
The third workshop, held April 29, 2022, featured four presentations about screening for malnutrition in older adults, followed by a panel discussion with the speakers. Presentation topics included experiences with screening for malnutrition in the United States and internationally and how food insecurity can negatively affect nutritional status. Gordon Jensen, University of Vermont, and Clare Corish, University College Dublin, moderated the workshop.
A U.S. EXPERIENCE WITH SCREENING FOR MALNUTRITION: THE NUTRITION SCREENING INITIATIVE TO 2022
Jensen provided a brief historical overview of screening for deteriorating nutritional status and/or malnutrition in older U.S. adults from the 1990s development and implementation of the Nutrition Screening Initiative1 to the present day. The risk factors for a deterioration in nutritional status are many, including poor food intake, food insecurity, poverty, isolation, functional limitations, disease, polypharmacy, poor dentition, alcohol and substance use, depression, and dementia. Screening approaches have incorporated these risk factors; he clarified the clear differences between screening for risk of malnutrition and assessment of the condition. Nutrition screening identifies risk for a specific outcome related to nutritional status, such as functional decline, health care resource use, or malnutrition, whereas nutrition assessment is an in-depth, specific, detailed evaluation to clarify etiology, severity, and appropriate intervention and the intervention outcomes that require monitoring thereafter. He emphasized that screening is less comprehensive and thus requires fewer resources than assessment, which is a more robust evaluation that is more time consuming and takes higher levels of training and skills.
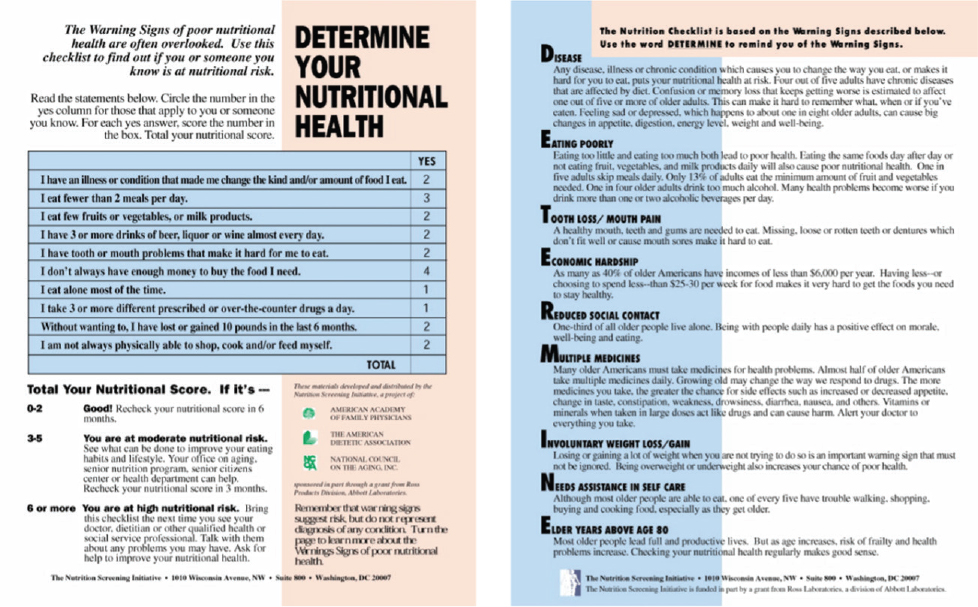
Jensen recounted details of the Nutrition Screening Initiative, which was introduced in the late 1990s through a collaboration of the American Academy of Family Physicians, American Dietetic Association, and National Council on Aging as the first major initiative to promote screening of nutritional status in older adults. The most widely promoted aspect was the Determine Your Nutritional Health checklist, which captured nine risk factors and enabled older adults to tally their self-reported nutritional health status and determine their standing of low, moderate, or high risk (Figure 4-1).
The checklist, meant as a tool to raise public and self-awareness, ended up being used in many applications (e.g., full nutrition assessments in hospitals) for which it was neither intended nor validated, and validation highlighted some limitations. He referenced one example, a 1993 study that examined its application in a Medicare beneficiary population and found that its sensitivity was poor for identifying low nutrient ingestion or perceived poor health (Posner et al., 1993). A few years later, another study reported that some checklist items were significantly associated with mortality. Overall consideration of study results suggested that the checklist might best serve as an awareness and educational tool for older adults and their caregivers (Sahyoun et al., 1997).
___________________
1https://www.sciencedirect.com/topics/medicine-and-dentistry/nutrition-screening#:~:text=Nutrition%20Screening%20Initiative%20(NSI)&text=It%20was%20created%20as%20part,in%20different%20settings%20%5B17%5D (accessed September 14, 2022).
SOURCE: Presented by Gordon Jensen on April 29, 2022.
The Nutrition Screening Initiative released two further tools, a Level I screen that he described as “a step toward assessment” and a Level II screen that was a full-fledged nutrition assessment tool. The Level II screen was intended for use by health care professionals in acute, chronic, and long-term care settings. Jensen explained that it combined the Level 1 screen with more formal assessment variables, which included physical signs and symptoms of deficiency, laboratory testing, and evaluation of cognitive and emotional status using questions from the Mini-Mental State Exam (MMSE) and questions on depression.
According to Jensen, neither tool had widespread application, but he referenced the Level II screen’s use in the Geisinger Rural Aging Study (GRAS) (see Chapter 3) in rural central Pennsylvania. It was administered during enrollment clinic visits in the late 1990s, during which participants completed self-report questions with nurse-measured height and weight. More than 21,600 people 65 years and older enrolled during 1994–1999, and they have received follow-up questionnaires by mail every 3–4 years. The researchers also received data in the form of annual downloads of deidentified electronic health record data from the Geisinger Healthcare System. Over the past 25 years, they have continued to monitor mortality and health outcomes in relation to nutrition risk status.
Jensen referred to Mitchell’s presentation about GRAS (see Chapter 3) in highlighting the comprehensive evaluations conducted with representative subsets of the study cohort. He reiterated what she shared in terms of key findings from the two-plus decades of GRAS research: high prevalence of poor-quality diets, obesity, and poor health; association of obesity with comorbidity and functional decline; and association of low diet quality with lower body mass index (BMI) and increased mortality (Jensen et al., 1997). The study has 177 confirmed centenarians, and its researchers are examining nutrition risk, quality of life, and health outcomes as predictors of living to 100.
Jensen shared results from an evaluation of malnutrition screening focused on older adults (the Mini Nutrional Assessment [MNA]2) that included BMI, calf circumference, weight loss, living environment, mobility, mental status, medications, pressure wounds, dietary habits, self-perceived health, and nutrition. Discriminate analysis comparing the MNA to a comprehensive gold standard of clinical, anthropometric, laboratory, and dietary measures indicated its high levels of sensitivity (96 percent), specificity (98 percent), and predictive value (97 percent) (Vellas et al., 1999). Jensen highlighted that the authors of that work published a paper in 2021 summarizing their 25 years with the MNA, which has included develop-
___________________
2https://www.mna-elderly.com/sites/default/files/2021-10/mna-mini-english.pdf (accessed September 14, 2022).
ing full, short-form, and self-reported MNAs, and the completion of 2,000 reported studies using the MNA (Guigoz and Vellas, 2021).
Jensen described a more recent (Silva et al., 2020) systematic review that examined malnutrition risk screening tools for older adults with COVID-19. It included studies that examined a variety of different screening and assessment tools. The authors noted that most of the instruments had high sensitivity for identifying risk of malnutrition, but none stood out as the best (Silva et al., 2020). The implication of this finding is that it may be about developing tools for not only specific cohorts but possibly even specific types of diseases and disorders, acknowledging that developing and validating a screening tool is a considerable undertaking.
AN INTERNATIONAL EXPERIENCE WITH SCREENING FOR MALNUTRITION
Marian de van der Schueren, Han University, described a European experience with screening older adults for malnutrition. She began with a definition of the screening: a quick and easy procedure using a valid tool, designed to identify those who are malnourished or at risk of malnutrition and may benefit from nutritional intervention from a registered dietitian or clinician with nutrition training (Kondrup et al., 2003). She echoed Jensen’s delineation between screening and assessment and added that screening is only the first step in the nutritional management of older adults.
She observed that a plethora of screening tools have been developed during the past 10–20 years, many of which have been designed and validated for older adults. She explained that most tools are developed to serve one of three purposes: to identify risk of malnutrition, predict outcomes related to nutritional status, or predict response to nutritional support. In the Netherlands, the Short Nutritional Assessment Questionnaire (SNAQ)3 is often used to identify risk of malnutrition, and other tools for this purpose include the Nutritional Risk Screening (NRS),4 MNA,5 Nutritional Risk Index (NRI),6 and Malnutrition Universal Screening Tool (MUST).7 She explained that although each tool was developed and validated specifically for one of the three listed purposes, the reality is that tools intended for malnutrition are also used for the other two purposes and vice versa.
___________________
3https://www.fightmalnutrition.eu/toolkits/summary-screening-tools (accessed September 14, 2022).
4https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6679209 (accessed September 14, 2022).
5https://www.mna-elderly.com/sites/default/files/2021-10/mna-mini-english.pdf (accessed September 14, 2022).
6https://www.sciencedirect.com/science/article/pii/B9780128179901000469 (accessed September 14, 2022).
7https://www.bapen.org.uk/pdfs/must/must_full.pdf (accessed September 14, 2022).
Similarly, some tools developed and validated for older adults (e.g., the MNA and the Geriatric Nutrition Risk Index [GNRI]) are used for younger adults and vice versa.
She discussed her experience as a collaborator on the European Malnutrition in the Elderly project (MaNuEL).8 She described three of the project studies: a review of the validity of malnutrition screening tools used in older adults, development of a scoring system to rate these tools in older adults, and a systematic review of malnutrition risk among older adults in Europe. All three focused on protein-energy malnutrition specifically in older adults.
The review of the validity of malnutrition screening tools examined 48 tools that had been applied in studies with older adults and found that 34 were validated for use in one of four settings: community, rehabilitation, residential care institutions, or hospitals (Power et al., 2018). Some validated tools had been used in only one study and others in as many as nine studies. The tool(s) with greatest evidence of validity for each setting was the SCREEN II instrument (community), the Nutritional Form for the Elderly (NUFFE) (rehabilitation), SNAQ (residential care institutions), and MUST and the Malnutrition Screening Tool (MST; hospitals).
She then discussed the scoring system to rate malnutrition screening tools, which sought to identify which tools rated most highly for being quick, simple, and valid in the same four settings examined in the first MaNuEL study (Power et al., 2019). The research team examined the 48 tools identified in that review and observed that each tool consisted of different items: biochemical measures, anthropometric measures, subjective measures of physical functioning (e.g., difficulty with mobility), social function (e.g., financial situation, access to food), cognitive function (e.g., mental distress/illness, living alone, loss of a partner, dementia), or a combination of these items.
The team developed a rating system underpinned by scientific literature and expert consensus, de van der Schueren said, and scored the 48 tools for their validation, scientific evidence for the included parameters in assessing risk of malnutrition in older adults, and practicability. She explained that each tool was evaluated based on whether it had been validated for use in older adults, the type of validity assessed (construct, criterion, or predictive), the gold standard against which it had been validated, the results (e.g., sensitivity and specificity), and the number of validation studies performed. The team identified 54 parameters with varying levels of evidence. For example, some parameters were deemed not suitable for use (e.g., serum albumin) compared to others (e.g., questions about recent weight loss and appetite). In terms of practicability, the tools were rated based on
___________________
8https://www.healthydietforhealthylife.eu/index.php/news/232-manuel-the-knowledge-hub-on-malnutrition-in-the-elderly (accessed September 14, 2022).
the time required, associated costs, availability in multiple languages, and how widely the tool could be used (i.e., a tool that required staff trained in nutrition scored less well than one that could be used by all staff with minimal training). The tools with the highest scores for each setting were the Determine Your Health Checklist (community), NUFFE (rehabilitation), SNAQ (residential care), and MNA and MST (hospital).
Moving onto the third study, de van der Schueren explained that the systematic review of malnutrition risk in older adults in Europe was based on studies that had used the 22 best-rated malnutrition screening tools (according to the prior MaNuEL studies) validated for use in older adults (Leij-Halfwerk et al., 2019). The research team identified 223 study populations that were examined across the four settings (138 populations were hospital inpatients) comprising more than 500,000 hospital inpatients, almost 3,000 from rehabilitation settings, more than 22,000 from residential care settings, and more than 30,000 from community settings.
The pooled prevalence rates of malnutrition risk in European older adults, combined for health care settings, countries, and malnutrition screening tools, were 22.6 percent for high risk and 48.4 percent for moderate plus high risk (Leij-Halfwerk, 2019, p. 24). She described these results as an important public health consideration, adding that when examined by individual country, the pooled prevalence rates for moderate plus high malnutrition risk ranged from 41 percent in Spain to 67 percent in Finland.
The team also examined malnutrition risk by four of the screening tools (combined for all countries and health care settings) for which adequate power was available, finding that different prevalence rates for both high and moderate plus high malnutrition resulted for each tool (Leij-Halfwerk, 2019, p. 24). The greatest prevalence of high (40.6 percent) and moderate plus high (62.3 percent) risk came from the NRS-2002, for example, and the lowest (19.0 and 39.7 percent, respectively) from the GNRI. When malnutrition risk was examined by health care setting, the highest risk was from hospital settings (28.0 percent for high risk and 53.0 percent for moderate plus high risk) and the lowest from community settings (8.5 and 32.7 percent, respectively).
The key results of the meta-analysis were that close to 23 out of 100 European older adults are at high risk for malnutrition and nearly 50 percent are at any risk for malnutrition. Older age (>80 years) and female gender were associated with higher risk, and differences were observed by health care setting, country, and tool. The results led the researchers to conclude that standardized use of one preferred screening tool per health care setting is strongly recommended.
The three MaNuEL studies occurred just before the 2019 launch of the Global Leadership Initiative in Malnutrition (GLIM), de van der Schueren said, which aims to develop a consensus-based, standardized framework for malnutrition risk screening and diagnosis in adults across settings and
countries (Cederholm et al., 2019; Jensen et al., 2019). GLIM was the first globally accepted approach to malnutrition diagnosis despite broad use of several select malnutrition indicators across continents and countries. In addition, in many regions of the world, access to skilled nutrition professionals and resources is limited, making it necessary to develop and disseminate a simplified approach. The GLIM framework is a global consensus project to help address these issues. The key steps in the framework are to conduct malnutrition risk screening using validated tools, perform a diagnostic assessment consisting of phenotypic and etiologic criteria, and determine if the patient meets criteria for a malnutrition diagnosis. She noted that GLIM continues to be refined, highlighting that one challenge in this process is that different tools have different goals (are screening for different things).
To illustrate the different goals of various tools, de van der Schueren described her team’s effort to screen 200 community-dwelling older adults (without known specific nutritional problems) for malnutrition risk (Borkent et al., 2020). The team used the SNAQ65+ (a version of the questionnaire for adults ≥65 years of age) and the Seniors in the Community: Risk Evaluation for Eating and Nutrition (SCREEN II). The SNAQ65+ screens for malnutrition (characterized by weight loss, impaired muscle mass, and functional difficulties), whereas the SCREEN II screens for risk factors associated with the development of malnutrition. The prevalence of malnutrition was close to 14 percent according to SNAQ65+ and 69 percent according to SCREEN II. It is likely that these differences would influence malnutrition prevalence using GLIM or other approaches to diagnosis.
She shared several take-home messages about malnutrition screening. First, it is important for older adults, given that malnutrition appears to affect up to half of this population, and it is critical to use tools validated for older adults compared to those validated for the general adult population. The choice of tool depends on the goal of screening, such as the example illustrating the differences between the SNAQ and SCREEN II, and also on the setting of the screening. She urged implementation of a system to screen for malnutrition in all health care settings. In the Netherlands, for example, malnutrition risk screening is mandatory in everyone admitted to the hospital; she thinks that has helped advance the nutritional care of older adults.
SCREENING FOR FOOD INSECURITY
Heather Eicher-Miller, Purdue University, discussed food insecurity in older adults, its relationship to poverty, and the association between poor nutrient intake and dietary quality and living in a low-income, food insecure situation. She stated that the prevalence of low incomes among U.S. adults aged 65 and older is about 9 percent (U.S. Census Bureau, 2021), and
having low income presents both nutrition and health risks. This is because a limited income constrains food selection to more economical options that are then subject to other decision-making considerations, such as time and equipment available for food preparation, cooking interest and skills, taste preferences, and cultural considerations.
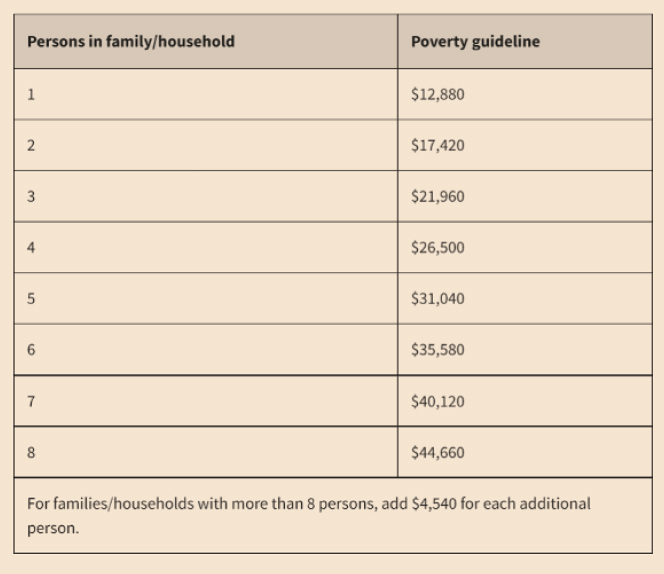
Low income is defined by federal poverty guidelines, which are based on official poverty thresholds that vary by family size and composition and are updated annually (Figure 4-2). If a family’s total income is less than the family threshold, it is considered to be “in poverty.” This is the only population segment officially defined by income level, and the poverty threshold includes the criterion that one-third or more of a household’s expenses after taxes is needed to purchase food (based on the cost of USDA’s thrifty food plan).
Food insecurity, defined as household uncertainty of having or being able to acquire enough food to meet all members’ needs because of insufficient money, is most prevalent among households with incomes near or below the poverty line (Marshall, 2010). Eicher-Miller pointed out that
SOURCE: Presented by Heather Eicher-Miller on April 29, 2022 (ASPE, 2021).
despite some degree of subjectivity in self-reporting sufficient food, this is highly associated with income. Food security can be quantified using the U.S. Household Food Security Survey, an 18-item, self-report questionnaire that assesses concerns about having enough food and whether a household is eating differently because of not having enough resources for food. The results classify households as having food security, low food security (i.e., self-reported reduced dietary quality), or very low food security (i.e., self-reported reduced amount of food consumed). In 2020, 89.5 percent of households were classified as food secure, 6.6 percent as low food secure, and 3.9 percent as very low food secure (Coleman-Jensen et al., 2021). A 2014 survey examined food insecurity among older adults (ages 65–84) specifically, finding that 20 percent of those with a poverty-income ratio of less than three were food insecure (Miller et al., 2020). That ratio is defined as “the ratio of income to the poverty threshold set by the U.S. Census Bureau (adjusted for inflation and family size)” (Miller et al., 2020).
Eicher-Miller discussed the association of poor health and diet with living in a low-income, food insecure situation. Populations that experience food insecurity and low income have poorer nutrient intakes and dietary quality and higher prevalence of overweight, obesity, and chronic diseases, such as diabetes, heart disease, and cancer, compared to populations that are food secure (Bailey et al., 2017; Cowan et al., 2019; Hiza et al., 2013; Holben and Pheley, 2006; Pan et al., 2012; Seligman et al., 2010). A research gap exists in that more studies have examined different or broader age groups than older adults with low incomes and/or food insecurity. The nutrition risks associated with older age (i.e., reduced metabolic rate, decreased bodily functions and mobility, and reduced digestion and absorption of nutrients) are compounded by low income and food insecurity, such that their increased nutrition needs may be harder to achieve. For example, older adults may have reduced access to transportation to obtain food, reduced physical mobility for preparing food, fewer resources for food, and lower access to health care and other wellness resources (Barbagallo et al., 2009; Luhrmann et al., 2009; Russell, 2001; Veldurthy et al., 2016; Volpi et al., 2004).
Eicher-Miller pointed out that nutrients that support healthy aging and that might be of greater need for older adults (protein, calcium, magnesium, zinc, vitamins A, B6, B12, C, D, E and folate) are the same (save vitamin B12) as the list of those that have lower intake in low- versus high-income groups and food-secure versus food-insecure groups (Barbagallo et al., 2009; Luhrmann et al., 2009; Russell, 2001; Veldurthy et al., 2016; Volpi et al., 2004). She reported that 75 percent of older adults (71 years and older) and 66 percent of older adults with incomes less than 130 percent of the poverty level use dietary supplements, which pose an extra expense but indicate that the nutritional risk of older adults is modifiable with
dietary supplement use (Cowan et al., 2018, 2019). Another research gap is that usual nutrient intake from foods is poor among older adults with low incomes, but this group’s usual nutrient intake from total sources (food plus dietary supplements) is unknown.
Eicher-Miller explained that some food assistance is available based on income level and sometimes age. One federal program, the Supplemental Nutrition Assistance Program (SNAP), formerly known as the Food Stamp Program, provides monthly benefits to households with income less than or equal to 130 percent of the poverty level. Other programs are community based, such as food pantries that do not have income restrictions and provide foods to local communities. Community meal and meal delivery programs serve older adults aged 60 years and over at reduced or no cost. Recent changes to the Farm Bill will allow SNAP benefits to be used for dietary supplements, which she believes may help meet known nutrient gaps among older adults but could divert this population’s limited food-purchasing resources to products that do not provide energy. More information about the characteristics of dietary supplement users and nonusers and their effect on dietary quality in older adults with low incomes is required to inform decision-making for SNAP benefits.
Eicher-Miller described her research study to determine, among U.S. older adults with low incomes, the percentage that have food insecurity and the percentage that use dietary supplements. The study then sought to understand, for each population, its usual nutrient intakes (from food alone and from food plus supplements) and dietary quality. The sample was drawn from NHANES 2007–2016 data on individuals aged 60 years or older with incomes below 130 percent of the poverty line. Among the full sample of 2,347 individuals, nearly 40 percent had low or very low food insecurity, up to about 20 percent were using at least one food assistance program, and close to 60 percent were using dietary supplements.
Eicher-Miller reported that usual nutrient intakes from food were generally poor among the study sample; specifically, at least half of the sample did not meet dietary intake recommendations for six (whole grains, sodium, dairy, fatty acids, and vitamin D) of 10 dietary components examined (Jun et al., 2020). For two nutrients, vitamin D and vitamin E, nearly 100 percent did not meet requirements. Nutrient intake improved when both food and supplement sources were considered. The sample’s dietary quality was poor based on the Healthy Eating Index (HEI) score of 58.7 out of 100, and its subscores for individual dietary components within the index were particularly poor for whole grains, sodium, dairy, and fatty acids. When results were stratified to compare dietary supplement users and nonusers, users were more likely to be female, 70 years and older, non-Hispanic White, and of higher educational attainment. Total dietary quality was not significantly different between supplement users and nonusers, she reported, nor was food security status or food assistance use.
Eicher-Miller offered a number of conclusions from the study, beginning with the statement that low income differentiates nutritional risk among older adults. A high prevalence of older adults with low incomes are at risk of inadequate nutrient intakes from foods alone, but dietary supplements play a key role in meeting recommended intakes and are used by about 60 percent of this group. Supplement use greatly affected their nutrition status, and supplements commonly used by the older adult population at large (e.g., calcium) were also the most impactful. Eicher-Miller thought that this supported supplement use to improve situations where low income and food insecurity make it difficult to meet nutrient needs.
Eicher-Miller suggested three research ideas to help close the evidence gap on how to improve nutrient intakes for all older adults, particularly the 40 percent who do not use dietary supplements: examine household resource management and prioritization of foods or supplements, strategies to close the gap between food assistance eligibility and enrollment, and additional characteristics of dietary supplement users and nonusers. Such knowledge could indicate how program and policy changes may support nutrition for older adults with low incomes and food insecurity.
DANISH EXPERIENCES WITH SCREENING
Sussi Friis Buhl, University of Southern Denmark, discussed nutritional challenges among advanced age, self-reliant, community-dwelling adults. She began by noting an important difference between Denmark and other countries: the Danish health care system is publicly financed, primarily through taxes of 37–53 percent. The health care system exists at national, regional, and local levels, and the local level is responsible for many aspects of older adult services, including disease prevention and health promotion, rehabilitation outside of hospitals, home care services, and nursing homes.
One of Denmark’s mandated national disease prevention strategies is preventive home visits for older adults, which are offered annually from 82 years or individually planned for those 65 or over who are at risk of low social, psychological, and physical function (Danish Ministry of Social Affairs, 2015). Buhl explained that the aim is to identify older adults at risk of loss of physical function and those who may transfer into settings where more health care services are needed. Healthy foods are promoted and malnutrition risk assessed during the home visits.
Buhl stated that the issue with this advanced age group is that little is known about their nutritional challenges, because adults over 75 are not included in the Danish national dietary survey, and this self-reliant, community-dwelling population is not systematically screened for nutritional status. Protein malnutrition is of interest in this population; European and Nordic dietary recommendations call for higher protein intakes
to support optimal health while aging for older compared to younger adults, consistent with global recommendations (Deutz et al., 2014; Nordic Council of Ministers, 2014). If protein intake falls short of requirements or the turnover of protein is not balanced by dietary intake, muscle protein synthesis is reduced and muscle mass can decrease (Tome et al., 2021).
Buhl described a study called “I’m Still Standing” that sought to understand if protein malnutrition is a nutritional challenge in adults of advanced age and if it could be addressed within primary prevention strategies (Buhl et al., 2020). The cross-sectional study included two home visits with self-reliant adults aged 80 years and older. Participants completed a 4-day food record in detail, which was used to calculate protein intake, and underwent assessment of risk factors associated with malnutrition via validated screening tools. Of the 126 participants with completed food records, 54 percent had average protein intake below the European minimum recommended level of 1.0 gram per kilogram of body weight. Participants with low protein intakes were older and more likely to have high BMI and low physical function than those at the recommended intakes. Buhl emphasized that unintentional weight loss did not differ between the two groups, although those with low protein intake more frequently reported reduced appetite and mouth dryness. Using the MNA, 83 percent of participants with low protein intake were categorized as normal nutritional status. Buhl concluded that the results indicate a high prevalence of protein malnutrition in these adults, leading to a study to examine whether population screening during preventive home visits can detect risk factors for low protein intake.
Buhl described the Welfare Innovation in Primary Prevention study’s effort to develop and test a screening tool that could identify older adults at risk of losing physical function early (Buhl, 2020, pp. 1-13). It was developed and tested in close collaboration with health care workers and academia. Researchers wanted to know if selected nutrition-related risk factors were associated with accelerated aging or diminished physical function, which they parsed through questions about poor dental status, dysphagia, unintentional weight loss, recent illness, BMI (>27 or <22 kg/m2), and an assessment tool for physical frailty. Participants were 1,430 older adults with an average age of 81 and nearly 61 percent female. The prevalence of physical frailty was 2.7 percent, although nearly half the sample was pre-frail. One or more nutritional risk factors were self-reported for 60.2 percent, and those that were independently associated with physical pre-frail or frail condition were weight loss, dental status, dysphagia, and high BMI. Moreover, presence of two or more nutritional risk factors was associated with more than a twofold increased risk for pre-frail/frail status.
Buhl highlighted that a major challenge in detecting protein malnutrition via primary prevention programs is that specialized equipment is not available in these settings to estimate muscle mass. Anthropometric
measurements are often not feasible within primary prevention, and robust reference ranges do not exist for adults of advanced age, in particular those with coexisting excess weight and reduced muscle mass. Research can inform how to operationalize this in populations with advanced age and high body mass.
PANEL DISCUSSION WITH SPEAKERS
The four speakers answered questions from the workshop’s planning committee members and attendees about best practices, knowledge gaps, and research priorities for nutritional screening of older adults. Topics included food insecurity among older adults during the COVID-19 pandemic, screening for malnutrition in federal food assistance programs, stigma associated with participation in those programs, calf circumference as a surrogate for lean body mass, choice of screening tool for different settings, follow-up actions for individuals identified at home visits as having nutritional risks, and gaps and research priorities for screening.
Food Insecurity Among Older Adults During the COVID-19 Pandemic
Eicher-Miller responded to a question about prevalence of food insecurity during the pandemic. National data are available for 2020 and data on certain segments of time during that year. Overall, data suggest an episodic spike in food insecurity at one point during 2020, but data for the full year suggest that food insecurity rates were relatively unchanged compared with 2019. Eicher-Miller shared that a hypothesis to explain this stability is that quickly implemented changes and flexibilities granted to SNAP and other food assistance programs and the community response of food bank and food pantry support were able to mitigate any spikes. However, data suggest that some racial and ethnic minority groups experienced disproportionately higher rates of food insecurity.
Screening for Malnutrition in Federal Food Assistance Programs
Eicher-Miller explained that SNAP eligibility is based primarily on income and includes certain older U.S. adults with higher incomes than the standard 130 percent poverty threshold cutoff. To her knowledge, the only federal food assistance program that includes a malnutrition screening component, which is offered to participants deemed to be at nutritional risk, is the Special Supplemental Nutrition Program for Women, Infants, and Children. She noted that individuals across the spectrum of BMI can be at risk for malnutrition and added that overweight, obesity, and underweight
are prevalent among older adults with low incomes, unlike younger segments of the low-income population, where underweight is less prevalent.
According to Keller, this situation indicates that the metric to detect malnutrition should be not body weight but unintentional weight loss and change in body weight and foods consumed. It is important that screening tools can detect these factors, and she echoed van der Schueren’s observation that most screening tools focus on significant weight loss, underweight, and the like, which do not capture the full breadth of upstream factors driving malnutrition.
Stigma Associated with Participation in Federal Food Assistance Programs
Carol Boushey, University of Hawai‘i Cancer Center and chair of the workshop planning committee, and Eicher-Miller agreed that they think federal food assistance program participants generally appreciate the opportunity. Eicher-Miller qualified that she has not studied stigma among participants but suggested that some older adults may be reluctant to use these programs out of a desire to be self-reliant. The transition to electronic benefit transfer cards for SNAP benefits was in part due to an attempt to reduce stigma.
Heather Keller, University of Waterloo (UW) and Schlegel-UW Research Institute for Aging, said that Canada does not have an equivalent to SNAP; it has food banks, but older adults do not use these as much as younger adults do, due to location and accessibility. Canada provides a significant advanced age security component that supports food security among older adults, which is the population with the lowest rates of food insecurity.
Keller referenced qualitative research about messaging nutrition risk, reporting that some older adults become offended when told they are at nutrition risk or are malnourished or are in denial. Language sensitivities may be different across countries, and she urged consideration of the language used to convey that nutritional concerns exist and should be addressed.
Calf Circumference as a Surrogate for Lean Body Mass
A planning committee member asked the speakers to describe any evidence to support the use of calf circumference measurements as a surrogate for lean body mass. Jensen replied that validation research has been done and that this measure is easy to use, portable, and practical. He wondered how it compares to other portable measures of muscle in terms of predictive value for lean body mass; it would be a major breakthrough if a portable imaging or ultrasound technique for measuring lean mass were developed and validated for older adults.
A recent GLIM paper promoted calf circumference as a proxy measure for lean body mass, de van der Schueren said, because GLIM is intended to be used worldwide (Barazzoni et al., 2022, pp. 1425–1433). Low-income countries and other countries that want to use GLIM in the community do not have CT or MRI in those settings, so anthropometric measures were added to the phenotypic criteria to enable muscle mass assessment. Keller concurred that calf circumference is easy to measure in the community, requires little training, and is highly correlated with standardized measures of malnutrition, such as the Subjective Global Assessment or MNA.
Calf circumference could be used in preventive home visits in Denmark, Buhl said, given its ease of use in primary prevention. A potential concern is that an increasing number of older adults are both overweight and malnourished, and she wondered if malnutrition is still detectable via calf circumference for them.
Jensen said that malnutrition among older adults with overweight or obesity has become a concern. As an example, he shared that micronutrient deficiencies are common in older Pennsylvanians who have obesity, but screening is not typically conducted for these. On the other hand, he said, screening for unintentional weight loss among older adults with obesity could raise a red flag. Jensen said that he was not aware of any fully validated malnutrition risk screening tools for older adults with overweight or obesity. The GLIM approach is one of few that readily facilitates malnutrition diagnosis among overweight or obese individuals.
Choice of Screening Tool for Different Settings
A workshop attendee asked what screening tool would be best for population studies, home-delivered and congregate meal settings, and assisted-living facilities. The participants in each of those settings are different, Keller pointed out, and therefore so are the malnutrition risk factors, which would call for a different screening tool in each setting. Corish said that according to the MaNuEL project’s tool scoring system, those with the highest scores for different settings were the Determine Your Health Checklist (community), NUFFE (rehabilitation), SNAQ (residential care), and MNA and MST (hospital). For a large cohort study, de van der Schueren suggested keeping questions simple and asking about involuntary weight loss and BMI status.
Follow-Up Actions for Individuals with Nutrition Risks as Identified at Home Visits
Buhl said that Danish health care personnel conduct the preventive health visits for older adults, such as physical or occupational therapists, nurses, or clinical dietitians. The visits are financed by federal tax dollars
as part of a preventive strategy; this is a voluntary offer but also a targeted intervention to prevent the need for in-home services or nursing home care.
A new guideline from the Danish health authority is expected soon that will recommend follow-up action if unintentional weight loss is identified during a home visit. She suggested a systematic approach whereby a standardized question about unintentional weight loss is asked at all such visits. Health care staff who conduct the visits cover many topics during the 45 minutes or so, and a specific guideline could help ensure that nutrition is addressed.
An attendee asked Buhl what happens after an individual is identified as having protein insufficiency or other malnutrition. She responded that it depends on where the individual lives, because the municipalities that provide preventive home visits also offer different follow-up strategies to address any conditions identified. Many municipalities have clinical dietitians or other professionals with nutritional expertise, who visit affected individuals to provide dietary advice.
Gaps and Research Priorities for Nutritional Screening
In this era of multiple screening tool options, de van der Schueren said, the next steps are to determine what are the goals of screening, which tools fit those goals, and how screening can best be implemented and connected to interventions to address any abnormalities. Corish concurred and praised GLIM’s progress in harmonizing global malnutrition screening efforts, urging further global collaboration to advance progress in the coming decades.
REFERENCES
ASPE (Office of the Assistant Secretary for Planning and Evaluation). 2021. 2021 poverty guidelines for the 48 contiguous states and the District of Columbia. ASPE.
Bailey, R. L., S. R. Akabas, E. E. Paxson, S. V. Thuppal, S. Saklani, and K. L. Tucker. 2017. Total usual intake of shortfall nutrients varies with poverty among U.S. adults. Journal of Nutrition Education and Behavior 49(8):639–646 e633.
Barazzoni, R., G. L. Jensen, M. I. T. Correia, M. C. Gonzalez, T. Higashiguchi, H. P. Shi, S. C. Bischoff, Y. Boirie, F. Carrasco, A. Cruz-Jentoft, and V. Fuchs-Tarlovsky. 2022. Guidance for assessment of the muscle mass phenotypic criterion for the Global Leadership Initiative on Malnutrition (GLIM) diagnosis of malnutrition. Clinical Nutrition 41(6):1425–1433.
Barbagallo, M., M. Belvedere, and L. J. Dominguez. 2009. Magnesium homeostasis and aging. Magnesium Research 22(4):235–246.
Borkent, J. W., L. T. Schuurman, J. Beelen, J. O. Linschooten, H. H. Keller, A. J. C. Roodenburg, and M. A. E. De van der Schueren. 2020. What do screening tools measure? Lessons learned from SCREEN II and SNAQ(65). Clinical Nutrition ESPEN 38:172–177.
Buhl, S. F., A. M. Beck, B. Christensen, and P. Caserotti. 2020. Effects of high-protein diet combined with exercise to counteract frailty in pre-frail and frail community-dwelling older adults: Study protocol for a three-arm randomized controlled trial. Trials 21(1):1–13.
Cederholm, T., G. L. Jensen, M. Correia, M. C. Gonzalez, R. Fukushima, T. Higashiguchi, G. Baptista, R. Barazzoni, R. Blaauw, A. Coats, A. Crivelli, D. C. Evans, L. Gramlich, V. Fuchs-Tarlovsky, H. Keller, L. Llido, A. Malone, K. M. Mogensen, J. E. Morley, M. Muscaritoli, I. Nyulasi, M. Pirlich, V. Pisprasert, M. A. E. de van der Schueren, S. Siltharm, P. Singer, K. Tappenden, N. Velasco, D. Waitzberg, P. Yamwong, J. Yu, A. Van Gossum, C. Compher, GLIM Core Leadership Committee, and GLIM Working Group. 2019. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. Clinical Nutrition 38(1):19.
Coleman-Jensen, A., M. P. Rabbitt, C. A. Gregory, and A. Singh. 2021. Household food security in the United States in 2020. U.S. Department of Agriculture, Economic Research Service.
Cowan, A. E., S. Jun, J. J. Gahche, J. A. Tooze, J. T. Dwyer, H. A. Eicher-Miller, A. Bhadra, P. M. Guenther, N. Potischman, K. W. Dodd, and R. L. Bailey. 2018. Dietary supplement use differs by socioeconomic and health-related characteristics among U.S. adults, NHANES 2011–2014. Nutrients 10(8).
Cowan, A. E., S. Jun, J. A. Tooze, H. A. Eicher-Miller, K. W. Dodd, J. J. Gahche, P. M. Guenther, J. T. Dwyer, N. Potischman, A. Bhadra, and R. L. Bailey. 2019. Total usual micronutrient intakes compared to the Dietary Reference Intakes among U.S. adults by food security status. Nutrients 12(1).
Danish Ministry of Social Affairs. 2015. Consolidation act on social services. https://english.sm.dk/media/14900/consolidation-act-on-social-services.pdf (accessed September 14, 2022).
Deutz, N. E., J. M. Bauer, R. Barazzoni, G. Biolo, Y. Boirie, A. Bosy-Westphal, T. Cederholm, A. Cruz-Jentoft, Z. Krznaric, K. S. Nair, P. Singer, D. Teta, K. Tipton, and P. C. Calder. 2014. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN expert group. Clinical Nutrition 33(6):929–936.
Guigoz, Y., and B. Vellas. 2021. Nutritional assessment in older adults: MNA® 25 years of a screening tool and a reference standard for care and research; what next? Journal of Nutrition, Health & Aging 25(4):528–583.
Hiza, H. A., K. O. Casavale, P. M. Guenther, and C. A. Davis. 2013. Diet quality of Americans differs by age, sex, race/ethnicity, income, and education level. Journal of the Academy of Nutrition and Dietetics 113(2):297–306.
Holben, D. H., and A. M. Pheley. 2006. Diabetes risk and obesity in food-insecure households in rural Appalachian Ohio. Preventing Chronic Disease 3(3):A82.
Jensen, G. L., K. Kita, J. Fish, D. Heydt, and C. Frey. 1997. Nutrition risk screening characteristics of rural older persons: Relation to functional limitations and health care charges. American Journal of Clinical Nutrition 66(4):819–828.
Jensen, G. L., T. Cederholm, M. Correia, M. C. Gonzalez, R. Fukushima, T. Higashiguchi, G. A. de Baptista, R. Barazzoni, R. Blaauw, A. J. S. Coats, A. Crivelli, D. C. Evans, L. Gramlich, V. Fuchs-Tarlovsky, H. Keller, L. Llido, A. Malone, K. M. Mogensen, J. E. Morley, M. Muscaritoli, I. Nyulasi, M. Pirlich, V. Pisprasert, M. de van der Schueren, S. Siltharm, P. Singer, K. A. Tappenden, N. Velasco, D. L. Waitzberg, P. Yamwong, J. Yu, C. Compher, and A. Van Gossum. 2019. GLIM criteria for the diagnosis of malnutrition: A consensus report from the global clinical nutrition community. Journal of Parenteral and Enteral Nutrition 43(1):32–40.
Jun, S., A. E. Cowan, A. Bhadra, K. W. Dodd, J. T. Dwyer, H. A. Eicher-Miller, J. J. Gahche, P. M. Guenther, N. Potischman, J. A. Tooze, and R. L. Bailey. 2020. Older adults with obesity have higher risks of some micronutrient inadequacies and lower overall dietary quality compared to peers with a healthy weight, National Health and Nutrition Examination Surveys (NHANES), 2011–2014. Public Health Nutrition 23(13):2268–2279.
Kondrup, J., S. P, Allison, M. Elia, B. Vellas, M. Plauth, Educational and Clinical Practice Committee, and European Society of Parenteral and Enteral Nutrition. 2003. ESPEN guidelines for nutrition screening 2002. Clinical Nutrition 22(4):415–421.
Leij-Halfwerk, S., M. H. Verwijs, S. van Houdt, J. W. Borkent, P. R. Guaitoli, T. Pelgrim, M. W. Heymans, L. Power, M. Visser, C. A. Corish, M. A. E. de van der Schueren, and MaNuEL Consortium. 2019. Prevalence of protein-energy malnutrition risk in European older adults in community, residential and hospital settings, according to 22 malnutrition screening tools validated for use in adults ≥65 years: A systematic review and meta-analysis. Maturitas 126:80–89.
Luhrmann, P. M., R. Bender, B. Edelmann-Schafer, and M. Neuhauser-Berthold. 2009. Longitudinal changes in energy expenditure in an elderly German population: A 12-year follow-up. European Journal of Clinical Nutrition 63(8):986–992.
Marshall, E. L. 2010. Examining the relationship between weight, food insecurity, food stamps, and perceived diet quality in school-aged children. University of Kentucky Master’s Theses (45).
Miller, L. M. S., D. J. Tancredi, L. L. Kaiser, and J. T. Tseng. 2020. Midlife vulnerability and food insecurity: Findings from low-income adults in the U.S. National Health Interview Survey. PLoS One 15(7):e0233029.
Nordic Council of Ministers. 2014. Nordic nutrition recommendations 2012. https://norden.diva-portal.org/smash/get/diva2:704251/FULLTEXT01.pdf (accessed September 14, 2022).
Pan, L., B. Sherry, R. Njai, and H. M. Blanck. 2012. Food insecurity is associated with obesity among U.S. adults in 12 states. Journal of the Academy of Nutrition and Dietetics 112(9):1403–1409.
Posner, B. M., A. M. Jette, K. W. Smith, and D. R. Miller. 1993. Nutrition and health risks in the elderly: The Nutrition Screening Initiative. American Journal of Public Health 83(7):972–978.
Power, L., D. Mullally, E. R. Gibney, M. Clarke, M. Visser, D. Volkert, L. Bardon, M. A. E. de van der Schueren, C. A. Corish, and MaNuEL Consortium. 2018. A review of the validity of malnutrition screening tools used in older adults in community and healthcare settings—A MaNuEL study. Clinical Nutrition ESPEN 24:1–13.
Power, L., M. A. E. de van der Schueren, S. Leij-Halfwerk, J. Bauer, M. Clarke, M. Visser, D. Volkert, L. Bardon, E. Gibney, C. A. Corish, and MaNuEL Consortium. 2019. Development and application of a scoring system to rate malnutrition screening tools used in older adults in community and healthcare settings—A MaNuEL study. Clinical Nutrition 38(4):1807–1819.
Russell, R. M. 2001. Factors in aging that effect the bioavailability of nutrients. Journal of Nutrition 131(4 Suppl):1359S-1361S.
Sahyoun, N. R., P. F. Jacques, G. E. Dallal, and R. M. Russell. 1997. Nutrition screening initiative checklist may be a better awareness/educational tool than a screening one. Journal of the American Dietetic Association 97(7):760–764.
Seligman, H. K., B. A. Laraia, and M. B. Kushel. 2010. Food insecurity is associated with chronic disease among low-income NHANES participants. Journal of Nutrition 140(2):304–310.
Silva, D. F. O., S. Lima, K. C. M. Sena-Evangelista, D. M. Marchioni, R. N. Cobucci, and F. B. Andrade. 2020. Nutritional risk screening tools for older adults with COVID-19: A systematic review. Nutrients 12(10).
Tome, D., S. Benoit, and D. Azzout-Marniche. 2021. Protein metabolism and related body function: Mechanistic approaches and health consequences. Proceedings of the Nutrition Society 80(2):243–251.
U.S. Census Bureau. 2021. Figure 8. Number in poverty and poverty rate: 1959 to 2020: Current Population Survey, 1960 to 2021 Annual Social and Economic Supplements (CPS ASEC).
Veldurthy, V., R. Wei, L. Oz, P. Dhawan, Y. H. Jeon, and S. Christakos. 2016. Vitamin D, calcium homeostasis and aging. Bone Research 4:16041.
Vellas, B., Y. Guigoz, P. J. Garry, F. Nourhashemi, D. Bennahum, S. Lauque, and J. L. Albarede. 1999. The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition 15(2):116–122.
Volpi, E., R. Nazemi, and S. Fujita. 2004. Muscle tissue changes with aging. Current Opinion in Clinical Nutrition and Metabolic Care 7(4):405–410.




















