
1
Introduction
Rapid detection of recognized or emerging infectious disease outbreaks is essential for timely public health response. The COVID-19 pandemic illuminated the strengths and limitations of the U.S. public health infrastructure, particularly the challenges to implementing widespread clinical testing, tracking asymptomatic infections, and anticipating community disease outbreaks. During the COVID-19 pandemic, wastewater surveillance1 gained traction as an additional epidemiological tool to monitor trends and anticipate disease incidence in communities.
Wastewater surveillance systems collect samples of untreated municipal wastewater that are then analyzed for the presence of biomarkers of infection, most commonly pathogen deoxyribonucleic acid (DNA) or ribonucleic acid (RNA) that are shed by infected persons (see Box 1-1; Figure 1-1). Whereas clinical laboratory testing and health services track individual cases of infection, testing for a pathogen at a wastewater treatment plant (also known as community-level wastewater surveillance) provides aggregate data from an entire community sewershed (i.e., the community population consisting of homes, businesses, and other institutions that share a common sewer system or drainage area). It does not track or identify
___________________
1 In this report and more broadly across the field of public health, “wastewater surveillance” describes the ongoing collection, analysis, and interpretation of and response to data related to the transmission of pathogens in wastewater for public health purposes. The committee acknowledges that the word “surveillance” is a charged term also used in other contexts to describe careful watching by the police, although that use is not intended in this report. See Chapter 4 for a discussion about privacy considerations associated with implementing a national wastewater surveillance system.
infectious disease for an individual person or household; rather, it detects the presence and changing quantities of a pathogen within the larger community. In the United States, 84 percent of households are connected to a wastewater treatment plant (U.S. Census, 2022). The sizes of communities served by an individual wastewater treatment plant can range widely, from very small plants that serve as few as 100 people to large plants that serve a few million people, with a median of approximately 45,000 people (A. Kirby, CDC, personal communication, 2022). The remaining unsewered
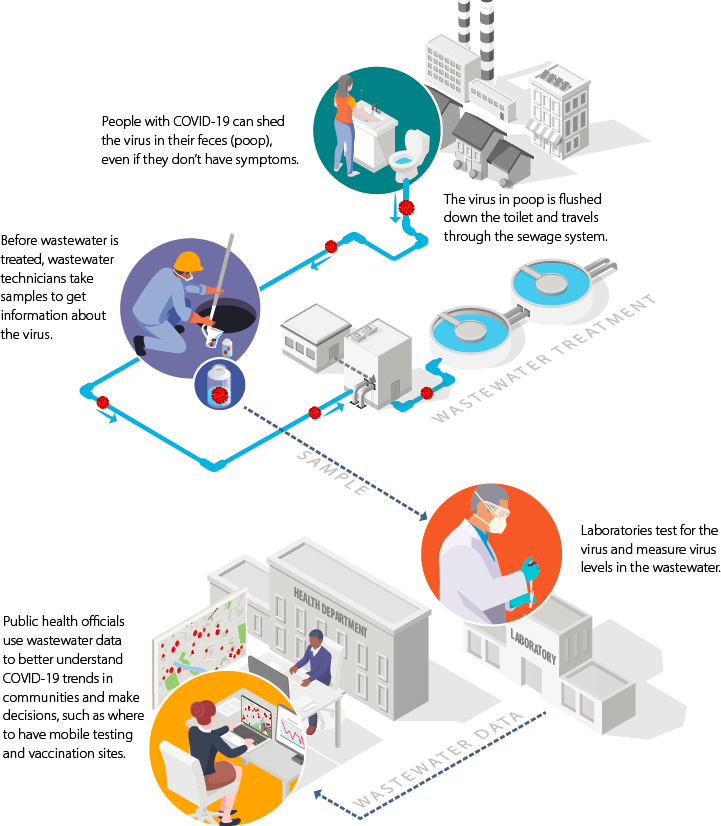
SOURCE: Adapted from https://www.cdc.gov/healthywater/surveillance/pdf/Wastewater-COVID-infographic-h.pdf.
population is not directly addressed by this epidemiological approach, although some members of this population regularly commute to sewered areas for work, school, or other activities.
Wastewater surveillance detects the genetic biomarkers of disease agents that have been discharged into a sewer. The measurement is inherently an indicator of the magnitude of the agent’s loading to wastewater, which can be interpreted to understand the prevalence of infection in a community. Wastewater surveillance can capture pre-symptomatic cases as well as infections across the spectrum of disease severity, including asymptomatic cases that may not result in an infected individual seeking medical care. However, interpretation of data may be confounded by variability in shedding levels and patterns, pathogen stability, and other factors.
The concept of wastewater-based epidemiology first emerged in the 1940s (Paul and Trask, 1941; Paul et al., 1940). A variety of wastewater surveillance initiatives occurred in the 1990s, 2000s, and 2010s, including the use of surveillance in global polio eradication efforts (see Box 1-2), to detect prevalence of the flu, and monitor the use of pharmaceutical and illicit drugs (Safford et al., 2022). The experience of applying wastewater surveillance to poliovirus and coronavirus has highlighted the unique value of wastewater surveillance as well as potential limitations to its application. (See Chapter 2 for an in-depth discussion of how wastewater surveillance has been useful in the COVID-19 pandemic.) In the remainder of this chapter, the committee discusses the development of the National Wastewater Surveillance System (NWSS) and the motivation for this study.
DEVELOPMENT OF THE NATIONAL WASTEWATER SURVEILLANCE SYSTEM
During the COVID-19 pandemic, broad interest in the potential usefulness of wastewater surveillance emerged. This led to the independent development of many local (e.g., sewershed and sub-sewershed; see Box 1-3) and hyperlocal (e.g., building or institution-based) wastewater surveillance efforts. As proof-of-concept was established for the feasibility and potential public health value of SARS-CoV-2 RNA detection and variant sequence identification, the implementation of these systems expanded. Wastewater surveillance was deployed at several locations across the United States and internationally to forecast and monitor disease outbreaks (see Table 1-1) and was found to be effective in capturing information about both asymptomatic and symptomatic infections as well as in predicting outbreaks (see Chapter 2 for more detail). Recognizing the need for centralization and coordination of these efforts, the U.S. Centers for Disease Control and Prevention (CDC) launched the NWSS in partnership with the U.S. Department of Health and Human Services (HHS) in September 2020. The NWSS
TABLE 1-1 Selected Examples of Ongoing Wastewater Surveillance Programs as of July 2022, Including Both Community and Institutional Scales
| Wastewater Program | Surveillance | Unique Aspects of the Program |
|---|---|---|
| State Programs | Missouri | Missouri was one of the first states to initiate wastewater surveillance testing. This project is a collaborative effort among the Missouri Department of Health and Senior Services, the Missouri Department of Natural Resources, and the University of Missouri. This project tracks SARS-CoV-2 viral load in the wastewater of more than 100 participating community water systems across Missouri.a |
| Ohio | The program involves large-scale collaboration among multiple state agencies, the U.S. Environmental Protection Agency Office of Research and Development, and numerous universities. Wastewater treatment plants are sampled throughout the state. The state developed a public-facing dashboard that depicts trends in wastewater results. | |
| Local Programs | Houston, Texas | The city collects wastewater samples from the 39 wastewater treatment plants within the city, as well as at lift stations within the sewershed and individual facilities. The city uses the wastewater data, along with other data sources such as individual clinical testing results and vaccination rates, to identify ZIP code-level “hot spots” for targeted public health intervention. The data are also used to monitor for early alerts of waves alongside other data such as emergency visits, general hospital bed use, and intensive care unit bed use. |
| Tempe, Arizona | The city quickly developed and implemented a wastewater surveillance program for SARS-CoV-2 by building off its existing opioid wastewater surveillance program. The City of Tempe, in partnership with Arizona State University’s Biodesign Institute, generates and uses sewage data to inform city decisions and operational strategies. | |
| Privately Funded Programs | San Francisco Bay Area, California | The privately funded Sewer Coronavirus Alert Network project is led out of Stanford University in collaboration with an industry partner. The project analyzes daily primary settled solids from 11 wastewater treatment plants in the San Francisco Bay Area, serving approximately 10,000 to more than 1,000,000 people. Originally focused on SARS-CoV-2, the project now reports the wastewater levels of a number of pathogens.b |
| New Haven, Connecticut | The Rothberg Fund supports a SARS-CoV-2 wastewater surveillance program at New Haven, Connecticut’s wastewater treatment facility, with joint efforts by Yale University and the New Haven Water Pollution Control Authority. Daily samples are collected, and results are updated weekly. This facility serves 200,000 people in the area.c |
| Wastewater Program | Surveillance | Unique Aspects of the Program |
|---|---|---|
| University Programs | University of California, San Diego | Under this ongoing program that started in May 2020, 340 buildings are monitored for viral activity, and more than 200 wastewater samplers are situated across the campus.d |
| University of Arizona, Tucson | The university first analyzed samples for SARS-CoV-2 from utilities across the country and then began analyzing samples collected on campus. The university has developed action levels for its campus wastewater surveillance program and used the wastewater data to prevent outbreaks. |
NOTE: Table includes both NWSS-funded community wastewater surveillance programs and privately funded programs.
a See https://storymaps.arcgis.com/stories/f7f5492486114da6b5d6fdc07f81aacf.
b See https://returntolearn.ucsd.edu/dashboard/index.html.
c See https://www.yalecovidwastewater.com.
d See http://wbe.stanford.edu.
SOURCE: Adapted from EPA (2021) unless otherwise noted.
is the first national-level wastewater disease surveillance system in the United States, and it coordinates with state-, tribal-, local-, and territorial-level health departments to design and integrate wastewater surveillance data to inform public health decisions. The mission of the NWSS is to
- offer technical assistance to public health departments and wastewater utilities implementing wastewater surveillance;
- coordinate a centralized and standardized data portal for tracking of disease presence across the country;
- establish working groups for health departments, public health laboratories, and wastewater utilities for knowledge sharing; and
- strengthen epidemiological and laboratory capacity for wastewater surveillance at health departments (Kirby et al., 2021).
Implementation
The rapid expansion and coordination of wastewater surveillance across the United States was an emergency response to the COVID-19 pandemic. SARS-CoV-2 was first detected in the United States in January 2020, and several wastewater surveillance efforts were under way in the spring of 2020, with support from local and state funding, federal emergency response grants, nongovernmental organizations, and philanthropic partners. By September 2020, formal pilot wastewater surveillance sites were established
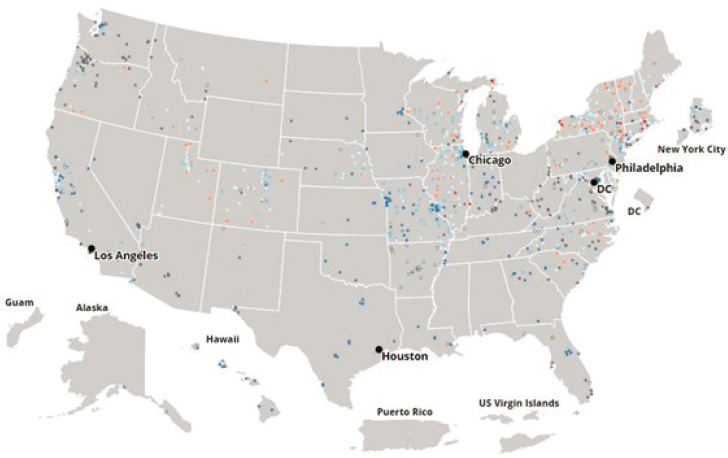
in eight states as part of the NWSS. As of October 2022, the NWSS comprises more than 1,250 sampling sites, covering a population of more than 133 million individuals. In fiscal year (FY) 2022, CDC awarded funding to support wastewater surveillance programs across 42 states, 5 cities, and 10 tribes.2 To supplement jurisdiction-led wastewater surveillance programs, the NWSS provides testing capacity for an additional 500 sites through a commercial testing contract.3 The NWSS continues to expand to new sites (Kirby, 2022). A map of participating sites and the distribution of sites as of October 2022 is illustrated in Figure 1-2. As shown by the map, the geographic distribution of sites is generally clustered near major metropolitan areas with a paucity of sites across the southern and intermountain western United States. NWSS sites are based in municipal wastewater systems; communities and populations that are unsewered are only captured in a wastewater surveillance system to the extent that individuals commute to a monitored sewershed for work, school, or other activities.
Implementation at NWSS-participating sites depends upon three primary entities—the health department, local wastewater utility, and analytical laboratory—to collect, test, and analyze samples and interpret the data (see Figure 1-1). Typically, local wastewater utilities collect, store, and distribute samples, which are used only for the NWSS and have no water quality regulatory implications. A public health, commercial, or academic laboratory partner analyzes the samples, and the public health department interprets the data to identify trends regarding infection prevalence within a community, integrate the wastewater data with other surveillance data, and determine the appropriate public health response. The multidisciplinary nature of a national wastewater surveillance system requires extensive collaboration between and across health departments, testing laboratories, and wastewater utilities. Historically, there has been limited collaboration between public health and wastewater departments (Clason, 2022), and active relationships across agencies rarely existed (McClary-Gutierrez et al., 2021).
At the national level, CDC provides funding support for these systems. CDC initially provided $2.5 million to support eight pilot NWSS sites, funded through the 2020 Coronavirus Aid, Relief, and Economic Security (CARES) Act.4 The number of sites was expanded through an additional $33 million provided through the Paycheck Protection Program. Initial funding for participating NWSS sites came from Epidemiology and Labora-
___________________
2 See https://www.cdc.gov/healthywater/surveillance/wastewater-surveillance/progress/index.html and https://www.cdc.gov/budget/fact-sheets/covid-19/funding/index.html.
3 See https://sam.gov/opp/c68491abc61e4f6392b14d1e1abaf7c7/view.
4Coronavirus Aid, Relief, and Economic Security Act of 2020, Public Law 116-136, 116th Cong., 2nd sess. (March 27, 2020).
SOURCE: https://covid.cdc.gov/covid-data-tracker/#wastewater-surveillance.
tory Capacity for Prevention and Control of Emerging Infectious Diseases (ELC) Cooperative Agreement grants provided by CDC to eligible health departments (i.e., state health departments, territories, and some large cities and counties).5 An additional $200 million in grants were made available from the ELC Enhancing Detection and Enhancing Detection Expansion program, supported by the Coronavirus Response and Relief Supplemental Appropriations Act of 2021.6 Finally, the NWSS was granted $384 million through the American Rescue Plan,7 starting in FY 2022 for use through 2025. In FY 2022, the NWSS supported wastewater surveillance initiatives in 42 states and 5 cities, with a total of $64 million in funding. The average amount awarded to each jurisdiction in FY 2022 was approximately $900,000.8 In addition, the NWSS has provided funding to 10 tribal communities to develop wastewater surveillance capacity through the Tribal
___________________
5 All 50 states, 5 cities, 1 county, and 8 territories have been awarded ELC funding. See https://www.cdc.gov/ncezid/dpei/elc/elc-recipient-history.html.
6Coronavirus Response and Relief Supplemental Appropriations Act of 2021, Public Law 116-260, 116th Cong., 2nd sess. (December 27, 2020).
7American Rescue Plan Act of 2021, Public Law 117–2, 117th Cong., 1st sess. (March 11, 2021).
8 See https://www.cdc.gov/budget/fact-sheets/covid-19/funding/index.html.
Public Health Capacity Building and Quality Improvement cooperative agreement.9
CDC also plays an important role in aggregating data and sharing the results from participating wastewater surveillance sites across the country. Data from the NWSS are communicated to the public, health officials, and policy makers through a variety of mechanisms, including a public-facing data dashboard, weekly summarized data briefs,10 a restricted-access data dashboard for health departments (Data Collation and Integration for Public Health Event Response [DCIPHER]), and weekly briefs for federal policy makers.11 The goal of the NWSS is for these data to be interpreted by public health officials and used to inform community health interventions, to raise public awareness of disease transmission within communities, and to track pathogen dynamics across the nation. CDC also coordinates Communities of Practice to build capacity among the participating localities and hosts monthly meetings with cohorts of participants across jurisdictions to share experiences and keep health officials apprised of updates or program improvements.
As part of the federal support for the NWSS, CDC and HHS also convene the National Sewage Surveillance Interagency Leadership (NSSIL) Committee, in which additional federal agencies collaborate and coordinate to exchange information and discuss agency-specific roles and activities.12 CDC, U.S. Environmental Protection Agency, U.S. Department of Defense, U.S. Department of Homeland Security, U.S. Geological Survey (USGS), National Institutes of Health, and U.S. Department of Veterans Affairs support implementing sewage sampling and developing guidance documents for use by public health officials. CDC and USGS coordinate to provide surge capacity for wastewater testing when needed. Federal agencies also coordinate to prioritize federal research on wastewater sampling, analysis, and interpretation. Finally, NSSIL coordinates with several nongovernmental organizations, including the Association of Public Health Laboratories, the Association of State and Territorial Health Officials, the Water Environment Federation, and the Water Research Foundation (see Figure 1-3).
Current Status and Future Outlook
As the COVID-19 pandemic continues with ongoing monitoring of emerging variants and subvariants and possibly transitions from emer-
___________________
9 See https://www.cdc.gov/tribal/cooperative-agreements/tribal-capacity-building-OT18-1803.html.
10 See https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html.
11 See https://covid.cdc.gov/covid-data-tracker/#wastewater-surveillance.
12 See https://www.cdc.gov/healthywater/surveillance/wastewater-surveillance/federal-coordination-partnering-wastewater-surveillance.html.
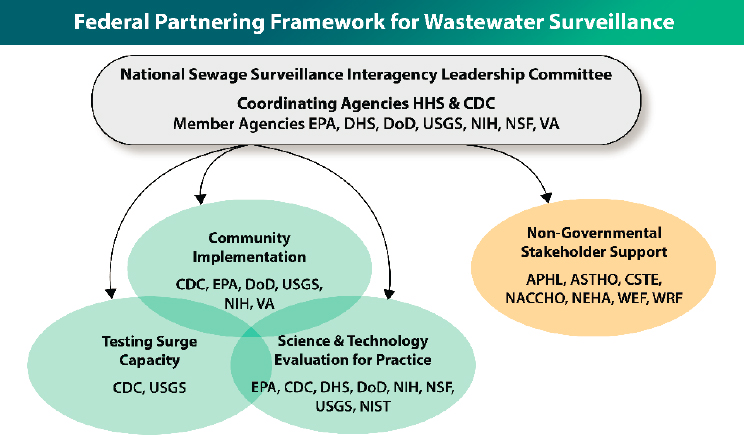
NOTES: APHL = Association of Public Health Laboratories; ASTHO = Association of State and Territorial Health Officials; CDC = U.S. Centers for Disease Control and Prevention; CSTE = Council of State and Territorial Epidemiologists; DHS = U.S. Department of Homeland Security; DoD = U.S. Department of Defense; EPA = U.S. Environmental Protection Agency; NACCHO = National Association of County and City Health Officials; NEHA = National Environmental Health Association; NIH = National Institutes of Health; NIST = National Institute of Standards and Technology; NSF = National Science Foundation; USGS = U.S. Geological Survey; VA = U.S. Department of Veterans Affairs; WEF = Water Environment Foundation; WRF = Water Research Foundation.
SOURCE: https://www.cdc.gov/healthywater/surveillance/wastewater-surveillance/federal-coordination-partnering-wastewater-surveillance.html.
gency response to endemic disease management, the application of wastewater surveillance as a public health tool will evolve. In particular, state, tribal, local, and territorial public health professionals; public utilities; and CDC are reviewing the usefulness of wastewater surveillance to inform public health decisions for SARS-CoV-2 as well as potential applications to other infectious pathogens. The surveillance system is also at a point of transition from an ad hoc collection of willing state and local participants seeking all useful information for local emergency pandemic response to a forward-looking national wastewater surveillance system that serves state, tribal, local, territorial, and national public health objectives simul-
taneously. Questions remain about what a standardized national wastewater surveillance system should look like, including ethical and privacy considerations; standard methodological approaches for data sampling, analysis, and interpretation; coordination or standardization among jurisdictions; and fundamental considerations of the technical feasibility of wastewater surveillance to monitor emerging diseases beyond COVID-19 in the United States. In addition, uncertainty remains around the use of wastewater surveillance to inform public health response, particularly how this form of disease monitoring can contribute to and complement traditional public health surveillance through clinical data and syndromic surveillance.
MOTIVATION FOR THE STUDY
CDC charged the National Academies of Sciences, Engineering, and Medicine to appoint a committee of academic and public health experts to review community-level wastewater surveillance and its potential value toward understanding and preventing infectious disease in the United States. The committee’s work has been divided into two parts as described in Box 1-4. The first phase, which is the focus of this report, provides an assessment of the usefulness of current community-level wastewater surveillance in the United States and its potential value for infectious disease beyond COVID-19. As explained in the statement of task, in the context of this study, “community-level” wastewater surveillance includes “sampling
at wastewater treatment plants” and does not include “local surveillance at neighborhood or institutional scales.” However, in committee discussions with the sponsor, hyperlocal sampling at specifically designated sentinel sites, such as likely points of entry of infectious disease, was deemed to be within the scope of the study because the intent of these sites is to provide data of value to the nation (see also Chapter 3). In addition, a few examples of sub-sewershed and institutional-scale surveillance are included in the report to accurately portray the range of wastewater surveillance efforts that took place during the COVID-19 pandemic, and to highlight lessons learned that may be applicable to community-scale efforts. The committee was not asked to assess non-infectious agents or surveillance in global settings. The Phase 2 study (see Box 1-4) will offer a detailed technical evaluation and needs assessment for an ongoing national wastewater surveillance program.
To address its Phase 1 statement of task, the committee held two information-gathering meetings. Speakers were selected to complement the broad and interdisciplinary experiences of the committee members, in particular representing perspectives from utility, public health, and ethics stakeholder groups engaged in wastewater surveillance. These discussions served as the initial basis for the committee’s deliberations, which were further informed by a review of relevant literature and the committee’s collective expertise.
REPORT STRUCTURE
This report describes the usefulness of a robust community-level wastewater surveillance system for the United States and highlights approaches for integrating wastewater surveillance data into a public health response for a variety of pathogens. Chapter 2 provides a retrospective assessment of how wastewater surveillance was used in understanding and informing the public health response during the COVID-19 pandemic, including early challenges that were encountered. Chapter 3 describes a vision for a national wastewater disease surveillance system, including key characteristics of a robust system. Chapter 4 discusses strategies for implementing the committee’s vision for a national wastewater-based infectious disease surveillance system beyond COVID-19, discussing future challenges and strategies to collaborate across federal, state, and local jurisdictions.
















