and effect between a treatment and its outcomes and benefits. Gone explained that once there is substantial evidence of proven benefits for a given intervention across numerous studies, that evidence can be incorporated into formal clinical practice guidelines.
Evidence Base for Mainstream Suicide Interventions
Gone explained that there are different forms of suicide interventions, and not all mainstream suicide interventions have been shown to work. He added that research data on suicide interventions is complex and evolving. Gone shared data from two analyses to highlight the complexity of what is considered evidence based for mainstream interventions (Hofstra et al., 2020; Mann et al., 2021). First, he shared data from a meta-analysis to examine the effectiveness of suicide prevention interventions in terms of reducing attempted and completed suicides, and to examine whether the effectiveness
of an intervention differs across settings in which the intervention is delivered (Hofstra et al., 2020). The researchers included a total of 15 controlled studies that were published from 2011 to 2017, with a total of 29,071 participants, altogether reporting 62 suicides and 1,006 suicide attempts in the meta-analysis. Gone pointed out that the findings revealed that the effect size (a measure of the strength of the relationship between two variables in a population) differed depending on which outcome was studied (i.e., attempts vs. completion) (Hofstra et al., 2020). Also, the effectiveness of the interventions differed depending on the intervention setting. For example, suicide prevention interventions for patients admitted to a psychiatric ward in a general hospital and community-level interventions showed large effects in reducing completed suicides. Interventions in other settings showed no significant effect. Additionally, the researchers found that combined, multilevel interventions led to better outcomes.
The second study was a review to identify scalable evidence-based suicide prevention strategies (Mann et al., 2021). The analysis included 97 randomized controlled trials and 30 epidemiological studies published between 2005 and 2019, focused on suicide, attempted suicide, or suicidal ideation. The researchers classified the interventions as effective and scalable interventions, unproven but promising and scalable interventions, and interventions labeled ineffective but that had been well studied. Gone emphasized that there are forms of suicide intervention that work, and combining more than one type into multilevel approaches is even better.
Evidence Base for Indigenous Suicide Interventions
Gone said that robust intervention outcome research is challenging and therefore rare in Indigenous communities. He explained this point by sharing the findings of two systematic reviews. The first was a systematic review of intervention outcomes associated with suicide interventions that aimed to answer the question of what intervention works to prevent suicide among Indigenous people (Pham et al., 2021). The researchers used broad inclusion criteria to identify 28 studies with 23 unique interventions that were published between 1976 and 2020. The studies used direct measures of suicidal behavior (e.g., suicide attempt and suicidal ideation) or indirect measures of proxy variables that are associated with suicide (e.g., hopelessness or alcohol abuse). Gone noted that, overall, each study reported improvement on at least one of their targeted outcomes; however, only 11 studies included assessments for changes in direct suicide outcomes. Among these 11 studies, only three ascertained their outcomes using a controlled trial. All other studies either used noncontrolled study designs or measured indirect variables only. Gone said the major finding was that the designs of these studies preclude conclu-
sions about effectiveness. There were only a few controlled studies, and there were no comparison groups to assess whether the outcomes were better for people who received the intervention. Gone said that the findings from the systematic review indicated that it is not possible from this current body of data to scientifically conclude which interventions work to prevent suicide among Indigenous people.
Gone also discussed a second systematic review aimed at understanding what interventions are effective at preventing suicidal behaviors among Indigenous populations (Pham et al., 2022). The authors identified 32 studies with 24 distinct interventions published between 1976 and 2020 that were focused on various attributes and characteristics of the programs. The researchers classified the studies according to established CDC strategies to prevent suicide (CDC, 2022). The strategies include promoting connectedness, creating protective environments, identifying and supporting people at risk, teaching coping and problem-solving skills, strengthening access and delivery of suicide care, lessening harms and preventing future risk, and strengthening economic supports. Several of the studies focused on connectedness as a main strategy for prevention, followed by interventions that create positive environments and identify and support people at risk. Gone said that the findings indicate that most Indigenous communities both adopt and adapt mainstream suicide prevention strategies. Additionally, the processes of intervention adoption and adaptation are responsive to community orientations and commitments. Again he noted that the effectiveness of the adapted community interventions remains an open scientific question because of the dearth of rigorously designed outcome studies.
In closing, Gone said that development of evidence-based practice requires scientific research on intervention outcomes. He added that honing in on specific recommendations on best practices for suicide prevention in Indigenous communities could be difficult due to the diversity of those communities. He suggested four questions that would need to be answered concerning evidence-based suicide interventions for Indigenous communities:
- How confident are Indigenous populations that mainstream evidence-based suicide interventions deserve special recognition and promotion in their communities?
- What are the prospects for adopting and adapting additional mainstream evidence-based interventions?
- How can multilevel suicide intervention programs be designed across care providers, domains, and settings?
- What resources are available to Indigenous communities to develop more comprehensive suicide prevention services and to assess the impacts of those services?
SUICIDE PREVENTION RESOURCE CENTER
Dolores Subia BigFoot, an enrolled member of the Caddo Tribe and a child psychologist at the University of Oklahoma Health Sciences Center, presented an overview of the Suicide Prevention Resource Center (SPRC),9 which she directs. She said the SPRC is the only federally supported resource center devoted to advancing the implementation of the National Strategy for Suicide Prevention. BigFoot noted that the SPRC builds capacity and infrastructure for effective suicide prevention through consultation, training, and resources for state and tribal health/behavioral health and community systems; professionals and professional education programs; and national public and private partners. “Diversity, inclusion, and equity guide our mission,” BigFoot stressed.
She said the SPRC develops toolkits that offer best practices and promising practices for the implementation of culturally appropriate suicide interventions (SPRC, 2022). For example, the SPRC provides support and resources for Indigenous Two-Spirited people, a topic discussed in Box 5. BigFoot said that one of the toolkits to be released in late 2022 is based on the first tribal needs assessment for 2022, to assess the diverse array of suicide prevention resources and activities across states, territories, and a selection of tribes and tribal organizations. She said preliminary findings show that there is great interest in preventive services to help individuals avoid reaching the point of suicidal thoughts. There is also interest in integrating culturally based knowledge into suicide prevention programs. Reiterating Warne’s suggestion on integrating cultural practices into suicide prevention, BigFoot emphasized that cultural practices within communities have continued for several generations and have potential benefits in suicide prevention.
Examples of Suicide Intervention Models in Indigenous Communities
Several speakers presented an overview of a range of current suicide intervention models and strategies across diverse Indigenous communities.
Zero Suicide
Sadé Heart of the Hawk Ali, of the First Nations Mi’kmaq from the Sturgeon Clan, and tribal lead for the Zero Suicide initiative, said that Zero Suicide is a way to improve suicide care within health and behavioral health systems. The foundational belief of Zero Suicide is that suicide deaths for individuals under the care of these systems are preventable. Ali noted that Zero Suicide is based on the realization that people experiencing suicidal thoughts
___________________
9 See https://www.sprc.org/states/oklahoma (accessed August 21, 2022).
and urges often fall through the cracks in a health care system that is often fragmented and distracted. Ali said that the Zero Suicide framework includes evidence-based screenings and tools to identify people at risk, create safety plans, provide transitional care and referrals, and follow up.
Ali said that the Zero Suicide framework has seven essential elements, including both implementation and clinical elements, for safer system-wide suicide care. These elements are Lead, Train, Identify, Engage, Treat, Transition, and Improve.10 The first element, Lead, emphasizes that top leadership commitment and dedicated frontline champions are both necessary for success. The second implementation element, Train, highlights the importance of training a competent, confident, and caring workforce. The Identify element provides guidelines to identify individuals with suicide risk via comprehensive screening and assessment. The Engage element ensures pathways to care for all individuals at risk of suicide using a suicide care management plan. The Treat element emphasizes the importance of directly treating suicidal thoughts and behaviors using evidence-based treatments. The sixth element is Transition, which highlights the need for universal and continuing interventions and support following discharge of individuals at risk of suicide. The seventh element, Improve, emphasizes the need to improve policies and procedures through continuous quality improvement.
Ali emphasized that Zero Suicide is not a model but a framework that is flexible enough to promote the incorporation of various healing ways to support individuals and families while honoring the need for cultural resonance (see Figure 3).
Ali said that the Zero Suicide initiative has published a companion toolkit, Best and Promising Practices for the Implementation of Zero Suicide in Indian Country, which indigenizes the Zero Suicide framework and serves as a resource for cultural adaptation of the Zero Suicide toolkit for health systems
___________________
10 See https://zerosuicide.edc.org/about/framework (accessed August 21, 2022).
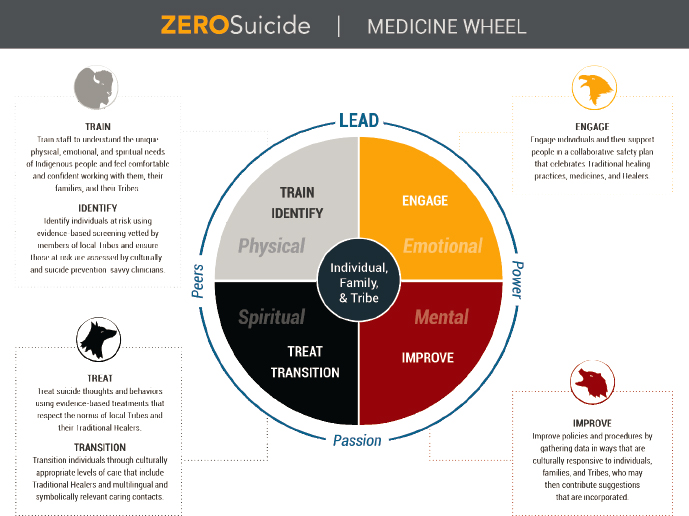
SOURCE: Ali presentation, 2022. https://zerosuicide.edc.org/toolkit/toolkit-adaptations/indian-country (accessed July 28, 2022).
serving Indigenous communities.11 The toolkit contains recommendations for the implementation of Zero Suicide in Indian Country, forms and tools others have used in their own implementation, and videos featuring a variety of Indigenous health systems that have committed to the implementation and indigenization of the Zero Suicide framework for their communities. The toolkit also offers suggestions for health systems serving Indigenous communities on how to create implementation teams that include tribal government, elders, traditional medicine people, and youth. Additionally, it offers guidance on how to frame the conversation around loss to reflect promotion of life rather than suicide. Every tribe has their own language, healing ways, medicines, creation stories, dances, songs, and regalia. “The understanding that a combination of traditional and western medicine could be highly effective and useful in Indigenous populations is very important,” Ali said.
Ali said that evaluation studies have shown that Zero Suicide is effective (Layman et al., 2021; Stapelberg et al., 2021). The Chickasaw Nation was one
___________________
11 See https://zerosuicide.edc.org/toolkit/toolkit-adaptations/indian-country (accessed August 21, 2022).
of the early adopters of a Zero Suicide framework adapted for Indian Country (Dial et al., 2019). Notably, the most successful implementation of Zero Suicide observed in Indian Country employed traditional medicine and started with a tribal resolution by the chief governor, president, or chairperson, with the input of the elders and the youth. When asked by a participant about what changes might increase uptake of Zero Suicide in Indian Country, and what advocates could do to assist in this aim, Ali responded that it is essential to find ways to talk to the communities and frame the conversation in respectful ways.
Celebrating Life
Novelene Goklish and Francene Larzelere, who are both from the White Mountain Apache Tribe and are research associates at the Center of American Indian Health at Johns Hopkins Bloomberg School of Public Health, presented on the Celebrating Life Suicide Prevention Program in the White Mountain Apache community. The White Mountain Apache Tribe has more than 17,500 enrolled members, with around 13,000 residing on their reservation in Arizona, which is geographically isolated in a mountain region.12
Goklish provided background on the establishment of the Celebrating Life program.13 She said that in 2001, after a cluster of youth suicides, the White Mountain Apache Tribe established a taskforce and mandated that all community members report suicide deaths, attempts, and ideation to a surveillance system. The mandate required the creation of a referral form for all first responders and taskforce members to fill out after interacting with individuals expressing suicidal behaviors. She said that this suicide surveillance system became one of the first registries in the United States to gather data on suicidal behavior from both community and clinical settings (Cwik et al., 2014). In 2010 the mandate was expanded to include reporting of nonsuicidal self-injury and binge substance use (Cwik et al., 2014; Haroz et al., 2020). Goklish noted that with the help of tribal leaders and researchers from Johns Hopkins University, the program has expanded to improve its surveillance and database to track details on suicide and related behaviors, as well as risk and protective factors in the community.
Goklish explained that the program has three main components: (1) tribally mandated active surveillance within a closed reservation system, (2) in-person follow-up and case management provided by Apache Community Mental Health Specialists, and (3) community outreach and education about the program (Cwik et al., 2016). Figure 4 shows a model of how the components of the program are connected with the intervention activities.
___________________
12 See http://www.wmat.us/history.html (accessed August 21, 2022).
13 See https://caih.jhu.edu/programs/surveillance-systems (accessed August 21, 2022).
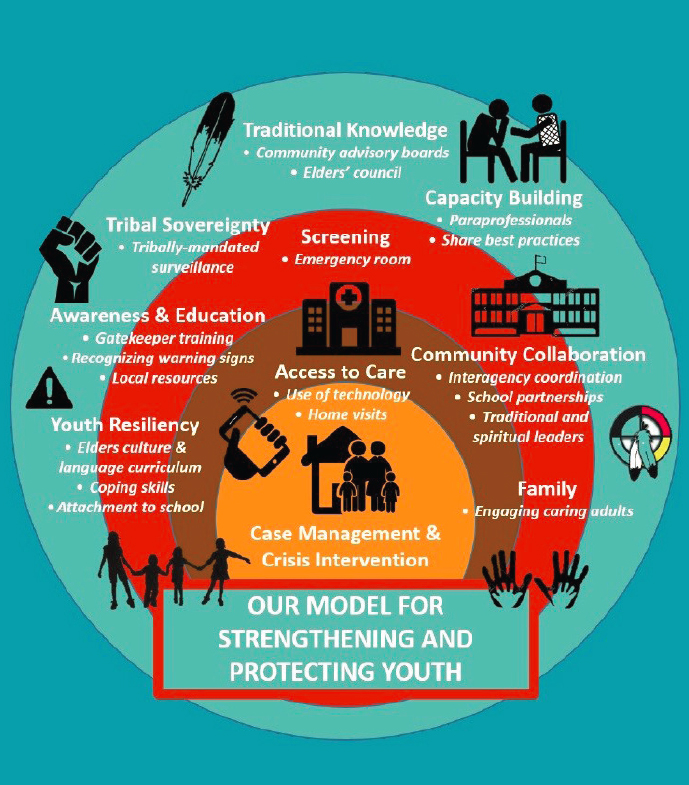
SOURCES: Goklish and Lazalere presentation, May 13, 2022; Johns Hopkins Center for Indigenous Health, 2019.
After a referral is received, program staff typically have 90 days to locate the individual and help them identify resources, including transportation or assistance with completing any required forms. “When contact is made with an individual, there is no time restraint and no limit to how long dialogue is continued,” Goklish stressed.
Larzelere shared the findings of a study that evaluated the impact of the Celebrating Life program among the White Mountain Apache of Arizona (Cwik et al., 2016). She said that researchers used data from the Celebrating Life surveillance system, and compared the rates and characteristics of suicide
deaths and attempts from 2007 to 2012 with those from 2001 to 2006. The study reported that deaths by suicide among the White Mountain Apache in Arizona dropped by nearly 40 percent between 2007 and 2012 compared to the previous six-year period, while national rates remained stable or rose (Cwik et al., 2016). This included a 60 percent decrease among those between the ages of 25 to 34 and a 37 percent decline among those between the ages of 20 and 24. “Dedication to the community has shown that a surveillance system works, in-person follow-up works, and connecting to individuals on a one-on-one basis is key in suicide prevention and can greatly assist with accurate data collection,” Larzelere emphasized.
The White Mountain Apache Tribe is currently working with other Indigenous communities to implement similar interventions. Larzelere mentioned that limited internet access to some rural locations poses a great challenge to supporting the database for the program.
Qungasvik (Tools for Life)
Stacy Rasmus, director of the Center of Alaska Native Research in the Institute of Artic Biology at the University of Alaska, Fairbanks, and research director in the Center of Health at the Northwest Indian College, presented on the Qungasvik, an upstream intervention developed by Yup’ik communities to reduce and prevent alcohol use disorder and suicide in Yup’ik Alaska Native youth (Rasmus et al., 2014). She emphasized the importance of culture to both the successful implementation and the effectiveness of health interventions among Indigenous populations.
Rasmus said Qungasvik builds on protective factors, such as social connectedness and reasons for life and sobriety. The intervention and the underlying Yup’ik Indigenous theory of change promote growth in culturally based protective factors. Qungasvik engages community members in the development of intervention modules, which consist of episodes of engagement with Yup’ik teachings and local cultural activities. It is a strengths-based, community-level intervention grounded in a multilevel theory of protection and utilizes the theory-driven Qasgiq model employing Indigenous knowledge in interventions to address youth suicide and substance use disorders within social, cultural, spiritual, and ecological systems (Allen et al., 2014; Rasmus et al., 2014, 2019). The Qasgiq model begins with the community-mobilizing process of identifying activities better able to produce protective factors. “We want to build those protective factors and we will do that by creating protective experiences through activities for young people that connect them to their culture and to the elders and knowledge bearers,” Rasmus said. Many of the activities include survival skills, such as hunting, fishing, and gathering and building, which young people learned over a two-year period primarily out on the land. Rasmus explained that
the Qasgiq model acknowledges the problem of suicide as a collective harm within the community. Thus, the solutions must come from within.
Rasmus noted that the intervention is unique in many ways. First, it is an upstream effort to work with young people in the community to build protective factors early, shifting the focus from individual risk to building community and cultural strengths across rural Yup’ik communities. Additionally, the intervention was initiated by the community, with researchers becoming involved by invitation from the community. In addition, the intervention was built on existing infrastructure, expertise, and programming from within the community in order to involve existing culturally meaningful settings and to create new ones, through a locally controlled process. Moreover, the intervention can be feasibly implemented to produce dose-related measurable effects (Allen et al., 2018; Mohatt et al., 2014).
James Allen, a professor in the Department of Family Medicine and Behavioral Health at the University of Minnesota Medical School, agreed with Rasmus noting that there is emergent evidence that Qungasvik increases protective factors and reduces suicide-related behavior. Allen shared data of a nonrandomized study that compared the effectiveness of Qungasvik in one community that intensively utilized the intervention to a community with lower intensity intervention (Allen et al., 2018). The researchers found that higher levels of intervention led to higher-impact results, particularly among males, demonstrating that the Qungasvik intervention is emerging as a promising practice and should be evaluated further.
Coordinated Care Model and Medication Management
Lieutenant Commander Teresa Grund, lead faculty at Indian Country ECHO, and certified psychiatric pharmacist who practices as an advanced practice clinical pharmacist in a behavioral health medication management clinic at the Red Lake IHS in Minnesota, discussed opportunities to use an interdisciplinary health care team approach to suicide prevention, and the role of pharmacists in individual-level suicide prevention efforts.
Many Indigenous health care facilities are located in remote areas, which limits access to mental and behavioral health care. Grund said that in rural Minnesota, the limited access to mental health care services prompted a collaboration between the Red Lake Indian Health Service Hospital and the University of Minnesota to train pharmacists to provide medication management for mental health. She continued that the initial assessment to determine the comfort level of pharmacists to screen for suicide and other mental health issues found that many pharmacists were not trained or comfortable with handling suicidal ideation that may be elucidated when doing these screenings. Knowing that screening for untreated depression is an upstream approach to
reducing suicidality motivated the development of a training program for Red Lake Pharmacy staff in suicide assessments, Grund said. Incorporating the culture into prevention was the first step in program development.
In 2018, all pharmacy staff members in Red Lake were trained to administer the Patient Health Questionnaires 2 and 9 (PHQ-2 and PHQ-9)14 and to use the Question, Persuade, and Refer (QPR) emergency mental health intervention for people who can serve as gatekeepers—to be in a position to recognize a crisis and the warning signs that someone may be contemplating suicide. The QPR training is intended to increase awareness of suicide prevention strategies so that people feel less apprehensive when talking with someone who may be experiencing suicidal thoughts. Grund compared QPR to cardiopulmonary resuscitation used in cardiac arrest. She said that QPR is a cost-effective training that is applicable in any setting and added that screening for depression and other mental health conditions in Red Lake clinics increased after the trainings. Screening for depression and other mental health issues became a standard of routine care in Red Lake clinics.
Studies have found that, after suicide prevention trainings, pharmacists are more confident to intervene with a patient at risk for suicide (Painter et al., 2018; Stover et al., 2022). Grund said that the program at Red Lake has had a positive impact, and plans are under way to scale up this model across other IHS health facilities. Pharmacists can assess for mental wellness because they are more accessible to the public (Manolakis and Skelton, 2010; Mospan et al., 2019). She concluded that with minimal training, pharmacists can help improve mental health care through routine screening for mental wellness.
Promoting Community Conversations about Research to End Suicide
Lauren White, a citizen of the Choctaw Nation of Oklahoma and a PhD candidate at the University of Michigan, and Josie Garnie, an Inupiaq and counselor supervisor with Behavioral Health Services at Norton Sound Health Corporation, discussed the invention known as Promoting Community Conversations About Research to End Suicide (PC CARES).15 PC CARES is a community health intervention designed, supported, and implemented in Yupik and Inupiaq Northwestern Alaska communities in a collaboration among researchers and community and tribal leaders and organizations. She said that while most mainstream suicide prevention approaches tend to be very focused on individual risk factors and treatments for individuals who are in crisis, the research on social disparities in many Indigenous communities points to the need to think about community-level contexts, and in turn,
___________________
14 Self-administered tools for assessing depression.
15 See http://www.pc-cares.org/about (accessed August 21, 2022).
community-level solutions to reduce youth suicide (Beaudoin et al., 2018; Bush and Qeaden, 2020).
PC CARES is a community mobilization approach that builds communities of practice among local and regional service providers, community members, friends, and families, to spark multilevel and sustained efforts for suicide prevention. Additionally, it prioritizes integration of local ways of knowing in research on multilevel and sustained efforts for suicide prevention (Wexler at el., 2016). PC CARES engages community members as active generators of meaning and analysis of research information rather than passive recipients of research information and its meaning and how it is to be applied to their communities. White said that informed by these insights, PC CARES is focused on bolstering social connections as an upstream approach to prevention.
The intervention addresses the need for culturally responsive suicide prevention practices through a series of community learning circles. Learning circles offer participants chances to share stories relevant to the content in the section on “what do we think,” and to envision how they can apply the new information in their home community, as they discuss possible solutions and next steps in the “what do we want to do” section (Wexler et al., 2016). Learning circles supported by local facilitators foster personal and collective learning about suicide prevention in order to spur practical action on multiple levels to prevent suicide and promote health. “At the end of each session, there is a group discussion and reflection on what communities and individuals can do locally, followed by prayers, songs, and meditations, also often led by an elder,” White added. A study that examined how participants of PC CARES learning circles made sense of and decided whether and how to use research evidence presented in the intervention reported that many of the participants learned useful information and skills for prevention, developed new ways of working with others in their community to promote wellness, and took actions for prevention and health in their villages (White et al., 2022). “PC CARES’ focus remains building life and not simply preventing death,” White concluded.
Honoring Native Life
Teresa Gomez, a tribal member of the Pueblo of Isleta and program manager of the Honoring Native Life program16 at the University of New Mexico (UNM) Department of Psychiatry and Behavioral Sciences in the Division of Community Behavioral Health, said that this program was established in March 2011 when the New Mexico state legislature passed legislation establishing what is called the Clearinghouse for Native American Suicide Prevention.
___________________
16 See https://hsc.unm.edu/medicine/departments/psychiatry/cbh/hnl/ (accessed August 21, 2022).
In consultation with the New Mexico Indian Affairs Department and the Interagency Behavioral Health Purchasing Collaborative, the Clearinghouse was created to provide culturally appropriate suicide prevention, intervention, and post-intervention assistance statewide. The establishment of the Clearinghouse grew out of recognition that, although New Mexico’s different tribes are unique in their cultures and communities, there would be some benefit to creating a central site to provide suicide prevention and intervention information, data, training, and other support, Gomez said.
The name “Clearinghouse” evolved into the Honoring Native Life program after individuals involved with establishment of the legislation and community leaders believed “Honoring Native Life” was a more appropriate and culturally relevant name for the program, given the difficult and often taboo topic for tribal communities. Gomez said that the Honoring Native Life staff comprises a multidisciplinary team of UNM faculty and staff with expertise in Native American behavioral health and organizations and deep cultural connections to their tribal communities.
The mission of the program is to provide a centrally based resource and support to improve health and well-being among Indigenous populations in order to achieve the overall aim of suicide reduction through capacity building, community-based program support, and youth engagement. Gomez explained that the Honoring Native Life Program has developed three focus areas based on public health approaches: (1) tribal leadership and youth engagement to support protective factors, (2) tribal community support through education and programmatic technical assistance, and (3) building tribal capacity for crisis intervention and post-intervention services. “It is really important to us at the university to engage in building relationships with the tribal communities themselves, the tribal programs, and also other urban programs that serve Native Americans here in New Mexico,” Gomez said.
Gomez said that the program has developed direct relationships with each of the 23 tribal nations and their health and wellness programs that encompass behavioral health, and it continues to increase outreach and direct community support. “The activities that we conduct are in consultation with and in partnership with communities and agencies that serve Native American populations throughout New Mexico,” Gomez emphasized.
Gomez noted that throughout the years, Honoring Native Life has hosted several statewide summits, bringing together hundreds of people, including youth, tribal leadership, and partners, and behavioral health staff to discuss important issues such as community readiness, crisis response planning, and suicide prevention practices. In partnership with the New Mexico Department of Indian Affairs, the program offers trainings that are community based and focused on screenings, community readiness, and supporting tribal communities (Indian Affairs Department, 2021). Honoring Native Life conducts
trainings in the community, Gomez noted, because “we really want to ensure that we are listening to the voices, including the voices of people in our tribal communities. We want to make sure that our voices [are included] at the various decision-making tables so that we can promote suicide prevention, intervention and post-intervention efforts.”
Gomez concluded by saying that in order to provide interventions that support Indigenous comminutes, it is important to effectively and intentionally communicate about the topic of suicide, especially in certain types of communities, and to get the support of tribal leadership to do programming and provide some interventions. She continued that there are some difficulties in recognizing suicidal ideation as a real problem within tribal communities.
American Indian Life Skills (Formerly, Zuni Life Skills)
Teresa LaFromboise, professor of developmental and psychological sciences within the Graduate School of Education and chair of Native American Studies at the School of Humanities and Sciences at Stanford University, discussed American Indian Life Skills (AILS), formerly, Zuni Life Skills. AILS is a community-driven, school-based, and culturally sensitive suicide prevention program for American Indian adolescents of the Zuni Pueblo. LaFromboise said that school-based suicide prevention programs in the United States have existed for many decades (Office of the Surgeon General and National Action Alliance for Suicide Prevention, 2012), based on the recognition that a significant amount of suicidal behavior occurs among students who seem to be well functioning.
LaFromboise emphasized that Zuni leaders originally initiated the development of a universal suicide prevention program for all students in high school, with the goal of building protective factors in youth and preventing suicidal ideation. The program primarily utilizes scenarios that convey Indigenous knowledge to develop its curriculum and in the selection of its activities. The curriculum emphasizes social–cognitive skills training and includes seven main themes: (1) building self-esteem, (2) identifying emotions and stress, (3) increasing communication and problem-solving skills, (4) recognizing and eliminating self-destructive behavior, (5) information on suicide, (6) suicide intervention training, and (7) setting personal and community goals (LaFromboise and Lewis, 2008).17 She explained that even though this intervention has a heavy
___________________
17https://sprc.org/online-library/american-indian-life-skills-developmentzuni-life-skills-development#:~:text=The%20curriculum%20emphasizes%20social%E2%80%93cognitive,on%20suicide%2C%206)%20suicide%20intervention (accessed October 30, 2022).
skills component, it is saturated with constant, positive health messages that aim to increase the cognitive flexibility needed for executive function, instill optimism, reinforce cultural pride, increase a sense of school belonging, and increase perceived competence. LaFromboise said that, after the program was evaluated over a three-year period, the Zuni gave permission to broaden the program to include American Indian Life Skills (LaFromboise and Lewis, 2008).
LaFromboise concluded that schools are often overlooked as sites for suicide prevention. She noted that school-based suicide prevention interventions have shown positive outcomes across an array of settings. “Many Indigenous youths have benefited from school-based suicide prevention interventions and approaches, but overall, these types of interventions are understudied,” she added.
Wakȟáŋyeža (Little Holy One)
Lawrence Wetsit (Many Eagle Tailfeathers), an Assiniboine from northeast Montana and traditional healer, provided background on the initiation of Wakȟáŋyeža, or Little Holy One. The Fort Peck Assiniboine and Sioux tribes developed this program in partnership with Teresa Brockie, a member of White Clay (A’aninin) Nation and an assistant professor at Johns Hopkins University. Wetsit said that the Little Holy One project is a community-based participatory research project that resulted from previous research conducted at Fort Peck, which showed that historical trauma is associated with suicidal ideation in adolescents (Brockie et al., 2015; Willmon-Haque and BigFoot, 2008). Wetsit said that as a traditional healer, the findings of the study, to him, highlighted the role culture plays in how people look at themselves and what they think about life.
Wetsit explained that the intervention aims to instill traditional values in children to help prevent adolescent suicide and substance use, to teach parents and caregivers methods for coping with trauma and stress, and to teach positive parenting practices. He noted that one of the components within the Little Holy One project is to teach Indigenous culture to the children in the Head Start program, with cooperation and participation by 3-to-5-years-old and their primary caregiver. Beginning with children at that early age offers opportunities for children to establish their position in the community and their responsibilities to the community. He said that staying engaged with families for the long term is vital, and any research being conducted needs to involve local people and their families. Additionally, it is essential for interventions to be developed at the community level and to include spiritual, traditional, and cultural knowledge keepers.
Brockie shared that the timeline for the collaborative work used to develop these components emphasized the community-based participatory
research approach taken at all phases of development for the Little Holy One (see Figure 5). In 2011, Brockie conducted a study on the risk and protective factors for youth suicide in the Fort Peck Sioux and Assiniboine tribes. This study collected data from 288 Assiniboine and Sioux youth, 15–24 years of age, and found that historical trauma was associated with suicide ideation and attempts (Brockie, 2012). Brockie also found that communal mastery or group efficacy, tribal identity, and attachment to education was protective against substance use and suicide risk. Brockie emphasized that the findings from the study provided baseline data for developing Little Holy One.
Brockie explained that the goal of Little Holy One is to increase protective factors and decrease risk factors related to youth suicide and substance abuse, starting in early life. This goal is addressed through an intervention curriculum with 12 lessons: (1) four mental health-focused lessons designed to help parents/caregivers address their own experiences of stress and trauma, adapted from common elements treatment approach, (2) four lessons focused on developing parenting skills, adapted from Family Spirit,18 and (3) four cultural components designed to increase tribal identity and communal mastery and address contemporary and historical traumas. A randomized controlled trial is currently ongoing to determine whether and how the prevention program works to improve outcomes, and the immediate impact of cultural components on caregiver functioning (Brockie et al., 2021). If it is found to be effective, Little Holy One will be implemented at all Head Start sites in Fort Peck. Little Holy One is a starting point for future intervention in Fort Peck, Brockie concluded.
RESEARCH IN INDIGENOUS COMMUNITIES
Denise Dillard, an Inupiaq Eskimo, and the director of research for Southcentral Foundation, and Jennifer Shaw, who is of Ashkenazi Jewish and French-Canadian descent, and a medical anthropologist and senior researcher at Southcentral Foundation, discussed lessons learned from conducting research with Indigenous communities and described suicide prevention research conducted at Southcentral Foundation.
Dillard shared some historical experiences of research conducted in Indigenous communities. She said that biological samples have been used for research and stored in the Alaska Area Specimen Bank (AASB) for more than 70 years. In 2004, Alaska Native Tribal Health Organizations assumed
___________________
18 Family Spirit is an evidence-based home-visiting model designed by and for Indigenous families, and addresses intergenerational behavioral health problems, applies local cultural assets, and overcomes deficits in the professional health care workforce in low-resource communities. See https://caih.jhu.edu/programs/family-spirit (accessed August 21, 2022).
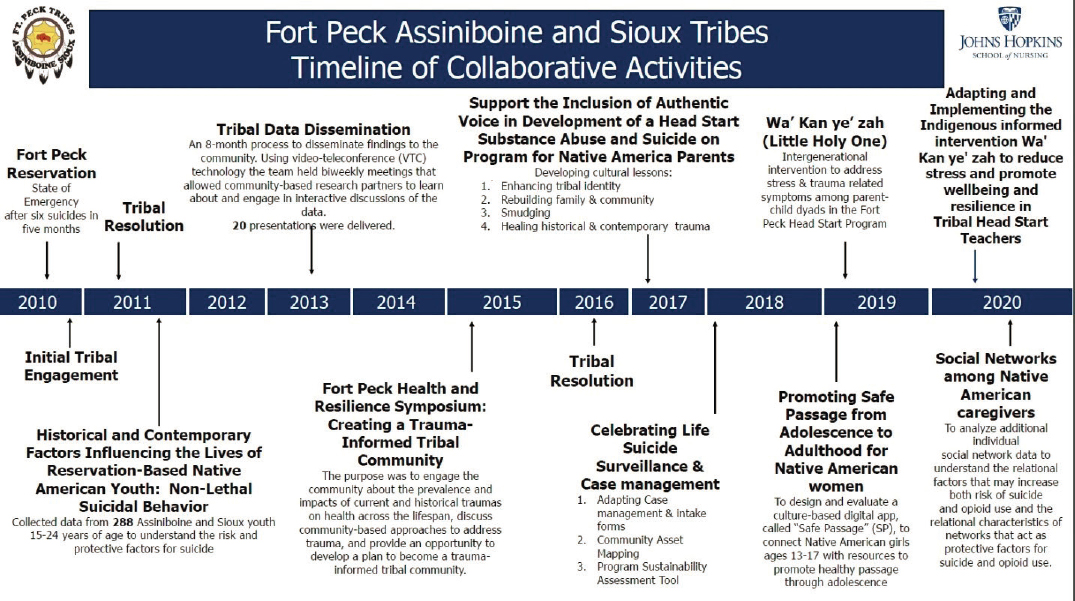
SOURCE: Brockie presentation, May 13, 2022. © 2022, Brockie, Johns Hopkins University, Use with permission only, all rights reserved.
shared ownership and management of the AASB with the CDC, and tribal leaders asked for research to explore how community members viewed storing biological samples for research. Researchers used a community-based participatory research approach with tribal and federal partners to explore the views of biobanking research among Indigenous community members and leaders (Hiratsuka et al., 2012a). Twenty-nine focus groups were conducted in 14 locations, with participation from 82 community members and 81 tribal leaders. Researchers identified five themes that contributed to participants’ views on biobanking. The themes were prior experiences with research and medical care; stigmatizations, relevance, and applicability; effects of governmental and cultural change; concerns about unknown capability of future technologies; and benefit for future generations. Respondents also raised specific cultural concerns along with global ethical concerns, as well as the potential promise of research in improving the health of Indigenous people.
Dillard said that researchers derived key lessons from the study about transparency, accessibility, and seeking community and participant input. These include the importance of being readily available to answer potential participants’ questions; gaining awareness of past research projects; working with the community to determine how to treat collected data and specimens with respect; providing clear, jargon-free information in consent forms (including a data and specimen destruction date); giving participants options through tiered consent; sharing information on progress throughout the research; returning results to participants and the community; and having community leaders review and approve study findings prior to publication and presentation (Hiratsuka et al., 2012b).
Dillard also shared the findings from another study that utilized four focus groups to examine perceptions of pharmacogenetics among Indigenous people, and participants saw both potential benefits and harms (Shaw et al., 2013). Study participants perceived pharmacogenetics to have potential benefits of improved health and health care as well as capacity building, but that it was a “double-edged sword” with the potential to both harm and help in Alaska Native communities, depending on how it was used. Study participants also discussed contingent conditions that could mitigate risks and increase acceptability of pharmacogenetics. Tribal people, governments, and health organizations are increasingly active as not only participants in research, but as agents of research, including the policies and procedures that regulate research and protect Indigenous research participants and communities, Dillard added. Southcentral Foundation maintains tribal sovereignty over research. All research that is conducted within its region must be approved by its board of directors, comprised entirely of Alaska Native people. Researchers must obtain not only approval for the detailed protocol but also concept approval prior to developing a full research plan. “The general idea is it needs
to be approved before any application for funding and there is approval of the very detailed plan of research, including all of the consent forms and any materials that go before participants” Dillard concluded.
Shaw also discussed two Southcentral Foundation studies supported by the Alaska IDeA Networks of Biomedical Research Excellence (INBRE) at the University of Alaska, Fairbanks, and the National Institute of General Medical Science on the use of predictive algorithms to identify risk of suicide in the tribal health system. Health systems are important sites for suicide prevention because they are part of the community in which people live and where they seek care for health issues. Shaw pointed out that self-report screening tools are important but limited in detecting suicide risk, and she explained that predictive analytic approaches hold promise for improving clinical suicide prevention efforts (Simon et al., 2018).
One study evaluated the accuracy of an electronic health record-based algorithm, developed by the Mental Health Research Network, for predicting suicide risk among Indigenous people in primary care settings (Shaw et al., 2022). The researchers analyzed electronic health records of patients aged 13 years and older with behavioral health diagnoses and primary care visits between October 1, 2016, and March 30, 2018, and identified 47,413 qualifying primary care visits. Suicide attempt occurred after 1.2 percent, or 589 visits. By applying the Mental Health Research Network19 algorithm to these data, researchers found that visits stratified in the top 5th percentile of predicted risk accounted for 40 percent of actual attempts during the study period. “That is, if we were to apply the algorithm in the health care system doing outreach or intervention with people whose visits were classified in that top 5 percentile, we could potentially intervene and prevent 40 percent of all actual suicide attempts” Shaw said.
Shaw also shared preliminary results of a recent study where tribal health system participants were interviewed to identify strategies for implementing the algorithm for suicide prevention in ways that are culturally acceptable, clinically effective, and operationally feasible within the tribal health system.20 A total of 30 participants, including 15 patients and 15 health system leaders and clinicians, were interviewed. Forty percent of the participants had a personal history of suicide ideation or attempt, and almost all had provided clinical care or informal support to a loved one who had experienced suicidality in some way. The participants universally endorsed using risk algorithms to prevent suicide in the health system, but also expressed some concerns. Shaw emphasized that there is support in a large tribal health system for an approach to suicide prevention that uses routinely collected medical record data, but she
___________________
19 See https://mhresearchnetwork.org/ (accessed August 21, 2022).
20 The article is currently in peer review.
suggested that implementation strategies for using risk algorithms to prevent suicide should include intentional, well-planned strategies for communication with individuals and the community about the use, intent, and application of this approach to suicide prevention. Secondly, the implementation should account for increased workload, referrals, and care coordination needs among staff tasked with outreach, assessment, intervention, and referral. In addition, the implementation should balance safety concerns with privacy concerns to ensure timely intervention and to sustain patients’ trust in the health system.
Data Governance in Indigenous Communities and Community Wellness
Stephanie Russo Carroll, of Ahtna and Sicilian descent, a citizen of the Native Village of Kluti-Kaah, and assistant professor as well as associate director of the Native Nations Institute at the University of Arizona, discussed the links between Indigenous governance, data sovereignty, the environment, and community wellness. Carroll defined Indigenous data as information and knowledge, in any format, that impacts Indigenous Peoples, nations, and communities at the collective and individual levels. “Indigenous Peoples have always been data creators, data users, and data stewards,” she emphasized. She noted that data were and continue to be embedded in Indigenous instructional practices and cultural principles, and transmitted orally as well as recorded through winter counts and other physical objects such as calendar sticks and totem poles.
Carroll said that ongoing colonization of Indigenous Peoples and globalization of Western ideas, values, and lifestyles have resulted in the suppression and co-optation of Indigenous knowledge and data systems (Carroll et al., 2019). These processes have limited the ability of Indigenous Peoples to recover, develop, and sustain their knowledge, an ability that is central to Indigenous Peoples’ capacity to realize their human rights and fulfill their roles and responsibilities. Indigenous Peoples bear the burden of disproportionately high disease and mortality rates in the United States, and Carroll said that while these rates vary across tribes, they result in high rates of premature death in Indigenous People. “The root of these health inequities lies in the systematic, coordinated, ongoing efforts to control, diminish, erase, and subjugate Indigenous Peoples while disconnecting them from their land,” Carroll said.
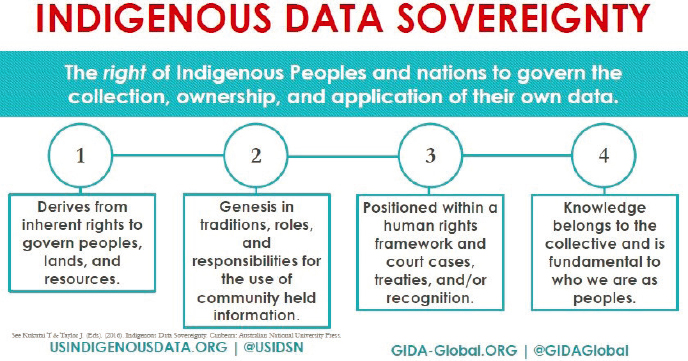
Carroll said that Indigenous data sovereignty is key to improving the overall well-being of Indigenous People. Indigenous data sovereignty is defined as the right of Indigenous Peoples and nations to govern the collection, ownership, and application of their own data (Rainie et al., 2017). It derives from the inherent right of Native nations to govern their peoples, lands, and resources, a right acknowledged in treaties and other legal mechanisms negotiated on a nation-to-nation basis with settler–colonial governments (see
Figure 6). She added that the concept of Indigenous data sovereignty as a collective right also may be positioned within an international Indigenous rights framework (Rainie et al., 2017).
Carroll said that the current movement toward open data and open science does not fully acknowledge the rights and interests of Indigenous Peoples. Focusing on greater data sharing alone creates a tension for Indigenous Peoples who are also asserting greater control over the application and use of Indigenous data and Indigenous knowledge for collective benefit. In response to this, academics and practitioners in the International Indigenous Data Sovereignty Interest Group within the Research Data Alliance led the development of the “CARE Governance for Indigenous Data Governance” (Collective Benefit, Authority to Control, Responsibility, and Ethics) published through the Global Indigenous Data Alliance (Carroll et al., 2020).
The CARE principles for Indigenous data governance empower Indigenous Peoples by shifting the focus from regulated consultation to value-based relationships that position data approaches within Indigenous cultures and knowledge systems to the benefit of Indigenous Peoples (Carroll et al., 2021). The principles set forth critical considerations for nontribal data creators, stewards, and users, and are designed to guide the inclusion of Indigenous Peoples in data governance and to advance Indigenous Peoples’ self-determination and collective benefit (Carroll et al., 2020; see Figure 7). Carroll explained that the CARE principles complement the existing data-centric approach represented in the FAIR (Findable, Accessible, Interoperable, and Reusable) principles (Wilkinson et al., 2016), which aim to increase data sharing. Applying FAIR with CARE
SOURCE: Carroll presentation, June 10, 2022.
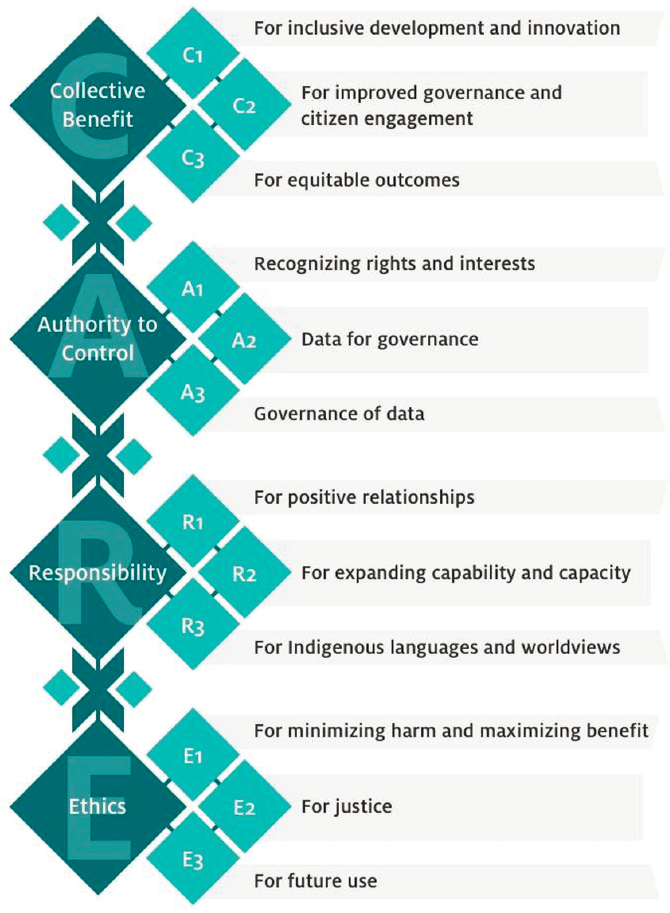
SOURCE: Carroll presentation, June 10, 2022; Carroll et al., 2020.
allows Indigenous Peoples to access their data and share their data on their own terms (Carroll et al., 2021).
Carroll said that it is essential to make ethical Indigenous data governance a reality and to create laws, policies, ethics, and infrastructure that support Indigenous rights to Indigenous data throughout the data lifecycle and across the
data ecosystem. Protecting and strengthening these rights would require making changes across data actors such as research institutions, repositories, publishers, and funders. She presented six suggestions for institutions to advance data governance. The suggestions include centering Indigenous Peoples in leadership and scholarship, enriching metadata, recognizing Indigenous intellectual property through appropriate authorship and acknowledgement, protecting both personal and community identifiable information, formalizing voluntary guidelines, and tracking the use and reuse of Indigenous data for research reporting and compliance. Carroll concluded that “these integrative strategies hold dual benefit for addressing historic inequities and barriers faced by Indigenous and marginalized peoples while also facilitating self-determined Indigenous and community-led efforts that allow for mobilization of Indigenous knowledge.”
OPPORTUNITIES TO IMPROVE INTERVENTIONS FOR SUICIDE PREVENTION
The section that follows discusses policy, programs, and research opportunities to advance suicide prevention efforts across Indigenous communities.
Policy Opportunities
The Honorable Tina Smith, United States Senator from Minnesota, and Richard McKeon, chief of the Suicide Prevention Branch at the Substance Abuse and Mental Health Services Administration (SAMHSA), spoke about policy opportunities to advance suicide prevention efforts across Indigenous communities.
Native Behavioral Health Access Improvement Act
Honorable Smith said that generations of trauma and systemic underfunding of tribal housing, health, education, and other programs have caused serious harm to Indigenous communities in the United States. Mental health care is especially difficult to access in Indian country. She said only 39 percent of IHS facilities provide 24-hour mental health crisis intervention services and 10 percent of IHS facilities do not provide any crisis intervention services (Levinson, 2011).
Honorable Smith said that with this in mind, she and Senator Kevin Cramer, United States Senator from North Dakota introduced the Native Behavioral Health Access Improvement Act, a bipartisan bill to create a special mental health care program for Indigenous people. She mentioned that the program would be modeled after the Special Diabetes Program for
Indians21 and it would support the work of tribes to improve the mental health of their communities. “We have a responsibility to make sure all Native communities on tribal lands and in urban areas have the resources they need to provide culturally competent mental health care across the whole continuum. This includes prevention, treatment, and recovery care,” Honorable Smith said. “We can all help to break the stigma by checking in on each other and having open and honest conversations about mental health,” she concluded.
Garrett Lee Smith State/Tribal Youth Suicide Prevention Grant Program and Tribal Behavioral Health Grant Program
Richard McKeon, chief of the Suicide Prevention Branch at SAMHSA, described two SAMHSA suicide prevention grant programs that focus on suicide prevention among Indigenous youth. First, McKeon talked about the Garrett Lee Smith (GLS) Memorial Suicide Prevention Program. Passed in 2004, the GLS Memorial Act established and authorized several suicide prevention programs including the National Suicide Prevention Resource Center, the Campus Suicide Prevention Program, and the GLS State and Tribal Youth Suicide Prevention Grant Program (U.S. Congress, 2004). The GLS State and Tribal Suicide Prevention Grant Program was designed to assist states and tribes with providing funding and technical support for comprehensive youth suicide prevention activities. Since the passage of the law, more than 200 grants have been awarded to all 50 states and Washington, DC, two territories, and more than 50 tribes.
McKeon said that grantees have implemented a broad array of prevention strategies such as screening; community gatekeeper training; developing coalitions and partnerships across various youth-serving agencies (e.g., schools, foster care systems, juvenile justice, and care providers for mental health and substance use disorders); developing policies and protocols; and supporting hotlines. Of all of these different activities, the most commonly supported activity is gatekeeper training, in which different groups in the community are trained on identifying the warning signs of suicide and what to do in response. One grant requirement is to follow up with youth who are discharged from emergency departments or from inpatient units because of suicide attempts in order to reduce the significant risk of future attempts.
Several studies have been conducted to examine the impact of the GLS State and Tribal Youth Suicide Prevention Grant Program on suicide mortality in counties that have implemented the program (Godoy Garraza et al., 2015,
___________________
21 See https://www.ihs.gov/sdpi/ (accessed August 21, 2022).
2019; Goldston et al., 2010; Walrath et al., 2015). McKeon shared data from a study that examined whether a reduction in youth suicide mortality that occurred between 2007 and 2010 could be attributed to GLS program efforts (Walrath et al., 2015). The researchers found that counties implementing GLS training had significantly lower suicide rates among the population aged 10 to 24 years in the year after GLS training than did similar counties that did not implement GLS training. The researchers did not find a significant difference in terms of adult suicide mortality rates in those counties.
McKeon also shared data from a study to determine whether the GLS program had an effect on nonfatal suicide attempts. He said that for different methodological reasons, the researchers focused on ages 16 to 23 years across 46 states and 12 tribal communities (Godoy Garraza et al., 2015). They compared 466 counties implementing the GLS program between 2006 and 2009 with 1,161 counties that shared key pre-intervention characteristics but were not exposed to the GLS program. The researchers found that counties implementing GLS program activities had significantly lower suicide attempt rates among youths 16 to 23 years of age in the year following implementation of the GLS program than did similar counties that did not implement GLS program activities. However, the effect of the program dissipated a year after the implementation. He said that led to a number of questions: “Was there any difference in youth suicide mortality as a result of the grant that could extend beyond the first year after implementation? Also, did the years of exposure to these grants make a difference? And was the impact different in rural communities?”
McKeon said that in 2019, another study was conducted to try to answer these questions (Godoy Garraza et al., 2019). Researchers focused on counties that were initially exposed to GLS programs before 2010 for which there were up to six years of follow-up information available at the time. They compared 525 counties exposed to the GLS program activities with unexposed matched control counties on county-level suicide mortality rates among youth ages 10 to 24. One year after implementing program activities, youth suicide mortality rates were 0.9 per 100,000 deaths lower among exposed counties than control counties. Two years after implementation of program activities, youth suicide mortality rates continued to be lower in exposed communities than control communities. Researchers found that those counties exposed to multiple consecutive years of program implementation saw a larger decrease in youth suicide mortality rates compared to counties with a single year of exposure. Additionally, researchers found a 20 percent stronger impact in rural counties than in non-rural counties. Again, no effect was seen for adult suicide mortality or nonsuicidal youth mortality. McKeon emphasized that youth suicide prevention needs to be embedded on an ongoing basis. It cannot be one-and-done. “You can’t stop
the funding and then hope the impact will continue. It needs to be continually funded to be able to have the impact,” he added.
The second program that McKeon described was the Native Connections Grant Program, also referred to as Tribal Behavioral Health grants. This five-year grant program is available only to federally recognized tribes, tribal organizations, and tribal consortia to help Indigenous communities identify and address the mental health needs of Native youth. Over 240 grants have been awarded since this program was first initiated six years ago.22 The program was designed with the recognition that each tribe has a unique culture and intensive efforts are undertaken to study the needs and the strengths of each community. The program supports grantees in reducing suicidal behavior and substance use among Native youth up to age 24, easing the impacts of substance use, mental illness, and trauma in tribal communities, and supporting youth as they transition into adulthood.
McKeon listed the key principles for the Native Connections Grant program: Funded activities should be community driven, strengths-based, grounded in community readiness, identify the gaps, pilot solutions, foster partnerships and innovation in serving Indigenous youth, supported by Indigenous technical assistance, and evaluated for effectiveness in saving lives. McKeon concluded that the first year of a Native Connections grant involves understanding the cultural and political context, doing a community systems analysis and a community readiness assessment, and then working toward development of a strategic action plan that includes a crisis and follow-up protocol development.
Research Opportunities
Lisa Wexler, professor in the School of Social Work and research professor in the Research Center for Group Dynamics in the Institute of Social Research at the University of Michigan, Ann Arbor, discussed some broad challenges in suicide prevention research in Indigenous communities, as well as opportunities for advancement. Wexler said that the core component of the initial work to make suicide a “never event” in Indigenous communities is to acknowledge structural violence and historical and ongoing colonization, and to uplift the culture and context of Indigenous communities. Wexler emphasized that it is essential for academic institutions and social services to engage with tribal communities in partnerships and as advocates toward self-determination on both a personal and collective level for suicide prevention. She said that “building on strength means that we need to begin to invest in communities
___________________
22 See https://www.samhsa.gov/native-connections (accessed August 21, 2022).
as a whole and to support upstream strategies as well as those that are more dominantly invested in the United States.”
Wexler noted that suicide research and care is underfunded in the United States given that suicide is among the top causes of death in the United States (Fortgang and Nock, 2021). The national investment in reducing deaths from suicide is the lowest compared to the other causes of death, Wexler stressed. She highlighted a few challenges in current suicide research in the United States. First, she said that most of the current research on suicide is focused specifically on individual-level risk and acute risk. By limiting the focus to individual risks, researchers miss significant strategies that are more holistic and integrated, which can decrease risk in entire populations (Wexler et al., 2015). She emphasized that research focused on individual risk can amplify deficits and ignore strengths. Additionally, the vast majority of suicide prevention research focuses only on the present situation and ignores the past and historical collective experiences that put certain populations at greater risk. She said that the “decontextualized scientific perspective” being perpetuated in most U.S. suicide research tends to ignore community and familial relationships, including those that span spirituality, interpersonal relationships, community, and tribes. Wexler emphasized that “Indigenous suicide research requires looking at historical trauma and intergenerational views.”
Moreover, Wexler said that current research tends to be problem focused, partly because of current funding mechanisms (Trout et al., 2018). Often these types of research are about developing programs or only specific kinds of interventions (Allen et al., 2022). This, however, misses out on shared risk and protective factors. Limiting research to only the development of specific kinds of interventions misses opportunities to promote health and well-being across communities, especially those that are suffering because of intentional past marginalization and disempowerment. Wexler said that research that instead focuses on shared risk and protective factors can decrease suicide risk and increase well-being overall because people do not live “problem-focused lives.”
Wexler said that current suicide prevention research often becomes integrated and aggregated across time at the expense of missing potential learning from specificity. Combining estimates of suicide rates and other data overlooks the distinct identities among Indigenous communities and the ways people take care of and protect each other. Wexler emphasized that Indigenous communities are diverse and can have significantly different practices, leadership structures, ways of supporting spirituality, and languages. Additionally, Wexler said that using “top-down” types of interventions that may be effective in other populations ignores tribal relationships and the meaning of existing complex systems. She said that one limitation of the “top-down” approach is that it misses out on locally specific innovations that might be incredibly important to protecting the well-being of people within their communities.
In conclusion, Wexler said that suicide is almost exclusively seen as a mental health issue. Current interventions concentrate on identifying people in acute crisis and referring them to systems of professionalized care outside of the communities and families in which the individual lives, despite the strong cultural and family values of Indigenous communities that can be used to build strength-based systems of care. Additionally, current suicide research often ignores factors that negatively affect outcomes, including marginalization, racism, colonialism, lack of housing, lack of access to resources, lack of employment, and other social determinants that influence people’s lives (Levit, 2019). It is essential to acknowledge harms and move toward a more equitable system, Wexler said, concluding that “It is important to begin to move from risk-only research to understand the strengths of communities, think of research as ceremony and process creation with the inclusion of local leaders and voices to improve empowerment, self-determination, and community development, and honor scientific and Indigenous knowledge.”
WRAP-UP
Brockie reflected that this workshop on suicide prevention in Indigenous communities convened experts who are currently doing work across Indigenous communities to examine suicide risk and protective factors in Indigenous populations, discuss culturally appropriate and effective suicide prevention policies and programs, explore existing data systems and how data can be used for tracking suicide rates, and consider gaps and challenges in providing the continuum of care services for substance use and mental health disorders in multiple health care settings across Indigenous communities.
Throughout the series of webinars, the strengths and resiliency of Indigenous communities were highlighted as well as the risks for suicide. Brockie noted that acknowledging the structural violence in Indigenous communities is critical to enhancing resilience of Indigenous populations and reducing their risk of suicide. She observed that several participants emphasized the importance of learning from Indigenous communities. Several other participants stressed the importance of engaging families and local supports, focusing on health promotion and well-being, and self-governance and self-determination. “Looking toward solutions, we must first assess our challenges,” she added.
Several participants called attention to the role and importance of culture and traditional and spiritual leaders in health promotion and suicide intervention programs. Cultural knowledge and practices based on traditional beliefs, such as prayer, familial bonds, connections to the land, and language are foundational to the health and well-being of Indigenous people. Traditional and spiritual community leaders, healers, and members are a critical part of promoting this protective culture.
The approaches taken to prevent suicide in Indigenous communities need to consider the unique characteristics and practices of different tribes and communities, and development of successful interventions for suicide prevention requires culturally appropriate research and a community-based approach. Aggregated research data on Indigenous populations assumes a monolithic identity for all tribes, thus ignoring fundamental differences in cultural beliefs, practices, language, and leadership structure between tribes.
Brockie observed that several speakers emphasized the importance of improving data collection to advance suicide prevention efforts. Current data on suicide rates among Indigenous populations are often incomplete because of racial misclassification and inconsistent data collection. Additionally, data on the risks among subgroups within the communities, such as Two-Spirit people, are often incomplete. She emphasized that Indigenous populations are more willing to take part in research and data collection when the process is transparent and informs participants about how the data will be used. Brockie urged all participants to continue to pursue culturally appropriate opportunities to prevent suicide among Indigenous populations and to improve community well-being.
REFERENCES
Allen, J., G. V. Mohatt, C. C. T. Fok, D. Henry, and R. Burkett. 2014. A protective factors model for alcohol abuse and suicide prevention among Alaska Native youth. American Journal of Community Psychology 54(1–2):125–139.
Allen, J., S. M. Rasmus, C. C. T. Fok, B. Charles, and D. Henry. 2018. Multi-level cultural intervention for the prevention of suicide and alcohol use risk with Alaska Native youth: A nonrandomized comparison of treatment intensity. Prevention Science 19(2):174–185.
Allen, J., L. Wexler, and S. Rasmus. 2022. Protective factors as a unifying framework for strength-based intervention and culturally responsive American Indian and Alaska Native suicide prevention. Prevention Science 23(1):59–72.
Angelino, A., T. Evans-Campbell, and B. Duran. 2020. Assessing health provider perspectives regarding barriers American Indian/Alaska Native transgender and Two-Spirit youth face accessing healthcare. Journal of Racial and Ethnic Health Disparities 7(4):630–642.
Beaudoin, V., M. Séguin, N. Chawky, W. Affleck, E. Chachamovich, and G. Turecki. 2018. Protective factors in the Inuit population of Nunavut: A comparative study of people who died by suicide, people who attempted suicide, and people who never attempted suicide. International Journal of Environmental Research and Public Health 15(1):144.
Best, A. F., E. A. Haozous, A. Berrington de Gonzalez, P. Chernyavskiy, N. D. Freedman, P. Hartge, D. Thomas, P. S. Rosenberg, and M. S. Shiels. 2018. Premature mortality projections in the USA through 2030: A modelling study. The Lancet Public Health 3(8):e374–e384.
Brockie, T. N. 2012. Historical and contemporary factors influencing non-lethal suicidal behavior among reservation-based Native American youth. PhD diss., Brockie, Teresa N.: Baltimore, MD: The Johns Hopkins University ProQuest Dissertations Publishing.
Brockie, T., E. E. Haroz, K. E. Nelson, M. Cwik, E. Decker, A. Ricker, S. Littlepage, J. Mayhew, D. Wilson, L. Wetsit, and A. Barlow. 2021. Wakȟáŋyeža (little holy one)—an intergenerational intervention for Native American parents and children: A protocol for a randomized controlled trial with embedded single-case experimental design. BMC Public Health 21(1).
Brockie, T. N., G. Dana-Sacco, G. R. Wallen, H. C. Wilcox, and J. C. Campbell. 2015. The relationship of adverse childhood experiences to PTSD, depression, poly-drug use and suicide attempt in reservation-based Native American adolescents and young adults. American Journal of Community Psychology 55(3–4):411–421.
Bush, A., and F. Qeadan. 2020. Social support and its effects on attempted suicide among American Indian/Alaska Native youth in New Mexico. Archives of Suicide Research 24(sup1):337–359.
Carroll, S. R., D. Rodriguez-Lonebear, and A. Martinez. 2019. Indigenous data governance: Strategies from United States Native nations. Data Science Journal 18(1):31.
Carroll, S. R., I. Garba, O. L. Figueroa-Rodríguez, J. Holbrook, R. Lovett, S. Materechera, M. Parsons, K. Raseroka, D. Rodriguez-Lonebear, R. Rowe, R. Sara, J. D. Walker, J. Anderson, and M. Hudson. 2020. The care principles for Indigenous data governance. Data Science Journal 19.
Carroll, S. R., E. Herczog, M. Hudson, K. Russell, and S. Stall. 2021. Operationalizing the CARE and FAIR principles for Indigenous data futures. Scientific Data 8(1).
CDC (Centers for Disease Control and Prevention). 2021. Tribal suicide prevention. https://www.cdc.gov/suicide/programs/tribal/index.html (accessed July 26, 2022).
CDC. 2022. Prevention strategies. https://www.cdc.gov/suicide/prevention/index.html (accessed August 3, 2022).
Center for American Indian Health. 2021. Culture forward: A strengths and culture based tool to protect our native youth from suicide. Johns Hopkins University. https://caih.jhu.edu/assets/documents/CULTURE_FORWARD_FULL_GUIDE_Web.pdf (accessed August 15, 2022).
Cwik, M. F., A. Barlow, N. Goklish, F. Larzelere-Hinton, L. Tingey, M. Craig, R. Lupe, and J. Walkup. 2014. Community-based surveillance and case management for suicide prevention: An American Indian tribally initiated system. American Journal of Public Health 104 Suppl 3(S3):e18–23.
Cwik, M. F., L. Tingey, A. Maschino, N. Goklish, F. Larzelere-Hinton, J. Walkup, and A. Barlow. 2016. Decreases in suicide deaths and attempts linked to the White Mountain Apache suicide surveillance and prevention system, 2001–2012. American Journal of Public Health 106(12):2183–2189.
Dial, S., A. Anderson, B. Underwood, D. Carpitche, and T. Scalise. 2019. Outcome story: Chickasaw Nation Departments of Health and Family Services. Zero Suicide, Education Development Center. https://zerosuicide.edc.org/evidence/outcome-story/chickasaw-nation-departments-health-and-family-services (accessed August 15, 2022).
Ehlman, D. C. 2022. Changes in suicide rates—United States, 2019 and 2020. MMWR: Morbidity and Mortality Weekly Report 71.
Felitti, V. J., R. F. Anda, D. Nordenberg, D. F. Williamson, A. M. Spitz, V. Edwards, M. P. Koss, and J. S. Marks. 1998. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. American Journal of Preventive Medicine 14(4):245–258.
Felitti, V. J., R. F. Anda, D. Nordenberg, D. F. Williamson, A. M. Spitz, V. Edwards, M. P. Koss, and J. S. Marks. 2019. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) study. American Journal of Preventive Medicine 56(6):774–786.
Fortgang, R. G., and M. K. Nock. 2021. Ringing the alarm on suicide prevention: A call to action. Psychiatry 84(2):192–195.
Freemantle, J., I. Ring, T. G. Arambula Solomon, F. C. Gachupin, J. Smylie, T. L. Cutler, and J. A. Waldon. 2015. Indigenous mortality (revealed): The invisible illuminated. American Journal of Public Health 105(4):644–652.
Godoy Garraza, L., C. Walrath, D. B. Goldston, H. Reid, and R. McKeon. 2015. Effect of the Garrett Lee Smith Memorial Suicide Prevention Program on suicide attempts among youths. JAMA Psychiatry 72(11):1143.
Godoy Garraza, L., N. Kuiper, D. Goldston, R. McKeon, and C. Walrath. 2019. Long-term impact of the Garrett Lee Smith Youth Suicide Prevention Program on youth suicide mortality, 2006–2015. Journal of Child Psychology and Psychiatry 60(10):1142–1147.
Goldston, D. B., C. M. Walrath, R. McKeon, R. W. Puddy, K. M. Lubell, L. B. Potter, and M. S. Rodi. 2010. The Garrett Lee Smith Memorial Suicide Prevention Program. Suicide and Life-Threatening Behavior 40(3):245–256.
Gone, J. P., and J. E. Trimble. 2012. American Indian and Alaska Native mental health: Diverse perspectives on enduring disparities. Annual Review of Clinical Psychology 8(1):131–160.
Gonzalez, M. B., B. D. Aronson, S. Kellar, M. L. Walls, and B. L. Greenfield. 2017. Language as a facilitator of cultural connection. Ab-Original 1(2):176–194.
Hallett, D., M. Chandler, and C. Lalonde. 2007. Aboriginal language knowledge and youth suicide. Cognitive Development 22:392–399.
Haroz, E. E., C. G. Walsh, N. Goklish, M. F. Cwik, V. O’Keefe, and A. Barlow. 2020. Reaching those at highest risk for suicide: Development of a model using machine learning methods for use with Native American communities. Suicide and Life-Threatening Behavior 50(2):422–436.
Hartmann, W. E., and J. P. Gone. 2016. Psychological-mindedness and American Indian historical trauma: Interviews with service providers from a Great Plains reservation. American Journal of Community Psychology 57(1–2):229–242.
Hiratsuka, V., J. Brown, and D. Dillard. 2012a. Views of biobanking research among Alaska Native people: The role of community context. Progress in Community Health Partnerships 6(2):131–139.
Hiratsuka, V., J. K. Brown, T. J. Hoeft, and D. A. Dillard. 2012b. Alaska Native people’s perceptions, understandings, and expectations for research involving biological specimens. International Journal of Circumpolar Health 71(1):18642.
Hofstra, E., C. Van Nieuwenhuizen, M. Bakker, D. Özgül, I. Elfeddali, S. J. De Jong, and C. M. Van Der Feltz-Cornelis. 2020. Effectiveness of suicide prevention interventions: A systematic review and meta-analysis. General Hospital Psychiatry 63:127–140.
IHS (Indian Health Services). 2022. About IHS. https://www.ihs.gov/aboutihs (accessed August 8, 2022).
Indian Affairs Department. March 8, 2021. New Mexico Indian Affairs Department partners with honoring Native life to host a suicide prevention training series for behavioral health providers in tribal communities. Press Release. https://indiancountrytoday.com/the-press-pool/new-mexico-indian-affairs-department-partners-with-honoring-native-life-to-host-a-suicide-prevention-training-series-for-behavioral-health-providers-in-tribal-communities (accessed July 26, 2022).
Kahn-John, M. 2016. The path to development of the Hózhó Resilience Model for nursing research and practice. Applied Nursing Research 29:144–147.
Kahn-John, M., and M. Koithan. 2015. Living in health, harmony, and beauty: The Diné (Navajo) Hózhó wellness philosophy. Global Advances in Health and Medicine 4(3):24–30.
Kahn-John, M., T. Badger, M. M. McEwen, M. Koithan, D. S. Arnault, and T. M. Chico-Jarillo. 2021. The Diné (Navajo) Hózhó lifeway: A focused ethnography on intergenerational understanding of American Indian cultural wisdom. Journal of Transcultural Nursing 32(3):256–265.
Kalweit, A., M. Clark, and J. Ishcomer-Aazami. 2021. Determinants of racial misclassification in COVID-19 mortality data: The role of funeral directors and social context. American Indian Culture and Research Journal 44(3):15–36.
Kazdin, A. E. 2008. Evidence-based treatment and practice: New opportunities to bridge clinical research and practice, enhance the knowledge base, and improve patient care. American Psychologist 63(3):146–159.
Kegler, S. R., T. R. Simon, M. L. Zwald, M. S. Chen, J. A. Mercy, C. M. Jones, M. C. Mercado-Crespo, J. M. Blair, D. M. Stone, P. G. Ottley, and J. Dills. 2022. Vital signs: Changes in firearm homicide and suicide rates—United States, 2019–2020. MMWR: Morbidity and Mortality Weekly Report 71(19):656–663.
Khan, S. Q., A. Berrington De Gonzalez, A. F. Best, Y. Chen, E. A. Haozous, E. J. Rodriquez, S. Spillane, D. A. Thomas, D. Withrow, N. D. Freedman, and M. S. Shiels. 2018. Infant and youth mortality trends by race/ethnicity and cause of death in the United States. JAMA Pediatrics 172(12):e183317.
LaFromboise, T. D., and H. A. Lewis. 2008. The Zuni Life Skills Development Program: A school/community-based suicide prevention intervention. Suicide and Life-Threatening Behavior 38(3):343–353.
Layman, D. M., J. Kammer, E. Leckman-Westin, M. Hogan, J. Goldstein Grumet, C. D. Labouliere, B. Stanley, J. Carruthers, and M. Finnerty. 2021. The relationship between suicidal behaviors and zero suicide organizational best practices in outpatient mental health clinics. Psychiatric Services 72(10):1118–1125.
Leavitt, R. A., A. Ertl, K. Sheats, E. Petrosky, A. Ivey-Stephenson, and K. A. Fowler. 2018. Suicides among American Indian/Alaska Natives—National Violent Death Reporting System, 18 states, 2003–2014. MMWR: Morbidity and Mortality Weekly Report 67(8):237–242. http://dx.doi.org/10.15585/mmwr.mm6708a1.
Levinson, D. R. 2011. Access to mental health services at Indian Health Service and tribal facilities. Rockville, MD: Department of Health and Human Services, Office of Inspector General. https://oig.hhs.gov/oei/reports/oei-09-08-00580.pdf (accessed August 16, 2022).
Levit, R. 2019, April 26. The empty promise of suicide prevention. The New York Times.
Mann, J. J., C. A. Michel, and R. P. Auerbach. 2021. Improving suicide prevention through evidence-based strategies: A systematic review. American Journal of Psychiatry 178(7):611–624.
Manolakis, P. G., and J. B. Skelton. 2010. Pharmacists’ contributions to primary care in the United States collaborating to address unmet patient care needs: The emerging role for pharmacists to address the shortage of primary care providers. American Journal of Pharmaceutical Education 74(10):S7.
Mohatt, G. V., C. C. T. Fok, D. Henry, and J. Allen. 2014. Feasibility of a community intervention for the prevention of suicide and alcohol abuse with Yup’ik Alaska Native youth: The Elluam Tungiinun and Yupiucimta Asvairtuumallerkaa studies. American Journal of Community Psychology 54(1–2):153–169. https://doi.org/10.1007/s10464-014-9646-2.
Mospan, C. M., C. Gillette, J. McKee, and S. S. Daniel. 2019. Community pharmacists as partners in reducing suicide risk. The Journal of the American Board of Family Medicine 32(6):763–767.
NCIPC (National Center for Injury Prevention and Control). 2020. Suicide Prevention. https://www.cdc.gov/suicide/ (accessed August 5, 2022).
NCIPC. 2022. NCIPC suicide prevention funding. https://www.cdc.gov/injury/budget/suicidepreventionpolicy/SuicidePreventionInvestment.html (accessed July 26, 2022).
NIMH (National Institute of Mental Health). 2022. Suicide. https://www.nimh.nih.gov/health/statistics/suicide (accessed July 26, 2022).
Office of the Surgeon General (U.S.) and National Action Alliance for Suicide Prevention. 2012. Appendix C: Brief history of suicide prevention in the United States. Washington, DC: U.S. Department of Health and Human Services.
Painter, N. A., G. M. Kuo, S. P. Collins, Y. L. Palomino, and K. C. Lee. 2018. Pharmacist training in suicide prevention. Journal of the American Pharmacists Association 58(2):199–204.e192.
Pham, T. V., A. K. Fetter, A. Wiglesworth, L. F. Rey, M. L. Prairie Chicken, M. Azarani, A. Riegelman, and J. P. Gone. 2021. Suicide interventions for American Indian and Alaska Native populations: A systematic review of outcomes. SSM—Mental Health 1:100029.
Pham, T. V., A. Pomerville, R. L. Burrage, and J. P. Gone. 2022. An interview-based evaluation of an Indigenous traditional spirituality program at an urban American Indian health clinic. Transcultural Psychiatry: February 2022. https://doi.org/10.1177/13634615221076706.
Rainie, S. C., D. Rodriguez-Lonebear, and A. Martinez. 2017. Policy brief: Indigenous data sovereignty in the United States. Tucson, AZ: Native Nations Institute, University of Arizona. http://nni.arizona.edu/application/files/1715/1579/8037/Policy_Brief_Indigenous_Data_Sovereignty_in_the_United_States.pdf (accessed August 15, 2022).
Rasmus, S. M., B. Charles, and G. V. Mohatt. 2014. Creating Qungasvik (a Yup’ik intervention “toolbox”): Case examples from a community-developed and culturally-driven intervention. American Journal of Community Psychology 54(1–2):140–152. https://doi.org/10.1007/s10464-014-9651-5.
Rasmus, S. M., E. Trickett, B. Charles, S. John, and J. Allen. 2019. The Qasgiq model as an Indigenous intervention: Using the cultural logic of contexts to build protective factors for Alaska native suicide and alcohol misuse prevention. Cultural Diversity & Ethnic Minority Psychology 25(1):44–54. https://doi.org/10.1037/cdp0000243.
Robinson, M. 2020. Two-Spirit identity in a time of gender fluidity. Journal of Homosexuality 67(12):1675–1690.
Shaw, J. L., R. Robinson, H. Starks, W. Burke, and D. A. Dillard. 2013. Risk, reward, and the double-edged sword: Perspectives on pharmacogenetic research and clinical testing among Alaska Native people. American Journal of Public Health 103(12):2220–2225. https://doi.org/10.2105/AJPH.2013.301596.
Shaw, J. L., J. A. Beans, C. Noonan, J. J. Smith, M. Mosley, K. M. Lillie, J. P. Avey, R. Ziebell, and G. Simon. 2022. Validating a predictive algorithm for suicide risk with Alaska Native populations. Suicide Life and Life-Threatening Behavior 52(4):696–704. https://doi.org/10.1111/sltb.12853.
Simon, G. E., E. Johnson, J. M. Lawrence, R. C. Rossom, B. Ahmedani, F. L. Lynch, A. Beck, B. Waitzfelder, R. Ziebell, R. B. Penfold, and S. M. Shortreed. 2018. Predicting suicide attempts and suicide deaths following outpatient visits using electronic health records. The American Journal of Psychiatry 175(10):951–960. https://doi.org/10.1176/appi.ajp.2018.17101167.
Spillane, S., M. S. Shiels, A. F. Best, E. A. Haozous, D. R. Withrow, Y. Chen, A. Berrington de González, and N. D. Freedman. 2020. Trends in alcohol-induced deaths in the United States, 2000–2016. JAMA Network Open 3(2):e1921451. https://doi.org/10.1001/jamanetworkopen.2019.21451.
SPRC (Suicide Prevention Resources Center). 2022. Resources and programs. https://www.sprc.org/resources-programs (accessed August 4, 2022).
Stapelberg, N. J. C., J. Sveticic, I. Hughes, A. Almeida-Crasto, T. Gaee-Atefi, N. Gill, D. Grice, R. Krishnaiah, L. Lindsay, C. Patist, H. V. Engelen, S. Walker, M. Welch, S. Woerwag-Mehta, and K. Turner. 2021. Efficacy of the Zero Suicide framework in reducing recurrent suicide attempts: Cross-sectional and time-to-recurrent-event analyses. The British Journal of Psychiatry 219(2):427–436. https://doi.org/10.1192/bjp.2020.190.
Stover, A. N., J. E. Lavigne, and D. M. Carpenter. 2022. A scoping review of suicide prevention training programs for pharmacists and student pharmacists. American Journal of Pharmaceutical Education 8917. https://doi.org/10.5688/ajpe8917.
Stringer, H. 2018. The healing power of heritage. Monitor on Psychology 49(2).
Trevor Project. 2020. The Trevor Project Research Brief: American Indian/Alaskan Native Youth Suicide Risk. https://www.thetrevorproject.org/wp-content/uploads/2021/07/American-Indian-Alaskan-Native-LGBTQ-Youth-Research-Brief-Nov-2020.pdf (accessed July 29, 2022).
Trout, L., D. McEachern, A. Mullany, L. White, and L. Wexler. 2018. Decoloniality as a framework for Indigenous youth suicide prevention pedagogy: Promoting community conversations about research to end suicide. American Journal of Community Psychology 62(3–4):396–405. https://doi.org/10.1002/ajcp.12293.
U.S. Congress. 2004. S.2634—Garrett Lee Smith Memorial Act. https://www.congress.gov/bill/108th-congress/senate-bill/2634 (accessed August 19, 2022).
Walrath, C., L. G. Garraza, H. Reid, D. B. Goldston, and R. McKeon. 2015. Impact of the Garrett Lee Smith Youth Suicide Prevention Program on suicide mortality. American Journal of Public Health 105(5):986–993. https://doi.org/10.2105/ajph.2014.302496.
Walters, K. L., T. Evans-Campbell, J. M. Simoni, T. Ronquillo, and R. Bhuyan. 2006. “My spirit in my heart”: Identity experiences and challenges among American Indian Two-Spirit women. Journal of Lesbian Studies 10(1–2):125–149.
Warne, D., K. Dulacki, M. Spurlock, T. Meath, M. M. Davis, B. Wright, and K. J. McConnell. 2017. Adverse childhood experiences (ACE) among American Indians in South Dakota and associations with mental health conditions, alcohol use, and smoking. Journal of Health Care for the Poor and Underserved 28(4):1559–1577.
Warne, D., and D. Lajimodiere. 2015. American Indian health disparities: Psychosocial influences. Social and Personality Psychology Compass 9(10):567–579.
Wexler, L., M. Chandler, J. P. Gone, M. Cwik, L. J. Kirmayer, T. LaFromboise, T. Brockie, V. O’Keefe, J. Walkup, and J. Allen. 2015. Advancing suicide prevention research with rural American Indian and Alaska Native populations. American Journal of Public Health 105(5):891–899.
Wexler, L., D. McEachern, G. Difulvio, C. Smith, L. F. Graham, and K. Dombrowski. 2016. Creating a community of practice to prevent suicide through multiple channels: Describing the theoretical foundations and structured learning of PC CARES. International Quarterly of Community Health Education 36(2):115–122.
White, L. A., L. Wexler, A. Weaver, R. Moto, T. Kirk, S. Rataj, L. Trout, and D. McEachern. 2022. Implementation beyond the clinic: Community-driven utilization of research evidence from PC CARES, a suicide prevention program. American Journal of Community Psychology: 1–14. https://doi.org/10.1002/ajcp.12609.
WHO (World Health Organization). 2022. World mental health report: Transforming mental health for all. Geneva: World Health Organization. https://www.who.int/publications/i/item/9789240049338 (accessed August 15, 2022).
Wilkinson, M. D., M. Dumontier, I. J. Aalbersberg, G. Appleton, M. Axton, A. Baak, N. Blomberg, J.-W. Boiten, L. B. Da Silva Santos, P. E. Bourne, J. Bouwman, A. J. Brookes, T. Clark, M. Crosas, I. Dillo, O. Dumon, S. Edmunds, C. T. Evelo, R. Finkers, A. Gonzalez-Beltran, A. J. G. Gray, P. Groth, C. Goble, J. S. Grethe, J. Heringa, P. A. C. ’T Hoen, R. Hooft, T. Kuhn, R. Kok, J. Kok, S. J. Lusher, M. E. Martone, A. Mons, A. L. Packer, B. Persson, P. Rocca-Serra, M. Roos, R. Van Schaik, S.-A. Sansone, E. Schultes, T. Sengstag, T. Slater, G. Strawn, M. A. Swertz, M. Thompson, J. Van Der Lei, E. Van Mulligen, J. Velterop, A. Waagmeester, P. Wittenburg, K. Wolstencroft, J. Zhao, and B. Mons. 2016. The fair guiding principles for scientific data management and stewardship. Scientific Data 3(1):160018. https://doi.org/10.1038/sdata.2016.18.
Willmon-Haque, S., and S. D. BigFoot. 2008. Violence and the effects of trauma on American Indian and Alaska Native populations. Journal of Emotional Abuse 8(1–2):51–66.
This page intentionally left blank.




















































