
The second workshop, held April 22, 2022, featured five presentations about advances and key issues in dietary assessment of older adults, followed by a panel discussion with the speakers. These topics were explored through case studies and examples from a variety of longitudinal cohorts that have assessed dietary intakes among older adults. Diane C. Mitchell, Penn State University, and Carol Boushey, University of Hawai‘i Cancer Center and chair of the workshop planning committee, moderated the second workshop.
ASSESSING NUTRITION RISK AMONG COMMUNITY-DWELLING RURAL OLDER ADULTS: THE GEISINGER RURAL AGING STUDY
Mitchell introduced the second workshop’s topic and discussed the application and development of methods used in the Geisinger Rural Aging Study (GRAS)1 and the effectiveness of a brief assessment tool for use in this cohort. She reiterated the importance of developing more feasible, valid, and reliable dietary assessment methods for older adults given the rapidly
___________________
1https://portal.nifa.usda.gov/web/crisprojectpages/0427231-rural-aging-study-geisinger.html (accessed September 14, 2022).
aging global population with a high prevalence of obesity, malnutrition, and poor eating habits.
Mitchell began with a description of the GRAS cohort, which was recruited from a pool of more than two million people in central Pennsylvania, a mostly rural area where the leading industry is agriculture. This population is largely White, native to Pennsylvania, and sparse (population density of 14–475 people per square mile), with greater than 20 percent of residents in many counties aged 60 years and older. The Geisinger Healthcare System service area has one of the largest U.S. concentrations of rural older persons, and it implemented a regional nutrition screening program in 1994 that targeted all members in a Medicare risk contract. It enrolled participants through 1999, which established the GRAS cohort.
Mitchell elaborated on the screening process, which occurred in baseline clinic visits. After enrollment, participants were screened using a one-page questionnaire that was slightly modified from the original Level I and II nutrition screening questionnaires developed in the early 1990s. The screening initiative resulted in a GRAS cohort of 21,645 older adults outside of assisted living (community-dwelling adults) (Bailey et al., 2007, p. 12).
Mitchell explained that the GRAS objectives—to characterize dietary patterns and examine relationships between nutrition risk and health outcomes, including BMI, quality of life, diet quality, various comorbidities (cardiovascular disease, diabetes, hypertension), and mortality—have remained consistent during the study’s nearly 25 years. Researchers plan to add variables collected at baseline, to study food insecurity and neurological outcomes. Now in year 3 of the fifth 5-year cycle of data collection, the study has only 15–25 percent of its participants still living, all of whom are 85 or older.
Mitchell provided a high-level overview of the GRAS methodology. Follow-up screening questionnaires were mailed to participants every 3–4 years, and a more specific tool (Dietary Screening Tool [DST]) was added in the 2009 wave of rescreening. Since the early 2000s, researchers have been able to access deidentified electronic health record data for the full cohort, and in three sequential cycles, a series of comprehensive diet assessments were conducted with a representative subset.
The comprehensive diet assessments were part of a broader evaluation conducted with each subset, which included an eligibility criterion of an acceptable score on the Mini-Mental State Exam (MMSE),2 a test for cognitive ability and geriatric depression using the Geriatric Depression
___________________
2https://www.healthdirect.gov.au/mini-mental-state-examination-mmse#:~:text=about%20the%20MMSE-,What%20is%20a%20Mini%2DMental%20State%20Examination%20(MMSE)%3F,communication%2C%20understanding%20and%20memory) (accessed September 14, 2022).
SOURCE: Presented by Diane Mitchell on April 22, 2022.
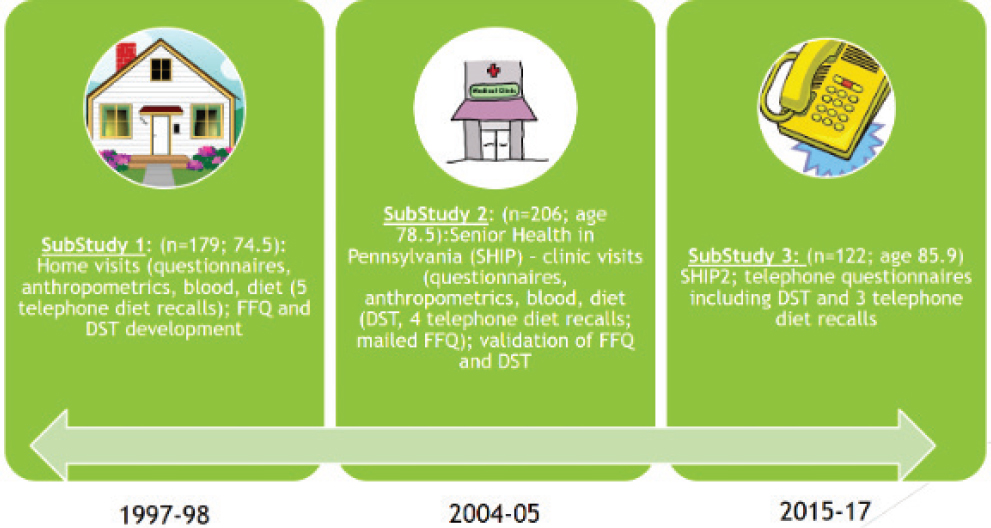
Scale.3 The first substudy (1997–1998) conducted home visits with 179 participants (average age 74.5) to collect a health questionnaire, anthropometrics, and a blood draw. Next, participants completed five telephone dietary recalls over 1 year (approximately every other month), comprised of unannounced calls on 2 weekend days and 3 weekdays. In addition, an existing food frequency questionnaire (FFQ) was modified and validated for the GRAS population, and a new diet quality questionnaire was developed (the DST). The latter evolved as researchers examined dietary recall data and gradually characterized participants’ diets to identify a set of factors and behaviors that could indicate diet quality in the age group represented in GRAS (Bailey et al., 2007). Researchers recognized that the DST would be more feasible, practical, and lower cost for inadequate dietary intake and poor diet quality than traditional methods for assessing diet.
The DST was tested and validated in the second substudy (2004–2005), which included 206 participants (average age 78.5) and was referred to as the “Senior Health in Pennsylvania” study. The DST was administered during clinic visits where research staff also collected height, weight, and other information. A validation process that included comparison with four dietary recalls and nutritional status biomarkers determined that the DST is an effective tool for screening dietary intake; it is the first of its kind to be developed for older adults. Mitchell added that the FFQ was sent and collected via mail—although 75 percent of participants required follow-up telephone calls for incomplete sections—and was validated relative to four unannounced telephone dietary recalls (Mitchell et al., 2012).
The third substudy (2015–2017) included 122 participants (average age 85.9), and all assessments and questionnaires were by telephone. Dietary assessment comprised three dietary recalls and the DST. Mitchell added that the DST has been adapted and used in other populations (Ford et al., 2014; Greene et al., 2018; Jacka et al., 2017; Ventura Marra et al., 2018).
Mitchell presented a comparison of dietary patterns in the first and third substudies, clarifying that each had different participants and slight variation in methods for grouping foods. Cluster analysis was used to generate dietary patterns, which consistently resulted in two distinct patterns (clusters) for both studies: less and more nutrient dense. In both substudies, the less nutrient-dense patterns had higher intakes of desserts and other sweets, for example, and the more nutrient-dense patterns had higher intakes of fruits, vegetables, fish, and eggs.
When nutrient intakes and weight status were examined by dietary pattern in the first substudy, the more nutrient-dense clusters were characterized by higher intakes of protein, fiber, and key vitamins and minerals;
___________________
3https://wwwoundcare.ca/Uploads/ContentDocuments/Geriatric%20Depression%20Scale.pdf (accessed September 14, 2022).
lower intakes of energy and fat; and lower waist circumference (but not body mass index [BMI]). The diets were more homogenous in the third substudy, Mitchell said, but the two patterns were still distinguishable, with the more nutrient-dense cluster characterized by higher intakes of fiber, potassium, and several vitamins, and higher Healthy Eating Index (HEI) and DST scores.
Mitchell summarized key findings from the 23-year duration of research with the GRAS cohort. A high prevalence of poor-quality diets, obesity, and ill health has been observed among the cohort, and GRAS was among the first studies to recognize that obesity in older adults is characterized by poor diet quality, comorbidities, and functional decline. She noted that a poor-quality diet is also associated with low BMI and increased mortality. With respect to the diet assessment methods, telephone dietary recalls remain a gold standard method for quantifying nutrients and foods in older adults despite their limitations (e.g., cost, cognitive issues, and high prevalence of chronic disease that likely influences diet). The GRAS FFQ is a valid assessment of dietary risk as defined by diet quality and poor dietary intake but may not be the best choice for older adults, given the high rate of incomplete assessments returned by participants during the second substudy. Finally, she confirmed that the DST is a valid, brief, and effective screening tool used to measure dietary risk defined by diet quality and nutrient intakes in older adults, but its validity is mostly limited to the GRAS population. Others could follow the GRAS model to develop, test, and validate the DST to create a brief assessment tool for their own populations.
GEORGIA CENTENARIAN STUDY
Mary Ann Johnson, University of Nebraska–Lincoln, shared findings about potentially modifiable risk factors related to nutritional status among participants in the Georgia Centenarian Study. In 2020, it was estimated that 573,000 centenarians live in the world, and the projected figure for 2100 is 19 million (Statista, 2022). Johnson shared her sentiments that it is highly rewarding to study society’s oldest individuals, reflecting on an example of a Black centenarian in Atlanta who had been born at a time when women and Black people could not vote and lived to cast her ballot for Barack Obama, the country’s first Black president.
The study began in 1988, but the data she presented were collected from 2003 to 2005. The study’s objectives are to identify physical, mental, social, nutritional, and genetic factors related to well-being late in life. The cohort is drawn from 44 counties in northeast Georgia: 244 individuals aged 98 and older (the centenarians) and 80 individuals aged 80–89. Participants were identified from skilled nursing facilities, personal care homes, and registered voter lists, and they or their proxies responded to questions and provided informed consent (Poon et al., 2007).
Johnson shared findings on nutrition biomarkers among study participants, beginning with vitamin D. Serum vitamin D was lower in the centenarians than the 80-year-old participants and lower in Black than in White participants, and levels varied by season (highest in fall, lowest in spring) independent of dairy intake and place of residence (facility versus community) (Johnson et al., 2008). Vitamin D insufficiency was 22.5 percent of 80-year-olds and 36.7 percent of the centenarians; 30 percent of White and 61 percent of Black centenarians had insufficiency (Johnson et al., 2008). Prevalence was lower among centenarians who consumed a vitamin-D-containing supplement (20 percent) than those who did not (50 percent) (Johnson et al., 2008). These findings are generally consistent with those of 80+ year-old participants in NHANES III, which was conducted at the same time (Looker et al., 2002). Another study at the time reported undetectable vitamin D levels in 99 of 104 centenarians in northern Italy, but this region is mountainous, cloudy, and rainy, and food fortification and supplement intake were uncommon (Passeri et al., 2003). Johnson summarized that these study results suggest that supplement use is a modifiable risk factor for enhanced vitamin D status among older adults.
Moving on to vitamin B12, Johnson pointed out that the proportion of women, Black or African American individuals, B-vitamin supplement users, and consumers of >2 servings/day of animal foods were similar in both of the study’s age groups. Mean serum vitamin B12 was similar in the two age groups (Johnson et al., 2010) and in a Korean cohort where more than 30 percent of vitamin B12 intake was derived from fermented plant foods (Kwak et al., 2010). Vitamin B12 deficiency was significantly higher among the centenarians (35 versus 23 percent) (Johnson et al., 2010), of whom White individuals had a nearly twofold higher B12 deficiency than Black or African American individuals, and supplement use was lower in those who were deficient. Severe atrophic gastritis, which interferes with acid production in the stomach—an intrinsic factor needed for B12 absorption—was significantly more common in the deficient group (Johnson et al., 2010). Johnson reiterated that as with vitamin D, supplement use appears to be a modifiable risk factor for vitamin B12 status, and a culture’s dietary patterns also play a role in its aging population’s nutrition risk factors.
Johnson described the Georgia Centenarian Study’s focus on brain health and the role of nutrients such as docosahexaenoic acid (DHA) and lutein. Thirty-one percent of the centenarian age group agreed to donate their brains to science upon their death (Shaw et al., 2012), and upon examination of the half of the brains without dementia, DHA was the fatty acid category most strongly associated with better scores on 11 of the 14 cognitive tests administered (Mohn et al., 2013). Among centenarians, xanthophylls (i.e., lutein, zeaxanthin, and cryptoxanthin) appear to be preferentially accumulated in the brain compared to the serum (Johnson et al.,
2013), a distribution that may indicate a special function of xanthophylls in the brain. Another study found that lutein and beta-carotene were higher in centenarians with normal cognitive function and lowest in those with mild cognitive impairment (Johnson et al., 2013).
Johnson raised a few limitations of the Georgia Centenarian Study, such as its participant demographic characteristics (e.g., 20 percent Black and 80 percent White), which may limit applicability of the findings to more diverse populations. Supplement intake was also self-reported, often from a proxy reporter.
To summarize key findings, Johnson referenced a high prevalence of poor vitamin D and B12 status, which she called measurable and correctable; a positive association between supplement intake and higher vitamin D and vitamin B12 status; low prevalence of folate deficiency, likely related to U.S. food fortification and relatively widespread supplement use; an apparent positive association of DHA, lutein, and zeaxanthin with cognition and brain health, so the plant sources of these nutrients may be important; and large ranges in the concentrations of these biomarkers in blood and brain tissue, which suggests persistent responsiveness to the nutrition environment even late into life.
IMPLEMENTING DIVERSE DIETARY ASSESSMENT METHODS AMONG COMMUNITY-DWELLING ADULTS OR CLINICAL NURSING HOME RESIDENTS
Jeanne de Vries, Wageningen University, described her experience with applying different dietary assessment tools in the Netherlands’ older population. Older adult populations are heterogenous, she began, with a wide age range (60+ to centenarians), physical function (from physically active to fully dependent on care), and degree of mental and physical impairment. She clarified that her studies addressed both healthy and “more fragile” older adults.
With respect to surveillance of dietary intake in older people, de Vries referenced an Efcosum project4 that raised the need for confirmation of the hypothesis that food intake measurements using retrospective methods would be unsuitable for older people. The project also raised a lack of empirical data indicating that older people face specific problems to completing such dietary assessments. The project added that 24-hour dietary recalls and FFQs may give more accurate information, and accuracy probably depends on the respondent’s health status, such that memory deficits
___________________
4https://ec.europa.eu/health/ph_projects/1999/monitoring/fp_monitoring_1999_frep_10_en.pdf (accessed September 14, 2022).
or other physical or cognitive impairments may introduce inaccuracies or challenges completing the assessment.
She summarized highlights from a journal article that recounted experiences from studies to assess dietary intake of older adults in the Netherlands (de Vries et al., 2009), beginning with the Survey in Europe on Nutrition and the Elderly: A Concerted Action longitudinal cohort study. Participants were 75 on average, and researchers were interested in the mean and distribution of usual intake and ranking of intake at the individual level. The method was a modified dietary history (which included a 3-day estimated food record and a dietary history interview) plus a questionnaire that gathered information about food habits and nutrition attitudes. When reported energy and nutrient intakes from the interview were compared with those from the estimated food record, the interview underestimated protein and overestimated energy, vitamin B1, and calcium, although the correlation coefficients for these were approximately 0.7 to 0.8 (de Vries et al., 2009).
She recounted a study to validate an FFQ in older Dutch men (average age of 76) in a controlled feeding trial, which provided the opportunity to compare their reported intake per the FFQ against their energy needs during the trial (de Vries et al., 2009). The FFQ was developed based on their intake according to the Dutch national food consumption survey, and the results indicated a difference in reported energy intake and energy needs of about 13 percent (the FFQ underestimated energy intake). This degree of underestimation of energy intake was similar in a study of women that compared a diet history with indirect calorimetry (Visser et al., 1995).
In nursing homes, three trained observers per ward were needed to record the daily intakes of 25 residents in fragile physical condition with cognitive decline (but not severe dementia). When compared with indirect calorimetry, the food record underestimated energy expenditure by 5 percent, and both measures reflected very low daily energy intakes.
She discussed a series of more recent (during the past decade or so) efforts to develop and improve dietary assessment tools for older adults in the Netherlands. She maintained that increasing the readability of tools is critical, such as by using drawings or icons for clarification, avoiding or at least explaining difficult words, using a different color or bolding for important words, increasing font size, shortening sentences to no more than 10 words, and adding a button for reading digitally based instruments aloud.
Next, de Vries shared an effort to develop an online screener of protein intake for hospital patients. The protein requirement is estimated based on height, weight, age, and vegetarian status, and then protein intake is assessed by questionnaire. The tool also includes information about achieving adequate intake. A similar screener for calcium was less successful, likely due to the limited number of questions asked about consumption of calcium-containing foods (Rasch et al., 2017). She mentioned another tool
that used duplicate portions to assess the gluten content of diets in patients with celiac disease, which indicated that some foods contained gluten despite gluten-free claims (van der Fels-Klerx et al., 2021).
She highlighted a tool called Eetscore5 for medical specialists to use to assess hospital patients. A short questionnaire is scored using the Dutch Healthy Diet Index,6 and the results guide dietary advice provided to patients. Eetscore has also been adapted for use in home care via a telemonitoring intervention to improve nutritional status (Balvers et al., 2020), which can increase patients’ nutritional status. A specific application of the Eetscore to monitor micronutrient status is called NutriProfiel,7 which combines a patient’s scores with their vitamin status measured by blood biomarkers. These two metrics provide a more complete picture about vitamin sufficiency—whether insufficient status may be more likely related to dietary intake or pathophysiology—and help tailor guidance for dietary improvement and supplement intake. A study of NutriProfiel indicated that micronutrients most commonly requested for assessment are vitamin D and vitamin B12, followed by folic acid and vitamin B6, and that patients were most likely to be deficient in vitamin D.
In summary, de Vries stated that because all self-reported methodologies resulted in a relatively small underestimation of dietary intake—although most populations were comprised of healthy, educated participants—24-hour recalls or FFQs in are equally effective methods for dietary assessment in healthy older and younger people. Diet history and observation methods are burdensome, she said, and all assessment tools would benefit from further validation, particularly in lower socioeconomic populations. She also called for more information on cognitive capabilities (cognition, vision, hearing, or writing ability) to be included in evaluations of dietary assessment tools for older adults, as well as further investigation of the relationship between functionality and accurate reporting in diverse older adult populations.
ASSESSING DIETARY INTAKES AMONG OLDER ADULTS FROM DIVERSE POPULATIONS
Katherine L. Tucker, University of Massachusetts Lowell, discussed assessing dietary intakes of older adults from diverse populations. She began by reviewing challenges of dietary assessment in general, which
___________________
5https://www.wur.nl/en/show/eetscore.htm (accessed September 14, 2022).
6https://www.researchgate.net/publication/229434908_The_Dutch_Healthy_Diet_index_DHD-index_An_instrument_to_measure_adherence_to_the_Dutch_Guidelines_for_a_Healthy_Diet (accessed September 14, 2022).
7https://www.wur.nl/en/show/nutriprofiel.htm (accessed September 14, 2022).
include difficulty obtaining valid and reliable measures of nutrient intake and usual intakes over time (particularly to examine diet in relation to health outcomes), a wide diversity of populations for which assessment tools must be tailored, and the high cost and participant and/or researcher burden of doing dietary assessment well.
Tucker briefly described strengths and limitations of three traditional methods—dietary records, 24-hour dietary recalls, and FFQs. Dietary records used to be the method of choice, but they require participant literacy and cooperation, so they are often incomplete or not returned, and people tend to change their eating behavior when recording their intake.
Twenty-four-hour dietary recalls are useful and valid and have been automated and enhanced to capture intake more comprehensively, but a key limitation is that they capture only a single day. This lack of insight into day-to-day variability in intake can lead to misclassification, which she illustrated with a graph of total fat intakes of women at the 10th, 50th, and 90th percentiles over a 1-month period. Although the three percentiles are clearly separated, on a given day, the person in the 10th percentile could have been rated as the highest and the person in the 90th percentile rated quite low.
Tucker explained that the effect of that random error is that it pulls out the distribution, increasing the size of the tail by overestimating the prevalence of extreme intakes (high or low) because anyone can have an (atypical) extreme intake on a given day (Beaton, 1994). Random error also flattens the slope of the regression line, which attenuates any existing association between intake and health outcome (Beaton, 1994). True intake and more accurate distributions are more likely to be attained (particularly for foods/nutrients for which daily intake is more variable) if dietary intake is collected for a greater number of days and averaged (Basiotis et al., 1987), but the cost and burden of this approach makes it infeasible for most studies.
Tucker explained that in response to this limitation of 24-hour dietary recalls, the National Cancer Institute developed a statistical approach to adjust for day-to-day variability if at least two recalls are available for a large subset of a study population. It is useful for adjusting a population distribution and can include covariates (e.g., age, sex, ethnicity, income) but still does not accurately classify individuals (adjustments for episodically consumed foods can be applied at the population level but not on an individual level because comprehensive individual intake over the long term is not available).
The challenges of 24-hour dietary recalls have led dietary studies to rely primarily on FFQs, which provide long-term measures of usual intake with a single administration. Because FFQs cannot provide exhaustive lists of
foods, they use food groupings, which can limit specificity and detail during analysis. They also make assumptions about portion sizes and recipe composition, which limit assessment of true variation and can severely underestimate intake for people with unusual intake patterns. It has been suggested that older adults with cognitive impairment cannot adequately recall intake to complete an FFQ, but with mild-to-moderate cognitive impairment and dementia, episodic memory or recall of specific details becomes reduced, whereas pattern memory (what is needed to complete an FFQ) is generally maintained (Arsenault et al., 2009; Craik et al., 1987).
Tucker highlighted the major challenges of using FFQs for diverse populations, which center on the failure of most FFQs to equally represent diets of different groups. Limited food lists may miss important ethnic foods, and cross-population differences in typical portion sizes may exist for certain foods depending on their prominence in the culture’s diet. Another challenge is that differences in recipes are almost always underappreciated, even when modifications to the FFQ are attempted. These issues can produce severe bias in multicultural studies, particularly when comparing populations within a study.
Tucker elaborated on the limitations of using FFQs in diverse study populations. FFQs are designed to capture the diet of the majority group and make compromises by grouping foods and making assumptions about their relative consumption. For example, an FFQ cannot include an exhaustive list of fruits and so may have a category for “other fruits,” which are assigned a weighted average and corresponding nutrient values based on population dietary intake data. However, that category may not include some or all of the fruits that certain cultures consume, which removes important variation within the study cohort. FFQs also assume standard recipes for certain foods, such as soup. The most common soup consumed in the United States is canned, so the nutrient values are based on weighted averages of popular canned varieties. But Puerto Rican populations, for example, make their own soups and consume them in larger quantities, which also contributes to bias. For example, when using well-known FFQs in certain population groups, such as Black or African American and Hispanic or Latinx individuals, bias leads to extremely low validity coefficients because important food sources of nutrients were omitted (Freeman Sullivan & Co., 1994).
Tucker discussed strategies for adapting an FFQ to a new population, based on learnings from her team’s effort to modify an FFQ for a Puerto Rican adult population. The process is complicated and resource intensive, she cautioned, and starts by examining a set of representative 24-hour recalls to develop the food list (keeping in mind a country’s seasonal variations for intake of certain foods). The next step is to determine the contribution weight behind the foods on the list and adjust recipes and
portion sizes as needed. Tucker recounted that her team compared dietary intake information from the Hispanic Health and Nutrition Examination Survey (HHANES) against NHANES III8 to compile its food list, rank food contributions to nutrients, modify portion sizes, and adjust recipes to reflect their contributions to nutrient intake. For example, existing FFQs assume that rice is cooked with water and a little salt, but the Puerto Rican adults eat rice in relatively large quantities and prepare it with oil. They also use tomato sauce and sofrito in many stew and bean recipes, meaning that vegetable intake would be underestimated if another recipe were used for those dishes. When the team compared both the original and modified FFQs to 24-hour recalls among Hispanic or Latino elders in Massachusetts, they observed that the original FFQ underestimated intake of all nutrients (Tucker et al., 1998).
Tucker pointed out that dietary intake differs by not only ethnicity but also region. She shared brief details about an effort to create a new FFQ for dietary assessment studies conducted in southern states in the Delta region. Many foods that were not included in well-known FFQs needed to be added to reflect the regional food sources, such as biscuits, fried catfish, cracklings, different kinds of greens, gumbo, ham hocks, sweet potato pie, and sweet tea (Tucker et al., 2005). After creating the Delta FFQ, Tucker’s team was asked to produce a shortened version for the Jackson site of the Atherosclerosis Risk in Communities Study, because the study’s FFQ seemed less valid in the Jackson site due to its lack of southern foods (Carithers et al., 2005).
Tucker concluded by reiterating that chronic diseases are accelerating as the world ages and urged investment in optimal dietary assessment to better understand diet’s contribution to health and disease in diverse populations. She maintained that despite the desire for quick, inexpensive methods, such shortcuts do not exist when the goal is to ensure validity in intakes of different populations under study.
USING TECHNOLOGICAL APPROACHES TO RECORD DIETARY INTAKES AMONG OLDER ADULTS
Marie Kainoa Fialkowski Revilla, University of Hawai‘i at Mānoa, discussed the use of technological approaches to record dietary intakes among older adults. She began by stating that this population may have physical and cognitive barriers to using technology, skeptical attitudes about its benefits, or difficulties learning how to use it (Smith, 2014). Internet usage has been rising in all age groups since 2000 and reached nearly 75 percent by 2018 among older adults (65 and older) (Faverio, 2022). For smartphones
___________________
8https://wwwn.cdc.gov/nchs/nhanes/hhanes/default.aspx (accessed September 14, 2022).
specifically, 71 percent of 65–74-year-olds and 43 percent of those 75 years and older owned one in 2021 (Gordon and Hornbrook, 2018). Technology became a key channel for connection during the COVID-19 pandemic, including among older adults (Kakulla, 2021).
Fialkowski Revilla described and image-based methods to incorporate technology into dietary assessment. A popular automated method is the Automated Self-Administered 24-hour Dietary Assessment Tool (ASA24™), a free, web-based and mobile-ready tool that can perform multiple, automatically coded, self-administered 24-hour diet recalls and/or single or multiday food records (NIH National Cancer Institute Division of Cancer Control & Population Sciences, 2022). It was used in older adults for the Interactive Diet and Activity Tracking in AARP (IDATA)9 study, which included more than 1,100 adult AARP members aged 50–74. Participants completed six nonconsecutive ASA24s in 1 year; the method was deemed to perform as well as multiple food records and have results comparable to objective recovery biomarkers (Park et al., 2018). With respect to feasibility, 92 percent of men and 87 percent of women completed at least three ASA24s and about 75 percent overall completed at least five, a level of compliance that exceeded the levels for multiple food records or FFQs. Two-thirds or more of participants were able to complete the ASA24 on the first attempt, and more than 90 percent completed it on the second attempt; the median time to completion declined with subsequent recalls (Subar et al., 2020).
Fialkowski Revilla discussed another study that used the ASA24, the Canadian Longitudinal Study on Aging.10 It examined the feasibility of using the ASA24-Canada-2014 version with older adults. Almost all (220) of the 232 participants completed four nonconsecutive ASA24s, although 36 percent had to do one or more by phone interview due to technological difficulties, computer literacy issues, or length (they were unable to finish independently). Results of a usability study indicated that half of participants agreed that the survey was unnecessarily complex and half said it was easy to use (Gilsing et al., 2018).
Fialkowski Revilla shared a third use of ASA24, the MoveStrong study.11 This pilot study of 39 adults with an average age of 78 administered the ASA24-Canada by phone interview on 3 separate days. Whereas IDATA study participants took about 50 minutes to complete the ASA24 on their own, the MoveStrong study recorded average completion times of 26 minutes. The caveat to this method was that it took about six telephone calls to reach participants to complete the assessment at baseline and seven
___________________
9https://prevention.cancer.gov/research-groups/biometry/interactive-diet-and-activity (accessed September 14, 2022).
10https://www.clsa-elcv.ca (accessed September 14, 2022).
11https://the-ria.ca/project/movestrong (accessed September 14, 2022).
calls for follow-up assessments, and participants reported frustration with its specificity and repetitiousness (Wei et al., 2022).
Fialkowski Revilla discussed dietary assessment methods that rely on images. One is passive, which requires the participant to wear a device, such as a camera attached to a glasses frame, that takes images throughout the day without requiring user engagement. A contrasting approach is active, requiring the user to capture images of foods consumed throughout the day. The passive approach generates significantly more images (e.g., one image per 5 seconds or about 400,000 images/day) than the active approach (about 6–12 images/day), but most of them are not related to food and must go through a process to extract the relevant ones. An advantage of the active approach is the ability to gather information about the meal’s energy, nutrients, food groups, context and location, time stamp (a marker of eating duration), and food waste.
As an example of a novel finding about temporal eating patterns and context that was enabled by using images, Fialkowski Revilla shared a study of east Asian adults (35–55 years) who completed a mobile food record with images followed by a paper food record. The number of recorded eating events was similar, but large differences existed in the times at which eating occasions were reported. The manual record showed consistent eating schedules, whereas the mobile record indicated day-to-day differences (Yonemori et al., 2022).
Fialkowski Revilla emphasized that a dietary assessment system using a mobile food record has been used to capture intake of participants across the life span, from only a few months old up to 66 years. A valuable opportunity exists to use this method along with passive methods for older adults. Research suggests that most users have compatible devices for downloading a mobile food record and are willing to do so, with the use of one’s own device expected to positively influence compliance (Boushey, 2017, 312).
Fialkowski Revilla shared an incidental finding in one of her studies; grandparents were serving as surrogate reporters of infant dietary intake, which was collected via mobile food record. This finding occurs in the context of increasing U.S. prevalence of multigenerational households and provides additional evidence to suggest that older adults are willing and able to navigate the technology (Fialkowski et al., 2022). On the other hand, older adults sometimes need surrogate reporters as proxies, especially in the presence of cognitive decline. A small study of 26 older adults (65–94 years) found that when caregivers completed a 24-hour recall, the proportion of unreported foods was reduced by about 50 percent compared to when the patient did so (Pardío et al., 2016). The implication is that surrogate reporting could be a tactic for dietary assessment of older adults.
Fialkowski Revilla reiterated that smartphone ownership and Internet usage is on the rise in older adults, which presents an opportunity but
must be informed by future research to assess how technology can advance dietary assessment in this population.
PANEL DISCUSSION WITH SPEAKERS
Speakers answered questions from workshop planning committee members about identifying an FFQ for a specific population and trade-offs between assessment burden and data quality.
Choosing an FFQ for Retirement Home Residents in Canada
A planning committee member noted that older adults in retirement homes where all food is provided may not have information about portion sizes or a recipe’s ingredients or cooking method and may also have some degree of cognitive impairment. She asked what FFQ would be appropriate for such a population, specifically in Canada. Tucker responded that she was not aware of an FFQ that would be suitable, and she suggested developing one tailored to the target population if there are plans to examine its dietary intakes in repeated studies over time. This process begins by collecting 24-hour recalls, and comparing results to existing FFQs to evaluate whether they sufficiently capture all types of foods reported in the recalls, especially foods that might be specific to the culture or region. Boushey agreed and added that her group developed a tailored FFQ for a multiethnic cohort of native Hawaiian, Japanese American, Latino, non-Hispanic White, and African American participants. Much work was required to ensure representation of appropriate foods for these five populations, but the FFQ has worked well and complemented other assessment methods.
Trade-Offs Between Assessment Burden and Data Quality
A planning committee member recalled de Vries’ comment that it took three trained observers per ward to record the daily intakes of 25 nursing home residents. She asked if it is preferable to get higher-quality data on small numbers of people than lower-quality data on large populations; de Vries acknowledged the high burden of this observational method but suggested that it is important for capturing accurate information. She noted that observers could ask kitchen staff for information about recipes and portion sizes. Another planning committee member shared her experience collecting weighted food records in a long-term care facility, which she said was “extremely labor-intensive but incredibly worthwhile” in terms of the rich data obtained. In her opinion, this level of effort is necessary for capturing intake of vulnerable populations. Tucker added that observational and weighted methods are helpful for estimating the proportion of meals
that are uneaten, which she thought was important given the prevalence of poor appetites among long-term care residents. Fialkowski Revilla suggested that passive image-based methods may have utility for capturing this information in those settings.
REFERENCES
Arsenault, L. N., N. Matthan, T. M. Scott, G. Dallal, A. H. Lichtenstein, M. F. Folstein, I. Rosenberg, and K. L. Tucker. 2009. Validity of estimated dietary eicosapentaenoic acid and docosahexaenoic acid intakes determined by interviewer-administered food frequency questionnaire among older adults with mild-to-moderate cognitive impairment or dementia. American Journal of Epidemiology 170(1):95–103.
Bailey, R. L., D. C. Mitchell, C. K. Miller, C. D. Still, G. L. Jensen, K. L. Tucker, and H. Smiciklas-Wright. 2007. A dietary screening questionnaire identifies dietary patterns in older adults. Journal of Nutrition 137(2):421–426.
Balvers, M., M. De Rijk, A. Slotegraaf, J. K. Gunnewiek, and J. De Vries. 2020. Development and implementation of online tools for personalized dietary advice at home or in a clinical setting: Eetscore and NutriProfiel. Proceedings of the Nutrition Society 79(OCE2):E526.
Basiotis, P. P., S. O. Welsh, F. J. Cronin, J. L. Kelsay, and W. Mertz. 1987. Number of days of food intake records required to estimate individual and group nutrient intakes with defined confidence. Journal of Nutrition 117(9):1638–1641.
Beaton, G. H. 1994. Approaches to analysis of dietary data: Relationship between planned analyses and choice of methodology. American Journal of Clinical Nutrition 59(1 Suppl):253S–261S.
Boushey, C. J., M. Spoden, E. J. Delp, F. Zhu, M. Bosch, Z. Ahmad, Y. B. Shvetsov, J. P. DeLany, and D. A. Kerr. 2017. Reported energy intake accuracy compared to doubly labeled water and usability of the mobile food record among community dwelling adults. Nutrients 9(3):312.
Carithers, T., P. M. Dubbert, E. Crook, B. Davy, S. B. Wyatt, M. L. Bogle, H. A. Taylor, Jr., and K. L. Tucker. 2005. Dietary assessment in African Americans: Methods used in the Jackson Heart Study. Ethnicity and Disease 15(4 Suppl 6):S6-49–55.
Craik, F. I. M., M. Byrd, and J. M. Swanson. 1987. Patterns of memory loss in three elderly samples. Psychology and Aging 2(1):79–86.
de Vries, J. H., L. C. de Groot, and W. A. van Staveren. 2009. Dietary assessment in elderly people: Experiences gained from studies in the Netherlands. European Journal of Clinical Nutrition 63(Suppl 1):S69–S74.
Faverio, M. 2022. Share of those 65 and older who are tech users has grown in the past decade. Washington, DC: Pew Research Center.
Fialkowski, M. K., J. Kai, C. Young, G. Langfelder, J. Ng-Osorio, Z. Shao, F. Zhu, D. A. Kerr, and C. J. Boushey. 2022. An active image-based mobile food record is feasible for capturing eating occasions among infants ages 3–12 months old in Hawai’i. Nutrients 14(5).
Ford, D. W., T. J. Hartman, C. Still, C. Wood, D. Mitchell, P. Y. Hsiao, R. Bailey, H. Smiciklas-Wright, D. L. Coffman, and G. L. Jensen. 2014. Diet-related practices and BMI are associated with diet quality in older adults. Public Health Nutrition 17(7):1565–1569.
Freeman Sullivan and Co. 1994. WIC Dietary Assessment Validation Study. Alexandria, VA: U.S. Department of Agriculture Food and Nutrition Service.
Gilsing, A., A. J. Mayhew, H. Payette, B. Shatenstein, S. I. Kirkpatrick, K. Amog, C. Wolfson, S. Kirkland, L. E. Griffith, and P. Raina. 2018. Validity and reliability of a short diet questionnaire to estimate dietary intake in older adults in a subsample of the Canadian Longitudinal Study on Aging. Nutrients 10(10).
Gordon, N. P., and M. C. Hornbrook. 2018. Older adults’ readiness to engage with ehealth patient education and self-care resources: A cross-sectional survey. BMC Health Services Research 18(1):220.
Greene, G. W., I. Lofgren, C. Paulin, M. L. Greaney, and P. G. Clark. 2018. Differences in psychosocial and behavioral variables by dietary screening tool risk category in older adults. Journal of the Academy of Nutrition and Dietetics 118(1):110–117.
Jacka, F. N., A. O’Neil, R. Opie, C. Itsiopoulos, S. Cotton, M. Mohebbi, D. Castle, S. Dash, C. Mihalopoulos, M. L. Chatterton, L. Brazionis, O. M. Dean, A. M. Hodge, and M. Berk. 2017. A randomised controlled trial of dietary improvement for adults with major depression (the “SMILES” trial). BMC Medicine 15(1):23.
Johnson, E. J., R. Vishwanathan, M. A. Johnson, D. B. Hausman, A. Davey, T. M. Scott, R. C. Green, L. S. Miller, M. Gearing, J. Woodard, P. T. Nelson, H. Y. Chung, W. Schalch, J. Wittwer, and L. W. Poon. 2013. Relationship between serum and brain carotenoids, alpha-tocopherol, and retinol concentrations and cognitive performance in the oldest old from the Georgia Centenarian Study. Journal of Aging Research 951786.
Johnson, M. A., A. Davey, S. Park, D. B. Hausman, L. W. Poon, and The Georgia Centenarian Study. 2008. Age, race and season predict vitamin D status in African American and White octogenarians and centenarians. Journal of Nutrition, Health & Aging 12(10):690–695.
Johnson, M. A., D. B. Hausman, A. Davey, L. W. Poon, R. H. Allen, S. P. Stabler, and The Georgia Centenarian Study. 2010. Vitamin B12 deficiency in African American and White octogenarians and centenarians in Georgia. Journal of Nutrition, Health & Aging 14(5):339–345.
Kakulla, B. April 2021. 2021 tech trends and the 50-plus: Top 10 biggest trends. Washington, DC: AARP Research.
Kwak, C. S., M. S. Lee, S. I. Oh, and S. C. Park. 2010. Discovery of novel sources of vitamin B(12) in traditional Korean foods from nutritional surveys of centenarians. Current Gerontology and Geriatrics Research 374897.
Looker, A. C., B. Dawson-Hughes, M. S. Calvo, E. W. Gunter, and N. R. Sahyoun. 2002. Serum 25-hydroxyvitamin D status of adolescents and adults in two seasonal subpopulations from NHANES III. Bone 30(5):771–777.
Mitchell, D. C., K. L. Tucker, J. Maras, F. R. Lawrence, H. Smiciklas-Wright, G. L. Jensen, C. D. Still, and T. J. Hartman. 2012. Relative validity of the Geisinger Rural Aging Study food frequency questionnaire. Journal of Nutrition, Health & Aging 16(7):667–672.
Mohn, E., R. Vishwanathan, W. Schalch, A. Lichtenstein, N. Matthan, and L. Poon. 2013. The relationship of lutein and DHA in age-related cognitive function. Paper presented at the Experimental Biology Conference, Boston, MA.
NIH National Cancer Institute Division of Cancer Control & Population Sciences. 2022. Automated Self-Administered 24-hour (ASA24) Dietary Assessment Tool. https://epi.grants.cancer.gov/asa24/ (accessed September 14, 2022).
Pardío, J., P. Arroyo, A. Loría, S. Torres-Castro, M. Agudelo-Botero, B. L. Jiménez Herrera, and A. T. Serrano Miranda. 2016. Accuracy of 24-hr food-registry method in elderly subjects: Role of a surrogate respondent. Journal of Aging Research Clinical Practice 5(4):217–219.
Park, Y., K. W. Dodd, V. Kipnis, F. E. Thompson, N. Potischman, D. A. Schoeller, D. J. Baer, D. Midthune, R. P. Troiano, H. Bowles, and A. F. Subar. 2018. Comparison of self-reported dietary intakes from the automated self-administered 24-h recall, 4-D food records, and food-frequency questionnaires against recovery biomarkers. American Journal of Clinical Nutrition 107(1):80–93.
Passeri, G., G. Pini, L. Troiano, R. Vescovini, P. Sansoni, M. Passeri, P. Gueresi, R. Delsignore, M. Pedrazzoni, and C. Franceschi. 2003. Low vitamin D status, high bone turnover, and bone fractures in centenarians. International Journal of Clinical Endocrinology and Metabolism 88(11):5109–5115.
Poon, L. W., M. Jazwinski, R. C. Green, J. L. Woodard, P. Martin, W. L. Rodgers, M. A. Johnson, D. Hausman, J. Arnold, A. Davey, M. A. Batzer, W. R. Markesbery, M. Gearing, I. C. Siegler, S. Reynolds, and J. Dai. 2007. Methodological considerations in studying centenarians: Lessons learned from the Georgia Centenarian Studies. Annual Review of Gerontology and Geriatrics 27(1):231–264.
Rasch, L. A., M. A. de van der Schueren, L. H. van Tuyl, I. E. Bultink, J. H. de Vries, and W. F. Lems. 2017. Content validity of a short calcium intake list to estimate daily dietary calcium intake of patients with osteoporosis. Calcified Tissue International 100(3):271–277.
Shaw, K., M. Gearing, A. Davey, M. Burgess, L. W. Poon, P. Martin, and R. C. Green. 2012. Successful recruitment of centenarians for post-mortem brain donation: Results from the Georgia Centenarian Study. Journal of Biosciences and Medicines 2(1).
Smith, A. 2014. Older adults and technology use. Washington, DC: Pew Research Center.
Statista. 2022. Number of people aged 100 and older (centenarians) worldwide from 2010 to 2100 (in 1,000s). Hamberg, Germany: Statista.
Subar, A. F., N. Potischman, K. W. Dodd, F. E. Thompson, D. J. Baer, D. A. Schoeller, D. Midthune, V. Kipnis, S. I. Kirkpatrick, B. Mittl, T. P. Zimmerman, D. Douglass, H. R. Bowles, and Y. Park. 2020. Performance and feasibility of recalls completed using the Automated Self-Administered 24-hour Dietary Assessment Tool in relation to other self-report tools and biomarkers in the Interactive Diet and Activity Tracking in AARP (IDATA) study. Journal of the Academy of Nutrition and Dietetics 120(11):1805–1820.
Tucker, K. L., L. A. Bianchi, J. Maras, and O. I. Bermudez. 1998. Adaptation of a food frequency questionnaire to assess diets of Puerto Rican and non-Hispanic adults. American Journal of Epidemiology 148(5):507–518.
Tucker, K. L., J. Maras, C. Champagne, C. Connell, S. Goolsby, J. Weber, S. Zaghloul, T. Carithers, and M. L. Bogle. 2005. A regional food-frequency questionnaire for the U.S. Mississippi Delta. Public Health Nutrition 8(1):87–96.
van der Fels-Klerx, H. J., N. G. E. Smits, M. Bremer, J. M. Schultink, M. M. Nijkamp, J. J. M. Castenmiller, and J. H. M. de Vries. 2021. Detection of gluten in duplicate portions to determine gluten intake of coeliac disease patients on a gluten-free diet. British Journal of Nutrition 125(9):1051–1057.
Ventura Marra, M., S. V. Thuppal, E. J. Johnson, and R. L. Bailey. 2018. Validation of a dietary screening tool in a middle-aged Appalachian population. Nutrients 10(3).
Visser, M., L. C. De Groot, P. Deurenberg, and W. A. Van Staveren. 1995. Validation of dietary history method in a group of elderly women using measurements of total energy expenditure. British Journal of Nutrition 74(6):775–785.
Wei, C., J. B. Wagler, I. B. Rodrigues, L. Giangregorio, H. Keller, L. Thabane, and M. Mourtzakis. 2022. Telephone administration of the automated self-administered 24-hour dietary assessment in older adults: Lessons learned. Canadian Journal of Dietetic Practice and Research 83(1):30–34.
Willett, W. 2013. Nutritional epidemiology. U.S.: Oxford University Press.
Yonemori, K. M., L. Zuccarelli, L. Le Marchand, F. M. Zhu, D. Kerr, and C. J. Boushey. 2022. Temporal patterns of eating by mode of data collection from the baseline dietary intakes of participants in the Healthy Diet and Lifestyle Study. Journal of Food Composition and Analysis 107:104296.
This page intentionally left blank.




















