
The fourth and final workshop, held May 6, 2022, featured four presentations that highlighted policies, practices, and related challenges that affect older adults, followed by a panel discussion with the speakers. Presentation topics included education policy, food policy, health care payment policy, and the policy landscape.
Elbert Huang, University of Chicago, and Rose Ann DiMaria-Ghalili, Drexel University, co-moderated the session. Huang briefly outlined the role of policy in moving the field toward optimal dietary assessment. The field will determine optimal approaches to nutritional screening and dietary assessment and which are most suitable for community, long-term care, and hospital settings. In his ideal world, screening and assessment would be applied universally and the results translated into targeted nutritional interventions that produce enhanced outcomes for older adults (Figure 5-1).
Huang raised three examples of policy questions that relate to his diagram (Figure 5-1). First, who is responsible for delivery of screening and assessment, and how should that workforce be educated? Second, what role should health care and health insurance systems play in both screening and assessment and targeted nutritional interventions? Third, what is the role of federal food assistance programs, and how can they incorporate the latest findings in assessment?
Huang pointed out that multilayered influences beyond individual factors, such as knowledge and preferences, affect food choices, such as various sociocultural, community, agricultural, government, and even global factors (Mozaffarian et al., 2018). Interest is heightened in nutrition policy;
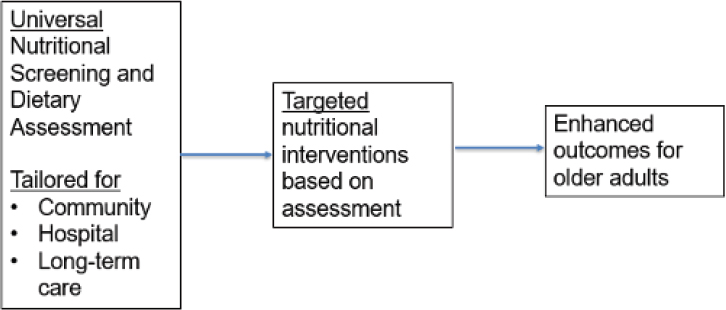
SOURCE: Presented by Elbert Huang on May 6, 2022.
he shared the example that the Biden-Harris administration announced the White House Conference on Hunger, Nutrition, and Health for September 2022.1 This is only the second-ever White House conference on these topics since 1969, and it will release a national strategy for ending hunger and improving nutrition and physical activity by 2030 so that fewer Americans experience diet-related chronic diseases.
EDUCATION POLICY: TEACHING ABOUT FOOD AND NUTRITION IN MEDICINE
Timothy Harlan, George Washington University, discussed nutrition education for health care professionals beyond registered dietitians (e.g., physicians, residents, medical and nursing students). Many physicians think that their patients do not listen to them, he said, when it comes to healthy lifestyle counseling. But evidence suggests that patients listen to physician advice about health behavior change (Kreuter et al., 2000), and when physicians disclose healthy personal behaviors, it improves their credibility and ability to motivate patients to adopt healthy habits (Frank et al., 2000). In other words, patients are more likely to follow physicians who “talk the talk” and “walk the walk.” This principle is borne out in the smoking cessation literature, which indicates that prevalence of physician smoking fell from nearly 60 percent in 1945 to around 5 percent in 1985 as the health
___________________
1https://health.gov/our-work/nutrition-physical-activity/white-house-conference-hunger-nutrition-and-health#:~:text=The%202022%20White%20House%20Conference,close%20the%20disparities%20surrounding%20them (accessed September 14, 2022).
effects became apparent (Smith, 2008). The decrease in smoking prevalence among the public is not as drastic but follows a similar trajectory, and Medicare reimburses physicians to discuss smoking cessation.
Harlan said that despite the evidence that suggests the positive effect of health care professional counseling on patient behavior change few policies exist in terms of educating the workforce in nutrition principles and counseling strategies. He referenced a report on nutrition education in medical schools (National Research Council Committee on Nutrition in Medical Education, 1985), which was one of the first attempts to issue policy recommendations. It recommended a minimum of 25–30 classroom hours in nutrition during the preclinical years; in 2002, the National Institutes of Health (NIH) set forth a nutrition curriculum guide that describes what physicians and health care professionals need to know to be equipped to discuss diet and dietary behaviors with patients (Curriculum Committee of the Nutrition Academic Award Program, 2002). Nonetheless, a 2010 survey of accredited U.S. medical schools indicated that most do not meet that minimum recommendation (Adams et al., 2006). A standardized nutrition curriculum for medical schools does not exist, although the Liaison Committee on Medical Education (the accrediting body for educational programs at U.S. and Canadian schools of medicine) and Association of American Medical Colleges (Kushner et al., 2014) have also issued recommendations. Each medical school sets its own curriculum; he shared an example from his own institution, where approximately 1 percent of the objectives required of first- and second-year students are related to nutrition. Harlan pointed out that nutrition encompasses a broad range of topics, such as physiologic aspects (e.g., digestion, absorption, and metabolism) and dietary assessment and behavior change counseling.
Harlan mentioned a nonprofit organization, the Culinary Medicine Specialist Board, a group of several dozen medical schools and partner sites with a vision to “empower healthier lifestyles and reshape the course of chronic disease in America by integrating the science of medicine into culinary tradition” (Stauber et al., 2022, pp. 214-220). The core of this initiative is community programming delivered directly to patients, which includes hands-on cooking classes at teaching kitchens in medical schools and hospitals.
Another component is medical student programming on nutrition and culinary topics; it empowers students to be what he called “force multipliers” by providing the opportunity to help deliver the community programming. First- and second-year students in 10 medical schools are required to take a 3-hour course that introduces them to nutrition, cooking techniques, and techniques for patient communication about dietary behaviors (Pang et al., 2019). Hands-on cooking classes combine case- and team-based learning that connect the physiological aspects of nutrition to the food-related patient conversations. An eight-module culinary medicine elective is also
available for students interested in additional coursework; it includes 33 modules that schools may include. These cover a range of foundational topics and nutrition for various life stages and conditions (e.g., heart disease, diabetes, celiac disease, food allergies, HIV, and eating disorders), which emphasizes that nutrition spans a wide variety of topics. He highlighted a module on geriatrics, admitting that it is relatively short and could be expanded substantially.
Harlan discussed the Mediterranean-style diet, which is a focus of the programming for both community members and medical professionals. It is emphasized based on evidence supporting its effectiveness for weight loss (Sacks et al., 2009), reduced risk of cardiovascular disease events (de Lorgeril et al., 1999), and positive outcomes for a number of other common chronic diseases. Based on evidence indicating that patients in the highest tertile of diet scores experienced significantly lower risk of all-cause mortality compared to patients with lower scores (Trichopoulou et al., 2003), program participants are encouraged to improve their scores by consuming more vegetables, legumes, fruits and nuts, whole grains, and seafood; better-quality oils and fats; and less dairy and meat. Medical students learn how to administer a 24-hour dietary recall, assess the results, and provide counseling to help improve a patient’s scores.
Harlan said that programming is also being implemented at culinary schools, based on the impact potential of educating culinarians in how to deliver high-quality, nutrient-rich foods that positively affect health. In addition, programming is available for practicing health care professionals, such as continuing medical education courses, a 60-credit-hour Certified Culinary Medicine Specialist program, and an annual Culinary Medicine Conference. Standardized policies on integrating these topics in medical education do not exist, but he recommended this.
Harlan shared 7 years of data collected to assess the effectiveness of the culinary medicine elective (Leong et al., 2014). It includes 25 core competencies, and students were assessed for their level of improvement in demonstrating each one compared to a control group of nonparticipants. The first year of data indicated a statistically insignificant improvement in most competencies. After rebuilding the courseware, the results dramatically improved for the second and third years. A key factor was involving the students, to understand what they needed to succeed. The program had additional learnings as more medical schools implemented it and contributed results data, and by the seventh year, participants satisfactorily achieved all 25 competencies. Participants are four times more likely to understand Mediterranean or DASH diet principles and have a meaningful conversation with patients about these approaches.
Harlan said that the programming for community members has been found to improve Mediterranean diet scores, attitudes toward cooking, and
healthy eating habits, and likelihood of engaging in positive dietary behaviors, with 3 years of data on approximately 500 participants indicating that scores improved notably after the revision (Stauber et al., 2022). In a randomized trial of families, a six-module series was delivered to improve parents’ and children’s scores. Dramatic improvements were observed compared to a control group, and grocery store receipts were used to project that a family of four would save almost $6,000 per year.
Harlan briefly raised the issue of reimbursement for health care services, which is key when it comes to health care professionals providing nutritional counseling for a range of conditions. He estimated that more than half of patients present for a diet-related condition or disease, and even those who do not will have questions about food. Despite the high importance of food to many patients, medical professionals, outside of dietitians, are not explicitly reimbursed for counseling or guidance.
FOOD POLICY: MEALS ON WHEELS
Ucheoma Akobundu, Meals on Wheels, began with an overview of the national association; it has a network of 5,000+ local and community-based organizations (CBOs) dedicated to addressing social isolation and hunger among older adults. It serves virtually every U.S. community and has more than two million staff and volunteers who deliver nutritious meals and conduct friendly visits and safety checks to enable recipients to live nourished lives with independence and dignity. The national association provides expertise, funding, leadership, education, research, and advocacy support to empower and strengthen local organizations and their staff of aging services, nutrition and food service management, and social service professionals.
Akobundu said that older adults proactively reach out to local Meals on Wheels programs and are screened for nutrition risk and assessed for nutrition needs before receiving services. This helps ensure that services align with their personal lifestyle and culture and any medical needs. Screening is conducted by generalist staff and volunteers, but more specialized nutrition education, counseling, and dietary supplements are provided by registered dietitians.
Akobundu discussed opportunities for policy actions to support nutrition in light of the pandemic’s effects on both national and community issues, such as availability of and access to safe and nutritious food, health and nutrition services and interventions, and social support. These challenges have exposed opportunities for reinvention and reimagination in both policy and programmatic areas, which has resulted in targeted, smart policy changes that allow food assistance and nutrition services to flow to older adults most in need. Such changes impacted food production,
processing, marketing, and distribution, to promote greater equity among vulnerable groups and provide improved food accessibility and availability.
Akobundu discussed the food policy landscape that governs these services, focusing on the Older Americans Act (OAA).2 It is a partially federally funded, state-administered social services program to assist older adults and their families, it undergirds Meals on Wheels services nationwide. The act includes establishing an “Aging Network,” composed of federal, state, and local agencies to plan and provide services that help individuals to live independently in their homes and communities. This network develops programming for populations with the greatest social and economic need, particularly those who have low incomes, are of minority racial/ethnic backgrounds, reside in rural areas, have limited English proficiency, or are at risk for malnutrition and institutionalization.
Akobundu explained that within OAA, Title III-C (the nutrition services program)3 aims to reduce hunger, food insecurity, and malnutrition; promote socialization; and improve the health and well-being of older adults by helping them access nutrition and other disease prevention and health promotion services, delaying the onset of adverse outcomes. Since OAA’s establishment in 1972, it had three reauthorizations that changed its focus and funding priorities in response to evolving social, demographic, and economic conditions. The first phase focused on life-enhancing or age-mitigating services, pursued mainly through congregate dining programs and home-delivered meal services. In the 1980s, the focus shifted to mitigating vulnerability; in the 1990s, it became integrating care and chronic disease management. Akobundu predicted a focus on integrating technology, noting that “seismic challenges” from the pandemic have accelerated the Aging Network’s pivot to technology adoption.
Akobundu elaborated on these challenges, such as shelter-in-place requirements, closing of congregate dining sites, loss of access to senior centers where older adults received services, the impact of social distancing, and reduced home visits. The resulting focus on technology provides opportunities to better support, evolve, and accelerate how aging and nutrition services are provided in the community, leading to positive effects on reach, uptake, and outcomes. For example, technological approaches can facilitate collection of nutrition assessment information in homes and communities by Meals on Wheels program staff and nutrition professionals. Despite these advances, Akobundu emphasized the value of the high-touch,
___________________
2https://uscode.house.gov/view.xhtml?path=/prelim@title42/chapter35&edition=prelim (accessed September 14, 2022).
3https://acl.gov/sites/default/files/programs/2019-01/AoA_Issue_Brief_Food_Sources.pdf (accessed September 14, 2022).
in-person, in-home services that are at the heart of OAA and still desired by older adults.
Poverty, social isolation, food insecurity, and disability were challenges for older adults prior to the pandemic and worsened in its wake. Food insecurity among older adults rose from 2.8 to 4.9 percent between 2019 and 2020 (Kinderknecht et al., 2022), and Meals on Wheels programs reported delivering an average of up to 100 percent more meals weekly during 2020. Many older adults, particularly those with physical limitations, had to quickly learn new ways of preparing food, navigating the loss of employment and/or transportation, and adhering to stay-at-home orders while also avoiding exposure to the virus. Akobundu highlighted present challenges, including rising food and gas prices, supply chain issues, hiring and retaining sufficient staff, and a lack of registered community dietitians with expertise in geriatric nutrition.
Akobundu described how Meals on Wheels pivoted early in the pandemic to adapt services to safely meet client needs. Almost all programs changed how services were provided, such as reworking home-delivered meal options and logistics. About half of them tapped local partnerships to help fill gaps and provide emergency meals, and a similar proportion served congregate meal clients in alternative formats, such as grab-and-go, drive-thru, or curbside pick-up. She added that more than half developed opportunities to address social isolation.
With respect to policy pivots during COVID-19, Akobundu listed responses such as expanding eligibility and enrollment criteria to serve more people, decreasing administrative burdens, and facilitating greater access to nutrition services. As an example, she recalled that the Administration for Community Living leveraged flexibilities that were already in statute to ensure that programs could expand to reach older adults in need, such as shifting models to grab-and-go services that could continue to use existing funding streams. Another example is a Coronavirus Aid, Relief, and Economic Security Act provision4 that enables transferring funding from one service stream to another while bypassing usual administrative processes.
Akobundu shared evidence on the pandemic’s impact on older adult dietary intakes, nutrition status, and food security, noting that COVID-19 mitigation policies and practices results in a shift in how food is accessed and consumed. Recent systematic reviews suggest that older adults’ food access, diet quality, and nutritional status were maintained or even improved during the pandemic, but these results are not consistent within or across studies (Nicklett et al., 2021). Furthermore, local providers across the Meals
___________________
4https://www.kff.org/coronavirus-covid-19/issue-brief/the-coronavirus-aid-relief-and-economic-security-act-summary-of-key-health-provisions (accessed September 14, 2022).
on Wheels network report food access constraints and negative impacts on their nutritional status.
Akobundu suggested that a shared advocacy agenda includes doubling federal funding for OAA nutrition programs, which are a “proven antidote” to loneliness, hunger, and malnutrition. She also appealed for advancing policies and innovations that support community-based nutrition programs as they strive to serve more older adults and strengthening and expanding the broader network of nutrition and social programs—especially within the charitable sector—that provide vital services and assistance to older adults and their families. She urged policies that support an infusion of focused, targeted funding, programming, time, and outreach effectively used by CBOs to meet the nutrition and well-being needs of older adults.
Akobundu underscored that pandemic-driven food insecurity and hunger are likely to persist as society moves into a post-pandemic era. Older adults will continue to need responsive, safe, person-centered access to services that support their nutrition and wellness needs, and she listed three strategies for addressing these needs during the “next normal.” First is to continue expanding effective policy approaches and scaling them in different areas of the country. Second is to “build bridges to build a bigger table,” by expanding connections to community-based senior nutrition programs to other service sectors. Health care providers are often in a position to regularly monitor food insecurity in patients, for example, and make referrals to community-based services to meet identified patient needs. Third is to prioritize nutrition security to mitigate the risk of malnutrition among older adults.
HEALTH CARE PAYMENT POLICY: NEW OPPORTUNITIES TO USE MEDICARE DOLLARS TO ADDRESS NUTRITION AND SOCIAL DETERMINANTS OF HEALTH
Marshall Chin, University of Chicago, discussed new opportunities to use health care payment policy levers to address nutrition and social determinants of health. He began by referencing data on the U.S. total health service expenditures, which make up more than half of the country’s gross domestic product (GDP). This makes the United States an outlier compared to many other Organisation for Economic Co-operation and Development (OECD) countries, he pointed out, where social service expenditures are a majority of the GDP (Bradley et al., 2011). Chin noted a tension and bias in medicine and health care because topics such as food insecurity and social determinants of health are seen as outside the realm of medicine and health care spending.
Most consumer advocacy groups have traditionally focused on improving access to health care (i.e., access to and expansion of health insurance coverage), although more recently, they have expanded their efforts to
include quality of care and payment policy, recognizing that both levers are powerful in terms of the flow of health care dollars. Although these two topics are a little arcane, he pointed out that “this is where a lot of the action is emerging” with respect to the potential to impact food insecurity and social determinants of health among older adults. He urged attendees to understand how these and other payment policy levers could affect food and added that the levers also interact with each other and should not be viewed in isolation.
Chin provided context for his presentation’s frame of health equity and social determinants of health. He shared the World Health Organization (WHO) definition of equity, noting its nod to social justice: “Equity is the absence of avoidable or remediable differences among groups of people, whether those groups are defined socially, economically, demographically, or geographically. Health inequities therefore involve more than inequality with respect to health determinants, access to the resources needed to improve and maintain health or health outcomes. They also entail a failure to avoid or overcome inequalities that infringe on fairness and human rights norms.”5 He shared an illustration (Figure 5-2) that depicts the difference between providing the same solution to diverse individuals versus providing individually tailored solutions to meet their different needs and maximize their potential.
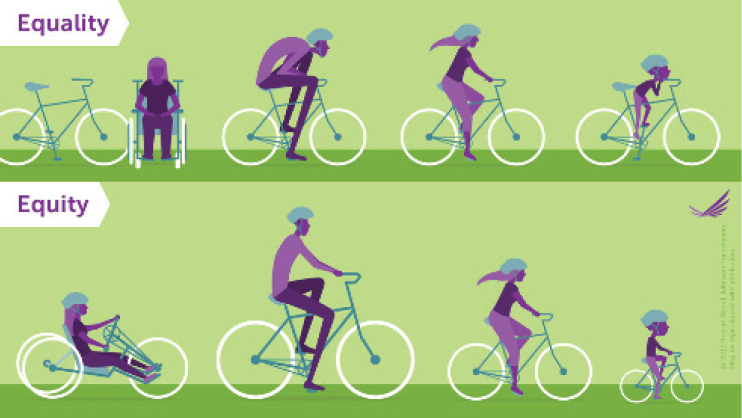
SOURCE: Presented by Marshall Chin on May 6, 2022 (Robert Wood Johnson Foundation, 2017).
___________________
5https://www.who.int/health-topics/health-equity#tab=tab_1 (accessed September 14, 2022).
Chin described a framework for advancing health equity (Figure 5-3). He referenced the right side of the framework, which emphasizes payment reform that supports and incentivizes care transformation to advance health equity. He also noted the importance of cross-sectional partnerships to address medical and social drivers of health. He underscored that if advancing health equity is to become a reality, actors must be intentional and commit to the mission of maximizing health among diverse individuals and populations. The classic route in health care is to examine one’s data to assess whether a disparate outcome has occurred, conduct a root cause analysis to identify why the disparity exists, and design and implement specific care interventions that address the root causes. Creating a culture of equity is of paramount importance, which includes understanding one’s own personal biases and identifying system structures that bias against and oppress marginalized populations. All of these things affect individual and population health as well as health care equity.
WHO defines social determinants of health as “the conditions in which people are born, grow, live, work, and age. These circumstances are shaped by the distribution of money, power, and resources at global, national, and local levels. The social determinants of health are mostly responsible for health inequities, the unfair and avoidable differences in health status seen within and between countries.”6 Chin observed a growing recognition that social drivers of health are very powerful causes of inequities in health outcomes.
Chin referenced his work with the Robert Wood Johnson Foundation’s Advancing Health Equity program, which works with state Medicaid agencies, Medicaid managed care organizations, and health care organizations to achieve health equity. The program has a Health Care Payment Learning & Action Network, an active group of several hundred public and private health care leaders dedicated to providing thought leadership, strategic direction, and ongoing support to accelerate the U.S. health care system’s adoption of alternative payment models for Medicare and Medicaid. A theme of that work is that the field needs to do a better job of connecting the dots in terms of advancing payment reform that supports and incentivizes care transformation to address medical and social needs and advance health equity.
Chin said that the predominant U.S. health care system is a fee-for-service approach; payment is rendered for individual services, which incentivizes service volume. A shift toward value-based payment is occurring, which rewards the quality—instead of the quantity—of health care services
___________________
6https://www.who.int/westernpacific/activities/taking-action-on-the-social-determinants-of-health#:~:text=Social%20determinants%20of%20health%20are,themselves%20influenced%20by%20policy%20choices (accessed September 14, 2022).
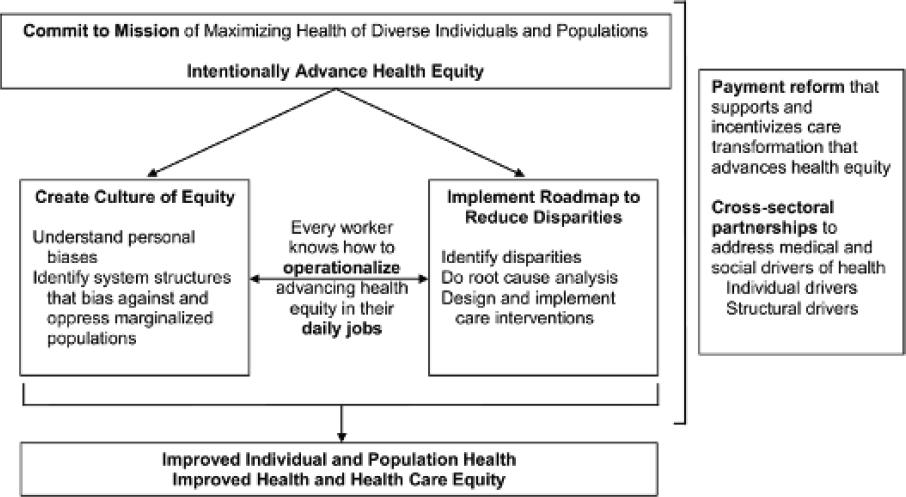
SOURCE: Presented by Marshall Chin on May 6, 2022 (Chin, 2020).
and health outcomes. The word “value” is embedded in both health outcomes and cost, and alternative payment models promote both value and cost efficiency. Organizations take on financial risk to deliver high-quality care at lower costs; he cited accountable care organizations (ACOs) as an example. ACOs are responsible for the health and costs of a predetermined population of patients, and the rewards and penalties for meeting quality and cost metrics are built into the system. This model is very different from the fee-for-service model, which can be described simply as “the more you do, the more money you get.”
Chin listed three principles for the aforementioned payment reform: reward reduction of disparities, provide up-front money for investments in infrastructure (e.g., to address social determinants of health), and implement risk-adjusted payment for the safety net. The rationale for the third principle is that because safety-net clinics and hospitals care for patients with a higher medical and social risk, they would otherwise be penalized for taking care of patients with more challenging health issues, which may cost more.
Chin elaborated on the differences between prospective and retrospective payment models, noting that the latter reward and incentivize reducing disparities and advancing health equity. An example is pay-for-performance, which rewards the outcome rather than providing payment up front (prospective payment). For example, up-front payment may be capitated payments, global budgets, shared savings, or per-member per-month, and he underscored that the basic framework is that the money is available for various uses, which could include addressing social determinants of health, providing the infrastructure and workforce (e.g., community health workers, information technology systems to track equity metrics) for interventions.
Chin raised a series of questions to ask about payment. First, what is being incentivized (or at financial risk)? The most powerful systems are the ones where the total costs of care are at risk. If a health system is responsible for the total cost of care for a given geographic population, it is incentivized to invest in addressing the social determinants of health to keep people healthy and out of the hospital. A related question is the magnitude of the incentive or financial risk. A third question is what patients and populations the health system is responsible for. A fourth is about the appropriate payment targets to advance health equity such as reaching a particular benchmark of achievement, attaining a certain level of improvement in a given metric, or reducing disparities based on a predetermined measure of success. It gets more complicated when one begins to examine alternative payment models, which entail more complicated frameworks. However, these frameworks boil down to the three principles of payment system, payment structures, and process for measuring and rewarding performance.
Chin shared a series of examples of alternative payment models. The first is the Center for Medicare & Medicaid Services (CMS) ACO realizing equity, access, and community health model, which developed a health equity plan that identified disparities in patient outcomes and identified specific actions to mitigate those disparities. This model is a redesign of the CMS Global and Professional Direct Contracting Model in response to new government priorities, which include a commitment to advancing health equity, stakeholder feedback, and participant experience. The purpose is to improve health care for people with Medicare through “better care coordination, reaching and connecting health care providers and beneficiaries, including those beneficiaries who are underserved.”7 They needed to adjust certain health equity benchmarks to better support care delivery and coordination for those in underserved communities, which has required collecting beneficiary-reported demographic and social needs data.
Chin cited another example of alternative payment models, state Medicaid plans, explaining that each state has contracting arrangements with Medicaid managed care organizations. Oregon is the most advanced state, as it is on version 2.0 of what it calls a “coordinated care organization” (McConnell, 2016). This is essentially a network of ACOs with risk-adjusted global budgets and bonuses for meeting performance metrics. Health-related services include flexible services, such as community benefit initiatives, that address social determinants of health, which could include food insecurity. Screening for social determinants is an incentive metric, with requirements to invest in social determinants of health and equity and increase community investment. With this financial flexibility and incentive structure, Oregon has found that more money is spent on health-related services for community benefit (e.g., housing, food security, community capacity building) than the traditional services for individual benefit. Challenges include burdensome reporting and lack of adequate data systems for tracking, measuring, and linking health and social needs, referrals, and feedback.
Chin cited Minnesota’s Medicaid plans, which require formal, sustainable partnerships between health care organizations and CBOs, such as food banks. The state’s plans have focused on screening, referral, eligibility, assessment, service delivery, and coordination in linking social needs and health care (Martinson et al., 2006). In Massachusetts, contracts are required between ACOs and CBOs. The state assesses health-related social needs of the enrolled population, the available community resources, and gaps in community services (Kaye, 2021). Payment is adjusted for social risk, with incentives to address social determinants via partnerships with CBOs and flexible services. He raised two challenges of linking clinical and
___________________
7https://innovation.cms.gov/innovation-models/aco-reach (accessed September 14, 2022).
community sectors: a fear of health care stakeholders using their muscle in non-health-care spaces (where he suggested they are better suited as partners) and the difficulty of aligning incentives and implementing common metrics across sectors such as housing, criminal justice, and health care.
Local initiatives to improve population health and advance equity through partnerships with community organizations must be viewed within the context of the wider policy challenges, Chin advised, which involve overall health care financing policies and global payment models.
He ended with a quote about caring for diverse populations in current society: “Clinicians must have self-insight and true understanding of heterogeneous patients, knowledge of evidence-based interventions, ability to adapt messaging and approaches, and facility with systems change and advocacy. Advancing health equity requires both science and art; evidence-based roadmaps and stories that guide the journey to better outcomes; judgment that informs how to change the behavior of patients, providers, communities, organizations, and policy makers; and passion and a moral mission to serve humanity” (Chin, 2021).
THE BIG PICTURE AND NEW LEGISLATION
Bob Blancato, Defeat Malnutrition Today coalition, maintained that, in light of the clear connections between dietary intake and health, a focus on older adult nutrition is needed to help achieve healthier aging. He urged a congressional and regulatory focus on what he called the “triple threat” to older adult health: hunger, food insecurity, and malnutrition. The Defeat Malnutrition Today coalition comprises more than 100 organizations and stakeholders that recognize that malnutrition is a key indicator and vital sign of older adult health.
Recent legislation for older adult nutrition has been dominated by responses to the COVID-19 pandemic, such as four emergency funding bills passed by Congress between March 2020 and March 2021; $1.6 billion was provided for OAA as the program underwent its biggest conversion in its 50-year history. One indicator of this conversion is that before the pandemic, 66 percent of older adults served received meals in congregate settings. By the first month of the pandemic, more than 90 percent of them were receiving home-bound or grab-and-go meals, leading to major increases in demand and cost (Blancato and Whitmire, 2021). The emergency funding bills helped address this situation, particularly given rising costs of food and gas, both of which are central to older adult food programs. The bills also supported other nutrition programs that serve older adults, such as SNAP and the Commodity Supplemental Food Program.
Blancato discussed new legislation that will provide funding for fiscal year (FY) 2023 (which begins October 1, 2022, for the federal government).
He noted that the funds included in the emergency spending bills passed for FY 2022 were intended to last through the end of the COVID-19 public health emergency but may run out sooner, and any significant funding reduction levels will lead to a “service cliff” in nutrition programs for older adults nationwide, whereby recipients would lose access to meals. Therefore, a legislative focus is funding for FY 2023 and advocacy groups (e.g., Meals on Wheels America, National Association of Nutrition and Aging Services Programs) are seeking doubled funding for OAA nutrition programs. Funding and increasing accessibility of nutrition programs is key, especially when it comes to directing older adults to programs to which they are entitled. Despite progress in this area, eligible older adults have low SNAP participation; only 42 percent of them participate, compared to 82 percent of eligible persons in the general population (Gray and Cunnyngham, 2016).
Blancato highlighted that advocacy groups are also seeking increased flexibility in meal programs. The pandemic funding increased reimbursement and flexibility for the OAA Congregate Meal Program, but it follows firm guidelines, including low reimbursement rates, strictly balanced meals (i.e., little flexibility to accommodate different dietary preferences, such as vegetarian or kosher), providing only one-third of daily meal requirements (although this stipulation was waived with the emergency pandemic funding), prohibiting food to leave the room, and restricting innovation of the congregate meal space. Increasing flexibility in these areas can increase accessibility of congregate programs as they reopen. Examples of such flexibilities include evaluating and increasing reimbursement rates more frequently, increasing options for meals to fit special dietary needs and/or accommodate specific preferences (e.g., cultural preferences), adding options for additional servings or take-home meals, modernizing meal spaces and meal options, and making grab-and-go options permanent.
Blancato mentioned the relationships between nutrition and other issues that affect older adults: falls, mental health, and elder abuse. Malnutrition and low body weight are significant risk factors for falls, and rates of depression among older adults increase with age. One-quarter of adults 65 years and older are considered to be socially isolated, which increases the risk of premature death more than smoking, obesity, and inactivity. Social isolation also increases risk of elder abuse, especially self-neglect and financial abuse (NASEM, 2020). The OAA nutrition programs are more than just a meal—they are a source of social and community connection; provide screenings that can help identify malnutrition, food insecurity, fall risk, isolation, and mental health issues; and promote evidence-based disease prevention and health promotion programs to help improve health and well-being and reduce disease and injury.
Blancato discussed regulatory developments that relate to older adult nutrition. A major opportunity to improve care for malnourished older
adults in hospitals is the Global Malnutrition Composite Score,8 a quality measure that was included in the proposed rule for the CMS Inpatient Prospective Payment System and endorsed by the National Quality Forum. The measure calculates the average of the performance scores of four components of the electronic quality measure for people 65 and older: malnutrition screening, nutrition assessment for risk of malnutrition, appropriate malnutrition diagnosis, and nutrition care plan documentation in the medical record for malnourished individuals. To illustrate how this measure would benefit both older adults and hospitals, Blancato reported that malnutrition is estimated to affect more than 30 percent of hospitalized adults but diagnosed in only 9 percent (Barker et al., 2011). Malnourished patients experience poor health outcomes and burden the health care system with higher hospitalization costs, higher readmission rates, and longer average length of stay (Barker et al., 2011), which is why advocates for older adult nutrition want the Global Malnutrition Composite Score quality measure to be included in the final rule.
Blancato circled back to the White House Conference on Hunger, Nutrition, and Health. According to the legislation that paved the way for the conference (H.R.5724), its purpose is to develop a road map to end hunger and improve nutrition by 2030 and to review existing and cross-departmental strategies and consider new approaches to improve health by eliminating hunger, reducing prevalence of chronic diseases, and improving access to and consumption of nutritious foods in accordance with the Dietary Guidelines for Americans. Blancato added that the 2025–2030 edition of the guidelines is anticipated to include a focus on nutritional guidance for older adults (GAO, 2019), and he hoped that the conference will give adequate attention to older adults’ unique nutrition needs and dietary assessment considerations. He recalled that based on his experience as a participant in four White House conferences on aging, they can produce recommendations that become the basis for new legislation.
Blancato also touched on Senate bill 1536, the Medical Nutrition Therapy Act of 2021. It would expand the conditions eligible for medical nutrition therapy coverage under Medicare (which covers diabetes and renal disease only) and therefore expand access for more patients to see a registered dietitian to receive medical nutrition therapy counseling. The bill was included in a major House of Representatives bill (H.R.7585) introduced at the end of April 2022 (Health Equity and Accountability Act of 2022).
Blancato asserted that access to nutrition is a public health issue and called for national and state public health goals to address malnutrition,
___________________
8https://www.eatrightpro.org/practice/quality-management/quality-initiatives/global-malnutrition-composite-score (accessed September 14, 2022).
particularly for older adults. Such goals should be part of Healthy People 2030 and be included in year-to-year state plans under OAA. An expanded evidence base on older adult nutrition needs is also needed, along with increased NIH funding for such research, especially evidence on malnutrition’s effect on health equity and health outcomes.
Blancato shifted to nutrition security and promotion of nutrition through the life span. In a 2021 JAMA Viewpoint article, nutrition security was defined as having “consistent access, availability, and affordability of foods and beverages that promote well-being and prevent (and if needed, treat) disease” (Mozaffarian et al., 2021). The article suggested that prioritizing nutrition security could address a gap in clinical and public health screening tools for food insecurity: a lack of assessment of diet quality or nutrition. It added that “[i]n recognition of the rapid increase in the prevalence of several diet-related diseases and longstanding racial disparities in access to nutritional foods and diet conditions, it is time to embrace the concept of nutrition security.” Blancato endorsed this statement, adding that food deserts are an example of the kind of disparity in food access that should be eliminated. In terms of nutrition throughout the life course, access to and affordability of nutrition solutions is important for all generations. One solution is to change pricing policies so that nutrient-dense foods are less expensive relative to nutrient-poor foods, and another is to promote nutrition education during childhood and adolescence, given that many chronic conditions in older adults can be prevented with proper nutrition earlier in life.
Blancato emphasized that sound nutrition is vital for physical and mental health, and he urged a focus on policies that neither reward nor subsidize poor nutrition but instead promote the availability, accessibility, and affordability of nutrient-dense foods.
PANEL DISCUSSION WITH SPEAKERS
The four speakers answered questions from the workshop’s planning committee members and attendees about topics that included connecting the dots between health care and community services; meeting the nutrition needs of frail, older adults; legislation and funding mechanisms to address the needs of the oldest old; and key takeaways for health care providers.
Connecting the Dots Between Health Care and Community Services
Chin responded to a question about how to close the loops of screening for health and social needs in health care and community settings. A goal for health care is to be able to refer patients to CBOs that can address social
needs identified in the health care setting. To be successful, health care needs to have a database of relevant community partners and a feedback loop by which the provider could be informed of whether the patient acted on the referral to the CBO. This has been a challenge in practice, although regional demonstration projects have been undertaken and are being evaluated. Despite a lot to learn about how to do this well, Chin said that it is a step in the right direction of coordinated care systems and care transformations that lead to better outcomes.
Blancato shared his observation that private equity firms have inserted themselves into the traditional information and referral space, which is a problem when they bypass existing community-based structures (e.g., 2-1-1s) that have been doing referrals for a long time and already have databases and experience. He suggested building better alliances and communication channels between health care and community-based entities. Akobundu agreed and added that it has been a challenge to break out of the siloes that have prevented effective bidirectional communication to document patient needs. She called for incentives for building an infrastructure that enables these clinical and community linkages.
In response to a follow-up question about connecting the dots at the federal level, Blancato indicated that the connections between federally funded health care and community programs are inadequate. Medicare Advantage is moving deeper into nonmedical supplemental services at the community level, including nutrition, which may create an opportunity for closer linkages to programs like Meals on Wheels.
Chin suggested that systems are set up to be relatively siloed, such that health care or any other sector is designed to respond to incentive structures and metrics for rewards and accountability within its own space rather than thinking about what is best for each patient. A challenge of promoting cross-sector collaboration is the need to establish commonly aligned metrics and incentives, which he characterized as a relatively uncharted space but also a “huge frontier” for advancing health equity.
Meeting the Nutrition Needs of Frail Adults of Advanced Age
The Meals on Wheels network takes pride in providing meals that are responsive to its population’s needs, Akobundu said; older adults receive an initial nutrition screening and have access to more in-depth opportunities for evaluation of their lifestyle, religious, medical, and cultural needs. Those needs are met to the extent possible in partnership with the program, so that each individual receives the optimal set of nutrition services. Sometimes programs can also provide assistive devices to support the needs of frail older adults, so they can better manage mealtimes at home.
Legislation and Funding Mechanisms to Address the Needs of the Oldest Old
In response to a question about future legislative opportunities, Blancato said that the Administration for Community Living administers OAA and can instruct what programming is added to state or area plans. If nutrition is lacking in a particular geographic area, that it is the advocate’s job to lobby for greater emphasis on nutrition in future plans.
Chin observed a difference in how funding streams work in emergency versus nonemergency situations. Emergency funds typically use existing mechanisms to funnel money, because it is hard to create a new funding mechanism during an emergency. He suggested that the reason some of the initial CARES Act funding for health care organizations was not necessarily weighted toward the greatest needs or most vulnerable populations was that it had to go through existing channels. Chin suggested that more integrative funding streams could be established to better support the linkages between medical and social needs and facilitate the bidirectional flow of information between these sectors.
Key Takeaways for Health Care Providers
In DiMaria-Ghalili’s view, the take-home message is the importance of training all health care providers across the care continuum to screen older adults for nutrition risk, including during office and home care visits. Screening should also occur at both hospital admission and discharge, and the latter is important for indicating what services a patient might need at home.
Akobundu built on DiMaria-Ghalili’s contribution, commenting that much of health care happens outside of the walls of health care institutions. She urged building a bigger loop of clinical and community partners who can play different roles in intervening, screening, assessing, and transferring information. As an example, she suggested that dentists could ask older adults about their nutrition habits and refer to food and nutrition assistance programs.
According to Harlan, the first step is to make food part of conversations between health care providers and patients. Physicians are trained to conduct physical exams and collect a family medical history, and he posited that a dietary history might be more important than a family medical history. Food conversations can broach the topic of food security by asking where a patient gets food. He shared a web link for a free CME course on food security.
Chin suggested that advocacy is inherent to the work of health care providers, although it may be perceived as taboo by some. Providers can
be advocates in a variety of ways, and those opportunities may vary over time or in one’s professional versus citizen role. This could include working with health care leadership to improve connections between health care and CBOs or writing or speaking to the community about the importance of these connections. Blancato concurred and told health care providers and others with frontline experience—whether at the medical, hospital, or community level—that they are the most authentic advocates.
From Huang’s perspective, the workshop presentations and discussions make it clear that a shift is coming in how people in medicine and policy circles think about the importance of nutrition and dietary assessment in public health. It is a purposeful shift for those who were trained in the medication-oriented model of addressing health, toward more opportunities and funding for educating providers about nutrition and providing nutrition services in the community. DiMaria-Ghalili added that training on social determinants of health is being integrated into health care provider curricula, which is a major shift but one that sets the stage for better equipping providers to address food and nutrition insecurity and malnutrition.
REFERENCES
Adams, K. M., K. C. Lindell, M. Kohlmeier, and S. H. Zeisel. 2006. Status of nutrition education in medical schools. American Journal of Clinical Nutrition 83(4):941S–944S.
Barker, L. A., B. S. Gout, and T. C. Crowe. 2011. Hospital malnutrition: Prevalence, identification and impact on patients and the healthcare system. International Journal of Environmental Research and Public Health 8(2):514–527.
Blancato, R., and M. Whitmire. 2021. The crucial role of federal nutrition programs in promoting health among low-income older adults. Generations 45(2):1–11.
Bradley, E. H., B. R. Elkins, J. Herrin, and B. Elbel. 2011. Health and social services expenditures: Associations with health outcomes. BMJ Quality and Safety 20(10):826–831.
Chin, M. H. 2020. Advancing health equity in patient safety: A reckoning, challenge and opportunity. BMJ Quality and Safety.
Chin, M. H. 2021. New horizons—addressing healthcare disparities in endocrine disease: Bias, science, and patient care. International Journal of Clinical Endocrinology and Metabolism 106(12):e4887–e4902.
Curriculum Committee of the Nutrition Academic Award Program. 2002. Nutrition curriculum guide for training physicians. https://www.nhlbi.nih.gov/sites/default/files/media/docs/NAA%20Nutrition%20Curriculum%20Guide.pdf (accessed September 14, 2022).
de Lorgeril, M., P. Salen, J. L. Martin, I. Monjaud, J. Delaye, and N. Mamelle. 1999. Mediterranean diet, traditional risk factors, and the rate of cardiovascular complications after myocardial infarction: Final report of the Lyon Diet Heart Study. Circulation 99(6):779–785.
Frank, E., J. Breyan, and L. Elon. 2000. Physician disclosure of healthy personal behaviors improves credibility and ability to motivate. Archives of Family Medicine 9(3):287–290.
GAO (United States Government Accountability Office). 2019. Nutrition assistance programs: Agencies could do more to help address the nutritional needs of older adults. GAO.
Gray, K.F. and Cunnyngham, K., 2016. Trends in supplemental nutrition assistance program participation rates: Fiscal year 2010 to fiscal year 2015 (No. 83167c08faee4195a-b0168e9f16dffd5). Mathematica Policy Research.
Kaye, N. 2021. Massachusetts fosters partnerships between Medicaid accountable care and community organizations to improve health outcomes. https://www.nashp.org/massachusetts-fosters-partnerships-between-medicaid-accountable-care-and-community-organizations-to-improve-health-outcomes (accessed August 8, 2022).
Kinderknecht, K., G. Rampersad, J. Romero, and T. Simmons. 2022. Hunger health equity. Health Equity Action League of Feeding America.
Kreuter, M. W., S. G. Chheda, and F. C. Bull. 2000. How does physician advice influence patient behavior? Evidence for a priming effect. Archives of Family Medicine 9(5):426–433.
Kushner, R. F., L. Van Horn, C. L. Rock, M. S. Edwards, C. W. Bales, M. Kohlmeier, and S. R. Akabas. 2014. Nutrition education in medical school: A time of opportunity. The American Journal of Clinical Nutrition 99(5):1167S–1173S.
Leong, B., D. Ren, D. Monlezun, D. Ly, L. Sarris, and T. S. Harlan. 2014. Teaching third and fourth year medical students how to cook: An innovative approach to training students in lifestyle modification for chronic disease management. Medical Science Educator 24(1):43.
Martinson, K., R. Koralek, E. Harbison, and L. Wherry. 2006. Early implementation of the Minnesota Integrated Services Project. Washington, DC: The Urban Institute
McConnell, K. J. 2016. Oregon’s Medicaid coordinated care organizations. JAMA 315(9):869–870.
Mozaffarian, D., S. Y. Angell, T. Lang, and J. A. Rivera. 2018. Role of government policy in nutrition-barriers to and opportunities for healthier eating. BMJ 361:k2426.
Mozaffarian, D., S. Fleischhacker, and J. R. Andres. 2021. Prioritizing nutrition security in the U.S. JAMA 325(16):1605–1606.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2020. Social isolation and loneliness in older adults: Opportunities for the health care system. Washington, DC: The National Academies Press.
National Research Council Committee on Nutrition in Medical Education. 1985. In Nutrition education in U.S. medical schools. Washington, DC: National Academies Press.
Nicklett, E. J., K. E. Johnson, L. M. Troy, M. Vartak, and A. Reiter. 2021. Food access, diet quality, and nutritional status of older adults during COVID-19: A scoping review. Frontiers in Public Health 9:763994.
Pang, B., Z. Memem, C. Diamant, E. Clarke, S. Chou, and H. Gregory. 2019. Culinary medicine and community partnership: Hands-on culinary skills training to empower medical students to provide patient-centered nutrition education. Medical Education Online 24(1):1630238.
Robert Wood Johnson Foundation. 2017. Visualizing health equity: One size does not fit all infographic. https://www.rwjf.org/en/library/infographics/visualizing-health-equity.html (accessed September 14, 2022).
Sacks, F. M., G. A. Bray, V. J. Carey, S. R. Smith, D. H. Ryan, S. D. Anton, K. McManus, C. M. Champagne, L. M. Bishop, N. Laranjo, M. S. Leboff, J. C. Rood, L. de Jonge, F. L. Greenway, C. M. Loria, E. Obarzanek, and D. A. Williamson. 2009. Comparison of weight-loss diets with different compositions of fat, protein, and carbohydrates. New England Journal of Medicine 360(9):859–873.
Smith, D. R. 2008. The historical decline of tobacco smoking among United States physicians: 1949–1984. Tobacco Induced Diseases 4:9.
Stauber, Z., A. C. Razavi, L. Sarris, T. S. Harlan, and D. J. Monlezun. 2022. Multisite medical student-led community culinary medicine classes improve patients’ diets: Machine learning-augmented propensity score-adjusted fixed effects cohort analysis of 1381 subjects. American Journal of Lifestyle Medicine 16(2):214–220.
Trichopoulou, A., T. Costacou, C. Bamia, and D. Trichopoulos. 2003. Adherence to a Mediterranean diet and survival in a Greek population. New England Journal of Medicine 348(26):2599–2608.






















